Chapter13Hypersensitivity
拜谨芬(Rylaze)产品说明书

Rylaze™ (asparaginase Erwinia chrysanthemi (recombinant)-rywn) (Intramuscular)-E-Document Number: IC-0655 Last Review Date: 12/01/2022Date of Origin: 02/01/2022Dates Reviewed: 02/2022, 05/2022, 12/2022I.Length of AuthorizationCoverage will be provided for 6 months and may be renewed.II.Dosing LimitsA.Quantity Limit (max daily dose) [NDC Unit]:•Rylaze 10 mg/0.5 mL solution in a single-dose vial: 25 vials per 7 daysB.Max Units (per dose and over time) [HCPCS Unit]:•2,500 billable units (250 mg) per weekIII.Initial Approval Criteria 1Coverage is provided in the following conditions:•Patient is at least 1 month of age; ANDUniversal Criteria 1•Patient must not have a history of serious pancreatitis, thrombosis, or hemorrhagic events with prior L-asparaginase therapy; AND•Used as a component of multi-agent chemotherapy; ANDAcute Lymphoblastic Leukemia (ALL)/Lymphoblastic Lymphoma (LBL) † Ф1-3,5•Used as a substitute for E. coli-derived asparaginase (e.g., pegaspargase) in cases of hypersensitivity (e.g., systemic allergic reactions or anaphylaxis) §§ Definition of Hypersensitivity Reactions (CTCAE v5.0) 7,8Allergic Reaction−Grade 1: Systemic intervention not indicated−Grade 2: Oral intervention indicated−Grade 3: Bronchospasm; hospitalization for clinical sequelae; IV intervention indicated−Grade 4: Life-threatening consequences; urgent intervention indicated−Grade 5: DeathAnaphylaxis−Grade 1 or 2: N/A−Grade 3: Symptomatic bronchospasm, with or without urticaria; parenteral intervention indicated;allergy-related edema/angioedema; hypotension−Grade 4: Life-threatening consequences; urgent intervention indicated−Grade 5: DeathPreferred therapies and recommendations are determined by review of clinical evidence. NCCNcategory of recommendation is taken into account as a component of this review. Regimens deemedequally efficacious (i.e., those having the same NCCN categorization) are considered to betherapeutically equivalent.† FDA Approved Indication(s); ‡ Compendia recommended indication(s); Ф Orphan DrugIV.Renewal Criteria 1Coverage can be renewed based upon the following criteria:•Patient continues to meet universal and other indication-specific relevant criteria such as concomitant therapy requirements (not including prerequisite therapy), performancestatus, etc.identified in section III; AND•Disease stabilization or improvement as evidenced by a complete response [CR] (i.e., morphologic, cytogenetic or molecular complete response CR), complete hematologicresponse or a partial response by CBC, bone marrow cytogenic analysis, QPCR, or FISH;AND•Absence of unacceptable toxicity from the drug. Examples of unacceptable toxicity include:severe hypersensitivity reactions including anaphylaxis, pancreatitis, thrombosis,hemorrhage, hepatotoxicity, etc.V.Dosage/Administration 1All Indications When replacing a long-acting asparaginase product, there are two Rylaze regimens that can be used. (See table below for duration of administration as a replacement therapy).•Rylaze 25 mg/m2 administered intramuscularly every 48 hours; OR •Rylaze 25 mg/m2 administered intramuscularly on Monday and Wednesday morning, and 50 mg/m2 on Friday afternoon (Administer the Friday afternoon dose 53 to 58 hours after the Wednesday morning dose (e.g., 8:00 am on Monday and Wednesday, and 1:00 pm to 6:00 pm on Friday)RYLAZE™ -E- (asparaginase erwinia chrysanthemi recombinant-When RYLAZE is Administered: Recommended Duration ofRYLAZE to ReplaceCalaspargase Pegol ProductsRecommended Duration ofRYLAZE to ReplacePegaspargase Products25 mg/m2 intramuscular every 48 hours Replace one dose ofcalaspargase