Schecter
腹膜透析的现状和将来-余学清

腹膜透析的现状与进展中山大学附属第一医院肾内科余学清一、腹膜透析的历史PD是治疗ESRD)的重要肾替代疗法之一。
20年代初,在动物实验中就发现腹膜具有透析膜的功能。
1923年德国医生Ganter首次将腹透用于人体,一直到50年代腹透仍是尿毒症治疗的最后选择。
60年代,Maxwell 和Boen等相继发展了瓶装透析液和简单的透析装置。
70年代,Tenckhoff和Schecter发明了Tenckhoff管,1975年Popovich等首次提出了CAPD概念,1次/3-4 病人月, CAPD的开展一度又陷入低谷。
1980年末和90年代,Stephen Vas确定腹膜炎诊断和治疗原则,提出'连接后冲洗'的概念,O型, Y型) 等技术的引入使腹膜炎发生率明显降低,同时对残余肾功能和尿素清除率重要性得到普遍重视的认识。
CCPD),NIPD), TPD) 的开展,也明显提高了腹透的方便性和改善了透析效能。
60年代开展了PD疗法,70年代开展了CAPD治疗,80年代CAPD治疗在国内已具规模化,90年代以后透析液,管道技术逐渐与国际接轨,充分性、营养、超滤和溶质转运等问题逐步被重视。
迄今为至, 腹透在中国的开展己取得了长足的进步。
但受经济、文化背景、教育水平的影响,对腹透治疗的选择仍有误区,国际上先进的PD方法、技术尚未广泛采用,故与国际上腹透开展较好的国家比较我们仍差距明显。
二、腹膜透析的现状目前CAPD和自动腹膜透析(Automated Peritoneal Dialysis, APD)己占了全球透析患者的15%左右, 但腹膜透析的开展地区差异很大。
在ESRD患者腹膜透析治疗中,墨西哥占总透析患者的95%, 中国香港占78%, 北美占30-45%, 欧州占25-40%左右, 中国CAPD 大约为10%,APD在欧美国家开展,约20-30%,但在发展中国家比例较低。
随着腹膜透析技术的不断进步,透析管道系统不断更新和新型腹膜透析液的不断出现,腹膜透析患者人数不断攀新。
二恶英对环境的污染及对人类的危害

二恶英对环境的污染及对人类的危害人类对二恶英的认识1999 年5 月比利时的二恶英污染事件, 引起全球震惊,美国、加拿大、中国、日本、香港等40 多个国家和地区的政府禁止进口和销售比利时、法国等四国可能受污染的食品。
这一事件造成巨大的经济损失和社会影响, 被认为是本世纪最大的化学毒物污染食品事件。
二恶英是一类有机氯化合物的俗称, 美国环保局确认的二恶英类物质有30 种, 其中包括多氯二苯二恶英(PCDDs) 7种、多氯二苯呋喃(PCDFs) 10 种、多氯联苯(PCBs) 13 种, 以毒性大、致癌作用强的2 , 3 , 7 , 82四氯双苯并二恶英( TCDD)为代表。
50 年代, 人类首次发现二恶英类化合物能引起一系列的健康问题,但那仅仅是在一些生产杀虫剂的生产工人中发现。
60~70 年代,以DD T 、六六六为代表的杀虫剂被广泛使用。
一种称为“橙剂”的化合物作为落叶剂在越南战场上使用。
然而人们很快发现由于这类化合物在环境中能长期存在, 不被破坏,对人类有难以估计的危害。
1962 年,美国的卡松女士在她的《寂静的春天》一书中叙述了这样一个事实: 美国密西根州东兰辛市为了杀灭榆树上的甲虫,用DD T 喷洒杀虫。
秋天树叶落在地上, 蠕虫吃了树叶, 来年春天, 树上的知更鸟吃了蠕虫, 一周之内, 全市的知更鸟几乎全部死光。
卡松女士描写的使用有机氯杀虫剂后荒芜、寂静的地球景象震惊了整个世界。
这一举动直接导致了美国环境保护局的成立,同时使有机氯杀虫剂被世界大多数国家禁止生产和使用。
80 年代, 人们发现二恶英不仅仅来源于杀虫剂, 而更广泛来源于其它含氯的工业品。
例如用氯漂白的纸张、妇女用卫生棉条、婴儿用纸尿布, 以及PVC(聚氯乙烯) 塑料制成的一次性输液用品、儿童玩具、餐具等等。
上述工业品使用后的废弃物,作为垃圾被焚烧时产生有强毒性和致癌性的TCDD ,污染空气、水体、土壤和野生动植物,从局部的农场到海洋深处,甚至北极,无所不在。
美国CDC-SSI预防指南2017
Centers for Disease Control and Prevention Guideline for the Prevention of Surgical Site Infection,2017Sandra I.Berríos-Torres,MD;Craig A.Umscheid,MD,MSCE;Dale W.Bratzler,DO,MPH;Brian Leas,MA,MS;Erin C.Stone,MA;Rachel R.Kelz,MD,MSCE;Caroline E.Reinke,MD,MSHP;Sherry Morgan,RN,MLS,PhD;Joseph S.Solomkin,MD;John E.Mazuski,MD,PhD;E.Patchen Dellinger,MD;Kamal M.F.Itani,MD;Elie F.Berbari,MD;John Segreti,MD;Javad Parvizi,MD;Joan Blanchard,MSS,BSN,RN,CNOR,CIC;George Allen,PhD,CIC,CNOR;Jan A.J.W.Kluytmans,MD;Rodney Donlan,PhD;William P.Schecter,MD;for the Healthcare Infection Control Practices Advisory CommitteeInvited CommentarySupplemental contentAuthor Affiliations:Authoraffiliations are listed at the end of this article.Group Information:The Healthcare Infection Control Practices Advisory Committee members are listed at the end of this article.Corresponding Author:Erin C.Stone,MA,Division of Healthcare Quality Promotion,Centers for Disease Control and Prevention,1660Clifton Rd NE,Mail Stop A07Atlanta,GA 30329(ecstone@ ).Clinical Review &EducationJAMA Surgery |Special CommunicationE1S urgical site infections(SSIs)are infections of the incision or organ or space that occur after surgery.1Surgical patients ini-tially seen with more complex comorbidities2and the emer-gence of antimicrobial-resistant pathogens increase the cost and challenge of treating SSIs.3-5The prevention of SSI is increasingly im-portant as the number of surgical procedures performed in the United States continues to rise.6,7Public reporting of process,out-come,and other quality improvement measures is now required,8,9 and reimbursements10for treating SSIs are being reduced or de-nied.It has been estimated that approximately half of SSIs are preventable by application of evidence-based strategies.11MethodsThis guideline focuses on select areas for the prevention of SSI deemed important to undergo evidence assessment for the ad-vancement of the field.These areas of focus were informed by feed-back received from clinical experts and input from the Healthcare Infection Control Practices Advisory Committee(HICPAC),a fed-eral advisory committee to the Centers for Disease Control and Prevention(CDC).This guideline was a systematic review of the literature.No institutional review board approval or participant in-formed consent was necessary.This guideline’s recommendations were developed based on a targeted systematic review of the best available evidence on SSI prevention conducted in MEDLINE,EMBASE,CINAHL,and the Cochrane Library from1998through April2014.To provide explicit links between the evidence and recommendations,a modified Grad-ing of Recommendations,Assessment,Development,and Evalua-tion(GRADE)approach was used for evaluating the quality of evi-dence and determining the strength of recommendations.12-15The methods and structure of this guideline were adopted in2009by CDC and HICPAC.16,17The present guideline does not reevaluate sev-eral strong recommendations offered by CDC’s1999Guideline for Prevention of Surgical Site Infection18that are now considered to be accepted practice for the prevention of SSI.These recommen-dations are found in eAppendix1of the Supplement.A detailed description of the Guideline Questions,Scope and Purpose,and Methods,as well as the Evidence Summaries supporting the evi-dence-based recommendations,can also be found in eAppendix1 of the Supplement.The detailed literature search strategies,GRADE Tables,and Evidence Tables supporting each section can be found in eAppen-dix2of the Supplement.Results of the entire study selection pro-cess are shown in the Figure.Of5759titles and abstracts screened,896underwent full-text review by2independent reviewers.Full-text articles were excluded if:1)SSI was notFigure.Results of the Study Selection ProcessCDC indicates Centers for Disease Control and Prevention;GRADE,Grading of Recommendations,Assessment,Development,and Evaluation;RCTs,randomized controlled trials;SRs,expand;and SSI,surgical site infection.Clinical Review&Education Special Communication CDC Guideline for the Prevention of Surgical Site Infection,2017E2JAMA Surgery Published online May3,©2017American Medical Association.All rights reserved.reported as an outcome;2)all patients included had“dirty”surgi-cal procedures(except for Q2addressing the use of aqueous iodo-phor irrigation);3)the study only included oral or dental health procedures;4)the surgical procedures did not include primary closure of the incision in the operating room(eg,orthopedic pin sites,thoracotomies,or percutaneous endoscopic gastrostomy [PEG]procedures,or wounds healing by secondary intention);or 5)the study evaluated wound protectors used postincision. Evidence-based recommendations in this guideline were cross-checked with those from other guidelines identified in a system-atic search.CDC completed a draft of the guideline and shared it with the expert panel for in-depth review and then with HICPAC and mem-bers of the public at committee meetings(June2010to July2015). CDC posted notice in the Federal Register for the following2peri-ods of public comment:from January29to February28,2014,and from April8to May8,ments were aggregated and re-viewedwiththewritinggroupandatanotherHICPACmeeting.Based on the comments received,the literature search was updated,and new data were incorporated into a revised draft.Further input was provided by HICPAC during a public teleconference in May2015.Fi-nalHICPACinputwasprovidedviaavotebymajorityruleinJuly2015. After final HICPAC input,CDC updated the draft document and obtained final CDC clearance and coauthor approval.Recommendation CategoriesRecommendations were categorized using the following standard system that reflects the level of supporting evidence or regulations:•Category IA:A strong recommendation supported by high to mod-erate–quality evidence suggesting net clinical benefits or harms.•Category IB:A strong recommendation supported by low-quality evidence suggesting net clinical benefits or harms or an accepted practice(eg,aseptic technique)supported by low to very low–quality evidence.•Category IC:A strong recommendation required by state or fed-eral regulation.•Category II:A weak recommendation supported by any quality evidence suggesting a trade-off between clinical benefits and harms.•No recommendation/unresolved issue:An issue for which there is low to very low–quality evidence with uncertain trade-offs be-tween the benefits and harms or no published evidence on out-comes deemed critical to weighing the risks and benefits of a given intervention.RecommendationsCore SectionIn2006,approximately80million surgical procedures were per-formed in the United States at inpatient hospitals(46million)7and ambulatory hospital–affiliated or freestanding(32million)settings.6 Between2006and2009,SSIs complicated approximately1.9%of surgical procedures in the United States.19However,the number of SSIs is likely to be underestimated given that approximately50% of SSIs become evident after discharge.20Estimated mean attrib-utablecostsofSSIsrangefrom$10443in2005USdollarsto$25546 in2002US dollars per infection.3-5,11Costs can exceed$90000per infection when the SSI involves a prosthetic joint implant21,22or an antimicrobial-resistant organism.23The Core Section of this guide-line(eAppendix1of the Supplement)includes recommendations for the prevention of SSI that are generalizable across surgical proce-dures,with some exceptions as mentioned below.Parenteral Antimicrobial Prophylaxis1A.1.Administer preoperative antimicrobial agents only when indi-cated based on published clinical practice guidelines and timed such that a bactericidal concentration of the agents is established in the serum and tissues when the incision is made.