亚低温治疗缺氧缺血性脑病
亚低温治疗新生儿缺氧缺血脑损伤有疗效
亚低温治疗新生儿缺氧缺血脑损伤有疗效新生儿缺氧缺血性脑病(hypoxic-ischemic encephalopathy, HIE)是指新生儿在围产期(指怀孕28周到产后一周)窒息而导致脑的缺氧缺血性损害。
是因在围生期出现窒息从而导致新生儿的脑部出现缺氧缺血性的损伤,包含神经病变和病理生理病变,部分的患儿还会出现不同程度的神经系统后遗症。
截止到目前为止,新生儿缺氧缺血性脑损伤是造成新生儿和小儿致残的主要疾病之一。
因此现阶段要加强对新生儿缺氧缺血脑损伤的重视程度,通过提高预防和加强治疗的方式来避免因脑损伤造成的死亡和损伤。
婴儿期指一岁以内的小儿,因此在一岁以内的小孩,任何导致婴儿缺氧的因素都可能会引起婴儿缺血缺氧性脑病,这里面主要说,新生儿缺氧缺血性脑病,新生儿缺血缺氧性脑病它的核心是缺氧,缺氧新生儿它分为生前生时和生后,生前缺氧的主要因素是包括,孕母胎盘和胎儿,孕母合并有严重的心肺疾病,孕母有妊高症孕母有糖尿病,孕母严重的营养不良,胎盘的因素,胎盘功能不成熟胎盘过小,脐带受压脐带打劫脐带过长,脐带过细导致胎儿缺氧,胎儿本身的原因,有严重的心脏病,胎儿有严重遗传代谢病,也导致生前新生儿缺氧,生后和生时的新生儿缺氧,也会导致新生儿缺血缺氧性脑病,生时新生儿缺氧可能是生前新生儿,胎儿缺氧的一种延续,也可能是在分娩时因为复苏,不及时或者复苏的措施不得当,或者复苏效果不良引起,新生儿呼吸循环抑制,导致缺氧引起脑损伤,生后新生儿的缺氧,缺血缺氧性脑病的发生几率比较小,主要可能的因素发生误吸或者喉梗阻,或者呼吸道的异常,导致新生儿生后缺氧缺血引起脑病。
新生儿缺氧缺血脑损伤的发病机制分为三个方面:第一脑血流分布不平衡。
缺氧缺血时,全身血流重新分配,血液优先供应一些重要器官,如心、脑、肾上腺等。
尽管脑血流量增加,但并非脑内各区域的供血都均匀增加,首先保证代谢最旺盛的部位,如基底核、丘脑、脑干和小脑等,而在脑动脉终末供血区域仍然是血流分布最薄弱部位。
亚低温护理在新生儿缺氧缺血性脑病中的效果和护理质量评价

亚低温护理在新生儿缺氧缺血性脑病中的效果和护理质量评价发布时间:2023-02-06T07:12:25.319Z 来源:《医师在线》2022年30期作者:张易平[导读] 目的:分析亚体温护理应用于新生儿缺氧缺血性脑病的效果与护理质量评价。
方法:从本院2张易平成都市第一人民医院新生儿病房四川成都610000摘要:目的:分析亚体温护理应用于新生儿缺氧缺血性脑病的效果与护理质量评价。
方法:从本院2019年5月~2021年6月期间收治的缺氧缺血性脑病患儿抽取94例,按照时间段2019年5月~2020年5月为对照组(n=47),2020年6月~2021年6月为试验组(n=47),对照组进行常规护理方法,试验组在对照组基础上使用亚低温护理方法,对比两组干预后的生长发育情况与护理满意度。
结果:试验组生发育情况与护理满意度均高于对照组,两者差异具有统计学方面意义(P<0.05)。
结论:在新生儿缺氧缺血性脑病治疗期间应用亚低温护理措施效果显著。
关键词:新生儿缺氧缺血性脑病;生长发育情况;护理措施新生儿缺氧缺血性脑病主要是因为围生期间由于各种外界因素导致新生儿窒息,从而导致引发该疾病,具有较高的致残率,亚低温护理可以改善患儿的临床症状,保护中枢神经,降低脑组织能量代谢,对疾病发展起到延缓的作用,接下来,本文将就常规护理与亚低温护理方法不同的试验效果做出对比研究:1资料与方法1.1一般资料从我院2019年5月~2021年6月收治的缺氧缺血性脑病患儿抽取94例作为观察对象,按照时间段分配为对照组与试验组,各为47例,对照组男性23例,女性24例,患儿胎龄范围在35~41周,平均孕周为(38.00±1.00)周;试验组男性24例,女性23例,患儿胎龄范围在36~40周,平均孕周为(38.00±0.67)周。
两组对比无明显差异(P<0.05)。
1.2方法对照组:给予常规护理方法:治疗期间遵医嘱为患儿进行基础护理措施,其中包括:输液、测量体温、供氧护理、饮食护理等,24h家口监测患儿生命体征。
亚低温治疗新生儿缺氧缺血性脑病的护理

亚低温治疗新生儿缺氧缺血性脑病的护理[ 07-12-06 13:47:00 ] 作者:庞金玲,刘桂华,于春编辑:studa20【关键词】新生儿缺氧缺血性脑病;亚低温;护理[关键词]新生儿缺氧缺血性脑病;亚低温;护理Nursing of Second Low Temperature Treated HIEKey words: HIE; Second low temperature; Nursing新生儿缺氧缺血性脑病(HIE)是由于围产期窒息导致的脑缺氧和/或缺血而形成的一种新生儿时期最常见的脑损伤疾病,其致死率,致残率较高。
近年来研究表明动物模型中低体温对窒息后的脑损伤有保护作用,亚低温对新生动物缺氧缺血性脑损伤的神经保护作用得到证实[1]。
本科自2003年1月至2004年4月住院的17例新生儿HIE采用头部亚低温治疗,并随访存活者18个月与对照组相比发生脑瘫、癫痫或智力低下后遗症明显降低。
现将治疗组护理报告如下。
1 资料与方法1.1 资料病例按1996年杭州会议制定的新生儿HIE诊断依据及临床分度的标准进行选择。
