Pitavastatin_Calcium_SDS_MedChemExpress
坎地沙坦西来替昔酯的合成工艺改进

收稿日期:2002-09-29作者简介:朱彦民(1959-),男(汉族),黑龙江哈尔滨人,高级工程师;宫平(1964-),男(汉族),新疆乌鲁木齐人,博士,教授,主要从事药物化学研究,Tel :(024)23882925。
文章编号:1005-0108(2003)01-0031-03坎地沙坦西来替昔酯的合成工艺改进朱彦民1,景士云1,王钝2,吴秀静2,宫平2(11哈尔滨制药集团制药总厂,黑龙江哈尔滨150086;21沈阳药科大学制药工程学院,辽宁沈阳110016)摘 要:目的完成坎地沙坦西来替昔酯(TCV 2116)的合成,并得到文献报道的C 2晶型产物。
方法设计了以32硝基21,22苯二甲酸为起始原料,经酯化、氯化、Curtis 重排、取代、还原、两步环合、酯基碱水解、酯化、转晶共10步反应,制备得到目标化合物的合成路线。
结果与结论制备得到目标化合物,与文献报道的合成路线相比,反应步骤简化,还原反应有改进。
经红外、粉末X 2射线衍射及热分析,证明产物晶型为C 晶型。
关键词:药物化学;制备;工艺研究;坎地沙坦西来替昔酯中图分类号:R91415 文献标识码:A 坎地沙坦西来替昔酯(candesartan cilexitil ,TCV 2116)简称坎地沙坦酯,是由日本武田药品公司研制开发的一种选择性血管紧张素Ⅱ21型(Ang Ⅱ21)受体拮抗剂,已在瑞士上市。
本品具有强效、作用持续时间长、生物利用度好以及不受食物影响等特点。
1 合成路线坎地沙坦酯的合成已有文献报道[1~3],文献[1,2]中是以32硝基21,22苯二甲酸为起始原料,经酯化、氯化、Curtis 重排得到中间体4,该中间体在氢化钠存在下与42(22氰基苯基)212溴甲苯(5)发生取代反应,产物6经还原、环合及酯基水解得到中间体10,三苯氯甲烷作为保护剂对10的四氮唑环1位氮进行保护后,在碳酸钾存在下,采用12碘乙基环己基碳酸酯为烃化剂进行酯化反应,最后脱去N 2保护基而得到目标产物坎地沙坦酯。
氟伐他汀钠缓释片

【注意事项】
肝功能
某些他汀类药物有致死性或非致死性肝功能衰竭的上市后报告,其中包括氟伐他汀钠。尽管此类肝功能衰竭尚无法确认与本品的因果关系,但仍建议患者应报告一切与肝功能衰竭有关的潜在症状或体征(如:恶心、呕吐、食欲降低、黄疸、肝功能损伤、皮肤易破损及出血)。如现在以上症状因考虑停药。
和其他降脂药物一样,所有患者要在开始服用药物之前及开始治疗后第12周或者剂量增加前进行肝功能检测,并在治疗期间定期监测肝功能。
慎用于有肝脏疾病或大量饮酒的患者。
骨骼肌
服用其他HMG-CoA还原酶抑制剂的患者有发生肌病(包括肌炎和横纹肌溶解症)的报告。
使用氟伐他汀很少有肌病的报道.肌炎和横纹肌溶解的报道极为罕见。如出现不明原因的弥漫性肌肉疼痛,触痛或无力和/或明显的肌酸激酶(CK)水平升高要考虑肌病肌炎或横纹肌溶解。因此应该告知患者出现上述情况要立及报告,特别是伴有无力或发热,无论是否确诊出现肌肉相关疾病,只要CK水平显著升高,则应停止氟伐他汀治疗。
治疗过程中
如果在接受氟伐他汀治疗的患者中出现肌肉相关的症状如疼痛,无力或痉挛,应该测定CK水平如果CK水平明显升高(超过正常上限5倍)应该停止治疗。
如果出现严重的肌肉症状导致日常生活不适,即使CK水平小于等于正常上限5倍,也应该考虑停止治疗。
如果症状缓解,CK水平恢复正常,可以考虑在密切监测下重新使用最低剂量氟伐他汀或其他他汀类药物。
Pimecrolimus_SDS_MedChemExpress

Inhibitors, Agonists, Screening LibrariesSafety Data Sheet Revision Date:May-24-2017Print Date:May-24-20171. PRODUCT AND COMPANY IDENTIFICATION1.1 Product identifierProduct name :PimecrolimusCatalog No. :HY-13723CAS No. :137071-32-01.2 Relevant identified uses of the substance or mixture and uses advised againstIdentified uses :Laboratory chemicals, manufacture of substances.1.3 Details of the supplier of the safety data sheetCompany:MedChemExpress USATel:609-228-6898Fax:609-228-5909E-mail:sales@1.4 Emergency telephone numberEmergency Phone #:609-228-68982. HAZARDS IDENTIFICATION2.1 Classification of the substance or mixtureGHS Classification in accordance with 29 CFR 1910 (OSHA HCS)Acute toxicity, Oral (Category 4),H302Acute aquatic toxicity (Category 1),H400Chronic aquatic toxicity (Category 1),H4102.2 GHS Label elements, including precautionary statementsPictogramSignal word WarningHazard statement(s)H302 Harmful if swallowed.H410 Very toxic to aquatic life with long lasting effects.Precautionary statement(s)P264 Wash skin thoroughly after handling.P270 Do not eat, drink or smoke when using this product.P273 Avoid release to the environment.P301 + P312 IF SWALLOWED: Call a POISON CENTER or doctor/ physician if you feel unwell.P330 Rinse mouth.P391 Collect spillage.P501 Dispose of contents/ container to an approved waste disposal plant.2.3 Other hazardsNone.3. COMPOSITION/INFORMATION ON INGREDIENTS3.1 SubstancesSynonyms:SDZ⁻ASM 981Formula:C43H68ClNO11Molecular Weight:810.45CAS No. :137071-32-04. FIRST AID MEASURES4.1 Description of first aid measuresEye contactRemove any contact lenses, locate eye-wash station, and flush eyes immediately with large amounts of water. Separate eyelids with fingers to ensure adequate flushing. Promptly call a physician.Skin contactRinse skin thoroughly with large amounts of water. Remove contaminated clothing and shoes and call a physician.InhalationImmediately relocate self or casualty to fresh air. If breathing is difficult, give cardiopulmonary resuscitation (CPR). Avoid mouth-to-mouth resuscitation.IngestionWash out mouth with water; Do NOT induce vomiting; call a physician.4.2 Most important symptoms and effects, both acute and delayedThe most important known symptoms and effects are described in the labelling (see section 2.2).4.3 Indication of any immediate medical attention and special treatment neededTreat symptomatically.5. FIRE FIGHTING MEASURES5.1 Extinguishing mediaSuitable extinguishing mediaUse water spray, dry chemical, foam, and carbon dioxide fire extinguisher.5.2 Special hazards arising from the substance or mixtureDuring combustion, may emit irritant fumes.5.3 Advice for firefightersWear self-contained breathing apparatus and protective clothing.6. ACCIDENTAL RELEASE MEASURES6.1 Personal precautions, protective equipment and emergency proceduresUse full personal protective equipment. Avoid breathing vapors, mist, dust or gas. Ensure adequate ventilation. Evacuate personnel to safe areas.Refer to protective measures listed in sections 8.6.2 Environmental precautionsTry to prevent further leakage or spillage. Keep the product away from drains or water courses.6.3 Methods and materials for containment and cleaning upAbsorb solutions with finely-powdered liquid-binding material (diatomite, universal binders); Decontaminate surfaces and equipment by scrubbing with alcohol; Dispose of contaminated material according to Section 13.7. HANDLING AND STORAGE7.1 Precautions for safe handlingAvoid inhalation, contact with eyes and skin. Avoid dust and aerosol formation. Use only in areas with appropriate exhaust ventilation.7.2 Conditions for safe storage, including any incompatibilitiesKeep container tightly sealed in cool, well-ventilated area. Keep away from direct sunlight and sources of ignition.Recommended storage temperature:Powder-20°C 3 years4°C 2 yearsIn solvent-80°C 6 months-20°C 1 monthShipping at room temperature if less than 2 weeks.7.3 Specific end use(s)No data available.8. EXPOSURE CONTROLS/PERSONAL PROTECTION8.1 Control parametersComponents with workplace control parametersThis product contains no substances with occupational exposure limit values.8.2 Exposure controlsEngineering controlsEnsure adequate ventilation. Provide accessible safety shower and eye wash station.Personal protective equipmentEye protection Safety goggles with side-shields.Hand protection Protective gloves.Skin and body protection Impervious clothing.Respiratory protection Suitable respirator.Environmental exposure controls Keep the product away from drains, water courses or the soil. Cleanspillages in a safe way as soon