中文样本法国艾力锋
ABClonal Rat IL-1 beta ELISA Kit RK00009说明书
Rat IL-1beta ELISA KitCatalog NO.:RK00009version:2.0This package insert must be read in its entirety beforeusing this productIntroductionThe kit is a sandwich enzyme immunoassay for in vitro quantitative measurement of IL-1beta in rat serum,plasma,cell culture supernatants.Principle of the AssayThis assay employs the quantitative sandwich enzyme immunoassay technique.An antibody specific for rat IL-1beta has been pre-coated onto a microplate.Standards and samples are pipetted into the wells and any IL-1beta present is bound by the immobilized antibody.After washing away any unbound substances, and then a detection antibody specific for IL-1beta is added to the wells and binds to the combination of capture antibody IL-1beta in sample.Following a wash to remove any unbound combination,and enzyme conjugate is added to the wells. Following incubation and wash steps,a substrate solution is added to the wells and color develops in proportion to the amount of IL-1beta bound in the initial step.The color development is stopped and the absorbance is measured.Material Provided&Storage ConditionsUnopened kits can be stored at2-8°C for1year,and opened products must be used within1month.Part Size Cat.No.Storage ofopened/reconstituted materialAntibody Coated Plate 8×12RM00064Put the unused slats backin the aluminum foil bagwith the desiccant andreseal them.They can bestored at2-8°C for1month.Standard Lyophilized 2vials RM00061It is not recommended touse again afterredissolving.Concentrated BiotinConjugate Antibody(100×)1×120ul RM00062Store at2-8°c for1month*Streptavidin-HRP Concentrated(100×)1×120ul RM00063Store at 2-8°c for 1month *Standard/SampleDiluent (R1)1×20mL RM00023Store at 2-8°c for 1month *Biotin-Conjugate AntibodyDiluent (R2)1×12mL RM00024Streptavidin-HRP Diluent(R3)1×12mL RM00025WashBuffer(20x)1×30mL RM00026TMB Substrate1×12mL RM00027Stop Solution1×6mL RM00028Plate Sealers4Strips Specification 1Other Supplies Required1.Microplate reader capable of measuring absorbance at450nm,with the correction wavelength set at630nm or570 nm.2.Pipettes and pipette tips.3.Deionized or distilled water.4.Squirt bottle,manifold dispenser,or automated microplatewasher.5.Incubator.6.Test tubes for dilution of standards and samples.Precautions1.Any variation in diluent,operator,pipetting technique,washing technique,incubation time or temperature,and kitage can cause variation in binding.2.Variations in sample collection,processing,and storagemay cause sample value differences.3.Reagents may be harmful,if ingested,rinse it with anexcess amount of tap water.4.Stop Solution contains strong acid.Wear eye,hand,andface protection.5.Please perform simple centrifugation to collect the liquidbefore use.6.Do not mix or substitute reagents with those from other lotsor other sources.7.Adequate mixing is particularly important for good result.Use a mini-vortexer at the lowest frequency.8.Mix the sample and all components in the kits adequately,and use clean plastic container to prepare all diluents.9.Both the sample and standard should be assayed in duplicate,and reagents should be added in sequence in accordance with the requirement of the specification.10.Reuse of dissolved standard is not recommended.11.The kit should not be used beyond the expiration date onthe kit label.12.The kit should be away from light when it is stored orincubated.13.To reduce the likelihood of blood-borne transmission ofinfectious agents,handle all serum,plasma,and other biological fluids in accordance with NCCLS regulations.14.To avoid cross contamination,please use disposablepipette tips.15.Please prepare all the kit components according to theSpecification.If the kits will be used several times, please seal the rest strips and preserve with desiccants.Do use up within2months.16.This assay is designed to eliminate interference by otherfactors present in biological samples.17.Until all factors have been tested in this assay,thepossibility of interference cannot be excluded.18.The48T kit is also suitable for the specification.Sample Collection&StorageThe sample collection and storage conditions listed below are intended as general guidelines.Sample stability has not been evaluated.Samples containing the correlated IgG as in this kit may interfere with this assay.Cell Culture Supernatant:Remove particulates by centrifugation. Assay immediately or aliquot and store samples at≤-20°C. Avoid repeated freeze-thaw cycles.Serum:Use a serum separator tube(SST)and allow samples to clot for30minutes at room temperature before centrifugation for15 minutes at1000x g.Remove serum and assay immediately or aliquot and store samples at≤-20°C.Avoid repeated freeze-thaw cycles.Plasma:Collect plasma using EDTA or Heparin as an anticoagulant. Centrifuge for15minutes at1000×g within30minutes of collection.Assay immediately or aliquot and store samples at ≤-20℃.Avoid repeated freeze-thaw cycles.(Note:Citrateplasma has not been validated for use in this assay.)Note:It is suggested that all samples in one experiment be collected at the same time of the day.Avoid hemolytic and hyperlipidemia sample for serum and plasma.Reagent PreparationBring all reagents to room temperature before use.If crystals have formed in the concentrate,Bring the reagent to room temperature and mix gently until the crystals have completely dissolved.Standard-Reconstitute the Standard Lyophilized with 1.0mL Standard/Sample Diluent(R1).This reconstitution produces a stock solution of8000pg/mL.Mix the standard to ensure complete reconstitution and allow the standard to sit for a minimum of 15minutes with gentle agitation prior to making dilutions. Use the8000pg/mL standard stock to produce a dilution series (below)with Standard/Sample Diluent(R1).Mix each tube thoroughly and change pipette tips between each transfer(recommended concentration for standard curve:4000,2000,1000,500,250,125,62.5,0pg/mL).Use diluted standards within 60minutes of preparation.Working Biotin Conjugate Antibody -Dilute 1:100of Concentrated Biotin Conjugate Antibody (100x)with Biotin-Conjugate Antibody Diluent (R2)before use,for example:Add 20μL of Concentrated Biotin Conjugate Antibody (100x)to 1980μL Biotin-Conjugate Antibody Diluent (R2)to prepare 2000μL Working Biotin Conjugate Antibody Buffer.Working Streptavidin-HRP -Dilute 1:100of Concentrated Streptavidin-HRP (100x)with Streptavidin-HRP Diluent (R3)before use,for example:Add 20μL of Concentrated Streptavidin-HRP (100x)to 1980μL Streptavidin-HRP Diluent (R3)Std 250μL 250μL 250μL 250μL 250μL 250μL 250μL 250μL 1000pg/mL R11000μL 8000pg/mL 250μL 4000pg/mL 250μL 250pg/mL 250μL 500pg/mL 250μL 125pg/mL 250μL 2000pg/mL 250μL 62.5pg/mL 250μL 0pg/mLto prepare2000μL Working Streptavidin-HRP Buffer.Wash Buffer-If crystals have formed in the concentrate,warm to room temperature and mix gently until the crystals have completely dissolved.Dilute1:20with double distilled or deionized water before use,for example:Add20mL of Wash Buffer Concentrate to380mL of deionized or distilled water to prepare 400mL of Wash Buffer.Assay ProcedureBring all reagents and samples to room temperature before use. It is recommended that all standards,controls,and samples be assayed in duplicate.1.Prepare all reagents,working