将35例重度HIE患儿随机分为两组,治疗组17例,男11例,女6例,年龄1 h~12 h;出生体重3.0 kg~3.5 kg 9例,3.5 kg~4.0 kg 6例,>4.0 kg 2例;胎龄37周~40周12例,40周~42周5例。
对照组18例,男8例,女10例;年龄1 h~12 h;出生体重3.0 kg~3.5 kg 7例,3.5 kg~4.0 kg 9例,>4.0 kg 2例;胎龄37周~40周13例,40周~42周5例。
1.2 方法治疗组17例患儿均于入院后施行选择性头部降温。
采用中国人民解放军第六九零四工厂生产的YYM1B型颅脑降温仪,降温帽置于新生儿头部,以鼻咽温度为温控标准,有计算机自动控制调整降温帽水温维持鼻咽温度为(34.5±0.2)℃,维持肛温(36±0.2)℃。
亚低温治疗新生儿缺氧缺血性脑病的护理

亚低温治疗新生儿缺氧缺血性脑病的护理刘素哲;刘翠青;李丽;纪素粉【摘要】Objective: Observation and care of vital sign that selective head cooling with mild hypothermia treating of neonate hyacidepoxic - ischemic en-cephalopathy( HIE ). Methods:To select 50 full - term newborn infant which of severe asphyxia, within 24 hours birth, the patients were randomized in a non -blinded manner to two groups which of 25 patients. The therapy group received by treatment of head cooling with hypothermia,rectal temperature maintained at( 35 ±0.2 )℃ ,head temperature maintained at( 34 ±0. 3 )℃ ,to reduce the temperature maintained 72 hours, control group received conventional therapy. Monitoring parameters of blood pressure,heart,breathing and percutaneous oxygen saturation. The data were to be carry on statistics processing used of statistical analysis SPSS 10.0 statistics software. Results:The therapy group except the heart to descend obviously than control group in 72 hours( P <0.01 ),the rest index were no significant difference. Conclusion:In nursing,except monitoring body temperature,maintained rectal temperature at( 35 ±0.2 )℃ , we also ought to monitoring the change of vital sign.%目的:选择性头部降温治疗新生儿缺氧缺血性脑病时的生命体征的观察与护理.方法:选择重度窒息、生后24 h内的足月新生儿50例,随机分为两组,每组25例.治疗组用选择性头部降温的方法,维持直肠温度在(35±0.2)℃,头部温度维持在(34±0.3)℃,维持头部降温72 h;对照组不进行降温治疗.分别对两组进行心率、呼吸、血压、经皮血氧饱和度监测,用SPSS 10.0统计软件对监测数据进行检验.结果:治疗组除心率在72 h与对照组相比存在明显下降外(P<0.01),其余指标均无显著性差异.结论:在护理上除严密监测患儿的体温、保持直肠温度在(35.±0.2)℃外,还应监测生命体征的变化.【期刊名称】《护理实践与研究》【年(卷),期】2011(008)021【总页数】3页(P65-67)【关键词】新生儿;缺氧缺血性脑病;亚低温【作者】刘素哲;刘翠青;李丽;纪素粉【作者单位】050031,河北省儿童医院新生儿科;050031,河北省儿童医院新生儿科;050031,河北省儿童医院新生儿科;050031,河北省儿童医院新生儿科【正文语种】中文新生儿缺氧缺血性脑病(HIE)是围生期各种因素引起脑缺氧、缺血,所导致的脑损伤综合征,易造成新生儿早期死亡及小儿智能发育障碍、脑性瘫痪和癫痫,是造成儿童中枢神经损伤最常见的原因之一[1]。
亚低温治疗新生儿缺氧缺血性脑病专家共识(2022)重点梳理
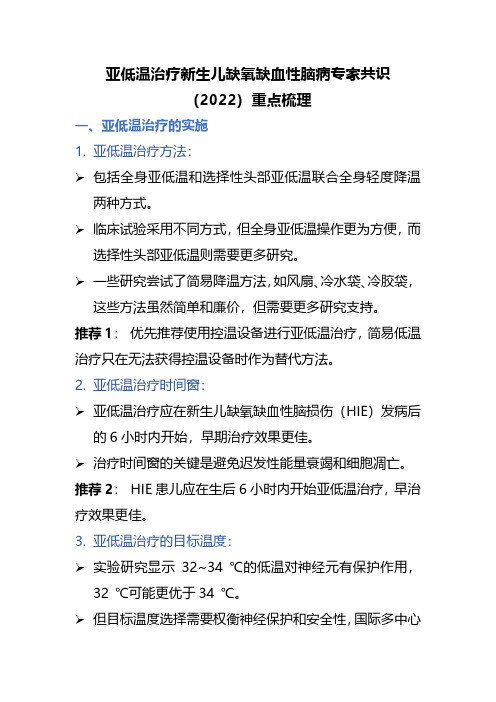
亚低温治疗新生儿缺氧缺血性脑病专家共识(2022)重点梳理一、亚低温治疗的实施1.亚低温治疗方法:➢包括全身亚低温和选择性头部亚低温联合全身轻度降温两种方式。
➢临床试验采用不同方式,但全身亚低温操作更为方便,而选择性头部亚低温则需要更多研究。
➢一些研究尝试了简易降温方法,如风扇、冷水袋、冷胶袋,这些方法虽然简单和廉价,但需要更多研究支持。
