RHPS4_端粒酶抑制剂_390362-78-4_Apexbio
端粒酶抑制剂伊美司他治疗血小板增多IF56
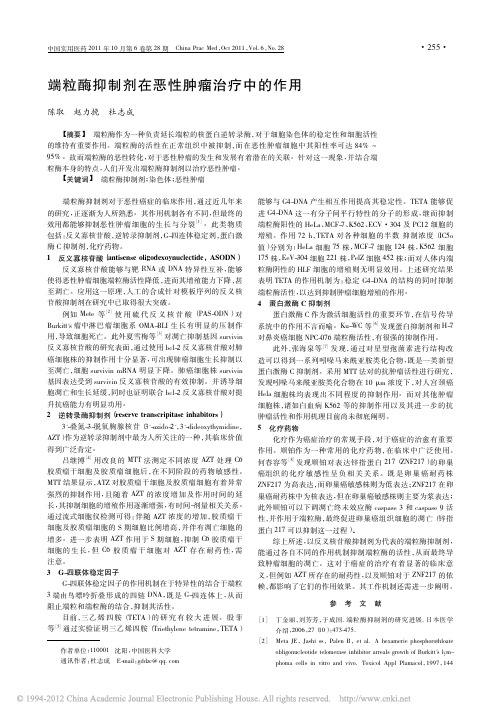
T h e ne w engl a nd jour na l o f medicineFrom the Department of Hematology, University Hospital of B ern and Univer-sity of B ern, B ern, Switzerland (G.M.B., E.O.L., M.D.); the Department of Hema-tology, School of Medicine, Cardiff Uni-versity, Cardiff, United Kingdom (O.G.O.); Upstate Oncology Associates, Greenville, SC (G.S.); the Section of Hematology and Oncology, University of Chicago, Chica-go (O.O.); the Divisions of Hematologic Malignancies and Hematology, Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins University School of Med-icine, B altimore (M.A.M.); the Depart-ment of Hematology, University Hospital Essen, Essen, Germany (A.R.); and Geron, Menlo Park (B.B., M.S.), and the Depart-ment of Hematology and Hematopoietic Cell Transplantation, City of Hope, Gehr Family Center for Leukemia Research, Duarte (D.S.S.) — both in California. Ad-dress reprint requests to Dr. Baerlocher at the Department of Hematology, Stem Cell and Molecular Diagnostics Labora-tory, Freiburgstr. 4, Inselspital, University Hospital of Bern, CH-3010 Bern, Switzer-land,or at g abriela.b aerlocher@i nsel.c h. N Engl J Med 2015;373:920-8.DOI: 10.1056/NEJMoa1503479Copyright © 2015 Massachusetts Medical Society.BACKGROUNDImetelstat, a 13-mer oligonucleotide that is covalently modified with lipid exten-sions, competitively inhibits telomerase enzymatic activity. It has been shown to inhibit megakaryocytic proliferation in vitro in cells obtained from patients with essential thrombocythemia. In this phase 2 study, we investigated whether ime-telstat could elicit hematologic and molecular responses in patients with essential thrombocythemia who had not had a response to or who had had unacceptable side effects from prior therapies.METHODSA total of 18 patients in two sequential cohorts received an initial dose of 7.5 or9.4 mg of imetelstat per kilogram of body weight intravenously once a week until attainment of a platelet count of approximately 250,000 to 300,000 per cubic milli-meter. The primary end point was the best hematologic response.RESULTSImetelstat induced hematologic responses in all 18 patients, and 16 patients (89%) had a complete hematologic response. At the time of the primary analysis, 10 pa-tients were still receiving treatment, with a median follow-up of 17 months (range, 7 to 32 [ongoing]). Molecular responses were seen in 7 of 8 patients who were positive for the JAK2 V617F mutation (88%; 95% confidence interval, 47 to 100). CALR and MPL mutant allele burdens were also reduced by 15 to 66%. The most common adverse events during treatment were mild to moderate in severity; neu-tropenia of grade 3 or higher occurred in 4 of the 18 patients (22%) and anemia, headache, and syncope of grade 3 or higher each occurred in 2 patients (11%). All the patients had at least one abnormal liver-function value; all persistent elevations were grade 1 or 2 in severity.CONCLUSIONSRapid and durable hematologic and molecular responses were observed in patients with essential thrombocythemia who received imetelstat. (Funded by Geron; number, NCT01243073.)ABSTR ACTTelomerase Inhibitor Imetelstat in Patients with Essential ThrombocythemiaGabriela M. Baerlocher, M.D., Elisabeth Oppliger Leibundgut, Pharm.D.,Oliver G. Ottmann, M.D., Gary Spitzer, M.D., Olatoyosi Odenike, M.D., Michael A. McDevitt, M.D., Ph.D., Alexander Röth, M.D., Michael Daskalakis, M.D., Bart Burington, Ph.D., Monic Stuart, M.D.,and David S. Snyder, M.D.Imetelstat in Essential ThrombocythemiaE ssential thrombocythemia, a myelo-proliferative neoplasm, is a clonal disorderof a multipotent hematopoietic progenitor cell.1,2 The disease is associated with an in-creased risk of thrombotic complications, hemor-rhagic complications, or both, and can evolve into myelofibrosis or, in rare cases, can trans-form to acute leukemia.3 Common mutations associated with essential thrombocythemia are found in the Janus kinase 2 (JAK2) gene, the gene encoding the thrombopoietin receptor (MPL), and the calreticulin (CALR) gene.4-8 Cur-rent standard therapies for high-risk patients with essential thrombocythemia induce nonspe-cific reductions in platelet counts but do not typically eliminate or alter the biologic charac-teristics of the disease.9-12We have reported that telomerase activity in malignant cells obtained from patients with es-sential thrombocythemia and induced telomerase activity in cells isolated from healthy donors were inhibited by the telomerase inhibitor imetelstat.13 However, imetelstat inhibited spontaneous pro-liferation of megakaryocytic colonies obtained from patients with essential thrombocythemia but did not inhibit cytokine-induced megakaryo-cytic colonies from healthy donors. These find-ings suggest an intrinsic sensitivity of essential-thrombocythemia megakaryocytes to telomerase inhibition.13Imetelstat, a 13-mer thiophosphoramidate oli-gonucleotide that is covalently modified with lipid extensions, inhibits telomerase enzymatic activity14 (see the Supplementary Background sec-tion in the Supplementary Appendix, available with the full text of this article at ). In this phase 2 study, we investigated whether im-etelstat could elicit hematologic and molecular responses in patients with essential thrombocy-themia who had disease that was refractory to prior therapies or who had had unacceptable side-effects from previous therapies.MethodsEligibility CriteriaPatients who were 18 years of age or older and had received a diagnosis of essential thrombocy-themia defined according to World Health Orga-nization criteria15 (Table S1 in the Supplemen-tary Appendix) were eligible for enrollment if they required cytoreduction because of a platelet count higher than 600,000 per cubic millimeter and if they had not had a response to or had had unacceptable side effects from at least one prior therapy or if they declined to receive standard therapy. Additional inclusion and exclusion cri-teria are described in the Supplementary Ap-pendix.Study DesignThis was a phase 2, open-label study that was conducted at seven sites in the United States, Germany, and Switzerland; enrollment occurred during the period from January 2010 through January 2013. Patients were enrolled into se-quential cohorts that received weekly doses of 7.5 or 9.4 mg of imetelstat per kilogram of body weight, intravenously, until a platelet count of approximately 250,000 to 300,000 per cubic milli-meter was achieved or toxic effects occurred. Maintenance dosing at a reduced frequency be-gan after a patient had a complete or partial hematologic response (Table S2 in the Supple-mentary Appendix), with doses (7.5 to 11.7 mg per kilogram) adjusted according to the patient’s response and the side-effect profile of the drug. Additional details regarding the study design are provided in the Supplementary Appendix.The primary end point of the study was the best overall hematologic response, which was defined according to the platelet response com-ponent of the 2009 European LeukemiaNet (ELN) response criteria16 (Table S2 in the Supplemen-tary Appendix). Secondary end points included the frequency and severity of adverse events, the duration of hematologic response, the ELN “clin-icohematologic” response, and the molecular response in patients with JAK2 V617F mutations (Table S2 in the Supplementary Appendix), MPL W515L or MPL W515K mutations, or CALR mu-tations.All patients were assessed for JAK2 V617F, MPL W515L, MPL W515K, and CALR mutations at baseline and were reassessed every 12 weeks (±4 weeks) (see the Supplementary Methods sec-tion in the Supplementary Appendix). Patients who were enrolled in Europe underwent testing of spontaneous growth inhibition of mega-karyocyte colony-forming units (CFUs) (see the Supplementary Methods section in the Supple-mentary Appendix).T h e ne w engl a nd jour na l o f medicineSafety AssessmentData were collected on the extent of imetelstat exposure and on all adverse events. Adverse events were summarized according to terms used in the Medical Dictionary for Regulatory Activities, and severity was assessed with the use of the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE),17 version 4.03. For events with varying severity, the maxi-mum reported grade was used in summaries. Laboratory abnormalities were defined accord-ing to normal laboratory ranges from each insti-tution and converted to CTCAE grades.Study OversightThis phase 2 study was approved by the institu-tional review board at each participating site. The