standards,and samples asdirected in the previous sections.2.Remove excess microplate strips from the plate frame,return them to the foil pouch containing the desiccant pack, and reseal properly.3.Add wash buffer350μL/well,aspirate each well afterholding40seconds,repeating the process two times fora total of three washes.4.Add100μL Standard/sample Diluent(R1)in a blank well.5.Add100μL different concentration of standard or samplein other wells,Cover with the adhesive strip provided.Incubate for2hours at37℃.record the plate layout ofstandards and sample assay.6.Prepare the Concentrated Biotin Conjugate Antibody(100x)Working Solution15minutes early before use.7.Repeat the aspiration/wash as in step 3.8.Add100μL Working Biotin Conjugate Antibody in each well,cover with new adhesive Sealer provided.Incubate for1hour at37℃.9.Prepare the Streptavidin-HRP Concentrated(100x)WorkingSolution15minutes early before use.10.Repeat the aspiration/wash as in step 3.11.Add100μL Working Streptavidin-HRP in each well,coverwith new adhesive Sealer provided.Incubate for0.5hourat37℃.12.Repeat the aspiration/wash as in step 3.13.During the incubation,turn on the microplate reader towarm up for30minutes before measuring.14.Add100μL TMB Substrate to each well.Incubate for15-20minutes at37℃.Protect from light.15.Add50μL Stop Solution,determine the optical density ofeach well within5minutes,using a Microplate reader setto450nm.If wavelength correction is available,set to570nm or630nm.If wavelength correction is not available, subtract readings at570nm or630nm from the readingsat450nm.This subtraction will correct for opticalimperfections in the plate.Readings made directly at450nm without correction may cause higher value and lessaccurate result.Assay Procedure SummaryPrepare the standard and reagentsWash3times↓Add100ul of standards or test samples to each well Incubate for2hours at37℃,then wash3times↓Add100ul Working Biotin Conjugate AntibodyIncubate for1hour at37℃,then wash3times↓Add100ul Working Streptavidin-HRPIncubate for0.5hour at37℃,then wash3times↓Add100ul Substrate SolutionIncubate for15-20min at37℃under dark condition↓Add50ul Stop Solution↓Detect the optical density within5minutes under450nm.Correction Wavelength set at570nm or630nmCalculation of Results1.Average the duplicate readings for each standard,controland sample,and subtract the average zero standard optical density(O.D.).2.Create a standard curve by reducing the data using computersoftware capable of generating a four-parameter logistic (4-PL)curve-fit.As an alternative,construct a standard curve by plotting the mean absorbance for each standard on the Y-axis against the concentration on the X-axis and draw a best fit curve through the points on a log/log graph.The data may be linearized by plotting the log of the IL-1 beta concentrations versus the log of the O.D.on a linear scale,and the best fit line can be determined by regression analysis.3.If samples have been diluted,the concentration read fromthe standard curve must be multiplied by the dilution factor.Typical DataThe standard curves are provided for demonstration only.A standard curve should be generated for each set of IL-1beta assayed.Detection Range62.5-4000pg/mLSensitivityThe minimum detectable dose(MDD)of IL-1beta typically less than13.22pg/mL.The MDD was determined by adding two standard deviations to the mean optical density value of twenty zero standard replicates and calculating the corresponding concentration.SpecificityThis assay recognizes both recombinant and natural rat IL-1beta. The factors listed below were prepared at50ng/ml and assayed for cross-reactivity.No significant cross-reactivity was observed with the following:Recombinant rat:Recombinant human:IL-10IL-1IFN-γIL-2IL-1αIL-6IL-2IL-4IL-6IL-8TNF-αNote:Limited by current skills and knowledge,it is impossible for us to complete the cross-reactivity detection between IL-1beta and all the analogues,therefore,cross reaction may still exist.PrecisionIntra-plate Precision3samples with low,middle and high level IL-1beta were tested 20times on one plate,respectively.Intra-Assay:CV<10%Inter-plate Precision3samples with low,middle and high level IL-1beta were tested on3different plates,20replicates in each plate.Inter-Assay:CV<15%Intra-Assay Precision Inter-Assay Precision Sample123123 n202020202020 Mean(pg/mL)116522683535116022593542 Standard deviation47.879.4137.975.4162.6219 CV(%) 4.1 3.5 3.9 6.57.2 6.2RecoveryMatrices listed below were spiked with certain level of IL-1beta and the recovery rates were calculated by comparing the measured value to the expected amount of IL-1beta in samples.Sample Average Recovery(%)Range(%)Cell Culture Media(n=5)10495-113 Serum(n=5)9990-108LinearityThe linearity of the kit was assayed by testing samples spiked with appropriate concentration of IL-1beta and their serial dilutions.The results were demonstrated by the percentage of calculated concentration to the expected.Cell Culture Media(n=5)Serum(n=5) //Average of Expected(%)103951:2Range(%)98-10887-102Average of Expected(%)981021:4Range(%)84-11189-114 Average of Expected(%)961001:8Range(%)86-10692-108Average of Expected(%)981061:16Range(%)91-10596-115Trouble ShootingProblem Possible Cause SolutionHigh Background Insufficient washingSufficiently wash plates asrequired.Ensure appropriateduration and number of washes.Ensure appropriate volume of washbuffer in each well.Incorrect incubationprocedureCheck whether the duration andtemperature of incubation are set upas required.Cross-contamination ofsamples and reagentsBe careful of the operations thatcould cause cross-contamination.Use fresh reagents and repeat thetests.No signal or weak signal Incorrect use ofreagentsCheck the concentration anddilution ratio of reagents.Makesure to use reagents in properorder.Incorrect use ofmicroplate readerWarm the reader up before use.Makesure to set up appropriate mainwavelength and correctionwavelength.Insufficient colourreaction timeOptimum duration of colour reactionshould be limited to15-25minutes.Read too late after stopping the colour reaction Read the plate in5minutes after stopping the reaction.Matrix effect ofsamplesUse positive control.Too much signal Contamination of TMBsubstrateCheck if TMB substrate solutionturns e new TMB substratesolution.Plate sealers reusedUse a fresh new sealer in each stepof experiments.Protein concentrationin sample is too highDo pre-test and dilute samples inoptimum dilution ratio.Poor Duplicates Uneven addition ofsamplesCheck the pipette.Periodicallycalibrate the pipette.Impurities andprecipitates insamplesCentrifuge samples before use.Inadequate mixing ofreagentsMix all samples and reagents wellbefore loading.*For research purposes only.Not for therapeutic or diagnostic purposes.。
国际神经精神访谈MINI 6.0(调查问卷)

e-mail: dsheehan@
tel: +33 (0) 1 53 80 49 41; fax : +33 (0) 1 45 65 88 54
e-mail: even-sainteanne@orange.fr
M.I.N.I. 6.0.0 (October 10, 2010) (10/10/10)
过去的 2 周 既往发作情况
a 您的食欲几乎每天是减少还是增加呢? 您的体重是否会在不刻意努力的情况下减 否
是
否
是
少或增加(例如,在一个月里,对一个体重为 160 磅/ 70 公斤的人而言,体重增减
大约 5%或 8 磅,或 3.5 公斤)呢?
如果对任何一个问题的回答为“是 ”,则标记为“ 是”。
b 您是否几乎每晚都有睡眠问题(难以入睡、半夜醒来、早上醒得过早或睡眠过 多)?
F50.0 F41.1
F60.2
M.I.N.I. 6.0.0 (October 10, 2010) (10/10/10)
2
M.I.N.I - China/Mandarin - Version of 16 Jan 12 - Mapi Institute.
