UPPER EXTREMITY-2
上肢功能指数的跨文化处理和信度与效度研究

functional
index,UEFI)评定量表是一种自评量表,该
量表将上肢作为一个功能整体,不受损伤部位和疾病 类型等因素影响。相关研究表明,UEFI量表具有较高 的信度、效度及反应度"…。本研究旨在描述UEFI评 定量表跨文化的适应处理过程,并评估汉化版UEFI
Upper extremity functional indexes;
be used for study and in the clinical evaluation of
upper extremity
【Key words】
Reliability;
Validity
手在日常生活活动及劳动中容易遭受创伤,约占 创伤总人数的1/3以上¨。,大多数患者遗留有不同程 度功能障碍。目前国内针对上肢功能障碍的评价指标 主要包括关节活动度、肌力、感觉以及x线、肌电图检 查等心3,但这些检查都是从医源性角度对功能进行评 价,不能反映患者主观感受、心理因素等对上肢功能的 影响,同时评定内容繁多、耗时较长。 目前国外针对上肢多部位、复杂病伤的评定工具 主要有臂肩手残疾调查问卷、上肢功能指数、上肢功能 量表(the
scale,UEFS)以及
颈和上肢指数(the
neck and upper limb
index,NULI)
等p1,但关于其相应中文版评定量表的研究较少卜3。 Stratford等"o创立的上肢功能指数(upper
extremity
DOI:10.3760/cma.j.issn,0254-1424.2012.012.006 作者单位:430022武汉,华中科技大学同济医学院附属协和医院康 复科 通信作者:杨朝辉,Email:annyha0430@yahoo.COrn.CN
常见上肢骨折的作业治疗PPT课件
支具
保持手部功能 保持复位后的稳定 防止关节挛缩和变形 防止和矫正畸形
关节运动
消肿 保持手部功
功能训练
编辑版ppt
8
一、肱骨颈骨折
肱骨颈是松质骨和密质骨 交接处,有臂丛神经和血 管经过,此骨折可合并有 神经,血管损伤。中、老 年为多,尤其是骨质疏松 者
术后4~6W:开始肩、肘、腕抗阻练习 术后6~8W:可适当增加阻力和ROM的幅度,争取上肢功能的
全面恢复 在整个治疗的过程中要注意患者的体温以防感染。
编辑版ppt
27
治疗
未经手术内固定者制动时间要长一些; 可制作支具来增加复位后骨折的稳定性; 2周后开始功能训练,根据恢复情况更进治疗处方直
ROM 训练
编辑版ppt
12
固定
(1)三角巾3~4周
(2)小夹板,U型石膏
(3)小夹板固定后,肩 外展70度位外展支架
(4)严重者、年龄大、
全身情况很差、三角巾; 手术,松质骨螺钉固定 近端,再T型钢板固定 或张力带钢丝固定。
13
编辑版ppt
OR + IF for fracture of humeral neck
编辑版ppt
24
编辑版ppt
25
处不稳理定 或病理性
◦ 麻醉下复位 + 肩关节固定 ◦ OR +IF (钢板 & 螺钉) ◦ 对于开放性/感染的骨折:OR + EF
编辑版ppt
26
治疗
术后1W:制动、休息;手、腕屈伸;上臂前臂的等长收缩练 习;消肿止痛的处理
术后2~3W:以无痛为限,可做肩周围肌群的收缩练习;前臂 内外旋练习;肘关节的主动收缩练习
76-34-2上肢骨、关节损伤 内容详实

1.幼儿青枝骨折:三角巾悬吊3W。 2.有移位的骨折
手法复位:横行8字绷带固定,3-4W, 注意上肢血管、神经压迫症状,随时 调整。 3.切开复位内固定
外科学————上肢骨、关节损伤(关节脱位)
• 切开复位内固定的指征
• (1)不能忍受8字绷带的痛苦 • (2)复位后再移位,影响外观 • (3)合并神经血管损伤 • (4)开放性骨折 • (5)陈旧骨折不愈合 • (6)锁骨外端骨折合并喙锁韧带断裂
第一节 锁骨骨折
Fracture of the Clavicle
外科学————上肢骨、关节损伤(关节脱位)
解剖概要 Anatomy summary
锁骨是上肢与躯干的连接和支撑装置,呈S形。 近端与胸骨柄形成胸锁关节,远端与肩峰形成肩 锁关节。外侧有喙锁韧带固定锁骨。
骨折好发于中1/3处或中外1/3交接处
Neer 分类
第三型 在第二型的基础上,合并有大结节或小结节骨 折,又称为“三部分骨折”。如合并大结节和小结节同 时骨折,又称为“四部分骨折”。
第四型 在第一型的基础上,合并大结节撕脱骨折伴有 明显移位,或大结节的一个面骨折。常伴有肩袖损伤。
第五型 有小结节骨折伴有移位。
第六型 肱骨近端骨折合并肱盂关节脱位。
外科学————上肢骨、关节损伤(关节脱位)
临床表现和诊断
Clinical Findings and Diagnosis
1.伤后局部肿胀、压痛。触及骨折端。
2.患肢活动障碍。(幼儿呈不愿上肢活动,穿衣伸 手泣啼应考虑)。
3.合并刺破皮肤或臂丛神经及锁骨下血管损伤,少 见。
外科学————上肢骨、关节损伤(关节脱位)
外科学————上肢骨、关节损伤(关节脱位)
中文版上肢技巧质量量表在脑性瘫痪患儿上肢功能评定中的信

2016年,第31卷,第1期中文版上肢技巧质量量表在脑性瘫痪患儿上肢功能评定中的信度和效度*王军1陈静1朱登纳1袁俊英1牛国辉1孙二亮1程萍萍1摘要目的:评估中文版上肢技巧质量量表(quality of upper extremity skills test,QUEST)在痉挛型脑瘫患儿上肢功能评定中的信度和效度。
方法:将英文版QUEST翻译并完善成中文版,研究对象为75例在我院就诊的痉挛型脑瘫儿童,检测其重测信度及评定者间信度。
同时进行Peabody运动发育量表的精细运动部分(peabody developmental motor scale fine motor, PDMS-FM),精细运动能力(fine motor function measure scale,FMFM),分析PDMS-FM原始分、FMFM各区分数与中文版QUEST各分测试项原始分之间的相关性,评估量表的平行效度。
结果:中文版QUEST分测试项得分及总分具有优良的重测信度及评估者间信度(ICC值均>0.890),中文版QUEST 分测试项原始分与PDMS-FM、FMFM各区原始分间具有较好的平行效度(Pearson/Spearson秩相关系数分别为r1=0.563—0.816、r2=0.389—0.830)。
结论:中文版QUEST量表具有良好的信度和效度,可以作为评估痉挛型脑瘫患儿上肢运动功能的首选方法。
关键词上肢技巧质量评估量表;上肢功能评定;痉挛型;脑性瘫痪;信度;效度中图分类号:R742.3,R493文献标识码:A文章编号:1001-1242(2016)-01-0041-04Reliability and validity of the Chinese version of the quality of upper extremity skills test on upper limb function of children with cerebral palsy/WANG Jun,CHEN Jing,ZHU Dengna,et al.//Chinese Journal of Rehabilitation Medicine,2016,31(1):41—44AbstractObjective:To investigate the reliability and validity of the Chinese version of the quality of upper extremity skills test(QUEST)applying to measure the upper limb function in children with cerebral palsy.Method:English version QUEST was translated and improved into Chinese version.Seventy-five children with spastic cerebral palsy participated.All children accepted QUEST assessments,and the test-retest reliability and inter-rater reliability data were collected.Peabody developmental motor scale fine motor(PDMS-FM)and fine motor function measure scale(FMFM)assessments were taken at the same time.The correlation between the PDMS-FM,FMFM original points and QUEST raw score of each domain were analysed.Result:Four domains scores and total of Chinese version QUEST have excellent test-retest reliability and inter-rater reliability(ICC>0.890).The strong association between QUEST and PDMS-FM(Pearson/Spearson r1=0.563—0.816),and the correlation index with FMFM(Pearson/Spearson r2=0.389—0.830)was demonstrated.Conclusion:The study confirmed that the Chinese version QUEST has good reliability and validity.It can be the first assessment tool as the evaluation of upper limb movement in spastic cerebral palsy children.Author's address The Third Affiliated Hospital of Zhengzhou University,Zhengzhou,450052DOI:10.3969/j.issn.1001-1242.2016.01.009*基金项目:河南省医学科技攻关计划项目(201203053)1郑州大学第三附属医院小儿脑瘫康复中心,郑州,450052作者简介:王军,女,博士,教授;收稿日期:2015-05-2841Chinese Journal of Rehabilitation Medicine,Jan.2016,Vol.31,No.1痉挛型脑性瘫痪(脑瘫)是脑性瘫痪最常见的类型,约占60%—70%,该型儿童患侧肢体运动均受到不同程度的损害,其中上肢功能障碍表现为异常姿势、手腕和手指屈曲畸形及肘部伸展受限,这将进一步影响患儿日常生活能力,而上肢运动能力的丧失较下肢活动障碍对患儿影响更甚[1—4],但至今国内仍无一个专门针对上肢的评估量表。
血管型胸廓出口综合征

Treatment-VTOS
Stenosis After VTOS Decompression Surgery (7%-64%) Balloon:typically 10–14 mm;high pressure non-compliant balloons; cutting balloons Stent:may be needed,not routine treatment.
