前列腺
前列腺是什么

前列腺是什么前列腺是男性生殖系统中重要的一部分,位于膀胱下方,围绕着尿道。
它是一种腺体,产生和分泌液体,为精子提供营养和保护。
前列腺在男性生殖健康中起着至关重要的作用。
本文将介绍前列腺的结构、功能以及可能出现的常见问题。
前列腺结构前列腺是一个类似于胡桃的腺体,大小约为栗子大小,位于膀胱和阴茎之间。
它围绕着尿道,是尿液和精液的通道。
前列腺主要由柱状上皮细胞和双层立方上皮细胞组成。
它还包括平滑肌、结缔组织和腺体。
良好的前列腺结构对于正常的生殖系统功能非常重要。
前列腺功能前列腺的主要功能是产生和分泌前列腺液体,这种液体是精液的主要成分之一。
它的主要成分包括水、酸性的磷酸盐、碳酸氢盐、氨基酸、酶和锌等。
前列腺液体为精子提供能量和润滑,并保护精子免受尿道内酸性环境和细菌的损害。
此外,前列腺还参与了射精的过程,通过肌肉的收缩将精液从睾丸输送至尿道。
前列腺相关问题前列腺相关问题包括前列腺炎、前列腺增生和前列腺癌。
前列腺炎是前列腺的炎症,常见症状包括尿频、尿急、尿不尽和会阴部不适。
前列腺增生是前列腺逐渐增大导致尿流变弱和尿频等症状,尽管这种情况通常是良性的。
而前列腺癌是一种最常见的男性恶性肿瘤,常见症状包括尿频、尿急、尿不尽、血尿和性功能障碍等。
前列腺健康的维护为了维护前列腺的健康,男性们可以采取一些措施。
首先,保持一个健康的生活方式,包括均衡饮食、适度运动和减少疲劳。
其次,定期进行体检,包括前列腺检查以及相关的血液检查和影像学检查。
此外,避免过多的饮酒和咖啡因摄入,适量饮水也十分重要。
保持适当的水分摄入可以稀释尿液,减轻尿道刺激和细菌感染的可能。
最后,定期进行性生活,并保持良好的性卫生。
结论前列腺作为男性生殖系统中的重要腺体,扮演着至关重要的角色。
正常的前列腺结构和功能对于男性的生殖健康至关重要。
然而,前列腺相关问题如前列腺炎、前列腺增生和前列腺癌是常见的男性健康问题。
通过采取适当的保健措施,男性们可以维护良好的前列腺健康,保持正常的生殖功能。
前列腺大小的正常标准是多少

前列腺大小的正常标准是多少前列腺是男性特有的生殖器官,位于膀胱下方,环绕着尿道。
它的大小对男性的健康至关重要,因为它与尿道和生殖系统的正常功能密切相关。
那么,前列腺的大小到底应该是多少才算是正常呢?首先,我们需要了解一下正常前列腺的大小范围。
一般来说,正常成年男性的前列腺大小在20毫升到30毫升之间被认为是正常的。
这个范围是根据医学研究和临床实践得出的结论,也是临床医生在诊断前列腺疾病时的重要参考标准。
那么,如何确定自己的前列腺大小是否正常呢?最简单的方法就是通过医学影像技术进行检查,比如超声波检查或MRI检查。
这些检查可以清晰地显示前列腺的大小和形态,帮助医生判断是否存在异常情况。
除了前列腺的大小之外,还有一些其他指标可以帮助评估前列腺的健康状况。
比如,医生可能会关注前列腺的质地、形态和表面特征,以及是否存在结节或肿块。
这些都是判断前列腺是否健康的重要因素。
另外,前列腺的大小也会随着年龄的增长而发生变化。
一般来说,随着年龄的增长,前列腺会逐渐增大,这是由于前列腺组织的增生和激素水平的变化所致。
因此,对于不同年龄段的男性来说,对前列腺大小的评估标准也会有所不同。
除了年龄因素之外,前列腺的大小还受到遗传、生活习惯、饮食等多种因素的影响。
比如,长期饮酒、吸烟、饮食不均衡等不良生活习惯都可能对前列腺健康产生不良影响,导致前列腺增生、炎症等问题。
总的来说,前列腺大小的正常标准是一个相对而言的概念,需要结合个体的实际情况来进行评估。
如果你对自己的前列腺健康状况有疑问,建议尽快就医进行检查,及时发现问题并进行治疗。
同时,保持良好的生活习惯,定期进行体检也是非常重要的。
综上所述,前列腺大小的正常标准应该是在20毫升到30毫升之间,但具体的评估还需要结合个体情况和多种因素进行综合考量。
希望每位男性朋友都能保持良好的前列腺健康,远离前列腺疾病的困扰。
前列腺肥大分度标准

前列腺肥大分度标准
一、前列腺体积
前列腺体积是判断前列腺肥大程度的重要指标。
正常的前列腺体积约为20毫升,而肥大的前列腺体积会超过这个标准。
根据前列腺体积的大小,可以将前列腺肥大分为轻度、中度和重度三个等级。
轻度的前列腺肥大体积在21-30毫升之间,中度的前列腺肥大体积在31-40毫升之间,重度的前列腺肥大体积则超过40毫升。
二、前列腺特异性抗原(PSA)水平
PSA是前列腺癌的特异性标志物,也是判断前列腺健康的重要指标。
PSA水平越高,表示前列腺肥大的程度越严重。
一般来说,正常的前列腺特异性抗原(PSA)水平应该低于4.0ng/ml。
如果PSA水平高于此标准,可能表示前列腺肥大或前列腺癌的风险增加。
三、症状表现
症状表现也是判断前列腺肥大程度的重要依据。
轻度前列腺肥大的患者可能无明显症状或仅出现轻微的排尿异常,如尿线无力、尿频、尿急等。
而中度和重度前列腺肥大的患者可能会出现更加明显的症状,如尿潴留、血尿、尿路感染等。
如果症状严重且持续,可能需要通过手术或药物治疗来缓解。
综上所述,判断前列腺肥大程度需要考虑前列腺体积、PSA水平和症状表现三个方面。
如果出现排尿异常等症状,应及时就医并进行相关检查,以便早期发现和治疗。
前列腺

前列腺特殊的解剖位置和生理结构,需采取 综合性的疗法,要彻底治愈,疗程也会长一 些,费用自然就比一般的炎症要高。
❖ 3、频繁手淫为什么也会引起前列腺炎? ❖ 答:频繁手淫会造成泌尿生殖系刺激,反复
充血,引起无菌性的炎症,不及时治疗容易 诱发慢性前列腺炎或是无症状性前列腺炎。
前列腺增生肥大
❖ 定义:
前列腺
一、前列腺解剖结构和生理功能; 一、前列腺炎; 二、前列腺增生肥大
编辑: 周凯
前列腺解剖结构
前列腺生理功能
❖ 1、构成了部分的尿道壁,包括尿道内括约肌;
❖ 2、最大的附属性腺,对男性生殖功能具有特 殊的作用;
❖ 3、外分泌功能—前列腺液,是精液的重要组 成部分
前列腺液的成分及作用
❖ 在正常情况下,前列腺液是一种乳白色的稀薄液体, 呈弱酸性,是精液的重要组成成分。
❖ 病因:
❖ 前列腺增生病因目前还不能明确,考虑可能 跟一下几种相关:
❖ 1、性激素的作用;雌、雄激素的平衡改变会 诱发前列腺增生。
❖ 2、前列腺细胞为胚胎再唤醒 ; ❖ 3、多肽类生长因子 ; ❖ 4、可能跟高脂肪、高蛋白的过多摄入相关; ❖ 5、可能跟前列腺炎刺激有关。
❖ 临床表现:
❖ 1、膀胱刺激症状:尿频、尿急、夜尿增多及 急迫性尿失禁。
❖ 滴虫与霉菌:正常情况下前列腺液内无滴虫和霉菌。 当有滴虫和霉菌感染时可在前列腺液内检出。
前列腺
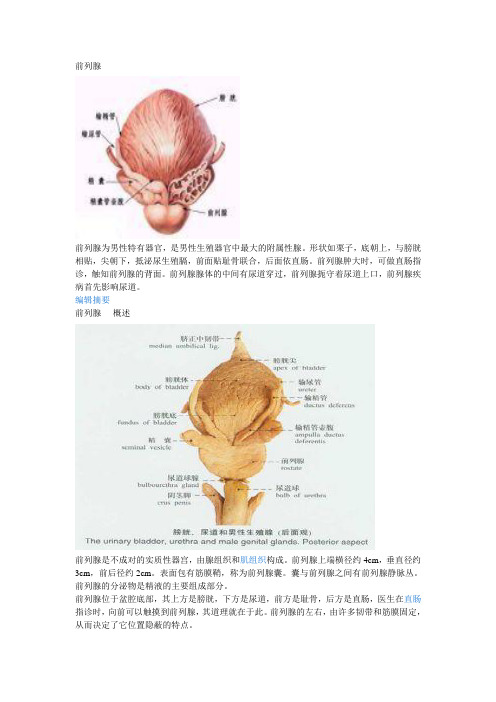
前列腺前列腺为男性特有器官,是男性生殖器官中最大的附属性腺。
形状如栗子,底朝上,与膀胱相贴,尖朝下,抵泌尿生殖膈,前面贴耻骨联合,后面依直肠。
前列腺肿大时,可做直肠指诊,触知前列腺的背面。
