6Pressuretargetedventilation
呼吸机参数的设置和调整-最终版
SIMV
• 调节参数:FiO2,VT,RR,I/E,触发灵敏度
• 特点:支持水平可调范围大(0~100%),能保 证一定的通气量,同时在一定程度上允许自主呼 吸参与,防止呼吸肌萎缩,对心血管系统影响较 小;自主呼吸时不提供通气辅助,需克服呼吸机 回路的阻力
SIMV
• SlMV缺点: (1)如患者自主呼吸良好,会使SlMV频率增加,可 超过原先设置的频率 (2)同步触发的强制通气量,再加上患者自主呼吸 的潮气量可导致通气量的增加。例如,患者的自主 呼吸的潮气量为200ml,设定的呼吸机SIMV潮气量 为600ml,则此时的一次潮气量可达800ml (3)如病情恶化,患者的自主呼吸突然停止,则可 发生通气不足 (4)自主呼吸在一定程度上可增加呼吸功,如使用 不当将导致呼吸肌群的疲劳
应用
• 中枢或外周驱动能力很差者
• 对心肺功能贮备较差者,可提供最大的呼吸支持, 以减少氧耗量。如:躁动不安的ARDS患者、休 克、急性肺水肿患者
• 需过度通气者:如闭合性颅脑损伤
容量控制通气: 吸气的进行
Tinsp Tinsp Ttot x Insp% Vt / flow
1.
I
1
2
2.
在设置的f及Ti内以 恒定流速的方式给 予预置的Vt 吸气流速恒定, 由医 生设定
呼吸机参数的设置和调整
中山一院神经科ICU
2018.11.15
主要内容
• 一 初步参数设置
• 二 呼吸参数调整 • 三 神经-肌肉疾病呼吸机使用
机械通气概述
机械通气定义
• 机械通气:通过呼吸机建立气道口与肺泡之间压 力差,形成肺泡通气的动力和提供不同氧浓度, 增加通气量、改善换气,降低呼吸功,达到改善 或纠正缺氧、CO2潴留和酸碱失衡,防治多脏器功 能损害 • 机械通气给呼吸衰竭(呼衰)患者予以呼吸支持, 维持生命,为基础疾病治疗、呼吸功能改善和康 复提供条件
美国鸟牌呼吸机使用
特点:该模式由自主呼吸触发,并决定RR和I/E, 因胸而肺有呼较吸好力的学人特机性协(调气。道而阻V力T和与胸预肺置顺的应压性力)支及持吸水气平、 努力的大小有关。当吸气努力大,而气道阻力较小和 胸大肺。顺应性较大时,相同的压力支持水平送入的VT较
容量控制通气(volume controlled ventilation, VCV)
❖ 概和念吸:气潮流气量量完(全V由T呼)吸、机呼来吸控频制率。(RR)、吸呼比(I/E) ❖ 调节参数:吸氧浓度(FiO2),VT,RR,I/E. ❖ 特点:能保证潮气量的供给,完全替代自主呼吸,有利于
呼吸肌休息;易发生人机对抗、通气不足或通气过度,不 利于呼吸肌锻练。
SIMV的通气波形
Flow L/m
调节参数:FiO2,VT,RR,I/E。SIMV需设置触发灵敏度。 特点:支持程度可调(0~100%),能保证一定的通气量,同时允许自主
呼吸参与,对心血管系统影响较小;自主呼吸时不提供通气辅助,而需克服 呼吸机回路的阻力,故对呼吸肌有锻炼作用。 应用:有自主呼吸,可逐渐下调IMV辅助频率,向撤机过渡;若自主呼吸 频率过快,采用此种方式可降低自主呼吸频率和呼吸功耗。
如何使用呼吸机?
Pressure Flow
Volume
报警静音、 报警重置、 冻结、吸气 末屏气(最长6秒钟 、手 不可以呼气) 动呼吸(在一次呼
吸的呼气相期间按下该按 钮,进行一次强制呼吸。 如果在吸气相按该按钮则
、呼 不执行呼吸) 气末屏气、 同步雾化器、 100 % 02、 面板锁定、 接受
机械通气参数设置 英文

机械通气参数设置英文Mechanical ventilation is a critical component of critical care medicine, used to support or replace spontaneous breathing in patients who are unable to maintain adequate gas exchange. The parameters of mechanical ventilation must be carefully set to ensure optimal patient outcomes while minimizing the risk of ventilator-induced lung injury.In setting mechanical ventilation parameters, several factors need to be considered, including the patient's age, weight, height, underlying lung disease, and the etiology of respiratory failure. The ventilator mode, tidal volume, respiratory rate, FiO2 (fraction of inspired oxygen), and PEEP (positive end-expiratory pressure) are among the key parameters that need to be adjusted.Ventilator Mode.The ventilator mode determines how the ventilatordelivers breaths to the patient. The most common modes are volume-controlled ventilation (VCV), pressure-controlled ventilation (PCV), and assist-control ventilation (ACV). In VCV, the ventilator delivers a fixed tidal volume at a set respiratory rate, regardless of the patient's effort. In PCV, the ventilator delivers a fixed pressure, and thetidal volume is determined by the patient's compliance and resistance. In ACV, the ventilator provides breaths at a set rate, but allows the patient to trigger additional breaths as needed.Tidal Volume.Tidal volume refers to the volume of air delivered to the patient during each breath. It is typically measured in milliliters (mL) and is adjusted based on the patient's weight and lung compliance. In adults, a tidal volume of 6-8 mL/kg of predicted body weight is generally recommended. However, this may need to be adjusted based on thepatient's clinical condition and response to ventilation.Respiratory Rate.Respiratory rate refers to the number of breaths delivered to the patient per minute. It is typically set based on the patient's baseline respiratory rate and adjusted as needed to maintain normocapnia (normal carbon dioxide levels). In adults, a respiratory rate of 12-20 breaths/minute is generally recommended. However, this may need to be increased or decreased based on the patient's condition and response to ventilation.FiO2。
VELA呼吸机
2. 潮气量 〔 tidal volum VT 〕 按 6 - 8 - 12 ml/Kg 设置
3. 频率 〔 frequency f 〕 按 12 - 20/min 设置
4. 吸入氧浓度〔 fracture of inspiratory oxgen FiO2 〕
• 长期使用呼吸机吸入氧浓度应在40% 以 下, 以免发生氧中毒
