3cataract surgery
白内障入院宣教流程及内容
白内障入院宣教流程及内容英文回答:Cataract is a common eye condition that affects the clarity of vision. When a patient is admitted to the hospital for cataract surgery, it is important to provide them with education and information to ensure they arewell-prepared for the procedure and recovery process. Here is a step-by-step guide on the cataract admission education process and the content that should be covered.1. Introduction and explanation of cataract: I would start by introducing myself as the healthcare provider and explaining what cataract is. I would use simple language and avoid medical jargon to ensure the patient understands. For example, I would say, "Hello, my name is [name]. I am here to help you understand cataract, which is a condition that causes clouding of the lens in your eye. This clouding can make your vision blurry or hazy."中文回答:白内障是一种常见的眼部疾病,会影响视力的清晰度。
眼科常用单词

眼科常用单词1. Eye: 眼睛2. Vision: 视力3. Optic nerve: 视神经4. Retina: 视网膜5. Cornea: 角膜6. Iris: 虹膜7. Lens: 晶状体8. Glaucoma: 青光眼9. Cataract: 白内障10. Macula: 黄斑11. Optometry: 验光12. Ophthalmology: 眼科学13. Eyeglasses: 眼镜14. Contact lenses: 隐形眼镜15. Prescription: 处方16. Eye drops: 眼药水17. Eye examination: 眼部检查18. Vision test: 视力测试19. Refraction: 屈光20. Astigmatism: 散光21. Myopia: 近视22. Hyperopia: 远视23. Presbyopia: 老花眼24. Eye surgery: 眼部手术25. Laser surgery: 激光手术26. Cataract surgery: 白内障手术27. Glaucoma surgery: 青光眼手术28. Corneal transplantation: 角膜移植29. Eye trauma: 眼外伤30. Eye infection: 眼部感染31. Conjunctivitis: 结膜炎32. Keratitis: 角膜炎33. Uveitis: 葡萄膜炎34. Optic neuritis: 视神经炎35. Macular degeneration: 黄斑变性36. Diabetic retinopathy: 糖尿病视网膜病变37. Strabismus: 斜视38. Amblyopia: 弱视39. Nystagmus: 眼球震颤40. Diplopia: 复视41. Blindness: 失明42. Eye pain: 眼部疼痛43. Eye fatigue: 眼疲劳44. Eyestrain: 眼疲劳45. Tearing: 流泪46. Red eye: 红眼47. Itchy eye: 眼睛痒48. Watery eye: 眼睛流泪49. Dry eye: 干眼症50. Eyelid twitching: 眼睑抽搐51. Eyelid edema: 眼睑水肿52. Eyelid drooping: 眼睑下垂53. Ptosis: 上睑下垂54. Entropion: 睑内翻55. Ectropion: 睑外翻56. Convergence insufficiency: 集合不足57. Exotropia: 外斜视58. Esotropia: 内斜视59. Lazy eye: 弱视眼60. Eyelashes: 睫毛61. Eyelid margin: 睑缘62. Eyelid lashes: 睑睫毛63. Eyelid reflex: 眼睑反射64. Eyelid cancer: 眼睑癌65. Eyelid hygiene: 眼睑卫生66. Eyelid surgery: 眼睑手术67. Eyelid spasms: 眼睑痉挛68. Eyelid massage: 眼睑按摩69. Eyelid wipes: 眼睑擦拭70. Eyelid stickers: 眼睑贴71. Eyelid bags: 眼睑袋72. Eyelid puffiness: 眼睑肿胀73. Eyelid twitching: 眼睑抽搐74. Eyelid eczema: 眼睑湿疹75. Eyelid fungus: 眼睑真菌感染76. Eyelid cyst: 眼睑囊肿77. Eyelid tumor: 眼睑肿瘤78. Eyelid laceration: 眼睑撕裂伤79. Eyelid trauma: 眼睑外伤80. Eyelid ulcer: 眼睑溃疡81. Eyelid abscess: 眼睑脓肿82. Eyelid edema: 眼睑水肿83. Eyelid infection: 眼睑感染84. Eyelid inflammation: 眼睑炎85. Eyelid allergy: 眼睑过敏86. Eyelid bump: 眼睑肿块87. Eyelid cancer: 眼睑癌88. Eyelid surgery: 眼睑手术89. Eyelid lift: 眼睑提升术90. Eyelid reconstruction: 眼睑重建术91. Eyelid plasty: 眼睑整形术92. Eyelid脂肪切除术: 眼睑脂肪切除手术93. Eyelid injection: 眼睑注射94. Eyelid filler: 眼睑填充物95. Eyelid tattoo: 眼睑纹身96. Eyelid makeup: 眼睑化妆97. Eyelid primer: 眼睑打底98. Eyelid liner: 眼睑眼线99. Eyelid shadow: 眼睑眼影100. Eyelid mascara: 眼睑睫毛膏。
白内障指南2021

白内障指南2021Introduction.Cataracts, the clouding of the lens of the eye, are the leading cause of blindness worldwide. Cataract surgery isthe most common surgical procedure performed globally, with over 20 million surgeries performed annually. The American Academy of Ophthalmology (AAO) and the American Society of Cataract and Refractive Surgery (ASCRS) have recently updated their guidelines for cataract surgery. These guidelines provide evidence-based recommendations for the diagnosis, management, and treatment of cataracts.Diagnosis.Cataracts are diagnosed primarily through a comprehensive eye examination. This includes a visualacuity test, slit-lamp examination, and dilated fundus examination. The symptoms of cataracts can include blurred vision, glare, difficulty seeing at night, and faded colors.Management.The primary treatment for cataracts is surgery. However, there are certain cases where observation may be appropriate. For example, cataracts that are small and do not cause significant visual impairment may not require immediate surgery.Surgery.Cataract surgery involves removing the clouded lens of the eye and replacing it with an artificial lens implant. There are several different techniques for cataract surgery, including phacoemulsification, extracapsular cataract extraction, and laser cataract surgery. The choice of surgical technique depends on the individual patient'sneeds and preferences.Postoperative Care.After cataract surgery, patients will need to followspecific instructions for postoperative care. This may include using eye drops, wearing an eye patch, and avoiding strenuous activity. Most patients will experience a significant improvement in their vision within a few days after surgery.Conclusion.Cataract surgery is a safe and effective procedure that can significantly improve vision. The AAO and ASCRS guidelines provide evidence-based recommendations for the diagnosis, management, and treatment of cataracts.中文回答:2021年白内障指南。
介绍眼睛手术的英语作文
介绍眼睛手术的英语作文Eyes are the windows to the soul, but sometimes they need a little help to see clearly. Eye surgeries are medical procedures that can correct vision problems and improve the quality of life for many individuals.One common eye surgery is LASIK, which stands for Laser-Assisted in Situ Keratomileusis. This procedure reshapes the cornea using a laser to correct refractive errors like myopia, hyperopia, and astigmatism. LASIK is quick, with mostsurgeries taking only about 10 minutes per eye.Cataract surgery is another essential procedure, particularly for older adults. A cataract is a clouding ofthe eye's natural lens, which can cause vision to become blurry. During cataract surgery, the cloudy lens is removed and replaced with an artificial one, restoring clear vision.Glaucoma, a condition that can lead to vision loss, is treated with various surgical options. One such option is a trabeculectomy, which creates a new drainage pathway for the eye's fluid to lower pressure within the eye and preventfurther damage.Strabismus surgery corrects misaligned eyes, where the eyes do not look in the same direction simultaneously. This surgery adjusts the muscles that control eye movement,helping to improve both the appearance and function of theeyes.Retinal detachment surgery is a critical procedure for those experiencing a separation of the retina from the back of the eye. If left untreated, this condition can lead to permanent vision loss. The surgery involves reattaching the retina to prevent further complications.Post-operative care is vital after any eye surgery. Patients are usually advised to avoid rubbing their eyes, follow a prescribed medication regimen, and attend follow-up appointments to monitor healing and vision improvement.In conclusion, eye surgeries are an integral part of modern medicine, offering solutions to a variety of vision problems. With advancements in technology and techniques, these procedures continue to become safer and more effective, enhancing the lives of those who undergo them.。
眼的屈光和调节晶状体病
40-45million blindness,46% ?
55~60 3.9-10% 65~74 14.3 -23.5% >75 38.8-45.9%
The Beaver Dam Eye Study Baltimore Eye Study
白内障的定义
Definition of Cataract
Cataract is the turbid lens. That is, opacity of the lens of the eye, causing impairment of vision or blindness.
The light is strongly scattered by the opacity
视功能
Visual functional examination
Visual acuity
视力
Contrast sensitivity test
Macular function test
Visual electrophysiology test
对比敏感度 黄斑功能检查 视觉电生理检查
The lens is transparent and biconvex. The lens can be divided into three parts: nucleus, cortex, capsular bag. The normal lens is an avascular structure with no blood supply or lymphatic channels.
膨胀期白内障 Intumescent Stage
晶状体体积增大
瞳孔阻滞
前房变浅,房角关闭
眼科词汇中英文对照要点

v眼科词汇中英文对照A型超声图A-scan ultrasonographyB型超声图Maddox杆测验白内障Nd:Y AG激光囊切开术SRK公式,人工晶体状体度数测定二期人工晶状体植入术人工晶状体(IOL)上皮上皮水肿子午线晶状体干燥性角结膜炎无前房或浅前房无晶状体无晶状体眼镜无缝线白内障手术毛果芸香碱出血外伤性白内障外眼病外眼检查对比敏感度平坦部玻璃体切除术白内障手术白内障囊内摘除术(ICCE)白内障囊外摘除术(ECCE)皮质皮质性白内障皮质类固醇先天性白内障全身麻醉关节炎后房后房型人工晶状体后囊混浊地塞米松异物成熟期白内障红光反射老年性白内障冷冻器B—scan ultrasonographymaddox rod testingcataractNd:YAG laser capsulotomySRK formula, for IOL powersecondary intraocular lensintraocular lensesepitheliumepithelial edemameridianslenskeratoconjunctivitis siccaflat or shallow anterior chamberAphakiaAphakic spectaclesNo—stitch cataract surgerypilocarpinehemorrhagetraumatic cataractsexternal eye diseaseexternal eye examinationcontrast sensitivitypars plana lensectomycataract surgeryintracapsular cataract extraction (ICCE) extracapsular cataract extraction (ECCE) cortexcortical cataractscorticosteoridscongenital cataractsgeneral anesthesiaArthritisposterior chamberposterior chamber intraocular lenses posterior capsular opacification dexamethasoneforeign bodiesmature cataractsred reflexAge-related cataractsCryoprobe局部麻醉折叠式人工晶状体角巩膜切口角膜角膜水肿角膜曲率计角膜病变赤道周边部虹膜切除术屈光屈光不正表面麻醉视力视网膜色素变性视网膜脱离视轴青光眼青光眼斑点前房前房积血复视,单眼性玻璃体穿孔伤穿通伤结合膜瓣结膜切口脉络膜上腔出血脉络膜脱离虹膜虹膜切除术剥脱综合症(假性剥脱)恶性青光眼核核性白内障缺血性调节调节幅度透明质酸钠高度近视眼婴儿期白内障接触镜检眼镜检查球后麻醉球旁(周)麻醉local anesthesiafoldable intraocular lenses corneal-scleral incisioncornealcorneal edemakeratomtrykeratoplastyequatorperipheral iridectomyrefractionrefraction errortopical anesthesiavisual acuityretinitis pigmentosaretinal detachmentoptic axisglaucomaglaukomfleckenanterior chamberhyphemadiplopia,monocularvitreousperforating injurypenetrating injury, see also Trauma conjunctival flapconjunctical incisionsuprachoroidal hemorrhagechoroidal detachmentirisiridectomyexfoliation syndrome (pseudoedfoliation)malignant glaucomanucleusnuclear cataractischemiaaccommodationamplitude of accommodationsodium hyaluronatehigh myopiainfantile cataractscontact lensesophthalmoscopyretrobulbar anesthesiaperibulbar anesthesia眼内压升高眼内异物眼内炎眼压增高眼底粘弹剂维生素缺乏黄斑功能黄斑变性黄斑囊样水肿睑板腺炎睑缘炎裂隙灯检查超声晶状体乳化术睫状阻滞睫状麻痹剂解剖碱性烧伤缩瞳剂糖尿病阿托品,弱视治疗AC/A比率,比值,调节性复辏/调节比值弱视病因极性白内障手术杯/盘比眼外肌鼻泪道系统结膜炎新生儿眼炎眼眶早产儿视网膜病变视网膜母细胞瘤剥夺性弱视视神经萎缩角膜映光法垂直肌下斜上斜视力评估垂直性偏离下直肌不全麻痹elevated intraocular pressureintraocular foreign bodies endophthalmitis increased intraocular pressurefundusviscoelasticsvitamin deficienciesmacular functionmacular degenerationcystoid macular edemameibomianitisblepharitisslit-lamp examinationultrasound for phacoemulsificationciliary blockciliary-block glaucomaanatomyalkali injuriesmioticsdiabetes mellitusatropine in amblyopia treatmentAC/A ratio, See accommodative convergence/accommodation ratio amblyopiaetiologypolarcataract surgerycup/disc ratioextraocular musclesnasolacrimal systemconjunctivitisophthalmia neonatorumorbitalretinopathy of prematurityretinoblastomadeprivation amblyopiaoptic atrophycorneal light reflexvertical rectus muscleshypotropiahypertopiavisual assessmentvertical deviationsinferior rectus muscle上斜肌垂直性非共同性同视机单眼剥夺单眼抑制单眼运动麻痹不全麻痹调节性幅辏调节性内斜对侧的复视对抗肌E图表房角切开分离性垂直性偏离幅辏,集合分散下直肌异侧一致性,同侧复视检查巩膜巩膜扣带固视(视觉)光凝硅胶管植入过敏反应脉络膜葡萄膜虹膜炎虹膜睫状体炎后马托品后葡萄膜炎后退后粘连化脓性化学烧伤黄斑变性Hering运动一致法则Hess屏法Horner综合症眼压superior oblique vertical inconitancy amblyoscopemonocular deprivationmonocular suppressionmonocular eye movementspalsy, paralysisparesisaccommodative convergence accommodative esotropia contralateraldiplopiaagonist musclesIlliterate Egoniotomydissociated vertical deviation convergencedivergenceinferior rectus muscles heteronymoushomonymousdipiopiasclerascleral bucklingfixation (visual) photocoagulationsilicon intubationallergic reactionchoroidsuvealiritisiridocyclitishomatropineposterior uveitisrecessionposterior synechiaepyogenicchemical burnsmacular degengrationHering’s law of motor correspondence Hess screen testHorner’s syndromeintraocular pressureGraves(甲状腺)眼病激光治疗(激光手术)营养障碍假性外斜假性斜视间歇性睑外翻睑下垂交替抑制角膜角膜病变角膜曲率计角膜炎角膜移植术拮抗肌睫状肌麻痹性睫状体近点近点集合近点联合运动反射痉挛泪点泪囊泪囊鼻腔吻合术泪小管类风湿性关节炎棱镜眼球震颤棱镜检查立体感觉立体视觉立体视觉检查眼睑协同肌内毗赘皮内斜屈光性后天性共同性非调节性假性内斜内旋内隐斜皮质类固醇Graves (thyroid)eye disease laser therapy (laser surgery) dystrophy pseudoexotropia pseudostrabismus intermittentectropion blepharoptosis alternating suppression corneakeratopathy keratometrykeratitiskeratoplasty antagonist muscles cycloplegicciliary bodynear point ofnear point of convergence near synkinetic reflex spasm oflacrimal puncta lacrimal sac dacryocystorhinostomy canaliculirheumatoid arthritis prismsnystagmusprism test stereoscopic perception stereopsisstereo acuity testing eyelidssynergistsepicanthusesotropiarefractiveacquiredcomitant nonaccommodative pseudoesotropiaincycloesophoria corticosteroids偏中心固视交感性眼炎前房角镜强的松角膜混浊发生率青光眼植入阀青霉素眼部护理穹窿部切口球筋膜屈光不正屈光参差性热烧伤融合感觉性和运动性双眼视觉融合性集合融合性散开沙眼上睑下垂上直肌失明视交叉视力评估视盘视神经萎缩视神经炎视网膜遗传性全身病视网膜出血视网膜对应视网膜竞争视网膜色素变性同向运动瞳孔瞳孔光反射瞳孔散大瞳孔缩小托品卡胺外斜外侧直肌外伤eccentric