推荐1:优先推荐使用控温设备进行亚低温治疗,简易低温治疗只在无法获得控温设备时作为替代方法。
2.亚低温治疗时间窗:➢亚低温治疗应在新生儿缺氧缺血性脑损伤(HIE)发病后的6小时内开始,早期治疗效果更佳。
➢治疗时间窗的关键是避免迟发性能量衰竭和细胞凋亡。
推荐2:HIE患儿应在生后6小时内开始亚低温治疗,早治疗效果更佳。
3.亚低温治疗的目标温度:➢实验研究显示32~34 ℃的低温对神经元有保护作用,32 ℃可能更优于34 ℃。
➢但目标温度选择需要权衡神经保护和安全性,国际多中心研究的目标温度为34 ℃。
推荐3:亚低温治疗的目标温度为34 ℃,允许波动范围在33~35 ℃之间。
4.亚低温治疗维持时间:➢多中心研究采用维持72小时的低温治疗,这种治疗方式在新生儿HIE神经保护上取得了成功。
➢短时间的低温治疗时间(24~72小时)尚未在临床研究中得到证实。
推荐4:新生儿HIE亚低温治疗的持续时间为72小时。
5.复温方法:➢关于亚低温治疗后的复温方法尚无充分的临床研究。
➢国际多中心研究采用缓慢复温,复温时间≥5小时,复温速度≤0.5 ℃/小时。
➢快速复温可能引发一系列不良反应,应密切监测患儿并在必要时暂停复温。
推荐5:应采取缓慢复温,复温速度≤0.5 ℃/小时,复温时间≥5小时。
二、亚低温治疗获益人群1.亚低温治疗纳入标准:1)出生胎龄≥35周或36周,出生体重≥2,000克。
2)缺氧缺血证据包括:a)胎儿宫内窘迫的证据,如子宫和/或胎盘破裂、胎盘早剥、脐带脱垂或严重胎心异常变异或晚期减速。
亚低温治疗新生儿缺氧缺血性脑病方案(2011)
1 亚低温治疗新生儿缺氧缺血性脑病( H I E ) 的医生资质 及必备能力要求 应当具备新生儿专业的主治医师及以上职称。①具备 进行神经功能评估( 如意识状态、 肌张力、 原始反射、 惊厥、 脑干体征等) 的能力; 并能具体指导团 ② 具备熟练掌握 ( 并能具体 队) 亚低温治疗流程和复温流程的能力; ③ 具备( 指导团队) 对亚低温治疗期间监护指标及其临床意义有深 刻理解的能力。 2 亚低温治疗新生儿 H I E患儿父母及监护人的知情告知 亚低温治疗新生儿 H I E是一种新的治疗方法, 必须征 得患儿父母及监护人同意并应签署书面的知情同意书。医 生与患儿父母及监护人的谈话内容应记录在病程记录中。 医生应告知: ● 目前多项高质量研究证据表明, 亚低温治疗可以降 低新生儿 H I E的病死率和 1 8个月时严重伤残的发生率, 但 I E患儿家长及监护人可选择, 远期效果不确定。新生儿 H 也可不选择亚低温治疗, 亚低温治疗中也可随时提出终止。 ● 适合进行亚低温治疗的新生儿 H I E是有标准的。 ● 亚低温治疗过程中, 严密监测可能出现的不良反应, 包括①循环系统: 严重心律失常、 严重栓塞、 严重低血压和 肺动脉高压; 凝血功能异常和血小板减少; ②血液系统: ③ 呼吸系统: 低氧血症; 低血糖、 高血糖、 低血钙、 ④代谢紊乱: 低钠血症和高钠血症; 肾功能损害; 破溃、 坏 ⑤ 肝、 ⑥ 皮肤: 死和硬肿。 5 亚低温治疗新生儿 H I E的选择标准 胎龄≥3 6周和出生体重≥25 0 0g , 并且同时存在下列 情况: ①有胎儿宫内窘迫的证据; ② 有新生儿窒息的证据; I E或 a E E G脑功能监测异常的证据。 ③有新生儿 H ● 胎儿宫内窘迫的证据至少包括以下 1项: ① 急性围 生期事件, 如胎盘早剥或脐带脱垂或严重胎心异常变异或
头部亚低温辅治新生儿缺氧缺血性脑病效果观察
我院新生儿科 住院 的中 、重度新生 儿缺氧 缺血性脑病 患儿
1 0例 ,所 有 病例 均于 入 院 时做 头 颅 C 和 B超 ,符 合 我 国 6 T
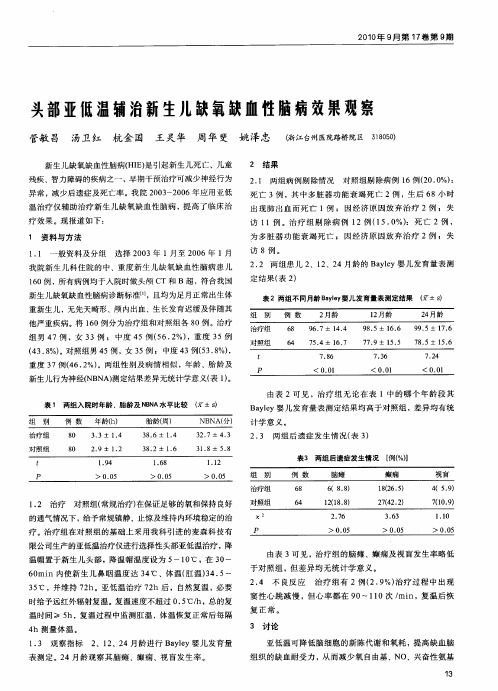
2 2 两 组患儿 2 2 4月龄的 Ba ly婴儿 发育量表 测 . 、1 、2 ye 定结果 ( 2 表 )
表 2两组不 同月龄 B ye 婴儿发育量表测定结果 a ly ( ±s )
超过 0. ℃/ 5 h,总 的复 温时 间 ≥ 5 h,否 则容易 出现低血容 量性休克 ,因此必 须注意新生儿尿量及血压的变化 。 资料 有 显示 ,亚低温治疗 可能会出现高血钾及凝血功能障碍 ,但本
次研究 未发 现。
以上 是 对足 月 新 生 儿 的研 究 ,目前 尚 无对 早 产儿 的 研 究 。亚低 温 治疗 作 为 目前最 有 效 的 非药 物性 脑 保 护措
疗 。治疗组在对 照组的基 础上采 用我科 引进 的麦森科 技有 限公司生产的亚低温治疗仪进行选择性头部亚低温治疗 ,降 温帽置于新生 儿头部 ,降温 帽温 度设为 5 0 ~1 ℃,在 3 ~ 0 6 mi 内使新 生儿 鼻咽温 度达 3 ℃、体温( 温) 4 5 0 n 4 肛 3.~ 3 ℃ ,并维持 7 h。亚低 温治疗 7 h后 ,自然复 温 ,必要 5 2 2 时给予远 红外辐射复温 。复温速度不超过 0 5 h,总的复 . ℃/ 温时间 ≥ 5 h,复温过程 中监测肛温 ,体温恢复正 常后每隔
4 测量 体 温 。 h 1 3 观 察 指标 . 2 2 4月 龄 进 行 B ye 、1 、2 al y婴 儿 发 育 量
由表 3可见 ,治疗 组 的脑 瘫 、癫痫 及视盲 发生率 略低
