KDIGO 2012 Clinical Practice Guideline
2012年KDIGO儿童激素耐药型肾病综合征的诊断与治疗指南与2008年国内西安指南比较

它堡塞旦』L塾!堕鏖盘查!Q!!笙!旦筮垫鲞箜!!塑堡!垫!垒P丛竺!尘!!!!坐!!!£!!竺!竺!!!!!!!!:垫!墅:17
[8]Durkan
AM,Hosdon childhood nephrotic syndrome:a meta.analysis of
与临床医学密切结合,在循证依据基础上提倡科学、合理、规范 的医疗决策,改变了传统的以经验为基础的临床医学模式。近 年来,各类肾脏疾病的临床循证研究和循证治疗指南不断涌 现,为临床医师提供了临床思路和治疗规范。 但从两部指南可以看出,目前关于儿童Ns治疗的循证依 据和推荐级别尚需要更多RCTs加以支撑,尤其在免疫抑制剂 治疗INS的RCTs资料更为缺乏;因此,尽管两部指南均在RCTs 基础上制订了相关循证指南,但显然需要进一步完善。国内尤 其需要充分利用病源和病种优势开展高质量的多中心RCTs研 究。诚然,循证基础上的个体化治疗尽管是医学临床治疗的理 想目标,但还需要儿科肾脏疾病工作者们的艰辛探索。 参考文献
毛建华,王文静
【摘要】 激素抵抗型肾病综合征(SRNS)是指应用常规糖皮质激素治疗不能取得完全缓解的病理状态,在 儿童肾脏疾病的实践工作中具有十分重要的临床意义。中华医学会儿科学分会肾脏病学组曾于2008年10月西 安会议期间制定了儿童SRNS诊治指南,2012年6月改善全球肾脏病预后组织(KDIGO)又发布了新的关于肾小 球肾炎,包括1—18周岁儿童SRNS的诊治指南。与前者比较,2012年KDIGO指南在判断SRNS标准(强调8周 的规范激素治疗)、肾穿刺活检(如果要检测到5%的。肾小球病变或有95%的信心排除病变,那么至少需要活检到 20个以上的肾小球)、治疗策略[推荐使用钙调神经磷酸酶抑制剂(CNIs),不建议使用环磷酰胺,而大剂量激素或 霉酚酸酯适用于CNIs无效的患者]等方面存在一定差异,值得在今后的临床实践中进一步验证完善。
KDOQI关于2012年KDIGO-CKD
Table 11, from KDIGO CKD Guideline. KI. 2012.
CKD的病情评估—— cause
Chronicity Cause GFR Albuminuria 病因评估:评价临床资料,包括个人与家 族史,社会和环境因素,药物,体格检查, 实验室检查,影像学检查,以及病理诊断, 来确定肾脏病的原因。(Not Graded)
National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(suppl 2):S1-S266.
16
CKD的危险因素
临床因素
•糖尿病
•高血压 •系统性感染 •尿路感染 •尿路结石 •尿路梗阻
•肿瘤
•有CKD家族史 •肾脏质量减少 •使用某些药物 •低体重
•自身免疫性疾病 •曾有急性肾损伤
社会人口学因素
•老年
•人种差异 •暴露于某些化学或环境因素 •低收入/教育水平
17
NKF-KDOQI CKD Guideline. AJKD 2002
8
GFR: glomerular filtration rate 肾小球滤过率 AER: albumin excretion rate 尿白蛋白排泄率 ACR: albumin-to-cretinine ratio 尿白蛋白肌酐比(肾病指数)
CKD的分期
2002 KDOQI 采用GFR分期系统 分期 GFR (ml/min/1.73m2) 描述
KDIGO临床实践指南

3.1 CKD-MBD 的诊断:生化指标异常
3.1.1 对于成人患者,推荐从 CKD3 期开始监测血清钙、磷、PTH 及碱性磷酸酶活性的水平 (1C)。 对于儿童患者,建议从 CKD2 期开始以上监测(2D)。 3.1.2 对于 CKD 3-5D 期患者,根据生化指标异常及其严重程度与 CKD 进展速度来决定监测 血清钙、磷及 PTH 水平的频率是合理方案(证据未分级)。 合理的监测间隔时间包括: � CKD 3 期:每隔 6-12 个月检查血清钙、磷水平;根据 PTH 基线水平和 CKD 进展情况
KDIGO 临床实践指南 慢性肾脏病-矿物质和骨异常(CKD-MBD)的诊断、评估、预防和治疗
执行概要
本文件引用格式: Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease–mineral and bone disorder (CKD–MBD). Kidney International 2009; 76 (Suppl 113): S1–S130.
微量尿蛋白的实验室检测
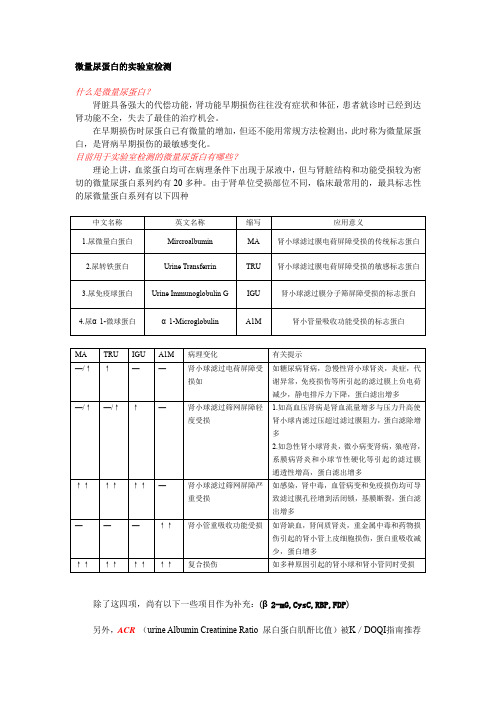
微量尿蛋白的实验室检测什么是微量尿蛋白?肾脏具备强大的代偿功能,肾功能早期损伤往往没有症状和体征,患者就诊时已经到达肾功能不全,失去了最佳的治疗机会。
在早期损伤时尿蛋白已有微量的增加,但还不能用常规方法检测出,此时称为微量尿蛋白,是肾病早期损伤的最敏感变化。
目前用于实验室检测的微量尿蛋白有哪些?理论上讲,血浆蛋白均可在病理条件下出现于尿液中,但与肾脏结构和功能受损较为密切的微量尿蛋白系列约有20多种。
由于肾单位受损部位不同,临床最常用的,最具标志性的尿微量蛋白系列有以下四种中文名称英文名称缩写应用意义1.尿微量白蛋白Mircroalbumin MA 肾小球滤过膜电荷屏障受损的传统标志蛋白2.尿转铁蛋白Urine Transferrin TRU 肾小球滤过膜电荷屏障受损的敏感标志蛋白3.尿免疫球蛋白Urine Immunoglobulin G IGU 肾小球滤过膜分子筛屏障受损的标志蛋白4.尿α1-微球蛋白α1-Microglobulin A1M 肾小管量吸收功能受损的标志蛋白MA TRU IGU A1M 病理变化有关提示—/↑↑——肾小球滤过电荷屏障受损如如糖尿病肾病,急慢性肾小球肾炎,炎症,代谢异常,免疫损伤等所引起的滤过膜上负电荷减少,静电排斥力下降,蛋白滤出增多—/↑—/↑↑—肾小球滤过筛网屏障轻度受损1.如高血压肾病是肾血流量增多与压力升高使肾小球内滤过压超过滤过膜阻力,蛋白滤除增多2.如急性肾小球肾炎,微小病变肾病,狼疮肾,系膜病肾炎和小球节性硬化等引起的滤过膜通透性增高,蛋白滤出增多↑↑↑↑↑↑—肾小球滤过筛网屏障严重受损如感染,肾中毒,血管病变和免疫损伤均可导致滤过膜孔径增到活闭锁,基膜断裂,蛋白滤出增多———↑↑肾小管重吸收功能受损如肾缺血,肾间质肾炎,重金属中毒和药物损伤引起的肾小管上皮细胞损伤,蛋白重吸收减少,蛋白增多↑↑↑↑↑↑↑↑复合损伤如多种原因引起的肾小球和肾小管同时受损除了这四项,尚有以下一些项目作为补充:(β2-mG,CysC,RBP,FDP)另外,ACR(urine Albumin Creatinine Ratio 尿白蛋白肌酐比值)被K/DOQI指南推荐用于高危人群筛查(MicroAlbuminuria 微量白蛋白尿)。
KDIGOAKI诊疗指南解读
KDIGO,2012
ConceptualModel model for Conceptual forAKI AKI
