colorectal cancer stem cell
肿瘤TNM分期

区域淋巴结(N)Nx 区域淋巴结不能评价 PNx 无区域淋巴结取材标本N0 无区域淋巴结转移 pN0 无区域淋巴结转移N1 区域淋巴结转移(一个或多个) pN1 区域淋巴结转移(一个或多个)远处转移(M)Mx 远处转移无法评估M0 无远处转移M1 有远处转移M1a 有区域淋巴结以外的淋巴结转移M1b 骨转移(单发或多发)M1c 其它器官组织转移(伴或不伴骨转移)分期编组I期 T1a N0 M0 G1II期 T1a N0 M0 G2,3-4T1b N0 M0 任何GT1c N0 M0 任何GT1 N0 M0 任何GT2 N0 M0 任何GIII期 T3 N0 M0 任何GIV期 T4 N0 M0 任何G任何T N1 M0 任何G任何T 任何N M1 任何G病理分级GX 病理分级不能评价G1 分化良好(轻度异形)(Gleason 2-4)G2 分化中等(中度异形)(Gleason 5-6)G3-4 分化差或未分化(重度异形)(Gleason 7-10)(四)、前列腺癌危险因素分析根据血清PSA、Gleason 评分和临床分期将前列腺癌分为低、中、高危三类,以便指导治疗和判断预后。
低危中危高危PSA(ng/ml)4~10 10.1~20 >20Gleason 评分≤6 7 >8临床分期≤T2a T2b ≥T2c鼻咽癌TNM分期原发肿瘤TT1 肿瘤局限于鼻咽腔内T2 肿瘤扩展到口咽软组织和或鼻腔T2a 咽旁间隙无侵犯T2b 咽旁间隙有侵犯T3 骨结构和或鼻窦有侵犯T4 肿瘤侵入颅内,和或脑神经、颞下窝、下咽、眼眶受侵区域淋巴结NNX 区域淋巴结无法评价N0 淋巴结无转移N1 单侧淋巴结转移直径≤6cm淋巴结位于锁骨上窝以上部位N2 双侧淋巴结转移直径≤6cm淋巴结位于锁骨上窝以上部位N3 颈淋巴结转移N3a 淋巴结转移直径>6cmN3b 锁骨上窝淋巴结转移远处转移MMX 远处转移无法判断M0 无远处转移M1 有远处转移临床分期Ⅰ期T1N0M0Ⅱa期T2aN0M0Ⅱb期T1N1M0;T2aN1M0;T2bN0M0;T2bN1M0Ⅲ期T1N2M0;T2N2M0;T3N0M0;T3N1M0;T3N2M0Ⅳa期T4N0M0;T4N1M0;T4N2M0Ⅳb期任何TN3M0Ⅳc期任何T任何NM1大肠癌临床分期1、Astler-coller改良Dukes分期Dukes A 期病变局限于粘膜或粘膜下层Dukes B1期病变侵入粘膜肌层Dukes B2期病变侵及肠壁全层或邻近组织,但能完整切除,无淋巴结转移Dukes C1期病变限于肠壁内,伴有淋巴结转移Dukes C2期病变侵及肠壁全层,伴有淋巴结转移Dukes D 期有远处转移或侵及邻近脏器不能完整切除2、我国大肠癌临床分期A期肿瘤局限于肠壁A0期肿瘤局限于粘膜层A1期肿瘤侵及粘膜下层A2期肿瘤侵犯肌层B期肿瘤穿透肠壁,甚至侵及邻近器官组织,但能完整切除C期不论肿瘤局部侵犯范围如何,已有淋巴结转移C1期肿瘤附近淋巴结转移C2期肠系膜淋巴结和或肠系膜血管根部淋巴结转移D期远处脏器转移(肝、肺、肾、脑等)远处淋巴结转移(如锁骨上淋巴结转移)肠系膜淋巴结和或肠系膜血管根部淋巴结转移,无法全部切除者腹膜广泛转移无法切除者肿瘤局部广泛侵润,侵及邻近脏器组织不能完整切除肺癌TNM分期原发肿瘤TTx 原发肿瘤不能评价;痰、支气管冲洗液虽找到癌细胞但影像学或支气管镜没有可视肿瘤T0 没有原发肿瘤证据Tis 原位癌T1 肿瘤直径≤3cm,周围为肺或脏层胸膜包绕,镜下没有累及叶支气管以上1T2 符合以下任何一点:肿瘤最大径>3cm;累及主支气管,但距隆突≥2cm;累及脏层胸膜;扩展到肺门的肺不张或阻塞性肺炎,但不累及全肺T3 任何大小肿瘤直接侵犯下列之一:胸壁(上沟瘤)、膈肌、纵隔、胸膜、心包;肿瘤位于距隆突2cm以内的主支气管但未累及隆突;全肺的肺不张或阻塞性肺炎T4 任何大小肿瘤直接侵犯下列之一:纵隔、心脏、大血管、气管、食管、椎体、隆突;原发肿瘤同一叶内的单个或多个卫星灶;原发肿瘤伴恶性胸水或心包积液2区域淋巴结NNx 区域淋巴结不能评价N0 没有区域淋巴结转移N1 转移至同侧支气管周围淋巴结和或同侧肺门淋巴结;原发肿瘤直接侵及肺门淋巴结N2 转移至同侧纵隔和或隆突下淋巴结N3 转移至对侧纵隔、对侧肺门淋巴结,同侧或对侧斜角肌或锁骨上淋巴结远处转移MMx 远处转移不能评价M0 没有远处转移M1 有远处转移3临床分期隐性癌TxN0M0原位癌TisⅠa T1N0M0Ⅰb T2N0M0Ⅱa T1N1M0Ⅱb T2N1M0;T3N0M0Ⅲa T3N1M0;T1N2M0;T2N2M0;T3N2M0;Ⅲb T4NM0;TN3M0ⅣTNM1说明:1任何大小的表浅肿瘤只要局限于支气管壁,即使累及主支气管也为T1;2胸腔积液为非血性和渗出性的,多次细胞学检查未能找到癌细胞的,判断该胸水与肿瘤无关,不影响分期;3原发肿瘤所在肺叶内出现癌性卫星灶为T4;在其他叶内(包括同侧)出现的癌性结节为M1;心包积液原则上等同于胸腔积液宫颈癌FIGO分期0期原位癌Ⅰ期癌灶局限于宫颈Ⅰa 肉眼未见癌灶,仅显微镜下见肿瘤侵润深度≤5cm宽度≤7cmⅠa1 肿瘤侵润深度≤3cm宽度≤7cmⅠa2 肿瘤侵润深度>3cm但≤5cm,宽度≤7cmⅠb 临床癌灶局限于宫颈,肉眼可见浅表侵润癌或临床前病灶>Ⅰa 期Ⅰb1 临床癌灶体积≤4cm3Ⅰb2 临床癌灶体积>4cm3Ⅱ期癌灶超出宫颈,但未达盆壁;癌累及阴道,但未及阴道下1/3Ⅱa 癌累及阴道为主,无明显宫旁侵润Ⅱb 癌累及宫旁为主,无明显阴道侵润Ⅲ期癌超出宫颈,累及阴道下1/3;宫旁侵润达盆壁,有肾盂积水或肾功能不全Ⅲa 癌累及阴道为主,已达下1/3Ⅲb 癌累及宫旁为主,侵润达盆壁,有肾盂积水或肾功能不全Ⅳ期癌播散超出真骨盆或癌侵润膀胱粘膜及直肠粘膜Ⅳa 癌侵润膀胱粘膜及直肠粘膜Ⅳb 癌播散超出真骨盆,有远处转移卵巢恶性肿瘤分期Ⅰ期肿瘤局限于卵巢Ⅰa 肿瘤局限于一侧卵巢,包膜完整,表面无肿瘤,无腹水Ⅰb 肿瘤局限于两侧卵巢,包膜完整,表面无肿瘤,无腹水Ⅰc Ⅰa或Ⅰb期,但卵巢表面有肿瘤,或包膜破裂,或腹水含恶性细胞,或腹腔冲洗液阳性Ⅱ期一侧或两侧卵巢肿瘤,伴盆腔内播散Ⅱa 蔓延或种植到子宫和或输卵管Ⅱb 蔓延到其他盆腔组织Ⅱc Ⅱa或Ⅱb期,但卵巢表面有肿瘤,或包膜破裂,或腹水含恶性细胞,或腹腔冲洗液阳性Ⅲ期一侧或两侧卵巢肿瘤,盆腔外有腹膜种植或腹膜后或腹股沟淋巴结阳性,仅肝表面转移者定为Ⅲ期Ⅲa 肉眼见肿瘤局限于真骨盆,淋巴结阴性,但组织学证实腹膜表面有显微镜下种植Ⅲb 一侧或两侧卵巢肿瘤,组织学证实腹膜表面种植,直径≤2cm,淋巴结阴性Ⅲc 腹膜种植直径>2cm,或腹膜后或腹股沟淋巴结阳性Ⅳ期一侧或两侧卵巢肿瘤,有远处转移。
黏蛋白型O-糖基化与结直肠癌基础和临床研究进展
·综述·黏蛋白型O⁃糖基化与结直肠癌基础和临床研究进展汪泽慧张军*南京医科大学附属南京医院消化内科(210006)摘要O⁃糖基化为黏蛋白常见的翻译后修饰,普遍存在于正常细胞和肿瘤细胞中。
结直肠癌(CRC )细胞内O⁃糖基化相关的糖基转移酶、分子伴侣和表面的Tn 抗原、sTn 抗原、T 抗原出现不同程度的失调,且以其特有方式参与CRC 的发生、发展,包括侵袭和转移、异常凋亡和增殖、免疫逃逸等,并作为新型肿瘤生物学标志物和潜在治疗靶点被广泛研究。
本文就黏蛋白型O⁃糖基化与CRC 的发生、发展及其临床应用的研究进展作一综述。
关键词黏蛋白型O⁃糖基化;结直肠肿瘤;糖基转移酶类;sTn 抗原Progress of Basic and Clinical Research on Mucin ⁃type O ⁃Glycosylation and Colorectal Cancer WANG Zehui,ZHANG Jun.Department of Gastroenterology,Nanjing Hospital Affiliated to Nanjing Medical University,Nanjing (210006)Correspondence to:ZHANG Jun,Email:**********************AbstractO⁃glycosylation is a common post⁃translational modification of mucins,widely present in both normal andtumor cells.In colorectal cancer (CRC)cells,there is a varying degree of dysregulation in O ⁃glycosylation ⁃relatedglycosyltransferases,molecular chaperones,and surface Tn antigen,sTn antigen,and T antigen.These dysregulations playa distinctive role in the occurrence and development of CRC,including invasion and metastasis,abnormal apoptosis and proliferation,immune escape,etc.They are extensively studied as novel tumor biomarkers and potential therapeutic targets.This article provides a comprehensive review of progress of research on mucin⁃type O⁃glycosylation and its relevance to the occurrence and development of CRC and its clinical application.Key wordsMucin⁃Type O⁃Glycosylation;Colorectal Neoplasms;Glycosyltransferases;sTn AntigenDOI :10.3969/j.issn.1008⁃7125.2023.03.005*本文通信作者,Email:**********************O⁃糖基化是指丝氨酸/苏氨酸/酪氨酸的羟基共价连接碳水化合物残基的过程,根据初始聚糖的不同,可进一步细分为O ⁃连接α⁃N ⁃乙酰半乳糖胺(N ⁃acetylgalactosamine,GalNAc )和O⁃连接β⁃N⁃乙酰氨基葡萄糖。
三药化疗联合靶向治疗在转移性结直肠癌的临床研究进展

一线治疗的发展历程
1.1 F0 LF0 X 旧丨在m C R C 治疗中的首次亮相 2 0 0 2 年 意 大 利 Falcone教 授 团 队 在 Journal of
Clinical Oncology (JC0 ) 发表 F0 LF0 XIRI 三药双周 化 疗 治 疗 mCRC的 初步研究结果[9],这 是 F0 LF0X IRI三 药 化 疗 方 案 首 次 登 上 历 史 舞 台 。该 研 究 是 一 项 II期临床研究,目的为探究F0 LF0 XIRI三药化 疗抗肿瘤治疗的疗效、安 全 性和药物剂量。试验共 入 组 4 2 名 患 者 ,有 5 例 患 者 (11.9 % ) 治疗后达到 完 全 缓 解 ( complete remission, CR ) ,25 例 患 者 (59. 5 % )部 分 缓 解 ( partial remission,PR) ,客观有 效 率 ( overall response rate,0 RR) 为 71. 4 % ( 9 5 % C/:47% ~ 83% ) , 中 位 无 进 展 生 存 期 ( median progression free survival,mPFS)为 10. 4 个 月 ,中位总生 存 期 ( median overall survival,mOS)达到 26. 5 个 月 。 主要毒副反应包括腹泻和粒细胞缺乏,2 1 % 患者出 现 3 级腹泻,55%患者出现4 级中性粒细胞减少。
[收稿曰期] [基金项目] [通讯作者]
2〇2〇]2-〇2 [ 修 回 曰 期 ] 2〇2丨-〇3-〇5 •国家重点研发计划(编号:2〇l6YFCl3〇3602) 么金永东,E-mail:cccjin@ 163. com
结直肠癌干细胞研究进展