于对照 组 ,但差 异均无统 计学 意义 。
亚低温治疗仪在新生儿缺氧缺血性脑病治疗中的应用效果分析

亚低温治疗仪在新生儿缺氧缺血性脑病治疗中的应用效果分析引言新生儿缺氧缺血性脑病是新生儿常见的一种危重病,严重影响儿童的生长发育和智力发育。
亚低温治疗是目前治疗新生儿缺氧缺血性脑病的有效方法之一、亚低温治疗仪通过将新生儿的体温控制在较低的水平,减少脑细胞的死亡,降低脑水肿和炎症反应,从而改善患儿的预后。
本文将就亚低温治疗仪在新生儿缺氧缺血性脑病治疗中的应用效果进行详细的分析。
1.亚低温治疗仪的原理和特点亚低温治疗是指将患儿的体温控制在32-34℃之间,维持48-72小时,然后逐渐升温至正常体温。
该治疗方法可以有效减少脑细胞的死亡,降低脑水肿和炎症反应,促进脑组织的修复和再生。
亚低温治疗仪是通过控制患儿的体温来实现治疗的,具有操作简单、安全可靠、无创伤等特点。
2.亚低温治疗仪在新生儿缺氧缺血性脑病治疗中的应用效果亚低温治疗仪在新生儿缺氧缺血性脑病治疗中有着显著的应用效果。
研究表明,亚低温治疗可以有效改善患儿的神经系统功能,减少脑损伤的程度,提高存活率和生存质量。
同时,亚低温治疗还可以减少患儿的并发症和症状,降低治疗的费用和时间成本。
3.亚低温治疗仪的临床应用实例以医院为例,该医院引进了亚低温治疗仪并应用于新生儿缺氧缺血性脑病的治疗中。
经过一年的实践,该医院发现亚低温治疗仪在新生儿缺氧缺血性脑病治疗中具有显著的疗效,患儿的神经系统功能明显改善,并发症的发生率明显降低,患儿的生存率和生存质量明显提高。
4.亚低温治疗仪的不足和改进方向尽管亚低温治疗仪在新生儿缺氧缺血性脑病治疗中具有显著的应用效果,但仍存在一些不足之处。
例如,亚低温治疗仪的成本较高,操作过程中需要严格控制患儿的体温,且治疗过程中需要监测患儿的生命体征等。
为了进一步提高治疗效果和降低治疗成本,未来可以引进更先进的亚低温治疗仪,改善治疗的技术和方法。
结论综上所述,亚低温治疗仪在新生儿缺氧缺血性脑病治疗中具有显著的应用效果,可以有效改善患儿的预后,提高存活率和生存质量。
亚低温治疗新生儿缺氧缺血性脑病的观察护理
院 的 中 重度 HIE患 儿 36例 ,男 26例 ,女 lO例 ,胎 龄 37~ 42 周 ,出 生 体 质 量 为 2 500~ 4 000 g;生 后 6 h 内 出 现 意 识 障 碍 ,肌 张 力 改 变 ,原 始 自 身 反 射 异 常 ,惊 厥 等 临 床 表 现 。 5 rain Apgar评 分 < 6分 ,CT 及 脑 电 图 (EEG)异 常 ,HIE 诊 断 符 合 2004年 度 长 沙 会 议 制 定 的 《新 生 儿 缺 氧 缺 血 性 脑 病 诊 断 标 准 》。将 符 合 上 述 条 件 的 36例 患 儿 随 机 分 为 观 察 组 2O 例 ,出 生 体 质 量 (3 392± 312)g;对 照 组 1 6例 ,出 生 体 质 量 (3 248-+-253)g;2组 患 儿 在 胎 龄 、性 别 、生 后 5min Apgar评 分 差 异 无 统 计 意 义 ,观 察 组 患 儿 家 属 被 告 知 病 情 ,同 意 实 施 亚 低 温 治 疗 。
4 讨 论 换 血 疗 法 能 有 效 去 除体 内过 高 的 间 接 胆 红 素 ,使 之 下 降
至 安全 水 平 ,防 止 胆 红 素 脑 病 .并 去 除 附 有 抗 体 的 红 细 胞 及
存 在 血 中 的 游 离 抗 体 ]。换 血 疗 法 经 历 了 由 采 用 脐 静 脉 到 外 周 动 脉 ,由人 工 控 制 到 微 量 泵 全 自动 控 制 等 发 展 过 程 。 我科 采 用 经外 周 动 静 脉 全 自动换 血 疗 法 ,整 个 过 程 均 在 密 闭 系 统 中 完 成 ,输 入 血 、排 出 血 速 度 恒 定 ,血 压 稳 定 ,减 少 了 血 压 波 动 和 血 液 动 力 学 紊 乱 ,避 免 了 颅 内 出 血 等 并 发 症 的 发 生 ,降 低 了空 气 栓 塞 和 血 块 栓 塞 的 危 险 ,并 减 少 了感 染 机 会 。
亚低温治疗仪在新生儿缺氧缺血性脑病治疗中的应用效果分析

亚低温治疗仪在新生儿缺氧缺血性脑病治疗中的应用效果分析引言新生儿缺氧缺血性脑病(HIE)是指由于新生儿在出生过程中受到缺氧和缺血的影响导致脑组织损伤的一种疾病。
缺氧缺血性脑病是新生儿重症中最常见的一种,它会给患儿的大脑造成不同程度的损伤,严重时还可能导致智力障碍和运动障碍等后遗症。
在治疗方面,亚低温治疗仪是目前比较常用的一种治疗手段,通过将患儿体温降至32~34摄氏度并保持48~72小时,来减缓脑损伤的进程,降低患儿的死亡率和严重后遗症的发生率。
本文将对亚低温治疗仪在新生儿HIE治疗中的应用效果进行分析,以期为临床实践提供参考和指导。
一、亚低温治疗仪的原理亚低温治疗仪是一种通过对新生儿进行低温治疗来减缓脑组织损伤的设备。
其治疗原理主要是通过将患儿的体温降低至32~34摄氏度,维持48~72小时,从而减缓脑损伤的进程,减轻脑水肿,降低脑代谢率,抑制细胞凋亡和炎症反应,减少缺血再灌注损伤,最终达到保护脑组织的目的。
亚低温治疗仪需要严格控制患儿的体温,并监测患儿的生命体征,以确保治疗效果和患儿的安全。
二、亚低温治疗仪在新生儿HIE治疗中的应用效果1. 降低死亡率亚低温治疗仪在新生儿HIE治疗中能够有效降低患儿的死亡率。