included a large number of patients who presented with subacute or even chronic thrombus.
——Guzzo JL, Chang K, Demos J, Black JH, Freischlag JA. Preoperative thrombolysis and venoplasty affords no bene fi t in patency following fi rst rib resection and scalenectomy for subacute and chronic subclavian vein thrombosis. J Vasc Surg. 2010;52(3):658–62, discussion 62–3.
Etiology
22-year-old dance student ,motor accident caused shoulder injury. Numbness and tingling in the left upper extremity for 2.5y.
ATOS
VTOS
NTOS
Pain Paresthesia Weakness Raynaud’s phenomena
手外伤后上肢功能指数量表与关节主动活动度系统评定的对比研究

discharge were 0.863 and 0.824 respectively(P<0.0O1).TAM scores were all higher t han UEFI scores at the 2 time points(P<O.o0t).But the percentage of improved scores of TAM was lower t han that of UEFI(P<0.0or).
correlations and t-tests between UEFI and TAM measures were a n alysed. Result: UEFI and TAM were significantly correlated,the correlation coef i cients of TAM —UEFI at admission and
Science a n d Technology,W uHan,43o0 22
Key word hand injury;upper extremity function;assessment
—
—
—
—
.....—
—
手外伤是我 国多发病 ,致 伤原 因主要是 机械切 割 、建筑砸伤 、车祸等 。手外 伤后常 可导致手 及整个 上 肢的功能 障碍 。手外伤术 后早期 介入康 复治疗 能 有 效促进上 肢功能恢 复 ,降低 致残率ll-8]。但 是 ,有关
Comparat ive study on the m ethods for evaluat ing upper extremity funct ion of the pat ients after hand
injury/YANG Zhaohul ,HUANG Qm,XIA Xiaoxuan//Chinese Journal of Rehabilitat ion Medicine,2011,26(2):
X线检查身体部位表(一)
身体部位表(一)
1.Thorax胸部:
Adult Chest(成人胸部) Peds Chest(小儿胸部) Ribs(肋骨) Sternum(胸骨)
2.Spine椎体:
C-Spine(颈椎) T-Spine(胸椎) L-Spine(腰椎)
3.Cranium头骨:
Skull(颅骨) Sinus(鼻窦) Facial Bones(面骨) Nasal Bones(鼻骨) Mandible(下颌骨) Orbits(眼眶)Mastoids (乳突)
4.Abdomen腹部:
Abdomen(腹部) Pediatric Abdomen(小儿腹部)
5.Contrast Studies造影检查:
UGI(上消化道造影检查) BaE single contrast(钡剂单造影)BaE Air contrast(气-钡双对比造影)
IVP(静脉肾盂造影) IVP Hypertensive(压力性静脉肾盂造影) 6.Upper Extremity上肢:
Shoulder(肩关节) Clavicle(锁骨) AC joints(肩锁关节)Hurmerus(肱骨) Elbow(肘关节) Forearm(尺挠骨)
Wrist(腕关节) Hand(手) Finger/Thumb(手指/拇指)Scapula(肩胛骨)
7.Lower Extremity下肢:
Pelvis(骨盆) Sacrum(骶骨) SI joints(骶髂关节)Coccyx(尾骨) Hip(髋关节) Femur(股骨)
Knee(膝关节) Tiba-Fibula(胫腓骨) Ankle(踝关节)
Foot(足) Calcaneous(跟骨) Toe(趾)
8.Other其它:。
香港版偏瘫上肢功能测试评定脑卒中患者上肢功能的效度和信度研究重点
bilitation,Union Hospital,Tongii Medical College,Huazhong University of Science and Technology,Wuhan 430022, China
Corresponding author:Huang
Qin,Email:judyl 130@126.com
FTHUE-
Validity and reliability of the Hong Kong version of the functional test for the upper extremities of hemiplegic
stroke patients
Zhang Yanzhao‘,Huang Qin,Wang Gang,Li Kaiyuan,Pei Ya,Liu Yongfin.+Department of Reha—
重要。
行¨J,针对整个偏瘫上肢功能进行评定,后在2004年 经香港作业治疗师方乃权等进行修改,并结合东方人 种的生活和文化习惯汉化为香港版本(functional HK),发表于香港作业治疗杂志(Hong
Occupational
test
for the hemiplegic upper extremity-Hong Kong,FTHUE-
表3
FTHUE.HK各效度检验的r值
注:+P<0.Ol;一表示不存在
三、FTHUE—HK的信度检验 重测组内信度:同一评估者的评定结果A1、A2之
万方数据
・828‘
主堡塑理匿堂皇壁复苤查!!!!生!!旦箜!!鲞箜!!塑
堡!堕!里!z!丛型曼!!!些!!堕!!竺!竺!!!!!!!!:!!!塑!:!!
导管相关性血栓
静脉置管导致血流淤滞的机制:
二:导管大小直接影响:
当导管直径超过所在血管直径 的一半(50%)时,就会显著 的影响到血流动力学,并导致 该区域血流淤滞。
• When the diameter of a catheter is greater than one-half the diameter of the blood vessel,blood flow is markedly impaired and this can lead to areas of venous stasis.
• 血管内置管常见于中心静脉导管(CVC)和 经外周穿刺中心静脉导管(PICC)以及血管 介入手术用导管
11
涉及到导管相关性血栓形成机制的的因素包括:
穿刺针对血管壁的损伤: 放置导管所致的血流淤滞或闭塞: 导管尖端的位置; 导管材质; 注入药物的性质。
静ቤተ መጻሕፍቲ ባይዱ置管导致血管损伤的机制:
物理性:Mechanical: • 静脉穿刺和导管置入可以直接剥离
内皮细胞导致内皮损伤。 Venipuncture and catheter advancement may cause direct endothelial damage by stripping endothelial cells.
• 管尖与血管内皮直接接触,在呼吸 和肢体运动时持续刺激血管内皮。 The catheter tip may be in direct contact with the endothelium causing continuous irritation with respiration or limb movement.