ID6273 / MINI6.0_AU11.0_cmn-CN.doc
评分指导:
必须对所有的问题评分。 通过圈选每个问题右边的“是”或“否”来进行评分。 访谈员的临床判断应当被用来标记患者 的回答。 访谈员在提出问题和对答案进行评分时,需要特别注意文化信仰的多样化。 访谈员应当在必要时要求获 得一些例子,以确保对回答做准确的标记。 应当鼓励患者对任何不完全清楚的问题提出澄清的要求。 临床医生必须确保患者会考虑到问题的各个方面(例如,时间范围、频率、严重程度和/或其它选择)。 在 M.I.N.I.中,最有可能由于器质性原因或者因酒精或药物的使用而引发的症状不应当被标记为肯定的回答。
实验室质量评价EQA

Quality specifications in EQA schemes:from theory to practiceLaura Sciacovelli *,Lorena Zardo,Sandra Secchiero,Mario PlebaniCentro di Ricerca Biomedica,Via Ospedale 18,31033Castelfranco Veneto (TV),ItalyReceived 13February 2004;accepted 22February 2004AbstractBackground :External quality assessment (EQA)is a tool for quality management in clinical laboratories and its main objectives are assessment of participants and methods performance,training and advice.This paper describes the quality specifications used in EQA schemes of the Centre of Biomedical Research (CRB),in order to design schemes that can assess laboratory reliability performances,meet the changing needs and quality recommendations.Methods :Quality specifications for control materials,statistical procedures and goals to assess laboratory performance have been applied and introduced in EQA schemes managed by CRB.Results :The application of well-defined quality specifications has demonstrated effective.In particular,we report results on alkaline phosphatase and cholesterol obtained using commercial control materials and human serum controls,in two different EQA surveys;the inter-laboratory variability (CVinter%)for troponin I analysed with a diagnostic system and assigned values of CK-MB mass obtained using four different diagnostic systems;the percentage of acceptable performances obtained by means of the application of goals based on clinical criteria,biological variation,state-of-the-art and used for EQA schemes,and referring to some analytes with significant clinical values such as cholesterol,glucose,glycated hemoglobin and sodium.Conclusions :The design of reliable EQA schemes based on evidence-based quality specifications is a pre-requisite for supporting the quality improvement of clinical laboratories.D 2004Elsevier B.V .All rights reserved.Keywords:External quality assessment;Analytical performance laboratory;Analytical total error;EQA control material;EQA statistical procedure1.IntroductionMedical laboratories must provide high quality service to clinicians by producing accurate,precise,relevant and comprehensive data that can be applied to the medical management of patients.They must,therefore,produce analytically reliable results,and the information required for the correct interpretation anduse of results.The mechanism for achieving these objectives is encompassed in total quality manage-ment [1–5].The analytical process and its control are becoming increasingly reliable thanks to the improvements made to instruments and methods,and the application of internal quality control (IQC)and external quality assessment (EQA)procedures.However,the large variety of laboratory methods available can hamper measurements and the comparability of results,thus potentially compromising patient management.Medical laboratories have a long tradition of EQA procedures but,continuous progress made in labora-0009-8981/$-see front matter D 2004Elsevier B.V .All rights reserved.doi:10.1016/cn.2004.02.037*Corresponding author.Tel.:+39-423-732823;fax:+39-423-732826.E-mail address:laurasciacovelli@libero.it (L.Sciacovelli)/locate/clinchimClinica Chimica Acta 346(2004)87–97tory medicine,imposes a constant development and change in the EQA design.As a logical evolution in quality management,EQA organizers must arrange their schemes according to quality specifications in order to constantly encourage improvement in labo-ratory to higher and higher standards,thus striving to meet laboratories’needs.In the modern medical laboratory,the main objec-tives in using the EQA programs are:to assess participants’performance and method performance, and provide training and advice.The EQA,which should be considered a tool for quality management within the ambit of total quality management,must help laboratory staff to:identify any problems in the laboratory,provide insight into the quality of routine laboratory work,promote continuous improvement in performance,inter-laboratory comparability of results and harmonization of methods,and train staff to use EQA information effectively[6,7].The numerous publications that have emerged on quality management in recent years stress the impor-tance of the EQA schemes and use of the data from EQA surveys for assessing participants’performance. The design of each scheme differs according to goals chosen,and schemes for the same constituent can, under the management of different organizers,pro-duce varying information on laboratory performance. Such discrepancies are mainly due to the use of different quality specifications.These variations de-pend,in particular,on difference in methods used for the selection of control materials,statistical proce-dures(identification of assigned value and outliers), and the assessment of laboratory performance.1.1.Control materialsThe EQA scheme organizer is responsible for the appropriate selection of control materials.In compli-ance with quality standards and scientific recommen-dations,the materials should simulate fresh human serum as closely as possible in order to avoid inter-ference from the matrix or other components[8–14]. The use of human serum poses several difficulties (identification and retrieval of human donors,ethical considerations and consent problems,risk of agents causing infections)and,for practical reasons,com-mercial control materials(animal sera)are commonly employed.In this sphere,it is essential for the EQA organizer to be able to demonstrate the quality of materials.In particular,the control materials should be:commutable in order to simulate the measurement process in patient serum as closely as possible(ap-propriate matrix);sufficiently homogenous(if non-homogenous material is used,it should be the best available on the market,and the uncertainty of assigned values must be taken into account);suffi-ciently stable to ensure that they will not undergo any significant change during the entire survey period;and in compliance with all relevant safety standards. 1.2.Statistical procedureAn appropriate statistical procedure is a crucial tool for allowing participating laboratories to compare their results with those of other laboratories,obtained on the same sample.Thus,if a patient’s sample is analysed in different laboratories,any variation in results should be such as not to alter the clinical interpretation.Careful considerations should be made concerning the number of results(to allow a statistical significance),identification of method,data classifica-tion(all results independently from method,method/ diagnostic system related results),and the procedure used to identify outliers and to estimate the assigned value.The statistical analysis of results must provide reliable estimates of the assigned value(A V)and inter-laboratory variability,data needed for the imple-mentation of proper measures to improve both inter-laboratory and inter-method agreement.EQA infor-mation can differ depending on the criteria used for data processing,and different techniques can be applied to achieve different objectives and provide different information.The EQA organizer must decide whether to use a parametric or a non-parametric approach,above all analysing the distribution of results and the number of results.The non-parametric method,which is known to be robust,is suggested when the distribution of results is non-gaussian,the number of results is poor, and when a new scheme has been set-up.Therefore, this approach is usually preferred to a parametric evaluation for robustness of median and spread. Usually,in the EQA scheme,the A V is a consensus value,which is the average of results reported by participants in EQA,and is considered an estimationL.Sciacovelli et al./Clinica Chimica Acta346(2004)87–97 88of the‘‘true value’’,which can be determined only by using definitive methods.When the consensus value is calculated on the basis of all results or is related to each method,it can be influenced by the predominant diagnostic system.In this case,it could be more appropriate to use the consensus value related to each diagnostic system,and the EQA organizers should have to decide when this approach is appropriate(i.e., analyte structure,method principle).However,special attention must be paid to the classification of results in the different groups in order to guarantee homogene-ity of data and to facilitate interpretation[8–14]. 