2011 NCCN Myeloid Growth Factors
结肠癌NCCN解读ppt课件

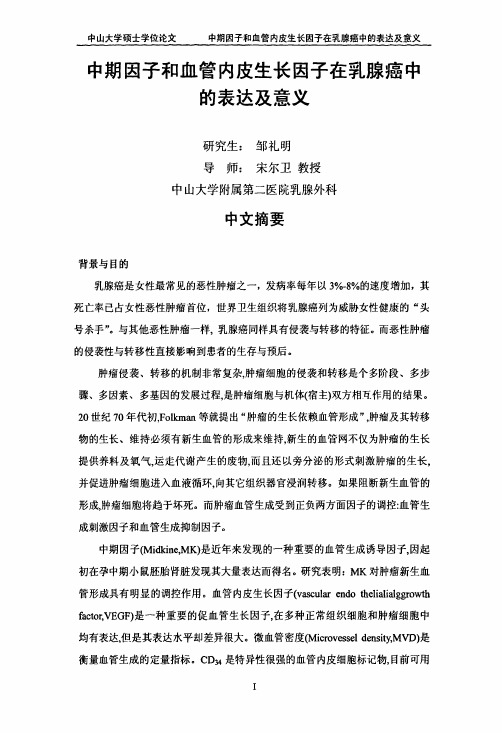
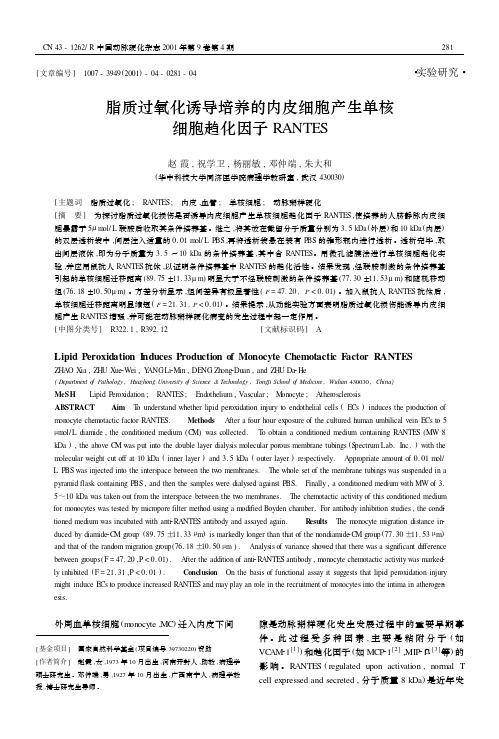
0.2 HR (95% CI): 0.82 (0.60–1.13) Stage II
0.1
0.75 (0.62–0.89) Stage III
0.0 0 6 12 18 24 30 36 42 48 54 60 66
月
de Gramont et al. ASCO 2005;Abstract 3501
大肠癌NCCN指南解读
复旦大学肿瘤医院 肿瘤内科 李 进
2011年我们关注什么?
1. 辅助治疗有没有新方案 2. 如何制定个体化的化疗方案 3. 如何提高患者生存质量 4. 如何延长复发患者生存
辅助治疗的进展
无淋巴结转移的患者需要辅助化疗吗?
QUASAR: 总生存 (II期)
生存率
100 90 80 70 60 50 40 30 20 10 0 0
IIIA
IIIB
IIIC
(T1–2N1) (T3–4N1) (TanyN2)
(M1)
O’Connell et al., 2004.
高危的II期病人指至少含以下一项
– T4 – 肠梗阻 – 肿瘤穿孔 – 低分化肿瘤 – 脉管侵犯 • 送检淋巴结<10个
遗憾的是我 们到现在尚 未找到直接 的与预后有 关的生物标 记物。
如何克服5-Fu的骨髓毒性?
NO16968: 试验设计
III期结肠癌 术后≤8 周
N=1886
n=944
随 机 化
n=942
• 主要终点: DFS • 次要终点: RFS, OS, 耐受性
XELOX (6 months)
卡培他滨 1000 mg/m2 bid d1–14 奥沙利铂130 mg/m2 d1 q3w 8 个周期
中期因子及血管内皮生长因子在乳腺癌中的表达及意义
中期因子和血管内皮生长因子在乳腺癌中的表达及意义
中期因子和血管内皮生长因子在乳腺癌中 的表达及意义
研究生:
导师:
邹礼明 宋尔卫教授
中山大学附属第二医院乳腺外科
中文摘要
背景与目的 乳腺癌是女性最常见的恶性肿瘤之一,发病率每年以3%.8%的速度增加,其 死亡率已占女性恶性肿瘤首位,世界卫生组织将乳腺癌列为威胁女性健康的“头 号杀手”。与其他恶性肿瘤一样,乳腺癌同样具有侵袭与转移的特征。而恶性肿瘤 的侵袭性与转移性直接影响到患者的生存与预后。 肿瘤侵袭、转移的机制非常复杂,肿瘤细胞的侵袭和转移是个多阶段、多步 骤、多因素、多基因的发展过程,是肿瘤细胞与机体(宿主)双方相互作用的结果。 20世纪70年代初,Foll(Inml等就提出“肿瘤的生长依赖血管形成”,肿瘤及其转移 物的生长、维持必须有新生血管的形成来维持,新生的血管网不仅为肿瘤的生长 提供养料及氧气,运走代谢产生的废物,而且还以旁分泌的形式刺激肿瘤的生长, 并促进肿瘤细胞进入血液循环,向其它组织器官浸润转移。如果阻断新生血管的 形成,肿瘤细胞将趋于坏死。而肿瘤血管生成受到正负两方面因子的调控:血管生
(F=lO.217 p---0.026)。
(4)MK、VEGF的表达的相关性分析 66例乳腺癌组织中MK VEGF表达共阳性者37例,MK和VEGF表达共阴 性者10例,MK表达阳性而VEGF表达阴性者“例,MK表达阴性而VEGF表
达阳性者8例,表达~致率为71.21%(47/66),Spearman等级相关分析表明二
peroxidase
method)检测MK、VEGF、CD34
在乳腺癌、癌旁正常乳腺及良性乳腺肿瘤组织中的表达情况并计数MVD。 ER、PR为乳腺癌术后常规检查项目。
结直肠癌患者血清中血管内皮生长因子和一氧化氮表达水平及其临床意义
结直肠癌患者血清中血管内皮生长因子和一氧化氮表达水平及其临床意义武汉市普爱医院姜齐宏方向明*陈艳,武汉430033摘要目的:探讨结直肠癌患者血清中血管内皮生长因子(VEGF)和一氧化氮(NO)表达水平及其临床意义。
方法:分别采用酶联免疫吸附测定(ELISA)法和分光光度法检测74例结直肠癌患者术前和45例结直肠腺瘤患者以及40例健康人血清中VEGF和NO的含量。
结果:结直肠腺瘤患者血清VEGF和NO含量与健康人无明显差异(P>0.05);结直肠癌患者血清VEGF和NO表达水平分别较结直肠腺瘤组以及健康人明显增高(P<0.01),且结直肠癌浸润深度、有无淋巴结转移以及Dukes分期与血清VEGF和NO含量呈明显正相关(r=0.834,P<0.01)。
结论:VEGF和NO与结直肠癌的发生发展密切相关,术前检测血清VEGF和NO含量可作为判断结直肠癌浸润转移以及Dukes分期的有效生物学指标。
关键词结直肠癌血管内皮生长因子一氧化氮中图分类号R735.3文献标识码AExpressions of serum vascular endothelial growth factor and nitric oxide in patients with colorectal cancer and their clinical significance JIANG Qi-hong,FANG Xiangming,CHEN Yan.Wuhan Puai Hospital,Wuhan430030,China Abstract Objective:To investigate the expressions of serum vascular endothelial growth factor(VEGF)and nitric ox-ide(NO)in patients with colorectal cancer and their clinical significance.Methods:Serum levels of VEGF and NO were measured by enzyme-linked immunosorbent assay(ELISA)and spectrophotometry in74patients with colorectal cancer and 45patients with colorectal adenomas as well as40healthy individuals.Results:There were no significant difference in serum levels of VEGF and NO between patients with colorectal adenomas and healthy subjects(P>0.05).Serum levels of VEGF and NO were significantly higher in patients with colorectal cancers than those with colorectal adenomas and healthy subjects (P<0.01).There was a positive correlation between serum levels of VEGF,NO and depth of tumor invasion,lymph node metastasis and Dukes stage(r=0.834,P<0.01).Conclusions:Serum levels of VEGF and NO are related to the growth,development and metastasis of colorectal cancer.Serum levels of VEGF and NO may be sensitive predictors of invasion,me-tastasis and Dukes stage before surgery in patients with colorectal cancer.Key words Colorectal cancer Vascular endothelial growth factor Nitric oxide血管内皮生长因子(vascular endothelial growth factor,VEGF)在肿瘤新生血管形成以及肿瘤的生长、转移中起重要作用[1,2]。
聚乙二醇化重组人粒细胞刺激因子与重组人粒细胞刺激因子临床疗效比较

聚乙二醇化重组人粒细胞刺激因子与重组人粒细胞刺激因子临床疗效比较目的:比较乳腺癌TAC方案化疗后,应用聚乙二醇化重组人粒细胞刺激因子和人粒细胞刺激因子预防粒细胞减少的临床疗效。
方法:选取2013年1-8月入院接受TAC方案化疗的乳腺癌患者共60例。
30例为试验组,化疗结束后48 h 给予聚乙二醇化重组人粒细胞刺激因子(PEG-rhG-CSF);30例为对照组,化疗结束后48 h给予重组人粒细胞刺激因子(rhG-CSF)。
结果:试验组化疗间歇期中性粒细胞减少、感染病例明显少于对照组,差异有统计学意义(P<0.05)。
结论:乳腺癌TAC方案化疗后应用聚乙二醇化重组人粒细胞刺激因子预防中性粒细胞减少疗效确切,值得临床推广应用。
标签:乳腺癌;聚乙二醇化重组人粒细胞刺激因子;粒细胞减少近年来乳腺癌发病率急速上升,已成为威胁女性身心健康的恶性肿瘤之首[1]。
乳腺癌重要治疗手段之一是全身化疗,TAC方案作为乳腺癌的一线化疗,已得到临床医师的广泛认可[2]。
该化疗方案作为治疗乳腺癌的强效治疗方案,在提高乳腺癌的无病生存率(DFS)及总生存率(OS)的同时,也带来众多毒副反应,如中性粒细胞减少、粒细胞减少引起的发热、感染等[3],这不仅给患者身体造成一定伤害,还可能会延迟治疗时间,影响疗效,甚至威胁生命。
重组人粒细胞集落刺激因子(rhG-CSF)是防治肿瘤化放疗引起的中性粒细胞减少症的有效药物,但半衰期短,需每日给药。
聚乙二醇化重组人粒细胞集落刺激因子(PEG-rhG-CSF)是将聚乙二醇与rhG-CSF结合而成的长效制剂,与常规rhG-CSF 相比,能减少给药次数,避免患者反复接受注射的痛苦[4]。
笔者现将接受TAC 方案化疗的乳腺癌患者随机分为两组,分别给予PEG-rhG-CSF与rhG-CSF,对比两组疗效及毒付反应,总结如下。
1 资料与方法1.1 一般资料选取2013年1-8月本中心接受TAC方案至少2个标准疗程化疗的60例乳腺癌患者。
一例使用重组人粒细胞刺激因子治疗白细胞减少的病例分析
一例使用重组人粒细胞刺激因子治疗白细胞减少的病例分析1.病例介绍:1.1病史资料石长河,女,74岁,住院号:973937,身高:167cm,体重:60kg,体表面积:1.63m2,患者2017年5月10日因腹痛就诊于当地医院,行急诊阑尾手术治疗,剖腹后查见阑尾无异常,升结肠占位性病变。
行胸腹部增强CT提示结肠肝曲附近升结肠肠壁似有增厚,局部管腔狭窄:占位性病变可疑?升结肠及相邻小肠不全性肠梗阻。
术前检查CEA:22.8ng/ml↑,CA19-9:52.92ng/ml↑,于5月11日全麻下行剖腹探查术,术后病理结果:升结肠中分化腺癌侵及浆膜层,两切缘未见癌组织累及,见脉管内癌栓,未见明确神经侵犯,肠壁局部淋巴结见癌组织转移(6/11),阑尾组织显慢性炎,临床分期ⅢC期(T4aN2bM0)。