fixation sympathetic ophthalmia gonioscopy prednisonecorneal opacityincidenceglaucoma implant procedures pencillinophthalmic carefornix incisionfascia bulbiisoametropic anisometropicthermal burnsfusionsensory and motor binocular visionfusional convergence fusional divergence trachomaptosissuperior rectusblindnessoptic chiasmvisual assessmentoptic discoptic atrophyoptic neuritisretinahereditarysystemic diseaseretinal hemorrhagesretinal correspondence retinal rivalrypigmentosaversionspupilspapillary light reflex mydriasismiosistropicamideexotropialateral rectus muscle trauma外旋外旋转外隐斜外展Worth四点检查法下斜肌下斜视下直肌霰粒肿新生儿淋球菌眼炎小梁切除术A型垂直肌无力调节缝线切口适应症新生儿眼炎眼镜调节性内斜结缔组织恶性色素上皮分离性眼位异常视网膜对应隐斜拥挤现象圆锥角膜YAG激光正位眼痣肿瘤眼球表面周边的轴长注视位置配偶肌板层角膜移植术表层角膜切除术带状疱疹单纯疱疹病毒干眼巩膜炎过敏性反应Excyclo-Extorsion (excycloduction)Exophoria AbductionWorth’s four-dot testInferior oblique muscleHypotropiaInferior rectuschalaziagonococcal ophthalmia neonatorum trabeculotomyA patternmyasthenia gravisadjustable suturesincisionindicationophthalmic neonatorumspectacleaccommodative esotropiaconnective tissuemalignantpignent epithelialdissociatedalignmentabnormal (anomalous) retinal correspondence phoria, heterophoriacrowding phenomenonkeratoconusYAG laserorthophorianevitumorsepibulbarperipheralaxial lengthgazeyoke musclelamellar keratoplastysuperficial keratectomyherpes zosterherpes simplex virusdry eyesscleritisallergic reaction虹膜切除术虹膜脱出红霉素化学烧伤环丙沙星间断缝合法碱性化学烧伤角膜磨削术角膜切开术角膜咬切器角膜移植术接触镜结膜瓣结膜结石金霉素,氯化四环素局部异体植片排斥片泪囊炎泪腺炎利福平睑板腺睑板腺炎氯霉素绿脓杆菌麦粒肿前房积血前房消失前房蓄脓强的松龙青霉菌属霰粒肿三叉神经散光色素沉着沙眼新生血管形成血管翳远视眼真菌翳状赘肉Goldmann眼底接触镜Goldmann压平眼压计Humphrey视野分析仪Maddox杆阿熙提iridectomyprolapse of iris erythromycin chemical burnsciprofloxacininterrupted suture closure technique alkaline burnkeratomileusiskeratotomycorneal puncheskeratoplastycontact lensconjunctival flapconjunctival concretions chlortetracyclineallograft rejection dacryocystitisdracyoadenitisrifampinmeibomian glandsmeibomitischloramphenicolpseudomonas aeruginosa hordeolumhyphemaflat anterior chamberhypopyonprednisolonepenicilliumchalaziontrigeminal nerveastigmatismpigmentationtrachomaneovasculariationpannushyperopiafungipterygiumGoldmann fundus contact lens Goldmann applanation tonometer Humphrey vision analyzer Maddox rodapostib等效镜度低视力助视器地形图第一焦点调节调节不足调节的近点调节反应调节范围调节范围(域)调节幅度调节痉挛调节麻痹对比敏感度干涉滤片光轴几何光学假性老视检眼镜检影镜检影镜法交叉柱镜法焦点焦度计角膜曲率计角膜移植术内皮细胞睫状肌麻痹验光界面近视近视力助视器老花棱镜棱镜度内皮细胞镜检查内皮显微镜逆动逆规散光前房角镜屈光参差屈光度屈光度人工晶体(IOL)人工晶体计算equivalent power low-vision aids topography primary focal point accommodation insufficiencynear point of accommodation responserangerange of accommodation amplitude of accommodation spasmparalysiscontrast sensitivity interferenceoptical axisgeometrical optics pseudopresbyopia ophthalmoscopy shiascopyretinoscopycross cylinderfocal pointsfocimeterkeratometerkeratoplastyendothelialcycloplegic refraction interfacesmyopianear—vision aids presbyopiaprismsprism diopterspecular microscopy specular microscopy against motionagainst-the-rule astigmatism gonioscopy anisometropiadiopteroptical powerintraocular lensesIOL calculation人工晶体曲率计算散光镜片色差试验镜片,镜片箱双眼调节雾视氩激光眼底照相机眼镜处方隐斜视主观验光柱镜柱镜度闭角型青光眼玻璃体后脱离玻璃体牵引玻璃体前脱离,挫伤性玻璃体切除术玻璃体视网膜手术巩膜加压巩膜扣带光损伤硅油激光光凝术激光治疗(激光手术)旁中心凹区色觉色盲视网膜出血视网膜色素变性视网膜色素上皮视网膜水肿视网膜脱离视网膜中央动脉视网膜中央动脉阻塞视网膜中央静脉阻塞眼科仪器眼内异物低眼压光凝术虹膜结节脉络膜脱离皮质类固醇眼内炎calculation,IOL power astigmatic lenses chromatic trial lensesbinocular amplitudefoggingargon laserfundus cameraprescribing glassesheterophoria correctionsubjective refractioncylindrical lenscylinder axisangle-closure glaucomaposterior vitreous syndromevitreous tractionanterior vitreous detachment contusion vitrectomyvitreoretinal surgerysclera indentationsclera bucklephotic damagesilicone oillaser photocoagulationlaser therapy (laser surgery)parafoveal areacolor visionachromatopsia, color blindness retinal hemorrhagesretinitis pigmentosaretinal pigment epithelium (RPE) retinal edemaretinal detachmentcentral retinal arterycentral retinal artery occlusion central retinal vein occlusion ophthalmic instrumentation intraocular foreign bodieshypotonyphotocoagulationnodules of irischoroidal detachment corticosteroidendophthalmitisCT扫描,计算机断层摄影重建术眦角倒睫眶骨折睑下垂交感性眼炎甲状腺相关性眶病变眶减压术眶内容切除术泪囊鼻腔吻合术内翻瘢痕性内眦赘皮外翻眼球摘除术眼球突出内皮营养障碍溃疡穿刺术地塞米松发育性青光眼房水甘露醇甘油高渗剂假性剥脱角巩膜撕裂伤角膜擦伤角膜穿通伤角膜异物冷冻摘出术冷冻治疗盲点毛果芸香碱囊膜切除术囊膜切开术前房角切开术青光眼斑全视网膜光凝术视神经萎缩视网膜电图视网膜中央阻塞视野检查computed tomography (CT scan) reconstructioncanthal trichiasisorbital fracturesptosissympathetic ophthalmia thyroid related orbitopathy decompression exenteration dacryocystitisentropioncicatricialepicanthusectropionenucleationexopthalmosendothelial dystrophyulcerparacentesis dexamethasone developmental glaucoma aqueousmannitolglycerinhyperosmotic agent pseudoexfoliation corneoscleral laceration corneal abrasion penetrating injury of cornea cornea foreign body cryoextraction cryotherapyblind spotpilocarpine capsulectomy capsulotomygoniotomy glaukomflecken panretinal photocoagulation optic atrophy electroretinogram (ERG)central retinal vein occlusion perimetry视诱发电位酸烧伤缩瞳剂碳酸酐酶抑制剂通知同意书瞳孔瞳孔放大瞳孔缩小瞳孔阻滞小梁成形术小梁切除术小梁切开术小梁网眼前段巩膜外的巩膜环扎术视网膜前膜剥离视网膜切除术视网膜切开术娩核翼状胬肉visual evoked potential VEP (evoked response)acid burnsmiotics agentcarbonic anhydrase inhibitorinformed consentpupilmydriasismiosispapillary blocktrabeculoplastytrabeculectomytrabeculomytrabecular meshworkanterior segmentepiscleralscleral encircling operationpreretinal membrane peelingretinectomyretinotomynucleus deliverypterygium。
妥布霉素地塞米松滴眼液对白内障术后干眼症患者眼部症状改善情况和泪膜稳定性的影响

DOI:10.19368/ki.2096-1782.2024.05.053妥布霉素地塞米松滴眼液对白内障术后干眼症患者眼部症状改善情况和泪膜稳定性的影响蒋宁南京市六合区中医院眼科,江苏南京211500[摘要]目的探究妥布霉素地塞米松滴眼液对白内障术后干眼症患者眼部症状改善情况和泪膜稳定性的影响。
方法选取2022年7月—2023年6月南京市六合区中医院收治的98例白内障手术后发生干眼症的患者为研究对象,经电脑随机分为两组,对照组(49例)行重组牛碱性成纤维细胞生长因子眼用凝胶治疗,观察组(49例)配合运用妥布霉素地塞米松滴眼液治疗。
经过30 d的持续治疗,对比两组眼部症状、泪膜稳定性、不良反应发生情况。
结果观察组眼表疾病指数量表(Ocular Surface Disease Index, OSFI)评分和角膜荧光染色(Corneal Fiuoresence Staining Score, CFS)评分低于对照组,差异有统计学意义(P均<0.05);治疗后,观察组泪膜破裂时间、泪液分泌试验、泪膜厚度指标均优于对照组,差异有统计学意义(P均<0.05);观察组不良反应发生率为8.16%,低于对照组的12.24%,差异无统计学意义(χ2=0.446,P=0.505)。
结论妥布霉素地塞米松滴眼液能够良好治疗白内障术后干眼症患者,改善眼部症状,保持泪膜稳定。
[关键词]妥布霉素地塞米松滴眼液;白内障手术;干眼症;眼部症状;泪膜稳定性[中图分类号]R77 [文献标识码]A [文章编号]2096-1782(2024)03(a)-0053-04Effects of Tobramycin Dexamethasone Eye Drops on the Improvement of Ocular Symptoms and Tear Film Stability in Patients with Dry Eye after Cataract SurgeryJIANG NingDepartment of Ophthalmology, Nanjing Liuhe District Hospital of Traditional Chinese Medicine, Nanjing, Jiangsu Province, 211500 China[Abstract] Objective To investigate the effects of tobramycin dexamethasone eye drops on the improvement of ocular symptoms and tear film stability in patients with dry eye after cataract surgery. Methods A total of 98 patients with dry eye after cataract surgery treated in Nanjing Lihe District Hospital of Traditional Chinese Medicine from July 2022 to June 2023 were selected as the study subjects. They were randomly divided into two groups by computer. The con⁃trol group (49 cases) received recombinant bovine basic fibroblast growth factor eye gel treatment, and the observation group (49 cases) received tobramycin and dexamethasone eye drops treatment. After 30 days of continuous treatment, the ocular symptoms, tear film stability and adverse reactions occurence of the two groups were compared. Results The ocular surface disease index (OSFI) scores and corneal fiuoresence staining (CFS) scores in the observation group were lower than those in the control group, and the differences were statistically significant (both P<0.05). After treat⁃ment, the indexes of tear film breakup time, Schirmer Ⅱtext and tear film thickness in observation group were better than those in control group, and the differences were statistically significant (all P<0.05). The incidence of adverse re⁃actions in the observation group was 8.16%, lower than 12.24% in the control group, and the difference was not statis⁃tically significant (χ2=0.446, P=0.505). Conclusion Tobramycin dexamethasone eye drops can be a good treatment for patients with dry eye after cataract surgery, promoting benign improvement of ocular symptoms and maintaining tear [作者简介] 蒋宁(1966-),男,本科,副主任医师,研究方向为白内障。
前房巨眼白内障手术及特殊考虑说明书

Cataract surgery and anterior megalophthalmos:Custom intraocular lens and special considerationsFabio Marques Vaz,MD,Robert H.Osher,MDWe report a patient who presented with anterior megalophthalmos:corneal diameter of nearly17.0mm,anterior chamber depth of7.0mm,mild lens subluxation,and nuclear sclerotic cataract.Surgical management consisted of a scleral tunnel incision,capsule staining,a predeterminedcapsulorhexis size,microcoaxial phacoemulsification with torsional ultrasound,and implantationof a custom IOL to ensure endocapsular fixation.Special consideration must be given to thepatient with a very large anterior segment.J Cataract Refract Surg2007;33:2147–2150Q2007ASCRS and ESCRSAnterior megalophthalmos is a rare hereditary condi-tion with a constellation of findings that includes a hor-izontal corneal diameter greater than13.0mm (macrocornea),ciliary ring enlargement,anterior em-bryotoxon,mosaic corneal dystrophy,Krukenberg’s spindle,hyper-deep anterior chamber,iris hypoplasia, large capsular bag,and lens subluxation.1,2Cataract surgery in a megalophthalmic eye is challenging be-cause of the compromised view,cavernous chamber, unusually large dimensions that alter the surgeon’s prospective,thin peripheral cornea,and loose zonules. If each hurdle of the procedure is overcome,the surgeon must still confront a large lens that may lead to decentration of a standard intraocular lens(IOL) implanted in the capsular bag.We report a surgical approach using a scleral tunnel incision,estimation of the capsulorhexis size,capsule staining,slow-motion microcoaxial phacoemulsification with torsional ultrasound,and a custom IOL designed for this very large eye.CASE REPORTA43-year-old physician was referred with bilateral gradual loss of vision.On examination,the best corrected visual acu-ity(BCVA)was20/160in the right eye and20/40in the left eye;the refractive error wasÀ4.75C2.50Â104andÀ3.25 C3.50Â75,respectively.The corneal diameter was16.25mm in the right eye and16.50mm in the left eye(Figure1). Mosaic corneal dystrophy and posterior crocodile shagreen with dense Krukenberg’s pigmentary spindles were present (Figure2).The anterior chambers were cavernous(Figure3), and each pupil measured7.0mm in ambient light.The pu-pils were slightly eccentric,with atrophy of the iris stroma and multiple transillumination defects.Each lens showed moderate nuclear sclerosis;the left lens was mildly sublux-ated(Figure4).Gonioscopy revealed dense pigmentation on the trabecular meshwork.The ocular motility,visual fields,intraocular pressures,and fundi were unremarkable. Pachymetry was421m m in the right eye and424m m in the left eye.Keratometry measurements were41.00/43.27@112 and40.81/43.49@82,respectively.With the IOLMaster (Carl Zeiss Meditec),the anterior chamber depth was 6.9mm in the right eye and6.7mm in the left eye;the axial length was28.09mm and27.69mm,respectively.Ultra-sound biomicroscopy was unavailable.Because of the very large anterior segment dimensions, IOL companies were canvassed for assistance in designing a custom IOL for this patient.With assistance from Nick Ma-malis,MD,an IOL with a7.0mm optic and an overall length of16.0mm was designed.Bausch&Lomb volunteered to manufacture the IOL in a3-piece design with a silicone optic and a power of C11.00diopters.The first eye was scheduled for surgery to be followed by the second eye several months later.Using a retrobulbar block in the first eye and topical anes-thesia in the second eye,a4.0mm3-plane scleral tunnel in-cision was constructed.The anterior chamber was enteredAccepted for publication July26,2007.From the Hospital do Olho de Rio Preto and the Hospital de Olhos Jose Eutropio(Marques Vaz),Salvador,Brazil;and the University of Cincinnati(Osher),College of Medicine,and the Cincinnati Eye In-stitute,Cincinnati,Ohio,USA.Robert H.Osher,MD,is a paid consultant to Alcon,AMO,and Bausch&Lomb.Dr.Vaz has no financial or proprietary interest in any material or method mentioned.Corresponding author:Robert H.Osher,MD,Cincinnati Eye Insti-tute,1945CEI Drive,Cincinnati,Ohio45242,USA.E-mail: *************************.with a 2.2mm diamond keratome;a vial of an ophthalmic viscosurgical device (OVD)(sodium hyaluronate 2.3%[Hea-lon5])was necessary to partially fill the chamber.The ante-rior capsule was stained with trypan blue (Vision Blue),and a caliper was used to mark a 7.0mm zone on the ing the corneal marks as a guide,the capsulorhexis was completed with a