APRV Biphasic 同步气道压力释放通气
• 当肺功能严重受损时〔如ARDS〕,肺组织接受 机械通气治疗选择余地已很少,机械通气对肺的 外加干预作用可能会进一步损害残存正常肺组织 引发一连串副反映。机械通气对肺组织的剪刀力 可使残存组织受到损伤,造成组织液和血流渗入 肺泡产生肺不张,其结果是通气区域进一步减少, 产生恶性循环。APRV通气模式允许自主呼吸存 在于机械通气过程中,因而防止了人机对抗现象, 减少镇静药的应用,病人呼吸未受减弱,经过一 段时间辅助通气后,增加的自主呼吸可使原已闭 陷的肺泡再次充盈,扩大了肺的气体交换区域。 使通气压力下降,自主呼吸进一步得到恢复,产 生良性循环
6.PaO2 <正常值1/3。
7.P〔A-a〕 O2>50mmHg〔FiO2=0.21,吸空气〕 者。
8.P〔A-a〕 O2>300mmHg〔FiO2=1.0,吸纯O2〕 者。
9.最大吸气压力<25cmH2O者〔闭合气路, 努力吸气时的气道负压〕。
10.肺内分流〔QS/QT〕>15%者
其他
1.大咯血或严重误吸引起的窒息性呼吸 衰竭。
机械通气的目的
呼吸机治疗的目的主要为:
1.维持适当的通气量,使肺泡通气量满足 机体需要。改善气体交换功能,维持有效 的气体交换。
2.减少呼吸肌的作功。
呼吸机常用术语英汉对

呼吸机常⽤术语英汉对呼吸机常⽤术语英汉对照Assist 辅助Apnea 窒息Applicable 适⽤的Anesthtics ⿇醉的Adaption 适应Adult 成⼈AUTO ⾃动Auto flow ⾃动流速ASV adaptive support ventilation 适应性通⽓APRV airway pressure release ventilation 压⼒释放通⽓A/C Assist/Control 辅助/控制Above 在------上⾯Accept, enter 确认Airway ⽓道Alarm 报警APV adaptive pressure ventilation 适应性压⼒通⽓Automatic ⾃动的Adimit 接收Additional 补充的Activate 激活,使运⾏BiPAP Bi-level positive airway pressure 双⽔平正压通⽓Brightness 明亮度Biomedical ⽣物医学的Breath 呼吸Battery 电池Basic 基础的Barometer ⽓压计C , compliance 顺应性Cell 电池Comprehensive 综合的comptent 适当的CMV 控制性机械通⽓controlled mechanical ventilationCPAP 持续⽓道正压continous positive Airway pressurecalibration 定标curve 曲线configuration 配置Cstat , static compliance 静态顺应性current 当前的Cdyn , dynamic compliance 动态顺应性continue 继续Cycle 循环CMV controlled mandatory ventilation 控制指令通⽓Close 关闭Clear 清楚Copy 复制Code 编码Data 数据Charge 充电Combustible Compensation 补偿Check 检查Caution 警告Cassette 盒capacity 容量Concentration /cnc. 浓度cursor 光标Calibrate 标准刻度Disable 使不起作⽤Decrease 递减Diagnotic 诊断的Diplay 显⽰Defaults 默认的Disconnection 管道脱开dicimal ⼗进制的Exit 退出EST 扩展⾃检EXP.TRIG 呼⽓触发Exp.pause 呼⽓暂停Error 错误External 外部的Exhaled 呼出的Exhaled valve 呼出阀E呼出触发灵敏度Et CO2 呼出⽓⼆氧化碳ETS ,SENSFreeze 冻结format 板式fast 快 filter 过滤器 low-by 持续基础⽓流 fuse 保险丝TOT f 总的呼吸频率f, respiratory rate 呼吸频率 spontf ⾃主呼吸频率flammable 易燃的graphics 图形 gas trapping ⽓体陷闭humidifier 加热器 flow 流量 HME ⼈⼯⿐ History 历史 Hour ⼩时 Heat 加热 Hazard 危险Insp cycle off =ETS 呼⽓触发灵敏度 Ignition 燃烧 Internal 内部的 Interval 间隔的 Insp.pause 吸⽓暂停 Insp./exp.Hold 吸⽓/呼⽓保持 ILV ,independent ventilation 分侧肺通⽓ IRV ,inverse ratido ventilation 反⽐通⽓ I:E 吸呼⽐ infant 婴⼉I.TRIG 吸⽓触发 installed 已安装的 IPPV intermittent positive pressure ventilation 间歇正压通⽓leak 漏⽓ lung 肺 liter 升 limb 分⽀ log ⽇志 lock 加锁 limit 限制 loop 环monitoring 监护 manual Insp ⼿动吸⽓ MMV mandatoey minute ventilation 分钟指令通⽓ mute 静⾳ medium 中间的 menu 菜单 manual ⼿动的measure 测量 MVspont , Espont V ⾃主呼吸分钟通⽓量 mask ⾯罩 mode 模式MV ,minute volume ,E V 分钟通⽓量 mandatory 机器的 Membrane 薄膜 maintenance 保养 Modules 模块nebulizer /nebulization 雾化 nebulized inhalation 雾化吸⼊ NPPV non-invasive positive support ventilation ⽆创正压通⽓ on 开 off 关oxygen 氧⽓ obstruct 挡住 option 选择pediatric ⼩⼉ panel ⾯板procedure 程序 power 电源PEEP ,positive end-expiratory pressure 呼⽓末正压 PEEPi ,auto PEEP 内源性PEEP Plot 平⾯图 PS , SUPP P (pressure support) 压⼒⽀持Pmean ⽓道平均压 Plateau 平台PPS proportional pressure support ventilation 成⽐例压⼒⽀持通⽓ PC ,pressure control 压⼒控制 Pramp 压⼒上升斜率1.0P ⼝腔闭合压 Ppeak 峰压 Proposed 预设的 P-SIMV 压控的SIMV P-TRIG 压⼒触发 Patient 病⼈ Pressure 压⼒ Pass 通过PSV , SPONT , ASB 压⼒⽀持通⽓P m ax maximal airway pressure 最⼤⽓道压⼒Pplat plateau airway pressure 平台⽓道压⼒Peak inspiration flow 峰值吸⽓流速 Peak P peak airway pressure 峰值⽓道压⼒mean P mean airway pressure ⽓道平均压⼒personnalPrevious 先前的 P-V loop 压⼒-容量环 Probe 探头 Profile 描绘轮廓I P 吸⽓压L p低压 H P⾼压 END I PPost开机⾃检PRVC 压⼒调节容量控制 pressure requlated volune control Preventive 预防性的Qualified 有资格的R , risistance 阻⼒ RSBI 浅快呼吸指数 Rexp 呼⽓阻⼒ Respiration 呼吸 Rstat 静态顺应性 Rdyn 动态顺应性 Rise time 上升时间 Review 回顾 RAMP 三⾓波 Result 结果 Recommend 推荐的Setting 设置 Status 状态 Setup 组织 SST 快速⾃检 Switchover 切换 sensor 传感器 second 秒 special 特别 slope 斜率 slow 慢 spontaneous ⾃主的 system 系统 spont ⾃主呼吸 sensitivity 灵敏度 square ⽅波 standby 待机SIMV 同步间歇指令通⽓synchronized intermittent mandatory ventilation Suction 抽吸 Sweep 清除 Scale 范围 Speed 速度Screen 屏幕 Silence 静⾳Sound 声⾳Sigh 叹息 Smart sigh 智能叹息 separator 分离器Throughly E T 