Stages defined by creatinine and urine output are surrogates Complications Complications
GFR
Normal Normal Increased Increased risk risk Damage Damage GFR GFR Kidney Kidney failure failure Death Death
– KDIGO Clinical Practice Guideline for Acute Kidney Injury
KDIGO,2012
AKI流行病学ห้องสมุดไป่ตู้状
• • • • • • 患病率:1%(社区)~ 7.1%(医院) 人群发病率:486~630 pmp/y AKI需要RRT发病率:22~203pmp/y 医院获得AKI死亡率:10~80% 合并多脏器功能衰竭死亡率:>50% 需要RRT治疗者死亡率:高达80%
About AKI guideline
• ADQI:2002, RIFLE • AKIN:2005, modified definition and staging system • KDIGO: 2011, First clinical guideline for AKI – Waiting for published in this summer • AKI guideline for AKI :2011 – UK Renal Association Final Version 08.03.11 • AKI guidline—KDIGO 2012
2012年改善全球肾脏病预后组织KDIGO贫血指南解读
g/L(<10.0 g/d1)的成人CKD非透析患者,建
议需根据患者Hb下降程度、先前对铁剂治疗的反
应、输血的风险、ESA治疗的风险和贫血合并症状, 决定是否开始ESA治疗。成人HD患者Hb下降速
・168・
』盟!P!翌Biblioteka 些i型!!堕里!P!!堕!!!:!j
盟!:!
垒P!:!!!1
・医学继续教育・ 2012年改善全球肾脏病预后组织(KDIGO) 贫血指南解读
陈楠李娅
摘要2001年美国肾脏病基金会的肾脏疾病与透析患者生存质量指导指南(K/DOQI)颁布了慢性肾脏病 (CKD)贫血治疗指南、2004年发布了欧洲最佳实践指南(EBPGs)、2006年及2007年K/DOQI对指南的部分内容进 行了更新,之后2003年成立的改善全球肾脏病预后组织(KDIGO)颁布了2012年CKD贫血临床实践指南,该指南 在建立过程中遵循明确的证据审查和评价体系,对伴贫血或有贫血风险的CKD患者[非透析、血液透析、腹膜透 析、肾移植受者和儿童]提供临床指导、诊断、评价和管理策略。指南包含CKD贫血的诊断和评估、使用药物治疗 (铁剂、红细胞生成刺激剂和其他药物)及输注红细胞治疗贫血等。指南建议是基于相关试验的系统评价,每个章 节提出针对性治疗方法。根据分级推荐的评估方法(GRADE)系统评估证据质量和推荐强度,每一条推荐建议按 照强度分为1级(我们推荐)、2级(我们建议)和未分级;根据相关支持证据的质量高、中、低、很低分为A、B、c和D 级。本文将对上述指南中的某些重要问题作一解读。 关键词 慢性肾脏病改善全球肾脏病预后组织 贫血指南
KDIGO肾小球肾炎临床实践指南
KDIGO肾小球肾炎临床实践指南介绍KDIGO(Kidney Disease: Improving Global Outcomes)是一个国际性非营利组织,其目标是提高全球肾脏疾病诊治水平。
该组织制定了一系列指南,以促进和改进肾脏疾病的临床实践。
本文主要介绍了KDIGO关于肾小球肾炎的临床实践指南。
肾小球肾炎是一种重要的肾脏疾病,常见于不同年龄段的患者。
临床上,肾小球肾炎的表现较为复杂,治疗策略也较为复杂。
因此,有必要制定临床实践指南,以指导医生在诊断和治疗肾小球肾炎时的决策。
诊断根据KDIGO指南,诊断肾小球肾炎需要进行详细的病史收集和体格检查。
常见的症状包括蛋白尿、血尿、水肿等。
同时,还需要进行肾脏功能检查和肾活检等辅助检查来确认诊断。
分类根据肾活检结果,肾小球肾炎可分为许多亚型,包括IgA肾病、膜性肾病、系膜增生性肾炎等。
每种亚型的治疗策略略有不同,因此在制定治疗方案时需要明确病理类型。
治疗对症治疗对症治疗是肾小球肾炎的重要组成部分,旨在缓解症状和改善肾功能。
常用的对症治疗方法包括限制蛋白摄入、控制血压、使用利尿剂等。
免疫抑制治疗免疫抑制治疗在一些肾小球肾炎亚型的治疗中起到重要作用。
该类治疗方法包括糖皮质激素、免疫抑制剂等药物的使用。
然而,免疫抑制治疗也会增加患者感染的风险,因此在使用时需要谨慎权衡利弊。
替代治疗对于进展较快的肾小球肾炎或终末期肾脏疾病患者,可能需要进行替代治疗,如透析或肾移植。
随访与预防患者在接受治疗后需要定期进行随访,以评估治疗效果和监测疾病进展情况。
此外,肾小球肾炎的复发风险较高,因此在预防复发方面也需要重视。
结论KDIGO肾小球肾炎临床实践指南提供了诊断和治疗肾小球肾炎的重要指导。
对于医生来说,遵循这些指南能够更好地管理肾小球肾炎患者,提高其生活质量和预后。
参考文献:1.KDIGO Clinical Practice Guideline forGlomerulonephritis. Kidney International Supplements.2012; 2(2): 139-274.2.Rovin BH, et al. KDIGO Clinical Practice Guideline forGlomerulonephritis: Executive Summary. KidneyInternational. 2017; 92(3): 628-632.。
2012改善全球肾脏病预后组织(KDIG0)临床实践指南:肾小球肾炎
改善全球肾脏病预后组织( KDIGO) 临床实践 指南: 肾小球肾炎
李世军 译 刘志红 校
[译自: Kidney Int,2012,2 ( Suppl 2) : 143 - 153]
关键词 改善全球肾脏病预后组织( KDIGO) 临床实践指南 肾小球肾炎
儿童激素敏感型肾病综合征( SSNS)
儿童 SSNS 的初始治疗 1. 推荐糖皮质激素( 泼尼松或甲泼尼龙) 治疗 至少 12 周( 1B) 。 2. 推荐 单 次 口 服 泼 尼 松 ( 1B ) ,初 始 剂 量 60 mg / ( m2·d) 或 2 mg / ( kg·d) ( 最大剂量 60 mg / d) ( 1D) 。 3. 推荐至少 4 ~ 6 周每日口服泼尼松( 1C) ,续
建议 CNIs 治疗至少 12 个月( 2C) 。 5. 建议 霉 酚 酸 酯 ( MMF) 作 为 替 代 激 素 药 物
( 2C) 。 由于停 MMF 后多数儿童会复发,建议 MMF 起
始剂量 1. 2 g / ( m2·d) ,分两次服用,至少持续 12 个 月( 2C) 。
6. 建议利妥昔单抗( rituximab) 治疗仅限于最 佳联合( 泼尼松和激素替代药物) 治疗后仍然频繁 复发和 ( 或) 发 生 治 疗 严 重 不 良 反 应 的 激 素 依 赖 SSNS 儿童( 2C) 。