bent 22-gauge needle,followed by gentle hydrodissection.Slow-motion microcoaxial phacoemulsifi-cation with torsional ultrasound was performed (Figure 5);the cortex was removed with a silicone irrigation/aspiration tip.The posterior capsule was vacuumed,and the capsular bag was expanded with another vial of the OVD.The inci-sion was enlarged to 4.0mm,and the custom IOL was folded and inserted without difficulty (Figure 6).The OVD was removed,the pupil was constricted with acetylcholine chlo-ride (Miochol),and a 10.0horizontal suture was passed to ensure a water-tight closure.The eye was dressed with pro-phylactic pilocarpine 2%,brimonidine (Alphagan),lantano-prost (Xalatan),timolol (Timoptic 0.5%),and moxifloxacin (Vigamox).A periocular triamcinolone (Kenalog)injection (1.0cc)was given through the lower lid.Postoperatively,the BCVA improved to 20/25in the right eye and 20/25in the left eye,with a refractive error of À0.25C 2.00Â112and C 0.25C 3.00Â78,respectively.The IOLs remained well centered without pseudophacodonesis.Thepatient,who was a surgeon,was very pleased with the visual result and was able to perform endoscopies within several days of surgery.DISCUSSIONThere are several challenges in performing cataract sur-gery in patients with megalophthalmos.The incision has to be carefully constructed because the cornea in these eyes is often quite thin.Barrett reported severe leakage of a clear corneal incision despite a small phaco and stab incision (presented as a video in the Interna-tional Video Symposium of Challenging Cases and Complication Management,ASCRS Symposium on Cataract,IOL and Refractive Surgery,San Diego,California,USA,May 2004).Therefore,in our patient,we made a scleral tunnel incision and sutured it.It is noteworthy that the stab incision leaked enough to require stromal hydration in each eye.Because the corneal dystrophy and extreme anterior chamber depth may compromise visualization,we chose to stain the capsule with Vision Blue,similartoFigure 2.Mosaic corneal dystrophy inmegalophthalmos.Figure 1.Slitlamp appearance ofmacrocornea.Figure 3.Cavernous 7.0mm anteriorchamber.Figure 4.Moderate nuclear sclerosis with mild lens subluxation.2148CASE REPORT:ANTERIOR MEGALOPHTHALMOSthe case of Lee et al.,3using a 3-step technique.4How-ever,establishing the proper capsulorhexis size can be difficult when all the landmarks and dimensions are abnormal.Therefore,we used an unpublished tech-nique to determine the capsulorhexis size (Frederico Marques,MD,and Robert Osher,MD,2003):In 10pa-tients with white cataract,the anterior capsule was stained with trypan blue.Following the capsulorhexis,the excised anterior capsule was placed on the corneal surface and the ratio of the diameter of the stained ex-cised capsule to the diameter of the underlying stained intracameral capsulorhexis edge was determined.The white background of the cortex made the contrast easy to photograph,and the mean magnification was ap-proximately 20%.Therefore,a caliper was set at 7.0mm,placing 2marks on the cornea to facilitate about a 5.5mm capsulorhexis in this patient.The phacoemulsification was uneventful,although the cortical behavior was stubborn,perhaps because of the mild zonular compromise.Although capsulartension rings were available,it was not necessary to implant one in either eye,as previously reported.5The big challenge was selection of the IOL.Cases of IOL malposition with endocapsular fixation have been reported.5–8Surgeons have tried to prevent this com-plication by implanting an iris-supported Binkhorst IOL,9suturing an anterior chamber IOL,7suturing the optic or haptic to the anterior capsule and iris,10and placing an iris-clip IOL in the posterior chamber.3Kwitko et al.6experienced dislocation of a standard size posterior chamber IOL.As a result,a special Sin-skey posterior chamber IOL with an optic of 7.0mm and an overall length of 18mm was implanted in the second eye.The authors recommended using a larger IOL diameter in patients with megalocornea.We considered using an anterior or posterior optic capture technique to achieve stable centration of the IOL.11We were fortunate that Bausch &Lomb was willing to manufacture a custom IOL for this patient.Unfortunately,the process took almost 1year and the patient was unwilling to wait the same period of time for the second eye when we realized that a stron-ger power would likely achieve a residual refractive error closer to emmetropia.Nevertheless,he was pleased with the visual outcome and the IOLs have remained perfectly centered (Figure 7).In summary,special considerations must be given to the patient with megalophthalmos who requires cata-ract surgery.While a candid discussion of the increased risk is necessary,it is likely that a well-planned approach will be successful.REFERENCES1.Duke-Elder S.Anomalies of the size of the cornea:anterior meg-alophthalmos.In:Duke-Elder S,ed,System of Ophthalmology.St.Louis,MO,CV Mosby,1964;vol.3,pt 2:Normal and Abnor-mal Development;Congenital Deformities;498–505Figure 6.Insertion of custom IOL into the capsularbag.Figure 5.Slow-motion microcoaxial phacoemulsification with tor-sionalultrasound.Figure 7.Appearance of megalophthalmic eye 2months postoperatively.2149CASE REPORT:ANTERIOR MEGALOPHTHALMOS2.Skuta GL,Sugar J,Ericson ES.Corneal endothelial cell mea-surements in megalocornea.Arch Ophthalmol1983;101:51–53 3.Lee GA,Hann JV,Braga-Mele R.Phacoemulsification in ante-rior megalophthalmos.J Cataract Refract Surg2006;32:1081–10844.Marques DMV,Marques FF,Osher RH.Three-step techniquefor staining the anterior lens capsule with indocyanine green or trypan blue.J Cataract Refract Surg2004;30:13–165.De Sanctis U,Grignolo FM.Cataract extraction in X-linked meg-alocornea;a case report.Cornea2004;23:533–5356.Kwitko S,Belfort R Jr,Omi CA.Intraocular lens implantation in an-terior megalophthalmus;case report.Cornea1991;10:539–541 7.Sharan S,Billson FA.Anterior megalophthalmos in a family with3female siblings.J Cataract Refract Surg2005;31:1433–1436 8.Javadi MA,Jafarinasab MR,Mirdehghan SA.Cataract surgeryand intraocular lens implantation in anterior megalophthalmos.J Cataract Refract Surg2000;26:1687–16909.Neumann AC.Anterior megalophthalmos and intraocularlens implantation.Am Intra-Ocular Implant Soc J1984;10: 220–22210.Dua HS,Azuara-Blanco A,Pillai CT.Cataract extraction andintraocular lens implantation in anterior megalophthalmos.J Cataract Refract Surg1999;25:716–71911.Gimbel HV,DeBroff BM.Intraocular lens optic capture.J Cata-ract Refract Surg2004;30:200–206First author:Fabio Marques Vaz,MDHospital do Olho de Rio Preto and Hospitalde Olhos Jose Eutropio,Salvador,Brazil2150CASE REPORT:ANTERIOR MEGALOPHTHALMOS。
蔡司 IOLMaster 500 生物测量仪说明书

IOLMaster 500 from ZEISS Defining biometry2// RELIABILITYMADE BY ZEISSTrusting the experience of 100 million IOL power calculations.ZEISS IOLMaster 5003The IOLMaster ® from ZEISS revolutionized the field of IOL power calculations. For over a decade, wehave partnered with surgeons like you to continue improving the gold standard in biometry.More than 3 out of 4 surgeonsworldwide working with optical biometers trust theIOLMaster devices for their IOL power calculation.1More than 270 IOL modelscan be found in the User Group for Laser InterferenceBiometry (ULIB) with optimized A-constants for theIOLMaster.2More than 50,000 surgeriescontributed to enhancing IOL power calculation with theIOLMaster by providing optimized A-constants in the ULIB.2More than 100 million power calculationshave already been successfully performed with theZEISS IOLMaster.Gold standard biometry withthe ZEISS IOLMaster 5001)Leaming DV, 2010 Practice Styles and Preferences of U.S. ASCRS Members Survey 2)Haigis W, http://www.augenklinik.uni-wuerzburg.de/ulib/4Working with gold standard biometry The ZEISS IOLMaster 500 highlightsWhen you work with the ZEISS IOLMaster 500 you not only directly experience the result of continuous refinement; you also get a piece of cutting-edge technology that points the way to the future ofoptical biometry.Improving refractive outcomesExclusive formula integration, morethan 270 optimized lens constantsand unique telecentric keratometryfor refractive outcomes you can trust.3Advanced measurementof challenging eyesUp to 20 % higher measurement successratio for dense cataracts.4 Measurementalong the visual axis, even with staphyloma,pseudophakic and silicone-filled eyes.Proven toric outcomesToric outcomes proven by large numberof peer-reviewed, published scientificpapers.5Markerless toric IOL alignment Reference image capabilities, as the starting point of a game-changing,streamlined markerless toric workflow.Ease of useWell-designed user interface, plausibility checks, distance-independent measurements and speedy readings for one-of-a-kind usability and reduced chairtime.6Superb connectivity: Ties in theA-scan ultrasound Universal ultrasound interface to connect the dedicated ultrasound A-scan device for a better workflow and improved quality.3)Aristodemou P, Knox Cartwright NE, Sparrow JM, Johnston RL, Intraocular lens formula constant optimization and partial coherence interferometry biometry: Refractive outcomes in 8108 eyes after cataract surgery, J Cataract Refract Surg. 2011 Jan;37(1):50-624)Rivero L, IOLMaster Version 5 vs. Lenstar LS900, presented at 2010 AAO – MEACO Joint Meeting in Chicago, Illinois.5)Bullimore MA, The IOLMaster and determining toric IOL Power, White Paper, Carl Zeiss Meditec, 20136)Chen YA, Hirnschall N, Findl O, Evaluation of 2 new optical biometry devices and comparison with the current gold standard biometer, J Cataract Refract Surg. 2011 Mar;37(3):513-51756Improving refractive outcomes Holladay 2 integratedThe ZEISS IOLMaster 500 has the recognized Holladay 2formula on board. You can continuously minimize yourprediction error for IOL power calculation. Just enter thepostoperative refraction of your patients – all other data isautomatically fed into the Holladay 2 software calculation.Over 50,000 cataract surgeries evaluated for betterrefractive resultsThe extensive clinical experience of the ZEISS IOLMaster 500is reflected by the User Group for Laser Interference Biometry(ULIB) website. The ULIB database contains more than270 lens constants continuously optimized with over50,000 sets of patient data created with the ZEISS IOLMaster– absolutely unique in the industry.2Telecentric keratometryOnly the ZEISS IOLMaster family features distance-independent telecentric keratometry. It enables robustand repeatable measurements due to constant spot centerdistances. Thus the ZEISS IOLMaster 500 shows excellentagreement with manual keratometry while achieving superiorprecision performance, making its keratometry the mosttrusted among cataract surgeons.7Prof. Kenneth J. Hoffer, M.D.Santa Monica, USA“The IOLMaster has significantly changed the way biometry is performed and continues to do so.”2)Haigis W, http://www.augenklinik.uni-wuerzburg.de/ulib/7)Bullimore MA, Buehren T, Bissmann W, Agreement between a partial coherence interferometer and 2 manual keratometers, J Cataract Refract Surg. 2013 in press7Prof. Dr. Wolfgang HaigisWürzburg, GermanyAdvanced measurementof challenging eyesDense cataractsIn denser cataracts the ZEISS IOLMaster 500 achieves ameasurement success ratio that is up to 20 % higher thanthat of other optical biometry devices.4 The underlyingcomposite signal evaluation not only significantly increasesthe fraction of cataracts measurable with optical technology,but it also greatly increases signal-to-noise values.Post-LVC eyesThe ZEISS IOLMaster 500 includes the Haigis-L formula whichis dedicated to myopic and hyperopic post-LVC cases andis very convenient as it requires no clinical history data.8Staphyloma, pseudophakic and silicone-filled eyesEven with staphyloma, pseudophakic and silicone-filled eyesthe ZEISS IOLMaster 500 measures along the visual axis,yielding the relevant axial distance.Reliable and accurate IOL powercalculation for post-LVC patientswith the Haigis-L formula.The ZEISS IOLMaster 500 simplifies IOL power calculation for patients with prior laser vision correction.“For me, there are only few innovations which have revolutionized cataract surgery. The IOLMaster is one of them.”4)Rivero L, IOLMaster Version 5 vs. Lenstar LS900, presented at 2010 AAO – MEACO Joint Meeting in Chicago, Illinois.8)Haigis W, Intraocular lens calculation after refractive surgery for myopia: Haigis-L formula. J Cataract Refract Surg. 2008 Oct;34(10):1658-63.