4080501_Melamine_phosphate
鱼酚氧化酶(PO)试剂盒说明书含量

鱼酚氧化酶(PO)酶联免疫分析(ELISA)试剂盒使用说明书本试剂仅供研究使用目的:本试剂盒用于测定鱼血清,血浆,及相关液体样本中酚氧化酶(PO)的含量。
实验原理:本试剂盒应用双抗体夹心法测定标本中鱼酚氧化酶(PO)水平。
用纯化的鱼酚氧化酶(PO)抗体包被微孔板,制成固相抗体,往包被单抗的微孔中依次加入酚氧化酶(PO)再与HRP标记的酚氧化酶(PO)抗体结合,形成抗体-抗原-酶标抗体复合物,经过彻底洗涤后加底物TMB 显色。
TMB在HRP酶的催化下转化成蓝色,并在酸的作用下转化成最终的黄色。
颜色的深浅和样品中的酚氧化酶(PO)呈正相关。
用酶标仪在450nm波长下测定吸光度(OD值),通过标准曲线计算样品中鱼酚氧化酶(PO)浓度。
试剂盒组成:试剂盒组成48孔配置96孔配置保存说明书1份1份封板膜2片(48)2片(96)密封袋1个1个酶标包被板1×481×962-8℃保存标准品:900pg/ml0.5ml×1瓶0.5ml×1瓶2-8℃保存标准品稀释液 1.5ml×1瓶 1.5ml×1瓶2-8℃保存酶标试剂3ml×1瓶6ml×1瓶2-8℃保存样品稀释液3ml×1瓶6ml×1瓶2-8℃保存显色剂A液3ml×1瓶6ml×1瓶2-8℃保存显色剂B液3ml×1瓶6ml×1瓶2-8℃保存终止液3ml×1瓶6ml×1瓶2-8℃保存浓缩洗涤液(20ml×20倍)×1瓶(20ml×30倍)×1瓶2-8℃保存样本处理及要求:1.血清:室温血液自然凝固10-20分钟,离心20分钟左右(2000-3000转/分)。
仔细收集上清,保存过程中如出现沉淀,应再次离心。
2.血浆:应根据标本的要求选择EDTA或柠檬酸钠作为抗凝剂,混合10-20分钟后,离心20分钟左右(2000-3000转/分)。
超高效液相色谱-串联质谱法同时检测地龙药材中4种黄曲霉毒素含量及阳性结果确证

分析测试经验介绍 (104 ~ 109)超高效液相色谱-串联质谱法同时检测地龙药材中4种黄曲霉毒素含量及阳性结果确证郭 晶1,张 进1,李文君1,李正刚2(1. 通化市食品药品检验所,吉林 通化 134000;2. 四平市食品药品检验所,吉林 四平 136000)摘要:建立超高效液相色谱-串联质谱法同时测定地龙药材中黄曲霉毒素B 1、B 2、G 1、G 2的含量,并对阳性结果进行确证. 样品经70%甲醇提取、免疫亲和柱净化、超高效液相色谱柱分离、三重四极杆质谱检测,并采用离子峰度比进行阳性结果确证. 结果表明,4种黄曲霉毒素的线性关系良好(r >0.999 5),回收率在91.2%~95.6%范围内.黄曲霉毒素B 1、B 2、G 1、G 2的检出限分别为0.10、0.038、0.11、0.038 µg/kg. 方法专属性好,灵敏度高,准确性好,可以进行最终阳性检出的判定. 15批地龙药材中6批黄曲霉毒素确证阳性检出, 证明地龙药材较易被黄曲霉毒素污染.关键词:地龙;超高效液相色谱-串联质谱;黄曲霉毒素;阳性结果确证中图分类号:O657. 63 文献标志码:B 文章编号:1006-3757(2024)02-0104-06DOI :10.16495/j.1006-3757.2024.02.005Simultaneous Determination of Four Aflatoxins in Pheretima by Ultra Performance Liquid Chromatography Tandem Mass Spectrometry andConfirmation of Positive ResultsGUO Jing 1, ZHANG Jin 1, LI Wenjun 1, LI Zhenggang2(1. Tonghua Institute for Food and Drug Control , Tonghua 134000, Jilin China ;2. Siping Institute for Food andDrug Control , Siping 136000, Jilin China )Abstract :A method for simultaneous determination of aflatoxins B 1, B 2, G 1, and G 2 in pheretima was been established by ultra performance liquid chromatography tandem mass spectrometry (UPLC-MS/MS), and the positive results was confirmed. The samples were extracted by 70% methanol, purified by a immunoaffinity columns, separated by UPLC-MS/MS, detected by triple quadrupole mass spectrometry, and confirmed by ion peak ratio. The results showed that the linear relationship of the four aflatoxins were good (r >0.999 5), and the recoveries ranged from 91.2% to 95.6%. The limits of detection for aflatoxin B 1, B 2, G 1, and G 2 were 0.10, 0.038, 0.11, 0.038 µg/kg, respectively. The method has a good specificity, high sensitivity, good accuracy, and can be used to determine the final positive detection. Aflatoxin were positively detected in 6 out of 15 batches of pheretima , which proved that the Pheretima were more susceptible to contamination by aflatoxins.Key words :Pheretima ;UPLC-MS/MS ;aflatoxin ;confirmation of positive results收稿日期:2024−01−10; 修订日期:2024−03−05.基金项目:吉林省中药材标准及中药饮片炮制规范(项目编号:JLPZGF-2020-052)作者简介:郭晶(1979−),女,副主任药师,研究方向为药品质量标准通信作者:李正刚(1982−),男,硕士,医药工程师,研究方向为中药质量标准,E-mail :*****************.第 30 卷第 2 期分析测试技术与仪器Volume 30 Number 22024年3月ANALYSIS AND TESTING TECHNOLOGY AND INSTRUMENTS Mar. 2024黄曲霉毒素(aflatoxins, AF)是一种毒性极强的剧毒物质,被各个国家的癌症研究机构列为Ⅰ类致癌物. 黄曲霉毒素主要是由黄曲霉、寄生曲霉产生的次生代谢产物,是一组化学结构类似的化合物[1-2],主要包括AFB1、AFB2、AFG1、AFG2,多存在于土壤、动植物、各种坚果中[3],在湿热环境下出现黄曲霉毒素污染的概率最高. 黄曲霉毒素的危害性在于对人及动物肝脏组织的慢性毒性作用,长期积累可导致肝癌甚至死亡[4-5]. 各国药典均对黄曲霉毒素在中药材或中草药中的限量作了规定,如《欧洲药典》规定AFB1、AFB2、AFG1、AFG2总量在中草药中的限量不得高于4 µg/kg,《美国药典》规定AFB1、AFB2、AFG1、AFG2总量在中草药中的限量不得高于20µg/kg,《中华人民共和国药典》规定其总量在中药材中的限量不得高于10 µg/kg[6].地龙药材标准收载在《中华人民共和国药典》2020版一部[7]. 采收时需要及时剖开腹部,除去内脏和泥沙. 由于地龙生长在土壤环境中,故其被AF污染的风险较大. 目前AF测定的方法主要有液相色谱-柱后碘衍生化法或光化学衍生化法-荧光检测器以及酶联免疫法,但以上方法均存在假阳性的误判可能性,当超出标准限值时均需要采用质谱检测器进行阳性确证[8]. 本研究采用超高效液相色谱-串联质谱法(UPLC-MS/MS)同时测定不同产地多批次地龙药材中AFB1、AFB2、AFG1、AFG2的含量,并对阳性结果进行确证,从而准确的判定检出情况,为地龙药材中AF污染情况提供参考.1 试验部分1.1 仪器和试剂BT125D型电子天平(北京赛多利斯仪器天平有限公司),TDL-5-A型离心机(上海安亭科学仪器厂),AB SCIEX QTRAP® 5500型超高效液相色谱-三重四极杆质谱(美国AB SCIEX公司). 超高压液相色谱柱(岛津科技有限公司),免疫亲和柱(青岛普瑞邦生物工程有限公司,规格:3 mL,批号:2J1J24-4).AF混合对照品溶液:AFB1、AFB2、AFG1、AFG2标示质量浓度分别为1.04、0.38、1.08、0.38µg/mL,批号:610001-202006,来源于中国食品药品检定研究院. 氯化钠和醋酸铵(国药集团化学试剂有限公司,分析纯),甲醇和乙腈(Flsher Scientific,色谱纯),纯化水为自制.本次收集到不同产地和批次的地龙药材共15批,基本信息如表1所列.表 1 地龙药材样品基本信息Table 1 Basic informations of Pheretima samples药材编号样品名称产地DL1广地龙海南文昌DL2广地龙广东肇庆DL3广地龙广东韶关DL4广地龙广东韶关DL5广地龙广西玉林DL6广地龙广西北海DL7沪地龙湖北襄阳DL8沪地龙河南濮阳DL9沪地龙河南安阳DL10沪地龙浙江嘉兴DL11沪地龙河南焦作DL12沪地龙浙江金华DL13沪地龙江西赣州DL14沪地龙江西九江DL15沪地龙江西宜春1.2 仪器工作条件1.2.1 色谱条件色谱柱:Shim-pack XR-ODS,3.0 mm×75 mm (1.8 µm);以10 mmol/L醋酸铵溶液为流动相A,甲醇为流动相B;柱温:25 ℃;流速:0.3 mL/min. 按表2中的程序进行梯度洗脱.表 2 梯度洗脱程序Table 2 Gradient elution procedure时间/min流动相A/%流动相B/%0~4.565~1535~854.5~615~085~1006~6.50~65100~356.5~1065351.2.2 质谱条件离子源:电喷雾离子源(ESI源);监测模式:正离子扫描下的多反应监测模式(MRM);喷雾压强:0.21 MPa;干燥气流速:8 L/min;干燥气温度:550 ℃;毛细管电压:5 500 V;三重四极杆离子对及相关电压参数设定如表3所列.第 2 期郭晶,等:超高效液相色谱-串联质谱法同时检测地龙药材中4种黄曲霉毒素含量及阳性结果确证1051.3 标准曲线绘制分别精密量取AF混合对照品溶液100、50、25µL于10 mL容量瓶中,用甲醇稀释至刻度,摇匀,即得标准曲线溶液1、2、3. 分别精密量取1 mL标准曲线溶液2、0.1 mL标准曲线溶液1于10 mL容量瓶中,用甲醇稀释至刻度,摇匀,即得标准曲线溶液4、5. 精密量取1 mL标准曲线溶液4于10 mL 容量瓶中,用甲醇稀释至刻度,摇匀,即得标准曲线溶液6.1.4 供试品溶液制备取供试品粉末约15 g(过四号筛网),精密称定,置于均质瓶中,加入氯化钠3 g、70%甲醇溶液75 mL,12 000 r/min高速搅拌2 min,4 500 r/min离心5 min,取上清液15.0 mL,置于50 mL量瓶中,用水稀释至刻度,摇匀,4 500 r/min离心10 min,取续滤液20.0 mL. 通过免疫亲合柱,流速3 mL/min,用20 mL水洗脱,洗脱液弃去,使空气进入免疫亲合柱,将水挤出,再用适量甲醇洗脱,收集洗脱液,置于2 mL量瓶中,加甲醇稀释至刻度,摇匀,用微孔滤膜(0.22 µm)滤过,取续滤液,即得.2 结果与讨论2.1 免疫亲和柱技术和质谱测定法的优势免疫亲和柱技术是利用抗原、抗体之间高度特异性结合对目标物进行净化富集的一种实验技术,预置在柱体内的特异性抗体选择性结合样本中的待测物,杂质不被结合流出柱外,柱上结合的目标物再被洗脱液洗脱,从而实现目标物的高效净化和浓缩[9].质谱法是使待测化合物产生气态离子,再按质荷比(m/z)将离子分离、检测的分析方法,检测限可达10−15~10−12 mol数量级. 相比较液相色谱法,测试样品需要的量较少,其检测灵敏度也大幅度提高,且其较好的专属性可以作为液相色谱检出情况的进一步确证,大大降低误判阳性检出的情况[10-13]. 2.2 线性范围和检出限分别精密吸取1.3项下系列混合对照品溶液5µL,注入液相色谱仪,测定峰面积,以进样质量浓度(ng/mL)为横坐标,峰面积为纵坐标,绘制标准曲线.结果如表4所列,4种黄曲霉毒素的线性关系良好(r>0.999 5).取不含AF的样品15 g,加入0.15 mL标准曲线溶液1,余下操作同1.4项下供试品溶液制备,1.2项下仪器工作条件测定,以信噪比(S/N)为3作为4种黄曲霉毒素的检出限(limit of detection,LOD),结果如表4所列,AFB1、AFB2、AFG1、AFG2的LOD分别为0.10、0.038、0.11、0.038 µg/kg,表明方法灵敏度较高.表 4 回归方程、线性范围和检出限Table 4 Regression equations, linear ranges and limits of detection组分名称回归方程r线性范围/(ng/mL)LOD/(µg/kg)S/N AFB1y=33 600x –1 3600.999 90.104~10.4000.10 4.5AFB2y=30 900x – 4 8800.999 80.038~3.8000.038 3.1AFG1y=26 150x – 6 3400.999 80.108~10.8000.11 4.2AFG2y=21 200x + 2 9200.999 80.038~3.8000.038 3.32.3 精密度考察取5 µL 1.3项下标准曲线溶液1,在1.2项下仪器条件及测定方法下分别连续进样6次,测定各组分的色谱峰面积. 测试结果:AFB1、AFB2、AFG1、表 3 质谱条件Table 3 Conditions of mass spectrometer序号组分名称母离子/(m/z)子离子/(m/z)碎裂电压/V碰撞能量/eV1AFB1313.1285.1*16034241.0207512AFB2315.1287.1*18937259.1200393AFG1329.1243.1*16338311.1180314AFG2331.1313.1*18535245.118842注:*定量离子对106分析测试技术与仪器第 30 卷AFG2色谱峰面积相对标准偏差(RSD)分别为1.3%、2.2%、1.8%和2.2%,表明仪器的精密度良好.2.4 稳定性试验取1.3项下标准曲线溶液1,分别于0、4、8、16、18、24 h 按1.2项下仪器条件进样5 µL,记录所测各组分峰面积. 测试结果:AFB1、AFB2、AFG1、AFG2色谱峰面积RSD分别为2.6%、2.2%、2.5%和2.3%,结果表明在24 h内测定结果稳定.2.5 重复性和回收率试验由于15批次地龙药材中仅部分检出AFB1、AFB2,故在加标回收试验中进行方法的重复性考察.称取不含AF的地龙药材(编号:DL1)粉末约15 g,各6份,分别精密加入AF混合对照品溶液75 µL,其余操作同2.1.2项下供试品溶液制备,按2.2项下条件分别测定各组分的色谱峰面积,结果如表5所列. 由表5可见,AFB1、AFB2、AFG1、AFG2的平均回收率分别为95.6%、93.4%、93.2%、91.2%,加标测定值的RSD分别为1.9%、2.0%、1.7%和2.6%,表明该方法的回收率满足要求,方法的重复性良好.2.6 样品测定取15批次地龙药材,按照1.4项下方法制备供试品溶液,1.2项下仪器条件进行测定,结果如表6所列,结果表明在6批地龙样品中检测出AFB1和AFB2,质谱总离子流图如图1所示.表 6 样品测定结果Table 6 Determination results of samples/(µg/kg)样品编号AFB1质量分数AFB2质量分数AFG1质量分数AFG2质量分数总质量分数DL1/////DL2/////DL3/////DL4 6.80.53//7.33 DL5/////DL6/////DL77.80.35//8.15 DL8 6.50.31// 6.81 DL9 4.30.24// 4.54 DL10/////DL11/////DL12/////DL13 3.10.43// 3.53 DL14 2.50.31// 2.81 DL15/////注:“/”:未检出2.7 阳性结果确证中药组成成分相较于西药组成成分复杂多样,三重四极杆质谱是以母离子及子离子组成的离子对进行检测,由于样品基质成分的复杂性,单个离子对出现干扰的情况在试验过程中偶有发生. 然而一个化合物在质谱检测器的离子源中被固定碰撞电压击碎产生的多个碎片离子之间具有相对固定的比例,故采用离子对峰面积的比值进行比较更具有专属性,UPLC-MS/MS法通常采用离子峰度比对结果进一步确证阳性检出,即:如果样品检出色谱峰的保留时间与对照品一致,并且在扣除背景后的表 5 方法的重复性和回收率试验结果Table 5 Experimental results of repeatability andrecovery of method添加质量分数加入质量/ng实测质量/ng回收率/%平均回收率/%RSD/%AFB1 (5 µg/kg)78.0074.2195.1495.6 1.9 78.0073.1193.7378.0075.5396.8378.0076.5298.1078.0072.9993.5878.0075.2396.45AFB2 (2 µg/kg)28.5026.1291.6593.4 2.0 28.5025.2390.7728.5026.7893.9628.5027.0194.7728.5027.3295.8628.5026.5593.16AFG1 (5 µg/kg)81.0077.4495.6093.2 1.7 81.0075.2692.9181.0075.3693.0481.0074.8292.3781.0076.3594.2681.0073.7891.09AFG2 (2 µg/kg)28.5025.1591.0591.2 2.6 28.5026.2292.0028.5025.4789.3728.5025.1188.1128.5027.0194.7728.5026.2892.21第 2 期郭晶,等:超高效液相色谱-串联质谱法同时检测地龙药材中4种黄曲霉毒素含量及阳性结果确证107质谱图中,所选择的监测离子对均出现,而且所选择的监测离子对峰面积比与对照品的监测离子对峰面积比一致,则可判定样品中存在该真菌毒素.经计算本试验检出的6批阳性样品的离子峰度比AFB 1分别为75.3%、75.2%、75.1%、75.3%、75.2%、75.1%,相对平均偏差均小于0.2%. AFB 2分别为85.0%、85.1%、85.1%、85.2%、85.3%、85.0%,相对平均偏差均小于0.2%. 均在允许偏差±20%内,确证样品阳性检出.3 结论由多批次样品检验情况可以初步得出,地龙药材中黄曲霉毒素的污染主要为黄曲霉毒素B 1和B 2.地龙药材在产地初加工过程中需去除泥沙,而泥沙为黄曲霉毒素污染的重要来源,如果泥沙去除不净、保存不当、遇湿热环境,则黄曲霉毒素含量容易超标[14-17]. 因此地龙药材的黄曲霉毒素监测检验非常必要[18-21]. 试验结果表明,UPLC-MS/MS 法操作简便、专属性好、灵敏度高、重复性好,能够对地龙药材的阳性结果作出准确判定,故将在中药材的黄曲霉毒素污染检测中发挥重要作用.参考文献:刘丽娜, 李海亮, 李耀磊, 等. 中药真菌毒素质量控制概况、限量标准制定及有关问题的思考[J ]. 中草药,2023,54(19):6197-6207. [LIU Lina, LI Hailiang, LI Yaolei, et al. Overview on quality control of mycotox-ins in traditional Chinese medicine, limit requirements and discussion on related issues [J ]. Chinese Tradition-al and Herbal Drugs ,2023,54 (19):6197-6207.][ 1 ]沈立, 汤燕, 陈铁柱, 等. 固相萃取液质联用测定川产道地药材黄精、麦冬中10种真菌毒素[J ]. 药物分析杂志,2023,43(8):1369-1380. [SHEN Li, TANG[ 2 ]Yan, CHEN Tiezhu, et al. Determination of 10 my-cotoxins in Polygonati Rhizoma and Ophiopogonis Radix as a genuine regional drug of Sichuan by solid-phase extraction coupled with LC-MS/MS [J ]. Chinese Journal of Pharmaceutical Analysis ,2023,43 (8):1369-1380.]徐晓艳, 王宇, 王梦瑶, 等. 中药材中真菌毒素的检测与脱毒研究进展[J ]. 中草药,2024,55(2):657-669.[XU Xiaoyan, WANG Yu, WANG Mengyao, et al.Research progress on detection and detoxification of mycotoxins in Chinese medicinal materials [J ].Chinese Traditional and Herbal Drugs ,2024,55 (2):657-669.][ 3 ]李正刚, 程焱, 王丹彧, 等. 地龙药材中黄曲霉毒素B 1、B 2、G 1、G 2的含量检测[J ]. 化学工程师,2023,37(8):34-37. [LI Zhenggang, CHENG Yan, WANG Danyu, et al. Detection of aflatoxins B 1、B 2、G 1、G 2 in Pheretima materials [J ]. Chemical Engineer ,2023,37(8):34-37.][ 4 ]莫紫梅. 黄曲霉毒素B 1降解产物及其安全性评价研究进展[J/OL ]. 中国油脂, 2023:1-12[2024-02-29].https:///10.19902/ki.zgyz.1003-7969.230329. [MO Zimei. Research progress on degrada-tion products of aflatoxin B 1 and its safety evaluation [J/OL ]. China Oils and Fats, 2023:1-12[2024-02-29]. https:///10.19902/ki.zgyz.1003-7969.230329.][ 5 ]孙艳杰, 李正刚, 赵磊, 等. 制貂肾中黄曲霉毒素的测定方法研究及暴露风险评估[J ]. 中国药物评价,2023,40(3):249-252. [SUN Yanjie, LI Zhenggang,ZHAO Lei, et al. Determination method of aflatoxin in processed mustela and risk assessment [J ]. Chinese Journal of Drug Evaluation ,2023,40 (3):249-252.][ 6 ]国家药典委员会. 中华人民共和国药典(一部)[S ].北京: 中国医药科技出版社, 2020: 127.[ 7 ]许晓辉, 李晨曦, 吴福祥, 等. QuEChERS-分散固相萃取-液质联用法快速测定地龙中黄曲霉毒素[J ].分析测试技术与仪器,2021,27(1):18-23. [XU[ 8 ]1×1042×1043×104(a)(b)4×1045×1046×1047×104t /minI n t e n s i t y /c p sI n t e n s i t y /c p st /min1×1042×1043×1044×1045×1046×104AFB 2AFB 1AFG 2AFB 2AFB 1AFG 1图1 样品测定图谱(a )对照品质谱总离子流图,(b )样品质谱总离子流图Fig. 