as possible.9. PHYSICAL AND CHEMICAL PROPERTIES9.1 Information on basic physical and chemical propertiesAppearance White to off-white (Solid)Odor No data availableOdor threshold No data availablepH No data availableMelting/freezing point No data availableBoiling point/range No data availableFlash point No data availableEvaporation rate No data availableFlammability (solid, gas)No data availableUpper/lower flammability or explosive limits No data availableVapor pressure No data availableVapor density No data availableRelative density No data availableWater Solubility No data availablePartition coefficient No data availableAuto-ignition temperature No data availableDecomposition temperature No data availableViscosity No data availableExplosive properties No data availableOxidizing properties No data available9.2 Other safety informationNo data available.10. STABILITY AND REACTIVITY10.1 ReactivityNo data available.10.2 Chemical stabilityStable under recommended storage conditions.10.3 Possibility of hazardous reactionsNo data available.10.4 Conditions to avoidNo data available.10.5 Incompatible materialsStrong acids/alkalis, strong oxidising/reducing agents.10.6 Hazardous decomposition productsUnder fire conditions, may decompose and emit toxic fumes.Other decomposition products - no data available.11.TOXICOLOGICAL INFORMATION11.1 Information on toxicological effectsAcute toxicityClassified based on available data. For more details, see section 2Skin corrosion/irritationClassified based on available data. For more details, see section 2Serious eye damage/irritationClassified based on available data. For more details, see section 2Respiratory or skin sensitizationClassified based on available data. For more details, see section 2Germ cell mutagenicityClassified based on available data. For more details, see section 2CarcinogenicityIARC: No component of this product present at a level equal to or greater than 0.1% is identified as probable, possible or confirmed human carcinogen by IARC.ACGIH: No component of this product present at a level equal to or greater than 0.1% is identified as a potential or confirmed carcinogen by ACGIH.NTP: No component of this product present at a level equal to or greater than 0.1% is identified as a anticipated or confirmed carcinogen by NTP.OSHA: No component of this product present at a level equal to or greater than 0.1% is identified as a potential or confirmed carcinogen by OSHA.Reproductive toxicityClassified based on available data. For more details, see section 2Specific target organ toxicity - single exposureClassified based on available data. For more details, see section 2Specific target organ toxicity - repeated exposureClassified based on available data. For more details, see section 2Aspiration hazardClassified based on available data. For more details, see section 212. ECOLOGICAL INFORMATION12.1 ToxicityNo data available.12.2 Persistence and degradabilityNo data available.12.3 Bioaccumlative potentialNo data available.12.4 Mobility in soilNo data available.12.5 Results of PBT and vPvB assessmentPBT/vPvB assessment unavailable as chemical safety assessment not required or not conducted.12.6 Other adverse effectsNo data available.13. DISPOSAL CONSIDERATIONS13.1 Waste treatment methodsProductDispose substance in accordance with prevailing country, federal, state and local regulations.Contaminated packagingConduct recycling or disposal in accordance with prevailing country, federal, state and local regulations.14. TRANSPORT INFORMATIONDOT (US)This substance is considered to be non-hazardous for transport.IMDGUN number: 3077Class: 9Packing group: IIIEMS-No: F-A, S-FProper shipping name: ENVIRONMENTALLY HAZARDOUS SUBSTANCE, SOLID, N.O.S.Marine pollutant: Marine pollutant.IATAUN number: 3077Class: 9Packing group: IIIProper shipping name: Environmentally hazardous substance, solid, n.o.s.15. REGULATORY INFORMATIONSARA 302 Components:No chemicals in this material are subject to the reporting requirements of SARA Title III, Section 302.SARA 313 Components:This material does not contain any chemical components with known CAS numbers that exceed the threshold (De Minimis) reporting levels established by SARA Title III, Section 313.SARA 311/312 Hazards:No SARA Hazards.Massachusetts Right To Know Components:No components are subject to the Massachusetts Right to Know Act.Pennsylvania Right To Know Components:No components are subject to the Pennsylvania Right to Know Act.New Jersey Right To Know Components:No components are subject to the New Jersey Right to Know Act.California Prop. 65 Components:This product does not contain any chemicals known to State of California to cause cancer, birth defects, or anyother reproductive harm.16. OTHER INFORMATIONCopyright 2017 MedChemExpress. The above information is correct to the best of our present knowledge but does not purport to be all inclusive and should be used only as a guide. The product is for research use only and for experienced personnel. It must only be handled by suitably qualified experienced scientists in appropriately equipped and authorized facilities. The burden of safe use of this material rests entirely with the user. MedChemExpress disclaims all liability for any damage resulting from handling or from contact with this product.Caution: Product has not been fully validated for medical applications. For research use only.Tel: 609-228-6898 Fax: 609-228-5909 E-mail: tech@Address: 1 Deer Park Dr, Suite Q, Monmouth Junction, NJ 08852, USA。
比伐卢定简介

比伐卢定旳作用机制
比伐卢定不与血浆蛋白,红细胞结合,不与P450作用, 在血浆中游离存在,静脉注射后5min能够达峰。以浓度方 式延长血清中旳活化部分凝血酶时间(aPPT)、凝血时间 (TT)、凝血酶原时间(PT)。血清中游离旳及血栓中结合 旳凝血酶均能被克制,不受血小板释放物质旳影响。进入 人体内被蛋白酶清除,经肾脏排出,在肾功能正常状体下 半衰期为25min。
比伐卢定-----进口品未进国内,深圳信立泰产品将于今年年底上 市,单纯抗IIa因子克制剂,主推PCI手术
比伐卢定旳作用机制
活性部位
活性部位 N
C
结合部位
结合部位
凝血酶
活性部位
N
C
结合部位
直接旳、 特异旳、 可逆性克制凝血酶(Ⅱa)
Maraganore JM ,etc . Biochemistry ,1990 ,29 (30) :7095.
PCI
PPI
比伐卢定 旳利用
急性心肌梗死(AMI) HIT:血小板降低症
VBT:管内放射手术
ห้องสมุดไป่ตู้
比伐卢定旳作用机制
因凝血酶可水解本品多肽顺序中 Arg3 和 Pro4 之间旳 肽键 ,使本品失活 ,所以本品对凝血酶旳克制作用是可逆而 短暂旳。
Phe Pro Arg Pro Gly Gly Gly Gly Ans Gly
Glu Ile Glu Glu Phe Asp Gly Asn Glu Try Leu Maraganore JM ,etc . Biochemistry ,1990 ,29 (30) :7095.
