TransientHypogammaglobulinemia of Infancy
抗体免疫缺陷病(原发性免疫缺陷病)

抗体免疫缺陷病(原发性免疫缺陷病)【病因】(一)发病原因体液免疫缺陷病包括,Bruton免疫球蛋白缺乏症,可变异型免疫球蛋白缺乏症,选择性IgA缺乏,选择性IgM缺乏。
1.Bruton免疫球蛋白缺乏症又称先天性免疫球蛋白缺乏症(congenital agammaglobulinemia)。
先天性免疫球蛋白缺乏。
2.常见的可变异型免疫球蛋白缺乏症(common variable agammaglobulinemia) 又称特发性晚发免疫球蛋白缺乏症(idiopathic late onset immunoglobulin deficiency),可变异型免疫球蛋白缺乏。
3.选择性IgA缺乏这是一组乳糜性腹泻的病因。
大多数选择性IgA缺乏者包括儿童,存有自身抗体,自身免疫性疾病则是这些人常见的。
4.选择性IgM缺乏也是产生多种感染疾患的原因。
(二)发病机制原发性免疫缺陷症是属于细胞免疫缺陷病,主要是胸腺发育不全,T细胞功能不足或是由于T细胞数少而导致B细胞功能缺陷。
如Di George综合征其病因是胚胎期中Ⅲ、Ⅳ咽囊发育障碍导致胸腺发育不良、甲状旁腺功能减退和人血管畸形等。
在临床免疫学检验上,表现为TH细胞数低下,抗体形成能力受到限制。
Nezelof综合征及核苷磷酸化酶缺陷为常染色体隐性遗传性疾病,致使胸腺发育不全和细胞免疫功能缺陷。
体液免疫缺陷病的直接表现是免疫球蛋白总量减少,或免疫球蛋白种类不全、或IgG的亚类不全。
也可以在总量上不明显减少,但某一种类免疫球蛋白突出减少。
Bruton免疫球蛋白缺乏症属于伴性型隐性遗传导致的免疫球蛋白减少。
其他类型免疫球蛋白减少,有的也可查到家族病史。
在免疫球蛋白缺乏的患者中,有的是B细胞功能不足,有的则是由于T细胞功能影响,或TH和TS细胞比例倒置。
【症状】1.X性连锁无丙种球蛋白血症(X-linked agammaglobulinemia) 临床上表现为:病人均为男性。
毛细管电泳对异常球蛋白的检测

Various questions can be answered with a serum protein electrophoresis
血清蛋白电泳可解决不少问题
Confirm a pathological diagnosis in association with other parameters: inflammation, hepatitis, cirrhotic or nephrotic profile
毛细管电泳对血清蛋白分成6组份
SEBIA CAPILLARYS PROTEIN
a-1 acid glycoprotein a-1 antitrypsin Haptoglobin a-2 macroglobulin
Gammaglobulins C3 complement Transferrin
Hemopexin
电泳是一种多目的检测方法,可对多种疾病提供重要的信息(肝硬化,多发性硬化症….)
There is currently no alternate assay for determining the immunoglobulin monoclonality, evidence of a bone myeloma
By Genevieve HENNACHE
Director of SEBIA Diagnostic Department
Protein Electrophoresis (蛋白电泳技术)
The electrophoresis assay is easy to operate, not very expensive, and can be performed routinely in most pathology laboratories to separate, quantify or identify proteins in different fluids (serum, urine, CSF…)
考试试卷复旦大学医学院儿科2005预防、基础A卷

复旦大学2004~2005学年第二学期期末考试试卷(A)(02级预防医学、基础医学)2005.6课程名称:儿科学课程代码:356.010.1.01 开课院系:儿科学系姓名:学号:专业:一.选择题(每题1分,共40分)A型题1.What is the most important clinical feature of nephritic syndrome?A. ProteinuriaB. EdemaC. HypertensionD. HypoalbuminemiaE. Hypercholesteolemia2. The range of serum natrium concentration in isonatremic dehydration should beA. 120~140mmol/LB. 130~160mmol/LC. 140~160mmol/LD. 140~150mmol/LE. 130~150mmol/L3. Which is main difference between dehydration of severe degree and moderate degree?A. poor skin resiliencyB. orbit pittingC. oliguria or anuriaD. metabolic acidosisE. peripheral circulatory failure4. What time is better for weaning in breast feeding baby?A. 4-5 months of ageB. 6-9 months of ageC. 10-12 months of ageD. 13-15 months of ageE. 18 months of age5. The ratio of Calcium and Phosphorus in breastmilk isA. 1:2B. 1.5:1C. 2:1D. 1.2:1E. 1.5:26. During fetal life, the earliest synthesized immunoglobin isA. IgMB. IgDC. IgGD. IgAE. IgE7. Very low birthweight infant is the newborn whose birth weight is less thanA. 2500gB. 2000gC. 1500gD. 1000gE. 800g8. The major manifestation of Tuberculous meningitis in children isA. A tense anterior fontanealB.ConvulsionC.StuporD.Cranial nerve palsiesE.Mood changes9. If the mother’s Rh blood type is CcDee and the fetus is CcDEe, then Rh incompatibility should beA. C antigenB. c antigenC. D antigenD. E antigenE. e antigen10. DTP (Diphtheria, tetanus, pertussis vaccine), Primary immunization should be takenA.Just one timeB.Once a month, two timesC.Once a month, three timesD.Once a week, two timesE.Once a week, three times11. Physiologic weight lower of a normal newborn will be recovered inA.1~3daysB.3~5 daysC. 5~7 daysD.7~10 daysE.10~14 days12. A healthy boy, one year and six months old, how much calorie and water should he require every day ?calorie (kj) /kg water(ml) /kgA. 418 (100 kcal) 100B. 460 (110 kcal) 100C. 418 (100 kcal) 110D. 418 (100 kcal) 125E. 925 (220 kcal) 15013. Intrauterine life comprises two stages: embryonic and fetal, the fetal period is usually considered to be:A.the end of 6th week of gestation to 40th week of gestationB.the end of 8th week of gestation to 40th week of gestationC.the end of 10 th week of gestation to 40 th week of gestationD.the end of 12 th week of gestation to 40 th week of gestationE.the end of 12 th week of gestation to 37 th week of gestation14. A newborn baby, gestational age 268 days, birth weight 2.45kg,height 47.5cm,head circumference 34cm,chest circumference 32cm, he isA.pre-term, large for gestational age babyB.full-term, appropriate for gestational age babyC.full-term, small for gestational age babyD.post-term,small for gestational age babyE.full-term,large for gestational age baby15. Which one of the following statement isn’t the clinical finding of febrile convulsionA.with a family history of seizuresB.often occur in neonatal periodC.associated with a rapidly rising temperatureD.less than 10 to 15 minutes episodeE.typical generalized seizures16. Physiologic hypogammaglobulinemia is commonly seen inA. Immediately after birthB. 