1 Total ion flow diagrams of samples108分析测试技术与仪器第 30 卷Xiaohui, LI Chenxi, WU Fuxiang, et al. QuEChERS-dispersed solid phase extraction-ultra performance li-quid chromatography-tandem mass spectrometry for rapid determination of aflatoxin in pheretima [J ]. Ana-lysis and Testing Technology and Instruments ,2021,27 (1):18-23.]马彧, 李正刚, 程焱, 等. 超声萃取-免疫亲和柱净化-柱后光化学衍生高效液相色谱法同时测定蜂房药材中4种黄曲霉毒素[J ]. 化学分析计量,2023,32(2):20-23, 56. [MA Yu, LI Zhenggang, CHENG Yan, et al. Simultaneous determination of four aflatox-ins in Nidus Vespae by ultrasonic extraction-immun-oaffinity column purification-post column photochem-ical derivatization HPLC [J ]. Chemical Analysis and Meterage ,2023,32 (2):20-23, 56.][ 9 ]龚敏, 陈明亮, 金鹏, 等. QuEChERS 结合UPLC-MS/MS 测定水产品中4种黄曲霉毒素及其裂解规律研究[J ]. 热带农业科学,2023,43(10):35-40.[GONG Min, CHEN Mingliang, JIN Peng, et al. De-termination of four aflatoxins in aquatic product by QuEChERS combine UPLC-MS/MS method and study on fragmentation pathway [J ]. Chinese Journal of Tropical Agriculture ,2023,43 (10):35-40.][ 10 ]袁正宁, 李梁子涵, 王艳敏, 等. 黄曲霉毒素对肝脏和脾脏的毒理作用研究[J ]. 中国畜禽种业,2023,19(4):91-95. [YUAN Zhengning, LI Liangzihan,WANG Yanmin, et al. Toxicological effects of aflatoxin on liver and spleen [J ]. The Chinese Live-stock and Poultry Breeding ,2023,19 (4):91-95.][ 11 ]何洁, 余婷婷, 梁松, 等. 高通量高效快速净化方法结合UPLC-MS/MS 测定粮食中黄曲霉毒素[J/OL ]. 中国测试, 2023:1-12 [2024-02-29]. https:///kcms/detail/51.1714.TB.20230421.1514.008.html.[HE Jie, YU Tingting, LIANG Song, et al. Determina-tion of aflatoxins in grains using the high-throughput high efficient flow-through clean-up method and ultra-high performance liquid chromatography tandem mass spectrometry [J/OL ]. China Measurement & Test,2023:1-12 [2024-02-29]. https:///kcms/de-tail/51.1714.TB.20230421.1514.008.html.][ 12 ]李正刚, 谢秋红, 邵大志, 等. 高效液相色谱-荧光检测法同时测定人参归脾丸中4种黄曲霉毒素[J ]. 中国卫生工程学, 2022, 21(5):714-716. [LI Zhenggang,XIE Qiuhong, SHAO Dazhi, et al. Simultaneous de-termination of content of four Aflatoxins Ginseng spleen-invigorating bolus by HPLC-FLD [J ]. Chinese Journal of Public Health Engineering, 2022, 21(5):714-716.][ 13 ]陈莉. 超高效液相色谱串联三重四极杆质谱法同时测定舒眠胶囊(片)中4种黄曲霉毒素含量[J ]. 中国药业,2022,31(22):77-80. [CHEN Li. Simultaneous[ 14 ]determination of four aflatoxins in Shumian capsules(tablets) by UPLC-QQQ/MS [J ]. China Phar-maceuticals ,2022,31 (22):77-80.]夏仕青, 李晓慧, 吴桃丽. 超高效液相色谱-串联质谱法测定辣椒粉中4种黄曲霉毒素的含量[J ]. 微量元素与健康研究,2023,40(1):57-60. [XIA Shiqing, LI Xiaohui, WU Taoli. Determination of four aflatoxins in Chili Powder by UPLC-MS/MS [J ]. Studies of Trace Elements and Health ,2023,40 (1):57-60.][ 15 ]淦露. 黄曲霉毒素检测技术研究进展[J ]. 现代食品,2022,28(15):114-117. [GAN Lu. Research progress of aflatoxin detection technology [J ]. Modern Food ,2022,28 (15):114-117.][ 16 ]杨昊, 公丕学, 王骏, 等. 基于石墨烯净化的超高效液相色谱串联质谱快速测定乳制品中黄曲霉毒素[J ].中国食品卫生杂志,2023,35(3):396-402. [YANG Hao, GONG Pixue, WANG Jun, et al. Fast determina-tion of aflatoxin in dairy products by ultra-high per-formance liquid chromatography-tandem mass spec-trometry based on purification of graphene [J ].Chinese Journal of Food Hygiene ,2023,35 (3):396-402.][ 17 ]赵飞. QuEChERS 结合超高效液相色谱-三重四极杆质谱法测定坚果中黄曲霉毒素[J ]. 当代化工,2022,51(3):752-756. [ZHAO Fei. Determination of aflatoxins in nuts by QuEChERS coupled with ultra-li-quid chromatography-mass spectrometry [J ]. Contem-porary Chemical Industry ,2022,51 (3):752-756.][ 18 ]谭丽盈. 超高效液相色谱-串联质谱法同时测定醋延胡索药材中4种黄曲霉毒素[J ]. 化学分析计量,2021,30(10):27-32. [TAN Liying. Simultaneous de-termination of four kinds of aflatoxins in vinegar cory-dalis by UPLC-MS/MS [J ]. Chemical Analysis and Meterage ,2021,30 (10):27-32.][ 19 ]周颖, 祝清岚, 马临科, 等. 免疫亲和柱净化-柱后光化学衍生-高效液相色谱法检测蜚蠊中的黄曲霉毒素[J ]. 中国药物评价,2020,37(5):358-361.[ZHOU Ying, ZHU Qinglan, MA Linke, et al. De-termination of aflatoxins in periplaneta Americana by immunoaffinity column and high performance liquid chromatography coupled with post-column photo-chemical derivatization [J ]. Chinese Journal of Drug Evaluation ,2020,37 (5):358-361.][ 20 ]刘宁, 王萌萌, 金红宇, 等. 高效液相色谱-柱后光化学衍生法测定参苓白术散中黄曲霉毒素G 2、G 1、B 2、B 1[J ]. 中国药事,2012,26(5):442-445. [LIU Ning,WANG Mengmeng, JIN Hongyu, et al. Determination of aflatoxin G 2, G 1, B 2, B 1 in Shenling Baizhu Powder by HPLC with post column photochemical derivatiza-tion [J ]. Chinese Pharmaceutical Affairs ,2012,26 (5):442-445.][ 21 ]第 2 期郭晶,等:超高效液相色谱-串联质谱法同时检测地龙药材中4种黄曲霉毒素含量及阳性结果确证109。
CelLyticTM系列蛋白裂解液

高效率 操作步骤简单,省时 高得率 得率远优于传统冻融或超声法 高活性 温和非变性条件下抽提活性蛋白 高兼容 与蛋白酶抑制剂、鳌合剂、离液剂等很好兼容 抽提的蛋白无需去除CelLyticTM 试剂即可进行下游实验: 亲和纯化 Western blot 凝胶迁移检测 报告基因检测……
566.28 2136.42 566.28 3758.04 2535.39 3938.22
501.93 3320.46
566.28 2084.94 3989.7
527.67 3629.34 5302.44
促销价¥
384.81 2375.80 685.97 2375.80 409.91 1505.79 2651.86 1054.05 1648.00 393.18 1187.90 217.50 711.07 4341.69 368.08 1271.56
哺乳动物细胞和组织裂解
C2978
CelLytic™ M Cell Lysis Reagent
C3228
CelLytic™ MT Cell Lysis Reagent
CE0500 NXTRACT
R0278
CelLytic™ MEM Protein Extraction Kit CelLytic™ NuCLEAR™ Extraction Kit For mammalian tissue or cultured cells RIPA Buffer
P8215
Protease Inhibitor Cocktail for use with fungal and yeast extracts
P8465
Protease Inhibitor Cocktail for use with bacterial cell extracts
冬虫夏草中腺苷含量的测定

摘要目的:建立用HPLC 法测定冬虫夏草及含片中腺苷的含量。
方法:C18(4.6mm× 250mm,5um)色谱柱,0.05mol L·-1磷酸二氢钾+甲醇(90+10)为流动相,流速为 1.0ml·min-1 检测波长260nm,柱温为35℃。
结果:腺苷含量在0.005~0.2ug(r=0.9998)范围内呈良好的线性关系。
平均回收率为99.49%,RSD=1.47%。
结论:方法准确可靠、、结果稳定、重现性好,分析速度快,可有效控制制剂的质量。
关键字:HPLC;冬虫夏草菌粉;含片;腺苷;DADAbstractObjective: to determine the content of adenosine Cordyceps powder andtablets by HPLC method. Methods: kromasil--C18 ( 4.6mm × 250mm ,5um) column, using methanol two hydrogen 0.5mol ? L-1 phosphoric acid (90:10) as mobile phase, thef low rate was 1.0ml ? min-1, the detection wavelength was 260nm, the column temperature was 35℃. Results: adenosine in 0.005 ~ 0.2ug (r=09998) showed a good linear relationship in the range of. The average recovery was 101.16%, RSD=1.47%. Conclusion: the method isConclusion: the method is accurate and reliable, strong specificity, results stability, good reproducibility, which can effectively control the quality of the preparation. Keywords: Cordyceps sinensis powder; tablet; adenosine; HPLC目录摘要 (I)Abstract ................................................................. I.I. ..1. 前言 (2)1.1仪器与试药..............................................2...2. 实验条件 (2)2.1供试品提取溶剂的选择.................................... 2...2.2检测波长的选择.......................................... 2...2.3流动相的选择............................................3...3. 试验方法与结果.............................................. 3...3.1分析溶液 (3)3.1.1 ..................................................................................................... 对照品溶液制备 ............................................ 3...3.1.2 ..................................................................................................... 供试品溶液制备 ............................................ 3...3.2色谱条件 (3)3.3分析方法学考察.......................................... 3...3.3.1 ..................................................................................................... 系统适应性试验 ............................................ 3...3.3.2 ..................................................................................................... 标准曲线绘制及线型范围考察 ................................. 4..3.3.3 ..................................................................................................... 精密度试验 ................................................ 4...3.3.4 ..................................................................................................... 重复性试验 ................................................ 4...3.3.5 ..................................................................................................... 稳定性试验 ................................................ 4...3.3.6 ..................................................................................................... 加样回收率试验 ............................................ 4...3.3.7 ..................................................................................................... 样品测定 .................................................. 5...4. 讨论 (5)4.1 (5)4.2 (5)4.3 (5)参考文献: (6)致谢 (7)1. 前言冬虫夏草,仅仅是我国190 多种虫草中的一种,也是中药传统的滋补药材。
注射用头孢洛林酯说明书(美国,英文)

1 23 4 5 678 91011 12 1314151617 18192021 22 23242554HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use TEFLARO safely and effectively. See full prescribing information for TEFLARO®.TEFLARO® (ceftaroline fosamil) injection for intravenous (IV) use Initial U.S. Approval: 2010To reduce the development of drug-resistant bacteria and maintain theeffectiveness of Teflaro and other antibacterial drugs, Teflaro should be used onlyto treat infections that are proven or strongly suspected to be caused by bacteria.-----------------------RECENT MAJOR CHANGES------------------------------------ Dosage and Administration (2.3) XX/2012 --------------------------INDICATIONS AND USAGE--------------------------------Teflaro ® is a cephalosporin antibacterial indicated for the treatment of the following infections caused by designated susceptible bacteria:• Acute bacterial skin and skin structure infections (ABSSSI)(1.1) • Community-acquired bacterial pneumonia (CABP) (1.2) ------------------------DOSAGE AND ADMINISTRATION-------------------------• 600 mg every 12 hours by IV infusion administered over 1 hour in adults ≥ 18 years of age (2.1) • Dosage adjustment in patients with renal impairment (2.2)Estimated CreatinineClearance # (mL/min) Teflaro Dosage Regimen > 50 No dosage adjustment necessary > 30 to ≤ 50 400 mg IV (over 1 hour) every 12 hours ≥ 15 to ≤ 30 300 mg IV (over 1 hour) every 12 hours End-stage renal disease (ESRD), including hemodialysis200 mg IV (over 1 hour) every 12 hours#As calculated using the Cockcroft-Gault formula -----------------------DOSAGE FORMS AND STRENGTHS -----------------------600 mg or 400 mg of sterile Teflaro powder in single-use 20 mL vials. (3) 26--------------------------CONTRAINDICATIONS---------------------------- 27 ∙Known serious hypersensitivity to ceftaroline or other members of28 the cephalosporin class. (4)29 -----------------------WARNINGS AND PRECAUTIONS----------------- 30 ∙Serious hypersensitivity (anaphylactic) reactions have been31 reported with beta-lactam antibiotics, including ceftaroline. 32 Exercise caution in patients with known hypersensitivity to beta33 lactam antibiotics. (5.1) 34 ∙Clostridium difficile -associated diarrhea (CDAD) has been35 reported with nearly all systemic antibacterial agents, including36 Teflaro. Evaluate if diarrhea occurs. (5.2)37 ∙Direct Coombs’ test seroconversion has been reported with38 Teflaro. If anemia develops during or after therapy, a diagnostic 39 workup for drug-induced hemolytic anemia should be performed 40 and consideration given to discontinuation of Teflaro. (5.3) 41 -----------------------------ADVERSE REACTIONS------------------------42 The most common adverse reactions occurring in >2 % of patients are 43 diarrhea, nausea, and rash. (6.3) 44 45 To report SUSPECTED ADVERSE REACTIONS, contact Forest46 Pharmaceuticals, Inc., at 1-800-678-1605 or FDA at 1-800-FDA47 1088 or /medwatch. 