前列腺腺体的中间有尿道穿过,前列腺扼守着尿道上口,前列腺疾病首先影响尿道。
编辑摘要前列腺- 概述前列腺是不成对的实质性器宫,由腺组织和肌组织构成。
前列腺上端横径约4cm,垂直径约3cm,前后径约2cm。
表面包有筋膜鞘,称为前列腺囊。
囊与前列腺之间有前列腺静脉丛。
前列腺的分泌物是精液的主要组成部分。
前列腺位于盆腔底部,其上方是膀胱,下方是尿道,前方是耻骨,后方是直肠,医生在直肠指诊时,向前可以触摸到前列腺,其道理就在于此。
前列腺的左右,由许多韧带和筋膜固定,从而决定了它位置隐蔽的特点。
前列腺位于膀胱颈的下方、包绕着膀胱口与尿道结合部位,尿道的这部分因此被称为“尿道前列腺部”,即是说前列腺中间形成的管道构成尿道的上口部分。
可以这样说,前列腺扼守着尿道上口,前列腺有病排尿首先受影响的道理就在于此。
前列腺与输精管、精囊紧密相邻,射精管由上部进入前列腺,并开口于前列腺中间的隐窝之中,这种生理位置就很容易解释为什么前列腺有病常常累及性功能,甚至可以称“前列腺炎与精囊炎是一对”难兄难弟了。
其体积较小,可以说是人体最小的器官之一,重约20克,不足50克。
位置隐蔽,不易诊察。
前列腺外形如同一个倒放的栗子,医学书中常称其为圆锥体,似乎不如栗子更形象。
它的底部横径4厘米,纵径3厘米,前后径2厘米。
前列腺- 结构位置男性的尿道分为四段男性的尿道分为四段,它们是尿道前列腺部、尿道膜部、尿道的球部和阴茎。
男性的尿道前列腺在最里面,后尿道最深处离膀胱最近的这段尿道的主要脏器称为前列腺。
它外形像一个毛荔枝,通过肛门用手指头可以摸到,包裹在尿道之外。
前列腺的上面是膀胱的径部,左侧和右侧是男性精囊腺,下方是男性的尿道,前方是耻骨联合部,后方是背靠着男性的直肠。
前列腺解剖

• 前列腺一般分为5个叶:前叶、中叶、后叶 和两侧叶。中叶呈楔形,位于尿道与射精 管之间。40岁以后,中叶可变肥大,向上 凸顶膀胱,使膀胱垂明显隆起,并压迫尿 道引起排尿困难。
医学资料
• 仅供参考ห้องสมุดไป่ตู้用药方面谨遵医嘱
前列腺解剖
• 前列腺位于膀胱与原生殖膈之间。前列腺底与 膀胱颈、精囊腺和输精管壶腹相邻。前方为耻 骨联合,后方为直肠壶腹。直肠指诊时可触及 前列腺的后面,以诊断前列腺是否肥大等,向 上并可触及输精管壶腹和精囊腺。小儿的前列 腺甚小,性成熟期腺部迅速生长。老年时,前 列腺退化萎缩。如腺内结缔组织增生,则形成 前列腺肥大。
前列腺核磁共振评分3分

前列腺核磁共振评分3分前列腺核磁共振(Magnetic Resonance Imaging,MRI)是一种非侵入性的影像学技术,可以用于评估前列腺疾病。
前列腺核磁共振评分3分是指前列腺核磁共振图像表现为低信号,表示前列腺组织的正常结构和形态。
前列腺是男性生殖系统中的重要器官,位于膀胱下方,环绕尿道。
它的主要功能是产生精液的一部分,帮助精子的运输和存活。
然而,前列腺疾病是常见的男性健康问题之一。
前列腺核磁共振评分3分通常用于评估前列腺癌的临床分期。
前列腺癌是男性最常见的癌症之一,早期诊断和治疗对于患者的生存率至关重要。
前列腺核磁共振评分3分的图像表示前列腺组织呈现低信号,通常意味着前列腺癌的风险较低。
这种评分可以帮助医生确定治疗方案和预测预后。
前列腺核磁共振评分3分还可以用于评估其他前列腺疾病,如前列腺增生和前列腺炎。
前列腺增生是指前列腺组织的非恶性增生,常见于中老年男性。
前列腺炎是前列腺组织的感染和炎症,常见于年轻男性。
前列腺核磁共振评分3分的图像可以帮助医生确定疾病的类型和程度,指导治疗方案的选择。
虽然前列腺核磁共振评分3分可以提供有关前列腺疾病的重要信息,但它并不能单独用于诊断。
诊断前列腺疾病通常需要结合临床症状、体检和其他检查结果进行综合评估。
因此,如果发现前列腺相关症状,如尿频、尿急、尿痛等,建议及时就医,并按医生的建议进行相关检查。
在进行前列腺核磁共振评分3分之前,患者需要做好准备工作。
首先,需要告知医生自己是否有金属植入物,如心脏起搏器、人工关节等,因为磁共振时会产生磁场。
其次,需要空腹,避免进食2-4小时,以减少胃肠道气体对图像质量的影响。
在进行核磁共振检查时,患者需要躺在磁共振仪的检查床上,保持平静,听从医生的指导。
前列腺核磁共振评分3分可以提供有关前列腺疾病的重要信息,对于前列腺癌的诊断和治疗具有指导意义。
然而,它并不能单独用于诊断,需要结合其他临床信息进行综合评估。
如果有前列腺相关症状,建议及时就医,并按照医生的建议进行相关检查和治疗。
《男性前列腺》课件

前列腺位于膀胱和直肠之间, 是男性生殖系统的一部分,具 体位置在骨盆底部的中央。
前列腺的前方是耻骨联合,后 方是直肠,下方是尿生殖膈。
前列腺包绕着尿道,与膀胱颈 和精囊腺紧密相邻。
前列腺的生理功能
分泌前列腺液
前列腺是男性生殖系统中的重要腺体 ,能够分泌前列腺液,前列腺液是精 液的主要成分之一,为精子提供营养 和保护。
《男性前列腺》PPT课件
BIG DATA EMPOWERS TO CREATE A NEW
ERA
• 前列腺概述 • 前列腺常见疾病 • 前列腺疾病的预防与治疗 • 前列腺疾病的日常保健
目录
CONTENTS
01
前列腺概述
BIG DATA EMPOWERS TO CREATE A NEW
ERA
前列腺的生理位置
注意个人卫生,保持会阴部清洁。
前列腺炎的治疗
药物治疗:根据前列腺炎的病原体和病情严重程度,选择合适的抗生素 进行治疗。
前列腺炎的预防与治疗
物理治疗
如微波、射频等物理治疗方法,可缓解前列腺炎的症状。
生活方式调整
如改善生活习惯、加强锻炼等,有助于缓解前列腺炎的症状。
前列腺增生的预防与治疗
前列腺增生的预防 控制体重,避免过度肥胖。
总结词:合理饮食是预防前列腺疾病的重要措施,应注重 营养均衡,适量摄入蛋白质、脂肪和维生素等。
在此添加您的文本16字
详细描述
在此添加您的文本16字
增加蔬菜、水果的摄入,提供丰富的维生素和矿物质。
在此添加您的文本16字
选择低脂肪、低盐、低糖的食物,避免过度刺激前列腺。
在此添加您的文本16字
适量摄入蛋白质,如鱼、瘦肉、豆类等,以满足身体需求 。
前列腺高潮的益处从医学角度看

前列腺高潮的益处从医学角度看前列腺高潮是指男性在性行为中,通过刺激前列腺而产生的高潮感。
前列腺高潮在医学上有着很多益处,对男性身体和性健康有着积极的作用。
本文将从医学角度探讨前列腺高潮带来的益处,分析其对男性健康的重要性。
一、促进前列腺健康前列腺是男性生殖系统中的一个重要器官,它位于膀胱下方,环绕着尿道。
前列腺的主要功能是分泌液体,帮助稀释精液,提供营养物质,从而增加精液的存活时间和活动力。
而前列腺高潮可以通过刺激前列腺,促进其功能的正常运作,有利于维护和改善前列腺的健康。
研究表明,前列腺高潮可以增强前列腺的血液循环,促进养分的输送,帮助预防前列腺炎等前列腺疾病的发生。
