LPR corelation
门诊以咽部异物感为主诉患者咽喉反流性疾病的流行病学调查
门诊以咽部异物感为主诉患者咽喉反流性疾病的流行病学调查目的:調查笔者所在医院耳鼻咽喉科门诊以咽部异物感为主诉患者咽喉反流性疾病(LPRD)的患病率及其相关因素。
方法:对首诊于笔者所在科门诊共5 023例患者进行调查,对其中以咽部异物感为第一主诉的365例首诊患者进行问卷调查。
采用反流症状指数(RSI)量表简化汉字版及反流体征指数(RFS)量表简体中文版进行调查,并分析各相关因素。
结果:以咽部异物感为第一主诉患者占门诊就诊患者比例为7.27%。
其中LPRD患者187例,占咽部异物感患者51.23%,占门诊所有患者3.72%。
不同年龄段、不同职业及不同病程患病率比较,差异均有统计学意义(字2=23.905、25.065、69.445,P<0.01)。
而不同性别组、体重指数组患病率比较,差异均无统计学意义(字2=0.017、1.632,P>0.05)。
咽部异物感与胃灼热、胸痛、胃痛及持续清嗓有相关性(r=0.418、0.383);与红斑/充血及弥漫性喉水肿相关(r=0.608、0.576)。
结论:年龄、职业和病程与LPRD 相关;性别、体重指数与LPRD无关;咽部异物感与胃灼热、胸痛、胃痛及持续清嗓以及红斑/充血及弥漫性喉水肿关系最大。
[Abstract] Objective:To assess the prevalence of laryngopharyngeal reflux disease(LPRD)and its associated factors among patients presented to the otolaryngology clinic in our hospital with foreign body sensation in pharynx.Method:A total of 5 023 patients were surveyed during their first visit to our clinics.Among them,365 patients presented with foreign body sensation in pharynx as the first chief complaint,and their reflux symptoms were assessed using simplified Chinese version of reflux symptom index(RSI)and reflux finding score(RFS)questionnaires.The associated factors were analyzed.Result:Patients presented with foreign body sensation in pharynx as the first chief complaint constitue was 7.27% of all patients surveyed in the clinics.There were 187 patients who had LPRD,51.23% among patients with foreign body sensation in pharynx and 3.72% among all patients surveyed.There were significant differences in terms of age,occupation,and duration of the symptoms in patients with and without LPRD(字2=23.905,25.065,69.445,P<0.01).The differences in gender and BMI were not statistically significant(字2=0.017,1.632,P>0.05).The sensation of foreign body in the pharynx was associated with pharynx and heartburn/chest pain/stomachache,frequent throat clearing (r=0.418,0.383),associated with erythema/hyperemia and diffuse larynx edema (r=0.608,0.576).Conclusion:Age,occupation,and duration of symptoms has significant correlation with LPRD.Gender or BMI were not correlated with LPRD.The foreign body sensation in pharynx has highest correlation with heartburn/chest pain/stomachache,frequent throat clearing,erythema/hyperaemia,and diffuse laryngeal edema.[Key words] Paraesthesia pharynges;Laryngopharyngeal reflux;Signs and symptoms;Epidemiology以咽部异物感为主诉而就诊于耳鼻咽喉科的患者占门诊患者的比例很高。
LPR有关知识介绍

报价行的类型, 在原有的全国性银行基 础上增加城市商业银行、 农村商业银行、外资银 行和民营银行,共计 家。
(二) 的今生
取数方式的变化
(二) 的今生
增加期限品种
由 年期一个期限品 种基础上,增加 年期以上的 期限品种,这样完善 期限 结构,也能为银行发放住房 抵押贷款等长期贷款的利率 定价提供参考。
消费下滑
(一)经济下行压力加大
全球降息潮和人民币汇率破“ ”
(一)经济下行压力加大
全球降息潮和人民币汇率破“ ”
汇率破 带来的负面影响: 楼市价格有可能带来一定的负面冲击 导致部分居民消费能力下降 对我国企业尤其是进口企业的生产经营将带来一定负面影响 对中国 股带来一定的负面影响
(二)央行不愿意降低基准利率
宽松的货币政策,叠加放松的金融监管以及金融产品创新,共同影响 非标准债券融资成本
(三)市场利率传导不畅
各类利率走势情况
(三)市场利率传导不畅
各类利率走势情况
(三)市场利率传导不畅
各类利率走势情况
(三)市场利率传导不畅
各类利率走势情况
(三)市场利率传导不畅
银行的业务分类
债券 债券市场业务是高度市场化的,其融资来自于市场,而投资也面向
(二) 的今生
公开市场操作利率为什么选择
市场化的质押式回购利率( )和同业拆借利率(
),容易
受到季节性因素或者风险事件影响,变动不居,如果 按照 或
进行加点,会造成报价利率和贷款实际利率的失真,也加大了银行报价和贷
款管理的难度。而且他们是市场化的产品,不受央行控制。
中期借贷便利( )利率是是央行于 年 月创立的货币政策工 具,发挥中期政策利率的作用。作为利率走廊期限结构的中段,已有较大市 场规模,能够根据经济形势和政策目标灵活调整,央行也完全可以通过调整 其利率水平来影响全市场利率形态,具有一定的市场化基准利率特征。
单词统计特性在情感词自动抽取和商品评论分类中的作用
*
要:单词的统计特征在自然语言处理中具有广泛的应用。针对统计特征对关键词抽取和文本分类精确度的影响,
分析了八种常见的统计特征,通过情感词抽取和商品评论分类,研究统计特征在情感分析领域中的作用。情感词提取 实验的结果表明,通过结合统计特征与词性,情感词提取的准确率能够达到 76.4%,显著高于基于统计特征或单词词 性的情感词提取算法。商品评论分类的测试结果表明,与传统的基于单词的文本情感分类相比,基于统计特征的商品 评论分类的准确率提高了 10.8%。利用八种统计特征构造文本向量空间模型,替代基于单词构造文本向量空间模型的 方法,能够降低文本向量的维度,具有隐形语义空间 (LSA/SVD)的压缩效果,在保证分类结果准确率的前提下有效降 低了算法的复杂度,能够替代传统的向量空间模型。 关键词:统计特征;情感词提取;商品评论分类 中图分类号:TP391 doi: 10.3969/j.issn.1001-3695.2017.09.0913
——————————
基金项目:国家教育部人文社会科学研究一般项目基金资助项目(15YJA740054) 作者简介:韩彤晖(1991-) ,男,山东滨州人,硕士研究生,主要研究方向为自然语言处理(kevinsdj@) ;杨东强(1970-) ,男,副教授,博士, 主要研究方向为人工智能;马宏伟(1969-) ,男,教授,博士,主要研究方向为计算机网络应用.
————————————————————————————————————————————————
单词统计特性在情感词自动抽取和商品评论分类中的作用
作者 机构 基金项目 预排期卷 摘要 韩彤晖,杨东强,马宏伟 山东建筑大学 计算机科学与技术学院 国家教育部人文社会科学研究一般项目基金资助项目(15YJA740054) 《计算机应用研究》 2019 年第 36 卷第 3 期 单词的统计特征在自然语言处理中具有广泛的应用。针对统计特征对关键词抽取和文本分类 精确度的影响,分析了八种常见的统计特征,通过情感词抽取和商品评论分类,研究统计特 征在情感分析领域中的作用。情感词提取实验的结果表明,通过结合统计特征与词性,情感 词提取的准确率能够达到 76.4%,显著高于基于统计特征或单词词性的情感词提取算法。商 品评论分类的测试结果表明,与传统的基于单词的文本情感分类相比,基于统计特征的商品 评论分类的准确率提高了 10.8%。利用八种统计特征构造文本向量空间模型,替代基于单词 构造文本向量空间模型的方法, 能够降低文本向量的维度, 具有隐形语义空间(LSA/SVD)的压 缩效果,在保证分类结果准确率的前提下有效降低了算法的复杂度,能够替代传统的向量空 间模型。 关键词 作者简介 统计特征;情感词提取;商品评论分类 韩 彤 晖 ( 1991- ) ,男,山东滨州人,硕士研究生,主要研究方向为自然语言处理 (kevinsdj@) ;杨东强(1970-) ,男,副教授,博士,主要研究方向为人工智能;马 宏伟(1969-) ,男,教授,博士,主要研究方向为计算机网络应用. 中图分类号 访问地址 发布日期 引用格式 TP391 /article/02-2019-03-010.html 2018 年 4 月 17 日 韩彤晖 , 杨东强 , 马宏伟 . 单词统计特性在情感词自动抽取和商品评论分类中的作用 [J/OL]. 2019, 36(3). [2018-04-17]. /article/02-2019-03-010.html.