pegol productswith 11 doses of RYLAZEReplace one dose ofpegaspargase products with7 doses of RYLAZE25 mg/m2 intramuscular on Monday morning and Wednesday morning, and 50 mg/m2 intramuscular on Friday afternoon Replace one dose ofcalaspargase pegol productswith 9 doses of RYLAZEReplace one dose ofpegaspargase products with6 doses of RYLAZEVI.Billing Code/Availability InformationHCPCS Code:•J9021 – Injection, asparaginase, recombinant, (rylaze), 0.1 mg; 1 billable unit = 0.1 mgNDC(s):•Rylaze 10 mg/0.5 mL solution in a single-dose vial: 68727-0900-xxVII.References (STANDARD)1.Rylaze [package insert]. Palo Alto, CA; Jazz Pharmaceuticals, Inc.; November 2022.Accessed November 2022.2.Referenced with permission from the NCCN Drugs & Biologics Compendium (NCCNCompendium®) for Asparaginase Erwinia chrysanthemi (recombinant)-rywn. NationalComprehensive Cancer Network, 2022. The NCCN Compendium® is a derivative work ofthe NCCN Guidelines®. NATIONAL COMPREHENSIVE CANCER NETWORK®, NCCN®,and NCCN GUIDELINES® are trademarks owned by the National Comprehensive CancerNetwork, Inc. To view the most recent and complete version of the Compendium, go online to . Accessed November 2022.3.Pieters R, Hunger SP, Boos J, et al. L-asparaginase treatment in acute lymphoblasticleukemia: a focus on Erwinia asparaginase. Cancer. 2011 Jan 15; 117(2): 238–249.4.Raetz EA, Salzer WL. Tolerability and Efficacy of L-Asparaginase Therapy in PediatricPatients With Acute Lymphoblastic Leukemia, Journal of Pediatric Hematology/Oncology:October 2010 - Volume 32 - Issue 7 - p 554-563 doi: 10.1097/MPH.0b013e3181e6f0035.Maese L, Rau RE, Raetz EA, et al. A phase II/III study of JZP-458 in patients with acutelymphoblastic leukemia (ALL)/lymphoblastic lymphoma (LBL) who are hypersensitive to E.coli-derived asparaginases. DOI: 10.1200/JCO.2020.38.15_suppl.TPS7568 Journal of Clinical Oncology 38, no. 15_suppl6.Lin T, Hernandez-Illas M, Rey A, Jenkins J, et al. A Randomized Phase I Study to Evaluatethe Safety, Tolerability, and Pharmacokinetics of Recombinant Erwinia Asparaginase (JZP-RYLAZE™ -E- (asparaginase erwinia chrysanthemi recombinant-458) in Healthy Adult Volunteers. Clin Transl Sci. 2021 May;14(3):870-879. doi:10.1111/cts.12947. Epub 2021 Mar 23.7.Stock W, Douer D, DeAngelo DJ, et al. Prevention and management ofasparaginase/pegasparaginase-associated toxicities in adults and older adolescents:recommendations of an expert panel. Leuk Lymphoma 2011:52;2237-2253.mon Terminology Criteria for Adverse Events (CTCAE) v5.0. NIH National CancerInstitute: Division of Cancer Treatment & Diagnosis – Cancer Therapy Evaluation Program.Available at:https:///protocoldevelopment/electronic_applications/ctc.htm#ctc_50VIII.References (ENHANCED)1e.Referenced with permission from the NCCN Drugs & Biologics Compendium (NCCN Compendium®) for Acute Lymphoblastic Leukemia. Version 1.2022. NationalComprehensive Cancer Network, 2022. The NCCN Compendium® is a derivative work ofthe NCCN Guidelines®. NATIONAL COMPREHENSIVE CANCER NETWORK®, NCCN®,and NCCN GUIDELINES® are trademarks owned by the National Comprehensive CancerNetwork, Inc. To view the most recent and complete version of the Compendium, go onlineto . Accessed November 2022.2e.Vrooman LM, Kirov II, Dreyer ZE, et al. Activity and Toxicity of Intravenous Erwinia Asparaginase Following Allergy to E. coli-Derived Asparaginase in Children andAdolescents With Acute Lymphoblastic Leukemia. Pediatr Blood Cancer. 