“The reference image allows precisealignment of toric IOLs andsimplifies workflow. That s definitelythe future of cataract surgery.”Prof. Oliver Findl, M.D.Vienna, Austria89Reference ImageThe Reference Image is the starting point of amarkerless toric IOL workflow: An image of the eyeis taken along with the keratometry measurement.Both reference image and keratometry data aretransferred to the ZEISS CALLISTO eye ® computer-assisted cataract surgery system. Finally, all dataneeded for precise and markerless toric IOLalignment is injected in color and high resolutionwhere it is needed – in the eyepiece of the surgicalmicroscope from ZEISS.Automatic astigmatism detectionThe ZEISS IOLMaster 500 automatically acquiresthe Reference image in case of astigmatism.It is displayed on the report so your practice staffcan recognize the astigmatism and you can takethe treatment option of a toric IOL into account.Markerless toric IOL alignment The Reference Image for a markerless toric IOL workflow.As landmarks for intra-operative matching,small blood vessels are used.Ease of useWell-designed user interfaceThe highly intuitive ZEISS IOLMaster 500 design sets standardsin easy-to-delegate biometry. Common sources of error areeliminated through an easy-to-understand traffic light indicator.Plausibility checksWith the integrated automatic mode right-eye and left-eye valuesfor axial length and corneal radii are compared and checkedfor plausibility – providing confidence especially for challenging eyes.Automated workflowThe Dual Mode facilitates measurements of axial length andkeratometry without the need for manual interaction – minimizingacquisition and chairtime.Distance independenceThe unique distance-independent telecentric keratometry isone of the reasons for the phenomenal ease of use of theZEISS IOLMaster 500. Focusing becomes much easier.ChairtimeThe average time needed to take a reading on the ZEISS IOLMaster 500is up to 4 times faster compared to other optical devices.6 A differenceyou, your team and your patients will notice every day.“If you asked my staff which opticalbiometer they would go for,the answer would clearly be: the IOLMaster.”Prof. Sabong Srivannaboon, M.D.Bangkok, Thailand6)Chen YA, Hirnschall N, Findl O, Evaluation of 2 new optical biometry devices and comparisonwith the current gold standard biometer; J Cataract Refract Surg. 2011 Mar;37(3):513-51710IOL calculation formulas Ha igis, Hoffer® Q, Holladay 1 and 2, SRK® II, SRK® / TClinical history and contact lens fitting method forcalculation of corneal refractive power followingrefractive corneal surgeryHaigis-L IOL calculation for eyes followingmyopic / hyperopic LASIK / PRK / LASEK surgeryCalculation of phakic anterior and posteriorchamber implantsOptimization of IOL constantsInterfaces Ultrasound data linkZEISS eyecare data management system FORUM®ZEISS computer-assisted cataract surgery systemCALLISTO eye (via USB)Data interface for electronic medical record (EMR) /patient management systems (PMS)Data export to USB storage mediaExport database for Holladay IOL Consultant andHIC.SOAP ProEthernet port for network connection andnetwork printerLine voltage100 – 240 V ± 10 % (self sensing)Line frequency50 – 60 HzPerformanceconsumptionmax. 75 VALaser class1Join theCataract CommunityGet quick and easy access to clinical cases, videosand more regarding the ZEISS IOLMaster 500.Discover the latest findings in optical biometry, shareyour opinion and discuss with peers.Visit 11E N _32_010_0022I I P r i n t e d i n G e r m a n y C Z -V I /2016T h e c o n t e n t s o f t h e b r o c h u r e m a y d i f f e r f r o m t h e c u r r e n t s t a t u s o f a p p r o v a l o f t h e p r o d u c t i n y o u r c o u n t r y . P l e a s e c o n t a c t o u r r e g i o n a l r e p r e s e n t a t i v e f o r m o r e i n f o r m a t i o n . S u b j e c t t o c h a n g e i n d e s i g n a n d s c o p e o f d e l i v e r y a n d a s a r e s u l t o f o n g o i n g t e c h n i c a l d e v e l o p m e n t . I O L M a s t e r ,F O R U M a n d C A L L I S T O e y e a r e e i t h e r t r a d e m a r k s o r r e g i s t e r e d t r a d e m a r k s o f C a r l Z e i s s M e d i t e c AG . © C a r l Z e i s s M e d i t e c A G , 2016. A l l c o p y r i g h t s r e s e r v e d .Carl Zeiss Meditec AG Goeschwitzer Strasse 51–5207745 Jena Germany/iolmaster0297。
医院科室及眼科类的相关翻译
medical department/department of internal medicine:内科gastroenterology dept。
消化科nephrology dept. 肾内科cardiology dept。
心脏科surgical deparment;department of surgery:外科pediatrics department:小儿科obstetrics and gynecology department:妇产科ophtalmology department: 眼科dental department: 牙科ENT(ear—nose-throat) department: 耳鼻喉科urology department: 泌尿科dermatology department; skin department:皮肤科department of general surgery 普通外科orthopedic surgery department: 矫形外科traumatology department:创伤外科plastic surgery: 整形外科anesthesiology department:麻醉科pathology department: 病理科cardiology department:心脏病科psychiatry department:精神病科orthopedics department:骨科department of cardiac surgery:心脏外科department of cerebral surgery:胸外科neurology department:神经科neurosurgery department:神经外科thoracic surgery department:脑外科department of anus & intestine surgery 肛肠外科department of hepatobiliary surgery 肝胆外科department of traditional Chinese medicine:中医科department of infectious diseases 传染病科geriatrics department: 老人病专科hematology department:血液科department of rheumatism 风湿科department of endocrinology 内分泌科department of plastic surgery 医学整形科hepatology department:肝病专科nephrology department:肾脏科department of venereology 性病专科department of physiotherapy 理疗科electrotherapy room 电疗科heliotherapy room 光疗科wax-therapy room 蜡疗科hydrotherapy room 水疗科nuclear medicine dept。
糖尿病病人白内障超声乳化术后黄斑区视网膜厚度及视力的变化分析
[收稿日期]2018-07-30 [修回日期]2019-10-18[基金项目]安徽省卫生和计划生育委员会科研计划项目(2016QK057)[作者单位]蚌埠医学院第一附属医院眼科,安徽蚌埠233004[作者简介]赵思婕(1990-),女,硕士,住院医师.[通信作者]王剑锋,主任医师.E⁃mail:7852978@[文章编号]1000⁃2200(2019)12⁃1605⁃04㊃临床医学㊃糖尿病病人白内障超声乳化术后黄斑区视网膜厚度及视力的变化分析赵思婕,余芝红,王剑锋[摘要]目的:观察糖尿病(DM)病人白内障超声乳化摘除联合后房型人工晶状体植入术后中心黄斑区的视网膜厚度及视力的变化㊂方法:选取行白内障超声乳化联合人工晶体植入术的病人90例,其中DM 合并白内障病人45例(45眼,观察组),年龄相关性白内障病人45例(45眼,对照组)㊂分别于术前㊁术后1d㊁1周㊁1月及3月使用光学相干层析成像扫描(OCT)检查中心黄斑区的视网膜厚度(CMT)和最佳矫正视力(BCVA)㊂分析2组间及组内各时间点CMT 及视力的变化,并探讨CMT 与BCVA 之间的关系㊂结果:观察组术后1个月及3个月的CMT 较对照组均增厚(P <0.01和P <0.05);其中,观察组术后1个月的CMT 增厚达最高值(P <0.01)㊂2组手术后各时间点的logMAR BCVA 值与术前对比均呈现下降的趋势(P <0.01);观察组术后1个月和3个月的logMAR BCVA 水平均高于对照组(P <0.01)㊂观察组的术后1个月㊁3个月logMAR BCVA 与CMT 呈正相关(r =0.47㊁0.36,P <0.05),对照组的术后各时间点logMAR BCVA 与CMT 无相关性(P >0.05)㊂结论:DM 病人接受白内障超声乳化摘除联合人工晶状体植入手术后,CMT 显著增加㊂2组病人术后BCVA 虽均有改善,但部分DM 病人在随访期间出现了显著BCVA 的再次下降,可能与术后的CMT 增加有关㊂[关键词]糖尿病;白内障;超声乳化术;中心黄斑区视网膜厚度;最佳矫正视力;光学相干断层扫描[中图法分类号]R 587.1 [文献标志码]A DOI :10.13898/ki.issn.1000⁃2200.2019.12.008Analysis of the retinal thickness in macular areaand visual acuity after cataract phacoemulsification in diabetic patientsZHAO Si⁃jie,YU Zhi⁃hong,WANG Jian⁃feng(Department of Ophthalmology ,The First Affiliated Hospital of Bengbu Medical College ,Bengbu Anhui 233004,China )[Abstract ]Objective :To measure the changes the retinal thickness in macular area and visual acuity after cataractphacoemulsification combined with posterior chamber intraocular lens implantation in diabetic patients.Methods :Ninety patients treated with phacoemulsification combined with posterior chamber intraocular lens implantation,which included 45cases with diabetes mellitus complicated with cataract (45eyes,observation group )and 45cases with age⁃related cataract (45eyes,control group ),were investigated.The central macular thickness(CMT)and best corrected visual acuity(BCVA)in two groups were detected using the optical coherence tomography before operation,and after 1day,1week,1month and 3months of operation.The changes of the CMT and BCVA at each time⁃point were analyzed between two groups,and the relationship between CMT and BCVA was investigated.Results :The CMT in observation group after 1and 3months of operation thickened compared with the control group(P <0.01and P <0.05),and the most thickness of CMT in observation group was after 1month of cataract surgery(P <0.01).The post⁃operative logMAR BCVA value in two groups decreased compared with before operation(P <0.01),and the levels of logMAR BCVA in observation group were higher than that in control group after 1and 3months of phacoemulsification(P <0.01).The logMAR BCVA in observation group after 1and 3months of phacoemulsification were positively correlated with CMT(P <0.05),and there were not correlation between logMAR BCVA and CMT in control group at all postoperative time points(P >0.05).Conclusions :The CMT significantly increases indiabetic patients treated with phacoemulsification combined with posterior chamber intraocular lens implantation.The BCVA in two groups are improved,and the BCVA declines obviously in partial diabetic patients during the following⁃up,which may be related to the increasing of CMT after surgery.[Key words ]diabetes mellitus;cataract;phacoemulsification;central macular thickness;best corrected visual acuity;optical coherence tomography 引发全球可逆性致盲的主要原因是白内障,约占视力损失或盲的51%[1]㊂据各项有效实验数据报道,94%~98%的病人可以通过白内障手术提高至20/40及更好的矫正视力[2]㊂根据临床的实验研究表明,糖尿病(diabetes mellitus,DM)合并白内障5061蚌埠医学院学报2019年12月第44卷第12期的手术后视力常发生较大的波动,约有20%病人的术后视力会出现短期内的上升,而后伴随再度下降的情况[3]㊂出现此情况的可能原因是高糖㊁炎症等通过损坏黄斑结构和功能,造成视力损伤[4]㊂光学相干断层扫描(optical coherence tomography,OCT)是一种无损伤㊁高分辨率的横断面光学成像检查,已在眼科广泛使用,特别对黄斑区视网膜疾病的诊断㊁治疗后的评估与随访提供客观的依据㊂本研究使用OCT来研究超声乳化手术前后DM合并白内障病人中心黄斑区的视网膜厚度(central macular retinal thickness,CMT)的变化情况及其与视力相关性,旨在为临床上DM病人白内障术后出现视力再次下降的原因提供一定程度上的理论依据,为及时采取措施干预提供相关的参考资料㊂1 资料与方法1.1 一般资料 选取2017年在我科行单眼白内障超声乳化摘除手术联合眼内后房型人工晶状体植入术的90例病人(90眼),共分为2组㊂观察组:45例病人(45眼),均为DM同时合并白内障㊂对照组是与之年龄相匹配的白内障病人,共45例(45眼)㊂2组病人性别㊁年龄㊁合并高血压率及术前CMT值差异均无统计学意义(P>0.05)(见表1),具有可比性㊂排除标准:DM性视网膜病变2期及以上,屈光间质影响眼底检查者,晶状体核硬度超过Ⅳ级者,合并玻璃体积血,变性近视㊁青光眼㊁眼底黄斑视网膜疾病等其他眼部疾病,先前眼部手术史,重度干眼症,术前已患有黄斑水肿㊂所有病人均了解治疗的益处和风险,自愿参加此项临床试验,符合医学伦理学要求㊂表1 2组病人一般资料的比较(x±s)分组n年龄/岁男女高血压术前CMT/μm 对照组4564.8±10.6232222211.9±16.6观察组4564.0±12.021*******.6±19.7 t 0.330.18* 2.96*0.44P >0.05>0.05>0.05>0.05 *示χ2值1.2 方法 1.2.1 观察指标 (1)所有病人均在术前㊁术后1d㊁1周㊁1个月㊁3个月行眼部裂隙灯检查及散瞳后行OCT下的CMT检查㊂(2)视力执行BCVA检测,并将视力十进制转换为最小分辨单位的对数以进行统计学分析㊂1.2.2 手术方法和术后处理 手术均由同一位主任医师完成,常规行超声乳化手术联合眼内后房型人工晶状体植入㊂所有白内障核的混浊程度为Ⅱ~Ⅲ级㊂术中操作的负压设为340mmHg,超声波能量最大设定为40%~50%,流速为34mL/min,注/吸负压设置为500mmHg㊂所有病人术前及术后的处理相同㊂1.3 统计学方法 采用χ2检验㊁t检验㊁方差分析和q检验㊁wilcoxon秩和检验㊁pearson相关分析㊂2 结果2.1 2组CMT比较 观察组术后1d和1周CMT 较术前差异均无统计学意义(P>0.05),术后1个月和3个月的CMT值均显著厚于术前(P<0.01),而对照组术后各时间点CMT较术前差异均无统计学意义(P>0.05)㊂观察组术后1个月和3个月的CMT均较术后1d和1周增厚(P<0.01),术后3个月较术后1个月降低(P<0.05)㊂2组间比较:术后1个月㊁3个月,观察组CMT均比对照组厚(P< 0.01和P<0.05)(见表2)㊂2.2 2组logMAR BCVA比较 2组手术后各时间点的logMAR BCVA值与术前对比均呈现下降的趋势(P<0.01)㊂术后1个月和3个月,观察组logMAR BCVA水平均高于对照组(P<0.01)(见表3)㊂2.3 2组CMT与logMAR BCVA的相关性 2组术前的logMAR BCVA和CMT无相关性(P>0.05)㊂对照组:术前㊁术后各时间点的logMARBCVA和CMT之间无相关性(P>0.05)㊂观察组:术前和术后1d㊁1周logMARBCVA和CMT无相关性(P> 0.05),但在术后1个月㊁和3个月两者呈正相关性(P<0.05),其中,在术后1个月时两者的相关性最强(P<0.01)(见表4)㊂3 讨论 一部分DM性白内障病人会随着手术后的时间延长,其术后视力会发生先上升后下降的波动㊂研究[5]表明,黄斑部位的视网膜病变对视力的影响起主要作用,而白内障病人术后的并发症中,最不容易评估的并发症就是该部位的改变㊂眼底OCT检查是一项提供高分辨率㊁对眼内视网膜及脉络膜的结构变化提供横断面图片的诊断项目㊂可清楚显示视网膜每一层组织结构,且其重复性较好,准确度约10μm,可以定量测量出黄斑区视网膜微细结构及视网膜厚度,允许我们客观地评估6061J Bengbu Med Coll,December2019,Vol.44,No.12疾病的进展和治疗的效果㊂研究[6]发现,由于其高度的敏感性,OCT在手术后6个月仍能够清晰地显示出黄斑中心凹旁的视网膜厚度极轻微的增加㊂表2 2组术后1d㊁1周㊁1个月㊁3个月与术前CMT比较(x±s;μm)分组n术前术后1d术后1周术后1个月 术后3个月 F P MS组内对照组45211.9±16.6211.1±15.2212.2±16.8213.2±15.3 212.5±16.9 0.10>0.05261.708观察组45213.6±19.7212.8±18.7215.5±18.0231.1±25.0**△△##223.1±24.0**△△##+6.01<0.01452.556 t 0.440.480.90 4.08 2.42 P >0.05>0.05>0.05<0.01<0.05 q检验:与术前比较**P<0.01;与术后1d比较△△P<0.01;与术后1周比较##P<0.01;与术后1月比较+P<0.05表3 2组各时间点logMAR BCVA[中位数(四分位数)]的比较分组n术前术后1d术后1周 术后1个月 术后3个月H P 观察组450.7(0.6,1.0)0.2(0.2,0.2)**0.2(0.2,0.2)**0.2(0.2,0.3)**△△##0.2(0.2,0.3)**146.017<0.01对照组450.5(0.5,0.7)0.2(0.1,0.2)**0.2(0.1,0.2)**0.2(0.1,0.2)**0.2(0.1,0.2)**108.326<0.01 Z -1.57-1.58-1.86-4.46-3.38 P >0.05>0.05>0.05<0.01<0.01 wilcoxon秩和检验:与术前比较**P<0.01;与术后1d比较△△P<0.01;与术后1周比较##P<0.01表4 2组术后CMT与logMAR BCVA相关性(r)分组术前术后1d 术后1周 术后1个月术后3个月观察组-0.02-0.12-0.06 0.47**0.36*对照组0.03-0.14-0.06-0.23-0.02 *P<0.05,**P<0.01 相关研究[7]表明,超声乳化术,若手术医生经验丰富,术中前房稳定,手术经时较短,那么其术后CMT可无明显改变㊂而本研究结果显示DM病人白内障术后,CMT的增加较对照组更为明显㊂然而对于超声乳化术的DM病人来说,其术后CMT增厚的具体机制目前仍不明确㊂患有中㊁重度非增殖期甚至增殖期的T2DM并发视网膜病变(DR)病人白内障术后CMT出现显著增高[8];DR病人行白内障术后,虽然黄斑区厚度增加,但脉络膜厚度并未出现明显改变,推测可能与血-视网膜内屏障相关[9]㊂在高血糖的状态下,视网膜微循环紊乱,手术操作可致眼内循环中血浆蛋白和炎性因子的增加;然而, SETHLA等[10]在对DM病人白内障术后黄斑区的视网膜的厚度变化的实验发现,糖尿病病人体内糖化血红蛋白水平的高低与术后CMT及BCVA的变化无相关性,可能不是短期内术后黄斑水肿发生的危险因素㊂术中晶状体后囊膜的破裂,眼压不稳定,玻璃体对黄斑区视网膜的牵拉,手术显微镜的光学毒性及手术后的视网膜对外界的紫外线暴露增加等[11-12],均会致血-视网膜内屏障的完整性受损,黄斑区视网膜毛细血管通透性增加,导致黄斑囊样水肿的发生[13]㊂同时,与非DM病人相比,DM病人在行超声乳化摘除术后眼内的房水中白细胞介素㊁人单核细胞趋化蛋白-1㊁血管内皮生长因子等细胞因子的含量明显增加,表明这些因素的改变可能其与黄斑厚度相关[14]㊂本研究结果显示DM病人术后1周CMT开始增加,术后1个月最高,且术后1个月㊁3个月CMT均较术前明显增厚㊂BAKER等[4]研究发现,DM病人在行白内障超声乳化摘除术后第16周,黄斑水肿发生的病人术后视力及视敏度的提高明显低于未出现黄斑水肿的病人㊂本研究结果显示:DM合并白内障的病人从术后第1周开始,CMT值开始呈现增加的趋势,但在此阶段病人的BCVA一直保持稳定㊂而在手术后1个月后,CMT厚度呈显著式增长,在此阶段的CMT厚度为整个阶段的最高值,与此同时BCVA的下降也最为明显,这表明病人的视力与黄斑水肿呈负相关[15]㊂综上,对于需行白内障超声乳化手术的DM病人,应在手术前进行常规眼底检查㊂OCT已广泛应用于临床,它可对术后CMT的改变做出定量的检测,有助于我们对病人的术后视力情况做出评估,进一步对DM性白内障病人术后黄斑区并发症的早发现㊁早诊断㊁早治疗做出有效指导㊂对于手术前眼底情况窥不清者,手术后对眼底及时多次检查,那么对于病人术后黄斑区疾病的诊断㊁及时有效治疗及病因分析将更加有益㊂(下转第1613页)[11] WRIGHT RS,ANDERSON JL,ADAMS CD,et al.2011ACCF/AHA focused update of the guidelines for the management ofpatients with unstable Angina/Non⁃ST⁃Elevation myocardialinfarction(updating the2007guideline):a report of the AmericanCollege of Cardiology Foundation/American Heart AssociationTask Force on practice guidelines[J].Circulation,2011,123(18):2022.