PEDF in Diabetic Retinopathy a protective effect of oxidative stress
色素上皮衍生因子在视网膜疾病中的应用研究进展

色素上皮衍生因子在视网膜疾病中的应用研究进展作者:胡鹭萍徐国兴来源:《海峡科学》2007年第03期【摘要】色素上皮衍生因子(pigment epithelium-derived factor, PEDF)是一种多效的神经营养因子和新生血管抑制因子,其在视网膜的生长发育及许多疾病病理过程中起着神经分化、神经营养、神经保护和抑制新生血管形成等作用,并可抗肿瘤和调控一些炎症反应。
本文主要是综述目前对PEDF的生物学特点、作用及其在视网膜疾病中的应用研究状况,并推测其可能作用机制,展望其在视网膜疾病的临床治疗中的应用前景。
【关键词】色素上皮衍生因子视网膜神经营养神经保护神经分化新生血管1.前言随着社会的发展和人口的老龄化,许多视网膜变性性疾病和新生血管性疾病正逐渐成为一些西方国家和我国主要的难治性致盲性眼病,如年龄相关性黄斑变性(age-related macular degeneration, AMD)和增殖性糖尿病视网膜病(proliferating diabetic retinopathy, PDR)等,这些疾病常导致严重的视力损害,而目前尚无确切有效的治疗方法[1]。
早产儿视网膜病变(retinopathy of prematurity, ROP)和遗传性视网膜色素变性、遗传性视锥细胞营养不良、Leber先天性黑蒙、Sorsby黄斑营养不良、Stargardt's病等遗传性视网膜变性性疾病均可导致不同程度的视网膜变性损伤或异常血管增生而引起视功能障碍,将严重影响着小儿的生活质量,并给社会带来负担,而目前仍无有效治疗方法来阻止或逆转这些疾病的视力损害[1,2]。
此外,视网膜脱离、光损伤、缺血-再灌注损伤(如青光眼和视网膜血管阻塞等)和H202氧化损伤等也可引起不同程度的视网膜变性损伤而影响视力。
因此,寻找有效的防治视网膜变性和新生血管形成的治疗方法,已成为国内外研究热点。
多效的神经营养因子和新生血管抑制因子——色素上皮衍生因子(Pigment epithelium-derived factor, PEDF)的发现及随后的大量研究不断的带给人们惊喜。
白内障超声乳化吸除术眼内液中细胞因子的改变
白内障是全球首位的致盲性眼病,在中国有 567%的 致盲和视力损伤患者是由白内障引起。白内障超声乳化吸 除术凭借组织损伤小、切口愈合快、术后屈光状态稳定等优 点逐步推广。
三、白内障超声乳化术后并发症与细胞因子的关系 1.黄斑囊样水 肿 (cystoidmacularedema,CME) CME 是白内障术后视力不良的主要原因之一。据报道,白内障超 声乳化术后 CME的发生率从 4% ~11%不等[7,8],发病的高 峰期是术后 4~6周。具体发病机制尚不明确,但细胞因子 的改变是其主要因素。超声乳化术后多种细胞因子表达升 高,通过增强免疫细胞的迁移破坏了血眼屏障并使血管通 透性增加。细胞内外的液体异常聚集,形成黄斑区外丛状层 和内核层典型的囊样改变及视网膜增厚。活化的内皮细胞、 小胶质细胞、浸润性单核细胞和视网膜 Müller细胞是视网膜 中促炎因子的主要来源[9]。Chu等 收 [10] 集了 288例白内障 患者 超 声 乳 化 术 前 的 房 水,术 后 4周 CME的 发 生 率 为 813%,与无 CME组比较,CME组 IL1β(50pg/ml)、IL6 (170pg/ml)、MCP1(1340pg/ml)和 VEGF(760pg/ml) 明显升高,而 IL10(50pg/ml)明显降低。其中 IL1β、IL6、 MCP1是重要的促炎因子,而 IL10是一种由单核 /巨噬细 胞产生的抗炎因子。IL10通过抑制细胞因子受体的激活和 表达来减少促炎因子 IL1和 TNFα等的合成,从而抑制炎 症[11]。此外,IL10还可以通过下调 VEGF的表达来阻止血 管生成[12]。因此,促炎因子 IL1β、IL6、MCP1、VEGF的升 高和抗炎因子 IL10的下降可能是非糖尿病患者白内障超 声乳化术后黄斑厚度改变及 CME发生的主要原因并具有潜 在的预测 CME的价值。 术前有 DR,术后眼前节炎症反应较重的糖尿病患者, DR进展更快,DME的发生率更高(20% ~30%)[13]。大量 研究表明 VEGF增强血管通透性可能是 DME发生的主要原 因。其中 VEGFA是 VEGF亚型中血管生成的关键调节剂, 它与两种酪氨酸激酶受体,即血管内皮生长因子受体 VEG FR1和 VEGFR2结合,通过增加细胞旁和跨细胞的通透性 来介导血管的高通透性。检测眼内液中的 VEGF可以作为 预测 DME的 一 种 手 段。DME患 者 房 水 和 玻 璃 体 液 中 的 VEGF均明显升高。Funatsu等[14]将白内障术后黄斑水肿的
英文《JOSLIN成人糖尿病临床指南》最新更新
Copyright © 2009 by Joslin Diabetes Center. All rights reserved. Any reproduction of this document which omits Joslin’s name or copyright notice is prohibited. This document may be reproduced for personal use only. It may not be distributed or sold. It may not be published in any other format without the prior, written permission of Joslin Diabetes Center, Publications Department, 617-226-5815.
If history of severe hypoglycemia or hypoglycemia unawareness (a condition in which the patient is unable to recognize symptoms of hypoglycemia until they become severe): Assess for changes in daily routine such as decreased food intake or increased activity [1C] Refer to DE for evaluation, DSME and hypoglycemia prevention; encourage family/friend attendance Review use of glucagon Consider loosening A1C goal [2C] Communicate goals to patient Adjust medications accordingly If insulin-treated, consider use of a more physiologic insulin replacement program [1C] Consider and screen for other medical causes [1C] Consider referral for blood glucose awareness training, if available [1B] Schedule follow-up appointment within 1-2 months. If history of recent, severe hypoglycemia or change in pattern of hypoglycemia, recommend increase in frequency of communicating blood glucose levels to provider or diabetes educator [பைடு நூலகம்B] GLUCOSE MONITORING Self-monitoring of blood glucose (SMBG) is an important component of the treatment program for all people with diabetes. Its use is to gauge treatment efficacy, help in treatment design, provide feedback on the impact of nutritional intake and activity, provide patterns that assist in medication selection, and for those on insulin, assist in daily dose adjustments. [1A] Goals for glycemic control for people with diabetes are: Fasting plasma glucose: 70-130 mg/dl 2- hour postprandial plasma glucose: <180 mg/dl Bedtime glucose: 90-150 mg/dl The frequency of SMBG is highly individualized and should be based on such factors as glucose goals, medication changes and patient motivation. Most patients with type 1diabetes should monitor at least 3 times per day [1A]; for patients with type 2 diabetes, the frequency of monitoring is dependent upon such factors as mode of treatment and level of glycemic control. [1C] To obtain meaningful data for treatment decisions, it is helpful for the patient to monitor for several consecutive days (e.g., 2-4 days). In addition to obtaining fasting and preprandial glucose levels, consider glucose readings 2-3 hours postprandially, as postprandial hyperglycemia has been implicated as a cardiovascular risk factor [1B] Postprandial monitoring is particularly recommended for patients who: Have an elevated A1C but fasting glucose is at target.
康柏西普联合微创玻璃体切割术对增殖型糖尿病视网膜病变患者视功能及疾病相关因子水平的影响
·17JOURNAL OF RARE AND UNCOMMON DISEASES, DEC. 2023,Vol.30, No.12, Total No.173【第一作者】昝晓宁,女,住院医师,主要研究方向:眼科。
E-mail:157****************【通讯作者】昝晓宁·论著·康柏西普联合微创玻璃体切割术对增殖型糖尿病视网膜病变患者视功能及疾病相关因子水平的影响*昝晓宁* 尚利晓 李 琰河南科技大学第一附属医院眼科 (河南 洛阳 471000)【摘要】目的 探讨接受微创玻璃体切割术的增殖型糖尿病视网膜病变患者联合康柏西普治疗后视功能与疾病相关因子水平的变化情况。
方法 此次研究所选病例数共98例,均为河南科技大学第一附属医院2020年10月至2022年12月所收治的增殖型糖尿病视网膜病变患者,将其纳入至研究后分成治疗方式为接受微创玻璃体切割术治疗的A组以及切割术联合康柏西普治疗的B组,例数相等,均为49例,患眼共98只,分组方式为随机数字表法。
两组患者均随访3个月。
比较两组患者治疗后的临床疗效,治疗前后视功能、血清血管内皮生长抑制因子(VEGI)、色素上皮衍生因子(PEDF)、胎盘生长因子(PIGF)、血管内皮生长因子(VEGF)水平,随访期间并发症的发生情况。
结果 治疗后,B组与A组临床总有效率比较结果显示前者更高;两组最佳视力矫正、血清VEGI、PEDF水平均较治疗前升高,前者较后者更高,黄斑中心区厚度、中央视网膜厚度、血清PIGF、VEGF水平均较治疗前降低,前者较后者更低;比较B组、A组随访期间并发症总发生率后得出,前者较后者显著更低(均P <0.05)。
结论 增殖型糖尿病视网膜病变患者应用康柏西普联合微创玻璃体切割术治疗可显著改善其视功能,调节疾病相关因子,减少术后并发症的发生,临床疗效显著,安全性较高。
【关键词】增殖型糖尿病视网膜病变; 康柏西普; 微创玻璃体切割术; 视功能; 疾病相关因子【中图分类号】R774.1【文献标识码】A【基金项目】2022年河南省职业教育和继续教育精品在线开放课程项目(2022YB0638) DOI:Effects of Conbercept Combined with Minimally Invasive Vitrectomy on Visual Function and Levels of Disease-related Factors in Patients with Proliferative Diabetic Retinopathy*ZAN Xiao-ning *, SHANG Li-xiao, LI Yan.Department of ophthalmology, The First Affiliated Hospital of Henan University of Science and Technology, Luoyang 471000, Henan Province, ChinaAbstract: Objective To investigate the changes of visual function and disease-related factors in patients with proliferative diabetic retinopathy who neededto undergo vitrectomy combined with Conbercept. Methods A total of 98 patients with proliferative diabetic retinopathy admitted to the first affiliated hospital of Henan University of Science and Technology from October 2020 to December 2022 were selected for this study, the patients were divided into two groups according to the random number table: the group A treated with micro-invasive vitrectomy and the group B treated with micro-invasive vitrectomy combined with conbercept injection, there were 49 cases with 98 eyes. Both groups were followed up for 3 months. The clinical efficacy after treatment, visual function, serum levels of vascular endothelial growth inhibitory factor (VEGI), pigment epithalium-derived factor (PEDF), placental growth factor (PIGF) and vascular endothelial growth factor (VEGF) before and after treatment, and the occurrence of complications during follow-up were compared between the two groups. Results After treatment, the total effective rate of the group B was higher than that of the group A. After treatment, the best visual acuity correction, serum VEGI and PEDF levels of the group B and the group A were higher than before treatment, and the former was higher than the latter . Macular central area thickness, central retina thickness, serum PIGF and VEGF levels were lower than before treatment, and the former was lower than the latter . The total incidence of complications of the group B was significantly lower than and the group A during the follow-up period(all P <0.05). Conclusion The treatment of patients with proliferative diabetic retinopathy with Conbercept combined with minimally invasive vitrectomy can significantly improve their visual function, regulate disease-related factors, reduce the occurrence of postoperative complications, with significant clinical efficacy and high safety.Keywords: Proliferative Diabetic Retinopathy; Conbercept; Minimally Invasive Vitrectomy; Visual Function; Disease-related Factor 增殖型糖尿病视网膜病变是临床中较为常见的一类糖尿病微血管病变,若患者发病后未能及时接受治疗则可引起其出现视力障碍,严重可致失明,此后果危险程度相对较高[1]。
色素上皮衍生因子(PEDF)
研究背景
NA0022
• 色素上皮衍生因子(PEDF)是丝氨酸蛋白酶抑制剂基因家族中的成员,是一种分 子量为50kDa的分泌型糖蛋白
• 首次在人类视网膜色素上皮细胞中被发现,是一种神经营养因子,具有抗氧化、抗 炎症、抗血管生成的作用
• 在细胞、动物学研究中发现,PEDF对糖尿病微血管损伤具具有保护性作用,可能 参与早期糖尿病肾病的病理改变
Hui E, Yeung CY, et al. J Clin Endocrinol Metab. 2014;99(11):E2169-77.