(Category IB–strong recommendation;accepted practice.)1A.2.No further refinement of timing can be made for preoperative antimicrobial agents based on clinical outcomes.(No recommenda-tion/unresolved issue.)1B.Administer the appropriate parenteral prophylactic antimicro-bial agents before skin incision in all cesarean section procedures. (Category IA–strong recommendation;high-quality evidence.)1C.The literature search did not identify randomized controlled trials that evaluated the benefits and harms of weight-adjusted paren-teral antimicrobial prophylaxis dosing and its effect on the risk of SSI.Other organizations have made recommendations based on ob-servational and pharmacokinetic data,and a summary of these rec-ommendations can be found in the Other Guidelines section of the narrative summary for this question(eAppendix1of the Supple-ment).(No recommendation/unresolved issue.)1D.The search did not identify sufficient randomized controlled trial evidence to evaluate the benefits and harms of intraoperative re-dosing of parenteral prophylactic antimicrobial agents for the pre-vention of SSI.Other organizations have made recommendations based on observational and pharmacokinetic data,and a summary of these recommendations can be found in the Other Guidelines sec-tion of the narrative summary for this question(eAppendix1of the Supplement).(No recommendation/unresolved issue.)1E.In clean and clean-contaminated procedures,do not administer additional prophylactic antimicrobial agent doses after the surgical incision is closed in the operating room,even in the presence of a drain.(Category IA–strong recommendation;high-quality evidence.)Nonparenteral Antimicrobial Prophylaxis2A.1.Randomized controlled trial evidence suggested uncertain trade-offs between the benefits and harms regarding intraopera-tive antimicrobial irrigation(eg,intra-abdominal,deep,or subcuta-neous tissues)for the prevention of SSI.Other organizations have made recommendations based on the existing evidence,and a sum-mary of these recommendations can be found in the Other Guide-lines section of the narrative summary for this question(eAppen-dix1of the Supplement).(No recommendation/unresolved issue.)2A.2.The search did not identify randomized controlled trials that evaluated soaking prosthetic devices in antimicrobial solutions be-fore implantation for the prevention of SSI.(No recommendation/ unresolved issue.)CDC Guideline for the Prevention of Surgical Site Infection,2017Special Communication Clinical Review&Education JAMA Surgery Published online May3,2017E3©2017American Medical Association.All rights reserved.2B.1.Do not apply antimicrobial agents(ie,ointments,solutions,or powders)to the surgical incision for the prevention of SSI.(Cat-egory IB–strong recommendation;low-quality evidence.)2B.2.Application of autologous platelet-rich plasma is not neces-sary for the prevention of SSI.(Category II–weak recommendation; moderate-quality evidence suggesting a trade-off between clinical benefits and harms.)2C.Consider the use of triclosan-coated sutures for the prevention of SSI.(Category II–weak recommendation;moderate-quality evi-dence suggesting a trade-off between clinical benefits and harms.)2D.Randomizedcontrolledtrialevidencesuggesteduncertaintrade-offs between the benefits and harms regarding antimicrobial dress-ings applied to surgical incisions after primary closure in the oper-ating room for the prevention of SSI.(No recommendation/ unresolved issue.)Glycemic Control3A.1.Implement perioperative glycemic control and use blood glu-cose target levels less than200mg/dL in patients with and with-out diabetes.(Category IA–strong recommendation;high to mod-erate–quality evidence.)3A.2.The search did not identify randomized controlled trials that evaluated lower(<200mg/dL)or narrower blood glucose target lev-els than recommended in this guideline nor the optimal timing,du-ration,or delivery method of perioperative glycemic control for the prevention of SSI.Other organizations have made recommenda-tions based on observational evidence,and a summary of these rec-ommendations can be found in the Other Guidelines section of the narrative summary for this question(eAppendix1of the Supple-ment).(No recommendation/unresolved issue.)3B.The search did not identify randomized controlled trials that evaluated the optimal hemoglobin A1C target levels for the preven-tion of SSI in patients with and without diabetes.(No recommen-dation/unresolved issue.)Normothermia4.Maintain perioperative normothermia.(Category IA–strong rec-ommendation;high to moderate–quality evidence.)5.The search did not identify randomized controlled trials that evaluated strategies to achieve and maintain normothermia,the lower limit of normothermia,or the optimal timing and duration of normothermia for the prevention of SSI.Other organizations have made recommendations based on observational evidence,and a summary of these recommendations can be found in the Other Guidelines section of the narrative summary for this question (eAppendix1of the Supplement).(No recommendation/ unresolved issue.)Oxygenation6A.Randomizedcontrolledtrialevidencesuggesteduncertaintrade-offs between the benefits and harms regarding the administration of increased fraction of inspired oxygen(F IO2)via endotracheal in-tubation during only the intraoperative period in patients with nor-mal pulmonary function undergoing general anesthesia for the pre-vention of SSI.(No recommendation/unresolved issue.)6B.For patients with normal pulmonary function undergoing gen-eral anesthesia with endotracheal intubation,administer increased F IO2during surgery and after extubation in the immediate postop-erative period.To optimize tissue oxygen delivery,maintain peri-operative normothermia and adequate volume replacement.(Cat-egory IA–strong recommendation;moderate-quality evidence.)6C.Randomizedcontrolledtrialevidencesuggesteduncertaintrade-offs between the benefits and harms regarding the administrationof increased F IO2via face mask during the perioperative period in patients with normal pulmonary function undergoing general an-esthesia without endotracheal intubation or neuraxial anesthesia(ie, spinal,epidural,or local nerve blocks)for the prevention of SSI.(No recommendation/unresolved issue.)6D.Randomized controlled trial evidence suggested uncertain trade-offs between the benefits and harms regarding the admin-istration of increased F IO2via face mask or nasal cannula during only the postoperative period in patients with normal pulmonary function for the prevention of SSI.(No recommendation/ unresolved issue.)7.The search did not identify randomized controlled trials that evalu-ated the optimal target level,duration,and delivery method of F IO2 for the prevention of SSI.Other organizations have made recom-mendations based on observational studies,and a summary of these recommendations can be found in the Other Guidelines section of the narrative summary for this question(eAppendix1of the Supple-ment).(No recommendation/unresolved issue.)Antiseptic Prophylaxis8A.1.Advise patients to shower or bathe(full body)with soap(an-timicrobial or nonantimicrobial)or an antiseptic agent on at least the night before the operative day.(Category IB–strong recommenda-tion;accepted practice.)8A.2.Randomized controlled trial evidence suggested uncertain trade-offs between the benefits and harms regarding the optimal timing of the preoperative shower or bath,the total number of soap or antiseptic agent applications,or the use of chlorhexidine glu-conate washcloths for the prevention of SSI.(No recommendation/ unresolved issue.)8B.Perform intraoperative skin preparation with an alcohol-based antiseptic agent unless contraindicated.(Category IA–strong rec-ommendation;high-quality evidence.)8C.Application of a microbial sealant immediately after intraopera-tive skin preparation is not necessary for the prevention of SSI.(Cat-egory II–weak recommendation;low-quality evidence suggesting a trade-off between clinical benefits and harms.)8D.The use of plastic adhesive drapes with or without antimicro-bial properties is not necessary for the prevention of SSI.(Category II–weak recommendation;high to moderate–quality evidence sug-gesting a trade-off between clinical benefits and harms.)9A.Consider intraoperative irrigation of deep or subcutaneous tis-sues with aqueous iodophor solution for the prevention of SSI.In-traperitoneal lavage with aqueous iodophor solution in contami-nated or dirty abdominal procedures is not necessary.(Category II–weak recommendation;moderate-quality evidence suggesting a trade-off between clinical benefits and harms.)Clinical Review&Education Special Communication CDC Guideline for the Prevention of Surgical Site Infection,2017E4JAMA Surgery Published online May3,©2017American Medical Association.All rights reserved.9B.The search did not identify randomized controlled trials that evaluated soaking prosthetic devices in antiseptic solutions before implantation for the prevention of SSI.