correlation判定ok的标准
在撰写这篇文章前,我们首先需要明确 correlation(相关性)作为一个统计学术语的定义。
Correlation是用来衡量两个变量之间的关联程度的统计指标,它可以帮助我们了解两个变量是如何一起变化的。
在统计学中,correlation通常用来衡量两个变量之间的线性关系。
而correlation判定ok的标准则是我们在进行统计分析和数据处理时应该非常关注的问题。
我们需要明确的是correlation判定ok的标准应该基于相关系数的大小而定,这是一个最基本的判断。
相关系数的取值范围为[-1, 1],当相关系数为1时,表示两个变量之间存在完全的正相关关系;当相关系数为-1时,表示两个变量之间存在完全的负相关关系;而当相关系数为0时,表示两个变量之间不存在线性关系。
我们可以根据相关系数的大小来判断correlation是否ok。
为了更全面地评估correlation是否ok,我们还需要考虑P值的大小。
在统计学中,P值是用来衡量我们观察到的样本数据与假设之间的一致性的指标。
一般来说,当P值小于0.05时,意味着我们有足够的证据来拒绝原假设,即两个变量之间存在相关性;而当P值大于0.05时,我们则无法拒绝原假设,即无法确定变量之间是否存在相关性。
P值的大小也是判断correlation是否ok的重要依据之一。
我们还需要考虑样本量的大小。
在实际统计分析中,样本量的大小会对相关系数的稳定性产生影响。
当样本量较小时,计算出的相关系数可能会受到较大的波动,而当样本量较大时,计算出的相关系数则更加稳定。
为了更准确地判断correlation是否ok,我们需要根据实际情况来考虑样本量的大小。
correlation判定ok的标准应该是基于相关系数的大小、P值的大小和样本量的大小来综合评估。
只有当相关系数较大且P值小于0.05,并且样本量足够大时,我们才能确定correlation是ok的。
这样的判定标准能够更全面、更准确地评估变量之间的相关关系,从而帮助我们做出合理的统计分析和数据处理。
lpr通俗理解
lpr通俗理解
今天,LPR(活期基准利率)在我国金融领域引起了许多关注。
目前,我国的LPR正处于一种重要的转折点与传统的贷款基准利率(LPR)有较大差异。
因此,金融机构和客户应在一定程度上识别LPR,使其能够有效地应对汇率变动,提高金融管理水平。
本文旨在通过简要介绍LPR,使读者更好地理解LPR及其对金融市场的影响,从而更好地管理金融风险。
首先,LPR是指金融机构向客户放贷时使用的基准利率。
它是一种由中国人民银行决定的浮动利率,其利率水平与宏观经济状况及市场情绪紧密相关,是金融市场的主要参照点。
此外,它还可以用来衡量市场价格,帮助金融机构预测未来债券收益率水平。
其次,LPR的变动会直接影响贷款利率的变化。
LPR的变动将会对客户的贷款有很大的影响。
如果LPR上调,客户贷款利率也会随之上调。
因此,LPR的变动将会带来贷款成本的变化,直接影响到客户的财务状况。
此外,LPR对金融市场也有很大的影响。
由于LPR是金融市场上主要参照点,LPR的变动将会引起金融市场中各种金融产品价格的变化,从而影响金融活动,甚至影响宏观经济。
最后,LPR在金融风险控制上也起着重要作用。
由于LPR的变动会直接影响到贷款利率和金融市场价格,客户和金融机构应及时关注LPR的变动情况,以有效地管理金融风险。
以上就是LPR的通俗理解。
LPR是一种宏观经济指标,是金融市
场上的主要参照点,也是金融风险管理的重要工具。
客户和金融机构应及时关注LPR的变动情况,以有效地管理金融风险。
lpr利息计算方法
lpr利息计算方法 贷款利息计算是金融领域中非常重要的一项工作。
近年来,中国央行推出了基于LPR (贷款市场报价利率)的新型贷款利率定价机制,这一机制为贷款利息计算带来了全新的方法和规则。
本文将详细介绍LPR利息计算方法,并通过实例说明其具体应用。
一、了解LPR1.1 LPR概念 LPR(Loan Prime Rate)是中国人民银行发布的贷款市场报价利率,是银行对贷款利率的报价。
它根据市场供求情况和LPR形成机制确定,是商业银行对外报价的重要参考基准。
1.2 LPR的意义 LPR作为新型的贷款利率定价基准,取代了以前的贷款基准利率制度,更加市场化和透明化。
它具有更高的时效性和灵活性,能够更好地反映市场利率的变动,为金融机构和消费者提供更加公平、合理的利率环境。
2.1 LPR计算公式LPR利息计算方法一般采用以下公式:贷款利息= 贷款金额× LPR × 贷款期限2.2 贷款金额 贷款金额是指借款人获得的贷款总额,一般与贷款合同中约定的金额一致。
在LPR利息计算中,贷款金额是计算利息的重要变量。
2.3 LPR LPR是银行确定的贷款利率水平,在LPR定价机制下,银行会根据借款人的信用状况和市场上的供求情况,浮动调整LPR水平。
因此,在利息计算中,需要根据实际LPR水平来确定具体的利率。
2.4 贷款期限 贷款期限是指借款人与银行签订的贷款合同约定的还款期限,通常以月为单位。
贷款期限的长短直接影响利息计算的金额。
三、利息计算实例 为了更好地理解LPR利息计算方法的应用,下面给出一个实例。
假设小王向银行贷款10万元人民币,贷款期限为12个月,LPR为4.5%。
按照LPR利息计算方法,可以计算出小王需要支付的利息: 贷款利息= 10万元× 4.5% × 12 = 5,400元。
这样,小王需要根据合同约定,按照每月450元的利息支付金额来偿还贷款利息。
LPR利息计算方法是充分利用LPR这一新型贷款利率定价机制进行利息计算的方法。
LPR值趋势
LPR值趋势LPR(Liquidity Preference Ratio)是指银行体系中商业银行对现金持有的偏好程度,也可解释为商业银行倾向于持有流动性(现金、存款准备金等)资产而非非流动(贷款等)资产的倾向。
LPR值反映了商业银行对流动性的需求和倾向,对宏观经济环境和政策也具有一定的参考价值。
LPR值是受多种因素影响的,其中最重要的因素是货币政策、经济增长和金融市场情绪。
随着宏观政策的调整和经济形势的变化,LPR值也会相应发生变化。
下面将从这几个方面来分析LPR值的趋势。
首先,货币政策是影响LPR值的关键因素之一。
央行通过调整货币政策来控制货币供应量和银行间利率,从而影响商业银行的LPR值。
当央行采取紧缩的货币政策时,提高存款准备金率、上调存款利率等措施会使银行倾向于持有更多的现金和流动性资产,LPR值也会相应上升。
相反,当央行采取宽松的货币政策时,降低存款准备金率、降低存款利率等措施会使银行更倾向于放贷,LPR值则会下降。
其次,经济增长也会影响LPR值的趋势。
经济增长带来的商业信心和市场需求增加,通常会促使银行倾向于提供更多的贷款,从而降低LPR值。
而经济衰退或不确定性加大,则可能会导致银行增加现金储备,提高LPR值。
最后,金融市场情绪的变化也会对LPR值产生影响。
当金融市场出现风险偏好较高的情况时,投资者更倾向于将资金流入股市、债市等,而非存款。
这种情况下,商业银行可能会面临流动性压力,倾向于增加储备现金,提高LPR值。
相反,当金融市场风险偏好降低,投资者更倾向于将资金投入低风险资产,商业银行的流动性压力减轻,LPR值可能会下降。
综上所述,LPR值的趋势受到货币政策、经济增长和金融市场情绪的影响。
当央行采取紧缩货币政策、经济增长放缓或金融市场出现风险偏好下降时,LPR值通常会上升;而央行采取宽松货币政策、经济增长加速或金融市场风险偏好增加时,LPR值通常会下降。
因此,监测和分析LPR值的趋势对于了解银行体系的流动性状况,以及对宏观经济政策的制定都具有重要意义。
correlation

correlationCorrelationIntroductionCorrelation is a statistical measure that determines the degree to which two variables are related to each other. It is an important concept in many fields, including statistics, economics, social sciences, and healthcare. In this document, we will explore the concept of correlation, its types, and its significance in various applications.What is Correlation?Correlation quantifies the statistical relationship between two variables. It measures how changes in one variable correspond to changes in another variable. Correlation is typically represented by the correlation coefficient, which ranges from -1 to +1. A positive correlation indicates a direct relationship, while a negative correlation indicates an inverse relationship. A correlation coefficient close to zero indicates a weak or no relationship between the variables.Types of CorrelationThere are three main types of correlation: positive correlation, negative correlation, and zero correlation.1. Positive Correlation: When two variables increase or decrease together, they are said to have a positive correlation. For example, there is a positive correlation between the amount of study time and test scores. As the study time increases, the test scores also tend to increase. The correlation coefficient for a positive correlation ranges from 0 to +1.2. Negative Correlation: In contrast to a positive correlation, a negative correlation exists when one variable increases while the other decreases. For instance, there is a negative correlation between the number of hours spent watching TV and academic performance. As the hours spent watching TV increase, the academic performance tends to decrease. The correlation coefficient for a negative correlation ranges from 0 to -1.3. Zero Correlation: Zero correlation, as the name suggests, implies no relationship between the variables. The changes in one variable do not correspond to any changes in the othervariable. When the correlation coefficient is close to zero, it indicates a weak or no correlation.Significance of CorrelationCorrelation has several practical applications in different fields.1. Statistics: Correlation analysis is used to determine the strength and direction of the relationship between variables. It helps statisticians to understand the patterns and trends in data. Correlation coefficients are widely used in regression analysis and predictive modeling.2. Economics: In economics, correlation analysis helps to identify relationships between different economic variables such as inflation and unemployment rates, interest rates and investment, or GDP and consumer spending. Understanding these relationships is essential for making informed economic decisions.3. Social Sciences: Correlation is used in social sciences to study various phenomena, such as the relationship between education and income, crime rates and poverty, or healthbehaviors and disease outcomes. Correlation can provide insights into social trends and patterns.4. Healthcare: Correlation plays a crucial role in healthcare research. It helps to identify risk factors, assess treatment effectiveness, and understand the relationship between lifestyle choices and health outcomes. For example, studying the correlation between smoking and lung cancer can help healthcare professionals develop effective prevention strategies.ConclusionCorrelation is a powerful statistical tool that measures the relationship between two variables. It helps us understand how changes in one variable relate to changes in another variable. By analyzing correlation coefficients, we can determine the strength and direction of the relationship. Correlation has wide-ranging applications in statistics, economics, social sciences, healthcare, and other fields. Understanding correlation is essential for making informed decisions and drawing meaningful conclusions from data.。
lpr利率名词解释
lpr利率名词解释
LPR是“贷款市场报价利率”的缩写,是中国银行间市场交易商协会发布的贷款基准利率。
它是中国金融市场上的一种利率定价基准,也是中国改革利率形成机制的一部分。
LPR是以贷款利率为基准,由人民银行和中国银行间市场交易商协会共同制定并公布的。
LPR的形成机制是由人民银行和市场利率形成机制相结合的产物,旨在更好地反映市场供求关系和市场利率变动情况,以更加市场化的方式来确定贷款利率。
LPR的发布频率为每月一次,其定价机制主要由贷款市场报价利率和市场利率形成机制共同决定。
LPR的发布对于银行贷款利率的形成具有指导作用,也为金融市场的稳定运行提供了更加透明和市场化的利率定价机制。