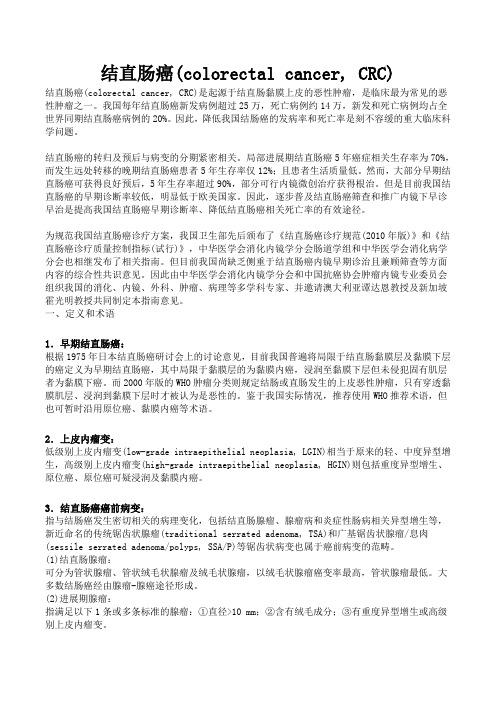
结直肠癌⼲细胞研究进展wcjd@/doc/10f17e13a2161479171128d5.html⽂献综述 REVIEW结直肠癌⼲细胞研究进展杨治⼒, 王志刚, 郑起杨治⼒, 王志刚, 郑起,上海交通⼤学附属第六⼈民医院外科上海市 200233作者贡献分布: 本⽂综述由杨治⼒与王志刚完成, 郑起审校.通讯作者: 郑起, 教授, 200233, 上海市, 上海交通⼤学附属第六⼈民医院外科.zhengqi1957@/doc/10f17e13a2161479171128d5.html收稿⽇期: 2009-12-16 修回⽇期: 2010-01-09接受⽇期: 2010-01-26 在线出版⽇期: 2010-03-28Advances in research on colorectal cancer stem cells Zhi-Li Yang, Zhi-Gang Wang, Qi ZhengZhi-Li Yang, Zhi-Gang Wang, Qi Zheng,Department of Surgery, Shanghai Sixth People's Hospital Affiliated to Shanghai Jiao Tong University, Shanghai 200233, China Correspondence to:Professor Qi Zheng, Shanghai Sixth People's Hospital Affiliated to Shanghai Jiao Tong Univer-sity, Shanghai 200233, China.zhengqi1957@/doc/10f17e13a2161479171128d5.html Received: 2009-12-16 Revised: 2010-01-09 Accepted: 2010-01-26 Published online: 2010-03-28AbstractColorectal cancer is a worldwide enormous cancer burden and a major therapeutic chal-lenge as other solid tumors. The cancer stem cell hypothesis provides a cellular mechanism to account for the development, progression, recurrence and metastasis of colorectal can-cer. The aim of this paper is to review the ad-vances in research on colorectal cancer stem cells.Key Words: Colorectal cancer; Cancer; Stem cellYang ZL, Wang ZG, Zheng Q. Advances in research on colorectal cancer stem cells. Shijie Huaren Xiaohua Zazhi 2010;18(9): 913-919摘要结直肠癌与其他实体肿瘤⼀样是我国乃⾄世界范围的重要疾病负担, 其治疗也⾯临许多挑战. 近⼏年, ⽇益受到重视的癌症⼲细胞理论似乎可以解释结直肠癌的发⽣发展、复发转移的细胞学机制. 本⽂就结直肠癌⼲细胞的研究进展作⼀综述.关键词: 结直肠癌; 癌症; ⼲细胞杨治⼒, 王志刚, 郑起. 结直肠癌⼲细胞研究进展. 世界华⼈消化杂志 2010; 18(9): 913-919 /doc/10f17e13a2161479171128d5.html/1009-3079/18/913.asp0 引⾔结直肠癌与其他实体肿瘤⼀样是我国乃⾄世界范围的重要疾病负担, 其治疗也⾯临许多挑战. 近⼏年, ⽇益受到重视的癌症⼲细胞(cancer stem cell, CSC)理论似乎可以解释结直肠癌的发⽣发展、复发转移的细胞学机制, 可能为改进结直肠癌的治疗策略提供理论依据, 从⽽改善结直肠癌患者的预后.1 CSC理论的提出与初步证据同⼀组织的恶性肿瘤存在不同的病理学分类, 且表达不同的⽣物标志. 随着基因芯⽚与蛋⽩组学技术的进展, 对同⼀组织的恶性肿瘤分类已达到分⼦⽔平. 这些肿瘤⽣物学现象可以理解为不同亚型的肿瘤起源于不同的细胞. 然⽽, 同⼀细胞来源的肿瘤经常显⽰出细胞在功能上的异质性(functional heterogeneity), 表现为不同的增殖与分化能⼒[1,2]. ⽬前, 能解释此现象的CSC模型(图1)越来越被⼤多数学者所接受. CSC是指具有⾃我更新及产⽣组成肿瘤不同细胞能⼒的肿瘤细胞亚群[3-5]. 这些细胞显⽰出⼲细胞样特性与持续维持致瘤的能⼒. Lapi d ot等对急性粒系⽩⾎病细胞的研究⾸次证实CSC的存在[6]: ⼤约占⽩⾎病细胞总数的0.01%-1%的细胞移植⼊免疫缺陷⼩⿏后能诱导形成⽩⾎病. 尤其值得关注的是在实体肿瘤中也被证实CSC的存在. Al-Hajj 等从乳腺癌组织中分离出CD44+CD24-/low的细胞亚群, 并发现他们具有起始肿瘤的能⼒[7]. Singh等利⽤CD133作为分选标志分离并鉴定出脑肿瘤中的CSC[8]. 此后, ⽇益增加的证据显⽰⼏乎所有的实体肿瘤包括结肠、肝[9]、胰[10]、前列腺[11]、卵巢[12]、肺[13]、⿊⾊素瘤[14]等都被特有的CSC亚群按等级组织与维持. ⾄今, 乳腺癌与脑恶性肿瘤的CSC研究更为深⼊. 已有证据显⽰CSC的⽣物学⾏为随/doc/10f17e13a2161479171128d5.html ?■背景资料近⼏年,⽇益受到重视的癌症⼲细胞(C S C)理论似乎可以解释结直肠癌的发⽣发展、复发转移的细胞学机制, 可能为改进结直肠癌的治疗策略提供理论依据, 从⽽改善结直肠癌患者的预后.■同⾏评议者王晓艳, 副教授,湖南长沙中南⼤学湘雅三医院消化内科; 朴云峰,教授,吉林⼤学第⼀临床医院消化科整个肿瘤⽣长进展或经受临床⼲预过程⽽变化(图2), Barabe 等[15]研究显⽰⽩⾎病⼲细胞具有随时间积累⽽出现进化潜能, 表现为从最初细胞类型到含有重分配的免疫球蛋⽩H 基因, 这⼀研究提⽰CSC 本⾝可能出现克隆进化(clonal evolution); Clark 等[16]报道肿瘤细胞体内系列移植可产⽣更多的侵袭性肿瘤; Creighton 等[17]对经历常规内分泌与化学治疗后残余乳腺癌的研究显⽰其中CD44+CD24-/low 表型的CSCs 出现更多间质标志基因表达. 这些研究报道均提⽰CSCs受其所处⼩境(niche)的影响可能出现⽣物学特性的变化.2 结直肠癌⼲细胞存在的实验证据⾸次报道结直肠癌⼲细胞存在的两个研究⼩组是O'Brien 等[18]与Ricci-Vitiani 等[19], 前者在17例原发与转移结肠癌组织中⽤FACS 分析显⽰原发结肠癌组织中CD133+细胞占7.5%-15.9%, 转移结肠癌中CD133+细胞占3.2%-24.5%, 分选出CD133+与CD133-细胞后, 分别植⼊NOD/SCID⼩⿏肾囊内鉴定肿瘤起始细胞(colon cancer-initiating cell, CC-IC), 结果显⽰262个CD133+肿瘤细胞中有1个CC-IC; 后者的19例结肠癌组织中有16例含有C D133+细胞, 约占总细胞的0.7%-6.1%, 另3例未检出CD133+细胞, 通过体内外实验显⽰⼀⼩群未分化的C D133+细胞⽪下植⼊NOD/SCID ⼩⿏能产⽣与⽗代相似的结肠癌. 随后, To d aro 等[20]报道在21例结肠癌组织中CD133表达为0.3%-3%, 裸⿏⽪下移植结果显⽰2×106 CD133-细胞在15 wk 的观察期间⽆肿瘤⽣长, ⽽2.5×103 CD133+细胞⽣成肿瘤体积在1.5 cm 3左右; 进⼀步分析显⽰CD133+细胞能通过⾃分泌IL-4保护这些细胞免于凋亡以及抵抗常规治疗. ⾄此, CD133作为结直肠CSC 的标志已被⼤多数学者所认可.除了C D133作为结直肠C S C 的标志外,CD44与结直肠CSC 的研究也有报道. Dalerba等[21]对⼈类结肠C S C s 的表型研究显⽰:(EpCAM)high /CD44+表型的结肠癌细胞为CSC,914 ISSN 1009-3079 CN 14-1260/R 世界华⼈消化杂志 2010年3⽉28⽇第18卷第9期同时对此表型的细胞表⾯标志谱分析发现CD166也能作为CSC 的表型; 此外, 作者还发现CD44+细胞代表了CD133+细胞群中的⼩部分亚群细胞. 即与CD133+结肠癌细胞⽐较, CD44+结肠癌细胞中更有效地富集了CSCs. Du 等[22]利⽤慢病毒R N A ⼲扰技术敲出结直肠癌细胞中的CD44或CD133基因后显⽰: 仅CD44基因敲出能明显阻⽌癌细胞克隆形成以及抑制移植模型中细胞的致瘤性. 该研究提⽰CD44在结直肠CSC 中具有很重要的功能意义. 为了验证再⽣⼀个异质性结直肠癌的能⼒是否存在于⼀个单克隆结直肠癌细胞群体或依靠多个不同的CSCs, 也即按⽬前研究所定义的单个结直肠C S C 是否确实具有多向分化潜能. Vermeulen 等[23]对原发与肝转移结直肠癌细胞⾏结肠球培养, 这些球能在免疫缺陷⼩⿏中成瘤, 从球分离成单个癌细胞培养结果显⽰20个细胞中⼤约有1个细胞能形成克隆, 同时在球培养中⼤约16个CD133+细胞中有1个细胞能形成球, ⽽CD133-细胞需250个中有1个细胞能形成球; 在与CD133共表达的标志如CD44、CD166、CD24、CD29中, 以CD133+CD24+细胞有更⾼的克隆形成能⼒(约20%); 通过对单细胞克隆的结肠CSCs 的体内外研究显⽰CSCs 具有多向分化潜能, PI3K 信号通路参与了CSCs 分化的决定. 该研究⽀持了拥有多向分化潜能的CSC 导致了组成肿瘤的细胞层级的假说. 为了解决单⽤免疫⽅法检测C D133表达的不确定性, Shmelkov 等[24]建⽴了在CD133基因的启动区域敲进报道基因lacZ 的遗传⼩⿏模型, 结果发现CD133⼴泛表达在成年⼩⿏结肠上⽪细胞;⽤CD133抗体检测成年⼈正常结肠上⽪显⽰其表达在绝⼤多数分化的上⽪细胞; 在原发的⼈结肠癌标本中免疫染⾊也显⽰CD133⼴泛表达在所有恶性上⽪细胞中; 随后的Il10-//doc/10f17e13a2161479171128d5.html CSC克隆进化CSC2图 1 CSC模型.图 2 CSC⽣物学特征的变化.■研发前沿⽬前所有的结直肠CSC 的研究, 尽管在分选标志上的差异, 甚⾄有⽭盾的结果, 但仍可认为在结直肠癌中存在⼲细胞样的细胞亚群, 其特异性细胞表型还需深⼊研究.⼀、⾷道癌早期症状1.咽下梗噎感最多见,可⾃⾏消失和复发,不影响进⾷。
黑色素瘤免疫组化诊断标准

黑色素瘤免疫组化诊断标准
一、肿瘤细胞免疫表型
1.黑色素瘤细胞通常表达HMB45、S100、Melan-A、tyrosinase 等黑色素细胞特异性抗原。
这些抗原有助于明确肿瘤细胞的身份。
2.肿瘤细胞也可能表达vimentin等中间丝蛋白,但并不特异。
3.通常,肿瘤细胞不表达或者仅低表达p63、p75NTR、INI1等基底细胞和神经外胚层抗原。
二、细胞增殖活性
1.Ki-67是一种反映细胞增殖活性的标记物,高表达的Ki-67提示肿瘤细胞增殖活跃,恶性程度较高。
2.PCNA(增殖细胞核抗原)也是反映细胞增殖活性的标记物,可以在黑色素瘤中表达。
三、细胞凋亡
1.黑色素瘤细胞的凋亡情况可以通过TUNEL等检测方法进行评估。
高凋亡率可能提示肿瘤细胞的自我清除能力较强,预后可能较好。
2.Bcl-2、Bcl-xL等抗凋亡蛋白可能在黑色素瘤中表达,这些蛋白的表达情况可以影响肿瘤细胞的生存能力和对治疗的反应。
四、血管生成
1.血管生成是肿瘤生长和转移的重要过程,可以通过CD31、CD34等标记物检测血管生成情况。
高血管生成可能提示肿瘤生长迅速,预后较差。
2.VEGF(血管内皮生长因子)可能在黑色素瘤中表达,是促进血
管生成的重要因子。
其表达情况可能影响肿瘤的生长和转移能力。
总结:在黑色素瘤的免疫组化诊断中,我们通过检测肿瘤细胞的免疫表型、细胞增殖活性、细胞凋亡和血管生成等情况,可以更全面地了解肿瘤的生物学特性,为疾病的诊断、治疗和预后评估提供重要依据。
结直肠癌(colorectal cancer, CRC)
结直肠癌(colorectal cancer, CRC)结直肠癌(colorectal cancer, CRC)是起源于结直肠黏膜上皮的恶性肿瘤,是临床最为常见的恶性肿瘤之一。
我国每年结直肠癌新发病例超过25万,死亡病例约14万,新发和死亡病例均占全世界同期结直肠癌病例的20%。
因此,降低我国结肠癌的发病率和死亡率是刻不容缓的重大临床科学问题。
结直肠癌的转归及预后与病变的分期紧密相关。
局部进展期结直肠癌5年癌症相关生存率为70%,而发生远处转移的晚期结直肠癌患者5年生存率仅12%;且患者生活质量低。
然而,大部分早期结直肠癌可获得良好预后,5年生存率超过90%,部分可行内镜微创治疗获得根治。
但是目前我国结直肠癌的早期诊断率较低,明显低于欧美国家。
因此,逐步普及结直肠癌筛查和推广内镜下早诊早治是提高我国结直肠癌早期诊断率、降低结直肠癌相关死亡率的有效途径。
为规范我国结直肠癌诊疗方案,我国卫生部先后颁布了《结直肠癌诊疗规范(2010年版)》和《结直肠癌诊疗质量控制指标(试行)》,中华医学会消化内镜学分会肠道学组和中华医学会消化病学分会也相继发布了相关指南。
但目前我国尚缺乏侧重于结直肠癌内镜早期诊治且兼顾筛查等方面内容的综合性共识意见。
因此由中华医学会消化内镜学分会和中国抗癌协会肿瘤内镜专业委员会组织我国的消化、内镜、外科、肿瘤、病理等多学科专家、并邀请澳大利亚谭达恩教授及新加坡霍光明教授共同制定本指南意见。
一、定义和术语1.早期结直肠癌:根据1975年日本结直肠癌研讨会上的讨论意见,目前我国普遍将局限于结直肠黏膜层及黏膜下层的癌定义为早期结直肠癌,其中局限于黏膜层的为黏膜内癌,浸润至黏膜下层但未侵犯固有肌层者为黏膜下癌。
而2000年版的WHO肿瘤分类则规定结肠或直肠发生的上皮恶性肿瘤,只有穿透黏膜肌层、浸润到黏膜下层时才被认为是恶性的。
鉴于我国实际情况,推荐使用WHO推荐术语,但也可暂时沿用原位癌、黏膜内癌等术语。
A Living Biobank of Breast Cancer Organoids Captures Disease Heterogeneity