3-4 months of ageC. 10-12 months of ageD. 1-2 years of ageE. 3 years of age17. Which one is the most common type of Tuberculosis in childrenA. Primary pulmonary tuberculosisB. Miliary tuberculosisC. Tuberculosis meningitisD. Tubeculosis lymphadenitisE. Tuberculous pleurisy18.Which one is the cyanotic type of congenital heart diseaseA. ventricular septal defectB. atrial septal defectC. tetralogy of FallotD. Patent ductus arteriosusE.pulmonary stenosis19. The major manifestations of acute glomerulonephritis areA.hypertension, hematuria, proteinuriaB.proteinuria, hypertensionC.edema, hypertension, hematuriaD.oliguria, edema, hypertension, hematuriaE.oliguria, edema, hematuria, hypercholesteolemia20. PPD test is a reliable diagnostic test for tuberculosis, an infected patient respounds positively of infectionA. immediatelyB. within 1-2 weekC. within 2-4 weekD. within 4-10 weekE. after 10 week21. 生理性体重下降的范围一般是出生体重的A.1%~5%B.3%~9%C.5%~10%D.10%~15%E.15%~20%22. 母乳的成分中哪项是错误的?A.初乳中含有分泌型IgAB.人乳中的碳水化合物主要是乳糖C.母乳中的脂肪以长链脂肪酸为主D.母乳对酸碱的缓冲力大E.母乳提供较多的酶23. 下列哪项不是新生儿窒息Apgar评分的内容?A. 皮肤颜色B. 心率C. 呼吸D. 肌张力E. 拥抱反射24. 下列哪一项与新生儿肺透明膜病的发病关系最不密切?A. 肺表面活性物质缺乏B. 早产儿C. 足月儿小样儿D. 糖尿病母亲婴儿E. 剖宫产25. 男孩,7岁,低热三天,两下肢及臀部有出血性皮疹,突出皮面,伴腹痛及便血一次,可能诊断为A.过敏性紫癜B.血小板减少性紫癜C.消化性溃疡D.流行性脑脊髓膜炎E.以上都不是26. 感染性腹泻最主要的病原是A.病毒B.致病性大肠杆菌C.空肠弯曲菌D.沙门氏菌E.真菌27. 婴儿腹泻,等渗脱水,第一天补液时应选用哪一种含钠液最恰当?A.1/2 张液B.1/3 张液C.2/3张液D. 等张液E.1/5张液28. 下列哪项不是腹泻病合并低钾血症的主要表现?A.腱反射迟钝或消失B.腹胀、肠鸣音减弱C.心音低钝D.心电图示ST段降低T波平坦E.心电图示T波高尖29. 鉴别金葡菌肺炎是否合并脓胸的最有意义的临床表现为A. 高热持续不退B. 中毒症状不断加重C. 呼吸困难突然加重D. 听诊两侧呼吸音消失E. 一侧胸壁叩诊呈浊音30. 呼吸道合胞病毒肺炎最突出的特点为A. 喘憋症状显著B.肺部功能残气量减少C.鼻翼煽动伴严重紫绀D.肺部广泛细湿罗音E.肺部罗音不明显31. 小儿肺炎的停止用药标准一般为A. 症状体征消失B. 症状体征消失3天C. 体温正常3天D. 治疗2周E. 治疗3~4周32. 先天性心血管畸形通常发生在哪个胚胎发育时期?A.2~8周B.2~3个月C.3~6个月D.6~9个月E.9个月以后33. 室间隔缺损的典型杂音是A.胸骨左缘2~3肋间Ⅲ级以上连续性杂音B.胸骨左缘2~3肋间Ⅲ级以上舒张期杂音C.胸骨左缘3~4肋间Ⅲ级以上收缩期杂音D.胸骨左缘3~4肋间Ⅲ级以上舒张期杂音E.以上都不是34. 下列哪项不符合房间隔缺损A.胸骨左缘第2、3肋间可听到Ⅱ~Ⅲ级收缩期杂音B.肺动脉瓣区第二心音增强或固定分裂C.胸部X线示肺血管影纤细D.心电图示不完全性右束枝传导阻滞E.右心房血氧含量高于上、下腔静脉血氧含量35. 下列哪一项不是急性肾炎的主要临床表现?A.水肿B.血尿C.蛋白尿D.高脂血症E.高血压36. 肾病综合征最根本的病理生理变化是A.大量蛋白尿B.低蛋白血症C.高脂血症D.血尿E.水肿37.小儿下尿路感染抗生素治疗的疗程一般为A.3~5天B.5~7天C.7~10天D.10~14天E.1个月38. 营养性缺铁性贫血铁缺少期,下列哪一指标已出现异常?A.血红蛋白B.血清铁蛋白C.红细胞游离原卟啉D.血清铁E.骨髓可染铁39. 单纯性高热惊厥有以下特点,但除外下列哪项?A.有明显的遗传倾向B.发作前后神经系统无异常C.惊厥多为部分性发作D.惊厥持续多在10分钟以内E.有年龄特点40. 心跳骤停的临床诊断依据是,但除外:A. 心音消失,大动脉搏动消失,血压测不到B.意识丧失C.皮肤发绀D.呼吸停止E.心电图显示心室颤动或心电活动消失二.问答题(每题15分,共60分)1. 试述新生儿肺透明膜病的诊断与防治。
2例儿童先天性粒细胞减少症的基因诊断
2例儿童先天性粒细胞减少症的基因诊断乔明吟;刘炜;李彦格;毛彦娜;管玉洁【摘要】目的提高对先天性粒细胞减少症(CN)的认识,通过检测基因突变类型,探讨其分子学发病机制.方法使用DNA直接测序法分析患儿全基因组,分析其有意义的突变类型,查找数据库进行相应序列对比,再进行一代测序(Sanger法)验证.结果先证者一存在G6PC3基因存在双重杂合子突变:IVS3+1G>T及c.915(E6):缺失G,先证者二存在CXCR4基因突变:c.1004(exon1)-c.1005(exon1)缺失AA.结论 2例先天性粒细胞减少症的患儿均存在异常的基因突变,基因诊断对先天性粒细胞减少症的诊断有重大意义,对临床研究及治疗提供依据.【期刊名称】《临床荟萃》【年(卷),期】2018(033)004【总页数】5页(P314-318)【关键词】中性粒细胞减少;基因;CXCR4基因;G6PC3基因【作者】乔明吟;刘炜;李彦格;毛彦娜;管玉洁【作者单位】郑州儿童医院血液肿瘤科,河南郑州 450000;郑州儿童医院血液肿瘤科,河南郑州 450000;郑州儿童医院血液肿瘤科,河南郑州 450000;郑州儿童医院血液肿瘤科,河南郑州 450000;郑州儿童医院血液肿瘤科,河南郑州 450000【正文语种】中文【中图分类】R557.3粒细胞减少症是临床上常见的一种疾病,其中大部分病人与感染、化疗、自身免疫性疾病等因素有关,即获得性粒细胞减少。
而重型先天性中性粒细胞减少症(severe congenital neutropenia, SCN),此类疾病目前我们的认识还比较少,它是原发性免疫缺陷病中的一类。
最早由瑞典儿科医师Kostmann在1956年报道。
SCN是以外周血成熟中性粒细胞缺乏为主要症状的一类异质性疾病,并且已被证实SCN与多种基因突变有关[1]。
近年来越来越多的报道基因诊断在临床诊疗过程中发挥着重要作用[2]。
本文先后对2例粒细胞减少患儿进行基因测序,发现分别存在CXCR4基因突变及G6PC3基因突变,本文意在揭示其基因类型与临床表现的关系,为本病的临床研究及基因诊断提供依据。
血液病专业英语词汇