一些研究表明,采用亚低温治疗仪治疗HIE患儿的死亡率相较于传统治疗方法有所降低,其中一项回顾性研究显示,接受亚低温治疗的HIE患儿的死亡率明显低于未接受亚低温治疗的患儿。
亚低温治疗仪在新生儿HIE治疗中能够显著降低患儿的死亡率。
2. 减轻严重后遗症的发生除了降低死亡率外,亚低温治疗仪还能够减轻患儿严重后遗症的发生。
由于亚低温治疗能够减缓脑损伤的进程,降低脑代谢率,抑制细胞凋亡和炎症反应,使得患儿出现严重后遗症的风险明显降低。
一些临床研究显示,接受亚低温治疗的HIE患儿在随访时智力和运动功能的发育情况要优于未接受亚低温治疗的患儿,说明亚低温治疗能够减轻患儿严重后遗症的发生。
三、亚低温治疗仪的局限性和不足虽然亚低温治疗仪在新生儿HIE治疗中具有明显的优势,但是其也存在一些局限性和不足之处。
亚低温治疗新生儿缺氧缺血性脑病的护理体会

亚低温治疗新生儿缺氧缺血性脑病的护理体会(柳州市妇幼保健院;广西科技大学附属妇产医院、儿童医院、新生儿一区;广西柳州545001)新生儿缺血缺氧性脑病(HIE)是指由于是指由于围生期窒息引起的部分或完全缺氧、脑血流减少或暂停而导致胎儿或新生儿脑损伤。
HIE是引起新生儿急性病死和慢性神经系统损伤的主要原因之一。
据统计[1] ,我国新生儿 HIE 发生率约为活产儿的3‰~6‰,其中15%~20%的HIE患儿在新生儿期内病死,存活者中 20%~30%可能遗留下不同程度的神经系统后遗症。
因此对HIE 患儿的神经保护治疗显得尤为重要。
近年来,多项研究[2-5]证明,全身亚低温疗法能有效降低HIE患儿病死率改善其神经系统发育障碍,是目前最值得推广的神经保护措施。
2017年12月至2019年12月我院新生儿重症监护病房对25例患儿行全身亚低温治疗,经精心护理,效果满意。
现将护理体会报告如下。
1 资料与方法1.1一般资料入选标准[6]:(1)生后6 h以内,越早越好。
(2)胎龄≥35周,体重≥1800g。
(3)有围产期窒息的证据,至少满足下列一项:①生后10minApgar评分≤5分);②脐带血或生后1 h内动脉血/静脉血/毛细血管血血气分析pH<7.0或BE≤-12 mmol/L;③生后10 min仍需机械通气或正压通气。
(4)生后6小时内有中到重度HIE表现,如惊厥、不同程度的意识障碍、自主活动减少、肌张力低下、原始反射减弱或消失、多器官损伤。
aEEG脑功能监测异常。
符合入选标准患儿25例;男14例,女11例;胎龄36+3W~40+2W;出生时间1~6小时;出生体重2500g~3800g;生后10minApgar评分≤5分10例,6~8分15例;均有中到重度的HIE临床表现。
1.2 亚低温治疗方法在常规护理的基础上采用亚低温治疗,采用医用控温仪BLANKETROL超级恒温系统,通过热传导器降低患儿的体温或将患儿体温维持在某一定值。
新生儿缺血缺氧性脑病使用亚低温治疗的观察和护理

新生儿缺血缺氧性脑病使用亚低温治疗的观察和护理摘要】总结了应用亚低温疗法治疗重度窒息复苏后新生儿的相关护理措施,护理重点为治疗期间维持目标体温的稳定,密切监测神经系统症状,持续心肺监护,严密监测生命体征及尿量的变化,加强全身皮肤护理。
认为亚低温疗法作为新的治疗新生儿缺血缺氧性脑病(HIE)方法,虽有一定的风险,但在亚低温治疗过程中,严格掌握亚低温疗法的适应症与体温控制,严密观察各系统的临床表现,制定完善的护理措施,可以更好地护理患者,提高亚低温疗法的成功率,降低风险。
结果:本组新生儿重症窒息12例,治愈8例、好转2例、死亡1例,未出现1例严重并发症。
【关键词】新生儿;缺氧缺性脑病;亚低温;护理【中图分类号】R272.1 【文献标识码】A 【文章编号】2096-0867(2016)-07-346-02新生儿缺氧缺血性脑病(HIE)发病率约为活产儿的1‰~8‰,其中10%~20%在新生儿期死亡,存活者中25%~30%可留有远期神经发育后遗症[1]。
新生儿窒息为新生儿最常见症状,也是新生儿死亡、脑瘫和智力低下的主要原因之一。
亚低温疗法是一种以物理方法将患者体温降低到预期水平而达到治疗疾病的一种方法。
一般将28~35℃划为亚低温的范畴,但由于32℃以下低温在临床上可能带来许多并发症,故通常使用32~35℃亚低温治疗。
亚低温对脑血流有调节作用,可降低脑氧代谢率和改善细胞能量代谢,减少兴奋性氨基酸的释放,减少氧自由基的生成,减少神经元坏死和凋亡,促进细胞间信号传导的恢复,减轻脑水肿和降低颅内压等效果。
有实验证实,体温每降低1℃,脑部耗氧率就可减少5%。
亚低温具有简捷、快速、有效等优点,便于复苏后即刻实施,应用亚低温疗法的最佳时机在6h之内,愈早效果愈好。
以我院收治的12例窒息患儿,护理效果显著,具体报道内容如下。
1资料及方法1.1一般资料入选标准[2]:2014年2月~2015年2月我院收治的12例窒息患儿,男4例,女8例,最小38周,最大42周,平均体重(3148.3±212.5)g。
足月儿缺氧缺血性脑病亚低温治疗

温度探头放置后应标记位置,作为操作后无滑 脱的检验指示。
23
如何选择冰帽、冰毯
• 选择合适的冰帽或冰毯冰帽应大小适 中,覆盖头部,应不遮盖眼睛;冰毯 应大小适中,覆盖躯干和大腿
• 特别提示冰帽或冰毯均不能覆盖新生儿 颈部。
24
皮肤温度 探头
低温(衣)毯
动脉置管和血压检测
如何拓展治疗时间窗?