2016Feb;63(2):228-33. doi: 10.1002/pbc.25757. Epub 2015 Sep 16.3e.Magellan Health, Magellan Rx Management. Rylaze Clinical Literature Review Analysis.Last updated November 2022. Accessed November 2022.Appendix 1 – Covered Diagnosis CodesC83.50 Lymphoblastic (diffuse) lymphoma, unspecified siteC83.51 Lymphoblastic (diffuse) lymphoma, lymph nodes of head, face, and neckC83.52 Lymphoblastic (diffuse) lymphoma, intrathoracic lymph nodesC83.53 Lymphoblastic (diffuse) lymphoma, intra-abdominal lymph nodesC83.54 Lymphoblastic (diffuse) lymphoma, lymph nodes of axilla and upper limbC83.55 Lymphoblastic (diffuse) lymphoma, lymph nodes of inguinal region and lower limbC83.56 Lymphoblastic (diffuse) lymphoma, intrapelvic lymph nodesC83.57 Lymphoblastic (diffuse) lymphoma, spleenC83.58 Lymphoblastic (diffuse) lymphoma, lymph nodes of multiple sitesC83.59 Lymphoblastic (diffuse) lymphoma, extranodal and solid organ sitesRYLAZE™ -E- (asparaginase erwinia chrysanthemi recombinant-C91.00 Acute lymphoblastic leukemia not having achieved remissionC91.01 Acute lymphoblastic leukemia, in remissionC91.02 Acute lymphoblastic leukemia, in relapseAppendix 2 – Centers for Medicare and Medicaid Services (CMS)Medicare coverage for outpatient (Part B) drugs is outlined in the Medicare Benefit Policy Manual (Pub. 100-2), Chapter 15, §50 Drugs and Biologicals. In addition, National Coverage Determination (NCD), Local Coverage Determinations (LCDs), and Local Coverage Articles (LCAs) may exist and compliance with these policies is required where applicable. They can be found at: https:///medicare-coverage-database/search.aspx. Additional indications may be covered at the discretion of the health plan.Medicare Part B Covered Diagnosis Codes (applicable to existing NCD/LCD/LCA): N/AJurisdiction Applicable State/US Territory ContractorE (1) CA, HI, NV, AS, GU, CNMI Noridian Healthcare Solutions, LLCF (2 & 3) AK, WA, OR, ID, ND, SD, MT, WY, UT, AZ Noridian Healthcare Solutions, LLC5 KS, NE, IA, MO Wisconsin Physicians Service Insurance Corp (WPS)6 MN, WI, IL National Government Services, Inc. (NGS)H (4 & 7) LA, AR, MS, TX, OK, CO, NM Novitas Solutions, Inc.8 MI, IN Wisconsin Physicians Service Insurance Corp (WPS) N (9) FL, PR, VI First Coast Service Options, Inc.J (10) TN, GA, AL Palmetto GBA, LLCM (11) NC, SC, WV, VA (excluding below) Palmetto GBA, LLCL (12) DE, MD, PA, NJ, DC (includes Arlington &Novitas Solutions, Inc.Fairfax counties and the city of Alexandria in VA)K (13 & 14) NY, CT, MA, RI, VT, ME, NH National Government Services, Inc. (NGS)15 KY, OH CGS Administrators, LLCRYLAZE™ -E- (asparaginase erwinia chrysanthemi recombinant-。
免疫学复习资料

医学免疫学复习思考题Chapter 1 免疫学概论1.什么是免疫?免疫有什么特点?2.免疫的三大功能是什么?免疫的三大功能异常和正常各表现为什么?3.免疫应答的类型包括和。
4.简述免疫系统的组成。
Chapter 2 免疫器官和组织1.免疫器官包括哪些?各免疫器官的功能是什么?2.人的中枢免疫器官包括哪些?人的外周免疫器官包括哪些?各有何主要功能?Chapter 3 抗原1.什么是抗原(Antigen)、完全抗原、半抗原、共同抗原、异嗜性抗原、超抗原和佐剂?2.抗原的两个基本特性是什么?3.简述影响抗原免疫原性的因素。
4.什么是抗原决定簇?抗原决定簇有什么功能?5.抗原的特异性是由什么决定的?6.哪些情况下自身物质可以成为抗原?7.什么是TD-Ag和TI-Ag?两者有什么区别?8.医学上重要的同种异型抗原有和。
9.人的T细胞和B细胞丝裂原主要有哪些?11.试述超抗原与普通抗原的异同点。
Chapter 4 免疫球蛋白Immunoglobulin1.什么是Immunoglobulin?什么是Antibody?两者有什么关系?2.简述Immunoglobulin的基本结构。
3.根据将Immunoglobulin分5类,其相应的重链分别是。
4.简述Immunoglobulin的功能区及其功能。
5. IgG经木瓜蛋白酶水解后可得到和片段,经胃蛋白酶水解后可得到片段。
6. J链和分泌片各存在于什么Immunoglobulin中?各有什么功能?7.简述Immunoglobulin的功能。
8.在5类Immunoglobulin中,可通过胎盘,分子量最大,在个体发育及抗原刺激后最早产生的Immunoglobulin是,外分泌液中最多的Immunoglobulin是,介导I型超敏反应的Immunoglobulin是,亲细胞抗体是指, 初乳中含量最多的Ig是,血清中含量最多的Ig 是, 参与局部免疫的抗体是,溶血作用最强的抗体是,抗毒素抗体主要是。
2.08.10.-.Teschovirus Encephalomyelitis 猪铁士古病毒性脑脊髓炎