NA0022
AGE advanced glycation end products
总结
NA0022
• 糖尿病是促使CKD发生、发展的主要病因,早期发现糖尿病患者的CKD、严密监 测进程发展至关重要
• 该研究显示:PEDF是T2DM患者CKD进展的独立预测因子 • PEDF有望成为临床上预测T2DM患者CKD进展状况的新指标
T2DM type 2 diabetes mellitus eGFR estimated GFR
ACR albumin creatinine ratio ELISA enzyme-linked immuno sorbent assay
基线时,PEDF水平与eGFR呈显著负相关
r=-0.435,P<0.001
PEDF pigment epithelium-derived factor
研究设计
NA0022
• 前瞻性、纵向、观察性研究
• 入选标准:2008-2013年,港西糖尿病注册中心, 2型糖尿病(T2DM),年龄 ≥30岁,中国籍,n=1136
• 排除标准:基线时已开始透析或肾移植
PEDF对氧诱导视网膜病变小鼠视网膜MCP-1表达的影响
PEDF对氧诱导视网膜病变小鼠视网膜MCP-1表达的影响王亚娜;张磊【摘要】目的:观察色素上皮衍生因子(pigment epithelium-derivedfactor,PEDF)在氧诱导视网膜病变(oxygen-induced retinopathy,OIR)中对小鼠视网膜新生血管(retinal neovascularization,RNV)和单核细胞趋化因子-1(monocyte chemoattractant protein-1,MCP-1)表达的影响,探讨PEDF对缺血缺氧性视网膜病变的保护作用和机制.方法:取7日龄C57BL/6J新生小鼠160只,将120只7日龄小鼠与哺乳母鼠共同置于氧浓度为(75±2)%的氧环境内饲养5d,然后返回正常氧环境中饲养5d,建立OIR模型;40只小鼠始终置于正常氧环境饲养.分别于12日龄和14日龄给予PEDF药物治疗组小鼠右眼玻璃体腔注射PEDF(2μg/μL)各1μL,给予PBS治疗对照组和正常对照组小鼠右眼玻璃体腔注射等量的磷酸盐缓冲液(phosphate buffered saline,PBS).所有小鼠于17日龄麻醉处死后取视网膜,采用视网膜铺片和Lectin染色法观察各组小鼠病理性新生血管的生成情况;Western-blot检测PEDF和MCP-1蛋白在各组小鼠视网膜的表达;实时荧光定量逆转录多聚酶链反应(RT-PCR)检测各组小鼠视网膜PEDF和MCP-1 mRNA的表达.结果:视网膜铺片和Lectin染色结果显示OIR模型组RNV面积较正常组显著增大,差异有统计意义(P<0.01),PEDF药物治疗组RNV面积较PBS治疗对照组明显减小,差异有统计意义(P<0.01).Western-blot和RT-PCR结果显示,OIR模型组MCP-1蛋白和mRNA的表达水平均明显高于正常组,差异有统计意义(均P<0.05);OIR模型组PEDF蛋白和mRNA的表达水平均明显低于正常组,差异有统计意义(均P<0.01);PEDF药物治疗组MCP-1蛋白和mRNA的表达量较PBS治疗对照组均显著减少,差异有统计意义(均P<0.05);PEDF药物治疗组MCP-1蛋白和mRNA的表达量较正常对照组升高,但差异均无统计学意义(均P>0.05).结论:PEDF能够抑制OIR小鼠视网膜新生血管形成,同时下调MCP-1在OIR小鼠视网膜的表达,后者可能是其抑制新生血管形成从而发挥视网膜保护作用的机制之一.【期刊名称】《国际眼科杂志》【年(卷),期】2019(019)001【总页数】5页(P21-25)【关键词】氧诱导视网膜病变;色素上皮衍生因子;单核细胞趋化因子-1;视网膜新生血管【作者】王亚娜;张磊【作者单位】200137 中国上海市,上海中医药大学附属第七人民医院眼科;200137 中国上海市,上海中医药大学附属第七人民医院眼科【正文语种】中文0引言视网膜新生血管(retinal neovascularization,RNV)的形成是缺血缺氧性视网膜病变中最重要的病理过程,病变进一步发展可导致视功能不可逆性损害甚至丧失[1]。
糖尿病视网膜神经节细胞损伤的研究进展

糖尿病视网膜神经节细胞损伤的研究进展李东洁;吴迪;张旭乡【摘要】Diabetic retinopathy ( DR ) is one of the severe complications of diabetes, which could lead to severe visual impairment. Retinal ganglion cell ( RGC) apoptosis has been confirmed both in vivo and in vitro prior to the definite micro - vascular damages. RGC impairment contributes to an early deterioration of vision. Hyperglycemia, oxidative stress, neuron growth factor deficiency and glutamate excitotoxicity were found to be involved in retinal ganglion cell apoptosis. Some neuron protective agents have been showed to prevent the apoptosis of RGC in experimental diabetic retinopathy. Clinical evidences about effectiveness and security also suggested potential treatments for the diabetic retinal neuron.%糖尿病性视网膜病变( diabetic retinopathy,DR)是糖尿病严重并发症之一,可对患者造成严重视功能损害。
在视网膜出现微血管病变之前,已经出现视网膜神经节细胞(retinal ganglion cell, RGC)的病变。
关于如何预防糖尿病的英语作文

The Importance of Preventing DiabetesIn recent years, diabetes has become a significanthealth concern worldwide, affecting millions of people. Itis a chronic disease that occurs when the body cannot produce enough insulin or cannot effectively use theinsulin it produces. The consequences of diabetes can be severe, including heart disease, stroke, blindness, kidney failure, and amputations. Therefore, it is crucial to understand the importance of preventing diabetes and take necessary measures to protect oneself.Maintaining a healthy weight is one of the mosteffective ways to prevent diabetes. Obesity is a major risk factor for type 2 diabetes, as extra body weight can leadto insulin resistance. Regular physical activity and a balanced diet are essential for maintaining a healthy weight. Engaging in at least 150 minutes of moderate-intensity aerobic activity per week, such as walking, cycling, or swimming, can help reduce the risk of diabetes. Eating a balanced diet is also crucial for diabetes prevention. A diet rich in fruits, vegetables, whole grains, and lean protein can help maintain a healthy weight andprovide the body with essential nutrients. Avoiding sugary drinks and foods high in saturated and trans fats can help reduce the risk of diabetes. Additionally, limiting salt intake can help prevent high blood pressure, which is a common complication of diabetes.Moreover, regular health screenings can help detect diabetes early and prevent its progression. People at risk of diabetes should have their blood sugar levels checked regularly. If diabetes is detected, prompt treatment can help manage the condition and prevent complications.In addition to lifestyle changes, some people may benefit from taking medication to prevent diabetes. Medications such as metformin or GLP-1 agonists can help lower blood sugar levels and reduce the risk of diabetes in people with prediabetes. However, it is important to consult a healthcare provider before taking any medication. In conclusion, preventing diabetes is crucial for maintaining good health. By maintaining a healthy weight, eating a balanced diet, engaging in regular physical activity, limiting salt intake, and undergoing regular health screenings, people can reduce their risk ofdeveloping diabetes. Additionally, taking medication as prescribed by a healthcare provider can help prevent diabetes in those with prediabetes. Remember, prevention is always better than cure, and taking proactive steps to prevent diabetes can help enjoy a healthy and fulfilling life.**糖尿病预防的重要性**近年来,糖尿病已成为全球范围内的重要健康问题,影响着数百万人。
神经妥乐平治疗痛性糖尿病神经病变的疗效分析
神经妥乐平治疗痛性糖尿病神经病变的疗效分析孔凡明济宁市兖州区铁路医院神经内科,山东济宁272100[摘要]目的探究神经妥乐平治疗痛性糖尿病神经病变的疗效。
方法选取济宁市兖州区铁路医院2020年1月—2022年6月收治的60例痛性糖尿病周围神经病变(painful diabetic peripheral neuropathy, PDPN)患者作为研究对象。
采取随机数表法分为对照组、研究组,每组30例。
对照组予以口服卡马西平片治疗,研究组在基础治疗基础上加用神经妥乐平静脉注射治疗。
对比两组临床疗效。
结果研究组治疗效果、神经传导速度均优于对照组,且TSS评分低于对照组,疼痛缓解时间短于对照组,差异有统计学意义(P<0.05);两组治疗过程中均无明显不良反应发生。
结论神经妥乐平治疗DPN疗效确切、安全性较高,可改善患者神经传导速度及疼痛程度、缓解时间。
[关键词] 神经妥乐平;痛性糖尿病神经病变;疗效[中图分类号] R587.1 [文献标识码] A [文章编号] 1672-4062(2023)04(b)-0178-04 Efficacy of Neurotropin in the Treatment of Painful Diabetic Neuropathy KONG FanmingDepartment of Neurology, Yanzhou District Railway Hospital, Jining, Shandong Province, 272100 China [Abstract] Objective To explore the efficacy of Neurotropin in the treatment of painful diabetic neuropathy.Methods 60 patients with painful diabetic peripheral neuropathy (PDPN) who were admitted to Yanzhou District Railway Hospi‐tal from January 2020 to June 2022 are selected as the study objects. Random number table method was used to di‐vide 30 cases into control group and 30 cases into study group. The control group was treated with oral carbamazepine tablets, while the study group was treated with intravenous injection of neurotropin on the basis of basic treatment. The clinical efficacy of the two groups was compared.Results The treatment effect and nerve conduction velocity of the study group were better than those of the control group, and the TSS score was lower than that of the control group, and the pain relief time was shorter than that of the control group, the difference was statistically significant (P<0.05); no obvious adverse reactions occurred in the two groups during the treatment.Conclusion Neurotropin has a definite therapeutic effect and high safety in the treatment of DPN, which can improve the patient´s nerve conduction velocity, pain level, and relief time.[Key words] Neurotropin; Painful diabetic neuropathy; Curative effect糖尿病神经病变发生率约占糖尿病的20%,痛性糖尿病周围神经病变(painful diabetic peripheral neuropathy, PDPN)发病率为13%~26%。
叶黄素对糖尿病视网膜病变的作用和机制
叶黄素对糖尿病视网膜病变的作用和机制王俐媛;韩悦;张强;郭芳;马乐【摘要】叶黄素(Lutein)是一种含氧的类胡萝卜素.由于人体不能合成,其主要来源为食物.多项研究显示,叶黄素对包括糖尿病视网膜病变在内的年龄相关性退行性眼病具有保护作用.动物和细胞研究提示叶黄素可通过缓解高血糖诱导的氧化应激反应,起到保护视网膜血管内皮细胞,减少视网膜新生血管形成,达到减轻视网膜损伤的效用.本文将阐述叶黄素在预防和控制糖尿病视网膜病的发生发展等方面作用机制和研究现状.%Lutein belongs to the xanthophyll family of carotenoids, which are mainly synthesized from dark green leafy plants.Evidence from several studies has shown that patients with age-related degenerative eye disease including diabetic retinopathy (DR),may benefit from oral luteinintake.Animal and cell researches suggest that lu-tein,through oxidative stress induced by hyperglycemia remission,could protect retinal vascular endothelial cells, reduce formation of retinal neovascularization,and therefore mitigating possible retinal damages.This article re-views the results and possible mechanisms of lutein on DR at cellular and molecular level,offering insights in preven-tion and control measures of DR.【期刊名称】《国外医学(医学地理分册)》【年(卷),期】2015(036)004【总页数】3页(P311-313)【关键词】叶黄素;糖尿病视网膜病变;机制研究【作者】王俐媛;韩悦;张强;郭芳;马乐【作者单位】西安交通大学医学部公共卫生学院,西安 710061;西安交通大学医学部公共卫生学院,西安 710061;西安交通大学医学部公共卫生学院,西安 710061;西安交通大学医学部公共卫生学院,西安 710061;西安交通大学医学部公共卫生学院,西安 710061【正文语种】中文【中图分类】R774糖尿病视网膜病变(diabetic retinopathy,DR)是糖尿病常见的微血管并发症,目前尚无行之有效的治疗手段,致盲率高,目前已成为发达国家的主要致盲原因。
