portal hypertension
急性生理与慢性健康评分(APACHEII)评分细则

Class I 日常活动无症状 Class II 日常活动有症状 Class III 轻微活动就会有明显症状 Class IV 休息时也出现症状
呼吸
• 慢性阻塞性、梗阻性或血管性肺疾病导致活动重
度受限,即不能上楼或不能做家务;
• 明确的慢性低氧
• CO2潴留
• 昏迷程度以E、V、M三者分数加总来评估,正常人的昏迷
指数是满分15分,昏迷程度越重者的昏迷指数越低分。
• 轻度昏迷:13分到14分。
• 中度昏迷:9分到12分。
• 重度昏迷:3分到8分
参数取得时间问题
• 如果APACHE-Ⅱ能在急诊室或刚入抢救室或ICU时进行 评定,意义更大,因为这样可以最大限度地消除治疗对评
– A项:即急性生理学评分(APS),共12项生理参数。
– B项:即年龄评分。 – C项:即慢性健康评分。
APACHE-Ⅱ急性生理学评分标准(1)
APACHE-Ⅱ急性生理学评分标准(2)
注:如无血气分析,则以静脉血碳酸氢根(HCO3)浓度代替动脉血pH; FiO2≥0.5时只记录(A-a)DO2,FiO2<0.5时只记录PaO2; 急性肾功能衰竭时Cr分值加倍。
氧合
• 鼻导管 面罩
氧流量(lpm) 1 FiO2
2
3
4
5
6
8
15
重复吸入 0.70
0.23 0.25
0.27 0.30 0.35 0.40 0.45 0.50
•
注:使用鼻导管时氧流量应 < 6 lpm
•
•
如 FiO2 < 0.5,根据 PaO2 进行评分,此时估测 FiO2 的准确性不会影响评分结果
(整理)常见疾病名称

(整理)常见疾病名称常见疾病名称Internal Medicine 内科Acidosis 酸中毒Adams-Stokes syndrome 亚-斯氏综合症alcoholism, alcoholic intoxication 酒精中毒alkalosis 碱中毒anaphylaxis 过敏症anemia 贫血iron deficiency anemia 缺铁性贫血megaloblastic anemia 巨幼红细胞性贫血aplastic anemia 再生障碍性贫血angiitis 脉管炎angina pectoris 心绞痛arteriosclerosis 动脉硬化apoplexy 中风auricular fibrillation 心房纤颤auriculo-ventricular block 房室传导阻滞bronchial asthma 支气管哮喘bronchitis 支气管炎bronchiectasis 支气管扩张bronchopneumonia 支气管肺炎carcinoma 癌cardiac arrhythmia 心律紊乱cardiac failure 心力衰竭cardiomyopathy 心肌病cirrhosis 肝硬化coronary arteriosclerotic heart disease 冠状动脉硬化性心脏病Crohn disease 克罗恩病Cushing's syndrome 库欣综合症diabetes 糖尿病diffuse intravascular coagulation 弥散性血管凝血dysentery 痢疾enteritis 肠炎gastric ulcer 胃溃疡gastritis 胃炎gout 痛风hepatitis 肝炎Hodgkin's disease 霍奇金病hyperlipemia 高脂血症,血脂过多hyperparathyroidism 甲状旁腺功能亢进hypersplenism 脾功能亢进hypertension 高血压hyperthyroidism 甲状腺功能亢进hypoglycemia 低血糖hypothyroidism 甲状腺功能减退infective endocarditis 感染性心内膜炎influenza 流感leukemia 白血病lobar pneumonia 大叶性肺炎lymphadenitis 淋巴结炎lymphoma 淋巴瘤malaria 疟疾malnutrition 营养不良measles 麻疹myeloma 骨髓瘤myocardial infarction 心肌梗死myocarditis 心肌炎nephritis 肾炎nephritic syndrome 肾综合症obstructive pulmonary emphysema 阻塞性肺气肿pancreatitis胰腺炎peptic ulcer 消化性溃疡peritonitis 腹膜炎pleuritis 胸膜炎pneumonia 肺炎pneumothorax 气胸purpura 紫癜allergic purpura 过敏性紫癜thrombocytolytic purpura 血小板减少性紫癜pyelonephritis 肾盂肾炎renal failure 肾功能衰竭rheumatic fever 风湿病rheumatoid arthritis 类风湿性关节炎scarlet fever 猩红热septicemia 败血症syphilis 梅毒tachycardia 心动过速tumour 肿瘤typhoid 伤寒ulcerative colitis 溃疡性结肠炎upper gastrointestinal hemorrhage 上消化道血Neurology 神经科brain abscess 脑脓肿cerebral embolism 脑栓塞cerebral infarction 脑梗死cerebral thrombosis 脑血栓cerebral hemorrhage 脑出血concussion of brain 脑震荡craniocerebral injury 颅脑损伤epilepsy 癫痫intracranial tumour 颅内肿瘤intracranial hematoma 颅内血肿meningitis 脑膜炎migraine 偏头痛neurasthenia 神经衰弱neurosis 神经官能症paranoid psychosis 偏执性精神病Parkinson's disease 帕金森综合症psychosis 精神病schizophrenia 精神分裂症Surgery 外科abdominal external hernia 腹外疝acute diffuse peritonitis 急性弥漫性腹膜炎acute mastitis 急性乳腺炎acute pancreatitis 急性胰腺炎acute perforation of gastro-duodenal ulcer急性胃十二指肠溃疡穿孔acute pyelonephritis 急性肾盂肾炎anal fissure 肛裂anal fistula 肛瘘anesthesia 麻醉angioma 血管瘤appendicitis 阑尾炎bleeding of gastro-duodenal ulcer 胃十二指肠溃疡出血bone tumour 骨肿瘤breast adenoma 乳房腺瘤burn 烧伤cancer of breast 乳腺癌carbuncle 痈carcinoma of colon 结肠炎carcinoma of esophagus 食管癌carcinoma of gallbladder 胆囊癌carcinoma of rectum 直肠癌carcinoma of stomach 胃癌cholecystitis 胆囊炎cervical spondylosis 颈椎病choledochitis 胆管炎cholelithiasis 胆石症chondroma 软骨瘤dislocation of joint 关节脱位erysipelas 丹毒fracture 骨折furuncle 疖hemorrhoid 痔hemothorax 血胸hypertrophy of prostate 前列腺肥大intestinal obstruction 肠梗阻intestinal tuberculosis 肠结核lipoma 脂肪瘤lithangiuria 尿路结石liver abscess 肝脓肿melanoma 黑色素瘤osseous tuberculosis 骨结核osteoclastoma 骨巨细胞瘤osteoporosis 骨质疏松症osteosarcoma 骨质疏松症osteosarcoma 骨肉瘤Paget's disease 佩吉特病perianorecrtal abscess 肛管直肠周围脓肿phlegmon 蜂窝织炎portal hypertension 门静脉高压prostatitis 前列腺炎protrusion of intervertebral disc 椎间盘突出purulent arthritis 化脓性关节炎pyogenic ostcomyclitis 化脓性骨髓炎pyothorax 脓胸rectal polyp 直肠息肉rheumatoid arthritis 类风湿性关节炎rupture of spleen 脾破裂scapulohumeral periarthritis 肩周炎tenosynovitis 腱鞘炎tetanus 破伤风thromboangiitis 血栓性脉管炎thyroid adenocarcinoma 甲状腺腺癌thyroid adenoma 甲状腺腺瘤trauma 创伤urinary infection 泌尿系感染varicose vein of lower limb 下肢静脉曲张Paediatrics 儿科acute military tuberculosis of the lung 急性粟粒性肺结核acute necrotic enteritis 急性坏死性结肠炎anaphylactic purpura 过敏性紫癜ancylostomiasis 钩虫病ascariasis 蛔虫病asphyxia of the newborn 新生儿窒息atrial septal defect 房间隔缺损birth injury 产伤cephalhematoma 头颅血肿cerebral palsy 脑性瘫痪congenital torticollis 先天性斜颈convulsion 惊厥Down's syndrome 唐氏综合症glomerulonephritis 肾小球肾炎hemophilia 血友病infantile diarrhea 婴儿腹泻intracranial hemorrhage of the newborn 新生儿颅内出血intussusception 肠套叠necrotic enterocolitis of newborn 新生儿坏死性小肠结膜炎neonatal jaundice 新生儿黄疸nutritional iron deficiency anemia 营养性缺铁性贫血nutritional megaloblastic