C H A P T E R2.8.10.T E S C H O V I R U S E N C E P H A L O M Y E L I T I S (p r e v i o u s l y e n t e r o v i r u s e n c e p h a l o m y e l i t i s o rT e s c h e n/T a l f a n d i s e a s e)SUMMARYTeschovirus encephalomyelitis was first described as a particularly virulent, highly fatalencephalomyelitis of pigs and was previously known as Teschen disease (or enterovirusencephalomyelitis). It is caused by strains of porcine teschovirus serotype 1 (PTV-1) of the genusTeschovirus, family Picornaviridae. Less severe forms of the disease were first recognised in theUnited Kingdom, where it was called Talfan disease, and in mainland Europe, where it was calledpoliomyelitis suum or benign enzootic paresis. In addition to PTV-1 strains, the milder form of thedisease can be caused by other PTV serotypes, including PTV-2, -3, -4, -5, -6, -9 and -10.The disease was first described in Teschen, Czechoslovakia in 1929. During the 1940s and 1950s itcaused serious losses in European countries and was spread to other continents. The clinicaldisease is now rare and has not been reported in Western Europe since 1980. However, there hasbeen serological evidence that virus variants, that are not pathogenic or of low pathogenicity,circulate in pig populations.Identification of the agent: The virus has affinity for the central nervous system and thereforesuspensions of brain and spinal cord from affected pigs are used as inocula for virus isolation. Thevirus propagates successfully on monolayers derived from swine tissue, in particular from kidney. IfPTV is present, it gives rise to specific cytopathic effects characterised by rounded refractile cells.For PTV identification and serotyping, suitable tests are employed using specific antisera ormonoclonal antibodies against standard strains of PTV. Virus neutralisation tests and indirectfluorescent antibody tests are preferred. Reverse-transcription polymerase chain reactionamplification of parts of the viral genome is possible, but as yet no specific tests have formally beenaccepted for diagnosis.Serological tests: Because the seroprevalence of PTV-1 may exceed 60% in healthy pigpopulations in Central Europe, and identical clinical signs may be caused by other viruses, includingother serotypes of PTV, a single serological test for PTV-1 giving positive results does not indicatethat the neurological signs observed are actually caused by a PTV-1 infection. A four-fold rise intitre together with typical signs should be considered to be an indication that PTV-1 infection causedclinical disease. For screening for specific antibodies in pig populations, it is recommended to usethe virus neutralisation test in microtitre plates or the enzyme-linked immunosorbent assay.Requirements for vaccines and diagnostic biologicals: When clinical disease was common,vaccines were available and used; however, as the disease is now rare, vaccines are no longeravailable.A. INTRODUCTIONTeschovirus encephalomyelitis (previously Teschen/Talfan diseases, and later enterovirus encephalomyelitis) is an acute condition of pigs characterised by central nervous system (CNS) disorders. Teschen is the name of the town in the Czech Republic where the disease was first recognised in 1929 (4, 5). In the 1950s, the disease spread throughout Europe and caused huge losses to the pig breeding industry. Less severe forms of the disease were first recognised in the United Kingdom, where it was called Talfan disease, and in Denmark, where it was called poliomyelitis suum; these were benign enzootics of swine. Teschovirus encephalomyelitis has not been reported in Western Europe since 1980 (Austria) and the disease is now considered rare. In the last 12 years (since 1996) disease was reported to the OIE by the following countries: Belarus (1996, 1999 and 2005), Japan (2002), Latvia (1997 and 2000–2002), Madagascar (1996–2000, 2002 and 2004–2005), Moldavia (2002–2004),Romania (2002), Russia (2004), Uganda (2001) and