[12] OLEDZKI S,KORNACEWICZ⁃JACH Z,SAFRANOW K et al.Variability of platelet response to clopidogrel is not related toadverse cardiovascular events in patients with stable coronaryartery disease undergoing percutaneous coronary intervention[J].Eur J Clin Pharmacol,2017,73(9):1085.[13] SPALDING TW,LYON LA,STEEL DH,et al.Aerobic exercisetraining and cardiovascular reactivity to psychological stress insedentary young normotensive men and women[J].Psychophysiology,2004,41(4):552.[14] ZHAO Q,JI Z,LI X,et al.Analysis of the clinical value offractional flow reserve for prognosis evaluation of patients ofpercutaneous coronary intervention[J].Exp Ther Med,2018,15(1):673.[15] LIN GM,YANO Y.The role of mean blood pressure at admissionin patients undergoing primary percutaneous soronary intervention[J].Int Heart J,2016,5(5):1.[16] WELLS CC,WHOOLEY MA,KARUMANCHI SA,et al.VitaminD deficiency and cardiovascular events in patients with coronaryheart disease:data from the Heart and Soul Study[J].Am JEpidemiol,2014,179(11):1279.[17] CONZADE R,KOENIG W,HEIER M,et al.Prevalence andpredictors of subclinical micronutrient deficiency in German olderadults:results from the population⁃based KORA⁃Age study[J].Nutrients,2018,66(5):S352.[18] GIOVANNUCCI E,LIU Y,HOLLIS BW,et al.25⁃hydroxyvitaminD and risk of myocardial infarction in men:a prospective study[J].Arch Int Med,2008,168(11):1174.[19] MOZAFFARI⁃KHOSRAVI H,LOLOEI S,MIRJALILI MR,et al.The effect of vitamin D supplementation on blood pressure inpatients with elevated blood pressure and vitamin D deficiency:arandomized,double⁃blind,placebo⁃controlled trial[J].BloodPress Monit,2015,20(2):83.[20] MANN MC,EXNER DV,HEMMELGARN BR,et al.The VITAHTrial Vitamin D supplementation and cardiac autonomic tone inhemodialysis:a blinded,randomized controlled trial[J].BMCNephrol,2014,15:129.[21] CABRERA⁃SOLE RM,RIVERA LU,LUCAS CT,et al.Isolatesystolic hypertension and central pressures in elderly patients.differences between men and women with similar peripheralpressures[J].J Am Soc Hypertens,2016,10Suppl1:2. [22] WADHWANIA R.Is Vitamin D deficiency implicated inautonomic dysfunction?[J].J Pediatr Neurosci,2017,12(2):119.(本文编辑 刘璐)(上接第1607页)[参考文献][1] BOURNE RR,STEVENS GA,WHITE RA,et al.Causes of visionloss worldwide,1990-2010:a systematic analysis[J].LancetGlob Health,2013,1(6):e339.[2] DAY A,DONACHIE P,SPARROW J,et al.The Royal College ofOphthalmologists′national ophthalmology database study ofcataract surgery:Report1,visual outcomes and complications[J].Eye(Lond),2015,29(4):552.[3] REITMEIR P,LINKOHR B,HEIER M,et mon eyediseases in older adults of southern German:results from theKORA⁃age study[J].Age Ageing,2017,46(3):481. [4] BAKER CW,ALMUKHTAR T,BRESSLER NM,et al.Macularedema after cataract surgery in eyes without pre⁃operative central⁃involved diabetic macular edema[J].JAMA Ophthal,2013,131(7):870.[5] KWON SI,HWANG DJ,SEO JY,et al.Evaluation of changes ofmacular thickness in diabetic retinopathy after cataract surgery[J].Korean J Opthalmal,2011,25(4):238.[6] BIRO Z,BELLA Z,KOVACS B.Change of foveal and perifovealthickness measured by OCT after phacoemulsification and IOLimplantation[J].Eye(Lond),2008,22(1):8.[7] 杨琦,刘辉,李金瑛.OCT对白内障超乳术后黄斑厚度的研究[J].中华全科医学,2011,9(4):536.[8] COLIN J,ROBERT L,CHARLOTTE B,et al.Risk factors andincidence of macular edema after cataract surgery:a databasestudy of81984eyes[J].Opthalmology,2016,123(2):316.[9] HAMIDREZA T,MOHAMMAD S,KHOSROW J,et al.Choroidalthickness changes following cataract surgery in patients with type2diabetes mellitus[J].Current Opthalmol,2019,31:49e54. [10] SETHIA R,MEHTA PK,KOTHARI R,et al.A correlation ofglycemic index and macular thickness after phacoemulsification indiabetics[J].Delhi J Ophthalmol,2019,10(5):e107869. [11] GHARBIYA M,CRUCIANI F,CUOZZO G,et al.Maullarthickness changes evaluated with spectral domain opticalcoherence tomography after uncomplicated phacoemulsification[J].Eye(Lond),2013,27(5):605.[12] ROMERO⁃AROCA P.Targeting the pathophysiology of diabeticmacular edema[J].Diabetes Care,2010,33:2484. [13] AZZA B,EI⁃REMESSY,MOHAMED AI,et al.Neuroprotectiveand blood⁃retina barrier⁃preserving effects of cannabidiol inexperimental diabetes[J].Am J Pathol,2016,168(1):235.[14] DONG N,XU B,CHU L,et al.Study of27aqueous humorcytokines in type2diabetic patients with or without macularedema[J].PLoS One,2015,10(4):e0125329. [15] JINA V,HAN,DIPIKA V,et al.Cystoid macular oedemafollowing cataract surgery:a review[J].Clin Exper Ophthalmol,2019,47(3):e12513.(本文编辑 刘璐)。
眼科学复试专业英语词汇汇总

眼科学复试专业英语词汇汇总以下是一些常见的眼科学复试专业英语词汇:1. 眼科学 Ophthalmology2. 角膜 Cornea3. 虹膜 Iris4. 晶状体 Lens5. 视网膜 Retina6. 眼轴 Eye axis7. 近视 Nearsightedness8. 远视 Farsightedness9. 散光 Astigmatism10. 青光眼 Glaucoma11. 白内障 Cataract12. 视网膜脱离 Retinal detachment13. 黄斑病变 Macular degeneration14. 角膜溃疡 Corneal ulcer15. 结膜炎 Conjunctivitis16. 角膜炎 Keratitis17. 视力 Vision18. 矫正视力 Corrected vision19. 裸眼视力 Unaided vision20. 盲 Blindness21. 低视力 Low vision22. 屈光不正 Refractive error23. 视力检查 Vision test24. 眼压检查 Intraocular pressure test25. 视野检查 Visual field test26. 眼底检查 Fundus examination27. 眼科手术 Ophthalmic surgery28. 角膜移植 Corneal transplantation29. 白内障手术 Cataract surgery30. 青光眼手术 Glaucoma surgery31. 视网膜手术 Retinal surgery32. 视力矫正 Sight correction33. 眼镜 Glasses34. 隐形眼镜 Contact lenses35. 人工晶状体 Intraocular lens (IOL)36. 角膜塑形镜 Orthokeratology (OK) lenses37. 眼药水 Eye drops38. 眼膏 Eye ointment39. 眼部按摩 Eye massage40. 眼部护理 Eye care41. 视觉训练 Vision training42. 眼部疾病预防 Eye disease prevention43. 眼部健康 Eye health44. 眼外伤 Eye trauma45. 眼肿瘤 Eye tumor46. 眼炎 Eye inflammation。
白内障心得体会范文
白内障心得体会范文英文回答:Cataract is a common eye condition that affects many people, especially the elderly. I recently had the opportunity to undergo cataract surgery and would like to share my personal experience and insights.First and foremost, I must say that the entire process was smooth and well-organized. From the initial consultation with the ophthalmologist to the post-operative care, everything was carefully explained and executed. The medical staff were professional, friendly, and attentive, which made me feel at ease throughout the entire journey.The surgery itself was quick and painless. I was given a local anesthetic to numb my eye, and the surgeonskillfully removed the cloudy lens and replaced it with an artificial one. I could hardly feel any discomfort during the procedure, and it was over before I knew it. Theimprovement in my vision was almost immediate, and I was amazed at how clear and vibrant everything appeared.The recovery period was relatively short. I was advised to take it easy for a few days and avoid any strenuous activities. I experienced some mild discomfort and sensitivity to light initially, but these symptoms gradually subsided. Regular follow-up visits with the ophthalmologist ensured that my eye was healing properly and that my vision was improving as expected.Having gone through this experience, I have gained a deeper appreciation for the importance of regular eyecheck-ups. Cataracts can develop gradually over time, andit is crucial to detect and treat them early to prevent further deterioration of vision. I would strongly encourage everyone, especially those at higher risk, such as the elderly or individuals with certain medical conditions, to prioritize their eye health and seek professional advice if necessary.In conclusion, my experience with cataract surgery wasextremely positive. The procedure itself was painless, the recovery was smooth, and the results were remarkable. I am grateful to have regained clear vision and would highly recommend cataract surgery to anyone facing similar vision problems.中文回答:白内障是一种常见的眼部疾病,尤其常见于老年人。
白内障手术准备流程
白内障手术准备流程英文回答:Preoperative Preparation for Cataract Surgery.Cataract surgery is a common and generally safe procedure to restore vision and improve the quality of life for individuals with cataracts. However, like any surgery, cataract surgery requires careful preoperative preparation to ensure optimal outcomes and minimize complications. The following is a comprehensive guide to the preoperative preparation process for cataract surgery:Comprehensive Eye Examination.A thorough eye examination is essential before cataract surgery. This examination typically includes:Visual acuity testing to assess the level of vision impairment caused by the cataracts.Slit-lamp examination to inspect the cornea, iris, lens, and other structures of the eye.Dilated fundus examination to evaluate the retina and optic nerve.Measurement of intraocular pressure to rule out any underlying conditions.Biometry to determine the proper power of the intraocular lens (IOL) that will be implanted during surgery.Medical History and Current Medications.Provide your surgeon with a complete medical history, including any current medications you are taking. Certain medications, such as blood thinners, may need to be adjusted or discontinued before surgery.Lifestyle Modifications.Certain lifestyle modifications may be necessary in preparation for cataract surgery, including:Smoking cessation: Smoking can interfere with wound healing and increase the risk of complications.Avoiding alcohol: Alcohol can dehydrate the body and increase the risk of bleeding during surgery.Adjusting diet: A balanced diet is important for overall health before surgery.Preoperative Instructions.Your surgeon will provide specific preoperative instructions that may include:Fasting: Avoid eating or drinking anything for a specified period before surgery.Showering: Shower the night before or morning ofsurgery using antibacterial soap.Remove jewelry and makeup: Remove all jewelry, including earrings, necklaces, and rings, and avoid wearing makeup on the day of surgery.Arrive on time: Arrive at the surgery center as directed by your surgeon.On the Day of Surgery.On the day of surgery, the following steps will typically occur:Check-in and preparation: You will be asked to confirm your identity and provide consent for surgery. You may be given preoperative medications to relax you.Anesthesia: Cataract surgery is typically performed under local anesthesia, which will numb the eye and surrounding area.Surgical procedure: The surgeon will make a small incision in the cornea and create an opening in the lens. The cloudy lens will be removed and replaced with a new artificial lens.Postoperative care: After surgery, you will be taken to a recovery area where your vision will be checked. You will be given instructions on how to care for your eye and when to follow up with your surgeon.中文回答:白内障手术术前准备流程。
澳大利亚眼科医生的眼科手册说明书