比伐卢定旳理化性质
中文名:比伐卢定 英文名称:bivalirudin, AngiomaxTM(Medicines 企业) 抗凝成份:一种20肽旳水蛭素衍生片段,分子量: 2180,剂型:注射剂
匹伐他汀钙的合成与表征
匹伐他汀钙的合成与表征匹伐他汀钙(Pitavastatin Calcium),作为羟甲基戊二酸单酰辅酶A(HMG-CoA)还原酶抑制剂,用于临床治疗高脂血症,于1999年11月在日本注册,在美国进行Ⅱ期临床试验。
它不仅具有其它他汀类药物的优点,而且起效时间更短、用药剂量更低,副作用更小,耐受性更好,具有良好的市场前景。
匹伐他汀钙已被列入全球18种销售潜力最大的新药,有专家预言,该药与罗伐他汀一道将成为未来几年内引领他汀类药物市场的两种主要药物。
目前,匹伐他汀钙开发存在的主要问题是:结构复杂,合成难度大和合成成本高,国内还没有匹伐他汀钙的工业化生产工艺。
因此,开发高效率、低成本、低污染的合成工艺十分必要。
综合文献报道,匹伐他汀钙的合成方法主要有外消旋体拆分法、手性试剂法及其它方法。
手性试剂法的缺陷是侧链合成难度大;其它方法中要用到昂贵的试剂,成本高;本论文研究采用外消旋体拆分法合成匹伐他汀钙,选择外消旋体拆分法的优点是其工艺条件可控性强,操作简便。
为了保证最后产品的质量,本论文运用HPLC法对起始原料中的Z式异构体杂质进行了限量控制研究。
研究结果表明,原料中的E式烯键在光(紫外线)照射下转变成能量较高的不稳定异构体(Z式),但受热后(浓缩成固体过程)又回复到热力学稳定的E式异构体。
在匹伐他汀钙及其中间体的合成过程中,考察了反应溶剂、物料的摩尔配比、重结晶溶剂及手性拆分剂对反应结果的影响,优选出的较佳工艺条件为:以3-(2′-环丙基-4′-(4〞-氟苯基)-喹啉3′-基)-丙烯醛为起始原料,在氢化钠/正丁基锂催化下与乙酰乙酸乙酯进行缩合得到中间体3;以四氢呋喃-甲醇做溶剂,物料的摩尔比:中间体3:二乙基甲氧基硼:硼氢化钠=1:1.25:1.34,温度:-70℃的条件下合成了中间体4,收率98.0%;中间体4经氢氧化钠水解,盐酸中和后得到游离酸,再用D(+)-a-甲基苄胺拆分,形成了复盐6。
当摩尔比:中间体4:D(+)-a-甲基苄胺=1:1.25,用乙醇与甲基异丁基酮的混合溶剂结晶时,收率较高为29.2%;最后复盐6在水溶液中用氢氧化钠成钠盐再与氯化钙作用,一步合成了匹伐他汀钙。
降钙素杂质列表-杂质对照品

降钙素杂质列表-杂质对照品杂质标准品降钙素杂质――孟成科技(上海)有限公司名称信息结构式降钙素杂质Calcitonin Impurity分子式/Molecular Formula :C136H231N43O46S2分子量/Molecular Weight :3268.72降钙素杂质Calcitonin Impurity 分子式/Molecular Formula :C138H233N43O47S2分子量/Molecular Weight :3310.76降钙素杂质Calcitonin Impurity 分子式/Molecular Formula :C147H242N44O49S2分子量/Molecular Weight :3473.93降钙素杂质Calcitonin Impurity 分子式/Molecular Formula :NA分子量/Molecular Weight :3429.70降钙素杂质Calcitonin Impurity 分子式/Molecular Formula :NA分子量/Molecular Weight :3471.72杂质标准品降钙素杂质Calcitonin Impurity 分子式/Molecular Formula: NA分子量/Molecular Weight:3430.70降钙素杂质Calcitonin Impurity 分子式/Molecular Formula: NA分子量/Molecular Weight:3430.70降钙素杂质Calcitonin Impurity 分子式/Molecular Formula: NA分子量/Molecular Weight:3232.60感谢您的阅读,祝您生活愉快。
莽草酸脱氢酶(SD)活性检测试剂盒说明书__紫外分光光度法UPLC-MS-4468

莽草酸脱氢酶(SD)活性检测试剂盒说明书货号:UPLC-MS-4468规格:50T/48S紫外分光光度法产品组成:使用前请认真核对试剂体积与瓶内体积是否一致,有疑问请及时联系工作人员。
试剂名称规格保存条件提取液液体60mL×1瓶4℃保存试剂一液体20mL×1瓶4℃保存试剂二粉剂×1瓶4℃保存试剂三粉剂×2瓶-20℃保存溶液的配制:1、提取液:内含不溶物,用前摇匀。
2、试剂二:临用前加入10mL蒸馏水溶解。
3、试剂三:临用前每瓶加入11mL蒸馏水溶解。
4、工作液的配制:根据用量按照试剂一:试剂二:试剂三为7:4:8的体积比例充分混匀,现用现配,用前25℃预热15min。
产品说明:莽草酸途径是存在于植物和微生物中的一条重要的代谢途径,莽草酸脱氢酶(EC1.1.1.25)是莽草酸合成代谢途径中催化第四步反应的关键酶。
莽草酸脱氢酶催化莽草酸和NADP产生NADPH,检测340nm下的吸光值增加速率来表示SD活性。
注意:实验之前建议选择2-3个预期差异大的样本做预实验。
如果样本吸光值不在测量范围内建议稀释或者增加样本量进行检测。
需自备的仪器和用品:紫外分光光度计、台式离心机、水浴锅、1mL石英比色皿、可调式移液枪、研钵/匀浆器、冰和蒸馏水。
操作步骤:一、样本处理(可适当调整待测样本量,具体比例可以参考文献)1、组织:按照组织质量(g):提取液体积(mL)为1:5~10的比例(建议称取约0.1g组织,加入1mL提取液(加入前摇匀))进行冰浴匀浆,然后8000g,4℃,离心10min,取上清置于冰上待测。
2、细胞:先收集细菌或细胞到离心管内,离心后弃上清;按照细胞数量(104个):提取液体积(mL)为500~1000:1的比例(建议500万细胞加入1mL提取液),冰浴超声波破碎细胞(功率300w,超声3秒,间隔7秒,总时间3min);然后8000g,4℃,离心10min,取上清置于冰上待测。
Pitavastatin Calcium_CAS号147526-32-7说明书_AbMole中国
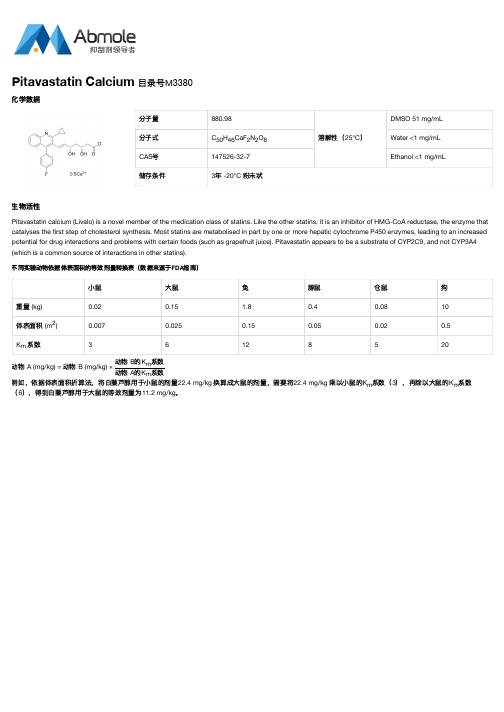
分子量880.98溶解性(25°C )DMSO 51 mg/mL 分子式C H CaF N O Water <1 mg/mL CAS 号147526-32-7Ethanol <1 mg/mL储存条件3年 -20°C 粉末状生物活性Pitavastatin calcium (Livalo) is a novel member of the medication class of statins. Like the other statins, it is an inhibitor of HMG-CoA reductase, the enzyme that catalyses the first step of cholesterol synthesis. Most statins are metabolised in part by one or more hepatic cytochrome P450 enzymes, leading to an increased potential for drug interactions and problems with certain foods (such as grapefruit juice). Pitavastatin appears to be a substrate of CYP2C9, and not CYP3A4(which is a common source of interactions in other statins).不同实验动物依据体表面积的等效剂量转换表(数据来源于FDA 指南)小鼠大鼠兔豚鼠仓鼠狗重量 (kg)0.020.15 1.80.40.0810体表面积 (m )0.0070.0250.150.050.020.5K 系数36128520动物 A (mg/kg) = 动物 B (mg/kg) ×动物 B 的K 系数动物 A 的K 系数例如,依据体表面积折算法,将白藜芦醇用于小鼠的剂量22.4 mg/kg 换算成大鼠的剂量,需要将22.4 mg/kg 乘以小鼠的K 系数(3),再除以大鼠的K 系数(6),得到白藜芦醇用于大鼠的等效剂量为11.2 mg/kg 。
匹伐他汀钙药品说明书(英文)

HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use LIVALO® safely and effectively. See full prescribing information for LIVALO.LIVALO (pitavastatin) Tablet, Film Coated for Oral useInitial U.S. Approval: 2009RECENT MAJOR CHANGESDosage and AdministrationDosage in Patients with Renal Impairment (2.2) 8/2011INDICATIONS AND USAGELIVALO is a HMG-CoA reductase inhibitor indicated for:•Patients with primary hyperlipidemia or mixed dyslipidemia as an adjunctive therapy to diet to reduce elevated total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), apolipoprotein B (Apo B), triglycerides (TG), and to increase high-density lipoprotein cholesterol (HDL-C) (1.1)Limitations of Use (1.2):•Doses of LIVALO greater than 4 mg once daily were associated with an increased risk for severe myopathy in premarketing clinical studies. Do not exceed 4 mg once daily dosing of LIVALO.•The effect of LIVALO on cardiovascular morbidity and mortality has not been determined.•LIVALO has not been studied in Fredrickson Type I, III, and V dyslipidemias.DOSAGE AND ADMINISTRATION•LIVALO can be taken with or without food, at any time of day (2.1) Dose Range: 1 mg to 4 mg once daily (2.1)•Primary hyperlipidemia and mixed dyslipidemia: Starting dose 2 mg. When lowering of LDL-C is insufficient, the dosage may be increased to a maximum of 4 mg per day. (2.1)•Moderate and severe renal impairment (glomerular filtration rate 30 –59 and 15 - 29 mL/min/1.73 m2, respectively) as well as end-stage renal disease on hemodialysis: Starting dose of 1 mg once daily and maximum dose of 2 mg once daily (2.2)DOSAGE FORMS AND STRENGTHS•Tablets: 1 mg, 2 mg, and 4 mg (3)CONTRAINDICATIONS•Known hypersensitivity to product components (4)•Active liver disease, which may include unexplained persistent elevations in hepatic transaminase levels (4)•Women who are pregnant or may become pregnant (4, 8.1)•Nursing mothers (4, 8.3)•Co-administration with cyclosporine (4, 7.1, 12.3)WARNINGS AND PRECAUTIONS•Skeletal muscle effects (e.g., myopathy and rhabdomyolysis): Risks increase in a dose-dependent manner, with advanced age (≥65), renal impairment, and inadequately treated hypothyroidism. Advise patientsto promptly report report unexplained and/or persistent muscle pain, tenderness, or weakness, and discontinue LIVALO (5.1)•Liver enzyme abnormalities : Persistent elevations in hepatic transaminases can occur. Check liver enzyme tests before initiating therapy and as clinically indicated thereafter (5.2)ADVERSE REACTIONSThe most frequent adverse reactions (rate ≥2.0% in at least one marketed dose) were myalgia, back pain, diarrhea, constipation and pain in extremity. (6)To report SUSPECTED ADVERSE REACTIONS, contact Kowa Pharmaceuticals America, Inc. at 1-877-334-3464 or FDA at 1-800-FDA-1088 or /medwatch.To report SUSPECTED ADVERSE REACTIONS, contact at or FDA at 1-800-FDA-1088 or /medwatchDRUG INTERACTIONS•Erythromycin: Combination increases pitavastatin exposure. Limit LIVALO to 1 mg once daily (2.3, 7.2)•Rifampin: Combination increases pitavastatin exposure. Limit LIVALO to 2 mg once daily (2.4, 7.3)•Concomitant lipid-lowering therapies : Use with fibrates or lipid-modifying doses (≥1 g/day) of niacin increases the risk of adverse skeletal muscle effects. Caution should be used when prescribing with LIVALO. (5.1, 7.4, 7.5)USE IN SPECIFIC POPULATIONS•Pediatric