呼⽓时间Tracheal intuation ⽓管插管 TC ,time constant 时间常数Trap 陷闭 I T吸⽓时间Ta 窒息时间 Type 类型 Tool ⼯具 Temperature 温度 tachypnoea 呼吸急促 Test 测试 Total TOT 总的Trigger 触发Unlocked 解除锁定VS 容量⽀持Ventilator 呼吸机Ventilation 通⽓ VT ,tidal volume 潮⽓量 Ve ,expiraory volume 呼⽓量 Vi ,inspired volume 吸⽓量 Valve 阀门 Velocity 流量 TE V 呼出⽓潮⽓量DS V 死腔量V-TRIG 流量触发 V olume 容积VSV ,volume support ventilation 容量⽀持通⽓V APSV ,volume assured pressure support ventilation 容量保证压⼒⽀持通⽓ Version 版本,说明 value 值WOBv ,work of breathing by ventilator 呼吸机做功 WOBp work of breathing by patient 病⼈⾃主做功 Waveform 波形 Wire导线 wye Y 型管%IBM 理想体重百分⽐Use knob to adjust 使⽤圆柄调整To cancle touch the setting button 要退出请按设置键 applies to mannal INSP ONL Y 尽使⽤于⼿动吸⽓时last 2 spont breath <low/high frequency 低的/⾼的呼吸频率 O2 cell Calibration required 需要氧电池定标↑/↓ Vte mand 机控呼出⽓量增加/减少low AC power 低交流电压↑/↓Vte spont ⾃主潮⽓量增加/减少 low/high minute volume 低/⾼分钟通⽓量no compressor air 压缩泵没有空⽓↑↓PEAK 峰压上升/下降high/low pressure ⾼压/低压device alert 设备警告low pressure O2/air inlet ⼊氧⽓/空⽓压⼒过低Exhalation valve leak 出阀漏⽓1标准⼤⽓压=76cmHg=1033cmH2O=103Kpa50PSI(1磅⼒每平⽅英⼨)=3500cmH2O/cm.cm=350Kpa/cm.cm=3.5kg/cm.cm840快速⾃检SST Flow sensor 快速⾃检流量传感器Connect circuit with insp filter and without humidifier 脱开湿化器,管路与吸⼊过滤器连接Block wye 阻断Y型接⼝Test …….. 测试进⾏中Connect humidifier if applicable 如有湿化器请连接Circuit pressure test 管路压⼒测试Circuit leak 管路漏⽓Disconnect at from-patient port 脱开病⼈呼出端⼝Expiratory filter 呼出过滤器Connect to from-patient port 连接病⼈呼出端⼝Unblock wye 开放Y型接⼝Circuit resistance 管路阻⼒Compliance calibration 顺应性校准Is water in humidifier ? 湿化器内是否有⽔If yes : press ACCEPT : if no : press CLEAR若有,请按确认键;若没有,请按清除键To exit : touch EXIT SST 退出,触摸“退出SST”键。
机械通气最基础的名词解释
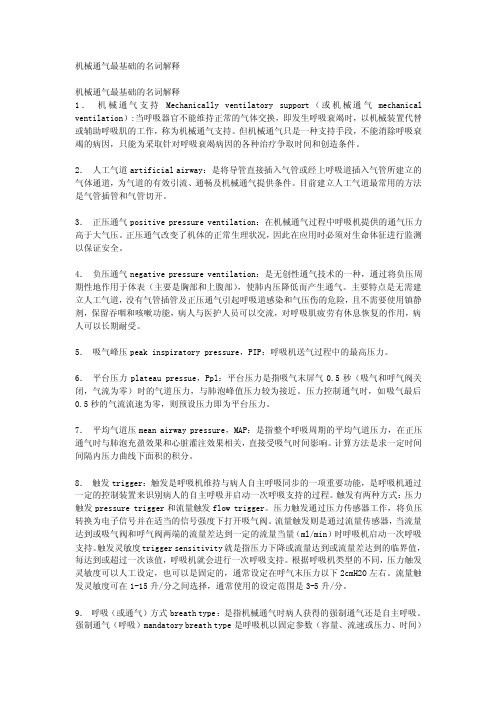
机械通气最基础的名词解释机械通气最基础的名词解释1.机械通气支持Mechanically ventilatory support(或机械通气mechanical ventilation):当呼吸器官不能维持正常的气体交换,即发生呼吸衰竭时,以机械装置代替或辅助呼吸肌的工作,称为机械通气支持。
但机械通气只是一种支持手段,不能消除呼吸衰竭的病因,只能为采取针对呼吸衰竭病因的各种治疗争取时间和创造条件。
2.人工气道artificial airway:是将导管直接插入气管或经上呼吸道插入气管所建立的气体通道,为气道的有效引流、通畅及机械通气提供条件。
目前建立人工气道最常用的方法是气管插管和气管切开。
3.正压通气positive pressure ventilation:在机械通气过程中呼吸机提供的通气压力高于大气压。
正压通气改变了机体的正常生理状况,因此在应用时必须对生命体征进行监测以保证安全。
4.负压通气negative pressure ventilation:是无创性通气技术的一种,通过将负压周期性地作用于体表(主要是胸部和上腹部),使肺内压降低而产生通气。
主要特点是无需建立人工气道,没有气管插管及正压通气引起呼吸道感染和气压伤的危险,且不需要使用镇静剂,保留吞咽和咳嗽功能,病人与医护人员可以交流,对呼吸肌疲劳有休息恢复的作用,病人可以长期耐受。
5.吸气峰压peak inspiratory pressure,PIP:呼吸机送气过程中的最高压力。
6.平台压力plateau pressue,Ppl:平台压力是指吸气末屏气0.5秒(吸气和呼气阀关闭,气流为零)时的气道压力,与肺泡峰值压力较为接近。
压力控制通气时,如吸气最后0.5秒的气流流速为零,则预设压力即为平台压力。
7.平均气道压mean airway pressure,MAP:是指整个呼吸周期的平均气道压力,在正压通气时与肺泡充盈效果和心脏灌注效果相关,直接受吸气时间影响。
有创正压机械通气

压力(cmH2O) 预设压力 支持水平
流速(LPM) 峰流速
PSV:压力限制、流速切换
吸气时间
时间(s)
25%峰流速 时间(s)
容量SIMV
压力(cmH2O)
6秒
6秒
PSV
PSV
时间 (s)
SIMV
SIMV
♪触发窗概念:指令通气前,呼吸周期的25%。 如10次SIMV,则触发窗为1.5s
SIMV
呼吸机自动显示
呼吸机自动显示 or 吸气末阻断法测定
呼吸机自动显示
内源性PEEP(autoPEEP)
呼气末阻断法测定
平均气道压(Pmean)
❖ 呼吸系统顺应性(C) ❖ PEEP(外源性) ❖ 气道峰压(PIP) ❖ 吸气时间(Ti)
♪ 对一名个体而言,决定平均气道压最重 要的因素是PEEP
内源性PEEP(PEEPi/PEEPauto)
流速(LPM) 方波
平均流速 (LPM)= 潮气量(升)/ 吸气时间(秒)×60(秒)
吸气峰流速 (PIF)
减速波
正弦波
时间(s)
♪常用为方波和减速波。目前没有证据说明各种吸气流速波形之间有优劣区别
♪吸气流速范围:60~100L/min
♪COPD和重症哮喘患者应给予高吸气流速(80~100L/min),通过提高吸 气流速来降低呼吸功,缩短吸气时间,呼气时间延长,有效对抗PEEPi
对抗PEEPi的方法
❖ 加用外源性PEEP≈85% PEEPi ❖ 提高吸气流速,延长呼气时间(Te)的绝对值 ❖ 减少潮气量(VT) ❖ 降低气道阻力:解痉平喘、充分吸痰、大口径插管
外源性PEEP≈85% PEEPi
❖ 如何测定PEEPi 1)呼吸机“呼气暂停”键(expiration hold):不准确 2)食管内压测定
新生儿机械通气参数调节

Positioning is critical Poor sensitivity, artifacts
二、机械通气的监测
监测项目
1、临床表现:自主呼吸
2、血气分析:PaO2,PaCO2,pH
3、胸
片:肺部病变吸收情况
4、呼吸力学:反应最早
波形和环给您第三只眼睛 实时了解肺力学的变化
肺功能波型及图形监测
(二)呼气末压(PEEP)
调高PEEP:肺泡实变,肺水肿
RDS, 5 – 6 cmH2O 肺出血,6 – 8 cmH2O 调低PEEP:吸入性肺炎、肺气肿
一般 3 cmH2O
(二)呼气末压(PEEP)
高PEEP,导致肺泡过度扩张,气漏 早产儿,尤其是超低体重儿PEEP不能太高!
RDS患者非均匀性的肺泡
Volume (mL)
Paw (cm H2O)
Preset PIP
肺过度膨胀
A = inspiratory pressure
B = upper inflection point C = lower inflection point0Leabharlann 4VTLITERS
0.6
A
0.2
B
Paw
cmH2O
C
-60 -40 -20 0 20 40 60
A
DANGER!!!
Low FRC due to atelectasis Poor lung compliance, hypoxemia
压力
PIP太高, PEEP适当
E I
VT
FRC P CCP COP
!
压力
PEEP
Friend or Foe?