48 ---------------------------USE IN SPECIFIC POPULATIONS-------------49 ∙Dosage adjustment is required in patients with moderate or severe50 renal impairment and in ESRD patients, including patients on51 hemodialysis.(2.2, 12.3) 52 53See 17 for PATIENT COUNSELING INFORMATIONRevised:XX/2012 5556 FULL PRESCRIBING INFORMATION: CONTENTS* 84 8.4 Pediatric Use85 8.5 Geriatric Use 57 1 INDICATIONS AND USAGE86 8.6 Patients with Renal Impairment58 1.1 Acute Bacterial Skin and Skin Structure 87 10 OVERDOSAGE59 Infections 88 11 DESCRIPTION 60 1.2 Community-Acquired Bacterial Pneumonia 89 12 CLINICAL PHARMACOLOGY61 1.3 Usage90 12.1 Mechanism of Action62 2 DOSAGE ANDADMINISTRATION 91 12.2 Pharmacodynamics 63 2.1 Recommended Dosage 92 12.3 Pharmacokinetics64 2.2 Patients with Renal Impairment 93 12.4 Microbiology65 2.3 Preparation of Solutions 94 13 NONCLINICAL TOXICOLOGY66 3 DOSAGE FORMS AND STRENGTHS 95 13.1 Carcinogenesis,Mutagenesis, Impairment of 67 4 CONTRAINDICATIONS 96 Fertility 68 5 WARNINGS AND PRECAUTIONS 97 14 CLINICAL TRIALS69 5.1 Hypersensitivity Reactions 98 14.1 Acute Bacterial Skin and Skin Structure70 5.2 Clostridium difficile -associated Diarrhea 99 Infections71 5.3 Direct Coombs’ Test Seroconversion 100 14.2 Community-Acquired Bacterial Pneumonia72 5.4 Development of Drug-Resistant Bacteria 101 15 REFERENCES 73 6 ADVERSE REACTIONS 102 16 HOW SUPPLIED/STORAGE AND HANDLING 74 6.1 Adverse Reactions from Clinical Trials 103 17 PATIENT COUNSELING INFORMATION 75 6.2 Serious Adverse Events and Adverse 10476 Events Leading to Discontinuation 77 6.3 Most Common Adverse Reactions 10578 6.4 Other Adverse Reactions Observed During 106 *Sections or subsections omitted from the full prescribing information79 Clinical Trials of Teflaro107 are not listed.80 7 DRUGINTERACTIONS 81 8 USE IN SPECIFIC POPULATIONS82 8.1 Pregnancy83 8.3 Nursing MothersPage 1 of 13108 FULL PRESCRIBING INFORMATION 109 1. INDICATIONS AND USAGE110 Teflaro® (ceftaroline fosamil) is indicated for the treatment of patients with the following infections caused by susceptible isolates of the designated 111 microorganisms. 112 1.1Acute Bacterial Skin and Skin Structure Infections113 Teflaro is indicated for the treatment of acute bacterial skin and skin structure infections (ABSSSI) caused by susceptible isolates of the following Gram114 positive and Gram-negative microorganisms:Staphylococcus aureus (including methicillin-susceptible and -resistant isolates), Streptococcus pyogenes ,115 Streptococcus agalactiae , Escherichia coli , Klebsiella pneumoniae, and Klebsiella oxytoca. 116 1.2Community-Acquired Bacterial Pneumonia117 Teflaro is indicated for the treatment of community-acquired bacterial pneumonia (CABP) caused by susceptible isolates of the following Gram-positive118 and Gram-negative microorganisms: Streptococcus pneumoniae (including cases with concurrent bacteremia),Staphylococcus aureus (methicillin119 susceptible isolates only), Haemophilus influenzae, Klebsiella pneumoniae, Klebsiella oxytoca, and Escherichia coli. 120 1.3 Usage121 To reduce the development of drug-resistant bacteria and maintain the effectiveness of Teflaro and other antibacterial drugs, Teflaro should be used to 122 treat only ABSSSI or CABP that are proven or strongly suspected to be caused by susceptible bacteria. Appropriate specimens for microbiological123 examination should be obtained in order to isolate and identify the causative pathogens and to determine their susceptibility to ceftaroline. When culture124 and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local125 epidemiology and susceptibility patterns may contribute to the empiric selection of therapy. 126 2. DOSAGE AND ADMINISTRATION 127 2.1Recommended Dosage128 The recommended dosage of Teflaro is 600 mg administered every 12 hours by intravenous (IV) infusion over 1 hour in patients ≥ 18 years of age. The129 duration of therapy should be guided by the severity and site of infection and the patient’s clinical and bacteriological progress. 130 The recommended dosage and administration by infection is described in Table 1.131Table 1: Dosage of Teflaro by InfectionInfection Dosage FrequencyInfusion Time(hours)RecommendedDuration ofTotal Antimicrobial TreatmentAcute Bacterial Skin and Skin Structure Infection(ABSSSI) 600 mg Every 12 hours 1 5-14 days Community-Acquired Bacterial Pneumonia (CABP)600 mg Every 12 hours 1 5-7 days 132133 2.2 Patients with Renal Impairment 134Table 2: Dosage of Teflaro in Patients with Renal Impairment 135 136 137 138 139 140 141Estimated CrCl a (mL/min) Recommended Dosage Regimen for Teflaro> 50No dosage adjustment necessary > 30 to ≤ 50 400 mg IV (over 1 hour) every 12 hours ≥ 15 to ≤ 30 300 mg IV (over 1 hour) every 12 hours End-stage renal disease,including hemodialysis b 200 mg IV (over 1 hour) every 12 hours c ab End-stage renal disease is defined as CrCl < 15 mL/min.cTeflaro is hemodialyzable; thus Teflaro should be administered after hemodialysis on hemodialysis days.2.3 Preparation of SolutionsAseptic technique must be followed in preparing the infusion solution. The contents of Teflaro vial should be constituted with 20 mL Sterile Water forInjection, USP; or 0.9% of sodium chloride injection (normal saline); or 5% of dextrose injection; or lactated ringer’s injection . The preparation of Teflaro solutions is summarized in Table 3.143 Table 3: Preparation of Teflaro for Intravenous UseDosage Strength(mg) Volume of Diluent To BeAdded(mL)Approximate Ceftarolinefosamil Concentration(mg/mL)Amount to Be Withdrawn400 20 20 Total Volume600 20 30 Total Volume144145 The constituted solution must be further diluted in 250 mL before infusion. Use the same diluent for this further dilution, unless sterile water for 146 injection was used earlier. If sterile water for injection was used earlier, then appropriate infusion solutions include: 0.9% Sodium Chloride 147 Injection, USP (normal saline); 5% Dextrose Injection, USP; 2.5% Dextrose Injection, USP, and 0.45% Sodium Chloride Injection, USP; or Lactated 148 Ringer’s Injection, USP. The resulting solution should be administered over approximately 1 hour.149 Constitution time is less than 2 minutes. Mix gently to constitute and check to see that the contents have dissolved completely. Parenteral drug products 150 should be inspected visually for particulate matter prior to administration.151 The color of Teflaro infusion solutions ranges from clear, light to dark yellow depending on the concentration and storage conditions. When stored as 152 recommended, the product potency is not affected.153 Studies have shown that the constituted solution in the infusion bag should be used within 6 hours when stored at room temperature or within 24 hours 154 when stored under refrigeration at 2 to 8º C (36 to 46º F).155 The compatibility of Teflaro with other drugs has not been established. Teflaro should not be mixed with or physically added to solutions containing other 156 drugs.157 3. DOSAGE FORMS AND STRENGTHS158 Teflaro is supplied in single-use, clear glass vials containing either 600 mg or 400 mg of sterile ceftaroline fosamil powder.159 4. CONTRAINDICATIONS160 Teflaro is contraindicated in patients with known serious hypersensitivity to ceftaroline or other members of the cephalosporin class. Anaphylaxis and 161 anaphylactoid reactions have been reported with ceftaroline.162 5. WARNINGS AND PRECAUTIONS163 5.1 Hypersensitivity Reactions164 Serious and occasionally fatal hypersensitivity (anaphylactic) reactions and serious skin reactions have been reported in patients receiving beta-lactam 165 antibacterials. Before therapy with Teflaro is instituted, careful inquiry about previous hypersensitivity reactions to other cephalosporins, penicillins, or 166 carbapenems should be made. If this product is to be given to a penicillin- or other beta-lactam-allergic patient, caution should be exercised because cross 167 sensitivity among beta-lactam antibacterial agents has been clearly established.168 If an allergic reaction to Teflaro occurs, the drug should be discontinued. Serious acute hypersensitivity (anaphylactic) reactions require emergency 169 treatment with epinephrine and other emergency measures, that may include airway management, oxygen, intravenous fluids, antihistamines, 170 corticosteroids, and vasopressors as clinically indicated.171 5.2 Clostridium difficile-associated Diarrhea172 Clostridium difficile-associated diarrhea (CDAD) has been reported for nearly all systemic antibacterial agents, including Teflaro, and may range in 173 severity from mild diarrhea to fatal colitis.174 Treatment with antibacterial agents alters the normal flora of the colon and may permit overgrowth of C. difficile.175 C. difficile produces toxins A and B which contribute to the development of CDAD. Hypertoxin-producing strains of C. difficile cause increased 176 morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all 177 patients who present with diarrhea following antibiotic use. Careful medical history is necessary because CDAD has been reported to occur more than 2 178 months after the administration of antibacterial agents.179 If CDAD is suspected or confirmed, antibacterials not directed against C. difficile should be discontinued, if possible. Appropriate fluid and electrolyte 180 management, protein supplementation, antibiotic treatment of C. difficile, and surgical evaluation should be instituted as clinically indicated [see Adverse 181 Reactions (6.3)].182 5.3 Direct Coombs’ Test Seroconversion183 Seroconversion from a negative to a positive direct Coombs’ test result occurred in 120/1114 (10.8%) of patients receiving Teflaro and 49/1116 (4.4%) of 184 patients receiving comparator drugs in the four pooled Phase 3 trials.185 In the pooled Phase 3 CABP trials, 51/520 (9.8%) of Teflaro-treated patients compared to 24/534 (4.5%) of ceftriaxone-treated patients seroconverted 186 from a negative to a positive direct Coombs’ test result. No adverse reactions representing hemolytic anemia were reported in any treatment group.187 If anemia develops during or after treatment with Teflaro, drug-induced hemolytic anemia should be considered. Diagnostic studies including a direct 188 Coombs’ test, should be performed. If drug-induced hemolytic anemia is suspected, discontinuation of Teflaro should be considered and supportive care 189 