1.3.Assessment of laboratory performanceIn setting total analytical error(TEa)in EQA schemes,the aim is to improve analytical quality performances within clinical laboratories in order to detect changes in the biological state of patients,a better follow-up of a treatment and an earlier diagno-sis.Consequently,acceptability criteria for laborato-ries’results in an EQA scheme are of crucial importance:if they are too loose,laboratories with lower performances will not be identified;if they are too stringent,good laboratories will be falsely rejected.The number of‘‘poor performers’’in schemes depends on the acceptability criteria used, but it can also be influenced by the statistical proce-dure used[8–14].In choosing acceptability criteria,it must be borne in mind that continuous improvement in laboratory performances is achieved when the total unaccept-able performances are limited to a fraction of the overall performances,thereby avoiding to specify limits that are difficult to attain and which discourage laboratories.The laboratory must set the quality specifications including imprecision and inaccuracy goals for each analyte that it uses to evaluate and monitor its work, guarantee its performance and ensure the diagnostic relevance of its results.Each test must satisfy require-ments in terms of accuracy and precision and,in every clinical situation,it is necessary to ensure the accuracy required to distinguish between a normal and a pathological result and the precision needed for de-ciding whether a variation in a result is clinically significant or whether it is due to the analytical variability of the test.The combination of imprecision and inaccuracy provides the TEa to achieve an ac-ceptable result.Numerous quality requirements have been defined over the last20years in order to establish analytical quality specifications.In1999,an International Con-ference in Stockholm,‘‘Strategies to Set Global An-alytical Quality Specifications in Laboratory Medicine’’,led to a consensus agreement defining a hierarchy of models that should be applied.Where available,and when appropriate for the intended purpose,models higher in the hierarchy must be preferred to those at lower levels[15].2.AimIn spite of numerous articles in the literature addressing the theoretical and practical bases to de-sign an appropriate scheme,many difficulties are still encountered in routine practice.Each scheme has its own particularities and can emphasize one or more goals.The aim of this paper is to describe the quality specifications used in our EQA schemes in order to design schemes that can assess the reliability of laboratory performance and meet the changing needs and quality recommendations.3.Material and methodsQuality specifications are specific performance standards that should be suggested by scientific soci-eties and expert opinions and be defined on the basis of theoretical and practical considerations[16–28]. We individuated the quality specifications in the literature and applied them to participating laborato-ries’results in EQA schemes managed by the Centre of Biomedical Research(CRB).In particular,we describe the quality specifications applied to:control materials,statistical procedure,and assessment of laboratory performance.3.1.Control materialsAlkaline phosphatase and cholesterol data obtained using commercial control material and human serum controls,in two different EQA surveys(2–2002and 1–2003)are reported.L.Sciacovelli et al./Clinica Chimica Acta346(2004)87–97893.2.Statistical procedureThe non-parametric procedure is used to process EQA results.The assigned value(A V)is the median calculated on method/diagnostic system related results,after the exclusion of values outside the range:median F3DSrob(outliers),where DSrob is (75j percentile–25j percentile)/1.349.The present paper reports the inter-laboratory variability(CV%) data of a diagnostic system obtained for troponin I and the A V data for the CK-MB mass in the2001 and2003cycles concerning the main diagnostic systems.3.3.Assessment of laboratory performanceWe identified three different approaches to set analytical goals using the model defined by the International Conference in Stockholm:(a)based on clinical criteria;(b)based on biological variation;(c) resulting from the state-of-the-art[15].For clinical criteria and biological variation,the goals of imprecision and inaccuracy provided in liter-ature have been used to calculate the TEa on the basis of Fraser’s formula:TEa=1.65Â(0.5CV I)+0.25 (CV I2+CV G2)1/2,where CV I is within-subject biologi-cal variation and CV G is between-subject biological variation[22,24,26].For state-of-the-art,on the other hand,the TEa is chosen as the mean of inter-laboratory coefficients of variation(CVinter%),calculated on homogeneous groups of method/diagnostic systems,after eliminat-ing outliers.We calculated the percentage of acceptable per-formances(AP)obtained using the TEa set accord-ing to the three approaches.The number of acceptable performances is obtained by comparing the bias percentage of each result with TEa.The bias percentage is calculated according to the formula:(EQA resultÀA V)/A VÂ100.When a bias is lower than TEa the performance is acceptable; when it is higher it is considered unacceptable.The present paper reports data of some analytes with a high clinic-diagnostic value(cholesterol,glucose, and glycated hemoglobin A1c)and analytes char-acterized by a low biological variation,such as sodium.4.Results and discussion4.1.Control materialsThe results obtained utilizing the4-nitrophenyl-phosphatase(4-NPP)method with2-amino-2-meth-yl-1-propanol(AMP)buffer or with diethanolamine (DEA)buffer on commercial materials(Fig.1)and on human serum materials(Fig.2),are reported.The distribution of results,obtained with the two different buffers,overlaps when commercial materialsare Fig.1.Results of participating laboratories obtained utilizing commercial control material.L.Sciacovelli et al./Clinica Chimica Acta346(2004)87–9790used and is clearly separated with human serum materials,such as the patients’samples where the known AMP/DEA ratio is0.42.In this case,the use of human serum materials is more appropriate be-cause it simulates the behaviour of patient’s serum and it does not present commutability problems.Fig.3reports the total cholesterol bias between the median value of a diagnostic system and the median value of cholesterol oxidase/amino-4antipyrine,per-oxidase method(COD-PAP),in two different control materials(commercial and human serum).Both mate-rials had a negative score,to a lesser extent in the case of human serum materials.When commercial control materials are used in EQA schemes,the diagnostic systems manufacturer involved usually explains this score as a commutabil-ity problem.The use of human serum materials confirms that the problem is linked to the lack of standardization and rules out any commutability prob-lem connected with commercialmaterials.Fig.3.Scores between the median of a diagnostic system and the median of the related method,obtained in eight EQA surveys utilizing commercial and human serum controlmaterials.Fig.2.Results of participating laboratories obtained utilizing human serum control material.L.Sciacovelli et al./Clinica Chimica Acta346(2004)87–9791The use of commercial control materials is advan-tageous in view of the large number of analytes and the large range of concentrations they can provide in the same material,good stability during storage and shipping,and lower costs.But a possible conflict of interests with manufacturers’diagnostic systems and non-commutability attributed to the modification of matrix materials may cause problems.While the use of human serum