study was conducted in accordance with the International Conference on Harmonisation Good Clinical Practice guidelines. All patients provid-ed written informed consent.The sponsor, Geron, provided the study drug and in collaboration with the authors designed the study and analyzed the data. The first author wrote the initial draft, and subsequent drafts were written by all authors with assistance from medical writers paid by Janssen Research and Development. All the authors made the decision to submit the manuscript for publication and vouch for the accuracy and completeness of the data and analyses and for adherence to the study protocol, which is available at . Clini-cal-trial agreements between the sponsor and the authors’ institutions included confidentiality provisions.Statistical AnalysisThe analysis of the primary end point of hema-tologic response included all patients who re-ceived at least one dose of imetelstat. The analy-sis of the duration of response included all patients who had a response. The analysis of molecular response included patients who re-ceived at least one dose of imetelstat and who had a JAK2 V617F, MPL W515L, MPL W515K, or CALR mutant allele burden at baseline. For re-sponse end points, exact 95% confidence inter-vals were calculated. The duration of hemato-logic response was estimated with the use of the Kaplan–Meier method. Patients who were lost to follow-up, discontinued the study, or began to receive other essential thrombocythemia–directed therapy before a hematologic response was documented and confirmed were counted as not having had a response. Safety analyses included all patients who received at least one dose of imetelstat.R esultsPatientsA total of 18 patients were enrolled in the study, and all had received one or more previous treat-ments; 17 had received hydroxyurea (94%), 13 had received anagrelide (72%), and 4 had received interferon (22%) (Table 1). Nine of the 18 pa-tients (50%) had disease that was resistant to at least one prior therapy, and 14 (78%) had had unacceptable side effects from prior therapy. The median time from the initial diagnosis ofe ssential thrombocythemia to enrollment was7.2 years (range, 0.3 to 24.9), and the median baseline platelet count was 788,000 per cubic millimeter (range, 521,000 to 1,359,000). Fifteen patients had baseline mutant allele burdens (8 with JAK2 V617F mutations, 2 with MPL W515L or MPL W515K mutations, and 5 with CALR mu-tations) (Table 1). Table S3 in the Supplementary Appendix describes additional baseline charac-teristics of the patients.Primary Efficacy End Point and Key Secondary Efficacy End PointOf the 18 patients who received imetelstat, 7 re-ceived an initial dose of 7.5 mg per kilogram and 11 received 9.4 mg per kilogram intravenously. The overall rate of hematologic response was 100% (95% confidence interval [CI], 83 to 100), and 16 of the 18 patients (89%) had a complete hematologic response (95% CI, 65 to 99) (Fig. 1A). In the 2 patients with a partial hematologic re-sponse, the lowest platelet counts were 261,000 per cubic millimeter at 23 weeks and 56,000 per cubic millimeter at 18 weeks, but neither response was sustained. Among the 16 patients who had a complete hematologic response, the median time to a complete response was 6.1 weeks (range, 5.1 to 12.1); the median time to a com-plete response was similar in JAK2 V617F–posi-tive and JAK2 V617F–negative patients. A trend was observed toward a more rapid response in patients in whom the initial dose was 9.4 mg per kilogram than in those in whom the initial dose was 7.5 mg per kilogram (median, 6.1 vs. 12.1Imetelstat in Essential Thrombocythemia weeks), although the difference was not signifi-cant (P = 0.71).During maintenance dosing, intermittent dos-ing was attempted in most patients and thefrequency of dosing generally decreased withtime; all the patients who had a complete hema-tologic response received a dose every 2 weeksor less frequently. At the time of the primaryanalysis, with a median follow-up of 17 months,10 of the 16 patients with a complete hemato-logic response (62%) were still receiving treat-ment, and the median duration of responsehad not been reached (follow-up range, 5 to 30months).While receiving the study treatment, one pa-tient had grade 2 bilateral retinal ischemia andwas recovering, and another had grade 2 lefthemiparesis and recovered; these thromboem-bolic events were assessed by the study investi-gators as being potentially related to underlyingessential thrombocythemia. The durations ofresponse ended at the reported onset of theseconditions, no further clinical follow-up infor-mation was obtained, and neither patient dis-continued imetelstat. Three patients had diseaseprogression from essential thrombocythemia tosecondary myelofibrosis, either during the studytreatment period or during the safety follow-upperiod.Other Secondary Efficacy End PointsMolecular ResponseA partial molecular response was detected inseven of eight patients with JAK2 V617F mutationsat baseline (88%; 95% CI, 47 to 100) (Fig. S1 inthe Supplementary Appendix). The median JAK2V617F mutant allele burden was reduced by 71%at month 3 after the initiation of treatment andremained reduced by 59% at month 12 despiteless frequent maintenance dosing (Fig. 1B).MPL W515L, MPL W515K, and CALR mutantallele burdens were also reduced, by 15 to 66%. Further information is provided in Table S4 in the Supplementary Appendix.Inhibition of ProliferationA megakaryocyte CFU assay was performed in five patients. It showed substantial inhibition of spontaneous proliferation at 1 month after ini-tiation of imetelstat treatment, with a median 92% reduction from baseline (Table S5 in the Supplementary Appendix).ELN “Clinicohematologic” ResponseResults with respect to the secondary end pointof a “clinicohematologic” response according toELN criteria16 (see Table S2 of the Supplementary Appendix) were similar to those of the primaryend point. A complete ELN clinicohematologic response was observed in 17 of the 18 patients (94%), and a partial response was observed in1 patient (6%). In 1 patient, splenomegaly thatwas palpable at 3 cm at baseline became nonpal-pable after the first cycle of treatment. None of* O ne patient did not meet the inclusion criteria for the minimum baseline platelet count, but the investigator thought that cytoreductive therapy was clinically indicated.† T hree patients had no mutation.T h e ne w engl a nd jour na l o f medicinethe 18 patients had constitutional symptoms at baseline.Telomerase Activity, Telomere Length, and Bone Marrow ResponseFigure S3 in the Supplementary Appendix shows telomerase activity. Assessments of telomere length and bone marrow response are described in the text of the Supplementary Appendix.S afetyThe most frequent adverse events that occurred during treatment (those that occurred in 50% or more of the patients and selected clinically sig-nificant adverse events) are listed in Table 2. All adverse events are listed in Table S6 in the Sup-plementary Appendix. Adverse events were re-ported in all patients, and 15 of the 18 patients (83%) reported at least one event of grade 3 or higher. Eighteen events of grade 3 or higher were attributed to imetelstat by the investigators, including neutropenia, headache, anemia, and a syncopal episode due to an infusion reaction (a second syncopal episode in the same patient was deemed to be unrelated to imetelstat). One grade 4 adverse event (a femoral-neck fracture) was reported by the treating clinician as being unrelated to imetelstat (Table S6 in the Supple-mentary Appendix). Eight of the 18 patients (44%) discontinued the study (Table S7 in the Supplementary Appendix).The most common nonlaboratory adverse events attributed to imetelstat were fatigue (in 15 of the 18 patients), nausea (in 12), diarrhea (in 11), and headache (in 8) (Table S8 in the Supplemen-tary Appendix). Infections occurred during treat-ment in 17 of the 18 patients (94%); 15 of these 17 patients (88%) had infections of grade 2 or lower. The most common infections were upper respiratory infections (in 39% of the patients), urinary tract infections (in 22%), and influenza (diagnosed on the basis of clinical and labora-tory findings), nasopharyngitis, and rash (each in 17%). The infections lasted less than 3 weeks in 81% of the patients and were not typically as-sociated with cumulative imetelstat exposure or with concurrent neutropenia or lymphopenia.At least one increase in grade, from baseline, in a liver-function value was observed in all 18 patients (Table 