(No recommendation/ unresolved issue.)10.Randomized controlled trial evidence was insufficient to evalu-ate the trade-offs between the benefits and harms of repeat appli-cation of antiseptic agents to the patient’s skin immediately before closing the surgical incision for the prevention of SSI.(No recommendation/unresolved issue.)Prosthetic Joint Arthroplasty SectionPreventioneffortsshouldtargetallsurgicalproceduresbutespecially those in which the human and financial burden is greatest.In2011, primary total knee arthroplasty accounted for more than half of the 1.2million prosthetic joint arthroplasty procedures(primary and re-vision)performed in the United States,followed by total hip arthro-plastyandhiphemiarthroplasty.24Primaryshoulder,elbow,andankle arthroplasties are much less common.By2030,prosthetic joint ar-throplasties are projected to increase to3.8million procedures per year.25-27Infection is the most common indication for revision in total knee arthroplasty28and the third most common indication in total hip arthroplasty.28By2030,the infection risk for hip and knee arthroplasty is expected to increase from2.18%22to6.5% and6.8%,respectively.25In addition,owing to increasing risk and the number of individuals undergoing prosthetic joint arthro-plasty procedures,the total number of hip and knee prosthetic joint infections is projected to increase to221500cases per year by2030,at a cost of more than$1.62billion.22,25The Prosthetic Joint Arthroplasty section contains recommendations that are applicable to these procedures(eAppendix1of the Supplement).Blood Transfusion11A.Available evidence suggested uncertain trade-offs between the benefits and harms of blood transfusions on the risk of SSI in prosthetic joint arthroplasty.Other organizations have made rec-ommendations on this topic,and a reference to these recommen-dations can be found in the Other Guidelines section of the narra-tive summary for this question(eAppendix1of the Supplement). (No recommendation/unresolved issue.)11B.Do not withhold transfusion of necessary blood products from surgical patients as a means to prevent SSI.(Category IB–strong recommendation;accepted practice.)Systemic Immunosuppressive Therapy12and13.Available evidence suggested uncertain trade-offs between the benefits and harms of systemic corticosteroid or other immunosuppressive therapies on the risk of SSI in pros-thetic joint arthroplasty.Other organizations have made recom-mendations based on the existing evidence,and a summary of these recommendations can be found in the Other Guidelines section of the narrative summary for this question(eAppendix1of the Supplement).(No recommendation/unresolved issue.)14.For prosthetic joint arthroplasty patients receiving systemic corticosteroid or other immunosuppressive therapy,recommen-dation1E applies:in clean and clean-contaminated procedures, do not administer additional antimicrobial prophylaxis doses after the surgical incision is closed in the operating room,even in the presence of a drain.(Category IA–strong recommendation;high-quality evidence.)Intra-articular Corticosteroid Injection15and16.Available evidence suggested uncertain trade-offs between the benefits and harms of the use and timing of preop-erative intra-articular corticosteroid injection on the incidence of SSI in prosthetic joint arthroplasty.Other organizations have made recommendations based on observational studies,and a summary of these recommendations can be found in the Other Guidelines section of the narrative summary for this ques-tion(eAppendix1of the Supplement).(No recommendation/ unresolved issue.)Anticoagulation17.Available evidence suggested uncertain trade-offs between the benefits and harms of venous thromboembolism prophylaxis on the incidence of SSI in prosthetic joint arthroplasty.Other organizations have made recommendations based on the existing evidence,and these references can be found in the Other Guide-lines section of the narrative summary for this question(eAppen-dix1of the Supplement).(No recommendation/unresolved issue.)Orthopedic Surgical Space Suit18.Available evidence suggested uncertain trade-offs between the benefits and harms of orthopedic space suits or the health care personnel who should wear them for the prevention of SSI in prosthetic joint arthroplasty.(No recommendation/unresolved issue.)Postoperative Antimicrobial Prophylaxis DurationWith Drain Use19.In prosthetic joint arthroplasty,recommendation1E applies:in clean and clean-contaminated procedures,do not administer addi-tional antimicrobial prophylaxis doses after the surgical incision is closed in the operating room,even in the presence of a drain.(Cat-egory IA–strong recommendation;high-quality evidence.)Biofilm20A.Availableevidencesuggesteduncertaintrade-offsbetweenthe benefits and harms regarding cement modifications and the pre-vention of biofilm formation or SSI in prosthetic joint arthroplasty. (No recommendation/unresolved issue.)20B.The search did not identify studies evaluating prosthesis modi-fications for the prevention of biofilm formation or SSI in prosthetic joint arthroplasty.(No recommendation/unresolved issue.)20C.The search did not identify studies evaluating vaccines for the prevention of biofilm formation or SSI in prosthetic joint arthro-plasty.(No recommendation/unresolved issue.)CDC Guideline for the Prevention of Surgical Site Infection,2017Special Communication Clinical Review&Education JAMA Surgery Published online May3,2017E5©2017American Medical Association.All rights reserved.20D.The search did not identify studies evaluating biofilm control agents,such as biofilm dispersants,quorum sensing inhibitors,or novel antimicrobial agents,for the prevention of biofilm formation or SSI in prosthetic joint arthroplasty.(No recommendation/ unresolved issue.)ConclusionsSurgical site infections are persistent and preventable health care–associated infections.There is increasing demand for evidence-based interventions for the prevention of SSI.The last version of the CDC Guideline for Prevention of Surgical Site Infection18was pub-lished in1999.While the guideline was evidence informed,most rec-ommendations were based on expert opinion,in the era before evi-dence-based guideline methods.CDC updated that version of the guideline using GRADE as the evidence-based method that pro-videsthefoundationoftherecommendationsinthisguideline.These new and updated recommendations are not only useful for health care professionals but also can be used as a resource for profes-sional societies or organizations to develop more detailed imple-mentation guidance or to identify future research priorities.The pau-city of robust evidence across the entire guideline created challenges in formulating recommendations for the prevention of SSI.None-theless,the thoroughness and transparency achieved using a sys-tematic review and the GRADE approach to address clinical ques-tionsofinteresttostakeholdersarecriticaltothevalidityoftheclinical recommendations.The number of unresolved issues in this guideline reveals sub-stantial gaps that warrant future research.A select list of these un-resolved issues may be prioritized to formulate a research agenda toadvancethefield.Adequatelypowered,well-designedstudiesthat assess the effect of specific interventions on the incidence of SSI are needed to address these evidence gaps.Subsequent revisions to this guideline will be guided by new research and technological advance-ments for preventing SSIs.ARTICLE INFORMATIONAccepted for Publication:March1,2017. Published Online:May3,2017.doi:10.1001/jamasurg.2017.0904Correction:This article was corrected on June21, 2017,to fix corrupted numbering and update abstract and methods.Author Affiliations:Division of Healthcare Quality Promotion,Centers for Disease Control and Prevention,Atlanta,Georgia(Berríos-Torres,Stone, Donlan);Center for Evidence-Based Practice, University of Pennsylvania Health System, Philadelphia(Umscheid,Leas,Kelz,Morgan); College of Public Health,The University of Oklahoma Health Sciences Center,Oklahoma City (Bratzler);Carolinas Healthcare System,Charlotte, North Carolina(Reinke);Department of Surgery, University of Cincinnati College of Medicine, Cincinnati,Ohio(Solomkin);Section of Acute and Critical Care Surgery,Washington University School of Medicine in St Louis,Saint Louis,Missouri (Mazuski);American College of Surgeons Representative,University of Washington Medical Center,Seattle(Dellinger);Surgical Infection Society Representative,Veterans Affairs Boston Healthcare System,Boston University and Harvard Medical School,Boston,Massachusetts(Itani); Musculoskeletal Infection Society Representative, Mayo Clinic College of Medicine,Rochester, Minnesota(Berbari);American Academy of Orthopaedic Surgeons Representative,Rush University Medical Center,Chicago,Illinois (Segreti);American Academy of Orthopaedic Surgeons Representative,Rothman Institute, Philadelphia,Pennsylvania(Parvizi);Quality Department,Littleton Adventist Hospital,Denver, Colorado(Blanchard);Association of Perioperative