light.Some of these lenses may also allow the eye to focus for near and distance(accommodate),removing the need for glasses.ConclusionThe treatment of cataracts has progressed enormously since the days when the“couchers”used to roam from town to town dislocating cataractous lenses with needles,and it continues to evolve in the21st century with an increasing trend towards customisation to the individual patient’s needs(fig4).What is clear, however,is that the provision of cataract surgery customised to the individual patient relies on far more than just the skill of the surgeon removing the cataract. Customised cataract surgery needs a multidisciplinary approach at several levels.Industry has a vital role in the development of new technologies,as do health services in the provision of appropriate eye care to populations.At the level of the individual patient such surgery involves the close cooperation of several professional groups,including physicians,anaes-thetists,surgeons,opticians,and nurses,sharing information to carefully plan,carry out,and assess the results of every procedure.The future for people with cataracts is bright.Contributors:MW did most of the background research,wrote the text and tables,referenced the paper,and created or sourced the figures.SS had the idea of writing the paper,helped to plan the content,and did much of the editing.RJS provided most of the information on the new developments in cataract surgery, helped to plan the preoperative assessment section,and edited the final paper.MW and SS accept full responsibility for the content of the paper and controlled the decision to publish. Funding:None.Competing interests:None declared.1Reidy A,Minassian DC,Vafidis G,Joseph J,Farrow S,Wu J,et al.Prevalence of serious eye disease and visual impairment in a north London population:population based,cross sectional study.BMJ 1998;316:1643-6.2Owsley C,McGwin G Jr,Sloane M,Wells J,Stalvey BT,Gauthreaux S.Impact of cataract surgery on motor vehicle crash involvement by older adults.JAMA.2002;288:841-9.3Royal College of Ophthalmologists.Cataract surgery:guidelines,Febru-ary2001.London:Royal College of Ophthalmologists,2001:7.Available at /publications/guidelines/cataract_surgery.html4Speaker MJ,Guerriero PN,Met JA,Coad CT,Berger A,Marmor M.A case-control study of risk factors for intraoperative suprachoroidal haemorrhage.Ophthalmology1991;98:202-10.5Olsen T.Sources of error in intraocular lens power calculation.J Cataract Refract Surg1992;18:125-9.6Findl O,Drexler W,Menapace R,Heinzl H,Hitzenberger CK,Fercher AF.Improved prediction of intraocular lens power using partial coherence interferometry.J Cataract Refract Surg2001;27:861-7.7Sanders DR,Kraff MC.Improvement of intraocular lens power calculation using empirical data[correction appears in Am Intra-Ocular Implant Soc J1981;7:82].Am Intra-Ocular Implant Soc J1980;6:263-7.8Retzlaff J.A new intraocular lens calculation formula.Am Intra-Ocular Implant Soc J1980;6:148-52.9Sanders DR,Retzlaff J,Kraff parison of the accuracy of the Binkhorst,Colenbrander,and SRK TM implant power prediction formulas.Am Intra-Ocular Implant Soc J1981;7:337-40.10Sanders DR,Retzlaff J,Kraff parison of empirically derived and theoretical aphakic refraction formulas.Arch Ophthalmol1983;101:965-7. 11Ernest P,Tipperman R,Eagle R,Kardasis C,Lavery K,Sensoli A,et al.Is there a difference in incision healing based on location?J Cataract Refract Surg1998;24:482-6.12Nielsen PJ.Prospective evaluation of surgically induced astigmatism and astigmatic keratotomy effects of various self-sealing small incisions.J Cataract Refract Surg1995;21:43-8.Corrections and clarificationsLassa fever:epidemiology,clinical features,and social consequencesA combination of editorial changes and an author oversight led to an error in this Clinical Reviewarticle by J Kay Richmond and Deborah J Baglole(29November,pp1271-5).In table2(“Clinicalstages of Lassa fever,”p1273)we should havestated that the table was adapted from reference2,the Merlin document“Licking”Lassa Fever,notfrom reference18,by McCarthy.Screening in brief intervention trials targeting excessivedrinkers in general practice:systematic review andmeta-analysisSome errors crept into this Primary Care paper byAnders Beich and colleagues(BMJ2003;327:536-42).In the results section we failed to spot asmall inconsistency between the text and table4.Inthe first paragraph(abridged and printed version;second paragraph in the full,web version)of thesection“Intervention effect and assessment efforts,”we said“NNTs[numbers needed to treat]of singlestudies ranged from5to61,”but the correct lowerlevel of this range should be6,as table4shows.Additionally,we inexplicably published a few wrongvalues in table5(full version).The screening effect inthe study by Fleming(ref42)is3.7[not0.7],and themaximum number of drinks for women in thestudies by Ockene and Fleming(ref41)is4[not3]and for men in the study by Anderson is11[not5]. Clinical review96BMJ on 25 December 2023 by guest. Protected by copyright./ BMJ: first published as 10.1136/bmj.328.7431.96-a on 8 January 2004. Downloaded from。
眼科英文病历( 眼科检查)

Sample History and Physical Note Charting Plus™ - Electronic Medical Records Note for John Doe on 6/6/02 - Chart 1124Chief Complaint: This 26 year old male presents today for a complete eye examination.Allergies: Patient admits allergies to aspirin resulting in disorientation, GI upset.Medication History: Patient is currently taking amoxicillin-clavulanate 125 mg-31.25 mg tablet, chewable medication was prescribed by A. General Practitioner MD, Adrenocot 0.5 mg tablet medication was prescribed by A. General Practitioner MD, Vioxx 12.5 mg tablet (BID).PMH: Past medical history is unremarkable.Past Surgical History: Patient admits past surgical history of (+) appendectomy in 1989.Social History: Patient denies alcohol use. Patient denies illegal drug use. Patient denies STD history. Patient denies tobacco use.Family History: Unremarkable.Review of Systems:Eyes: (-) dry eyes (-) eye or vision problems (-) blurred vision Constitutional Symptoms: (-) constitutional symptoms such as fever, headache, nausea, dizziness Musculoskeletal: (-) joint or musculoskeletal symptomsEye Exam: Patient is a pleasant, 26 year old male in no apparent distress who looks his given age, is well developed and nourished with good attention to hygiene and body habitus.Visual Acuity:Visual acuity - uncorrected: OD: 20/10 OS: 20/10 OU: 20/15Refraction:Lenses - final:OD: +0.50 +1.50 X 125 Prism 1.75OS: +6.00 +3.50 X 125 Prism 4.00 BASE IN FresnelAdd: OD: +1.00 OS: +1.00OU: Far VA 20/25Pupils: Pupil exam reveals round and equally reactive to light and accommodation.Motility: Ocular motility exam reveals gross orthotropia with full ductions and versions bilateral. Visual Fields: Confrontation VF exam reveals full to finger confrontation OU.IOP: IOP Method: applanation tonometry OD: 10 mmHg Medications: Alphagan; 0.2% Condition: improving.Keratometry:OD: K1 35.875K2 35.875OS: K1 35.875K2 41.875Lids/Orbit: Bilateral eyes reveal normal position without infection. Bilateral eyelids reveals white and quiet.Slit Lamp: Corneal epithelium is intact with normal tear film and without stain. Stroma is clear and avascular. Corneal endothelium is smooth and of normal appearance.Anterior Segment: Bilateral anterior chambers reveal no cells or flare with deep chamber.Lens: Bilateral lenses reveals transparent lens that is in normal position.Posterior Segment: Posterior segment was dilated bilateral. Bilateral retinas reveal normal color, contour, and cupping.Retina: Bilateral retinas reveals flat with normal vasculature out to the far periphery. Bilateral retinas reveal normal reflex and color.Test Results: No tests to report at this timeImpression: Eye and vision exam normal.Plan: Return to clinic in 12 month(s).Patient Instructions:Patient was given verbal and written instructions regarding eye care following pupil dilation.__________________________________ Dr. An. Ophthalmologist, MDSample Referral Letter Charting Plus™ - Electronic Medical Records 6/6/02Marcus Welby, M.D.1231 8th Street, Suite 222West Des Moines, IA 50265Dear Dr. Welby:John Doe was seen in my office in consultation as requested by you as a new patient for evaluation and care. The following is a summary of my findings and recommendations:Impression: Eye and vision exam normal.Plan: Return to clinic in 12 month(s).If I may be of any further assistance in the care of your patient, please let me know. Thank you for providing me the opportunity to participate in the care of your patients. Sincerely,An. Ophthalmologist, MDSample Prescription Charting Plus™ - Electronic Medical Records Dr. An. Ophthalmologist, MDDEA#:_________________________________________________________Doe6/6/02Date:JName:JohnOD: +0.50 +1.50 X 125 Prism 1.75OS: +6.00 +3.50 X 125 Prism 4.00 BASE IN FresnelAdd: OD: +1.00 OS: +1.00Dr._____________________________________________Sample Billing Statement Charting Plus™ - Electronic Medical RecordsBilling Statement - Thursday, June 06, 2002Provider:An. Ophthalmologist, MDPatient: John J Doe, Chart 1124123 E. Freckle St.Jersey City, NJ 07040Diagnoses1. V72.0 Examination Of Eyes And VisionTreatments1. 99213 Office or other outpatient visit - est. patient - 15 min.Related Diagnoses: V72.0Modifiers:Units:Referring Physician: A. General Practitioner, MDDate Last Seen: 07/26/2001Sample Patient Instructions Charting Plus™ - Electronic Medical Records Patient Instructions for John Doe on 6/6/02YOUR EYES HAVE BEEN DILATEDDilation drops temporarily increase the size of your pupils. This lets us accurately investigate the health of your eyes and other important general health aspects. Dilation of your eyes is a temporary inconvenience; however, benefits far outweigh the inconvenience.The effects of eye dilation drops will gradually decrease. It typically takes TWO to SIX HOURS for the effects to wear off. During this time, reading may be more difficult and sensitivity to light may increase. For a short time, wearing sunglasses may help. Notify us if you feel your long distance vision is blurred excessively before attempting to drive. Your patience during this very important procedure is appreciated!CALL MY OFFICE IMMEDIATELY AT 515-327-8850 IF YOU EXPERIENCE EXCESSIVE PAIN, DISCOMFORT OR NAUSEAREMEMBER TO HAVE REGULAR MEDICAL EYE EXAMINATIONS.Eye disease can occur at any age. Since most blindness is preventable if diagnosed and treated early, it is extremely important to have regular eye examinations. Keep in mind that many eye diseases are asymptomatic until after the damage to the eye has already occurred so early detection is the key. Use this as a reminder to plan for regular eye examinations to maintain sight throughout a lifetime._______________________________An. Ophthalmologist, MDCATARACTWhat is a cataract?* A cataract is the loss of transparency of the lens of the eye. It often appears like a window that is fogged with steam.What causes cataract formation?* Aging, the most common cause.* Family history.* Steroid use.* Injury to the eye.* Diabetes.* Previous eye surgery.* Long-term exposure to sunlight.How do I know if I have a cataract?* The best way for early detection is regular eye examinations by your medical eye doctor. There are many causes of visual loss in addition to the cataract such as problems involving the optic nerve and retina. If these other problems exist, cataract removal may not result in the return or improvement of vision. Your eye doctor can tell you how much improvement in vision is likely.Does it take a long time for a cataract to form?* Cataract development varies greatly between patients and is affected by the cause of the cataract. Generally, cataracts progress gradually over many years. Some people, especially diabetics and younger patients, may find that cataract formation progresses rapidly over a few months making it impossible to know exactly how long it will take for the cataract to develop. What is the treatment for cataracts?* The only way to remove a cataract is surgery. If the symptoms are not restricting your activity, a change of glasses may alleviate the symptoms at this time. No medications, exercise, optical devices or dietary supplements have been shown to stop the progression or prevent cataracts.It is important to provide protection from excessive sunlight. Making sure that the sunglasses you wear screen out ultraviolet (UV) light rays or your regular eyeglasses are coated with a clear, anti-UV coating will help prevent or slow the progression of cataracts.How do I know if I need surgery?* Surgery is considered when your vision is interfering with your daily activities. It is important to evaluate if you can see to do your job and drive safely. Can you read and watch TV in comfort? Are you able to cook, do your shopping and yard work or take your medications without difficulty? Depending on how you feel your vision is affecting your daily life, you and your eye doctor will decide together when it is the appropriate time to do surgery.What is involved with cataract surgery?* This surgery is generally performed under local anesthesia on an outpatient basis. With the assistance of a microscope, the cloudy lens is removed and replaced with a permanent intraocular lens implant.Right after the surgery you should be able to immediately perform all your normal activities except for the most strenuous ones. You will need to take eye drops as directed by your eye doctor. Follow-up visits are necessary to make sure the surgical site is healing without problems.This procedure is performed on over 1.4 million people each year in the United States alone, 95% without complications. With this highly successful procedure, 90% of the time vision improves unless a problem also exists with the cornea, retina or optic nerve. As with any surgery, a good result cannot be guaranteed._______________________________ An. Ophthalmologist, MD。