3). The majority of patients had grade 1 increases in alanine aminotransferase levels, with accompanying grade 1 increases in aspartate aminotransferase levels (the latter per-Figure 1. Hematologic and Molecular Responses in Patients Who Received Imetelstat.Panel A shows the hematologic response according to mutation status (cal-reticulin [CALR ], Janus kinase 2 [JAK2] V617F, MPL W515L or MPL W515K mutations, or no mutation). A complete hematologic response was observed in 16 of the 18 patients in the study (89%), and a partial hematologic response (“no complete response”) was observed in 2 patients (11%). The median time to a complete hematologic response was 1.4 months. Percentages shown are the best percent change in the mutant allele burden from base-line. Panel B shows the molecular response in JAK2 V617F–positive patients after treatment with imetelstat. The median JAK2 V617F mutant allele bur-den was reduced by 71% at month 3 and by 59% at month 12 despite less frequent maintenance dosing. I bars indicate 95% confidence intervals. The percent change shown is the median percent change in the JAK2 V617F mutant allele burden from baseline.CALR−31−36−48−55−15JAK2 V617FNo mutation04628121026181614282220243230MonthsB Molecular ResponseA Hematologic ResponseTime to first platelet count of 400×103/mm 3Time to complete responseNocomplete responseTreatment continuedM e d i a n J A K 2 V 617F (p e r c e n t c h a n g e f r o m b a s e l i n e )C h a n g e f r o m B a s e l i n e (%)−40−20−60−80−100Baseline 3691215MonthsP=0.001No. at Risk Percent Change88−718−688−727−595−52Discontinuation of treatment−96−82MPL−93−24−90−72−96−82−66−16−50−25Imetelstat in Essential Thrombocythemia sisted with ongoing imetelstat treatment). With-in 4 weeks after the initiation of imetelstat treat-aminotransferase level of 5 to 7 times the stan-dard upper limit of the normal range (grade 3)and concurrent increases in the aspartate ami-notransferase level of 2 to 6 times the standardupper limit of the normal range (grades 1 to 3)with dose reduction and did not recur with con-tinued treatment. With a longer duration oftreatment, persistent (≥6 weeks) grade 1 in-creases in alkaline phosphatase levels were ob-served in 14 of the 18 patients; these increaseswere associated with grade 1 or 2 unconjugated hyperbilirubinemia in 4 patients (Table 3).In post-study follow-up safety assessments,among the 14 patients who had persistent (≥6weeks) abnormalities in liver-function values, 11(79%) had values that reversed to normal orbaseline values. In 3 patients, the liver-functionvalues did not return to the upper limit of thenormal range; all hepatic biochemical abnor-malities in 2 of these patients improved, withcomplete resolution of the abnormal values, andthe 1 remaining patient whose condition wasnot improving at the end of follow-up had pro-patients who underwent extended follow-up forpersistent (≥6 weeks) abnormalities on liver-function tests, the median time to resolutionafter discontinuation of treatment was 12 weeks.The observed resolutions of these abnormalitiesfollowed permanent discontinuation of ime-telstat in all patients as the result of a full clini-cal hold issued by the Food and Drug Adminis-tration (FDA) (see the Discussion section).After the primary analysis was performed inOctober 2013, one patient who had received im-etelstat for approximately 3 years died frommonths after discontinuation of treatment. Cir-rhosis, secondary to hepatic steatosis, was thesuspected underlying disease. Although the pa-tient’s age (83 years), multiple coexisting condi-tions (including a history of exposure to hepati-tis B), and concomitant medications confoundedassessment, imetelstat could not be conclusivelyexcluded as a contributory agent.Hematologic toxic effects, defined according to changes in laboratory results from baseline values, are listed in Table 4. Thrombocytopenia of less than grade 3 was seen in 9 of the 18 pa-tients (50%). Neutropenia was observed in 15 pa-tients (83%), including 7 with grade 3 neutrope-nia (39%) and 3 with grade 4 neutropenia (17%).* I ncluded are the adverse events that occurred in 50% or more of the patients and selected clinically significant adverse events, regardless of whether they were deemed to be related to the study drug. The grade of adverse event was defined on the basis of the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE).* L aboratory abnormalities were defined on the basis of normal laboratory rang-es at each institution and were graded according to the CTCAE. The maximum grade was calculated for patients who had an increase in grade, as compared with the baseline grade. There were no grade 4 increases.na l o f medicineNo cases of febrile neutropenia were reported,and no patients with grade 4 neutropenia had a concurrent infection. Lymphopenia was reported in 6 patients (33%), with one grade 3 event. Fif-teen patients (83%) had anemia, and 3 (17%) had grade 3 anemia. Three patients required red-cell transfusions, including a patient who had a postsurgical hemorrhage. Three reported cases of cytopenia led to dose reductions: one for grade 1 thrombocytopenia, one for grade 3 ane-mia in a patient who required a red-cell transfu-sion, and one for grade 3 neutropenia; all three cases resolved.DiscussionIn this study, imetelstat rapidly induced hemato-logic responses in patients with essential throm-bocythemia who had disease that was refractory to conventional therapies or who had had unac-ceptable side effects from conventional therapies. All the patients had a hematologic response, and 89% had a complete hematologic response, a rate that exceeded rates observed with hydroxyurea, anagrelide, and interferon treatment.12,18-21 Else-where in this issue of the Journal , Tefferi et al. report the results of a pilot study of imetelstat therapy showing the induction of complete or partial remissions, as well as molecular remis-sions, in a subgroup of patients with myelofi-brosis.22JAK2 V617F may provide a useful marker of neoplastic proliferation, and current therapies elicit molecular responses in only a minority of patients with this mutation.12,20,23,24 In contrast,a rapid, substantial reduction in mutant allele burden was observed in all JAK2 V617F–positive patients in this study; 88% of patients had a partial molecular response. Attenuation and loss of a molecular response later during therapy may be due in part to reduced-frequency maintenance dosing; this suggests that the duration of ime-telstat treatment was insufficient to eliminate all mutated committed and clonal primitive hema-topoietic progenitors. The decrease in the CALR and MPL mutant allele burdens provides support for the hypothesis that imetelstat can reduce the various malignant clones observed in myelopro-liferative neoplasms. The decrease in the mutant allele burden appeared to be more pronounced for the JAK2 V617F mutations than for the CALR mutations, possibly because of activation of telomerase reverse transcriptase by the Janus kinase–signal transducer and activator of tran-scription (JAK-STAT) signaling pathway in pa-tients with essential thrombocythemia who had JAK2 V617F mutations.25,26Megakaryocyte CFU assays that were used to more directly measure inhibition of proliferation showed more than 90% inhibition of baseline proliferation activity within 1 month after the initiation of treatment in four of the five patients tested. These data suggest that imetelstat may have a selective inhibitory effect on the growth of the neoplastic clone or clones that drive es-sential thrombocythemia.Although all the patients had hematologic responses, there were subsequent fluctuations above normal platelet levels in all patients. Re-sponses were considered to be durable if inter-mittent dosing restored and maintained the platelet count (≤600,000 per cubic millimeter for a partial response or ≤400,000 per cubic milli-meter for a complete response). Once an initial response was achieved, patients with platelet counts that were not controlled by maintenance dosing (i.e., platelet counts that were >600,000 per cubic millimeter in patients with a partial response or >400,000 per cubic millimeter in patients with a complete response) for at least 8 weeks were considered to have a loss of re-sponse. The reported complete hematologic re-sponses were durable but required ongoing ime-telstat therapy; interpatient variability was noted in the frequency of dosing required to manage platelet levels (every 2 weeks to every 4 weeks or more) (Fig. S2 in the Supplementary Appendix).