Registered Nurses Representative,New York Methodist Hospital,Brooklyn(Allen);Laboratory for Microbiology and Infection Control,Amphia Hospital,Breda,the Netherlands(Kluytmans); Julius Center for Health Sciences and Primary Care, University Medical Center,Utrecht,the Netherlands (Kluytmans);Department of Surgery,San Francisco General Hospital,University of California,San Francisco(Schecter).Author Contributions:Dr Umscheid and Ms Stonehad full access to all of the data in the study andtake responsibility for the integrity of the data andthe accuracy of the data analysis.Study concept and design:Berríos-Torres,Umscheid,Bratzler,Leas,Stone,Kelz,Morgan,Mazuski,Dellinger,Itani,Berbari,Parvizi,Blanchard,Kluytmans.Acquisition,analysis,or interpretation of data:Berríos-Torres,Umscheid,Bratzler,Leas,Stone,Kelz,Reinke,Morgan,Solomkin,Mazuski,Dellinger,Segreti,Allen,Kluytmans,Donlan,Schecter.Drafting of the manuscript:Berríos-Torres,Umscheid,Leas,Stone,Kelz,Reinke,Morgan,Itani,Berbari,Segreti,Blanchard.Critical revision of the manuscript for importantintellectual content:Berríos-Torres,Umscheid,Bratzler,Leas,Stone,Kelz,Reinke,Solomkin,Mazuski,Dellinger,Itani,Berbari,Segreti,Parvizi,Allen,Kluytmans,Donlan,Schecter.Statistical analysis:Berríos-Torres,Umscheid,Leas.Administrative,technical,or material support:Berríos-Torres,Bratzler,Leas,Stone,Morgan,Itani,Parvizi.Study supervision:Berríos-Torres,Umscheid,Bratzler,Stone,Itani,Berbari,Parvizi.Conflict of Interest Disclosures:Drs Umscheid,Kelz,and Morgan and Mr Leas reported receivingfunding from the Centers for Disease Control andPrevention to support the guideline developmentprocess.Dr Bratzler reported being a consultant forthe Oklahoma Foundation for Medical Quality andfor Telligen(a nonprofit Medicaid external qualityreview organization)and reported that hisinstitution received payment for his lectures,including service on speakers’bureaus fromPremier and Janssen Pharmaceuticals.Dr Reinkereported receiving lecture fees from Covidien andreported being a paid consultant for Teleflex.DrSolomkin reported receiving grants for clinicalresearch from,receiving consulting fees regardingclinical trial data,serving on an advisory board for,or lecturing for honoraria from the following:Merck,Actavis,AstraZeneca,PPD,Tetraphase,Johnson&Johnson,and3M.Dr Mazuski reportedbeing a paid consultant for Bayer,CubistPharmaceuticals,Forest Laboratories,MedImmune,Merck/Merck Sharp and Dohme,and Pfizer;reported receiving lecture fees from ForestLaboratories,Merck/Merck Sharp and Dohme,andPfizer;and reported that his institution receivedfunding for his consultancy to AstraZeneca andgrants from AstraZeneca,Bayer,Merck/MSD,andTetraphase.Dr Dellinger reported receiving grantsfor clinical research from,serving on an advisoryboard for,or lecturing for honoraria from thefollowing:Merck,Baxter,Ortho-McNeil,Targanta,Schering-Plough,WebEx,Astellas,Care Fusion,Durata,Pfizer,Applied Medical,Rib-X,Affinium,and3M.Dr Itani reported that his institutionreceived grants from Merck,Cubist,Dr Reddy’s,Sanofi Pasteur,and Trius for research trials;reported clinical advisory board membership atForrest Pharmaceuticals;and reported payment fordevelopment of educational presentations for MedDirect and Avid Education.Dr Berbari reported thathis institution received a grant from Pfizer for aresearch trial for which he serves as the principalinvestigator.Dr Segreti reported receiving lecturefees from Pfizer,Merck,and Forest Laboratoriesand reported owning stocks in or having stockoptions from Pfizer.Dr Parvizi reported being a paidconsultant for Zimmer,Smith and Nephew,ConvaTec,TissueGene,CeramTech,and Medtronic;reported receiving royalties from Elsevier,WoltersKluwer,Slack Incorporated,Data Trace Publishing,and Jaypee Brothers Medical Publishers;andreported having stock options with Hip InnovationTechnologies,CD Diagnostics,and PRN.Dr Allenreported receiving lecture fees from Ethicon androyalties from Wolters Kluwer as an author forInfection Control:A Practical Guide for HealthcareFacilities.Dr Kluytmans reported being a paidconsultant for3M,Johnson&Johnson,and Pfizer.No other disclosures were reported.Funding/Support:The Centers for Disease Controland Prevention(CDC)supported the developmentof the guideline.The activities of Drs Umscheid,Kelz,and Morgan and Mr Leas were supportedthrough a short-term detail under contract at CDC(10IPA1004117,10IPA1004133,11IPA1106551,11IPA1106555,and11IPA1106565).Role of the Funder/Sponsor:Centers for DiseaseControl and Prevention conducted the full guidelinedevelopment process,directing the design andconduct of the systematic reviews;collection,Clinical Review&Education Special Communication CDC Guideline for the Prevention of Surgical Site Infection,2017E6JAMA Surgery Published online May3,©2017American Medical Association.All rights reserved.。
利奈唑胺的药理分析综述

利奈唑胺的药理分析综述作者:曲小艺来源:《中国科技博览》2016年第01期中图分类号:R9 文献标识码:A 文章编号:1009-914X(2016)01-0346-01利奈唑胺(linezolid)是一种人工合成的噁唑烷酮类抗菌药,对大多数革兰阳性致病菌都有良好的抗菌活性,与其他抗菌药多无交叉耐药现象,加之组织、体液分布广泛以及给药方法便捷,使得其治疗多重耐药革兰阳性菌感染的有效性和安全性均很好,在临床上受到广泛的关注。
1 作用机制和抗菌活性作为一种新型抗菌药,利奈唑胺作用于细菌的50S核糖体亚单位。
但与其他抗菌药不同,利奈唑胺不影响肽基转移酶活性而只是作用于翻译系统的起始阶段,通过抑制mRNA与核糖体连接、阻止70S起始复合物的形成,最终产生抑制细菌蛋白质合成的作用。
由于作用部位及方式独特,利奈唑胺与其他抗菌药多无交叉耐药现象。
在耐药菌日益流行的今天,利奈唑胺的这一特性具有重要临床意义。
体外药敏试验结果显示,利奈唑胺对几乎所有的致病性革兰阳性菌、非典型病原体、各种分枝杆菌、诺卡菌以及革兰阳性的厌氧菌都有较好的抗菌活性,但对革兰阴性杆菌不敏感,可能与革兰阴性杆菌的外排机制有关。
体外药敏试验还显示,包括耐甲氧西林的金黄色葡萄球菌、耐甲氧西林的凝固酶阴性的葡萄球菌在内的葡萄球菌和耐万古霉素的肠球菌在内的肠球菌对利奈唑胺都100%敏感。
10多年的临床应用经验表明,利奈唑胺对多种革兰阳性致病菌、包括耐药菌所致感染均有很好的疗效。
此外,利奈唑胺对日益常见的耐多药结核杆菌和泛耐药结核杆菌也有明显的抗菌活性和治疗疗效,但因利奈唑胺不是常规抗结核药,故目前尚无相应的体外药敏试验数据。
2 药动学特点利奈唑胺为时间依赖性抗菌药,口服后吸收完全、生物利用度近100%,可以经静脉给药-口服方法进行序贯治疗。
利奈唑胺的血浆蛋白结合率为31%,分布容积为40~50 L,每12小时口服给药600 mg后0.5~2 h达到血药峰浓度(15~27 mg/L),血药消除半衰期(3.4~7.4 h)较长,且对敏感菌有一定的抗生素后效应,可一日2次给药。
内隐记忆
内隐记忆(IMPMEMORY)简介:最早对内隐记忆这一心理现象进行描述的学者是法国近代哲学家笛卡尔,但直到上世纪60 年代末,心理学中对记忆的探讨仅仅限于意识状态下的记忆规律。
1968 起年英国学者Warrington 和Weiskrantzd[在对健忘症患者启动效应的研究中发现:健忘症患者虽然不能有意识地保持学习内容,在再认测验中无法辨认出先前学习过的单词,但在补笔测验中却对先前呈现过的单词表现出与正常人一样的保持效果。
这一特殊记忆现象的发现激起了人类对无意识记忆的探讨的兴起。
Schacter等1980年进行了一个实验研究。
首先让被试阅读一些单词,例如:assassin,octopus,avocado,mystery,sheriff,climate。
一小时后,再做两次实验:首先是再认测验,被试不会有任何困难;其次是补笔测验,向被试呈现一些有字母残缺的单词,要求尽可能地将残缺字母填补上,例如:ch__nk,o_t_us,_og_y_,_l_m_te。
在这次测验中,被试对其中的两个残缺单词很难做出正确解答,即chipmunk和bogeyman;而对其它单词就很容易了。
这是因为在一小时以前见过octopus和climate这两个词。
这种记忆被称为启动效应(priming effect)。
在实验中,Schacter等人对测验的时间间隔进行了控制,有的是在一小时后,有的是在一周后进行测试。
在这两种情况下,后者对所学单词的再认,即有意识的回忆,远不如前者准确,但对于补笔测验的结果,两种情况下完全等同。
这就是说,引起单词填补测验中的启动效应的,是在测验前看到这一单词所引起的某种并非自觉记忆的因素。
同样有意思的是,对某一单词而言,即使被试不记得在学习阶段看到过这一单词,启动效应也会产生。
事实上,不管被试记不记得在学习阶段看到过该单词,启动效应的强度是一样的。
这些研究结果似乎告诉我们:启动效应的产生不依赖于有意识的记忆。
吉他鉴别
弘力乐器关于近期Schecter仿冒琴的严正声明Schecter是北京弘力乐器有限公司的旗下代理品牌。
自Schecter进入中国市场以来,因其优良的产品质量而备受广大琴友的喜爱。
随着Schecter品牌不断深入人心,近期一些不法商贩在各地琴行以及淘宝等网络商城公然销售一些印有Schecter LOGO的假冒商品,并冠以“原单、正品、外单”等名目欺诈广大消费者。
这些质量粗糙的仿制品不仅侵害了消费者的合法权益,也严重影响了我司以及美国Schecter公司的合法权誉。
北京弘力乐器有限公司特此作出严正声明如下:望正在销售假冒Schecter商品的相关机构及个人认清自己行为的违法性,尽快将假冒商品下架。
如仍我行我素,继续销售该产品坑害广大消费者,北京弘力音响乐器有限公司将采取进一步的法律行动以维护消费者及我司的合法权益。
同时提醒广大消费者在购买相关产品时尽量选择我司指定的经销商,另请注意每支琴的琴头背面都有该琴独一无二的编码,在购买的时候可随时致电我司进行查询,查询电话:010-5869 1218。
下面详细描述一下这些假琴的基本特征及辨别方法:一,市场上流通假琴最多的几个型号:1.标有韩国制造的C-1 SheDevil(女妖);2.标有韩国制造及中国制造的C-1 Hellraiser FR(此型号从未在中国生产);3.标有中国制造的Damien-6 FR(此型号从未中国生产)、Omen-6 Extreme等;还有部分韩产及国产已停产或已改配置的型号,如C-1 FR、Tempest Custom、S-1、C-1 Plus (此型号我司从未引入国内)等。
二,假琴特征:1,韩产系列凡是以H09,或者09开头的一律为假琴!C-1 SheDevil(女妖)在中国市场的火爆程度相信大家是有目共睹的,完美的做工,魅惑的外观。
正是这些,造成了现在大量C-1 SheDevil仿琴的出现。
在此,明确的告知广大琴友,C-1 SheDevil在2008年年底就已停产,我司原有库存也早已销售一空,且我司最后一批次的C-1 SheDevil琴头编号为H08开头。
SCHECTER评测
祖国版SCHECTER评测传说中的祖国版DIAMOND系列祖国版SCHECTER评测传说中的祖国版DIAMOND系列DAMIEN 6再看品丝工艺,尤其注意品丝头儿,修的真的很不错,形状非常接近SCHECTER的USA CUSTOM(毫不夸张,只是USA的修的更圆)。
这种工艺在祖国琴中真的很少见。
这确实也是分辨工艺是否过关的一个尺度。
再看品标的镶嵌,虽然这东西和音色没什么大关系。
但也多少体现的工厂的认真程度,比如。
有没有出边儿啊。
有没有没压平的地方阿。
边缘的木头有没有多余的伤啊。
等等。
用以上标准来衡量的话。
镶嵌的确实不错。
在看拾音器。
EMG-HZ。
这款PICKUP不用多说什么了。
不好也不坏。
噪音小(其实多数质量没有问题的双线圈噪音都不大)声音和大家经常谈论的EMG81阿。
85啊。
89啊。
没什么太大关系。
失真稍散。
感觉声音略微靠后。
但原声不会像EMG 81或85那样直接过载。
也不是完全没有可取之处。
毕竟PICKUP的音色对使用者来说是各有所好。
喜欢就用。
不喜欢可以直接换。
换起来也不麻烦。
电路部分很简单。
三档TONE开关。
没有可以按下去或者拔起来的东西。
虽然韩国产的SCHECTER多数有可以拔起来切单的线路,但就我个人而言。
我就当它不存在。
这种切单我个人感觉就是。
声音变细了。
噪音加大了。
但真正单线圈那种诱人的力量却没得到。
索性就不要切了。
(以上是个人的略见)值得一提的是它3TONE开关的角度。
对习惯用小指快速换档的乐手来说,调的非常准确。
虽然这不是什么难事。
自己也可以拧松调好再紧上。
但我觉得。
这还是能充分体现了一个工厂或一个品牌的认真态度。
琴颈是4钉连接的,没什么特殊。
但我很喜欢这个牌儿~估计很多琴龄在10年左右的朋友都很习惯看到这种牌儿。
韩产的SMICK阿。
日产的JACKSON阿。
当年的很多品牌都用这种牌儿。
用高硕师傅的话讲:老物件了!琴头背后是GROVER的弦钮,手感很不错。
没有咯啦咯啦的感觉,很平滑。
比较好电吉他品牌介绍
比较好电吉他品牌介绍首先,PRS吉它是绝对物超所值的,它的材料、设计和技术纯熟度都经过详尽的研究。
如果不相信我们的话,您大可以向我们的竞争者问问,他们是否把木材的湿度降到7%以下我们的檀木指板的湿度为3%,是否每一道生产线的工人都是吉它手,或者是否他们会定期追加投资用于购买更好的机器和设备?PRS的吉他绝对可以"保值",因为我们的产品有很高的剩余价值,在二手市场上不断被吉它收藏者和鉴赏家们追捧。
事实上,许多我们的限量版吉它例如Dragon系列产品,目前的市场价比它当初的售价要高得多。
无疑,在高端吉它品牌中,PRS占据着绝对的优势。
Paul Reed Smith可是白手起家的。
在大学里,他独操作自己的研究课题,作出了自己第一把吉他,而他的梦想也就是有朝一日,能成为一个成功的吉他制造者。
1985年,他和一些难得的支持者如Carlos Sanata一起,且义无反顾地投身自己的梦想,在马里兰州的安那波利斯市开设了第一家工厂。
PRS Custom系列中,经典黄、深红色和皇家兰色以及现在闻名于世的小鸟品记都是这家工厂第一批的产品。
也是我们目前生产的核心产品。
1996年一月,PRS又开设了一间工厂,占地2万5千平方英尺,员工人数达125人,并始终如一地坚持制作高品质的吉它产品,Paul Reed Smith几乎每天呆在厂里,坚持严把质量关,精心维护PRS的出厂品质。
除此以外他还掌管R&D部门研究开发新的产品项目。
作为一个总裁,他还经常把玩一下吉他,这的确很少见的。
他自组的Dragons的乐队,几乎在全球各个交易会中都大显身手,并且参与了一系列的推广活动。
Schecter美国Schecter吉他,1976年创立于美国加州的Schecter GuitarResearch至今已有35年的历史。
从早期只制作高品质定制级录音室用琴,发展到今天将几百种型号的产品销往全球各地的知名大厂,Schecter以其优良的做工、出众的音色、超炫的外观和长高性价比成为新一代重型摇滚/金属吉他的典范,在全世界组成不计其数的Schecter军团。