anemia 营养性巨幼细胞性贫血patent ductus arteriosis 动脉导管未闭poliomyelitis 骨髓灰质炎premature infant 早产儿primary tuberculosis 原发性肺结核progressive muscular dystrophy 进行性肌肉营养不良pulmonary stenosis 肺动脉狭窄purulent meningitis 化脓性脑膜炎rickets 佝偻病sepsis of the newborn 新生儿败血症tetanus of the newborn 新生儿破伤风tetralogy of Fallot 法洛四联症thrush 鹅口疮,真菌性口炎varicella 水痘ventricular septal defect 室间隔缺损viral encephalitis 病毒性脑炎viral myocarditis 病毒性心肌炎Gynecology and Obstetrics 妇,产科abortion 流产adenomyosis 子宫内膜异位症amniotic fluid embolism 羊水栓塞Bartholin's cyst 巴氏腺囊肿carcinoma of cervix 子宫颈癌carcinoma of endometrium 子宫内膜癌carcinoma of ovary 卵巢癌cervicitis 宫颈炎chorio-epithelioma 绒毛膜上皮癌corpora luteum cyst 黄体囊肿dystocia 难产eclampsia 子痫edema-proteinuria-hypertension syndrome水肿蛋白尿高血压综合征(妊娠高血压综合征)endometriosis 子宫内膜异位症extrauterine pregnancy 子宫外孕hydatidiform mole 葡萄胎hyperemesis gravidarum 妊娠剧吐infertility 不育症irregular menstruation 月经失调lochia 恶露monilial vaginitis 念珠菌性阴道炎multiple pregnancy 多胎妊娠myoma of uterus 子宫肿瘤oligohydramnios 羊水过少ovarian tumour 卵巢肿瘤pelvic inflammatory disease 盆腔炎placenta previa 前置胎盘placental abruption 胎盘早期剥离pregnancy-hypertension syndrome 妊娠高血压综合症premature birth 早产premature rupture of membrane 胎膜早破postpartum hemorrhage 产后出血puerperal infection 产褥感染rupture of uterus 子宫破裂trichomonas vaginitis 滴虫性阴道炎uteroplacental apoplexy 子宫胎盘卒中vulvitis 外阴炎Ophthalmology and Otorhinolaryngology 五官科amblyopia 弱视amygdalitis, tonsillitis 扁桃体炎astigmatism 散光carcinoma of nasopharynx鼻咽癌carcinoma of larynx 喉癌cataract 白内障tinnitus 耳鸣chalazion 霰粒肿,脸板腺囊肿colour blindness 色盲deflection of nasal septum 鼻中隔偏曲deafness 聋furuncle of nasalvestibule 鼻前庭疖glaucoma 青光眼heterotropia 斜视hyperopia 远视injury of cornea 角膜损伤ceruminal impaction 耵聍嵌塞iritis 虹膜炎keratitis 角膜炎labyrinthitis 迷路炎,内耳炎laryngitis 喉炎mastoiditis 乳突炎myopia 近视nasal sinusitis 鼻窦炎otitis media 中耳炎obstruction of larynx 喉梗阻peritonsillar abscess 扁桃体中脓肿pharyngitis 咽炎rhinitis 鼻炎Dermatoloty 皮科acne 痤疮carcinoma of skin 皮肤癌bed sore 褥疮decubitus ulcer 褥疮性溃疡drug eruption 药皮疹eczema 湿疹herpes simplex 单纯疱疹herpes zoster 带状疱疹lupus erythematosis 红斑狼疮psoriasis 牛皮癣urticaria 荨麻疹wart 疣。
portal认证触发方式

portal认证触发方式英文回答:Portal Authentication Trigger Methods.Portal authentication is a security mechanism that allows network administrators to require users to authenticate themselves before accessing the network. This can be done through a variety of methods, including:HTTP Redirection: This is the most common method of portal authentication. When a user attempts to access a website that is protected by portal authentication, they will be redirected to a login page. Once the user enters their credentials, they will be redirected back to the website they were trying to access.DNS Redirection: This method of portal authentication uses DNS to redirect users to a login page. When a user tries to access a website that is protected by portalauthentication, their DNS request will be redirected to a server that hosts the login page. Once the user enterstheir credentials, they will be redirected to the website they were trying to access.IP Redirection: This method of portal authentication uses IP addresses to redirect users to a login page. When a user tries to access a website that is protected by portal authentication, their IP address will be redirected to a server that hosts the login page. Once the user enterstheir credentials, they will be redirected to the website they were trying to access.Certificate-Based Authentication: This method ofportal authentication uses digital certificates to authenticate users. When a user tries to access a website that is protected by portal authentication, they will be prompted to install a digital certificate. Once the certificate is installed, the user will be able to access the website.Two-Factor Authentication: This method of portalauthentication uses two-factor authentication toauthenticate users. When a user tries to access a website that is protected by portal authentication, they will be prompted to enter their password and a one-time password (OTP). The OTP can be sent to the user's mobile phone or email address.中文回答:Portal认证触发方式。
Portal hypertension

Nonselective shunts
Selective shunts
• the distal splenorenal shunt • the left gastric vena caval shunt • a vein graft between the left gastric
(coronary) vein and the inferior vena cava
established
Clinical manifestation
• Upper gastrointestinal hemorrhage • Ascite • Enlarged spleen 、 hypersplenia • Hepatic coma
Ascite
Laboratory tests
A three-dimensional reconstruction of a CT angiogram
Liver Biopsy
• A useful technique for establishing the cause of cirrhosis and for assessing activity of the liver disease.