• 产房内低温复苏? • 转运低温? • 低温治疗开始时间延迟到生后12小时或更长?
Tiffany D. Stafford,Therapeutic Hypothermia During Neonatal Transport: Active Cooling Helps Reach the Target,Ther Hypothermia Temp Manag. 2016
各中心累积资料收集表
数据
中心1 中心
低温前T>38(N)
2 改进 前
体温>38(N) 脐带血气(%)
早期病 B 人识别
1h内动脉血气(%) 多中心 B/C 达到目标温度时间 协作
4h内神经查体(%)
低温治 疗常规
B
MRI时间
MRI B
出院前神经查体 (%)
随访 B
随访(%)
父母亲 C 沟通
----------
– 入院时脐血pH <7.0 但临床表现无特殊 – 脑病的临床表现在生后6h内得到改善或好转 – 患儿在复温过程中或之后出现抽搐或抽搐加重 – HIE的诊断还不是很确定(病史不清或不全)或同时合并其他如严重感染、
低血糖等问题
部分符合标准的患儿
Smit E, Liu X, Jary S, Cowan F, Thoresen M.Acta Paediatr. 2015 Feb;104(2):138-45
亚低温治疗仪在新生儿缺氧缺血性脑病治疗中的应用效果分析
亚低温治疗仪在新生儿缺氧缺血性脑病治疗中的应用效果分析亚低温治疗仪是一种应用于新生儿缺氧缺血性脑病治疗的先进设备,通过降低患儿的体温来减缓脑损伤,减少细胞死亡,促进脑组织的修复,从而提高治疗效果。
近年来,亚低温治疗仪在新生儿脑病治疗中得到了广泛应用,并取得了一定的疗效。
本文将对亚低温治疗仪在新生儿缺氧缺血性脑病治疗中的应用效果进行分析,以期为临床实践提供参考。
1. 提高生存率2. 减轻神经功能障碍亚低温治疗仪在新生儿缺氧缺血性脑病治疗中还能够有效减轻神经功能障碍。
由于缺氧缺血会导致脑细胞损伤和神经功能障碍,而亚低温治疗能够降低体温,减缓脑损伤的进展,促进脑组织的修复,从而减轻神经功能障碍。
一些研究显示,通过应用亚低温治疗仪进行治疗,患儿的神经功能障碍得到了缓解,神经系统的损伤程度明显减轻,为患儿的康复奠定了基础。
3. 改善预后1. 设备昂贵亚低温治疗仪是一种高端医疗设备,价格比较昂贵,对一些医疗机构而言可能存在一定的经济压力。
一些医疗机构可能无法购买这样的设备,导致了亚低温治疗仪在一些地区的推广应用存在一定的困难。
2. 治疗过程复杂亚低温治疗仪在新生儿缺氧缺血性脑病治疗中的应用要求医护人员具备一定的专业技能,治疗过程相对复杂。
一些医疗机构可能由于技术和人员不足,无法有效地开展亚低温治疗,影响了其在临床中的推广和应用。
四、结语亚低温治疗仪在新生儿缺氧缺血性脑病治疗中具有显著的疗效,能够提高患儿的生存率,减轻神经功能障碍,改善预后。
由于设备昂贵和治疗过程复杂等原因,亚低温治疗仪在临床中的推广和应用还存在一定的困难。
需要政府和医疗机构的支持,加强技术培训和人员配备,推动亚低温治疗仪在新生儿缺氧缺血性脑病治疗中的应用,为更多的患儿带来康复的希望。
亚低温治疗新生儿缺氧缺血性脑病的护理
疗组 除心率在 7 与对照组相 比存在 明显下降Y ( O O ) 其余 指标均无显著性差 异。结 论 : 2h t P< . 1 , - 在护理上 除严 密监测患儿 的体温 、 持直肠温 保
度在 (5 0 2 ℃外 , 3 .± . ) 还应监测生命 体征的变化。
关键词 新 生 儿 ; 氧 缺 血性 脑 病 ; 低 温 缺 亚 d i1 .9 9j i n 1 7 o :O 3 6 /.s .6 2—9 7 .0 1 2 .3 s 66 2 1 . 1 04
Nu sng o l p h r a t e a y l w —b r t y c d p x c ic e c e c p l pa y r i fmid hy ot e mi h r p l e o n wih h a i e o i s h m n e ha o t . i h
护 理 实 践 与 研 究 2 1 年 第 8卷 第 2 期 ( 半 月 版 温 治 疗 新 生 儿 缺 氧 缺 血 性 脑 病 的 护 理
刘 素哲 刘翠 青
摘
李 丽 纪素粉
要 目的 : 择 性 头 部 降 温 治 疗 新 生 儿 缺 氧缺 血性 脑 病 时 的 生 命 体 征 的 观 察 与 护 理 。 方 法 : 择 重 度 窒 息 、 后 2 选 选 生 4h内 的 足 月 薪 生 儿 5 O
例, 随机分 为两组 , 每组 2 5例。治疗组用选择性头部 降温 的方法 , 维持直肠温 度在 (5± . ) , 部温度维 持在 (4± . )C, 3 02 ℃ 头 3 0 3 o 维持头部 降温
7 ; 照组 不进 行 降温 治 疗 。分 别 对 两 组 进 行 心 率 、 吸 、 压 、 皮 血 氧饱 和 度 监 测 , S S 0 0统 计 软 件 对 监 测 数 据 进 行 检 验 。结 果 : 2h 对 呼 血 经 用 P S1 . 治
亚低温治疗仪在新生儿缺氧缺血性脑病治疗中的应用效果分析
亚低温治疗仪在新生儿缺氧缺血性脑病治疗中的应用效果分析亚低温治疗是一种新生儿缺氧缺血性脑病的治疗方法,它通过降低新生儿的体温,减缓脑细胞的代谢,降低脑内的炎症反应,从而减少脑损伤并提高神经系统的康复能力。
本文旨在探讨亚低温治疗仪在新生儿缺氧缺血性脑病治疗中的应用效果,并对其临床应用进行分析。
一、亚低温治疗仪的原理及作用机制亚低温治疗是通过降低新生儿的体温到32~34摄氏度的范围,使得脑细胞的代谢率降低,减少脑损伤和细胞死亡。
低温还可以减轻脑组织内的炎症反应,减少脑水肿和细胞凋亡,从而减少脑损伤和提高神经系统的康复能力。
亚低温治疗仪是一种专门用于控制和维持新生儿体温的医疗设备,它能够实时监测新生儿的体温,并通过冷热水循环系统控制新生儿的体温在目标范围内。
1. 临床适应症亚低温治疗主要适用于新生儿缺氧缺血性脑病,包括新生儿窘迫症、先天性心脏病、窒息、颅内出血等病因所致的缺氧缺血性脑病。
2. 治疗过程及注意事项在进行亚低温治疗时,首先需要对新生儿进行全面的评估,包括脑电图、脑影像学检查等,并排除其他严重疾病。
在治疗过程中,需要密切监测新生儿的体温、呼吸、心率、血压等生命体征,并及时调整治疗参数以维持目标体温。
3. 临床疗效评估近年来,许多临床研究表明,亚低温治疗在新生儿缺氧缺血性脑病的治疗中具有显著的疗效。
一项对亚低温治疗的荟萃分析研究发现,与常规治疗相比,亚低温治疗可以显著降低新生儿缺氧缺血性脑病患儿的死亡率和神经系统残疾率。
许多临床试验也表明,亚低温治疗可以显著改善新生儿缺氧缺血性脑病患儿的神经系统功能和生存质量,减少脑损伤面积、缩短住院时间,并提高患儿的生存率和神经系统功能的康复率。
一些长期随访研究也发现,接受亚低温治疗的新生儿在长期随访中表现出更好的认知和神经发育水平,相对于未接受亚低温治疗的患儿,其智力发育水平更高,神经系统功能更正常。