总的来说,LPR是中国金融市场上的一种贷款利率基准,通过市场化的方式形成,具有更好地反映市场供求关系和市场利率变动情况的特点,对于中国金融市场的稳定运行和金融改革具有重要意义。
简析LPR政策执行的影响及对策lpr对金融机构的影响
简析LPR政策(zhèngcè)执行的影响及对策lpr对金融机构的影响2022年8月16日,中国人民银行发布关于中国人民银行决定改革完善(wánshàn)贷款市场报价利率(lpr)形成机制的公告〔2022〕第15号公告(gōnggào)〔以下简称(jiǎnchēng)公告〕,决定(juédìng)改革完善贷款市场报价利率〔lpr〕形成机制,自2022年8月20日起,授权全国银行间同业拆借中心于每月20日公布贷款市场报价利率,并要求自即日起,各银行应在新发放的贷款中主要参考贷款市场报价利率定价,并在浮动利率贷款合同中采用贷款市场报价利率作为定价基准。
一、定价机制改革是什么意思?〔一〕什么是lpr?所谓lpr〔loanprimerate〕,是指金融机构对其最优质客户执行的贷款利率,其他贷款利率可根据借款人的信用情况,考虑抵押、期限、利率浮动方式和类型等要素,在lpr根底上加减点确定。
lpr机制创设于在2022年10月,央行在2022年7月全面放开金融机构贷款利率管制,随后创设了lpr。
由10家大中型银行每天报价,并经银行间市场发布,为市场提供一个最优贷款利率供行业定价参考。
〔二〕lpr利率和基准利率有什么区别?1、法定基准利率:我们日常生活中常常听到的降息、加息,都是以这个基准利率为调整标准,法定基准利率,还分为存款基准利率跟贷款基准利率。
目前我们采用央行2022年10月24日最新基准利率:商业贷款:1年以内(含1年),年利率4.35%、1年到5年(含5年),年利率4.75%、5年以上,年利率4.90%公积金:5年以内(含5年),2.75%、5年以上,3.25%存贷款基准利率是央行制定的,给商业银行的贷款指导性利率,并非实际的贷款利率,而实际贷款利率,一般会高于法定基准利率。
2、lpr利率:改革后的lpr由18家银行共同报价产生,计算方法为去掉一个最高价和一个最低价,最后算术平均得出,每月20日重新报价计算,可以简单解读为,这是一个市场化利率的意思。
浅谈LPR

浅谈LPR作者:诸懿青来源:《现代经济信息》2020年第09期摘要:我国原有LPR集中报价和发布机制运行七年后,中国人民银行于2019年8月16日公布了改革完善后的贷款市场报价利率(LPR)形成机制。
本文深入对比了LPR机制改革前后的变化,深入阐述了此次LPR改革在利率市场化进程中的重要意义,对完善人民币利率衍生产品市场的积极作用,以及对国内商业银行和企业等市场参与者的重要影响,并给出了相应建议。
关键词:LPR;利率市场化;衍生产品一、什么是LIaRLPR即贷款基础利率,是英文Loan Prime Rate的首字母缩写,指的是银行对该行最优质客户提供的贷款利率价格。
我国LPR的集中报价和发布机制最早在2013年10月25日正式运行。
为进一步深化利率市场化改革,提高利率的传导效率,降低实体经济融资成本,中国人民银行于2019年8月16日发布第15号公告,公布了改革完善后的贷款市场报价利率(LPR)形成机制(以下称“LPR新机制”)。
此次LPR改革,在七个方面体现出“新”的变化。
(一)新的报价原则央行要求各报价行真正按照自身对最优质客户执行的贷款利率报价,充分体现市场化报价的形成原则。
(二)新的形成方式原来各报价行大多以央行贷款基准利率为参考,报出的LPR与央行贷款基准利率高度相关,未及时反映市场利率变动。
改革后的LPR按照公开市场操作利率加点的方式报价,加点幅度由各报价行根据自身情况确定,市场化程度明显提高。
(三)新的期限品种原来只有1年期报价,新机制增加了5年期以上报价,为银行长期限贷款定价提供参考。
(四)新的报价行在原有10家全国性银行(工商银行、农业银行、中国银行、建设银行、交通银行、中信银行、浦发银行、兴业银行、招商银行和民生银行)基础上扩大到18家(新增加的8家行为西安银行、台州银行、上海农商银行、广东顺德农商行、渣打中国、花旗银行、深圳前海微众银行、浙江网商银行),更进一步增强了LPR报价的代表性。
造纸词汇——精选推荐

制浆工艺impregnator预浸器refiner盘磨机preheater预加热器pre-steaming bin预蒸仓heat recovery热回收thickner浓缩机Twin-Roll Press双辊挤浆机Thickening浓缩HC-bleaching高浓漂白Reject chest渣浆池Reject refiner渣浆池Screw drainer螺旋卸料器Plug screw feeder料塞螺旋喂料器Primary screen一段筛Stator plate定盘Standpipe立管Flat zone平盘区Blow line喷放管线Pressure cyclone压力旋风分离器Gravity重力Impurity杂质Extractive抽取物Manganese锰Equalizing bin匀料仓Rotomixer转子混合器Bleaching liquor漂液Disc screen盘筛Level indicator液位指示器Metering screw计量螺旋Gyratory screen旋筛Reclaim卸料Screw feeder螺旋喂料器Distallition蒸馏Shive纤维束Barometric leg水腿Filtrate滤液White water chest白水池Dewater脱水Pressurized preheating常压预加热Single-disc refiner单盘盘磨机Latency潜能Preheater加热器Double-disc refiner双盘盘磨机Load split荷载分配Coarse fiber粗纤维Reject浆渣Single-stage refining一段磨浆Pilot scale中试厂Energy consumption能耗Tear strength撕裂强度Retention time滞留时间Overpressure超压Lamella薄片Fiber wall纤维墙Compressed steam压缩蒸汽Soft fiber软纤维Moisture content水份Softness柔软度Toughness硬度Tensile index抗张指数Tear index撕裂指数Light scattering光散射系数Bulk松厚度Yield得率Standard newsprint 标准新闻纸Improved newsprint改良新闻纸Saturated steam饱和蒸汽Suspended solid悬浮物Effluent treatment污水处理Dew point露点Screen basket筛鼓Fastening bolt 坚固螺栓Stuffing box填料箱Inspection hatch检查孔Hub轮毂spherical thrust roller bearing球墨止推滚柱轴承fastening screw紧固螺丝friction force摩擦力valve tray 填料方式bubble cap汽泡盖sieve tray滤网盘downcomer下导管weir堰板volatile component挥发元素Gap clearance盘隙Refining intensity磨浆强度Centrifugal force离心力Drag force拖拉力Residence time停留时间Long fiber content长纤维含量Conical refiner椎形盘磨机Breaker bar破碎棒Hydrogen peroxide过氧化氢Sodium hydroxide氢氧化钠Sodium silicate硅酸钠Sodium sulfite亚硫酸钠Hydrosulfite次硫酸钠transducer传感器thermometer温度计neutral point中性点dynamic balance动态平衡Short circuit current短回路电流The related vocabulary for A package (A包相关词汇)Approach flow system流送系统disc filter多盘Thick stock screening浓浆筛选super clear filtrate超清滤液Fiber recovery纤维回收clear filtrate清滤液Cleaner除砂器cloudy filtrate浊滤液Flying wing Deculator cord packing盘根with cleaner 飞翼式除气器 double suction pump双吸泵Headbox 流浆箱make-up water补充水Wire pit 机外白水槽accept良浆Condenser冷凝器reject尾渣V acuum pump真空泵interface衔接Centrifugal pump离心泵sight glass视镜Diagram pump隔膜泵votex nozzle涡流喷嘴Screw pump螺杆泵throttling valve节流阀Displacement pump置换泵recovered fiber回收纤维WW channel白水方管NBKP漂白针叶硫酸盐浆Dilution headbox screen稀释水筛BCTMP漂白化学热磨机械浆HB screen纸机筛poplar pulp杨木浆Broke thickener chest损纸浓缩浆池sweetener垫层浆Dry broke intermitted chest干损纸中间浆池DIP脱墨浆Silencer消音器broken损纸Seal pit水封池dilution water稀释水Manifolds上浆总管sealing water密封水Separator分离器defibrination纤维疏解V ibrations sensor振动传感器oscillating shower摆动喷淋FC motor变频电机flow sheet流程图Dosing chest配浆池emergency stop急停Mixing chest混合浆池manufacturing drawing制造图Machine chest抄前池foundation drawing基础图Stuffing box填料箱reference drawing参考图Header总管functional diagram功能图Distribution pipe布浆管interlocking diagram连锁图Deflector 导流板over flow溢流Suction side引程侧solid content固含量Head扬程buffer缓冲器Counter flange配对法兰furnish配比Anchor bolt地脚螺栓magnetic flow-meter电磁流量计Slid rail 滑轨periodical variation周期波动Tensioning equipment张紧装置random variation随机波动Wall ring大法兰(墙环)fiber orientation纤维定向Motor stand电机座scaling结垢Fastening element紧固件pressure pulsation压力脉冲Steam heater蒸汽加热器flow evenness均衡流量Plug flow滞流short circulation短循环Transition flow过渡流(混流) air pocket气袋slime腐浆turbulence flow紊流(湍流)Medium-consistency storage tower中浓储浆塔plunger pump潜水泵部分造纸术语:grade 纸种grammage 定量width on reel 卷取纸幅宽coating weight 涂布量moisture before coating 涂前水份moisture on reel 卷取水份steam pressure 蒸汽压力steam consumption 蒸汽灌消耗量wire speed 网速press speed 压榨速度reel speed 卷取速度furnish 浆料配比Temp.in HB 流浆箱浆料温度press data 压榨数据supplier 供应商installed date安装日期days running运行天数style型号basis weight克重tension张力felt width on stretcher张紧辊上毛毯宽度stretched/stretch to go张紧辊张紧位置uhle box 毛毯真空箱vaccum真空度air velocity空气流速vacuum system 真空系统edge shower边缘喷淋水lubrication shower低压润滑喷淋水HP shower高压喷淋水moisture profiles水份图像moisture point measurements水份测量点absorption capability透水度常用高得率浆中英文对照SGW (Stone Ground Wood) 磨石磨木浆PGW (Pressurized Ground Wood) 压力磨石磨木浆TGW (high Temperature Ground Wood) 高温磨石磨木浆RMP (Refiner Mechanical Pulp) 盘磨机械浆TMP (Thermo-Mechanical Pulp) 预热盘磨机械浆CMP (Chemi-Mechanical Pulp) 化学盘磨机械浆CTMP (Chemi-Thermo-Mechanical Pulp) 化学预热机械浆APMP (Alkaline Peroxide Mechanical Pulp) 碱性过氧化氢化学机械浆SCMP (Sulfonated Chemi-Mechanical Pulp) 磺化化学机械浆BMP (Bio-Mechanical Pulp) 生物机械浆SEP (Steam Explosion Pulping) 蒸汽爆破法制浆EMP (Extruder Mechanical Pulp) 挤压法机械浆SCP (Semi-Chemical Pulp) 半化学法浆NSSC (Neutral Sulphite Semi-Chemical pulp) 中性亚硫酸盐法半化学浆ASSC (Alkaline Sulphite Semi-Chemical pulp) 碱性亚硫酸盐法半化学浆各种缩写:AA = atomic absorption原子吸收ABS = acrylonitrile-buladrene styrene丙烯腈—丁;烯—苯乙烯ACAR = angular correlation of annihilation radiation消除辐射的角相关性AM = acrylamide丙烯酰胺AOX = adsorbable organic halides可吸附的有机卤化物AP = plkali pulp碱法纸浆APAM = anionic polyacrylamide阴离子型聚丙烯酰胺ASB = aerotion stabilization basin稳定曝气池AST = activated sludge treatment活性污泥处理BBCT = best convential pollutant cotrol technology最常用污染物控制技术BDMT = bone dry metric tons绝干公吨BME = bipolar membrane electro dialysis两极膜电透析BMP = best management practices最优管理实践BOD = biochemical oxygen demand生化耗氧量BP = boiling point沸点BPK = bleached papergrade kraft and soda(生产)白纸用硫酸盐和荷性纳法浆BPT = best practicable control technology最佳实用控制技术BTU = british thermal unit英热单位BW = basis weight定量CCAD = computer aided design计算机辅助设计CBLI = chemistry-based leak indicator化学(法)示漏器CC = consistency controller浓度调节器CFD = computational fluid dynamics计算流体动力学CI = colour index比色指数= cofidence interval置信区间CL = colored ledger彩色底板CLSM = confocal laser scanning microscopy共焦激光扫描显微镜CMC = carboxy methylated cellulose羧甲基纤维素COMS = compliance optimization modeling system寻优模型系统CP = chemical pulp化学浆= chemical pure化学纯CPPC = coordinated phosphate/pH chemistry controller配位磷酸盐/pH 调节器CR = consistency regulator浓度调节器CRP = chloride removal process氯化物排出法CSD = condensate steam distillation column冷凝汽馏塔CTMP = chemical treatment in terms of sulphonation硫化期间的化学处理= chemithermomechanical pulp化学热磨机械浆CTU = centigrade thermal unit公制热量单位CV = coefficient variation偏离系数= crystal violet结晶紫DD = dioxide二氧化物DAF = dissolved air floatation(溶)气浮DCS = dissolved and colloidal substances溶解与胶态物= distributed control system集散控制系统DELS = Doppler electrophoretic light scattering多普勒电泳光扫描DIP = deinked pulp脱墨纸浆DKP = deinked kraft pulp脱墨牛皮纸浆DLK = double-line clippings双线限位DMS = dynamic mechanical spectroscopy动力谱学DMSO = dimethyl sulfoxide二甲亚砜DMT = dimethyl terephthalate对邻苯二甲酸二甲酯DO = dissolved oxygen溶解氧DP = degree of polymerization聚合度DSC = differential scanning calorimetry微分扫描量热法DVC = digital valve controller数字伐控制器EEC = embedded costs插入成本ECF = elemental chlorine free无元素氯(漂白)EDTA = ethylene eiamine tetraacetic acid乙二胺四乙酸EPC = experimental prismatic calcite实验棱镜方解石ERV = estimated replacement value预计取代值ESP = electrostatic precipitator静电滤尘器= emergency shutdown procedure事故停机程序EVA = ethylene vinyl acetate乙烯乙酸乙烯酯ESPRA = empire state paper research associates国立造纸研究会EVOH = ethylene-vinyl alcohol乙烯-乙烯醇FFAS = formamidine sulfinic acid甲脒亚磺酸FBB = folding box board折叠箱纸板FBK = fully bleached kraft全漂牛皮纸FC = flow controller流量控制器FID = free induction decays自由感应衰减FP = freezing point冰点;凝固点GGDP = gross domestic product本国生产总值GEMS = general energy and materials balance system通用能量和物料平衡系统GLC = gas-liquid chromatography气液色谱GPC = gel permeation chromatographic analysis凝胶渗透色谱分析GPM = gallons per minute加仑/分钟HHC = high consistency高浓HCR = high consistency refiner高浓磨浆机HD = high density高密度HPR = high production rate高生产率HPSEC = high-performance size-exclusion chromatography高性能粒度筛析色谱法HRT = hydraulic retention time水力停留时间HTH = high test hypochlorite高级漂粉HV = high voltage高压HW = hardwood硬木IIMPM = interactive multiplanar model相互作用的多面模型IPST = institute of paper science and technology造纸科技研究院IWC = international water consultants国际水质顾问团JJIT = just-in-time正好;准时KKP = kraft pulp牛皮浆;硫酸盐浆LLC = level controller液面控制器LCC = lignin-carbohydrate complexes木素-碳水化合物复合体LCL = lower control limits控制下限LCR = level cotroller and recorder液面控制记录仪LDPE = low density poly ethylene低密度聚乙烯LDV = laser Doppler velocimetry激光多普勒测速法LIVG = low inlet velocity gasification process低入口速度气化工艺LPR = low production rate低生产率LRD = long rang dependence广范围相关LVDT = linear position transducer线性位移变送器LWC = lightweight coated低定量涂布的MMACT = maximum achievable control technology最大可达控制技术MAP = modified atmosphere packaging改良常压包装法MC = marginal cost边际成本= medium consistency中浓(度)MDI = methylendiphenyl diisocyanate亚甲苯二苯二异氰酸酯MeB = methylene blue亚甲基兰,四甲基兰MEK = methyl ethyl ketone甲(基)乙(基)酮MF = machine finished机械整饰的MG = machine glazed机械上光的= malachte green孔雀绿MISS = mixed liquor suspended solids (有机物与活性污泥 )混合液中悬浮固体MOW = mixed office waste混合办公废纸MRP = matal removal process金属(离子)脱除过程MSW = municipal solid waste城市固体废物MVP = moisture vapor permeability水蒸汽渗透性MWL = milled wood lignin磨木木素NNC = nitrocellulose 硝化纤维素NF = nanofiltration超滤 (毫微过滤)NMR = nuclear magnetic resonance核磁共振NSPS = new source performance standards新的资源性能标准NSSC = neutral sulfite semi-chemical pulp中性亚硫酸半化学浆OOCC = old corrugated container旧瓦楞纸箱OD = over dry绝干;烘干OEE = overall equipment efficiency总设备效率OIT = oxidative induction temperature氧化起始温度O&M = operating and maintenance 使用与维护ONP = old newspaper旧新闻纸OPP = oriented polypropylene取向聚丙烯OPR = oil penetration rates渗油率OWL = oxidized white liquor氧化白液PPAL = positron annihilation life time正电子湮没寿命PC = pressure controller压力调节器PCA = principal components analysis主成分分析PCC = precipitated calcium carbonate沉淀碳酸钙PCR = pressure controller and recorder压力调节记录仪PDSC = pressure differential scanning colorimetry压差扫描量热术PEMS = predictive emissions modeling system预测排放模型系统PEO = poly ethylene oxide聚氧化乙烯PGS = papergrade sulfite造纸用硫磺PGW = pressurized groundwood压力磨木浆PM = paper machine 造纸机;抄纸机PM/ECCM = preventive maintenance and essential care and condition monitoring预防维修/基本维修及状态监测PP = polypropylene聚丙烯PSES = pretreatment standards for existing sources现存资源预测标准PSM = process safety management(生产)过程安全管理PTFE = polytetrafluoroethylene聚四氟乙烯PTR = photothermal radiometry光热辐射分析法PVC = polyvinylchloride聚氯乙烯PVDC = polyvinyl dichloride聚二氯乙烯PVSK = polyvinylsulfate聚乙烯硫酸酯RRDH = rapid displacement heating快速置换加热法RH = relative humidity相对湿度RMP = refiner mechanical pulp木片磨木浆;盘磨机械浆RN = regular number纸板标准号RT = radiographic testing射线照相试验,X射线检验SSBK = solid bleached kraft(同质)漂白牛皮纸SBR = sequencing batch reactors程序化间歇反应器SC = super calendered超级压光的SDI = silt density index淤泥浓度指数SE = supplemental energy补充能量;辅助能SEC = size exclusion chromatographic粒度筛析色谱法SEM = scanning electron microscope扫描电子显微镜SEM-EDS = scanning electron microscope-energy dispersive spectrometry扫描电子显微镜—能量分散能谱测定法SGW = stone ground wood磨石磨木浆SIF = stress intensity factor应力强度系数;应力强化因子SOPs = standard operating procedures标准作业程序SP = sulphite pulp亚硫酸盐纸浆SPC = satislical process control过程控制SRT = solids retention time粒子留着时间SUB = solid unbleached board(同质)本色浆纸板SW = softwood软木;针叶树SWL = sulphite waste liguor亚硫酸盐废液TTAC = totally applied chlorine总用氯量TC = temperature controller温度调节器TCDF = tetrachlorodibenzofuran四氯二苯并呋喃TCF = totally chlorine-free全无氯(漂白)TCR = temperature controller and recorder温度调节记录仪TGA = thermal gravimetric analysis热重分析TLA = thin layer activation薄层活性化TMP = thermo mechanical pulp热磨机械浆TP = thermo-plastic热塑性的TQ = threshold quantity临界量(值)TRS = total reduced sulfur总还原硫TS = tensile strength抗张强度TSS = total suspended solids总悬浮固体量UUBB = unbeached board本色(浆)纸板UBK = unbeached kraft本色牛皮纸UCL = upper control limits控制上限UT = ultrasonic testing超声试验UV = ultraviolet紫外光VVOC = volatile organic compound挥发性有机化合物WWAS = waste-activated sludge废活性污泥WFMT = wet fluorescent magnetic particle test湿荧光磁粉试验WL = white ledger白色帐簿纸WLC = white-lined chipboard白浆衬里的粗纸板WP = wood pulp木浆WVTR = water vapor transmission rate水蒸汽传递速度YYI = yellow index返黄值;返黄指数YP = yield point屈服(软化)点。
covariance和correlation的计算公式
covariance和correlation的计算公式金融上投资组合这两个好像都表示的是两个组合的相关性具体怎么理解这两个的区别呢都表示相关程度协方差有单位相关性系数在协方差的基础上,除以了(标准差的乘积),变得没有单位了(无量纲量)。
Covariance是绝对值,体现了两组合之间绝对相关性的大小;Correlation是在两组数据基础上的相对值,消除了数据组本身大小对相关性的影响(eliminatetheeffectsofsize),着重描述其相对的相关性,从而使不同规模的数据组之间具有可比性和对照性。
打个比方,如果我们说一个Portfolio的潜在亏损额为10万,是绝对值;Correlation存在的意义,则是将类似“10万”的数值概念相对化——考虑到Portfolio投资总额为1,000万,那么其潜在风险为1%(相对值),这对于多数投资者来说都处在一个可以接受的区间。
但如果Portfolio的投资总额仅为100万,则潜在风险就变成了10%,相比上面的情况一下子扩大了10倍,也就大大超过了风险厌恶者的可接受阀值。
covariance是表示两个变量间同向或者反向变化关系,correlation表示变量间的线形关系Covariance被标准化后就是correlation。
这样做是为了方便比较。
两者是绝对值与相对值的差别,是非标准化与标准化的差别。
Covariance协方差:是绝对数值,自带单位unitCovariance的计算公式如下:当中,E是数学期望(expectation),也就是算术平均值啦。
可以看出,Covariance计算出来是一个绝对数值,自带单位的,范围是正无穷到负无穷。
用Covariance进行数据比较的时候,只有同类数据才可以比较,例如:大盘指数、收益率等。
协方差,从中文上就可以看出和方差是类似的概念,只是不同数据之间的比较。
基准利率转换lpr公式
基准利率转换lpr公式基准利率转换LPR公式随着中国金融体系的不断改革完善,人民银行于2019年8月17日推出了新的贷款市场报价利率(Loan Prime Rate,简称LPR)机制,用以取代原有的贷款基准利率。
LPR是商业银行对贷款利率的报价,是市场供求关系决定的,更加市场化、透明。
那么,基准利率如何转换为LPR?下面就来介绍一下基准利率转换LPR公式。
我们需要明确一些概念。
基准利率是由人民银行制定的,用于指导各类贷款利率的核定。
而LPR是由商业银行根据市场利率情况报价的利率,LPR的调整频率更高,更能反映市场供求关系的变化。
LPR的报价分为1年期、5年期、10年期和其他期限,分别对应不同贷款期限的利率。
基准利率转换LPR的公式如下:LPR = 基准利率 + 浮动利率其中,基准利率是人民银行制定的贷款基准利率,具体数值由人民银行根据经济形势和金融市场情况进行调整。
而浮动利率是商业银行根据借款人的信用状况和市场供求情况确定的,具体数值会在贷款合同中明确。
基准利率转换LPR的公式可以简单理解为,LPR是基准利率加上浮动利率得到的结果。
基准利率是由人民银行决定的,具有一定的稳定性;而浮动利率则根据市场情况和借款人的信用状况进行浮动,具有一定的灵活性。
那么,如何确定具体的浮动利率呢?商业银行会根据借款人的信用评级、还款能力等因素来确定浮动利率的水平。
一般来说,信用评级较高、还款能力较强的借款人可以享受较低的浮动利率,而信用评级较低、还款能力较弱的借款人则需要支付较高的浮动利率。
市场供求关系也会对浮动利率产生影响。
如果市场资金供应充足,借款需求较少,那么浮动利率可能会相对较低;反之,如果市场资金紧张,借款需求较大,那么浮动利率可能会相对较高。
需要注意的是,基准利率转换LPR的公式只是一个计算LPR的基本原理,具体的利率水平是由市场供求关系和商业银行的报价决定的。
因此,在实际操作中,借款人需要与商业银行进行详细的咨询和协商,了解具体的利率水平和还款方式。