http://hub4organoids.eu/organoid-technology/
The Living Biobank consists of a rapidly growing collection of organoids from patients with various forms of cancer (colon, prostrate, lung, pancreas) and cystic fibrosis. The organoids are characterized by genome sequencing, expression profiling and sensitivity to known drugs to establish a database linking genetic and transcriptional information to drug responsiveness.
Method of the year 2017
Overview of organoid methodologies
Therapeutic potential of organoids
Madeline A. Lancaster, et, al. Science, 2014. Organogenesis in a dish.
4.
5.
Figure 1. Establishing a Biobank of BC Organoids
Figure 2. Histology and Receptor Status of BC Organoids
In summary, we found that the majority of BC organoids matches the originating BC with respect to histopathology as well as hormone and HER2 receptor status.
Cell Death and Differentiation (2008)

ReviewCancer stem cells –old concepts,new insightsL Vermeulen 1,MR Sprick 1,K Kemper 1,G Stassi 2and JP Medema*,1Cancer has long been viewed as an exclusively genetic disorder.The model of carcinogenesis,postulated by Nowell and Vogelstein,describes the formation of a tumor by the sequential accumulation of mutations in oncogenes and tumor suppressor genes.In this model,tumors are thought to consist of a heterogeneous population of cells that continue to acquire new mutations,resulting in a highly dynamic process,with clones that out compete others due to increased proliferative or survival capacity.However,novel insights in cancer stem cell research suggest another layer of complexity in the process of malignant transformation and preservation.It has been reported that only a small fraction of the cancer cells in a malignancy have the capacity to propagate the tumor upon transplantation into immuno-compromised mice.Those cells are termed ‘cancer stem cells’(CSC)and can be selected based on the expression of cell surface markers associated with immature cell types.In this review,we will critically discuss these novel insights in CSC-related research.Where possible we integrate these results within the genetic model of cancer and illustrate that the CSC model can be considered an extension of the classic genetic model rather than a contradictory theory.Finally,we discuss some of the most controversial issues in this field.Cell Death and Differentiation (2008)15,947–958;doi:10.1038/cdd.2008.20;published online 15February 2008The idea that a cancer is constituted of a heterogeneous population of cells differing in morphology,marker expression,proliferation capacity and tumorigenicity has been around for over a century.1–3It is widely accepted that this heterogeneity can be explained by genetic and micro-environmental differences,together with the differentiation grade of indivi-dual cells.4However,the hypothesis that this occurs due tothe fact that a tumor is hierarchically organized,with its own stem cell compartment called the cancer stem cells (CSC),is to this point highly controversial.5,6Although the cancer stem cell model is an old idea,serious attempts to gain insight in its nature only began in the 1970’s.7The development of technical tools such as immunofluorescent flow cytometry revived research into the CSC theory,starting with malig-nancies of the hematopoietic system and later solid tumors.‘Cancer Stem Cells’In the cancer stem cell model malignancies are viewed as abnormal organs with a stem cell compartment that drives the growth.(Figure 1)Cancer stem cells have been defined in analogy to normal stem cells,as cells that have the capacity to (1)self-renew,meaning undergo divisions that allow the generation of more CSCs and (2)give rise to the variety of differentiated cells found in the malignancy.8To date,the practical translation of this definition,and the gold standard forshowing ‘stemness’of cancer cells,is the ability to generate a phenocopy of the original malignancy in immuno-compro-mised mice.This experiment demonstrates the ability of specific cells to generate the variety of differentiated cells present within the original tumor.In addition,the xenotrans-planted tumor must be serially transplanted into new recipient mice,which is believed to address the issue of self-renewal in this subset of cancer cells.The term ‘tumor-initiating cell’is also frequently used to describe cells with CSC capacities.Both terms can,and do,cause confusion about the cells they refer to.8CSC might imply that they are derived from normal stem cells that acquire the genetic hits necessary for malignant transformation.While this is likely to be a possibility in several malignancies,in other malignancies this seems to be more complex.9The term ‘tumor-initiating cell’more closely reflects the experimental evidence that is available at present,but suggests that the tumor-initiating cell is the actual cell from which the tumor derived in the first place.This is likely not the case since,there is clear evidence that the CSC or tumor-initiating cell population can undergo changes as the disease progresses.10,11Throughout this review we will use the term CSC and we will discuss their role in tumor growth.We will critically examine issues that relate to xenotransplantation,the plasticity of this cell population,their origin and the relation with the more classical genetic model.Received 05.12.07;revised 04.1.08;accepted 07.1.08;Edited by G Melino;published online 15.2.081LEXOR (Laboratory for Experimental Oncology and Radiobiology),Center for Experimental Molecular Medicine,Academic Medical Center (AMC),Amsterdam,The Netherlands and 2Department of Surgical and Oncological Sciences,Cellular and Molecular Pathophysiology Laboratory,University of Palermo,Palermo,Italy *Corresponding author:JP Medema,CEMM Room G2-131,Academic Medical Center (AMC),Laboratory for Experimental Oncology and Radiobiology LEXOR,Meibergdreef 9,Amsterdam 1105AZ,The Netherlands.Tel:þ31205667777;Fax:þ31206977192;E-mail:j.p.medema@amc.nl Keywords:cancer;cancer stem cell;tumor initiating cells;stem cells;differentiation;epigeneticsAbbreviations:CSC,cancer stem cell;CRC,colorectal cancer;CK-20,cytokeratin 20;HSC,hematopoietic stem cell;LIC,leukemia initiating cell;GMP,granulocyte–macrophage progenitor;AML,acute myeloid leukemia;CML,chronic myeloid leukemia;ALL,acute lymphoblastic leukemia;EGF,endothelial growth factor;bFGF,basic fibroblast growth factor;TAC,transit amplifying cells;NOD/SCID,non-obese diabetic/severe combined immune-deficient;ESA,epithelial-specific antigen;ABC,ATP-binding cassette;SP,side population;MDS,myelodysplastic syndromes;CTC,circulating tumor cell;B-ALL,B-cell acute lymphoblastic leukemiaCell Death and Differentiation (2008)15,947–958&2008Nature Publishing Group All rights reserved 1350-9047/08$30.00/cddIF 7.548分等级地类比连续地‘Cancer Stem Cells versus Genetics’It is well established that cancer is in essence a genetic disease.The sequential accumulation of mutations in oncogenes and tumor suppressor genes,leading to a malignant clone,is a highly accepted and widely used paradigm in oncology research.1,12If the CSC theory is correct,then the result of this accumulation of genetic hits is at least one cell with CSC features that can give rise to moreCSCs and to more differentiated progeny.At what stage in the process of malignant transformation this CSC arises,is highly disputed.An important aspect of the CSC model is the implication that in a malignancy with a defined set of genetic alterations,cells with a different malignant potential are present.In a tumor both differentiated cells that have lost the capacity to propagate a tumor,and cells that retain a clonogenic capacity,exist.This implies that cells showing the same genotypic alterations can show a completely different potential to initiate a tumor in mice.We will present evidence that this proposed difference in malignant potential is not as surprising as it may initially seem.It is believed that CSCs give rise to more differentiated progeny that have lost the ability for self-renewal and the capacity to initiate the formation of a tumor.(Figure 1)This would imply that remnant regulatory mechanisms remain present in cancer cells that guide the differentiation process in analogy to normal cell differentiation.Indeed,there are examples of malignant cells that are transformed in non-malignant cells by non-genetical means.13–16Epigenetics.From studies addressing the question of whether malignant cells can give rise to benign offspring,it is clear that mutations are not the only factors that predict themalignant potential of cells.13It was already described in 1971that malignant squamous cell carcinoma cells could give rise to more differentiated,non-malignant offspring.14In another study,performed in the 1970s,it was shown thatsubcutaneous injection of embryonal carcinoma cells gave rise to teratocarcinomas,while the same cells injected into a blastocyst gave rise to a normal chimeric mouse.15This concept was expanded in an elegant study by Hochedlinger et al .16They reported that transfer of a nucleus from a melanoma cell into an oocyte (to generate embryonic stem cells)generated chimeric mice with a normal phenotype,despite the fact that a clear increase in cancer incidence was found.16This work suggests that the epigenetic profile of a cell,in this case probably induced by the environment,and the proteins present in the cytoplasm of the oocyte at themoment of nuclear transfer,can compensate for mutations to a large extent.This difference in epigenetic profile could also explain the variety in tumorigenic potential in CSCs and differentiated cells in a malignancy.Indeed there is some evidence that epigenetic differences between CSCs and more differentiated cells exist,as there is for example,a hypermethylation described of TGF b -R2in the mammary carcinoma non-CSCs.17Clonal selection.The proposed hierarchical organization of a malignancy could be easily integrated in the classical clonal selection theory of Nowell.2(Figure 2)This theory views a malignancy as a clonally-derived cell population,which acquires new potentially advantageous mutations that give rise to new more rapidly proliferating clones.This leads to a process referred to as ‘tumor Darwinism’,which selects for the cell type most suitable for unlimited proliferation in the given environment.When one integrates the CSC theory inFigure 1Hierarchical organization of a malignant clone.Depicted is the proposed organization of a malignant clone as predicted by the CSC model.The CSC on the top of the hierarchy (red)has the ability to self-renew,meaning generating more CSCs,and to spin off more differentiated cells (gray).It is to date not clear if the more differentiated cells can revert back and regain a more stem cell phenotypeCritical review cancer stem cell modelL Vermeulen et al948Cell Death and Differentiation分层结构本质传播胚胎癌性细胞补偿this model,the selection pressure is predicted to act at the level of the CSC compartment,implying that certain new traits in CSCs result in an increase in expansion of the CSCs due to self-renewal by symmetrical divisions.This does not mean,however,that certain features present only in the more differentiated cells in the tumor could not be the subject of selection,especially if this increases the expansion rate of the CSCs from which they are derived.For example the more differentiated cells may provide the CSC from which they are derived and which they surround a possible advantage over other clones.In this respect one could think of growth factor production,promoting angiogenesis or the production of immunosuppressive cytokines.Although this suggests that purely genetic models of tumor selection could go hand in hand with the CSC hypothesis,several crucial issues remain.This will be discussed below.Hematological MalignanciesThe hematological system is one of the most intensely studied and best understood human systems.The hierarchical organization of this system has been appreciated for over four decades.18The rare long term self-renewing stem cells or ‘hematopoietic stem cells’(HSCs)at the top of the pyramid were identified by Weissman and coworkers in 1988.19This was achieved by sorting of a specific population of mouse bone marrow cells and subsequent transplantation into lethally-irradiated mice.19The HSCs give rise to more committed progenitors,the oligolineage precursors that subsequently produce all the different cellular blood compo-nents such as erythrocytes,B-cells,T-cells and macro-phages.In the 1970s Fialkow et al .20extrapolated the then present knowledge of the hematopoietic system and initiatedexperiments that addressed the hierarchical organization of leukemia’s.They showed that a variety of leukemias including acute myeloid leukemia (AML)and chronic myeloid leukemia (CML)contain a diversity of cells that vary in differentiation lineages they follow,but were monoclonal in origin.21In 1994,Dick et al .22were able to show that only the CD34þCD38Àcells in a human AML are able to transmit the disease into a NOD/SCID mouse.23This transplantation resulted in a phenocopy of the original leukemia,complete with a variety of more differentiated cells.Moreover,subse-quent propagation of the leukemia in mice was possible.This demonstrates that the leukemia equivalent of the HSC is a CD34þCD38Àcell,also called the leukemia-initiating cell (LIC).It seems,however,that not all AML types follow this simple principle.For example,in a specific AML subtype characterized by its PML/RARA translocation,CD34þCD38Àpurification did not result in engraftment.22,24Maybe the CSC in this type of AML expresses different markers which could imply a different cell of origin.After the identification of the CSC population in certain types of AML,other hematopoietic malignancies followed,including CML 25and myelodysplastic syndromes (MDS).26Much of the present insights and concepts in the CSC theory are derived from studies in leukemias.Although tempting,care should be exercised when generalizing concepts derived from specific human malignancies or models.Solid MalignanciesIn similarity with the hematopoietic system,other organ systems also contain a stem cell compartment.For instance,the rapid turnover of the epithelial lining in the intestinal tract is tightly regulated by stem cells located at the bottom oftheFigure 2Clonal selection of hierarchical organized clones.Cancer stem cells with tumor initiating and tumor growth driving capacity give rise to more differentiated non-tumorigenic offspring.In this model selection pressure is predicted to act on the CSC level.CSCs acquire additional genetic alterations (here depicted by different colors)that can be beneficial for the clone ‘blue’and ‘yellow’or dreadful‘red’Critical review cancer stem cell model L Vermeulen et al949Cell Death and Differentiationcrypts.These stem cells give rise to transit amplifying cells (TAC),which in turn provide the variety of differentiated cells found in the intestinal epithelium,including enterocytes,goblet cells and Paneth cells.27This analogy in hierarchical organization therefore induced speculation as to the existence of hierarchy in non-hematopoietic malignancies.Populationsof cancer cells that match the described criteria for CSCs,that is,self-renewal and the ability to give rise to a variety of differentiated cells,have since been identified in a diversity of human malignant tumors.The first solid tumor type from which a CSC population was isolated using cell surface markers was breast cancer.In 2003Al-Hajj et al .28showed that one hundred CD44þCD24low/ÀESA þcells from breast carcino-mas were able to grow a differentiated mammary carcinoma in SCID mice.This is in contrast to the CD44Àand CD24þtumor cells that were not able to grow a tumor even when 105cells were injected.Moreover,sequential transfer of the disease was possible in this setting.Currently,populations with CSC characteristics have been identified in brain tumors,including medulloblastoma and glioblastoma,head and neck squa-mous cell-,colon-,prostate-,lung-,pancreas-,ovarian-and hepatic carcinoma.29–38The CSCs in solid tumors are directly selected after dissociation based on the expression of cell surface proteins frequently associated with a primitive,non-mature cell type (Figure 3).These stem cell markers are oftenassociated with stem cells or progenitor cells in the specific tissue from which the cancer arose,like CD133in medullo-blastomas.29,39However,in other instances the marker protein used to enrich the CSC population was not associated with the stem cells in the normal tissue.For example,CD133is used to identify a colon CSC-containing population,but this is not known to be a stem cell marker in the normal colon.31,40,41In addition to the direct isolation of populations of CSCs,there are attempts to culture the CSCs under specialized conditions –initially developed for the culturing of neuronal stem cells.42To initiate a CSC culture,tumor tissue is enzymetically digested and the cells are cultured in mediumrich in EGF and bFGF.The cells are kept in low adhesion flasks,resulting in spheroid cultures.So far,reports of successful culture of populations of cells with CSC characteristics have been obtained for a diversity of brain tumors,colon carcinoma,breast cancer,lung cancer and melanoma.38,41,43–46The above described CSC cultures are highly enriched for cells expressing the same markers as used for direct sorting of the CSC population in the particular malignancy.Although in the case of breast cancer mammary sphere cultures,there is some discrepancy in epithelial-specific antigen (ESA)expres-sion,which is present on directly sorted breast CSCs but not on cultured mammary CSCs.28,45Primary human coloncarcinomaabCD133+cell derivedxenograftCD133+cellsFigure 3Direct isolation of cancer stem cell-containing populations in various malignancies.