腹膜透析的原理及方式

腹膜透析的发展史
20世纪20年代初 50年代
60年代 70年代 80年代末-90年代
在动物实验中就发现腹膜具有半透膜的功能 从1923年德国医生Ganter首次将腹透应用于人体治疗,一 直到5等相继发展了瓶装透析液和简单的透析装 置(我国开展PD疗法)
清除代谢废物 补充体内缺少的物质 排出多余水分
基本原理(一)弥散
• 如果血中某种溶质的浓度高于
腹腔内的透析液,而腹膜又能
透过者,则会弥散入透析液内。 反之,如透析液中浓度高者, 则该种物质也会进入血内。经
血液中的物质:肌酐、尿 素氮、钾、蛋白质
过一定时间的透析后,病人血
中的可透过溶质会与透析液内
的水平接近。透析液内的电解
腹膜结构
“三孔模型”学说,认为腹膜毛细血管壁的转运屏障作用具有分子大 小选择性,溶质和水经过毛细血管壁的转运是通过一系列的“孔” 进行 的。 小孔:数量很多,孔径在4-6nm,用于转运小分子溶质如尿素、肌酐、
葡萄糖、电解质等,可能就是内皮细胞间的裂隙; 大孔:数量很少,不到总孔数的0.1%,孔径>20nm。用于转运大分子
腹膜透析的原理及方式
XXX
XXXX年X月X日
主要内容
1、腹膜透析的概述 2、腹膜透析发展历史及发展现状 3、腹膜透析的原理 4、腹膜透析的方式 5、腹膜透析的必备条件及缺点
腹膜透析的概念
腹膜透析(peritoneal dialysis ,PD)是利用腹膜作为透析 膜,向腹腔注入透析液,膜一侧毛细 血管内血浆和另一侧腹腔内透析液借 助溶质浓度梯度和渗透压梯度,进行 溶质和水分的转运,并不断更换透析 液,以达到清除体内毒素,脱去多余 水分、纠正酸中毒和电解质紊乱的治 疗目的。
溶质如白蛋白等; 超微孔:孔径<0.8nm,仅能让水分子通过,其分子结构是内皮细胞
schecter tempest standard

schecter tempest standard
Schecter Tempest Standard 是一款吉他,它具有以下特点:
1. 设计:Schecter Tempest Standard 采用了经典的 Stratocaster 设计,具有双缺角、单切和舒适的弧形琴颈。
这种设计提供了良好的可玩性和人体工程学。
2. 木材:吉他的琴体通常由桤木或椴木制成,这两种木材提供了平衡的音色和良好的共鸣。
琴颈则通常采用枫木或枫木与玫瑰木的复合材料,以提供稳定性和舒适的手感。
3. 拾音器:Schecter Tempest Standard 配备了一对双线圈拾音器,这种拾音器类型通常产生较强的输出和丰富的音色,适合各种音乐风格,从摇滚到金属都能有出色的表现。
4. 硬件:吉他的硬件包括调弦器、琴桥和控制旋钮等,通常采用高质量的金属制成,以确保可靠性和长期使用。
5. 音色:由于其设计和拾音器的选择,Schecter Tempest Standard 可以产生明亮、有力且富有攻击性的音色,适合演奏重型音乐和高增益的音色。
总的来说,Schecter Tempest Standard 是一款适合中高端吉他手的乐器,无论是在舞台演出还是录音室录制中,它都能为你带来出色的表现。
然而,具体的评价还需要根据个人的喜好和演奏风格来确定,最好亲自试弹以了解其是否适合你。
Schecter Bass Guitar 电子路径图说明书

Free USA Shipping On Orders Over $79 006 Deluxe Wiring Diagram View Schecter 006 Elite Wiring Diagram View Schecter Basses Wiring Diagrams Ultra, S Customs, S Elites, C-4-5 View Schecter C1-Classic Wiring Diagram Older Spec View Schecter C1 Classic Wiring Diagram View Schecter C1 EA Wiring Diagram View Schecter C1 Exotic Wiring Diagram View Schecter C1-FR Floyd Rose Diagram C1FR View Schecter Damien 6 Wiring Diagram View Schecter Damien 7 Wiring Diagram View Schecter Hellraiser Avenger Wiring Diagram View Schecter Hellraiser C-7 Wiring Diagram View Hellraisers C-1 and C-1FR Floyd Rose View Schecter Omen 6 and Omen 7 Wiring Diagram View Schecter PT Fastback Wiring Diagram View Schecter Stiletto Deluxe Wiring Diagram View Schecter Stilletto Studio Wiring Diagram View Sch
schuster品牌介绍

schuster品牌介绍
Schuster 是一个历史悠久的德国品牌,以质量和技术为根本,拥有完整的产品线,目前整机在意大利工厂制造。
Schuster是Unical AG S.p.A.公司旗下的一个注册商标。
Unical AG S.p.A.公司是意大利前六大暖通公司之一,主要设计和制造壁挂炉、钢制模块锅炉、冷凝锅炉、商用大锅炉、蒸汽锅炉、地暖系统、太阳能系统、空气源热泵、空调、智能控制等系列暖通产品。
同时还为德、意、法、西、奥、英等国著名锅炉品牌提供壁挂炉、冷凝锅炉和钢制大锅炉的OEM贴牌生产。
1972年,Unical AG S.p.A.公司创立以来,先后在意大利中北部的Carbonara(卡博那拉)、Casteldario(曼多瓦)、Caorso (皮亚琴察)设立三处全自动生产基地。
Unical AG S.p.A.公司的冷凝锅炉技术和各项指标达到世界顶级水平,产品超过150种,拥有几十项国际专利技术,是目前世界上少数几家自主研发大功率冷凝模块锅炉的暖通厂家之一。
获得了多项国际认证:检测中心CE认证、各产品CE认证、ISO9001、ISO14001、OHSAS18001、美国ASME、澳大利亚SAI、TIFQ认证、俄罗斯CBPO-TNCK燃气认证等。
Unical AG S.p.A.公司秉承“科技创造美好生活”的现代理念,40年来一直致力于为用户提供舒适、安全、环保、低能耗、人性化的产品和服务,为现代生活提供想象和享受空间。
Schuster 品牌致力于成为全世界追求产品质量的人心目中技术、安全以及简单的代名词。
今天,Schuster 的系列产品行销全球,产品线全面覆盖从家用到工业用的所有领域,并且整机性价比高。
健忘症病人的内隐记忆

健忘症病人的内隐记忆implicit memory(内隐记忆),指在不需要意识或有意回忆的条件下,个体的过去经验对当前任务自动产生影响的现象,因为内隐记忆是在研究精神病患者的启动效应(priming effect) 中发现的,所以人们常把内隐记忆和启动效应作为同等概念使用。
最早对内隐记忆这一心理现象进行描述的学者是法国近代哲学家笛卡尔,但直到上世纪60 年代末,心理学中对记忆的探讨仅仅限于意识状态下的记忆规律。
1968 年起英国学者Warrington 和Weiskrantzd[在对健忘症患者启动效应的研究中发现:健忘症患者虽然不能有意识地保持学习内容,在再认测验中无法辨认出先前学习过的单词,但在补笔测验中却对先前呈现过的单词表现出与正常人一样的保持效果。
这一特殊记忆现象的发现激起了人类对无意识记忆的探讨的兴起。
1985 年Schacter 和Graf首次提出了内隐记忆这一概念,用以表述在无意识情况下,过去的经验或学习对人类行为产生影响的现象,从此内隐记忆成为心理学研究中的一个最重要课题。
国内心理学界对内隐记忆的研究始于上世纪80 年代,杨治良、朱滢教授是国内最早从事内隐记忆研究的学者,特别是杨治良教授20 年来一直致力于无意识心理现象的研究,为我国心理学在这一领域的发展做出了巨大的贡献。
最早可追溯到1991年杨治良发表在《心理学报》上的《内隐记忆的初步实验研究》。
就目前的研究状况来看,对内隐记忆可从以下几个方面来理解:1.从现象上看,内隐记忆是被试者在操作某任务时,不经有意识地回忆而存贮在大脑中的信息却会在操作中自动起作用的现象。
这就反映出了先前所学内容的存在和作用。
其特征是,被试者对信息的提取是无意识的。
2.从研究模式看,内隐记忆是启动效应的一种,这在内隐记忆与启动效应的关系中已有论述。
3.从测量上看,内隐记忆是另一类记忆任务,这类任务不要求被试者有意识地去回忆所学习的内容,而是要求被试者去完成某项操作,在被试者的操作中反映出其所学内容的作用。
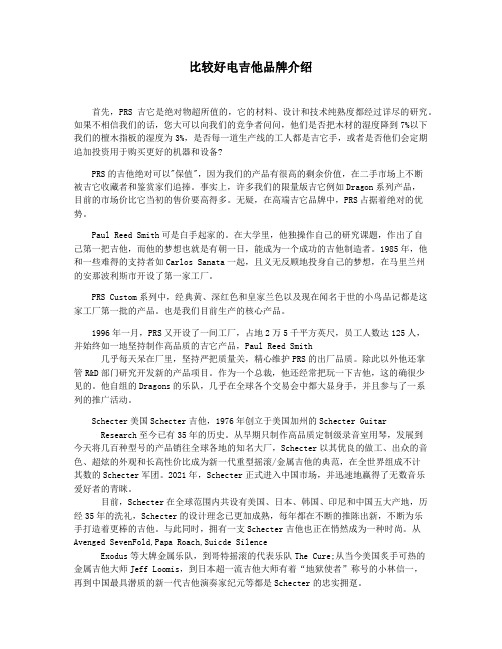
SWITCHERTOO电路
拾音器品牌比较多的比如DiMarzio Seymour Duncan EMG这样只做拾音器的公司包括他们的签名款和手工款之后还有又生产吉他又生产拾音器,或者拥有一些自己技术的比如FENDER ,Gibson Suhr,TOM ANDERSON ,Carvin ,schecter这样牌子包括他们的签名款和手工款。
还有一些小产量,长量不大的或者范围面比较少的吉他拾音器TV Jones,Bill Lawrence,SCHALLER,BKP,lollar low wing。
SWITCHERTOO电路这是TA独有的电路板式的电路,没有一般5-way的拨档三个三档开关分别控制三个拾音器状态,然后从总体电路上三个拾音器是并联在一起的,想单独用一个拾音器,就要把其他两个关上三个小开关的具体功能,拨到下是一般串联模式,中间是关掉拾音器,拨到上是要么并联要么切单,后边电路板上有一个具体决定并联还是切单的开关,还有个单独的小开关是可以直接切到琴桥串联的,方便solo根据TA的制琴理念,拾音器设计时就考虑到串联并联或切单的效果,变化的效果比其他厂牌的拾音器更加明显TA的单线圈除了VA系列拾音器之外,其他的都是叠起来的双线圈,下边是dummy线圈,切单后甩掉dummy的加载,声音会大很多,高频低频都有增加,像打了clean booster一样,尤其是被称为90年代最经典modern sc tone的sa系列,三个模式都很好用后来出的sf系列,因为设计时以“串联时就有sa切单的清亮”为目标,切单时反而太尖了而TA的双线圈虽然很单听很modern很紧,实际上输出并不大,大热门的H2+的输出还不到11K,切单后音量无法和TA的单线圈比,而H3等级的串联声音则和H2差很多可用的拾音器模式虽有3种,实际最常用的还是其中两种,单线圈的切单&串联,和双线圈的并联&串联TA的拾音器,反级反绕的不在中间,而是前拾音器,和其他厂牌合用比较麻烦TA的电位器等电子零件,用的是ahpha等货色,本来没五档开关就要拨拨拨拨拨拨拨调音色,就这样还不用寿命长点的。
Teaching_Cultural_Identity_through_Modern_Language

Teaching Cultural Identity through Modern Language: Discourse asa Marker of an Individual‟s Cultural IdentityPavel V. SysoyevAssociate Professor of American Studies and Applied LinguisticsTambov State UniversityTambov, Russia(JFDP)Lyn R. DonelsonVisiting Lecturer of English as a Foreign LanguageTambov State University, RussiaTambov, RussiaIntroductionThe dialectical connection between language and culture has always been a concern of second language (L2) teachers and educators. However, the degree to which L2 culture has been incorporated into L2 teaching has been a subject of rapid change throughout language teaching history. For example, if during the first decades of the 20th century researchers discussed the importance and possibilities of including a cultural component into L2 curriculum (e.g., Lado, 1954), more recent studies show inseparability between L2 and L2 culture teaching. In addition, a L2 culture is presented as an interdisciplinary core in many L2 curricula designs and textbooks (Byram, 1989; Byram & Fleming, 1998; Kramsch, 1993; Saphonova, 1996; Sysoyev, 1999, 2001a; Savignon & Sysoyev, 2002). Despite these facts, scholars still argue about what the final level of learners‟ sociocultural competence should be.The Modern National Curricula Standards for the Foreign Languages (U.S.A.) has published official requirements for sociocultural education in Europe and Russia that state that as a result of L2 culture teaching learners should develop cultural awareness, which includes the development of toleranceand empathy towards representatives of different cultures (ACTFL, 1999; Byram & Fleming, 1998; Byram & Risager, 1999; Saphonova, 1999; Savignon, 2002).In our previous research, we argued that cultural identity is the next level L2 learners should achieve after cultural awareness (Sysoyev, 2001a, b; Savignon, Sysoyev, 2002; Sysoyev, 2002a, b). After learning about other cultures in the mode “we” and “they” (for details see Hall, XXX), which often results in the creation of false negative or positive stereotypes andgeneralizations about a L2 society, L2 learners should come to anunderstanding of their own place within the spectrum of cultures. Such understanding means seeing commonalties and universals that exist beyondgeopolitical boarders of L1 and L2 countries and which unite people all over the world. Moreover, undertaking our research within the frames of postmodern theory, we argued that learners should see themselves as polycultural subjects with multiple group membership.When communicating or expressing themselves, people are perceived asmembers of certain groups. Such group membership may be based on race, ethnicity, gender, social class, occupation, territory, etc., and most often includes multiple factors. The reflection of a particular facet of cultural identity or group membership is facilitated in many cases through discourse. In this paper, we examine one of the possible ways of teaching cultural diversity – teaching discourse as a reflection of the sp eakers’ cultural identity. The argument is made that in communication speakers attempt to establish and construct the salient facet of their cultural identity through discourse. We also argue that awareness of how discourse varies between representatives of different ethnic, social class, gender, and age groups, as well as how the discourse of an individual varies depending on the role that he or she plays, will enable L2 learners to see people and societies polyculturally, aiding them in perceiving diversity as a norm in modern polycultural societies.Cultural Identity in L2 TeachingIdentity as a theoretical construct is not a new idea. It was originallydeveloped within the field of psychology, where the major focus of researchers was altering of an indi vidual‟s state and condition over time through changes in his or her contexts (e.g., Erikson, 1968). Initially however, for psychologists an individual’s identity represented a considerably stable construct, it was supposed to change only 4-5 times during an individual‟s life, usually when that person entered a new age group (e.g., child аyoung adult а grown up а elderly). Later on, the development of social psychology enabled a more advanced understanding of identity as a social construct. One of the notable leaders in the field, Tajfel, introduced the term social identity and defined it as “[T]hat part of an individual‟s