外科学的英文名词解释

外科学的英文名词解释外科学是医学领域中的一个重要分支,专注于对人体的各种疾病或损伤进行手术治疗。
外科学涵盖了广泛的领域,包括心脏外科、胸外科、神经外科、整形外科等等。
本文将对一些外科学的英文名词进行解释,以帮助读者更好地了解这一领域。
1. Cardiac Surgery(心脏外科)Cardiac Surgery is a subspecialty of surgery that focuses on surgical procedures involving the heart. It includes procedures such as coronary artery bypass grafting, valve repair or replacement, and heart transplantation. Cardiac surgeons are highly skilled in performing complex surgeries to treat various heart conditions.2. Thoracic Surgery(胸外科)Thoracic Surgery is a surgical specialty that deals with surgical procedures involving the chest, including the lungs, esophagus, and other thoracic organs. It includes procedures such as lung resection, mediastinal tumor removal, and esophageal surgery. Thoracic surgeons work closely with pulmonologists and other specialists to provide comprehensive care for patients with thoracic diseases.3. Neurosurgery(神经外科)Neurosurgery is a surgical specialty that focuses on the surgical treatment of disorders affecting the nervous system, including the brain, spinal cord, and peripheral nerves. Neurosurgeons perform procedures such as brain tumor removal, spinal fusion, and deep brain stimulation for Parkinson's disease. They also play a vital role in trauma care, treating severe head and spinal injuries.4. Orthopedic Surgery(骨科外科)Orthopedic Surgery is a surgical specialty that deals with the prevention, diagnosis, and treatment of disorders of the musculoskeletal system. It includes surgical procedures such as joint replacement, fracture fixation, and arthroscopy. Orthopedic surgeons workclosely with physical therapists and other specialists to provide comprehensive care to patients with bone, joint, and muscle disorders.5. Plastic Surgery(整形外科)Plastic Surgery is a surgical specialty that focuses on restoring, reconstructing, or altering the human body's form and function. It includes procedures such as breast augmentation, rhinoplasty, and facial reconstruction. Plastic surgeons also perform cosmetic procedures to enhance appearance, such as facelifts and liposuction.6. General Surgery(普外科)General Surgery is a surgical specialty that encompasses a broad range of surgical procedures across various organ systems. General surgeons are trained to perform surgeries in the abdomen, breast, neck, and other areas. They often treat conditions such as appendicitis, hernias, and gallbladder diseases. General surgeons also play a crucial role in emergency trauma care.7. Vascular Surgery(血管外科)Vascular Surgery is a surgical specialty that deals with the diagnosis and treatment of disorders affecting the blood vessels, such as arterial blockages and aneurysms. Vascular surgeons perform procedures such as bypass grafting, endovascular stenting, and surgical repair of blood vessel abnormalities. They work closely with cardiologists and interventional radiologists to provide comprehensive care for patients with vascular diseases.总结:外科学是医学领域中重要的分支,涵盖了多个专病领域。
Handtool for cataract surgery
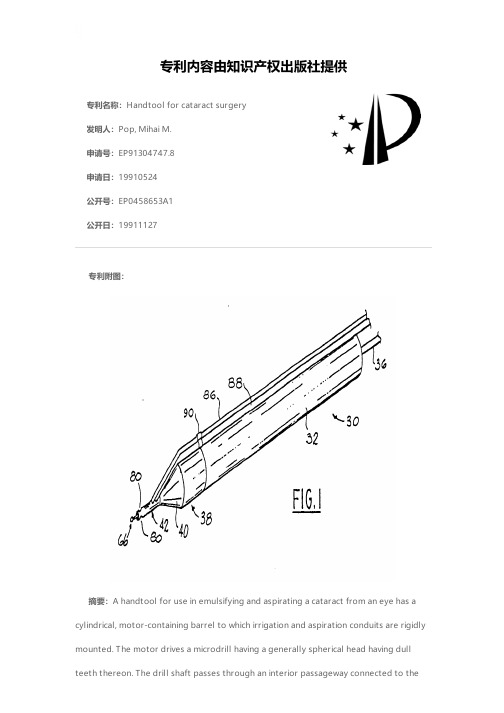
专利名称:Handtool for cataract surgery发明人:Pop, Mihai M.申请号:EP91304747.8申请日:19910524公开号:EP0458653A1公开日:19911127专利内容由知识产权出版社提供专利附图:摘要:A handtool for use in emulsifying and aspirating a cataract from an eye has a cylindrical, motor-containing barrel to which irrigation and aspiration conduits are rigidly mounted. The motor drives a microdrill having a generally spherical head having dull teeth thereon. The drill shaft passes through an interior passageway connected to theaspiration conduit and the irrigation conduit is connected to an annular passageway concentric to the interior passageway. The drill head can be inserted into contact with the cataract through an opening in the capsule surrounding the lens and as it rotates it churns the cataract material into an emulsion which is aspirated, along with irrigation fluid from the vicinity of the rotating drill head.申请人:Pop, Mihai M.地址:108 Beausoleil Gatineau, Quebec J8T 7H2 CA国籍:CA代理机构:Deans, Michael John Percy更多信息请下载全文后查看。
LOCS III 白内障分级 权威
Clinical application of the Lens Opacities Classification System III in the performance of phacoemulsificationJames A.Davison,MD,Leo T.Chylack Jr.,MDPurpose:To report the correlation of features of cataracts graded by the Lens Opacities Classification System,version III (LOCS III),with phacoemulsification energy expenditure and the balanced salt solution (BSS ®)volume used during cataract surgery.Setting:Wolfe Clinic,Marshalltown,Iowa,USA.Methods:This was a retrospective review of 2364cases operated on by a single surgeon from January 1998to July 2000in which the cataract had been graded at the slitlamp using the 4grading scales of the LOCS III:nuclear opalescence (NO),nuclear color (NC),cortical cataract (C),and posterior subcapsular cataract (P).Polynomial best-fit lines were derived using regression analysis correlating the 4preoperative LOCS III characteristics with 3intraoperative observations:ma-chine-measured phacoemulsification time,mean power expenditure,and BSS volume.Results:As determined by best-fit lines and their coefficient of determination (R 2),there were exponential relationships between machine-measured phaco-emulsification time and the degree of NC (R 2ϭ0.48)and NO (R 2ϭ0.40).Trends existed between NC and NO and the amount of BSS used (R 2ϭ0.08and R 2ϭ0.07,respectively).No relationships were observed between the LOCS III classes of cataract,C and P,at any intraoperative observation.Conclusions:Exponentially,greater phacoemulsification energy was required as NC and NO increased.The LOCS III cataract grading system enhanced the ability to estimate ultrasonic energy expenditure and BSS volume use during phaco-emulsification.Preoperative LOCS III cataract classification can help to create a more formally organized,integrated,customized operative plan.J Cataract Refract Surg 2003;29:138–145©2003ASCRS and ESCRSThe LensOpacitiesClassification System,versionIII (LOCSIII),isa widelyused,scientificallyvalid,standardizedphotographic comparisonsystemfor grad-ingthe featuresof thehuman age-relatedcataract.1–5It hasbeen used to grade the type and severity of cataract incross-sectional studies and the progression of cataract in longitudinal studies.It also has been used to grade cata-racts at the slitlamp.3Grading using LOCS III involves the assessment of 4features shown on 3sets of photographs on an 8.5-inch ϫ11-inch color transparency (Figure 1).The features of nuclear opacification and brunescence are graded according to 1set of 6photographs.The bright-ness of scatter from the nuclear region has been desig-nated nuclear opalescence (NO)and the intensity of brunescence,nuclear color (NC).The amount of corti-cal cataract (C)is determined by comparing the esti-mated aggregate of cortical spoking to that seen inAccepted for publication September 12,2002.From the Wolfe Clinic,Marshalltown,Iowa,USA.Presented at the Symposium on Cataract,IOL and Refractive Surgery,San Diego,California,USA,April 2001Reprint requests to James A.Davison,MD Wolfe Clinic,309East Church Street,Marshalltown,Iowa,USA.©2003ASCRS and ESCRS0886-3350/03/$–see front matter Published by Elsevier Science Inc.doi:10.1016/S0886-3350(02)01839-45separate photographs.Similarly,the estimated amountof posterior subcapsular cataract(P)is determined by comparing it to another5photographs depicting in-creasing amounts of posterior subcapsular cataract.The grade for each feature is derived by locating the image of the patient’s lens on the scale of severity for each feature represented in the color transparency.The NC and NO are graded on a decimal scale of0.1to6.9. The severity of C and P are graded on a decimal scale of 0.1to5.9.The final LOCS III grade comprises4deci-mal values,1each for NO,NC,C,and P.In the original publication describing the LOCS III system,1an assessment of within-grader and between-grader reproducibility was done and expressed as a“95% confidence interval”for each scale.On average,these 95%confidence intervals were approximately0.7units. The intervals were used to define a significant change in the severity of the cataract.For example,if the NO grade was2.3at baseline and1year later it was3.5,the increase in severity(3.5–2.3ϭ1.2)was greater than the95% confidence interval(0.7)and it was therefore reasonable to conclude that one was95%confident that the change was statistically significant.If the increase had been only 0.5units,the increase could more likely be the result of the intrinsic methodologic noise of the LOCS III system and not a true increase in the severity of the cataract.Since1998,LOCS III has been used systematically in the clinical practice of one author(J.A.D.).Preoper-ative LOCS III grading of all surgical patients was done at the slitlamp to improve clinical documentation in the clinical record.Parenthetical descriptions were rarely added but usually included the critical nature of the centrality within the visual axis of subtle localized inter-faced zones of NO and NC,cortical spokes,or subcap-sular opacities.There was consistency in grading over time,and patients could be told with greater confidence whether their cataracts were stable or progressing.It was also helpful to have accurate measures of cataract severity when discussing cases with third-party payer representa-tives;surgical interventional decisions to offer surgery to some patients could be better defended.Over time,LOCS III slitlamp grading was empiri-cally incorporated into the decision-making process and planning of upcoming surgeries.Ultimately,this re-sulted in a more organized,integrated,customized op-erative plan for each patient.Patients and MethodsIn this retrospective study,2364consecutive cases of phacoemulsification were analyzed with respect to the 4LOCS III characteristics and machine-measured phaco-emulsification time,average machine measured power(%), and the balanced salt solution(BSS)volume used.All data points had been recorded in2186cases.Surgery was per-formed from January1998to July2000by a single surgeon (J.A.D),who also performed LOCS III grading of all cataracts at the slitlamp.A standardized nuclear-fracture quadrant-aspiration phacoemulsification technique was used with a straight 45-degree0.9mm ABS MicroTip with the Alcon Legacy 20,000machine.6After topical anesthesia was administered,a temporal clear corneal incision was made.Grooving was ac-complished with the machine in memory I(phacoemulsifica-Figure1.(Davison)The LOCS III standard images in an8.5-inchϫ11-inch color transparency as used in the office at the slitlamp.The top row contains the standards for NO and NC.The second row contains the standards for grading C and the bottom row,for grading P.J CATARACT REFRACT SURG—VOL29,JANUARY2003139tion power maximum,90%;vacuum maximum,50mm Hg;aspiration flow rate,14cc/minute)(Figure 2).Wider,deeper grooves were made as nuclear hardness increased.The pos-terior nuclear plate was torn from the periphery toward the center by cross action with the phacoemulsification tip and a custom,modified,0.37mm cyclodialysis spatula (Figure 3).Quadrant aspiration was accomplished in memory III (phaco-emulsification power maximum,70%;vacuum maximum,500ϩmm Hg;aspiration flow rate,35cc/minute).The aspiration process was kept posterior to the iris plane within the capsular bag as much as possible to protect thecorneal endothelium from damage from fragment impact and abrasion (Figures 4to 6).Sodium hyaluronate 3.0%–chon-droitin sulfate 4.0%(Viscoat )was usually injected into the anterior chamber before quadrant aspiration when the NC was greater than 4.5.In some cases,Viscoat was reinjected before aspiration of the fourth quadrant because of the ten-dency of the capsular bag to flatten after the third quadrant had been removed,which forces the remaining process ante-rior to the iris plane.In some eyes,soft quadrants or the last fragment of the fourth firm quadrant were removed using reduced vacuum (maximum 300mm Hg),maximumpowerFigure 2.(Davison)After initial grooving is completed,a secondrotation of the nucleus allows for improved visualization while deeper grooving progresses in hardnuclei.Figure 3.(Davison)Nuclear cracking is created from the peripherytoward the center with a cross action of the phacoemulsi fication tip and the cyclodialysisspatula.Figure 4.