V
VT FRC 2 FRC 1 Delta P P
压力容器常用英语词汇
分类 classification design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design head head head head head peak stress pressure pressure setting
序号 No. 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94
分类 classification design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design design allowance for abrasion
热值仪中文说明
List of Illustrations------------------------------------------------------------- v
Chapter 1-------------------------------------------------------------------------- 1
符号
文件符号定义
标签
说明
WARNING
包括条件、惯例和步骤必须谨慎执行, 以防人员伤害和设备损坏。
CAUTION
包括条件、惯例和步骤必须谨慎执行, 以防人员伤害和设备损坏
CAUTION
电击或高温部分危险,如不采取适当的 警告,可导致人员伤害。
CAUTION
静电感应元件,要求正确地触摸,以防 损坏。
Flo-Cal 用户手册
ii 索引
Chapter 4 --------------------------------------------------------------------------17
Installation ....................................................................................................... 17 System Mounting .............................................................................................. 17 Unpacking and Inspection .................................................................... 17 Wall Mount Preparation and Procedure ............................................... 18 Free Standing Mount Instructions ........................................................ 20 Electrical Installation......................................................................................... 21 Gas & Air Supply Installation ........................................................................... 22
呼吸机波形分析
容量控制通气 1、Pressure-Time, 2、Flow-Time 3、Volume-Time Curves
Normal Time-based Curves(2)
压力控制通气 1、Pressure-Time, 2、Flow-Time 3、Volume-Time Curves
1、CPAP Mode 2、Assisted-Mode (Volume-targeted ventilation) 3、SIMV Mode 4、SIMV + Pressure Support 5、SIMV+PS+PEEP
1、CPAP Mode
CPAP mode :自主呼吸模式,仅有Pressure-Time Curves中设定基线水平 观察:基线水平5 cm H2O 、以及病人旳触发triggering
Flow-Volume Loops(2)
2、Increased resistance ——气道阻力增长 体现:呼气峰流速降低,呼气轨迹内陷。支气管扩张剂能够修正这种现象 常见:哮喘
Flow-Volume Loops(3)
3、Air trapping and auto-PEEP 体现:呼气末流速未能回到 0基线,从而产愤怒体陷闭和 auto-PEEP 。但不能定量。 注意: flow-time curve可 以监测到该种现象
原理 流速—时间曲线反应了吸气相和呼气相各自旳流速变化,流速旳单位为升/分(纵轴),而时间单位为秒(横轴),横轴上旳曲线为吸气流速,横轴下旳曲线为呼气流速,呼吸机输送旳容量是流速在时间上积分计算而得且等于流速曲线下面积。
流速 LPM
时间
1
4
5
3、方强p-v 与肺功能
Increased Normal Decreased
Volume (mL)
Paw (cm H2O)
Preset PIP
Overdistension
With little or no change in VT
Normal Abnormal
Volume (ml) Pressure (cm H2O)
Paw rismp x Flow
胸廓顺应性
dP = dV / Ccw
阻力和回缩力
动态特性
dP = dV / Cdyn
阻力
dPresistive = R x Flow
静态顺应性
dPdistensive = dV / Cst
dP = dPresist. + dP dist. dP = R x Flow + dV / C st
弥散
分子运动 浓度梯度
O2
CO2
灌注
三向弹簧
胸膜腔压力
呼吸道模型
管道 + 气囊的模型 气道 (管子) 肺泡 (气囊)
研究模型
近气道压
气管压
胸膜压
肺泡压
顺应性
Volume
D V C= D P
DV
DP
Pressure
静态和动态顺应性
Volume
静态顺应性曲线
TV 动态顺应性曲线
COMPLIANCE
Increased Normal Decreased
Volume (mL)
Paw (cm H2O)
PIP levels
Lung Compliance Changes and the P-V Loop
VT levels
Overview of Mechanical Ventilatory Support and Management of Patient

/cgi/external_ref?link_type=PERMISSIONDIRECT Personal use only. For copyright permission information:Published online © 2011 American Association of Critical-Care Nurses doi: 10.4037/ccn20115952011;31:30-44Crit Care Nurse Irene Grossbach, Linda Chlan and Mary Fran Tracyand Ventilator-Related ResponsesOverview of Mechanical Ventilatory Support and Management of Patient-/subscriptions/Subscription Information/misc/ifora.xhtml Information for authors/ccn Submit a manuscript/subscriptions/etoc.xhtml Email alertsby AACN. All rights reserved.© 2011 ext. 532. Fax: (949) 362-2049. Copyright 101 Columbia, Aliso Viejo, CA 92656. Telephone: (800) 899-1712, (949) 362-2050,Association of Critical-Care Nurses, published bi-monthly by The InnoVision Group Critical Care Nurse is the official peer-reviewed clinical journal of the Americanpatient-ventilator dyssynchrony.Responsibilities related to ventilator management may vary among acute care settings, but the nurse is usually the “first-line manager” challenged with patient- and ventilator-related problems. As a result, it is essential that nurses thoroughly understand the basics of ventilator support,including ventilator modes, settings,and alarms. It is also important to be skilled in promptly identifying and managing common patient-and ventilator-related problems in order to provide optimal patient-centered care and prevent compli-cations. Prompt recognition of problems and action by the nurse may resolve acute respiratory distress,dyspnea, and increased work of breathing and prevent adverse events. The purpose of this article is to present an overview of mechanical ventilation modes and the assess-ment and management of dyspnea and patient-ventilator dyssynchrony.Strategies are presented to manage patients’ responses to mechanical ventilatory support. Finally,Irene Grossbach, RN, MSN Linda Chlan, RN, PhDMary Fran Tracy, RN, PhD, CCNSOverview of Mechanical Ventilatory Support and Management of Patient- and Ventilator-Related Responsesmon therapy in subacute and long-term care settings. The primary goals of mechanical ventilatory support are to normalize arterial blood gas levels and acid-base imbalance by providing adequate ventilation and oxygenation.Mechanical ventilation can decrease the patient’s work of breathing by unloading respiratory muscles in a synchronous manner.1Mechanical ventilation can also maintain long-term respiratory support of patients with chronic ventilatory problems.Critical care nurses encounter numerous issues related to ventila-tor support, including physiological conditions that impede optimal ventilator function, dyspnea, andMechanical ventila-tory support is routinely needed for critically ill adults in inten-sive care units and is also a com-Nurses must be knowledgeable about the function and limitations of ventilator modes, causes of respiratory distress and dyssynchrony with the ventilator, and appropriate management in order to provide high-quality patient-centered care.Prompt recognition of problems and action by the nurse may resolve acute respira-tory distress, dyspnea, and increased work of breathing and prevent adverse events.This article presents an overview of mechanical ventilation modes and the assess-ment and management of dyspnea and patient-ventilator dyssynchrony. Strategies to manage patients’ responses to mechanical ventilatory support and recommenda-tions for staff education also are presented. (Critical Care Nurse.2011;31[3]:30-45)©2011 American Association of Critical-Care Nurses doi: 10.4037/ccn2011595This article has been designated for CE credit.A closed-book, multiple-choice examination follows this article, which tests your knowl-edge of the following objectives:1. Differentiate various (common) modes of mechanical ventilation2. Identify management strategies for patient responses to mechanical ventilatory support3. Discuss assessments and causes of patient-ventilator dyssynchronyCE Continuing Education30C riticalC are N urse Vol 31, No. 3, JUNE 2011Featurefor more in-depth information.1-10percent oxygen, tidal volume and/ormizing patients’ care to meet the overall oxygenation and ventilation goals, maintain safe lung pressures,and provide breathing comfort (Table 1).Mode of ventilation refers to the method of inspiratory support provided by the mechanical ventila-tor. It is the specific combination of breathing pattern and control variables to deliver inspiration.4Selection of mode is based on the clinician’s familiarity and experienceIrene Grossbach has practiced as a pulmonary clinical nurse specialist for 28 years and is an adjunct assistant professor in the school of nursing at the University of Minnesota in Minneapolis.Linda Chlan is an associate professor in the school of nursing at the University of Minnesota in Minneapolis.Mary Fran Tracy is a critical care clinical nurse specialist at the University of Minnesota Medical Center, Fairview in Minneapolis.AuthorsCorresponding author: Irene Grossbach, RN, MSN,3043 East Calhoun Parkway, Minneapolis, MN 55408 (e-mail:igrossbach@).To purchase electronic or print reprints, contact The InnoVision Group, 101 Columbia, Aliso Viejo, CA 92656.Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; e-mail, reprints@.C ritical C are N urse Vol 31, No. 3, JUNE 201131and the institutional preferences.11 Some modes guarantee a constant volume (volume-targeted or volume-controlled) with each machine breath, whereas other modes guarantee a constant pressure (pressure-targeted or pressure-controlled). An additional option on some ventilators is a dual-controlled mode that combines the features of volume- and pressure- targeted ventilation to ensure a mini-mum tidal volume (V t) or minute ventilation (V·E) while limiting pres-sure. Table 2 summarizes differences between volume- and pressure- targeted ventilation.Volume-Targeted ModesIn a volume-targeted mode, V t is the targeted parameter, and a fixed V t is delivered with each breath. Volume-targeted modes are the most com-monly used modes.12The mode may be labeled by different names, includ-ing controlled mandatory ventilation, continuous mandatory ventilation, and assist/control mode ventilation.In volume-targeted modes, the ventilator delivers machine-guaranteed breaths at the set respiratory rateand V t if the patient is not makingrespiratory efforts due to sedation,paralysis, or other factors affectingdrive to breathe. For example, if theclinician sets the V t at 600 mL andthe respiratory rate at 10 breaths perminute, the V·E delivered is 6 L/min(600 mL ×10 breaths per minute).The ventilator sensitivity dial iscommonly set so that it takes mini-mal effort (-1 to -2 cm H2O) for thepatient to trigger the machine breath.If the patient is making inspiratoryefforts, inspiration is triggered andthe machine delivers additionalmachine breaths at the set V t. Theinspiratory flow rate, or the speedat which the breath is delivered, isfixed; therefore, it does not changeto match the patient’s respiratoryrate and breathing pattern.Studies have shown that patients’work of breathing can be substantialin assist/control mode, occurringthroughout the inspiratory phase,especially if the patient is air hungryand the inspiratory flows providedby the ventilator are low.2The patientis dependent upon the clinician toreadjust the flow rate setting todecrease work of breathing. Forexample, a patient who breathesfaster requires adjustment to ahigher flow rate to match inspira-tory efforts. If the flow rate doesnot match inspiratory efforts, it iscommon for the patient to experi-ence shortness of breath, anxiety,and agitation and for various othersigns and symptoms of increasedwork of breathing to develop.Immediate adjustment to an appro-priate flow rate setting may be thekey intervention that prevents oralleviates breathing discomfort.Pressure-Targeted ModesPressure is the ventilator’s tar-geted parameter in pressure sup-port ventilation. Breaths in thismode are triggered by the patientand augment or support a patient’sspontaneous inspiratory effortwith a preset positive pressurelevel. Inspiration ends after deliv-ery of the set inspiratory pressure.Two pressure-targeted modes are32C ritical C are N urse Vol 31, No. 3, JUNE common: pressure support ventila-tion and pressure control mode.Pressure Support Ventilation.In pressure support ventilation, vol-ume is variable, rather than a fixed V t as in volume-targeted modes, and is determined by the patient’s effort or drive, preset pressure level, and various airway resistance and lung compliance factors. Flow rate is also variable, depending on the patient’s needs and not fixed by a clinician as it is in volume-targeted modes. The clinician does not set a respiratory rate setting, and the mode does not function if the patient is apneic. Although pressure sup-port ventilation is commonly thought of as a weaning mode with low pres-sure support levels set to overcome resistance in the endotracheal tube and ventilator circuit, high pressure support levels may also provide almost total ventilator support.13 Pressure Control Mode.Pressure control ventilation operates in a manner similar to pressure support ventilation in that it relies on a pre-set pressure to determine the vol-ume delivered and volume is variable depending on various factors that affect airway resistance and/or lung compliance. However, in pressure control mode, a respiratory rate is set by the clinician in order to sup-port patients with apnea or an unre-liable respiratory drive. Pressure control mode may be used in patients with acute respiratory distress syn-drome to control plateau pressures and V t. Patients with acute respira-tory distress syndrome have low lung compliance; therefore, inappropri-ately high V t and pressure settings can overstretch and injure the lung. Current strategies in such patients should be focused on limiting V t and maximal lung stretch. An initialV t of 6 mL/kg ideal body weight is areasonable starting point and maybe decreased to maintain maximallung distending pressures less than30 to 35 cm H2O.14,15Dual-Controlled ModesNewer ventilators offer hybridmodes that combine features ofvolume-targeted and pressure-targeted ventilation in an attemptto avoid both the high peak airwaypressures of volume ventilation andthe varying tidal volumes that mayoccur with pressure ventilation.2Volume and pressure control vari-ables adjust automatically to ensurea minimum V t or V·E. Several manu-facturers incorporate this mode intheir ventilators, with manufacturersusing different names for the samedual-controlled modes. Examples ofthis type of mode are pressure-regulated volume control (Servo300 and Servo-I, AVEA, CareFusion,San Diego, California) and volumeventilation plus (Puritan Bennett840, Covidien Puritan Bennett,Boulder, Colorado). Pressure-targetedlogic is used when the ventilatordetermines after each breath if thepressure applied to the airway wasadequate to deliver the desired V t.If the V t did not meet the set tar-get, the ventilator adjusts the pres-sure applied on the next breath.With some modes, such as volume-assured pressure support ventilation(Bird 8400 Sti, CareFusion) andpressure augmentation (BEAR 1000,CareFusion), inspiratory support isprovided in the same manner as inpressure support ventilation, butthe inspiratory pressure is adjustedwithin the current breath to obtainthe assured V t if the set V t is notbeing achieved.3,12Although thistechnology seems promising, objec-tive evidence has not shown thatany of the alternative methods ofventilation are more successful thanconventional mechanical ventilationwith proper attention to V t. Nofindings from randomized trialsindicate improved outcomes,including mortality.16Other ModesSynchronized Intermittent Manda-tory Ventilation (SIMV) Plus PressureSupport.Two modes are in opera-tion on the SIMV plus pressure sup-port mode: mandatory breaths arevolume-targeted and spontaneousbreaths are pressure-targeted. Thepatient receives a preset number ofvolume-targeted mandatory breathsat a set V t. For example, if the SIMVrate is set at 4 breaths per minuteand the V t at 600 mL, the patientreceives the mandatory V t of 600mL and 4 breaths, resulting in a V·Eof 2400 mL/min (600 mL ×4 breathsper minute). Between mandatorybreaths, the patient breathes spon-taneously on pressure supportedbreaths. The ventilator recognizesspontaneous breaths and deliversmandatory breaths only betweenthe spontaneous breaths, therebypreventing competition betweenthe 2 breath types. Pressure supportis routinely provided in SIMV modeto overcome circuit and tube resist-ance, thereby preventing increasedwork of breathing on the sponta-neous breaths. If the patient is nottaking spontaneous breaths whileon a low SIMV rate, it is essential toincrease the SIMV rate or switch toa full support mode like continuousmandatory ventilation in order toachieve adequate minute ventilation. C ritical C are N urse Vol 31, No. 3, JUNE 201133Continuous Positive Airway Pressure (CPAP).CPAP refers to delivery of a continuous level of positive airway pressure main-tained throughout the respiratory cycle. The ventilator does not pro-vide breaths during CPAP; the patient must initiate all breaths. Ifa patient is on CPAP of 5 cm H2O,5 cm of positive pressure is applied to the airway on inspiration and expiration. CPAP, similar to posi-tive end-expiratory pressure (PEEP), is used to restore and maintain the amount of air left in the lungs at end expiration, or func-tional residual capacity. The appli-cation of positive pressure to the airways during expiration may keep alveoli open and prevent early closure during expiration. The presence of