should be administered to the patient (i.e. transfusion) if clinically indicated.191192 5.4 Development of Drug-Resistant Bacteria193 Prescribing Teflaro in the absence of a proven or strongly suspected bacterial infection is unlikely to provide benefit to the patient and increases the risk 194 of the development of drug-resistant bacteria.195 6. ADVERSEREACTIONS196 The following serious events are described in greater detail in the Warnings and Precautions section197 ∙Hypersensitivity reactions [see Warnings and Precautions (5.1)]198 ∙Clostridium difficile-associated diarrhea [see Warnings and Precautions (5.2)]199 ∙Direct Coombs’ test seroconversion [see Warnings and Precautions (5.3)]200 6.1 Adverse Reactions from Clinical Trials201 Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in clinical trials of a drug cannot be compared 202 directly to rates from clinical trials of another drug and may not reflect rates observed in practice.203 Teflaro was evaluated in four controlled comparative Phase 3 clinical trials (two in ABSSSI and two in CABP) which included 1300 adult patients treated 204 with Teflaro (600 mg administered by IV over 1 hour every 12h) and 1297 patients treated with comparator (vancomycin plus aztreonam or ceftriaxone) 205 for a treatment period up to 21 days. The median age of patients treated with Teflaro was 54 years, ranging between 18 and 99 years old. Patients treated 206 with Teflaro were predominantly male (63%) and Caucasian (82%).207 6.2 Serious Adverse Events and Adverse Events Leading to Discontinuation208 In the four pooled Phase 3 clinical trials, serious adverse events occurred in 98/1300 (7.5%) of patients receiving Teflaro and 100/1297 (7.7%) of patients 209 receiving comparator drugs. The most common SAEs in both the Teflaro and comparator treatment groups were in the respiratory and infection system 210 organ classes (SOC). Treatment discontinuation due to adverse events occurred in 35/1300 (2.7%) of patients receiving Teflaro and 48/1297 (3.7%) of 211 patients receiving comparator drugs with the most common adverse events leading to discontinuation being hypersensitivity for both treatment groups at a 212 rate of 0.3% in the Teflaro group and 0.5% in comparator group.213 6.3 Most Common Adverse Reactions214 No adverse reactions occurred in greater than 5% of patients receiving Teflaro. The most common adverse reactions occurring in > 2% of patients 215 receiving Teflaro in the pooled phase 3 clinical trials were diarrhea, nausea, and rash.216 Table 4 lists adverse reactions occurring in ≥ 2% of patients receiving Teflaro in the pooled Phase 3 clinical trials.217 Table 4: Adverse Reactions Occurring in ≥ 2% of Patients Receiving Teflaro in the Pooled Phase 3 Clinical TrialsSystem Organ Class/ Preferred TermPooled Phase 3 Clinical Trials(four trials, two in ABSSSI and two in CABP)Teflaro(N=1300)Pooled Comparators a(N=1297) Gastrointestinal disordersDiarrhea 5 % 3 %Nausea 4 % 4 %Constipation 2 % 2 %Vomiting 2 % 2 %InvestigationsIncreased transaminases 2% 3 %Metabolism and nutrition disordersHypokalemia 2 % 3 %Skin and subcutaneous tissue disordersRash 3%2%Vascular disordersPhlebitis 2%1% 218 a219 IV every 24h in the Phase 3 CABP trials.220221222 6.4 Other Adverse Reactions Observed During Clinical Trials of Teflaro223 Following is a list of additional adverse reactions reported by the 1740 patients who received Teflaro in any clinical trial with incidences less than 2%. 224 Events are categorized by System Organ Class.225 Blood and lymphatic system disorders - Anemia, Eosinophilia, Neutropenia, Thrombocytopenia226 Cardiac disorders - Bradycardia, Palpitations227 Gastrointestinal disorders -Abdominal pain228 General disorders and administration site conditions - Pyrexia229 Hepatobiliary disorders - Hepatitis230 Immune system disorders - Hypersensitivity, Anaphylaxis231 Infections and infestations -Clostridium difficile colitis232 Metabolism and nutrition disorders - Hyperglycemia, Hyperkalemia233 Nervous system disorders -Dizziness, Convulsion234 Renal and urinary disorders - Renal failure235 Skin and subcutaneous tissue disorders - Urticaria236 7. DRUGINTERACTIONS237 No clinical drug-drug interaction studies have been conducted with Teflaro. There is minimal potential for drug-drug interactions between Teflaro and 238 CYP450 substrates, inhibitors, or inducers; drugs known to undergo active renal secretion; and drugs that may alter renal blood flow [see Clinical 239 Pharmacology (12.3)].240 8. USE IN SPECIFIC POPULATIONS241 8.1 Pregnancy242 Category B243 Developmental toxicity studies performed with ceftaroline fosamil in rats at IV doses up to 300 mg/kg demonstrated no maternal toxicity and no effects 244 on the fetus. A separate toxicokinetic study showed that ceftaroline exposure in rats (based on AUC) at this dose level was approximately 8 times the 245 exposure in humans given 600 mg every 12 hours. There were no drug-induced malformations in the offspring of rabbits given IV doses of 25, 50, and 246 100 mg/kg, despite maternal toxicity. Signs of maternal toxicity appeared secondary to the sensitivity of the rabbit gastrointestinal system to broad247 spectrum antibacterials and included changes in fecal output in all groups and dose-related reductions in body weight gain and food consumption at > 50 248 mg/kg; these were associated with an increase in spontaneous abortion at 50 and 100 mg/kg. The highest dose was also associated with maternal 249 moribundity and mortality. An increased incidence of a common rabbit skeletal variation, angulated hyoid alae, was also observed at the maternally toxic 250 doses of 50 and 100 mg/kg. A separate toxicokinetic study showed that ceftaroline exposure in rabbits (based on AUC) was approximately 0.8 times the 251 exposure in humans given 600 mg every 12 hours at 25 mg/kg and 1.5 times the human exposure at 50 mg/kg.252 Ceftaroline fosamil did not affect the postnatal development or reproductive performance of the offspring of rats given IV doses up to 450 mg/kg/day. 253 Results from a toxicokinetic study conducted in pregnant rats with doses up to 300 mg/kg suggest that exposure was ≥ 8 times the exposure in humans 254 given 600 mg every 12 hours.255 There are no adequate and well-controlled trials in pregnant women. Teflaro should be used during pregnancy only if the potential benefit justifies the 256 potential risk to the fetus.257 8.3 Nursing Mothers258 It is not known whether ceftaroline is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when Teflaro 259 is administered to a nursing woman.260 8.4 Pediatric Use261 Safety and effectiveness in pediatric patients have not been established.262 8.5 Geriatric Use263 Of the 1300 patients treated with Teflaro in the Phase 3 ABSSSI and CABP trials, 397 (30.5%) were ≥65 years of age. The clinical cure rates in the 264 Teflaro group (Clinically Evaluable [CE] Population) were similar in patients ≥65 years of age compared with patients < 65 years of age in both the 265 ABSSSI and CABP trials.266 The adverse event profiles in patients ≥ 65 years of age and in patients < 65 years of age were similar. The percentage of patients in the Teflaro group who 267 had at least one adverse event was 52.4% in patients ≥ 65 years of age and 42.8% in patients < 65 years of age for the two indications combined.268 Ceftaroline is excreted primarily by the kidney, and the risk of adverse reactions may be greater in patients with impaired renal function. Because elderly 269 patients are more likely to have decreased renal function, care should be taken in dose selection in this age group and it may be useful to monitor renal 270 function. Elderly subjects had greater ceftaroline exposure relative to non-elderly subjects when administered the same single dose of Teflaro. However, 271 higher exposure in elderly subjects was mainly attributed to age-related changes in renal function. Dosage adjustment for elderly patients should be based 272 on renal function [see Dosage and Administration (2.2) and Clinical Pharmacology (12.3)].275 8.6 Patients with Renal Impairment276 Dosage adjustment is required in patients with moderate (CrCl > 30 to ≤50 mL/min) or severe (CrCl ≥ 15 to ≤30 mL/min) renal impairment and in 277 patients with end-stage renal disease (ESRD – defined as CrCl < 15 mL/min), including patients on hemodialysis (HD) [see Dosage and Administration 278 (2.2) and Clinical Pharmacology (12.3)].279 10. OVERDOSAGE280 In the event of overdose, Teflaro should be discontinued and general supportive treatment given.281 Ceftaroline can be removed by hemodialysis. In subjects with ESRD administered 400 mg of Teflaro, the mean total recovery of ceftaroline in the 282 dialysate following a 4-hour hemodialysis session started 4 hours after dosing was 76.5 mg (21.6% of the dose). However, no information is available on 283 the use of hemodialysis to treat overdosage [see Clinical Pharmacology (12.3)].284 11. DESCRIPTION285 Teflaro is a sterile, semi-synthetic, broad-spectrum, prodrug antibacterial of cephalosporin class of beta-lactams (β-lactams). Chemically, the prodrug, 286 ceftaroline fosamil monoacetate monohydrate is (6R,7R)-7-{(2Z)-2-(ethoxyimino)-2-[5-(phosphonoamino)-1,2,4-thiadiazol-3-yl]acetamido}-3-{[4-(1287 methylpyridin-1-ium-4-yl)-1,3-thiazol-2-yl]sulfanyl}-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylate monoacetate monohydrate. Its molecular 288 weight is 762.75. The empirical formula is C22H21N8O8PS4.C2H4O2.H2O.289 Figure 1: Chemical structure of ceftaroline fosamil290291292293294295296297298299300 301 302 Teflaro vials contain either 600 mg or 400 mg of anhydrous ceftaroline fosamil. The powder for injection is formulated from ceftaroline fosamil monoacetate monohydrate, a pale yellowish-white to light yellow sterile powder. All references to ceftaroline activity are expressed in terms of the prodrug, ceftaroline fosamil. The powder is constituted for IV injection [see Dosage and Administration (2.3)].303 Each vial of Teflaro contains ceftaroline fosamil and L-arginine, which results in a constituted solution at pH 4.8 to 6.5. 304 12. CLINICAL PHARMACOLOGY305 Ceftaroline fosamil is the water-soluble prodrug of the bioactive ceftaroline [see Clinical Pharmacology (12.3)]. 