Aabnormal hemoglobinopathy异常血红蛋白病acanthocytosis刺状红细胞增多acute arrest of hemopoiesis急性造血停滞acute histocytic leukemia急性组织细胞白血病acute leukemia急性白血病acute lymphoblastic leukemia,ALL急性淋巴细胞白血病acute monocytic leukemia,AMOL急性单核细胞白血病acute myeloblastic leukemia,AML急性粒细胞白血病acute myelo-monocytic leukemia,AMMOL急性粒-单核细胞白血病acute non-lymphocytic leukemia,ANLL急性非淋巴细胞白血病acute plasma cell leukemia急性浆细胞白血病acute promyelocytic leukemia,APL急性早幼粒细胞白血病acute stem cell leakenia急性干细胞白血病acute transformation of chronic myelocytic leukemia慢性粒细胞白血病急变acute unclassified leukemia急性未定型白血病acute undifferentiated cell leukemia急性未分化细胞白血病afibrinogenemia纤维蛋白原缺乏血症agranulocytosis粒细胞缺乏angio-immunoblastic lymphadenopathy血管免疫母细胞淋巴结病aplastic anemia再生障碍性贫血autoimmune hemolytic anemia自身免疫性溶血性贫血Bbasophilia嗜碱粒细胞增多basophilic cell leukemia嗜碱粒细胞白血病Bernard-Soulier syndrome巨血小板综合征blast crisis of chronic myelocytic leukemia慢性粒细胞白血病原始细胞危象Burkitt lymphoma伯基特淋巴瘤Ccentral nervous system leukemia中枢神经系统白血病chloroma绿色瘤chronic lymphocytic leukemia,CLL慢性淋巴细胞白血病chronic myelocytic leukemia,chronic granulocytic leukemia,CML,CGL慢性粒细胞白血病congenital aplastic anemia先天性再生障碍性贫血congenital non-spherocytic hemolytic anemia先天性非球形红细胞溶血性贫血Ddisseminated inravascular coagulation,DIC弥散性血管内凝血dysfibrinogenemia异常纤维蛋白原血症Eechinocytosis棘状红细胞增多eosinopenia嗜酸粒细胞减少eosinophilia嗜酸粒细胞增多eosinophilic cell leukemia嗜酸粒细胞白血病eosinophilic granuloma嗜酸细胞肉芽肿erythrocytosis红细胞增多症erythroleukemia,EL红白血病Ffactor Ⅴdeficiency因子Ⅴ缺乏〔症〕factor ⅤII deficiency因子Ⅶ缺乏〔症〕factor Ⅹdeficiency因子Ⅹ缺乏〔症〕factor ⅩII deficiency因子ⅩII缺乏〔症〕factor ⅩIII deficiency因子ⅩIII缺乏〔症〕factor Ⅺdeficiency因子Ⅺ缺乏〔症〕Fanconi anemia范科尼贫血favism蚕豆病fibrinolysis syndrome纤维蛋白溶解综合征GGaucher disease戈谢病(曾用名“高雪病”)glucose-6-phosphate dehydrogenase deficiency,G6PD葡萄糖-6-磷酸脱氢酶缺乏症(又称“6-磷酸葡萄糖脱氢酶缺乏症”)graft versus host disease,GVHD移植物抗宿主病granulocytosis粒细胞增多Hhairy cell leukemia,HCL多毛细胞白血病Hand-Schǖller-Christian disease汉-许-克病heavy chain disease重链病hemachromatosis血色病hematology 血液学hematopathy血液病hemoglobinopathy血红蛋白病hemoglobinuria,PNHhemolytic anemia of newborn新生儿溶血性贫血hemolytic anemia溶血性贫血hemolytic disease of newborn新生儿溶血症hemolytic uremic syndrome溶血尿毒症综合征hemophilia A血友病Ahemophilia B血友病Bhemosiderosis含铁血黄素沉着症hereditary elliptocytosis遗传性椭圆形红细胞增多症hereditary hemorrhagic telangiectasia遗传性出血性毛细血管扩张症hereditary spherocytosis遗传性球形红细胞增多症Hodgkin disease霍奇金病(又称“何杰金病”)hypergammaglobulinemia高丙球蛋白血症hypersplenism脾功能亢进hyperviscosity syndrome高粘滞综合征hypogammaglobulinemia低丙球蛋白血症Iidiopathic thrombocytopenic purpura,ITP特发性血小板减少性紫癜immune hemolytic anemia免疫性溶血性贫血immunologic thrombocytopenic purpura,ITP免疫性血小板减少性紫癜infectious lymphocytosis传染性淋巴细胞增多症infectious mononucleosis传染性单核细胞增多症iron deficiency anemia缺铁性贫血KKaposi sarcoma卡波西肉瘤LLetterer-Siwe disease莱特勒-西韦病leucocytopenia,leukopenia白细胞减少leukemoid reaction类白血病反应leukocytosis白细胞增多lymphocytosis淋巴细胞增多lymphoma cell leukemia淋巴瘤细胞白血病lymphopenia 淋巴细胞减少lymphoproliferative diseases淋巴细胞增生性疾病Mmacroglobulinemia巨球蛋白血症malignant histocytosis恶性组织细胞病malignant lymphoma恶性淋巴瘤march hemoglobinuria行军性血红蛋白尿症megakaryocytic leukemia巨核细胞白血病megaloblastic anemia巨幼细胞贫血meningeal leukemia脑膜白血病methemoglobinemia高铁血红蛋白血症microangropathic hemolytic anemia微血管病性溶血性贫血monocytosis单核细胞增多multiple myeloma,MM多发性骨髓瘤mycosis fungoides蕈样肉芽肿病myelodysplastic syndrome,MDS骨髓增生异常综合征myelofibrosis骨髓纤维化〔症〕myelopathic anemia,myelophthisic anemia骨髓病性贫血myeloproliferative diseases骨髓增生性疾病myelosclerosis骨髓硬化症NNiemann-Pick disease尼曼-皮克病non-Hodgkin lymphom非霍奇金淋巴瘤(又称“非何杰金淋巴瘤”)a Pparoxysmal cold hemoglobinuria阵发性冷性血红蛋白尿症paroxysmal nocturnal阵发性睡眠性血红蛋白尿症pernicious anemia恶性贫血plasmocytoma浆细胞瘤polycythemia vera,PV真性红细胞增多症porphyria卟啉病preleukemia白血病前期prolymphocytic leukemia,PLL幼淋巴细胞白血病prothrombin deficiency凝血酶原缺乏〔症〕pure red cell aplasia纯红细胞再生障碍pyruvate kinase deficiency 丙酮酸激酶缺乏症Rreactive histocytosis反应性组织细胞增多reactive plasmacytosis反应性浆细胞增多Ssickle cell anemia镰状细胞贫血sideroblastic anemia铁粒幼细胞贫血stomatocytosis口形红细胞增多sulfhemoglobinemia硫化血红蛋白血症Tthalassemia珠蛋白生成障碍性贫血(又称“地中海贫血”)thrombocytasthenia血小板无力症thrombocytopathy血小板病thrombocytopenia血小板减少thrombocytosis血小板增多thrombotic thrombocytopenic purpura, TTP血栓性血小板减少性紫癜Vvitamin K deficiency维生素K缺乏〔症〕von Willebrand disease血管性血友病。
原发性免疫缺陷病 (Primary immunodeficiencies)

机体免疫系统
特 异性
细胞免疫
体液免疫
非特异性
吞噬系统
补体 系统
T细胞
B细胞
MC/M⊙单核/巨噬细胞
PMN中性粒细胞
补 体
趋化、吞噬、杀菌
细胞因子 亚群失衡 免疫球蛋白
B细胞量减少
放大 吞噬
IL IFN TFN IgG IgM IgA IgD IgE
小儿非特异性免疫( Non-specific immunity)
原发性免疫缺陷病PID 与 继发性免疫缺陷病SID 的区别(Difference)
单基因缺失、功能受损 严重、不可逆(Beyond retrieve)、终身性(For life)、需免疫重建
(Immune reconstitution therapy)方可恢复正常。
发病早、程度重、并发 肿瘤(Tumour)和自身免 疫性疾病(Autoimmune disease)机会多。
原发性免疫缺陷病的分类(Classify)
⑵细胞免疫缺陷病 (10%) (cellular immunity deficiency) 先天性胸腺发育不全(DiGeorge 综合征)
伴核苷磷酸化酶(Adenosine deaminase)缺乏的免疫缺 陷症 ⑶联合免疫缺陷病 (20%) (combined immunity deficiency)
(2%)
诊 断 篇
免疫缺陷病的诊断思路(Diagnose approach)
是否有免疫缺陷?