(a )Colorectal cancer can be serially transplanted by isolation of the CD133þcell fraction.CD133Àcells do not have the ability to initiate a subcutaneous xenograft in mice.The typical morphology of the colorectal cancer and marker expression are preserved.(b )Table describing the direct isolation of cancer stem cell containing populations in various malignanciesCritical review cancer stem cell modelL Vermeulen et al950Cell Death and Differentiation隐窝成神经管细胞瘤祖细胞烧瓶It is described that cells cultured under stem cell conditions are able to obtain a more differentiated morphology and expression of differentiation markers,when cells are trans-ferred to differentiating culture conditions.For glioblastoma cells it is shown that the differentiated cells lose the CD133 stem cell marker and gain GFAP and Tuji expression,glial and neuronal cell markers respectively.44,47In the case of colon CSC cultures,differentiation of CSC in matrigel results in crypt-like structures that lose CD133expression and start to express CK20and villin,proteins normally expressed in differentiated colon cells41,48(Figure3a).In addition,the differentiated cells start producing mucin,which indicates functional differentiation into a goblet-like cell type.48Once these cultured CSC have undergone differentiation these cells no longer retain tumorigenic potential upon injection into mice41or show a completely different morphology to the original tumor,with less differentiation and invasive growth.44Whether this in vitro differentiation program is reversible,and whether such cells can regain their original tumorigenicity remains to be established,as does the relationship between in vitro and in vivo differentiated CSCs. CaveatsAs highlighted by others,the practice used to identify CSCs in a given malignancy causes some concern with regards to interpretation of the results so far.5,6,8The fact that testing for CSC capabilities of cell populations involves xenotransplanta-tion and,in the case of solid malignancies,complete tissue disruption during dissociation,could mean that we simply select for cells better equipped for survival in mice,or for cells that are more independent of their microenvironment. In addition,the non-orthotopic injection of cancer cells,for example subcutaneous for colorectal cancer,provides the cells with a completely different environment.This could also influence the outgrowth potential of certain cancer cell subsets.Finally,immuno-compromised mice are not completely devoid of an immune system.The remnant immune response observed in for example NOD/SCID mice could be one mode of selective pressure–to explain the observation that only a subset of tumor cells is able to give rise to a phenocopy of the original human malignancy.In most studies performed to date human material was transplanted into mice.This possibly introduces a so called xenotransplantation bias.A bias possibly caused by mouse chemokines having different affinities for human receptors and altered downstream signaling features.In apparent agreement with this potential criticism is the observation that transplantation of leukemic cells derived from a variety of transgenic mouse strains into other non-immuno-compro-mised,syngeneic mice showed that an invariably high percentage of cells was able to propagate the disease.49 The authors conclude from this that the relative low frequency of LIC(e.g.one in every106cells in human AML)is due to the fact that only a very limited number of leukemia cells are capable of rapid adaption to a foreign,mouse milieu.Whether this observation is due to the nature of these particular mouse models or is a general phenomenon when tumors are transplanted into a syngeneic background needs to be further elucidated.In a comment to the above mentioned study by Kennedy et al.50emphasis was paid to experimental data showing a comparable LIC frequency in xenografts versus syngeneic approaches for a particular form of B-cell acute lymphoblastic leukemia.In addition,Kennedy et al.50stressthat the definition of a CSC does not refer to any of the relative amount of CSCs present in a malignancy.It is highly possiblethat certain less differentiated,homogeneous malignancies contain high relative numbers of cells fulfilling the criteria for CSCs.In solid malignancies,examples of mouse–mouse transfers exist,where it is indeed only a subset of malignant cells expressing markers associated with immature cell types thatare able to initiate a new malignancy.For example in a recentstudy using the MMTV-Wnt-1mouse model for breast cancerit was observed that only the Thy1þCD24þpopulation,that makes up about1–4%of total tumor cells,is able to propagatethe disease in a syngeneic background.51This illustrates thatthe differences in tumor propagating capacities between subsets of malignant cells cannot be explained only by human-to-mouse transplantation biases.Lastly,the ability of certain cells to grow a complete newtumor in a mouse does not necessarily reflect their growth promoting capacities and features within a malignancy.CSC entity.In the studies performed so far populations of cells,often as little as102,enriched for CSC markers are injected.However,this raises doubt as to whether the‘entity’with CSC features is a single cell or whether the diversity of injected cells is necessary to grow the tumor.28,29,31The lastpoint is significant since,due to technical limitations,these injected populations invariably show a marked(0.2–5%) contamination with cells showing a non-CSC pheno-type.28,29,31This allows for alternative interpretations of the data,that is,the cells bearing the CSC markers only facilitatethe outgrowth of the non-CSCs.There are even some indications that the non-CSCs in mammary cancer,though clonally related to their CSCs,sometimes show a different genotype to the CSCs,suggesting two parallel operating clones.17Seminal studies on HSCs and mammary epithelial stemcells have shown that one single stem cell can give rise to a complete hematopoietic system and a functional mammarygland respectively.52,53In analogy with these observations,we have addressed this question by single-cell cloning ofcolon CSCs and transplanting their progeny subcutaneouslyinto a mouse.The single CSC-derived tumors that arose were similar to the original parental human tumor in morphologyand marker expression and were able to give rise to new CSC cultures.We found evidence for differentiated progeny(gobletcell-like,enterocyte-like and neuroendocrine-like)within these tumors(submitted data).Using single cell propagation,similar results have been obtained for teratocarcinomas54and breast cancer cells,55although the latter study was performed usinga rat mammary carcinoma cell line that has been in culture for almost30years.Therefore,this data shows that,in principle,a single CSC contains all the information necessary to grow a phenotypically identical tumor.Because by definition,single-cell propagation of a malignancy results in a monoclonal cancer,the heterogeneity in a tumor with respect to theCritical review cancer stem cell modelL Vermeulen et al951Cell Death and Differentiation恶性胶质瘤同基因的异质性presence of genetically different CSC clones cannot be investigated in this manner.Of major importance to begin answering the questions that relate to transplantation biases will be the development of methods to isolate the CSCs in mouse models of solid cancer. This will give insight into the possible xenotransplantation bias in relation to the functional definition so far.For the study of hematological malignancies,mouse models are frequently used and the mouse CSCs in leukemias are much better characterized than the human equivalents.However,in solid malignancies there are currently no studies describing the isolation of a CSC population in a mouse model. Plasticity.Widespread pluripotency and‘plasticity’are features that have been observed in normal adult stem cells.For example,bone marrow-derived stem cells that give rise to hepatocytes,56and neuronal stem cells have been shown to transdifferentiate into hematopoietic stem cells.57 This raises questions about the very concept of a stem cell. Is a stem cell a concrete,cellular entity,or possibly a more functional entity(reviewed in Blau et al.58and Zipori59)?The same question applies to CSCs.In case of CSCs the inherent features may reflect a transient state that is regulated by micro-environmental parameters,rather than by cell intrinsic properties.Throughout this review we will use the term ‘plasticity’to describe the phenomenon that phenotypically differentiated cells can de-differentiate and acquire stem cell features such as self-renewal and the capacity to generate cells in a variety of differentiation lineages.This possible plasticity of the CSC compartment in a malignancy is a much debated issue within the CSC model.When de-differentiation of differentiated tumor cells into CSCs exists,this would imply that the CSC compartment is not stable over time.This issue will be addressed in more detail below.With respect to the potential existence of plasticity of the CSC compartment careful examination of the CSC cultures is potentially useful.CSC cultures provide an enormous potential,but could also beflawed by cellular selection.There is evidence that culturing of dissociated tumor cells,under stem cell conditions,minimizes genetic alterations,which are normally found when primary cancer cells are cultured under classical conditions in an attempt to generate a cell line.44In addition,the tumors that arise after transplantation of the cells cultured under stem cell conditions are genotypically and phenotypically more closely related to the original malignancy, than the tumors that arise after injection of adherent culturesfrom the same malignancy.This indicates that CSC cultures are a major improvement in comparison with the regular method of cancer cell line generation.But,caution is warranted since the limited success rate of culture initiation may reflect selection for CSCs that contain special character-istics,such as niche-independent growth.The question arises as to whether the CSC culturing method gives the CSCs a selective advantage over the non-CSC,or whether the culture environment may induce a ‘stemness’program in the more differentiated cells.Both bFGF and EGF,which are added to the medium of CSC cultures,have been described to be able to induce this de-differentiation.60,61If de-differentiation occurs in vitro,this would imply that the differentiation program is in principle reversible.Extrapolating this to the situation in a tumor would mean that the CSC population in a malignancy is unstable over time.However,it is also reported that CD133Àcells in medulloblastoma are not able to initiate a CSC spheroid culture,indicating that this plasticity is not a frequent event in vitro.47We observed the same for CD133Àcolon carcinoma cells.(Vermeulen et al.submitted)However,the situation in an established tumor could be completely different.The existence of a CSC niche that not only prevents differentiation, but possibly even induces de-differentiation,and the induction of a CSC phenotype of more differentiated tumor cells could support this idea.13,62If this is the case this would severely change the CSC model,since it implies that the hierarchical organization of a malignancy is not as rigid as proposed. (Figure1)In addition,the therapeutic benefit of drugs that specifically target the CSCs would be considerably limited. More extensive and intriguing insights into the role and importance of the CSC compartment in the development and preservation of a malignancy is expected from the develop-ment of technically challenging mouse models,in which the CSCs can be targeted specifically.A pre-requisite of these models must be the possibility to selectively impair the CSC function by either killing,inactivating or differentiating the CSC after a malignancy occurs.This will address the question of whether there is a need for CSCs in the expansion of a given malignancy together with the question of whether plasticity concerning the CSC population exists.CSC markers.The membrane markers used to identify CSC populations,such as CD133,CD44and CD24as well as the functional characteristic of Hoechst33342exclusion, which indicates a side population(SP)of cells that express high levels of ATP-binding cassette transporter proteins,ask for a more careful examination.Many of the markers are associated with a stem cell phenotype in the tissue the malignancy occurred in.The term‘marker’implies that those proteins are simply a read out for a particular stem cell phenotype,but possibly the proteins themselves fulfill an important role in the process of engraftment that is eventually used to determine the tumorigenic potential of this population.For example,CD44,which is suggested to be a CSC marker in colon cancer,has also been described to enhance the engraftment of colorectal cancer cell lines in both a subcutaneous,and a liver injection model.63In analogy,the SP analysis that is performed to select cells with stem cell characteristics leads to‘loading’of the non-SP cells with Hoechst33342that is potentially toxic and hampering the viability and thus engraftment of those cells.64More insight as to the functions of the markers used for identification of CSC is required,together with studies addressing the contribution of the proteins used for selection on the engraftment potential of certain subpopulations of cells.Origin of the Cancer Stem CellAs appreciated from the definition of a CSC,this cell is not necessarily derived from a normal tissue stem cell.Although it is tempting to speculate that normal stem cells,which are present for long enough in the human body to acquire theCritical review cancer stem cell modelL Vermeulen et al 952Cell Death and Differentiation推断ATP结合盒转运体A1•iABCA1•j移植妨碍推测。
泛素特异性蛋白酶44在肝细胞癌中的表达及预后价值_NormalPdf

