differential diagnosis in cardiac diseas
西医鉴别诊断英文版 (Differential-Diagnosis-in-Western-Medicine-1

f.recognising situations in which the working diagnosis suggests that:
responsibility for the health problems identified in a specific patient should be accepted
Objective of the module
Upon completion of this Course, students shall be able to:
1.Recognise the clinical presentation of important visceral disorders by integrating physical and historical data and identifying the pathophysiological processes responsible for the patients complaint;
2.to apply western medical terminologies in practice
3.to apply western medicine principles and diagnosis skills in diagnosis of disease,.
4.to refer to other practitioners, particularly medical practitioners, when appropriate in a timely manner,
Since there is terminology peculiar to western medicine, western medicine terminology included in the course will contribute to achievement of communication capabilities that will be important in the work force, for example, practitioner communication with patients, their families, other health professionals, regulatory bodies, herbal / acupuncture instrument suppliers and the general public effectively.
非痴呆型血管性认知功能障碍的研究进展
发现除了精神活动之外 , 即刻语言回忆能 FA ) 。通过 DTI发现所谓的白质病变并不 痴呆的患者升高 , 其可以作为有用的阴性
够很好地鉴别 V - C IND 患者和卒中后无 一定是缺血性病变 , 有些只是一些轴突脱 指标 。
认知功能损害的患者 。
失 [ 22 ] 。D TI最终也使每个传导束神经纤 5 治疗
214 日常生活功能受损 由于 V - C IND 维的数量和其所连接功能区域个数测量成
目前关于 V - C IND 的有效治疗是对
存在不同的认知功能损害 , 其日常生活能 为现实 。磁共振波谱分析 (MRS) 能提 于影响认知功能和卒中的血管性危险因素
C IND 在词语记忆方面存在很大的困难 。 和临床表现之间的关系 [21 ] 。白质病变损 的脑脊液中明显升高 , Tarkow ski等 [32 ] 研
同样 Stephens等 [13 ] 也证实与卒中后无认 害神经元通路的完整性 , 在 D TI上出现高 究表明神经丝蛋白还可能与轴索脱失 、脱
q iuyun tu@ 1261 com
再进行随访 , 发现 30%有不同程度的认 执行功能和视觉记忆方面受损 , 但是执行
·338·
功能的损害与脑白质病变 (WML ) 的严 的老年人进行研究 , 他们将接近脑室 , 且 险 。
重程度有关 , 与梗死灶的数目没有关联 。 长轴与室壁平行的白质规定为脑室周围白 412 脑脊液生物学标志物 与血清生物
- C IND ) 是由血管因素导致的认知功能 1 流行病学
者简易精神状态检查 (MM SE) 量表评分
损害的异质群体 , 其认知损害的程度尚未
目前 V - C IND 的研究受到选用标准 、 总分提高 2分 。 Ingles等 [9 ]发现影响 V -
急诊胸痛中英文双语教学

Acute Chest Pain 急性胸痛
Decision-making on Acute Chest pain at Early Stage
早期识别高危胸痛
Recognize the dangerous of acute chest pain,
especially with those life-threatening 识别胸痛的危险程度,特别是威胁生命的胸痛 Establish pain management center to offer a comprehensive range of services for patients with treatment on acute chest pain. 国外建立疼痛中心建立一系列胸痛诊疗程序
Simultaneous phenomenon of chest pain胸痛的伴随症状
Cough: trachea, bronchi and pleural diseases
胸痛常伴咳嗽:气管、支气管、胸膜疾
病所致。 Dysphagia: diseases of esophageal and mediastinum
medicine (丰富的医学基础知识) 2. Having rich clinical experience (丰富的临 床经验) 3. Master the principals of decision-making in emergency medicine (正确的急诊临床 思维)
4. Skilled techniques for emergency(娴熟的
Non-trauma 非创伤性急诊(内科、外科、
儿科 ) trauma 创伤 Disaster medicine 灾难医学 first aid 院前急救
脊髓髓内转移性肿瘤的MRI诊断及鉴别诊断
脊髓髓内转移性肿瘤的MRI诊断及鉴别诊断MR imaging diagnosis and differential diagnosis ofintramedullary spinal cord metastasisZH A N G Ji ng 1,W A N G Pei -j un 1*,Y UA N X iao -dong 2,T A N G J un -j un 1,W U Gang 1,WA N G Guo -l iang 1(1.Dep ar tment of I maging,T ongj i H os p ital of T ongj i Univ er sity ,S hanghai 200065,China;2.D ep ar tment of R adiolog y ,Chang hai H osp ital ,Shanghai 200433,China)[Abstract] Objective T o analy ze the M RI appearance o f intr amedullary spinal cor d metastasis (ISCM )and the differ ence betw een ISCM and o ther common tumor s o f inner spinal co rd for impr ov ing the know ledge o f the disease.Methods Eleven cases of ISCM wer e analyzed retr ospectively.M R ex aminations including pr e -co ntr ast and G d -DT PA enhancement wer e per -fo rmed in all the cases.Results M RI appear ance of 4cases clinically and 7cases patholog ically pro ved w ere analyzed (av er -ag e age o f onset w as 46.4?2.8y ear s).M ultiple lesions occur red in 6cases distributing in cer vical co rd,thor acic co rd,co -nus o r cauda equina.M ono -lesion occurr ed in 5cases:3o ccurr ed in conus,1occur red in cervica l co rd,1occurred in the bo undary o f cervical cor d and bulbus medullae.ISCM mainly display ed hypointensity or iso intensity on T 1WI and hetero ge -neousc hy per intensit y on T 2WI.O n co nt rast study ,all tumo rs sho wed mar ked enhancement,appearing patching ,ring -shaped,mottling and no dosity enhancement.A ffiliated sig ns included spinal co rd thickening,peripheral edema,spinal co rd cav ity et al.Conclusion M RI can w ell demo nstr ate the inner str ucture and sig nal cha racter of ISCM ,identif y the ex tension and dev elo pment of lesion,thus can contribute the diag no sis and differentia l diagnosis;how ever ISCM have no character istic manifestat ions on M RI,clinical data should be analyzed comprehensively to draw the final diag no sis.[Key words] Spinal cor d neoplasms;M etastasis;M agnetic r eso nance imag ing ;Differential diagnosis 脊髓髓内转移性肿瘤的MRI 诊断及鉴别诊断张静1,王培军1*,袁⼩东2,唐俊军1,武刚1,王国良1(1.上海同济⼤学附属同济医院放射科,上海 200065; 2.上海长海医院放射科,上海 200433)[摘要] ⽬的分析脊髓髓内转移性肿瘤(ISCM )M RI 表现及其同髓内常见肿瘤的鉴别要点,提⾼对脊髓内肿瘤的认识和诊断⽔平。
核磁共振成像MRI的一些小知识(AlittleknowledgeofMRIinMRI)