术后2周复查CEA、CA19-9降至正常水平。
术后予以CapeOX方案(奥沙利铂200mg d1+卡培他滨片1500mg 2/日d1-14,每21天一周期)化疗,化疗期间副反应轻,化疗前三次复查CEA、CA19-9均在正常范围内,第四次化疗前复查CEA:5.1ng/ml↑,CA19-9:43.11ng/ml↑,完善胸腹部增强CT未见复发转移证据,继续原方案第五次化疗。
患者于2017-10-20入我科,第六次化疗前复查CEA:6.59ng/ml↑,CA19-9:53.6ng/ml↑,予完善全ras检测,并于10-23继续原方案化疗1周期。
鉴于CEA、CA19-9持续增高,建议其行贝伐珠单抗注射液加化疗,但患者拒绝使用贝伐珠单抗注射液,遂调整化疗方案为“奥沙利铂甘露醇注射液 200ml d1+替吉奥胶囊 50mg bid po d1-14”。
患者目前精神尚可,体力正常,食欲正常,睡眠正常,体重无明显变化,大便正常,排尿正常,为进一步检查及治疗入院。
1.2入院诊断:结肠癌化疗后ⅢC期(T4aN2bM0,K-ras检查突变型,MSS)、2型糖尿病1.3治疗过程:患者74岁老年男性,ECOG评分1分,疼痛评分1分,营养评分1分,结肠癌ⅢC期诊断明确,已行根治性手术。
慢性肾衰竭血清瘦素、胰岛素样生长因子—1水平及意义

慢性肾衰竭血清瘦素、胰岛素样生长因子—1水平及意义瘦素(Leptin)是近几年来发现的一种由脂肪细胞产生的蛋白,它对调节机体食欲、体重和器官的能量消耗有重要作用。
肾脏是瘦素清除的主要器官,同时瘦素又可对肾脏直接发挥作用。
瘦素是慢性肾功能不全(CRF)时体内聚积的毒素之一,它与胰岛素样生长因子-1(IGF-1)共同作用于慢性肾功能衰竭患者的营养状况。
本文主要探讨慢性肾功能衰竭(CRF)血清瘦素和IGF-1的水平及意义。
一瘦素研究概况1994年hzang等首次鉴定并克隆出了人的肥胖基因,其与小鼠具有高度同源性,同时发现该基因编码的一种含167个酸的蛋白,分子量为16KD,为ob基因的表达产物,被命名为瘦(Leptin)[1]。
瘦素的生理功能包括:感受机营养状态[2],进而抑制食物摄入:刺激或维持能量消耗;影响生殖泌系统;作为一种代谢激素促进一系列代谢过程,如胰岛素释放、糖的解作用、转运等。
瘦素缺乏或瘦素受体缺陷可导胖和垂体功能异常。
二 RCF患者血浆瘦素的变化及影响因素近期的研究认为肾功能衰竭患者同肥胖患者一样,血浆瘦素水平常明显高于正常。
由于瘦素分子量是16KD,可能通过肾小球滤过,假设人的瘦素清肾脏,那么有人做了这方面的研究,KumarS等测定了不同程度能损伤患者的主动脉和肾静脉血浆瘦素水平,发现瘦素的清除在与肾功能有关,同时连续测量通过肾脏的不同浓度和肾血流比率,计算出肾脏瘦素的净排出率为480ng/min,同时也发现在中度肾损伤患者肾脏没有瘦素清除[3],另外监测到尿的瘦素水平低也表明在肾脏降解。
人体处于炎症状态时常常会表现食欲下降,有人用CRP(反应蛋白)增高代表机体存在炎症,研究发现尿毒症患者CRP瘦素确有相关关系,CRP高的患者往往血浆瘦素水平也高。
同时调查蛋白质摄入情况发现,CRP高的患者蛋白质摄入明显低于CRP正常患者。
提示炎症所致的食欲下降与它引起的瘦素增高有关[4]。
三瘦素水平相对增高对CRF病人的影响瘦素对慢性肾衰患者的不利影响可能不止是对机体营养状态的,瘦素增高交感神经兴奋性可能参与了慢性肾衰患者的血压异常,并且因为瘦素无法有效清除而致血压难以控制;慢性肾衰患者高瘦素血症与高胰岛素血症可能互为因果,互相促进;可能导致高脂血症。
拟黑多刺蚁肌细胞增强因子2_MEF2_生物信息学分析解读

拟黑多刺蚁肌细胞增强因子2 WORD文档使用说明:拟黑多刺蚁肌细胞增强因子2 来源于本WOED文件是采用在线转换功能下载而来,因此在排版和显示效果方面可能不能满足您的应用需求。
如果需要查看原版WOED文件,请访问这里拟黑多刺蚁肌细胞增强因子2 文件原版地址:/d1dd5df7170b1a40fffdaf26.pdf拟黑多刺蚁肌细胞增强因子2|PDF转换成WROD_PDF阅读器下载昆虫知识 Chinese Bulletin of Entomology2010, 47(5):881 ~ 885拟黑多刺蚁肌细胞增强因子 2 ( MEF2)生物信息学分析 * 郭新军(1. 陕西师范大学生命科学学院西安 1, 2奚耕思1? ? 西安 710065 )710062 ; 2. 西安文理学院生命科学系2 ? Bioinformatics analysis of MEF2 gene of Polyrhachis vicina. GUO Xin-Jun 1 ,, Geng-Si1 ?( 1. College of XILife Science, Shaanxi Nomal University,Xi ’an an University of Arts and Science,Xi’ Abstract710062, China; 2. Department of Life Science,Xi ’an710065,China)The analytical tools NCBI,ExPASy and CBS wereadopted to analyze the bioinformatic properties ofthe PvMEF2 protein,such as sequence characteristics,physicochemical properties,structure and functional domains. The results show that PvMEF2 has conserved MADS and MEF2 domains and that its physicochemical properties, secondary and tertiary structures are similar to those of the MEF2 protein of Drosophila melanogaster. PvMEF2 protein may play an importantrole in myogenesis in Polyrhachis vicina Roger. Key words Polyrhachis vicina, myocyte enhancer factor 2 ( MEF2), bioinformatics analysis摘要ExPASy 在线核苷酸序列分析工具、 CBS 生物学序列分析工具及应用 NCBI 上的常用程序、SABLE 在线分析软件等对拟黑多刺蚁 Polyrhachis vicina Roger 肌细胞增强因子 2 ( PvMEF2 )进行了生物信息学分析,获得了 PvMEF2 因子的序列特征及理化性质,并对其结构和功能结构域进行了预测。
胰岛素样生长因子-1在稳定动脉粥样硬化斑块中的作用
・综述・ 胰岛素样生长因子-1在稳定动脉粥样硬化斑块中的作用李飞虹1尚茹茹2张锦2吕淑萍1王兴兴2文仙仙2刘晓红2【摘要】 心脑血管疾病已成为中国居民第一位死亡原因,冠心病的死亡率明显上升。
动脉粥样硬化斑块是动脉粥样硬化的重要病理过程,不稳定斑块的形成,突发的斑块破裂,大量的血栓形成,出现急性血栓事件,即急性冠状动脉综合征。
研究发现胰岛素样生长因子-1有稳定斑块的作用,因此可能成为防治急性心血管事件新的干预靶点。
本文就胰岛素样生长因子-1在稳定斑块中的作用进行阐述。
【关键词】 动脉粥样硬化;胰岛素样生长因子1;肌细胞,平滑肌;泡沫细胞;巨噬细胞Role of insulin like growth factor 1 in preventing atherosclerotic plague vulnerability Li Feihong1,Shang Ruru2, Zhang Jin2, Lyu Shuping1,Wang Xingxing2, Wen Xianxian2, Liu Xiaohong2. 1Shanxi MedicalUniversity, Taiyuan 030000, China; 2Department of Special Ward, Shanxi Provincial People's Hospital,Taiyuan 030000, ChinaCorresponding author: Liu Xiaohong, Email: docliuxh@【Abstract】Cardiovascular and cerebrovascular disease has become the first cause of human deathin China, the mortality of coronary heart disease increases obviously. Atherosclerotic plaque is an importantpathological process of atherosclerosis. The formation of unstable plaque, sudden plaque rupture andthrombosis, eventually cause acute thrombotic events-acute coronary syndrome. Research found thatinsulin like growth factor-1 has the characteristic of stabilizing plaque, which may become a new target forthe prevention and treatment of acute cardiovascular events. This review focused on the effect of insulinlike growth factor 1 on plague stability.【Key words】 Atherosclerosis; Insulin like growth factor 1; Myocytes, smooth muscle; Foamcells; Macrophages动脉粥样硬化是一个慢性炎症过程,是冠心病的主要病理基础。
中国药物经济学评价指南(2011版)

中国药物经济学评判指南(2011版)药物经济学评判是一项重要的探究领域,旨在为决策者提供有关药物疗效和成本效益的信息,以指导药物的使用和支付策略。
是中国卫生部和全国药品经济学探究中心联合制定的一个重要参考文件,目标是规范和增进药物经济学评判的探究和应用。
该指南起首介绍了药物经济学评判的背景和意义。
随着医疗费用的不息增加和药品种类的扩展,药物经济学评判的重要性日益凸显。
评判药物的疗效和成本效益可以援助决策者选择最具价值的药物,提高医疗资源的利用效率。
指南接着详尽介绍了药物经济学的基本观点和评判指标。
通过诸如成本-效果分析、成本-效用分析和成本-效益分析等方法,可以综合思量药物治疗的效果、患者的生命质量和医疗资源的使用成本。