随着医疗技术的不断进步和临床研究的不断深入,亚低温治疗仪在新生儿缺氧缺血性脑病治疗中的应用前景十分广阔。
亚低温治疗仪在新生儿缺氧缺血性脑病治疗中的应用效果分析

亚低温治疗仪在新生儿缺氧缺血性脑病治疗中的应用效果分析一、亚低温治疗仪的原理及优势亚低温治疗仪是一种通过将患儿的体温降低到较低水平,从而减缓细胞代谢、减少细胞损伤的设备。
其原理是通过降低体温,减缓细胞代谢,降低氧需求,减少细胞内钙离子流入和氧自由基的产生,减少细胞损伤,同时可减少缺血- 再灌注时所产生的炎症反应,并减少脑细胞凋亡。
亚低温治疗仪在治疗新生儿缺氧缺血性脑病中具有显著的优势。
亚低温治疗仪在新生儿缺氧缺血性脑病的治疗中,通常在4-6小时内将患儿的体温降低至33-34摄氏度,维持24-72小时。
在这个过程中,临床医生会密切监测患儿的生命体征,确保患儿的身体可以适应亚低温治疗,并且密切观察患儿是否出现低温相关的并发症。
在临床实践中,亚低温治疗仪被广泛应用于新生儿缺氧缺血性脑病的治疗中。
通过对一系列临床案例的观察和分析,可以得出结论:亚低温治疗仪在新生儿缺氧缺血性脑病治疗中具有显著的疗效。
研究表明,亚低温治疗可以显著降低新生儿缺氧缺血性脑病的死亡率和导致严重神经系统后遗症的风险。
三、亚低温治疗仪的应用效果分析1. 降低新生儿缺氧缺血性脑病的死亡率亚低温治疗仪通过降低身体温度,减缓细胞代谢,从而减少细胞损伤,对新生儿缺氧缺血性脑病起到了良好的治疗效果。
研究表明,通过亚低温治疗,可以显著降低新生儿缺氧缺血性脑病患儿的死亡率,提高患儿的生存率。
2. 减少严重神经系统后遗症的风险新生儿缺氧缺血性脑病是一种严重的疾病,容易导致患儿出现严重的神经系统后遗症,如脑瘫、智力障碍等。
亚低温治疗仪在治疗新生儿缺氧缺血性脑病中,可以减少患儿出现严重神经系统后遗症的风险,改善患儿的预后情况。
3. 提高患儿生活质量亚低温治疗仪在治疗新生儿缺氧缺血性脑病中,不仅可以降低患儿的死亡率,减少严重神经系统后遗症的风险,还可以提高患儿的生存质量。
经过亚低温治疗后的患儿,通常可以更好地进行康复训练,提高患儿的生活质量。
四、亚低温治疗仪的潜在挑战和未来发展虽然亚低温治疗仪在新生儿缺氧缺血性脑病治疗中取得了显著的疗效,但是也面临着一些挑战。
2022亚低温治疗新生儿缺氧缺血性脑病专家共识
2022亚低温治疗新生儿缺氧缺血性脑病专家共识(最全版)亚低温治疗是指采用物理降温,使体核温度维持在30~35 C,以达到治疗目的。
新生儿缺氧缺血性脑病(hypoxic ischemic encephalopathy,HIE )的亚低温治疗是指采用主动降温的方法,使体核温度降低到33.0~34.0 C,并维持72 h,然后缓慢复温,以达到神经保护效果。
国际多中心大样本的研究证实亚低温治疗新生儿HIE不仅能够显著降低HIE患儿的病死率,同时可降低存活者不良神经发育结局和脑瘫的发生率,随访到学龄前期亚低温治疗的保护效果仍然存在。
亚低温治疗已经成为新生儿HIE常规治疗手段,2021年的调查研究提示中国新生儿HIE 亚低温治疗开展率仅有54%,英国和加拿大的研究提示各医疗机构亚低温治疗的纳入标准、实施方法等也存在差异。
为进一步推动和规范化我国新生儿HIE亚低温治疗实施,中华医学会儿科学分会新生儿学组和中华儿科杂志编辑委员成立了新生儿HIE亚低温治疗临床管理规范专家组,广泛征求各专家的意见和建议,以国内外的循证医学证据为基础,结合我国国情制定了“亚低温治疗新生儿缺氧缺血性脑病专家共识2022 )” (简称本共识)。
本共识通过近1年的研讨制定,读者范围包括从事儿科、新生儿、围生医学的医护人员。
本共识的适用人群为出生胎龄>35周的新生儿HIE 患者。
一、亚低温治疗的实施1.亚低温治疗方法:已经发表的多中心临床研究均采用设计合理的控温设备进行亚低温治疗,分为全身亚低温和选择性头部亚低温联合全身轻度降温。
5项临床试验采用全身亚低温,2项采用选择性头部亚低温,相比选择性头部亚低温,全身亚低温操作更为方便,尚无证据表明哪种降温方式临床效果和安全性更好。
有少数研究采用简易降温方法包括风扇、冷水袋、冷胶袋,低温相变材料等进行亚低温治疗,该方法虽然操作简单、费用低,但温度波动大,可发生体温过低或降温效果不理想。
Meta分析显示采用简易降温方法进行低温治疗可降低出院前和6~24月龄的病死率,降低出院前神经功能障碍的发生率。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
• 呼吸机调节无特殊,三支持(血气、血糖 、血压),三对症同未用亚低温时
• 查血气时注意标注当时体温。
复温
– Gunn, 1998; 22 patients, head cooling – no adverse effects compared with control
– Azzopardi, 2000; 16 patients, whole body cooling – no adverse effects
– Latent (>6 hours)
• “Delayed neuronal death”
– Multiple mechanisms » Hyperemia 充血 » Cytotoxic edema 细胞毒性水肿 » Mitochondrial failure 线粒体·损伤 » Accumulation of excitotoxins 兴奋性氨基酸 » Active cell death » Nitric oxide synthesis NO失衡 » Free radical damage and cytotoxic actions of activated microglia
consistent with diagnosis of moderate to severe HIE
p
• Intervention:
– Cooling Cap fitted to head for 72h
• Small thermostatic cooling unit with a pump to circulate water through the cap
亚低温治疗缺氧缺血性脑病
目的 了解亚低温疗法的由来 明确亚低温治疗对缺血缺氧性脑病的 疗效 掌握我院亚低温疗法的方案
History of Therapeutic Hypothermia
• First scientific report was published in 1945 by Dr. Temple Fay
– Gluckman PD, Wyatt JS, Azzopardi D, Ballard R, Edwards AD, Ferriero DM, Polin RA, Robertson CM, Thoresen M, Whitelaw A, Gunn AJ
– Lancet. 2005 Feb 19-25;365(9460):663-70
• Initial water temperature 8° to 12°C • Radiant warmer, servo-controlled to abdominal