* L aboratory abnormalities were defined on the basis of normal laboratory rang-es at each institution and were graded according to the CTCAE. The maxi-mum grade was calculated for patients who had an increase in grade, as com-pared with the baseline grade.Imetelstat in Essential ThrombocythemiaAfter discontinuation of treatment, increases in platelet counts were consistent with the main-tenance interval during treatment. Patients with longer treatment intervals had more gradual increases after discontinuation of treatment, whereas patients who required more frequent dosing had more rapid increases.At the time of the primary analysis, 10 pa-tients were still receiving treatment, with a median follow-up of 17 months (range, 7 to 32 [ongoing]). Of the adverse events attributed to imetelstat, most were mild to moderate; 18 events were of grade 3 or higher (Table S8 in the Sup-plementary Appendix). Upper respiratory infec-tions, which were reported in 6 of 18 patients (33%), were mostly mild to moderate and were not associated with myelosuppression or disease progression. Three patients had disease progres-sion from essential thrombocythemia to second-ary myelofibrosis, either during the study treat-ment period or during the safety follow-up period, and JAK inhibitor therapies were initiat-ed. Among these 3 patients, one had an unrelated grade 2 upper respiratory tract infection and grade 3 osteomyelitis and another had grade 2 influenza.In a study involving 1104 patients, the rates of progression from essential thrombocythemia and from early or prefibrotic primary myelofi-brosis to overt myelofibrosis were 0.8% and 12.3%, respectively, at 10 years and 9.3% and 16.9%, respectively, at 15 years.26 The prognostic variables associated with death or progression to leukemia or myelofibrosis were bone marrow histologic features (early or prefibrotic primary myelofibrosis vs. essential thrombocythemia), age (>60 years), history of thrombosis, leukocy-tosis, and anemia.27 The 3 patients in our study who had disease that progressed to myelofibro-sis had essential thrombocythemia for 12, 13, and 21 years and were 67, 61, and 56 years old, respectively, when myelofibrosis was diagnosed. Two of the 3 patients received the diagnosis near the date of their last dose of imetelstat, and 1 received the diagnosis 6 months after the last dose, during extended follow-up of liver func-tion. At baseline, 2 of the 3 patients had 1+ and 2+ reticulin fibrosis in the bone marrow, and the hemoglobin level in all 3 patients was lower than 12 g per deciliter. The rate of progression to myelofibrosis in the current study (17%; 3 of 18 patients) is higher than historical estimates; however, the small number of patients in this study and the presence of prognostic factors make cross comparisons difficult.Abnormal results of liver-function tests were observed frequently but were mostly mild in grade; one fatal event of bleeding esophageal varices occurred after the primary-analysis time point. On March 11, 2014, the FDA issued a full clinical hold on imetelstat, citing a lack of evi-dence of reversibility of hepatotoxicity, concern regarding a risk of chronic liver injury, and a lack of adequate follow-up in patients who had hepatotoxic effects. All the patients who were still receiving the study medication permanently discontinued active treatment and were observed for safety. Follow-up safety data showed that treatment-related abnormalities on liver-function tests resolved in most patients (Table S9 in the Supplementary Appendix), and the FDA lifted the clinical hold on October 31, 2014.In conclusion, imetelstat, a telomerase inhibi-tor, had a clinically significant effect on disease burden in patients with essential thrombocythe-mia who had not had a response to previous treatment or who had had unacceptable side ef-fects from conventional therapies. Neutropenia and abnormal liver-function tests were the main adverse events. Furthermore, molecular respons-es were observed in patients with mutated JAK2 and CALR molecular signatures; this finding suggests therapeutic activity in the malignant clones that are the underlying source of essential thrombocythemia.Supported by Geron.Disclosure forms provided by the authors are available with the full text of this article at .We thank the patients who volunteered to participate in this study and the study site staff who cared for them: Renata Bünter, Ursina Sager, Regula Jäggi, and Dr. Stephan Reichenbach at the Clinical Trials Unit of the University of Bern, Switzerland; Drs. Alexandre Theocharides, Gabi Vetsch, Giuseppe Colucci, and other members of the Clinical Hematology Team of the Univer-sity Hospital of Bern; Dr. Monika Haubitz, Dr. Meike Dahlhaus, Ingrid Helsen, Barbara Hügli, Elisabeth Ischi, and other mem-bers of the Experimental Hematology, Molecular Diagnostics, and Stem Cell Laboratory of Hematology teams of the University of Bern and University Hospital of Bern; the staff of Geron who were involved in data collection and analyses, including Dr. Joi Ninomoto for contributions to study design, and Ted Shih, Neeru Batra, Dianne Morfeld, and Raheela Kauser Steiner of Geron for their contributions to data acquisition, review, and interpreta-tion in previous studies and throughout the span of the trial; and Dr. Tracy T. Cao of Source One Technical Solutions and Dr. Namit Ghildyal of Janssen Research and Development, for edi-torial assistance with an earlier version of the manuscript.。
端粒酶抑制剂在恶性肿瘤治疗中的作用
[2] Meta JE,Jashi ss,Palen B,et al. A hexamerie phosphorothloate obligonucleotide telomerase inhibitor arreals growth of Burkitt's lymphoma cells in vitro and vivo. Toxicol Appl Plamacol,1997,144
老年人经常患各种疾病,且所患疾病大多为慢性病,病程 长且不易治愈,因此许多老年人不仅需要常年反复用药,而且 还联合使用多种药物,所以往往出现“服药能力下降”如添服 多服等。老年人常用药物有: 抗高血压药,强心药,抗心律失 常药,安眠药,降糖药,抗凝血药,泻药等。因此护士在给药过 程中应撕去包装( 锡纸) 按时送给患者并亲自照顾其服用,内 服药与外用药应分开放置标记鲜明并向患者讲解清楚。夜间 式睡眠中给老人服药一定要把老人叫醒后再服药,以防似醒 非醒时服药误入气管,从而造成呛咳。服用镇静催眠药易引 起有头晕、思睡,服药后应指导患者卧床休息避免走动; 服用 降压药易发生体位性低血压,应告知患者起床及改变体位时 动作宜缓慢; 降糖药应按要求在餐前或进餐时正常服用,并督 促患者按时进餐,以防引起低血糖; 对于泻药的服用,应根据 患者的排便规律合理安排服药时间,尽量避免晚上排便,以免 患者受凉及夜间病情变化。对老年患者使用的一些特殊药物 如: 心得安利多卡因、安定、抗凝血药、洋地黄等,因其存在代 谢缓慢,半衰期延长,血药浓度增高等,用药时护士应严密观 察用药后的反应; 对有医嘱但属患者自备的药物如: 抗血小板 聚集的硫酸氯吡咯雷片,抗肿瘤的环孢素 A 胶囊,及激素类
最新抗衰老手段,NMN的真实效果,你不知道就Out了!

最新抗衰老手段,NMN的真实效果,你不知道就Out了!我们总以为抗衰老是中老年女性的专利,殊不知25-29岁才是抗衰老的黄金时期,因为女性一旦过了30岁,不管是容颜还是身材,都开始走下坡路。
2018年世界卫生组织在《国际疾病法典》中宣布,衰老是一种可以治疗的疾病。
如果能研究出一种有效治疗衰老的“不老神药”,那我们就能活得更久了,想想也是很美好的。
抗衰老领域中,有种可以让DNA保持稳定性的物质叫“端粒”,端粒的长度过低,会导致DNA 损伤,基因组的稳定性一旦打破了平衡,就会使细胞衰老。
所以,端粒缩短就是衰老的标志之一。
细胞中负责端粒延长的是一种酶,叫做“端粒酶”,它由催化蛋白和RNA模板构成,可以将端粒延长并修复,从而弥补端粒的损耗。
只可惜,端粒酶只存活于干细胞内,无法填补随衰老的端粒缩短。
端粒与衰老的关系如此紧密,科学家便试图通过延长端粒的长度,看能否避免因端粒缩短而引起的寿命缩短以及随着年龄增加而导致的相关疾病。
2019年10月17日,CNIO(西班牙国立癌症中心)的研究人员建立了携带超长端粒的小鼠模型,将右图绿色的小鼠胚胎的P1代胚胎干细胞进行体外培养,培养出含超长端粒的胚胎干细胞,随后将这个胚胎干细胞注射到C57BL6的小鼠桑葚胚中,等待它孕育出生。
此嵌合体小鼠经检验后显示,100%细胞都含有超长端粒,不仅能降低小鼠DNA的损伤水平,还能延缓衰老。
虽说超长端粒小鼠平均寿命相较于端粒正常的小鼠提升了12.75%,但研究表明,人类端粒的延长却可能增加致癌率。
超长端粒是否可以改变衰老相关的表征暂未可知,但NMN的抗衰老表现已经得到了验证,并且得到了大佬们的追捧,就连香港首富李嘉诚都投资了这一行业,前景可谓一片光明。
NMN凭什么能获得大佬们的青睐?NMN的中文名称是β-烟酰胺单核苷酸,参与人体上千种反应,可以逆转衰老,让50岁的身体指标回归到30岁状态。
NMN是NAD+的前体,它能在体内转换成NAD+,被坊间称为“长生不老药”。
端粒酶抑制剂
端粒酶抑制剂在肿瘤治疗中的最新研究进展摘要:端粒酶是一种特殊的逆转录酶,能以自身的 RNA为模板,反转录成端粒的重复单元TT AGGG加到人染色体末端,阻止端粒随细胞分裂而缩短,使细胞绕过衰老途径成为永生化细胞,导致人类肿瘤的发生。
以端粒酶为靶点,可以有多种治疗途径,本文主要介绍了端粒酶抑制剂的研究现状及新进展,重点对新型G ‐四联体稳定剂类端粒酶抑制剂、逆转录酶抑制剂及其他新型端粒酶抑制剂的研究进展进行介绍。
关键词:端粒酶抑制,G‐四联体,逆转录酶抑制剂,肿瘤,研究进展The newest research progress of the telomerase inhibitorsin cancer therapyKeywords:telomerase inhibitors,G-quadrplex DNA,Reverse transcriptase inhibitors,Tumor,research progress引言:端粒酶作为一种负责延长端粒的核蛋白逆转录酶,对于细胞染色体的稳定性和细胞活性的维持有重要作用,端粒酶的活性在正常组织中被抑制,而在恶性肿瘤细胞中其阳性率可达 84% ~95%,人体绝大部分恶性肿瘤的发生发展过程与端粒酶活性有非常紧密的联系,针对这一现象,并结合端粒酶本身的特点,人们开发出端粒酶抑制剂,应用不同端粒酶抑制剂针对端粒酶的不同组分及作用途径进行破坏或阻断,从而抑制端粒酶活性最终限制肿瘤的生长及发展,这是近年来国内外学者积极探索的一个方向。
1端粒与端粒酶概述端粒是位于真核细胞染色体末端的一种特殊结构,由DNA片段和蛋白组成,其主要功能是维护染色体的完整性,端粒长度随着有丝分裂逐渐缩短,当缩短至不能维护染色体稳定时,则导致细胞凋亡。
人端粒是染色体末端的一段富含GC 的重复序列,其生物学功能主要有:①保护染色体末端完整性;②参与染色体的定位和复制,保证细胞的正常分化与繁殖;③与细胞凋亡和永生化关系密切[1],在细胞分裂过程中,染色体末端逐渐缩短(图 1、2),当端粒缩短至l隔界值(4kb)以下时细胞趋向凋亡。
Trelagliptin_DPP-4抑制剂_865759-25-7_Apexbio

特别声明
产品仅用于研究, 不针对患者销售,望谅解。 每个产品具体的储存和使用信息显示在产品说明书中。ApexBio 产品在推荐的条件下是稳定 的。产品会根据不同的推荐温度进行运输。许多产品短期运输是稳定的,运输温度不同于长 期储存的温度。我们确保我们的产品是在保持试剂质量的条件下运输的。收到产品后,按照 产品说明书上的要求进行储存。
曲格列汀每周服用一次[1].已在日本开展临床试验,通过与已批准的药剂(即阿格列汀)比较来 检测曲格列汀的效果.结果表明,每周服用一次曲格列汀的功效和安全性与每日服用一次的阿 格列汀类似,这表明曲格列汀可能是一种有用的\每周服用一次的新抗糖尿病药物[2]. 在日本,曲格列汀(SYR-472)已用于治疗 2 型糖尿病患者的 2 期和 3 期临床试验中,结果表明其 效用和安全性与每日服用一次的阿格列汀类似,在临床上和统计学上均可显著改善血糖控制 且耐受性良好[2, 3]. 参考文献:
Store at -20°C
For obtaining a higher solubility , please warm the tube at 37°C and shake iock solution can be stored below -20°C for several months.