OMOMLFLPR关系?

OMOMLFLPR关系?OMO MLF LPR关系OMO:全称为公开市场操作,是中央银行吞吐基础货币,调节市场流动性的主要货币政策工具,通过中央银行与指定交易商进行有价证券和外汇交易,实现货币政策调控目标。
MLF:全称为中期借贷便利,由中国人民银行在2014年9月设立。
麟龙投顾指出,MLF是央行的一种货币政策工具,用来提供中期基础货币,保障银行体系流动性总体平稳适度,支持货币信贷合理增长。
主要面向符合宏观审慎管理要求的商业银行、政策性银行,以通过招标的方式开展。
LPR:全称为贷款市场报价利率,是商业银行对其最优质的客户执行的贷款利率,其他贷款利率可以在此基础上加减点生成。
LPR由18家报价行于每月20日(遇节假日顺延)9时前,以0.05个百分点为步长,向全国银行间同业拆借中心提交报价,全国银行间同业拆借中心按去掉最高和最低报价后算术平均,向0.05%的整数倍就近取整计算得出LPR,并于当日9点30分公布。
SLF:全称为常备借贷便利,它是中国人民银行正常的流动性供给渠道,主要功能是满足金融机构期限较长的大额流动性需求,在银行体系流动性出现临时性波动时相机运用。
SLF主要面对的是政策性银行和全国性商业银行,期限为1-3个月,利率水平则根据货币政策调控、引导市场利率的需要等因素综合确定。
央行运用SLF 的方式是用抵押的方式发放,银行需要提供合格的抵押品,如高信用评级的债券类资产及优质信贷资产等。
公开市场利率是什么从公开市场业务的角度行,公开市场利率是联结财政政策和货币政策的纽带。
公开市场操作是中央银行通过买卖有价证券而调节货币供应量。
公开市场利率央行公开市场操作手段主要有两种:正(逆)回购和买卖央票。
公开市场利率正(逆)回购期限较短。
短者可至7天。
央行票据分为3个月、1年和3年等。
央行票据的期限长于正(逆)回购。
从功能上讲,公开市场利率两者都有调控商业银行流动性的效果。
较央行票据而言,公开市场利率正(逆)回购将减少运作成本,同时锁定资金效果较强。
lpr货币政策的传导机制

lpr货币政策的传导机制lpr货币政策的传导机制引言:LPR(Loan Prime Rate)是中国推出的一种贷款基准利率,作为利率市场化改革的重要一环,它不仅影响着市场利率水平的形成,也直接关系到个人和企业的借贷成本。
了解LPR货币政策的传导机制对于我们深入理解中国金融体系的运行具有重要意义。
一、LPR的形成与运行机制1. LPR的定义及发展历程LPR是由央行每个月发布的一种贷款利率,其基准利率主要由央行根据市场情况和宏观经济状况决定。
LPR的发展历程可以追溯到2013年,当时央行推出了首个LPR试点。
随着金融市场改革的深入,LPR逐渐成为金融机构贷款利率的重要参考标准。
2. LPR与MLF的关系央行通过公开市场操作使用MLF(中期借贷便利)交易来提供资金支持,而LPR则是其放贷利率的参考标准。
MLF利率的上调或下调会直接对LPR形成影响,因为LPR的定价机制中,MLF利率起着重要作用。
3. LPR的定价机制LPR的定价机制分为两个层次,一是市场利率的形成,二是银行机构的定价。
市场利率的形成会受到央行货币政策、市场供求状况和经济形势等因素的影响,而银行机构则会根据自身成本、风险和市场竞争等因素来确定相应的贷款利率。
二、LPR货币政策的传导机制1. 金融市场与实体经济的联系LPR作为金融市场的一种利率,其变动会通过多种途径影响实体经济。
LPR的调整会直接影响到企业和个人的借贷成本,这对于促进实体经济发展和消费需求具有一定的推动作用。
LPR的变动也会对股市、债市和房地产市场等资产价格产生影响,从而进一步影响到实体经济的发展。
2. 传导渠道的作用机制LPR货币政策通过多种传导渠道影响实体经济。
一是信贷传导渠道,即通过调整LPR影响银行机构的贷款利率,从而影响企业和个人的借贷成本。
二是利率传导渠道,即通过调整LPR影响市场利率的走势,进而影响资本市场的运行和资金流动。
三是预期传导渠道,即通过LPR的调整,影响市场参与者对未来货币政策走势的预期,进而对市场利率和借贷行为产生影响。
corr方法
corr方法CORR(Correlation)方法是一种统计分析方法,用于衡量两个变量之间的线性关系。
该方法被广泛应用于金融、统计和计算机科学等领域,用于分析和处理数据,从而获得更好的理解和预测。
该方法依赖于皮尔逊相关系数(Pearson Correlation Coefficient),这是一种衡量两个变量之间线性关系强度的标准方法。
皮尔逊相关系数的值介于-1和1之间,其值越接近1(-1),则表明两个变量之间的线性关系越强,正(负)相关性越高;其值越接近0,则表明两个变量之间的线性关系越弱,不存在(弱)相关性。
CORR方法在金融领域中有广泛的应用。
例如,用于分析股票市场中各个股票之间的相关性,以及对股票价格走向的预测。
通过对股票相关性的分析,我们可以发现某些股票价格波动趋势与其他股票价格波动趋势存在高度相关性,从而优化投资组合,减少风险。
此外,CORR方法还广泛用于数据挖掘和机器学习领域。
例如,在自然语言处理中,我们可以使用CORR方法来分析不同单词之间的相关性,从而提高文本分类和情感分析的准确性。
在图像识别中,我们可以使用CORR方法来分析图像特征之间的相关性,以及帮助识别模式和提高准确性。
在统计学中,CORR方法也是非常重要的。
例如,在样本数据分析中,我们可以使用CORR方法来分析两个变量之间的相关性,以及识别决定数据集中差异的关键因素。
在统计建模中,我们可以使用CORR方法来评估模型的拟合情况和预测准确性,以及确定最佳拟合模型。
综上所述,CORR方法是一种非常强大的分析工具,可以用于数据分析、金融学、机器学习、自然语言处理、图像识别等各种领域。
通过使用CORR方法,我们可以更好地理解和预测复杂数据的关系,并为实践决策提供有力支持。
回购利率 lpr计息条款
回购利率 lpr计息条款回购利率LPR计息条款是指在回购交易中,利息的计算方式采用贷款市场报价利率(Loan Prime Rate,简称LPR)来确定的一种条款。
LPR是中国人民银行定期公布的一种参考利率,根据市场供求和风险评估等因素形成。
回购是金融市场中常见的一种交易方式,即借出方出借资金给借入方,约定一定期限后,借入方以债券等作为抵押向借出方购回资金,并支付一定利息。
而LPR计息条款就是在这样的回购交易中,利息的计算方式采用LPR。
LPR计息条款的引入有助于提高回购交易的透明度和市场化程度。
传统上,回购交易的利率计算方式多为基于银行间同业拆借利率(Shibor)或人民银行公开市场操作利率(OMO利率)。
而LPR作为一种更为市场化的利率,其引入可以更好地反映市场供求状况,使回购利率更具公平性和准确性。
在使用LPR计息条款的回购交易中,借出方和借入方会事先约定借款期限和回购利率,其中回购利率即为LPR。
根据中国人民银行公布的LPR水平,借出方和借入方可以确定回购交易的利息额,并在交易到期时进行结算。
这样一来,LPR的变动会直接影响到回购交易的利息水平,使利息更加与市场挂钩。
LPR计息条款的引入对于金融市场的发展具有积极意义。
首先,通过采用LPR作为回购利率,可以降低金融机构之间的信贷风险,提高市场的流动性。
其次,LPR计息条款的引入可以促进金融市场的利率市场化改革,推动利率市场化进程。
最后,LPR计息条款的使用还有助于提高回购交易的透明度和公平性,为投资者提供更多选择。
回购利率LPR计息条款的引入对于金融市场的发展具有重要意义。
通过使用LPR来确定回购利率,可以提高回购交易的公平性和准确性,促进金融市场的利率市场化进程。
这将有助于推动金融市场的发展,提高金融机构之间的信贷风险管理能力,为投资者提供更多选择。
LPR利率查询(2021年02月LPR利率)
LPR利率查询(2021年02月LPR利率)LPR利率查询(2021年02月LPR利率)2021年02月最新央行LPR利率:一年期lpr利率:3.85%五年期lpr利率:4.65%01月LPR利率(目前1年期LPR与5年期LPR利率分别为3.85%及4.65%,连续8个月持平。
)lpr利率长期趋势:lpr利率是什么意思央行基础利率lpr,意思是央行推行以lpr利率为贷款定价基准利率,各银行只能来在此利率上加自码,而不能下调。
而lpr利率是以18家银行共同报价,去掉一个最高值和一个最低值,再取平均值得出的,每月20号更新。
从2019年10月8日起,房贷利率将进入月时代,实际贷款利率以放贷银行的审批结果为准。
已有房贷要不要转lpr这个问题的核心就在于你对LPR未来是上调还是下调的一个判断了,对于绝大多数人而言,这是个难题,基本上没几个人能够有能力做出判断。
其实就是专家也没法判断到底LPR会上调还是下调。
目前网上大多都在说LPR会下调,比如,有人从国家级别层面去判断,纵观世界,日本,意大利等国家基本上都在1-2个百分点,而中国作为发展中国家,4.8个百分点,的确高,判断为下调;还有一部分人从经济的角度去考虑,因为LPR参考了18家商业银行的意见,很显然,商业银行要赚钱的,上调必定是有利于商业银行的,所以从这个角度看,未来要上调(当然,前提是经济转好)。
综上所述,个人觉得,如果你的房贷利率高,那就转,如果低,比如4.165,就没什么必要了。
LPR之所以让大家伙闹腾不知道该不该转,就是因为它的可变性,未来谁也不知道会有什么政策,会有什么因素导致LPR上调还是下调,所以还可以按照自己的性格来,喜欢稳定,不喜欢变数的话,就不转,如果想跟随市场变化,那就转,毕竟,如果上调,那就说明经济好,经济好的话,你赚的也是多,总体来看,差不了多少。
lpr利率历史数据(最近更新2021年01月20日)2021/02/20:1年期3.85%,5年期以上4.65%2021/01/20:1年期3.85%,5年期以上4.65%2020/12/21:1年期3.85%,5年期以上4.65%2020/11/20:1年期3.85%,5年期以上4.65%2020/10/20:1年期3.85%,5年期以上4.65%2020/09/21:1年期3.85%,5年期以上4.65%2020/08/20:1年期3.85%,5年期以上4.65%2020/07/20:1年期3.85%,5年期以上4.65%2020/06/20:1年期3.85%,5年期以上4.65%2020/05/20:1年期3.85%,5年期以上4.65%2020/04/20:1年期3.85%,5年期以上4.65%2020/03/20:1年期4.05%,5年期以上4.75%2020/02/20:1年期4.05%,5年期以上4.75%lpr利率和基准利率一、基准利率1、基准利率是人民银行制定的具有指导意义的一个利率。
贷款市场报价利率(LPR)(截止2022-10-20日)
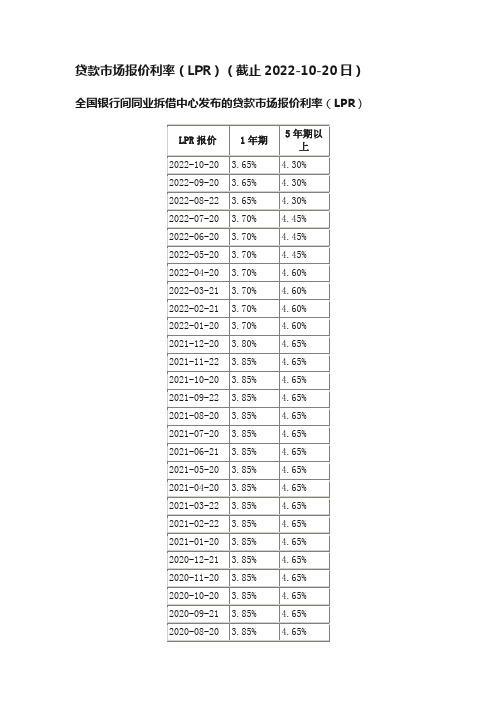
贷款市场报价利率(LPR)(截止2022-10-20日)全国银行间同业拆借中心发布的贷款市场报价利率(LPR)
【贷款市场报价利率】
贷款市场报价利率(Loan Prime Rate,简称LPR)是指由各报价行根据其对最优质客户执行的贷款利率,按照公开市场操作利率加点形成的方式报价,由中国人民银行授权全国银行间同业拆借中心计算得出并发布的利率。
各银行实际发放的贷款利率可根据借款人的信用情况,考虑抵押、期限、利率浮动方式和类型等要素,在贷款市场报价利率基础上加减点确定。
LPR报价行现由18家商业银行组成,报价行应于每月20日(遇节假日顺延)9时前,按公开市场操作利率(主要指中期借贷便利利率)加点形成的方式,向全国银行间同业拆借中心报价。
全国银行间同业拆借中心按去掉最高和最低报价后算术平均的方式计算得出贷款市场报价利率。
目前,LPR包括1年期和5年期以上两个期限品种。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
The LaryngoscopeLippincott Williams&Wilkins,Inc.©2005The American Laryngological,Rhinological and Otological Society,Inc.Correlation between Symptoms and Laryngeal Signs in Laryngopharyngeal RefluxMohammed A.Qadeer,MD;Jason Swoger,MD,MPH;Claudio Milstein,PhD;Douglas M.Hicks,PhD; Jeff Ponsky,MD;Joel E.Richter,MD;Tom I.Abelson,MD;Michael F.Vaezi,MD,PhD,MSepiObjective/Hypothesis:Laryngopharyngeal reflux (LPR)is diagnosed by the presence of laryngeal signs and symptoms.Some studies have noted that signs and symptoms may be nonspecific and may have poor correlation.However,many such studies were either observational or had short-term follow-up.Therefore, we conducted subgroup analysis of a prospective con-current controlled study with a1year follow-up to study the correlation between signs and symptoms. Study Design:Prospective study.Methods:Seventy-two patients with suspected gastroesophageal reflux disease related laryngeal symptoms/signs received a4 month trial of aggressive acid-suppressive therapy. Four month symptomatic nonresponders(<50%im-provement)with continued laryngeal inflammation and normalized esophageal acid exposure were then offered laparoscopic Nissen fundoplication.The pri-mary outcome was laryngeal symptom-sign correla-tion at1year postsurgery.Results:Twenty-five of72 (35%)patients remained unresponsive after4months of aggressive acid suppressive therapy.Ten(40%)pa-tients agreed to undergo surgical fundoplication (mean age؍50,male؍4).The most common laryn-geal symptoms were sore throat(40%),hoarseness (30%),and cough(20%),whereas the most common signs were medial arytenoid wall erythema/edema (60%),interarytenoid erythema(50%),and arytenoid complex erythema/edema(50%).At1year postfundo-plication,laryngeal symptoms improved in only1of 10(10%)patient,whereas signs improved in8of10 (80%)patients.Conclusions:There appears to be poor correlation between signs and symptoms of LPR,par-ticularly when monitoring therapeutic outcomes.In patients unresponsive to twice-daily proton-pump in-hibitor therapy for4months,further aggressive ther-apy is unlikely to bring additional symptomatic ben-efit.Key Words:Laryngopharyngeal reflux(LPR), symptom-sign correlation,twice-daily PPI, fundoplication.Laryngoscope,115:1947–1952,2005 INTRODUCTIONLaryngopharyngeal reflux(LPR)or reflux laryngitis is one of the most common extra-esophageal manifesta-tions of gastroesophageal reflux