此外,前列腺高潮还可以通过排出乳酸和废物,清洁前列腺的管道,减少炎症的风险。
因此,经常进行前列腺高潮可以帮助维持前列腺的健康状态,减少前列腺相关疾病的风险。
二、促进性生活质量前列腺高潮作为一种特殊的性快感,对于提升性生活质量,增加性满足感具有显著的影响。
在性快感过程中,前列腺高潮可以增加性欲的满足感和快感体验,提高性高潮的强度和愉悦感。
同时,前列腺高潮还可以延长性快感的时间,增加性交持续时间,提升性生活的欢愉度。
具体来说,前列腺高潮可以引发勃起,增加性交时的刺激感,进而增加快感的强度和全身的放松感。
此外,适当地刺激前列腺还可以增加射精量,提高精液质量,进一步增加性满足感。
因此,通过经常进行前列腺高潮,男性可以提升性生活的质量,让性经历更加愉悦和满足。
三、缓解压力和改善心理健康性行为和性高潮对于缓解压力和改善心理健康有着重要的作用。
在性高潮时,大脑会释放多巴胺和内啡肽等快乐激素,带来快感和满足感,有助于缓解焦虑和压力。
前列腺高潮作为一种独特的性快感方式,可以激发额外的快感和放松感,对缓解压力和焦虑有更为显著的效果。
此外,前列腺高潮还可以改善男性的心理健康状况。
性高潮能够促进大脑皮层的兴奋,增加快感和满足感的体验,激发积极的情绪和情感表达,帮助减轻抑郁和焦虑等负面情绪。
前列腺专业知识销售话术

前列腺专业知识销售话术1. 引言:什么是前列腺?大家好,今天咱们聊聊前列腺。
听起来是不是有点尴尬?嘿,别担心,这可是关乎健康的大事。
前列腺其实是个小巧的腺体,位于男性的膀胱下方,形状像个小核桃。
它的主要任务就是分泌一种液体,这种液体是精液的主要成分之一,帮助小伙子们在生育方面出一份力。
说白了,前列腺就像是咱们身体里的一个小工厂,默默无闻地支持着大局。
不过,有时候,这个“小工厂”也会出现点小问题,导致一些烦人的症状,比如尿频、尿急,甚至疼痛。
听起来是不是有点严肃?其实,很多人对这方面知识都不太了解,所以今天就来给大家普及一下,轻松又愉快地聊聊这个话题。
2. 前列腺常见问题2.1 前列腺炎先说说前列腺炎,这个名字听着就让人觉得不舒服。
它可是个常见的“老朋友”,大多数男性在一生中可能会碰到它。
这种病的症状真的是五花八门,有时候尿道刺痛,有时候腹部隐隐作痛,甚至还有人感觉腰部也跟着“搭便车”。
总之,你会觉得这小腺体像是个不安分的家伙,时不时就搞出点动静来。
对了,很多人以为前列腺炎就是年轻人的专利,其实不然,老中青都有可能中招。
医生常常会建议多喝水,多走动,当然,别忘了要保持愉快的心情,心情好了,病也好得快呀!2.2 前列腺增生说完炎症,再聊聊前列腺增生。
这个可不是小事,许多上了年纪的男性朋友可能都碰过。
简单来说,前列腺增生就像是这个腺体“变得有点大”,就像你家里的树长得太茂盛,影响了周围的环境。
结果,尿路被挤压,尿不畅,老是想上厕所,尤其是在晚上,几乎像被“尿鬼”缠上了一样。
要知道,晚上的好梦可是金贵的啊!很多人为了躲避这个问题,可能就开始考虑手术了,不过在做决定之前,还是要多咨询医生的意见,毕竟这是个比较重要的选择。
3. 预防和护理3.1 健康生活方式那么,咱们该如何预防这些烦人的问题呢?首先,保持健康的生活方式至关重要。
饮食方面,少吃油腻和辛辣的食物,多吃蔬菜水果,像是西红柿、南瓜等,对前列腺特别有好处。
人体解剖学中的前列腺结构与功能
物理治疗
如微波、射频等物理治疗方法,可用 于缓解慢性前列腺炎等引起的疼痛和
不适感。
手术治疗
对于前列腺癌等严重疾病,手术切除 是主要的治疗方法,包括根治性前列 腺切除术和放疗等。
生活方式调整
保持良好的生活习惯,如戒烟、限酒 、规律作息等,有助于预防和缓解前 列腺疾病。
预防措施
定期体检
定期进行前列腺相关的检查, 如直肠指诊和PSA检测,有助
直肠指检
医生通过直肠指检触摸前列腺 ,有助于发现前列腺肥大、炎 症等病变。
前列腺超声检查
通过超声检查可以观察前列腺 形态、大小及有无异常回声等 。
前列腺液检查
通过前列腺按摩采集前列腺液 ,检查前列腺液的成分和炎症 指标。
及时就医
01
02
03
关注身体症状
如出现尿频、尿急、尿痛 、排尿困难等症状时,应 及时就医。
前列腺癌
病因
与遗传、环境、生活习惯等多种因素有关。
症状
早期无明显症状,随着肿瘤的增大,可能出现尿 频、尿急、尿痛、排尿困难等症状。
治疗
治疗方法包括手术切除、放疗、化疗等,根据病 情选择合适的治疗方案。
04
前列腺疾病的诊断与治疗
诊断方法
直肠指诊
医生通过手指触摸直肠前壁,检查前列腺的大小、质地和是否有硬结 等异常情况。
前列腺特异性抗原(PSA)检测
通过抽取血液样本,检测血液中PSA的水平,辅助判断前列腺癌的可 能性。
超声检查
利用高频声波显示前列腺的形态和大小,观察内部结构是否正常。
核磁共振成像(MRI)
高分辨率的影像技术,能够清晰显示前列腺的解剖结构和异常病变。
治疗方法
药物治疗
关于前列腺的描述

关于前列腺的描述前列腺是男性生殖系统中的一个重要器官,其功能和健康对男性的性生活和生育能力有着重要影响。
下面将对前列腺的结构、功能和常见疾病进行详细介绍。
前列腺位于男性盆腔底部,围绕着尿道的一部分,呈现出类似于桃子的形状。
它的大小和形状因个体差异而有所不同,一般来说,前列腺的大小约为栗子或核桃的大小。
前列腺由腺体和平滑肌组成,腺体主要负责分泌前列腺液,平滑肌则协助射精过程。
前列腺的主要功能是分泌前列腺液,这种液体是精液的重要组成部分,约占精液的30%。
前列腺液的主要成分是水、蛋白质、酶和矿物质等,它为精子提供了营养和保护,有助于精子在女性生殖道内存活和游动。
此外,前列腺液还能中和尿道内的酸性环境,保护精子免受酸性环境的损害。
然而,前列腺也容易发生一些疾病,常见的有前列腺炎、前列腺增生和前列腺癌等。
前列腺炎是前列腺最常见的疾病之一,常见症状包括尿频、尿急、尿痛、会阴不适等,严重的时候还可能出现发热和寒战等全身症状。
前列腺增生是指前列腺细胞的异常增生导致前列腺体积增大,常见症状包括尿频、尿急、尿痛、排尿困难等。
前列腺癌是男性常见的恶性肿瘤之一,早期往往无明显症状,晚期可出现尿频、尿急、尿痛、血尿、性功能障碍等症状。
为了维护前列腺健康,男性需要注意一些生活习惯和饮食。
首先,保持规律的生活作息,充足的睡眠和适当的运动对前列腺健康非常重要。
其次,避免长时间久坐或久站,因为这会增加前列腺充血的机会。
此外,保持适当的性行为频率也有助于前列腺的健康,过于频繁或过于稀少的性行为都可能对前列腺产生不良影响。
在饮食方面,一些食物被认为对前列腺健康有益。
例如,番茄和西红柿制品中富含的番茄红素被认为对前列腺有保护作用。
此外,坚果、鱼类、花生和豆类等富含Omega-3脂肪酸的食物也有助于前列腺健康。
此外,适当的饮水量和避免过量摄入辛辣食物也对前列腺健康有积极影响。
前列腺是男性生殖系统中的重要器官,其分泌的前列腺液对精液的营养和保护起着重要作用。
你了解前列腺吗? 前列腺都有哪些功能?