Evaluation sample solution : ship with blue ice All other available size: ship with RT , or blue ice upon request
生物活性
靶点 :
Proteases
信号通路:
DPP-4
产品描述:
曲格列汀(SYR-472)是一种选择性的 DPP-4 抑制剂,是用于治疗 2 型糖尿病(T2DM)的药剂[1]. 二肽基肽酶(DPP)-4,也称为腺苷脱氨酶络合蛋白 2 或 CD26,是在大多数细胞类型的表面表达 的一种抗原酶,其在调节免疫系统\信号转导和细胞凋亡方面发挥着重要作用[2, 3]. 曲格列汀(SYR-472)是一种强效的 DPP-4 抑制剂,与其他已批准药剂类型(每日服用一次)不同,
【高中生物】新药观察:潜在重磅抗体药物盘点
【高中生物】新药观察:潜在重磅抗体药物盘点单克隆抗体类药物以其治疗效果好、靶点明确、副作用小等优势受到医生和患者的青睐。
像修乐美、类克、美罗华等单抗类药物都在全球最畅销的药物排行榜前列,单抗类药物也是各制药公司研发的重点,我们就盘点一下处于临床研究阶段,即将上市的值得关注的抗体药物。
1、埃洛图珠单抗elotuzuma抗体是针对表面糖蛋白cs1的抗体,艾伯维与百时美施宝贵共同拥有它,此药用于治疗骨髓瘤。
早期试验显示将10mg/kg的elotuzumab和dexamethasone加入revlimid使病人的无进展生存期延长至33个月,有治疗效果的病人达到了92%,这个结果很令人印象深刻。
fda最近给了它突破性治疗的地位。
距离商业化还有一定的距离。
双剂量的类型没有显示出类似的效果。
坏消息是临床试验同时发现继发性癌症,和高达15%的终止率。
iii期临床试验现在被推迟到了2021年第一季度,但是它的毒性令人担忧,一个新的临床ii期安全性研究已经开展,试验结果将在2021年第四季度出来。
预计上市时间:2021年。
2、莫昔单抗阿斯利康的moxetumumab抗体是抗cd22抗体,阿斯利康宣称它比辉瑞的inotuzumab在多种不同的血液癌症中更有效,一个在毛细胞白血病的临床iii期研究正在进行中,将在2021年完成。
预计上市时间:2021年。
3、 med9-551阿斯利康的med9-551是一个糖基修饰的抗cd19单克隆抗体,正在研发用于治疗多种不同的b细胞淋巴瘤。
有两个对照美罗华的针对难治的慢性髓系淋巴瘤和弥散性大b细胞淋巴瘤临床ii期研究正在进行中,临床研究结果将于2021年出来。
有几个竞争性的产品抗cd19单克隆抗体正在研究中,包括安进,bristol,赛诺菲和seattlegenetics,我们也将拭目以待哪个疗效最好。
预计上市时间:2021年。
4、利利鲁单抗百时美施宝贵的抗kir单克隆抗体lirilumab还在继续招募急性髓系淋巴瘤(aml)病人,临床试验结果将在2021年得出,lirilumab是节点(checkpoint)抑制剂,阻止在癌细胞上白细胞抗原分子与病人自身癌细胞上的自然杀伤细胞互相作用。
端粒酶RNA特异性核酶抑制卵巢癌细胞端粒酶的活性

端粒酶RNA特异性核酶抑制卵巢癌细胞端粒酶的活性王红英;辛晓燕;马越云;苏明权【期刊名称】《第四军医大学学报》【年(卷),期】2002(023)014【摘要】目的研究端粒酶RNA特异性核酶对卵巢癌细胞活性的抑制作用. 方法用脂质体法将构建好的核酶逆转录病毒载体转染至卵巢癌HO-8910细胞,以MTT比色法检测细胞的生长,应用流式细胞仪分析细胞周期细胞,观察细胞的增殖情况,同时扩增端粒重复序列,结合杂交分析,检测细胞的端粒酶活性. 结果 MTT检测发现转染核酶后的细胞生长的潜伏期延长(48→72 h),对数生长期减缓(4→5 d),流式细胞仪结果显示其G1期比例明显增高(70.0%→80.5%, P<0.01),S期细胞比例明显降低(19.0%→13.7%, P<0.01),细胞增殖下降,细胞的端粒酶活性亦降低. 结论端粒酶RNA特异性核酶能抑制卵巢癌细胞端粒酶活性,抑制细胞增殖.【总页数】3页(P1274-1276)【作者】王红英;辛晓燕;马越云;苏明权【作者单位】第四军医大学西京医院妇产科,陕西,西安,710033;第四军医大学西京医院妇产科,陕西,西安,710033;第四军医大学西京医院临床分子生物学实验室,陕西,西安,710033;第四军医大学西京医院临床分子生物学实验室,陕西,西安,710033【正文语种】中文【中图分类】R737【相关文献】1.针对端粒酶的HDV核酶的设计及其对端粒酶活性抑制研究 [J], 吕盈盈;袁孟彪;靳大川;高艳景2.RNA干扰人端粒酶逆转录酶基因对膀胱尿路上皮癌BIU-87细胞株端粒酶活性抑制的研究 [J], 景抗震;高建平;程文;张征宇;葛京平3.人端粒酶逆转录酶核酶抑制端粒酶活性的实验研究 [J], 屈艺;刘菽秋;彭文珍;刘柏林4.人端粒酶逆转录酶核酶抑制端粒酶活性的实验研究 [J], 屈艺;刘菽秋;彭文珍;刘柏林5.端粒酶锤头状核酶抑制肺癌细胞端粒酶活性及细胞增殖的实验研究 [J], 何霞;周俊宜;朱振宇;黄小荣;谢金卫;王于;柏芸;米洋;陶莎因版权原因,仅展示原文概要,查看原文内容请购买。
BIBR 1532_端粒酶新型的选择性抑制剂_321674-73-1_Apexbio
化学性质
产品名: Cas No.: 分子量: 分子式:
BIBR 1532 321674-73-1 331.36 C21H17NO3
产品名: BIBR 1532 修订日期: 6/30/2016
化学名: SMILES: 溶解性: 储存条件: 一般建议:
运输条件:
2-[[(E)-3-naphthalen-2-ylbut-2-enoyl]amino]benzoic acid
ApexBio Technology
和三氧化二砷抑制细胞增殖能力和端粒酶活性[3]。
参考文献: [1]. Damm, K.; Hemmann, U.; Garin-Chesa, P.; Hauel, N.; Kauffman, I.; Priepke, H.; Niestroj, C.; Daiber, C.; Enenkel, B.; Guilliard, B.; Lauritsch, I.; Muller, E.; Pascolo, E.; Sauter, G.; Pantic, M.; Martens, U. M.; Wenz, C.; Linger, J.; Kraut, N.; Rettig, W. J.;Schnapp, A. A highly selective telomerase inhibitor limiting human cancer cell proliferation. EMBO J. 2001, 20, 69586968. [2]. Bashash D1, Ghaffari SH, Mirzaee R, Alimoghaddam K, Ghavamzadeh A. Telomerase inhibition by non-nucleosidic compound BIBR1532 causes rapid cell death in pre-B acute lymphoblastic leukemia cells. Leuk Lymphoma. 2013 Mar;54[4]:561-8. doi: 10.3109/10428194.2012.704034. Epub 2012 Sep 28. [3]. Bashash D1, Ghaffari SH, Zaker F, Kazerani M, Hezave K, Hassani S, Rostami M, Alimoghaddam K, Ghavamzadeh A. Anticancer Agents Med Chem. 2013 Sep;13(7):1115-25. BIBR 1532 increases arsenic trioxide-mediated apoptosis in acute promyelocytic leukemia cells: therapeutic potential fo应用
端粒酶抑制剂研究进展

端粒酶抑制剂研究进展作者:左利娟李洪雪来源:《中国实用医药》2010年第05期【摘要】端粒酶是一种特殊的逆转录酶,能以自身的RNA为模板,反转录成端粒的重复单元TTAGGG加到人染色体末端,阻止端粒随细胞分裂而缩短,使细胞绕过衰老途径成为永生化细胞,导致人类肿瘤的发生。
以端粒酶为靶点,可以有多种治疗途径,本文主要介绍了端粒酶抑制剂的研究现状及进展,重点对最新型的寡核苷酸类及G四联体稳定剂类端粒酶抑制剂进行介绍。
【关键词】端粒;端粒酶; G四联体;寡核苷酸近年来,端粒及端粒酶的研究已成为生物学热点,也是人类抗肿瘤药物研究的新“靶点”。
根据目前已经检测出的肿瘤组织标本的统计学分析,恶性肿瘤组织端粒酶活性的阳性率达到85%~95%,而良性肿瘤和正常组织的端粒酶活性检出率仅为4%左右[4]。
因此,端粒酶抑制剂的开发成为了抗肿瘤药物研究的又一热点。
1 端粒及其在DNA复制过程中的作用端粒(Telomere)是由位于真核细胞染色体末端的DNA及蛋白质构成的天然末端,是由富含鸟嘌呤(G)的核苷酸经5’3’方向串联组成。
不同物种端粒的重复序列和长度不一样,但每种生物体都有其特定的序列和平均长度。
人类端粒重复序列是5’TTAGGG3’,端粒长度在5~15Kb之间[5]。
端粒有维持染色体稳定和基因组完整的功能,防止染色体末端被化学修饰或被核酸降解、端端融合和重排,并参与染色体在核内的定位及基因表达调控[6]。
研究证明,端粒与细胞的寿命密切相关。