核磁共振成像MRI的一些小知识(A little knowledge of MRI in MRI)1. What is MRI?MRI is an abbreviation of the English Magnetic Resonance Imaging, or MRI. It is a new method of high-tech imaging examination in recent years, which was applied to the clinical medical imaging diagnosis of new technology in the early 1980s. It has no ionizing radiation (radiation) damage; Non-skeletal pseudo shadow; Multi-parameter imaging with multiple directions (transverse, coronal, sagittal plane, etc.); Height of soft tissue resolution; There is no need to use contrast agents to show the unique advantages of vascular structure. Therefore, it is regarded as another important development in the field of medical imaging.What is T1 and T2?T1 and 12 is organized in a certain time interval after a series of pulses to accept physical change in the characteristics of different groups have different T1 and T2, it depends on the rf pulse of the hydrogen protons on magnetic field in the organization of the reaction. By setting the MRI imaging parameters (TR and TE), TR is repeated time namely rf pulse interval, TE is applying rf pulse echo time namely from to accept to ask the time signal, TR and TE units are milliseconds (ms), can make organization Tl or T2 characteristics respectively from the images (T1 - or T2 - weighted images; t2-weighted through imaging parameters setting can also make both Tl and T2 characteristic image, called proton density weighted.3. What is the signal strength change characteristic of hematoma?The signal strength of hematoma varies with time as a result of the change in the nature of hemoglobin (e.g., oxyhemoglobin transformation into deoxyhemoglobin and orthopaemia). These characteristics help to determine the period of hemorrhage, acute hemorrhage (oxygen or deoxyhemoglobin) T1 weighted image is low signal or other signal, and subacute hematoma is high signal; Chronic hematoma is a low signal in all sequences due to the deposition of hemosiderin.4. What are the clinical applications of MRI?Mri images are very similar to CT images, both of which are "digital images" and show the anatomical and pathological cross-sectional images of different structures with different grayscale. Like CT, magnetic resonance imaging can also be applied to various systemic diseases, such as tumors, inflammation, trauma, degenerative diseases, and various congenital diseases. Magnetic resonance imaging (fmri) without bony artifact, can make more direct direction (transection, coronal, sagittal, or any Angle) layer, the brain, spinal cord and spinal anatomical and pathological changes of display, especially superior to CT, magnetic resonance imaging by its "empty effect", but without vascular contrast, showed that the vascular structures, therefore, in the "no damage" to show blood vessel (except for tiny blood vessels), as well as to the tumor, lymph node and differentiate between vascular structures, are unique. Magnetic resonance imaging (mri) has a soft tissue resolution capability that is higher than thatof CT, and it can sensitively detect changes in water content in the composition of tissues, so it can be more effective and early detection of lesions than CT. In recent years, the research of magnetic resonance blood imaging technology has made it possible to measure blood flow and blood flow rate in living organisms. Heart switch control the use of magnetic resonance imaging can clearly, fully display the heart, myocardial, pericardium, and other fine structure of the heart, for nondestructive inspection and diagnosis of acquired and congenital heart diseases, including coronary heart disease, etc.), and heart function examination, provides a reliable way. With a variety of rapid scanning sampling sequence and 3 d scanning technology research and successfully applied to clinical, magnetic resonance angiography and new technology has entered clinical film photography, and perfected. Recently, to realize the combination of the magnetic resonance imaging (fmri) and local spectroscopy (i.e., the combination of MRI and MRS), as well as other nuclei, such as fluorine except hydrogen proton magnetic resonance imaging (fmri), sodium, phosphorous, etc, these achievements will be able to more effectively improve the magnetic resonance imaging in the diagnosis of specificity, also broadened its clinical use. Main disadvantages of magnetic resonance imaging technique is needed for it to scan for a long time, so for some checkill-matched patients often difficult, organ in the sport, such as gastrointestinal tract due to lack of proper contrast agent, often show is not clear;For the lungs, the imaging effects are not satisfactory due to the low concentration of hydrogen protons in the breathing exercise and the alveolar. Mri imaging of calcification andbone lesions is not as accurate and sensitive as CT. The spatial resolution room of magnetic resonance imaging is still to be improved.1, the brain and spinal cord MRI of brain lesions, encephalitis, brain white matter lesions, cerebral infarction, cerebral CT is more sensitive than the diagnosis of congenital anomaly, etc, can be found early pathological changes, and more accurate positioning. The lesions on the base of the skull and the brain stem were more clearly visible without the artifact. MRI does not show cerebral blood vessels by contrast agent, and it is found that there are aneurysms and arteriovenous malformations. MRI can also directly display cranial nerves, which can be found in the early lesions that occur in these nerves. MRI can directly show the full appearance of the spinal cord, and therefore has important diagnostic value for spinal tumor or internal tumor of the spinal cord, leukodystrophy, spinal cord injury, spinal cord injury, etc. For disc lesions, MRI can show its denaturation, prominence, expansion or removal. It shows that the spinal canal stenosis is also better. For cervical and thoracic vertebra, CT often showed dissatisfaction, while MRI showed clearly. In addition, MRI is also very sensitive to the presentation of vertebral metastatic tumors.2. The neoplastic lesions of the head and neck MRI in the eye and ear nose and throat were shown to be good, such as the invasion of the skull base and cranial nerve by nasopharyngeal carcinoma, and the MRI showed more clearly