第42卷第5期2021年9月Vol.42No.5September2021中山大学学报(医学科学版)JOURNAL OF SUN YAT⁃SEN UNIVERSITY(MEDICAL SCIENCES)泛素特异性蛋白酶44在肝细胞癌中的表达及预后价值王随境1,赖杰怡1,张丽红1,李孜孜2,张新科1,陈杰伟1(1.华南肿瘤学国家重点实验室//中山大学肿瘤防治中心病理科,广东广州510060;2.中山大学附属第五医院病理科,广东珠海519000)摘要:【目的】探讨泛素特异性蛋白酶44(USP44)在肝细胞癌(HCC)中的表达及其临床病理学意义。
【方法】运用免疫组化方法,检测USP44蛋白在161例肝细胞癌中的表达水平,统计分析其与临床病理参数之间的相关性及其预后价值。
【结果】在161例HCC患者中,98例(60.9%)高表达USP44蛋白,Pearson′s卡方检验结果显示USP44在HCC中的表达水平与临床分期(χ2=14.44,P<0.001)、肿瘤单灶及多灶性(χ2=8.04,P=0.005)显著相关;Kaplan-Mei⁃er分析结果显示,低表达组患者平均生存时间59.6个月,显著低于高表达组患者的平均生存时间185.0个月(Log-rankχ2=20.77,P<0.001);多因素Cox比例风险模型揭示USP44是HCC患者的独立预后危险因素。
【结论】USP44蛋白高表达的HCC患者具有良好的生存期,检测其蛋白表达可作为筛选预后良好的肝细胞癌患者的一种手段。
关键词:泛素特异性蛋白酶USP44;肝细胞癌;免疫组化;预后中图分类号:R735.7文献标志码:A文章编号:1672-3554(2021)05-0746-10DOI:10.13471/ki.j.sun.yat-sen.univ(med.sci).2021.0513Expression of USP44in Hepatocellular Carcinoma and Its Correlation with the Prognosis WANG Sui-jing1,LAI Jie-yi1,ZHANG Li-hong1,LI Zi-zi2,ZHANG Xin-ke1,CHEN Jie-wei1(1.State Key Laboratory of Oncology in South China//Department of Pathology,Sun Yat-Sen University Cancer Center,Guangzhou510060,China;2.Department of Pathology,the Fifth Affiliated Hospital of Sun Yat-sen University,Zhuhai519000,China)Correspondence to:CHEN Jie-wei;E-mail:chenjiew@Abstract:【Objective】To investigate the expression of Ubiquitin specific protease44(USP44)and its clinical signifi⁃cance in hepatocellular carcinoma(HCC).【Methods】Immunohistochemistry was used to detect the expression of USP44 protein in161cases of hepatocellular carcinoma.The correlation between the expression of USP44protein and clinicopath⁃ological parameters,and its prognosis value were analyzed.【Results】Immunohistochemical analysis showed USP44dis⁃played elevated expression in98HCC cases out of161cases.Pearson′s chi-square test indicated the expression of USP44 in HCC was significantly correlated with clinical stage(χ2=14.44,P<0.001)and tumor multiplicity(Unifocal or Multifocal)(χ2=8.04,P=0.005).Kaplan-Meier analysis indicated patients with low USP44expression correlated with poor overall sur⁃vival(Log-rankχ2=20.77,P<0.001).The overall mean survival time was59.6months in low USP44expression patients and185.0months in high USP44expression patients.The Cox proportional hazard model analysis showed USP44was an in⁃dependent prognostic risk factor for HCC patients.【Conclusion】USP44is an independent prognostic risk factor for HCC patients,and the expression of USP44protein could be used to screen patients with good prognosis for HCC.Our study may provide evidence for USP44as a potential therapeutic target for HCC patients.Key words:ubiquitin specific protease44;hepatocellular carcinoma;immunohistochemistry;prognosis[J SUN Yat⁃sen Univ(Med Sci),2021,42(5):746-755]·临床研究·收稿日期:2021-05-18基金项目:国家自然科学基金(81902420);广东省食管癌研究所科技计划项目(Q201903)作者简介:王随境,技师,研究方向:肿瘤标记物,E-mail:wangsj@;陈杰伟,通信作者,副主任技师,研究方向:肿瘤标记物,E-mail:chenjiew@第5期王随境,等.泛素特异性蛋白酶44在肝细胞癌中的表达及预后价值原发性肝癌是全球最常见的恶性肿瘤之一,发病率排世界第6位,是全球第3大癌症致死原因[1]。
芦可替尼治疗骨髓增殖性肿瘤的疗效和安全性研究进展演示稿件

汇报人:XXX
2024-01-08
目录
• 引言 • 芦可替尼的药理作用 • 芦可替尼治疗骨髓增殖性肿瘤的
临床研究 • 芦可替尼的安全性评价 • 结论与展望
01
引言
研究背景
骨髓增殖性肿瘤(MPN)是一组起源于骨髓造血干细胞的肿瘤性疾病,包括慢性粒细 胞白血病、真性红细胞增多症、原发性血小板增多症和骨髓纤维化等。
总生存期
芦可替尼治疗骨髓增殖性肿瘤的总生 存期较对照组有所延长。
生活质量
接受芦可替尼治疗的患者生活质量得 到改善,疼痛缓解、功能改善等方面 表现良好。
04
芦可替尼的安全性评价
不良反应类型及发生率
常见不良反应
芦可替尼治疗骨髓增殖性肿瘤的常见不良反应包括口腔溃疡、皮疹、恶心、呕吐、腹泻等。其中,口腔溃疡的发 生率较高,需要引起关注。
随机对照试验
将骨髓增殖性肿瘤患者随机分为芦可替尼组和对照组 ,以评估芦可替尼的治疗效果。
观察性研究
对接受芦可替尼治疗的骨髓增殖性肿瘤患者进行观察 ,记录治疗过程和疗效。
剂量探索试验
确定芦可替尼治疗骨髓增殖性肿瘤的最佳剂量和给药 方案。
疗效评估指标
缓解率
评估接受芦可替尼治疗的患者中达
芦可替尼与化疗药物、免疫治疗药物 和其他靶向药物的联合应用显示出协 同抗肿瘤作用,能够提高疗效并降低 毒副作用。
例如,芦可替尼与干扰素α联合治疗骨 髓增殖性肿瘤,能够增强干扰素α的抗 肿瘤效果,减少剂量依赖性毒副作用 。
03
芦可替尼治疗骨髓增殖性肿 瘤的临床研究
临床试验设计
预防措施
预防芦可替尼不良反应的措施包括控制剂量、避免与其他药物同时使用、定期 监测肝功能等。此外,患者在治疗期间应保持良好的生活习惯和饮食结构,以 提高身体免疫力。
铁死亡诱导剂在结直肠癌中的研究进展

- 180 -end-expiratory pressure alone minimizes atelectasis formation in nonabdominal surgery:a randomized controlled trial[J].Anesthesiology,2018,128(6):1117-1124.[39] KIM N,LEE S H,CHOI K W,et al.Effects of positive end-expiratory pressure on pulmonary oxygenation and biventricular function during one-lung ventilation:a randomized crossover study[J].J Clin Med,2019,8(5):740.[40] KATZ J A,LAVERNE R G,FAIRLEY H B,et al.Pulmonaryoxygen exchange during endobronchial anesthesia:effect of tidal volume and PEEP[J].Anesthesiology,1982,56(3):164-171.[41] SENT ÜRK N M,DILEK A,CAMCI E,et al.Effects ofpositive end-expiratory pressure on ventilatory and oxygenation parameters during pressure-controlled one-lung ventilation[J]. J Cardiothorac Vasc Anesth,2005,19(1):71-75.[42] KANG W S,KIM S H,CHUNG J parison of pulmonarygas exchange according to intraoperative ventilation modes for mitral valve repair surgery via thoracotomy with one-lung ventilation:a randomized controlled trial[J].J Cardiothorac Vasc Anesth,2014,28(4):908-913.(收稿日期:2023-03-03) (本文编辑:田婧)*基金项目:安溪县科技计划项目(2022S002)①福建省安溪县医院 福建 安溪 362400通信作者:许永鹏铁死亡诱导剂在结直肠癌中的研究进展*陈伟鸿① 苏小苹① 苏宇超① 黄栋钦① 许永鹏① 【摘要】 结直肠癌(colorectal cancer,CRC)是全球第三大常见癌症,传统治疗方案对CRC 晚期患者的疗效不佳,因此,发现新的治疗策略可能有助于改善CRC 患者的治疗和预后。
肠癌PPT

CpG岛甲基化(CIMP)相关基因: hMLH1、hMSH2、p16、p14、MYF、 MDR1、E-cadherin
2、干细胞在大肠癌发生中的作用
• 干细胞表面标志物: RNA结合蛋白Musashi-1(Msi-1) CD29
Nishimura S,Wakabayashi N,Toyoda K,et al.Expression of Musashil in human normal colon crypt cells:a possible stem marker of human colon epithetlium [J].Dig Dis Sci,2003,48(8):1523-1529. Fujimoto K,Beauchamp RD,Whitehead RH,el al.Identification and isolation of candidate human colonic clonogenic cells based on cell surface integrin expression [J].Gastroenterology,2002,123(6):1941-1948. Barker N,van Es JH,Kuipers J,et al.Identification of stem cells in small intestine and colon by marker gene Lgr5 [J].Nature,2007,449(7165):1003-1007. Arena V, Caredda E, Cufino V, et al. Differential CD133 expression pattern during mouse colon tumorigenesis.[J]. Anticancer Res. 2011,31(12):4273-5. Takaishi S,Okumura T,Tu S,et al.Identification of gastric cancer stem cells using the cell surface marker CD44 [J].Stem Cells,2009,27(5):1006-1020. Li C,Heidt DG,Dalerba P,et al.Identification of pancrestic cancer stem cells [J].Cancer Res,2007,67(3):1030-1037.
CBMDisc 数据库实习题

C B MD i s c数据库实习题1、检索“视网膜再灌注损伤与半胱氨酸天冬氨酸蛋白酶”表达的相关文献。
方法1:关键词、缺省、题名均可:视网膜 and再灌注损伤 and 半胱氨酸天冬氨酸蛋白酶方法2:#1缺省:视网膜 and再灌注损伤#2 关键词:视网膜 and再灌注损伤#3 半胱氨酸天冬氨酸蛋白酶/全部副主题词#1 and #3 或 #2 and #32、检索《中华实验外科杂志》上肝移植的免疫学方面的文献。
#1 刊名:中华实验外科杂志#2 主题检索:肝移植 / 免疫学#1 and #23、检索有关儿童肥胖与糖尿病的关系的文献方法1:#1主题检索:糖尿病/全部副主题词#2 关键词:肥胖(限定儿童)#1 and #2方法2:题名:儿童 and 肥胖 and 糖尿病4、检索有关血液透析治疗急性肾功能衰竭方面的文献。
#1 主题检索:肾功能衰竭,急性/全部副主题词#2 关键词:血液透析#1 and #21.(1)本例的中英文关键词:维生素A缺乏…Vitamin A Deficiency(2)检索步骤①.#1 Vitamin A Deficiency②.通过Limits从时间、年龄、语种方面进行限定。
2.利用主题途径(MeSH Database),查近5年来“青少年肾功能衰竭的并发症或死亡率”临床实验(Clinical Trial)方面的文献。
(加权检索)(1)本例的中英文关键词:肾功能衰竭… Renal failure并发症… Complication死亡率… mortality(2)分析课题本例讨论的是肾功能衰竭的并发症或死亡率,故副主题词选择并发症或死亡率,二者的逻辑关系是逻辑或。
(3)检索步骤①.点击Pubmed主页的MeSH Database,进入主题检索页面;②.输入检索词renal failure并点击go;③.点击主题词Kidney Failure,并在Subheadings(副主题词)选中complication(并发症) 和mortality (死亡率);④.在Restrict Search to Major Topic headings only选项前打标记(加权检索);⑤.点击Send to下拉菜单 Search Box with AND,系统进入⑥. 点击Search PubMed将显示检索结果;⑦.点击Limits: Ages中选Adolescent(13-18岁)、Type ofArticle中选(Clinical Trial)、输入起止年份2003-2008,点击search ,系统返回检索结果。
浅析染色质免疫沉淀(ChIP)技术在DNA与蛋白质相互作用研究中的重要性

浅析染色质免疫沉淀(ChIP)技术在DNA与蛋白质相互作用研究中的重要性染色质免疫沉淀(ChIP)是研究蛋白质-DNA相互作用的一项强大技术,广泛用于多个领域的染色质相关蛋白的研究(如组蛋白及其异构体,转录因子等),特别适用于已知启动子序列或整个基因位点的组蛋白修饰分析研究。
这项技术采用特定抗体来富集存在组蛋白修饰或者转录调控的DNA片段,通过多种下游检测技术(定量PCR,芯片,测序等)来检测此富集片段的DNA序列。
ChIP技术自诞生之后,已成功的应用于人或动物细胞和组织[1] 、植物组织[2]、酵母[3] 以及细菌、质粒[4] 。
由于在信号转导和表观遗传研究中的突出作用,ChIP 在肿瘤[5-7]、神经科学[8-10]、植物发育[11-13] 等领域中应用非常广泛,同时有关细胞凋亡[14]、雌激素信号转导[15] 、胰岛素抵抗[16] 、组织发育[1]的文献中也用到ChIP。
目前,最常见的有以下两种ChIP实验技术:1. nChIP:用来研究DNA及高结合力蛋白,采用微球菌核酸酶(micrococcal nuclease)消化染色质,然后进行片段富集及后续分析,适用于组蛋白及其异构体,例如[17-19] ;2. xChIP:用来研究DNA及低结合力蛋白,采用甲醛或紫外线进行DNA和蛋白交联,超声波片段化染色质,然后进行片段富集及后续分析,适用于多数非组蛋白的蛋白,例如[9, 15, 20]。
X-ChIP试验的一般过程以上两种方法在分离DNA-蛋白质复合物之后,对DNA进行PCR扩增,验证目标序列的存在。
除验证实验外,ChIP DNA也可以进行测序分析,这种方法被称为ChIP-seq[22];也可做芯片分析,这种方法被称为ChIP on CHIP或ChIP-CHIP[23] 。
这两种方法都可用于分析感兴趣蛋白结合的未知序列,而不需要知道目标序列的详细信息,因此可以进行探索性的研究。
当需要对DNA结合的蛋白复合物(两个或两个以上蛋白共同结合在DNA上)进行研究时,可以采用reChIP技术对DNA蛋白复合物进行再次富集,从而分析两种蛋白同时结合的DNA片段,例如转录调控因子及其受体复合物[24]。
肿瘤研究新手必看经典文献