色素上皮衍生因子与胰岛素抵抗的相关性
色素上皮衍生因子与胰岛素抵抗的相关性色素上皮衍生因子(pigment epithelium-derived factor,PEDF)是具有多种生理活性的糖蛋白,包括抗血管新生、降低血管通透性、抗肿瘤以及神经营养活性。
最近研究表明PEDF能够调节糖代谢和脂代谢,与胰岛素抵抗的有一定的联系。
本文就PEDF引起胰岛素抵抗这方面的研究做一综述,阐述了PEDF与代谢性疾病的广泛联系,并总结了PEDF引起胰岛素抵抗的可能机制。
[Abstract] Pigment epithelium-derived factor(PEDF)is a glycoprotein with a variety of physiological activities including anti-angiogenic,anti-vasopermeability,anti-tumor,and neurotrophic activities.Recent studies have shown that PEDF is a metabolic regulatory protein that plays a casual role in glucose and lipid metabolism.This review focus on researches which regard PEDF as the causes of insulin resistance,describes the extensive contacts between PEDF and metabolic diseases,and summarizes the probable mechanisms adopted by PEDF to induce insulin resistance.[Key words] PEDF;Metabolism;Insulin resistance;MechanismsPEDF是在人視网膜色素上皮细胞的分泌物中发现并纯化的50-KDa糖蛋白。
糖尿病早期视网膜神经变性-研究综述
糖尿病早期视网膜神经变性【摘要】糖尿病性视网膜病变(diabetic retinopathy,DR)在过去通常被认为是一种原发性血管病变,而最近的研究数据提示了糖尿病视网膜神经变性(diabetic retinal neurodegeneration,DRN)在糖尿病眼部损伤中的重要作用。
糖尿病患者人群中,DRN常与DR同时存在,并且先于DR发生,因此猜测DRN可能是DR的起始因素之一,但目前二者相互关系尚未能阐明。
糖尿病引起视网膜神经变性的机制,以及视网膜神经变性与DR因果关系如果能得到证实,则可以对糖尿病性视网膜病变进行早期临床干预,从而延缓糖尿病患者的视力丧失。
【关键词】糖尿病性视网膜病变;糖尿病视网膜神经变性;凋亡;糖尿病糖尿病性视网膜病变(diabetic retinopathy, DR)是最常见的视网膜血管病。
目前DR主要以视网膜血管变化进行临床分期。
但视网膜诸多细胞在检眼镜可见的视网膜微血管异常之前,可能已经发生变性及功能改变,如:对比敏感度降低、mfERG潜时(IT;implicit time.闪光开始到波峰或波谷出现的时间)延长、色觉及微视野检查结果异常等。
在动物实验模型中,视网膜神经细胞凋亡可在诱导糖尿病后1个月发生;在眼底检查未达DR诊断标准的人类糖尿病患者中,也可见类似的视网膜神经节细胞丢失。
[1]在一项无DR糖尿病患者为期4年的随访中,视网膜以每年0.54µm的速率进行性变薄,且伴随功能的改变。
[2]这些证据均提示糖尿病患者未发生DR前已发生DRN。
视网膜神经节细胞是凋亡率最高且受影响最早的细胞。
[3]然而,在外核层和视网膜色素上皮细胞(RPE)中也观察到凋亡率升高。
[4]此外,除了细胞凋亡,视网膜神经性变性的另一个特征是神经胶质细胞活化。
[5]糖尿病视网膜发生神经变性过程中,高血糖的毒性作用和谷氨酸水平升高可能起了重要作用。
[6]但是,单独的神经毒性因子的水平并不能决定糖尿病视网膜神经变性(diabetic retinal neurodegeneration,DRN)的存在与否,而是神经毒性因子和神经保护因子水平的失衡起了决定性作用。
糖尿病视网膜病变的临床特点及治疗进展研究

糖尿病视网膜病变的临床特点及治疗进展研究张思睿,王玉清佳木斯大学附属第一医院眼科,黑龙江佳木斯154000[摘要]糖尿病性视网膜病变是一种较为常见的糖尿病微血管并发症之一。
其病程复杂、治疗难度大,糖尿病性视网膜病变是现阶段较为严重的致盲性眼病,严重影响了患者的视力功能和生活质量。
随着医学技术的不断进步,治疗手段也在不断创新发展。
本文阐述了糖尿病视网膜病变的概念、病因和发病机制,并对糖尿病视网膜病变的治疗方法进行梳理,深入探讨其在临床实践中的应用和前景,旨在提升治疗效果、降低治疗风险,最大限度地提高患者生活质量。
[关键词] 糖尿病视网膜病变;临床特点;治疗方法;进展[中图分类号] R587.2 [文献标识码] A [文章编号] 1672-4062(2024)02(b)-0190-05Study on the Clinical Characteristics and Treatment Progress of Diabetic RetinopathyZHANG Sirui, WANG YuqingDepartment of Ophthalmology, the First Affiliated Hospital of Jiamusi University, Jiamusi, Heilongjiang Province, 154000 China[Abstract] Diabetic retinopathy is one of the more common microvascular complications of diabetes. With its complex course and difficult treatment, diabetic retinopathy is a serious blinding eye disease, which seriously affects the visual function and quality of life of patients. With the continuous progress of medical technology, the treatment means are constantly innovating and developing. This paper describes the concept, etiology and pathogenesis of diabetic retinopa⁃thy, and combs through the treatment methods of diabetic retinopathy to discuss its application and prospects in clini⁃cal practice, aiming to enhance the therapeutic effect, reduce the therapeutic risk, and maximize the quality of life of patients.[Key words] Diabetic retinopathy; Clinical characteristics; Therapeutic approach; Progress糖尿病是临床常见的慢性代谢性疾病,近年来我国糖尿病发病率随着人口老龄化加剧和生活、饮食习惯的改变而持续增加[1]。
2.糖尿病视网膜病变防治专家共识
2.糖尿病视⽹膜病变防治专家共识中华糖尿病杂志2018年4⽉第10卷第4期ChinJDiabetesMellitus,April2018,Vol.10,No.4·247·specificityofnonmydriaticdigitalstereoscopicretinalimaging[48]ChaturvediN,PortaM,KleinR,etal.Effectofcandesartan indetectingdiabeticretinopathy[J].DiabetesCare,2006,29onprevention(DIRECT-Prevent1)andprogression (10):2205-2209.DOI:10.2337/dc06-0295.(DIRECT-Protect1)ofretinopathyintype1diabetes:[33]SolomonSD,ChewE,DuhEJ,etal.Diabeticretinopathy:arandomised,placebo-controlledtrials[J].Lancet,2008,372 positionstatementbytheAmericanDiabetesAssociation[J].(9647):1394-1402.DOI:10.1016/S0140-6736(08)61412-9. DiabetesCare,2017,40(3):412-418.DOI:10.2337/dc16-2641.[49]Sj?lieAK,KleinR,PortaM,etal.Effectofcandesartanon [34]WaltonOB,GaroonRB,WengCY,etal.Evaluationofprogressionandregressionofretinopathyintype2diabetes automatedteleretinalscreeningprogramfordiabetic(DIRECT-Protect2):arandomisedplacebo-controlledtrial[J]. retinopathy[J].JAMAOphthalmol,2016,134(2):204-209.DOI:Lancet,2008,372(9647):1385-1393.DOI:10.1016/S0140-673610.1001/jamaophthalmol.2015.5083.(08)61411-7.[35]彭⾦娟,黄建南,陆丽娜,等.糖尿病视⽹膜病变远程筛查[50]MauerM,ZinmanB,GardinerR,etal.Renalandretinal系统的研究进展[J].中华眼科杂志,2016,52(11):868-871.effectsofenalaprilandlosartanintype1diabetes[J].NEnglJ DOI:10.3760/cma.j.issn.0412-4081.2016.11.014.Med,2009,361(1):40-51.DOI:10.1056/NEJMoa0808400.[36]中华医学会糖尿病学分会微⾎管并发症学组.糖尿病肾病[51]EmdinCA,RahimiK,NealB,etal.Bloodpressurelowering防治专家共识(2014年版)[J].中华糖尿病杂志,2014,6(11):intype2diabetes:asystematicreviewandmeta-analysis[J]. 792-801.DOI:10.3760/cma.j.issn.1674-5809.2014.11.004.JAMA,2015,313(6):603-615.DOI:10.1001/jama.2014.18574.[37]ScottishIntercollegiateGuidelinesNetwork.Managementof[52]WangB,WangF,ZhangY,etal.EffectsofRASinhibitorsondiabetes:anationalclinicalguideline[DB/OL].Edinburg:diabeticretinopathy:asystematicreviewandmeta-analysis[J]. ScottishIntercollegiateGuidelinesNetwork,HealthcareLancetDiabetesEndocrinol,2015,3(4):263-274.DOI:10.1016/ ImprovementScotland,2010(2017-11-05)[2017-12-15].http://S2213-8587(14)70256-6./assets/sign116.pdf.[53]KeechAC,MitchellP,SummanenPA,etal.Effectoffenofibrate[38]NationalInstituteforHealthandCareExcellence.Type2ontheneedforlasertreatmentfordiabeticretinopathy(FIELD diabetesinadults,management[DB/OL].London:Nationalstudy):arandomisedcontrolledtrial[J].Lancet,2007,370(9600):InstituteforHealthandCareExcellence,2015(2015-12-02)1687-1697.DOI:10.1016/S0140-6736(07)61607-9.[2017-11-25].https:///guidance/ng28/resources/[54]ChewEY,AmbrosiusWT,DavisMD,etal.Effectsofmedical type-2-diabetes-in-adults-management-pdf-1837338615493.therapiesonretinopathyprogressionintype2diabetes[J].N[39]全国防盲技术指导组.糖尿病视⽹膜病变分级诊疗服务技EnglJMed,2010,363(3):233-244.DOI:10.1056/术⽅案[J].中华全科医师杂志,2017,16(8):589-593.DOI:NEJMoa1001288.10.3760/cma.j.issn.1671-7368.2017.08.005.[55]NoonanJE,JenkinsAJ,MaJX,etal.Anupdateonthe[40]AntonettiDA,KleinR,GardnerTW.Diabeticretinopathy[J]. molecularactionsoffenofibrateanditsclinicaleffectsonNEnglJMed,2012,366(13):1227-1239.DOI:10.1056/ diabeticretinopathyandothermicrovascularendpointsinNEJMra1005073.patientswithdiabetes[J].Diabetes,2013,62(12):3968-3975.[41]CanadianDiabetesAssociationClinicalPracticeGuidelineDOI:10.2337/db13-0800.ExpertCommittee.Retinopathy[J].CanJDiabetes,2013,37[56]BergerhoffK,ClarC,RichterB.AspirinindiabeticSuppl1:S137-141.DOI:10.1016/j.jcjd.2013.01.038.retinopathy:asystematicreview[J].EndocrinolMetabClin[42]AmericanAcademyofOphthalmology.DiabeticRetinopathy[DB/NorthAm,2002,31(3):779-793.DOI:10.1016/S0889-8529OL].SanFrancisco,CA:AmericanAcademyofOphthalmology,(02)00017-8.2017(2017-12-01)[2017-12-22].https:///preferred-[57]ZhangX,LiuW,WuS,etal.Calciumdobesilatefordiabeticpractice-pattern/diabetic-retinopathy-ppp-updated-2017.retinopathy:asystematicreviewandmeta-analysis[J].Sci [43]KleinR,LeeKE,GangnonRE,etal.The25-yearincidenceChinaLifeSci,2015,58(1):101-107.DOI:10.1007/ofvisualimpairmentintype1diabetesmellitusthewisconsins11427-014-4792-1. epidemiologicstudyofdiabeticretinopathy[J].Ophthalmology,[58]中华中医药学会糖尿病分会.糖尿病视⽹膜病变中医诊疗2010,117(1):63-70.DOI:10.1016/j.ophtha.2009.06.051.标准[J].世界中西医结合杂志,2011,6(7):632-637.DOI:[44]KleinR,KleinBE.Istheprevalenceofvisualimpairment10.3969/j.issn.1673-6613.2011.07.027.risingorfallinginthepeoplewithdiabetesmellitus?It[59]邓辉,⾦明,苑维,等.复⽅丹参滴丸治疗早期糖尿病视⽹dependsonwhoyoustudy[J].JAMAOphthalmol,2013,131(7):膜病变的临床观察[J].中国中医眼科杂志,2005,15(2):948-950.72-74.DOI:10.3969/j.issn.1002-4379.2005.02.004.[45]LiewG,MichaelidesM,BunceC.Acomparisonofthecauses[60]叶晓峰,徐格致.复⽅⾎栓通胶囊对糖尿病⼤⿏视⽹膜氧ofblindnesscertificationsinEnglandandWalesinworkingage化应激损伤保护作⽤的观察[J].中华眼底病杂志,2010,26adults(16-64years),1999-2000with2009-2010[J].BMJOpen,(2):176-178.DOI:10.3760/cma.j.issn.1005-1015.2010.02.21.2014,4(2):e004015.DOI:10.1136/bmjopen-2013-004015.[61]GundersonEP,LewisCE,TsaiAL,etal.A20-year[46]KilpatrickES,RigbyAS,AtkinSL,etal.Doessevereprospectivestudyofchildbearingandincidenceofdiabetesin hypoglycaemiainfluencemicrovascularcomplicationsintypeyoungwomen,controllingforglycemiabeforeconception:the 1diabetes?ananalysisofthediabetescontrolandCoronaryArteryRiskDevelopmentinYoungAdultscomplicationstrialdatabase[J].DiabetMed,2012,29(9):(CARDIA)Study[J].Diabetes,2007,56(12):2990-2996.DOI:1195-1198.DOI:10.1111/j.1464-5491.2012.03612.x.10.2337/db07-1024.[47]HarindhanavudhiT,MauerM,KleinR,etal.Benefitsofrenin-angiotensinblockadeonretinopathyintype1diabetes(收稿⽇期:2018-03-04)varywithglycemiccontrol[J].DiabetesCare,2011,34(8):1838-1842.DOI:10.2337/dc11-0476.(本⽂编辑:杨颖)。