细胞分裂时,胚系细胞可以重建与延长端粒DNA,而体细胞则随着细胞的分裂,端粒不断缩短,缩短速度为50~200 bp/次分裂。
当其长度减小到一定的临界值时,细胞即趋向于衰老、死亡,因此,端粒被认为是绝大多数体细胞的“生物钟”[7]。
2 端粒酶及其与肿瘤发生的关系端粒酶(Telomerase)是位于细胞核内的一种逆转录酶[9],由人类端粒酶RNA(hTR)、端粒酶相关蛋白1(hTP1)和端粒酶逆转录酶(hTERT)三部分构成。
端粒酶逆转录酶的结构分析和抑制剂发现

端粒酶逆转录酶的结构分析和抑制剂发现端粒酶逆转录酶(Telomerase Reverse Transcriptase, TERT)是一种独特的酶,它包含有催化功能和RNA模板区两个重要部分。
它的生物学功能主要是维持染色体末端的长度稳定性,在几个生命过程中都有重要作用,比如在某些细胞里参与细胞的增殖和肿瘤的生长,还有可能延长人的寿命。
TERT在细胞核中形成凹槽型三级结构,由四个不同的区域组成:催化区(CAT)、RNA模板区(TR)、催化区与TR之间的连接区(CR4/5)和N端蛋白质结构域(N)。
结构域的存在是为了提供TERT活性所必须的配体分子,其中,TR和CAT区域是最重要的部分。
TR位于核酮糖绳中,它的核酮糖环是一个典型的3'-OH端,可以通过磷酸二酯键连接反式嘌呤。
磷酸二酯键被短端序列(named as P6 and P7)固定。
催化区由独特的P-loop、封锁序列和四个高度保守的胺基酸组成,它们在CAT功能中起了至关重要的作用。
由于TERT在肿瘤中具有非常重要的功能,因此TERT已成为肿瘤生物学研究的一个研究热点。
因为如果我们能够寻找到具有选择性抑制TERT功能的小分子抑制剂,那么就会对治疗癌症提供帮助。
近年来,科学家们在TERT的结构理解和抑制剂发现方面取得了重大进展。
例如,一项基于核磁共振分析的研究揭示了人类TERT的结构(TOT1),并提供了TERT催化凹槽中TMS结合位点的谷氨酸残基的详细结构。
另一个研究组,使用物理方法提取了TERT蛋白质中的CAT域,然后结合孪生法发现了TERT催化凹槽与TMS的非共价相互作用。
除此之外,近几年来还发现了许多TERT抑制剂。
例如,模拟TR的人工RNA寡核苷酸可以选择性地抑制催化功能;quindoline作为一种TR抑制剂和TERT的催化抑制剂,表现出良好的细胞外抑制活性;quinacrine被证明可以抑制TERT的催化活性,但对其他整合层次的端粒酶活性不产生影响; Celastrol也可以靶向TERT,在肿瘤的体内和体外模型中表现出较强的抗癌活性。
高血压病患者外周血单个核细胞端粒酶活性变化意义的探讨
高血压病患者外周血单个核细胞端粒酶活性变化意义的探讨谢长江;李昭骥【期刊名称】《广州医学院学报》【年(卷),期】2002(030)004【摘要】目的:探讨高血压患者外周血单个核细胞的端粒酶活性变化,并对其可能的机制进行探讨,以期进一步了解端粒酶在高血压发病中的作用.方法:对高血压病患者外周血单个核细胞进行提取,用PCR-ELISA测定端粒酶活性,与健康对照组进行比较,并对端粒酶活性的影响因素进行分析.通过对正常人外周血淋巴细胞在体外不同条件下培养,并检测其端粒酶活性,在体外探讨端粒酶上调的机制.结果:高血压病组外周血单个核细胞端粒酶阳性率为45%,对照组为18.5%,A值分别为0.39±0.32和0.17±0.15,二者差异有显著性.单因素分析表明,血压值、治疗与否、危险度分级等不是影响端粒酶的主要因素,而高血压的有无是影响端粒酶的主要因素.Logistic回归表明端粒酶活性与高血压病程负相关.细胞培养结果表明,PHA及CD3单抗可使培养细胞端粒酶活性上调,且与细胞计数正相关. 结论:(1)高血压病患者外周血单个核细胞端粒酶活性上调,高血压病的有无,是影响端粒酶活性的关键因素,端粒酶活性与高血压病程长短负相关;(2)淋巴细胞在体外可通过增殖(有丝分裂原刺激)及免疫活化途径使端粒酶活性激活.(3)端粒酶是理想的细胞增殖的分子水平标志.【总页数】5页(P25-29)【作者】谢长江;李昭骥【作者单位】广州医学院第二附属医院内科,广州,510260;广州医学院第二附属医院内科,广州,510260【正文语种】中文【中图分类】R544.1【相关文献】1.外周血单个核细胞端粒酶活性及IL-2、IL-12水平与老年性肺炎关系的研究 [J], 刘建;周朕;刘晓晴2.肝癌患者外周血单个核细胞端粒酶活性表达与临床相关性研究 [J], 战淑慧;李宁;宣世英;李清华3.老年肺炎患者外周血单个核细胞端粒酶活性与气道脱落细胞高尔基体应激水平的相关性 [J], 贾李侠;白翠林;纪玉强;张彦海4.高血压病患者外周血单个核细胞分泌白细胞介素1β水平的变化 [J], 李全忠;邓勤;阳跃忠;黄文新5.补肾调和肝脾法对慢性再生障碍性贫血患者外周血单个核细胞端粒酶活性的影响[J], 顾士稳;崔璨;王京华;杨桂茂;王树庆;王海霞因版权原因,仅展示原文概要,查看原文内容请购买。
端粒酶抑制剂对顺铂不同敏感性卵巢癌细胞株的影响
端粒酶抑制剂对顺铂不同敏感性卵巢癌细胞株的影响李雪梅;姚嘉斐【期刊名称】《实用妇产科杂志》【年(卷),期】2006(22)2【摘要】目的:通过检测顺铂(CDDP)敏感株和耐药株在经CDDP处理前后的端粒酶活性变化,了解端粒酶活性与CDDP耐药性的关系,及端粒酶抑制剂叠氮胸苷(AZT)和全反式维甲酸(ATRA)对CDDP不同敏感性的卵巢癌细胞株的影响,试图寻找一个解决常规化疗耐药问题的新方法.方法:将卵巢癌CDDP敏感株A2780和耐药株CAOV3、OVCAR3在不同浓度的CDDP、AZT和ATRA中培养,TRAP-ELISA法检测端粒酶活性,MTT法检测药物对细胞增殖的影响.结果:未加CDDP时,敏感株和耐药株的端粒酶活性没有明显差别,经CDDP处理后敏感株的端粒酶活性明显降低,而耐药株没有明显变化.端粒酶抑制剂对CDDP敏感株和耐药株的细胞增殖都有明显的抑制作用.结论:通过不同方式抑制端粒酶活性,均可抑制CDDP敏感株和耐药株的细胞增殖.端粒酶的活性与卵巢癌细胞株对CDDP的耐药性有关.【总页数】3页(P86-88)【作者】李雪梅;姚嘉斐【作者单位】辽宁省肿瘤医院,辽宁,沈阳,110043;杭州师范学院临床医学院,浙江,杭州,310018【正文语种】中文【中图分类】R737.31【相关文献】1.miR-199在对顺铂敏感性不同的卵巢癌细胞株中的表达及其意义 [J], 柳长青;徐汉杰;周颖;赵卫东2.苦参碱对上皮性卵巢癌细胞株顺铂敏感性的影响及其机制研究 [J], 张继荣3.Twist下调影响卵巢癌细胞株A2780顺铂敏感性的研究 [J], 马园园; 毛小梅; 乔谷媛; 吕小慧; 张晓红; 姚芳; 王建4.龙胆苦苷对人卵巢癌细胞株A2780/DDP顺铂化疗敏感性的影响及机制探讨 [J], 井晶;刘梦;郭静;田二斌5.ATM对卵巢癌细胞株CaOV3顺铂敏感性的影响 [J], 梁江红;罗蕊丽;刘永珍因版权原因,仅展示原文概要,查看原文内容请购买。
抗肿瘤药物端粒酶抑制剂的研究进展
抗肿瘤药物端粒酶抑制剂的研究进展
朱雍;陆涛
【期刊名称】《海峡药学》
【年(卷),期】2007(19)5
【摘要】端粒酶是维持端粒长度的逆转录酶,对细胞增殖、衰老及永生化和癌变起重要作用,在多数肿瘤中表达较高.端粒酶已成为肿瘤治疗的重要靶点.端粒酶抑制剂被认为是一类潜在的高选择性的抗癌药物,抑制剂的开发研究为恶性肿瘤的早期诊断和治疗开辟了新的途径.本文就端粒酶抑制剂与肿瘤治疗的研究进展作一综述.【总页数】4页(P4-7)
【作者】朱雍;陆涛
【作者单位】中国药科大学有机化学教研室,南京,210009;中国药科大学有机化学教研室,南京,210009
【正文语种】中文
【中图分类】R927.2
【相关文献】
1.端粒酶抑制剂的研究进展 [J], 彭帮国(综述);吴成秋(审校)
2.反义寡核苷酸和小分子干扰RNA作为端粒酶抑制剂的研究进展 [J], 陈金亮;胡英;高建青;梁文权
3.端粒酶抑制剂研究进展 [J], 左利娟;李洪雪
4.端粒酶和端粒酶抑制剂研究进展 [J], 葛晶
5.端粒酶抑制剂的研究进展 [J], 丁金丽;刘芳芳;于成国
因版权原因,仅展示原文概要,查看原文内容请购买。
Cell:破解端粒酶抗衰老之谜
Cell:破解端粒酶抗衰老之谜生物通报道,来自西班牙国立癌症研究中心分子癌症项目端粒与端粒酶研究小组,肿瘤抑制研究小组,巴伦西亚大学生理系,马德里Complutense大学动物医学与外科学院的科学家最近通过动物模型实验破解了端粒酶抗衰老的机制,相关的成果发布在11月14日的Cell期刊上。
端粒酶,是基本的核蛋白逆转录酶,可将端粒DNA加至真核细胞染色体末端。
端粒在不同物种细胞中对于保持染色体稳定性和细胞活性有重要作用,端粒酶能延长缩短的端粒(缩短的端粒其细胞复制能力受限),从而增强体外细胞的增殖能力。
因此,科学家把端粒酶也称为抗衰老的酶。
但是,端粒酶抗衰老的机制却一直是个谜,今天西班牙的科学家将拨开重重迷雾,找出端粒酶抗衰老的神奇机制。
免费索取:MMI单细胞获取自动化工作站技术资料为了研究端粒酶的抗衰老功能,研究小组表达了端粒酶的其中一种成分,端粒酶逆转录酶(telomerase reverse transcription,TERT),并将这种基因引入对癌症有耐受力(在小鼠体内高度表达抗癌基因p53,p16和19ARF)的小鼠体内。
结果发现,大量表达TERT有助提高上皮细胞的活力,尤其是皮肤细胞和肠细胞,与一般的小鼠相比,可全面地研究小鼠的寿命,延缓小鼠的衰老过程。
这些结果表明,大量表达TERT是提升生命机体抗衰老能力的关键。