加强临
原发性或继发性?(Primary or secondary 床) 思维 持续性或暂时性?(durative or transient) 能力!
免疫系统缺陷的部位与程度?(Place or
哈尔西·泰勒非冷藏冻抗性焕发说明书

97811C (Rev. C - 4/05)Halsey Taylor Owners ManualNon-Refrigerated Freeze Resistant FountainsIMPORTANTALL SERVICE TO BE PERFORMED BY AN AUTHORIZED SERVICE PERSONOVLEBPFROVLSBPFR OVLSEBPFRIMPORTANT! INSTALLER PLEASE NOTE.THE GROUNDING OF ELECTRICAL EQUIPMENT SUCH AS TELEPHONE, COMPUTERS, ETC. TO WATER LINES IS A COMMON PROCEDURE. THIS GROUNDING MAY BE IN THE BUILDING OR MAY OCCUR AWAY FROM THE BUILDING. THIS GROUNDING CAN CAUSE ELECTRICAL FEEDBACK INTO A FOUNTAIN, CREATING AN ELECTROLYSIS WHICH CAUSES A METALLIC TASTE OR AN INCREASE IN THE METAL CONTENT OF THE WATER. THIS CONDITION IS AVOIDABLE BY USING THE PROPER MATERIALS AS INDICATED. ANY DRAIN FITTINGS PROVIDED BY THE INSTALLER SHOULD BE MADE OF PLASTIC TO ELECTRICALLY ISOLATE THE FOUNTAIN FROM THE BUILDING PLUMBING SYSTEM.OVL - EBPFR/SBPFR/SEBPFR COOLER INSTALLATIONThe freeze resistant package must be mounted on an interior wall in a heated area. The room temperature of the interior heated area must be 50° F (10° C) or higher. The freeze resistant package may be surface or re-cessed mounted. If recess mounted the surface of the cover must be flush with the interior wall surface. The package is furnished with screws for mounting the cover to the box. If the box is recess mounted, do not fasten the top and bottom of the cover to the box. Use the holes on the front only.1.Wall should already be framed for the fountain using the rough-in dimensions shown in Fig's. 1, 2, 3, 4, 5, or6. Shown dimensions pertain to installation location (framing must support up to 150 Lbs. weight for singlefountain and 300 Lbs. for dual fountains). These dimensions are required for compliance with ANSI Standard A117.1 and ADA (Framing shown for reference).2. Attach wall plate assembly to wall as shown in Fig's. 3, 4, or 6 using 5/16" x 2" long bolts and flat washers(not provided). Tighten securely, (Fastener must match wall type, i.e. lag screws for wood studs, bolts and anchors for masonry construction).3. Install back panel. Place the upper edge of the panel above hanger on the wall. Slide the panel down until itengages the hanger. Be sure back panel is firmly engaged before releasing it.4. Remove bottom access panel from fountain basin and save screws. Install the fountain to the back paneland wall using (4) 5/16" x 3/4" long bolts and washers (provided) thru holes in back panel. A washer is used on the bottom two (2) holes only. Tighten securely.5. Assemble the operating cable to the fountain bracket. (Fountain should be mounted to exterior wall)Create a loop in the cable and thread the free end of the cable through the wall into the freeze resistant box.The adjustment nuts should be in the middle of threaded area on the operating cable. See Figure 7.6.Connect free end of operating cable to the valve-operating bracket. The end of the cables must be recessedinto the indents on the pivot brackets. Remove cable free play by adjusting the jam nuts on the ends of the operating cable. See Figure 7.7.Connect water line from fountain bubbler into freeze resistant box. The connection to the box uses a quickconnect water fitting. Position the water line, in the fountain, to drain back into interior mounted box. Any water left standing, in the exterior line, can freeze . See Fig. 13.To insert tubing, push tube straight into fitting until it reaches a positive stop. To remove tubing from the fittings, relieve water pressure, push in on dark gray collar while pulling out on the tubing. See Figure 12. 8.Connect drain and water supply lines to the freeze resistant fountain. Refer to Figure 1, 2, 3, 4, 5 or 6 forcomponent positions. Inline strainer must be used on the inlet water line. See Fig. 11.Start-up1.Turn on building water supply and check all connections for leaks. Repair as required.2.Stream height is factory set at 45-50 PSI. If stream height (See Fig. 14) needs to be changed adjust theregulator in the freeze resistant package. Clockwise adjustment raises stream height, counter clockwise adjustment will lower stream.3.Adjust operating cable as required. Cable system should have a minimal amount of free play to allow forproper valve operation. If the system is too tight the valve will stay in the on position creating constant water flow. Too much free play will result in non-operation of the valve with the push-buttons.4.Note: Water from the drain back tube in the freeze resistant package, will continue to run while the valve isactuated.5.After cable system is adjusted properly stuff flexible insulation into any openings between the outside walland the interior box.6.Recheck all connections. If all connections are leak free replace cover(s) on the freeze resistant box(es)and fountain(s).97811C (Rev. C - 4/05)PAGE 297811C (Rev. C - 4/05)PAGE 3T O P V I E W R O U G H -I N F O R O V L S B P F R /O V L E B P F RF IG . 1F IG . 297811C (Rev. C - 4/05)PAGE 4F IG . 