306 12.1 Mechanism of Action307 Ceftaroline is an antibacterial drug [see Clinical Pharmacology (12.4)].308 12.2 Pharmacodynamics309 310 311 As with other beta-lactam antimicrobial agents, the time that unbound plasma concentration of ceftaroline exceeds the minimum inhibitory concentration (MIC) of the infecting organism has been shown to best correlate with efficacy in a neutropenic murine thigh infection model with S. aureus and S. pneumoniae.312 313 314 Exposure-response analysis of Phase 2/3 ABSSSI trials supports the recommended dosage regimen of Teflaro 600 mg every 12 hours by IV infusion over 1 hour. For Phase 3 CABP trials, an exposure-response relationship could not be identified due to the limited range of ceftaroline exposures in the majority of patients.315 Cardiac Electrophysiology316 317 318 In a randomized, positive- and placebo-controlled crossover thorough QTc study, 54 healthy subjects were each administered a single dose of Teflaro 1500 mg, placebo, and a positive control by IV infusion over 1 hour. At the 1500 mg dose of Teflaro, no significant effect on QTc interval was detected at peak plasma concentration or at any other time.319 12.3 Pharmacokinetics320 321 322 The mean pharmacokinetic parameters of ceftaroline in healthy adults (n=6) with normal renal function after single and multiple 1-hour IV infusions of 600 mg ceftaroline fosamil administered every 12 hours are summarized in Table 5. Pharmacokinetic parameters were similar for single and multiple dose administration.323326 Table 5: Mean (Standard Deviation) Pharmacokinetic Parameters of Ceftaroline IV in Healthy AdultsParameter Single 600 mg Dose Administered asa 1-Hour Infusion(n=6)Multiple 600 mg Doses Administered Every12 Hours as 1-Hour Infusions for 14Days(n=6)C max (mcg/mL) 19.0 (0.71) 21.3 (4.10)T max (h)a 1.00 (0.92-1.25) 0.92 (0.92-1.08)AUC (mcg h/mL) b 56.8 (9.31) 56.3 (8.90)T1/2 (h) 1.60 (0.38) 2.66 (0.40)CL (L/h) 9.58 (1.85) 9.60 (1.40)a Reported as median (range)b AUC0-∞,for single-dose administration; AUC0-tau, for multiple-dose administration; C max, maximum observed concentration; T max, time of C max; AUC0-∞, area under concentration-time curve from time 0 to infinity; AUC0-tau, area under concentration-time curveover dosing interval (0-12 hours); T1/2, terminal elimination half-life; CL, plasma clearance327328 The C max and AUC of ceftaroline increase approximately in proportion to dose within the single dose range of 50 to 1000 mg. No appreciable 329 accumulation of ceftaroline is observed following multiple IV infusions of 600 mg administered every 12 hours for up to 14 days in healthy adults with 330 normal renal function.331 Distribution332 The average binding of ceftaroline to human plasma proteins is approximately 20% and decreases slightly with increasing concentrations over 1-50 333 mcg/mL (14.5-28.0%). The median (range) steady-state volume of distribution of ceftaroline in healthy adult males (n=6) following a single 600 mg IV 334 dose of radiolabeled ceftaroline fosamil was 20.3 L (18.3-21.6 L), similar to extracellular fluid volume.335 Metabolism336 Ceftaroline fosamil is converted into bioactive ceftaroline in plasma by a phosphatase enzyme and concentrations of the prodrug are measurable in plasma 337 primarily during IV infusion. Hydrolysis of the beta-lactam ring of ceftaroline occurs to form the microbiologically inactive, open-ring metabolite 338 ceftaroline M-1. The mean (SD) plasma ceftaroline M-1 to ceftaroline AUC0-∞ ratio following a single 600 mg IV infusion of ceftaroline fosamil in 339 healthy adults (n=6) with normal renal function is 28% (3.1%).340 When incubated with pooled human liver microsomes, ceftaroline was metabolically stable (< 12% metabolic turnover), indicating that ceftaroline is not a 341 substrate for hepatic CYP450 enzymes.342 Excretion343 Ceftaroline and its metabolites are primarily eliminated by the kidneys. Following administration of a single 600 mg IV dose of radiolabeled ceftaroline 344 fosamil to healthy male adults (n=6), approximately 88% of radioactivity was recovered in urine and 6% in feces within 48 hours. Of the radioactivity 345 recovered in urine approximately 64% was excreted as ceftaroline and approximately 2% as ceftaroline M-1. The mean (SD) renal clearance of ceftaroline 346 was 5.56 (0.20) L/h, suggesting that ceftaroline is predominantly eliminated by glomerular filtration.347 Specific Populations348 Renal Impairment349 Following administration of a single 600 mg IV dose of Teflaro, the geometric mean AUC0-∞ of ceftaroline in subjects with mild (CrCl > 50 to ≤ 80 350 mL/min, n=6) or moderate (CrCl > 30 to ≤50 mL/min, n=6) renal impairment was 19% and 52% higher, respectively, compared to healthy subjects with 351 normal renal function (CrCl > 80 mL/min, n=6). Following administration of a single 400 mg IV dose of Teflaro, the geometric mean AUC0-∞ of 352 ceftaroline in subjects with severe (CrCl ≥ 15 to ≤30 mL/min, n=6) renal impairment was 115% higher compared to healthy subjects with normal renal 353 function (CrCl > 80 mL/min, n=6). Dosage adjustment is recommended in patients with moderate and severe renal impairment [see Dosage and 354 Administration (2.2)].355 A single 400 mg dose of Teflaro was administered to subjects with ESRD (n=6) either 4 hours prior to or 1 hour after hemodialysis (HD). The geometric 356 mean ceftaroline AUC0-∞ following the post-HD infusion was 167% higher compared to healthy subjects with normal renal function (CrCl > 80 mL/min, 357 n=6). The mean recovery of ceftaroline in the dialysate following a 4-hour HD session was 76.5 mg, or 21.6% of the administered dose. Dosage 358 adjustment is recommended in patients with ESRD (defined as CrCL < 15 mL/min), including patients on HD [see Dosage and Administration (2.2)]. 359 Hepatic Impairment360 The pharmacokinetics of ceftaroline in patients with hepatic impairment have not been established. As ceftaroline does not appear to undergo significant 361 hepatic metabolism, the systemic clearance of ceftaroline is not expected to be significantly affected by hepatic impairment.362 Geriatric Patients363 Following administration of a single 600 mg IV dose of Teflaro to healthy elderly subjects (≥65 years of age, n=16), the geometric mean AUC0-∞ of 364 ceftaroline was ~33% higher compared to healthy young adult subjects (18-45 years of age, n=16). The difference in AUC0-∞ was mainly attributable to。
哈西奈德倍他米松等糖皮质激素类原料药简介.doc

东康源糖皮质激素类原料药简介1.醋酸地塞米松醋酸地塞米松又叫做醋酸氟甲强的松龙,国际上叫做Dexamethasone-17-acetate,属于糖皮质激素类原料药,具有抗炎、抗过敏作用,适用于类风湿性关节炎和其他胶原性疾病等,可用于生化研究。
醋酸地塞米松的CAS登入号是1177-87-3,分子式是C24H31FO6,分子量为434.5。
外表为白色或类白色结晶性粉末,无臭,味微苦。
醋酸地塞米松在丙酮中易溶,在甲醇或乙醇中溶解,在乙醇或氯仿中略溶,在乙mi中极微溶解,在水中不溶。
熔点215-227℃。
2.泼尼松龙磷酸钠泼尼松龙磷酸钠又叫做氢化泼尼松磷酸钠,国际上叫做Prednisolone phosphate sodium,属于糖皮质激素类原料药,具有抗炎、抗过敏作用,可用于生化研究。
泼尼松龙磷酸钠的CAS登入号是125-02-0,分子式是C21H27Na2O8P,分子量为484.39。
外表为白色或类白色结晶性粉末,无臭。
3.地塞米松磷酸钠地塞米松磷酸钠又叫做21-磷酸地塞米松,国际上叫做Dexamethasone 21-phosphate disodium salt,属于糖皮质激素类原料药,具有抗炎、抗过敏、抗毒素、抗休克四大作用,可用于生化研究。
地塞米松磷酸钠的CAS登入号是2392-39-4,分子式是C22H28FNa2O8P,分子量为516.4。
外表为白色或类白色结晶性粉末,无臭。
4.醋酸曲安奈德醋酸曲安奈德又叫做曲安奈德醋酸酯,国际上叫做Triamcinolone acetonide 21-acetate,属于糖皮质激素类原料药,为曲安西龙(去炎松)的衍生物,作用与曲安西龙相似,具有抗炎、抗过敏、抗瘙痒和收缩毛细血管的作用,其水钠潴留作用微弱,而抗炎、抗过敏作用均比氢化可的松(10~30倍)、泼尼松强而持久,气雾吸入治疗支气管哮喘,作用强且持久。
对局部作用疗效较曲安西龙好。
醋酸曲安奈德的CAS登入号是3870-07-3,分子式是C26H33FO7,分子量为476.5344232。
美索巴莫注射液标准

美索巴莫注射液标准美索巴莫注射液是一种中枢性肌肉松弛剂,主要用于治疗急性骨骼肌疼痛或不适症状。
以下是关于美索巴莫注射液的一些标准信息:1. 中文通用名:美索巴莫注射液2. 英文通用名:Methocarbamol Injection3. 标准号:ws-10001-(hd-0269)-20024. 药品名称:美索巴莫注射液5. 药品英文名:Methocarbamol Injection6. 主要成分:本品为美索巴莫的灭菌聚乙二醇,400水溶液。
含美索巴莫(c11h15no5)应为标示量的95.0%~105.%。
7. 处方:具体处方应根据医生建议和患者病情来确定。
8. 性状:本品为无色或几乎无色略带黏稠的澄明液体。
9. 鉴别:通过化学分析和物理测试等方法来鉴别美索巴莫注射液的真伪和质量。
10. 作用类别:中枢性肌肉松弛剂11. 药理毒理:本品对中枢神经系统有选择作用,特别对脊椎中神经元作用明显。
抑制与骨骼肌痉挛有关的神经突触反射,有抗士的宁和电刺激所致惊厥的作用,并有解痉、镇痛和抗炎作用。
其作用机制主要是阻断脊髓内中枢神经元从而使骨骼肌松弛。
12. 药代动力学:美索巴莫注射液在体内的吸收、分布、代谢和排泄过程。
13. 适应症:主要用于急性骨骼肌疼痛或不适症状的辅助治疗。
14. 用法用量:美索巴莫注射液的用法主要是采用静脉滴注或者是静脉推注的方式给药。
如果是用于静脉推注时,患者在静卧的条件下缓慢推注,给药的速度每分钟不可以超过3ml,注射之后应该至少休息10~15分钟。
如果是用于静脉滴注时,将药品配在9%的氯化钠注射液或者是5%的葡萄糖注射液当中,滴注的速度不宜过快。
使用剂量和次数根据病情和治疗效果来决定。
成人一次使用剂量为1.0g,一日最大剂量为3.0g,连续使用不得超过3天。
轻度病例静注后应改为口服给药以维持治疗。
15. 不良反应:使用美索巴莫注射液可能出现的不良反应,如头痛、恶心、呕吐、皮疹等。
16. 禁忌症:对美索巴莫过敏者、肝肾功能不全者、哺乳期妇女禁用。
植物病害诊断试剂盒
植物病害诊断试剂盒美国阿格迪agdia 公司是全球最大的植物病害诊断试剂生产商,产品品种最多,可检测项目多达200多个。
包装规格最全,不同的包装规格适合不同规模的实验室。
从中您一定能发现适合您使用的产品。
选购试剂说明,请仔细阅读。
1,kit, 订货号PSAxxxxx/xxxx 或PSPxxxxx/xxxx 为完整的试剂盒包装,包括样品提取缓冲液、包被好抗体的微孔板(可拆分)、酶标记物、稀释液、缓冲液、底物发色剂、阳性质控(如果应该供应)。
特别注明Indirect ELISA 方法的kit 包括未包被的微孔板及联接用的抗体,所含有的其他组分同上。
2, Reagent Set, 订货号SRAxxxxx/xxxx ,XRAxxxxx/xxxx或SRPxxxxx/xxxx 只含有未包被的微孔板、包被需要的抗体或联接用的抗体、酶标记物。
其他试剂如样品提取缓冲液、稀释液、缓冲液、底物发色剂、质控物需另外订购或自己配制。
我公司销售原厂的上述试剂,详见目录。
3, Bacterial Reagent Set, 订货号BRAxxxxx/xxxx 只含有未包被的微孔板、包被需要的抗体或联接用的抗体、酶标记物。
其他试剂如样品提取缓冲液、稀释液、缓冲液、底物发色剂、质控物需另外订购或自己配制。
我公司销售原厂的上述试剂,详见目录。
4, Bacterial ID订货号BIDxxxxx/xxxx 为完整的试剂盒包装,包括样品提取缓冲液、包被好抗体的微孔板(可拆分)、酶标记物、稀释液、缓冲液、底物发色剂、质控(如果应该供应)。
用于鉴定培养基中或有病症植物提取液中的细菌。
操作简便快速。
5, PS A或SR A中的A代表碱性磷酸酶标记;PS P或SR P中的P代表过氧化物酶标记。
6, Immunostrip test, 为检试纸条,操作简单,几分钟内得到结果,非常适合于现场检测。
该试条必须与相应的样品提取缓冲液配套使用。
实验室需要单独购买该样品提取缓冲液,详见目录。
碧云天生物技术柠檬酸钠-EDTA抗原修复液(40X)说明书

碧云天生物技术/Beyotime Biotechnology 订货热线:400-1683301或800-8283301 订货e-mail :******************技术咨询:*****************网址:碧云天网站 微信公众号柠檬酸钠-EDTA 抗原修复液(40X) 产品编号产品名称 包装 P0086 柠檬酸钠-EDTA 抗原修复液(40X) 125ml产品简介:碧云天生产的柠檬酸钠-EDTA 抗原修复液(Citrate-EDTA Antigen Retrieval Solution)是一种常用的抗原修复液,结合了柠檬酸钠和EDTA 进行抗原修复的优点,可以用于石蜡切片、冰冻切片等样品使用多聚甲醛、甲醛或其它醛类试剂固定后的抗原修复。
细胞或组织用多聚甲醛、甲醛或其它醛类试剂固定后,会导致蛋白之间的交联(cross-link),从而遮蔽样品的抗原位点,导致免疫染色时染色信号减弱,甚至出现一些假阳性染色结果。
本抗原修复液采用了常用的柠檬酸钠缓冲液和EDTA ,结合了两者修复抗原的优点,并经过适当优化,可以更加有效地去除醛类固定试剂导致的蛋白之间的交联,充分暴露石蜡切片等样品中的抗原表位,从而大大改善免疫染色效果。
通常石蜡切片都需进行抗原修复处理,而冰冻切片可以不进行抗原修复处理。
抗原修复会大大改善石蜡切片的免疫染色效果,但对于冰冻切片的染色效果很多文献资料表明也有显著改善。
特别是当冰冻切片免疫染色效果欠佳时,可以考虑尝试进行抗原修复。
从原理上来看,无论冰冻切片还是细胞爬片等,只要是用多聚甲醛、甲醛或其它醛类试剂固定的样品,进行抗原修复都会有效去除蛋白之间的交联,充分暴露抗原表位,从而大大改善免疫染色效果。
本产品适用于石蜡切片,也可以用于冰冻切片等其它样品。
关于碧云天生产的各种抗原修复液的主要特点和差异可参考我们的相关网页:/support/antigen-retrieval-solution.htm 。
美罗培南三水化合物JP日本药典标准翻译
美罗培南三水化合物按无水物计算,美罗培南三水化合物的含量不得低于900μg/mg。
美罗培南三水化合物的量用美罗培南(C17H25N3O5S:383.46)表示。
性状:美罗培南三水化合物呈白色至微黄色结晶性粉末。
本品微溶于水,几乎不溶于乙醇(95)。
鉴别:(1)将0.01g美罗培南溶于2mL水中,加3mL盐酸羟铵乙醇试剂,静置5分钟,再加1mL酸性硫酸铵铁试液(Ⅲ),摇匀:红棕色沉淀。
(2)按紫外分光光度法测定美罗培南三水化合物和美罗培南三水化合物标准品(3→100000)的吸收光谱图,比较图谱:相同波长下两者的吸光度相似。
(3)按红外光谱法,将美罗培南三水化合物和美罗培南三水化合物标准品用溴化钾制成圆片状,记录红外光谱图,比较图谱:在相同的波数下两者的透光率相似。
旋光度[]20α:-17—-21°(称取0.22g(按无水物计算)溶于50ml水D中,100mm)。
pH将0.2g的美罗培南三水化合物溶于20ml水中:pH为4.0~6.0。
纯度(1)溶液的澄清度和颜色—另有规定(2)重金属—将2.0g美罗培南三水化合物根据方法2进行测试。
对照溶液中加入2.0ml标准铅溶液(不得过10ppm)。
(3)有关物质—另有规定。
水分11.4%~13.4%(0.15g,按库仑滴定法在140℃蒸发温度条件下用配有水分蒸发设备的滴定仪测定。
)炽灼残渣 另有规定细菌内毒素 <0.12EU/mg (含量)。
含量 精密称取0.05g (含量)美罗培南和美罗培南标准品,精确加入10ml 内部标准溶液溶解,加pH5.0磷酸三乙胺缓冲液定容至100ml,分别作为样品溶液和对照品溶液。
根据液相色谱条件分别进样5μL 样品溶液和对照品溶液进行测试,计算出美罗培南峰面积Q T 和美罗培南标准品峰面积Q S 的比值。
美罗培南(C 17H 25N 3O 5S )的量(μg 含量)=美罗培南三水化合物标准品的量(mg 含量)×ST Q Q ×1000 内标溶液—将乙醇苯甲基和磷酸三乙胺缓冲液(pH5.0)按1:300混合。
常用蛋白酶切割位点

LifeSensors
Ni-NTA (6His recomb. enzyme)
Kex-2
-Arg-X-Lys/Arg-Arg▼
Invitrogen – Life Technologies,
Ni-NTA (6His recomb. enzyme)
Ni-NTA (6His recomb. TEV)
PreScission(PreScisபைடு நூலகம்ion蛋白酶)
Leu-Glu-Val-Leu-Phe-Gln▼Gly-Pro
L-E-V-L-F-Q▼G-P
Amersham-Biosciences
GSTrap for GST fusion enzyme
TAGZyme(标记酶)
Factor Xa(Xa因子)
Ile-Glu/Asp-Gly-Arg▼?