糖尿病视网膜病
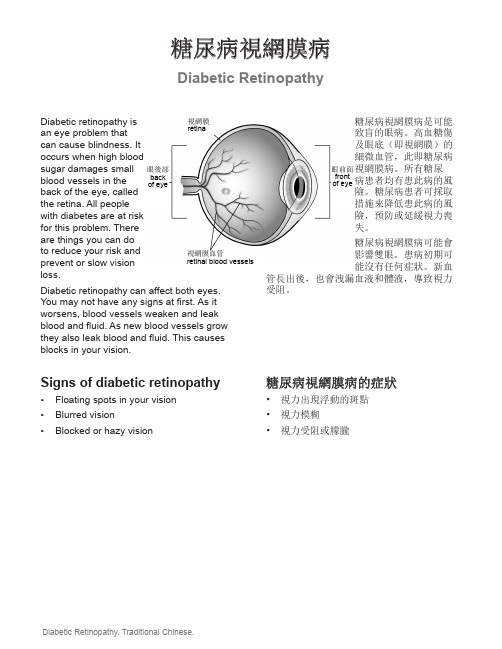
Diabetic Retinopathy 糖尿病視網膜病Diabetic retinopathy isan eye problem thatcan cause blindness. Itoccurs when high bloodsugar damages smallblood vessels in theback of the eye, calledthe retina. All peoplewith diabetes are at riskfor this problem. Thereare things you can doto reduce your risk andprevent or slow visionloss.Diabetic retinopathy can affect both eyes. You may not have any signs at first. As it worsens, blood vessels weaken and leak blood and fluid. As new blood vessels grow they also leak blood and fluid. This causes blocks in your vision.Signs of diabetic retinopathy • Floating spots in your vision• Blurred vision• Blocked or hazy vision糖尿病視網膜病是可能致盲的眼病。
高血糖傷及眼底(即視網膜)的細微血管,此即糖尿病視網膜病。
所有糖尿病患者均有患此病的風險。
糖尿病患者可採取措施來降低患此病的風險,預防或延緩視力喪失。
糖尿病視網膜病可能會影響雙眼。
患病初期可能沒有任何症狀。
新血管長出後,也會洩漏血液和體液,導致視力受阻。
糖尿病視網膜病的症狀• 視力出現浮動的斑點• 視力模糊• 視力受阻或朦朧視網膜retina眼後部back of eye眼前面frontof eye視網膜血管retinal blood vessels2© 2007 - November 21, 2016, Health Information Translations.Unless otherwise stated, user may print or download information from for personal, non-commercial use only. The medical information found on this website should not be used in place of a consultation with your doctor or other health care provider. You should always seek the advice of your doctor or other qualified health care provider before you start or stop any treatment or with any questions you may have about a medical condition. The Ohio State University Wexner Medical Center, Mount Carmel Health System, OhioHealth and Nationwide Children’s Hospital are not responsible for injuries or damages you may incur as a result of your stopping medical treatment or your failure to obtain treatment.Your careTo help reduce your risk of vision loss:• Keep your blood sugar levels wellcontrolled. This is one of the best ways to protect your vision. Work with your doctor, nurse and dietitian.• Keep your blood pressure and blood cholesterol levels normal. You may need to take medicine.• Have an eye exam each year by an eye specialist that includes eye dilation. An eye exam can detect early changes before you have any signs.• Call your doctor if you have any changes in your vision.There is no cure for diabetic retinopathy, but laser treatment or surgery may be done to prevent or slow vision loss.Talk to your doctor or nurse if you have any questions or concerns.護理為了降低視力喪失的危險:• 控制好血糖水平。
糖尿病的预防英语作文
糖尿病的预防英语作文I think preventing diabetes is really important. We need to watch what we eat and make sure we exercise regularly. It's all about taking care of our bodies and staying healthy. 。
One way to prevent diabetes is to avoid eating too much sugar and processed foods. These can cause spikes in blood sugar levels and lead to insulin resistance. Instead, we should focus on eating whole foods like fruits, vegetables, and whole grains.Exercise is also key in preventing diabetes. It helps to keep our weight in check and improves insulin sensitivity. Plus, it's a great way to reduce stress and improve overall health. So, whether it's going for a run, taking a dance class, or just going for a walk, staying active is crucial.Another important aspect of diabetes prevention isgetting regular check-ups with our doctor. They can help monitor our blood sugar levels and catch any potential issues early on. It's always better to be proactive when it comes to our health.In addition to diet, exercise, and regular check-ups, it's also important to manage stress and get enough sleep. Stress can affect our blood sugar levels and sleep is crucial for overall health. So, finding ways to relax and unwind, as well as prioritizing sleep, are important steps in preventing diabetes.Overall, preventing diabetes is all about taking care of ourselves and making healthy choices. By watching what we eat, staying active, getting regular check-ups, managing stress, and getting enough sleep, we can reduce our risk of developing diabetes and live a healthier life.。
褪黑素治疗糖尿病视网膜病变的研究进展
脂质过氧化标记物硫代巴比妥酸反应物和蛋白 质氧化标记物氧化蛋白产物在 DR患者血清和糖尿 病大鼠视 网 膜 中 表 达 升 高[17]。 褪 黑 素 可 降 低 糖 尿 病大鼠视网膜中脂质过氧化物水平,抑制 NOS活性, 减少一氧化 氮 (NO)的 产 生,恢 复 过 氧 化 氢 酶 活 性。 作为活性氧 的 直 接 清 除 剂,褪 黑 素 可 中 和 糖 尿 病 脂
方面发挥了良好作用。新近研究表明,2型糖尿病患 者与正常人相比,夜间褪黑素的分泌量较低,给予褪 黑素缓释剂(2mg)5个月后可显著降低患者糖化血 红蛋白 和 血 糖 的 水 平[8],且 较 大 剂 量 的 褪 黑 素 (6 mg)能够更好地控制 2型糖尿病患者的血糖浓度[9]。
眼 科 新 进 展 2021年 7月 第 41卷 第 7期 RecAdvOphthalmol Vol.41No.7July2021
部疾病临床医学研究中心,上海市 量活性氧自由基(ROS)。而过量的 ROS又会激活上述四条途径,攻击视网膜
眼底病重点实验室,上海眼视 觉 与 光医学工程技术研究中心,上海 市
蛋白质、脂质、核酸及细胞膜内酶系统,破坏细胞内生物大分子,导致视网膜微
眼科疾病精准诊疗工程技术研究中 血管病变、神经元及神经胶质细胞病变,加重视网膜“神经血管单元”损伤,参
羟苯磺酸钙分散片联合明目地黄丸治疗NPDR的临床疗效
羟苯磺酸钙分散片联合明目地黄丸治疗NPDR的临床疗效阿依努·努拉厚;王雁;卜倩;赵勇【摘要】目的:探讨羟苯磺酸钙分散片联合明目地黄丸治疗非增殖期糖尿病视网膜病变(NPDR)患者的临床疗效、以及对视网膜新生血管相关因子及血脂水平的影响.方法:选择2017-01/2018-03在我院进行治疗的100例NPDR患者作为研究对象,将其随机分为对照组(50例,采用羟苯磺酸钙分散片进行治疗)以及观察组(50例,在对照组基础上加用明目地黄丸进行治疗).比较两组治疗前后临床评价指标、视网膜新生血管相关因子及血脂水平.结果:治疗前,两组患者临床评价指标、视网膜新生血管相关因子及血脂水平无差异(P>0.05).治疗2个疗程后,两组患者视野灰度值、血管瘤体积、黄斑厚度、出血斑面积、血管内皮生长因子、胰岛素样生长因子-1(IGF-1)、组织因子(TF)、总胆固醇(TC)、甘油三酯(TG)及低密度脂蛋白胆固醇(LDL-C)水平均较治疗前显著降低(P<0.05);视力、色素上皮衍生因子及高密度脂蛋白胆固醇(HDL-C)水平则较治疗前显著升高(P<0.05);且观察组视野灰度值、血管瘤体积、黄斑厚度、出血斑面积、VEGF、IGF-1、TF、TC、TG及LDL-C水平较对照组降低明显(P<0.05),视力、PEDF及HDL-C水平较对照组升高明显(P<0.05).结论:羟苯磺酸钙分散片联合明目地黄丸治疗能显著改善患者临床评价指标、抑制血管新生及改善血脂水平.【期刊名称】《国际眼科杂志》【年(卷),期】2019(019)006【总页数】5页(P992-996)【关键词】明目地黄丸;非增殖期糖尿病视网膜病变;视网膜血管新生;血脂【作者】阿依努·努拉厚;王雁;卜倩;赵勇【作者单位】830001 中国新疆维吾尔自治区乌鲁木齐市,新疆医科大学附属中医医院眼科;830001 中国新疆维吾尔自治区乌鲁木齐市,新疆医科大学附属中医医院眼科;830001 中国新疆维吾尔自治区乌鲁木齐市,新疆医科大学附属中医医院眼科;830001 中国新疆维吾尔自治区乌鲁木齐市,新疆医科大学附属中医医院眼科【正文语种】中文0引言目前,随着人们经济水平及生活方式的不断提高与改变,糖尿病患者的数量日趋增多,已严重影响到患者的生活质量[1]。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Hindawi Publishing CorporationJournal of Biomedicine and BiotechnologyVolume2012,Article ID580687,8pagesdoi:10.1155/2012/580687Review ArticlePEDF in Diabetic Retinopathy:A Protective Effect ofOxidative StressXiao-feng Zhu and Hai-dong ZouDepartment of Ophthalmology,Shanghai First People’s Hospital,Shanghai Jiao Tong University,Shanghai200080,ChinaCorrespondence should be addressed to Hai-dong Zou,zouhaidong@Received8December2011;Accepted8February2012Academic Editor:Takeshi YabeCopyright©2012X.-f.Zhu and H.