同时,指南还对评判的透亮度、可靠性和一致性进行了要求,以确保评判结果的科学性和可比性。
该指南的核心部分是药物经济学评判的探究方法和步骤。
起首,探究者需要明确探究的目标和对象,确定评判的视角和时间范围。
其次,数据采集是评判的基础,探究者需要收集相关的药物使用数据、临床效果数据和费用数据。
然后,探究者可以选择适合的评判方法,并进行适当的数据分析和结果诠释。
最后,探究者应该对评判的结果进行谈论,评估评判的风险和不确定性,提出相关政策建议。
此外,指南还介绍了药物经济学评判在我国的现状和挑战。
虽然药物经济学评判在我国已经取得了一定的进展,但仍面临着数据质量、方法学水平宁应用推广等方面的问题。
指南提出了若干解决这些问题的建议,包括加强数据收集和管理、提高探究人员的培训和能力、完善药物经济学评判的政策环境等。
在文章的结尾,指南强调了药物经济学评判的重要性和应用前景。
通过合理的评判和利用药物经济学评判结果,可以为决策者提供科学的依据,增进药物的合理使用和医疗资源的优化配置。
同时,指南呼吁各相关方加强合作,推动药物经济学评判在中国的进步和应用。
综上所述,在药物评判领域具有重要的指导作用。
通过该指南的推广和应用,将有助于提高我国药物经济学评判的水平宁质量,为决策者提供更好的药物政策支持,增进我国药物经济的可持续进步综上所述,对于药物评判的方法和应用提供了重要的指导作用。
脂质过氧化诱导培养的内皮细胞产生单核细胞趋化因子RANTES
[文章编号] 1007-3949(2001)-04-0281-04・实验研究・脂质过氧化诱导培养的内皮细胞产生单核细胞趋化因子RANTES赵霞,祝学卫,杨丽敏,邓仲端,朱大和(华中科技大学同济医学院病理学教研室,武汉430030)[主题词 脂质过氧化; RANTES; 内皮,血管; 单核细胞; 动脉粥样硬化[摘 要] 为探讨脂质过氧化损伤是否诱导内皮细胞产生单核细胞趋化因子RANTES,使培养的人脐静脉内皮细胞暴露于5μm ol/L联胺后收取其条件培养基。
继之,将其放在截留分子质量分别为3.5kDa(外层)和10kDa(内层)的双层透析袋中,间层注入适量的0.01m ol/L P BS,再将透析袋悬在装有P BS的锥形瓶内进行透析。
透析完毕,取出间层液体,即为分子质量为3.5~10kDa的条件培养基,其中含RANTES。
用微孔滤膜法进行单核细胞趋化实验,并应用鼠抗人RANTES抗体,以证明条件培养基中RANTES的趋化活性。
结果发现,经联胺刺激的条件培养基引起的单核细胞迁移距离(89.75±11.33μm)明显大于不经联胺刺激的条件培养基(77.30±11.53μm)和随机移动组(76.18±10.50μm)。
方差分析显示,组间差异有极显著性(F=47.20,P<0.01)。
加入鼠抗人RANTES抗体后,单核细胞迁移距离明显缩短(F=21.31,P<0.01)。
结果提示,从功能实验方面表明脂质过氧化损伤能诱导内皮细胞产生RANTES增强,并可能在动脉粥样硬化病变的发生过程中起一定作用。
[中图分类号] R322.1,R392.12[文献标识码] ALipid Peroxidation I nduces Production of Monocyte Chemotactic F actor RANTESZH AO X ia,ZH U Xue2Wei,Y ANGLi2Min,DE NG Zhong2Duan,and ZHU Da2He(Department o f Pathology,Huazhong University o f Science&Technology,Tongji School o f Medicine,Wuhan430030,China)MeSH Lipid Peroxidation; RANTES; Endothelium,Vascular; M onocyte; AtherosclerosisABSTRACT Aim T o understand whether lipid peroxidation injury to endothelial cells(ECs)induces the production of m onocyte chem otactic factor RANTES. Methods A fter a four hour exposure of the cultured human umbilical vein ECs to5μm ol/L diamide,the conditioned medium(C M)was collected. T o obtain a conditioned medium containing RANTES(MW8 kDa),the above C M was put into the double layer dialysis m olecular porous membrane tubings(S pectrum Lab.Inc.)with the m olecular weight cut off at10kDa(inner layer)and3.5kDa(outer layer)respectively. Appropriate am ount of0.01m ol/ L P BS was injected into the interspace between the tw o membranes. The whole set of the membrane tubings was suspended in a pyramid flask containing P BS,and then the sam ples were dialysed against P BS. Finally,a conditioned medium with MW of3.5~10kDa was taken out from the interspace between the tw o membranes. The chem otactic activity of this conditioned medium for m onocytes was tested by micropore filter method using a m odified Boyden chamber.F or antibody inhibition studies,the condi2 tioned medium was incubated with anti2RANTES antibody and assayed again. R esults The m onocyte migration distance in2 duced by diamide2C M group(89.75±11.33μm)is markedly longer than that of the nondiamide2C M group(77.30±11.53μm)and that of the random migration group(76.18±10.50μm). Analysis of variance showed that there was a significant difference between groups(F=47.20,P<0.01). A fter the addition of anti2RANTES antibody,m onocyte chem otactic activity was marked2 ly inhibited(F=21.31,P<0.01). Conclusion On the basis of functional assay it suggests that lipid peroxidation injury might induce ECs to produce increased RANTES and may play an role in the recruitment of m onocytes into the intima in atherogen2 esis. 外周血单核细胞(m onocyte,MC)迁入内皮下间[基金项目] 国家自然科学基金(项目编号39730220)资助[作者简介] 赵霞,女,1973年10月出生,河南开封人,助教,病理学硕士研究生。
血清糖化血红蛋白、C 肽及胰岛素生长因子-1水平与肺癌的相关性
• 3950 •张美云,等 血清糖化血红蛋白、C肽及胰岛素生长因子-1水平与肺癌的相关性erative effects of gefitinib and docetaxel on non -small cell lungcancer (N S C L C) cells and the possible mechanism [ J ].PLoSO n e,2014,9(12) :e l 14074.[14]Kubota K,S a ka i H,K a ta ka m i N,e t al. A randomized phase I I I trial of oral S - 1 plus cisplatin versus docetaxel plus cisplatin inJapanese patients w ith advanced non -small cell lung cancer:TCOG0701 CATS tria l [ J]. A nn O ncol, 2015,26( 7 ) :1401 -1408.[15]Barlesi F,C h o u aid C,C re q u it J,e t al. A randomized tria l comparing adjuvant chemotherapy w ith gemcitabine plus cisplatin w ithdocetaxel plus cisplatin in patients w ith completely resected non -small - cell lung cancer w ith q uality of life as the prim ary objec-[16 ] Khodadad K, Khosravi A, Esfahani - Monfared Z, et al. Comparingdocetaxel plus cisplatin w ith paclitaxel plus carboplatin in chemotherapy -naive patients w ith advanced non -sm all -cell lungcancer: a single institute study [ J]. Iran J Pharm R es, 2014,13(2):575 -581.[17]Ikem ura S,N a o k i K, Yasuda H,e t al. A phase I I study of S -1and irinotecan combination therapy in previously treated patientsw ith advanced non -small cell lung cancer [ J ].Jpn J C lin Oncol ,2015 ,45 (4):356 -361.