an artificial airway allows intrathoracic pressure to decrease to zero, which is below the usual level of intrathoracic pressure. PEEP/CPAP levels of5 cm H2O are often used to provide “physiologic PEEP.”17CPAP may be used as a last step in the process of discontinuing mechanical ventila-tion. It is also used as a noninvasive method of providing a pneumatic splint to the airways in patients with obstructive sleep apnea.3,11 Opening the airways with positive pressure prevents the upper airway from collapsing with each breath.A thorough understanding of the ventilator being used, includ-ing delivery modes, function of settings, and specific patient set-tings assists in appropriately evaluating and managing patients’responses. This understanding can allow nurses to more quickly troubleshoot problems when they arise.Patient- and Ventilator-Related ProblemsGeneral Considerations andTroubleshooting InterventionsPatients not tolerating mechani-cal ventilation support may beworking to breathe and appear anx-ious, restless, agitated, and in respi-ratory distress. They may try to talkand sit up to improve breathingcomfort. The ventilator may appearto be “out of sync” with breathingefforts, and ventilator alarms maysound. Usual signs and symptomsof problems may not be observed ifpatients are sedated, unconscious,paralyzed, or experiencing neuro-muscular weakness. It is essential toappropriately set and interpret ven-tilator alarms and to promptly iden-tify and correct patient- and/orventilator-related problems. Table 3provides a detailed list of physiolog-ical, psychological, and ventilatorfactors that contribute to respiratorydistress and focuses on interventionsfor optimal care of all ventilator-dependent patients.The troubleshooting process isguided by the severity of the distressand the stability of the patient’scondition. If the patient is in severeacute respiratory distress or is hemo-dynamically unstable, the patientshould be immediately disconnectedfrom the ventilator and manuallyresuscitated with 100% oxygen. Ifthe patient quickly improves withmanual resuscitation, the likelyproblem is the ventilator settings orcircuit.12When the patient appearsanxious or short of breath, or if ven-tilator alarms sound, it is importantto make immediate, systematicassessments. The initial focus shouldbe patient-centered and not machine-centered. It is important to avoidthe false sense of security that,because the patient is supported bythe ventilator, he/she is receivingadequate ventilation. The ventilatoralarm can be silenced for up to 2minutes, during which the nursecan perform an assessment. Thepatient should be assessed forhemodynamic stability, adequateoxygenation, excess secretions,secure tubing connections to theventilator, and other conditionssuch as anxiety or pain. Furtherassessments of the ventilator asneeded include verification thatventilator settings and ventilatorfunction are appropriate and con-fir m a t ion that connections aresecure and tubings are not kinked.Alarm silencing once or repeatedalarm silencing without evaluatingand correcting the problem maycause prolonged periods of inade-quate ventilation. Sedated or para-lyzed patients may be severelyhypoventilated and in deterioratingcondition but not exhibit signs ofrespiratory distress because of theeffects of sedative and other med-ications and conditions that bluntthe normal responses to hypoxemiaand hypercapnia. Patients may beunable to communicate distressthrough facial expressions and ges-tures. Pulse oximetry measurementsof oxygen saturation (Sp O2) mayremain greater than 90%, despitesevere hypoventilation. If the patientinitially has a high Sp O2(eg, 98%),but is hypoventilated and respira-tory acidemia develops, Sp O2meas-urements will decrease but maycontinue to be 90% or greater. Staffmay be comfortable with the valueand not question why the Sp O2decreased from 98% to 90%. As theSp O2reading decreases, the F IO234C ritical C are N urse Vol 31, No. 3, JUNE C ritical C are N urse Vol 31, No. 3, JUNE 201135may be increased without analyzing and correcting the underlying prob-lems that are causing the oxygen desaturation, such as inadequate ven-tilation. Hypoventilation may result in both hypoxemia and hypercapnia.The resulting severe acute respiratory acidemia can lead to decreased blood pressure, cardiovasculardecompensation, and cardiac arrest.Factors Influencing Volume Delivery Targets.The ability of the ventilator to deliver the preset tidal volume is influenced by the amount of pres-sure required to deliver that vol-ume. Peak airway pressure, or force required to deliver the preset V t , is variable and increases with increased airway resistance, decreased lung compliance, and factors that make it difficult for the chest wall toexpand. Increased airway resistance describes mechanical factors that narrow the airway and impede the flow of inspired air to the lungs.Increased airway resistance can be caused by a smaller diameter endo-tracheal tube, biting on the endo-tracheal tube, obstruction withsecretions, and bronchospasm. Faster respiratory rates also increase resist-ance because of greater air turbulence.Lung compliance measures the ease of expansion of the lung and thorax. Decreased lung compliance requires more pressure to deliver volume and expand the lung because of various conditions including atelectasis, pulmonary edema,fibrosis, and pneumonia. Chest wall or extrapulmonary factors that con-tribute to increased peak airway pres-sure include certain positions that may restrict expansion of the chest wall and lung, abdominal distention,forced abdominal muscle contrac-tions, and shivering (Figure 1).20Asairway resistance increases or lung compliance decreases, the peak inspiratory airway pressure increases to deliver the preset V t . The preset V t is delivered unless the specified upper airway pressure alarm limit is reached. At that point, the ventila-tor stops delivery of volume.Loss of the preset volume occurs if an air leak develops in the endo-tracheal or tracheostomy tube cuff or the ventilator system. A low vol-ume alarm sounds if the V t or V·E is less than the preset low volume limit set by the clinician. With volume losses, it is common for patients to exhibit anxiety, restlessness,increased work of breathing, and other signs and symptoms of acute respiratory distress. It is essential to correct airway resistance and/or lung compliance problems to main-tain V t delivery.Factors Influencing Pressure Delivery Targets.Tidal volume in pressure-controlled modes is vari-able and changes with various fac-tors that affect airway resistance and/or lung compliance. For exam-ple, the set pressure used to provide adequate V t and breathing comfort may become inadequate if the patient develops mucous plugs or bron-chospasm, resulting in respiratory36C ritical C are N urse Vol 31, No. 3, JUNE 2011Figure 1Factors that increase airway resistance and decrease lung compliance.Reprinted from Grossbach 20with permission.Factors that decrease lung compliance • Pulmonary edema (cardiac, noncardiac)• Pneumonia • Atelectasis• Endotracheal tube displacement • Pneumothorax“Extrapulmonary” factors • Positions restricting expansion• Forced abdominalcontractions on expiration • Increased abdominal pressure against diaphragm due to ascites, gas distention • Shivering, other muscle contractions • Chest wall injury, malformationFactors that increase airway resistance • Biting down on tube• Endotracheal tube obstructed,narrowed, displaced • Cough • Secretions • Bronchospasm• Fast respiratory rate[distress and potential cardiopul-monary deterioration if the problem is not resolved. A sudden resolution of the resistance or compliance problem may increase V t to an amount larger than desired. Clini-cians must be alert to monitoring the patient’s V t and properly setting V t and V·E alarm limits, and be pre-pared to make frequent ventilator adjustments when managing a patient whose pulmonary status may change rapidly, as in acute asthma or pulmonary edema. Volume-targeted or dual-controlled strate-gies are favored to maintain a con-stant V t in situations where the patient has frequent changes in air-way resistance or pressure.12Pressuresupport ventilation is contraindi-cated if the patient is apneic or has an unreliable