这些改变通过血小板粘附开始激发 内源性凝血过程
肿瘤患者PICC相关上肢无症状静脉血栓的临床调查研究

论著Research Papers肿瘤患者PICC相关上肢无症状静脉血栓的临床调查研究罗蕾王国蓉郭琴苏畅李吟枫[摘要]目的:分析肿瘤患者PICC相关上肢无症状静脉血栓形成的临床特点,为血栓早期预防提供理论依据。
方法:选取2017年4月至2018年10月PICC置管的肿瘤患者127例,在置管前和置管后第2、7、14、21、28、35、42天应用彩色多普勒超声对置管侧上肢静脉的穿刺点、穿刺点上方2cm处、肘窝上方10cm处和腋窝4个部位进行随访检测,记录无症状静脉血栓发生时间、部位、血栓分级和统计发生率。
多因素分析所采用Logistic回归模型;采用受试者工作特征曲线(ROC)探寻危险临界值。
结果:无症状静脉血栓发生率为48.82%,发生无症状血栓中位时间为3天;62例无症状血栓患者共检测出81处静脉血栓,其中深静脉血栓占23.46%,浅静脉血栓占76.54%;血栓分级:I级占51.85%,II级占37.04%,DI级占11.11%。
美东地区肿瘤协作组评分(OR=9.185, 95%CI4.770〜28.262,PV0.001)、静脉血液流速(OR=0・577,95%CI0.506〜0.858,P=0.002)与无症状血栓发生相关。
静脉血液流速的危险临界值为4.78cm/s(曲线下面积为0.739,95%CI0.649〜0.830)。
结论:肿瘤患者PICC相关上肢无症状血栓发生率高,发生时间早,多发生于穿刺点上方2〜10cm贵要静脉处,以浅静脉血栓为主。
建议对活动能力低下,静脉血液流速<4.78cm/s的高危人群进行有目的置管前筛查和干预措施,预防无症状静脉血栓的发生。
[关键词]肿瘤患者;PICC;导管相关性静脉血栓;无症状静脉血栓[中图分类号]R47[DOI]10.3969/j.issn.l672-1756.2021.01.007A clinical investigation ofPICC-related upper extremity asymptomatic venous thrombosis in cancer patients/LUO Lei,WANG Guorong,GUO Qin,SU Chang,LI Yinfeng//Department of Internal Medicine,Sichuan Cancer Hospital&Institute, School of Medicine,University of Electronic Science and Technology of China,Chengdu,610041,China III Chinese Nursing Management-2021,21(1):25-30[Abstract]Objective:To investigate the clinical characteristics of PICC-related upper extremity asymptomatic venous thrombosis in cancer patients,and to provide theoretical basis for the early prevention of venous thrombosis.Methods:A total of127cancer patients with PICC catheterization from April2017to October2018were selected.Doppler ultrasound was used to examine the puncture point,2cm above the puncture point,10cm above the elbow fossa and armpit of the upper extremity on the side of the catheter.The examinations were before catheterization and on days2nd,7th,14th,21st,28th, 35th,and42nd after catheterization.Results:The incidence of asymptomatic venous thrombosis was48.82%and the median time of t hrombosis was3day.A total of81thrombosis were detected in62patients,of which deep vein thrombosis accounted for23.46%and superficial vein thrombosis accounted for76.54%.The rates of thrombus classification(I,II,III)were51.85%,37.04%,11.11%respectively.Logistic regression analysis showed that ECOG(OR=9.185,95%CI4.770-28.262,P<0.001),venous flow velocity(OR=0.577,95%CI0.506-0.85&P=0.002)were associated with the development of asymptomatic thrombosis.ROC curve analysis of the risk value of venous flow velocity was4.78cm/s(AUC is0.739,95%CI0.649-0.830).Ckmchision:The incidence of PICC-related asymptomatic thrombosis in cancer patients is high.It mostly occurs2-10cm above the puncture site.It is suggested that pre-catheterization screening and intervention measures should be conducted in high-risk population with low activity and venous flow rate<4.78cm/s to prevent the occurrence of a symptomatic venous thrombosis.[Keywords]cancer patients;PICC;catheter-related venous thrombosis;asymptomatic venous thrombosis基金项目:四川省卫生健康委科研项目(130225)作者单位:四川省肿瘤医院•研究所肿瘤内科,电子科技大学医学院,610041成都市(罗蕾,郭琴,苏畅);护理研究室(王国蓉儿护理部(李吟枫)作者简介:罗蕾,硕士,副主任护师,总护士长通信作者:王国蓉,博士,主任护师,硕士生导师,护理研究室主任,E-mail:553999838@国的启示.中华现代护理杂志,2018,24(30):3714.[17]Brandao MP,Martins L,Philp I,et al.Reliability and validity of the EASYCare-2010Standard to assess elderly people inPortuguese Primary Health Care.AtenPrimaria,2017,49(10):576-585.[18]Udo C,Svenningsson I,Bjorkelund C,et al.An interview study of the care managerfunction:opening the door to continuity ofcare for patients with depression in primarycare.Nursing Open,2019,6(1):112-116.[收稿日期:2020-02-11][修回日期:2020-07-30](编辑:孙蓊英文编辑:林可可)论著Research Papers美国输液护士协会(Infusion Nurses Society,INS)在2016年版的临床实践指南m中指出,PICC是经过外周静脉穿刺置入的中心静脉导管,尖端位于上腔静脉与右心房的交接处。
上肢静脉血栓诊疗指南
上肢静脉血栓诊疗指南一、概述上肢静脉血栓(Upper Extremity Deep Vein Thrombosis, UEDVT)是指血液在四肢静脉中形成血栓,常见于上肢。
上肢静脉血栓可能会导致疼痛、肿胀、功能障碍,严重时可能引发肺栓塞等并发症。
本指南旨在为上肢静脉血栓的诊断和治疗提供参考。
二、诊断病史询问详细询问患者病史,包括症状发生的时间、性质、程度,以及既往病史、家族史、手术史、长期卧床史等。
体格检查1. 观察患肢的色泽、温度、湿度,检查患肢的肿胀程度。
2. 触诊患肢的浅静脉,观察其怒张、触痛、硬度等情况。
3. 评估患肢的活动度和功能。
辅助检查1. 超声检查:彩色多普勒超声检查是诊断上肢静脉血栓的首选方法,可显示静脉内血栓的部位、范围、性质等。
超声检查:彩色多普勒超声检查是诊断上肢静脉血栓的首选方法,可显示静脉内血栓的部位、范围、性质等。
2. 放射性核素静脉显像:可显示静脉内的血栓。
放射性核素静脉显像:可显示静脉内的血栓。
3. 磁共振静脉成像(MRV):显示静脉及其内血栓的情况。
磁共振静脉成像(MRV):显示静脉及其内血栓的情况。
4. 静脉造影:在必要时进行,可显示静脉病变的详细情况。
静脉造影:在必要时进行,可显示静脉病变的详细情况。
三、治疗上肢静脉血栓的治疗原则为抗凝、溶栓、取栓、抗血小板聚集等。
治疗方案应根据患者的具体情况制定。
抗凝治疗抗凝治疗是上肢静脉血栓的基础治疗,可防止血栓增大,降低肺栓塞的风险。
常用的抗凝药物包括华法林、肝素、低分子肝素等。
溶栓治疗溶栓治疗适用于大面积血栓、症状严重患者。
通过溶栓药物(如尿激酶、链激酶等)溶解血栓,改善静脉通畅。
取栓治疗对于大面积血栓、药物溶栓无效的患者,可考虑行取栓手术。
手术过程中,将血栓取出,恢复静脉通畅。
抗血小板聚集治疗抗血小板药物(如阿司匹林、氯吡格雷等)可降低血小板聚集,预防血栓形成。
四、预防上肢静脉血栓的预防措施包括:1. 避免长时间久坐、久站,定期活动四肢,促进血液循环。
JBL AC2215 95 双向喇叭说明书
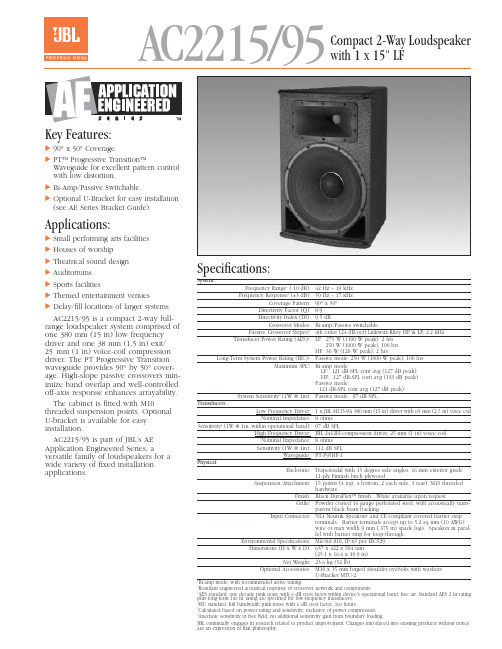
AC2215/95Compact 2-Way Loudspeaker with 1 x 15" LFKey Features:᭤90°x 50°Coverage.᭤PT™ Progressive Transition™Waveguide for excellent pattern control with low distortion.᭤Bi-Amp/Passive Switchable.᭤Optional U-Bracket for easy installation (see AE Series Bracket Guide).Applications:᭤Small performing arts facilities ᭤Houses of worship᭤Theatrical sound design ᭤Auditoriums ᭤Sports facilities᭤Themed entertainment venues᭤Delay/fill locations of larger systems AC2215/95 is a compact 2-way full-range loudspeaker system comprised of one 380 mm (15 in) low frequency driver and one 38 mm (1.5 in) exit/25mm (1 in) voice-coil compression driver. The PT Progressive Transition waveguide provides 90°by 50°cover-age. High-slope passive crossovers min-imize band overlap and well-controlled off-axis response enhances arrayability. The cabinet is fitted with M10threaded suspension points. Optional U-bracket is available for easy installation.AC2215/95 is part of JBL’s AE Application Engineered Series, aversatile family of loudspeakers for a wide variety of fixed installation applications.Specifications:System:Frequency Range 1(-10 dB):42 Hz – 19 kHz Frequency Response 1(±3 dB):50 Hz – 17 kHz Coverage Pattern:90°x 50°Directivity Factor (Q):8.9Directivity Index (DI):9.5 dBCrossover Modes:Bi-amp/Passive switchablePassive Crossover Slopes 2:4th order (24 dB/oct) Linkwitz-Riley