• Blood test • Hepatic function: aminotransferase
alkaline phosphatase serum bilirubin level • α-fetoprotein level • CT CTA • Magnetic resonance imaging • ultrasound Doppler ultrasonography
Operative method
• a shunt procedure • a nonshunt operation • hepatic transplantation
portal认证时无法推送portal认证页面问题的解决办法
问题描述:Portal网页认证时认证页面无法弹出;解决方案:1.页面提示“portal server获取不到设备信息或者没有回应req_info报文”时,请参考百度文库“portal server获取不到设备信息或者没有回应req_info报文时的解决办法”;2.浏览器的HTTP报文头不符合规范时会导致portal页面无法弹出,表现为部分终端正常,部分终端弹出空白页面,对于v7版本iMC需要将如下选项改成“否”对于V5版本iMC需要修改配置文件iMC\portal\conf\portal.properties解决,将如下参数修改为“false”即可;3.使用IE8有问题,使用其他浏览器没有问题;IE8浏览器本身有些问题,建议更换浏览器使用;4.确认认证终端是否可以ping通portal server服务器的IP地址;portal认证时,确认认证终端可以ping通服务器地址,否则页面无法弹出;5.确认jserver(plat与eia集中式部署)或者webserver(分布式部署)进程是否正常;6.确认中间网络防火墙有无放开对应的端口,portal页面认证时需要放通终端到iMC服务器的8080或者80端口;7.输入IP地址可以弹出,输入域名无法弹出portal页面,这是由于认证终端不能访问DNS服务器导致,在设备侧增加一条到NDS server的free-rule即可;8.确认设备侧配置的重定向URL是否正确,正确配置为:Portal server xx ip key xxx url附:portal认证典型配置iMC UAM结合WX 3010做无线portal认证并基于不同SSID/操作系统推送不同认证页面的典型配置一、组网需求:Portal网页认证方式简单,无需客户端,且适用于各种终端如PC、手机、pad等。
本案例介绍了无线AC结合iMC进行portal网页的认证方式,并且能够实现根据不同的SSID或者操作系统推送不同的认证页面,从而满足客户多样化的需求。
英文 肝硬化

Consequences of portal hypertension[II] 3. Ascites (腹水)
• • •
Theories of ascites formation Underfilling theory (灌注不足假说) Overflow theory (泛溢假说) Arterial vasodilation theory (动脉扩张假说)
Mechanisms of HRS[II]
Clinical features[I]
Compensated cirrhosis (代偿期)
Many people experience few symptoms at the onset of cirrhosis,symptoms are typically vague and nonspecific. ---Fatigue and loss of energy. ---Loss of appetite and nausea. ---Spider angiomas ---liver function is normal
degradation of matrix proteins
Pathogenesis: chronic, progressed,
diffuse • Hepatocyte injury leading to necrosis. • Chronic inflammation - (hepatitis). • Capillarization (肝窦毛细血管化) of the space of Disse is a key event. • Bridging fibrosis. • Regeneration of remaining hepatocytes proliferate as round nodules surrounded by fibrous septa. • Loss of vascular arrangement results in regenerating hepatocytes ineffective. • Cirrhosis may lead to liver failure, portal hypertension, or development of hepatocellular carcinoma
血浆胶体渗透压变化对机体的影响

血浆胶体渗透压变化对机体的影响【关键词】血浆随着人们对机体内环境的不断探究,更深入地发现在人体这一巨大系统中,每一个生命活动的基本单元都是相当复杂的,其中渗透压是维持内环境稳定的重要因素。
现就近年来对渗透压方面特别是血浆胶体渗透压方面的研究综述如下。
1 渗透压和血浆渗透压的概念1.1 渗透压的概念渗透压(osmotic pressure)指的是溶液中电解质及非电解质类溶质微粒通过半透膜对水的吸引力,其大小是由溶液中溶质颗粒总数决定的,与溶液中溶质种类和颗粒大小无关[1]。
1.2 血浆渗透压(plasma osmotic pressure)的概念血浆渗透压包括血浆晶体渗透压和血浆胶体渗透压。
正常人血浆渗透压约为300mmol/L(280~320mmol/L),相当于770kPa。
血浆晶体渗透压(plasma crystal osmotic pressure)由血浆中晶体物质所形成,如Na+、Cl-、葡萄糖、尿素等,Na+和Cl-占80%;血浆晶体渗透压调节细胞内外水平衡,维持红细胞正常形态。
血浆胶体渗透压(plasma colloid osmotic pressure,COP)由血浆中蛋白质形成,调节血管内外水平衡,维持血容量。
由于白蛋白分子量较小(约为66 000Da),数目较多(白蛋白>球蛋白>纤维蛋白原),因此成为决定血浆COP的主要因素。
白蛋白是所有可溶性蛋白中唯一一种不能穿透毛细血管壁的蛋白。
血浆COP的75%~80%靠白蛋白维持[2]。
约为1.3mmol/L,相当于3.3kPa或25mmHg[1]。
2 血浆COP的生理作用细胞膜是体内的一种半透膜,它将细胞内液和细胞外液隔开,K+、Na+等离子物质不易自由通过。
因此,水在细胞内外的流通,就要受到盐所产生的晶体渗透压的影响。
晶体渗透压对维持细胞内外水分的相对平衡起着重要作用。
临床上常用晶体物质溶液来纠正某些疾病所引起的水盐失调。
Pathogenesis of portal hypertension: an update

l ia I
a n
d
E n d
(
o c a n n a b a n a n d a m lcle
In
.
id s 2 A G
o
-
V S M c
e
ll
re c e
I
p to
r s
E n d o t h e h a I r e le a s e o f N O o p r o s t a m o id s a n d / r e n d o t h e l i a l d e r i v e d h y p e r p o ta n z m g f a c t o r S t m ~ u l a t io n o f r a d i i Io i d r e c e p t o r s s u b s e q L ~e n t o n s e N &o l Y n e rv e s r e la t e d r e le a s e o f c a l c it o n i n g e n e
A
c t iv a t io n
f
e n
o th e f l a I a n
re c
d
re c e
p to
rs
v S M c e li C G R P
e
p
to rs
A N P
C
a r
d ia
c
p
o
d
u c tio n
In
In d
la
r
u c
t io n
o f C
a M p p
r o
d
u c t i o n1 .