use: Safety and effectiveness have not been established. (8.4)•Renal impairment: Limitation of a starting dose of LIVALO 1 mg once daily and a maximum dose of LIVALO 2 mg once daily for patientswith moderate and severe renal impairment as well as patients receiving hemodialysis (2.2, 8.6)See 17 for PATIENT COUNSELING INFORMATIONRevised: 11/2012FULL PRESCRIBING INFORMATION: CONTENTS *1 INDICATIONS AND USAGE1.1 Primary Hyperlipidemia and Mixed Dyslipidemia1.2 Limitations of Use2 DOSAGE AND ADMINISTRATION2.1 General Dosing Information2.2 Dosage in Patients with Renal Impairment2.3 Use with Erythromycin2.4 Use with Rifampin3 DOSAGE FORMS AND STRENGTHS4 CONTRAINDICATIONS5 WARNINGS AND PRECAUTIONS5.1 Skeletal Muscle Effects5.2 Liver Enzyme Abnormalities5.3 Endocrine Function6 ADVERSE REACTIONS6.1 Clinical Studies Experience6.2 Postmarketing Experience:7 DRUG INTERACTIONS7.1 Cyclosporine7.2 Erythromycin7.3 Rifampin7.4 Gemfibrozil7.5 Other Fibrates7.6 Niacin7.7 Warfarin8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.3 Nursing Mothers8.4 Pediatric Use8.5 Geriatric Use8.6 Renal Impairment8.7 Hepatic Impairment10 OVERDOSAGE11 DESCRIPTION12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.2 Pharmacodynamics12.3 Pharmacokinetics13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility13.2 Animal Toxicology and/or Pharmacology14 CLINICAL STUDIES14.1 Primary Hyperlipidemia or Mixed Dyslipidemia16 HOW SUPPLIED/STORAGE AND HANDLING17 PATIENT COUNSELING INFORMATION17.1 Dosing Time17.2 Muscle Pain17.3 Pregnancy17.4 Breastfeeding17.5 Liver Enzymes* Sections or subsections omitted from the full prescribing information are not listedFULL PRESCRIBING INFORMATION1 INDICATIONS AND USAGEDrug therapy should be one component of multiple-risk-factor intervention in individuals who require modifications of their lipid profile. Lipid-altering agents should be used in addition to a diet restricted in saturated fat and cholesterol only when the response to diet and other nonpharmacological measures has been inadequate.1.1 Primary Hyperlipidemia and Mixed DyslipidemiaLIVALO® is indicated as an adjunctive therapy to diet to reduce elevated total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), apolipoprotein B (Apo B), triglycerides (TG), and to increase HDL-C in adult patients with primary hyperlipidemia or mixed dyslipidemia.1.2 Limitations of UseDoses of LIVALO greater than 4 mg once daily were associated with an increased risk for severe myopathy in premarketing clinical studies. Do not exceed 4 mg once daily dosing of LIVALO.The effect of LIVALO on cardiovascular morbidity and mortality has not been determined.LIVALO has not been studied in Fredrickson Type I, III, and V dyslipidemias.2 DOSAGE AND ADMINISTRATION2.1 General Dosing InformationThe dose range for LIVALO is 1 to 4 mg orally once daily at any time of the day with or without food. The recommended starting dose is 2 mg and the maximum dose is 4 mg. The starting dose and maintenance doses of LIVALO should be individualized according to patient characteristics, such as goal of therapy and response.After initiation or upon titration of LIVALO, lipid levels should be analyzed after 4 weeks and the dosage adjusted accordingly.2.2 Dosage in Patients with Renal ImpairmentPatients with moderate and severe renal impairment (glomerular filtration rate 30 – 59 mL/min/1.73 m2 and 15 – 29 mL/min/1.73 m2 not receiving hemodialysis, respectively) as well as end-stage renal disease receiving hemodialysis should receive a starting dose of LIVALO 1 mg once daily and a maximum dose of LIVALO 2 mg once daily.2.3 Use with ErythromycinIn patients taking erythromycin, a dose of LIVALO 1 mg once daily should not be exceeded [see Drug Interactions (7.2)].2.4 Use with RifampinIn patients taking rifampin, a dose of LIVALO 2 mg once daily should not be exceeded [see Drug Interactions (7.3)].3 DOSAGE FORMS AND STRENGTHS1 mg: Round white film-coated tablet. Debossed “KC” on one side and “1” on the other side of the tablet.2 mg: Round white film-coated tablet. Debossed “KC” on one side and “2” on the other side of the tablet.4 mg: Round white film-coated tablet. Debossed “KC” on one side and “4” on the other side of the tablet.4 CONTRAINDICATIONSThe use of LIVALO is contraindicated in the following conditions:•Patients with a known hypersensitivity to any component of this product. Hypersensitivity reactions including rash, pruritus, and urticaria have been reported with LIVALO [see Adverse Reactions (6.1)].•Patients with active liver disease which may include unexplained persistent elevations of hepatic transaminase levels [see Warnings and Precautions (5.2), Use in Specific Populations (8.7)].•Women who are pregnant or may become pregnant. Because HMG-CoA reductase inhibitors decrease cholesterol synthesis and possibly the synthesis of other biologically active substances derived from cholesterol, LIVALO may cause fetal harm when administered to pregnant women. Additionally, there is no apparent benefit to therapy during pregnancy, and safety in pregnant women has not been established. If the patient becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to the fetus and the lack of known clinical benefit with continued use during pregnancy [see Use in Specific Populations (8.1) and Nonclinical Toxicology (13.2)].•Nursing mothers. Animal studies have shown that LIVALO passes into breast milk. Since HMG-CoA reductase inhibitorshave the potential to cause serious adverse reactions in nursing infants, LIVALO, like other HMG-CoA reductase inhibitors, is contraindicated in pregnant or nursing mothers [see Use in Specific Populations (8.3) and Nonclinical Toxicology (13.2)].•Co-administration with cyclosporine [see Drug Interactions (7.1) and Clinical Pharmacology (12.3)].5 WARNINGS AND PRECAUTIONS5.1 Skeletal Muscle EffectsCases of myopathy and rhabdomyolysis with acute renal failure secondary to myoglobinuria have been reported with HMG-CoA reductase inhibitors, including LIVALO. These risks can occur at any dose level, but increase in a dose-dependent manner. LIVALO should be prescribed with caution in patients with predisposing factors for myopathy. These factors include advanced age (≥65 years), renal impairment, and inadequately treated hypothyroidism. The risk of myopathy may also be increased with concurrent administration of fibrates or lipid-modifying doses of niacin. LIVALO should be administered with caution in patients with impaired renal function, in elderly patients, or when used concomitantly with fibrates or lipid-modifying doses of niacin [see Drug Interactions (7.6), Use in Specific Populations (8.5, 8.6) and Clinical Pharmacology (12.3)].There have been rare reports of immune-mediated necrotizing myopathy (IMNM), an autoimmune myopathy, associated withstatin use. IMNM is characterized by: proximal muscle weakness and elevated serum creatine kinase, which persist despite discontinuation of statin treatment; muscle biopsy showing necrotizing myopathy without