-d.Zou.This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use,distribution,and reproduction in any medium,provided the original work is properly cited.Diabetic retinopathy(DR)is a major cause of blindness in working age adults,and oxidative stress plays a vital role in the pathogenesis of DR.Pigment-epithelium-derived factor(PEDF),a multifunctional protein,has shown to inhibit the development of DR by accumulating evidence.This paper highlights the current understanding of probable mechanism about how PEDF blocks the deterioration of DR through its antioxidative properties and application prospects of PEDF as a novel therapeutic target in DR.Gene therapy of PEDF is becoming more and more acceptable and will widely be applied to the actual treatment in the near future.1.IntroductionDiabetic retinopathy(DR)is the leading cause of acquired vision loss among adults of working age in developed countries worldwide and has been perceived as the most common microvascular complications of diabetes[1–3]. Therefore,within three tofive years after the onset of type 1diabetes and shortly after the diagnosis of type2diabetes, the diabetic patients are recommended to be screened for retinopathy with an initial dilated and comprehensive eye examination by an ophthalmologist regularly[4].Chronic hyperglycemia which is well documented is a primary initiator of DR[5].In principle,intensive glycemic control can delay the development of DR[5].However,it is noteworthy that some patients may still develop DR even with good glycemic control[6,7].This remaining effect, prior to glycemic control,suggests a“metabolic memory”phenomenon.Furthermore,a growing number of studies have shown that the retina experience increased oxidative damage continuously,even in tight glycemic control,and oxidative stress plays a vital role in the pathogenesis of DR [6,8].The molecular mechanisms of hyperglycemia-induced DR are not fully clear,and the majority of publications focus on multiple biochemical pathways,including the augmenta-tion of polyol pathway[9],protein kinase C(PKC)activation [10],increased advanced glycation endproducts(AGEs) formation,the receptor for AGEs and its activating ligands [11],and overactivity of the hexosamine pathway[12]. However,all the mechanisms are activated by a single event: aberrant production of the mitochondria-derived reactive oxygen species(ROS)to increase the level of oxidative stress [13].Therefore,antioxidant therapy is being studied to prevent induction of the various pathogenic mechanisms of DR.With the failure of demonstrating that dietary supplementations of multiantioxidants have beneficial effects clinically[14],an antioxidant which could specifically target pathogenesis of DR is no time to delay.Pigment-epithelium-derived factor(PEDF),a50-kDa secreted glycoprotein, recently is shown to inhibit the development of DR through its antioxidative properties.This paper summarizes the probable protective mechanism of PEDF in high-glucose-induced oxidative stress and application prospects of PEDF as a novel therapeutic target in DR.2.PEDF and Its Potential Protective Roleof Oxidative Stress in Diabetic Retinopathy 2.1.PEDF and Its Biological Function.PEDF is a418-aminoacid,50-KDa protein which wasfirst purified fromconditioned medium from both fetal and adult retinal pig-ment epithelial(RPE)cells[15–18]and it is a noninhibitory member of the serine protease inhibitor(serpin)family. PEDF is widely expressing throughout the body,especially in the nervous system and the retina.According to current research,PEDF has shown that it is a multifunctional protein with demonstrable neurotrophic[19,20],antiangiogenic [16],antivasopermeability[21],antiinflammatory[22], antifibrosis[23],and antitumorigenic[24]properties and inhibited the development of DR through its antioxidative properties by accumulating evidence[25–28].Earlier clinical studies demonstrated an inverse correla-tion of the levels of intraocular PEDF and the development of abnormal angiogenesis in some ocular diseases,such as proliferative diabetic retinopathy(PDR)[16,29–32]. Similarly,in mouse model of type2diabetes mellitus,lower vitreous or aqueous humour levels of PEDF are associated with early phase of experimental DR[16,31,33],and decreased protein levels of PEDF in the retina are associated with ischemia-induced retinal neovascularization in the oxygen-induced retinopathy(OIR)model as well[34].Therefore,existing research data demonstrated that upregulation or substitution of PEDF may be a promising therapeutic target for DR[16,25,35–37],especially oxidative stress-involved retinal tissue damage[38].Then,experimen-tal interventions to increase locally PEDF concentrations, either by an adenovirus expressing human PEDF or a purified recombinant PEDF protein,have shown to attenuate retinal tissue damage in different animal models[22,39]. Thus,finding a good way for controlling PEDF expression and action in the retina has become a research focus.In addition,PEDF suppresses vascular endothelial growth-factor-induced(VEGF-induced)retinal microvascu-lar endothelial cell proliferation and migration[40]and inhibits VEGF activation in human retinal endothelial cells in vitro condition[41].In contrast,PEDF has a synergistic action with VEGF on cell proliferation in endothelial cells cultured in the presence of VEGF[42].Moreover,the VEGF and PEDF expression in M¨u ller cells is unbalanced under high-glucose concentration,which contributes to retinal neovascularization in DR[43].Since VEGF plays a pivotal role in the formation of ROS,to defining the specific effects of PEDF,high-glucose-induced oxidative stress will also be important.2.2.Antioxidative Properties of PEDF in Diabetic Retinopathy 2.2.1.Inhibit AGEs-Induced Injury.AGEs,senescent macro-proteins formed at an accelerated rate in diabetes,cause apoptotic cell death in retinal pericytes[44,45].Studies have found AGEs significantly decreased endothelial mRNA levels of PEDF in endothelial cells[46],and PEDF proteins protect cultured retinal pericytes from AGEs-induced injury probably via oxidative stress generation[25].Thus,we will introduce the different possible mechanisms of PEDF to inhibit AGEs-induced injury in DR.Retinal Pericytes.Earlier studies have found that loss of pericytes and increased vascular permeability,followed by microvascular occlusion in the retinas,ultimately leaded to the development of DR[47,48].Experimental analysis revealed that pericytes possessed of a membrane protein with binding affinity for PEDF which significantly inhib-ited AGEs-induced ROS generation and the subsequent decrease in DNA synthesis and apoptotic cell death in pericytes.Furthermore,PEDF proteins completely restored the downregulation of bcl-2(an antiapoptotic molecule) gene expressing in AGEs-exposed pericytes[25].Similarly, the studies have demonstrated that PEDF completely blocked high-glucose-or H2O2-induced intracellular ROS generation and an increased ratio of bax to bcl-2mRNA level with subsequent activation of caspase-3in pericytes[49].In addition,PEDF protected high glucose-(30mM)or H2O2-induced pericyte apoptosis and dysfunction through its antioxidative properties via glutathione peroxidase(GPx) induction.Simultaneously,the study also found that PEDF’s mRNA levels themselves were downregulated in high-glucose (HG-)or H2O2-exposed pericytes.These results all demonstrated that PEDF proteins pro-tected cultured pericytes from AGEs-induced cytotoxicity through its antioxidative properties,and substitution of PEDF proteins may be a promising strategy in treatment of patients with DR.Monocyte Chemoattractant Protein-1(MCP-1).Further work have shown that PEDF prevented the AGEs-induced upregulation of monocyte chemoattractant protein-1 (MCP-1)mRNA contents as well as protein production in microvascular endothelial cells(ECs)[50].Moreover,levels of MCP-1in vitreousfluids have been correlated with the severity of PDR[51].Rage.There is a growing body of evidence that RAGE is a signal-transducing receptor for AGEs,and that engagement of RAGE by AGEs elicits vascular inflammation and alters gene expression in retinal vascular wall cells,thereby it is involved in the development and progression of DR[45,50, 52–54].Recent studies have shown that PEDF could inhibit diabetes-(in the eye of diabetic rats)or AGEs-induced(in vitro)RAGE gene expression by blocking the superoxide-mediated NF-kappaB activation[36].Endothelial NO Synthase(eNOS).Studies have shown that PEDF prevented the AGEs-elicited endothelial NO synthase (eNOS)reduction through its antioxidative properties in AGEs-exposed human umbilical vein ECs(HUVECs)[55]. And endothelial dysfunction due to reduced synthesis and/or bioavailability of nitric oxide(NO)is an initial step of atherosclerotic vascular disease in diabetes[56–58]. Platelet Activation and Aggregation.There is accumulating evidence that the oxidative stress generation is involved in platelet activation and