ventilatory drive due to central nervous depression from drugs or other situations.18Dyspnea.Dyspnea is described in many ways, including feeling short of breath, having difficult or uncomfortable breathing, feeling breathless, running out of air, “hard to breathe,” “can’t get a deep breath,”“can’t breathe,” feel like suffocating, a heavy chest, or “chest tightness.”It is frequently described as air hunger, choking, or heavy breath-ing.21,22In general, only patients with chronic obstructive pul-monary disease, but not healthy individuals, volunteered affective words such as “frightening,” “wor-ried,” “helpless,” “depressed,” and “awful” to describe their breathing difficulty.22These affective descrip-tions are intended to convey the threat perceived by the patients to their breathing difficulty.23,24Various clinical conditions con-tribute to dyspnea.25,26Common situations or events can trigger acycle of anxiety, agitation, frustration,fear, helplessness, and dyspnea.Examples include inability to com-municate needs, unclear or inade-quate explanations from caregivers,and inappropriate ventilator modesor settings that do not match thepatient’s respiratory demands. Evensmall losses in V t can cause signifi-cant acute respiratory distress. Bron-chospasm may worsen in patientswith chronic obstructive pulmonarydisease or asthma or in other sus-ceptible patients, which furtherincreases airway resistance, work ofbreathing, and shortness of breath.Increased work of breathing mayincrease anxiety, stress, and oxygenrequirements and may result inhypoxemia and respiratory acidemiaif the patient does not receive appro-priate intervention (Figure 2).18Signs of respiratory distressinclude increased respiratory rate,changes in mental state, anxiety,restlessness, distressed appearance,nasal flaring, making attempts tobreathe through the mouth, diaphore-sis, sitting upright or attempting tosit up in bed, use of accessory mus-cles in the neck, and forced abdomi-nal muscle contractions duringexpiration. Blood pressure andheart rate may or may not changesignificantly, depending on thevasoactive medications the patientis receiving. Also, patients who areheavily sedated or experiencingsevere muscle weakness or non-chemical paralysis will not exhibitthe increased respiratory muscleactivity normally observed. Respira-tory distress and increased work ofbreathing may be caused by a com-bination of factors related to thepatient and factors related to theequipment: air leaks, increased air-way resistance, decreased lung com-pliance, inadequate ventilatorsettings, and anxiety or pain.A patient-centered approach tooptimal ventilator managementshould include routine assessmentfor dyspnea27by using an appropriateinstrument for assessing dyspnea.25 C ritical C are N urse Vol 31, No. 3, JUNE 201137dyssynchrony, a common cause of dyspnea and respiratory distress.Patient-Ventilator DyssynchronyPatient-ventilator dyssynchrony is defined as a situation in which the patient’s breaths fail to coincide or match exactly with the ventilator-assisted breaths. This common phenomenon can affect patients’outcomes, including duration of mechanical ventilation 31-35and hos-pital length of stay.36Patients exhibit various signs and symptoms of respiratory distress when the ventilator is not appropri-ately configured to meet the patient’s inspiratory and expiratory demands.Sensations of “fighting the ventila-tor,” being out of sync, and working to breathe are due to dyssynchrony between the patient’s respiratory efforts and the ventilator. A nurse’s first inclination may be to encourage the patient to “calm down,” “relax,”slow your breathing,” and “breathe with the machine” rather than adjusting the ventilator to match the patient’s demands, clearing the airway of secretions, or determin-ing what the patient is trying to communicate in efforts to meet other needs, such as pain or a strong desire to see a family member.Dyssynchrony often is serious during all 3 phases of breath delivery:the trigger phase, the flow delivery phase, and the breath cycling off phase.31To achieve patient-ventilator synchrony, the ventilator must sense and respond quickly to inspiratory efforts, provide inspiratory flow of oxygen gas that matches the patient’s inspiratory demands, terminate the breath with the patient’s termination of inspiration, and cycle to expirationto match the patient’s exhalation phase. To optimize patients’ com-fort and reduce the work of breath-ing, it is crucial that the machine be adjusted to meet the patient’s requirements, including appropri-ate trigger sensitivity settings, inspi-ratory flow, inspiratory time, V t ,and an exhalation phase that matches the patient’s expiratory pattern. The patient is dependent upon the nurse to make accurate observations of the ventilator inter-face. Simple observations of the ventilator being “in sync” with the patient’s efforts show easy ability to trigger the ventilator breath, deliv-ery of the breath coinciding with inspiration, appropriate breath ter-mination when the patient appears to stop inspiration, and the ventila-tor exhalation phase properly timed to coincide with when the patient appears to be exhaling. The patient appears comfortable, conveys breathing comfort, and is able to rest and sleep. Causes for and man-agement of patient-ventilator dys-synchrony are described next.Causes of DyssynchronyAppropriate ventilator modes must be selected and settings adjusted to match and be in syn-chrony with the patient’s inspira-tory efforts. Dyssynchrony may be due to delayed or ineffective trigger-ing, auto-triggering, insufficient flow to meet the patient’s demands, dou-ble triggering, and an exhalation phase that is out of sync with the patient’s breathing pattern (Table 4).Delayed or Ineffective Triggering.The most common cause of dyssyn-chrony is ineffective triggering,37which is defined as failure of the patient’s inspiratory muscle effort38C ritical C are N urse Vol 31, No. 3, JUNE 2011Dyspnea assessment is useful to determine whether ventilator adjustments and various interven-tions, such as positioning, use of a fan, music, or other relaxation tech-niques, improve breathing comfort.One dyspnea evaluation protocol asked responsive patients: “Are you feeling short of breath right now?”and, if yes, “Is your shortness of breath mild, moderate, or severe?”28These 3 broad dyspnea ratings limit patients’ responses to changes in dyspnea. The 2 most common instruments used to measure dysp-nea in critical care are the visual analog scale (VAS) and the Borg scale.25,29The VAS is a 100-mm hori-zontal line with endpoints of 0 (no shortness of breath) and 100 (worst possible shortness of breath). The patient rates the degree of shortness of breath on this line. The modified Borg scale is a 12-item instrument with numbers corresponding to descriptions regarding the amount of dyspnea,14with no dyspnea rated as 0 and worst imaginable dyspnea rated as 10. Correlations between the 2 scales are strong, and validity and reliability have been deter-mined with critically ill patients.30The use of these instruments requires that patients be alert and oriented.Furthermore, each instrument is 1-dimensional; only intensity or dis-tress of dyspnea is measured.25Various physiological, psychological,and equipment factors contribute to dyspnea and acute respiratory distress. Evidence supports best practice in the assessment and man-agement of critically ill patients experiencing dyspnea.25The follow-ing section describes the patient-ventilator interaction, focusing on the causes and management of。
Mode of Ventilation

• Pressure- controlled ventilation
Pressure vs. Volume Ventilation
Pressure vs. Volume Ventilation: Advantages
• • • • • • PC & PSV Variable flow rate Reduced WOB Max Palveolar = Max Pairway (or less) Palveolar controlled Variable P-time & pattern (PS) Better with leaks
Factors that affect volume delivery during pressure ventilation
1. Pressure Setting • ↑ pressure setting → ↑ volume ( vice versa). 2. Pressure Gradient (ΔP) 3. Patient Lung Characteristics • compliance • Raw 4. Inspiratory Time • ↑Ti → ↑ volume delivery . • flow returns to zero before inspiration ends, ↑ Ti doesn’t ↑ volume. 5. Patient Effort • Active inspiration by the patient can increase volume delivery.
