Sci Transl Med-2012-Edelman-135fs14
吉西他滨或多西他赛联合铂类对晚期肺鳞癌的疗效评价

吉西他滨或多西他赛联合铂类对晚期肺鳞癌的疗效评价胡琴;韦永明;王可武;王银华;宛新安【摘要】Objective To observe the curative effect of gemcitabine combined with platinum (GP group)and docetaxel combined with platinum (DP group)chemotherapy for patients with advanced lung squamous cell carcinoma.Methods fifty-four cases of squamous cell carcinoma were treated by gemcitabine combined with platinum,or docetaxel combined with platinum chemotherapy.Clinical evalu-ation was conducted by chest CT every 2 cycles.Results In GP group and DP group,the median survival periods and 1-year survival rates were 1 1 .8 months vs 9.7 months,48% vs 20.6%,respectively with statistically significant difference(P<0.05);the clinical ef-fective rates and clinical benefit rates were 36%vs 34.4%,84%vs 79.3%,respectively.The GP scheme was slightly higher,yet there was no statistically significant difference(P>0.05 ).Conclusions Similar curative effect of advanced lung squamous cell carcinoma treatment is achieved in both groups,but the GP group performs better survival advantage.%目的:观察吉西他滨联合铂类(GP组)和多西他赛联合铂类(DP组)化疗对晚期肺鳞癌的疗效差异。
bioengineering and translational medicine简介

bioengineering and translational medicine简介《Bioengineering & Translational Medicine》是一本专注于工程生物医学领域的学术期刊。
以下是关于该期刊的简要介绍:
- 该期刊由美国化学工程师协会(AlChE)于2016年创办,现为AlChE会刊,每年出版3期,现在由Wiley出版管理,期刊主编为哈佛大学的Samir Mitragotri 教授。
- 该期刊旨在及时、准确、全面地报道国内外工程生物医学工作者在该领域的科学研究等工作中取得的经验、科研成果、技术革新、学术动态等。
- 该期刊已被多个数据库收录,包括SCIE、BIOSIS Previews、STM Source、PubMed via PMC deposit (NLM)、Biotechnology Source等。
- 该期刊发表的文章类型以研究文章(Article)为主,同时也有综述(Review)、社论(Editorials)等。
- 该期刊主编Samir Mitragotri教授是美国哈佛大学的工程与应用科学教授,也是Bioengineering & Translational Medicine的期刊主编。
他是一位在药物靶向输送、生物医学材料、生物启发工程等领域有深入研究的科学家,已经撰写及合著了210余篇期刊论文,并拥有约150项专利。
总的来说,《Bioengineering & Translational Medicine》是一本在工程生物医学领域具有较高影响力和权威性的学术期刊,为该领域的科研工作者提供了重要的学术交流平台。
《2024年小分子化合物CHIR-99021与白血病抑制因子诱导和维持人脊髓样神经干细胞》范文

《小分子化合物CHIR-99021与白血病抑制因子诱导和维持人脊髓样神经干细胞》篇一小分子化合物CHIR-99021与白血病抑制因子在诱导和维持人脊髓样神经干细胞高质量中的关键作用一、引言近年来,随着干细胞研究的深入发展,神经干细胞的研究和应用越来越受到关注。
小分子化合物CHIR-99021与白血病抑制因子作为两个重要的研究工具,其在诱导和维持人脊髓样神经干细胞(hNSCs)的方面所发挥的巨大作用被广泛关注。
本文将通过一系列实验研究这两个因子如何有效提高hNSCs的质量,并探讨其作用机制。
二、小分子化合物CHIR-99021小分子化合物CHIR-99021是一种GSK-3β的抑制剂,具有促进神经干细胞增殖和分化的作用。
在实验中,我们发现CHIR-99021能够显著提高hNSCs的增殖速度和分化效率,且在维持其多能性方面表现出色。
此外,CHIR-99021还能够改善hNSCs的生存环境,降低其凋亡率,提高其存活率。
三、白血病抑制因子白血病抑制因子(LIF)是一种在胚胎发育过程中起关键作用的细胞因子,对维持hNSCs的自我更新和分化具有重要作用。
实验表明,LIF能够与CHIR-99021协同作用,共同促进hNSCs的增殖和分化。
此外,LIF还能够增强hNSCs对外界刺激的抵抗力,提高其稳定性。
四、CHIR-99021与LIF的协同作用通过实验研究,我们发现CHIR-99021与LIF在诱导和维持hNSCs的过程中具有显著的协同作用。
两者共同作用能够显著提高hNSCs的质量,包括其增殖速度、分化效率、生存能力和稳定性等。
此外,这种协同作用还能够促进hNSCs向神经元和胶质细胞的分化,为神经系统的修复和再生提供更多的可能性。
五、作用机制探讨根据实验结果和文献资料,我们推测CHIR-99021与LIF的作用机制可能涉及多个方面。
首先,两者能够通过调节相关信号通路,如Wnt/β-catenin和JAK/STAT3等,来影响hNSCs的增殖和分化。
《临床肝胆病杂志》推荐使用的规范医学名词术语

临床肝胆病杂志第40卷第3期2024年3月J Clin Hepatol, Vol.40 No.3, Mar.2024[3]XIA SL, LIU ZM, CAI JR, et al. Liver fibrosis therapy based on biomi⁃metic nanoparticles which deplete activated hepatic stellate cells[J]. J Control Release, 2023, 355: 54-67. DOI: 10.1016/j.jconrel.2023.01.052.[4]LIU YW, DONG YT, WU XJ, et al. The assessment of mesenchymalstem cells therapy in acute on chronic liver failure and chronic liver disease: A systematic review and meta-analysis of randomized con⁃trolled clinical trials[J]. Stem Cell Res Ther, 2022, 13(1): 204. DOI:10.1186/s13287-022-02882-4.[5]ZHANG ZL, SHANG J, YANG QY, et al. Exosomes derived from hu⁃man adipose mesenchymal stem cells ameliorate hepatic fibrosis by inhibiting PI3K/Akt/mTOR pathway and remodeling choline me⁃tabolism[J]. J Nanobiotechnology, 2023, 21(1): 29. DOI: 10.1186/ s12951-023-01788-4.