HP & LP, 2.2 kHz Transducer Power Rating (AES)3:LF: 275 W (1100 W peak), 2 hrs250 W (1000 W peak), 100 hrs HF:30 W (120 W peak), 2 hrsLong-Term System Power Rating (IEC)4:Passive mode: 250 W (1000 W peak), 100 hrsMaximum SPL 5:Bi-amp mode:LF: 121 dB-SPL cont avg (127 dB peak)HF: 127 dB-SPL cont avg (133 dB peak)Passive mode:121 dB-SPL cont avg (127 dB peak)System Sensitivity 6(1W @ 1m):Passive mode: 97 dB SPLTransducers:Low Frequency Driver: 1 x JBL M115-8A 380 mm (15 in) driver with 63 mm (2.5 in) voice coil Nominal Impedance:8 ohmsSensitivity 6(1W @ 1m, within operational band):97 dB SPLHigh Frequency Driver:JBL 2412H compression driver, 25 mm (1 in) voice coil Nominal Impedance:8 ohms Sensitivity (1W @ 1m):112 dB SPLWaveguide:PT-F95HF-1Physical:Enclosure:Trapezoidal with 15 degree side angles, 16 mm exterior grade11-ply Finnish birch plywoodSuspension Attachment:15 points (4 top, 4 bottom, 2 each side, 3 rear), M10 threadedhardwareFinish:Black DuraFlex™ finish. White available upon request.Grille:Powder coated 14 gauge perforated steel, with acoustically trans-parent black foam backing.Input Connector:NL4 Neutrik Speakon ®and CE-compliant covered barrier stripterminals. Barrier terminals accept up to 5.2 sq mm (10 AWG)wire or max width 9 mm (.375 in) spade lugs. Speakon in paral-lel with barrier strip for loop-through.Environmental Specifications:Mil-Std 810; IP-x3 per IEC529.Dimensions (H x W x D): 637 x 422 x 504 mm(25.1 x 16.6 x 19.9 in)Net Weight:23.6 kg (52 lb)Optional Accessories: M10 x 35 mm forged shoulder eyebolts with washersU-Bracket MTU-2Bi-amp mode, with recommended active tuning.Resultant engineered acoustical response of crossover network and components. AES standard, one decade pink noise with 6 dB crest factor within device's operational band, free air. Standard AES 2 hr rating plus long-term 100 hr rating are specified for low-frequency transducers.IEC standard, full bandwidth pink noise with 6 dB crest factor, 100 hours.Calculated based on power rating and sensitivity, exclusive of power compression.Anechoic sensitivity in free field, no additional sensitivity gain from boundary loading.JBL continually engages in research related to product improvement. Changes introduced into existing products without noticeare an expression of that philosophy.᭤AC2215/95 Compact 2-Way Loudspeaker with 1 x 15" LFHorizontal 1/3 Octave PolarsSS AC2215/95CRP 10M 7/02᭤AC2215/95 Compact 2-Way Loudspeaker with 1 x 15" LFVertical 1/3 Octave PolarsJBL Professional8500 Balboa Boulevard, P.O. Box 2200Northridge, California 91329 U.S.A.©Copyright 2002 JBL ProfessionalAHarman International Company。
153-上肢截肢(英文)

Upper Limb Prosthetics
• Function to position the hand in space. • Limb length and joint salvage are directly related to functional outcome. • Sensation important for function. • Early fitting (85% if in 30 days, 50% with late fitting)
Indications for Amputation
• Trauma
– Severe open fracture with extensive skin and muscle loss, neurologic injury – Flail limb (brachial plexus injury)
Wrist Disarticulation
• Retains distal radio-ulnar joint and therefore forearm rotation. • Preservation distal radius improves prosthetic fitting. • No need to retain carpal bones. • Should perform tenodesis of major forearm muscle groups.
Wrist Disarticulation
• Disadvantages:
– Harder to fit for myoelectric units because less space is available.
Hand Amputations
数字震动感觉阈值检查对慢性肾功能不全血液透析患者周围神经病变早期筛查的临床意义
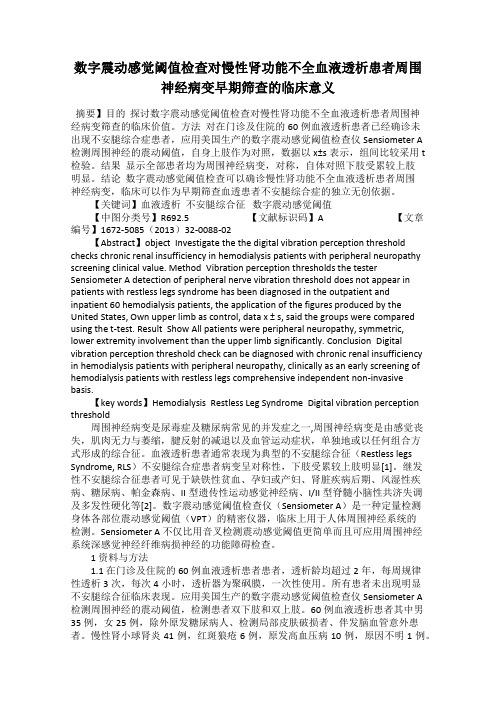
数字震动感觉阈值检查对慢性肾功能不全血液透析患者周围神经病变早期筛查的临床意义摘要】目的探讨数字震动感觉阈值检查对慢性肾功能不全血液透析患者周围神经病变筛查的临床价值。
方法对在门诊及住院的60例血液透析患者已经确诊未出现不安腿综合症患者,应用美国生产的数字震动感觉阈值检查仪Sensiometer A检测周围神经的震动阈值,自身上肢作为对照,数据以x±s表示,组间比较采用t 检验。
结果显示全部患者均为周围神经病变,对称,自体对照下肢受累较上肢明显。
结论数字震动感觉阈值检查可以确诊慢性肾功能不全血液透析患者周围神经病变,临床可以作为早期筛查血透患者不安腿综合症的独立无创依据。
【关键词】血液透析不安腿综合征数字震动感觉阈值【中图分类号】R692.5 【文献标识码】A 【文章编号】1672-5085(2013)32-0088-02【Abstract】object Investigate the the digital vibration perception threshold checks chronic renal insufficiency in hemodialysis patients with peripheral neuropathy screening clinical value. Method Vibration perception thresholds the tester Sensiometer A detection of peripheral nerve vibration threshold does not appear in patients with restless legs syndrome has been diagnosed in the outpatient and inpatient 60 hemodialysis patients, the application of the figures produced by the United States, Own upper limb as control, data x ± s, said the groups were compared using the t-test. Result Show All patients were peripheral neuropathy, symmetric, lower extremity involvement than the upper limb significantly. Conclusion Digital vibration perception threshold check can be diagnosed with chronic renal insufficiency in hemodialysis patients with peripheral neuropathy, clinically as an early screening of hemodialysis patients with restless legs comprehensive independent non-invasive basis.【key words】Hemodialysis Restless Leg Syndrome Digital vibration perception threshold周围神经病变是尿毒症及糖尿病常见的并发症之一,周围神经病变是由感觉丧失,肌肉无力与萎缩,腱反射的减退以及血管运动症状,单独地或以任何组合方式形成的综合征。
局部麻醉(英文)
CNS Excitation
Dizziness Tinnitus Feelings of drowsiness Muscle Twitching
CNS Depression
Consciousness Convulsions
Respiratory Depression Respiratory Arrest
36
Sciatic Nerve Blocks
37
Surface landmarks
38
Complications
• Hematoma: Avoid multiple needle insertions, particularly in anticoagulated patients
• Local anesthetic toxicity
intubationmaintainingadequateventilationcardiovascularsystemdepressionusingivfluidscardiacarrestcardiopulmonaryresuscitationtreatmentanatomytechniqueupperextremityblocksbrachialplexusblockadelowerextremityblockslumbarplexusnerveblockssciaticnerveblocksfemoralnerveblocksblocksneckblocksabdomenupperextremityblocksbrachialplexusblockadebrachialplexusblockadeupperextremityblocksbrachialplexusblockadebrachialplexusblockade正中神经肌皮神经腋神经桡神经正中神经肌皮神经正中神经桡神经尺神经桡神经正中神经interscaleneblockinterscaleneblockblockcanpatientshandarmupperarmshoulderclaviclesurgeryulnarnerveblockadeoftenincompletelowrisklasolutionsubarachnoidspacesaxillaryblockaxillaryblockaxillaryblocksurgicalproceduresupperarmshouldersupraclavicularblocksupraclavicularblockblockcanpatientsarmanypositionprovideexcellentanesthesiaelbowforearmhandsurgeryhighriskpneumothoraxlowerextremityblockslowerextremityblockslumbarplexusnerveblockssciaticnerveblocksfemoralnerveblockslowerextremityblockslowerextremityblockslumbarplexusnerveblockssciaticnerveblocksfemoralnervebloc