I-E/D-G-R▼
Amersham-Biosciences,
New England Biolabs,
Roche
Benzamidine-Agarose
Enterokinase(肠激酶)
Asp-Asp-Asp-Asp-Lys▼
D-D-D-D-K▼
His-tag removal by Exoproteolytic Digestion
Qiagen
Ni-NTA (6His recomb. enzyme)
Intein Site(内含肽)
dithiothreitol cleavage(二硫苏糖醇清除)
New England Biolabs
DTT elimination by dialysis?(透析)
New England Biolabs,
巴斯夫叶黄素酯Xangold

安全技术说明书页: 1/10 巴斯夫安全技术说明书按照GB/T 16483编制日期 / 本次修订: 27.05.2023版本: 4.0日期/上次修订: 28.02.2022上次版本: 3.0日期 / 首次编制: 12.02.2014产品: 叶黄素酯Product: Xangold® 10% (Beadlet)(30530885/SDS_GEN_CN/ZH)印刷日期 28.08.20231. 化学品及企业标识叶黄素酯Xangold® 10% (Beadlet)推荐用途和限制用途: 饮食补充, 食品工业原料公司:巴斯夫(中国)有限公司中国上海浦东江心沙路300号邮政编码 200137电话: +86 21 20391000传真号: +86 21 20394800E-mail地址: **********************紧急联络信息:巴斯夫紧急热线中心(中国)+86 21 5861-1199巴斯夫紧急热线中心(国际):电话: +49 180 2273-112Company:BASF (China) Co., Ltd.300 Jiang Xin Sha RoadPu Dong Shanghai 200137, CHINA Telephone: +86 21 20391000Telefax number: +86 21 20394800E-mail address: ********************** Emergency information:Emergency Call Center (China):+86 21 5861-1199International emergency number: Telephone: +49 180 2273-1122. 危险性概述纯物质和混合物的分类:根据 GHS 标准,该产品不需要进行分类。
巴斯夫安全技术说明书日期 / 本次修订: 27.05.2023版本: 4.0产品: 叶黄素酯Product: Xangold® 10% (Beadlet)(30530885/SDS_GEN_CN/ZH)印刷日期 28.08.2023 标签要素和警示性说明:根据GHS标准,该产品不需要添加危险警示标签其它危害但是不至于归入分类:在一定条件下,产品可形成粉尘爆炸。
FTY720 (S)-Phosphate说明书
1. PRODUCT AND COMPANY IDENTIFICATION1.1 Product identifierProduct name :FTY720 (S)-Phosphate Catalog No. :HY-15382CAS No. :402616-26-61.2 Relevant identified uses of the substance or mixture and uses advised against Identified uses :Laboratory chemicals, manufacture of substances.1.3 Details of the supplier of the safety data sheetCompany:MedChemExpress USA Tel:609-228-6898Fax:609-228-5909E-mail:1.4 Emergency telephone numberEmergency Phone #:609-228-68982. HAZARDS IDENTIFICATION2.1 Classification of the substance or mixtureNot a hazardous substance or mixture.2.2 GHS Label elements, including precautionary statementsNot a hazardous substance or mixture.2.3 Other hazardsNone.3. COMPOSITION/INFORMATION ON INGREDIENTS3.1 SubstancesSynonyms:(S)-FTY720P; (S)-FTY720 phosphate Formula:C 19H 34NO 5P Molecular Weight:387.45CAS No. :402616-26-64. FIRST AID MEASURES4.1 Description of first aid measuresEye contactRemove any contact lenses, locate eye-wash station, and flush eyes immediately with large amounts of water. Separate eyelids with fingers to ensure adequate flushing. Promptly call a physician. Skin contactSafety Data SheetRevision Date:Feb.-22-2021Print Date:Jan.-22-2023Inhibitors •Screening Libraries•ProteinsRinse skin thoroughly with large amounts of water. Remove contaminated clothing and shoes and call a physician.InhalationImmediately relocate self or casualty to fresh air. If breathing is difficult, give cardiopulmonary resuscitation (CPR). Avoid mouth-to-mouth resuscitation.IngestionWash out mouth with water; Do NOT induce vomiting; call a physician.4.2 Most important symptoms and effects, both acute and delayedThe most important known symptoms and effects are described in the labelling (see section 2.2).4.3 Indication of any immediate medical attention and special treatment neededTreat symptomatically.5. FIRE FIGHTING MEASURES5.1 Extinguishing mediaSuitable extinguishing mediaUse water spray, dry chemical, foam, and carbon dioxide fire extinguisher.5.2 Special hazards arising from the substance or mixtureDuring combustion, may emit irritant fumes.5.3 Advice for firefightersWear self-contained breathing apparatus and protective clothing.6. ACCIDENTAL RELEASE MEASURES6.1 Personal precautions, protective equipment and emergency proceduresUse full personal protective equipment. Avoid breathing vapors, mist, dust or gas. Ensure adequate ventilation. Evacuate personnel to safe areas.Refer to protective measures listed in sections 8.6.2 Environmental precautionsTry to prevent further leakage or spillage. Keep the product away from drains or water courses.6.3 Methods and materials for containment and cleaning upAbsorb solutions with finely-powdered liquid-binding material (diatomite, universal binders); Decontaminate surfaces and equipment by scrubbing with alcohol; Dispose of contaminated material according to Section 13.7. HANDLING AND STORAGE7.1 Precautions for safe handlingAvoid inhalation, contact with eyes and skin. Avoid dust and aerosol formation. Use only in areas with appropriate exhaust ventilation.7.2 Conditions for safe storage, including any incompatibilitiesKeep container tightly sealed in cool, well-ventilated area. Keep away from direct sunlight and sources of ignition.Recommended storage temperature:Powder-20°C 3 years* The compound is unstable in solutions, freshly prepared is recommended.Shipping at room temperature if less than 2 weeks.7.3 Specific end use(s)No data available.8. EXPOSURE CONTROLS/PERSONAL PROTECTION8.1 Control parametersComponents with workplace control parametersThis product contains no substances with occupational exposure limit values.8.2 Exposure controlsEngineering controlsEnsure adequate ventilation. Provide accessible safety shower and eye wash station.Personal protective equipmentEye protection Safety goggles with side-shields.Hand protection Protective gloves.Skin and body protection Impervious clothing.Respiratory protection Suitable respirator.Environmental exposure controls Keep the product away from drains, water courses or the soil. Cleanspillages in a safe way as soon as possible.9. PHYSICAL AND CHEMICAL PROPERTIES9.1 Information on basic physical and chemical propertiesAppearance SolidOdor No data availableOdor threshold No data availablepH No data availableMelting/freezing point No data availableBoiling point/range No data availableFlash point No data availableEvaporation rate No data availableFlammability (solid, gas)No data availableUpper/lower flammability or explosive limits No data availableVapor pressure No data availableVapor density No data availableRelative density No data availableWater Solubility No data availablePartition coefficient No data availableAuto-ignition temperature No data availableDecomposition temperature No data availableViscosity No data availableExplosive properties No data availableOxidizing properties No data available9.2 Other safety informationNo data available.10. STABILITY AND REACTIVITY10.1 ReactivityNo data available.10.2 Chemical stabilityStable under recommended storage conditions.10.3 Possibility of hazardous reactionsNo data available.10.4 Conditions to avoidNo data available.10.5 Incompatible materialsStrong acids/alkalis, strong oxidising/reducing agents.10.6 Hazardous decomposition productsUnder fire conditions, may decompose and emit toxic fumes.Other decomposition products - no data available.11.TOXICOLOGICAL INFORMATION11.1 Information on toxicological effectsAcute toxicityClassified based on available data. For more details, see section 2Skin corrosion/irritationClassified based on available data. For more details, see section 2Serious eye damage/irritationClassified based on available data. For more details, see section 2Respiratory or skin sensitizationClassified based on available data. For more details, see section 2Germ cell mutagenicityClassified based on available data. For more details, see section 2CarcinogenicityIARC: No component of this product present at a level equal to or greater than 0.1% is identified as probable, possible or confirmed human carcinogen by IARC.ACGIH: No component of this product present at a level equal to or greater than 0.1% is identified as a potential or confirmed carcinogen by ACGIH.NTP: No component of this product present at a level equal to or greater than 0.1% is identified as a anticipated or confirmed carcinogen by NTP.OSHA: No component of this product present at a level equal to or greater than 0.1% is identified as a potential or confirmed carcinogen by OSHA.Reproductive toxicityClassified based on available data. For more details, see section 2Specific target organ toxicity - single exposureClassified based on available data. For more details, see section 2Specific target organ toxicity - repeated exposureClassified based on available data. For more details, see section 2Aspiration hazardClassified based on available data. For more details, see section 2Additional informationThis information is based on our current knowledge. However the chemical, physical, and toxicological properties have not been completely investigated.12. ECOLOGICAL INFORMATION12.1 ToxicityNo data available.12.2 Persistence and degradabilityNo data available.12.3 Bioaccumlative potentialNo data available.12.4 Mobility in soilNo data available.12.5 Results of PBT and vPvB assessmentPBT/vPvB assessment unavailable as chemical safety assessment not required or not conducted.12.6 Other adverse effectsNo data available.13. DISPOSAL CONSIDERATIONS13.1 Waste treatment methodsProductDispose substance in accordance with prevailing country, federal, state and local regulations.Contaminated packagingConduct recycling or disposal in accordance with prevailing country, federal, state and local regulations.14. TRANSPORT INFORMATIONDOT (US)Proper shipping name: Not dangerous goodsUN number: -Class: -Packing group: -IMDGProper shipping name: Not dangerous goodsUN number: -Class: -Packing group: -IATAProper shipping name: Not dangerous goodsUN number: -Class: -Packing group: -15. REGULATORY INFORMATIONSARA 302 Components:No chemicals in this material are subject to the reporting requirements of SARA Title III, Section 302.SARA 313 Components:This material does not contain any chemical components with known CAS numbers that exceed the threshold (De Minimis) reporting levels established by SARA Title III, Section 313.SARA 311/312 Hazards:No SARA Hazards.Massachusetts Right To Know Components:No components are subject to the Massachusetts Right to Know Act.Pennsylvania Right To Know Components:CAS No.FTY720 (S)-Phosphate402616-26-6New Jersey Right To Know Components:CAS No.FTY720 (S)-Phosphate402616-26-6California Prop. 65 Components:This product does not contain any chemicals known to State of California to cause cancer, birth defects, or anyother reproductive harm.16. OTHER INFORMATIONCopyright 2023 MedChemExpress. The above information is correct to the best of our present knowledge but does not purport to be all inclusive and should be used only as a guide. The product is for research use only and for experienced personnel. It must only be handled by suitably qualified experienced scientists in appropriately equipped and authorized facilities. The burden of safe use of this material rests entirely with the user. MedChemExpress disclaims all liability for any damage resulting from handling or from contact with this product.Caution: Product has not been fully validated for medical applications. For research use only.Tel:609-228-6898Fax:609-228-5909E-mail:***********************Address: 1 Deer Park Dr, Suite Q, Monmouth Junction, NJ 08852, USA。
膜蛋白相互作用Manual_mbSUS