[作者单位] 南京军区南京总医院 全军肾脏病研究所 ( 南京,210016)
以隔日口服( 泼尼松 40 mg / m2 或 1. 5 mg / kg,最大剂 量 40 mg / 隔日) ( 1D) ,持续治疗 2 ~ 5 个月( 1B) 后 逐渐减量。
复发型 SSNS 的激素治疗 1. 儿童非频繁复发型 SSNS 的激素治疗: 建议 泼尼松 60 mg / ( m2·d) 或2 mg / ( kg·d) ( 最大剂量 60 mg / d) ,完全缓解≥3d 后开始减量( 2D) 。 2. 获得完全缓解后,建议泼尼松改为隔日顿服 ( 每次 40 mg / m2 或 1. 5 mg / kg,最大剂量 40 mg) 至 少 4 周( 2C) 。 反复复发和激素依赖 SSNS 1. 建议反复复发或激素依赖的 SSNS 儿童,采用 每日一次的激素治疗,诱导获得完全缓解≥3d 后可
KDIGO肾小球肾炎临床实践指南

MMF
• MMF用于儿童MCD治疗中,在成人中仅有少数临床病例报告
Eknoyan G, et al. Kidney inter, Suppl. 2012;2:139-274
缓解率(%)
环孢素A组缓解率与环磷酰胺相当
前瞻、随机、多中心、开放、平行对照研究,包括MCD和FSGS的一组FR和(或)SD型肾病综合征患者,随机环 磷酰胺或环孢素A治疗: ➢环磷酰胺:2.5mg/kg/d,治疗8周 ➢环孢素A:5mg/kg/d,治疗9个月
“不同于儿童患者,在成人MCD患者中缺乏良好设计的RCTs” ——KDIGO MCD指南
安慰剂 强的松治疗
28例MCD患者,随机给予安慰剂或强的松治疗,共2个月。强的松:每隔一天125mg Coggins CH. Trans Am Clin Climatol Assoc. 1986; 97:18-26
Ø 他克莫司治疗1个月缓解率 即高于CTX组
达到缓解的平均时间(天)
他克莫司相比CTX缓解SR-MCD早37天
非随机病例匹配试验,纳入39例中国激素抵抗型MCD患者,随机治疗如下治疗方案: Ø他克莫司组:n=19,起始剂量0.05 mg/kg/d,维持血药浓度5 -10 ng/mL,治疗1年 Ø环磷酰胺组:n=14,起始剂量1g/1.73 m2,调整剂量10g/1.73 m2,治疗1年 Ø两组均接受强的松治疗 Ø激素抵抗型微小病变性肾病综合征(SR-MCN)
约有10%的成人MCD患者为激素抵抗型,即正规激素治 疗16周无效
Eknoyan G, et al. Kidney inter, Suppl. 2012;2:139-274
继发性MCD的病因
恶性肿瘤
霍奇金淋巴瘤和非霍奇金淋巴瘤 白血病
2012kdigo指南ckd诊断标准

2012kdigo指南ckd诊断标准Chronic kidney disease (CKD) is a significant health issue affecting millions of people worldwide. The KDIGO (Kidney Disease: Improving Global Outcomes) guidelines provide essential information for the diagnosis and management of CKD. These guidelines are crucial for healthcare professionals in identifying and treating patients with this condition.慢性肾脏疾病(CKD)是影响全球数百万人的重要健康问题。
KDIGO(肾脏疾病:改善全球结果)指南为CKD的诊断和管理提供了重要信息。
这些指南对于医疗专业人员在识别和治疗患有这种疾病的患者方面至关重要。
One of the key aspects of the 2012 KDIGO guidelines concerning CKD diagnosis is the classification of the disease based on the level of kidney function and the presence of kidney damage. This classification system helps healthcare providers determine the severity of the disease and tailor treatment plans accordingly. By following these guidelines, healthcare professionals can ensure that patients receive appropriate care and interventions to slow the progression of CKD.2012 KDIGO指南关于CKD诊断的关键方面之一是根据肾功能水平和肾脏损伤的程度对疾病进行分类。
急性肾功能不全分期标准
急性肾功能不全分期标准急性肾功能不全(AKI)是一种常见的临床病症,其发生率逐年增加。
在临床实践中,对于急性肾功能不全的分期标准,既有国际上通用的标准,也有各个地区或医院根据自身情况制定的标准。
本文将就急性肾功能不全的分期标准进行详细介绍,以期为临床医生提供参考。
一、急性肾功能不全的定义。
急性肾功能不全是指由于各种原因导致肾小球滤过率急剧下降,肾小管功能障碍,从而导致血肌酐和尿素氮等血液中毒物质潴留,引起一系列临床症状和体征的综合征。
二、急性肾功能不全的分期标准。
1. 根据AKIN标准(Acute Kidney Injury Network):①AKIN-1期,血清肌酐水平升高≥0.3mg/dl或相对于基线水平的上升≥50%,或尿量<0.5ml/kg/h持续6小时以上。
② AKIN-2期,相对于基线水平的血清肌酐上升≥100%,或尿量<0.5ml/kg/h持续12小时以上。
③ AKIN-3期,相对于基线水平的血清肌酐上升≥200%,或血清肌酐≥4.0mg/dl(≥353.6μmol/L),或需要透析治疗。
2. 根据KDIGO标准(Kidney Disease: Improving Global Outcomes):根据尿量和肌酐水平的变化将急性肾功能不全分为3期,其中包括:① KDIGO-1期,尿量<0.5ml/kg/h持续6小时以上,或相对于基线水平的血清肌酐上升≥0.3mg/dl(≥26.5μmol/L)。
② KDIGO-2期,尿量<0.5ml/kg/h持续12小时以上,或相对于基线水平的血清肌酐上升≥2倍。
③ KDIGO-3期,尿量<0.3ml/kg/h持续24小时以上,或血清肌酐≥4.0mg/dl(≥353.6μmol/L),或需要透析治疗。
三、急性肾功能不全的治疗。
针对不同分期的急性肾功能不全,治疗方法也各有不同。
对于轻度的急性肾功能不全,可以通过积极的对症治疗和支持疗法来改善肾功能,包括纠正液体和电解质紊乱,保持水电解质平衡,避免使用肾毒性药物等。
2012KDIGO贫血治疗指南与kdoqi指南的比较解读

2.
3.