3L E G E N D :A = 1-1/4" O .D . W a s t e T u b e (T r a p A n d E l b o w P r o v i d e d )B = 1/4" O .D . F r e e z e R e s i s t a n t C a b l e C = 1/4" O .D . P l a s t i c T u b e (B u b b l e r W a t e r S u p p l y )D = 1/4" (6m m ) D I A . H o l e s F o r M o u n t i n g P l a t e T o W a l lR O U G H -I N F O R O V L E B P FR97811C (Rev. C - 4/05)PAGE 5F I G . 4R O U G H -I N F O R O V L S B P F RL E G E N D :A = 1-1/4" O .D . W a s t e T u b e (T r a p A n d E l b o w P r o v i d e d )B = 1/4" O .D . F r e e z e R e s i s t a n t C a b l e C = 1/4" O .D . P l a s t i c T u b e (B u b b l e r W a t e r S u p p l y )D = 1/4" (6m m ) D I A . H o l e s F o r M o u n t i n g P l a t eT o W a l l97811C (Rev. C - 4/05)PAGE 6T O P V I E W R O U G H -I N F O R O V L S E B P F RF IG . 597811C (Rev. C - 4/05)PAGE 7F I G . 6R O U G H -I N F O R O V L S E B P F RL E G E N D :A = 1-1/4" O .D . W a s t e T u b e (T r a p A n d E l b o w P r o v i d e d )B = 1/4" O .D . F r e e z e R e s i s t a n t C a b l e C = 1/4" O .D . P l a s t i c T u b e (B u b b l e r W a t e r S u p p l y )D = 1/4" (6m m ) D I A . H o l e s F o r M o u n t i n g P l a t e T o W a ll97811C (Rev. C - 4/05)PAGE 8CABLE SHEATH ADJUSTMENTTo Increase Free PlayTo Reduce Free PlayFIG. 7FIG. 8FIG. 997811C (Rev. C - 4/05)PAGE 9OPERATION OF QUICK CONNECT FITTINGSSIMPLY PUSH IN TUBE TO ATTACHTUBE IS SECURED IN POSITIONPUSH IN COLLET TO RELEASE TUBEPUSHING TUBE IN BEFORE PULLING IT OUT HELPS TORELEASE TUBE.1/4" O.D. TUBE WATER INLETNOTE: WATER FLOW DIRECTIONBUILDING WATERINLET3/8" O.D. UNPLATED COPPER TUBE CONNECT COLD WATER SUPPLYSERVICE STOP (NOT FURNISHED)FIG. 10FIG. 12FIG. 11SEE FIG. 8SEE FIG. 997811C (Rev. C - 4/05)PAGE 10FIG. 13308209311718129222114, 15122271319 6 72526242328 81141631052897811C (Rev. C - 4/05)PAGE 11DESCRIPTION 27688C 27689C 50595C 51546C 10032274056016027050864010157054056051575C 11034622055010163745155016163730864015008C 10002334056016157080855045663C 75672C 27006C 27000C 11262754389055919C 45662C 550011385500113927945C 27946C 40045C 4020600056092C 70425C 50198C 51468C 22797C22799C26958C28120C28121C28168C45730C75541C11157724389012345678910111213141516171819202122232425262728293031NS NS NSP ART NO.Bottom Cover (OVL-S)Bottom Cover (OVL-E)Bushing - Snap Bubbler Gasket - Black Strainer Plate Drain Gasket Packing Ring Lock Nut - 1-1/2"-11-1/2Friction Ring Drain Plug Bubbler Nipple Assembly Gasket - Neoprene Slip Nut Push Button Sleeve Screw - Cap Basin Basin Liner Screw # 10-24 x 1/2" Long Push Button Extension Push Button Arm (OVL-S-FR)Arm (OVL-E-FR)Basin Bracket Basin Pivot Bracket Nut - Hex (unplated)Retainer Tube - Poly (cut to length)Rod - Pivot Bushing Snap Bumper - Reg. Valve Assy Back Panel (OVL-EBP)Back Panel (OVL-SBP)Back Panel (OVL-SEBP)Wall Plate Assembly - OVL-SBP Wall Plate Assembly - OVL-SEBP Wall Plate Assembly - OVL-EBP Drain Tube Washer-Flat .339/.359ID Steel Screw-Mach. 5/16-18 x 3/4" Long ITEM NO.PARTS LIST2222 CAMDEN COURTOAK BROOK, IL 60523PRINTED IN U.S.A.TROUBLE SHOOTING AND MAINTENANCEOrifice Assy: Mineral deposits on orifice can cause water flow to spurt or not regulate. Mineral deposits may be removed from the orifice with a small round file or small diameter wire. CAUTION: DO NOT file or cut orifice material.Stream Regulator: If orifice is clean, regulate flow as in“STREAM HEIGHT ADJUSTMENT” instructions on pg 2. If replacement is necessary, see parts list for correct regulator part number.Actuation of Quick Connect Water Fittings: Fountain is pro vided with lead-free connectors which utilize an o-ring water seal. To remove tubing from the fitting, relieve water pressure, push in on the gray collar while pulling on the tubing.(see Fig.12) To insert tubing, push tube straight into fitting until it reaches a positive stop, approximately 3/4".FIG. 14。
原发性免疫缺陷病
我国常见PID
(一)联合免疫缺陷病 T和B细胞均有缺陷,细胞免疫和抗体反应均缺陷,外周血 淋巴细胞减少,以T细胞为明显,婴儿期致死性感染
1. 严重联合免疫缺陷病(severe combined immunodeficiency,SCID)
(2)T和B细胞均缺如(T-B-SCID):为常染色体隐性遗传。 ① 重组活化基因(RAG-1/-2)缺陷 ② 腺苷脱氨酶(ADA) ③ 网状发育不良:淋巴干细胞髓前体细胞发育障碍 ④ DCLREIC(Artemis)、DNAPKcs缺陷
plasma
IgG
IgA
B
plasma
IgA
IgE
B
plasma
IgE
小儿免疫系统发育特点
1. 单核/巨噬细胞(MC/MΦ)
新生儿MΦ 发育已完善,由于缺乏辅助因子,使其趋化、黏 附、吞噬、杀菌、产生G-CSF、IL、INF-γ和抗原提呈能力 较成人差。
2. 中性粒细胞(PMN)
胚胎34周PMN趋化、吞噬和杀菌功能基本成熟,生后头2 周上述功能暂时性低下,补体水平低下,缺乏趋化因子, 导致中性粒细胞功能不足。
新生儿各补体成分低于成人,生后3~6个月补体浓度和活 性接近成人。
6. 其他免疫分子
血浆甘露聚糖结合蛋白(MBP)水平比成人低,在婴儿阶 段抗体发育不全发挥作用。未成熟儿儿生后10~20周, 才达足月新生儿水平。
PID发病率
• 仅美国有50万病例,每年新增1万病例 • 其总发病率以活产婴的发病数计,约为1:10000 • 我国每年2500万新生儿中,将会新增加2500例
differentiation) 体液免疫:B淋巴细胞
BM ?
SC SL
THYRUM Epi CD3+
血液病专业英语词汇