significant inflammation; improvement with immunosuppressive agents.LIVALO therapy should be discontinued if markedly elevated creatine kinase (CK) levels occur or myopathy is diagnosed or suspected. LIVALO therapy should also be temporarily withheld in any patient with an acute, serious condition suggestive of myopathy or predisposing to the development of renal failure secondary to rhabdomyolysis (e.g., sepsis, hypotension, dehydration, major surgery, trauma, severe metabolic, endocrine, and electrolyte disorders, or uncontrolled seizures). All patients should be advised to promptly report unexplained muscle pain, tenderness, or weakness, particularly if accompanied by malaise or fever or if muscle signs and symptoms persist after discontinuing LIVALO.5.2 Liver Enzyme AbnormalitiesIncreases in serum transaminases (aspartate aminotransferase [AST]/serum glutamic-oxaloacetic transaminase, or alanine aminotransferase [ALT]/serum glutamic-pyruvic transaminase) have been reported with HMG-CoA reductase inhibitors, including LIVALO. In most cases, the elevations were transient and resolved or improved on continued therapy or after a brief interruption in therapy.In placebo-controlled Phase 2 studies, ALT >3 times the upper limit of normal was not observed in the placebo, LIVALO 1 mg, or LIVALO 2 mg groups. One out of 202 patients (0.5%) administered LIVALO 4 mg had ALT >3 times the upper limit of normal.It is recommended that liver enzyme tests be performed before the initiation of LIVALO and if signs or symptoms of liver injury occur.There have been rare postmarketing reports of fatal and non-fatal hepatic failure in patients taking statins, including pitavastatin. If serious liver injury with clinical symptoms and/or hyperbilirubinemia or jaundice occurs during treatment with LIVALO, promptly interrupt therapy. If an alternate etiology is not found do not restart LIVALO.As with other HMG-CoA reductase inhibitors, LIVALO should be used with caution in patients who consume substantial quantities of alcohol. Active liver disease, which may include unexplained persistent transaminase elevations, is a contraindication to the use of LIVALO [see Contraindications (4)].5.3 Endocrine FunctionIncreases in HbA1c and fasting serum glucose levels have been reported with HMG-CoA reductase inhibitors, including LIVALO.6 ADVERSE REACTIONSThe following serious adverse reactions are discussed in greater detail in other sections of the label:•Rhabdomyolysis with myoglobinuria and acute renal failure and myopathy (including myositis) [see Warnings and Precautions (5.1)].•Liver Enzyme Abnormalities [see Warning and Precautions (5.2)].Of 4,798 patients enrolled in 10 controlled clinical studies and 4 subsequent open-label extension studies, 3,291 patients were administered pitavastatin 1 mg to 4 mg daily. The mean continuous exposure of pitavastatin (1 mg to 4 mg) was 36.7 weeks (median 51.1 weeks). The mean age of the patients was 60.9 years (range; 18 years – 89 years) and the gender distribution was 48% males and 52% females. Approximately 93% of the patients were Caucasian, 7% were Asian/Indian, 0.2% were African American and 0.3% were Hispanic and other.6.1 Clinical Studies ExperienceBecause clinical studies on LIVALO are conducted in varying study populations and study designs, the frequency of adverse reactions observed in the clinical studies of LIVALO cannot be directly compared with that in the clinical studies of other HMG-CoA reductase inhibitors and may not reflect the frequency of adverse reactions observed in clinical practice.Adverse reactions reported in ≥ 2% of patients in controlled clinical studies and at a rate greater than or equal to placebo are shown in Table 1. These studies had treatment duration of up to 12 weeks.Table 1. Adverse Reactions* Reported by ≥2.0% of Patients Treated with LIVALO and > Placebo in Short-Term Controlled StudiesAdverse Reactions* PlaceboN= 208LIVALO1 mgN=309LIVALO2 mgN=951LIVALO4 mgN=1540Back Pain 2.9% 3.9% 1.8% 1.4% Constipation 1.9% 3.6% 1.5% 2.2% Diarrhea 1.9% 2.6% 1.5% 1.9%Myalgia 1.4% 1.9% 2.8% 3.1%Pain in extremity 1.9% 2.3% 0.6% 0.9%* Adverse reactions by MedDRA preferred term.Other adverse reactions reported from clinical studies were arthralgia, headache, influenza, and nasopharyngitis.The following laboratory abnormalities have also been reported: elevated creatine phosphokinase, transaminases, alkaline phosphatase, bilirubin, and glucose.In controlled clinical studies and their open-label extensions, 3.9% (1 mg), 3.3% (2 mg), and 3.7% (4 mg) of pitavastatin-treated patients were discontinued due to adverse reactions. The most common adverse reactions that led to treatment discontinuation were: elevated creatine phosphokinase (0.6% on 4 mg) and myalgia (0.5% on 4 mg).Hypersensitivity reactions including rash, pruritus, and urticaria have been reported with LIVALO.6.2 Postmarketing Experience:The following adverse reactions have been identified during postapproval use of LIVALO. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.Adverse reactions associated with LIVALO therapy reported since market introduction, regardless of causality assessment, include the following: abdominal discomfort, abdominal pain, dyspepsia, nausea, asthenia, fatigue, malaise, hepatitis, jaundice, fatal and non-fatal hepatic failure, dizziness, hypoesthesia, insomnia, depression, interstitial lung disease, erectile dysfunction and muscle spasms. There have been rare postmarketing reports of cognitive impairment (e.g., memory loss, forgetfulness, amnesia, memory impairment, confusion) associated with statin use. These cognitive issues have been reported for all statins. The reports are generally nonserious, and reversible upon statin discontinuation, with variable times to symptom onset (1 day to years) and symptom resolution (median of 3 weeks).There have been rare reports of immune-mediated necrotizing myopathy associated with statin use [see Warnings and Precautions (5.1)].7 DRUG INTERACTIONS7.1 CyclosporineCyclosporine significantly increased pitavastatin exposure. Co-administration of cyclosporine with LIVALO is contraindicated [see Contraindications (4), and Clinical Pharmacology (12.3)].7.2 ErythromycinErythromycin significantly increased pitavastatin exposure. In patients taking erythromycin, a dose of LIVALO 1 mg once daily should not be exceeded [see Dosage and Administration (2.3) and Clinical Pharmacology (12.3)].7.3 RifampinRifampin significantly increased pitavastatin exposure. In patients taking rifampin, a dose of LIVALO 2 mg once daily should not be exceeded [see Dosage and Administration (2.4) and Clinical Pharmacology (12.3)].7.4 GemfibrozilDue to an increased risk of myopathy/rhabdomyolysis when HMG-CoA reductase inhibitors are coadministered with gemfibrozil, concomitant administration of LIVALO with gemfibrozil should be avoided.7.5 Other FibratesBecause it is known that the risk of myopathy during treatment with HMG-CoA reductase inhibitors is increased with