skin temperature, adjusted to maintain the rectal temperature at 34–35°C • Initially, warmer off for 20-30 mins to speed cooling
缺氧缺血性脑病HIE
围生期窒息引起的部分或完全缺氧、脑血 流减少或暂停导致的胎儿、新生儿脑损伤
我国HIE发病率3-6‰,其中15-20%在新生 儿期死亡。 存活者中20-30%有不同程度神经系统后遗 症
HIE in Neonates
• Diagnostic criteria are vague
– Low Apgar scores at 5 mins – Change in consciousness – Signs of significant hypoperfusion (ie acidosis) – Requirement for ventilation – Seizures – Other
Pathophysiology of Brain Injury due
to Hypoxic-Ischemic Insult
• 2 phases of neuronal death
– Immediate
• “Primary neuronal death”
– cellular hypoxia with exhaustion of the cell’s high energy stores (primary energy failure)
• Recently this therapy has emerged as therapy for infants suffering HIE related to birth
Therapeutic Hypothermia in Babies
• Small human studies with encouraging results
– Esophageal probe then removed – Thereafter, skin temperature was controlled
by the radiant warmer's servomechanism
• Warmer temp was set 0.5°C higher than the skin temperature and increased 0.5°C every hour until the set point of the warmer reached 36.5°C
Wagner, 2002 – Rats
Gunn, 1997 - Lambs
Tooley, 2003 – Piglets
Summary
• Multiple lines of evidence suggest therapeutic hypothermia may be neuroprotective
– Significant proportion of total injury
Figure 2. Patterns of brain injury in mild to moderate hypoperfusion
Chao, C. P. et al. Radiographics 2006;26:S159-S172
– Rewarmed < 0.5°C/h until temperature was normal
亚低温 33-34℃
CoolCap
CoolCap
CoolCap – Subgroup Analysis
Whole-Body Hypothermia
• Whole-Body Hypothermia for Neonates with Hypoxic–Ischemic Encephalopathy
– Esophageal probe was inserted
• Esophageal temperature was lowered to 33.5°C by the blanket's servomechanism
• Needed a second blanket as a thermal sink
– No other sources of warming provided during the cooling period
Whole-Body Hypothermia
• After 72 hours
– Set point of the cooling system was increased by 0.5°C per hour for six hours
Copyright ©Radiological Society of North America, 2006
Pathophysiology of Brain Injury due to Hypoxic-Ischemic Insult
• Latent phase provides window of therapeutic intervention
CoolCap
• Inclusion criteria:
– >35 weeks EGA – Apgar score ≤ 5 at 10 mins; or pH <7 or base
deficit >16 mmol/L within 60 mins of birth – Sarnat score and amplitude-integrated EEG
准入条件
1 胎龄大于36周,生后6小时内进入亚 低温程序。 2 围生期窒息缺氧史。 3 5分钟Apgar小于6。 4 脐血或生后1小时内PH小于7。 5 生后需要通气支持超过10分钟。
排除标准
1 六小时内不能进行亚低温治疗。 2.严重先天畸形。 3 严重宫内发育迟缓出生体重小于1800
千克。 4 严重染色体缺陷病 5 <35周早产儿
Whole-Body Hypothermia
Whole-Body Hypothermia
Cochrane Review
Cochrane Review
Shah, Arch Pediatr Adolesc Med. 2007;161(10):951-958
Tooley, 2003 – Piglets
医嘱
1 特级护理 告病危
2多功能心电监护:心率维持在80-140 次/分,
3 监测SpO285-99%。
4 亚低温毯温度设置33-34摄氏度
监测
• 监测患儿体温Q15分钟×2-4小时,以后Q2 小时至低温疗法结束。
• 监测血糖Q8h×1day,Q12h×2day, Qd×4day,
• 血气分析Q1day, • 肝肾功能电解质Qd×3day, • 凝血相Qd×3day 。
• 2 recent, randomized controlled trials of ~ 500 infants
– CoolCap – NICHD whole-body hypothermia
CoolCap
• Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: multicentre randomised trial