上肢康复机器人联合弗伦克尔训练法在脑干卒中上肢协调障碍中的应用

上肢康复机器人联合弗伦克尔训练法在脑干卒中上肢协调障碍中的应用康良鸣,郭峰,戴文娟[摘要]目的探讨上肢康复机器人联合弗伦克尔(Frenkel)训练法在脑干卒中上肢协调障碍中的临床应用价值。
方法便利选取2021年9月—2023年7月赣州市人民医院收治的48例脑干卒中后上肢协调障碍患者为研究对象。
按照随机数表法分为两组,各24例。
对照组实施常规综合康复,治疗组在对照组的基础上运用上肢康复机器人联合Frenkel训练。
比较两组患者肱二头肌,三角肌前、中束,肱三头肌表面肌电均方根(Root Mean Square, RMS)值,干预前、干预1个月和干预3个月后国际合作共济失调量表(International Cooperative Ataxia Rating Scale, ICARS)、上田氏协调试验及改良Barthel指数得分变化,统计两组患者干预过程中Fugl-Meyer上肢运动功能评分(Fugl-Meyer As⁃sessment of Upper Extremity, FMA-UE)变化情况。
结果干预3个月后,治疗组肱二头肌,三角肌前、中束,肱三头肌表面肌电RMS值分别为(165.8±21.4)、(253.3±33.6)、(266.7±32.2)、(133.5±16.5)uV·s,均高于对照组,差异有统计学意义(t=3.830、8.792、10.432、40.354,P均<0.05);治疗组ICARS、上田氏协调试验及改良Barthel指数评分均高于干预前治疗组及干预后对照组,差异有统计学意义(P均<0.05);治疗组FMA-UE评分高于对照组,差异有统计学意义(P<0.05)。
结论针对脑干卒中后上肢协调障碍患者应用上肢康复机器人联合Frenkel训练法,对改善患者共济失调能力,提高上肢协调与运动能力,促进患者生活质量有积极作用。
coarctationoftheaorta

Coarctation of the AortaJo Ann Nieves, MSN, ARNP, CPN, PNP-BCNurse Practitioner, Adult Congenital Heart ProgramMiami Children’s HospitalMiami, FloridaDiana Arias, MSN, ARNP, FNP-C, CPNClinical Specialist, Cardiac Intensive Care UnitMiami Childre n’s HospitalMiami, FloridaI. EmbryologyA. Affects 5% to 8% of all newborns with congenital heart diseaseB. Occurs during the 6th to 8th week of gestation1. Cause of Coarctation of the Aorta (CoA) is unknown. Two theories (Beekman, 2008):a. Ductus Tissue Theory - Postnatal constriction of aberrant ductal tissueb. Hemodynamic Theory - Intrauterine alterations of blood flow through theaortic archII. Abnormal developmentA.Deformity of the aortic isthmus (where the ductus arteriosus joins the descending aorta) –characterized by narrowing of the proximal aorta or distal to the left subclavian artery. (Moon, 2011).1. Localized stenosis - a shelf-like infolding of the posterior aortic wall into the aorticlumen opposite, proximal and/or distal to the ductus arteriosus (Kaemmerer, 2011)2.Long hypoplastic segment- a tubular hypoplasia involving the aortic arch or the aortadistal to the origin of the left subclavian artery and the ductal area (Kaemmerer, 2011)Coarctation at aortic isthmus Illustrations reprinted from PedHeart Resource. .© Scientific Software Solutions, 2010. All rights reserved.B. Simple CoA - coarctation in the absence of other lesionsC. Complex CoA1. Include intracardiac and/or extracardiac lesions (Kaemmerer, 2011):a.Bicuspid Aortic valve – occurs in nearly 85%, the valve may be stenotic orthe annulus hypoplasticb.Ventricular septal defectc.Transposition of the great arteriesd.Noncardiac anomaly- aneurysm of circle of Willis in 3% to 5%D. Genetic component1. Turner XO syndrome- 35% of patients affectedIII. PhysiologyA.Left ventricular hypertension- narrowing of the aorta causes increased resistance to leftventricular outflow therefore elevating systolic pressure1. Upper extremity hypertension2. Lower extremity BP lower than the upper body BP3. “Gradient” is the difference between higher upper body & decreased lower body BP4. Fully oxygenated arterial blood – unless other lesions are presenta.Closure of foramen ovale & ductus arteriosus after birth causes entire cardiacoutput to flow through the stenotic aortic segment (Beekman, 2008)IV. Clinical Features:A. Cardinal features (Kaemmerer, 2011)1.Upper body hypertension; weak, delayed femoral pulses; a decrease in blood pressurebetween upper and lower extremities; palpable collateral arteries over the medialaspect of the scapulae, the lateral chest wall, and between the ribs2. Thrill- suprasternal notch or neck vessels3. Heave- no displaced heart soundB. Infant1. In severe CoA of the newborn, survival depends on patency of the ductus arteroisusa.When ductus arteriosus closes (approximately 8 to 10 days of life) the patientdevelops shock & heart failure. Metabolic disturbances, hypothermia,hypoglycemia can occur as well.b.Resulting in lower body & renal hypoperfusion, renal failure and/ornecrotizing enterocolitis (Beekman, 2008)C. Child or adolescent1. Upper extremity hypertensiona. Widened pulse pressure as patient gets olderb. Variability of Right and Left Arm pressures, dependent on location of CoA inrelation to the left & right subclavian artery2. Murmursa.Grade 2/6 to 3/6 systolic ejection murmur at the upper left sternal border, atthe base & left interscapular space (Beekman, 2008)D. Adults1.Patients typically diagnosed & treated earlier in life, but may rarely present withupper extremity hypertension as an adult with a native CoA (Daniels, 2008)V. Medical/surgical interventionsA. Diagnosis: most often via clinical exam, echocardiogram, and chest x-ray, MRI or CT1.Diagnostic cardiac catheterization (Beekman, 2008)a.With complex anatomy and hemodynamics, of associated lesionsb. With additional clinical questionsB. Treatment & Timing: Individualized to lesion, associated conditions1.Infant:a.If severe: signs occur in first hours of life(1) Immediate intervention required(2)Medical – initial stabilization, inotropic support(3)Prostaglandin E1 IVMaintain open ductus arteriosusAllows for flow from RV to enter MPA, cross the ductus,enter the aorta, and perfuse the descending aorta, renal andmesenteric arteriesb. Surgical CoA repair(1) Individualized to anatomy of CoA(2)Plan to include treatment of any additional cardiac defects2.Child, Adolescenta.Repair at 2 to 3 years of ageb.Upon diagnosisC. Surgery -4 Common types of repair- regardless of technique, usually performed via a left thoracotomy incision1. End-to-end anastomosis– 1954 by Crawford and Nylin (See illustration below)a. Surgical treatment of choice in most centersb. Excision of CoA area, circumferential anastomosis is completed withinterrupted sutures anteriorly (Beekman)Ductal SegmentEnd-to-End Anastomosis with removal of Ductal SegmentIllustrations reprinted from PedHeart Resource. .