self-concept which derives from his knowledge of his membership of a social group (or groups) together with the emotional significance attached to that membership” (Tajfel, 1974: 69). Though Tajfel and other contributors to his volume introduced a new concept of individual understanding of groupme mbership, Tajfel‟s social identity theory was criticised for focusingexcessively on the self, rather than on the dialogical interrelationship between self and group.In the field of applied linguistics, identity has been receiving increasedattention since the recognition of its importance in L2 learning, demonstrated by Bonny Norton Pierce (1993, 1995) in her study ofimmigrant women. Norton Pierce introduced the term social identity to refer to “how a person understands his or her relationship to the wo rld, how that relationship is constructed across time and space, and how that person understands possibilities for the future” (Norton (formerly Pierce), 2000,p.5). The study demonstrated that for the research subjects, possibilities for the future were strongly connected with L2 communicative competence. Such understanding of self within a linguistic milieu affected the way L2 learners perceived themselves and are perceived by others in an L2 environment. Therefore, Norton‟s social identity research was t he first theory that attempted to connect L2 teaching, language learners, and their understanding of themselves within a spectrum of cultures.In Europe, the term social identity has been widely used by Michael Byram(1998) and his colleagues (Byram, Zarate & Neuner, 1997; Byram & Risager, 1999) in their argument for promoting the importance of teaching L2 for the development of a common European identity among L2 learners. Knowledge of common roots as well as cultural and historical heritage of L2 learners is believed to be a major and essential step in the social unification of European societies. As a result, the “Identity” concept is currently being applied in various European L2 programs (Byram, Nichols & Stevens, 2001). Interest in the relationship b etween an individual‟s identity and L2 learning has recently been growing. In her comprehensive review, Norton (2000) demonstrates that researchers from various fields have brought diverse perspectives to our understanding of the relationship between language, language learning, and identity. The use of different theories and methodologies by different scholars has affected the ways in which researchers conceptualize identity, and it has also resulted in the simultaneous emergence and use of different terms that describe identity as a sociocultural construct. For example, Morgan (1997), Pierce (1993, 1995), Norton (2000), and Byram (1998), focus on social identity in their research, Duff and Uchida (1997) focus on sociocultural identity, Schecter and Bayley (1997) on cultural identity, and Leung, Harris and Rampton (1997) on ethnic identity. Norton (2000) argues that all of these terms, throughout many contexts, are likely to be used as synonyms; however, power relationships between the language learner and language speaker will determine which facet of one‟s identity is salient at a particular situation.In this scholarship, we chose to use the term cultural identity, which aftera comprehensive review of philosophical and psychological literature in our previous research (Sysoyev, 2001b), was defined as an individual’srealization of his or her place in the spectrum of cultures andpurposeful behavior directed on his or her enrollment and acceptance into a particular group, as well as certain characteristicfeatures of a particular group that automatically assign an individual’s group membership (pp. 37-38).Individuals‟ cultural identity as a construct consists of a countless number of facets. Most commonly referred to and described in literature are the following facets or types of one‟s cultural identity: racial, ethnic, social, economic, geopolitical, gender, religious, ability/disability, language, professional, etc. (see figure 1) Each of the facets represents a specific category, within which a person has specific membership(s).When understanding cultural identity as a multi-faceted construct, it is important to note that in communication the choice of portraying a specific facet of one‟s identity will be context specific and negotiated between the participants of the exchange. If a salient facet of the identities of both participants is the same, then it becomes invisible and a dialogue of cultures takes place (Bakhtin, 1981; Bibler, 1991; for discussion see Savignon & Sysoyev, 2002). However, as Heller (1987) warns, conflict occurs when both participants of the exchange belong to different groups within one facet (e.g. social facet: upper class and lower middle class). In such a situation, group membership may become visible and it may affect the outcomes of the exchange. Discourse then, in most cases becomes a key factor in establishing one‟s cultural identity (e.g., Ochs, 1993; Kramsch, 1998).Discourse and cultural identityWhen people use language to negotiate their meaning, they creatediscourse–“a continuous stretch of language – oral or written – which has been produced as a result of an act of communication and perceived to bemeaningful, unified, and purposeful” (Celce-Murcia & Olshtain, 2000, p. 237). Since language and culture are intertwined, it is commonly believed that there is a natural connection between discourse and an individual‟s cultural identity, where discourse is viewed as the reflection of one‟s group membership. By the language register, accent, word choice, and speech pattern of a person, he or she is perceived as a member of a particular social and cultural group. When people consciously or subconsciously choose certain languages or variants of the same language to associate themselves with particular groups, they engage in codeswitching. If how one wants to be seen and how one is perceived by others match, then the act of communication is completed successfully. However, problems occur when there is a mismatch between one‟s language (code) and that individual‟s group membership. A desire to refuse the same code or to adapting to the same language, when one interlocutor is definitely a member of a common culture, may be perceived as an affront. A vivid illustration given my Claire Kramsch (1998) representing cultural conflict generated by mismatched codes can be extracted from an interview between two American Disc Jockeys (DJ1, DJ2) and an American singer (SG), all members of a specific discourse community.1. DJ1: So whatz up wit da album shottie?2. SG: What‟s up with th e album shottie3. DJ1: Oh, excuse me. How are things progressing with your upcomingalbum? (laughter)Come on, girl! You know what I‟m sayin‟. You KNOW you know da terminology! Don‟t front!4. DJ2: Yeah, an‟ if ya don‟t know, now ya know (laughter)5. DJ1: Or at leas ack like ya know!6. SG: I know, I know, I‟m jus‟ messin‟ wit y‟all.(From Kramsch, 1998: 71)All three members belong to a specific discourse community in which thelanguage used differs from the “Standard” American English. DJ1 starts the conversation using the language of his and the other conversationalistsdiscourse communities. In Turn 2, the singer chooses not to associate herself with the Disc Jockeys‟ language community, which is characterized by the language used by DJ1. So, in reply, questioning the word “shottie” in turn 2, she makes it explicit that she is not participating within their discourse dialect. Her reaction made DJ1 reformulate his question and use Standard English [turn 3]. In turns 3-5, DJ1 and DJ2 implicitly remind the singer of their common group membership. These reminders pressure the singer to codeswitch in turn 6 from Standard English to the common dialect shared between the three conversationalists.Similar to codeswitching, the reflection of one‟s identity in discourse can beobserved on the semantic level. Let‟s look at the following e-mail exchange between an L2 student (L2S) who is sharing his impressions about Salt Lake City and the United States and a native speaker of American English (NS). Both participants of the conversation are males in their mid 20s.L2S: … Salt Lake City is surrounded by the Rocky Mountai ns. They arecovered with snow, which glitters in the sun. You can see them from everywhere. It is so beautiful. The air is very fresh too and you can easily feel that. People are extremely friendly. I love looking at the beautiful clothing and jewelry in the stores. Man, I love this city, I love this country. NS: Dude, let me explain something. We are men, and it‟s not manly to love …beautiful clothing and jewelry.‟ Next time tell me you went to …an awesome gun show‟ or …saw some powerful truck engines.