concurrent administration of other fibrates, LIVALO should be administered with caution when used concomitantly with other fibrates [see Warnings and Precautions (5.1), and Clinical Pharmacology (12.3)].7.6 NiacinThe risk of skeletal muscle effects may be enhanced when LIVALO is used in combination with niacin; a reduction in LIVALO dosage should be considered in this setting [see Warnings and Precautions (5.1)].7.7 WarfarinLIVALO had no significant pharmacokinetic interaction with R- and S- warfarin. LIVALO had no significant effect on prothrombin time (PT) and international normalized ratio (INR) when administered to patients receiving chronic warfarin treatment [see Clinical Pharmacology (12.3)]. However, patients receiving warfarin should have their PT and INR monitored when pitavastatin is added to their therapy.8 USE IN SPECIFIC POPULATIONS8.1 PregnancyTeratogenic effects: Pregnancy Category XLIVALO is contraindicated in women who are or may become pregnant. Serum cholesterol and TG increase during normal pregnancy, and cholesterol products are essential for fetal development. Atherosclerosis is a chronic process and discontinuationof lipid-lowering drugs during pregnancy should have little impact on long-term outcomes of primary hyperlipidemia therapy [see Contraindications (4)].There are no adequate and well-controlled studies of LIVALO in pregnant women, although, there have been rare reports of congenital anomalies following intrauterine exposure to HMG-CoA reductase inhibitors. In a review of about 100 prospectively followed pregnancies in women exposed to other HMG-CoA reductase inhibitors, the incidences of congenital anomalies, spontaneous abortions, and fetal deaths/stillbirths did not exceed the rate expected in the general population. However, this study was only able to exclude a three-to-four-fold increased risk of congenital anomalies over background incidence. In 89% of these cases, drug treatment started before pregnancy and stopped during the first trimester when pregnancy was identified.Reproductive toxicity studies have shown that pitavastatin crosses the placenta in rats and is found in fetal tissues at ≤36% of maternal plasma concentrations following a single dose of 1 mg/kg/day during gestation.Embryo-fetal developmental studies were conducted in pregnant rats treated with 3, 10, 30 mg/kg/day pitavastatin by oral gavage during organogenesis. No adverse effects were observed at 3 mg/kg/day, systemic exposures 22 times human systemic exposure at 4 mg/day based on AUC.Embryo-fetal developmental studies were conducted in pregnant rabbits treated with 0.1, 0.3, 1 mg/kg/day pitavastatin by oral gavage during the period of fetal organogenesis. Maternal toxicity consisting of reduced body weight and abortion was observed at all doses tested (4 times human systemic exposure at 4 mg/day based on AUC).In perinatal/postnatal studies in pregnant rats given oral gavage doses of pitavastatin at 0.1, 0.3, 1, 3, 10, 30 mg/kg/day from organogenesis through weaning, maternal toxicity consisting of mortality at ≥0.3 mg/kg/day and impaired lactation at all doses contributed to the decreased survival of neonates in all dose groups (0.1 mg/kg/day represents approximately 1 time human systemic exposure at 4 mg/day dose based on AUC).LIVALO may cause fetal harm when administered to a pregnant woman. If the patient becomes pregnant while taking LIVALO,the patient should be apprised of the potential risks to the fetus and the lack of known clinical benefit with continued use during pregnancy.8.3 Nursing MothersIt is not known whether pitavastatin is excreted in human milk, however, it has been shown that a small amount of another drug in this class passes into human milk. Rat studies have shown that pitavastatin is excreted into breast milk. Because another drug in this class passes into human milk and HMG-CoA reductase inhibitors have a potential to cause serious adverse reactions in nursing infants, women who require LIVALO treatment should be advised not to nurse their infants or to discontinue LIVALO [see Contraindications (4)].8.4 Pediatric UseSafety and effectiveness of LIVALO in pediatric patients have not been established.8.5 Geriatric UseOf the 2,800 patients randomized to LIVALO 1 mg to 4 mg in controlled clinical studies, 1,209 (43%) were 65 years and older. No significant differences in efficacy or safety were observed between elderly patients and younger patients. However, greater sensitivity of some older individuals cannot be ruled out.8.6 Renal ImpairmentPatients with moderate and severe renal impairment (glomerular filtration rate 30 – 59 mL/min/1.73 m2 and 15 – 29 mL/min/1.73m2 not receiving hemodialysis, respectively) as well as end-stage renal disease receiving hemodialysis should receive a starting dose of LIVALO 1 mg once daily and a maximum dose of LIVALO 2 mg once daily [see Dosage and Administration (2.2) and Clinical Pharmacology (12.3)].8.7 Hepatic ImpairmentLIVALO is contraindicated in patients with active liver disease which may include unexplained persistent elevations of hepatic transaminase levels.10 OVERDOSAGEThere is no known specific treatment in the event of overdose of pitavastatin. In the event of overdose, the patient should be treated symptomatically and supportive measures instituted as required. Hemodialysis is unlikely to be of benefit due to high protein binding ratio of pitavastatin.11 DESCRIPTIONLIVALO (pitavastatin) is an inhibitor of HMG-CoA reductase. It is a synthetic lipid-lowering agent for oral administration.The chemical name for pitavastatin is (+)monocalcium bis{(3R, 5S, 6E)-7-[2-cyclopropyl-4-(4-fluorophenyl)-3-quinolyl]-3,5-dihydroxy-6-heptenoate}. The structural formula is:The empirical formula for pitavastatin is C50H46CaF2N2O8 and the molecular weight is 880.98. Pitavastatin is odorless and occursas white to pale-yellow powder. It is freely soluble in pyridine, chloroform, dilute hydrochloric acid, and tetrahydrofuran, soluble in ethylene glycol, sparingly soluble in octanol, slightly soluble in methanol, very slightly soluble in water or ethanol, and practically insoluble in acetonitrile or diethyl ether. Pitavastatin is hygroscopic and slightly unstable in light.Each film-coated tablet of LIVALO contains 1.045 mg, 2.09 mg, or 4.18 mg of pitavastatin calcium, which is equivalent to1 mg,2 mg, or 4 mg, respectively of free base and the following inactive ingredients: lactose monohydrate, low substituted hydroxypropylcellulose, hypromellose, magnesium aluminometasilicate, magnesium stearate, and film coating containing the following inactive ingredients: hypromellose, titanium dioxide, triethyl citrate, and colloidal anhydrous silica.12 CLINICAL PHARMACOLOGY12.1 Mechanism of ActionPitavastatin competitively inhibits HMG-CoA reductase, which is a rate-determining enzyme involved with biosynthesis of cholesterol, in a manner of competition with the substrate so that it inhibits cholesterol synthesis in the liver. As a result, the expression of