对于需要铁剂的CKD ND患者,根据铁缺乏严重程度、静脉 通路的情况、之前对口服铁剂的反应情况、对之前口服或 静脉铁剂治疗的不良反应情况、患者依从性和药物价格等 因素选择常规的铁剂治疗方法(未分级)。
KDIGO Clinical Practice Guideline for Anemia in Chronic Kidney Disease
山东大学第二医院 柳刚
一、贫血的定义
Hb
Hct
2000指南中,男性和绝经期后女性的贫血定义为Hb < 120 g/l 2006中,定义为Hb < 135 g/l 2000指南中,对于未绝经女性的贫血定义为Hb < 110 g/l, 2006中,更新为Hb < 120 g/l
4. 对于所有未接受铁剂或ESA治疗的儿童CKD贫血患 者,当铁蛋白≤100 μ g/L时,
推荐使用口服铁剂治疗; [在CKD HD患者中,或可使用静脉铁剂治疗](1D)。
5. 对所有单纯接受ESA治疗(未补充铁剂)的儿童 CKD贫血患者,
推荐口服铁剂治疗; (在CKD HD中,或可使用静脉铁剂治疗)治疗以维持铁 蛋白>100 μ g/L(1D)。
J ASN 16: 3070-3080, 2005
给药途径
CKD HD:静脉
尿毒症患者口服吸收差,且治疗高磷血症的钙盐等药 物阻碍铁剂吸收
CKD PD&ND:口服or静脉
补铁方是铁状态评估低于目标值,给予静脉 补铁。
维持性补铁,即定期给予小剂量铁剂以维持铁离子于目 标范围内。
2012版KDIGO-AKI诊疗指南

AKI分期标准
指南推荐血清肌酐和尿量仍然作为AKI最好的标志物(1B)
2012版KDIGO-AKI诊疗指南
KDIGO,2012
RIFLE分级
2002 年急性透析质量倡议组(ADQI)制定了ARF的 RIFLE 分级诊断标准。
Bellomo R, et al. Crit Care 2004;8:R204-R212
2012版KDIGO-AKI诊疗指南
KDIGO,2012
AKI/CKD/AKD
肾功能改变
肾脏结构改变
AKI CKD
7天内血肌酐升高50% 2天内血肌酐升高0.3mg/dl 少尿
GFR<60ml/min/1.73m2 > 3个月
> 3个月
AKD NKD
AKI 3个月内在原来基础上,GFR下降35%或Scr上升50% GFR<60ml/min/1.73m2, <3个月
① 48小时内Scr升高超过26.5μmol/L(0.3 mg/dl); ② Scr 升高超过基线1.5倍—确认或推测7天内发生; ③ 尿量<0.5 ml/(kg·h),且持续6小时以上。
单用尿量改变作为判断标准时,需要除外尿路梗阻及其它导致尿量减少的原因
2012版KDIGO-AKI诊疗指南
KDIGO,2012
Chapter 2.2: Risk assessment
2012版KDIGO-AKI诊疗指南
KDIGO,2012
Chapter 2.2: Risk assessment
2012版KDIGO-AKI诊疗指南
KDIGO,2012
Definition and stagng of AKIAKI is defined as any of the following (Not Graded ):
产前超声诊断胎儿Berry综合征1例
KDIGO2012Clinical Practice Guideline for the Evaluation andManagement of Chronic Kidney Disease[J].Kidney Int,2012,3(Suppl):1-150.[9]Mitchell C,Rahko PS,Blauwet LA,et al.Guidelines for performing a comprehensive transthoracic echocardiographic examination inadults:recommendations from the American Society ofEchocardiography[J].J Am Soc Echocardiogr,2019,32(1):1-64.[10]Hansrivijit P,Chen YJ,Lnu K,et al.Prediction of mortality among patients with chronic kidney disease:a systematic review[J].World JNephro,2021,10(4):59-75.[11]王凯,郑颖颖,唐俊楠,等.血肌酐水平对肾功能正常的冠心病PCI术后患者预后的影响[J].郑州大学学报(医学版),2020,55(3):308-311.[12]Han X,Zhang S,Chen Z,et al.Cardiac biomarkers of heart failure in chronic kidney disease[J].Clin Chim Acta,2020,510(11):298-310.[13]付亚梦,刘昕.左房时相功能诊断冠状动脉粥样硬化性心脏病患者左室舒张功能障碍的价值[J].临床超声医学杂志,2023,25(1):39-43.[14]Katbeh A,De Potter T,Geelen P,et al.Heart failure with preserved ejection fraction or non-cardiac dyspnea in paroxysmal atrialfibrillation:the role of left atrial strain[J].Int J Cardiol,2021,323(6):161-167.[15]Inoue K,Khan FH,Remme EW,et al.Determinants of left atrial reservoir and pump strain and use of atrial strain for evaluation of leftventricular filling pressure[J].Eur Heart J Cardiovasc Imaging,2021,23(1):61-70.[16]Reddy YNV,Obokata M,Egbe A,et al.Left atrial strain and compliance in the diagnostic evaluation of heart failure withpreserved ejection fraction[J].Eur J Heart Fail,2019,21(7):891-900.[17]张瑞,朱慧珍,黄丹青,等.四维自动左心房定量分析技术评价原发性高血压患者左心房功能的应用价值[J].中华超声影像学杂志,2021,30(8):655-660.[18]季翔,李国杰,冯慧俊,等.峰值应变离散度评价慢性肾脏病患者左室收缩同步性的研究[J].临床超声医学杂志,2022,24(1):67-70.[19]Vasile VC,Jaffe AS.Natriuretic peptides and analytical barriers[J].Clin Chem,2017,63(1):50-58.[20]Prastaro M,Paolillo S,Savarese G,et al.N-terminal pro-B-type natriuretic peptide and left atrial function in patients with congestiveheart failure and severely reduced ejection fraction[J].Eur JEchocardiogr,2011,12(7):506-513.[21]Kaesler N,Babler A,Floege J,et al.Cardiac remodeling in chronic kidney disease[J].Toxins(Basel),2020,12(3):161.(收稿日期:2023-03-22)·病例报道·孕妇,31岁,孕3产2,孕25+6周,因外院产前超声检查提示胎儿三血管-气管(3VT)切面显示主-肺动脉间异常分流,今来我院进一步检查。
KDIGO指南解读_急性肾损伤的诊治_汤晓静
作者单位:第二军医大学长征医院肾内科解放军肾脏病研究所,上海200003通讯作者:梅长林,电子信箱:chlmei1954@指南与共识KDIGO 指南解读:急性肾损伤的诊治汤晓静,梅长林文章编号:1005-2194(2012)12-0914-04中图分类号:R 692.5文献标志码:A提要:急性肾损伤(AKI )是临床常见危重病症,发病率逐年增高,对于AKI 的诊断和防治仍存在许多争议。
因此,2011年12月国际改善全球肾脏病预后组织(KDIGO )制定了AKI 的指南,强调AKI 的早期诊断及治疗、危险因素的控制、肾脏替代治疗方法的应用等。
本文重点介绍AKI 定义、防治及透析干预方面的内容,并简介相应指南的背景及立论依据。
关键词:急性肾损伤;KDIGO ;诊治指南Interpretation of KDIGO guideline for diagnosis and treatment of acute kidney injury.TANG Xiao-jing ,MEIChang-lin.Department of Nephrology ,Kidney Institute of CPLA ,Changzheng Hospital ,Second Military Medical University ,Shanghai 200003,ChinaSummary :Acute kidney injury (AKI )has become a common emergency and is featured by an ever-increasing annual inci-dence rate.Regarding that diagnosis and treatment of AKI have been compelling ,the Kidney Disease :Improving Global Outcomes (KDIGO )established a preliminary clinical guideline for managing AKI in December 2011,for integrating the understandings and prevention measures.Early diagnosis and treatment of AKI ,control of risk factors and implementation of renal replacement therapy were outlined.This review focused on the definition ,prevention and treatment of AKI ,including dialysis intervention ,and briefly introduced the rationales and theoretical evidences of guideline drafting.Keywords :acute kidney injury ;KDIGO ;guideline梅长林,主任医师、教授、博士生导师、三级教授(少将级)。
KDIGO肾小球肾炎的临床实践指南2012中文版120620

KDIGO肾小球肾炎的临床实践指南2012中文版循证依据分级和推荐的等级在指南中,每条临床实践的建议都应该是基于循证医学证据,并对其潜在的益处和风险加以说明,但实际可获取的证据的质和量都是参差不齐的。
当缺乏临床证据时(通常因为没有临床试验),如果不给任何建议,医护人员常会转向咨询这一领域的专家。
而制定基于专家意见的建议至少能建立临床问题的解决框架,并在今后对这一问题优先进行临床试验。
对于肾脏病患者的治疗来说,专家意见仍有特殊意义,因为肾脏病学科的随机对照试验数量小于其他医学学科。
所以KDIGO决定将专家意见写进指南,让读者根据循证依据的分级来进行判断。
KDIGO采用了分级推荐的评估方法(GRADE)。
GRADE方法使得证据质量和推荐强度之间有明确的联系。
KDIGO GRADE方法将证据质量分为高、中、低和极低四个质量级(表4),将推荐等级分为1级和2级两个水准(表5)。
1级表示临床一般都应遵守指南建议,2级表示大多数情况下应遵守指南建议,但是还应根据患者情况权衡利弊,作出选择。
一般认为1级推荐的结论在以后的研究中也不太可能更改,而2级推荐就明确指明需要进一步的研究探索是否有更有效的治疗方法。
第三章 儿童激素敏感型肾病综合征(SSNS)3.1 SSNS初始治疗3.1.1 推荐给予至少12周的激素治疗(强的松或强的松龙)*(1B)3.1.1.1 推荐每日口服单次剂量强的松治疗(1B),起始剂量为60mg/m2/d或2mg/kg/d,最大剂量不超过60mg/d(1D)3.1.1.2 推荐每日口服单次剂量强的松治疗维持4-6周(1C),继之以单次口服强的松40mg/m2或1.5mg/kg的剂量隔日给药(最大剂量为40mg隔日口服)(1D),在以后的2-5月 内逐渐减量(1B)3.2 SSNS复发的激素治疗3.2.1 非频繁复发SSNS的激素治疗3.2.1.1 建议对于非频繁复发SSNS患儿给予每日单次剂量强的松治疗,起始剂量为60mg/m2或2mg/kg(最大剂量60mg/d)直至患儿完全缓解至少3天(2D)3.2.1.2 建议完全缓解后给予隔日单次剂量强的松治疗(40mg/m2或1.5mg/kg,最大剂量为40mg隔日)至少4周(2C)3.2.2 频繁复发(frequently relapsing,FR)和激素依赖(steroid-dependent,SD)SSNS的激素治疗3.2.2.1 建议对于FR或SD SSNS的患儿复发时给予每日强的松方案治疗,直至患儿病情缓解至少3天以后再给予隔日强的松方案治疗至少3月(2C)3.2.2.2 建议隔日强的松方案维持FR或SD SSNS患儿病情缓解时,给予不产生激素主要副作用的最小剂量(2D)3.2.2.3 当SD SSNS患儿使用隔日强的松方案不能维持缓解时,建议给予每日强的松治疗,以不产生激素主要副作用的最小剂量维持(2D)3.2.2.4 FR和SD SSNS患儿在给予隔日强的松方案治疗时,如果发生上呼吸道或者其他部位感染,建议增加激素剂量为同剂量每日口服以减少复发风险(2C) *相同的剂量的泼尼松和泼尼松龙是等效的,且都已经在根据原产地设计的RCTs研究中使用。