‟(Unpublished data from Pavel V. Sysoyev)There is no doubt that both speakers belong to different discoursecommunities – one to a community of native speakers, the second to a community of L2 speakers. There is nothing wrong with the “mistakes” the L2 student made, as English is not his native language and the major point of communication – getting the meaning across – was successfully achieved. It is plainly understood that he enjoyed the city very much. The native speaker corrected him and there would have not been anything else in this discourse, if not for the phrase “beautiful clothing and jewelry.” Since both interlocutors are males, the gender factor is supposed to be invisible. However, via this phrase –“beautiful clothing and jewelry” – gender identity comes into action. Ignoring political correctness and possible offence due to a sexist remark, the male native speaker tells what words and expressionsshould and should not be used, so there will not be a conflict between a L2 speaker‟s gender ide ntity and his or her reflection on the discourse. Application for L2 teachingOne of the major goals of humanitarian education in different parts of the world is to develop citizens of the world, who identify themselves culturally, and who see themselves within a broad spectrum of cultures. A foreign language is a prominent tool in achieving this goal. Therefore, teaching a L2 and a L2 culture for cultural identity will enable L2 learners to engage in the following:∙place themselves in the position of others;∙initiate and maintain intercultural contacts for the purpose of learning about values, norms, spiritual heritage, etc. of others, and act as representatives of native cultures;∙realize themselves as polycultural subjects with multiple group membership;∙accept diversity as a norm within modern polycultural societies;∙take an active part in the elimination and minimization of cultural inequality, cultural discrimination, cultural vandalism, and cultural aggression (for details see Sysoyev, 2002).Cultural identification as a psychological process happens through the selection of a pattern of behavior from a variety of patterns of behavior (or eclectic blending pattern) (for details see Sysoyev, 2001b). The only way to teach students to identify culturally is to teach them to see diversity within L1 and L2 polycultural communities. What is more important, L2 students should learn to see themselves as polycultural subjects with multiple group membership. Therefore, discourse analysis reflecting upon the polyculturality of people is a plausible way of teaching diversity and cultural identity. Reflection on one‟s cultural identity through discourse may appear to be a theoretical topic for students majoring in linguistics. After all, what is the importance of addressing this issue when teaching L2 students? In his theoretical research, based on the requirements for sociocultural education for schools with advanced exposure to modern languages (Saphonova, 1999), Sysoyev (2001a) lists a number of sociocultural strategies (within L2 communicative strategies) designed for establishing and maintaining international L2 contact in a spirit of peace and dialogue of cultures. Consequently, Savignon and Sysoyev (2002) provided empirical evidence that the ability to seek out and find one‟s position on a specific cultural topic provides hints for an individual‟s personal actions and gives L2 learners additional “space to maneuver.” On the one hand, it enables them to avoidnon-desirable cultural bumps and cultural conflicts. On the other – it maygive them new ideas and new opportunities for L2 communication. Introducing the elements of discourse analysis into L2 curriculum andteaching materials will give L2 learners the power and ability to enhance control over communicative events and in a long run will promote the dialogue of cultures to be established as a philosophy of interaction in modern polycultural communities.Conclusion This paper has examined one of the possible ways of teachingcultural diversity –teaching discourse as a reflection of the speakers’ cultural identity. We have demonstrated that in communication, speakers attempt to establish and construct the salient facet of their cultural identity through discourse. We have also argued that awareness of how discourse varies between representatives of different ethnic, social class, gender, and age groups, and how the discourse of an individual varies depending on the role that he or she plays, will enable L2 learners to see people and societies polyculturally, aiding them in perceiving diversity as a norm in modern polycultural societies.References1.Bakhtin, M. (1981). The dialogic imagination. Austin, TX: University of Texas Press.2.Bibler, V. (1991). M. M. Bakhtin, or the poetics of culture. Moscow: Politizdat Press.3.Byram, M. (1989). Cultural studies in foreign language education. Clevedon: Multilingual Matters.4.Byram, M., & Fleming, M. (1998). Language learning in intercultural perspective: Approaches through drama andethnography. Cambridge: Cambridge University Press.5.Celce-Murcia M., & Olshtain E. (2000). Discourse and context in language teaching. Cambridge: CambridgeUniversity Press.6.Ochs, E. Constructing social identity: A language socialization perspective. Research on Language and SocialInteraction, 26(3), 287-306.7.Pierce, B. (1993). Language learning, social identity, and immigrant women. Unpublished Doctoral Dissertation.Ontario: Institute for studies in education / University of Toronto.8.Pierce, B. (1995). Social identity, investment, and language learning. TESOL Quarterly, 29(1), 9-31.9.Saphonova, V. V. (1996). Teaching languages of international communication in the context of dialogue of culturesand civilization. Voronezh, Russia: Istoki.10.Saphonova, V. V. (1999). English as a foreign language curriculum for students in grades 10-11 of schools withadvanced exposure to modern languages. Moscow: Euroschool Press.11.Savignon, S. J. (Ed.). (2002). Interpreting communicative language teaching: Context and concerns in teachereducation. New Haven, CT: Yale University Press.12.Savignon, S. J., & Sysoyev, P. V. (2002). Sociocultural strategies for dialogue of cultures. The Modern LanguageJournal, 86(4), 508-524.13.Sysoyev, P. V. (1999). Sociocultural component in teaching American English (for schools with advanced exposure tomodern languages). Unpublished Doctoral Dissertation. Tambov, Russia: The Tambov State University.14.Sysoyev, P. V. (2001a).Individual’s cultural identity in the context of dialogue of cultures. Tambov, Russia: TheTambov State University Press.15.Sysoyev, P. V. (2001b). Language and culture: Looking for a new dimension in teaching L2 culture. ForeignLanguages at School Journal, 4, 12-18.16.Sysoyev, P. V. (Ed.). (2002). Identity, culture, and language teaching. Iowa City, IA: Center for Russian, EastEuropean, and Eurasian Studies.17.Sysoyev, P. V. (2002). Teaching foreign language culture for cultural identity and dialogue of cultures. In P. V.Sysoyev (Ed.), Identity, culture, and language teaching (pp. 7-28). Iowa City, IA: Center for Russian, East European, and Eurasian Studies.。
吉他品牌大全
FENDERGIBSONIBANEZJACKSONEPIPHONECORTSQUIERESPWashburnOVATIONAXLwaldenstarsunLandoFender是吉他史上的重要角色,Telecoaster;Stratocaster…ESP GUITAR日本手工吉他,美国也有做,品质不错,但很贵,有便宜的副牌。
Martin超有名木吉他,粉贵粉贵,但声音超好,很多录音室都有用。
Ovation著名的圆背吉他,每个名歌手都会拥有一支。
YAMAHA吉他的评价不如其他吉他产品,但Pacific和Weddington系列还不错。
Carving台湾很少见,品质不错。
Ibanez便宜又大碗,很好弹,喜爱摇滚型及他的人都会买一支来弹。
Epiphone很老的吉他厂,虽是Gibson的子公司,但历史比GIBSON更久。
TobiasGibson的Bass厂牌,高贵的好琴。
Cort韩国吉他,由美籍师傅设计,品质价格超正,不错喔。
STEINBERGER看过无头的碳纤维琴吗?RickenBacker独特的外型,有复古的风格。
ANDERSON超好的手工吉他。
Peavay也做便宜又大碗的AMP。
GODIN/SEAGULL加拿大吉他,但木吉他也不错。
史上最伟大的吉他之一,有空就看看吧,音质棒,烤漆赞。
HAMER不错的吉他,很多乐手私底下都有一把。
KAMAN MUSIC瞒有名的,但是台湾不多见。
MusicMan小而精致的外型,Edward Van Halan和Steve Steven的爱琴。
SCHECTER很贵的吉他。
ROBINROCK琴,有很多可爱的外型。
P.R.S手工吉他,他有GIBSON和FENDER的优点。
B.C.Rich很ㄅㄧㄤˋ的外型,重摇滚的外型,有会刺死人的吉他,外型尖。
Jackson/CharvelJackson和Charevl开的,但Jackson已出走至Washburn。
TakamineLine in木吉他。
降维方法与奇异性理论

现代非线性动力学的两个研究主题:降维方法与奇异性理论*曹登庆†陈予恕于海秦朝红哈尔滨工业大学航天学院137信箱,哈尔滨 150001摘要:随着复杂性科学和高技术的发展,高维、多场耦合、强非线性和复杂外部激励正逐渐成为我们面临的动力系统的主要特征。
本文综述近年来在复杂非线性动力系统的降维处理技术和奇异性理论在非线性动力学中的应用方面的研究成果。
在降维方面,主要介绍非线性动力学系统现有降维方法的基本思想、特点与局限性,这些方法包括:基于中心流形理论的降维方法,Lyapunov-Schmidt(L-S)方法,非线性Galerkin方法和Proper Orthogonal Decomposition (POD)方法,并简单介绍了基于正规形理论和快慢流形动力系统的降维方法。
在奇异性理论方面,主要涉及奇异性理论的基本思想、研究现状及其在共振系统、约束系统、对称系统、滞回系统、多参数系统和高余维分岔系统中的应用。
最后提出关于高维非线性动力系统降维以及奇异性理论在非线性动力学中德应用方面的一些新设想,并指出今后研究工作的方向。
关键词:非线性动力学,降维,Galerkin方法,POD,分岔,奇异性理论Two Research Topics in Modern Nonlinear Dynamics: DimensionReduction Methods and Singularity TheoryCAO Dengqing, CHEN Yushu, YU Hai and Qin Zhaohong The School of Astronautics, Harbin Institute of Technology, PO Box 137, Harbin 150001, ChinaAbstract:With the development of complexity science and high technology, high-dimensional, multiple fields coupling, strong nonlinear, and complexity external excitation are becoming primary characteristics of the dynamical systems to be dealt with. This paper is an attempt to categorize recent research achievements in dimension reduction techniques of complexity nonlinear dynamic systems and the applications of singularity theory in nonlinear dynamics. In aspect of dimension reduction, the basic concepts and the features and the limitations of the existing dimension reduction methods of nonlinear dynamic systems are presented. In addition to the typical dimension reduction methods (such as the model reduction method based on center manifold theorem, the Lyapunov-Schmidt method, the Galerkin method and the method of Proper Orthogonal Decomposition), the methods in terms of the normal form and the slow-fast dynamics are briefly presented. In aspect of singularity theory, the basic concepts, current research achievements and its applications in resonant systems, constrained systems, symmetric systems, hysteretic systems; multi-parametric systems, and high co-dimensional bifurcation systems are presented. Finally, considerations on both the dimension reduction of high-dimensional dynamical systems and the applications of singularity theory in nonlinear dynamics are proposed, and the future research directions are indicated.Keywords: Nonlinear dynamics; Dimension reduction; Galerkin method, POD; Bifurcations; Singularity theory1 引 言非线性科学是研究各个不同学科领域中非线性现象共性的一门国际前沿学科,它是在以非线性为特征的各门分支学科的基础上逐步发展起来的综合性学科。