and more accurately than the CT. MRI can also do angiography on the neck, showing abnormal blood vessels. In the neck mass, MRI can also show its range and features to help characterize it.3. Chest MRI can directly show myocardial and left ventricular cavity (heart gate control) to understand the condition of myocardial damage and determine cardiac function. The condition of the large blood vessels in the mediastinum can be clearly shown. The positioning of mediastinal tumor is also very helpful. The condition of pulmonary edema, pulmonary embolism and lung tumor can also be shown. Can distinguish the property of pleural effusion, distinguish the blood vessel section or the lymph node.4. The diagnosis of abdominal MRI on the liver, kidney, pancreas, spleen, adrenal and other substantive organ diseases can provide valuable information and help to confirm the diagnosis. Small lesions are also more likely to be shown, so early lesions can be found. MR pancreatic cholangiography (MRCP) can show biliary and pancreatic duct, which can be replaced by ERCP. MR urography (MRU) can show dilated ureteral and renal pelvis, especially for patients with renal dysfunction and IVU.5. Pelvic MRI can show the pathological changes of uterus, ovary, bladder, prostate and seminal vesicle. The endometrium and muscle layer can be seen directly, which can be helpful for early diagnosis of uterine tumor. The diagnosis of ovarian, bladder, prostate and other lesions is also very valuable.6. Posterior peritoneal MRI has great value for the tumor of the retroperitoneal membrane and the relationship with the surrounding organs. The abdominal aorta or other large vascular lesions can also be shown, such as abdominal aortic aneurysm, bu-cha syndrome, renal artery stenosis, etc.7. MRI of musculoskeletal system injury to cartilage disk, tendon and ligament in the joint, showing a higher rate than CT. Due to the sensitivity of bone marrow changes, bone metastasis, osteomyelitis, aseptic necrosis and leukemic bone marrow infiltration were detected early. The soft tissue block of bone tumor was shown clearly. There is also some diagnostic value for soft tissue injury.5. What are the advantages of MRI over CT?1. No ionizing radiation;2. Multi-azimuth imaging(cross-section, coronal plane, sagittal plane and inclined plane); The details of the anatomical structure are better; 4. More sensitive to subtle pathological changes of organizational structure (such as infiltration of bone marrow and cerebral edema); The type of the tissue (such as fat, blood and water) is determined by signal strength. 6. Organization comparison is better than CT.6. What are the types and indications of MRI contrast agent?1. Paramagnetic positive contrast agent. Commonly used Gd - DTPA (ma genevin), Mn - DPDP, etc. Its function mainly causes T1 to be shortened, and the T1 weighted image is high signal.2. Super paramagnetic substance. The most commonly used are super - paramagnetic iron oxide particles (SPIO), AMI - 25 and Resovist. Its function mainly causes T2 to be shortened,The T2 weighted image is the low signal. (2) indications: 1. Differential diagnosis of certain tumors. 2. Determine whetherthe blood-brain barrier is damaged. 3. Improve the detection rate of pathological changes.7. How to distinguish T1 weighted image from T2 weighted image?The TE and TR values of the image can be distinguished, the short can be 20ms, the length can be 80ms, the TR can be 600ms, and the length can be 3000 + ms. Short TE short TR for T1 weighted image, and TE. TR - length T2 - weighted image, short TE long TR - weighted image of proton density. Understanding the signal characteristics of water and fat helps to distinguish between a T1 weighted image and a T2 weighted image, especially if the image does not show characteristic TE and TR values. Look at liquid structures such as ventricles, arms or cerebrospinal fluid. If the liquid is bright, it is likely to be a t2-weighted image. If the liquid is dark, it may be a T1 weighted image. If the liquid is bright, and other structures are not like the t2-weighted image, and both TR and TE are short, it may be a gradient echo image.8. What are the common imaging sequences and methods used for magnetic resonance imaging?Magnetic resonance imaging is obtained by using specific imaging sequence scanning. At present, the most commonly used in clinic is the spin - echo sequence (SE sequence). Repeatedly time by changing the sequence of the TR (radio frequency) and TE (echo time) two parameters, respectively for proton density beta, T1 and T2 weighted images, three different imaging parameters of weighted images, each representing the three different kinds of magnetic resonance characteristic of theorganization, so as to distinguish the normal tissues and identify lesions. In addition, there is a reverse response sequence (IR sequence), which is obtained in this sequence, which can be heavily embodied in the T1 feature of the organization (heavy T1 weighting). The saturation response sequence (SR sequence) is the proton density plus only sequence; Partial saturation sequence (PS sequence) is a T1 - weighted sequence. None of these sequences are more popular than the SE sequence, and the applications are not widely available. The rapid imaging sequence effectively promotes the clinical application of magnetic resonance imaging. The RARE sequence introduced from west Germany, for example, is a severelyt2-weighted imaging sequence that has high sensitivity to the display of lesions. FLASH, FISH is also fast imaging sequences and their scanning imaging time in milliseconds (conventional