P
a tho
TREATMENT OF PORTAL HYPERTENSION AND RESTORATION O

专利名称:TREATMENT OF PORTAL HYPERTENSION AND RESTORATION OF HEPATIC FUNCTIONWITH L-ORNITHINE PHENYLACETATE发明人:RAJIV JALAN,ジャラン,ラジーヴ,KEITHANDERSON,アンダーソン,ケイス申请号:JP2015098205申请日:20150513公开号:JP2015163635A公开日:20150910专利内容由知识产权出版社提供摘要:PROBLEM TO BE SOLVED: To provide a new treatment of portal hypertension and disease resulting from portal hypertension.SOLUTION: A combined treatment includes the administration of at least one of phenylacetate and phenyl butyrate, and L-ornithine to a subject to be treated who has portal hypertension. The phenylacetate or phenyl butyrate is preferably a sodium salt of phenylacetic acid or phenylbutyric acid, or L-ornithine phenylacetate, respectively. In the combined treatment, the agents are combined and administered for the treatment of portal hypertension in acute hepatic failure or chronic hepatic disease such as cirrhosis. The combined treatment decreases the level of proinflammatory cytokines and/or increases the activity of endothelial nitric oxide synthase in the subject to be treated, which makes it possible to improve hepatic function, treat hepatic disease such as cirrhosis, treat variceal bleeding, decrease ascitic fluid, prevent brain damage, and the like.申请人:UCL BUSINESS PLC,ユーシーエル ビジネス ピーエルシー,OCERA THERAPEUTICS INC,オセラ セラピューティクス, インコーポレイテッド地址:イギリス国,ロンドン ダブリュ1ティー 4ティーピー,トッテナム コート ロード 97,ザ ネットワーク ビルディング,アメリカ合衆国 カリフォルニア州 92130 サンディエゴ ハイ ブラフ ドライブ 12651 スイート 230国籍:GB,US代理人:小林 浩,大森 規雄,鈴木 康仁更多信息请下载全文后查看。
出院小结英文5篇

出院小结英文5篇英文出院小结Discharge RecordPatient ID:0168220Name: xxAge:73-y-o Sex: Male/FemaleAdmission Date: xxOperation Date: xxDischarge Date: xxDiagnosis:Acute myocardial infraction……RCA pletely blocked……LCA has a 50% leision in the prox imal and LAD has 30-50% leisionsType 2 diabetes mellitus( 2-DM).Admission: Sudden chest pain for 4 hoursPatient History: 73-year-old man without significant heart problems presented with sudden chest pain for 4 hours. And the pain constantly radiated to the shoulder and back..The electrocardiogram(ECG) of thepatient showed the ST segment of the leads Ⅱ,Ⅲ,A VF raised 0.1-0.2 mv and was admitted for further evaluation and treatmentCardiovascular Riskfactors: 2-DM, FatPhysical Examination: Blood pressure 120/60mmHg, Pulse 60/minute.The lungs were clear. The heart rate was regular, 60 beats per minute. No murmur and pericardial rub was heard. The abdomen was unremarkable. There was no peripheral edema.Laboratory Results:Hb: 133g/L Glucose: 8.6 mmol/L(<6.1)CHOL:4.68mmol/L TG: 0.86 mmol/L LDL-C:3.07 mmol/L HDL:1.11 mmol/LCRP: 8.60mg/L (0-8 mg/L)CK-MB: 299.2 U/L (0-16 U/L) Troponin I: 0.24ng/ml (< 0.04 ng/ml) ECG: a normal rhythm at rate of 60/minute, ST segment raised 0.1-0.2 mv in leads Ⅱ,Ⅲ,A VF.Transthoracic Echocardiogram(TTE):The size of left atrium is 41.2mm and the other chambers were normal.EF:51%CAG: The middle of right coronary artery(RCA) pletely blocked and left coronary artery (LCA) has a 50% leision in the proximal and left anteriordescending(LAD) has some 30-50% leisions. After admission, we implant one stent.(3.5/15 mm) in the RCA..Treatment: After operation, trearment was started for the recovery .It was treated with Aspirin 100mg po qd , Plavix 75mg po qd, Dilatrend6.25mg bid, Imdur 60mg qd, and Clexane(low-molecular-weight heparxx sodium)5000 Usc q12h.. After 16 days of recovery , the patient is well. So we think the patient can discharge hospital.Medication:1.Medicines to improve heart function and their usesAspirin 100mg po 1-0-0Plavix 75mg po 1-0-0 for 9 monthsZocor(statin) 40mg po 0-0-1Micardis 40mg po 1-0-0Spironolactone 20mg po 1-0-0Dilatrend6.25mg po 1-0-12.Medicines to control blood sugar and their usesGlargine(xxulin) 34U ih 1-0-0Glucobay 50mg po 1-1-1Avandia 8mg po 1-0-0ments:1. No smoking and drinking and keep diet2. Strictly controll blood sugar3. Be attention to keep rest and do not do high-intensity exercises4. Eat medicines on time and follow-up visit after one month.Dotor: xx英文出院小结姓名Zhao xx 性别male 年龄51入院诊断Acute pancreatitis简要病史、体格检查和入院辅助检查plaints:”left upper abdominal pain for 1 day.” alcohol triggered. severe, constant pain with nausea & vomiting. more intense when supine, but relieved by staying with the trunk flexed and knees drawn up. no radiation. no abdominal distention. no gallstone history. Physical examination: low-grade fever. normal to elevated BP. distressed, anxious. jaundice(-). moderate abdominal tenderness, with no muscle rigidity. Laboratory data: serumamylase↑,serum lipase↑,urine amylase↑,white blood cells↑, plasma glucose↑. CT plaint scan: no indicative sign. gastroduodenal endoscopy: inflammatory changes, no ulcer observed. etc.