[18 ] Oshita F, M urakam i S, Kondo T, et al. Prospective study of paclitaxel and irinotecan for elderly patients w ith unresectable non -sm all cell lung cancer [J]. J Exp Ther Oncol ,2013,10 (3 ) :203tive [J].Interact Cardiovasc Thorac Surg, 2015,20 ( 6):783 -- 208.790. (编校:谈静)血清糖化血红蛋白、C肽及胰岛素生长因子-1水平与肺癌的相关性张美云,张新毅,刘晓燕The correlation of serum glycated hemoglobin,C peptide and insulin - like growth factor -1with lung cancerZhang Meiyun, Zhang Xinyi, Liu XiaoyanBaotou Cancer Hospital pinner Mongolia Baotou Q14Q3Q,China.【A b s tr a c t】O b je c tiv e:To explore i f H b A1c (glycosylated h e m o g lo b in),C - peptide and IG F—1(in s u lin- lik egrowth fa cto r- 1) as w e ll correlate the progression o f lu n g cancer re spectively.M e th o d s:Serum H b A^j C - peptideand IG F-1 were measured and com pared between80 he althy people and80 lu n g cancer pa tients.T h e ir correlatio n tothe histopathological types and the staging o f lu n g cancer was analyzed among the lung cancer pa tients.R e s u lts:Thelevels o f H b A j c,C- peptide and IG F- 1were s ig n ific a n tly increased in the lung cancer group com pared w ith the contro l group(P<0. 05) .W hen com paring the lu n g cancer w ith diabetes group(n=43) w ith the lu n g cancer group (n= 37) ,C- peptide and IG F- 1levels are s ig n ific a n tly h igh er in the study groups(P < 0. 05 ).C o n c lu s io n:SerumH b A1c,C- p e p tid e,and IG F—1are s ig n ific a n tly correlated w ith the developm ent and progress o f lung cancers.【K e y w o rd s】lu n g ca n ce r,H t^c,C- p e p tid e,IG F- 1M o dem Oncology2016,24(24) :3950 -3952【摘要】目的:探讨H b A lC(糖化血红蛋白)、C肽及I G F-l(胰岛素生长因子-1)与肺癌的相关性。
制备胰腺激素产生细胞的方法[发明专利]
![制备胰腺激素产生细胞的方法[发明专利]](https://img.taocdn.com/s3/m/f2b79617f705cc175427094b.png)
专利名称:制备胰腺激素产生细胞的方法专利类型:发明专利
发明人:细谷昌树,庄司昌伸
申请号:CN201180048849.0
申请日:20110808
公开号:CN103154240A
公开日:
20130612
专利内容由知识产权出版社提供
摘要:本发明的目的是提供由干细胞制备胰腺激素产生细胞的方法,所述细胞更接近胰腺生成的形式。
制备胰腺激素产生细胞的方法的特征在于使干细胞经历下列步骤(1)~(6):(1)在含有Rho激酶抑制剂的培养基中培养干细胞的步骤;(2)在含有GSK3抑制剂的培养基中培养上述步骤(1)中获得的细胞的步骤;(3)在含有GSK3抑制剂和活化素受体样激酶-4、7的激活剂的培养基中培养上述步骤(2)中获得的细胞的步骤;(4)从上述(3)中获得的细胞形成细胞团后,将该细胞团置于培养基中以悬浮状态培养的步骤;(5)将上述步骤(4)中获得的细胞在含有视黄酸受体激动剂、AMP活化蛋白激酶和/或活化素受体样激酶-2、3、6的抑制剂、活化素受体样激酶-4、5、7的抑制剂和细胞生长因子的培养基中培养的步骤;(6)在培养基中培养上述步骤(5)中获得的细胞的步骤。
申请人:武田药品工业株式会社
地址:日本大阪府
国籍:JP
代理机构:北京市柳沈律师事务所
更多信息请下载全文后查看。
营养风险评估指标(NRS2011)

营养风险评估指标(NRS2011)营养风险评估指标(NRS2011)一、概述营养风险评估是指对个体在营养方面可能出现的问题进行识别、评价和处理的过程。
营养风险评估指标(NRS2011)是一种广泛应用于临床的营养风险评估工具,由欧洲肠内营养学会(ESPEN)于2011年制定。
该评估指标旨在为医疗团队提供客观、科学的方法,以确定患者是否存在营养风险,从而为制定营养治疗方案提供依据。
二、评估指标NRS2011评估指标包括以下四个方面:1. 营养状况:通过体重、身高、年龄等参数计算体质指数(BMI),评估患者的营养状况。
BMI<18.5为营养不良,18.5≤BMI<24为正常营养状况,BMI≥24为肥胖。
2. 疾病严重程度:根据患者的急性病生理评分(APACHE II评分)或慢性疾病评分(CCI评分)来评估疾病严重程度。
APACHE II评分≥15或CCI评分≥30表示疾病严重。
3. 年龄:年龄≥70岁为高风险年龄段。
4. 应激状态:应激状态是指机体在遭受创伤、手术、感染等刺激时,产生的一系列生理、心理和代谢改变。
应激状态下的患者存在较高的营养风险。
三、评估流程1. 收集患者的基本资料,包括年龄、性别、体重、身高、疾病诊断等。
2. 计算BMI,评估患者的营养状况。
3. 根据疾病严重程度,选择合适的评分系统进行评估。
如APACHE II评分或CCI评分。
4. 判断年龄是否≥70岁。
5. 评估患者是否存在应激状态。
6. 根据上述评估结果,计算营养风险评分(NRS)。
NRS计算公式为:NRS = 疾病严重程度评分 + 营养状况评分 + 年龄评分 + 应激状态评分。
7. 根据NRS评分,判断患者是否存在营养风险。
NRS≥3分为存在营养风险,需制定营养治疗方案。
四、营养治疗方案1. 对于存在营养风险的患者,应进行营养评估,确定营养需求。
2. 根据患者的营养状况、疾病特点和治疗目标,制定个性化的营养治疗方案。
胰岛素样生长因子(Insulin-like growth factor)

胰岛素样生长因子(Insulin-like growth factor)Insulin-like growth factorBasic conceptShanghai Ya Xi (International) snow America authorized biomedical technology services center marketing P DepartmentInsulin-like growth factors (IGFs) is a class of multifunctional cell proliferation regulating factors. It plays an important role in cell differentiation, proliferation and individual growth and development. This paper reviews the general situation of IGFs and its relationship with growth and development.History of IGFSGrowth hormone and Daughaday on 1957 Salmon (growth hormone, referred to as GH) in the process of giving first found in hypophysectomized rats after GH serum can stimulate S into cultured cartilage, but directly into the liquid culture of GH has no effect, so that GH itself can directly stimulate the growth of cartilage, but through a "SF" role, this factor became known as growth regulator. 