您可能感兴趣的生物通精选文章:·Cell综述:寻找抗衰老的秘方(06-24)·上海生科院等揭示端粒酶蛋白亚基与RNA亚基的相互作用(05-22)·华人科学家Nature发布首张完整端粒酶图谱(04-16)·中山大学千人教授PNAS端粒酶研究新进展(03-20) ·Nature子刊聚焦端粒酶、炎症与癌症(11-23)原文摘要:Telomerase Reverse Transcriptase Delays Aging in Cancer-Resistant Mice【Summary】Telomerase confers limitless proliferative potential to most human cells through its ability to elongate telomeres, the natural ends of chromosomes, which otherwise would undergo progressive attrition and eventually compromise cell viability. However, the role of telomerase in organismalaging has remained unaddressed, in part because of the cancer-promoting activity of telomerase. To circumvent this problem, we have constitutively expressed telomerase reverse transcriptase (TERT), one of the components of telomerase, in mice engineered to be cancer resistant by means of enhanced expression of the tumor suppressors p53, p16, and p19ARF. In this context, TERT overexpression improves the fitness of epithelial barriers, particularly the skin and the intestine, and produces a systemic delay in aging accompanied by extension of the median life span. These results demonstrate that constitutive expression of Tert provides antiaging activity in the context of a mammalian organism.生物通张欢全基因组芯片技术突破基础研究和医学难题最新文献下载>> >>PALL鼓励中国科研工作者SCI文章发表活动30000奖金等着您!基因科技文献奖励活动火热进行中!在SCI收录期刊上发表文献采用了相关试剂盒,均有机会活动高达上千元的奖励!。
端粒、端粒酶及hTERT基因研究在乳腺癌基因治疗中进展
端粒、端粒酶及hTERT基因研究在乳腺癌基因治疗中进展王世清(综述);崔明(审校)【期刊名称】《西南国防医药》【年(卷),期】2014(000)005【摘要】端粒酶通过维持端粒的长度使细胞永生化,为抗衰老提供了光明前景,也为乳腺肿瘤治疗提供了新的希望。
乳腺肿瘤在治疗上一般首选手术治疗,术后再辅以放疗、化疗。
但是这种传统治疗创伤大,对肿瘤的敏感性差,副作用多。
而对端粒酶的研究,为乳腺癌基因治疗打开了一扇新的大门。
乳腺癌是全球妇女最常见的恶性肿瘤,也是女性恶性肿瘤发病率较高的一种疾病,尤其是在经济发展中国家,自2008年以来,全世界有1 383 500例新增乳腺癌患者,死亡458 400例。
现在端粒酶在肿瘤监测中的作用及研发端粒酶抑制州作为治疗乳腺肿瘤的创新药物,已成为近年医学研究的热点。
本研究通过查阅相关文献,对端粒、端粒酶研究及应用进展做一综述。
【总页数】2页(P573-574)【作者】王世清(综述);崔明(审校)【作者单位】650032 昆明,成都军区昆明总医院普通外科;650032 昆明,成都军区昆明总医院普通外科【正文语种】中文【中图分类】R737.9【相关文献】1.端粒逆转酶(hTERT)及端粒酶在膀胱癌诊治中的进展 [J], 马鹏程;邓建华2.人端粒酶逆转录酶(hTERT)特异性siRNA对乳腺癌细胞hTERT水平及细胞生长影响的研究 [J], 贲勇;杨冬;高磊;白春学3.人端粒酶逆转录酶(hTERT)启动子在肿瘤基因治疗中的应用 [J], 王峰;刁勇;许瑞安4.端粒酶及hTERT基因研究进展 [J], 朱舜丽;林邦和5.端粒酶研究在实体瘤诊治中的应用 : 针对端粒酶进行肿瘤基因治疗可能会引起肿瘤基因治疗的一场革命 [J], 李德志;陈正堂因版权原因,仅展示原文概要,查看原文内容请购买。
人端粒酶反转录酶转染的骨髓间充质干细胞移植治疗大鼠糖尿病

人端粒酶反转录酶转染的骨髓间充质干细胞移植治疗大鼠糖尿病赵海莲【期刊名称】《中国组织工程研究》【年(卷),期】2015(000)006【摘要】BACKGROUND:Human telomerase reverse transcriptase (hTERT) is the first choice for regulating the proliferation and directional differentiation, with multiple biological effects. OBJECTIVE:To observe the therapeutic effect of hTERT-transfected bone marrow mesenchymal stem cels transplantation in diabetic rats. METHODS: Bone marrow mesenchymal stem cels from Sprague-Dawley rats were culturedin vitro and transfected with retrovirus PLXSN carrying hTERT. RT-PCR was used to detect the hTERT expression in the bone marrow mesenchymal stem cels before and after transfection. Sixty male Sprague-Dawley rats were selected and equaly randomized into four groups: normal control group, transfection group, cel transplantation group, and model group. In the latter three groups, rats were injected with 45 mg/kg chain urea to establish diabetes models, and then injectedvia the tail vein with 0.2 mL hTERT-transfected bone marrow mesenchymal stem cels, 0.2 mL bone marrow mesenchymal stem cels, and 0.2 mL normal saline, respectively. RESULTS AND CONCLUSION:At 48 hours after hTERT transfection, the expression of hTERT mRNA was detected in the bone marrowmesenchymal stem cels, and mainly concentrated in the nuclei. At 14 days after transfection, the fasting glucose level in the model group was higher than that in the normal control group (P < 0.05). However, compared with the model group, the fasting glucose levels in the transfection and cel transplantation groups were significantly decreased (P < 0.05); compared with the cel transplantation group, the fasting glucose level in the transfection group was also significantly decreased (P < 0.05), which was similar to that in the normal control group (P > 0.05). These findings indicate that the transplantation of hTERT-transfected bone marrow mesenchymal stem cels is effective in the treatment of diabetic rats.%背景:人端粒酶反转录酶是调控增殖及定向分化的首选生长因子之一,具有多重生物学效应。
端粒酶抑制剂联合放射治疗对小鼠乳腺癌作用的实验研究