materials is highly desirable,their use is limited by:high costs,the difficulty in obtaining multiple analytes in large quantities in the same sample,and the difficulty in obtaining the presence of abnormal levels of analytes in the same sample. Therefore,the use of commercial materials in combi-nation with human serum materials appears the best possible solution in EQA schemes.4.2.Statistical procedureFig.4reports the inter-laboratory variability (CV%)obtained in the most recent EQA cycles for troponin I analysed with a diagnostic system.The increase in CV%,found in the first survey of the2003 scheme,corresponded to the introduction of a new kit formulation.This kit manufacturer’s,alarmed by this finding,promoted an inquiry in cooperation with the EQA organizers and kit users.Although the inquiry is still in progress,the corrective actions undertaken seem to have already improved the method perfor-mance(CV%:from23.4to11.4).The A V of the CK-MB mass obtained on the2001 and2003cycle samples using four different diagnos-tic systems is reported in Fig.5.The different diag-nostic systems(A–D)give different values and,in some cases,the between-assay differences are about twofold.In the last surveys(2003-4,2003-5,2003-6) these differences were slightly reduced.A correct analysis of these data shows that there are standard-ization problems.The growing number of commercially available test kits lead to values that differ from each other and the incomparability of results obtained with different kits hampers appropriate patient care,if inadequate reference ranges are used.A harmoniza-tion of test results must be achieved in different commercially available assays only through coopera-tion between manufacturers,laboratories and EQA organizers.An adequate statistical procedure allows us to obtain reliable A V and inter-variability coefficients in order to evaluate the variability of results from a method/diagnostic system,and the comparability of results obtained using different methods/diagnostic systems.These data should promote corrective actions designed to achieve agreement between meth-ods and to obtain improvements of each method performance.4.3.Assessment of laboratory performanceThe present paper reports,for four analytes,the percentage of acceptable performances obtained in the EQA results from the2003cycle by means of the application of goals based on:clinical criteria,biolog-Fig.4.Inter-laboratory variability(CV%)obtained in the most recent cycles for troponin I analysed with a diagnostic system.L.Sciacovelli et al./Clinica Chimica Acta346(2004)87–9792ical variation,and state-of-the-art.The TEa used in our EQA schemes,are also reported.We chose the specifications based on biological variation and com-pared them with the state-of-the-art,which seemed to be the most practical approach because clinical data are not always available.If the limits based on biological variation were too narrow (a high percent-age of laboratories having poor performances)or too wide (a high percentage of laboratories having good performances)we replaced them with other limits that are multiples or under-multiples of those derived from Fraser’s formula,so that no more than 25%of the results of laboratories considered had an unacceptable performance [27].Fig.5.Assigned values of CK-MB mass obtained in the 2001and 2003cycles samples involving four different diagnostic systems (A,B,C,D).L.Sciacovelli et al./Clinica Chimica Acta 346(2004)87–97934.4.Cholesterol and glucoseFor cholesterol and glucose,most of the results attained the analytical goals based on clinical criteria (cholesterol:90.5%;glucose:78.1%);a higher per-centage of results the biological goals (cholesterol:92.5%;glucose:90.0%).Otherwise,about 60%(cho-lesterol:61.1%;glucose:59%)of results were accept-able when goals based on state-of-the-art were applied.Our EQA goals,which are narrower goals in order to encourage laboratories to achieve quality improvement,are attained by 83.6%(cholesterol)and 79.1%(glucose)of results.Although current technology should allow the use of more restrictive goals (mean CV%=3.3%and 3.33%,for cholesterol and glucose,respectively),their advantages do not justify the efforts to maintain this quality level.Moreover,when TEa =3.3andTEa =3.33are used,the percentage of unacceptable results is too high (about 40%)and could discourage laboratories from attempting to improve upon quality (Table 1and Figs.6,7).4.5.SodiumThe clinical goal for sodium is not available and only 45%of results achieve the biological goal because the biological variation of sodium is very low.The percentage of acceptable results is 68.1%when the goal is based on state-of-the-art.The goal used in our EQA scheme seems to be the more appropriate one because it takes into consideration current methodological possibilities and only a low percentage of laboratories have unacceptable perform-ances.The manufacturers of diagnostic systems should improve upon the precision and accuracy ofTable 1Total percentage of acceptable performances obtained in the 2003cycleTotalAcceptable performances performances Clinical goal Biological goal State-of-the-art goal EQA goal NN (%)N (%)N (%)N (%)Cholesterol 4130373790.5382092.5252261.1345383.6Glucose 4190327278.1377190.0247259.0331379.1Sodium4031181445.0274568.1304875.6Glycated hemoglobin1710133878.266438.8103060.2130576.3Fig.6.Percentage of acceptable performances obtained in eight different control materials on applying the different goals.The data are shown with the sequential distribution of the 2003cycle and the median values obtained with cholesterol oxidase,amino-4antipyrine,peroxidase method (CHOD,PAP)ranging from 3.94mmol/L to 5.00mmol/L.L.Sciacovelli et al./Clinica Chimica Acta 346(2004)87–9794their methods to enable laboratories to achieve the biological goal (Fig.8).4.6.Glycated hemoglobinIn the case of glycated hemoglobin,the A V is determined using the DCCT method,which provides a more reliable evaluation of performances when the consensus value is used.The biological goal is attained by a low percentage of results (38.8%)[26].The percentage of laboratories that attained the other analytical goals ranged from 60.2%to 78.2%for all goals applied.The use of the value obtained with the DCCT method (as AV),chosen by a group of experts according to scientific recommendation,aims to stimulate the improvement of standardization between diagnostic systems and the agreement between laboratories results (Fig.9).The application of EQA goals,chosen using the above described criteria,was found to be effective.In fact,the laboratories’performances significantly im-proved over time.For example,in the cardiac markers scheme,the number of unacceptable performances,calculated on results obtained in the samelaboratories,Fig.7.Percentage of acceptable performances obtained in eight different control materials on applying the different goals.The data are shown with the sequential distribution in 2003cycle and the median values obtained with glucose oxidase,peroxidase method (GOD,POD)ranging from 4.60mmol/L to 6.38mmol/L.Fig.8.Percentage of acceptable performances obtained in eight different control materials on applying the different goals.The data are shown with the sequential distribution in 2003cycle and the median values obtained with indirect potentiometric method (ISE)ranging from 141.0mmol/L to 145.0mmol/L.L.Sciacovelli et al./Clinica Chimica Acta 346(2004)87–9795decreased (from 11.6%to 5.3%)and the number of optimum performances increased (from about 49%to about 60%)for troponin I.Similarly,unacceptable performances decreased for myoglobin (from 19.5%to 11.6%),and for the CK-MB mass (from 13.2%to 3.9%).5.ConclusionThe increased diagnostic value of the test results and their recognized impact on clinical outcome stress the importance of the laboratory test.Therefore,appropriate quality specifications should be estab-lished for each test in order to guarantee high-quality analytical performances.EQA is an important com-ponent in quality management,providing compari-sons with other laboratories and with established quality specifications.EQA schemes should be inte-grated in the laboratory process,as this will guarantee that the following are achieved:problems are focused on,the quality control system is constantly reviewed and updated,and efforts to bring about improvement are supported.To design reliable EQA schemes,it is very impor-tant to define the quality specifications required to promote quality improvement in laboratories.These must comply with quality requirements and scientific recommendations and their appropriateness enhances the value of laboratory test results and clinical prac-tice,and can be effective in evaluating the patient’s outcome.Cooperation between laboratories,EQAorganizers and manufacturers of diagnostic systems is crucial to establishing the most adequate possible quality specifications,which comply with criteria for efficiency and effectiveness.References[1]Wong ET.Improving laboratory testing:can we get physiciansto focus on outcome?Clin Chem 1995;41(8(B)):1241–7.