1963 Froesh found in the serum insulin like effect on muscle and fat cells are only a small part of the insulin antiserum inhibited the remaining soluble insulin like activity was not inhibited in acidified ethanol, and named NSILAS which is inhibited by insulin like activity (nonsuppressible insulin-like activity). In 1972, Pieron and Temin purified a cytokine from bovine serum that stimulated cell division, called proliferation stimulating activity".After the above three experiments were completed, it was found that the above three substances had an inhibitory insulin-like activity and a growth stimulatory effect. With the development of molecular biology, 1978 people purified two kinds of NSILA (I, II) and found its structure and proinsulin were named as similar, insulin-like growth factor I and II (IGF I, II) to emphasize their homology with insulin structure. It was also confirmed that the sulfation factor and the proliferation stimulating activity were members of the same polypeptide family as IGF.Composition, physical and chemical properties of IGFs systemThe IGFs family is composed of two low molecular polypeptides (IGF-, I, IGF- II), two specific receptors and six binding proteins. IGF- I is a single nucleotide protein with 70 amino acids, the molecular weight of 7649Da, heat resistance, while IGF- II is a single stranded weak acid protein with 67 amino acids, with a molecular weight of 7471Da and stable for 0.1%SDS. Both 70% are homologous, approximately 50% of the structure and function of human proinsulin. The biological function of IGFs is achieved by binding to receptors on specific target cell surfaces. At present, two kinds of IGF receptors with different structures are found: IGF- I receptor and IGF- II receptor (mannose -6 phosphate receptor), also known as type I receptor, type II receptor. The former structure and insulin receptor (Insulin receptor Ir) is similar to that of 2 beta 2 glycoprotein four dimer consisting of alpha and beta two subunit alpha, alpha subunit is a ligand binding site, beta subunit with intrinsic tyrosine kinase activity and tyrosinase activity. IGF and insulin (Insulin, Ins) on IGF receptoraffinity of the order of Ir is Ins > > IGF- I IGF- II; on IGF- receptor: IGF- I IGF- II > > Ins; on IGF- II receptor: IGF- > IGF- I and Ins II, with no cross reaction.Unlike other growth factors, IGFs is associated with a specific binding protein (Binding, Proteins, BPs) in serum, in extracellular fluid and in cell cultures, and in the form of inactive complexes. So far, 6 IGFBP1, 2, 3, 4, 5 and 6 have been found, and their characteristic structures constitute a correlation. The secretory protein families are low molecular peptides, similar in structure to 50%. They are high affinity with two IGF without binding to insulin. In the blood and tissue fluid, the IGFBP3 content is highest, and more than 80% of the IGF in the cycle is combined with IGFBP3 to form the 150kDa three molecular complex (an unstable acid subunit, a binding subunit and IGF peptide). IGFBP2,5,6 has a higher affinity with IGF- II, and IGFBP1, 3, and 4 are similar in affinity to IGF- I and IGF- ii. IGFBP has the function of prolonging the circulating level of IGF half-life and stabilizing IGF serum concentration. Normally, the affinity of IGF with its binding protein is greater than or approximately equal to its receptor binding. In addition, the low expression of the high affinity receptor leads to a balance between a small amount of free IGF and a large number of IGF/IGFBP complexes. At present, there are at least three mechanisms involved in the activation of IGF:(1) parallel movement. In specific cases, such as growth, development, or damage to the organism, high affinity receptors are abundantly expressed, competing for IGF and separating it from binding proteins;(2) chemical modification of IGF or IGFBP, such as phosphorylation, to reduce the affinity of the complexes and dissociate them;(3) binding protein hydrolase specific water samples IGFBP to release the IGF.IGFs and growth and developmentIGF- I and IGF- II have similar structures and in vitro activity, but their biological effects are not the same. The biological functions of IGFs are not limited to mitogenic stimuli, but they can also induce differentiation or promote the expression of differentiated functions. The precise biological effects depend on the state of cell development and the presence of other hormones or growth factors. Especially in different tissues and different growth stages, there is a considerable difference in the function and level of IGF- I and IGF- ii. IGF- I, dependent on GH, can promote proliferation of many cells in vitro and promote protein and DNA synthesis. Many tissues and cells in the body can autocrine and paracrine IGF- I. IGF- II, known as the major growth factor before birth, does not require growth hormone regulation and is expressed in a variety of tissues and organs.Studies have shown that in early pregnancy, trophoblast cells invade the endometrium is strictly controlled by the micro environment; progesterone regulating endometrium and decidua and villus development and promote embryo implantation are mediated by IGFs, the mechanism was to increase the adhesion of the extracellular matrix, invasion and migration of humantrophoblast cells to stimulate, promote