(Davison)The 45-degree phacoemulsi fication tip isturned sideways with its aperture facing the interior wall of the first nuclear quadrant.Low levels of emulsi fication energy are used to engage and impale the central portion of thequadrant.Figure 5.(Davison)A low level of ultrasonic energy and a higherlevel of vacuum allow the tip to adhere to the softer edge of the quadrant and drag it centrally.J CATARACT REFRACT SURG —VOL 29,JANUARY 2003140(50%),and a reduced aspiration flow rate (25cc/minute)(Figures 7and 8).Polynomial best-fit lines were derived by regression anal-ysis among the 4LOCS III characteristics and the 3phaco-emulsification observations.ResultsThe mean machine-measured phacoemulsification time increased as the NO and NC grades increased (Table 1).As determined by the best-fit lines and their coefficients of determination (R 2),there was an expo-nential relationship between NO and machine-mea-sured phacoemulsification time (R 2ϭ0.40).A trend existed between NO and the mean power (R 2ϭ0.15)and the amount of BSS used (R 2ϭ0.07)(Figure 9).A slightly stronger exponential relationship existed between NC and machine-measured phacoemulsifica-tion time (R 2ϭ0.48).A trend also existed between NC and mean power (R 2ϭ0.18)and the amount of BSS used (R 2ϭ0.08)(Figure 10).No relationships were observed between the LOCS III classes of cataract,C and P,and any intraoperative observation (Figures 11and 12).DiscussionIn the original LOCS III publication,the NO and NC scales were highly correlated with each other and the relationships between objective measures of NO,NC,and the LOCS III grade of the standard imageswereFigure 6.(Davison)The bulk of the quadrant is central while mod-erate ultrasonic energy,vacuum,and aspiration flow are used to remove the firm portions of thequadrant.Figure 7.(Davison)Aspiration can begin after an edge of the lastquadrant is lifted free of the posteriorcapsule.Figure 8.(Davison)The cyclodialysis spatula protects the poste-rior capsule as phacoemulsi fication power is applied during removal of the last quadrant.Lower levels of vacuum and aspiration flow rate help protect the posterior capsule from inadvertent aspiration.Table 1.Mean machine-measured ultrasound time(minutes).J CATARACT REFRACT SURG —VOL 29,JANUARY 2003141Figure9.(Davison)A significant relationship is seen betweenLOCS III NO and ultrasound time but not mean ultrasound power andBSS volume used.Figure10.(Davison)A significant relationship is seen betweenLOCS III NC and ultrasound time but not mean ultrasound power andBSS volume used.142J CATARACT REFRACT SURG—VOL29,JANUARY2003Figure11.(Davison)No relationship is seen between LOCS III Cand ultrasound time,mean ultrasound power,and BSS volume used.Figure12.(Davison)No relationship is seen between LOCS III Pand ultrasound time,mean ultrasound power,and BSS volume used. J CATARACT REFRACT SURG—VOL29,JANUARY2003143nearly linear.The NO was assessed independently with image analysis of optical density,and NC was assessed independently with fast spectral scanning colorimetry of each LOCS III standardized image.Highly different grades of NO and NC in the same cataract were un-likely.Similarly,the relationship between the expendi-ture of phacoemulsification energy and the LOCS III grades of NO and NC appears to be linear for LOCS III grades below approximately3.7.Above that,the rela-tionship between LOCS III grade and phacoemulsifica-tion energy expenditure seems to become exponential. Although in LOCS III NO and NC are graded sepa-rately,most clinicians are accustomed to describing nu-clear change by a single term,nuclear sclerosis.Both color change and increased light scattering are part of the pro-cess of nuclear sclerosis,and it is therefore not surprising to have found that both NO and NC are similarly pos-itively correlated with ultrasonic energy exposure.When viewing a cataractous lens with LOCS III NO and NC grades of4.0to5.0,most surgeons intu-itively anticipate increased phacoemulsification times. The nucleus is simply harder,so it will take more energy to emulsify.The LOCS III NC grade has been corre-lated with hardness of the central nucleus as measured by the resistance to a fine conical probe measured by a dynamometer.7Phacoemulsification energy recorded by cumulative delivered energy as well as by postopera-tive anterior chamber flare has been shown to be corre-lated with LOCS III NC and NO.8The surgeon in this study finds it useful to be able to accurately grade opalescence and brunescence(and the severity of C and P)to better estimate when prolonged ultrasonic time or increased ultrasonic energy is likely.It has proved advantageous to integrate LOCS III grading into routine operative planning.By doing so,the sur-geon will be better prepared to manage the more scle-rotic nucleus and his or her preoperative planning can be more patient specific.The surgeon in this study empirically formulated several recommendations for customizing a surgical plan using preoperative LOCS III grading as a part of a com-plete preoperative ophthalmic examination.These are listed below.1.A retentive viscoelastic material is recommended in cases in which the LOCS III NO or NC grade is4.0 or greater.2.If the LOCS III NO or NC grade is5.0,the capsulorhexis will be more easily visualized if indocya-nine green dye is used to stain the anterior capsule.3.If the pupil is smaller than4.5mm and the LOCS III NO or NC grade is greater than4.5,use of a pupil expansion/maintenance device should be considered.4.If zonular integrity is compromised and the LOCS III NO or NC grade is4.5or greater,a backup ciliary-sulcus-supported intraocular lens(IOL)or ante-rior chamber IOL should be available.5.Surgeons in training should learn and use LOCS III grading to enable them to select“normal”cases with nuclei of enough substance to easily manipulate yet readily emulsify.Very soft or very hard nuclei may present unnecessary challenges.6.The LOCS III is helpful and should be used in the trials of new technologies for cataract removal.For ex-ample,in one author’s experience(J.A.D.)with early AquaLase technology(Alcon Surgical),efficient removal of a nucleus with an NC grade greater than3.7was not possible.Of course,the relationships between LOCS III characteristics and phacoemulsification energy expendi-ture vary with the individual technique and equipment used.Despite this individual-specific variation,it is likely that the trends observed will be seen with other surgeons as long as a mechanical removal technique is used.Incorporating LOCS III grading into a preopera-tive regimen should not only improve surgical planning, it should also improve clinical documentation,commu-nication among providers and with third-party payers, and the accuracy of longitudinal follow-up.Most im-portant,preoperative LOCS III classification should contribute to more predictable and effective cataract surgery.References1.Chylack LT Jr,Wolfe JK,Singer DM,et al.The LensOpacities Classification System III;the Longitudinal Study of Cataract Study Group.Arch Ophthalmol1993;111:831–8362.Maraini G,Pasquini P,Tomba MC,et al.An independentevaluation of the Lens Opacities Classification System II (LOCS II);the Italian-American Cataract Study Group Ophthalmology1989;96:611–6153.Karbassi M,Khu PM,Singer DM,Chylack LT Jr.Evalu-J CATARACT REFRACT SURG—VOL29,JANUARY2003 144ation of Lens Opacities Classification System III applied at the slitlamp.Optom Vis Sci1993;70:923–928ton RD,Chylack LT Jr,Ko¨pcke W.Letters to theeditor.Ophthalmic Epidemiol1996;3:59–605.van den Berg TJTP,Coppens JC.Conversion of lens slitlamp photographs into physical light-scattering units.In-vest Ophthalmol Vis Sci1999;40:2151–21576.Davison JA.Performance comparison of the Alcon Legacy200001.1mm TurboSonics and0.9mm Aspiration By-pass System tips.J Cataract Refract Surg1999;25:1386–13917.Hu C,Zhang X,Hui Y,Chung H.[The nuclear hardnessand associated factors of age-related cataract].[Chinese] Yen Ko Tsa Chih2000;36:337–3408.Ursell PG,Spalton DJ,Tilling K.Relation between post-operative blood-aqueous barrier damage and LOCS III cataract gradings following routine phacoemulsification surgery.Br J Ophthalmol1997;81:544–547J CATARACT REFRACT SURG—VOL29,JANUARY2003145。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Optical Coherence tomography
several ultrasonic emulsifying machines • 蠕动泵 文丘里泵
16
IOL Monofocal Technology Advances
1949 PMMA 1983 SILICONE 1994 HYDROPHOBIC ACRYLIC Single-Piece Design 2005 + Aspheric Optic UV only UV and Blue Light Filtering
cataract abaissement Acupuncture of traditional chinese medicine
Phacoemulsification
(A) Povidone-iodine 5% is instilled;
(B) disinfect the skin around eye;
Corneal endothelium count
Eyes with decreased endothelial cell counts have increased vulnerability to postoperative decompensation secondary to operative trauma.
History of Cataract Surgery
This is the couching of Cataract in Europe between 2000BC to 1000 AD.
History of Cataract Surgery
• Jacques Daviel’s first scientific description of cataract extraction in 1752. • No anesthesia • No sutures • Sand bags to prevent movement of the head.
Topical anesthesia - 1993
• Dr. Freeman popularized the use of topical anesthesia in 1993. • Surgery can be performed without injection.
A story
1974, Chairmen Mao was diagnosed with a cataract , almost got blind for 1 year. 1975, Chairmen Mao took a cataract surgery.
The IOL is inserted into a cartridge for injection which is loaded into an injector handset
33
Sutureless Cataract Surgery 1991
• Dr. McFarland discovered that if he were to construct the incision as a valve, the incision would be self sealing. • Thus he started the “no stitch” cataract surgery.
Original Ridley Implant
Foldable implant - 1991
• In 1991, FDA approved the use of Silicone foldable implant. • With foldable implant inserted a 6 mm implant through a 3.2 mm incision opening. • One stitch surgery.
5
Preparation for operation
A detailed eye examination to predict postoperative vision - visual function -Introcular pressure, mydriasis, etc -A/B ultrasonic exam -IOL master -Corneal curvature -Corneal endothelium count
3
Examination method of cataract
• slit lamp
4
Preparation for operation
• elective surgery
• Systemic diseases control well, which is stable and the patients can tolerate operation , no active inflammation in the eye
(C) drapes isolate the eyelids from the operating field with insertion of a speculum.
• (A) Cortical lens matter is pulled centrally and aspirated: (B)
surgery of cataract
田甜
Treatment of cataract
• There isn’t any effective drug to the senile cataract. • It is major to operation.
2
Operative time
• At the immature or mature stage • The lens is extracted when the vision is affected or the complications occurred.
Numerous formulae have been developed which utilize keratometry and axial length to calculate the IOL power.
IOL master
• the IOL power • Depth of the anterior chamber Diameter of the cornea
Surgical management of unusual cataract
二、Case 1 --Cataract with obsolete uveitis
Female,67-year-old,Cataract,Obsolete Uveitis PE:VA 0.1(Left), Less circular pupil, Most posterior synechia, Brown lens opacity, Corneal endothelia cells 1036/mm2. Management:Phaco + IOL implantation + Pupil angioplasty, Postoperative VA 0.5, IOP 8mmHg
• Too hard lens nucleus may not adopt this method
44
Small incision manual cataract surgery
• (A)
Anterior chamber is entered; (B) capsulorhexis; (C) prolapse of nucleus into anterior chamber; (D) expression of nucleus; (E) cortical cleanup; (F) IOL in place
History of cataract surgery
• During World War II, Harold Ridley observed that aviators could tolerate shards of PMMA(polymethyl methacrylate)plastic from the aircraft canopies in their eyes. • He used this knowledge to create and to implant the first intraocular lens between 1949 and 1950.
– strongpoint:
• Self-healing wound • The corneal astigmatism after operation is fine • Visual restoration is soon
– Shortcoming:
• The apparatus s expensive
Preoperative
2 days postoperative
Case 2 --Complicated cataract after glaucoma surgery
History of cataract surgery.
• 1867 Henry Williams of England first described the use of sutures in cataract surgery.
History of cataract surgery
• In 1914, Van Lint of Brussels, described the use of anesthesia. • We are still using his technique – the Van Lint technique, to numb the eye.
Viscoelastic is injected into the anterior chamber
A-scan ultrasonography