[2]Plebani M.The clinical importance of laboratory reasoning.Clin Chim Acta 1999;280:35–45.[3]Plebani M.Appropriateness in programs for continuous qual-ity improvement in clinical laboratories.Clin Chim Acta 2003;333:131–9.[4]Waise A.Clinical audit and the contribution of the laboratoryto clinical outcome.Clin Chim Acta 1999;280:47–57.[5]Lewis LS.Quality control:good laboratory practice—an over-view of quality assurance.www.who.int .[6]Libeer JC.External quality assurance programmes in medicallaboratories.Accredit Qual Assur 2001;6:151–3.[7]Libeer JC.Role of external quality assurance schemes inassessing and improving quality in medical laboratories.Clin Chim Acta 2001;309(2):173–7.[8]Libeer JC.External quality assessment in clinical laboratories.European perspectives:today and tomorrow.Antwerpen:Uni-versitaire Instelling Antwerpen;1993.[9]International Federation of Clinical Chemistry (IFCC).Fun-damental for External Quality Assessment (EQA)1997.[10]ISO Guide 43.Proficiency testing by inter-laboratory compar-ison.Second ed.International Organization for Standardiza-tion (ISO);1997.[11]ing proficiency testing (PT)to improve the clinicallaboratory.Approved guideline GP27-A.1999;19(15).[12]ILAC-G13.Guidelines for the requirements for the compe-tence of providers of proficiency testing schemes.2000.[13]Clinical Pathology Accreditation (UK).Standards forEQAFig.9.Percentage of acceptable performances obtained in eight different control materials on applying the different goals.The data are shown with the sequential distribution in 2003cycle and the median values obtained with DCCT method ranging from 5.1%to 10.2%.L.Sciacovelli et al./Clinica Chimica Acta 346(2004)87–9796Schemes in Laboratory Medicine.Version4.01(September 2003).[14]NCCLS Using Proficiency Testing(PT)to improve the Clin-ical Laboratory.Approved Guideline,GP27-A.(August 1999);19(15).[15]Petersen HP,Fraser CG,Kallener A,Kenny D.Strategies toset global analytical quality specifications in laboratory med-icine.Scand J Clin Lab Invest1999;59(7):475–585. [16]Petersen HP,Groth T,de Verdier CH.Principles for assessinganalytical quality specifications and their use in design of control systems.Uppsala J Med Sci1993;98:195–214. [17]Fraser CG,Petersen PH.Desirable standards for laboratorytests if they are to fulfill medical needs.Clin Chem1993;39/7:1447–55.[18]Fraser CG,Petersen HP.Quality goals in external qualityassessment are best based on biology.Scand J Clin Lab Invest 1993;53(Suppl.212):8–9.[19]Petersen HP,Blaabjerg O,Irjala K,Ice`n A,Bjotro K.Elementsof analytical quality.Helsinki,Finland:Nordkem Clinical Chemistry Project,1994.p.187–94.[20]Stockl D,Baadenhuisjen H,Fraser CG,Libeer J-C,PetersenHP,Ricos C.Desirable routine analytical goals for quantities assayed in serum.Eur J Clin Chem Clin Biochem1995;33: 157–69.[21]Fraser CG,Hyltoft Petersen P,Libeer J-C,Ricos C.Proposalfor setting generally applicable quality goals solely based on biology.Ann Clin Biochem1997;34:1–8.[22]Sebastia`n-Ga`mbaro MA,Liron-hernandez FJ,Fuerte-ArdeiuX.Intra-and inter-individual biological variability data bank.Eur J Clin Chem Clin Biochem1997;35(11):845–52. [23]Fraser CG.General strategies to set quality specifications forreliability performance characteristics.Scand J Clin Lab Invest 1999;59:487–90.[24]Rico`s C,Alvarez V,Cava F,Garcia-Lario JV,Hernandez A,Jimenez CV,Minchinela J,Perich C,Simon M.Current data-bases on biological variation:pros,cons and progress.Scand J Clin Lab Invest1999;59:491–500.[25]Westgard JO.The need for a system of quality standards formodern quality management.Scand J Clin Lab Invest1999;59:483–6.[26]Garde AE,Hansen AM,Skovgaard LT,Christensen JM.Seasonal and biological variation of blood concentrations of total cholesterol,dehydroepiandrosterone sulfate,hemo-globin A1C,IgA,prolactin,and free testosterone in healthy women.Clin Chem2000;46(4):551–9.[27]Sciacovelli L,Secchiero S,Zardo L,Plebani M.Externalquality assessment schemes:need for recognised require-ments.Clin Chim Acta2001;309:183–99.[28]Secchiero S,Sciacovelli L,Zardo L,Plebani M.Appropriate-ness of cholesterol and triglycerides reporting checked by external quality assessment programs.Clin Chim Acta2003;333(2):221–30.L.Sciacovelli et al./Clinica Chimica Acta346(2004)87–9797。
血浆凝血酶调节蛋白活性功能测量的方法[发明专利]
![血浆凝血酶调节蛋白活性功能测量的方法[发明专利]](https://img.taocdn.com/s3/m/a01a6232a58da0116d17491b.png)
专利名称:血浆凝血酶调节蛋白活性功能测量的方法专利类型:发明专利
发明人:帕特里克·万德丹,奥雷莉·卢梭
申请号:CN200780044311.6
申请日:20071128
公开号:CN101605907A
公开日:
20091216
专利内容由知识产权出版社提供
摘要:本发明涉及体外测量凝血调节蛋白功能活性的方法,其中所述方法包括定量来自生物样品的生物介质中,蛋白C在凝血酶辅助因子即凝血调节蛋白存在下,通过凝血酶向激活的蛋白C(PCa)的激活,所述方法包括向样品血浆中加入蛋白C系统激活所需的试剂、加入纯化的蛋白C并且还加入纤维蛋白聚合抑制剂。
本发明还涉及该方法在检测凝集病理中的应用。
申请人:斯塔戈诊断公司
地址:法国阿涅尔
国籍:FR
代理机构:北京英赛嘉华知识产权代理有限责任公司
更多信息请下载全文后查看。
Alfa Laval Culturefuge 200产品介绍说明书
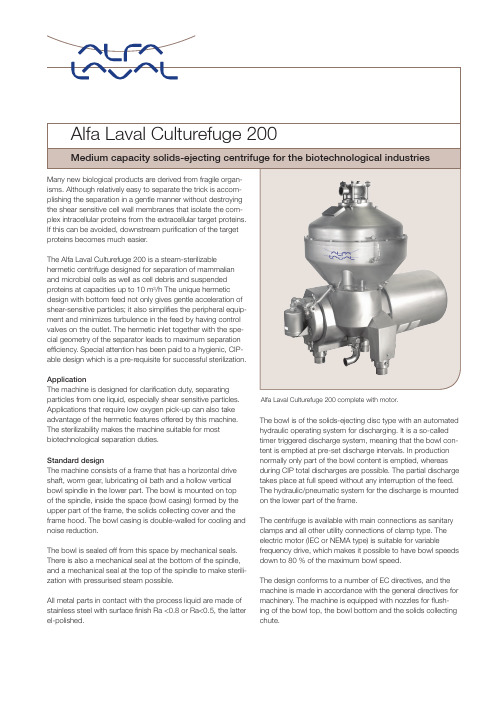
particles from one liquid, especially shear sensitive particles. Applications that require low oxygen pick-up can also take advantage of the hermetic features offered by this machine. The sterilizability makes the machine suitable for most biotechnological separation duties.Medium capacity solids-ejecting centrifuge for the biotechnological industriesAlfa Laval Culturefuge 200 complete with motor.Standard designThe machine consists of a frame that has a horizontal drive shaft, worm gear, lubricating oil bath and a hollow vertical bowl spindle in the lower part. The bowl is mounted on top of the spindle, inside the space (bowl casing) formed by the upper part of the frame, the solids collecting cover and the frame hood. The bowl casing is double-walled for cooling and noise reduction.The bowl is sealed off from this space by mechanical seals. There is also a mechanical seal at the bottom of the spindle, and a mechanical seal at the top of the spindle to make sterili-zation with pressurised steam possible.All metal parts in contact with the process liquid are made of stainless steel with surface finish Ra <0.8 or Ra<0.5, the latter el-polished.The bowl is of the solids-ejecting disc type with an automated hydraulic operating system for discharging. It is a so-called timer triggered discharge system, meaning that the bowl con-tent is emptied at pre-set discharge intervals. In production normally only part of the bowl content is emptied, whereas during CIP total discharges are possible. The partial discharge takes place at full speed without any interruption of the feed. The hydraulic/pneumatic system for the discharge is mounted on the lower part of the frame.The centrifuge is available with main connections as sanitary clamps and all other utility connections of clamp type. The electric motor (IEC or NEMA type) is suitable for variablefrequency drive, which makes it possible to have bowl speeds down to 80 % of the maximum bowl speed.The design conforms to a number of EC directives, and the machine is made in accordance with the general directives for machinery. The machine is equipped with nozzles for flush -ing of the bowl top, the bowl bottom and the solids collecting chute.A l f a L a v a l i s a t r a d e m a r k r e g i s t e r e d a n d o w n e d b y A l f a L a v a l C o r p o r a t e AB . [P r o d u c t n a m e ] i s a t r a d e m a r k o w n e d b y A l f a L a v a lC o r p o r a t e A B .P C H S 00128E N 1503Alfa Laval reserves the right to change specifications without prior notification.How to contact Alfa Laval Up-to-date Alfa Laval contact details for all countries arealways available on our website at Technical specificationHydraulic capacity 10 m 3/h 1)Bowl volume 15 l Bowl speed max. 7 200 rpm G-forcemax. 