你了解前列腺吗?前列腺都有哪些功能?
虽然前列腺是男人最重要的器官之一,但大部分男人对这个器官都不是很了解,只知道保护前列腺健康非常重要。
既然如此,今天就来告诉大家前列腺都有哪些功能,希望对大家今后的性福生活有一定帮助。
★1、具有外分泌功能
★
前列腺是男性最大的附属性腺,亦属人体外分泌腺之一。
它可分泌前列腺液,是精液的重要组成成分,对精子正常的功能具有重要作用,对生育非常重要。
前列腺液的分泌受雄性激素的调控。
★2、具有运输功能
前列腺实质内有尿道和两条射精管穿过,当射精时,前列腺和精囊腺的肌肉收缩,可将输精管和精囊腺中的内容物经射精管压入后尿道,进而排出体外。
综上所述,前列腺有四项重要的功能,在人体内发挥了重要作用。
★3、具有控制排尿功能
★
前列腺包绕尿道,与膀胱颈贴近,构成了近端尿道壁,其环状平滑肌纤维围绕尿道前列腺部,参与构成尿道内括约肌。
发生排尿冲动时,伴随着逼尿肌的收缩,内括约肌则松弛,使排尿顺利进行。
★4、具有内分泌功能
前列腺内含有丰富的5α-还原酶,可将睾酮转化为更有生理活性的双氢睾酮。
双氢睾酮在良性前列腺增生症的发病过程中起重要作用。
通过阻断5α-还原酶,可减少双氢睾酮的产生,从而使增生的前列腺组织萎缩。
前列腺ppt课件
前列腺增生
前列腺增生是老年男性常 见的良性疾病,主要表现 为排尿困难、尿流细弱等 。
前列腺癌
前列腺癌是男性常见的恶 性肿瘤之一,早期症状不 明显,晚期可出现血尿、 骨痛等。
02
前列腺炎
发病原因及危险因素
01
02
03
04
细菌感染
如大肠杆菌、金黄色葡萄球菌 等,通过尿道上行感染前列腺
。
生活习惯
长时间久坐、憋尿、饮食不规 律等不良生活习惯增加患病风
03
前列腺增生
发病原因及危险因素
年龄因素
随着年龄的增长,前列腺增生 的发病率逐渐上升。
遗传因素
家族中有前列腺增生病史的人 群,患病风险增加。
激素水平
雄激素和雌激素的平衡失调可 能导致前列腺增生。
生活方式
缺乏运动、饮食不当、长期久 坐等不良生活习惯可能增加患
病风险。
症状表现与诊断方法
症状表现
尿频、尿急、尿痛、排尿困难、尿潴留等。
注意个人卫生
保持外阴部清洁干燥,避免长时 间久坐,减少前列腺受压。
合理安排性生活
适度规律的性生活有助于前列腺 液的排出,减少炎症发生。
饮食结构调整建议
增加膳食纤维摄入
01
多食用蔬菜、水果等富含膳食纤维的食物,有助于改善肠道环
境,减少便秘对前列腺的影响。
控制脂肪和糖分摄入
02
减少高脂肪、高糖食物的摄入,以降低肥胖和代谢综合征的风
险,从而保护前列腺健康。
补充优质蛋白质
03
适量食用鱼、禽、蛋、奶等优质蛋白质食物,有助于维持肌肉
和免疫系统健康。
运动锻炼对前列腺的益处
改善血液循环
运动可以促进全身血液循环,包括前列腺部位的血液供应,有助于 炎症的消退和组织的修复。
前列腺健康科普——认识前列腺

前列腺健康科普——认识前列腺一、什么是前列腺?前列腺是男性特有的一种性腺器官,前列腺如栗子一般,底部朝上,和膀胱相贴,尖朝下,抵泌尿生殖膈,前面贴耻骨联合,后面依着直肠,因此前列腺肿大时可进行直肠指诊,触知前列腺的背面。
因尿道从前列腺体的中间部位穿过,因此可以说前列腺扼守尿道伤口,因此一旦前列腺出现功能障碍,那么首先受影响的就是排尿功能。
前列腺是人体少有、有着内外双重分泌功能的性分泌腺,其是外分泌腺,其每天分泌的前列腺液2ml,是精液的重要成分;其还是内分泌腺,因此前列腺分泌的激素也被称为“前列腺素”。
二、前列腺的生理功能1.外分泌功能男性最大的附属性腺为前列腺,其也是人体外分泌的一种分泌腺。
可通过其分泌前列腺液,是精液的重要一部分内容,可以全面发挥精子的正常功能,有利于其生育。
雄性激素的调控对其前列腺分泌产生较大的影响。
1.内分泌功能前列腺中含有的5α-还原酶相当丰富,可以让睾酮向双氢睾酮转变,且其具有生活理性。
良性前列腺增生症发病期间,双氢睾酮的作用不言而喻。
通过将5α-还原酶阻断,降低双氢睾酮的产生,避免已经增生的前列腺组织萎缩。
1.控制排尿功能前列腺包含了尿道,其和膀胱颈贴近,最终构成了近端尿道壁,尿道前列腺部被环状平滑肌纤维围绕,参与并构成了尿道括约肌。
排尿冲动时在逼尿肌的收缩中让内括约肌松弛,因此有利于顺利排尿。
1.运输功能尿道和两条射精管穿过前列腺实质,射精时精囊腺和前列腺的肌肉收缩,可以通过射精管将输精管和精囊腺中的内容物压入后尿道,最后排出体外。
总之,前列腺具有上述四大功能,均可以在人体中发挥相当重要的作用。
三、前列腺的感染途径1.经尿道直接蔓延前列腺感染诸多途径中经尿道直接蔓延是常见的一种。
细菌进入上尿道主要通过尿道口,之后通过前列腺导管侵入前列腺体,最终导致慢性前列腺炎或急性前列腺炎的发生。
但是,前列腺炎的发生与淋菌性尿道炎联系相当密切,且随着淋病在我国的发展,其已经成为引发慢性前列腺炎的重要原因。
前列腺医学基础知识(幻灯稿)
前列腺有哪些四个主要功能? 前列腺有哪些四个主要功能?
• 具有外分泌的功能 – 分泌前列腺液。前列腺液是精液的重要组成 ,为精子生存提供能量及其 分泌前列腺液。 活动创造条件。 活动创造条件。 • 具有内分泌的功能 – 分泌前列腺素等激素 • 控制排尿功能 – 环状平滑肌纤维围绕前列腺尿道部,参与构成尿道前列腺部 环状平滑肌纤维围绕前列腺尿道部, • 参与射精 – 将精囊和输精管中的内容物及腺泡腺管中的分泌物输入近端尿道
外周区: 外周区:
前列腺组织由哪几部分组成? 前列腺组织由哪几部分组成?