disease(GERD).1,2Popu-lation based studies found that the prevalence of symp-toms attributed to LPR was in the range of15%to20%.3,4 It is estimated that up to15%of all visits to the otolaryn-gology offices are because of manifestations of LPR.1,5,6 The symptoms that are commonly attributed to LPR are hoarseness,throat clearing,nocturnal laryngospasm, otalgia,postnasal drip,chronic cough,and dysphagia.1,7 Because many of these symptoms are nonspecific,confir-mation of the diagnosis usually requires laryngoscopic examination on which the presence of any of the following is considered LPR:erythema,edema,pseudosulcus,ven-tricular obliteration,and postcricoid hyperplasia.1How-ever,even these signs are not specific to LPR because of their high prevalence in general asymptomatic popula-tion.8,9Thus,it is possible that the presence of both symp-toms and signs might increase the likelihood of LPR diag-nosis.However,it is not known if there is symptom-sign correlation in these patients and whether this correlation could be used to monitor therapeutic outcomes.To assess the relationship between symptoms and laryngeal signs,we conducted analysis of a cohort of pa-tients who had chronic laryngitis unresponsive to aggres-sive acid suppressive therapy and having undergone lapa-roscopic fundoplication(definitive therapy for GERD) were followed for a period of1year.The aim of this analysis was to assess the strength of correlation between LPR signs and symptoms after definitive therapy of GERD.From the Department of Gastroenterology and Hepatology(M.Q.,J.S., J.E.R.,M.F.V.),Center for Swallowing and Esophageal Disorders,the Headand Neck Institute(C.M.,D.M.H.,T.I.A.),and the Department of General Surgery(J.P.),Cleveland Clinic Foundation,Cleveland,Ohio,U.S.A.Editor’s Note:This Manuscript was accepted for publication June22, 2005.Send Correspondence to Dr.Michael F.Vaezi,Department of Gas-troenterology and Hepatology,1501TVC,1301-22nd Avenue South,Nash-ville,TN37232-5280,U.S.A.E-mail:Michael.vaezi@DOI:10.1097/01.mlg.0000176547.90094.acMATERIALS AND METHODSPatient PopulationThe study cohort included the subgroup of patients who underwent laparoscopic fundoplication for chronic laryngeal symptoms after a failed4month trial of aggressive acid suppres-sive therapy.This subgroup was derived from the original cohort of patients with chronic laryngitis who were followed by the Department of Gastroenterology and Head and Neck Institute since1997.All these patients were evaluated by laryngoscopy, esophagogastroduodenoscopy,manometry,and24hour ambula-tory pH monitoring and treated with a4month trial of aggressive acid-suppressive therapy(omeprazole40mg twice daily or lan-soprazole60mg twice daily).Those who were unresponsive (Ͻ50%symptomatic improvement)to the above regimen were offered fundoplication as a definitive therapy for GERD.In the primary study,those patients who underwent fundoplication were compared with those who continued on aggressive proton-pump inhibitor(PPI)therapy for symptomatic improvement at1 year.10For the purpose of this analysis,we studied only the subgroup that underwent fundoplication and evaluated the cor-relation between laryngeal signs and symptoms at1year after fundoplication.Inclusion criteria were age greater than18years,chronic symptoms(cough,throat clearing,sore/burning throat,hoarse-ness,and globus),and laryngoscopic findings suggestive of LPR despite aggressive acid suppression.Patients were excluded from the study if they had Barrett’s esophagus,prior surgical therapy for GERD,or if they were unwilling to participate in the study.All patients meeting the inclusion criteria completed a four page nurse-administered questionnaire at the start of the study. The questionnaire consisted of demographic information,medical history,tobacco and alcohol use,current medication regimen,history of allergies,presence of other potential laryngeal irritants (asthma,sinusitis,sinus congestion,allergies,postnasal drip, viral illness,and vocal abuse),and description of specific laryn-geal symptoms.Patients were asked to report presence or ab-sence of symptoms(cough,hoarseness,throat clearing,sore throat,globus sensation,heartburn,regurgitation,problem swal-lowing,chest pain,and discomfort to talk)by answering yes or no on the questionnaire and score the severity using a scale of1to4 (1ϭrare[once a month or less];2ϭoccasional[once a week or less];3ϭfrequent[several times a week];4ϭall the time [several times daily]).After fundoplication,patients were monitored for1year.All subjects kept daily symptom diaries during the study period using the above severity scoring system.All patients also had blinded symptom assessment using a standard questionnaire at 1,3,6and12months postoperatively.Patients were asked to score their symptoms on a scale of0%to100%improvement. Response of laryngeal signs to surgical fundoplication was eval-uated at6and12months postfundoplication by a single endos-copist blinded to patients’symptomatic response status. LaryngoscopyPatients underwent a videotaped fiberoptic laryngoscopy at the Cleveland Clinic Head and Neck Institute before surgery and at6and12months postoperatively.The laryngoscopy was per-formed by one specialist(D.H.)who was blinded to patient symp-toms and group allocation.To ensure technical consistency,all examinations followed a standard protocol of subject instructions and tasks and used the same equipment.The subjects were seated comfortably and asked to sniff three sprays of a mixture of topical anesthetic and decongestant(1%neosynephrine;4%Xy-locaine)through one nostril.The flexible nasopharyngoscope (Pentax model FNL13S,Pentax Precision Instrument Corp,Ja-pan)was coupled to a color video camera(Toshiba model IK-C30A,Toshiba Corp,Japan)and was illuminated by a xenon light source(Karl Storz model610,Karl Storz Endoscopy–American Inc.,Culver City,CA).The scope was inserted into the nostril, passed along the nasal floor,and maneuvered to the oropharynx and upper hypopharynx.The subject was asked to perform a series of vegetative tasks(breathing,swallowing,coughing,sniff-ing,throat clearing)and vocal tasks(whistling,sustained phona-tion,alternate phonation/inhalation,and pitch glides)designed to allow visualization of the posterior pharyngeal wall,hypophar-ynx,and intrinsic larynx.Findings of erythema,edema,redun-dant tissue,surface irregularities,and other lesions were noted for each structure(posterior pharyngeal wall,posterior commis-sure[anterior cricoid wall],posterior cricoid wall,arytenoids com-plex,true and false vocal cords,anterior commissure,epiglottis, and aryepiglottic folds)and were recorded by the examiner on a checklist(Appendix).7,8Fig.1.Flow chart depicting the process of patient selection.TABLE I.Prevalence of Primary and Secondary Symptoms(nϭ10). Symptom Primary(%)Secondary(%) Chronic cough2010 Throat clearing010 Sore/burning throat4030 Globus010 Hoarseness3020 Dysphagia00 Other*00 None010 *Chest pain,shortness of breath,and regurgitation.Surgical InterventionAll the patients who underwent fundoplication were sub-jected to repeat pH monitoring(off-therapy),esophageal manom-etry,and barium esophagram before surgery and were docu-mented to have reflux on pH monitoring or esophagram.All these patients had their procedure performed by a single surgeon(J.P.) at the Cleveland Clinic Foundation Department of General Sur-gery.A standard360°laparoscopic Nissen fundoplication was performed in all10subjects.None of the