aggregation[59,60].These observa-tions suggest that the inhibition of platelet activation and aggregation may be a novel therapeutic target for preventing the development and progression of vascular complications in patients with diabetes.Further,the researchers have foundthat PEDF prevented platelet activation and aggregation in diabetic rats or AGEs-injected rats through its antioxidative properties by suppressing NADPH oxidase-driven superox-ide generation,deleterious effects of AGEs[61].The Src Pathway.PEDF inhibited AGEs-induced ROS gener-ation by increasing levels of SOD and GSH and also blocked the activation of caspase-3.Furthermore,PEDF induced cell survival via the Src pathway by Src phosphorylation at Y419, as evidenced by a pharmacological inhibitor and Src mutants [62].Phosphatidylinositol3-Kinase(PI3K)/Akt Pathway.Recent studies demonstrated that PEDF could inhibit the AGEs-BSA-induced permeability via phosphatidylinositol3-kinase (PI3K)/Akt pathway.AGEs-BSA increased the ECs perme-ability by stimulating ROS generation via NADPH oxidase activity and Akt phosphorylation at Ser473.PEDF decreased ROS generation in AGEs-BSA-exposed endothelial cells by suppressing the NADPH oxidase activity via downregu-lating the phosphorylation of p22PHOX at Thr147.This led to blockade of AGEs induction of PI3K/Akt activation in permeability.Furthermore,PEDF inhibited the AGEs-BSA-induced permeability by increased expression of tight junction protein zona occludens-1(ZO-1),coincident with an increase in barrier properties of endothelial monolayer [63].2.2.2.Inhibit Leptin-Induced Injury.PEDF was found to inhibit the leptin-induced ROS generation and upregulation of VEGF mRNA levels including any increase in DNA synthesis in microvascular ECs[64].Indeed,leptin levels in vitreous were correlated with PDR[65].2.2.3.Inhibit Tumor Necrosis Factor-α(TNF-α-)Induced Injury.The studies demonstrated that PEDF inhibited tumor necrosis factor-α(TNF-α-)induced redox-sensitive transcriptional factor NF-kappaB activation and subsequent interleukin IL-6overexpression at both mRNA and protein levels in human umbilical vein endothelial cell(HUVEC) by suppressing NADPH oxidase-mediated ROS generation [66].In addition,TNF-alpha which is initially involved in the pathogenesis of atherosclerosis[67,68]and the classic proinflammatory cytokines,downregulated PEDF mRNA levels[66].2.2.4.Inhibit Angiopoietin-II(Ang II-)Induced Injury.The researchers have found that Angiopoietin-II(Ang II)signifi-cantly induced NF-kappaB activation and subsequent MCP-1expression in HUVEC,both of which were completely inhibited by PEDF.Subsequently,PEDF inhibited Ang-II-induced upregulation of mRNA levels of p22PHOX,Nox4, and gp91PHOX/Nox2,which are membrane components of NADPH oxidase and its enzymatic activity in HUVEC[69]. Another study found that Ang II also significantly decreased PEDF mRNA levels in ECs,which was completely reversed by an Ang II type1receptor blocker,telmisartan[70].Fur-thermore,anti-PEDF Ab significantly inhibited the growth-stimulating effects of cocultured ECs on pericytes.These results demonstrated that PEDF,an EC-derived mitogen or survival factor for retinal pericytes,inhibited Ang-II-induced ECs activation by suppressing NADPH-oxidase-mediated ROS generation,and suppression by Ang II of the EC-derived PEDF may be involved in exacerbation of DR in patients with hypertension.In addition,PEDF was found to completely inhibit high-glucose-or H2O2-induced increase in a mRNA ratio of Ang II to Angiopoietin-I(Ang I)and upregulation of VEGF mRNA levels in pericytes.VEGF and angiopoietin (Ang)have been known that they were the major regulators of vascular integrity and involved in DR as well[71].2.2.5.Inhibit HOL-LDL-Induced Injury.PEDF ameliorated HOL-LDL-induced MCP-1and the subsequent NF-kappaB activation effectively.Moreover,PEDF significantly amelio-rated HOG-LDL-induced ROS generation through upregu-lation of superoxide dismutase1expression[72].This study represented a new mechanism for the salutary effect of PEDF in DR.2.2.6.Inhibit High-Glucose(HG)-Induced JAK2/STAT3Acti-vation.A recent report suggested that ACEI exerted a protective effect on DR,and this protective effect could be reflected by a decreased VEGF-to-PEDF ratio,which is a result of reduced mitochondrial ROS production itselfs caused by ACEI-induced increase of proliferator-activated receptor gamma(PPARγ)and subsequent upregulation of uncoupling protein-2(UCP-2)expression[73].Further work in vitro has demonstrated that PEDF could decrease mitochondria-derived ROS generation and subsequently downregulate VEGF expression,possibly through inhibiting HG-induced JAK2/STAT3activation[74].These studies pavea new way for future in treatment of DR.2.2.7.Regulation of PEDF Expression In Vivo.PEDF levels in aqueous humor or vitreous were associated with total antioxidant capacity in humans[38,75]and suggested that PEDF may act as an endogenous antioxidant in the eye and upregulation or substitution of PEDF may be a therapeutic target for oxidative stress-involved eye diseases,especially PDR.Retinal PEDF levels were reduced in diabetic rat,which were restored by PEDF injections.Decreased amplitudes of a-and b-wave in the ERG in diabetic rats,which were in parallel with GFAP overexpression in the M¨u ller cells,also could be blocked by PEDF injections.Further,retinal8-OHdG,p22PHOX,VEGF levels,and NADPH oxidase activity were increased,and BRB was broken in diabetic rats,both of which were ameliorated by the treatment of PEDF[26].In addition,studies with rats,intravenous administra-tion of AGEs,and simultaneous treatments with PEDF demonstrated that PEDF decreased ROS generation in AGEs-exposed endothelial cells by suppressing NADPH oxidase activity via downregulation of mRNA levels of p22PHOX and gp91PHOX and inhibited the AGEs-induced vascularhyperpermeability,the characteristic feature of early DR,by suppressing VEGF expression[76].Furthermore,the action of PEDF not only varied with the cell type but also depended on its concentration and environmental conditions[77].3.Application Prospects of PEDF inDiabetic RetinopathyLarge prospective clinical studies have shown that intensive blood glucose control reduced the incidence and progression of DR[5,48].However,strict control of hyperglycemia is often difficult to maintain and may increase the risk of severe hypoglycemia in diabetic patients.In addition, photocoagulation and vitrectomy,current conventional ther-apeutic options for the treatment of PDR,are limited by considerable side effects.Therefore,developing novel therapeutic strategies that specifically target pathogenesis of DR is desired for patients with diabetes.Based on the above role and regulation mechanism of PEDF in DR,the research on the treatment of PDR has turned to the regulation of angiogenesis inhibitors and growth factors.3.1.Current and Potential Molecular Therapie of PEDF3.1.1.PEDF and PEDF-Derived Peptide.The multifunctional PEDF,more effective than other antiangiogenic factors,is a good candidate for treatment of DR.Because a large part of endogenous PEDF-binding affinity to extracellular matrix components and cell-surface receptors,it would not achieve a protective effect.However,injection of exogenous PEDF,competitive binding of PEDF in the extracellular binding sites,will release PEDF from extracellular matrix and subsequently achieve therapeutic concentrations.The problems of current stage are as follow:(1)PEDF is a50-kDa protein,and its structural features limit practical application as pharmaceuticals;(2)underestimated the carrier itself could induce the inflammatory response;(3)currently there is no good control methods for PEDF which has secreted into the extracellular.However,many biologically active fragment of PEDF has been known,and if we canfind the active fragment,equivalent or near equivalent with PEDF,which is replaced with small peptides,we will avoid or reduce the inflammatory reaction by virus or other carriers through slow release of directly permeating sclera or intravitreal injection[78].A recent