scanning imaging time sequence, usually in seconds), therefore, to a great extent, overcome the magnetic resonance imaging (mri) scan time long Achilles' heel, for dynamic magnetic resonance imaging (mri) and magnetic resonance imaging (fmri) film photography, create the necessary conditions. For patients with magnetic resonance imaging, to avoid a paramagnetic material such as iron, such as watches, metal necklace, false teeth, metal buttons, metal ring into the examination room, because these items with a paramagnetic material, can affect the uniformity of the magnetic field, produce large no signal in the image artifacts, unfavorable to lesions of the display. Patients with pacemakers are not allowed to perform magnetic resonance imaging. The body has reserved metal shrapnel, postoperative with silver clip residues (silver clip composition may contain a small amount of paramagnetic substance), gold property in patients with fixed plate, suchas pseudarthrosis, magnetic resonance imaging to be treated cautiously, check to closely observe when necessary, the patient if there are any local discomfort, should immediately stop check, prevent the shrapnel, silver clip mobile in the high magnetic field, so that damage to nearby large blood vessels and important organization. During the mri scan, the patient must maintain a balanced breathing, reduce swallowing, and avoid autonomous or involuntary body and limb movements. For children or delirious patients who are unable to cooperate with the examination, some sedatives may be used as appropriate. During magnetic resonance imaging, still need to correctly choose layer cutting direction and different weighted imaging parameters of pulse sequence, so that as far as possible in a short time, the disease location and qualitative diagnosis of conventional for in addition to the examination of spinal column and spinal cord, most first as fast T2 weightedcross-sectional imaging, so that preliminary judge lesions and the length of the T2 values. Then, a t1-weighted coronary or sagittal plane image was further developed to determine the anatomical relationship between the lesion and its adjacent structure, and the length of T1 value of the lesion.If the above examination has not solved the problem, it can also be used as a long TR SE multiecho sequence as appropriate. The first echo of this sequence is a weighted image of proton density, and the anatomical resolution of soft tissue is higher. The fourth echo image is a T2 weighted image, which is beneficial to the comparison of tissues. The longer scan time of the multi-echo imaging sequence is its deficiency. Spine and spinal cord has walked up and down the anatomical features, appropriate to check for T2 weighted fast and SE sequencet1-weighted sagittal section imaging scans, finally can depend on is shown in suspicious lesion site, further for T2 and/or SE sequence T1 weighted imaging scans cross sectional tangent plane, to determine the characteristics of lesions and their relationship with the spinal cord, etc. An mri examination of the upper abdomen (liver, pancreas, kidney, adrenal, etc.) is suitable for an empty stomach, and the water that is drunk before the examination can make the boundary of the stomach and the left lobe of the liver and the spleen be more clearly displayed.9. What should patients prepare before an MRI exam?1. Before entering the examination room, the patient must take out all the metal objects, such as watches, keys, pens, COINS, glasses and various magnetic CARDS.2. Give moderate sedatives to infants, fidgety and melancholic patients. The abdomen examination is best empty abdomen, can serve the gastrointestinal contrast agent, also can not use. Abdominal straps may be used to reduce the pseudo shadow caused by respiratory movement.10. Which patients are not suitable for MRI scan?1. With cardiac pacemaker.2. Aneurysm after aneurysm surgery.3. Eyeball metal foreign body.4. Critically ill patients with various rescue equipment.5. Patients with various metal implants should be careful when checking.Are there any contraindications for MRI examination?The contraindication is that the patient is equipped with a magnetic susceptibility substance or device, and the loss of movement or function of these structures can cause adverse consequences. 1. Cardiac pacemaker; 2. Cochlear implant; Some artificial heart valves; 4. Skeletal growth stimulator and nerve stimulator (TENs); 5. Arterial clamp or ring; 6. Metal structure (box week); 7. Some prostheses. Prior to any MRI examination, the examination of the above contraindications is necessary for all patients. Some manufacturers have now produced non-ferromagnetic surgical clips and other devices and must consult radiologists if there is any safety problem.What is the signal strength?Signal strength according to the brightness of the signal generated by a certain organization, organization for high signal light (white), and dark organization for low signal, such as between signals, often used to judge the relationship between diseased tissue signals and its surrounding structures (such as a lump is high signal than the surrounding tissue). Note that MRI USES strength rather than density, and the concept of density is used on CT and X-ray plates。
病态窦房结综合征鉴别诊断标准
病态窦房结综合征鉴别诊断标准1.窦房结恶性病态综合征的鉴别诊断包括详细的病史询问和临床体征观察。
The differential diagnosis of sick sinus syndrome includes detailed medical history inquiry and clinical sign observation.2.心脏心电图和动态心电图对病态窦房结综合征的鉴别具有重要意义。
Electrocardiogram and Holter monitoring play a crucial role in the differential diagnosis of sick sinus syndrome.3.心脏彩色多普勒超声检查可以帮助识别病态窦房结综合征的可能原因。