[6]ZHAO T, SU ZP, LI YC, et al. Chitinase-3 like-protein-1 function andits role in diseases[J]. Signal Transduct Target Ther, 2020, 5(1): 201. DOI: 10.1038/s41392-020-00303-7.[7]YANG H, ZHAO LL, HAN P, et al. Value of serum chitinase-3-likeprotein 1 in predicting the risk of decompensation events in patients with liver cirrhosis[J]. J Clin Hepatol, 2023, 39(7): 1578-1585. DOI:10.3969/j.issn.1001-5256.2023.07.011.杨航, 赵黎莉, 韩萍, 等. 血清壳多糖酶3样蛋白1(CHI3L1)对肝硬化患者发生失代偿事件风险的预测价值[J]. 临床肝胆病杂志, 2023, 39(7): 1578-1585. DOI: 10.3969/j.issn.1001-5256.2023.07.011.[8]MA L, WEI J, ZENG Y, et al. Mesenchymal stem cell-originated exo⁃somal circDIDO1 suppresses hepatic stellate cell activation by miR-141-3p/PTEN/AKT pathway in human liver fibrosis[J]. Drug Deliv, 2022, 29(1): 440-453. DOI: 10.1080/10717544.2022.2030428. [9]NISHIMURA N, DE BATTISTA D, MCGIVERN DR, et al. Chitinase 3-like 1 is a profibrogenic factor overexpressed in the aging liver and in patients with liver cirrhosis[J]. Proc Natl Acad Sci U S A, 2021, 118(17): e2019633118. DOI: 10.1073/pnas.2019633118.[10]WANG CG, LI SZ, SHI JM, et al. Research progress in differentia⁃tion, identification, and purification methods of human pluripotent stem cells to mesenchymal-like cells in vitro[J]. J Jilin Univ Med Ed, 2023, 49(6): 1655-1661. DOI: 10.13481/j.1671-587X.20230634.王成刚, 李生振, 史嘉敏, 等. 体外人多能干细胞向间充质样细胞分化、鉴定和纯化方法的研究进展[J]. 吉林大学学报(医学版), 2023, 49(6): 1655-1661. DOI: 10.13481/j.1671-587X.20230634.[11]LI TT, WANG ZR, YAO WQ, et al. Stem cell therapies for chronicliver diseases: Progress and challenges[J]. Stem Cells Transl Med, 2022, 11(9): 900-911. DOI: 10.1093/stcltm/szac053.[12]YANG X, LI Q, LIU WT, et al. Mesenchymal stromal cells in hepaticfibrosis/cirrhosis: From pathogenesis to treatment[J]. Cell Mol Im⁃munol, 2023, 20(6): 583-599. DOI: 10.1038/s41423-023-00983-5. [13]ZHAO SX, LIU Y, PU ZH. Bone marrow mesenchymal stem cell-derived exosomes attenuate D-GaIN/LPS-induced hepatocyte apop⁃tosis by activating autophagy in vitro[J]. Drug Des Devel Ther, 2019, 13: 2887-2897. DOI: 10.2147/DDDT.S220190.[14]LEE CG, HARTL D, LEE GR, et al. Role of breast regression protein39 (BRP-39)/chitinase 3-like-1 in Th2 and IL-13-induced tissue re⁃sponses and apoptosis[J]. J Exp Med, 2009, 206(5): 1149-1166.DOI: 10.1084/jem.20081271.[15]HIGASHIYAMA M, TOMITA K, SUGIHARA N, et al. Chitinase 3-like 1deficiency ameliorates liver fibrosis by promoting hepatic macro⁃phage apoptosis[J]. Hepatol Res, 2019, 49(11): 1316-1328. DOI:10.1111/hepr.13396.收稿日期:2023-06-09;录用日期:2023-08-17本文编辑:邢翔宇引证本文:LIU PJ, YAO LC, HU X, et al. Effect of human umbilical cord mesenchymal stem cells in treatment of mice with liver fibrosis and its mechanism[J]. J Clin Hepatol, 2024, 40(3): 527-532.刘平箕, 姚黎超, 胡雪, 等. 人脐带间充质干细胞(hUC-MSC)对肝纤维化小鼠模型的治疗作用及其机制分析[J]. 临床肝胆病杂志, 2024, 40(3): 527-532.读者·作者·编者《临床肝胆病杂志》推荐使用的规范医学名词术语有关名词术语应规范统一,以全国自然科学名词审定委员会公布的各学科名词为准。
医药学类文献双语版_汉译英
介导性shRNA能抑制肺癌细胞中livin沉默基因的表达从而促进SGC-7901细胞凋亡背景—由于肿瘤细胞抑制凋亡增殖,特定凋亡的抑制因素会对于发展新的治疗策略提供一个合理途径。
Livin是一种凋亡抑制蛋白家族成员,在多种恶性肿瘤的表达中具有意义。
但是, 在有关胃癌方面没有可利用的数据。
在本研究中,我们发现livin基因在人类胃癌中的表达并调查了介导的shRNA能抑制肺癌细胞中livin沉默基因的表达,从而促进SGC-7901细胞凋亡。
方法—mRNA及蛋白质livin基因的表达用逆转录聚合酶链反应技术及西方吸干化验进行了分析。
小干扰RNA真核表达载体具体到livin基因采用基因重组、测序核酸。
然后用Lipofectamin2000转染进入SGC-7901细胞。
逆转录聚合酶链反应技术和西方吸干化验用来验证的livin基因在SGC-7901细胞中使沉默基因生效。
所得到的稳定的复制品用G418来筛选。
细胞凋亡用应用流式细胞仪(FCM)来评估。
细胞生长状态和5-FU的50%抑制浓度(IC50)和顺铂都由MTT比色法来决定。
结果—livin mRNA和蛋白质的表达检测40例中有19例(47.5%)有胃癌和SGC-7901细胞。
没有livin基因表达的是在肿瘤邻近组织和良性胃溃疡病灶。
相关发现在livin基因的表达和肿瘤的微小分化和淋巴结转移一样(P < 0.05)。
4个小干扰RNA真核表达矢量具体到基因重组的livin基因建立。
其中之一,能有效地减少livin基因的表达,抑制基因不少于70%(P < 0.01)。
重组的质粒被提取和转染到胃癌细胞。
G418筛选所得到的稳定的复制品被放大讲究。
当livin基因沉默,胃癌细胞的生殖活动明显低于对照组(P < 0.05)。