LDL-receptors followed by the uptake of LDL from blood to liver is accelerated and then the plasma TC decreases. Further, the sustained inhibition of cholesterol synthesis in the liver decreases levels of very low density lipoproteins.12.2 PharmacodynamicsIn a randomized, double-blind, placebo-controlled, 4-way parallel, active-comparator study with moxifloxacin in 174 healthy participants, LIVALO was not associated with clinically meaningful prolongation of the QTc interval or heart rate at daily doses up to 16 mg (4 times the recommended maximum daily dose).12.3 PharmacokineticsAbsorption: Pitavastatin peak plasma concentrations are achieved about 1 hour after oral administration. Both C max and AUC0-inf increased in an approximately dose-proportional manner for single LIVALO doses from 1 to 24 mg once daily. The absolute bioavailability of pitavastatin oral solution is 51%. Administration of LIVALO with a high fat meal (50% fat content) decreases pitavastatin C max by 43% but does not significantly reduce pitavastatin AUC. The C max and AUC of pitavastatin did not differ following evening or morning drug administration. In healthy volunteers receiving 4 mg pitavastatin, the percent change from baseline for LDL-C following evening dosing was slightly greater than that following morning dosing. Pitavastatin was absorbed in the small intestine but very little in the colon.Distribution: Pitavastatin is more than 99% protein bound in human plasma, mainly to albumin and alpha 1-acid glycoprotein, and the mean volume of distribution is approximately 148 L. Association of pitavastatin and/or its metabolites with the blood cells is minimal.Metabolism: Pitavastatin is marginally metabolized by CYP2C9 and to a lesser extent by CYP2C8. The major metabolite inhuman plasma is the lactone which is formed via an ester-type pitavastatin glucuronide conjugate by uridine 5'-diphosphate (UDP) glucuronosyltransferase (UGT1A3 and UGT2B7).Excretion: A mean of 15% of radioactivity of orally administered, single 32 mg 14C-labeled pitavastatin dose was excreted in urine, whereas a mean of 79% of the dose was excreted in feces within 7 days. The mean plasma elimination half-life is approximately 12 hours.Race: In pharmacokinetic studies pitavastatin C max and AUC were 21 and 5% lower, respectively in Black or African American healthy volunteers compared with those of Caucasian healthy volunteers. In pharmacokinetic comparison between Caucasian volunteers and Japanese volunteers, there were no significant differences in C max and AUC.Gender: In a pharmacokinetic study which compared healthy male and female volunteers, pitavastatin C max and AUC were 60 and 54% higher, respectively in females. This had no effect on the efficacy or safety of LIVALO in women in clinical studies. Geriatric: In a pharmacokinetic study which compared healthy young and elderly (≥65 years) volunteers, pitavastatin C max and AUC were 10 and 30% higher, respectively, in the elderly. This had no effect on the efficacy or safety of LIVALO in elderly subjects in clinical studies.Renal Impairment: In patients with moderate renal impairment (glomerular filtration rate of 30 – 59 mL/min/1.73 m2) and end stage renal disease receiving hemodialysis, pitavastatin AUC0-inf is 102 and 86% higher than those of healthy volunteers, respectively, while pitavastatin C max is 60 and 40% higher than those of healthy volunteers, respectively. Patients received hemodialysis immediately before pitavastatin dosing and did not undergo hemodialysis during the pharmacokinetic study. Hemodialysis patients have 33 and 36% increases in the mean unbound fraction of pitavastatin as compared to healthy volunteers and patients with moderate renal impairment, respectively.。
培非格司亭中英文介绍

王婕 913103860408NEULASTA(PEGFILGRASTIM)|培非格司亭注射液1.Introduction(简介)【产地英文商品名】:NEULASTA-6mg/0.6ml/Syringe【原产地英文药品名】:PEGFILGRASTIM【中文参考商品译名】:纽拉思塔-6毫克/0.6毫升/支【中文参考药品译名】:培非格司亭【生产厂家中文参考译名】:安进【生产厂家英文名】:Amgen, IncAmgen Announces Novel Drugs for Antitumor Chemotherapy Side Effects of FGT (TM) (pegfilgrastim), a drug developed by the US Food and Drug Administration (FDA), has been approved by the US Food and Drug Administration (FDA) Approval. Amphetamycin, the chief executive of Amgen, says that pemetrexedin will make it easier for healthcare workers to prevent chemotherapy-induced neutropenia and its serious complications.The third drug approved by Amgen in the past six months will significantly improve the prognosis of chemotherapy patients and is expected to enter the market in early April.BUSINESS WIRE 2002年2月1日美国加州THOUSAND OAKS消息,安进公司宣布抗肿瘤化疗副作用新药培非格司亭(TM) (pegfilgrastim)通过美国食品与药品管理局(FDA)的审批。
【安 吡 昔 康】
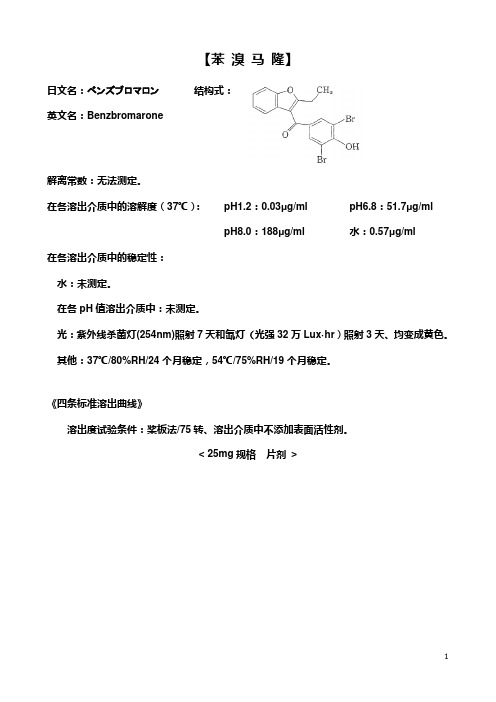
【苯溴马隆】日文名:ベンズブロマロン英文名:Benzbromarone 结构式:解离常数:无法测定。
在各溶出介质中的溶解度(37℃):pH1.2:0.03μg/ml pH6.8:51.7μg/mlpH8.0:188μg/ml 水:0.57μg/ml在各溶出介质中的稳定性:水:未测定。
在各pH值溶出介质中:未测定。
光:紫外线杀菌灯(254nm)照射7天和氙灯(光强32万Lux·hr)照射3天、均变成黄色。
其他:37℃/80%RH/24个月稳定,54℃/75%RH/19个月稳定。
《四条标准溶出曲线》溶出度试验条件:桨板法/75转、溶出介质中不添加表面活性剂。
< 25mg规格片剂>< 50mg规格片剂>《质量标准》取本品,照溶出度测定法(桨板法),以磷酸氢二钠-枸橼酸缓冲液(pH8.0)900ml为溶剂,转速为每分钟75转,依法操作,经45分钟时,取溶液适量滤过,弃去至少10ml初滤液,精密量取续滤液适量,加溶出介质稀释制成每1ml中含11.1μg的溶液,作为供试品溶液。
另精密称取经五氧化二磷干燥剂50℃减压(0.67kPa以下)干燥4小时的对照品56mg,置20ml量瓶中,加乙醇溶解并稀释至刻度,摇匀,精密量取5ml,置100ml量瓶中,加溶出介质稀释至刻度,摇匀,再精密量取4ml,置50ml量瓶中,加溶出介质稀释至刻度,摇匀,作为对照品溶液。
取上述两种溶液照紫外-可见分光光度法,在357nm的波长处测定吸光度,计算出每片溶出量,限度均为标示量的70%,应符合规定。
磷酸氢二钠-枸橼酸缓冲液(pH8.0) 取0.05mol/L磷酸氢二钠试液1000ml,用0.525%枸橼酸溶液调pH值至8.0,即得。
定量检测小颗粒低密度脂蛋白的方法[发明专利]
![定量检测小颗粒低密度脂蛋白的方法[发明专利]](https://img.taocdn.com/s3/m/aabe82dd87c24028905fc326.png)
专利名称:定量检测小颗粒低密度脂蛋白的方法专利类型:发明专利
发明人:伊藤康树,平野勉
申请号:CN200710101968.3
申请日:20031205
公开号:CN101051051A
公开日:
20071010
专利内容由知识产权出版社提供
摘要:本发明的目的是提供用于小颗粒LDL的分级检测的快速而简单的方法。
定量试样中小颗粒低密度脂蛋白的方法,该方法包括第一步将小颗粒低密度脂蛋白与其他低密度脂蛋白分离,和第二步检测所分离的小颗粒低密度脂蛋白中胆固醇、甘油三脂或者蛋白质。
申请人:电化生研株式会社
地址:日本东京都
国籍:JP
代理机构:中国专利代理(香港)有限公司
更多信息请下载全文后查看。
大鼠内脏脂肪特异性丝氨酸蛋白酶抑制剂vaspin酶联

大鼠内脏脂肪特异性丝氨酸蛋白酶抑制剂(vaspin)酶联免疫分析(ELISA)试剂盒使用说明书本试剂仅供研究使用目的:本试剂盒用于测定大鼠血清,血浆及相关液体样本中内脏脂肪特异性丝氨酸蛋白酶抑制剂(vaspin) 的含量。
实验原理:本试剂盒应用双抗体夹心法测定标本中大鼠内脏脂肪特异性丝氨酸蛋白酶抑制剂(vaspin) 水平。
用纯化的大鼠内脏脂肪特异性丝氨酸蛋白酶抑制剂(vaspin) 抗体包被微孔板,制成固相抗体,往包被单抗的微孔中依次加入内脏脂肪特异性丝氨酸蛋白酶抑制剂(vaspin) ,再与HRP标记的内脏脂肪特异性丝氨酸蛋白酶抑制剂(vaspin) 抗体结合,形成抗体-抗原-酶标抗体复合物,经过彻底洗涤后加底物TMB显色。
TMB在HRP酶的催化下转化成蓝色,并在酸的作用下转化成最终的黄色。
颜色的深浅和样品中的内脏脂肪特异性丝氨酸蛋白酶抑制剂(vaspin) 呈正相关。
用酶标仪在450nm波长下测定吸光度(OD值),通过标准曲线计算样品中大鼠内脏脂肪特异性丝氨酸蛋白酶抑制剂(vaspin) 浓度。
注意事项:1.浓洗涤液可能会有结晶析出,稀释时可在水浴中加温助溶,洗涤时不影响结果。
2.封板膜只限一次性使用,以避免交叉污染。
3.各步加样均应使用加样器,并经常校对其准确性,以避免试验误差。
一次加样时间最好控制在5分钟内,如标本数量多,推荐使用排枪加样。
4.试剂盒从冷藏环境中取出应在室温平衡15-30分钟后方可使用,酶标包被板开封后如未用完,板条应装入密封袋中保存。
5.请每次测定的同时做标准曲线,最好做复孔。
如标本中待测物质含量过高(样本OD值大于标准品孔第一孔的OD值),请先用样品稀释液稀释一定倍数(n倍)后再测定,计算时请最后乘以总稀释倍数(×n×5)。
6.底物请避光保存。
7.严格按照说明书的操作进行,试验结果判定必须以酶标仪读数为准.8.所有样品,洗涤液和各种废弃物都应按传染物处理。
高效液相色谱法测定降脂减肥片中二苯乙烯苷的含量
高效液相色谱法测定降脂减肥片中二苯乙烯苷的含量
刘彦臣;王勤华
【期刊名称】《黑龙江医药科学》
【年(卷),期】2006(29)3
【摘要】目的:采用高效液相色谱法测定降脂减肥片中二苯乙烯苷(2,3,5,4′-四羟基二苯乙烯-2-O-β-D-葡萄糖苷)含量.方法:以C18色谱柱为分析柱;流动相:乙腈-水(25:75);流速:1.0 ml/min;检测波长:320nm.结果:二苯乙烯苷的线性范围为0.31~3.1μg,r=0.9998,平均回收率98.35%(RSD=1.3%,n=5),方法精密度为(RSD=0.59%,n=5).结论:本方法具有准确性、灵敏性、专一性,为测定降脂减肥片中二苯乙烯苷的含量提供了新的方法.