© Scientific Software Solutions, 2010. All rights reserved.2. Left subclavian flap – 1966 by Waldhausen and Nahrwold (Beekman, 2008)a. Ligate left subclavian artery, open the proximal subclavian artery andbeyond the CoAb. Fold subclavian artery flap down over the CoA section and sutureinto placeSubclavian arteryFlapCoarctation Repair with Left Subclavian FlapIllustrations reprinted from PedHeart Resource. .© Scientific Software Solutions, 2010. All rights reserved.3. Prosthetic patch aortoplasty- 1961 by Vosschulte (Beekman, 2008)a. Longitudinal incision is made across the CoAb. Area enlarged with a Dacron or Gore-tex patch4. Bypass graft – a tube is sewn in between ascending and descending thoracic aortaD. Outcomes1. Mortality rates vary on patient age and associated lesions (Kaemmerer, 2011)a. Simple CoA- Less than 1% mortalityb. Age 2 to 5- best age to electively operate due to low surgical riskc. Death rates strongly related to complexity of lesionsd. After age 30 or 40- intraoperative mortality rate increases due to degenerativechanges to the aortic wall.2. Morbiditya. Post op –potential paradoxical hypertension, spinal cord ischemia & paralysis,recurrent laryngeal or phrenic nerve injury, chylothorax, bleeding, infectionE. Significant long term issues: See Section VII BVI. Cardiac Catheterization: Interventional (Beekman, 2008)A. Balloon angioplasty began 1982,1. Initially accepted for treatment of re-coarctaton2. Not completely accepted for treating primary CoA3. Balloon Angioplasty – enlarges CoA lumen, produces linear intimal andmedial tears at the CoA siteBalloon Angioplasty with Implantation of StentIllustrations reprinted from PedHeart Resource. .© Scientific Software Solutions, 2010. All rights reserved.4. Risk: Aneurysm from extension to adventitiaB. Stent implantation following CoA angioplasty (See illustration above)1. Endovascular buttress, supports dilated aortic segment2. Restenosis uncommon3. Redilatation may be needed as child growsC. Outcomes:1. Mortality- rare beyond newborn perioda. Higher rate has been reported for angioplasty for recurrent post op CoA versusnative CoA2. Acute complications (Beekman, 2008)a. Femoral artery injury and thrombosis- common in infants younger than 12monthsb. Femoral artery hemorrhagec. Cerebrovascular accident3.Long-term problemsa.Coronary artery stenosisb.Dilation of neo-aortic rootc.Aortic valve regurgitationVII. Long TermA. Excellent prognosis for normal growth, development when lesion successfullyrepaired in childhood (Beekman, 2008)B. Potential complications and risks1. May occur after all forms of repairs (Kaemmerer, 2011)2. Residual CoA – presence of gradient in aorta after repair3. Recurrent CoA– development of restenosis, gradient in aorta after an initiallysuccessful repaira. 8% to 54% (Daniels, 2008)b. Recoarctation- aortic isthmus and/or aortic archd.May cause systemic hypertension, heart failure, left ventricular wall mass,coronary artery disease4. Systemic arterial hypertensiona. At rest or during exercise (Kaemmerer, 2011)b. Related to re-coarctation, structural changes in the wall of vessels, reducedbaroreceptor sensitivity, changes in renin-angiotensin system, elevatedplasma levels of epinephrine and norepinephrine, or coexistence of essential hypertensionc. Higher risk of residual hypertension & early atherosclerotic disease if repairsoccur late in childhood and adolescence (Maron, 1973)d. Systolic hypertension may occur during dynamic exercise (Beekman, 2008)5. Coronary artery disease6. Progression valve disease, bicuspid aortic valve or mitral valve (Daniels, 2008a)a. Bicuspid aortic valve can progress to stenosis (59-81%) or regurgitation (13-22%) (Sabet, 1999)7. Aortic aneurysm at the site of CoA, ascending or descending aortaa. Highest after prosthetic patch aortoplastyb. Risk rupture (Kaemmerer, 2011) – dangerous, life threatening8. Other vascular problems: Aortic dissection, intracranial hemorrhage (may berelated to berry aneurysms in circle of Willis) (Beekman, 2008)9. Long term concerns may be greatly affected by associated cardiac lesions10. Left shoulder elevation- seen in adults due to left lateral thoracotomy11. Left arm – decreased pulse/ BP if surgery used left subclavian artery patch12. Sudden death (Daniels, 2008)13. Bacterial endocarditisa. Antibiotic prophylaxis prior to dental procedures no longer required byAmerican Heart Association, 2007b. Should seek additional information regarding status of other lesionsVIII. Adults with CoA repair: Routine cardiology careA. Annual visits: Complex congenital heart disease classification (Kaemmerer, 2011)1. Clinical evaluationa. Documentation of type of CoA repair is importantb. Monitor blood pressuresc. Assessment NOTE: Using four extremities BP needed(1)Monitor for upper body hypertension, weak femoral pulses, gradientbetween upper and lower body BP(2)If left subclavian artery u sed as part of repair, BP’s will be LOWERin the left arm (avoid use of arterial line here)(3)If aberrant subclavian artery present – must consider use of left armto obtain a BP which is proximal to CoA repaird. Electrocardiograme. Transthoracic echof. Cardiac magnetic resonance (MRI) or CT(1)Surveillance aorta for potential aneurysms, status of aortic repair,valvesg. Exercise test: Surveillance for exercise induced hypertensionh. Monitor new or different type headache(1) May be sign of possible cerebral aneurysmi. Monitor cholesterol; avoid obesity & smoking(1) Minimize additional risk for coronary artery disease)j. Education(1)Assess knowledge, review condition, life long care needs(Resources: American Heart Association (),Adult Congenital Heart Association ()(2)Pregnancy information website:/B. Care during pregnancy (Refer to problem section on pregnancy in adults