KDIGO2012指南

KDIGO2012指南KDIGO2012指南一.CKD贫血治疗指南铁剂在使用铁剂时,应平衡避免(或减少)输血及使用促红细胞生成素(ESA)的潜在获益与预防贫血相关症状发生风险之间的关系(未分级)。
对于未接受铁剂或ESA治疗的成年CKD贫血患者,若不用ESA 也有望使血红蛋白(Hb)浓度升高,且转铁蛋白饱和度(TSAT)≤30%且铁蛋白≤500μg/L,则推荐尝试使用静脉铁剂治疗[在CKD非透析(ND)患者中,或可尝试进行为期1~3个月的口服铁剂治疗](2C)。
?对于需要铁剂的CKD ND患者,根据铁缺乏严重程度、静脉通路的情况、之前对口服铁剂的反应情况、对之前口服或静脉铁剂治疗的不良反应情况、患者依从性和药物价格等因素选择常规的铁剂治疗方法(未分级)。
对于所有未接受铁剂或ESA治疗的儿童CKD贫血患者,当铁蛋白≤100μg/L时,推荐使用口服铁剂治疗[在CKD血液透析(HD)中,或可使用静脉铁剂治疗](1D)。
对所有单纯接受ESA治疗(未补充铁剂)的儿童CKD贫血患者,推荐口服铁剂(在CKD HD中,或可使用静脉铁剂治疗)治疗以维持铁蛋白>100μg/L(1D)。
ESA推荐在开始ESA治疗前,如果可能的话,应先处理所有可纠正的贫血原因(包括铁缺乏和炎症状态)(1A)。
在起始和维持ESA治疗时,推荐应在减少输血所致潜在获益与贫血相关症状所致可能风险(如卒中、高血压等)间进行平衡(1B)。
对有恶性肿瘤史的CKD患者,推荐应谨慎用ESA治疗(1B)。
对于Hb≥100g/L的CKD ND患者,建议不应开始使用ESA治疗(2D)。
对于Hb<100g/L的CKD ND患者,建议基于Hb下降率、需要输血的风险、与ESA治疗相关的风险以及贫血所致症状的出现等情况,个体化决定是否开始应用ESA治疗(2C)。
?对于CKD5期透析患者,当Hb为90~100g/L时,建议开始ESA治疗,以免Hb下降至90g/L以下(2B)。
守护滤清器:认识急性肾损伤与防范

守护滤清器:认识急性肾损伤与防范急性肾损伤(acute kidney injury,AKI)既往也称急性肾衰竭,近年发病率明显升高,全球每年约1300万人发生急性肾损伤(85%患者生活在发展中国家),约170万人死于急性肾损伤及其并发症[1]。
尽管对急性肾损伤的病因和发病机制有了进一步的认识,但在中低收入国家和地区,急性肾损伤的诊断、治疗和预防的措施相对较少,在一些发展中国家急性肾损伤住院患者的治疗已成为社会和家庭巨大的医疗负担,是目前严重影响全球社会经济的公共卫生问题,并受到重视。
本文介绍一下关于急性肾损伤的中西医结合防治。
急性肾损伤的概念:急性肾损伤(acute kidney injury, AKI)是突发但通常可逆的GFR降低。
这会增加血清中的BUN、肌酐及其他本应经肾脏排泄的代谢废物。
此外,如果尿量也减少,则可能导致液体潴留和容量超负荷。
发生急性肾损伤时,肾功能在数小时至数天内突然丧失,导致电解质和酸碱平衡被打破。
急性肾损伤与死亡、心血管事件和进展为慢性肾病的风险增加相关。
中医学中急性肾损伤的概念:祖国医学文献中并没有“急性肾损伤”的病名,急性肾损伤的主要临床表现为水肿、少尿、无尿等,可归属于中医“关格”、“癃闭”、“水肿”等病的范畴。
《伤寒杂病·平脉法》云: “寸口脉浮而大,浮为虚,大为实,在尺为关,在寸为格。
关则不得小便,格则吐逆。
”《证治汇补》说: “关格者…既关且格,必小便不通,旦夕之间,陡增呕恶,此因浊邪壅塞三焦,正气不得升降,所以关于下而小便闭,格于上而生吐呕,阴阳闭绝,一日即死,最为危侯。
”这段话对急性肾损伤的恶心、呕吐、少尿、无尿等症状做了病因的描述并对其预后进行了判断,指出了其预后的凶险。
《素问·奇病论》中描述道: “有病庞然,如有水状,切其脉大紧,身无痛不能食,喜惊,喜已,心气萎者死”。
描述了疾病过程中神经系统及心衰的症状。
《景岳全书·癃闭》曰: “小水不通,是为癃闭,此最危急证也,水道不通则上侵脾胃为胀,外侵肌肉而为肿,泛及中焦则为呕,再及上焦则为喘,数日不通,则夺迫难堪,必致危殆”。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
KDIGO2012Clinical Practice Guideline ckd classification rules out creati-nine clearance24hours urine collection?A.Ognibene,G.Grandi,M.Lorubbio,S.Rapi,B.Salvadori, A.Ter-reni,F.VeroniPII:S0009-9120(15)00310-0DOI:doi:10.1016/j.clinbiochem.2015.07.030Reference:CLB9097To appear in:Clinical BiochemistryReceived date:11February2015Revised date:12July2015Accepted date:26July2015Please cite this article as:Ognibene A,Grandi G,Lorubbio M,Rapi S,Salvadori B, Terreni A,Veroni F,KDIGO2012Clinical Practice Guideline ckd classification rules out creatinine clearance24hours urine collection?,Clinical Biochemistry(2015),doi: 10.1016/j.clinbiochem.2015.07.030This is a PDFfile of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting,typesetting,and review of the resulting proof before it is published in itsfinal form.Please note that during the production process errors may be discovered which could affect the content,and all legal disclaimers thatapply to the journal pertain.A C C E P T E D M A N U S C R I P TKDIGO 2012 C LINICAL P RACTICE G UIDELINE CKD CLASSIFICATION RULES OUT CREATININE CLEARANCE 24 HOURS URINE COLLECTION ?Ognibene A., Grandi G., Lorubbio M., Rapi S., Salvadori B., Terreni A., Veroni F.Laboratorio Generale – Azienda Ospedaliero-Universitaria Careggi - Firenze ItalyCorresponding author:Agostino Ognibenea.ognibene@med.unifi.itPhone: +39 3403460965Azienda Ospedaliero-Universitaria Careggi Largo Brambilla, 350134 Firenze ItalyAbbreviations: Creatinine Clearance (CrCl); Chronic Kidney Disease (CKD); Glomerular Filtration Rate (GFR); Chronic Kidney Disease Epidemiology Collaboration equations (CKD-EPI); estimation Glomerular Filtration Rate (eGFR); Modification of Diet in Renal Disease equation (MDRD).A C C E P T E D M A N U S C R I P TAbstractObjectives: The recent guideline for the Evaluation and Management of Chronic Kidney Disease recommends assessing GFR employing equations based on serum creatinine; despite this, creatinine clearance 24-hours urine collection is used routinely in many settings. In this study we compared the classification assessed from CrCl (creatinine clearance 24h urine collection) and e-GFR calculated with CKD-EPI or MDRD formulas.Design and Methods: In this retrospective study we analyze consecutive laboratory data: creatinine clearance 24h urine collection, serum creatinine and demographic data such as sex and age from 15777 patients >18 years of age collected from 2011 to 2013 in our laboratory at Careggi Hospital. The results were then compared to the estimated GFR calculated with the equations according to the recent treatment guidelines. Consecutive and retrospective laboratory data (creatinine clearance 24h urine collection, serum creatinine and, demographic data such as sex and age) from 15777 patients >18 years of age seen at Careggi Hospital were collected.Results: Comparison between e-GFR calculated with CKD-EPI or MDRD formulas and GFR according CrCl determinations, bias [95% CI] were 11.34 [-47,4/70.1] and 11.4 [-50.2/73] respectively. The concordance for 18/65 years aged group when compared e-GFR classification between MDRD vs CKDEPI, MDRD vs CrCl and CKD-EPI vs CrCl were 0.78, 0.34, and 0.41 respectively, while in the 65/110 years aged group the concordance Kappa were 0.84, 0.38, and 0.36 respectively.Conclusions: The use of CrCl provides a different classification than the estimation of GFR using a prediction equation. The CrCl is unreliable when it is necessary to identify CKD subjects with decrease of GFR of 5 ml/min/1.73 m 2/year.A C C E P T E D M A N U S C R I P TKey words: Glomerular Filtration Rate, Creatinine, MDRD, CKD-EPI, Creatinine Clearance, Chronic Kidney Disease, estimation GFR.IntroductionGlomerular Filtration Rate (GFR) is widely accepted as the best indicator of kidney function, yet in clinical practice except nephrology it is infrequently utilised moreover the GFR so calculated is a very mediocre to use as diagnostic test. GFR calculated by the clearance of exogenous markers such as iothalamate, or iohexol and inulin is considerably time-consuming, expensive, and requires the administration of substances not feasible in routine monitoring [1].GFR can be obtained also by the clearance of endogenous