Echocardiography can help identify possible causes of sick sinus syndrome.4.行心脏负荷试验可能有助于评估患者的窦房结功能。
Cardiac stress test may help evaluate the sinoatrial node function in patients.5.病态窦房结综合征的鉴别诊断需要排除其他引起类似症状的心脏疾病。
The differential diagnosis of sick sinus syndromerequires ruling out other cardiac conditions that may cause similar symptoms.6.体格检查和临床症状是病态窦房结综合征鉴别诊断的重要依据。
Physical examination and clinical symptoms are important bases for the differential diagnosis of sick sinus syndrome.7.定向电生理检查对病态窦房结综合征的诊断和评估具有重要价值。
腹部脂肪定量评估在克罗恩病中的临床应用进展

国际医学放射学杂志IntJMedRadiol2021Jan 鸦44穴1雪:72-75腹部脂肪定量评估在克罗恩病中的临床应用进展李璐梁宗辉*【摘要】克罗恩病(CD)是一种慢性非特异性炎症性肠病,其发病机制不明,可累及全胃肠道,随病程发展可出现肠道狭窄、穿孔、瘘管等多种并发症。
而脂肪组织,特别是肠系膜脂肪被认为在CD 的发病及病程进展中有重要作用,与疾病的活动性、严重程度以及预后密切相关。
目前常规CT 、能谱CT 、MRI 以及影像组学方法已用于CD 病人腹部脂肪的定量评估,对这些影像技术方法及其临床应用进展予以综述。
【关键词】克罗恩病;内脏脂肪;爬行脂肪;腹部脂肪面积中图分类号:R574;R445文献标志码:AClinical progresses in quantitative evaluation of visceral adipose tissue in Crohn ’s disease LI Lu,LIANGZonghui.Department of Radiology,Shanghai Jing ’an District Central Hospital of Fudan University,Shanghai 200040,China.Corresponding author:LIANG Zonghui,E-mail:***************.comAdvancemCrohn ’s disease (CD)is a chronic non-specific inflammatory bowel disease with unclear pathogenesis,itcan involve the entire digestive tract.As the disease progresses,multiple complications such as intestinal stenosis,perforation,and fistula may occur.Adipose tissue,especially mesenteric fat,is considered playing an important role in the pathogenesis and progression of CD.Adipose tissue is closely related to the activity,severity and prognosis of the disease.At present,conventional CT,energy spectral CT,MRI,and radiomics methods have been used for the quantitative assessment of abdominal fat in CD patients.These imaging techniques and their clinical progresses are reviewed in this article.【Keywords 】Crohn ’s disease;Visceral adipose tissue;Creeping fat;Visceral fat areaIntJMedRadiol,2021,44(1):72-75作者单位:复旦大学附属上海市静安区中心医院放射科,上海200040通信作者:梁宗辉,E-mail :***************.com *审校者基金项目:国家自然科学基金(81871423)DOI:10.19300/j.2021.Z18243综述腹部放射学克罗恩病(Crohn ’s diseases,CD )是一种可发生在全胃肠道的,以慢性炎症为特征的肠道疾病。
非痴呆型血管性认知功能障碍的结构及功能磁共振研究进展

共振新技 术如磁共振扩散张量成像 ( D T I ) 和功能磁共振 也应运 而生 , 因其易操 作性 和无创性 , 且 能 够 在 体 研 究 脑 结 构 及 脑功能方 面的改变 , 使 其 越 来 越 具 有 研 究 VC I ND 的生 理病 理 机 制 的 潜 在 性 , 本 文 就 其 在 VC I ND方 面 的研 究 进 展 进 行 综
wor ks ha v e r e c e i ve d m or e a nd mo r e a t t e nt i o n. So me n e w ma gn e t i c r e s o na nc e t e c h ni que s s uc h a s di f f us i o n t e ns o r i ma gi ng
( VCI ) . Va s c u l a r c o g n i t i v e i mp a i r me n t( VC I )i s c a u s e d b y v a s c u l a r f a c t o r s f r o m mi l d c o g n i t i v e i mp a i r me n t t o d e me n t i a s y n d r o me .S t u d i e s h a v e s h o wn t h a t t h e VC I ND c a n b e r e v e r s e d,S O i t s e a r l y i n t e r v e n t i o n h a s i mp o r t a n t s o c i a l s i g n i f i c a n c e . I n r e c e n t y e a r s ,wi t h t h e r e s e a r c h a n d a p p l i c a t i o n o f f u n c t i o n a l ma g n e t i c r e s o n a n c e ,s t u d y o f b r a i n s t r u c t u r e a n d b r a i n n e t —
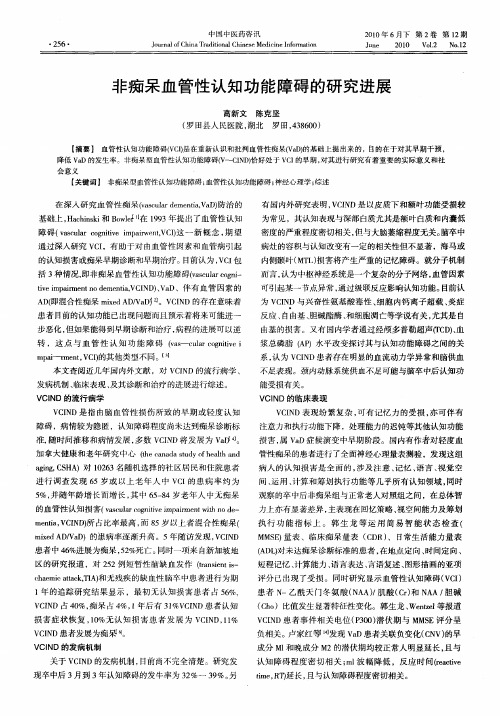
非痴呆血管性认知功能障碍的研究进展
转 ,这 点 与血 管 性 认知 功 能 障 碍 f s l r ont ei v —el giv a l c i a
m a m e t C) 他 类 型不 同 。 3 pi — n, I V 的其 【 】 本 文 查 阅近 几 年 国 内外文 献 ,对 V I D的 流 行病 学 、 CN
发病机制 、 临床表现 、 及其诊断和治疗的进展进行综述。
V N 的流 行 病学 ClD
V I D是指 由脑血 管性损伤所致 的早期或轻度认 知 CN 障碍 ,病情较为隐匿 ,认知障碍程度 尚未达到痴呆诊断标
准 , 时 间推 移 和 病 情 发 展 , 数 V I D将 发 展 为 V O 随 多 CN a 。 加 拿 大 健康 和老 年 研 究 中 心 ( e aaas d f el n t nd u y hahad hc t o t
V0 _ l 2 No 1 .2
非 痴 呆 血 管性 认知 功 能 障碍 的研 究进 展
高新 文 陈 克坚
( 田县人 民医院 , 罗 湖北
罗 田,3 6 0 4 80 )
【 摘要 】 血管性认知功能障碍(c) VI 是在重新认识和批判血管性 痴呆( a ) V D 的基础上提 出来的 , 目的在于对其早期干预 , 降低 V D的发生率。非痴呆型血管性认知功能 障碍(~cN ) a V ID恰好处于 V I C 的早期 , 对其进行研究有着重要 的实际意义和社
aigC H )对 12 3名随机选择 的社区居民和住院患者 g ,S A n 06
进行调查 发现 6 5岁 或 以 上 老 年 人 中 V I 患 病 率 约 为 C的 5 并 随年 龄 增 长 而 增 长 , 中 6 — 4岁 老 年 人 中无 痴呆 %, 其 58
《2024年老年原发性高血压患者认知功能障碍与sNFL水平的相关性研究》范文
《老年原发性高血压患者认知功能障碍与sNFL水平的相关性研究》篇一一、引言随着人口老龄化趋势的加剧,老年原发性高血压的发病率逐年上升。
高血压不仅影响心血管系统,还可能对大脑功能产生不良影响,导致认知功能障碍。
近年来,越来越多的研究开始关注血清神经元特异性烯醇化酶(sNFL)水平与认知功能之间的关系。
本研究旨在探讨老年原发性高血压患者认知功能障碍与sNFL水平的相关性。
二、研究背景与目的在过去的数十年里,众多研究报告指出,高血压与认知功能障碍之间存在密切联系。
而sNFL作为一种神经元损伤的生物标志物,在脑部损伤、神经退行性疾病及脑部肿瘤等疾病中发挥着重要作用。
因此,本研究旨在探讨老年原发性高血压患者sNFL 水平与认知功能障碍之间的关系,以期为高血压患者的早期诊断、治疗及预防提供参考依据。
三、研究方法本研究采用横断面研究设计,选取某医院老年原发性高血压患者为研究对象。
通过问卷调查、神经心理测试及血液检测等方法收集数据。
其中,神经心理测试包括蒙特利尔认知评估量表(MoCA)等,用于评估患者的认知功能;血液检测则用于测定sNFL水平。
四、研究结果1. 样本特征本研究共纳入100例老年原发性高血压患者,平均年龄为72.5±5.6岁,其中男性占60%。
所有患者均完成了神经心理测试及血液检测。
2. sNFL水平与认知功能障碍的关系研究结果显示,随着sNFL水平的升高,患者的认知功能明显下降。
其中,sNFL水平与MoCA评分之间存在显著负相关关系(P<0.05)。
表明sNFL水平越高,患者的认知功能越差。
3. 其他影响因素分析除了sNFL水平外,患者的年龄、性别、高血压病程、糖尿病史、吸烟史等因素也可能对认知功能产生影响。
然而,在本次研究中,这些因素对认知功能的影响并未达到统计学显著水平。
五、讨论本研究发现老年原发性高血压患者sNFL水平与认知功能障碍之间存在显著相关性。
sNFL作为一种神经元损伤的生物标志物,其水平的升高可能提示患者脑部神经元受损,进而导致认知功能下降。
医学英语课后翻译习题答案9-12

The brain, spine, bones, vessels, gallbladder, and uterus are termed the extraordinary or extra Fu-organs.
4.心为君主之官
The heart is considered to be the most important of all the internal organs, sometimes described as the “ruler” or “monarch” of the internal organs.
In case of little Yin deficiency, nourishing Yin and subdue Yang. In case of deficiency of both Yin and Yang, nourishing Yin and tonifying Yang.
6. 事物阴阳的属性是相对的
11.肾与膀胱相表里
The kidney has interior-exterior relationship with urinary bladder.
12.三焦主气化,通行元气、水液等
The triple jiao dominates all kinds of Qi, governs the “Qi-varying”of the human body and is pathways of Qi, fluid and foodstuff.
12 如果病人保持一个姿势时间过长, 就会出现类似“凝胶”的现象
A simillar ”gelling” phenomenon occurs when Patients remain in a single position for a prolonged period of time.