肿瘤研究新手必看经典文献由于关于肿瘤的文献超过160万篇,这令许多新手无法下手,在这里,根据我个人对肿瘤的理解,特推荐下列经典文章供新手参考,也希望抛砖引玉,高手们提供更多的文章。
1)癌基因和抑癌基因与肿瘤关系文章:Hahn WC, Weinberg RA. Modelling the molecular circuitry of cancer.Nat Rev Cancer. 2002 May;2(5):331-41. Review.Hanahan D, Weinberg RA. The hallmarks of cancer.Cell. 2000 Jan 7;100(1):57-70. Review. Weinberg RA. Tumor suppressor genes.Science. 1991 Nov 22;254(5035):1138-46. Review Weinberg RA. Oncogenes, antioncogenes, and the molecular bases of multistep carcinogenesis.Cancer Res. 1989 Jul 15;49(14):3713-21. Review.Land H, Parada LF, Weinberg RA. Cellular oncogenes and multistep carcinogenesis.Science. 1983 Nov 18;222(4625):771-8. Review.Kinzler KW, Vogelstein B. Lessons from hereditary colorectal cancer.Cell. 1996 Oct 18;87(2):159-70. Review.Fearon ER, Vogelstein B. A genetic model for colorectal tumorigenesis.Cell. 1990 Jun1;61(5):759-67. Review.Prehn RT. Many growth factors may not be growth factors.Cancer Res. 1992 Feb 1;52(3):501-7. Review.2)基因组不稳定与癌Rajagopalan H, Nowak MA, Vogelstein B, Lengauer C. The significance of unstable chromosomes in colorectal cancer. Nat Rev Cancer. 2003 Sep;3(9):695-701. Review.Lengauer C, Kinzler KW, Vogelstein B. Genetic instabilities in human cancers.Nature. 1998 Dec 17;396(6712):643-9. Review.Nowell PC. Mechanisms of tumor progression.Cancer Res. 1986 May;46(5):2203-7. Review Nowell PC. Tumor progression: a brief historical perspective.Semin Cancer Biol. 2002 Aug;12(4):261-6. Review.Loeb LA, Loeb KR, Anderson JP. Multiple mutations and cancer.Proc Natl Acad Sci U S A. 2003 Feb 4;100(3):776-81. Epub 2003 Jan 27. ReviewLoeb LA. Microsatellite instability: marker of a mutator phenotype in cancer.Cancer Res. 1994 Oct 1;54(19):5059-63. Review.3)肿瘤干细胞Al-Hajj M, Becker MW, Wicha M, Weissman I, Clarke MF. Therapeutic implications of cancer stem cells.Curr Opin Genet Dev. 2004 Feb;14(1):43-7. Review.Reya T, Morrison SJ, Clarke MF, Weissman IL. Stem cells, cancer, and cancer stem cells.Nature. 2001 Nov 1;414(6859):105-11. Review.Perez-Losada J, Balmain A. Stem-cell hierarchy in skin cancer.Nat Rev Cancer. 2003Jun;3:434-43. Review.Pardal R, Clarke MF, Morrison SJ. Applying the principles of stem-cell biology to cancer.Nat Rev Cancer. 2003 Dec;3(12):895-902. Review.4)肿瘤与端粒Sharpless NE, DePinho RA. Telomeres, stem cells, senescence, and cancer.J Clin Invest. 2004 Jan;113(2):160-8. Review.Maser RS, DePinho RA. Connecting chromosomes, crisis, and cancer.Science. 2002 Jul26;297(5581):565-9. Review.DePinho RA. The age of cancer.Nature. 2000 Nov 9;408(6809):248-54.5)肿瘤与进化和适应Farber E. The step-by-step development of epithelial cancer: from phenotype to genotype.Adv Cancer Res. 1996;70:21-48.Farber E, Rubin H. Cellular adaptation in the origin and development of cancer.Cancer Res. 1991 Jun 1;51(11):2751-61.Rubin H. Microenvironmental regulation of the initiated cell.Adv Cancer Res. 2003;90:1-62. Review.Rubin H. Selective clonal expansion and microenvironmental permissiveness in tobacco carcinogenesis.Oncogene. 2002 Oct 21;21(48):7392-411. Review.Rubin H. Selected cell and selective microenvironment in neoplastic development.Cancer Res. 2001 Feb 1;61(3):799-807. Review.6)肿瘤与非整倍体Duesberg P, Li R. Multistep carcinogenesis: a chain reaction of aneuploidizations.Cell Cycle. 2003 May-Jun;2(3):202-10. Review.Li R, Yerganian G, Duesberg P, Kraemer A, Willer A, Rausch C, Hehlmann R. Aneuploidy correlated 100% with chemical transformation of Chinese hamster cells.Proc Natl Acad Sci U S A. 1997 Dec 23;94(26):14506-11.Li R, Sonik A, Stindl R, Rasnick D, Duesberg P. Related Articles, LinksAneuploidy vs. gene mutation hypothesis of cancer: recent study claims mutation but is found to support aneuploidy.Proc Natl Acad Sci U S A. 2000 Mar 28;97(7):3236-41.7)肿瘤与免疫Prehn RT. Stimulatory effects of immune reactions upon the growths of untransplanted tumors.Cancer Res. 1994 Feb 15;54(4):908-14. Review.Gilboa E. The promise of cancer vaccines.Nat Rev Cancer. 2004 May;4(5):401-11.8)肿瘤与信号转到以及细胞周期Blume-Jensen P, Hunter T. Oncogenic kinase signalling.Nature. 2001 May 17;411(6835):355-65. Review.Hunter T. Oncoprotein networks.Cell. 1997 Feb 7;88(3):333-46. Review.Hartwell LH, Kastan MB. Cell cycle control and cancer.Science. 1994 Dec 16;266(5192):1821-8. Review.9)癌的启动和促进Dlugosz A, Merlino G, Yuspa SH. Progress in cutaneous cancer research.J Investig Dermatol Symp Proc. 2002 Dec;7(1):17-26. ReviewYuspa SH, Dlugosz AA, Denning MF, Glick AB. Multistage carcinogenesis in the skin.J Investig Dermatol Symp Proc. 1996 Apr;1(2):147-50.Yuspa SH. The pathogenesis of squamous cell cancer: lessons learned from studies of skin carcinogenesis--thirty-third G. H. A. Clowes Memorial Award Lecture.Cancer Res. 1994 Mar 1;54(5):1178-89. Review.10)两次打击Knudson AG. Two genetic hits (more or less) to cancer.Nat Rev Cancer. 2001 Nov;1(2):157-62. Knudson AG. Antioncogenes and human cancer.Proc Natl Acad Sci U S A. 1993 Dec 1;90(23):10914-21.站点推荐:非整倍体而不是基因突变是肿瘤产生的主要原因讨论区/bbs/post/view?bid=87&id=1003712&sty=1&tpg=2&age=0新的肿瘤发生机理假说讨论区/bbs/post/view?bid=87&id=1007269&sty=1&tpg=2&age=0『精华] 肿瘤经典文章,临床权威指南,欢迎推荐,学习,下载!/bbs/post/view?bid=87&id=690916&sty=1&tpg=1&age=-1[精华] 肿瘤干细胞与肿瘤干细胞起源说/bbs/post/view?bid=87&id=474853&sty=1&tpg=2&age=-1[精华] 肿瘤干细胞研究进展/bbs/post/view?bid=76&id=495491&sty=1&tpg=1&age=-1。
大肠原发癌和转移癌组织中肿瘤干细胞的检测与分选

大肠原发癌和转移癌组织中肿瘤干细胞的检测与分选贾茹;孙青【摘要】Purpose To detect and isolate cancer stem cells ( CSC) in fresh specimens of primary and metastatic carcinoma tissues from 10 cases of colorectal cancer to study the biological functions and mechanisms of migrating cancer stem cells. Methods Suspen-sions of primary and metastatic colorectal cancer cells were labeled with antibodies CD133-PE and CD44-FITC, and then flow cytometry was used to detect and isolate the CD133-PE-positive and CD44-FITC-positive cells. Results There were certain percentages of CD133-positive and CD44-positive cells present in primary and metastatic colorectal cancer and the proportion of CSC in metastatic colorectal cancer was higher than that in primary cancer tissue (P<0.05). Conclusions There are CSC in both primary and meta-static colorectal cancer and the proportion of CSC in metastatic colorectal cancer is significantly higher than that in primary cancer tis-sue, suggesting that CSC play an important role in the metastasis of colorectal cancer.%目的:对10例大肠癌新鲜标本的原发癌组织和转移癌组织中肿瘤干细胞( cancer stem cell, CSC)的含量进行检测并分选,为进一步探讨转移肿瘤干细胞( migrating cancer stem cell, MCSC)的生物功能和机制奠定基础。
Stem cells, cancer, and cancer stem cells-中文翻译

目前国外干细胞的研究如火如荼,《自然》发表的这篇综述从另一方面提出肿瘤的发生和发展与肿瘤干细胞的存在有关,肿瘤干细胞是否存在?还需要进一步的研究,但这毕竟把我们引入一片新的天地。
Stem cells, cancer, and cancer stem cells干细胞、癌症和肿瘤干细胞杜忆华(德国杜塞尔多夫大学博士生)译干细胞生物学已经成熟。
证明造血系统中存在干细胞的研究已让位于对一些组织特异性干细胞和祖细胞的分离与研究、对它们的特征和基因表达程序的阐述,以及在再生医学中对它们应用的研究。
也许干细胞最重要和最有用的特征是它的自我更新能力。
通过这一特征能够发现干细胞和癌细胞之间有惊人的相似:肿瘤可能通常起源于正常干细胞的转化,相似的信号通路可能既调节干细胞也调节癌细胞的自我更新,且癌细胞中可能包含有“肿瘤干细胞”(cancer stem cells)----它们是一些极少的具有自我更新不定潜能的驱使肿瘤形成的细胞。
干细胞被定义为永存的细胞,能通过自我更新和在特异组织中分化产生成熟细胞。
在多数组织中特异性干细胞是极少的。
为了研究干细胞的特征,干细胞需经过仔细纯化和预期的鉴定。
尽管有理由认为每种组织来自于一种组织特异性干细胞,但对这些干细胞的严格的鉴定和分离仅在极少的组织中成功的完成。
例如已自小鼠和人体中分离出造血干细胞(HSCs),并已显示它们负责血细胞和免疫系统的形成(图1)。
来自于多种器官的干细胞可能被用于未来的治疗,而 HSCs -----是骨髓移植中重要的成分,已广泛地用于临床治疗。
图1,造血干细胞的发育最近的研究发现骨髓和造血干细胞(HSCs)可产生非造血组织,提示这些细胞可能具有较以前设想的更为广泛的分化潜能。
这一过程尚需进一步用实验来证实。
骨髓细胞是否可产生不同的非造血组织,这些非造血组织是否真是来自于HSCs或来自于其它细胞。
如果进一步的研究支持造血干细胞具有可塑性,这无疑将开创对HSCs的发展潜能的了解,并进一步为临床治疗开辟新的途径。
结直肠癌CD133_细胞定量评估的意义