substances, very often urinary clearance of creatinine, computed from 24 hours urine collection (CrCl) [2]. Unfortunately, timed urinary collections are cumbersome and susceptible to error, making the 24 hour urine collections for the measurement of creatinine clearance no longer recommended routinely to estimate the level of kidney function [3].During the last decades, serum creatinine has been the most frequently employed marker to estimate GFR and serial measurements of creatinine are very useful for determining changes in kidney function. The K/DOQI guidelines emphasize the necessity to assess GFR employing equations based on serum creatinine and not to rely on serum creatinine concentration alone [1]. Specifically in the last few years, attention has been focused on two creatinine-based equations that are widely studied and applied, the Modification of Diet in Renal Disease (MDRD) [4] and Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equations [5]. The first one, the MDRD formula, was developed in 1999 and re-expressed in 2007; it estimates GFR adjusted for body-surface area using age and gender as variables and using a standardized method forA C C E P T E D M A N U S C R I P Tthe measurement of serum creatinine [6]. The second one, the CKD-EPI equation, was developed in order to create a more accurate and precise formula than the MDRD, especially when actual GFR is > 60 mL/min per 1.73 m2 [7,8,9].GFR estimation became of extreme importance especially after the publication of the guidelines by KDIGO 2012, Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease (CKD) that updates the 2002 KDOQI Clinical Practice Guidelines for Chronic Kidney Disease [1, 10]. Particular emphasize is given to the change from 5 to 6 categories based on GFR levels to predict risk for outcomes of CKD. In this retrospective study we analyze data collected during three years (2011-13) in our laboratory. Specifically, from the database of the laboratory were extracted all CrCl tests performed during the above period of time. The results were then compared to the equations estimated GFR (e-GFR) in order to verify the concordance between methods, following the recent classification of CKD.Material and methodsStudy populationConsecutive and retrospective laboratory data such as creatinine clearance 24h urine collection (CrCl), serum creatinine (Scr) and demographic data such as sex and age from 15777 patients >18 years of age seen at Careggi Hospital between January 2011 and December 2013 were collected. These data were imported into Microsoft Excel, which was used to perform the eGFR (CKD-EPI and MDRD) calculations.Laboratory assayAll serum and urine creatinine were measured by IDMS-traceable assay on the ADVIA 2400 systems (Siemens Diagnostics) using a creatininase/creatinase based enzymatic method (ECRE_2, Siemens Diagnostics).eGFR algorithmsA C C E P T E D M A N U S C R I P TGFR was estimated using the MDRD study equation (175 × standardized Scr −1.154 × age −0.203 ×1.212[if patient is black] × 0.742 [if patient is female]) and the CKD-EPI equation (CKD-EPI = 141 × min(Scr/k, 1)α × max(Scr/k,1)-1.209 × 0.993age × 1.018 [if patient is female] × 1.159 [if patient is black], where age is in years, k is 0.7 for females and 0.9 for males, α is −0.329 for females and −0.411 for males, min indicates the minimum of Scr/k or 1, and max indicates the maximum of Scr/k or 1). GFR is expressed in ml/min/1.73 m 2[5,6]. CrCl was calculated from urinary creatinine × urinary volume (24h) / serum creatinine. To allow comparison, CrCl were normalized to standard values of 1.73 m 2 BSA, and expressed in ml/min/1.73 m 2.Six GFR category according to KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease were: G1 (>90 ml/min/1.73 m 2), G2 (60-89 ml/min/1.73 m 2), G3a (45-59 ml/min/1.73 m 2), G3b (30-44 ml/min/1.73 m 2), G4 (15-29 ml/min/1.73 m 2), G5 (<15 ml/min/1.73 m 2) [10].Statistical analysisTo compare the effectiveness of the two equations studied we used a Bland and Altman plot. In particular the method calculates the mean difference between two methods of measurement and the 95% limits of agreement as the mean difference (1.96 SD) [11]. Paired-Samples T Test was used to compare the means; Cohen's and Fleiss Kappa were used measuring agreement between classifications [12]. An α <0.05 was considered statistically significant. The statistical analyses were performed with SPSS version 11.0.ResultsTable 1 shows the main characteristic of the study population, all parameters were statistically significant between two sexes except CrCl. Figure 1 shows Bland Altman plots for the comparison between e-GFR calculated with CKD-EPI or MDRD formulas and GFR according to CrCl determinations; mean bias [95% CI] were 11.34[-47.4, 70.1] and 11.4[-50.2, 73] respectively. Moreover when compared differences between e-GFR calculated with CKD-EPI or MDRDA C C E P T E D M A N U S C R I P Tformulas and GFR according CrCl determinations <60 ml/min, mean bias [95% CI] were -3.78[- 36.4, 28.8] and -2.7[-39.6, 34.1] respectively, while when CrCl determinations were >60 ml/min mean bias [95% CI] were 20.6[-43.6, 83.7] and 19.6[-47.6, 86.7] respectively (plots not showed).Figure 2 illustrates the standard error of the mean (SEM) of the differences of the CKD-EPI and MDRD with the mean of the two results, CrCl and CKD-EPI or CrCl and MDRD respectively. The differences were plotted in relation to age groups (A and B plot) and in relation to levels of GFR used for classification in 6 groups described in the recent guidelines for the progression of CKD (C and D plot). In tables 2, are shown the results of cross tabulation between the classification according to the KDIGO criteria, MDRD vs CKD-EPI and CrCl, and CKD-EPI vs CrCl; the concordance between classification tested with Cohen’s Kappa were 0.8, 0.35, and 0.4 respectively.Moreover in figure 3 were showed the comparison of e-GFR classification between CKD-EPI vs CrCl and MDRD vs CKD-EPI in two clusters of age 18/65 (10890/15777) and 65/110 years (4887/15777). The concordance Kappa for the 18/65 years aged group when compared e-GFR classification