脑梗死鉴别诊断

非酮症高血糖
一例62岁女性糖尿病患者,因主观性感觉右侧上肢无力和右足运动增加 就诊,被诊断为非酮症高血糖。MRI发现左侧豆状核弥散受限(A:DWI, B:ADC)和T1高信号(C)。CT显示左侧豆状核和尾状核头高密度 (D)。
非酮症高血糖
非酮症高血糖发生于2型糖尿病患者,与新 发舞蹈病、癫痫发作和局灶性神经功能缺损 有关。影像学表现可为单侧或双侧,可被误 诊为豆纹动脉缺血性卒中。非酮症高血糖在 CT上基底节呈高密度,MRI呈T1高信号、 T2低信号和弥散受限,无相关易感效应。 T1高信号可能与反应性星形胶质细胞中的锰 有关。弥散受限的病理生理机制仍存在争议, 包括蛋白脱水、髓鞘崩解、高粘血症、微钙 化和微出血等
一例72岁男性,精神状态改变,右下肢局灶性运动性癫痫持续状态,同时存在 发热伴分泌性咳嗽。最初被诊断为双侧ACA和MCA脑梗死。 最后患者被诊断为HSV脑炎,MRI显示双侧颞叶、额叶、岛叶、扣带回和丘脑非对称性 多灶性弥散受限(A-D,DWI)、T2/FLAIR高信号(图像未提供)
单纯疱疹病毒脑炎
东部马脑炎
一例43岁男性,发热、头痛、精神状态改变2天,发病2天前曾野营。入院MRI 显示双侧基底节、丘脑和岛叶T2-FLAIR(A)高信号和轻度弥散减低(B:DWI, C:ADC),左侧重于右侧。数天后MRI显示更为广泛的基底节和岛叶皮层受累 (D:FLAIR)
东部马脑炎
这是一种蚊子传播的虫媒病毒,临床表现 可从感冒样症状、意识模糊和嗜睡,到神经 功能缺损、癫痫发作和昏迷。约5%感染导 致脑炎,1/3患者死亡,存活患者遗留明显 残疾。典型病灶出现在双侧基底节、丘脑和 脑干T2-FLAIR高信号。皮层和脑室旁白质 受累相对少见
脑肿瘤
原发性脑肿瘤可以表现为急性神经功 能缺损。有时低级别胶质瘤伴轻度水肿 效应和皮层受累可能会与亚急性脑梗死 混淆,通过无血管分布、无明显弥散受 限和脑沟强化,较易与其鉴别。但是, 亚急性梗死伴出血和高级别出血性胶质 瘤可表现为局部弥散受限、不同程度强 化和占位效应,有时难以鉴别
支原体肺炎重症感染患儿外周血RDW与心脏不良事件的关系
支原体肺炎重症感染患儿外周血RDW与心脏不良事件的关系郭柯张瑜陈若才【摘要】目的探讨支原体肺炎重症感染患儿外周血红细胞分布宽度(RDW)与住院期间主要心脏不良事件(MA C E)的关系。
方法回顾性分析89例支原体肺炎重症感染患儿的临床资料。
观察所有患儿住院期间MA C E发生情况,统计患儿血清+反应蛋白(C R P)、RDW等,分析RDW对患儿住院期间MA C E的预测价值,并采用多因素L〇gls9回归分析法分析患儿住院期间MA C E的独立影响因素。
结果89例支原体肺炎重症感染患儿住院期间有12例出现MA C E,占13. 48%,其中恶性心律失常2例(16. 67% ),心力衰竭7例(58. 33% ),再发心肌梗死3例(25. 00% );77例患儿未出现MA C E,占86. 52%。
MA C E组血清C RP、RDW显著高于非MA C E组(! <0. 05),年龄、病程、发热持续时间、红细胞沉降率等其他基线资料较非MA C E组比较差异无统计学意义(! >0. 05)。
经ROC曲线分析,结果显示RDW对支原体肺炎重症感染患儿住院期间MA C E有一定预测价值,曲线下面积为0. 719,预测最佳截断值为14. 97%,敏感度为0. 667,特异度为0. 740。
多因素 L o g istic 回归分析显示,除血清C RP(OK = 1.814,95% 1 = 1. 574 ~2. 091)外,RDW(WK = 1.246,95%1=1.137 ~ 1.365)亦是支原体肺炎重症感染患儿住院期间MA C E的独立影响因素(! <0.05)。
结论支原体肺炎重症感染患儿外周血RDW与MA C E密切相关。
【关键词】支原体肺炎;重症感染;红细胞分布宽度;主要心脏不良事件;儿童R e l^tio n s liip b e tw e e n p e rip h e ra l b lo o d R D W a n d a d ve rse c a rd ia c eve nts in c h ild r e n w it lip n e u m o n ia in fe c tio nG U O K e,Z H A N G Y u,C H E N R u o-c a iS u i x i C o u n t y H o s p i t a l,H u a i b e i,A n h u i235100,C h i n a[A b s t r a c t* O b je c tiv e To explore th e re la tio n s h ip between th e d is trib u tio n w id th o f p e riphe ral blood redblood cells (R D W)and m a jo r adverse cardiac events (M A C E)d u rin g h o spitalizatio n in c h ild re n w ith plasm a pneum oniae in fe ctio n. M e th o d s The c lin ic a l data o f 89 c h ild re n w ith severe in fe c tio n o f mycoplasm apneum onia fro m January 2015 to Decem ber 2019 were analyzed retrospectively. The occurrence dren d u rin g hosf)italizatio n was observed,general data such as serum c-reactive p ro te in( C R P) and lected ,and the pre d ictive value o f R D W to M A C E d u rin g hosjDitalization was analyzed. M u ltiv a ria te lo g istic regressionanalysis was used to analyze the independent in flu e n c in g factors o f M A C d u rin g h o spitalizatio n. R e s u lts M A C E occurred in12 cases ( 13. 48%) o f the 89 cases o f severe m ycoplasm a p n e u m o n ia,in c lu d in g 2 cases o f m a lig nan t arrh yth m ia( 16.67%),7 cases o f heart fa ilu re( 58.33%),and 3 cases o f re curre nt m yo cardia l in fa rc tio n(25.00%).M A C E was absent in77 cases,accounting fo r 86.52%. Serum CRP and R D W in the M A C E groupwere s ig n ific a n tly h ig h e r than those in the non-m ace group (!< 0. 05 ),and oth er baseline o f disease,du ra tio n o f fe v e r,and erythrocyte sedim entation rate showed no sig n ifica n t difference com pared w ith thatin the non-m ace group ( P> 0. 05 ).ROC c urve analysis showed that R D W had ce rta in pre d ictive value fo r M A C Ed u rin g h o spitalizatio n o f c h ild re n w ith severe m ycoplasm a pn e u m o n ia,w ith an area of 0. 719 u n d c u to ff value o f 14. 97%, se n sitivity o f 0.667,and s p e c ific ity o f 0. 740. M u ltiv a ria te log istic regression analysisshowed that in a d d itio n to serum CRP ( O R= 1. 