研究还表明,IC50上的5-Fu 和顺铂在胃癌细胞的治疗上是通过shRNA减少以及刺激这些细胞(5-Fu proapoptotic和顺铂)(P < 0.01)。
《2024年基于生物信息学发现肝细胞癌标志性miRNA及作用与机制研究》范文

《基于生物信息学发现肝细胞癌标志性miRNA及作用与机制研究》篇一一、引言肝细胞癌(Hepatocellular Carcinoma,HCC)是一种常见的恶性肿瘤,其发病率和死亡率均较高。
由于HCC的早期诊断困难,治疗手段有限,因此寻找有效的诊断标志物和治疗方法成为当前研究的重点。
近年来,随着生物信息学的发展,microRNA (miRNA)在肿瘤发生、发展及转移中的作用逐渐受到关注。
miRNA是一种非编码单链小分子RNA,能够通过调控基因表达参与多种生物学过程。
本研究基于生物信息学方法,旨在发现肝细胞癌标志性miRNA及其作用与机制。
二、研究方法1. 数据收集与处理我们首先从公共数据库中收集了肝癌患者的miRNA表达谱数据,并进行了预处理,包括数据清洗、归一化等。
2. 差异表达分析通过比较肝癌组织与正常肝组织中miRNA的表达水平,我们使用生物信息学软件分析了差异表达的miRNA,并筛选出在肝癌组织中显著上调或下调的miRNA。
3. 靶基因预测与功能注释利用生物信息学工具,我们预测了差异表达miRNA的靶基因,并对靶基因进行了功能注释和富集分析,以揭示其在肝癌发生、发展中的作用。
4. 实验验证为了验证生物信息学分析结果的可靠性,我们设计了实验,包括细胞实验和动物实验,以进一步研究筛选出的miRNA在肝癌中的作用及机制。
三、结果与分析1. 差异表达miRNA的筛选通过生物信息学分析,我们筛选出在肝癌组织中显著上调的miRNA和显著下调的miRNA。
其中,miR-XXX和miR-YYY在肝癌组织中的表达水平最高。
2. 靶基因预测与功能注释我们预测了miR-XXX和miR-YYY的靶基因,并进行了功能注释和富集分析。
结果显示,这些靶基因主要参与细胞增殖、凋亡、侵袭和转移等生物学过程。
其中,某些靶基因与肝癌的发生、发展密切相关。
3. 实验验证通过细胞实验和动物实验,我们验证了miR-XXX和miR-YYY在肝癌中的作用及机制。
希森美康血凝仪
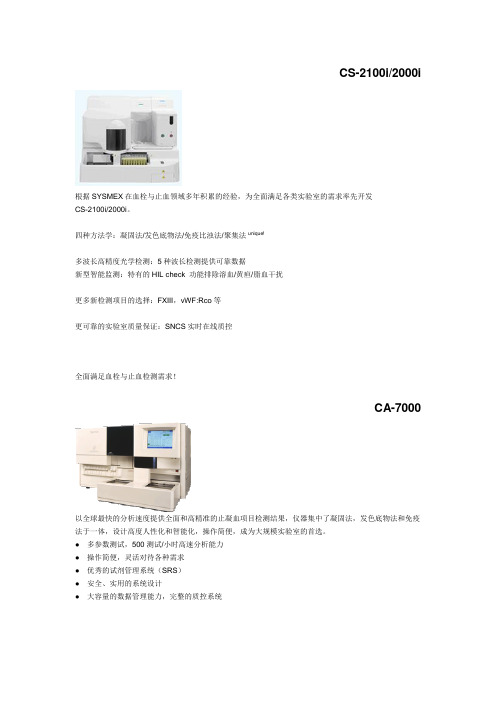
CS-2100i/2000i根据SYSMEX在血栓与止血领域多年积累的经验,为全面满足各类实验室的需求率先开发CS-2100i/2000i。
四种方法学:凝固法/发色底物法/免疫比浊法/聚集法unique!多波长高精度光学检测:5种波长检测提供可靠数据新型智能监测:特有的HIL check 功能排除溶血/黄疸/脂血干扰更多新检测项目的选择:FXIII,vWF:Rco等更可靠的实验室质量保证:SNCS实时在线质控全面满足血栓与止血检测需求!CA-7000以全球最快的分析速度提供全面和高精准的止凝血项目检测结果,仪器集中了凝固法,发色底物法和免疫法于一体,设计高度人性化和智能化,操作简便,成为大规模实验室的首选。
● 多参数测试,500测试/小时高速分析能力● 操作简便,灵活对待各种需求● 优秀的试剂管理系统(SRS)● 安全、实用的系统设计● 大容量的数据管理能力,完整的质控系统CA-1500汇集了当今血栓/止血分析仪最新的各种先进功能于一身,是市场上少见的性能/价格比极高的一台仪器,是大型教学医院,综合医院实验室的首选。
它具有快速处理能力,最快180测试/小时,集多种检测功能于一身:凝固法、发色底物法、免疫法。
具有全能随机组合能力,两种方法测定纤维蛋白质,适合常规大量和急诊使用。
● 拥有高速处理能力、随机测试功能和自动再检查功能● 三种分析方式,包括多规则监视的广泛质控文件和平行线生物分析功能● 卓越的性能可以灵活适应实验室的多样化需求CA-500系列CA-500系列包含了六款机型,设计新颖、符合经济原则,是各中小型实验室开展血栓/止血实验的最佳选择,也是半自动升级到全自动的理想机型。
小型台式仪实用可靠,具备三种检测系统即凝固法、发色底物法、免疫法的自由组合用户可根据需要选择相应机型。
CA-50设计上完全沿用了全自动CA系列的检测原理,锁定人为误差因素的设计确保它有别于其他半自动血凝仪,达到全自动仪器的准确性与重复性效果,四通道即可批量检测又可单独检测,内置质控文件,适用于小标本量实验室使用。
神经外科耗材1

型号 ECO-100AL5
非血管介入 一次性微波 耗材(内窥 消融针 镜耗材)
一次性微 南京 国 根 波消融针 亿高 产 经皮穿刺 胆道引流 Angio 进 套 导管 tech 口 /PTCD引 肾穿刺造 Angio 进 套 瘘套装 tech 口 聚醚砜膜 BELL 进 透析器 支 CO 口 (低通) 经皮穿刺 胆道引流 Angio 进 根 导管 tech 口 /PTCD引 经皮穿刺 胆道引流 Angio 进 导管 根 tech 口 /PTCD引 流套件
产品代码
产品名称
分类名称 一级目录 二级目录
单 产 品牌 位 地
规格 5kg/瓶 , 4瓶/箱
型号 过氧乙酸含量5%6% 柠檬酸含量24%28% 柠檬酸含量48%52%
医疗器械注册 证号
投标企业
备注
151201942
血液净化类 环凯牌过氧 其他血透 血液透析 环凯 国 及体外循环 瓶 乙酸消毒液 耗材 机消毒液 牌 产 类耗材 环凯牌柠檬 血液净化类 其他血透 血液透析 环凯 国 酸消毒液 及体外循环 瓶 耗材 机消毒液 牌 产 (25%) 类耗材 环凯牌柠檬 血液净化类 其他血透 血液透析 环凯 国 酸消毒液 及体外循环 瓶 牌 产 耗材 机消毒液 (50%) 类耗材
备注
LST140-A
产品代码
产品名称
分类名称 一级目录 二级目录
单 产 品牌 位 地
规格
型号
医疗器械注册 证号
投标企业
备注
非血管介入 无菌一次性 160814529 耗材(内窥 微波消融针 镜耗材)
其他
工作频率2450MHz,微波 辐射针头长度7±2mm,直 径1.9±0.5mm;消融针杆 长度170±30mm,直径1.9 ±0.5mm;配用机型KY2000、KY-2200; 工作频率2450MHz,微波 辐射针头长度7±2mm,直 径1.9±0.5mm;消融针杆 长度170±30mm,直径1.9 ±0.5mm;配用机型KY2000、KY-2200; 工作频率2450MHz,微波 一次性微 南京 国 根 辐射针头长度12±2mm, 波消融针 康友 产 直径1.9±0.5mm;消融针 杆长度130±30mm,直径 1.9±0.5mm;配用机型 KY-2000、KY-2200; 工作频率915MHz,微波 辐射针头长度22±2mm, 直径1.9±0.5mm;消融针 杆长度180±30mm,直径 1.9±0.5mm;配用机型 KY-2100、KY-2200; 工作频率915MHz,微波 辐射针头长度25±2mm, 直径1.9±0.5mm;消融针 1000ml/袋
赛默飞药敏分析仪Vizion 招标参数(1)(1)

自动接种药敏分析系统招标参数★1.功能用途自动接种药敏分析系统,用于临床和各研究项目标本中细菌革兰阴性菌和革兰阳性菌药敏、真菌药敏和分枝杆菌药敏检测和研究。
2.技术规格2.1检测原理:比浊法、比色法。
▲2.2药敏检测:完全遵照CLSI推荐的微量稀释法提供定量MIC结果,提供4-12个稀释浓度,可以检测真正的MIC值。
2.3 提供革兰氏阴性菌、革兰氏阳性菌、链球菌、嗜血杆菌、弯曲菌、厌氧菌药敏检测板,含有20-30种抗生素。
同时能检测ESBL、MRSA、VRE等耐药细菌。
2.4提供多种真菌药敏板,含有9种抗生素。
2.5提供分枝杆菌药敏板包括12中抗生素,可检测结核分枝杆菌、快速生长的分枝杆菌、缓慢生长的分枝杆菌以及奴卡氏菌和其他需氧放线菌。
3.检测试剂3.1 药敏板可提供4-12稀释浓度的全值板和1-4个稀释浓度的阈值板。
▲3.2 药敏板为96孔板,加入菌液后薄膜覆盖,确保实验室生物安全。
3.3 药敏板可常温保存18-24个月。
3.4 提供客户定制药敏板,超过240种抗生素可供选择。
4.仪器设备4.1采用电子比浊仪标准化制备菌悬液。
4.2采用全自动加样仪标准化加样。
1)加样原理:定量分配装置,无吸样过程,直接将试管中的样本(菌液)精确接种至96孔板中。
2)全封闭移液头,仅在每个孔位上方加样时开启。
3)加样量范围:50μL -200μL。
4)加样速度:完成96孔板加样时间≤ 40秒。
5)微电脑处理器,LCD触摸屏操作,图标式菜单选择。
6)分区域加样模式:可在96孔板上完成2-3个不同样本的接种;也可分别完成横排竖排的单独加样;多种模式可供选择。