study demonstrated that an antiangiogenic peptide,PEDF-34,reduced circulating endothelial cells during ischemia-induced neovasculariza-tion[79].Thus,the PEDF-34peptide could be a superior biological therapeutic for the treatment of PDR and has great potential for large-scale pharmaceutical development.A disadvantage,however,of using small peptide derivatives is that they tend to be cleared rapidly from tissues and thus may be less effective therapeutically unless they are protected from rapid enzymatic degradation and tissue clearance.3.1.2.Biodegradable Nanospheres.Nanospheres,biocompat-ible,biodegradable,and producer of fewer side effects,is one way to avoid disadvantage of peptide.Moreover, there is abundant experimental evidence that intravitreal injections of drugs encapsulated in PLGA-poly(lactide-co-glycolide)nanospheres are both useful and effective[80,81].A recent study has found that delivering PEDF82−121,a free peptide,in PLGA nanospheres is an effective way of achieving controlled release of therapeutically active levels of the peptide[82].Such delivery systems can be manipulated to provide controlled release of physiological levels of bioactive products for both short-and long-term needs[83].3.1.3.Gene Therapy.Gene therapy involves the replacement of a faulty gene or the insertion of a new gene.Treatment of angiogenic disease can be achieved by the insertion of genes that encode antiangiogenic proteins,including the vitreous body and subretinal injection.Adenovirus and adeno-associated virus(AAV)has shown particular promise in the delivery of antiangiogenic DNA.Thefirst human trial of recombinant PEDF introduced via the adenoviral vector AdPEDF.11suggested that intravitreal delivery is relatively well tolerated with the antiangiogenic effect of PEDF per-sisting for several months[84].PEDF transgenic(PEDF-Tg) mice that ubiquitously express human PEDF driven by the β-actin promoter inhibited neovascular disorders such as DR [85].These results have provided valuable information with regards to gene therapy for the treatment of DR.4.ConclusionPEDF,a multifunctional factor,has shown to inhibit the development of DR by accumulating evidence.This paper highlights the current understanding of probable mechanism about how PEDF blocks the deterioration of DR through its antioxidative properties and application prospects of PEDF as a novel therapeutic target in DR.Gene therapy is becoming more and more acceptable and widely applied to the actual treatment.PEDF and its fragments,transferred into virus vector or made of biodegradable implant for local injection,have broad application prospects in treatment of DR.However,the drug screening and selection of the best way to enter the human body need large number of researches.AcknowledgmentsThis paper was in part supported by Grants from the Natural Science Foundation of Shanghai Jiaotong University School of Medicine,China(11XJ21056),Magnolia Sci-ence and Technology Talent Fund(MTF)of Science and Technology Commission of Shanghai Municipality,China (11BA1409700),and medical-engineering cross fund of Shanghai Jiaotong University,China(YG2011MS11).References[1]S.Resnikoff,D.Pascolini,D.Etya’ale et al.,“Global data onvisual impairment in the year2002,”Bulletin of the World Health Organization,vol.82,no.11,pp.844–851,2004.[2]J.H.Kempen,B.J.O’Colmain,M.C.Leske et al.,“Eyediseases prevalence research group.The prevalence of diabetic retinopathy among adults in the United States,”Archives of Ophthalmology,vol.122,no.4,pp.552–563,2004.[3]J.B.Saaddine,A.A.Honeycutt,K.M.V.Narayan,X.Zhang,R.Klein,and J.P.Boyle,“Projection of diabetic retinopathy and other major eye diseases among people with diabetes mellitus: United States,2005–2050,”Archives of Ophthalmology,vol.126,no.12,pp.1740–1747,2008.[4]American Diabetes Association,“Standards of medical care indiabetes—2007,”Diabetes Care,vol.30,supplement1,pp.S4–S41,2007.[5]H.Shamoon,H.Duffy,N.Fleischer et al.,“The effect ofintensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus,”New England Journal of Medicine,vol.329, no.14,pp.977–986,1993.[6]R.A.Kowluru,M.Kanwar,and A.Kennedy,“Metabolicmemory phenomenon and accumulation of peroxynitrite in retinal capillaries,”Experimental Diabesity Research,vol.2007, Article ID21976,2007.[7]P.S.Chan,M.Kanwar,and R.A.Kowluru,“Resistance ofretinal inflammatory mediators to suppress after reinstitution of good glycemic control:novel mechanism for metabolic memory,”Journal of Diabetes and its Complications,vol.24,no.1,pp.55–63,2010.[8]R.A.Kowluru,“Effect of reinstitution of good glycemiccontrol on retinal oxidative stress and nitrative stress in diabetic rats,”Diabetes,vol.52,no.3,pp.818–823,2003. [9]K.Naruse,J.Nakamura,Y.Hamada et al.,“Aldose reductaseinhibition prevents glucose-induced apoptosis in cultured bovine retinal microvascular pericytes,”Experimental Eye Research,vol.71,no.3,pp.309–315,2000.[10]P.Geraldes,J.Hiraoka-Yamamoto,M.Matsumoto et al.,“Acti-vation of PKC-and SHP-1by hyperglycemia causes vascular cell apoptosis and diabetic retinopathy,”Nature Medicine,vol.15,no.11,pp.1298–1306,2009.[11]T.C.B.Moore,J.E.Moore,Y.Kaji et al.,“The role of advancedglycation end products in retinal microvascular leukostasis,”Investigative Ophthalmology and Visual Science,vol.44,no.10, pp.4457–4464,2003.[12]C.L.B.Kline,T.L.Schrufer,L.S.Jefferson,and S.R.Kimball,“Glucosamine-induced phosphorylation of theα-subunit of eukaryotic initiation factor2is mediated by the protein kinase R-like endoplasmic-reticulum associated kinase,”International Journal of Biochemistry and Cell Biology, vol.38,no.5-6,pp.1004–1014,2006.[13]M.Brownlee,“The pathobiology of diabetic complications:aunifying mechanism,”Diabetes,vol.54,no.6,pp.1615–1625, 2005.[14]R.Marchioli,C.Schweiger,G.Levantesi,L.Tavazzi,and F.Valagussa,“Antioxidant vitamins and prevention of cardiovas-cular disease:epidemiological and clinical trial data,”Lipids, vol.36,pp.S53–S63,2001.[15]D.W.Dawson,O.V.Volpert,P.Gillis et al.,“Pigmentepithelium-derived factor:a potent inhibitor of angiogenesis,”Science,vol.285,no.5425,pp.245–248,1999.[16]J.Spranger,M.Osterhoff,M.Reimann et al.,“Loss of theantiangiogenic pigment epithelium-derived factor in patients with angiogenic eye disease,”Diabetes,vol.50,no.12,pp.2641–2645,2001.[17]J.Tombran-Tink and L.V.Johnson,“Neuronal differentiationof retinoblastoma cells induced by medium conditioned byhuman RPE cells,”Investigative Ophthalmology and Visual Science,vol.30,no.8,pp.1700–1707,1989.[18]J.Ortego,J.Escribano,S.P.Becerra,and M.Coca-Prados,“Gene expression of the neurotrophic pigment epithelium-derived factor in the human ciliary epithelium:synthesis and secretion into the aqueous humor,”Investigative Ophthalmol-ogy and Visual Science,vol.37,no.13,pp.2759–2767,1996.[19]S.P.Becerra,A.Sagasti,P.Spinella,and V.Notario,“Pigmentepithelium-derived factor behaves like a noninhibitory serpin.Neurotrophic activity does not require the serpin reactive loop,”Journal of Biological Chemistry,vol.270,no.43,pp.25992–25999,1995.[20]T.Yabe,D.Wilson,and J.P.Schwartz,“NFκB ActivationIs Required for the Neuroprotective Effects of Pigment Epithelium-derived Factor(PEDF)on Cerebellar Granule Neurons,”Journal of Biological Chemistry,vol.276,no.46,pp.43313–43319,2001.[21]H.Liu,J.G.Ren,W.L.Cooper,C.E.Hawkins,M.R.Cowan,and P.Y.Tong,“Identification of the antivasopermeability effect of pigment epithelium-derived factor and its active site,”Proceedings of the National Academy of Sciences of the United States of America,vol.101,no.17,pp.6605–6610,2004. [22]S.X.Zhang,J.J.Wang,G.Gao,C.Shao,R.Mott,and J.X.Ma,“Pigment epithelium-derived factor(PEDF)is an endogenous antiinflammatory factor,”FASEB Journal,vol.20,no.2,pp.323–325,2006.[23]M.Matsuoka,N.Ogata,T.Otsuji,T.Nishimura,K.Takahashi,and M.Matsumura,“Expression of pigment epithelium derived factor and vascular endothelial growth factor in choroidal neovascular neovascular membranes and poly-poidal choroidal vasculopathy,”British Journal of Ophthalmol-ogy,vol.88,no.6,pp.809–815,2004.