治疗经过:fasting. intravenous fluids. nutritional support. nasogastric suction. prophylactic antibiotic. inhibiting pancreatic secretion. others including consultations.出院转归:resolution of abdominal pain出院诊断:Acute pancreatitis出院医嘱:avoidance of alcohol. fluid diet gradually to regular diet. symptoms observation. hospitalization when necessary.英文出院小结DICHARGE SUMMARYDISCHARGE DIAGNOSIS1. Unstable angina.2. Multi-vessel artery diease3. HyperlipidemaREASON FOR ADMISSIONMr.Zhou is a 69-year-old Chinese man who is actually a native of Beshing and in the United States visiting his daughter. he presented to the Heart Hospital emergency room with substernal disfort radiating to the arm. There was mild improvement with nitroglycerin. He had disfort on and off over a two-day period. He was admitted for further management.HOSPITAL COURSEMr.Zhou ruled out for a myocardial infarction by serial enzymes. An adenosine Cardiolite stress was performed. This showed anterior and inferior ischemia. Caridiac catheterization was then performed by Dr. Picone. Coronary arteriography revealed a subtotal proximal LAD followed by total occlusion mid vessel. The distal LAD filled via collaterals from the circumflex and looked small and diffusely diseased. The circumflex was patent. There was a 50 percent stenosis in the obtuse marginal. The right coronary artery had a 75 percent mid vessel stenosis and a 100 percent distal occlusion. There were right to right and left to right collaterals. Left ventriculography revealed an ejection fraction of 55 percent with anterior hypokinesis. Dr. Picone felt that he was not an ideal candidate for bypass surgery and remended medical management.Mr.Zhou was started on a bination of Imdur and metoprolol. Aspirin was continued. On April 26,xx,he was still having low chest disfort. It is difficult to get a plete story as the patient is Chinese speaking only, His daughter interpreted. I spent long periods with the family and describing the procedures and what was done and their implications. They will need to return to see Dr.Picone in two to three weeks.If he has more chest disfort, then he may require surgical intervention.DISCHARGE MEDICATIONSMedications on discharge are Imdur 60 mg p.o.q.d.,metoprolol 25 mg p.o.b.i.d.,Lescol 40 mg p.o.q.d.,aspirin 325 mg p.o.q.d.,and Norvasc2.5 mg p.o.q.d.FOLLOWUPFollow up with Dr.Picone in two to three weeks.出院小结name: 巴图吉亚age: 34sex: manmedical record number: 628848date of admission: 22.Dec.xx.date of discharge:6.Jan.xxattending physician: zhangchengpingpresent history:8 years ago,he felt jaundice with no inducing factors,he first consulted local hospital,blood laboratories tests showed HBsAg is positive,diagnosised as hepatitis B infection.he was given for treatment,and the liver function beed normal.1 year ago,he was given interferon for treatment after injection 2 times,the treatment stoped for higher ALT than before.since last year,he has taken intermittently pain in the upper abdomen after drunking.from the further treatment,he admitted to the liver disease department.prior to admission,he has examined liver function and other laboratories.