70%为腺体组 % 织
30%为肌肉纤维基质 %
表面有被膜覆盖包住
影响口服药物进入前列腺内部组织结构是怎样的? 影响口服药物进入前列腺内部组织结构是怎样的?
• 前列腺被膜的三层组织结构: 前列腺被膜的三层组织结构:
– 外层:为丰富的静脉和疏松结缔组织 外层: – 纤维鞘: 纤维鞘: – 肌层:肌层与间质组织内的大量肌肉 肌层: 纤维相联
缓解主要症状
排尿刺激症状 前列腺触痛 耻骨上疼痛 排尿刺激症状 夜尿增多 会阴部不适Fra bibliotek临床疗效
疗程
3个月
总有效率>70-80% 总有效率>70-80% >70
翁沥通胶囊
总有效率>80% 总有效率>80% >80 可减小增生的体积
3个月
泽桂癃爽胶囊
古今大量验方+临床验方, 古今大量验方+临床验方,行淤散 结,化气利水 多种疗效较好的中药直肠栓剂之一。 多种疗效较好的中药直肠栓剂之一。 排尿刺激症状 伴有便秘者效果更好 疼痛症状 基础用药,见效快。疗效确切、 基础用药,见效快。疗效确切、价 格低廉。耐受性、治疗差异大。 格低廉。耐受性、治疗差异大。一 过性体位性低血压和逆行射精。 过性体位性低血压和逆行射精。 副作用小,选择性高,价高。 副作用小,选择性高,价高。炎症 合并增生者。 合并增生者。 合并增生,具有明显疼痛、血尿、 合并增生,具有明显疼痛、血尿、 血精患者。需长期服用, 血精患者。需长期服用, 疼痛症状 排尿无力 疼痛症状 排尿无力 疼痛症状
前列腺与射精过程

前列腺与射精过程射精是男性性行为中关键的一部分,其中前列腺在射精过程中扮演着重要的角色。
本文将详细阐述前列腺的功能以及其与射精过程的关系。
前列腺是男性生殖系统的一部分,位于膀胱下方,紧邻尿道。
它是一种具有腺体功能的器官,主要由前列腺上皮细胞和前列腺液组成。
前列腺液是一种无色黏稠液体,富含蛋白质、糖类和离子等成分。
前列腺的主要功能是分泌前列腺液,将其储存于体内,随后在射精过程中将其释放出来。
前列腺液的主要成分占射精液的很大比例,它提供了维持和保护精子的营养,有助于其在女性生殖道中的存活。
此外,前列腺液还能够改变尿道酸碱度,提供较优的环境条件,使得精子在射精后能够顺利前进。
前列腺的功能与射精过程密切相关。
当性兴奋达到一定程度时,附睾会将精子输送至射精管开端,同时,前列腺开始分泌前列腺液。
在射精时,射精管壁的平滑肌开始收缩,将精子和前列腺液推入尿道腔内。
同时,膀胱颈部的平滑肌闭锁起来,阻止尿液进入尿道。
随后,射精肌收缩,将精液从尿道中排出。
前列腺疾病对射精过程有潜在的影响。
前列腺炎是最常见的前列腺疾病之一,可能导致前列腺功能障碍,如前列腺液分泌减少、质量下降等。
这些问题可能影响到精液的质量和精子的存活能力,从而对生育能力产生不利影响。
除了生殖功能外,前列腺还与尿道功能有密切关系。
射精过程中,前列腺液的释放有利于清洗尿道内的精子,减少尿道内的残留精子数量。
这样可以提高尿道的通畅性,预防尿道感染等问题的发生。
综上所述,前列腺是射精过程中不可或缺的一部分。
它通过分泌前列腺液,为精子提供了合适的环境和养分,同时在射精过程中起到排泄和保护的作用。
然而,前列腺疾病可能对射精和生育能力产生不利影响,因此,对前列腺的健康保护和疾病预防至关重要。
通过对前列腺与射精过程的探讨,我们更加深入地了解了男性生殖系统的重要组成部分以及其功能。
这对于维护男性生育能力和提高生活质量具有重要意义。
因此,在日常生活中,我们应该重视前列腺的健康,通过适当的生活方式、定期的体检和及时的治疗来保护前列腺的功能和健康。
前列腺 PPT课件

重解 返除 自排 由尿 生困 活扰
2019/9/16
28
④避免腹内压↑
⑤禁止灌肠、
肛管排气(一周内) 5、引流管护理 6、伤口及会阴部护理 7、早期活动
防血栓形成床上→下床活动 8、常规护理
健康教育
1、术后1-2月,避免剧烈活动------防出血 (跑 步、骑自行车、性生活) 2、TURP术后定期扩张尿道------防狭窄 3、功能训练(膀胱、盆底肌肉) 4、饮食及生活指导------避免诱因5、用药指导6、 门诊随访
3、膀胱痉挛护理
并发症的观察和护理
TUR综合症:术中大量冲洗液被吸收使血容量急剧增加,形成稀释性低
钠血症,病人表现出烦躁、恶心、呕吐、抽搐、严重者肺水肿、脑水肿等。 术后应加强病情观察,注意监测电解质变化。一旦出现,立即给予氧气吸入,遵 医嘱给予利尿剂、脱水剂,减慢输液速度,静脉注射3%氯化钠纠正低血钠。 出血
前列腺大小分度及估计
正常大小3.52.52.5cm, 重18~20g。 分度:I度 鸽子蛋大小,重20~25g
II度 鸡蛋大小, 重25~50g III度 鸭蛋大小, 重50~75g
英雄难过一“腺”关
W C
2019/9/16
15
治疗
等待观察 药物治疗 手术治疗 其他方法
处理原则
1、药物治疗:(1)α 1受体阻滞剂---有效降低膀胱颈 及前列腺平滑肌张力,减少尿道阻力,改善排尿功 能。常用药物有特拉唑嗪。(2)5α 还原酶抑制剂--激素类药物,在前列腺内阻止睾酮变为双氢睾酮 ,使前列腺体积缩小,改善排尿症状。一般服药后3 个月后见效,停药后易复发,需长期服用。(3)植 物类药----包括中草药
目前公认老龄和有功能的睾丸是BPH发
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
대한남성과학회지:제29권 제2호 2011년 8월Korean J Androl. Vol. 29, No. 2, August 2011/10.5534/kja.2011.29.2.101101접수일자: 2011년 8월 4일, 수정일자: 2011년 8월 21일,게재일자: 2011년 8월 22일Correspondence to: Du Geon MoonDepartment of Urology, Korea University Guro Hospital, Korea University Institute of Regener-ative Medicine, 97, Gurodong-gil, Guro 2-dong, Guro-gu, Seoul 152-703, KoreaTel: 02-2626-3201, Fax: 02-2626-1321E-mail: dgmoon@korea.ac.krBasic Principles of Laser for Prostate SurgeryJin Wook Kim, Du Geon MoonDepartment of Urology, Korea University Guro Hospital, Korea University Institute of Regenerative Medicine, Seoul, Korea=Abstract =Recent advances in laser technology have provided a varied arsenal for endoscopic treatment of benign prostatic hyperplasia. Laser is a collimated coherent radiation of photons generated by stimulated emission of gain media, allowing transfer of selective, controlled and focused energy to the targeted tissue. The application of laser to prostate surgery developed hand-in-hand with refinements to the equipment. Earlier lasers were low powered modalities with no significant tissue selectivity, aimed at thermal coagulation and resulted in significant side effects and recurrence. Since then, prostate lasers have developed towards a more high-powered and selective modality that allowed complete ablation of the tissue with fewer complications. Fiber technology has also developed to allow efficient and safe transfer of a continuously increasing energy output. It is important for the surgeon to understand these fundamental principles of laser and prostate surgery, not only to select the proper tools, but also to properly implement the technique as well.Key Words: Prostatic hyperplasia, Laser therapy, Solid-state lasersIntroductionLaser surgery represents a method for delivering precise controlled high levels of energy to relatively specific targets. Since the introduction of laser for practical use, the field of urology actively accepted its clinical applications. In the prostate, laser was widely adopted as a method to aid in reducing bleeding, effec-tively removing tissue without significant injury to the surrounding tissue for patients with benign prostatic hyperplasia (BPH).The theoretical outline of the laser was first estab-lished by Einstein in his seminal paper “Zur Quanten-theorie der Strahlung” in which he described the basis of stimulated emission of electromagnetic radiation. It was not long after that several applications were pre-sented, beginning with the MASER (Microwave am-plification by stimulated emission of radiation) at Bell laboratories by Townes. Later the application of this principle to the visible spectrum was suggested in-dependently by several researchers. In 1959, Gould proposed the acronym LASER (Light Amplification by Stimulated Emission of Radiation). However, it was in 1960 when Maiman completed the first functional la-ser, using ruby crystals as the gain medium.While the ruby crystal lasers were introduced to clinical applications early in the history of medical la-sers, development of prostate lasers was not actively pursued until the 1990s. Early attempts included The initial clinical approach to prostate laser surgery began with Costello’s use of the Nd:YAG laser.1 However, initial applications were fraught with difficulties, main-ly from technical shortcomings. Recent development of prostate laser surgery has allowed us access to sev-102대한남성과학회지: 제29권 제 2호 2011Fig. 1. Lasers are generated by stimulated emission, brought about by pumping the gain medium to an excited state. Released photons oscillate within the optical resonator to emit a collimated, coherent monochromatic electromagnetic radiation.eral different types of lasers and their appropriate methods of application. With such variety of choices, it is important for the surgeon to not only to be famil-iar with the basic principles behind its application, and to understand the difference between the various lasers and its peripherals, but more importantly to properly familiarize oneself with the proper method of surgical application based on such knowledge.1. Principles of LaserLaser is a device which emits monochromatic, colli-mate, coherent light by stimulated emission from again medium.2The gain medium of the laser is stimu-lated by an external energy source, which is typically an arc light or, in some cases, another semiconductor laser. When stimulated, electrons in the gain mediumare excited to a higher energy state. If sufficient en-ergy is applied, the electrons become more populated in a higher energy state than the resting state, achiev-ing population inversion. Light passing through the ac-tivated gain medium stimulates the release of electrons from the high energy state back to resting state, releas-ing electromagnetic radiation corresponding to the dif-ference in quantum energy levels. Light is amplified as the output from the gain medium is greater than thelight absorbed.3Furthermore, light is repeatedly passed through the gain medium by parallel reflectors, form-ing an optic resonator (Fig. 1).The frequency of electromagnetic radiation output is determined by the excitation state achieved by the gain medium, as well as further dopates that modify the en-ergy response. Typically yttrium aluminum garnet (YAG) crystals are used as a solid gain medium forprostate lasers.4Rare earth elements, such as neo-dymium, holmium and thulium are used as dopates to modify the energy level. The frequency of the laser is determined by the difference in quantum orbital states of excitation and resting, and is thus constant and