between CKD-EPI vs CrCl was 0.41 and 0.78 for MDRD vs CKD-EPI, while in the 65/110 years aged group was 0.36 and 0.84 respectively. Finally the overall concordance between MDRD, CKD-EPI and CrCl calculated by Fleiss Kappa test, was 0.52 when considered globally, while when considering separately each class were: 0.62 for G1, 0.41 for G2, 0.41 for G3a, 0.51 for G3b, 0.65 for G4 and 0.75 for G5.ConclusionsThis retrospective study compares three different methods to estimate GFR, two use the formulas MDRD and CKD-EPI and the other is an analytical determination CrCl; all are routinely used to assess kidney function [13].A C C E P T E D M A N U S C R I P TUnfortunately, for the peculiar characteristics of the study and the lack of the clinical outcome, we cannot here determine which of the methods is the most accurate. The main objective of the study is to verify the concordance of the three methods MDRD, CKD-EPI and CrCl, available in the clinical laboratory to estimate GFR.e-GFR is really a numerically-modified serum creatinine adjusted to minimize population variation from age, gender, and race. We know that the factors which may determine the extremely wide scatter seen between all e-GFR calculations, are numerous [14]. Surely the role of the clinical laboratory will be decisive for reducing the analytical bias but also to create the laboratory reports sufficient for the correct interpretation of the data [15]. As well known, small analytic changes in serum creatinine create major shifts in the distributions of eGFR, which can cause large differences in the classification of patients [14,15]. It is also true that while changes in Scr will certainly affect eGFR calculation, both the physiological and analytical changes in Scr are much smaller than the physiological and analytical variation of GFR measurements, whether by inulin or iothalamate. CrCl has at least one advantage over the others in that the blood concentration remains essentially constant during the clearance measurement.In this study, the creatinine enzymatic IDMS-traceable assay used allowed to minimize the analytical bias on the study of agreement between the three methods than non-enzymatic creatinine determination [16].The comparison of the differences from the Bland-Altman analysis shows a high bias of e-GFR obtained from the formulas MDRD or CKD-EPI when compared with CrCl (figure 1). The bias and the distribution of the differences is larger when we consider e-GFR> 90 and in subjects aged <71 years. When we consider the classes with e-GFR <90, the differences are lower but nevertheless the concordance in classification between the CrCl and e-GFR equations is very poor (table 2 and figure 3).The differences between the various age groups and between the levels of GFR are similar both for CKD-EPI for the MDRD compared with CrCl.A C C E P T E D M A N U S C R I P TInterestingly a lower variability of the differences for the CKD-EPI equation, for classes and G3a G3b, and in different age groups than the MDRD equation. This enhanced linearity is probably the result of a more effective normalization equation for estimating GFR (Figure 2).KDIGO (Kidney Disease: Improving Global Outcomes) in 2012 published an updated guideline[10] of “The National Kidney Foundation–Kidney Disease Outcomes Quality Initiative (NKFKDOQI) for evaluation, classification, and stratification of chronic kidney disease (CKD) published in 2002[1]. In particular, in this update of the guidelines the categories of the classification of CKD increased from 5 to 6 distinguishing stage 3 CKD in stage 3a (GFR of 45-59 mL / min / 1.73 m 2) and 3b (GFR of 30-44 mL /min/1.73 m 2). This distinction received approval from the scientific world, justified by the high risk in these categories of mortality and other negative outcomes [19, 20].Guidelines KDOQI and the latest updates KDIGO state that CrCl does not add any information compared to estimated GFR using a prediction equation. This new classification requires, regarding eGFR, greater accuracy but also a lower imprecision. CrCl, besides the overestimation of about 15% of CrCl due tubular secretion, is inconvenient and time consuming, but also imprecise and inaccurate, errors mainly due to reduced muscle mass and erroneous urine sampling [21].In the present study, there is an obvious lack of concordance between CrCl and e-GFR using a prediction equation. The low statistical concordance is more evident especially when we consider G2, G3a and G3b stages, in the table 2, and graphical representation of the concordance in the figure 3 showed the main differences in GFR estimation. These stages represent the groups that more likely will have a progression to renal damage with the highest incidence of risk of adverse events.The e-GFR obtained with the MDRD equation is underestimated in about 25% of the subjects, especially in classes G2, G3a, and G3b when compared with CKD-EPI e-GFR. This phenomenon is more evident when considering the subjects younger than 65 years of age (figure 3).A C C E P T E D M A N U S C R I P TIn light of these results we conclude that the use of CrCl provides a different classification than the estimation of GFR using a prediction equation. Stevens et al. [19] emphasizes the need to better understand the definitions of CKD progression and how they affect clinical practice and trials. The recent guidelines de facto excluded the CrCl for the evaluation and follow-up of patients with CKD, but there are n’t recommendations that advise against the use.Has been demonstrated that serial determinations of CrCl (each month for six months), have a variation greater than serial determinations of creatinine or cystatin C in healthy subjects [22].Then, in addition to the overestimation of CrCl due tubular secretion, the analytical variability of CrCl makes it inadequate and unreliable, especially when it is necessary to identify CKD subjects with progression of disease in presence of a decrease of GFR of 5 ml/min/1.73 m 2/year as recommended in recent guidelines.References[1] National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidneydisease. Am J Kidney Dis 2002;39:S1-S266.