7)选择加样模式后,屏幕显示96板的区域划分。
加样过程中,不同颜色标识每个区域的加样状态,包括已完成,进行中和待加样三种状态。
8)不同区域加样顺序可任意选择,直接点击目标区域即可。
9)适用于不同规格的96孔微孔板的加样。
▲4.3仪器配备实时照相设备,将每个药敏板的图像呈现到分析软件。
【实验】转基因植物产品检测实验室一览

【关键字】实验转基因植物产品检测实验室一览其他设备:细胞融合仪、核酸提取仪、紫外分光光度计、核酸蛋白检测仪磁力搅拌机杂交仪、-30℃低温冰箱、超低温冰箱、漩涡混合器、超声波细胞粉碎仪、自动恒温酶标。
7 操作步骤7.1 抽样参照 NY/T672 转基因植物及其产品检测通用要求和NY/T673 转基因植物及其产品检测抽样。
7.2 制样参照 NY/T672 转基因植物及其产品检测通用要求和NY/T673 转基因植物及其产品检测抽样(按照GB 5491中四分法制备样品进行送检)。
7.3 DNA模板的制备a称取200-400 mg试样,在液氮中磨碎,装入已经用液氮预冷的1.5 ml离心管中。
b加入1ml预冷至4 ℃的抽提液,剧烈摇动混匀后,在冰上静置5分钟,用13 000 r/min离心机,4 ℃离心15 min,弃去上清液。
c加入600 μl 预热到65 ℃的抽提裂解液,用玻棒搅拌上下颠倒充分混匀,在65 ℃的水浴锅中裂解40 min。
d用13 000 r/min离心机室温离心10 min,将上清液转至另一离心管中,加入5 μl RNase A (10 mg/ml),37 ℃水浴30 min。
e分别用等体积苯酚:氯仿:异戊醇(25:24:1)和氯仿:异戊醇(24:1)各抽提一次。
f用13 000 r/min离心机室温离心10 min,将上清转至另一离心管中。
加入2/3体积异丙醇,1/10 体积3M乙酸钠(pH 5.6),-20 ℃放置2-3 h,充分沉淀DNA。
g13 000 r/min,4 ℃离心15 min,用70%乙醇洗沉淀一次,倒出乙醇,晾干DNA。
加入50 μl TE(pH8.0)溶解DNA。
h把DNA溶液浓度用重蒸馏水调制为100ng/μl,储存于-20 ℃备用。
注意:I 1 g试样(如棉花种子)提取的DNA量应不小于200 μg。
II DNA的OD260/OD280的比值应在1.8左右,且OD260的值应在曲线的最高峰。
用于细胞靶向和诱导细胞凋亡的融合蛋白及其使用方法[发明专利]
![用于细胞靶向和诱导细胞凋亡的融合蛋白及其使用方法[发明专利]](https://img.taocdn.com/s3/m/1cc257d1a32d7375a51780ce.png)
专利名称:用于细胞靶向和诱导细胞凋亡的融合蛋白及其使用方法
专利类型:发明专利
发明人:维尼尔·大卫·B
申请号:CN02807666.4
申请日:20020528
公开号:CN1531552A
公开日:
20040922
专利内容由知识产权出版社提供
摘要:本发明公开了由细胞凋亡诱导蛋白组份和细胞靶向组份组成的融合蛋白。
本发明公开了由蛋白酶组份和细胞靶向组份组成的融合蛋白。
本发明公开了能靶向细胞并诱导细胞死亡的物质组成和方法。
申请人:宾西法尼亚大学托管人
地址:美国宾西法尼亚州费城坚果街3160,200室PA19104
国籍:US
代理机构:北京天平专利商标代理有限公司
代理人:李维真
更多信息请下载全文后查看。
用针对血管内皮生长因子的抗体和针对人表皮生长因子2型受体的抗

专利名称:用针对血管内皮生长因子的抗体和针对人表皮生长因子2型受体的抗体进行肿瘤治疗
专利类型:发明专利
发明人:托马斯·弗里斯,马克斯·哈斯曼,维尔纳·朔伊尔
申请号:CN200780009928.4
申请日:20070320
公开号:CN101405030A
公开日:
20090408
专利内容由知识产权出版社提供
摘要:本发明提供治疗在用抗VEGF抗体的在先治疗中失败的患者中的乳腺癌疾病的方法,该方法包括在继续所述抗VEGF抗体治疗的同时,给所述患者施用治疗有效量的抗HER2抗体。
本发明还提供相对应的产品和药物组合物的制品。
申请人:霍夫曼-拉罗奇有限公司
地址:瑞士巴塞尔
国籍:CH
代理机构:中科专利商标代理有限责任公司
代理人:柳春琦
更多信息请下载全文后查看。
《2024年丝胶对2型糖尿病大鼠海马损伤的保护作用》范文

《丝胶对2型糖尿病大鼠海马损伤的保护作用》篇一一、引言随着人们生活方式的改变和老龄化进程的加速,2型糖尿病的发病率逐年上升,已经成为严重威胁人类健康的全球性问题。
糖尿病不仅影响机体的代谢平衡,还会导致多种并发症,如心血管疾病、神经病变等。
海马是大脑中与记忆、学习等认知功能密切相关的结构,糖尿病引起的海马损伤是导致认知功能下降的重要原因之一。
丝胶作为一种天然生物活性物质,具有多种生物活性,包括抗氧化、抗炎、促进伤口愈合等作用。
本研究旨在探讨丝胶对2型糖尿病大鼠海马损伤的保护作用及其可能的作用机制。
二、材料与方法1. 实验动物与分组选用健康SD大鼠,随机分为正常对照组、糖尿病模型组、丝胶治疗组。
糖尿病模型通过高糖高脂饲料喂养和腹腔注射小剂量链脲佐菌素建立。
2. 丝胶处理丝胶治疗组大鼠每日口服丝胶,正常对照组和糖尿病模型组大鼠口服等体积的蒸馏水。
3. 实验方法与指标检测(1)生化指标检测:检测大鼠血糖、血脂等生化指标;(2)海马组织病理学检查:观察各组大鼠海马组织形态学变化;(3)免疫组化检测:检测海马组织中相关炎症因子、氧化应激指标的表达情况;(4)行为学测试:通过Morris水迷宫等行为学测试评估大鼠学习记忆能力。
三、实验结果1. 生化指标分析与正常对照组相比,糖尿病模型组大鼠血糖、血脂等生化指标显著升高。
丝胶治疗组大鼠的生化指标得到显著改善,接近正常水平。
2. 海马组织病理学检查海马组织病理学检查显示,糖尿病模型组大鼠海马组织出现明显的神经元损伤、胶质细胞增生等病理改变。
丝胶治疗组大鼠海马组织病理改变较轻微,接近正常水平。
3. 免疫组化检测结果免疫组化检测结果显示,糖尿病模型组大鼠海马组织中炎症因子、氧化应激指标表达升高。
丝胶治疗组大鼠海马组织中相关指标表达较低,与正常对照组接近。
4. 行为学测试结果Morris水迷宫等行为学测试结果显示,糖尿病模型组大鼠学习记忆能力显著下降。
丝胶治疗组大鼠学习记忆能力得到显著改善,接近正常水平。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
www.ScienceTranslationalMedicine .org 23 May 2012 Vol 4 Issue 135 135fs14 1W ith their interdisciplinary training and patient-centered objectives, clinician-investigators and translational bioscientists drive translational biomedical research and advances in clinical practice. Society and academic medical centers rightfully demand, not only that the community real-izes benef ts from the labors of those who dwell in their clinics and laboratories, but also that these professionals meet standards of excellence for a growing and increasing-ly complex array of knowledge, skills, and technologies in both domains. Yet attain-ment of excellence, dif cult in one domain, may be impossible when one works in mul-tiple spaces. Here, we introduce a series of articles in which early-career biomedical researchers each interview an established translational scientist about training and career