monochromatic.Wavelength characteristics also affect how the laser interacts with the target tissue. Wavelength determines how much energy is diffracted in the irrigant, how much energy is absorbed by the target tissue, and how much energy penetrates to what depth of the tissue, aswell.5More importantly, wavelength determines which types of tissue may better absorb the light energy, and influences the proportion of energy converted to heat. In some tissues, substances react to specific wave-lengths, better absorbing laser energy. These sub-stances, called chromophores, may include biological substances such as melanin, hemoglobin, bilirubin, porphyrin, carotene, and even common substances likewater.6In the prostate, hemoglobin and water are themajor chromophores.7Another important variable in the application of la-ser is laser power. Power influences the amount of en-ergy transfer to the tissue, resulting in varying tissue effects between coagulation, vaporization and evenmechanical tearing.8The amount of energy transfer, dictated by power, results in different levels of temper-Jin Wook KimㆍDu Geon Moon: Lasers in Prostate Surgery103 Table 1.Different tissue effects appear by level of energytransfer42<40o C 42∼45o C 45∼50o C 50∼100o C >60o C>100o C PhotobiomodulationHyperthermiaDesiccationCoagulation, irreversibleProtein denaturationCarbonization,vaporizationFig. 2.Tissue effect can also vary with the depth of penet-ration, due to different levels of temperature achieved withinthe affected zone.42Fig. ser wavelength and mode of emission can affect thedepth of penetration, leading to a varied profile of energydensity (HPS: high performance system, CW: continuouswave).42ature achieved within the tissue (Table 1, Fig. 2). The power generated from the laser is also ex-pressed in the mode of emission, either as a con-tinuous wave or a pulsed wave based on power output by time scale. To generate a continuous wave it is re-quired for population inversion of the gain medium to be continually replenished by a steady pump source. Some laser gain media cannot achieve a high output continuous wave sufficient for vaporization, as it would require pumping the laser at a very high con-tinuous power level that would destroy the gain me-dium by producing excessive heat.9Alternative meth-ods are used to modulate pulsed frequencies to either achieve higher peak output, using Q-switching, or maintaining semi-continuous output by pulse pumping.3 While continuous wave lasers can achieve a constant controlled clinical interaction with the tissue, pulsed wave laser can deliver forceful bursts of laser, which is now primarily used for fragmenting stone.The interaction of laser with tissue results in a series of fundamental optical phenomena that integrates to form a characteristic profile of each laser. Reflection occurs as the laser beam strikes the tissue surface due to difference in refractive indices of the irrigation fluid and prostate tissue.10For the Nd:YAG laser, approx-imately 50% is reflected due to the sudden change in refractive index.11Laser energy also scatters on con-tact with the irregular tissue surface. Scattering may occur either in a forward or backward direction. Only non-reflected and non-absorbed forward scattering photons are transmitted to either be absorbed or trans-mitted by the tissue. Wavelength is the primary varia-ble in all of these interactions, as it governs the index of refraction, as well as absorption and scattering coefficients.In a practical sense, laser tissue interactions can be summarized by two characteristic parameters, absorp-tion coefficient (AC) and the extinction length (EL).5 A higher AC denotes greater absorption of energy by the tissue, while a lower AC indicates significant transmission of energy to underlying structures. Ex-tinction length is defined as the depth of tissue at which energy transmission is reduced by 90%. It is generally considered the depth to which laser energy directly affects the tissue. Furthermore, a short ex-tinction length indicates high energy density, leading to a propensity for tissue ablation, while a longer ex-tinction length indicates lower energy density and a propensity for tissue coagulation (Fig. 3).2. Prostate lasersWhile in theory, the application of laser to the treat-ment of BPH seemed imminent, several technical dif-104대한남성과학회지: 제29권 제 2호 2011Table 3. Different lasers are characterized primarily by wavelengths. However, interactions with different chromophores, andmodes of generation also affect tissue interactions and depth of tissue effect10,20,37Wavelength (nm)Chromophore Extinction length (mm)Wave mode Tissue interaction Nd:YAG Ho:YAG KTP Tm:YAG Diode1,0642,100 5322,000940/980/1,470-WaterHemoglobin WaterWater and hemoglobin100.40.8 0.25VariablePulse or CW PulseQuasi-pulse CWPulse or CWCoagulation Vaporization Vaporization Vaporization VaporizationCW: continuous wave.Table 2. Prostate laser developed from the early low power Nd:YAG to the contemporary modalities through increased power and optimized wavelengths 29,37,43,44Year MethodLaser191719601993199419951995, 1996, 19971998200520072008Theory of stimulated emission of electromagnetic radiation First functional Laser VLAP CELAP ILCHoLAP, HoLRP, HoLEP PVPThulium laser resection of prostate Laser vaporization of the prostate PVPRuby Nd:YAGNd:YAG +Ho:YAGNd:YAG, Diode (70 W)Ho:YAGKTP (60∼80 W)Tm:YAGDiode (120∼200 W, 980 nm)HPS: KTP or LBO (120 W)VLAP: visual laser ablation of the prostate, CELAP: combined endoscopic laser ablation of the prostate, ILC: interstitial laser coagulation, HoLAP: holmium laser ablation of the prostate, HoLRP: holmium laser resection of the prostate, HoLEP: holmium laser enucleation of the prostate, PVP: photovaporization of the prostate, HPS: high performance system.ficulties had to be overcome. The most important tech-nical aspect was finding the right laser to achieve ef-fective ablation with few side effects. The initial de-velopment began with the widely used Nd:YAG laser, and progressed towards achieving more powerful out-put, more effective power usage, and safer treatment outcomes (Table 2, 3).1) Nd:YAG laser: Treatment of prostate using lasers was first introduced in 1986. However, it was with the introduction of side-firing Nd:YAG laser in the early 90s that achieved a more widespread use. The 1,064 nm was used to perform visual laser ablation of theprostate (VLAP).1The Nd:YAG laser, though cur-rently fallen out of favor, represents the first foray into laser surgery for prostatic enlargement. The 1,064 nm wavelength of this laser penetrates tissue up to 10 mm. Early VLAP involved a 40 W laser directed at rightangles to the prostatic tissue.12Compared to TURP, the VLAP was safe to perform on patients taking anti-coagulants, and carried no risk of developing TURsyndrome.13However, due to the low energy absorp-tion, tissue temperatures seldom rose above 65oC, re-sulting in broad tissue coagulation. Sloughing off of necrotic tissue followed treatment up to 6 months, ac-companied by dysuria, and patients often required pro-longed catheterization.14A different approach used the Nd:YAG fiber in con-tact with the tissue, as energy delivery is increased with decreasing breadth between the fiber and tissue,contact of the fiber could achieve vaporization.15However, with the limited power output, tissue abla-tion was too slow, and the procedure was limited to smaller lesions (<40 ml).Finally, interstitial laser coagulation (ILC) allowed for treatment of larger volumes by repeatedly inserting the fiber within the tissue, creating coagulation ne-crosis without sloughing, and even preserving theurothelium.9Despite these innovations, ILC showedJin Wook Kim ㆍDu Geon Moon: Lasers in Prostate Surgery105Fig. 4. Chromophores allow selective absorption of specific wavelengths, vastly improving the tissue effect of certain lasers. Early