11 900Motor speed synchronous 57,6 Hz (VFD) 1728 rpmInstalled motor power/protection 22/25 kW/IP 55; IE3 Feed inlet pressure required at inlet flange max. 50-100 kPa 2)Overhead hoist lifting capacity min. 300 kgSound pressure79 dB(A)3)1)Actual throughput depends on amount and type of solids in the feed,viscosity and required degree of clarification.2)At 5 m 3/h 3)According to ISO 3744Utilities consumption Electric power17.5 kW 1)Flushing liquid per discharge 10-30 l per dischargeOperating liquid1 l per discharge Steam @ 270 kPa pressure 20 kg per sterilizationCooling liquid for frame partsmax. 500 l/h1)At 3 m 3/h. Power consumption increases with the flow rate.Shipping data (approximate)Centrifuge excl. motor max 1288 kg Motor 177/211 kg Bowl max 292 kgGross weight2200 kgVolume6 m 3Material dataBowl body, bowl hood and lock ring s.s.1.4501 UNS 32760Frame top part and hood (ASME) s.s 1.4404 ASME SA-240Frame top part and hood (PED)s.s. 1.4404Frame bottom part Cast iron, clad withs.s 1.4301 UNS S 30200In-and outlet partss.s. 1.4401 UNS S 31600Gaskets and O-rings product-wetted EPDM rubber food grade and PTFE food grade Bowl seal ringPEEK food gradeSeal rings in- and outlet Resin impregn.Carbon Graphite food grade Wear ring in- and outlet Reaction bondedSilicon Carbide food gradeDesign features• Fully hermetic design for minimal shear stress andabsence of oxygen.• Different disc stacks for different sediment loading • Two different outlet impeller diameters available • Designed for easy cleaning-in-place (CIP).• The centrifuge system can be made fully contained • Design pressure of the bowl casing 300 kPa.• Design pressure for the cooling jacket 300 kPa forconnection to centralized cooling circuit.• Bowl casing and cooling jacket designed according toASME or PED.• Sterilizable (SIP) with 270 kPa steam in a 20-30 mincycle, including discharge system.• Most parts in contact with the process liquids availablewith two alternative surface finishes.• Product wetted parts passivated (optional).• All product wetted polymers and seal rings compliantwith FDA regulation.Working principleSeparation takes place inside a rotating bowl. The untreated feed is introduced to the bowlfrom the bottom through a hollow spindle (1), and isbefore entering the disc stack (3). The separation of the sedi-discs. The light phase moves towards the center and is discharged by an impeller (4). The heavy sediment phase is collected at the periphery and is ejected from the bowl intermittently at full operating speed. The variable volume partial discharge is achieved by a hydrau-lic system below the separation space. At preset intervals, this system forces the sliding bowl bottom (5) to drop down, thus opening the sediment ports (6) at the periphery.。
迈克沃伊和法默的中国体外诊断分销指南说明书

McEvoy and Farmer's Complete Guide to IVD Distribution in Chinahttps:///r/W875106C98AEN.htmlDate: May 2009Pages: 240Price: US$ 3,995.00 (Single User License)ID: W875106C98AENAbstractsWho is Who in Clinical Diagnostics in China, produced jointly with the firm McEvoy & Farmer, is the product of on-the-ground primary research on Chinese labs conducted in fall and winter 2008. Included in this report:Market Size Estimate by Major Category (Chemistry, Critical Care Chemistry, Urine Chemistry, Hematology, Flow Cytometry, Coagulation, Immunochemistry, Molecular Testing, Other IVD)Country Industry OverviewChinese Hospital StatisticsProfiles of 42 International Diagnostic Companies with operations in ChinaProfiles of 130 Domestic Diagnostic CompaniesProfiles of 24 Local Distributors, indicating the companies they distribute forThe Chinese market represents a significant opportunity for IVD diagnostic companies. But actionable information about this emerging market is often difficult to get. Only with an exhaustive, on-the-ground research team can a company truly understand the chinese market. Now, a resource is available that can make on-the-ground research available to all companies at a fraction of the cost.Published jointly with trusted Asian IVD market experts, this Kalorama report is acomplete survey of the IVD market in China today. Market size for major categories of the IVD market, products on the market, important Chinese market trends and intense company profiles are part of this exhaustive study.This country of 1.3 billion people is now America’s sixth largest export market, and China’s economy, while showing some effects of the world recession, has been less impacted than other nations and is showing growth, although not as rapid as in recent years. A number of recent events and trends in the Chinese healthcare environment are making China an increasingly attractive market opportunity for in vitro diagnostics companies. The increasing numbers of private laboratories and expanded reference laboratories are expanding the market for tests of all kinds.Although there are a number of challenges for diagnostic manufacturers to understand and overcome, the market for clinical diagnostics in China (both reagents and instruments) remains one of the most promising emerging markets in the world.ContentsCOUNTRY SUMMARYMarket TotalsWhat is New in ChinaThe Healthcare System in ChinaMedical InsuranceA Brief Guide to the BureaucracyPrivate and Reference LaboratoriesPrivate Medical PracticeProduct RegistrationReimbursementTendersReagent RentalQuality ControlVacuum Tube ConversionSecond hand InstrumentsImported and Domestic Sales INTERNATIONAL MANUFACTURER PROFILESAbbott LaboratoriesABXAcon Biotech/InvernessAdaltisAffymetrixAgilent TechnologiesApplied BiosystemsArkrayAudit DiagnosticsBeckman CoulterBDBioneer TradeBio Rad LaboratoriesbioMérieuxDiaSorinDiaSys Diagnostic SystemsEppendorfEuroimmunFujirebio/CanAg DiagnosticsHitachi High Technologies CorporationHospitexHumanInverness MedicalJei Daniel (JD) BiotechJokohMedicine Devices Company (MDC) Melet Schloesing LaboratoriesMP BiomedicalsOrtho ClinicalDiagnosticsPerkinElmerPromegaQiagenRadiometerRandoxR BiopharmRocheSiemens Healthcare Diagnostics StagoSysmex CorporationThermoFisherVirionSerionYD DiagnosticsDOMESTIC MANUFACTURER PROFILES3V BioengineeringAccuBio TechAddcare Bio TechAi De Diagnostic (IND)AmpllyAntai DiagnosticsAudicom Medical InstrumentAutobio DiagnosticsAVE Science & TechnologyB & E Scientific InstrumentBasoDiagnosticsBeijing Genomics Institute (BGI Healthcare)Biocell InstituteBiocreateBiocup Biotech CompanyBioer TechnologyBiosino BiotechnologyBiote CompanyBioway BiotechnologyBlue Cross Bio MedicalBowlinman Sunshine Science & TechnologyCaihong Analytical InstrumentCaltech GroupCapitalBio CorporationCaretium Medical InstrumentsChang Chun Brother BiotechChangdao BiotechnologyChemClin Bio Tech / China Diagnostics Medical Chemtron BiotechChina Medical/Yuande Bio Medical EngineeringCondor Teco Medical TechnologyCornley Hi TechDa An GeneDecipher BioscienceDirui IndustrialDL Medical BiotechDoubleQ LabDragon MedicalElikan Biological TechnologyFenghua BioengineeringFengHui Medical Science & Technology First Sun ElectronicFosun DiagnosticsGenetel PharmaceuticalsGenius ElectronicsGoldsite DiagnosticsHai Tai BiologicalHaoyuan BiotechnologyHeal Force/Nison InstrumentHealthDigitHongcheng (HC) BiopharmaceuticalHongshi Medical TechnologyHope Industry and TradeHua Sin ScienceHua Tong Medical InstrumentHuaguan Biochip CompanyHuatai Biotechnology IndustrialHuayang Analysis InstrumentHybriBioInTec ProductsJian Ye Medical EquipmentinSangTe Medicine InstrumentKanghua Biotech CompanyKehua Bio EngineeringKinghawk TechnologyLabnovation TechnologiesLandwind International Medical Science LaoLa ElectronicLeadman Biochemistry TechnologyLengguang TechnologyLingyi Medical ScienceLivzon GroupLongx TechnologiesMaker Science TechnologyMaysun TechnologyMaxcom ElectronicMD Pacific TechnologyMeiyilin Electronics InstrumentMerit Choice BioengineeringMindray Medical ElectronicsModern Gold BiotechnologyNanfen Medical Biochemical InstrumentNeusoft Medical SystemsNew