Manual for the use ofmating-based Split ubiquitin system"mbSUS"version APetr ObrdlikOctober 2004Introduction and general informationAbbreviationsX = prey peptide/ORFY = bait prey/ORFN = NubGC = CubPLV = protA-LexA-VP16 peptideHA tag = hemagglutinin epitope tagAde = adenineHis = histidineTrp = tryptophanLeu = leucineUra = uracilMet = methionineX-Gal = 5-bromo-4-chloro-3-indol-b-D-galactosidase ONPG = o-nitrophenylgalactopyranosideSC = synthetic complete mediumSD = synthetic dextrose / minimal medium SSDNA = carrier DNA from salmon spermmbSUS package contentsYou have received the package with mating-based Split ubiquitin system "mbSUS". This package contains:yeast strains THY.AP4 and THY.AP5vectors (resuspended in dH2O, ca. 50 ng/ul)1pXNgate21-3HA 2pNXgate33-3HA 3pX-NubWTgate 4pNubWT-Xgate 5pMetYCgatecontrol constructs (resuspended in dH2O, ca. 50 ng/ul)6KAT1-Cub (Arabidopsis K+ channel, Acc. At5g46240)7KAT1-N11N-KAT1-3HARestriction analysis:The maps of the vectors and control constructs are shown in the section "Maps of vectors and control constructs". The sequences of the vectors1-5 in genebank format are in the "Appendix".General information, protocols, maps and sequences of the vectors are included in this manual. For further information please check Obrdlik etal., 2004 and Ludewig et al., 2003.References and citationWhen citing the system, the vectors pXNgate21-3HA, pX-NubWTgate, pNubWT-Xgate and pMetYCgate, and the control constructs please refer to the publication Obrdlik et al., 2004, PNAS 101; 12242-12247.When citing the vector pNXgate33-3HA, please refer to C. Cappellaro and E. Boles, University of Frankfurt, unpublished.Differences to the vectors published in Obrdlik et al., 2004The vectors pXNgate21-3HA and pNXgate33-3HA are based on the corresponding vectors pXNgate and pNXgate in Obrdlik et al. (2004). Their additional feature is the triple HA tag, which allows the construction of ORF-NubG-3HA and NubG-ORF-3HA fusions. The triple HA tag is readily detectable with anti-HA antibodies. In addition, pNXgate33-3HA is a low-copy CEN plasmid and produces significantly higher signal/noise ratio when compared to pNXgate in Obrdlik et al. (2004).Please note that the control construct KAT1-N has not a triple but single HA-tag peptide fused to the C-terminus!The mbSUS in briefGeneral information-The vectors are designed for recombinational in vivo cloning in yeast: you need only one PCR-product of the gene of interest, which you can insert in any of the Nub or Cub vectors ("In vivo cloning into mbSUS vectors" and Fig. 4 and 5).- Big plus: the linkers in our system contain attB1 and attB2 sites, which are compatible with GATEWAY cloning (Invitrogen). Thus you can use either the PCR products or the resulting Split-ubiquitin constructs for further cloning into any of the GATEWAY destination vectors (Fig. 6). Nevertheless, keep in mind that the mbSUS vectors themselves are NOT DESTINATION VECTORS!-Expression of CubPLV fusions can be optimized since it is under the control of MET25 promoter. We routinely test interactions on different methionine concentrations.-We use two different yeast strains: THY.AP5 is Mat mating type strain and is designed for the transformation with Nub fusions, the second strain THY.AP4 [Mat a] is designed for transformation with CubPLV fusions. Therefore we can test the interactions by mating approach in diploid cells. (see "mbSUS tests protocol" and Fig. 5)-There are three reporter constructs in our yeast strains: lexA-HIS3, lexA-Ade2 and lexA-lacZ. Thus we can select the interacting partners via growth (on -Ade-His media), by white color on non-selective media (+Ade+His) or via ß-galactosidase assays (Fig. 3)-NubG vectors possess a 3 x HA tag at their C-termini, it is detectable in most of the Nub fusions tested. This is useful if you want to show, that the Nub fusions are indeed expressed. - There are also vectors for construction NubWT-X and X-NubWT fusions. Especially X-NubWT fusions can be useful since the affinity of NubG for Cub in X-NubG is often very low and hardly shows any interaction (see also below).- The empty NubWT-X gate vector (i.e. soluble NubWT peptide) should also be used as a positive control.Control constructs (C=Cub, N=NubG)The system works very well for KAT1 interactions: we use the homomerization of KAT1 as a positive control in our assays. Hence the KAT1-C, KAT1-N and N-KAT1-3HA are included as positive controls. KAT1-N contains a single HA tag at the C-terminus.NubG-X or X-NubG fusions ?In general, Cub has higher affinity to Nub fused to the N-termini of prey (Nub-X fusions) than to Nub fused to C-termini of prey (X-Nub fusions).When testing interactions with a set of X-NubG fusions (e.g. KAT1-Cub with X-NubG fusions) the signal/background ratio is usually very high. However you may not be able to detect "weak" interactions.When using NubG-X fusions it is important to test, that your CubPLV fusions do not show background activities in growth assays with different NubG-X fusions (false positives)! It is crucial to use several different NubG-X fusions as negative controls! An empty pNXgate33-3HA vector (soluble NubG peptide) is not enough!If you observe background problems you can perform quantitative -galactosidase assays (measuring lacZ activity, Obrdlik et al., 2004, Ludewig et al., 2003), which can distinguish between false and true interactions. Alternatively try to adjust a proper methionine concentration in the medium.Important!For in vivo cloning of the PCR product combined with direct interaction tests use pools of 5-10 independent clones as described in the protocol for screening "mbSUS tests protocol". In this way it is possible to suppress the effects of non-functional mutants. Such mutations can be caused by the RT-PCR as well as by the recombination events during in vivo cloning (rare but possible mutations in the vicinity of homologous regions).The sensitivity of the methods for detection of interaction:The growth assays via selection on media -Ade-His-Trp-Leu-Ura is the most sensitive one. The detection of interactions via lacZ-activity by X-Gal assays and liquid ONPG assays is not as sensitive but liquid assays are useful for quantitative analysis. The detection of interactions by monitoring the white (interaction) and red (no interaction) color of diploid cells (Fig. 3) is the least sensitive and can be used only in addition to the other detection methods.Check-list before you start your experiments with mbSUS1) In order to check CubPLV fusions, use the empty pNXgate33-3HA and pNubWT-Xgate vectors as negative and positive controls, respectively.2) It is not sufficient to use the empty pNXgate33-3HA vector as a negative control. Use also NubG fusions of several other membrane proteins as negative controls!3) If you want to construct X-Nub fusions, consider also creating X-NubWT fusions. X-NubWT fusions can provide specific results if you analyze the interactions via quantitative lacZ assays (but do not forget negative controls from 2!).4) For the production of a B1-ORF-B2 inserts by PCR ("In vivo cloning into mbSUS vectors" and Fig. 4) it is better to start from a sequenced DNA template. Using this you will reduce the risk of mistakes produced during PCR.ProtocolsThis section contains protocols adapted for mbSUS. General protocol s and the preparation of general media and chemical s shoul d be performed as described in "Methods in Yeast Genetics" (Adams et al., Cold Spring Harbor Lab. Press) and in "Current Protocols in Molecular Biology" (Ausubel et al., John Wiley & Sons Inc.).In vivo cloning into mbSUS vectors pNXgate33-3HA, pXNgate21-3HA, pNubWT-Xgate, pX-NubWTgate and pMetYCgatePrinciple of the in vivo cloning is described in Obrdlik et al., 2004 and in Fig. 4 of this manual.For in vivo cloning into mbSUS vectors the ORFs have to be flanked by B1 and B2 linkers via PCR. In parallel the vector pMetYCgate and the Nub vectors have to be restricted with PstI/HindIII and with EcoRI/SmaI, respectively.Both, the B1-ORF-B2 PCR product and the appropriate linear vector are used to co-transform either THY.AP4or THY.AP5 yeast (Fig. 4 and 5). Homologous recombination between B1 and B2 sequences of the B1-ORF-B2 and of the linear vector produces circular vector harboring the ORF. Transformants are selected on -Leu (CubPLV fusions) or on -Trp (Nub fusions).1): B1 and B2 linker sequences of the vectorsLinker B1attB1aca agt ttg tac aaa aaa gca ggc tct cca acc acc atgT S L Y K K A G S P T T MetLinker B2attB2 BamHItac cca gct ttc ttg tac aaa gtg gtt ggt ggt ggc gga tcc ggt gga ggt gga tca Y P A F L Y K V V G G G G S G G G G S The underlined B1 and B2 nucleotid sequences are crucial for GATEWAY cloning and may not be changed according to codon usage rules (even if the corresponding amino acid is the same)! (Invitrogen; Hartley et al. (2000) Genome Research 10: 1788; Walhout et al. (2000) Science 287:116).2): Primer design for in vivo cloning into mbSUS vectorsB2 B1-forward primer (5´strand)B1-linker start-ORFaca agt ttg tac aaa aaa gca ggc tct cca acc acc atg xxx-5´strand cDNAB2-reverse primer (3´strand)B2-linkertcc gcc acc acc aac cac ttt gta caa gaa agc tgg gta xxx-3´strand cDNA w/o stop!3): Enzymes for the cleavage of the mbSUS vectors for in vivo cloningpXNgate3HA, pX-NubWTgate:Eco RI & Sma IpNXgate3HA, pNubWT-Xgate: Eco RI & Sma IpMetYCgate:Pst I & Hind IIIMbSUS tests protocolSee also Fig. 3, 4 and 5Recombinational in vivo cloning:1. Cut the vectors with restriction enzymes as described in "In vivo cloning into mbSUS vectors". Purify the fragments via agarose gel.2. Make a B1-ORF-B2 insert by PCR using primers described in "In vivo cloning into mbSUS vectors". Purify the PCR fragments via affinity columns.3. Co-transform a linear vector and the B1-ORF-B2 insert into either THY.AP4 (Cubs)or THY.AP5 (Nubs) as described in "LiAc Transformation". Do not forget totransform the linear vector alone (negative control!). Plate on appropriate mediawithout Leu (Cub vectors in THY.AP4) or without Trp (Nub vectors in THY.AP5).Mating:4. Collect 5-10 independent clones and mix them in 0.1 ml dH2O. Use 20-100 µl of this suspension to inoculate 5ml of the appropriate SC media without G418 and 5 ml with G418 (starting cultures should be only slightly turbid).5. Grow cells over night to the stationary phase (stock culture). Cells carrying vectorswith inserts should not grow on G418.6. Concentrate 1ml of the cultures by centrifugation in a final volume of 200µl YPD.200 µl are enough for 13 crossings. For higher number of crossings use a highervolume of the culture (e.g. for 26 crossings concentrate 2ml culture in 400 µl YPD).Mating and replica plating is more efficient if the final suspension is not too thin!7. Mix 15 µl of the appropriate mating types for each cross. You can use microtiter platesfor large number of interactions.8. Drop 4 µl of the mixed suspensions on a YPD-plate (this should give a patch of about7mm). It takes a while for the liquid to be adsorbed. For that reason plates should be pre-dried under a hood.9. Mate the cells for 6-8h at 28°C.10. Replica plating on SC/+Ade+His; make minimum 2 replicas of each YPD plate11. Selection of diploid cells (2-3 days incubation at 28°C).Interaction growth tests:12. Replica plating of the cells on 4 different plates (synthetic minimal medium )a) + 0 mM methionine b) + 75 µM methionine c) + 150 µM methionine d) + 400 µM methionine13. In addition to replica plating it is recommended to streak out the colonies on syntheticminimal medium with different methionine concentrations to check for growthproperties!14. After two days at 30°C start to record the growth.X-gal tests:15. Replica plating of the cells on different plates(synthetic minimal medium +ADE, +HIS, )a) + 0 mM methionineb) + 150 µM methionine16. After 2-3 days test the -galactosidase activity by "X-Gal Overlay assay".Met stock: 67mmol/L(1g/100ml)0.112ml/100ml 0.224ml/100ml 0.597ml/100mlSynthetic minimal medium (SD)2% w/v Glucose0,17% w/v yeast nitrogen base without ammonium sulfate and amino acids0,5% ammonium sulfatepH adjusted to 6-6,3 with NaOHSynthetic complete medium (SC)like SD medium but add to 1L medium1,5g of "AHTLUM"-drop out (-Ade, -His, -Leu, -Trp, -Ura, -Met)add appropriate chemicals for auxotrophy selection (see below)AHTLUM minus drop-outstandard protocol for drop-out, but without Adenine, Histidine, Leucine, Tryptophan, Uracil, MethionineChemicals for auxotrophy selectionall dissolved in dH2O and sterilized by filteringchemical stock conc.vol (ml) stock