early embryo cultivation. In vitro experiment of Kniss and IGFs could promote early pregnancy decidua and villi on transport of glucose and amino acids, in a dose-dependent manner, suggesting that the fetal circulation before the embryo mainly from the surrounding environment and nutrition, through the role of IGFs. At the same time, a large number of studies have shown that during embryonic development, the level of IGF- II mRNA is much higher than that of IGF- I and mRNA, and has higher expression in embryonic tissues. With the increase of differentiation degree, the expression of it decreases. The expression of mRNA and IGF-I is affected by many factors, a large increase in liver, heart and kidney after birth than before birth; and significantly decreased in muscle, stomach and testis after birth than before birth; only IGF- in the brain and lung of mRNA showed a wavy change. Clinical studies have shown that the concentration of IGF- I in maternal circulation increases during pregnancy, and that fetal IGF- I is approximately 15 weeks pregnant. The levels of IGF-, I and IGFBP1 in umbilical artery and umbilical vein were similar. There was no significant difference between the two groups, indicating that the secretion of IGF- I in the mother and fetus was independent, and that IGF- I might not pass through the placenta. Some scholars detected the concentration of cord blood IGF- I, and the results showed that intrauterine fetal growth retardation, IGF- in cord blood was lower than that in gestational age group by about 40%, while that of gestational age IGF- was 8% to 10% higher than that in gestational age group. IGFBP1 increased significantly in preterm infants and small in gestational age infants, and negatively correlated with birth weight. There are serum levels and neonatal IGF- I reported the birth weight andlength were positively correlated, and as the main growth factor before the birth of IGF- II and the neonatal birth height and weight have no obvious correlation, and decreased rapidly after birth. Arsio IGF- concentration was measured in umbilical cord blood of 131 gestational age between 19 and 40 weeks of gestation by umbilical vascular puncture. The results showed that IGF- I was positively correlated with gestational age. In conclusion, the mechanism of IGFs's action on the fetus is not very clear, but its role in fetal growth and development has been widely recognized. This is also confirmed by genetic studies. Growth inhibition was first observed at 10.5 days after the mutation of IGF- I and IGF- II genes, and the weight of newborn rats at birth was only 30% of the normal weight of wild species. Another report: IGF- I and IGF- II deficient mice or IGF- II R and IGF- I R have defects in animal performance not only dwarf more serious, only 45% wild mice, these small animal have obvious muscle hypoplasia, the number of fiber cells in skeletal muscle and reduce serious skin hypoplasia. Births often die of respiratory failure. In conclusion, the expression of each of the IGF and IGF receptors is essential for normal embryo and fetal growth, and indicates that the two are absent and very few other components are up and down. Daughaday pointed out in 1988 that postnatal human plasma IGF- I and IGF- II concentration is inversely related to possible mechanisms for the competition between IGF-BP3 (1); (2) both inhibit the secretion of GH, and the GH of IGF- I IGF- II positive regulation; through the secretion of GH play a role of indirect inhibition of IGF-I. It can be assumed that it is precisely because of the interaction between IGF- I and IGF- II that the body's response is balanced. The process of growth and development of IGF- I was regulated by GH and other growthfactors. The expression level of IGF- I increased after birth was related to GH, and the tissue with decreased expression was related to specific factors. A large number of studies on the IGF- I and -GH axis have recently suggested that GH stimulates liver secretion of IGF- I, and IGF- I, in turn, inhibits GH. The complex of IGF and binding proteins in the cycle constitutes the major repository of IGF- I in circulation, and GH regulates its cycle levels. In the past, somatic cell theory suggested that most of GH's action was mediated by cyclic IGF- I during the linear growth of the organism,But recently, GH has been found to stimulate the production of IGF- I, a autocrine or paracrine action of IGF- I, which is important for normal growth in rodents, liver, and other tissues. Molecular biology studies were conducted using animal experiments to examine malnutrition in children due to inadequate caloric and protein intake. The results showed that malnutrition in children caused by growth arrest, the