[2] Van Lente F, Suit P. Assessment of renal function by serum creatinine and creatinineclearance: glomerular filtration rate estimated by four procedures. Clin Chem 1989;35:2326-30.[3] Stevens LA, Coresh J, Greene T, Levey AS. Assessing kidney function--measured andestimated glomerular filtration rate. N Engl J Med 2006;354:2473-83.A C C E PT EDM A NU SC R I P T[4]Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group.. Ann Intern Med 1999;130:461-70.[5]Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF,Feldman HI, Kusek JW et al. CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann Intern Med 2009;150:604-12.[6]Levey A.S., Coresh J., Greene T., Marsh J., Lesley A.S., et al. for Chronic Kidney DiseaseEpidemiology Collaboration. Expressing the Modification of Diet in Renal Disease Study Equation for Estimating Glomerular Filtration Rate with Standardized Serum Creatinine Values. Clin Chem 2007;53:766-72. [7]Horio M, Imai E, Yasuda Y, Watanabe T, Matsuo S. Modificaton of the CKD epidemiology collaboration (CKD-EPI) equation for Japanase: accuracy and use for population estimates. Am J Kidney Dis 2010;56:32-8[8]Mathew TH, Johnson DW, Jones GR; Australasian Creatinine Consensus Working Group. Chronic kidney disease and automatic reporting of estimated glomerular filtration rate: revised recommendations. Med J Aust 2007;187:459–63.[9]White SL, Polkinghorne KR, Atkins RC, Chadban SJ. Comparison of the prevalence and mortality risk of CKD Australia using CKD Epidemiology Collaboration (CKD-EPI) and Modification of Diet in Renal Disease (MDRD) Study GFR estimating equations: the AusDiab (Australian Diabetes Obesity and Lifestyle) Study. Am J Kidney Dis 2010;55:660-70.A C C E PT EDM A NU SC R I P T[10]KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Supp 2013;3:1-150.[11]Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986;2:307-10.[12]Hale CA1, Fleiss JL. Interval estimation under two study designs for kappa with binaryclassifications.. Biometrics 1993;49:523-4.[13]International Federation of Clinical Chemistry and Laboratory Medicine; Working Group on Standardization of Glomerular Filtration Rate Assessment (WG-GFRA), Panteghini M, Myers GL, Miller WG, Greenberg N.The importance of metrological traceability on the validity of creatinine measurement as an index of renal function. Clin Chem Lab Med 2006;44:1287-92.[14]Botev R, Mallie JP, Wetzels JF, Couchoud C, Schück O. The clinician and estimation of glomerular filtration rate by creatinine-based formulas: current limitations and quo vadis. Clin J Am Soc Nephrol. 2011; 6: 937-50[15] Toffaletti, John G. Clarifying the Fog of Natural and Manmade Renal Function Tests: Creatinine, Clearances, Glomerular Filtration Rate, and Estimated Glomerular Filtration Rate. Point of Care 2011;10:45-50A C C E PT EDM A NU SC R I P T[16]Klee GG, Schryver PG, Saenger AK, Larson TS.Effects of analytic variations in creatinine measurements on the classification of renal disease using estimated glomerular filtration rate (eGFR). Clin Chem Lab Med 2007;45:737-41.[17]Myers GL, Miller WG, Coresh J, Fleming J, Greenberg N, Greene T, et al. National Kidney Disease Education Program Laboratory Working Group. Recommendations for improving serum creatinine measurement: a report from the Laboratory Working Group of the National Kidney Disease Education Program. Clin Chem 2006;52:5-18.[18] Kuster N, Cristol JP, Cavalier E, Bargnoux AS, Halimi JM, Froissart M, et al. Société Française de Biologie Clinique (SFBC). Enzymatic creatinine assays allow estimation of glomerular filtration rate in stages 1 and 2 chronic kidney disease using CKD-EPI equation. Clin Chim Acta 2014;20:89-95.[19]Lesley A. Inker, Brad C. Astor, Chester H. Fox, Tamara Isakova, James P. Lash, Carmen A. Peralta, et al, KDOQI US Commentary on the 2012 KDIGO Clinical Practice Guideline for the Evaluation and Management of CKD. Am J Kidney Dis 2014;63:713-35[20]Paul E. Stevens, and Adeera Levin, for the Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members* Evaluation and Management of Chronic Kidney Disease: Synopsis of the Kidney Disease: Improving Global Outcomes 2012 Clinical Practice Guideline. Ann Intern Med 2013;158:825-30.[21]Burkhardt H1, Bojarsky G, Gretz N, Gladisch R. Creatinine clearance, Cockcroft-Gault formula and cystatin C: estimators of true glomerular filtration rate in the elderly? Gerontology 2002;48:140-6.A C C E PT EDM A NU SC R I P T[22]Toffaletti JG, McDonnell EH. Variation of serum creatinine, cystatin C, and creatinine clearance tests in persons with normal renal function. Clin Chim Acta. 2008;395:115-9.Legend to figure:Figure 1: Bland –Altman analysis, comparison between GFR according CrCl determinations and e-GFR calculated with CKD-EPI equation (right) bias were 11.34[95% CI -47.4;70.1] or MDRD equation (left), bias 11.4 [95% CI -50.2;73].Figure 2: Standard Error of the Mean (SEM) of the differences of the CKD-EPI and MDRD withthe mean of the two results, CrCl and CKD-EPI or CrCl and MDRD respectively. The SEM of thedifferences was in relation to age groups (A and B plot) and in relation to levels of GFR (C and D plot), in x axis N represent the number of subjects for each class of age or GFR categories.Figure 3: Comparison of GFR estimation between MDRD vs CrCl (A), CKD-EPI vs CrCl (B) and MDRD vs CKD-EPI in the subjects of 18-65 (C) and 65-110 (D) years of age, according KDIGO stages. In Y axis is reported number of subjects.ANU STable1: Characteristics of the studied population, data are expressed as mean ±SD.Table 2: Number of subjects included in the categories specified by the KDIGO guidelines 2012, according to the estimation of GFR with: CrCl, CKD-EPI and MDRD.A CC15Figure 1T16Figure 2 95% C I S E M (m l /m i n /1.73 m 2)95% C I S E M (m l /m i n /1.73 m 2)Figure 317A C C E PT EDM A NU SC R I P THighlights1 - Clearance of creatinine computed from 24-hour urine collection2 - KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of ChronicKidney Disease3 - Modification of Diet in Renal Disease (MDRD) and Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equations .。