Aabnormal hemoglobinopathy异常血红蛋白病acanthocytosis刺状红细胞增多acute arrest of hemopoiesis急性造血停滞acute histocytic leukemia急性组织细胞白血病acute leukemia急性白血病acute lymphoblastic leukemia,ALL急性淋巴细胞白血病acute monocytic leukemia,AMOL急性单核细胞白血病acute myeloblastic leukemia,AML急性粒细胞白血病acute myelo-monocytic leukemia,AMMOL急性粒-单核细胞白血病acute non-lymphocytic leukemia,ANLL急性非淋巴细胞白血病acute plasma cell leukemia急性浆细胞白血病acute promyelocytic leukemia,APL急性早幼粒细胞白血病acute stem cell leakenia急性干细胞白血病acute transformation of chronic myelocytic leukemia慢性粒细胞白血病急变acute unclassified leukemia急性未定型白血病acute undifferentiated cell leukemia急性未分化细胞白血病afibrinogenemia纤维蛋白原缺乏血症agranulocytosis粒细胞缺乏angio-immunoblastic lymphadenopathy血管免疫母细胞淋巴结病aplastic anemia再生障碍性贫血autoimmune hemolytic anemia自身免疫性溶血性贫血Bbasophilia嗜碱粒细胞增多basophilic cell leukemia嗜碱粒细胞白血病Bernard-Soulier syndrome巨血小板综合征blast crisis of chronic myelocytic leukemia慢性粒细胞白血病原始细胞危象Burkitt lymphoma伯基特淋巴瘤Ccentral nervous system leukemia中枢神经系统白血病chloroma绿色瘤chronic lymphocytic leukemia,CLL慢性淋巴细胞白血病chronic myelocytic leukemia,chronic granulocytic leukemia,CML,CGL慢性粒细胞白血病congenital aplastic anemia先天性再生障碍性贫血congenital non-spherocytic hemolytic anemia先天性非球形红细胞溶血性贫血Ddisseminated inravascular coagulation,DIC弥散性血管内凝血dysfibrinogenemia异常纤维蛋白原血症Eechinocytosis棘状红细胞增多eosinopenia嗜酸粒细胞减少eosinophilia嗜酸粒细胞增多eosinophilic cell leukemia嗜酸粒细胞白血病eosinophilic granuloma嗜酸细胞肉芽肿erythrocytosis红细胞增多症erythroleukemia,EL红白血病Ffactor Ⅴdeficiency因子Ⅴ缺乏〔症〕factor ⅤII deficiency因子Ⅶ缺乏〔症〕factor Ⅹdeficiency因子Ⅹ缺乏〔症〕factor ⅩII deficiency因子ⅩII缺乏〔症〕factor ⅩIII deficiency因子ⅩIII缺乏〔症〕factor Ⅺdeficiency因子Ⅺ缺乏〔症〕Fanconi anemia范科尼贫血favism蚕豆病fibrinolysis syndrome纤维蛋白溶解综合征GGaucher disease戈谢病(曾用名“高雪病”)glucose-6-phosphate dehydrogenase deficiency,G6PD葡萄糖-6-磷酸脱氢酶缺乏症(又称“6-磷酸葡萄糖脱氢酶缺乏症”)graft versus host disease,GVHD移植物抗宿主病granulocytosis粒细胞增多Hhairy cell leukemia,HCL多毛细胞白血病Hand-Schǖller-Christian disease汉-许-克病heavy chain disease重链病hemachromatosis血色病hematology 血液学hematopathy血液病hemoglobinopathy血红蛋白病hemoglobinuria,PNHhemolytic anemia of newborn新生儿溶血性贫血hemolytic anemia溶血性贫血hemolytic disease of newborn新生儿溶血症hemolytic uremic syndrome溶血尿毒症综合征hemophilia A血友病Ahemophilia B血友病Bhemosiderosis含铁血黄素沉着症hereditary elliptocytosis遗传性椭圆形红细胞增多症hereditary hemorrhagic telangiectasia遗传性出血性毛细血管扩张症hereditary spherocytosis遗传性球形红细胞增多症Hodgkin disease霍奇金病(又称“何杰金病”)hypergammaglobulinemia高丙球蛋白血症hypersplenism脾功能亢进hyperviscosity syndrome高粘滞综合征hypogammaglobulinemia低丙球蛋白血症Iidiopathic thrombocytopenic purpura,ITP特发性血小板减少性紫癜immune hemolytic anemia免疫性溶血性贫血immunologic thrombocytopenic purpura,ITP免疫性血小板减少性紫癜infectious lymphocytosis传染性淋巴细胞增多症infectious mononucleosis传染性单核细胞增多症iron deficiency anemia缺铁性贫血KKaposi sarcoma卡波西肉瘤LLetterer-Siwe disease莱特勒-西韦病leucocytopenia,leukopenia白细胞减少leukemoid reaction类白血病反应leukocytosis白细胞增多lymphocytosis淋巴细胞增多lymphoma cell leukemia淋巴瘤细胞白血病lymphopenia 淋巴细胞减少lymphoproliferative diseases淋巴细胞增生性疾病Mmacroglobulinemia巨球蛋白血症malignant histocytosis恶性组织细胞病malignant lymphoma恶性淋巴瘤march hemoglobinuria行军性血红蛋白尿症megakaryocytic leukemia巨核细胞白血病megaloblastic anemia巨幼细胞贫血meningeal leukemia脑膜白血病methemoglobinemia高铁血红蛋白血症microangropathic hemolytic anemia微血管病性溶血性贫血monocytosis单核细胞增多multiple myeloma,MM多发性骨髓瘤mycosis fungoides蕈样肉芽肿病myelodysplastic syndrome,MDS骨髓增生异常综合征myelofibrosis骨髓纤维化〔症〕myelopathic anemia,myelophthisic anemia骨髓病性贫血myeloproliferative diseases骨髓增生性疾病myelosclerosis骨髓硬化症NNiemann-Pick disease尼曼-皮克病non-Hodgkin lymphom非霍奇金淋巴瘤(又称“非何杰金淋巴瘤”)a Pparoxysmal cold hemoglobinuria阵发性冷性血红蛋白尿症paroxysmal nocturnal阵发性睡眠性血红蛋白尿症pernicious anemia恶性贫血plasmocytoma浆细胞瘤polycythemia vera,PV真性红细胞增多症porphyria卟啉病preleukemia白血病前期prolymphocytic leukemia,PLL幼淋巴细胞白血病prothrombin deficiency凝血酶原缺乏〔症〕pure red cell aplasia纯红细胞再生障碍pyruvate kinase deficiency 丙酮酸激酶缺乏症Rreactive histocytosis反应性组织细胞增多reactive plasmacytosis反应性浆细胞增多Ssickle cell anemia镰状细胞贫血sideroblastic anemia铁粒幼细胞贫血stomatocytosis口形红细胞增多sulfhemoglobinemia硫化血红蛋白血症Tthalassemia珠蛋白生成障碍性贫血(又称“地中海贫血”)thrombocytasthenia血小板无力症thrombocytopathy血小板病thrombocytopenia血小板减少thrombocytosis血小板增多thrombotic thrombocytopenic purpura, TTP血栓性血小板减少性紫癜Vvitamin K deficiency维生素K缺乏〔症〕von Willebrand disease血管性血友病. ..。
bovine gamma-globulin 分子量
bovine gamma-globulin 分子量法国生物学家Brachet和英国生物学家Hammersen于1932年发现,当新鲜的晒干黄疸猪血清在高盐条件下析出时,可得到一种Globulin。
它被称为γ-S-Globulin,后来又被称为γ-Globulin。
这种蛋白质是由220个氨基酸组成的多肽链,其中含有15个半胱氨酸(cysteine)并且没有碳酸酐基。
它的分子量约为146 kDa(千道尔顿),具体数值会受到具体实验方法和测量条件的影响。
牛源γ-球蛋白是一种来源于牛血清的γ-球蛋白,牛血清是一种天然的高分子混合物,包含多种不同的蛋白质。
γ-球蛋白是其中最丰富的成分之一,它在血浆中占总蛋白质的15-25%。
γ-球蛋白的分子量可以通过多种方法进行测定。
一种常用的方法是凝胶过滤法(gel filtration)或者凝胶电泳法(gel electrophoresis)。
在凝胶过滤法中,蛋白质溶液被滤过尺寸合适的凝胶柱,不同分子量的蛋白质会以不同速度通过凝胶柱,从而分离出不同大小的蛋白质。
通过测量不同蛋白质的迁移速度,可以计算出γ-球蛋白的分子量。
另外一种常用的方法是质谱分析(mass spectrometry),质谱分析可以直接测量蛋白质中各个氨基酸残基的质量,从而得到蛋白质的分子量。
这种方法通常需要先将蛋白质进行裂解和鉴定,然后使用质谱分析仪器进行测量。
除了实验方法外,还可以通过基因组学和蛋白质组学的方法进行分子量的预测。
通过测量物种基因组中相应的基因或者利用已知的蛋白质序列,可以利用计算机算法预测蛋白质的分子量。
γ-球蛋白在免疫系统中起着重要的作用。
它主要由免疫球蛋白IgG组成,具有抗体的功能。
γ-球蛋白能够识别并结合特定的抗原,从而触发免疫反应。
在牛源γ-球蛋白中,IgG是主要的成分,它可以通过免疫电泳等方法进行分离和纯化。
γ-球蛋白有很多重要的应用,包括医学和生物技术领域。
在医学方面,γ-球蛋白可以用于治疗免疫缺陷病和自身免疫性疾病。
ESD序贯APC治疗食管高级别上皮内瘤变致胃底多发溃疡和穿孔1例
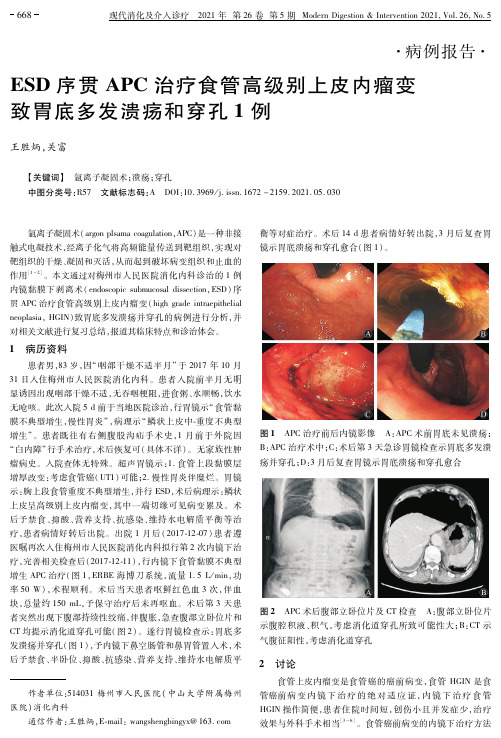
图 1 APC治疗前后内镜影像 A:APC术前胃底未见溃疡; B:APC治疗术中;C:术后第 3天急诊胃镜检查示胃底多发溃 疡并穿孔;D:3月后复查胃镜示胃底溃疡和穿孔愈合
图 2 APC术后腹部立卧位片及 CT检查 A:腹部立卧位片 示腹腔积液、积气,考虑消化道穿孔所致可能性大;B:CT示 气腹征阳性,考虑消化道穿孔
[6] JovenMH,PalalayMP,SonidoCY.Casereportandliterature reviewonGood′ssyndrome,aform ofacquiredimmunodeficiency associatedwith thymomas[J].HawaiiJMed PublicHealth, 2013,72(2):5662.