[24]H.Yang and H.E.Grossniklaus,“Constitutive overexpressionof pigment epithelium-derived factor inhibition of ocular melanoma growth and metastasis,”Investigative Ophthalmol-ogy&Visual Science,vol.51,no.1,pp.28–34,2010.[25]S.I.Yamagishi,Y.Inagaki,S.Amano,T.Okamoto,M.Takeuchi,and Z.Makita,“Pigment epithelium-derived factor protects cultured retinal pericytes from advanced glycation end product-induced injury through its antioxidative prop-erties,”Biochemical and Biophysical Research Communications, vol.296,no.4,pp.877–882,2002.[26]Y.Y oshida,S.I.Yamagishi,T.Matsui et al.,“Protective roleof pigment epithelium-derived factor(PEDF)in early phase of experimental diabetic retinopathy,”Diabetes/Metabolism Research and Reviews,vol.25,no.7,pp.678–686,2009. [27]S.I.Yamagishi,Y.Inagaki,K.Nakamura et al.,“Pig-ment epithelium-derived factor inhibits TNF-α-induced interleukin-6expression in endothelial cells by suppressing NADPH oxidase-mediated reactive oxygen species genera-tion,”Journal of Molecular and Cellular Cardiology,vol.37,no.2,pp.497–506,2004.[28]K.Nakamura,S.I.Yamagishi,T.Matsui et al.,“Pigmentepithelium-derived factor inhibits neointimal hyperplasia after vascular injury by blocking NADPH oxidase-mediated reactive oxygen species generation,”American Journal of Pathology,vol.170,no.6,pp.2159–2170,2007.[29]N.Ogata,J.Tombran-Tink,M.Nishikawa et al.,“Pigmentepithelium-derived factor in the vitreous is low in diabetic retinopathy and high in rhegmatogenous retinal detachment,”American Journal of Ophthalmology,vol.132,no.3,pp.378–382,2001.[30]B.O.Boehm,ng,B.Feldmann et al.,“Proliferativediabetic retinopathy is associated with a low level of thenatural ocular anti-angiogenic agent pigment epithelium-derived factor(PEDF)in aqueous humor.A pilot study,”Hormone and Metabolic Research,vol.35,no.6,pp.382–386, 2003.[31]B.O.Boehm,ng,O.Volpert et al.,“Low content ofthe natural ocular anti-angiogenic agent pigment epithelium-derived factor(PEDF)in aqueous humor predicts progression of diabetic retinopathy,”Diabetologia,vol.46,no.3,pp.394–400,2003.[32]N.Ogata,M.Matsuoka,K.Matsuyama et al.,“Plasma con-centration of pigment epithelium-derived factor in patients with diabetic retinopathy,”Journal of Clinical Endocrinology and Metabolism,vol.92,no.3,pp.1176–1179,2007.[33]M.P.Cohen,E.Hud,E.Shea,and C.W.Shearman,“Vitreousfluid of db/db mice exhibits alterations in angiogenic and metabolic factors consistent with early diabetic retinopathy,”Ophthalmic Research,vol.40,no.1,pp.5–9,2007.[34]L.Notari,ler,A.Mart´ınez et al.,“Pigment epithelium-derived factor is a substrate for matrix metalloproteinase type 2and type9:implications for downregulation in hypoxia,”Investigative Ophthalmology and Visual Science,vol.46,no.8, pp.2736–2747,2005.[35]V.Stellmach,S. E.Crawford,W.Zhou,and N.Bouck,“Prevention of ischemia-induced retinopathy by the natural ocular antiangiogenic agent pigment epithelium-derived fac-tor,”Proceedings of the National Academy of Sciences of the United States of America,vol.98,no.5,pp.2593–2597,2001.[36]S.I.Yamagishi,T.Matsui,K.Nakamura et al.,“Pigment-epithelium-derived factor suppresses expression of receptor for advanced glycation end products in the eye of diabetic rats,”Ophthalmic Research,vol.39,no.2,pp.92–97,2007. [37]N.Katakami,H.Kaneto,Y.Yamasaki,and M.Matsuhisa,“Increased serum pigment epithelium-derived factor levels in type1diabetic patients with diabetic retinopathy,”Diabetes Research and Clinical Practice,vol.81,no.1,pp.e4–e7,2008.[38]Y.Y oshida,S.I.Yamagishi,T.Matsui et al.,“Positivecorrelation of pigment epithelium-derived factor and total antioxidant capacity in aqueous humour of patients with uveitis and proliferative diabetic retinopathy,”British Journal of Ophthalmology,vol.91,no.9,pp.1133–1134,2007. [39]J.J.Wang,S.X.Zhang,R.Mott et al.,“Salutary effect ofpigment epithelium-derived factor in diabetic nephropathy: evidence for antifibrogenic activities,”Diabetes,vol.55,no.6, pp.1678–1685,2006.[40]E.J.Duh,H.S.Yang,I.Suzuma et al.,“Pigment epithelium-derived factor suppresses ischemia-induced retinal neovascu-larization and VEGF-induced migration and growth,”Inves-tigative Ophthalmology and Visual Science,vol.43,no.3,pp.821–829,2002.[41]S.Gurunathan and E.Duh,“PEDF inhibits VEGF activationof PI3Kinase/Akt and Src in human retinal endothelial cells,”Investigative Ophthalmology and Visual Science,vol.46,2005.[42]H.Hutchings,M.Maitre-Boube,J.Tombran-Tink,and J.Plou¨e ta,“Pigment epithelium-derived factor exerts opposite effects on endothelial cells of different phenotypes,”Biochem-ical and Biophysical Research Communications,vol.294,no.4, pp.764–769,2002.[43]H.Mu,X.M.Zhang,J.J.Liu,L.Dong,and Z.L.Feng,“Effectof high glucose concentration on VEGF and PEDF expression in cultured retinal M¨u ller cells,”Molecular Biology Reports,vol.36,no.8,pp.2147–2151,2009.[44]S.I.Yamagishi,C.C.Hsu,M.Taniguchi et al.,“Receptor-mediated toxicity to pericytes of advanced glycosylation end products:a possible mechanism of pericyte loss in diabeticmicroangiopathy,”Biochemical and Biophysical Research Com-munications,vol.213,no.2,pp.681–687,1995.[45]S.I.Yamagishi,S.Amano,Y.Inagaki et al.,“Advanced gly-cation end products-induced apoptosis and overexpression of vascular endothelial growth factor in bovine retinal pericytes,”Biochemical and Biophysical Research Communications,vol.290,no.3,pp.973–978,2002.[46]S.Yamagishi,T.Matsui,and H.Inoue,“Inhibition byadvanced glycation end products(AGEs)of pigment epithelium-derived factor(PEDF)gene expression in microvascular endothelial cells,”Drugs under Experimental and Clinical Research,vol.31,no.5-6,pp.227–232,2005. [47]L.J.Mandarino,“Current hypotheses for the biochemicalbasis of diabetic retinopathy,”Diabetes Care,vol.15,no.12, pp.1892–1901,1992.[48]R.N.Frank,“On the pathogenesis of diabetic retinopathy:a1990update,”Ophthalmology,vol.98,no.5,pp.586–593, 1991.[49]S.Amano,S.I.Yamagishi,Y.Inagaki et al.,“Pigmentepithelium-derived factor inhibits oxidative stress-induced apoptosis and dysfunction of cultured retinal pericytes,”Microvascular Research,vol.69,no.1-2,pp.45–55,2005. [50]Y.Inagaki,S.Yamagishi,T.Okamoto,M.Takeuchi,andS.Amano,“Pigment epithelium-derived factor prevents advanced glycation end products-induced monocyte chemoattractant protein-1production in microvascular endothelial cells by suppressing intracellular reactive oxygen species generation,”Diabetologia,vol.46,no.2,pp.284–287, 2003.[51]Y.Mitamura,S.Takeuchi,A.Matsuda,Y.Tagawa,Y.Mizue,and J.Nishihira,“Monocyte chemotactic protein-1in the vitreous of patients with proliferative diabetic retinopathy,”Ophthalmologica,vol.215,no.6,pp.415–418,2001.[52]A.W.Stitt,“The role of advanced glycation in the pathogenesisof diabetic retinopathy,”Experimental and Molecular Pathol-ogy,vol.75,no.1,pp.95–108,2003.[53]S.I.Yamagishi,Y.Inagaki,S.Amano,T.Okamoto,M.Takeuchi,and Z.Makita,“Pigment epithelium-derived factor protects cultured retinal pericytes from advanced glycation end product-induced injury through its antioxidative prop-erties,”Biochemical and Biophysical Research Communications, vol.296,no.4,pp.877–882,2002.[54]T.Okamoto,S.I.Yamagishi,Y.Inagaki et al.,“Angiogenesisinduced by advanced glycation end products and its preven-tion by cerivastatin,”The FASEB Journal,vol.16,no.14,pp.1928–1930,2002.[55]S.I.Yamagishi,S.Ueda,T.Matsui et al.,“Pigment Epithelium-Derived Factor(PEDF)prevents Advanced Glycation End products(AGEs)-elicited endothelial Nitric Oxide Synthase (eNOS)reduction through its anti-oxidative properties,”Protein and Peptide Letters,vol.14,no.8,pp.832–835,2007.[56]V.M.Victor and M.Rocha,“Targeting antioxidants tomitochondria:a potential new therapeutic strategy for cardio-vascular diseases,”Current Pharmaceutical Design,vol.13,no.8,pp.845–863,2007.[57]I.Sudano,L.E.Spieker,F.Hermann et al.,“Protection ofendothelial function:targets for nutritional and pharmaco-logical interventions,”Journal of Cardiovascular Pharmacology, vol.47,no.2,pp.S136–S150,2006.[58]S.I.Yamagishi,K.Nakamura,T.Matsui,S.I.Ueda,and T.Imaizumi,“Role of postprandial hyperglycaemia in cardiovascular disease in diabetes,”International Journal of Clinical Practice,vol.61,no.1,pp.83–87,2007.。