Nd:YAG lasers are generally nonspecific to either water or hemoglobin. Modern green light lasers are highly absorbed by hemoglobin, while modern infrared lasers are highly absorbed by water.5Fig. 5. Increased power allows the beam to be more collimated. The tissue laser interaction not only benefits from more power, but also from a more focused high intensity transfer of energy (HPS: high performance system, PV: photo vaporization).44poor results with urinary infection rates as high as 35%, and retreatment at 1 year as high as 15%. The fundamental limitation of the Nd:YAG laser and its 1,064 nm wavelength was its lack of corre-sponding tissue chromophores, which could enhance absorption despite its limited output and thus effec-tively achieve vaporization.2) 532 nm photovaporization: The GreenLight laser photoselective vaporization (American Medical Systems,Minnetonka, MN) was introduced by Malek in 1998.16The KTP is often hailed as a milestone in achieving a safe and effective prostate laser treatment through re-liable tissue vaporization. The wavelength of KTP is achieved by “frequency doubling” the Nd:YAG laser. Frequency doubling involves a primary pump laser that is passed through a secondary nonlinear crystal which creates a secondary harmonic wave that is dou-bled in frequency. The energy conversion rate is gen-erally high, with most frequency doubled energy at least 50% of the primary input, and in some laser ach-ieve above 80%.17Hence, with the Nd:YAG laser transformed by KTP crystals, the frequency is modi-fied from 1,064 nm to 532 nm. While the power of the output itself is decreased in comparison to the Nd:YAG laser, the KTP laser compensates by interact-ing with hemoglobin as a chromophore (Fig. 4).18The 532 nm KTP laser is fully transmitted through the irrigant and highly absorbed in the tissue by oxy-hemoglobin in the vessels. This allows energy to be highly transferred to tissue with high oxyhemoglobin content, such as prostatic tissue. With selective absorp-tion of wavelength, high tissue energy density is ach-ieved, and tissue temperatures can be successfully ele-vated above boiling temperature, inducing immediate vaporization. As most of the energy is dissipated with vaporization, and tissue depleted of chromophore form a barrier of inefficient energy transfer, the extinctionlength is significantly reduced to 0.8 mm.19Because of the efficacy of tissue vaporization, side-firing laser ablation with KTP is referred to as ‘photovaporizationof the prostate’ (PVP).20The initial KTP laser to gain popularity was the 80 W lasers delivered by side-firing fibers through a 23 F continuous flow cystoscope with normal salineirrigant.21The initial models conveyed the laser beam on pulsed wave, which compensated for the low power output of the original Nd:YAG lasers that were further burdened by energy loss from frequency doubling, byQ switching.4The shortcomings of the initial models were evident when the working distance increased and laser beams were diffracted, resulting in coagulationrather than vaporization.16Surgeons were advised to maintain a 0.5 mm working distance, termed “near contact”, for effective vaporization.Improvements in power output has seen progression106대한남성과학회지: 제29권 제 2호 2011from the prototype 60 W continuous wave to the 80 W Q switching pulsed wave to the 80 W continuous wave, and currently the 120 W high performance sys-tem (HPS). Modern HPS uses lithium triborate (LBO) crystals, instead of KTP, for frequency doubling. The arc light as pump energy has been replaced with diode lasers allowing higher output without over heating the gain medium. The improved output allowed a working distance of 3∼4 mm, while diode laser pump allowed for adjustable power outputs for either coagulation or vaporization (Fig. 5).Increase power output has also allowed for larger prostates to be treated. The prototype 60 W laser was limited to treat prostates up to 60 g in a reasonable time period. Improved vaporization speed with 80 W lasers allowed vaporization of 80 g prostates in 1 hour.22For larger prostates above 100 g, Sandhu et al23 reported mean operation times of 123 minutes, and re-operation rates of 5% at 1 year. Recently, long term follow up reports, average 30.6 months, showed sus-tained voiding parameter improvements and no rela-tionship with prostate volume.24Retrograde ejaculation (33%) is the most common complication in most long term reports, however transfusion is rarely necessary and reoperation rates are 0∼7% at 5 years.25-27The newer 120 W HPS lasers have yet to report long term results. Recent reports of 120 W laser, however, sug-gested that the high power also resulted in decreased hemostatic ability.28In such cases, modulation to low-er power settings may be useful.3) Ho:YAG laser: The use of holmium as the main dopate for YAG crystals was an early development, initially used for treating urinary calculi. Holmium la-sers also require addition of thulium and chromium to stabilize laser generation, as holmium alone results in severe overheating of the crystal. The benefit of Ho:YAG as a gain medium was its 2,140 nm infrared wavelength that was absorbed by water. Since the tis-sue is composed mainly of water, the majority of the holmium energy is absorbed superficially. The absorp-tion depth in prostatic tissue is 0.4 mm, resulting in tissues being heated above boiling temperature, leading to immediate vaporization without deep coagulation.29 Tissue studies with holmium laser have shown that zones of thermal injury associated with laser ablation range from 0.5∼1.0 mm, resulting in adequate hemo-stasis during ablation even for underlying vessels larg-er than 1.0 mm in diameter.30Holmium lasers typically operate by pulsed wave. In contrast to continuous wave lasers where heat is generated continuously in the target tissue, pulsed waves allow for thermal relaxation time. Tissues re-ceive less thermal injury and more ablative effect with pulsed waves, and the holmium laser, operating on 0.25 ms pulses have been shown to result in minimal thermal damage.While, intuitively, holmium absorption by water may seem that the laser may be ineffective when crossing irrigant fluid, van Leeuwen et al31suggested that laser was capable of penetrating irrigant fluid bar-riers by travelling across the vapor bubbles formed by initial absorption in the irrigant. Nevertheless, ex-cessive vapor bubble formation also results in ob-structed field of view for the surgeon, making direct contact methods the usual preferred choice of appli-cation.The surgical methods of holmium laser application have also undergone several iterations. The first sug-gested method was a hybrid technique using holmium lasers as incision tools, while applying Nd:YAG VLAP techniques for overall debulking by coagulation ne-crosis (CELAP; Combined Endoscopic Laser Ablation of the Prostate).11The CELAP technique, however suf-fered from deep thermal effects of Nd:YAG, resulting in recatheterization rate of 20∼25% of patients. Nd:YAG was then abandoned and holmium laser was used along by non-contact method, called HoLAP (Holmium laser ablation of the prostate).10As noted above, non-contact holmium laser ablation, while pos-sible, was less effective and tedious than direct contact method. HoLRP (holmium laser resection of the pros-tate) simulated TURP by excising prostatic chips by direct contact resection.32Despite the fact that hol-mium incision ablates nearly 75% of the prostatic tis-sue,29HoLRP was able to yield tissue available for histologic examination. A refinement of this method is the present day HoLEP (holmium laser enucleation of the prostate), whereby the holmium laser simulatesJin Wook KimㆍDu Geon Moon: Lasers in Prostate Surgery107open prostatectomy by removing the adenoma at the level of the surgical capsule.8The enucleated tissue is then removed by morcellator, allowing