Partial Ventilatory Support
• Mechanical ventilation < 6 breaths/mm and the patient participates in WOB to help maintain effective alveolar ventilation. (patient actively participates in ventilation to maintain adequate levels of PaCO2.) • PVS modes might include SIMV, PSV, VS, PAV, MMV. • PVS strategies : • when attempts to discontinue ventilator support. • avoided patients ventilatory muscle fatigue
呼吸机常用专业术语英汉对照

呼吸机常用专业术语英汉对照许峰accumulator贮气箱(装置)adapter接合器,接口adjusting tap调节柄air inlet filter空气输入滤过器airway pressure呼吸道压alarm indicator报警显示alveolar pressure肺泡内压amplifier增幅唇apnea呼吸暂停apnea indicator呼吸暂停显示装置assembly装置、组合assist/control mode,A/C辅助/控制通气back—up ventilation备用通气bacterial filter细菌滤过器bag囊ballon valve球囊式活瓣bellows风箱bleed regulator排气调节器blower鼓风机calibration校准、定标chamber腔check valve单向阀compensator代偿装置compressor压缩器、压缩装置continuous positive airway pressure(CPAP)持续呼吸道正压continuous flow持续气流control knob调节炳cooling fan冷却扇corrugated hose螺纹管、呼吸管道crossover soleniod交通电磁阀delay dial廷迟设定demand flow按需气流demand valve按需供气阀diaphragm隔膜digital ampli~r数字型增幅器drive system驱动系统electrical switch电子开关electrodynamic valve电动阀exhaled gas呼出气exhalation time呼出时间exhalation valve呼出阀exhaust valve气体排出活瓣(阀)expired minute volume呼气分钟通气量feed back servocontrol反馈伺服控制filling solenoid充气电磁阀(气流开关)filter滤过器flap valve平行阀flow control valve流量控制(调节)阀flowrate流速flow transducer流量传感器flow trigger流量触发(器)flush knob冲洗按键gas outlet气体出口gas samping pump气体采样泵gas supply气体供应generated pressure驱动压generator发生器,产生装置heat exchanger热交换器heat(heated)humidifier加热(温)湿化器high frequency ventilation(HFV)高频通气humidifier加湿气infant ventilator婴儿呼吸机inlet输入(口)inspiratory effort自主吸气努力(指示)intermittent positive pressure ventilation(IPPV)间歇正压通气intermittent mandatory ventilation(IMV)间歇指令通气jet喷射,喷射式joint连接器(装置)leak test漏气检查low inspiratory pressure sensor吸气低压传感器low pressure alert低压报警限magnetic valve电磁阀main compressor主压缩装置(泵)main power总电源manifold多歧管manometer压力计(表)manual手动master solenoid主电磁阀master/slave ventilation(MSV)双肺不同通气membrane膜,隔膜microprocessor微处理器microswitch微开关minute volume分钟通气量mixer混合器injector喷射器、射流装置mode模式motor步进电机moisture trap湿气(水分)清除置nebulizer雾化器(装置)needle valve针型阀one—way valve单向阀orifice孔、开口overflow valve满溢阀(活瓣)over—pressure relif valve过压释放阀oxygen percent control氧浓度调节(控制)oxygen sensor氧传感器parameter参数peak hold switch峰压保持键peak flow dial峰流设定plateau平台plunger插塞pneumotachometer气流速度计piston活塞pop of valve过压释放阀positive end expiratory pressure(PEEP)呼气末正压power supply电源preset volume(pressure)预置的容量(压力)pressure controlled ventilation(PCV)压力控制通气pressure gauge压力计、压力测量装置pressure manometer压力计(表)pressure—reducing valve减压阀pressure regulated volume control ventilation(PRVCV)调压容量控制通气pressure regulator压力调节器pressure relief valve压力释放阀pressure support压力支持pressure support ventilation(PSV)压力支持通气pressure transducer压力传感器proportional solenoid比例电磁阀proximal airway line呼吸道压测量联接管ratio率、比值regulator调节器(装置)reservoir hag贮气囊resetkey复原键、恢复键respiratory hag呼吸囊respiratory rate呼吸频率respiratory time吸入时问restrictor气流限制装置reverse flow逆流sensitivity敏感度sensor传感器、测量器sigh pressure息时压力silicone rubber tube硅橡胶管slipjoint滑动关节solenoid电磁阀、电控气流阀(开关)source gas气源spirometer肺活量计spontaneous bag自主呼吸囊spontaneous,spont自主呼吸spring弹簧stopcock气流开关suction吸引support arn1支持臂synchronised intermittent mandatory ventilation(SIMV)同步间歇指令通气synchronised intermittent positive pressure ventilation (SIPPV)同步间歇正压通气temperature sensor温度传感器test lung模拟肺thermister半导体温度计thermometer温度计tidal volume潮气量time preset key时间预调键tranducer传感器trigger level触发水平tubingcompliance管道顺应性variable orifice可变口valve阀、活瓣vent出口ventilation,vent通气ventilator呼吸机、通气机ventilator settings呼吸机设置· 1377·venturi文丘里装置volume controlled ventilation(VCV)容量控制通气volume suppofl ventilation(VSV)容量支持通气water trap除水装置waveform波形wick加湿器的芯子。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
– Flow pattern is always decelerating which provides best distribution in lung
Pressure is set
– Pressure in lung will not change with changing lung characteristics
Auto-PEEP
PCIRC Change PALV Change
Other Parameters
The following parameters have same effect as in VC
– Sensitivity – FiO2
Time Constants
Time Constants (TC)
Inspiratory Time (TI)
PC ventilation is always time cycled Once inspiration starts, the ventilator will
maintain the pressure control level for the length of time set by TI May be set directly as TI or indirectly using RR and I:E ratio
Expiratory Pause
Same as in VC Auto-PEEP will reduce VT during PC
ventilation because
– ∆P is from total PEEP level to PC level – ∆V in the lung (VT) is caused by ∆P in the
When PCIRC = PALV, flow waveform drops to zero flow
Time Constant Calculations
Calculate TC
– Compliance ( C ) = 100 ml/cmH2O – Resistance ( R ) = 1 cmH2O/L/sec
Respiratory Rate (RR)
Sets cycle time same as VC Can be increased by patient triggering TE is what is left of cycle time after TI
which is set
Flow in PC
lung – Ventilator does not “see” auto-PEEP, so
cannot compensate for it
Auto-PEEP Example
PC setting 20 cmH2O PEEP setting 5 cmH2O
– Maximum PALV reached 25 cmH2O – ΔP in the lung 20 cmH2O
– In PC, delivers the set pressure and TI each breath
PC Settings
Pressure control (PC) level Inspiratory time (TI) Rise time (flow acceleration) Respiratory rate (RR) PEEP Sensitivity FiO2 Expiratory pause
Pressure Control (PC) level
Sets the target pressure for inspiration Jumps to PC level at start of inspiration PC level set above 0 or above PEEP
depending on the ventilator
Flow
Time
Effect of Compliance (C) and Resistance (R) on VT
C Effect on VT
PC ventilation sets pressure in circuit VT changes always follow changes in C
With auto-PEEP of 10 cmH2O
– Maximum PALV reached is still 25 cmH2O – Total PEEP in lung 15 cmH2O – ΔP in the lung 10 cmH2O – ΔP is reduced, therefore ΔV (VT) is reduced
Predict PALV = PCIRC
You need greater than (>) 3 TC for the PCIRC = PALV
Calculate 3 TC
Compare TI to see if > 3 TC
– If yes, Palv = Pmouth (PCIRC) – If no, PALV less than (<) PCIRC
– PALV = PCIRC
If TI is less than 3 TC, then increasing R would reduce VT
– PALV further away from reaching PCIRC
Calculate TI for PCIRC = PALV (3 TC) (complete volume (VT) delivery)
– Pressure target 10 cmH2O – What VT will be delivered to the patient?
Time Constant Calculations
Time constants tell us how long it will take for PCIRC (PC level set on ventilator with or without PEEP) and PALV to become equal
1 TC (seconds)= compliance X resistance Compliance ( C ) L/cmH20 Resistance ( R ) cmH2O/L/sec
Flow is not set in PC ventilation Flow results from the difference in
pressure between PCIRC (PC level set on ventilator with or without PEEP) and PALV During inspiration
Slow rise time
– More gradual climb to PC level – More comfortable for patient with less
aggressive breathing – Prevents overshootime
PC Level and TI
Rise Time (flow acceleration)
Different names and different units from different companies
Determines how quickly the PC level is reached
– Not an issue if volume is monitored closely and appropriate changes are made when required
Pressure Control Assist Control (AC)
Pressure targeted, time cycled ventilation Provides full ventilatory support Patient or ventilator can trigger a breath Every breath delivers a mandatory breath
– Increasing C will increase VT – Decreasing C will decrease VT
Increased C will result in lower PALV if TI shorter than 3 TC
– However, increasing C increases length of time constant because of higher VT delivered
Fast vs Slow Rise Time
Fast rise time
– Jumps to PC level quickly – May use if patient is breathing aggressively
requiring high flows in early inspiration
Decreased Compliance
Increased Compliance
R Effect on VT
Remember ΔV in the lung (VT) is result of ΔP in the lung and C
As long as TI is longer than 3 TC, then changing R does not affect VT
▪ Barotrauma less likely
PC with patient effort
Disadvantages of Pressure Control (PC)
Does not maintain a constant tidal volume
– Volume delivered affected by changing compliance and resistance