(the result of test:ALT U/L,AST U/L,total bilirubin umol/L,total protein g/L,albumin g/L).hospital course:after the patient`s hostitalization,he was started on heparolysate 100mg I.V.qd,shuganning(舒肝宁注射液) 30ml I.V.qd, pound glycyrrhizin 160mg I.V.qd,wuzhi jiaonang(五酯胶囊) 22.5mg P.O.t.i.d,and jianpi yishen keli(健脾益肾颗粒) 10g P.O.t.i.d.he responded very well to the therapy.up to now,he changes for the better and no obvious unfortable.Laboratory data:ALT U/L,AST U/L,total bilirubin umol/L,total protein g/L,albumin g/L.White cell count ,hemoglobin ,hematocrit ,platelet count ,PT ,AFP mg/ml.admitting diagnosis:1.chronic viral hepatitis with HBVdischarge diagnosis:1.chronic hepatitis B infection.2.liver cirrhosis(mild). Contition on discharge: Stable.discharge xxtructions:diet:home diet.Activity:as tolerated. Discharge Medications: Continued:1.wuzhi jiaonang(五酯胶囊) 22.5mg P.O.t.i.d.2.jianpi yishen keli(健脾益肾颗粒) 10g P.O.t.i.d.New:1.yinzhihuang keli(茵枝黄颗粒)6g P.O.t.i.d.Medical follow up1.follow up blood routine,prothrombin time(PT),liver function and a-fetoprotein(AFP) in 1 month.2.follow up HBV-marker,HBV-DNA,AFP and liver ultrasonograph every 6 month..signature:出院小结(外科)Medical CertificateName: ----- sex: male age:24 inpatient number:-------Inpatient date: from Aug.16,xx to Sep.20 ,xxDiagnosis:portal hypertension, liver cirrhosisCourse of treatment: First, we had a thorough examination for this patient,including physical examination, blood examination and image examination(All the data mentioned above had been copied by the patient).Then we hadthe diagnosis: portal hypertension, liver cirrhosis. And, in Aug.26,xxwe underwent the operation:splenectomy with esophagus transection and anastomosis, and esophagogastric devascularization. After operationthe patient had got a basic recovery and was discharged on Sep.20 ,xx. xxtructions:1.It is suggested that he should rest for one month at home before resuming his work.2.See doctor and have some necessary examination regularly.3.See doctor anytime when feeling unfortable.Doctor in charge: Professor ----------xx-10-9。
portal 解决方案
Portal 解决方案简介Portal 解决方案是一个为企业提供的全面的门户网站解决方案。
它旨在提供一个集成的平台,使企业能够轻松地创建、管理和发布门户网站,并提供强大的功能和灵活的定制选项。
Portal 解决方案包含了一个易于使用的管理界面,使管理员能够轻松地配置和管理网站内容,并提供了多种设计和布局选项,以满足企业的特定需求。
除了提供传统的门户功能,如新闻公告、文档管理和用户管理,Portal 解决方案还支持集成其他企业应用程序和系统,如CRM、ERP和人力资源管理系统。
主要特点1. 简单易用的管理界面Portal 解决方案提供了一个直观的管理界面,使管理员能够轻松地配置和管理网站内容。
管理员可以使用该界面创建和编辑页面、添加和管理组件、设置访问权限等。
2. 强大的内容管理功能Portal 解决方案提供了一套强大的内容管理功能,使管理员能够轻松地创建、编辑和发布网站内容。
管理员可以使用富文本编辑器创建各种类型的内容,例如新闻公告、博客文章和产品介绍。
此外,管理员还可以使用附件管理功能上传和管理文件。
3. 多种设计和布局选项Portal 解决方案提供了多种设计和布局选项,以满足企业的特定需求。
管理员可以选择预定义的模板或自定义样式,还可以自由拖放组件来创建独特的页面布局。
此外,Portal 解决方案还支持响应式设计,以确保在不同设备上都能提供出色的用户体验。
4. 用户管理和访问控制Portal 解决方案提供完善的用户管理和访问控制功能。
管理员可以创建和管理用户账号,并设置不同的角色和权限。
这样,企业可以根据实际需求,为不同的用户提供个性化的访问权限,确保信息安全和数据保密。
5. 应用程序和系统集成Portal 解决方案支持与其他企业应用程序和系统的集成。
企业可以将各种应用程序和系统集成到门户网站中,与其他系统交换数据和信息。
例如,可以将CRM系统集成到门户网站,以便销售团队能够快速地了解客户信息和销售数据。
portal准入认证参数

portal准入认证参数
"Portal准入认证参数"通常指的是在网络安全领域中用于控制
用户访问网络资源的一系列参数。
这些参数可以包括但不限于以下
几个方面:
1. 用户身份认证参数,这些参数用于验证用户的身份,通常包
括用户名、密码、双因素认证等。
通过这些参数,系统可以确定用
户是否有权访问特定的网络资源。
2. 访问控制参数,这些参数用于定义用户可以访问的资源范围,包括访问时间、访问地点、访问设备等限制条件。
通过这些参数,
系统可以实现对用户访问行为的精细化控制。
3. 安全策略参数,这些参数用于定义网络资源的安全策略,包
括加密要求、防火墙规则、安全连接要求等。
通过这些参数,系统
可以保障网络资源的安全性。
4. 认证协议参数,这些参数用于定义认证过程中所采用的协议,包括RADIUS、LDAP、TACACS+等。
通过这些参数,系统可以与认证
服务器进行通信,实现对用户身份的认证。
综上所述,Portal准入认证参数涉及到用户身份认证、访问控制、安全策略和认证协议等多个方面,这些参数的合理配置能够有效地保障网络资源的安全,并实现对用户访问行为的精细化控制。
Portal服务器搭建

前言Portal认证主要针对用户上网流量(即所有穿过防火墙的流量)进行认证。
其中ARP报文、ICMP 报文和DNS报文可以直接通过不需要进行认证。
配置Portal认证,需要Portal服务器。
Portal的典型组网由三个基本要素组成:认证客户端、接入设备、Portal认证/计费服务器。
1)认证客户端安装于用户终端的客户端系统,为运行HTTP /HTTPS协议的浏览器。
2)接入设备交换机、路由器、防火墙等宽带接入设备的统称,主要有三方面的作用:在认证之前,将用户的所有HTTP请求都重定向到Portal服务器。
在认证过程中,与Portal认证/计费服务器交互,完成身份认证/安全认证/计费的功能。
在认证通过后,允许用户访问被管理员授权的互联网资源。
3)Portal认证/计费服务器接收Portal客户端认证请求的服务器端系统,提供免费门户服务和基于Web认证的界面,与接入设备交互认证客户端的认证信息。
常用拓扑配置步骤1. 开启本地安全aaa服务。
Web页面配置→系统→系统安全2. 配置portal服务器参数。
Web页面配置→用户认证→远程认证→Portal认证→Portal服务器配置完服务器相关参数,点击按钮。
Portal认证的端口默认使用8283端口进行通信,重定向的URL指的是Portal服务器提供的用户认证跳转到的认证页面地址,默认的访问端口为80端口。
3. 若要添加用户认证的规则,点击按钮进行添加。
4. 添加用户角色定义添加用户角色在:web配置页面→用户认证→远程认证→Portal认证→用户角色配置。
用户角色的定义,表示一个具有相同权限用户组的集合,通过用户角色的定义,能够区分不同的用户流量,把其加之在acl策略上就能灵活的控制,区分不同流量的权限。
其中,“用户流量检测”功能是对该用户的流量进行统计,根据配置的时间间隔,如图中则是每三秒钟,统计一次,如果开启了日志记录功能,则每三秒钟统计该用户的流量,并记录在日志中。
腹腔大出血个案护理

腹腔大出血个案护理第一篇:腹腔大出血个案护理一例门静脉高压脾切除术后腹腔大出血患者的护理关键词门静脉高压脾切除腹腔出血门静脉高压(portal hypertension)是一组由门静脉压力持久增高引起的症候群。
绝大多数病人由肝硬化引起,少数病人继发于门静脉主干或肝静脉梗阻以及一些原因不明的因素。
由门静脉高压致脾脏淤血造成的脾脏肿大和脾功能亢进,可行脾切除(laparoscopic splenectomy,LS)手术。