patients required con-version to an open procedure.After fundoplication,the complete-ness of the procedure was assessed by pH monitoring and ma-nometry at3months and12months.Statistical AnalysisOverall descriptive statistics including means,medians, and standard deviations for continuous variables and frequencies for categorical variables were calculated.Symptom improvement was recorded on a scale of0%to100%.This score was further classified into1of2categories:greater than50%improvement or 50%or less improvement.Pearson’s chi-square test and Fisher’s exact test were used as appropriate to compare the proportion of patients that report greater than50%improvement in their symptoms groups.The Wilcoxon rank sum test was used to study the differences in the global assessment symptom score.A signif-icance level of.05was used in the analyses.Calculations were performed using JMP5.1software(SAS Institute,Cary,NC). RESULTSDemographicsThe original cohort consisted of72patients of which 25(35%)did not respond to aggressive PPIs,reporting less than50%symptom improvement after4months of ther-apy.Ten of these25(40%)patients agreed to enroll in this prospective surgical protocol and formed the cohort for this analysis(Fig.1).The mean age of the patients in this cohort was50(SD9.55)years.All the patients were white; males were40%and females60%.Fifty percent of the cases were ex-smokers,whereas another50%were non-smokers.Seventy percent of the patients consumed alco-hol.Baseline Laryngeal FindingsThe most common symptoms in these patients were sore throat and burning throat(40%)followed by hoarse-ness(30%)and chronic cough(20%).Sore throat was also present in significant number of patients whose main symptom was hoarseness or chronic cough(Table I).The symptoms were moderate to severe with mean severity score of3.4(SE0.8)on a scale of1to4.Seven of10(70%) of the patients had heartburn.These symptoms were per-sistent despite normalization of pH levels after4month PPI therapy.The most common signs in these patients were medial arytenoid wall erythema/edema(60%),fol-lowed by interarytenoid erythema(50%)and arytenoid complex erythema/edema(50%)(Table II).Technical Success of Surgical Procedure The surgical procedure was technically successful in all the10patients.At baseline,8of10(80%)of subjects in the surgical group had an abnormal pH study,and theTABLE II.Laryngoscopic Findings(Baseline,6and12Months Postoperative).Postfundoplication(%)Baseline6Month12Month Posterior cricoid wall erythema/edema40200 Posterior pharyngeal wall erythema20100 True/false vocal cord erythema/edema40100 Arytenoid complex erythema/edema502010 Medial arytenoid wall erythema/granularity603010 Postpharyngeal cobblestoning000 Redundant tissue/pseudosulcus2000 Interarytenoid bar erythema50100TABLE III.Median(Interquartile Range)Percent of Time pHϽ4.Percent pHϽ4Baseline4-month PostPPI Therapy3Month Postoperative12Month Postoperative ProximalTotal 2.3(0.05–8.5)0.00.0-Upright 2.6(0.1–11.7)0.00.0-Supine0.0(0–1.2)0.00.0-DistalTotal8.6(4.0–11.9)0.00.00.3(0.0–0.7) Upright10.3(3.6–13.7)0.00.00.1(0.0–0.4) Supine 6.4(0.3–13.15)0.00.00.0PPIϭproton-pump inhibitor.remaining2patients had evidence of reflux by barium esophagram.However,all these patients had normalized pH monitoring after4month PPI therapy.At3and12 months postfundoplication,the degree of esophageal acid exposure was significantly(PϽ.001)less than baseline values but similar(Pϭ1.0)to those obtained while on twice-daily PPIs(Table III).Manometric data revealed that none of these patients had abnormal manometry at3 months except“incomplete relaxation of the LES(lower esophageal sphincter),”which is a common finding post-fundoplication.Outcome at12MonthsAt1year follow-up,laryngeal symptoms improved in only1of10(10%)of these patients(Ͼ50%subjective improvement).Despite lack of improvement in laryngeal symptoms,heartburn resolved in all the patients.Inter-estingly,laryngeal signs improved in80%of patients.Five of10(50%)subjects were noted to have resolution of their initial findings at the6month postoperative follow-up.An additional3of10(30%)subjects were noted to have nor-malized laryngoscopic examinations at the12month follow-up visit.An additional two patients had improve-ment in laryngeal symptoms after treatment for asthma and allergies after the completion of the study period. DISCUSSIONThe results of this prospective study suggest that there is poor correlation between laryngeal signs and symptoms when monitoring therapeutic outcomes.Thus, although laryngeal signs resolved in80%of patients within a year after technically successful surgery,symp-tomatic improvement occurred in only10%of patients. Thus,neither signs nor symptoms may be used as a sur-rogate for the other.The results of this study confirm the findings of an earlier study conducted by Belafsky et al.11in which6 month follow-up was performed for LPR patients treatedAPPENDIX.Larynx/Pharynx Findings.Name:Clinic No:Date:Presence of the Following:Yes No Yes No1.Posterior Pharyngeal Wall 6.True Vocal Foldsa.Erythema a.Erythemab.Edema b.Edemac.Cobblestoning c.Surface Irregularityd.Mass Lesions(polyps)2.Interarytenoid Bar7.False Vocal Foldsa.Present a.Erythemab.Erythema b.Edemac.Blanched c.Surface Irregularityd.Irregular3.Posterior Commissure8.Anterior Commissurea.Erythema a.Erythemab.Edemac.Surface Irregularity4.Posterior Cricoid Wall9.Epiglottisa.Erythema a.Erythemab.Edema(laryngeal surface)c.Redundant Tissue b.Erythema(petiole)5.Arytenoid Complex10.Aryepiglottic Foldsa.Apex Erythema a.Erythemab.Apex Edema b.Edemac.Medial Wall Erythemad.Medial Wall Erosione.Medial Wall Granularitywith twice-daily PPIs.In that study,symptom improve-ment ceased at2months,whereas signs continued to improve over the6months.In our study,however,pa-tients who had good response to the twice-daily PPIs were excluded after4month therapy(65%),leaving only symp-tomatic nonresponders(35%)for the study.Thus,it ap-pears that if symptoms do not improve in2to4months after aggressive acid suppression,they are unlikely to improve even after a follow-up of more than a year despite having definitive therapy for reflux(fundoplication),and signs and symptoms continue to be dissociated from one another.Common throat symptoms attributed to LPR include hoarseness,vocal fatigue,chronic throat clearing,postna-sal drip,chronic cough,dysphagia,and globus.1,7How-ever,many of these symptoms are nonspecific and may be caused by other conditions such as smoking,allergies, postnasal drip,and neurogenic mechanisms.1But these symptoms are attributed to GERD on the basis of the findings of laryngoscopic examination in which the pres-ence of edema and erythema are considered synonymous with GERD.1,7,12In our study as well,these two signs were the most common(approximately60%)findings responsi-ble for LPR diagnosis.This also appears to be the most prevalent method of LPR diagnosis in many ENT prac-tices across the country,irrespective of teaching or non-teaching status.13For example,in a survey of approxi-mately2,000gastroenterologists and ENT physicians, Ahmed et al.13reported that edema and erythema of the larynx were the most common reasons for LPR diagnosis.However,the specificity of these findings for LPR diagnosis is questionable because an earlier study by Hicks et al.8found that up to87%of healthy volunteers had at least one sign attributed to LPR.In a more recent study,Milstein et al.9found a similarly high percentage of healthy population