814,95%C l= 1. 574 ~ 2. 091),and R D W( O R= 1. 246,95%C l=1. 137 〜1. 365) was also an independent in flu e n c in g fa cto r o f M A C E in hospitalized c h ild re n w ith severe m ycoplasm a pneum onia ( P< 0. 05 ) . C o n c lu s io n R D W is closely related to M A C E in perijDheral blood o f c h ild re n w itli severe in fe c tio n o f m ycoplasm a pneum onia.[K e y w o r d s】M ycoplasm a pneum oniae; severe in fe c tio n; red blood c e ll volum e d is trib u tio n w id th; m a jo r cardiac adverse eve n ts;ch ild re nd o i:10.3969/j.issn. 1009 -6663.2021.03.014作者单位+ 235100安徽淮北,濉溪县医院支原体肺炎重症感染属临床儿科常见疾病,据 报道,近年来其患病率呈逐年增长趋势,具有较高的 病死率!1$。
临床时间所提出问题的构建包括题目和摘要
临床时间所提出问题的构建包括题目和摘要1.背景问题(background questions):背景问题是关于疾病的一般知识问题,涉及人类健康和疾病生物、心理及社会因素等。
是源于患者和所患疾病一般性知识的回答。
2.前景问题(foreground questions):前景问题是关于处理、治疗病人专门知识问题,也涉及与治疗有关的病人生物、心理及社会因素等。
是临床医师在对患者的诊治过程中从专业角度提出的问题,涉及到疾病诊断、治疗、预防及预后的所有环节及治疗有关的病人的生物、心理及社会因素等问题的构建:一.背景问题,背景问题通常包括两个基本成分:问题词根(谁、什么、怎样、何处、何时、为什么)+动词。
一种疾病或疾病的某个方面。
例如:“我患的是什么病?”“我怎么会患这种病?”“什么引起发热?”“胰腺炎通常什么时候出现并发症?”二、前景问题前景问题包括三或四个基本成分,可按PICO原则确定:患者或问题(patient或problem,P):应包括病人的诊断及分类;干预措施(intervention,I):包括一种暴露因素、一种诊断试验、一种预后因素、一种治疗方法等;对比措施(comparison,C):与拟研究的干预措施进行对比的措施,必要时用;结局指标或测量指标(outcome,O)。
循证医学的临床问题主要是围绕着临床决策的需要,涉及到临床决策的各个方面。
归纳起来包括10个方面的内容:1、临床发现(Clinicalfinding):全面收集和合理地从病史和体格检查中发现疑点,从而提出问题。
例如,一例32岁女性,以关节肿痛为主诉的病人,在病史和体格检查中发现病人伴有严重的龋齿。
如何解释这关节肿痛与严重的龋齿的关系,提示什么?2、病因研究(病因学Etiology):如何确定疾病的原因(包括医源性的因素)。
例如,一例32岁女性的类风湿关节炎患者,治疗中出现闭经,我们需要分析是什么原因导致闭经,疾病本身还是药物,那些药物可能导致闭经?3、临床表现(Clinicalmanifestationsofdiseases):一个疾病,有多大的机会和什么时候出现其临床表现。
《神经病学》-痴呆
《神经病学》笔记-痴呆
痴呆dementia:
定义:一种以认知功能障碍为核心症状,后天获得、进行性加重的临床综合症。
老年性痴呆≥65岁。
阿尔兹海默病AD:成年后发病,与弥漫性脑萎缩有关的逐渐进展的智能障碍,是原发性神经变性性痴呆中最常见的一种类型。
特点:隐袭起病,进行性智能衰退,多伴有人格改变。
记忆障碍是其核心症状。
病因:脑内β淀粉样蛋白异常沉积。
病理:老年斑、神经原纤维缠结、广泛神经元缺失、颗粒空泡变性、血管淀粉样变。
表现:①早期(记忆障碍);②中期(计算障碍、精神障碍、人格改变);③晚期(锥体系和锥体外系体征)。
鉴别诊断:①血管性痴呆(急性起病,波动性进展或阶梯型恶化,多见卒中史,影像见血管病变,病理见脑血管病变,多为缺血性);②路易体痴呆(三主征→波动性认知功能障碍、反复发生的视幻觉、自发性锥体外系功能障碍。
病理见神经元胞浆内路易小体形成。
)
治疗:胆碱酯酶抑制剂、美金刚(中低度亲和、非竞争性NMDA受体拮抗剂)
☞。
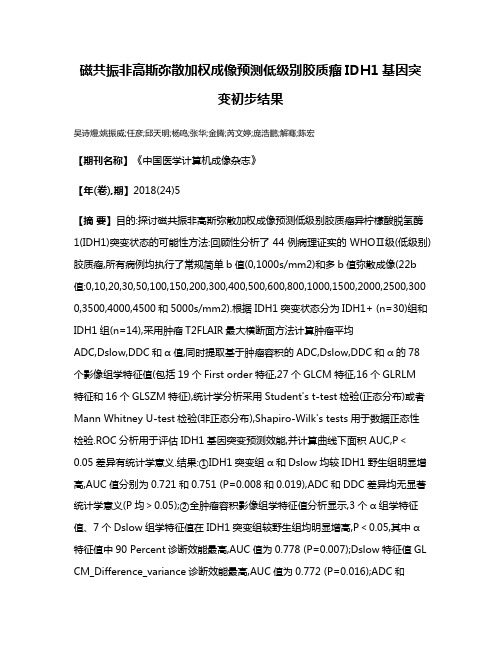
磁共振非高斯弥散加权成像预测低级别胶质瘤IDH1基因突变初步结果
磁共振非高斯弥散加权成像预测低级别胶质瘤IDH1基因突变初步结果吴诗熳;姚振威;任彦;邱天明;杨鸣;张华;金腾;芮文婷;庞浩鹏;解骞;陈宏【期刊名称】《中国医学计算机成像杂志》【年(卷),期】2018(24)5【摘要】目的:探讨磁共振非高斯弥散加权成像预测低级别胶质瘤异柠檬酸脱氢酶1(IDH1)突变状态的可能性方法:回顾性分析了44例病理证实的WHOⅡ级(低级别)胶质瘤,所有病例均执行了常规简单b值(0,1000s/mm2)和多b值弥散成像(22b 值:0,10,20,30,50,100,150,200,300,400,500,600,800,1000,1500,2000,2500,300 0,3500,4000,4500和5000s/mm2).根据IDH1突变状态分为IDH1+ (n=30)组和IDH1组(n=14),采用肿瘤T2FLAIR最大横断面方法计算肿瘤平均ADC,Dslow,DDC和α值,同时提取基于肿瘤容积的ADC,Dslow,DDC和α的78个影像组学特征值(包括19个First order特征,27个GLCM特征,16个GLRLM特征和16个GLSZM特征),统计学分析采用Student's t-test检验(正态分布)或者Mann Whitney U-test检验(非正态分布),Shapiro-Wilk's tests用于数据正态性检验.ROC分析用于评估IDH1基因突变预测效能,并计算曲线下面积AUC,P<0.05差异有统计学意义.结果:①IDH1突变组α和Dslow均较IDH1野生组明显增高,AUC值分别为0.721和0.751 (P=0.008和0.019),ADC和DDC差异均无显著统计学意义(P均>0.05);②全肿瘤容积影像组学特征值分析显示,3个α组学特征值、7个Dslow组学特征值在IDH1突变组较野生组均明显增高,P<0.05,其中α特征值中90 Percent诊断效能最高,AUC值为0.778 (P=0.007);Dslow特征值GL CM_Difference_variance诊断效能最高,AUC值为0.772 (P=0.016);ADC和DDC组学特征值在两组间差异均无统计学意义(P均>0.05).结论:磁共振非高斯弥散成像与低级别胶质瘤IDH1突变状态密切相关,Dslow和α具有预测低级别胶质瘤IDH1突变状态的潜能,IDH1野生型低级别胶质瘤比突变型具有更不均质的水分子弥散微环境.【总页数】7页(P410-416)【作者】吴诗熳;姚振威;任彦;邱天明;杨鸣;张华;金腾;芮文婷;庞浩鹏;解骞;陈宏【作者单位】复旦大学附属华山医院放射科;复旦大学附属华山医院放射科;复旦大学附属华山医院放射科;复旦大学附属华山医院神经外科;复旦大学类脑智能科学与技术研究院;复旦大学附属华山医院放射科;复旦大学附属华山医院放射科;复旦大学附属华山医院放射科;复旦大学附属华山医院放射科;复旦大学附属华山医院放射科;复旦大学附属华山医院病理科【正文语种】中文【中图分类】R445.2;R445.3【相关文献】1.低级别胶质瘤:动态磁敏感对比增强磁共振灌注成像预测肿瘤恶变和病人临床反应 [J], 章瑜;靳二虎2.脑胶质瘤IDH1基因突变HRM检测方法的初步建立 [J], 王银辉;张海燕;杨传红;张伟;赖晃文;陈晓东;王捷3.基于全肿瘤ADC图纹理特征预测术前WHO Ⅱ~Ⅲ级别胶质瘤IDH1基因表达类型效能的初步探讨 [J], 王晓青;曹梦秋;所世腾;张远大;张晓华;周滟4.人低级别胶质瘤IDH1基因突变与临床病理参数的关系 [J], 薛晶;桑伟;王嵌;苏丽萍;高海霞;张巍5.体素内不相干运动扩散加权成像预测脑胶质瘤IDH1基因突变的价值 [J], 冯盼盼;王超超;董海波;李亚迪;王洪财;梁良因版权原因,仅展示原文概要,查看原文内容请购买。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
CHF In Newborn
Impede Return of Flow to Left Heart