with CHD1. Recommendationsa. Consultation: Adult congenital heart cardiologist before pregnancyb. Multidisciplinary observation by experienced cardiologist during pregnancy, labor, delivery and for period of time post-partumc. Highest risks(1)Unrepaired CoA, arterial hypertension, residual CoA, aneurysm(Kaemmerer, 2011)References:Beekman RH. Coarctation of the Aorta. In Allen HD, Clark EB, Gutgesell HP, Driscoll D.J. Moss and Adams’ Heart Disease in Infants, Children’ and Adolescents, 6th Ed, Philadelphia, 2001, Lippincott Williams & Wilkins (p. 987-1005).Bromberg BI, Beekman RH, Rocchini AP, et al. Aortic aneurysm after patch aortoplasty repair of coarctation: A prospective analysis of prevalence, screening tests and risks. J Am Coll Cardiol 14:734-741, 1989.Daniesl CJ. The Adolesent and adult with congenial heart disease. In Allen HD, Clark EB, Gutgesell HP, Driscoll D.J. Moss and Adams’ Heart Disease in Infants, Children’ and Adolescents, 6th Ed, Philadelphia, 2008, Lippincott Williams & Wilkins (p. 1370-1397).Daniesl CJ. (a) Adult congenial heart disease: Lesion specific pathways. In Allen HD, Clark EB, Gutgesell HP, Driscoll D.J. Moss and Adams’ Heart Disease in Infants, Children’ and Adolescents, 6th Ed, Philadelphia, 2008a, Lippincott Williams & Wilkins (p. 1427-1430).Illustrations reprinted from PedHeart Resource. . © ScientificSoftware Solutions, 2010. All rights reserved.Kaemmerer H. Aortic coarctation and interrupted aortic arch. In Gatzoulis MA, Webb GD, Daubeney PEF. Diagnosis and Management of Adult congenital Heart Disease, 2nd Edition. Philadelphia , 2011, Elsevier (p. 261-270).Maron BJ, Humphries JO, Rowe RD, et al. Prognosis of surgically corrected coarctation of the aorta: A 20 year post-operative appraisal. Circulation 47:119-126, 1973.Sabet HY, Edwards WD, Tazelaar HD, Daly RC. Congenitally bicuspid aortic valves: A surgical pathology study of 542 cases (1991 through 1996) and a literature review of 2715 additional cases. Mayo Clinic Proc 74:14-26, 1999.8/2011Below is given annual work summary, do not need friends can download after editor deleted Welcome to visit againXXXX annual work summaryDear every leader, colleagues:Look back end of XXXX, XXXX years of work, have the joy of success in your work, have a collaboration with colleagues, working hard, also have disappointed when encountered difficulties and setbacks. Imperceptible in tense and orderly to be over a year, a year, under the loving care and guidance of the leadership of the company, under the support and help of colleagues, through their own efforts, various aspects have made certain progress, better to complete the job. For better work, sum up experience and lessons, will now work a brief summary.To continuously strengthen learning, improve their comprehensive quality. With good comprehensive quality is the precondition of completes the labor of duty and conditions. A year always put learning in the important position, trying to improve their comprehensive quality. Continuous learning professional skills, learn from surrounding colleagues with rich work experience, equip themselves with knowledge, the expanded aspect of knowledge, efforts to improve their comprehensive quality.The second Do best, strictly perform their responsibilities. Set up the company, to maximize the customer to the satisfaction of the company's products, do a good job in technical services and product promotion to the company. And collected on the properties of the products of the company, in order to make improvement in time, make the products better meet the using demand of the scene.Three to learn to be good at communication, coordinating assistance. On‐site technical service personnel should not only have strong professional technology, should also have good communication ability, a lot of a product due to improper operation to appear problem, but often not customers reflect the quality of no, so this time we need to find out the crux, and customer communication, standardized operation, to avoid customer's mistrust of the products and even the damage of the company's image. Some experiences in the past work, mentality is very important in the work, work to have passion, keep the smile of sunshine, can close the distance between people, easy to communicate with the customer. Do better in the daily work to communicate with customers and achieve customer satisfaction, excellent technical service every time, on behalf of the customer on our products much a understanding and trust.Fourth, we need to continue to learn professional knowledge, do practical grasp skilled operation. Over the past year, through continuous learning and fumble, studied the gas generation, collection and methods, gradually familiar with and master the company introduced the working principle, operation method of gas machine. With the help of the department leaders and colleagues, familiar with and master the launch of the division principle, debugging method of the control system, and to wuhan Chen Guchong garbage power plant of gas machine control system transformation, learn to debug, accumulated some experience. All in all, over the past year, did some work, have also made some achievements, but the results can only represent the past, there are some problems to work, can't meet the higher requirements. In the future work, I must develop the oneself advantage, lack of correct, foster strengths and circumvent weaknesses, for greater achievements. Looking forward to XXXX years of work, I'll be more efforts, constant progress in their jobs, make greater achievements. Every year I have progress, the growth of believe will get greater returns, I will my biggest contribution to the development of the company, believe inyourself do better next year!I wish you all work study progress in the year to come.。
提高普外二科患者上肢深静脉血栓预防措施的落实率PDC记录表

提高普外二科患者上肢深静脉血栓预防措施的落实率PDC记录表背景近年来,普外二科患者上肢深静脉血栓(Upper Extremity Deep Vein Thrombosis,UEDVT)的发病率有逐年上升的趋势。