【总页数】2页(P110-111)
【作者】刘彦臣;王勤华
【作者单位】黑龙江天宏药业有限公司,黑龙江,哈尔滨150025;黑龙江多多药业有限责任公司,黑龙江,佳木斯154007
【正文语种】中文
【中图分类】R927.2
【相关文献】
1.高效液相色谱法测定降脂减肥片中葛根素的含量 [J], 杜鹏;乔建军;来玉梅
2.高效液相色谱法测定减肥降脂片中大黄酸、大黄素的含量 [J], 郭澄;王雯佶;江春霞;刘皋林;张纯
3.HPLC法测定降脂减肥片中二苯乙烯苷的含量 [J], 李云涛;姜波;王守喜;张雷
4.高效液相色谱法测定降脂减肥片中大黄素的含量 [J], 王欣;王华;宋洋;王喜莉
5.高效液相色谱法测定降脂口服液中四羟二苯乙烯苷的含量 [J], 郭维烈;李建祥;谢昭明;李顺祥;朱如彩
因版权原因,仅展示原文概要,查看原文内容请购买。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Inhibitors, Agonists, Screening LibrariesSafety Data Sheet Revision Date:May-24-2017Print Date:May-24-20171. PRODUCT AND COMPANY IDENTIFICATION1.1 Product identifierProduct name :Pitavastatin (Calcium)Catalog No. :HY-B0144CAS No. :147526-32-71.2 Relevant identified uses of the substance or mixture and uses advised againstIdentified uses :Laboratory chemicals, manufacture of substances.1.3 Details of the supplier of the safety data sheetCompany:MedChemExpress USATel:609-228-6898Fax:609-228-5909E-mail:sales@1.4 Emergency telephone numberEmergency Phone #:609-228-68982. HAZARDS IDENTIFICATION2.1 Classification of the substance or mixtureNot a hazardous substance or mixture.2.2 GHS Label elements, including precautionary statementsNot a hazardous substance or mixture.2.3 Other hazardsNone.3. COMPOSITION/INFORMATION ON INGREDIENTS3.1 SubstancesSynonyms:Pitavastatin hemicalcium; NK⁻104Formula:C25H23FNO4 . 1/2 CaMolecular Weight:440.49CAS No. :147526-32-74. FIRST AID MEASURES4.1 Description of first aid measuresEye contactRemove any contact lenses, locate eye-wash station, and flush eyes immediately with large amounts of water. Separate eyelids with fingers to ensure adequate flushing. Promptly call a physician.Skin contactRinse skin thoroughly with large amounts of water. Remove contaminated clothing and shoes and call a physician.InhalationImmediately relocate self or casualty to fresh air. If breathing is difficult, give cardiopulmonary resuscitation (CPR). Avoid mouth-to-mouth resuscitation.IngestionWash out mouth with water; Do NOT induce vomiting; call a physician.4.2 Most important symptoms and effects, both acute and delayedThe most important known symptoms and effects are described in the labelling (see section 2.2).4.3 Indication of any immediate medical attention and special treatment neededTreat symptomatically.5. FIRE FIGHTING MEASURES5.1 Extinguishing mediaSuitable extinguishing mediaUse water spray, dry chemical, foam, and carbon dioxide fire extinguisher.5.2 Special hazards arising from the substance or mixtureDuring combustion, may emit irritant fumes.5.3 Advice for firefightersWear self-contained breathing apparatus and protective clothing.6. ACCIDENTAL RELEASE MEASURES6.1 Personal precautions, protective equipment and emergency proceduresUse full personal protective equipment. Avoid breathing vapors, mist, dust or gas. Ensure adequate ventilation. Evacuate personnel to safe areas.Refer to protective measures listed in sections 8.6.2 Environmental precautionsTry to prevent further leakage or spillage. Keep the product away from drains or water courses.6.3 Methods and materials for containment and cleaning upAbsorb solutions with finely-powdered liquid-binding material (diatomite, universal binders); Decontaminate surfaces and equipment by scrubbing with alcohol; Dispose of contaminated material according to Section 13.7. HANDLING AND STORAGE7.1 Precautions for safe handlingAvoid inhalation, contact with eyes and skin. Avoid dust and aerosol formation. Use only in areas with appropriate exhaust ventilation.7.2 Conditions for safe storage, including any incompatibilitiesKeep container tightly sealed in cool, well-ventilated area. Keep away from direct sunlight and sources of ignition.Recommended storage temperature:Powder-20°C 3 years4°C 2 yearsIn solvent-80°C 6 months-20°C 1 monthShipping at room temperature if less than 2 weeks.7.3 Specific end use(s)No data available.8. EXPOSURE CONTROLS/PERSONAL PROTECTION8.1 Control parametersComponents with workplace control parametersThis product contains no substances with occupational exposure limit values.8.2 Exposure controlsEngineering controlsEnsure adequate ventilation. Provide accessible safety shower and eye wash station.Personal protective equipmentEye protection Safety goggles with side-shields.Hand protection Protective gloves.Skin and body protection Impervious clothing.Respiratory protection Suitable respirator.Environmental exposure controls Keep the product away from drains, water courses or the soil. Cleanspillages in a safe way as soon as possible.9. PHYSICAL AND CHEMICAL PROPERTIES9.1 Information on basic physical and chemical propertiesAppearance White to off-white (Solid)Odor No data availableOdor threshold No data availablepH No data availableMelting/freezing point No data availableBoiling point/range No data availableFlash point No data availableEvaporation rate No data availableFlammability (solid, gas)No data availableUpper/lower flammability or explosive limits No data availableVapor pressure No data availableVapor density No data availableRelative density No data availableWater Solubility No data availablePartition coefficient No data availableAuto-ignition temperature No data availableDecomposition temperature No data availableViscosity No data availableExplosive properties No data availableOxidizing properties No data available9.2 Other safety informationNo data available.10. STABILITY AND REACTIVITY10.1 ReactivityNo data available.10.2 Chemical stabilityStable under recommended storage conditions.10.3 Possibility of hazardous reactionsNo data available.10.4 Conditions to avoidNo data available.10.5 Incompatible materialsStrong acids/alkalis, strong oxidising/reducing agents.10.6 Hazardous decomposition productsUnder fire conditions, may decompose and emit toxic fumes.Other decomposition products - no data available.11.TOXICOLOGICAL INFORMATION11.1 Information on toxicological effectsAcute toxicityClassified based on available data. For more details, see section 2Skin corrosion/irritationClassified based on available data. For more details, see section 2Serious eye damage/irritationClassified based on available data. For more details, see section 2Respiratory or skin sensitizationClassified based on available data. For more details, see section 2Germ cell mutagenicityClassified based on available data. For more details, see section 2CarcinogenicityIARC: No component of this product present at a level equal to or greater than 0.1% is identified as probable, possible or confirmed human carcinogen by IARC.ACGIH: No component of this product present at a level equal to or greater than 0.1% is identified as a potential or confirmed carcinogen by ACGIH.NTP: No component of this product present at a level equal to or greater than 0.1% is identified as a anticipated or confirmed carcinogen by NTP.OSHA: No component of this product present at a level equal to or greater than 0.1% is identified as a potential or confirmed carcinogen by OSHA.Reproductive toxicityClassified based on available data. For more details, see section 2Specific target organ toxicity - single exposureClassified based on available data. For more details, see section 2Specific target organ toxicity - repeated exposureClassified based on available data. For more details, see section 2Aspiration hazardClassified based on available data. For more details, see section 2Additional informationRTECS No.: MJ8047045This information is based on our current knowledge. However the chemical, physical, and toxicological properties have not been completely investigated.12. ECOLOGICAL INFORMATION12.1 ToxicityNo data available.12.2 Persistence and degradabilityNo data available.12.3 Bioaccumlative potentialNo data available.12.4 Mobility in soilNo data available.12.5 Results of PBT and vPvB assessmentPBT/vPvB assessment unavailable as chemical safety assessment not required or not conducted.12.6 Other adverse effectsNo data available.13. DISPOSAL CONSIDERATIONS13.1 Waste treatment methodsProductDispose substance in accordance with prevailing country, federal, state and local regulations.Contaminated packagingConduct recycling or disposal in accordance with prevailing country, federal, state and local regulations.14. TRANSPORT INFORMATIONDOT (US)This substance is considered to be non-hazardous for transport.IMDGThis substance is considered to be non-hazardous for transport.IATAThis substance is considered to be non-hazardous for transport.15. REGULATORY INFORMATIONSARA 302 Components:No chemicals in this material are subject to the reporting requirements of SARA Title III, Section 302.SARA 313 Components:This material does not contain any chemical components with known CAS numbers that exceed the threshold (De Minimis) reporting levels established by SARA Title III, Section 313.SARA 311/312 Hazards:No SARA Hazards.Massachusetts Right To Know Components:No components are subject to the Massachusetts Right to Know Act.Pennsylvania Right To Know Components:No components are subject to the Pennsylvania Right to Know Act.New Jersey Right To Know Components:No components are subject to the New Jersey Right to Know Act.California Prop. 65 Components:This product does not contain any chemicals known to State of California to cause cancer, birth defects, or anyother reproductive harm.16. OTHER INFORMATIONCopyright 2017 MedChemExpress. The above information is correct to the best of our present knowledge but does not purport to be all inclusive and should be used only as a guide. The product is for research use only and for experienced personnel. It must only be handled by suitably qualified experienced scientists in appropriately equipped and authorized facilities. The burden of safe use of this material rests entirely with the user. MedChemExpress disclaims all liability for any damage resulting from handling orfrom contact with this product.Caution: Product has not been fully validated for medical applications. For research use only.Tel: 609-228-6898 Fax: 609-228-5909 E-mail: tech@Address: 1 Deer Park Dr, Suite Q, Monmouth Junction, NJ 08852, USA。