challenges. T rough this collection of voices, we seek to compile educational and cultural interventions that may help young translational scientists negotiate their most debilitating career bottlenecks.MISSION IMPOSSIBLE?For some professionals, translation of scientif c knowledge requires clinical ex-posure, and for a time, there was mini-mal distinction between the clinician-investigator and the translational bioscien-tist. But science and medicine have evolved, and the veracity of this generalization must be reevaluated. Translational bioscientists acknowledge that the privilege of perform-ing clinically motivated scientif c investiga-tion ultimately requires clinical fulf llment. Clinician-investigators—who both care for patients and pursue biomedical research—take this mantra to an extreme, holding that an ef ective clinical presence requires com-plementary investigative research and that research performed by medical practitio-ners necessitates clinical benef t in return.T is integrated mission has been most ef ectively fulf lled when a physician who cares for patients and conducts labora-tory research performs both vocations as a single persona: that of the clinician-investigator (Fig. 1). However, the current state of biomedicine as well as economic and social conditions force us to explore whether it is possible to assume a seam-less identity that embraces excellence in both clinical and investigative sciences in the pursuit of improved human health and whether only one path and one profession-al identity can promote the translation of scientif c discoveries to clinical advances.A SEAMLESS BUT ELUSIVE IDENTITY Much has been written about the optimal career balance of the successful academicclinician-investigator. Some argue that the appropriate balance can be represented by a three-legged stool, with the legs rep-resenting clinical medicine, biomedical research, and education/mentoring; the stool is stable when the lengths of the legs are matched, indicating equal excellence in all three domains. T ose who hold this view claim that the simultaneous pursuit of excellence in all three areas drives achieve-ment in each domain to a higher level than could be reached if one focused primarily on a single leg of the stool. Others arguethat the translational bioscientist has simi-lar responsibilities—to teach, investigate, and assure clinical impact, propelling con-cepts into communal good.However, questions surround the viabil-ity of the clinician-investigator career path: Can medical practitioners who simultane-ously seek to become translational biosci-entists function ef ectively as full-f edgedclinician-investigators? T e deluge of bio-medical data, increasingly complex new technologies, and growing bases of special-ty knowledge propel research and discov-ery but also make it dif cult, if not impos-sible, for a single person to master all three legs of the stool in equal measure. Some argue that the legs grow asymmetrically, creating a precarious imbalance that makes sitting stably atop the stool impossible to achieve, unlikely to promote translation, and dangerous for patients and careers.How has this metastable platform changed the careers of newly minted clinician-investigators ? If the intangible concerns of junior clinician-investigators center about the ability to meet the con-comitant demands of two worlds, the quan-tif able and growing stresses forced by the intangibles are manifested as increases in the length of training and time to indepen-dence. In this era of integrated mechanistic medicine, long training times are required to become clinically prof cient, remain clin-ically adept, and complete scientif c rites of passage. A 2002–2003 study showed a median registered time to a Ph.D. degree in the life sciences of 7 years—up almost 20% from 5.9 years in 1978 (1)—and M.D.