Infantile coarctation Congenital aortic stenosis Hypoplastic left heart syndrome Congenital mitral stenosis Cor triatriatum Obstruction to venous return from lungs
7. Hypoplastic left heart
8. Coarctation of the aorta 9. TAPVR with infradiaphragmatic obstruction
What’s left
Left-to-right shunts
ASD PDA
Truncus arteriosus
Cyanosis With Decreased Vascularity
Tetralogy
Truncus-type IV Tricuspid atresia* Transposition* Ebstein's
* Also appears on DDx of Cyanosis with Vascularity
Causes of Pericardial Effusion 7
● 1.Viral pericarditis
● 2.Collagen-vascular disease, e.g. lupus ● 3.Uremia
● 4.TB
● 5.Trauma
● 6.Post myocardial infarction
Causes of Congestive Heart Failure 6
1.Coronary artery disease
2.Hypertension 3.Cardiomyopathy 4.Valvular lesions – AS, MS
5.Left-to-right shunts
● 1.Alcoholism
● 2.Coronary artery disease ● 3.Collagen-vascular disease ● 4.Myocarditis – e.g. rheumatic ● 5.Amyloidosis ● 6.Nutritional – e.g. Beriberi
6.Fluid overload
Causes of Marked of Cardiac Silhouette 3
● 1.Cardiomyopathy ● 2.Pericardial Effusion ● 3.Multiple valve disease
Causes of Cardiomyopathy 6
Bicuspid aortic valve
Most Commons
Most common type of ASD
Ostium secundum
Most common type of VSD
Membranoutype of TAPVR
Supracardiac
Cyanosis With Increased Vascularity
Truncus types I, II, III
TAPVR
Tricuspid atresia*
Transposition* Single ventricle
* Also appears on DDx of Cyanosis with Vascularity
Causes of Increased Flow Vascularity 6
● 1.Left-to-right shunts
■ 1.Atrial septal defect ■ 2.Ventricular septal defect
■ 3.Patent ductus arteriosus
■ 4.Total anomalous pulmonary venous return
TAPVR from below diaphragm
CHF In Chronologic Sequence
CHF In Newborn
Impede Return of Flow to Left Heart
Infantile coarctation Congenital aortic stenosis Hypoplastic Left Heart Syndrome Congenital mitral stenosis Cor triatriatum Obstruction to venous return from lungs
● 7.Mets
Most Commons
Most common cause of CHF in newborn
Hypoplastic left heart syndrome
Most common cause of CHF > 2 weeks
Coarctation of the aorta (infantile form)
TAPVR from below diaphragm
CHF In 2nd-3rd Week
Coarctation of the aorta Interruption of the aortic arch
CHF-later
Coarctation of the aorta –adult type
Most common L R shunt dx’d in adult
Atrial Septal Defect
Dz most commonly associated c R arch
Truncus arteriosus
Most common congenital cardiac lesion
Most common cyanotic heart disease
Tetralogy of Fallot
Most common dz associated c R arch
Tetralogy of Fallot
Most Commons
Most common L R shunt
Ventricular Septal Defect
Causes of Prominence of the Thoracic Aorta 7
1.Hypertension (entire) 2.Atherosclerosis (entire) 3.Aortic insufficiency (entire) 4.Aortic stenosis (ascending) 5.Aneurysm (ascending or entire) 6.Coarctation of the aorta (ascending) 7.Aortitis (ascending or entire)
Types of Left-to-Right Shunts 6
●Atrial Septal defect ●Ventricular Septal Defect ●Patent ductus arteriosus
●Anomalous pulmonary venous return
●AV communis ●Anomalous origin of left coronary artery from pulmonary artery
How to Use This File
And How Not to Use It
● Use the bookmarks on the left as cues for the differentials ● Try to recite the differential without looking ● Then click on the bookmark for the answers
Most Commons
Most common cardiac tumor
Other Differential Diagnoses
Causes of Left Atrium 6
● 1.CHF
● 2.Mitral stenosis ● 3.Mitral regurgitation ● 4.Prolapsed mitral valve ● 5.Papillary muscle dysfunction ● 6.Left atrial myxoma
Cardiomegaly with Normal Vasculature
Viral myocarditis Endocardial fibroelastosis
Aberrant left coronary artery
Cystic medial necrosis
Diabetic mother
■ 5.AV communis
● 2.High-output states
Causes of Pulmonary Arterial Hypertension 4
● 1.Primary or idiopathic ● 2.Secondary to
■ 1. Lung disease – COPD, fibrosis
■ 2. Pulm. arterial dz – arteritis, multiple emboli ■ 3. Chronic hypoxia – hi altitude