Ukraine (1996–2005). In most of these cases it is not known if diagnosis was made purely on clinical grounds or in conjunction with laboratory tests; the exception being in Japan in 2002 (17).The causal agent of teschovirus encephalomyelitis is porcine teschovirus serotype 1 (PTV-1), which belongs to the species Porcine teschovirus, genus Teschovirus, family Picornaviridae (2, 5). Originally the PTVs were classified within the genus Enterovirus and the original 11 porcine enterovirus (PEV) serotypes, PEV-1 to PEV-11, were placed in three groups – I, II and III – on the basis of cytopathic effect (CPE) produced, serological assays and replication in different cell cultures (7). PEV-1 to PEV-7 and PEV-11 to PEV-13 were identified as group I. Based on nucleotide sequencing and phylogenetic analysis, the PEV group I viruses have now been placed in the genus Teschovirus. PEV-1 to -7 have been renamed PTV-1 to -7 and PEV-11 to -13 were renamed PTV-8 to 10; an additional serotype, PTV-11, has also recently been described (8, 14). PEV group II contains PEV-8 (species Porcine enterovirus A) and group III consists of PEV-9 and PEV-10 (species Porcine enterovirus B). These two groups currently belong to the genus Enterovirus (14, 18), although it has been suggested that PEV-8 may be reclassified in another new picornavirus genus (8).PTV-2, -3, -4, -5, -6, -9 and -10 have been isolated from pigs with milder forms of the disease (16). PTV infections often do not produce clinical signs. Serotypes may be differentiated using a virus neutralisation (VN) test (2, 7), complement fixation test (6) or indirect fluorescent antibody (IFA) test (1, 13).PTV infections only occur in swine; other animal species are not known to be susceptible.Differential diagnoses include pseudorabies (Aujeszky’s disease) and classical swine fever (acute form). In addition, Japanese encephalitis, Streptococcus suis and haemagglutinating encephalomyelitis may occasionally produce similar clinical signs. Non-infectious aetiologies, in particular toxicities, must also be considered.PTV may be identified serologically using standard antisera that have been prepared by hyperimmunisation of guinea-pigs, rabbits, or colostrum-deprived piglets with standard strains of PTV serotypes 1–11.The virus enters the animal via the oral or nasal cavity. The incubation period is about 14 days. The main signs of the prodromal stage are fever up to 41.5°C, lassitude, anorexia and locomotor disturbances. This stage is followed by hypersensitivity, tremors, clonic spasms of the legs, flaccid paralysis, opisthotonos and nystagmus; convulsions may be observed in young pigs. In the final clinical stage, paralysis proceeding from the hind part through the loins to the fore part of the body is observed. Paralysis of the thermoregulatory centre results in hypothermy. When respiratory muscles are paralysed, the animal dies of suffocation.Laboratory diagnosis of the disease is based on typical clinical signs plus histological lesions of the brain and spinal cord, identification of the virus in the CNS of affected pigs, and on the detection of specific antibodies in the blood of convalescent animals.B. DIAGNOSTIC TECHNIQUES1. Histological examination and immunohistochemistryFor histological diagnosis, samples of cerebrum, cerebellum, diencephalon, medulla oblongata and cervical and lumbar spinal cord are collected. The samples are fixed in formaldehyde and sections are stained using conventional histological methods. The virus multiplies in the CNS causing a nonsuppurative polio-encephalomyelitis with lymphocytic perivasculr cuffs, especially in the spinal cord (4). Pathological