-Ph.D. trainees who graduated between 1998 and 2007 took 7.8 years to complete both de-grees (2). Residency training for M.D.s and M.D.-Ph.D.s lasts ~3 years, depending on the discipline, and expands with special-ization, adding up to an additional 4 years. Presumably, af er such intense, isolated clinical immersion, those who return to research must pursue postdoctoral scien-tif c training to master new methods and knowledge if they are to be competitive in the biomedical research arena.Af er completion of postgraduate stud-ies, clinician-investigators tread a lengthier and more tenuous path toward their f rst assistant professorships and f rst major in-dependent grants than ever before. In 1980, average ages at time of appointment to assis-tant professorship in the biomedical scienc-es were 33.5, 33.5, and 34.8 years for Ph.D.s, M.D.s, and M.D.-Ph.D.s, respectively, ris-ing in 27 years to 38.5, 37, and 39.9 years, respectively. Similarly, in 1980 the average ages of Ph.D.s, M.D.s, and M.D.-Ph.D.s in the biomedical sciences when they received their f rst U.S. National Institutes of Health (NIH) RO1 grants were 35.7, 37.7, and 36.1 years, respectively, rising to 41.7, 44.2, and 42.3 years, respectively, in 2007 (3). All tookE D U C AT I O N A N D T R A I N I N GClinician-Investigators as Translational Bioscientists: Shaping a Seamless IdentityElazer R. Edelman 1,2* and Kelly LaMarco 3*Corresponding author. E-mail: ere@ 1Harvard–MIT Division of Health Sciences and Technol-ogy, Massachusetts Institute of Technology, Cambridge, MA 02139, USA. 2Cardiovascular Division, Department of Medicine, Brigham and Women’s Hospital, HarvardMedical School, Boston, MA 02115, USA. 3ScienceTranslational Medicine , American Association for theAdvancement of Science, Washington, DC 20005, USA. E stablished biomedical scientists counsel early-career clinician-investigators and transla-tional bioscientists on mechanisms for molding successful research careers that advance clinical medicine.o n M a r c h 15, 2015s t m .s c i e n c e m a g .o r g D o w n l o a d e d f r o mwww.ScienceTranslationalMedicine .org 23 May 2012 Vol 4 Issue 135 135fs14 2substantially longer to gain fac-ulty slots and the R01 status of independence; M.D.s became faculty members sooner than those with Ph.D.s but became independent later. T us, it ap-pears that postdoctoral training nearly doubled in duration over this time period but was virtu-ally required before a clinician-investigator could achieve some level of professional security. Is it reasonable and sustainable to require more than two decades of training af er college ma-triculation before a clinician-investigator can take charge of his or her own professional fate?To function as clinician-investigators, young profes-sionals must juggle the need for training to excellence in clini-cal medicine with the need to spend more time doing science, just as the pace of research support has fallen well behind the rise in expense. But can a clinician-investigator ever be as competent a physician as s/he could be if s/he cared for patients alone, or as competi-tive a scientist as s/he could be if s/he had no clinical responsi-bilities to balance? In a recent survey (2), career data were collected from nearly 6000 cur-rent and former trainees in 24 NIH-funded M.D.-Ph.D. training programs. Among respondents who completed their M.D.