(收稿日期:20210220) (本文编辑:罗永华)
櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒櫒
(上接第 667页)
[5] RawatA,DhirV,GuptaA,etal.Good′ssyndromepresenting withrecurrentgiardiasis”[J].JClinImmunol,2014,34(7): 751752.
[7] MancusoA,GentiluomoM,VangeliM,etal.Diarrheaassole presentationofGood′ssyndromemimickingCrohn′sdisease[J].
ClinImmunol,2013,147(1):910. [8] VerneGN,Amann ST, CosgroveC, etal. Chronicdiarrhea
杂志,2016,33(1):318. [4] PrasadGA,WuTT,WigleDA,etal.EndoscopicandSurgical
Specific Immunodeficiencies概述
These infants have recurrent pyogenic infections of the lungs, sinuses, and bones with such organisms as pneumococcus, haemophilus, and streptococcus.
Sometimes there is an associated increased frequency of infection. The disorder results from a delay in the onset of Ig synthesis despite normal numbers of B cells. T helper cells may be reduced. Premature infants are especially at risk because of lower levels of transplacental IgG at birth. The disorder is not familial.
Treatment
Bone marrow transplantation has been successful. Some success has been achieved with fetal thymus transplants. The severity of the heart disease often determines the eventual prognosis. Partial deficiency is compatible with prolonged survival.
Abnormalities of chromosome 22q (eg, deletion or monosomy) can be identified in 90% of cases. There seems to be an interruption of normal development of pharyngeal pouch structures near the 8th wk of gestation.
内科学_各论_疾病:婴儿期短暂性低丙球蛋白血症_课件模板
内科学疾病部分:婴儿期短暂性低丙球蛋白血症>>>
治疗:
平很低,有必要补充γ-球蛋白,所用剂 量同先天性性联无γ-球蛋白血症。
(二)预后 这一缺陷可得到恢复,预后良好。
内科学疾病部分:婴儿期短暂性低丙球蛋白血症>>>
预防: 婴儿期短暂性低丙球蛋白血症预防_婴儿 期短暂性低丙球蛋白血症怎么调理
加强护理和营养以提高患者的抵抗力 和免疫力。预防感染。
内科学疾病部分:婴儿期短暂性低丙球蛋白血症>>>
科室: 血液科。
内科学疾病部分:婴儿期短暂性低丙球蛋白血症>>>
简介:
婴儿期短暂性低丙球蛋白血症(transient hypogammaglobulinemia of infancy)也 称新生儿暂时性低γ-球蛋白血症。属于 原发性体液免疫缺陷病。
内科学疾病部分:婴儿期短暂性低丙球蛋白血症>>>
病因:
婴儿期短暂性低丙球蛋白血症原因_由什 么原因引起婴儿期短暂性低丙球蛋白血症
(一)发病原因 正常婴儿在出生后3个月时,血中由母体 获得的90%γ-球蛋白被缓慢地分解代谢而 逐渐消失。从出生起开始合成IgM抗体, 水平迅速上升,至l岁时可达正常人的75% 水平。生后第3周开始合成IgA,至
内科学疾病部分:婴儿期短暂性低丙球蛋白血症>>>
相关疾病:
异常γ-球蛋白血症、先天性性联无γ-球 蛋白血症、继发性单克隆免疫球蛋白病、 原发性单克隆免疫球蛋白病、原发性巨球 蛋白血症。
谢谢!
内科学各论疾病部分 婴儿期短暂性低丙球蛋
白血症 内容课件模板
内科学疾病部分:婴儿期短暂性低丙球蛋白血症>>>
抗体免疫缺陷病有哪些症状?
抗体免疫缺陷病有哪些症状?*导读:本文向您详细介绍抗体免疫缺陷病症状,尤其是抗体免疫缺陷病的早期症状,抗体免疫缺陷病有什么表现?得了抗体免疫缺陷病会怎样?以及抗体免疫缺陷病有哪些并发病症,抗体免疫缺陷病还会引起哪些疾病等方面内容。
……*抗体免疫缺陷病常见症状:脾大、白细胞减少、恶性贫血、反复感染*一、症状1.X性连锁无丙种球蛋白血症(X-linked agammaglobulinemia) 临床上表现为:病人均为男性。
生长发育正常。
多数病例出生后6~9个月内表现正常,1~2岁后开始反复感染。
常见病原菌为葡萄球菌、肺炎球菌、链球菌、嗜血流感杆菌和脑膜炎球菌。
可发生支气管炎、支气管扩张、肺炎、中耳炎、脑膜炎和疖肿等。
部分病人可发生非化脓性关节炎,主要累及大关节;并容易罹患ECHO病毒脑脊髓炎。
ECHO病毒广泛播散,可致慢性肌炎、亚临床型肝炎、心肌炎以及肘膝关节屈曲挛缩。
胃肠道表现不多见。
2.常见变异型免疫缺陷病(common variable immunodeficiency,CVID) 临床上表现为:男女均可发病,通常6岁以后开始有症状,20~30岁明显加重。
主要表现是病人反复感染。
常有慢性腹泻、乳糖耐受不良、吸收不良和蛋白质丢失性肠病。
贾第鞭毛虫感染是腹泻的常见原因。
部分病人胃酸减少,其中半数缺乏内因子,此外尚有脾大以及贫血和白细胞减少、血小板减少。
本病自身免疫性疾病发病率较高,如溶血性贫血、血小板减少性紫癜、甲状腺炎和类风湿性关节炎。
3.选择性IgA缺乏症(selective IgA deficiency) 临床上表现为:多数病人无症状,偶尔在检查时发现。
有的则有明显症状,多在10岁内出现,均因IgA缺乏,呼吸道、胃肠道、泌尿道等部位局部免疫功能降低,容易发生感染,也可发生过敏反应。
此外,类风湿性关节炎、系统性红斑狼疮、甲状腺炎与恶性贫血等自身免疫疾病发生率增高。
4.婴儿暂时性低丙球蛋白血症(infantile transient hypogammaglobulinemia) 临床上表现为:男女均可发病,一般病程持续6~18个月。
Good综合征诊治一例
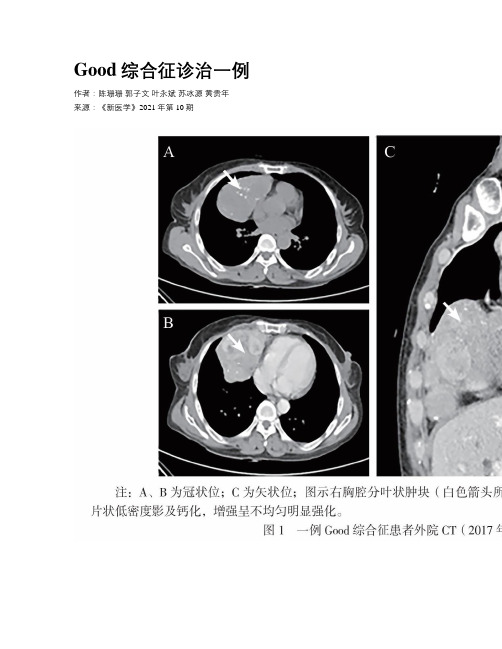
Good综合征诊治一例作者:陈珊珊郭子文叶永斌苏冰源黄贵年来源:《新医学》2021年第10期【摘要】 Good综合征(伴胸腺瘤的免疫缺陷症)是一种成人免疫缺陷病,特点是合并胸腺瘤及低丙种球蛋白血症。
该病有细胞和体液免疫双重缺陷,患者常表现为反复感染。
该文报道1例62岁AB型胸腺瘤女性患者,反复细菌、真菌和病毒感染,血清Ig低下,B淋巴细胞缺如、CD4+ T淋巴细胞下降、CD4+/CD8+ T淋巴细胞比值下降,诊断为Good综合征。
该患者同时有粒细胞缺乏、慢性病性贫血,进一步骨髓宏基因组测序发现KIT与ARID1A基因突变,予补充Ig及抗感染治疗,患者症状好转出院。
随访患者仍有Ig下降,予定时复查血常规、Ig,并适时补充Ig。
Good综合征相对罕见,临床表现复杂,容易延误诊断,临床医师需引起重视。