MoonNewScen Coast Bio PharmaceuticalOption Science & Technology Development Company Perlong GroupPG Biotech/QiagenPrecil InstrumentProcan ElectronicsRayto Life and Analytical SciencesRich Science IndustryRongsheng Biotech.Runbio Biotech .Sanco InstrumentSan Jose Medical Products..Sciarray BiotechSciendox Bio-Technology CompanySenlong Biotech..Share SunShensuo Medical DiagnosticsShenzhen New Industries Biomedical Engineering (SNIBE) Shining Sun TechnologySinnowa Medical Science & TechnologySTAC Medical Science & TechnologySteellex Scientific InstrumentStrong Biotechnologies...Success Technology DevelopmentSun BiotechSunostik Biomedical TechnologySym-Bio Lifescience.Tecom ScienceTechcompTellgen LifeTiangen Biotech...TianHai Medical Equipment (THME)Tianlong Science and TechnologyTigsun Biotinge Science & TechnologyTZD Technological.Urit Medical ElectronicWanCheng Bio-elect.Wantai BiologicalWasson An-Ze Bio-tech Company..WearmaxWeirikang Biological TechnologyW.H.P.M. Bioresearch & Technology/Hemosure Wondfo BiotechXun-Da Medical InstrumentYasen IndustrialYaxin Sheng WuZhong Tai BiotechZJ Bio-TechDISTRIBUTOR PROFILESAdvanced Clinical Laboratory Science (ACLS)Ailex Technology.....AusBio LaboratoriesBio-Asia DiagnosticsBiochem GroupBio-Star Technology DevelopmentChindex InternationalChinMax Medical SystemsDiamond BiotechnologyDong Hu Instrument/East LakeFu Li Tai (FLT) MeditecGene CompanyGiantech Medical Science & TechnologyGolden-Grand Medical Hongtex Bio-techLangkaNewtime TradingRainbow-Mega Scientific InstrumentScience International/Science LaboratoriesSunlionSuns-GroupTruth EnterpriseUnited Science InternationalVastec Medical..Zhi Cheng Biotech.Appendix: China’s Hospitals by Province.I would like to orderProduct name:McEvoy and Farmer's Complete Guide to IVD Distribution in ChinaProduct link:https:///r/W875106C98AEN.htmlPrice:US$ 3,995.00 (Single User License / Electronic Delivery)If you want to order Corporate License or Hard Copy, please, contact our CustomerService:*************************PaymentTo pay by Credit Card (Visa, MasterCard, American Express, PayPal), please, clickbutton on product page https:///r/W875106C98AEN.htmlTo pay by Wire Transfer, please, fill in your contact details in the form below:First name:Last name:Email:Company:Address:City:Zip code:Country:Tel:Fax:Your message:**All fields are requiredCustumer signature _______________________________________Please, note that by ordering from you are agreeing to our Terms& Conditions at https:///docs/terms.htmlTo place an order via fax simply print this form, fill in the information belowand fax the completed form to +44 20 7900 3970。
NAF中文样本2011-10-14
6
生产过程中的 智能化 Principles
从看板管理的库房中 取出零件
检查螺栓的 拉紧转矩
总装配
在试验台上进行 100%全面检查
我们的生产速度极快。即使是个人的小 批量订单,也是在我们高度现代化的具 有多个平台的加工中心,从多达300个 工具存放处取用工具,使用多达36个加 工处理平台的情况下完成的,这也就形 成了我们的一个流生产。不需要准备时 间,工作转换和预拼装在车间内自动进 行,精简的组织结构和其他大量的智能 化细节保证了我们客户产品的作业能力 始终保持在最高水平。我们始终在准备 并且已经准备好了应对市场的任何状 况。这是我们可以信守的承诺。”
彼得 • 伊利格是NAF的 销售部经理,他在“积 木式原理”的报告中 说,模块化生产的想法 不仅为大批量生产提供 了价格优势,小批量生 产同样适用。
模块化,而不是现成的 “我们的客户需要可靠同时价格合理的 传动解决方案,以保证他们的机械在全 球市场上的竞争力。所以,我们仔细分 析其工作环境,以将传动系统制作为最 合适的规格尺寸。另一方面,我们必须 尽可能的降低产品的成本,并且不受数 量影响。 我们是通过NAF内部的“积木式原理” 来做到这点的。这样,我们在生产过程 中,对部件和单个零件进行时间控制和 生产的灵活配置,最终完成独特的传动 方案。产品的成本优势效应发挥着巨大 的作用,我们的用户将最终受益。”
用于预防和治疗肥胖和有关障碍的化合物[发明专利]
![用于预防和治疗肥胖和有关障碍的化合物[发明专利]](https://img.taocdn.com/s3/m/7366d13fc381e53a580216fc700abb68a982ad0b.png)
专利名称:用于预防和治疗肥胖和有关障碍的化合物专利类型:发明专利
发明人:E·J·维拉弗兰卡
申请号:CN202080030234.4
申请日:20200302
公开号:CN114072376A
公开日:
20220218
专利内容由知识产权出版社提供
摘要:在某些方面,本文提供了通过给受试者施用本发明的化合物在受试者中治疗或预防肥胖、辅助或诱导重量减轻、抑制食欲或抑制重量增加的方法。
申请人:阿布雷克斯制药股份有限公司
地址:美国加利福尼亚
国籍:US
代理机构:中国贸促会专利商标事务所有限公司
代理人:李华英
更多信息请下载全文后查看。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
描述
TD 160 AL FC 100 x 32 FC 120 x 32 UD 80 A UDJ 125 A UDJ 160 A UD 250 A UD 400 A UDF 500 A FSJ FLG 250 FLG 400
第页
25 9 9 22 22 22 23 23 23 22 23 23
描述
UBS 1/5 TN UBS 4/5 TN UBS 4/5 T UBS 1/10 TN UBS 2/10 TN UBS 2/10 T UBS 3/10 TN 2 M 2 x 15,5 x 0,8 2 M 8 x 6 x 0,5 2 M 3 x 9 x 0,8 2 M 6 x 9 x 0,8 2 M 9 x 9 x 0,8 2 M 3 x 13 x 0,5 2 M 6 x 13 x 0,5 2 M 4 x 15,5 x 0,8 2 M 6 x 15,5 x 0,8 2 M 10 x 15,5 x 0,8 2 M 2 x 20 x 1 2 M 3 x 20 x 1 2 M 4 x 20 x 1 2 M 5 x 20 x 1 2 M 6 x 20 x 1 2 M 10 x 20 x 1 2 M 2 x 24 x 1 2 M 3 x 24 x 1 2 M 4 x 24 x 1 2 M 5 x 24 x 1 2 M 6 x 24 x 1 2 M 8 x 24 x 1 2 M 10 x 24 x 1 2 M 2 x 32 x 1 2 M 3 x 32 x 1 2 M 4 x 32 x 1 2 M 5 x 32 x 1 2 M 6 x 32 x 1 2 M 8 x 32 x 1 2 M 10 x 32 x 1 2 M 2 x 40 x 1 2 M 3 x 40 x 1 2 M 4 x 40 x 1 2 M 5 x 40 x 1 2 M 6 x 40 x 1 2 M 8 x 40 x 1 2 M 10 x 40 x 1 2 M 3 x 50 x 1 2 M 4 x 50 x 1 2 M 5 x 50 x 1 2 M 6 x 50 x 1 2 M 8 x 50 x 1 2 M 10 x 50 x 1 2 M 3 x 63 x 1 2 M 4 x 63 x 1 2 M 5 x 63 x 1 2 M 6 x 63 x 1 2 M 8 x 63 x 1 2 M 10 x 63 x 1 2 M 3 x 80 x 1 2 M 4 x 80 x 1 2 M 5 x 80 x 1 2 M 6 x 80 x 1 2 M 8 x 80 x 1 2 M 10 x 80 x 1
9
FC 80 x 50
9
HCBC 80
9
HCBC 100
9
HCBC 120
9
BC 30
9
BC 40
9
BC 50
9
BC 63
9
BC 80
9
BC 100
9
RFS 40-63
8
RFS 80-100
8
FS 24
8
FS 32
8
FS 40-63
8
FS 80-100
8
UFS Kit
8
ERIFLEX FLEXIDRILL R 26
FT KIT
26
STRIPPING KNIFE SOK 26
SOK SPARE BLADE SOK B 26
MFS
26
SPARE BLADE SET MFS-B 26
MFCB
26
MFB
26
TWISTING TOOL MFT 26
MFC
26
MCBB
26
UBS 1/10 TN 160
12
UBS 1/10 TN 200
25
BD 100/125 AL
25
TD 100/125 A
25
TD 100/1
25
NB 125 A
24
BD 80/100 A
24
BD 80/100 AL
24
TD 80/100 A
24
TD 80/100 AL
24
TD 80/100 ALL
24
型号
563990 568700 568730 569010 569020 569030 569040 569050 569060 569150 569160 569170
12
UBS 2/10 T 160
13
UBS 2/10 T 200
13
UBS 3/10 TN 160
13
UBS 3/10 TN 200
13
UBS 2/10 TN 160
13
UBS 2/10 TN 200
13
TD 160 A
25
NB 160 A
24
BD 40 A
24
TD 40 A
24
BD 100/125 A
艾力锋® 母线槽 (ERIFLEX® ERILINK)
7 8 10 12
目录
2 型号表
3-8 柔性连接件, 绝缘金属编织连接件, 艾力锋® 柔性母排 (ERIFLEX® FLEXIBAR)
9 铜排及夹件
10-19 母排支撑
20-25 分线盒
26 手动及气动工具
27 艾力锋® (ERIFLEX®) 软件,
9
20 12
40 A 7400 A 1000V AC 1500V DC
基础工业 • 钢铁 • 铝业 • 造纸 • 水泥 • 铜业
机械制造 • 焊接 • 电-化学侵蚀
1
交通运输 • 机车 • 造船 • 航空 • 汽车
基础建设 • 办公楼 • 工业厂房 • 医院 • 机场
型号表
型号
538650 541020 541060 541070 541090 541100 541110 541150 541160 541170 541180 541230 541240 541250 541260 541270 541300 541320 541380 544320 544330 544360 544370 544390 544400 544410 544420 544450 544460 544470 544480 544490 544500 544530 544540 544550 544560 544570 544580 544600 544610 544620 544680 544700 544740 544760 549300 549340 549350 549360 549370 549380 549390 549400 549410 549420 549430 549450 549460 549470 549480 549490
低压附件
艾力锋® (
)
低压配电系统的全系列附件产品
通用性
通过认证及测试
创新性
EN 60439-1
节省空间及时间
9
宜于安装
电气行业 • 线缆制造 • 变压器,发电机及电机 • 工程公司 • 计算机行业 • 盘柜部件生产商 • 电气设备生产商
化学工业 • 电解氯 • 电镀
21
电厂及能源设施 • 电力 • 天然气 • 海洋平台 • 可再生能源
第页
12 12 12 12 13 13 13 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7
型号
552940 552950 552960 552970 552980 552990 553020 553030 553040 553050 553060 553070 553100 553110 553120 553200 553210 553220 553230 553250 553260 553370 553380 553550 553560 553570 553580 553590 558600 558900 559050 559060 559100 559110 559120 559150 559160 559170 559190 561500 561510 561520 561530 561540 561550 561870 561880 563200 563201 563720 563740 563800 563810 563820 563830 563840 563841 563900 563910 563920 563930 563940
描述
第页
2 M 4 x 100 x 1
7
2 M 5 x 100 x 1
7
2 M 6 x 100 x 1
7
2 M 8 x 100 x 1
7
2 M 10 x 100 x 1
7
2 M 12 x 100 x 1
7
FC 50 x 24
9
FC 50 x 32
9
FC 50 x 40
9
FC 80 x 24
9
FC 80 x 32
描述
2 M 10 x 120 x 1 3 M 6 x 9 x 0,8 3 M 4 x 15,5 x 0,8 3 M 6 x 15,5 x 0,8 3 M 2 x 20 x 1 3 M 3 x 20 x 1 3 M 4 x 20 x 1 3 M 2 x 24 x 1 3 M 3 x 24 x 1 3 M 4 x 24 x 1 3 M 5 x 24 x 1 3 M 3 x 32 x 1 3 M 4 x 32 x 1 3 M 5 x 32 x 1 3 M 6 x 32 x 1 3 M 8 x 32 x 1 3 M 3 x 40 x 1 3 M 5 x 40 x 1 3 M 5 x 50 x 1 3 M TC 6 x 9 x 0,8 3 M TC 2 x 15,5 x 0,8 3 M TC 4 x 15,5 x 0,8 3 M TC 6 x 15,5 x 0,8 3 M TC 2 x 20 x 1 3 M TC 3 x 20 x 1 3 M TC 4 x 20 x 1 3 M TC 5 x 20 x 1 3 M TC 2 x 24 x 1 3 M TC 3 x 24 x 1 3 M TC 4 x 24 x 1 3 M TC 5 x 24 x 1 3 M TC 6 x 24 x 1 3 M TC 8 x 24 x 1 3 M TC 3 x 32 x 1 3 M TC 4 x 32 x 1 3 M TC 5 x 32 x 1 3 M TC 6 x 32 x 1 3 M TC 8 x 32 x 1 3 M TC 10 x 32 x 1 3 M TC 3 x 40 x 1 3 M TC 4 x 40 x 1 3 M TC 5 x 40 x 1 3 M TC 5 x 50 x 1 3 M TC 8 x 50 x 1 3 M TC 5 x 63 x 1 3 M TC 8 x 63 x 1 CABS APP CABS 4/5 TN MOD CABS 2/10 TN MOD CABS 3/10 TN MOD CABS 4/5 T MOD CABS 2/10 T MOD CABS 3/10 T MOD CABS T SET CABS E CABS M ADD. KIT CABS fixing CABS Bracket TH Kit CABS Bracket BT CABS Bracket SV CABS Bracket RV CABS Bracket PS