key is the diminutive of IGF- gene transcription level decreased, liver cell IGF- I decreased mRAN level, decrease of plasma IGF- content of clear, too fast. The mechanism of action may be the regulation of GH on the expression of IGF- I gene. Therefore, IGF- I is closely related to the growth and development of children.In addition, Urderwood reported the use of IGFs in the treatment of GH insensitive short stature patients, including Laron's syndrome and GH deficiency. Laron's patients lack GH receptors and do not respond to GH. Such patients have low levels of IGF- I, slow growth, but high levels of circulating GH, which is due to a decrease in GH feedback inhibition by IGF- I. The GHdeficient person mistakenly identified GH as an exotic protein, producing a large number of antibodies that weakened or disappeared the body's response to GH. One case of Laron's boys treated with GH showed no improvement in growth rate, but was treated with IGF- I for 2 years and grew at a rate of 10cm/ years. In addition, recent studies have shown that GH itself is not directly required for growth, and all the height development described by GH is actually done by IGF- I.The research of IGFs is a hotspot in the field of cell biology, and has been paid more and more attention to. It will probably become an important breakthrough for human beings to explore the mysteries of life. IGF is closely related to human embryo development and individual growth and development. However, the effect of IGF on many system tissues is only in vitro and animal experiments, so there is still much work needed to do further research on IGFs.ReferenceWH., Salmon, WD, Daughaday, A, hormonally, controlled, serum, factor, which, stimulates, sulfate, in, corporation, by,, cartilage, in, vitro., J,, Lab, Clin, Med, 1957,49:825-836.2 Froech ER. Antibody-suppressible and nosuppressible insulin-like acitivities in human serum and their physiologic significance. An insulin assay with adipose tissue of incneased precision and specificity. J Clin Invest, 1963,42:1816-1834.3 Pierson RW, Jr.The partial purification from calf serum ofa fraction with multiplication-stimulating activity forchicken firoblasts in cell culture and with non-suppressible insulin-like activity. J Cell Physiol, 1972,79:319-329., Grudice, IC.Insulin-like, factors, and, growth, ovarian, follicular, development.Endocrine, Reviews, 1992,13:641-665., Froesch, ER., of, insulin-like, Action, growth, factors., Ann, Rev, Physiol, 1985,47:443-467., Stylianopoulou, F.Pattern, of, the, insulin-like, growth, factor, II, gene, expression, during, rat, embryogenesis., Development, 1988103:497-506.Suface, Irving, JA, Lala, PK.Function, role, of, cell, integrins, on, human, trophoblast, cell, migration:regulation, by, TGF-beta,, IGF-, II, and, IGFBP1.Exp, Cell, Res, 1995217:419-427.The "Kniss DA.Insulin-like grouth factors:Their regulation of glucose and amino acid transport in placental trophoblasts isolated 1994,39:249-25. from first-trimester chorionic villi.J Report Med"9 Liu Baoying, Wang Li. Advances in the study of insulin growth factors. Foreign Medical Sciences, molecular biology section,.1996, 18:103-106.10 HS, Qu Xinzhong, Li Guilin. Effects of growth factors and hormones on the fetus. Foreign medical * maternal and Child Health Sciences, 1996, 7:162-163., Steven, D.The, growth, hormone/insulin-like, factor, axis, in, intrauterine, growth, growth, retardation:, Pathophysiological, and, therapeutic, implications., Endocrinology, 1996,6:294-300.,...12 children's longevity. Malnutrition molecular basis affect the children's growth: insulin-like growth factor gene expression in.Advances in Physiological Sciences, 1995, 26:144.1993,75:73-82., Julie, Baker, Liu, JP, Robertson, EJ, et, al.Role, of, insulin-like, growth, factors, in,, embryonic, and, postnatal, growth.Cell,...Perkins, Liu, JP, Baker, J, AS, et, al., Mice, carrying, null, mutations, of, the, genes, encoding, insulin-like, growth,, factor, I, and, the, typy,,, IGF, receptor.Cell,1993,75:59-72.15 Plilippe F, Backel Jauw. Louis E, Underwood et al. Prolonged treatment with recombinant insulin-like growth factor I in children with growth hormone insensitivity syndrome-A clinical research center study.J Clin Endocrinology and Metab.1996,8: 3312-3314.Shanghai Ya Xi (International) snow America authorized biomedical technology services center marketing P Department。
血清α-胡萝卜素浓度高则死亡风险低

血清α-胡萝卜素浓度高则死亡风险低
佚名
【期刊名称】《浙江中西医结合杂志》
【年(卷),期】2011(21)5
【摘要】美国一项流行病学调查显示,血清α-胡萝卜素浓度与全因、心血管疾病、肿瘤及其他原因所致死亡风险均呈负相关。
研究发表于《内科学文献》[ArchIntern Med 2001,171(6):507]。
【总页数】1页(P371-371)
【关键词】α-胡萝卜素;死亡风险;浓度;血清;流行病学调查;心血管疾病;科学文献;Med
【正文语种】中文
【中图分类】R151.3
【相关文献】
1.论低血清睾酮增加血液透析男性患者的死亡风险 [J], 陆恩峰;罗仕云;方如美;朱昭章;刘周;李松;莫艳珍
2.高盐低钾饮食增加死亡风险 [J], 莘桦;