【关键词】 Good综合征;伴胸腺瘤的免疫缺陷症;免疫缺陷;胸腺瘤;粒细胞缺乏Diagnosis and treatment of Good’s syndrome: a case report Chen Shanshan, Guo Ziwen, Ye Yongbin, Su Bingyuan, Huang Guinian. Division of Hematology, Affiliated Zhongshan Hospital, Sun Yat-sen University,Zhongshan 528403, ChinaCorresponding author, Huang Guinian, E-mail:***************【Abstract】Good’s syndrome (immunodeficiency with thymoma) is an adult immunodeficiency disease characterized by thymoma complicated with hypogammaglobulinemia. Due to dual deficiency of cellular and humoral immune functions, patients constantly present with recurrent infection. This article reported one 62-year-old female patient with type AB thymoma presenting with recurrent bacterial, fungal and viral infection, low serum immunoglobulin, B lymphocyte deficiency, decreased CD4+ T cells and CD4+/CD8+ T ratio, which were consistent with the diagnosis of Good’s syndrome. Meanwhile, the patient was complicated with agranulocytosis and anemia of chronic disease. Furthermore, bone marrow genetic detection revealed mutations in KIT and ARID1A genes. The patient was discharged after immunoglobulin supplement and anti-infection therapy. During follow-up, serum immunoglobulin level was declined. Routine blood test was performed on a regular basis. Immunoglobulin supplement was given when necessary. Good’s syndrome is relatively rare in clinical practice. It is likely to delay the diagnosis due to complex clinical manifestations, which is worthy of widespread attention from clinicians.【Key words】Good’s syndrome; Immunodeficiency with thymoma; Imm unodeficiency; Thymoma;AgranulocytosisGood综合征(伴胸腺瘤的免疫缺陷症)是罕见的成年发病的原发性免疫缺陷病,以胸腺瘤、低丙种球蛋白血症、CD4+/CD8+ T淋巴细胞比值下降(倒置)、低外周血B细胞和伴有CD4+ T淋巴细胞免疫缺陷为特点[1]。
激活PI3K-δ综合征合并关节炎1例并文献复习
激活PI3K-δ综合征合并关节炎1例并文献复习唐红霞;尹薇【摘要】目的探讨PIK3CD基因突变所致激活PI3K-δ综合征(APDS)合并关节炎的临床特点及诊断和治疗.方法回顾分析1例确诊APDS合并关节炎患儿的临床资料,并复习相关文献.结果患儿,男,4岁10个月,因肝、脾、淋巴结肿大,咳嗽伴发热就诊.既往有反复呼吸道感染病史.IgG< 0.07 g/L,IgA<0.26 g/L,IgM 1.78g/L.CD19+B细胞和CD4+T细胞数量减少及CD4+/CD8+比例倒置,考虑为原发免疫缺陷病.基因检测示PIK3CD基因c.G3061:p.E1021K点突变,为杂合突变,确诊APDS.住院期间患儿出现双膝关节肿胀,左侧明显,不能行走.给予静脉注射免疫球蛋白及口服萘普生后关节肿痛明显缓解,能独立行走.结论 APDS患儿可能会出现关节炎.【期刊名称】《临床儿科杂志》【年(卷),期】2018(036)011【总页数】4页(P858-861)【关键词】原发免疫缺陷病;激活PI3K-δ综合征;关节炎;基因【作者】唐红霞;尹薇【作者单位】华中科技大学同济医学院附属武汉儿童医院风湿免疫科湖北武汉430016;华中科技大学同济医学院附属武汉儿童医院风湿免疫科湖北武汉430016【正文语种】中文激活PI3K-δ综合征(activated phosphoinositide 3-kinase δ syndrome,APDS)是一种原发联合免疫缺陷病,通过常染色体显性遗传,是PIK3CD基因发生获得性功能突变,导致其编码的p110δ活性增强,信号通路PI3K-AKT-mTOR 过度激活,临床主要表现为反复呼吸道感染、肝脾、淋巴结肿大、对EB病毒及巨细胞病毒高度易感,并且易发生自身免疫系统疾病,其免疫特点和临床表现高度易变[1-4],且国内外报道不多。
现报告1例通过临床和免疫表型分析,以及基因检测确诊的APDS患儿的临床资料,以提高临床医师的认识。
goods综合征诊断标准
goods综合征诊断标准英文回答:Diagnosis of Good's syndrome requires the presence of both thymoma and hypogammaglobulinemia. Thymoma is a tumor of the thymus gland, which is an important part of the immune system. Hypogammaglobulinemia refers to a deficiency of gamma globulins, which are a type of antibody that helps the body fight infections.In addition to these two main criteria, patients with Good's syndrome often present with recurrent infections, particularly of the respiratory tract, as well as other autoimmune conditions such as autoimmune cytopenias and inflammatory bowel disease. The combination of these symptoms along with the presence of thymoma and hypogammaglobulinemia is highly suggestive of Good's syndrome.Laboratory tests play a crucial role in the diagnosisof Good's syndrome. This includes measuring the levels of different types of immunoglobulins, particularly IgG, IgA, and IgM. A marked reduction in these levels, especially in the presence of recurrent infections, can raise suspicion for Good's syndrome. Additionally, a biopsy of the thymoma may be performed to confirm its presence.It is important to differentiate Good's syndrome from other causes of hypogammaglobulinemia, such as common variable immunodeficiency (CVID) or X-linked agammaglobulinemia. This can be done through a thorough evaluation of the patient's medical history, physical examination, and laboratory tests.In summary, the diagnosis of Good's syndrome requires the presence of thymoma and hypogammaglobulinemia, along with a history of recurrent infections and possibly other autoimmune conditions. Laboratory tests and biopsy of the thymoma are essential for confirming the diagnosis.中文回答:Good综合征的诊断需要同时具备胸腺瘤和低免疫球蛋白血症的特征。