英语论文参考文献(全英文版)

英语论文参考文献(全英文版)英语论文参考文献(全英文版)关键词:英文版,参考文献,英语论文英语论文参考文献(全英文版)简介:参考文献是英文类学术论文、研究报告中不可缺少的一部分,不可随意“从略”,更不可马虎了事或错误百出,很多作者在引用英文参考文献时,会出现引用不当、格式错误等问题,为大家分享正确的英语论文参考文献格式及范例。
一、英文论文参考文献格式要求英文参考文献与中文参考文献的格式英语论文参考文献(全英文版)内容:参考文献是英文类学术论文、研究报告中不可缺少的一部分,不可随意“从略”,更不可马虎了事或错误百出,很多作者在引用英文参考文献时,会出现引用不当、格式错误等问题,为大家分享正确的英语论文参考文献格式及范例。
一、英文论文参考文献格式要求英文参考文献与中文参考文献的格式要求基本相同,但写英文参考文献要注意一点,外文作者姓名的着录格式采用姓在前(全拼,首字母大写),名在后(缩写为首字母),中间用空格;着作类文献题名的实词首字母大写,期刊文献题名的首词首字母大写,期刊名称请用全称,勿用缩写。
具体如下:1、单一作者着作的书籍姓,名字首字母.(年). 书名(斜体). 出版社所在城市:出版社.如:Sheril, R. D.(1956). The terrifying future: Contemplating color television. San Diego:Halstead.2、两位作者以上合着的书籍姓,名字首字母., 姓,名字首字母.(年). 书名(斜体). 出版社所在城市:出版社.如:Smith, J., Peter, Q. (1992).Hairball: An intensive peek behind the surface of an enigma. Hamilton, ON:McMaster University Press.3、文集中的如:Mcdonalds, A.(1993). Practical methods for the apprehension and sustained containment ofsupernatural entities. In G. L. Yeager (Ed.), Paranormal and occult studies:Case studies in application (pp. 42–64). London: OtherWorld Books.4、期刊中的(非连续页码)如:Crackton, P.(1987). The Loonie: God's long-awaited gift to colourful pocket change?Canadian Change, 64(7), 34–37.5、期刊中的(连续页码):姓,名字首字母.(年). 题目. 期刊名(斜体). 第几期,页码.如:Rottweiler, F. T., Beauchemin, J. L. (1987). Detroit and Narnia: Two foes on the brink ofdestruction. Canadian/American Studies Journal, 54, 66–146.6、月刊杂志中的如:Henry, W. A., III.(1990, April 9). Making the grade in today's schools. Time, 135, 28-31.二、英文论文参考文献范例。
Schecter Guitar Research S-1 Custom 电吉他说明书

.022S-1 CustomWiring Diagramshould be soldered.Sleeve (ground)Seymour Duncan ‘59 SH-1NCustom Custom SH-11NeckBridgepush/pull in DOWN position1push/pull in UP positionFortechnicalorwarrantyquestionspleaseemail:************************Diagram copyright Schecter Guitar Research 2011Duncan DesignedDuncan DesignedScale Length: 628mm/24.75”A: Width at Nut- 42mmB: Width at Last Fret- 56mm C: Thickness at 1st Fret- 20mm D: Thickness at 12th Fret- 22mm Radius: 355mm/14”S-1 Custom Neck Specs:Bridge PickupName: Model No: Construction: Magnet: Description:Seymour Duncan Custom Custom SH-11Humbucker Alnico IIOutput:14.4kThe Custom Custom is the SH-5 Duncan Custom humbucker with an Alnico II magnet for warm and smooth highs, more midrange, and a spongier bottom end than the SH-5. It's a good choice for players who need a traditional vintage tone with increased output.Neck PickupName: Model No: Construction: Magnet: Description:Seymour Duncan ‘59SH-1NHumbucker Alnico VOutput:7.43kLate-'50s, vintage-correct, humbucker sound. Warm and crystalline clean tones. Full and bright distorted tones. Smooth sustain. Classic appointments include plain enamel wire, long legged bottom plate. Compared to the SH-55 Seth Lover, the '59 has slightly more scooped mids and is vacuum wax potted for squeal-free performance.Strings6-String Guitar*Tuning: E-A-D-G-B-E Gauge: .046-.036-.026-.017-.013 .010 (EB Regular Slinky #2221)*Changing to different string gauges and/oralternate tunings may require minor neck/bridge adjustments for optimal performance. For Schecter setup tips refer to Schecter Setup Guide.TonePros Model T3BT Locking BridgeLocking Nashville style bridge with many improvements including; large posts, metric thread, intonation adjustment on the pickup side, Phillips head saddle adjustment screws, and pre-notched saddles.TonePros Model T1Z Locking TailpieceStandard style Locking Stop Bar Tailpiece. The T1Z features metric threads.This model is equipped with the world famous TonePros locking hardware! These are simply the best guitar hardware available! A normal bridge with standard mounting studs does not make full contact with the studs. Because of this, the hardware does not efficiently transfer string vibration to the guitar body. With TonePros hardware, you get every ounce of tone that your instrument is capable of producing. The string vibration is efficiently transferred to the wood of the guitar, and as a result, resonance and sustain are markedly improved. Standard tune-o-matic bridges have a considerable amount of “play” on the mounting posts, resulting in the same loss of tone. Unfortunately, the slightest shift of the bridge will also throw off the intonation, essentially ruining the instrument’s setup. With TonePros locking hardware, all of the shortcomings of traditional hardware have been addressed, giving you optimal setup and tone every time you pick up your guitar! And you get the added advantage that the bridge is firmly mounted to the guitar, so when you change your strings, they don't fall off and cause damage to your valuable finish! This completely preserves of your perfect set-up, which means no more readjusting your guitars action or intonation. Once your guitar is set up, it is locked and stays that way. And since your bridge is more stable being locked & frozen in place, your intonation settings are exact due to thereduction and/or removal of movement from loose components. Feel & hear the difference, you be the judge!This model is equipped with a Graph Tech Ivory TUSQ XL nut. The TUSQ XL delivers a rich and balanced tone with big open lows and a noticeable increase in overall sustain followed by a very balanced output from your strings. Laboratory-proven to enhance harmonic content up to 200% and sustain up to 16% and is engineered for maximum vibration transfer. Designed to transfer the right frequencies more efficiently from the string to the guitar body. Compared to standard materials such as bone, micarta or corian, you'll hear more harmonics with every note you play when you use TUSQ XL on your guitar. As compared to TUSQ, you will hear added midrange depth, and is impregnated with Teflonto improve the tuning performance of the guitar.。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
SCHECTER可以算是金属吉他里一个不折不扣的老牌子,他们已经有超过30年的历史了。虽然他们并不仅仅制作只适合重型音乐的吉他,但是无可非议的Байду номын сангаас他们在韩国和中国生产的一系列重型武器在最近几年迅速成为在各个国家乐器市场都很畅销的玩意儿。
于是,SCHECTER又辗转来到了洛杉矶落户,他们在新的日本东家(但是很快的,他们又和新东家“解约”,重新成为一个美国的独立乐器厂牌)的要求下在洛杉矶开办了一个小规模的只接受CUSTOM订制的小作坊,仅仅生产高价位(当时的定价是1500到5000美圆)的订做吉他。但是这个时期洛杉矶的唱片业很繁荣,很多音乐人和艺人都需要高品质的吉他来保证他们的演出。而SCHECTER的吉他也受到了越来越多的摇滚乐队的喜爱,从金属到PUNK乐队,在当时甚至说在MTV中看到乐队使用SCHECTER吉他的频率是一天30次。而这个时候的SCHECTER的CUSTOM SHOP最多一个月也只能生产40把吉他,并且这些吉他卖的又很贵。这远远不是市场所需要的。
所以,在1996年,SCHECTER开始改变了战略,保持CUSTOM SHOP的同时,打算进一步的扩大生产规模。1997年,SCHECTER在日本的东京乐器展会上,进一步的接触了一些亚洲的乐器制造商,最终决定在韩国开辟新的生产线,也就是目前最畅销的“钻石”系列。一年后,也就是1998年,在世界最大的现代乐器展会,美国的夏季NAMM SHOW上,SCHECTER展出了这一性价比极高的量产系列吉他,这在当时产生了很大的轰动。而SCHECTER并不象其他品牌那样满足于生产高端吉他的廉价翻版来赚钱,他们真正的在设计一系列低价位的高品质吉他,并且采取了很多新的设计。这个时候他们开始有远见的,更多的考虑新的摇滚乐手的需要,并且为他们设计吉他。于是,1999年的NAMM SHOW上,SCHECTER展出了一款也是世界上第一款真正适合新金属乐手的7弦吉他,也就是钻石系列的A7,同时,它又是一把人人能够买的起的高品质吉他。这款吉他一上市就受到了包括PAPA ROACH,POWERMAN 5000等大牌新金属乐队的喜爱。
与很多美国吉他品牌一样,SCHECTER也是以老板姓氏注册的品牌。品牌创始人DAVID SCHECTER在1976年就已经在加洲创办了公司。而在那个时代,高档的美国乐器制造重心并没有转移到NYC去,加洲地区的乐器制作代表了美国最高的水准。
在最开始的时候,SCHECTER包括老板在内只有四个员工,他们只是在接受一些客户的乐器维修/改装的订单。比如他们就曾经为“恐怖海峡”的吉他手MARK KNOPFLER以及THE WHO的吉他手PETE TOWNSHEND的TELE与LES PAUL进行过改造,并且后来PETE拿着这些被SCHECTER改装过的吉他出现在MTV中。但是很快的,象当时的SADOWSKY或者其他手工吉他改装商店一样,他们的改装越来越超出了“改装”的范围。他们不仅仅给客户的吉他换装拾音器,琴桥,NUT等一些小的配件,他们甚至开始自己采购一些稀有的高品质木材,制作NECK和BODY去替换乐手拿来的FENDER和GIBSON吉他!!在这个时期,我们不得不记住两个专门进行制作NECK和BODY工作的SCHECTER的新雇员的名字,因为这两位在后来成为了美国吉他制造界的明星和大师,他们就是——TOM ANDERSON 以及 JAMES TYLER!!当时他们俩都是SCHECTER的雇员,并且在SCHECTER工作的时候不仅提高了自己的吉他制作水平,也与很多客户保持了密切的联系,这些在SCHECTER工作的经历与后来他们能够自立门户有着密切相关的联系。可以说,TOM ANDERSON 与 JAMES TYLER两个品牌与SCHECTER的关系就好象后来的SUHR GUITAR与FENDER的关系一样。
在有了TOM ANDERSON 和 JAMES TYLER 这些人的加盟后,SCHECTER逐步开始进入吉他制造业。在1979年,他们就已经发表了很超前的设计——一系列使用稀有木材制作的FENDER STYLE的改进版的吉他和BASS,在当时,这是最时髦和顶级的代表。这个时期的设计无疑是对后来TOM ANDERSON,JAMES TYLER两人分别自立门户后自己制作的型号影响很大,在后来日本的SCHECTER TOKYO生产的手工吉他也延续了这个时期的SCHECTER的设计。
直到今天,SCHECTER拥有月产近万把吉他/BASS的生产能力,包括韩国和中国的钻石系列(其中韩国的钻石系列生产线包揽了这万把中的一半数量),以及在美国生产的高品质CUSTOM SHOP。使用者包括从POWERMAN5000,PAPA ROACH,CRAZY TOWN等大牌金属乐队到THE CURE的吉他手甚至是PRINCE和STEVE VAI。当你在演奏SCHECTER的时候,能够感受到最大的不同就是,他们是真的在用心为摇滚音乐人制作吉他。
到了80年代,他们在达拉斯开办了一个更大的吉他生产线。而他们之前的客户,“恐怖海峡”的MARK就是最早期使用SCHECTER独立生产的吉他的SCHECTER艺术家之一。不过80年代中期到90年代初的乐器市场是一个很大的泡沫,看似庞大其实仅仅是一个表面现象而已。这个时期,很多坚持“品质第一”的制作高品质乐器的公司纷纷走向滑坡从而被收购。比如MICHAEL TOBIAS的TOBIAS卖给了GIBSON,STUART SPECTOR的SPECTOR卖给了KRAMER(KRAMER在90年代初也被GIBSON收购),NED STEINBERGER的STEINBERGER也卖给了GIBSON,甚至连MUSIC MAN也被制作琴弦起家的ERNIE BALL收购,更甚至连这个时期的FENDER也开始用降低品质,寻找国外廉价生产线这些方法来维持生存。而SCHECTER虽然在这个时期设计发表了一系列高品质的经典吉他型号,但是仍然无法避免公司运做方面走下坡路的命运,终于,在1991年,SCHECTER被HISATAKE SHIBUYA(涉谷的久田家??这个只有日文拼音,不知道该怎么翻译,就直接把拼音打上来了),也就是收购了MI的人所收购。他同时还持有ESP吉他的所有权。