-Ph.D. programs and worked in academic medical centers, 82% were engaged in re-search, but close to two thirds of these not-ed that they spent only 50% of their time in the lab. Just 39% devoted more than 75% of their ef orts to research.T ere are few data that provide insight into what percentage of biomedical sci-entists truly embody the single persona of the clinician-investigator in their careers. Receipt and renewal of RO1 grants are met-rics for assessing research prof ciency, but it is unclear whether the focus is on basic research or science driven by unmet clini-cal needs. Comparable metrics for clinical prof ciency are dif cult to quantify. Data ex-ist on the career desires and f elds of interest of new M.D.s and M.D.-Ph.D.s when they enter the work force (4) but not on wheth-er these professionals ultimately practice medicine while conducting patient-driven research with the goal of improving clinical medicine. T is is information we need going forward if we are to establish a prognosis for the clinician-investigator.ORCHESTRATING AN INTERVENTION In the context of the heated debate on op-timal career balance, we seek to answer a basic set of questions: What do modern ca-reers in academic medicine and the trans-lational biosciences look like, and how can they be attained? Can the timeline of training that now entails full clinical and full research exposure be shortened and curriculum streamlined, or is the mastery of multiple trades by its very nature strenu-ous and time-consuming? Is combined ex-cellence in both clinical and investigative sciences required for the advancement of translational medicine? Last, how can one def ne, in a rigorous manner, how well the current training system is working and the potential impact of alterationsin the system of academic per-sonal development that af ect curriculum or training proto-cols (interventions)? Answers to such questions require de-lineation of the con% icts and bottlenecks faced by current early-career biomedical sci-entists and an analysis of pos-sible curricular and cultural interventions that may help circumvent obstacles to a suc-cessful and rewarding career as a clinician-investigator .In the new article series, weattempt to def ne such educa-tional interventions using an approach that is akin to the de-lineation process for any clinicalsyndrome and the evaluation protocol for any potential inter-vention. In medicine, case stud-ies of individual patients identify potential association of signs and symptoms with a disease pro-cess. Larger studies that examine a signif cant and scientif cally se-lected segment of the population can determine the incidence of disease. Increasingly broad sam-pling can ref ne the emerging list of signs and symptoms, of er a mechanism of action to explain the disease, create mechanistic and thematic models to grouppatients, and help suggest potential interven-tions. T ese interventions, however, can only be assessed in full-% edged clinical trials.Our strategy is to apply the same para-digm to def ne and evaluate educational interventions. We are now at the point ofaccumulating case reports to def ne com-monalities and derive mechanistic insights into critical issues that will then suggest interventions. To tap into the knowledge one achieves through experience, we start with case studies of early-career clinician-investigators and translational bioscientists who discuss a specif c set of challenges with senior clinical and translational scientists. T e questions raised re% ect the specif c needs of the emerging faculty member, and the answers re% ect the observations and guidance of the established faculty mem-ber—each based on their respective expe-riences. T e