基金项目:首都医学发展科研基金资助项目(2005-2052)作者单位:100730卫生部北京医院普外科(缪刚、李尧、黄美雄、韦军民);卫生部北京医院老年医学研究所(赵艳阳)通讯作者:韦军民,电子信箱:weijunmin@263.net结直肠癌CD133+细胞定量评估的意义缪刚李尧赵艳阳黄美雄韦军民摘要目的研究CD133+结直肠癌干细胞与肿瘤增殖、转移的相关性。
方法取得术后新鲜的结直肠癌组织后,立刻进行清洗、消化、培养等过程,得到了具有活性的原代结直肠癌单细胞。
特异性抗体CD133标记后运用流式细胞技术检测癌干细胞分布比例。
癌组织同时进行免疫组化和分子生物学研究,确定增殖蛋白Ki -67、抑制肿瘤转移相关蛋白e -cadherin 和细胞凋亡相关蛋白caspase -3的表达。
结果结直肠癌原代细胞分离、纯化和检测技术简明可行,所得数据客观准确。
研究病例按照CD133+癌干细胞比例≥3%和<3%分成两组。
结果显示CD133+癌干细胞≥3%组在肿瘤大小和淋巴转移有增大和增多趋势;肿瘤增殖特异性蛋白Ki -67增高具有显著性差异;抑制肿瘤转移相关蛋白e -cadherin 的表达降低;凋亡相关蛋白caspase -3的表达降低。
结论本研究成功建立了一套可行性高的结直肠癌CD133+干细胞准确定量评估系统。
结直肠癌干细胞的准确定量检测可以作为评估患者预后和化疗敏感度的一项重要指标。
本技术也为进一步提纯结直肠癌干细胞,并且最终研究对此靶点的攻击提供了平台。
关键词结直肠癌CD133肝癌干细胞Importance of Quantitative Evaluation of Colorectal Cancer CD133+Cells.Miao Gang ,Li Yao ,Zhao Yanyang ,Huang Meixiong ,WeiJunmin.Department of Surgery ,Beijing Hospital ,Beijing University School of Medicine ,Beijing 100730,ChinaAbstractObjectiveTo precisely quantify the percentage of CD133+cancer stem cells by isolation and purification of primarycolorectal cancer cells ,and to clarify its relationship with cancer proliferation and metastasis.MethodsPrimary colorectal cancer cellswere obtained after washing ,digesting and culturing fresh colorectal cancer tissues.Cancer stem cells were labeled with specific CD133antibody and analyzed by flow cytometry.Cancer tissues were also tested using immunostaining and Western blotting to detect expression of proliferative marker Ki -67,invasion suppressor related protein e -cadherin ,and apoptosis related protein caspase -3.ResultsIsola-tion ,purification and precisely quantification of primary colorectal cancer stem cells were efficiently modified as feasible procedures.Pa-tients were divided into two groups with percentage of CD133+cancer stem cells ≥3%or <3%.In the ≥3%group ,a increase of tumor size and lymphatic metastasis was observed ,expression of the specific proliferation protein Ki -67was significantly increased ,production of the tumor metastasis suppressor protein e -cadherin and the apoptotic protein caspase -3was decreased.ConclusionA preciselyquantitative evaluation system of the primary colorectal cancer stem cells was feasibly established in our study.The system can be used as indicators of prognosis and sensibility to chemotherapy in colorectal cancer patients.The technique also functions as a platform in purifica-tion of colorectal cancer stem cells and cancer -stem -cell -targeted therapy in the future.Key wordsColorectal cancer ;CD133;Tumor stem cell越来越多的证据表明肿瘤中存在肿瘤干细胞(cancer stem cells ),并且其与肿瘤的增殖、转移、复发和对化疗不敏感关系密切。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
C ANCER S TEM Concise Review: A RISTIDES G.V AIOPOULOSinjury,disease,or cancer[10–12].Colon shares this SC-basedhierarchical organization with many other tissues/systems thatare under constant renewal,including the hematopoietic systemand the skin[11].Originally,the Unitarian theory proposed themonoclonal nature of intestinal crypts[10].More recent evi-dence,however,implies that crypts are probably polyclonal atbirth and subsequently shift toward monoclonality by followinga pattern of neutral drift[7,13].An intestinal crypt containsapproximately16SCs and harbors two distinct pools of puta-tive SCs.The one pool is located at the crypt base and is char-acterized by the expression of leucine-rich repeat containing Gprotein-coupled receptor5(Lgr-5)and the other pool resides atþ4position and consists of B lymphoma Moloney murine leu-kemia virus(Mo-MLV)insertion region1homolog(Bmi-1)and telomerase reverse transcriptase(Tert)expressing cells[13,14].The contribution of each type of cell to the maintenanceof the SC pool is under debate.One possible suggestion is theexistence of a pool of equally contributing cells where eachcell’s behavior is defined by its entourage and in terms ofreplacement they follow a pattern of neutral drift[13].An al-ternative approach is that Lgr-5þSCs comprise the active pop-ulation of the crypt,whereas Bmi-1þor Tertþcells are quies-cent SCs that represent a reserve pool of SCs with the abilityto replace Lgr-5þcells in case of loss or injury[7,14].More-over,it has been proposed that Bmi-1þcells may not have animpact on Lgr-5þSCs,as Bmi-1knockout mice show normalcrypt morphology and have a normal intestinal epithelium[15].The functional importance of the intestinal microenvironment(niche)in the advanced control of SC life cycle is widelyaccepted.The niche consists of cellular and extracellular com-ponents that ensure the optimal conditions for SC mainte-nance through the secretion of various cytokines,growth fac-tors,and direct interactions[10,16].Interestingly,intestinalSCs may also be affected by components in the crypt lumen,derived from epithelial cells or from bacteria.Intestinal sube-pithelial myofibroblasts are key regulators of SC self-renewaland differentiation,mediate the crosstalk between epithelialand mesenchymal cells,and secrete a wide range of morpho-genetic factors[7].Epithelial–mesenchymal interactions regu-late the normal intestinal architecture and additionally definethe balance between proliferation and differentiation[10,16].Wingless/Int(Wnt),Hedgehog,bone morphogenetic protein(BMP),Notch,and platelet-derived growth factor pathwaysare involved in these interactions[7].Identification and isolation of SCs remain an issue of debate[8]due to the lack of specific molecular markers along withunsolved technical issues,forcing the use of a functional defi-nition based on the attributes of self-renewal and multipo-tency.Consequently,only assumptions can be made regardingtheir exact number and position[17].Several studies havebeen carried out,mostly on small intestine,which used DNAlabeling techniques to exploit the comparatively slower cy-cling rate of SCs[18]and led to the formulation of two dif-ferent models regarding their position[5].Theþ4positionmodel postulates that SCs are located at theþ4position ofthe small-intestine crypt just above the Paneth cells,whichoccupy the bottom.These cells express the markers Bmi-1and Tert.SCs divide into progenitor cells that migrate to thetop of the crypt and differentiate,while Paneth cells followthe exact opposite direction[7,16].Alternatively,theSC Figure1.Hierarchical organization of a normal colonic crypt—comparison between the stochastic and the CSC model.Colonic crypts are hier-archically organized.SCs divide into progenitor cells that migrate at top and produce terminally differentiated cells.In the stochastic model,all cells possess tumor initiation potential.In the CSC model,only CSCs are capable of tumor propagation and metastasis.Microenvironmental crosstalk, epigenetic,and genetic aberrations(yellow lightning bolt)may lead to clonal evolution(dark purple cells).Circumscribed cells represent the mutated types of their normal homologs(white polygons:A,asymmetrical division;S,symmetrical division).Abbreviations:BMP,bone morphogenetic pro-tein;CBCC,crypt base columnar cell;CSC,cancer stem cell;D,differentiated cell;P,progenitor cell;SC,stem cell;WNT,Wingless/Int.364Stem Cells inCRCzone model was proposed after discovering the presence of small immature cycling cells at the crypt base between Paneth cells.These cells were named crypt base columnar cells and express the Wnt target gene Lgr-5[19].Recently,many mole-cules,mostly located on the cell surface,have been proposed as putative stemness markers,at the same time allowing isola-tion by fluorescence-activated cell sorting [10].In summar-y,the molecules involved in critical stages of proliferation and differentiation are Musashi-1(Msi-1),CD29,Bmi-1,Lgr-5,aldehyde dehydrogenase 1(ALDH-1),Tert,and achaete scute-like 2[5,7,9,10,14,15].For a more detailed presenta-tion of the currently used markers,the reader is referred to Table 1.Colorectal carcinogenesis results from a series of genetic/epi-genetic alterations and interactions with microenvironmental and germ-line factors that transform the normal colonic mu-cosa into an aberrant phenotype [2,3].The questions which is the cell of origin and which cells propagate the tumor after initiation remain elusive despite extensive in vitro and in vivo experiments [7,8].The cell of origin is the cell that acquires tumorigenic mutations and becomes the first tumor cell.A cell of origin is different from the cells responsible for tumor propagation after its inception [8].Every normal cell (SC,progenitor,or differentiated)can accumulate mutations and become the cell of origin [8,10,24].Following its malignant transformation,it is possible to follow one of the two pro-posed models for the explanation of carcinogenesis and pro-gression,the stochastic or the CSC model (Fig.1).Even if a normal SC becomes the cell of origin,it can form a tumor according to the features of the stochastic or the CSC model [8].The stochastic model suggests that every cell within a tu-mor is capable of both initiation and propagation.After trans-formation,each cell can acquire further mutations.The heter-ogeneity within a tumor can be explained by the aggregation of random genetic aberrations as well as the divergent micro-environmental influence [8,25].Concomitantly,a diverse population of subclones with different properties is generated.Only selected clones can migrate and form metastases.The migrating clones can further accumulate mutations,resulting in a divergent metastatic tumor from the parent lesion [11].The newly introduced CSC model,on other hand,states that only a small portion of cells within a tumor is endowed with tumor propagation potential and thus named CSCs,whereas all other cells are not [26].According to the CSC model,sim-ilar to the normal tissue,cancers are also hierarchically organ-ized.Tumor heterogeneity results from the production by the multipotent CSCs (high proliferative)of a wide variety of progenitor (medium proliferative)and differentiated (nonproli-ferative)cells [11,27].In this model,only CSCs can migrate and as a result the metastatic tissue resembles the pattern of the original lesion.However,individual cell responses to microenvironmental stimuli,epigenetic modifications,and additional genetic aberrations may be observed within a can-cerous tissue,which in turn may lead to clonal evolution and gain or loss of CSC attributes.A new and improved CSC due to clonal evolution may arise,which will now drive tumor growth and metastasis instead of the initial CSC [8,28].CSCs are characterized by self-renewal,multipotency,limit-less proliferation potential,angiogenic,and immune evasion features [24].Intriguingly,CSCs are relatively highly resistant to traditional tumor therapeutic measures and thus responsible for tumor relapse due to the expression of DNA repair mecha-nisms,detoxifying enzymes,and drug transporters [29].Most likely,CSCs are derived from normal SCs due to their extended life span that alter their behavior as a result of genetic and epigenetic changes.It has also been discussed that progenitor,differentiated,or even cells from outside the tumor,for example,bone marrow-derived cells,might also serve as CSCs’ancestors [8,10,11,28,30].Concomitantly,through symmetric (CSC overproduction)or asymmetric (het-erogeneity)divisions,the entire crypt will be colonized from the mutated SCs and their descendants.Future alterationsmayVaiopoulos,Kostakis,Koutsilieris et al.365lead to a more aggressive and metastatic phenotype[5,31].Throughout CRC progression,the number of CSCs remainsapproximately1%of the number of total cells.However,theirfrequency appears to be highly variable[6,28].The CSCmodel modifies the classic Fearon and Vogelstein model,which is characterized by step-by-step genetic modificationsof the adenoma to carcinoma sequence,by placing the normalSC as the primary candidate for being the cell of origin,byunderlying the crucial importance of microenvironmental sig-nals,and by explaining tumor heterogeneity within the con-text of a clonally evolved CSC model[7,10].The intestinal homeostasis is under the surveillance of a com-plex crosstalk network of evolutionary conserved pathways,such as Wnt,Notch,and Hedgehog,which control the balancebetween proliferation,differentiation,migration,and renewal.The Wnt pathway is responsible for endoderm formation andexerts fundamental role in crypt development,maintenance,and proliferation,as it is depicted by the failure of Wnt knock-out mice to develop colonic crypts[8,18,32].C-myc,cyclinD1,and Lgr-5are included among its various targets.A Wntgradient loss of expression from the base to the top is closelyrelated with differentiation and expression of the ephrin familyproteins,which regulate positioning[5].Mutations in the APCgene(80%in sporadic cancer),b-catenin,or the regulatory pro-teins in the Wnt pathway result in constant activation[18].This may lead to uncontrolled proliferation,a shift from asym-metrical to symmetrical divisions,and augmented survival.Wnt signaling is also involved in the process of epithelial tomesenchymal transition(EMT)and invasion[7,8].Notch maydrive tumorigenesis,because it potentiates proliferation andinhibits differentiation[10].BMP and TGF-b belong to a fam-ily of ligands whose receptors interact with the intracellularcascade of the Smad proteins[33].BMPs are mostly expressedby stromal cells,have opposing actions to Wnt,and are mostlyactive at the top of the crypt.In the crypt bottom,they are alsoproduced,but they are kept inactive by binding to specificinhibitors[7,16].TGF-b is an inhibitor of intestinal epithelialcell proliferation and inducer of apoptosis[3,31,34].TheHedgehog proteins carry signals between stromal and epithelialcells.Although it seems that Hedgehog acts as a Wnt suppres-sor,probably through BMP,and is also expressed byþ4posi-tion stem-like cells,its role remains elusive[7].Finally,incolorectal carcinogenesis,activation of the phosphoinositide3-kinase(PI3K)pathway results in rapid and excessive prolifera-tion of intestinal SCs[12].Like the normal SCs,CSCs reside in a qualified microenvir-onment that has gained tumor-promoting traits[35].A recip-rocal interplay between SCs and their niche is behind malig-nant transformation.Genetic or epigenetic aberrations in theSCs compartment may lead to alteration of the niche and viceversa[28,36].This tumorigenic niche is composed of trans-formed myofibroblasts,recruited myeloid cells,other celltypes,and extracellular components,which produce variousgrowth factors and cytokines,including hepatocyte growthfactor(HGF),tumor necrosis factor a(TNF-a),and interleu-kin(IL)-6,which promote dedifferentiation,carcinogenesis,and invasiveness[7,36].Although Wnt activating APC muta-tions are common in CRC,tumors often present with a heter-ogeneous Wnt activity,indicating an alternative regulation.Myofibroblast-derived HGF is probably a major enhancer ofWnt activity[7,36].Nuclear b-catenin localization,whichindicates Wnt-triggering and cancer-stemness,is predomi-nantly observed in the invasive regions of colorectal carcino-mas[37].Experimental data revealed that mice carrying anAPC mutation combined with Smad4loss,and thus unrespon-sive to differentiation-inducing microenvironmental signals,showed increased susceptibility in the formation of highlyinvasive tumors combined with extensive stromal proliferation[38].In another study,it was shown that inactivation of stro-mal BMP may also lead to extensive proliferation of both thestroma and the overlying epithelium and eventually adenomaformation.Wnt activity was increased in epithelial cells andwas under the manipulation of other stromal pathways,suchas Forkhead Box L1(FOXL1)and phosphatase and tensinhomolog(PTEN)[12].In humans,evidence that supports thisrelationship is derived from observations in patients withinflammatory bowel disease,histopathological data of stromalimmune cells,and the beneficial role of nonsteroidal anti-inflammatory drugs in CRC.The chronic inflammatory mi-lieu,composed of infiltrating macrophages,lymphocytes,andstromal cells,which produce IL-1,IL-6,TNF-a,and vascularendothelial growth factor,disturbs epithelial homeostasis andthe SC reservoir[6].It has been postulated that a normal in-testinal niche can prevent tumor growth,even if transformedSCs are present[39].Metastasis