由于脾脏血管丰富、质脆并深藏于左上腹,增加了脾切除出血的风险,脾切除后腹腔内大出血是手术引起的较严重并发症,如不能及时发现,并处理得当,危险性极大,甚至是灾难性的[1]。
我科于2011年10月收治了1例肝硬化腹水并门静脉高压患者,行脾切除术,术后患者并发腹腔大出血,通过努力,最后取得了良好的治疗效果,护理报告如下。
1 病例简介患者,男,54岁,因“反复腹胀不适三年,乏力、纳差”于2011年10月27日入院。
CT示:肝硬化,脾大,食道胃底静脉曲张。
初步诊断“肝硬化、门静脉高压症”,完善相关检查后于10月31日行腹腔镜探查脾切除手术。
术毕入ICU监护治疗。
患者于当日19时40分突然出现腹腔引流进行性增多,口鼻腔出血,术部切口渗血,腹部高度膨隆,血压降至65/45mmHg,尿量减少。
怀疑腹部活动性出血。
急查红细胞1.64×1012/L,血红蛋白51.2g/L,血小板13×109/L,凝血酶原时间(PT)14.4 #sec,活化部分酶原时间(APTT)46.9#sec,纤维蛋白原浓度(FBG C)1.32#g/L,腹部超声检查示:腹部大量积血。
予输注悬浮红细胞7600ml,血浆4075ml血小板500ml凝血酶原复合物75ml,患者出血症状不能缓解。
至04:50患者脾窝引流出血性引流液7280ml,切口渗液550ml,予急行剖腹探查术,术后再次入ICU监护治疗。
经过监测生命体征,呼吸机辅助通气,加强止血、抗感染、抑酸,继续输注红细胞悬液,血浆,冷沉淀等,加强利尿,减轻水肿等措施,于11月05日拔除气管插管,生命体征平稳,次日转回原科室继续治疗。
Portal网络技术协议介绍

BAS:使用本地的 2000 端口监听 Portal Server 发送的 所有报文。使用目的端口 50100 向Portal Server 发送非 响应类报文。
CODE_PP_LOGOUT_REQUEST CODE_PP_LOGOUT_RESPONSE
REQ_LOGOUT
ACK_LOGOUT Radius-AccountingRequest Radius-AccountingResponse
16
Portal认证流程-iNode客户端认证方式
创建客户端Portal连接
portal server server-name ip ip-address [ key key-string | port port-id | url url-string ] *
配置举例: portal server iMC ip 192.168.0.1 key sharekey port 50100 url
19
异常情况分析(一)
PC异常下线(如PC掉电、直接关闭认证网页、iNode客 户端异常退出)
BAS
iNode
Portal Kernel
CODE_PP_HANDSHAKE CODE_PP_HANDSHAKE_RESPONSE
AAA Server
REQ_LOGOUT ACK_LOGOUT
..... Timeout
portal server imc user-sync //使能用户心跳
27
目录
Portal概述 Portal典型组网 Portal协议原理 Portal典型配置 FAQ
Portal认证提示“向设备发送请求超时”问题分析
Portal认证提示“向设备发送请求超时”问题分析一、问题描述:某局点反馈:Portal网页认证输入用户名密码点击,页面提示“向设备发送请求超时”。
二、解决方法正文:检查3A服务器侧端口使用情况,发现1812端口被非认证服务占用。
手动关闭禁用非法服务后,认证正常。
三、分析过程:“向设备发送请求超时”为portal服务器给终端的错误提示。
发生场景portal 服务器将报文发送设备后,设备无回应报文。
这里的设备就是做portal认证的网络设备。
具体有几种可能。
1.Portal服务器与设备通信异常。
通信报文为UDP报文,服务器侧IP为Portal服务器地址,端口为50100;设备侧未指定时,IP默认为网关IP(可在接口下配置“portal nas-ip”指定),端口默认为2000。
可先检查配置和排查网络。
2.设备收到portal服务器报文,并发起radius认证,但是radius服务器无回应。
Radius报文为UDP报文,其中源地址可在对应radius scheme下配置nas-ip指定,默认为设备上最接近radius服务器的接口IP,源端口不定。
目的地址为radius scheme中配置的地址,应该为radius服务器的地址,目的端口为1812(认证)、1813(计费)。
可通过设备收集信息、服务器抓包的方式确认设备发包和服务器收包的情况。
若服务器未收到报文,排查设备配置和网络。
若服务器收到报文不回应,排查radius服务器配置和状态。
服务器侧通常的原因有(1)未添加接入设备。
查看“用户>接入策略管理>接入设备管理>接入设备配置”。
其中必须有以radius报文源地址IP添加的设备。
(2)Radius服务器,认证端口1812被占用或异常。
正常情况为此时可以通过如下命令确认:netstat –aon | findstr 1812,(linux系统netstat –apn |grep 1812)现场只需要将占用UDP 1812的进程杀掉即可。
Portal Hypertension

门静脉高压症-病理生理(17)
portal hypertensive gastropathy (门脉高压性胃病)
★
hepatic or portosystemic encephylopathy (肝性脑病)
★
门静脉高压症-临床表现(1)
Clinical presentation
临床表现
熟悉内容
◆
(胃肠脾胰毛细血管—肝窦)
◆
No valves in portal vein system and the blood flow can be reversed
门静脉高压症-解剖(3)
◆
Four ramus communicans between portal and systemic circulations
门静脉高压症-病理生理(8)
门静脉高压症-病理生理(9)
门静脉高压症-病理生理(10)
门静脉高压症-病理生理(11)
门静脉高压症-病理生理(12)
门静脉高压症-病理生理(13)
门静脉高压症-病理生理(14)
门脉高压伴有侧支
门静脉高压症-病理生理(15)
3. ascites :
The most important cause for ascites
门静脉高压症-病理生理(6)
门静脉高压症-病理生理(7)
2. ramus communicans dilatation:
最重要
esophageal and gastric veins: varices
但出血与门脉 压力不成比例!
rupture and gastrointestinal hemorrhage inferior rectal-anal veins: hemorrhoid and bleeding anterior abdominal wall veins: paraumbilical varices (caput medusae) numerous retroperitoneal veins: dilatation and congestion
【国家自然科学基金】_portal hypertension_期刊发文热词逐年推荐_20140801
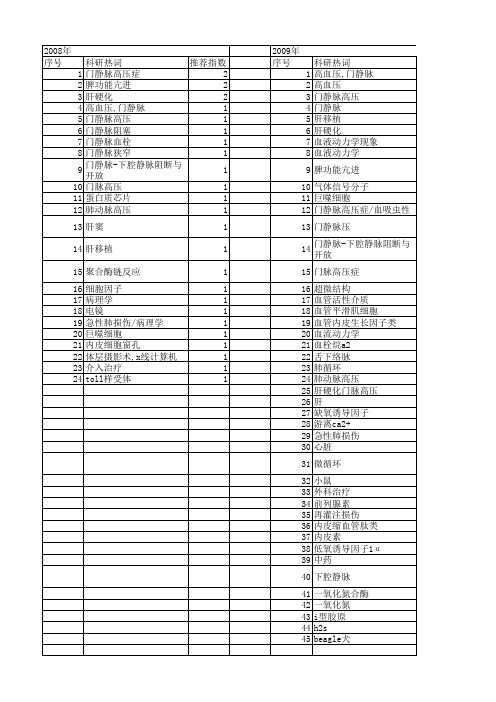
2014年 科研热词 推荐指数 序号 高血压,门静脉 5 1 门静脉高压症 5 2 肝硬化 5 3 portal hypertension 4 4 门静脉 2 5 肝星状细胞 2 6 声触诊组织量化 2 7 一氧化氮 2 8 高血压 1 9 高动力循环 1 10 雷帕霉素 1 11 门静脉高压 1 12 门腔分流术,外科 1 13 门体分流术,经颈静脉肝内 1 14 门-体分流术,经颈静脉肝内 1 15 超声检查,多普勒,彩色 1 16 超声检查 1 17 贲门周围血管离断术 1 18 血管病变 1 19 螺杆菌,幽门 1 20 药物耐受性 1 21 脾切除 1 22 脾 1 23 肠腔分流术 1 24 肠系膜动脉 1 25 肝脏储备功能 1 26 肝肿瘤 1 27 肝纤维化 1 28 肌源性反应 1 硫化氢 1 白细胞介素-1受体相关激酶-4 1 活血化瘀剂 1 活性氧 1 治疗学 1 放射学,介入性 1 抗坏血酸 1 慢性肝病 1 微循环 1 去唾液酸糖蛋白受体 1 单光子发射型计算机断层显像 1 再出血 1 内毒素血症 1 中草药 1 丙二醛 1 β -arrestin-2 1 variceal pressure 1 stasis-resolving 1 splenic artery embolization(sae) 1 schistosomiasis 1 rhoa/rock通路 1 rho associated coiled-coil forming 1 protein kinase propranolol 1
科研热词 肝硬化 门静脉高压 硫化氢 高血压 门静脉高压症 门静脉压力 门静脉 门脉高压症 血吸虫病 脾肿大 脾切除术 胱硫醚-γ -裂解酶 胰腺疾病 胃肠活动 肺 肠神经系统 肝窦微循环 硫氢化钠 炔丙基甘氨酸 小体积肝移植 孤立性胃静脉曲张 内皮素-1 体外培育牛黄复方制剂
门静脉高压症(英文)
Portal Hypertension
Questions
• Where is the portal vein?