greater yield of tissue and shorter operation time.The major drawback of this procedure is the diffi-cult learning curve, compared to KTP photovapori-zation.7Also, while it shows great tissue absorption, the wavelength does not closely math water absorption peak in tissue, which is located at 1,940 nm. Furthermore, holmium is limited to pulsed wave due to its inefficient energy consumption. The major ad-vantage of holmium laser is its extensive versatility, as it can also be used in various other urological pro-cedures such as laser lithotripsy and urethral stricture resection.294) Newer modalities: Thulium and Diode lasers: GreenLight (KTP or LBO) PVP and HoLEP currently boasts excellent results, possibly supplanting TURP entirely. As of 2008, prostate laser surgery consists of approximately 36.1% of prostate surgeries for bladder outlet obstruction.33Newer modalities have been in-troduced attempting to improve upon current short-comings.By adopting thulium as the dopate for YAG crys-tals, the thulium laser achieves adjustable wavelengths between 1,750 nm and 2,220 nm, allowing exact match of 1,940 nm for optimum water absorption.34 The decrease in wavelength, and optimization to water absorption, greatly reduces thermal damage. Thulium laser is also diode pumped, in contrast to arc lamp pumped holmium laser, allowing for alternating output modes of either continuous or pules waves. Finally, by stabilizing overheating typical of YAG crystals by thu-lium doping and diode pumping, thulium laser are en-ergy efficient, allowing for tabletop devices supplied by common domestic electric outlets to be used as an energy supply. Only few reports have been made, though they have been presented at least equivalent outcomes compared to previous lasers.35Finally, semiconductor diode (SCD) lasers have also been suggested as the next best alternative to KTP and holmium based lasers. As previously noted, 120 W KTP lasers achieve improved ablation abilities while sacrificing hemostasis, with frequencies optimal for hemoglobin absorbance. Conversely, holmium lasers achieve excellent hemostasis; however efficiency drops when not in direct contact. The 980 nm wavelength produced by SCD lasers is attractive as they present high absorption for both hemoglobin and water, thus theoretically providing both optimal hemostatic and ablative properties.36SCD laser, like thulium lasers, al-so use a secondary diode laser as the energy pump, allowing high efficiency/low energy consumption while providing variable wavelengths.37How these ad-vantages will translate to clinical outcomes have yet to be seen.3. Laser fibersOne of the principle advantages of using laser in en-dourology is its innate ability to transfer high levels of energy to difficult-to-reach locations. The primary mediator is the laser fiber that can convey high energy with minimum loss through a small diameter optical conductor, allowing reduction in instrument size. Laser fibers consist of a core optical fiber sur-rounded by two to three layers of optical insulators that act to contain laser within the core fiber by en-hancing the refractive index between the core and out-er layers.38Most high energy medical applications uti-lize fibers within a pure synthetic fused-silica core. Impure or doped cores can cause attenuation of the la-ser beam, leading to fiber failure.39However, the core silica often varies in saturation with hydroxyl (OH) groups. In general, infrared lasers use low OH silica, while visible to ultraviolet lasers use high OH silica. Manufacturing defects in the production of laser fi-bers can result in optical irregularities. Defects can lead to leakage, resulting in charring, or even ex-plosion. Other defects can result in decreased perform-ance, including poor polishing, scratching and dust irregularities. Fiber tip failure may also occur with ad-herence of carbonized tissue.40This increases heat ap-plied to the fiber and may result in thermal failure. Mechanical fiber failure can occur with excessive bending. Laser fibers typically withstand bending to 100 times the primary diameter. With core fiber diam-eters typically in rage of 500μm, this translates to ap-proximately a curve radius of 5 cm.39108대한남성과학회지: 제29권 제 2호 2011Fig. ser fibers also develop to accommodate the increased laser energy. Newer fibers are designed to allow more flexi-bility, less loss of energy and greater safety.41Recent advances in fiber technology have seen mod-ifications to improve durability and flexibility and de-crease irregularities. With increased focus on laser power output, modifications have also aimed to stabi-lize fiber temperature during prolonged use. MoXy fi-bers, for the GreenLight HPS not only increased the fiber diameter to allow increase energy flux through the fiber, but also adopted fiber irrigation to taper ther-mal escape from the fiber (Fig. 6).41ConclusionWith the advent of laser theory at the beginning of the 20th century, laser has shown drastic improvement and rapid clinical application. The present day prostate lasers continuously evolved from the early Nd:YAG laser through improved output, optimization of absorb-ance wavelengths, variable output modes and wave-lengths, and even improved fiber technology to assist in conveying output. However, constant revision of surgical technique has also closely followed each step of technological improvement. Hence it is imperative for the surgeon to understand the underlying principles of prostate laser to provide optimal treatment and to adapt to the rapidly developing technological frontier.REFERENCES1)Costello AJ, Bowsher WG, Bolton DM, Braslis KG,Burt J. Laser ablation of the prostate in patients with benign prostatic hypertrophy. Br J Urol 1992;69: 603-82)Yariv A, Kwong SK. Theory of laser oscillation inresonators with photorefractive gain. Opt Lett 1985;10:454-63)Yariv A. Energy and power considerations in in-jection and optically pumped lasers. P IEEE 1963;51:1723-314)Chen Y. Passive Q-switching of an intracavity fre-quency doubled diode-pumped Nd: YVO/sub 4//KTP green laser with Cr/sup 4+: YAG. Phot Tech Lett IEEE 1997;9:1481-35)Niemz MH. Laser-tissue interactions: fundamentalsand applications. 3 ed. Germany: Springer Verlag;2004;15-86)Bachmann A, Ruszat R. The KTP-(greenlight-) la-ser--principles and experiences. Minim Invasive Ther Allied Technol 2007;16:5-107)Sountoulides P, Tsakiris P. The evolution of KTP la-ser vaporization of the prostate. Yonsei Med J 2008;49:189-998)Gilling PJ, Kennett K, Das AK, Thompson D,Fraundorfer MR. Holmium laser enucleation of the prostate (HoLEP) combined with transurethral tissue morcellation: an update on the early clinical experi-ence. J Endourol 1998;12:457-99)Laguna MP, Alivizatos G, De La Rosette JJ. Intersti-tial laser coagulation treatment of benign prostatic hyperplasia: is it to be recommended? J Endourol 2003;17:595-60010)Gilling PJ, Cass CB, Cresswell MD, Malcolm AR,Fraundorfer MR. The use of the holmium laser in the treatment of benign prostatic hyperplasia. J Endourol 1996;10:459-6111)Gilling PJ, Cass CB, Malcolm AR, Fraundorfer MR.Combination holmium and Nd:YAG laser ablation of the prostate: initial clinical experience. J Endourol 1995;9:151-312)Cowles RS 3rd, Kabalin JN, Childs S, Lepor H,Dixon C, Stein B, et al. A prospective randomized comparison of transurethral resection to visual laser ablation of the prostate for the treatment of benign prostatic hyperplasia. Urology 1995;46:155-60 13)Hoffman RM, MacDonald R, Slaton JW, Wilt TJ.Laser prostatectomy versus transurethral resection for treating benign prostatic obstruction: a systematic review. J Urol 2003;169:210-514)Oesterling JE. Benign prostatic hyperplasia. Medicaland minimally invasive treatment options. N Engl J Med 1995;332:99-10915)Floratos DL, de la Rosette JJ. Lasers in urology.BJU Int 1999;84:204-1116)Malek RS, Barrett DM, Kuntzman RS. High-power。