having laryngeal abnormalities.Fur-thermore,they also found that the use of different endo-scopic instruments resulted in significantly different la-ryngoscopic findings.Thus,flexible endoscopy found abnormalities in93%of the population compared with 83%through rigid endoscope.Rightfully,they questioned the utility of these findings to diagnose LPR given a low specificity and positive predictive value.There is also sig-nificant inter-and intra-observer variability in diagnosis of LPR.14,15Thus,presence of laryngeal signs cannot be taken as evidence of LPR,and more significantly,an LPR label should not be rigidly applied on patients,especially when they do not respond to aggressive acid suppressive therapy.The results of this study further suggests a possible multifactorial etiology for LPR,further supported by the fact that,in most of our patients,symptom improvement occurred only after adjunctive therapy for other condi-tions.Given the lack of specificity of any of the diagnostic tests in this patient group,empiric therapy with aggres-sive acid suppression with PPIs is often advocated as the initial test to determine whether GERD is the cause of patients’chronic symptoms.1,16Medical therapy in pa-tients with suspected LPR results in an overall response rate of50%to70%.1On the basis of the results of our study,it is unlikely that patients’chronic laryngeal symp-toms will improve postfundoplication,given their previous lack of response to aggressive PPI therapy.Our study is the first to prospectively evaluate the role of fundoplica-tion in patients with suspected LPR unresponsive to PPI therapy.However,prior observational studies have sug-gested similar outcome in patients with classic GERD or other atypical symptoms.17–23For example,So et al.,17 studying150consecutive patients after fundoplication, found that only56%of patients had relief of atypical symptoms,whereas typical heartburn symptoms resolved in93%.Furthermore,the only preoperative predictors of relief of atypical symptoms were prior clinical response to pharmacologic acid suppression and abnormal hypopha-ryngeal pH results.More specifically,a recent uncon-trolled case series20evaluating the outcome of patients with LPR reported84%symptom improvement postfun-doplication.However,this study again demonstrated a poor outcome in those previously unresponsive to PPI therapy.Therefore,on the basis of the results of these studies,continued symptoms on aggressive acid suppres-sion is most likely an indication for investigating other allergy,sinus,or pulmonary causes for patients’residual symptoms.The results of our study are strengthened by a pro-spective design,a long period of follow-up,and inclusion of only aggressive PPI therapy nonresponders.Blinded symptom assessment and laryngoscopic examinations documented changes in laryngeal symptoms and signs up to12months postoperatively.The main weakness of the study appears to be small sample size.However,given the significantly different improvement rates between signs and symptoms in these patients at1year(80%vs.10%),it has enough power(Ͼ95%)to suggest a lack of correlation between signs and symptoms at an alpha level of0.01. CONCLUSIONSThere appears to be poor correlation between laryn-geal signs and symptoms for the diagnosis of LPR,partic-ularly when monitoring therapeutic outcomes in patients unresponsive to PPI therapy.Patients who do not respond to twice-daily PPIs for4months are unlikely to respond to even more aggressive therapies such as fundoplication. Therefore,other etiologies for the symptoms should be actively sought in PPI unresponsive patients. BIBLIOGRAPHY1.Vaezi MF,Hicks DM,Abelson TI,Richter ryngealsignsand symptoms and gastroesophageal reflux disease(GERD):a critical assessment of cause and effect associa-tion.Clin Gastroenterol Hepatol2003;1:333–344.2.Richter JE.Extraesophageal presentations of gastroesopha-geal reflux disease.Semin Gastrointest Dis1997;8:75–89.3.Locke GR,Talley NJ,Fett SL,et al.Prevalence and clinicalspectrum of gastroesophageal reflux:a population basedstudy in Olmstead County,Minnesota.Gastroenterology1997;112:1448.4.Jaspersen D,Kulig M,Labenz J,et al.Prevalence of extraoesophageal manifestations in gastro-oesophageal refluxdisease:an analysis based on the ProGERD Study.AlimentPharmacol Ther2003;17:1515–1520.5.DeVault KR.Overview of therapy for the extraesophagealmanifestations of gastroesophageal reflux disease.Am JGastro2000;95:S39–S44.6.Postma GN,Johnson LF,Koufman JA.Treatment of laryn-gopharyngeal reflux.ENT J2002;2:24–26.7.Koufman JA.The otolaryngologic manifestations of gastro-esophageal reflux disease:a clinical investigation of225patients using ambulatory24-hour pH monitoring and anexperimental investigation of the role of acid and pepsin inthe development of laryngeal ryngoscope1991;101(4Pt2Suppl53):1–78.8.Hicks DM,Ours TM,Abelson TI,et al.The prevalence ofhypopharynx findings associated with gastroesophagealreflux in normal volunteers.J Voice2002;16:564–579. stein C,Charbel S,Hicks DM,et al.Prevalence of laryn-geal irritation signs associated with reflux in asymptom-atic volunteers:impact of endoscopic technique(rigid vs.flexible scope).Laryngoscope2005.In press.10.Swoger J,Ponsky J,Hicks DM,et al.Surgical fundoplicationin laryngopharyngeal reflux(LPR)unresponsive to aggres-sive acid suppression:a prospective concurrent controlledstudy.Clin Gastroenterol Hepatol.In press.11.Belafsky PC,Postma GN,Koufman ryngopharyngealreflux symptoms improve before changes in physical find-ryngoscope2001;111:979–981.12.Gaynor ryngeal Complications of GERD.J Clin Gas-troenterol2000;30:S31–S34.13.Ahmed T,Ableson TI,Hicks DM,et al.Chronic laryngitis asso-ciated with GERD:a large scale prospective assessment ofdifferences in practice patterns between gastroenterologists and ENT physicians.Gastroenterology2005;128:M1769. 14.Merati AL,Reider AA.Normal endoscopic anatomy of thepharynx and larynx.Am J Med2003;115:10S–14S.15.Branski RC,Bhattacharyya N,Shapiro J.The reliability ofthe assessment of endoscopic laryngeal findings associatedwith laryngopharyngeal reflux ryngoscope2002;112:1019–1024.16.Koufman JA,Aviv JE,Casiano RR,Shaw ryngopha-ryngeal reflux:position statement of the committee onspeech,voice,and swallowing disorders of the AmericanAcademy of Otolaryngology–Head Neck Surgery.Otolaryn-gol Head Neck Surg2002;127:32–35.17.So JB,Zeitels SM,Rattner DW.Outcomes of atypical symp-toms attributed to gastroesophageal reflux treated by lapa-roscopic fundoplication.Surgery1998;124:28–32.18.Campos GM,Peters JH,DeMeester TR et al.Multivariateanalysis of factors predicting outcome after laparoscopic Nissen fundoplication.J Gastrointest Surg1999;3:292–300.19.Leeder PC,Watson DI,Jamieson paroscopic fundopli-cation for patients with symptoms but no objective evi-dence of gastroesophageal reflux.Dis Esophagus2002;15:309–314.20.Westcott CJ,Hopkins MB,Bach K,et al.Fundoplication forlaryngopharyngeal reflux disease.J Am Coll Surg2004;199:23–30.21.Oelschlager BK,Eubanks TR,Oleynikov D,et al.Symptom-atic and physiologic outcomes after operative treatment forextraesophageal reflux.Surg Endoscop2002;16:1032–1036.22.Hunter JG,Trus TL,Branum GD,et al.A physiologic ap-proach to laparoscopic fundoplication for gastroesophageal reflux disease.Ann Surg1996;223:673–687.23.Johnson WE,Hagen JA,DeMeester TR,et al.Outcome ofrespiratory symptoms after antireflux surgery on patientswith gastroesophageal reflux disease.Arch Surg1996;131:489–492.。