• What is portal hypertension?
• How do we handle with the patient of portal hypertension?
Etiology
1. Intrahepatic occlusion
Presinusoidal:
Schistosomiasis
Sinusoidal, post-sinusoidal: liver cirrhosis (alcoholic hepatitis, viral hepatitis, Wilson disease)
Backward theory vs. Forward theory
• High resistance Ohm Law ∆ P = Q×R
• High volume
It is currently believed that the principle and initial abnormality is increased vascular resistance to portal flow and that portal hypertension is then maintained by increased blood flow into the portal circulation.
Recently a talent artist died of the severe complication of liver cirrhosis combined with portal hypertension.源自A typical case
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Severe esophageal varices
3.Ascites About 1/3 of patients with ascites。 4.水母头(caput medusae)症:Portal blood flow through the umbilical vein to periumbilical abdominal wall vein.
The clinical manifestations
1.All of the patients have different degrees of Splenomegaly, and were associated with hypersplenism.
2.Hematemesis and melena
Surgical anatomy of portal vein system
The liver is the only body to accept the dual blood supply (portal vein and hepatic artery) organs, normal liver blood flow was 1500ml/min, equivalent to the cardiac output of 20% ~ 25%
Portal Hypertension
Basic Definition
As a result of the portal vein system pressure increased, the disease characterized with splenomegaly and
hypersplenism , esophageal gastric varices and hematemesis, ascites and other symptoms . Portal venous pressure normal 13-24 cm H2O, average 18 cm H2O.
Surgical anatomy of portal vein system
Anastomotic branch: 1.Gastric fundus and The lower esophagus 2.The lower section of rectum and The anal canal; 3.Anterior abdominal wall vascular plexus; 4.Retroperitoneal vascular plexus (Retizus) 。
Normal pressure is 1.27 ~ 2.35kPa, average 1.76kPa. If the pressure is higher than this limit, defined as the portal hypertension
Portal vein, vena cava of collateral circulation-A
Congestion of spleen
Because of the long-term spleen sinus congestion, hyperplasia of fibrous tissue in the spleen and regeneration of splenic myeloid cells Blood cell damage increased White blood cell, platelet reduction
Etiology
1.Increased resistance to flow
Pod portal blood flow
Prehepatic
Posthepatic
Congential atresia or stenosis
Thrombosis of portal vein or splenic vein
Pathological changes of portal hypertension
Splenomegaly, hypersplenism
Communicating branch expansion
Ascites
Congestive
Portal vein Pressure exceed high Hepatic dysfunction
Portal vein, vena cava of collateral circulation-B
the Summary of Anatomy
1、The main portal vein is made of superior mesenteric vein and splenic venous confluence. 2、The portal venous system located between the two capillary network, stomach, intestine, spleen end, pancreatic capillary network, the other side is the hepatic lobule of liver sinus. 3、Portal venous blood supply of liver in 75%, hepatic artery in 25%, but the oxygen supply two almost equal. (1100ml/min)
Prehepatic
Budd-Chiari syndrome
Constrictive pericarditis
Increased portal blood flow
Vein Artery
Arterial-portal venous fistula
Increased splenic flow:(1)Banti’s syndrome; (2)Splenomegaly(eg,tropic al splenomegaly,myeloid metaplasia)
5.Other symptoms
Liver palm Spider nevus
gynaecomasti
Jaundice
Diagnosis
1.Medical history: Hepatitis,Alcoholic, schistosomiasis 2.Three main clinical manifestations: Splenomegaly, hypersplenism; Hematemesis and melena; Ascites
The characteristics of portal vein: 1.The portal vein and its tributaries basically no Venous flap. 2.Both ends of the portal venous system were capillary network.
Summary
Increased resistance to flow
Portal pressure >10mm Hg
Portal hypertension Increased portal blood flow
Pathophysiology
Increased portal resistance A. mainly by the liver structure changes caused by mechanical factors (70%). 1.Hepatic sinusoid vascular compliance decreased; 2.collagen in Disse calm the liver sinusoidal narrow gap. 3.regenerative nodules oppression sinusoids and hepatic venous system leads to hepatic sinus and its outflow tract obstruction B.Another 30% factors can be controlled, such as Hepatic sinus endothelial increase and N0 caused a decrease in vascular resistance stellate cell contraction, 5HT contraction in portal vascular hormone receptor leads to increased and can stimulate the reactivity enhancement of α adrenergic.
Extrinsic compression(eg,tumors)
Hepatic
Cirrhosis
Acute alcoholic liver disease hepatic
Congenital hepatic fibrosis
Idiopathic portal hypertension
Schistosomiasis
About half of the patients have this symptom, bleeding a lot and critical characteristics to it, which is about 50% of the patients in the first bleeding can be directly due to shock or liver function damage induced by the death of acute liver failure
3.Auxiliary examination: blood, liver, esophageal barium swallow, B ultrasound