is responsible for approximately90%of cancer-associated mortality and can be divided into translocation andcolonization basically[40].As the CSC population representsthe only cells that propagate tumors,it can be extrapolatedthat these cells are responsible for metastasis formation[41,42].It is therefore a prerequisite that these cells must be ableto detach from the primary tumor,invade,access,and surviveat the circulation,disseminate at distant sites,transmigrateacross the endothelial lining of the target tissue,and form sec-ondary tumors(Fig.2)[43].A crucial step in the metastaticprocess is EMT.In this event,the simultaneous downregula-tion of the epithelial phenotype,along with enabling offibro-blast-like traits,enhances motility,invasiveness,and resist-ance to apoptosis[40,44].Cells that undergo EMT are alsoassumed to gain a stem-like phenotype[45,46].This processseems to be regulated by pathways that are linked with SCs,such as Wnt and TGF-b[28].Studies in CRCs revealed amixed epithelial(tumor center)and mesenchymal(invasivefront,EMT/stemness)phenotype in both the primary tumorand the metastasis[37,45].Removal of contextual signalingmay reverse this process[36,47].The proposed plasticity ofCSCs brings new insights in thefield,suggesting that notonly CSCs produce more differentiated descendants but alsonon-CSCs can be converted to CSCs through EMT.Thereprogramming is mediated by microenvironmental signals[7,36,47,48].To enlighten the microenvironmental-driven plas-ticity of CSCs,two models have been proposed.The intrinsicmodel suggests that certain cell population possesses CSCtraits from tumor initiation.Meanwhile,extrinsic signals,derived from recruited active stromal cells,force cells toundergo EMT and to adopt CSCs aspects[40,48].Therefore,the existence of a circulating tumor cell(CTC)with stem-likeproperties is speculated[40,49].Data from breast,lung,and 366Stem Cells inCRCcolon cancer patients indicate that not only current CTC detection techniques tend to underestimate the population of CTCs with stem-like and EMT traits but also that the pres-ence of stemness markers in the peripheral blood of cancer patients is associated with worse prognosis and recurrence [50–52].It seems that through EMT,CTCs adopt a more aggressive and SC-like phenotype.However,understanding the exact relation between EMT,CSCs,and CTCs will pro-vide additional tools for the diagnosis and therapy of cancer patients.Although CSCs have been implicated in colon carcinogenesis,their existence had not been experimentally demonstrated until recently.However,due to the complexity of their biol-ogy and unsolved technical issues,an unequivocally approved identification and isolation strategy is still a matter of debate [9,31].Experimental studies exploit basic,but not exclusive,features of CSCs,such as the long-term retention of DNA label,morphological traits,epigenetic modifications,or differ-ential gene expression [53–55].Most recently used and prom-inent techniques,such as immunohistochemistry and cell sort-ing isolation,are based on the expression of possible stemness markers [56,57].The tumorigenic potential of iso-lated cells is often evaluated by their ability to reproduce the full heterogeneous repertoire of the parent tumor when xeno-transplanted in immunodeficient mice or through colony form-ing assays [28].Certain speculations arise,however,regarding the reliability of these assays.The environment of the host or-ganism does not resemble exactly the original conditions and,additionally,cytokines and growth factors from different spe-cies may show limited affinity for their related receptors [12,26,28].The site of transplantation may also influence the ex-perimental outcome,as an orthotopic assay for colon CSCs has not been described yet.Further issues may occur due to the alteration of certain markers caused by culturing and sort-ing conditions [12,26,28].The presence of residual immune cells in the recipient organism and an altered vascular envi-ronment may influence the tumorigenic potential of injected cells [28].Several molecules have been proposed as CSC markers including CD133,CD44,CD24,CD166,Lgr-5,and ALDH-1(Table 2).CD133,a pentaspan transmembrane gly-coprotein implicated in the organization of plasma membrane [9],was first reported as a putative colorectal CSC marker in the studies of O’Brien et al.and Ricci-Vitiani et al.by inject-ing CD133positive and negative (sorted)cells in immunodefi-cient mice.Only a small subset of CD133þcells was capable of initiating tumor growth,while negative cells were not.In both studies,CD133expression was observed in normal co-lon,although at lower numbers,suggesting a possible relation between normal and cancer SCs [58,59].Following this breakthrough,several other groups investigated the expression patterns of CD133in CRC cell lines or biopsy specimens.CD133expression was independently correlated with SC potential,worse prognosis,and low survival.Moreover,its combined expression with other putative CSC markers was also evaluated [20,60-67].It seems,however,that most CD133antibodies target glycosylation-dependent epitopes [20],whose presence is related to the differentiation stage of the cell.Recent experimental data from colon and glioblas-toma cells suggest that the differential glycosylation of spe-cific epitopes may mask the presence of CD133on cells pre-viously characterized as negative [68,69].Nevertheless,data revealing that CD133is not restricted to normal or cancer SCs raised questions regarding its efficiency as a colorectal CSC marker.CD133was ubiquitously expressed in differenti-ated colonic epithelium and in tumor cells.Both CD133þ/Àisolated cells were able to form tumors when injected in mice [70].The cell adhesion molecule CD44was proposed asanFigure 2.The stem cell model of metastasis.The primary tumor releases in circulation CSCs that have underwent EMT and possibly clonally evolved (dark purple and dark purple ovular flattened cells)due to accumulating genetic and epigenetic modifications (yellow lightning bolt).These cells travel to distant organs,where they formulate metastases.The secondary organs may provide a niche for the tumor cells.Steps 1–5(white polygons)indicate the consequent stages required for the transition from local to metastatic disease.Abbreviations:CSC,cancer stem cell;D,differentiated cell;EMT,epithelial to mesenchymal transition;P,progenitor cell.Vaiopoulos,Kostakis,Koutsilieris et al.367alternative marker.CD44þcells exhibited CSC properties,as a single cell could form a sphere and a xenograft tumor that resembled the original lesion [71].Its expression in CRC has been negatively associated with the depth of invasion,lymph node infiltration,prognosis,and survival [72].Albeit CD133and CD44seem to be promising markers,as cells expressing this protein display tumorigenic potential in vitro and in vivo,a combination of markers is likely to be more suitable for detecting colorectal CSCs [73].The high heterogeneity of human cancers forces the thorough investigation of each indi-vidual subpopulation [55].Additional markers include CD166,epithelial cell adhesion molecule,ALDH-1,CD29,CD24,CD26,Msi-1,Lgr-5,and Wnt activity/b -catenin.The presence of these molecules was associated with stemness characteristics both in vitro and in vivo,breeding tumors that resemble the original lesion and displaying increased clono-genic ability,tumorigenicity,and multilineage potential.Asso-ciations were also made with tumor stage,differentiation,invasiveness,metastasis formation,prognosis,and survival.These markers were also used for further enrichment of iso-lated CSCs to enhance their tumorigenic ability [18,21–23,36,74-90].The pluripotency genes Oct-4,Sox-2,Nanog,Lin-28,Klf-4,and c-myc are regarded as promising surrogate markers.These genes seem to facilitate a shift toward an un-differentiated state [45,91].Their expression has been associ-ated with poor prognosis,relapse,and distant recurrence,as well as with resistance to conventional chemotherapy/radio-therapy [91–93].Interestingly,the CD133negative cell lineNANK displayed tumor initiating abilities when injected in mice.Despite lacking the expression of conventional CSC markers CD133and CD44as well as the self-renewal genes Oct-4and Nanog,NANK cells expressed the developmental markers CDX2and Bmi-1[94].According to the CSC model,tumor growth is sustained by a small population of cells that current therapeutic measures fail to eradicate.Although antitumor strategies eliminate the vast majority of cancer cells,leading to a reduction in tumor size and disease remission,they fail to prevent relapse by leaving intact the CSC reservoir.On the contrary,although a CSC-tar-geted therapy will not cause tumor-size shrinkage in short term,it will prevent future regrowth and metastasis [11,95].Experimental data support the notion that CSCs are responsi-ble for resistance to chemoradiotherapy and disease relapse [51,89,93,96].Resistance is exhibited either through a shift from active state to quiescence or a wide spectrum of protec-tive mechanisms (DNA damage repair,altered cell-cycle checkpoint control,malfunction of apoptosis,drug transport-ers,and detoxifying enzymes)[29,40,97].The proposed plasticity of CSCs complicates therapeutic approaches because not only CSCs and cancer cells with CSCs traits thatoccur368Stem Cells inCRCthrough EMT are more resistant to conventional treatment but also a strategy that targets only CSCs will fail to efficiently cure CRC [47].EMT and CSC plasticity participate in the ac-quisition of both de novo and acquired drug resistance [44].It is therefore essential to renovate our therapeutic arsenal by designing new curative methods that specifically target CSCs and also solve issues that arise from CSC flexibility by elimi-nating at the same time the non-CSC population and interven-ing in the process of EMT [44,47].Successful therapeutic interventions should dispatch all proliferating cells,eradicate the CSC reservoir,and then eliminate disseminated/circulating cells including those that may have become dormant [26,95].Several issues should be taken into account during the design of CSC-directed interventions.Possible adverse reactions may occur from the impact on normal SCs,which bear resem-blance to their tumor relatives.This potential toxic effect can be minimized by targeting molecules or pathways that are preferentially active in CSCs [57].Moreover,the development of resistance along with the heterogeneous nature of tumors points to the combination of agents [97].Monoclonal antibod-ies could be directed against cell surface molecules,such as CD133,CD44,or even drug transporters.Inhibition of these molecules may result in reduction of tumor size,metastatic potential,and resistance to chemoradiotherapy [24,57].Another rational target includes blockage of various self-renewal pathways,including Wnt,Notch,PTEN,and Hedge-hog [4].Small molecular inhibitors of Wnt and c -secretase inhibitors of Notch have been suggested as novel agents against CRC [10].An alternative approach is the induction of differentiation and the disruption of EMT.Differentiation therapy forces cells to shift into a mature phenotype,lose their self-renewal abilities,and therefore become vulnerable to conventional treatment.Targeting EMT will contribute to the depletion of new CSCs that arise as products of EMT and in the blockage of drug resistance.This strategy includes:(a)alterations in signaling cascades,for example,BMP4or PI3K,(b)application of microRNAs that alter gene expression pro-files,and (c)epigenetic therapy [24,44,95].BMP promoted differentiation and apoptosis in colorectal CSCs through mod-ulations in the Wnt signaling cascade.Administration of oxa-liplatin and 5-flouroucil,which enhance BMP antitumor action,resulted in the remission of colorectal CSC-derivedxenograft tumors [10].Reversing chemoresistance and radio-resistance represents a promising proposal.This can be achieved through interference with a plethora of cellular com-ponents,including inactivation of drug transporters and DNA checkpoint kinases,depletion of reactive oxygen species scav-engers,and inhibition of signal transduction pathways [97].Recently,inhibition of the IL-4pathway with an anti-IL-4antibody or an IL-4receptor antagonist in CD133þcolorectal CSCs augmented the antitumor effects of conventional che-motherapeutics.IL-4functions in an autocrine manner,pro-moting antiapoptotic pathways [98].The ‘‘malignant’’micro-environment has been proven to be essential for the maintenance and development of CSCs.Interruption of the crosstalk network between the elements of the niche and CSCs will drive the latter in restriction of growth and loss of their metastatic capacity [4,57].Evidence from other malig-nancies supports the notion that tumor initiation and propaga-tion may be mediated,at least in part,through evasion of host immune responses [57].The application of the bisphonate zolendronate on colorectal CSCs promoted an efficient immune T-cell response [10].The understanding of the molecular mechanisms implicated in the biology of CSCs as well as the identification of specific markers,which will permit efficient isolation,may aid efforts toward targeted treatment,more efficient diagnosis,and fol-low-up of CRC patients.CSCs are rational targets for the design of interventions that will enhance responsiveness to traditional therapeutic strategies and contribute in the reduc-tion of local recurrence and metastasis.The authors indicate no potential conflicts of interest.1Jemal A,Bray F,Center MM et al.Global cancer statistics.CA Can-cer J Clin 2011;61:69–90.2Markowitz SD,Bertagnolli MM.Molecular origins of cancer:Molecu-lar basis of colorectal cancer.N Engl J Med 2009;361:2449–2460.3Lampropoulos P,Zizi-Sermpetzoglou A,Rizos S et al.TGF-beta sig-nalling in colon carcinogenesis.Cancer Lett 2012;314:1–7.4Huang EH,Wicha MS.Colon cancer stem cells:Implications for pre-vention and therapy.Trends Mol Med 2008;14:503–509.5Ricci-Vitiani L,Fabrizi E,Palio E et al.Colon cancer stem cells.J Mol Med (Berl)2009;87:1097–1104.6Boman BM,Huang E.Human colon cancer stem cells:A new para-digm in gastrointestinal oncology.J Clin Oncol 2008;26:2828–2838.7Medema JP,Vermeulen L.Microenvironmental regulation of stemcells in intestinal homeostasis and cancer.Nature 2011;474:318–326.8Vries RG,Huch M,Clevers H.Stem cells and cancer of the stomachand intestine.Mol Oncol 2010;4:373–384.9Papailiou J,Bramis KJ,Gazouli M et al.Stem cells in colon cancer.A new era in cancer theory begins.Int J Colorectal Dis 2011;26:1–11.10Todaro M,Francipane MG,Medema JP et al.Colon cancer stemcells:Promise of targeted therapy.Gastroenterology 2010;138:2151–2162.11Dalerba P,Cho RW,Clarke MF.Cancer stem cells:Models and con-cepts.Annu Rev Med 2007;58:267–284.12Davies EJ,Marsh V,Clarke AR.Origin and maintenance of the intes-tinal cancer stem cell.Mol Carcinog 2011;50:254–263.13Lopez-Garcia C,Klein AM,Simons BD et al.Intestinal stem cellreplacement follows a pattern of neutral drift.Science 2010;330:822–825.14Tian H,Biehs B,Warming S et al.A reserve stem cell population insmall intestine renders Lgr5-positive cells dispensable.Nature 2011;478:255–259.15van der Flier LG,van Gijn ME,Hatzis P et al.Transcription factorachaete scute-like 2controls intestinal stem cell fate.Cell 2009;136:903–912.16Potten CS,Gandara R,Mahida YR et al.The stem cells of small in-testinal crypts:Where are they?Cell Prolif 2009;42:731–750.17Willis ND,Przyborski SA,Hutchison CJ et al.Colonic and colorectalcancer stem cells:Progress in the search for putative biomarkers.J Anat 2008;213:59–65.18Haegebarth A,Clevers H.Wnt signaling,Lgr5,and stem cells in theintestine and skin.Am J Pathol 2009;174:715–721.19Simons BD,Clevers H.Stem cell self-renewal in intestinal crypt.ExpCell Res 2011;317:2719–2724.20Zhu L,Gibson P,Currle DS et al.Prominin 1marks intestinal stemcells that are susceptible to neoplastic transformation.Nature 2009;457:603–607.21Barker N,van Es JH,Kuipers J et al.Identification of stem cells insmall intestine and colon by marker gene Lgr5.Nature 2007;449:1003–1007.Vaiopoulos,Kostakis,Koutsilieris et al.369。