storage(g/100ml) f or 1L mediumA adenine sulfate0.210RTU uracil0.210RTT L-tryptophan124°CL L-leucine1104°CH L-histidine HCl124°CMet L-methionine124°Call these can be added to the media before autoclaving !!!Verifying detected interactionsThe interactions identified in the directed mbSUS tests with the in-vivo cloned ORFs (Fig. 5 and "mbSUS tests protocol") have to be verified.1) isolate the plasmid DNA form yeast ("Lazy-bones method for rapid release of plasmid DNA from yeast")2) Amplify the plasmid DNA in E.coli.3) Isolate the plasmid DNA from E.coli and verify the expression cassette by restriction analysis and by sequencing4) Use the verified plasmid DNA instead of B1-ORF-B2 and linear vectors for mbSUS interaction tests as described "mbSUS tests protocol".LiAc transformation of yeast(modified protocol of Gietz & Schiestl, 1995)Work all the time under strictly sterile conditions!Making competent cells1. Incubate one colony of THY.AP5 and THY.AP5, each at 28°C for ca. 24 h (shaking in 5 ml YPAD)2. Early in the morning: Inoculate 100 ml pre-warmed YPAD with the pre-culture to an OD600 0.08-0,1.3. Incubate at 28°C and 180-200 rpm till OD600 0.5-0,6.Important: Minimal incubation time = time necessary for 2-3 duplications!4. Place cells in sterile tubes (FALCON), centrifuge at 2.500 x g for 5 min (20°C).5. Remove the medium, re-suspend pellets in 5 ml sterile ddH2O each and re-centrifuge againas described above.6. Remove ddH2O, re-suspend each pellet in 2,5 ml LiAc/TE, pool the suspensions togetherand mix carefully.7. Centrifuge (5 min; 2.500 x g, 20°C) and remove the supernatant.8. Re-suspend the pellet carefully in 0.5-0.8 ml LiAc/TE, let the suspension incubate for30min at RT (competent cells!). If you use the cells later than 30 min after this step than keep them at 4°C.Transformationbefore starting: boil the SSDNA for 3 min and chill it on ice immediately9. For each transformation add in the following order:-20 µl carrier-SSDNA (5 or 10 mg/ml)-20 µl DNA-mix: = 1x TE buffer and DNAeither: plasmid alone (0,1 - 10 µg)or: linear plasmid (100 ng) plus insert (>100 ng), (molecular ratio of vectorvs insert at least 1:10)! mix well !- 4,5 µl 1M LiAc! mix well !-50 µl competent cells, !mix well!-300 µl PEG/LiAc mix (prepare it fresh each time!!!) and mix well!!!13. Incubate shaking for 20 min at 30°C (thermo-mixer)14. Heat-shock in 42°C-waterbath for 20 min (keep the time!!!)15. Centrifuge at 6000 - 8000 rpm for 1 min and carefully remove the supernatant with a micropipette16. Resuspend the pellet carefully in 100µl sterile dH2O (or sterile 1x TE buffer) with thepipette.17. Streak the transformation on appropriate selective media (The media on petri dishes should be dry!).For transformation of THY.AP4 with Cub constructs: SC/+AHTUFor transformation of THY.AP5 with Nub constructs: SC/+AHL!!! For some purposes the transformation efficiency may be too high and it will be difficult to isolate single colonies from the plates! In that case resuspend the cells (step 16) in 1ml of sterile dH2O and streak out 100µl on the plate18. Grow for 2-4 days at 28°C (30°C) on selective media.Stock solutions:1M LiAc:LiAc in ddH2O, pH not adjusted!, sterilize by filtering10 x TE:100 mM Tris Cl,10 mM EDTA, pH 7,5; adjust with NaOH50% PEG 3350 (Roth ) or PEG 4000 (Fluka)sterilize by autoclaving5mg/ml salmon sperm DNA (SSDNA), in 1xTEmake aliquots and keep in -20°C2 x 100 ml sterile ddH2Ochemicals for auxotrophy selection:all solutions are in ddH2O and sterilized by filtering:amino acid stock conc.vol (ml) stock storage(g/100ml) f or 1L mediumA adenine sulfate0.210RTU uracil0.210RTT L-tryptophan1 24°CL L-leucine1104°CH L-histidine HCl1 24°CMet L-methionine1 24°Call these can be added to the media before autoclaving !!!Media:YPAD:add 10 ml of sterile adenine stock to YPD mediaAHTLUM minus drop-out:standard protocol for drop-out, but without Adenine, Histidine, Leucine, Tryptophan, Uracil, MethionineSC- (synthetic complete medium):for 1L:1,7 g yeast nitrogen base w/o amino acids and ammonium sulfate5,0 g (NH4)2SO420 g glucose1,5 g of AHTLUM minus drop-out20 g Oxoid Agar; adjust pH at 6,0-6,3 with NaOHAdd the appropiate amount of auxotrophy selection chemicals. Leu, Trp, Met, Ade, His and Ura can be added to the medium before autoclaving.SD- (synthetic dextrose minimal medium):the same protocol as SC-medium, but without the AHTLUM minus drop-out Solutions:LiAc/TE1 ml 10 x TE1 ml 1M LiAc8 ml ddH2OPEG/LiAc mix:0,5 ml 10 x TE0,5 ml 1M LiAc4,0 ml 50% PEGX-Gal assaysOverlay assay1): Dissolve 0.25g agarose in 50ml Z-buffer (pH 7.2) in the microwave. Do not overheat, otherwise precipitation may occur! 50ml is enough for 3-4 petri dishes.2): Cool down the solution to 50°C and add 1ml of 10% SDS and 1ml of X-Gal solution (40mg/ml in DMF). The final concentration of X-Gal is 0.8mg/ml, for weak interactions one can also use final concentration of 2mg/ml.3): Pour the solution carefully over the plate. Incubate at 37°C for 5min to several hours.SolutionsZ-bufferNa2HPO4 x 2H2O10,68g/L (60mM) or: Na2HPO4 x 7 H2O; 16.1 g/L (60 mM)NaH2PO4 x H2O 5.5 g/Lg/LKCl 0.75MgSO4 x 7H2O0.246 g/Ladjust to pH 7.0 and autolave40mg/ml X-Gal, in DMF,store at -20°C10% SDSFilter assay1): Cut nitorcellulose filter under sterile conditions and place it (use sterile forceps) on a selective media plate.2): Streak the clones on the filter and incubate the petri dish at 30 °C for 2-4 days.3): Remove the filter carefully from the plate and place it for 5-10 sec. in liquid N2. Take it out and let it thaw at RT for 1 min.4): Repeat the step 3).5): Place the filter with colonies facing up on Whatman paper soaked with 2ml of freshly prepared Z-buffer/X-Gal solution (in a petri dish). Incubate closed petri dish in the dark for 30 min to ON (RT or 30°C)Solutions:Z-bufferdescribed aboveX-Gal solution80 mg/ml in DMFeach time freshly prepared: Z-buffer/X-Gal solution100 ml Z-buffer0.27 ml -mercaptoethanol1.67 ml X-Gal solution (final X-Gal conc. ca. 1.4 mg/ml)"Lazy bones" method for rapid release of plasmid DNA from yeast (Adapted from Kaiser et al., Methods in yeast Genetics, CSHL Press, 1994)1:Incubate one yeast colony at 28°C in 5ml YPD (ON) or in selective medium (1-2 days)2:Pellet 1.5ml of ON yeast cell culture at 5000xg for 5 min. Discard the supernatant.3:Add 0.2ml of the DNA release solution and resuspend the pellet.4: Add 0.2ml phenol:chloroform:isomylalcohol (25:24:1) and 0.3ml of acid washed glas beads.5: Vortex at high speed for 5-10 min.6:Centrifuge for 5 min at RT and full speed (Eppendorf centrifuge).7:Transfer 120µl the aqueous layer (the upper layer) to a new tube. Precipitate the DNA with 1xVol isopropanol and wash with 1xVol 70% EtOH. Resuspend the pellet in 30µl dH2O.8:To transform chemo-competent E.coli use 5-10µl of the DNA. For electro-competent cells use 1µl of the DNA.SolutionsDNA release solution:2% Triton X-1001% SDS100mM NaCl10mM Tris HCl (8.0)1mM Na-EDTA! do not autoclave !Acid washed beads:Use 250-500 micron beads (0,7-1,0mm should also work), work under a fume hood !!!Wash 100ml glass beads in 200ml conc. HCl (stir them carefully from time to time) and let them stand ON in a fume hood.Discard the HCl and wash the beads several times with dH2O, to the pH >5.0(if the pH is still below pH 3.0 after several washing steps, make the last wash with20mM Na2CO3, pH 7.0).Dry the beads in a glass beaker at 70°C ON and transfer them into a bottle.FiguresFig. 1: Reporter yeast strain THY.AP4 and expression cassette of the vector pMetYCgate. pMetYCgate is suited for "Y-CubPLV” fusions of bait peptides “Y”. B1-KanMX-B2 is identical with the B1-KanMX-B2 cassettes of the Nub vectors (Fig. 2). Promoter is red, term marks the terminator, the linkers B1 and B2 are green and yellow, respectively. Marked restriction sites are used to produce linear vectors for in vivo cloning.…ATG“ and …stop“ mark the start and the stop codon in the expression cassette. Amp R refers to ampicillin resistance cassette. CEN/ARS refers to a low-copy yeast origin of replication. Formore details on the pMetYCgate sequence see the appendix.Fig. 2: Yeast strain THY.AP5 and the expression cassettes of the Nub vectors. Nub vectors are suited for ”X-Nub” or “Nub-X” fusions of prey peptides “X”. All B1-KanMX-B2 cassettes are identical (see also Fig. 1). pADH is the ADH1 promoter, tADH marks the ADH1 terminator, NubG, NubWT, HA tag and the linkers B1 and B2 are shown below. Marked restriction sites are used to produce linear vectors for in vivo cloning. …ATG“ and …stop“ mark the start and the stop codons in the expression cassettes. Amp R refers to ampicillin resistance cassette. 2µ refers to a high-copy, CEN to a low-copy yeast origin of replication. All vectors carry TRP1 and AmpR selection markers. For more details on the vector sequences see theappendix.Fig. 3: Detection of interactions with mbSUS. To enable interaction-dependent cleavage of the PLV peptide, NubG and Cub have to be on the cytosolic face of the membrane. The cleaved PLV transcription factor diffuses into the nucleus, binds lexA-regulated promoters and activates the reporter genes. Activation of the reporter genes Ade2 and His3 allows selection of interactions via growth. In addition, lacZ allows detection of interactions by X-Gal staining and Ade2 enables red/white selection of interacting proteins (white = interaction,red = no interaction). LacZ activity can also be measured with quantitative Gal assays.Fig. 4: Principle of in vivo cloning into mbSUS vectors. The figure shows the construction of CubPLV fusions. Nub fusions are constructed in similar way using linear pXNgate21-3HA,pNXgate33-3Ha, pX-NubWTgate or pNubWT-Xgate vectors.THY.AP4. Leu, Trp, Ade and His is leucine, tryptophan, adenine and histidine.Fig. 6: mbSUS as an entry point for versatile analysis of membrane proteins. B1-ORF-B2 PCR products as well as the mbSUS fusions can be used as entry points to subclone the inserts into different GATEWAY destination vectors. DONR marks the pDONR vectors of GATEWAY (Invitrogen). Please note that the mbSUS vectors are NOT DESTINATIONVECTORS and thus are not suitable for direct cloning via GATEWAY!Maps of vectors and control constructspXNgate21-3HA, 8194 bp (TRP1, AmpR, 2µ)pNXgate33-3HA, 6682 bp (TRP1, AmpR, CEN)pX-NubWTgate, 8120 bp (TRP1, AmpR, 2µ)pNubWT-Xgate, 8118 bp (TRP1, AmpR, 2µ)pMetYCgate, 10033 bp (LEU2, AmpR, CEN/ARS)KAT1-C, 10580 bp (LEU2, AmpR, CEN/ARS)KAT1-N, 8667 bp(TRP1, AmpR, 2µ)N-KAT1-3HA, 7229 bp(TRP1, AmpR, CEN)31。
美国CLIA88质量要求
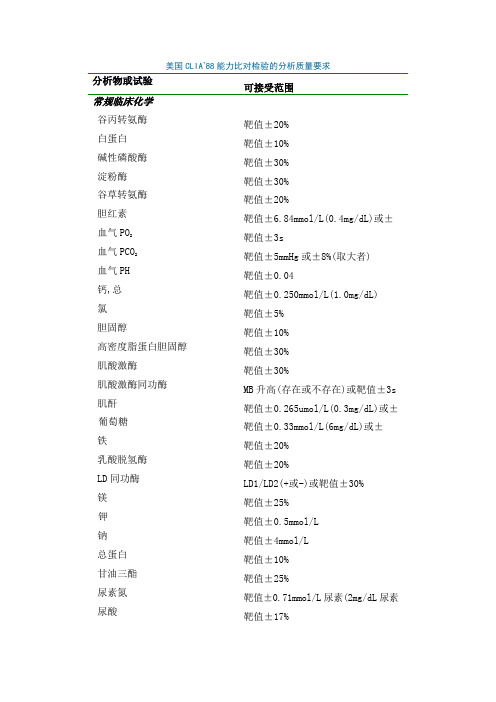
美国CLIA’88能力比对检验的分析质量要求分析物或试验可接受范围常规临床化学谷丙转氨酶靶值±20%白蛋白靶值±10%碱性磷酸酶靶值±30%淀粉酶靶值±30%谷草转氨酶靶值±20%胆红素靶值±6.84mmol/L(0.4mg/dL)或±血气PO2靶值±3s血气PCO2靶值±5mmHg或±8%(取大者)血气PH 靶值±0.04钙,总靶值±0.250mmol/L(1.0mg/dL)氯靶值±5%胆固醇靶值±10%高密度脂蛋白胆固醇靶值±30%肌酸激酶靶值±30%肌酸激酶同功酶MB升高(存在或不存在)或靶值±3s肌酐靶值±0.265umol/L(0.3mg/dL)或±葡萄糖靶值±0.33mmol/L(6mg/dL)或±铁靶值±20%乳酸脱氢酶靶值±20%LD同功酶LD1/LD2(+或-)或靶值±30%镁靶值±25%钾靶值±0.5mmol/L钠靶值±4mmol/L总蛋白靶值±10%甘油三酯靶值±25%尿素氮靶值±0.71mmol/L尿素(2mg/dL尿素尿酸靶值±17%内分泌皮质醇靶值±25%游离的甲状腺素靶值±3s人绒毛膜促性腺激素(HCG)靶值±3s或(阳性或阴性)T3 uptake 靶值±3s(方法)三碘甲状腺素原氨酸靶值±3s促甲状腺激素靶值±3s甲状腺素靶值±20%或12.9%(1.0ug/dL)(取大毒理学酒精,血靶值±25%血铅靶值±10%或±酰氨咪嗪(carbamazepine)靶值±25%地高辛(digoxin)靶值±20%或0.2ug/dL(更大)乙琥胺(ethosuximide)靶值±20%庆大霉素靶值±25%锂靶值±0.3mmol/L或±20%(更大)苯巴比妥(Phenobarbital)靶值±20%苯妥英(phenytion)靶值±25%扑痫酮(primidone)靶值±25%普鲁卡因酰氨(procainamid)(及代谢物) 靶值±25%奎尼丁(quinidine)靶值±25%茶碱(theophylline)靶值±25%妥布霉素(tobramycin)靶值±25%丙戊酸靶值±25%血液学细胞识别在分类上90%或更大的一致白细胞分类靶值±在不同类型白细胞百分数上红细胞计数靶值±6%血细胞容积靶值±6%血红蛋白靶值±7%白细胞计数靶值±15%血小板计数靶值±25%纤维蛋白原靶值±20%激活部分凝血酶时间靶值±15%凝血酶原时间靶值±15%一般免疫学1—抗胰蛋白酶靶值±3s抗核抗体靶值±2个稀释或(阳或阴)抗-HIV反应或不反应补体3靶值±3s补体4靶值±3s—甲胎蛋白靶值±3s肝炎(HBsAg,anti-HBc,HBeAg)反应(阳性)或不反应(阴性)IgA靶值±3sIgE靶值±3sIgG靶值±25%IgM靶值±3s传染性单核细胞增多(症)靶值±2个稀释或(阳性或阴性)类风湿因子靶值±2个稀释或(阳性或阴性)风疹(Rubella)靶值±2个稀释或(阳性或阴性)。