3.中国首个基于血清抗体的新冠病毒感染患病率大样本调查结果发布/经颅直流电刺激可有效治疗难治性癫痫!/注意缺陷多动障碍等精神疾病遗传风险影响患者高级认知功能/4万国人研究显示:45岁前血压高,死亡风险翻倍增! [J],
4.血清氯离子浓度与心力衰竭患者死亡风险的Meta分析 [J], 安嬿;侯丹华;范秀珍
5.低血清维生素D浓度与呼吸道感染风险相关联 [J],
因版权原因,仅展示原文概要,查看原文内容请购买。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Printed by sky script on 6/10/2011 11:12:38 PM. For personal use only. Not approved for distribution. Copyright © 2011 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Version 1.2011, 03/04/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines™ and this illustration may not be reproduced in any form without the express written permission of NCCN®.
Printed by sky script on 6/10/2011 11:12:38 PM. For personal use only. Not approved for distribution. Copyright © 2011 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Continue
Version 1.2011, 03/04/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines™ and this illustration may not be reproduced in any form without the express written permission of NCCN®.
NCCN Guidelines™ Version 1.2011 Panel Members Myeloid Growth Factors
* Jeffrey Crawford, MD/Chair † ‡
Duke Cancer Institute Jeffrey Allen, MD † St. Jude Children's Research Hospital/University of Tennessee Cancer Institute. James Armitage, MD Þ UNMC Eppley Cancer Center at The Nebraska Medical Center Douglas W. Blayney, MD † University of Michigan Comprehensive Cancer Center Spero R. Cataland, MD ‡ The Ohio State University Comprehensive Cancer Center - James Cancer Hospital and Solove Research Institute Mark L. Heaney, MD, PhD † ‡ Þ Memorial Sloan-Kettering Cancer Center Sally Htoy, PharmD å City of Hope Comprehensive Cancer Center Susan Hudock, PharmD å The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins Dwight D. Kloth, PharmD å Fox Chase Cancer Center David J. Kuter, MD, DPhil † ‡ Massachusetts General Hospital Cancer Center Gary H. Lyman, MD, MPH † ‡ Duke Cancer Institute
NCCN Guidelinesபைடு நூலகம்Index MGF Table of Contents Discussion
Brandon McMahon, MD Robert H. Lurie Comprehensive Cancer Center of Northwestern University David P. Steensma, MD † Dana-Farber/Brigham and Women’s Cancer Center
NCCN Guidelines Index MGF Table of Contents Discussion
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines™)
Myeloid Growth Factors
Version 1.2011
Printed by sky script on 6/10/2011 11:12:38 PM. For personal use only. Not approved for distribution. Copyright © 2011 National Comprehensive Cancer Network, Inc., All Rights Reserved.
Saroj Vadhan-Raj, MD Þ The University of Texas MD Anderson Cancer Center Peter Westervelt, MD, PhD † Siteman Cancer Center at Barnes-Jewish Hospital and Washington University School of Medicine Michael Westmoreland, PharmD å The University of Texas MD Anderson Cancer Center NCCN Mary Dwyer, MS Maria Ho, PhD
Version 1.2011, 03/04/11 © National Comprehensive Cancer Network, Inc. 2011, All rights reserved. The NCCN Guidelines™ and this illustration may not be reproduced in any form without the express written permission of NCCN®.
NCCN Guidelines Index MGF Table of Contents Discussion
Clinical Trials: The NCCN believes that the best management for any cancer patient is in a clinical trial. Participation in clinical trials is especially encouraged. To find clinical trials online at NCCN member institutions, click here: /clinical_trials/physician.html
Consensus: All recommendations are Category 2A unless otherwise specified. See NCCN Categories of Evidence and Consensus
The NCCN Guidelines™ are a statement of evidence and consensus of the authors regarding their views of currently accepted approaches to treatment. Any clinician seeking to apply or consult the NCCN Guidelines is expected to use independent medical judgment in the context of individual clinical circumstances to determine any patient’s care or treatment. The National Comprehensive Cancer Network® (NCCN®) makes no representations or warranties of any kind regarding their content, use or application and disclaims any responsibility for their application or use in any way. The NCCN Guidelines are copyrighted by National Comprehensive Cancer Network®. All rights reserved. The NCCN Guidelines and the illustrations herein may not be reproduced in any form without the express written permission of NCCN. ©2011.
NCCN Categories of Evidence and
Therapeutic Use of CSF For Febrile Neutropenia (MGF-3)
Examples of Disease Settings and Chemotherapy Regimens and Risk of Febrile Neutropenia (MGF-A) Patient Risk Factors for Developing Febrile Neutropenia (MGF-B) Myeloid Growth Factors for Prophylaxis and Treatment of Febrile Neutropenia and Maintenance of Scheduled Dose Delivery (MGF-C) Toxicity Risks with Growth Factors (MGF-D) Patient Risk Factors for Poor Clinical Outcomes or for Developing InfectionAssociated Complications (MGF-E)