端粒酶抑制剂联合放射治疗对小鼠乳腺癌作用的实验研究阮晓峰;周云峰【期刊名称】《癌症(英文版)》【年(卷),期】2001(020)003【摘要】目的:探讨端粒酶抑制剂对动物在体肿瘤的治疗价值及端粒酶抑制剂是否增加放射治疗的疗效。
方法:采用正交实验设计,应用端粒酶抑制剂[齐多夫啶(azidothymidine,AZT):300mg·kg-1·d-1;拉米夫啶(lamivudine):150mg·kg-1·d-1]联合放射(每周照射5次,每次DT2Gy,总量10Gy/周)治疗BALB/c小鼠移植性乳腺癌(MA782),观察其对肿瘤体积缩小和肿瘤内端粒酶表达的影响。
肿瘤体积用游标电子数显卡尺测量计算,并采用PCRELISA方法检测端粒酶活性。
结果:本研究结果表明,未治疗、单用lamivudine治疗的小鼠肿瘤体积分别增大2.7268、2.5130倍,表明单纯使用lamivudine作用不明显(P>0.05);而经AZT、放疗、AZT加放疗治疗的小鼠肿瘤体积分别缩小20.72%、47.43%、85.19%,提示AZT、放疗均能使肿瘤体积缩小(P<0.05),并且AZT与放疗的联合作用明显优于两者的单独作用(P<0.05)。
而肿瘤端粒酶活性检测表明,未处理,以及经AZT、lamivudine、放疗、AZT加放疗、AZT加lamivudine加放疗处理的肿瘤端粒酶A值分别为0.817、0.453、0.760、0.480、0.340、0.166,显示AZT、放疗、lamivudine均有减少肿瘤端粒酶活性的作用(P<0.05),且AZT与放疗有相加作用(P<0.05)。
结论:AZT、放疗均能降低小鼠乳腺癌MA782的端粒酶活性和缩小肿瘤体积,AZT能增加肿瘤的放射敏感性。
端粒酶是癌症治疗的一个较好的新靶点。
%Objective:This study was designed to evaluate the treatment value of telomerase inhibitors for animal tumor in vivo andinvestigate radiosensitive effects of telomerase inhibitors. Methods:With orthogonal experiment design, the telomerase inhibitors(azidothymidine AZT 300 mg· kg -1· d -1, lamivudine 150 mg· kg-1· d -1)and radiotherapy (RT, 10 gray in a week, 2 gray/Fx, 5 Fx/wk) were used to treat breast cancers (MA782)xenograft in BALB/c mice for evaluating their influence on tumor size and telomerase expression. The tumor size was measured witha digital vernier scale. Telomerase activity was examined by a PCR-based telomeric repeat amplification protocol (TRAP) coupled with ELISA. Results:The tumor size of mice increased 2.7268 times in untreated and 2.5130 times in lamivudine-administrated, which indicated lamivudine having no obvious effect on tumor volume (P >0.05); AZT, RT, and AZT combined with RT reduced tumor volume of 20.70% , 47.43% , and 85.19% , respectively, and combined model(AZT+ RT) was more effective than others used alone(P<0.05); The A value of tumor telomerase was untreated,0.817; AZT,0.453; lamivudine,0.760; RT,0.480; AZT 0.340 combined with RT; and AZT plus lamivudine plus RT,0.166 ; which suggested that AZT, RT and lamivudine could decrease the activity of tumor telomerase (P<0.05), and furthermore, AZT combined with RT have an additive effect (P< 0.05). Conclusion: Both AZT and radiotherapy are effective to treat murine breast cancer through decreasing telomerase activity and reducing tumor size. AZT can increase the radiation sensitivity for murine breast cancer MA782. Telomerase is a new target for anticancer treatment.【总页数】6页(P249-254)【作者】阮晓峰;周云峰【作者单位】湖北医科大学附属第二临床学院放化疗科,;湖北医科大学附属第二临床学院放化疗科,【正文语种】中文【中图分类】R730.55因版权原因,仅展示原文概要,查看原文内容请购买。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Soluble in DMSO
Store at -20°C
For obtaining a higher solubility , please warm the tube at 37°C and shake it in the ultrasonic bath for a while.Stock solution can be stored below -20°C for several months.
ApexBio Technology
产品说明书
化学性质
产品名: RHPS4 修订日期: 6/30/2016
产品名: Cas No.: 分子量: 分子式: 化学名:
SMILES:
溶解性: 储存条件: 一般建议:
运输条件:
RHPS4
390362-78-4
458.48
C23H20F2N2O4S
3,11-difluoro-6,8,quinolino[4,3,2-kl]acridin-13-ium methyl sulfate
Evaluation sample solution : ship with blue ice All other available size: ship with RT , or blue ice upon request
生物活性
靶点 :
DNA Damage/DNA Repair
信号通路:
Telomerase
特别声明
产品仅用于研究,
不针对患者销售,望谅解。
每个产品具体的储存和使用信息显示在产品说明书中。ApexBio 产品在推荐的条件下是稳定 的。产品会根据不同的推荐温度进行运输。许多产品短期运输是稳定的,运输温度不同于长 期储存的温度。我们确保我们的产品是在保持试剂质量的条件下运输的。收到产品后,按照 产品说明书上的要求进行储存。
参考文献: [1] Phatak P,Cookson JC,Dai F,Smith V,Gartenhaus RB,Stevens MF,Burger AM. Telomere uncapping by the G-quadruplex ligand RHPS4 inhibits clonogenic tumour cell growth in vitro and in vivo consistent with a cancer stem cell targeting mechanism. Br J Cancer.2007 Apr 23;96(8):1223-33.
产品描述:
在 5 天生长抑制测定中,作用于 M14 细胞,IC50 约为 3 μM。 RHPS4 是一种端粒酶抑制剂。 端粒调节染色体末端的保护、降解和重组。近期一项模型提出端粒可以在染色体末端形成帽。 因此,端粒帽完整性应该是完整的,以允许细胞分裂进行。 体外:研究发现,RHPS4 处理 UXF1138L 细胞导致端粒酶催化亚基(hTERT)从细胞核置换、
端粒启动的 DNA 损伤信号传导以及染色体融合的诱导。进一步报道,RHPS4 对作为集落生 长的癌细胞比作为单层生长的细胞更有效。此外,人脐带血和 HEK293T 胚胎肾细胞集落形 成单位对 RHPS4 更耐受[1]。 体内:动物研究发现,与对照相比,RHPS4 处理 UXF1138L 异种移植物可降低克隆形成,使 核 hTERT 表达丧失,并诱导有丝分裂异常。虽然 RHPS4 单独用药表现出有限的体内功效, 与有丝分裂纺锤体毒物 Taxol 的联合用药治疗导致肿瘤缓解和端粒功能障碍的进一步增强 [1]。 临床试验:到目前为止,RHPS4 仍处于临床前研究阶段。