collation of these cases will help to determine whether a syndrome can be def ned and a model created that cir-Fig. 1. Multiple missions, one persona. Despite a kaleidoscopic careerpath, a clinician-investigator embodies a single, integrated persona to care for patients and conduct research with the potential to transform clinical medicine. [Medicine by Austrian artist Gustav Klimt (1862–1918)] C R E D I T : S E E (6).o n M a r c h 15, 2015s t m .s c i e n c e m a g .o r g D o w n l o a d e d f r o mcumscribes the issues at hand and suggests interventions. T ese suggested changes might then be evaluated more formally in a trial that has specif c goals and metrics to determine the health of the system and impact of intervention.T e f rst interview, in this issue of Science Translational Medicine (5), pinpoints two es-sential ingredients for a high-impact career as a clinician-investigator: (i) contact with patients, which highlights unmet medical needs, and (ii) a willingness to change f elds and pursue risky research with uncertain outcomes. One possible intervention, then, would be for institutions and funders to cre-ate an environment in which taking risks is encouraged and rewarded. A second might be for clinician-investigator training pro-grams to institute a selection process that favors versatile and daring students who thirst for a deeper understanding of human physiology and pathophysiology.In future issues, we will address other as-pects of the changing landscape confrontingyoung investigators who are interested inclinically motivated translational research.We will present work and life issues of trans-lational scientists who have trained clini-cally without receiving a physician’s degree,those whose work is clinically motivatedbut not clinically involved, and those whogained exposure to translational science latein a medical career. We look forward to anextended discussion of critical career bot-tlenecks and transformative solutions thatshape biomedical scientists who are capableof advancing translation.REFERENCES AND NOTES1. T. B. Hoff er, V. Welch Jr., Infobrief: Time to degree of U.S. re-search doctorate recipients. (Directorate for Social, Behav-ioral, and Economic Sciences No. NSF 06-312) (Arlington,VA, National Science Foundation, March 2006).2. L. F. Brass, M. H. Akabas, L. D. Burnley, D. M. Engman, C.A. Wiley, O. S. Andersen, Are MD-PhD programs meetingtheir goals? An analysis of career choices made by grad-uates of 24 MD-PhD programs. Acad. Med.85, 692–701(2010).3. NIH Offi ce of Extramural Research, Data on new inves-tigators, NIH Workforce Discussions; PowerPoint presen-tation (September, 2007); available at http://grants.nih.gov/archive/grants/new_investigators/index.htm.4. D. A. Andriole, A. J. Whelan, D. B. Jeff e, Characteristicsand career intentions of the emerging MD/PhD work-force. JAMA300, 1165–1173 (2008).5. S. E. Henrickson, D. Altshuler, Risk and return for theclinician-investigator. Sci. Transl. Med.4, 135cm6 (2012).6. Image credit: This image is a faithful photographic re-production of an original two-dimensional work of artand is in the public domain. The work of art itself is in thepublic domain because its copyright has expired. Thisapplies to those countries (including the United States)with a copyright term of life of the author plus 70 years./wiki/Klimt_University_of_Vi-enna_Ceiling_Paintings.Citation: E. R. Edelman, K. LaMarco, Clinician-investigators astranslational bioscientists: Shaping a seamless identity. Sci.Transl. Med.4, 135fs14 (2012).10.1126/scitranslmed.3004109onMarch15,215stm.sciencemag.orgDownloadedfrom 23 May 2012 Vol 4 Issue 135 135fs14 3。