UEDVT 不仅会给患者带来较大的疼痛和不适,还可能导致肺栓塞等严重并发症。
因此,提高UEDVT预防措施的落实率对于提升患者的生活质量和减少并发症的发生具有重要意义。
目标本记录表的目标是提高普外二科患者上肢深静脉血栓预防措施的落实率(Prevention of Deep Vein Thrombosis in Upper Extremity,PDC)。
通过记录落实率相关数据,及时发现问题并采取相应的改进措施,提高预防措施的执行效果。
记录内容1. 患者基本信息:- 患者姓名:- 年龄:- 性别:- 入院日期:- 出院日期:2. 风险评估:- 是否进行了UEDVT风险评估(是/否):- 风险评估工具(若执行):3. 预防措施落实情况:- 医嘱是否明确规定了UEDVT预防措施(是/否):- 使用抗凝药物预防的方案(若使用):- 是否进行了机械性预防(如弹力袜、肢体活动等):- 预防措施的持续时间(天):- 其他预防措施(若有):4. 问题记录:- 如果存在预防措施未落实或不足的情况,请描述具体问题:5. 改进措施:- 针对问题记录的改进方案:6. 审核记录:- 记录表的填写人:- 填写时间:- 审核人:- 审核时间:使用说明1. 填写本记录表时,请务必填写患者的真实信息。
2. 风险评估工具可根据具体科室的标准选择相应的评估工具。
3. 如果存在多个患者,可以以表格形式依次填写每个患者的信息。
4. 填写问题记录时,请详细描述问题的具体情况,例如未执行的原因、未执行的具体预防措施等。
5. 填写改进措施时,可根据问题记录提出相应的改进方案,例如加强宣教、完善医嘱规定等。
6. 填写审核记录时,请填写记录表的填写人、填写时间、审核人和审核时间。
平山病的诊治进展

平山病的诊治进展郭剑;陈逊文;曹正霖【摘要】平山病为临床非常少见的一种良性自限性疾病,是一种与曲颈运动有关的颈髓病变.典型表现为:局限性上肢远端、手指及腕无力,伴远端肌肉萎缩、寒冷麻痹和手指伸展时束颤,肌电图表现为神经源性损害.在临床上与运动神经元病肌萎缩侧索硬化及脊髓进行性肌萎缩表现相似而预后截然不同,主要是男性青少年发病.【期刊名称】《海南医学》【年(卷),期】2010(021)014【总页数】3页(P129-131)【关键词】平山病;良性自限性疾病;屈性颈髓病;诊治【作者】郭剑;陈逊文;曹正霖【作者单位】广州中医药大学附属佛山市中医院骨一科,广东佛山,528000;广州中医药大学附属佛山市中医院骨一科,广东佛山,528000;广州中医药大学附属佛山市中医院骨一科,广东佛山,528000【正文语种】中文【中图分类】R685平山病(Hirayama disease,HD)最早是由日本学者平山慧造(Keizo Hirayama)等[1]在 1959年首先报道的一种良性自限性运动神经元疾病,主要特征为单侧前臂尺侧肌萎缩,故又称青少年上肢远端肌肉萎缩(Juvenile muscular atrophy of thedistal upper extremity)。
目前,全球报道不超过 1 500例,其中,相当大一部分在日本、亚洲其他国家及欧美等国家[2],散在发病,罕见家族史[3]。
本病起病隐匿,好发于青少年,15-25岁为发病高峰,男性多见,男女之比约20∶1[2]。
患者病后 1-5年病情开始稳定,但极少数患者肌肉萎缩仍缓慢进展。
随着世界医疗技术的不断提高,尤其影像学及辅助检查的广泛应用,我国对此病的报道随之增多,此病临床上与运动神经元病相似,但预后不同,故提高对此病的诊断和治疗是非常必要的,现就此病的诊治等介绍如下:1 临床表现典型的临床表现为一侧上肢远端肌肉萎缩、无力。
肌萎缩最早起于手部,随着病变的进展,少数至上臂;多数为单侧损害,亦有不对称的双侧损害,肌肉萎缩以手小肌肉为主(骨间肌,大、小鱼际肌,以尺侧明显),肱桡肌相对轻,呈“斜坡样”改变。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
CUBITAL FOSSA
CUBITAL FOSSA
STYLOID PROCESS
ANATOMICAL SNUFF BOX
AXILLA( ARMPIT)
• PYRAMIDAL SPACE BETWEEN THE UPPER LATERAL CHEST AND THE INNERSIDE OF THE ARM • BOUNDARIES -APEX –( BETWEEN THE CLAVICLE,SCAPULA AND 1ST RIB) -BASE-(AXILLARY FASCIA) -ANTERIOR ( PECTORALIS MAJOR AND MINOR MUSCLES) POSTERIOR( SUBSCAPULARIS,LATI SSIMUS DORSI AND TERES MAJOR) MEDIAL- ( FIRST 4 RIBS AND SERRATUS ANTERIOR MUSCLE) LATERAL-( BICEPETAL GROOVE OF THE HUMERUS)
CUBITAL FOSSA
• TRIANGULAR DEPRESSION ON THE ANTERIOR ASPECT OF ELBOW BOUNDARIES -BASE- LINE DRAWN BETWEEN THE EPICONDYLES OF THE HUMERUS LATERAL BOUNDARYBRACHIORADIALIS MEDIAL BOUNDARY- PRONATOR TERES APEX- WHERE THE MEDIAL AND LATREAL BOUNDARY MEET CONTENTS 1. MEDIAL CUBITAL VEIN 2. BRACHIAL ARTERY 3. TENDON OF THE BICEPS
IMPORTANT NERVES AND AREA OF SUPPLY
• • • 1. MEDIAN NERVE( FORMED FROM BOTH MEDIAL AND LATERAL CORD)A) SUPPLIES ALL THE FLEXORS OF THE FOREARM( EXCEPT FLEXOR CARPI ULNARIS AND MEDIAL HALF OF FDP) B) INTRINSIC MUSCLES IN THE LATERAL PALM INCLUDING THENAR EMINENCE) 2. ULNAR NERVE A) SUPPLIES THE MEDIAL HALF OF FDP AND THE FLEXOR CARPI ULNARIS B) SUPPLIES MOST OF THE INTRINSIC MUSCLES OF THE HAND INCLUDING THE HYPOTHENAR EMINENCE, AND SKIN ON THE MEDIAL SIDE OF THE HAND CLINICAL APPLICATION *INJURY TO MEDIAN NERVE-” APE HAND” INJURY TO ULNAR NERVE-” CLAW HAND”
VEINS OF UPPER LIMB
• SUPERFICIAL VEINS DORSAL VENOUS NETWORK CEPHALIC VEIN BASILIC VEIN AXILLARY VEIN( BASILIC+ BRACHIAL VEIN) MEDIAN CUBITAL VEIN MEDIAN VEIN OF FOREARM DEEP VEINS NAMED ACCORDING TO COMPANIAN ARTERIES RADIAL VEIN ULNAR VEIN BRACHIAL VEIN AXILLARY VEIN
CORDS ARE NAMED ACCORDING TO THEIR RELATIVE POSITIONS TO THE AXILLARY ARTERY
BRACHIAL PLEXUS
NERVES ARISING FROM THE CORDS
• 1. 2. MEDIAL CORD MEDIAL CUTANEOUS NERVE OF ARM- CUTANEOUS SUPPLY TO SKIN MEDIAL CUTANEOUS NERVE OF FOREARM-CUTANEOUS SUPPLY TO THE SKIN MEDIAL ROOT OF MEDIAL NERVE- JOINS WITH LATERAL ROOT TO FORM MEDIAN NERVE ULNAR NERVE MEDIAL PECTORAL NERVE LATERAL CORD LATERAL ROOT OF MEDIAN NERVE MUSCULOCUTANEOUS NERVE LATERAL PECTORAL NERVE
• •
• • • •
INPORTANT NERVES AND THEIR AREA OF SUPPLY
• A) MUSCULOCUTANEOUS NERVE SUPPLIES THE BICEPS, CORACOBRACHIALIS AND BRACHIALIS
AXILLARY NERVE SUPPLIES THE DELTOID AND TERES MINOR MUSCLE SUPPLIES THE SHOULDER JOINT RADIAL NERVE SUPPLIES THE TRICEPS SUPPLIES THE BRACHIORADIALIS SUPPLIES MOST OF THE EXTENSORS OF THE FOREARM * INJURY RESULTS IN “ WRIST DROP”
CARPAL TUNNEL
• TUNNEL FORMED BETWEEN THE CONCAVITY OF THE CARPAL BONES AND A LIGAMENT THAT COVERS THIS( FLEXOR RETINACULAM) • TENDONS OF THE FLEXORS PASS THROUGH • MEDIAN NERVE ALSO PASSES THROUGH • CROWDED TUNNEL CARPAL TUNNEL SYNDROME - CAUSED DUE TO COMPRESSION OF THE NERVE IN THE TUNNEL - CAUSES- 1. SWELLING OF THE TEDONS( OVERUSE) - 2. PREGNANCY( EDEMA) - 3. ARTHRITIS SYMPTOMS- TINGLING OR NUMBNESS-LATERAL PART OF HAND, WEAKNESS IN THUMB MOVEMENT TREATMENT- REST, SPLINTING,ANTI-INFLAMMATORY DRUGS, SURGERY
• • • • • •
• • • • • •
ROOTS C5 C6 C7 C8 T1
FORMATION OF TRUNKS UPPER
MIDDLE
LOWER FORMED IN THE NECK
DIVISIONS AND CORDS OF BRACHIAL PLEXUS
• TRUNKS DIVISIONS CORDS LATERAL CORD-ANTERIOR DIVISIONS OF UPPER AND MIDDLE TRUNK • UPPER TRUNK
3.
4. 5. • 1. 2. 3.
NERVES FROM THE POSTERIOR CORD
• • • • • 1. UPPER SUBSCAPULAR NERVE 2.LOWER SUBSCAPULAR NERVE 3.THORACODORSAL NERVE 4. RADIAL NERVE 5. AXILLARY NERVE
REST OF LATERAL 31/2 FINGERS AND HAND - RADIAL NERVE
• CONTENTS -AXILLARY LYMPH NODES
-AXILLARY ARTERY /VEIN -BRACHIAL PLEXUS
BRACHIAL PLEXUS
• • • • PLEXUS- IS A NETWORK OF NERVES BRACHIAL PLEXUSFOUND IN THE NECK AND AXILLA FORMED BY VENTRAL RAMI OF C5C8 AND T1 ( THERE MAY BE CONTRIBUTIONS FROM C4, T2) GIVES RISE TO NERVES THAT SUPPLY THE UPPER LIMB FORMATION ROOTS- C5-C8 AND TI( VENTRAL RAMI) TRUNKS-UPPER , MIDDLE, LOWER DIVISONS-ANTERIOR/POSTERIOR CORDSMEDIAL/LATERAL/POSTERIOR
PINKANTERIOR DIVISION
•
MIDDLE TRUNK
POSTERIOR CORDPOSTERIOR DIVISIONS OF ALL TRUNKS
MEDIAL CORD-ANTERIOR DIVISION OF LOWER TRUNK
• LOWER TRUNK
BLUE POSTERIOR DIVISION
UPPER EXTREMITY-2
DR VINIT K ASHOK ADJUNCT FACULTY
BLOOD SUPPLY
• ARTERIAL SUPPLY • -SUBCLAVIAN ARTERY(NECK) • - AXILLARY ARTERY( UPPER ARM;UPTO LOWER BARTERY(LOWER PART OF ARM) • RADIAL ARTERY( LATERAL) • ULNAR ARTERY( MEDIAL),COMMON INTEROSSEOUS • PALMAR ARCHES • DIGITAL