changes are observed in the grey matter of the diencephalon, cerebellum, medulla oblongata and in the ventral horns of the spinal cord, consistently including dorsal root ganglia and trigeminal ganglia (ganglioneurites) and to a lesser extent in the cerebral hemispheres. Lesions may involve the dorsal horns of the spinal cord in very young animals. Degeneration of neurons (swelling, chromatolysis, necrosis, neuronophagia, axonal degeneration) and their replacement by microgliosis (astrobytosis, astrogliosis) develops in the late stage of the disease.Detection of teschovirus antigens by immunohistochemistry on fixed, paraffin-embedded CNS sections is very difficult and not consistently possible. If suitable specific antisera or monoclonal antibodies are available, as well as specific detection techniques, correlation of pathological changes with the location of the agent may be possible on fixed, paraffin-embedded sections of the CNS.2. Identification of the agenta) Isolation of the virusProgress in diagnosis of teschovirus encephalomyelitis and vaccine production has been made possible by the propagation of virus in cell culture (9, 11).Samples of brain and spinal cord are collected from pigs slaughtered at an early clinical stage of the disease.When not processed immediately, the samples should be placed in a solution prepared from equal parts of phosphate buffered isotonic saline solution (PBS), pH 7.4, and glycerol. Pieces of tissue are minced to prepare a 10% (w/v) suspension in PBS. The suspension is centrifuged at 800 g for 10 minutes and the supernatant fluid is used for inoculation of cell cultures. Monolayer cultures of primary porcine kidney or established cell lines derived from porcine tissue are suitable for isolation of PTV.o Testproce d urei) Test tubes or tissue culture vessels with monolayer cell cultures are used. Growth medium is discardedand tubes or vessels are inoculated with 0.1 ml of suspect tissue homogenate.ii) Inoculated test tubes are placed on a roller drum or tissue culture vessels are placed on a tray and incubated for 1 hour at 37°C.iii) The inoculum is discarded; the tubes or tissue culture vessels are washed with PBS and replenished with 1–20 ml (depending on the type of tissue culture vessel used) of maintenance medium without calfserum.iv) The tubes are examined microscopically each day. If the sample contains PTV, characteristic CPE will be seen after 3–4 days. The CPE is characterised by small foci of rounded refractile cells. After severalpassages the virus grows better and produces complete CPE. The identity of PTV can be confirmed bythe use of specific antiserum or monoclonal antibodies. The VN or the IFA test is best suited to thispurpose. Once an isolate has been identified serologically as PTV, piglet inoculation is the only certainmeans of determining that the given isolate is pathogenic.b) Virus neutralisation test for porcine teschovirus identificationThe virus harvested from cell cultures is diluted in cell culture maintenance medium over the range 10–1 to 10–6 in tenfold steps. For teschovirus serotyping, 12 rows of each dilution are prepared; 50 µl of standard antisera to PTV-1–11 diluted 1/10 is added to rows 1–11 and 50 µl of negative serum is added to the last row. Mixtures are incubated overnight at 4°C or for 1 hour at 37°C and thereafter inoculated into roller tube cultures or into wells of microtitration plates with confluent monolayer cell cultures. The inoculated cell cultures are incubated at 37°C. Assessment is carried out 72 hours later and every following day up to day 10, depending on when the CPE is seen. The identification of a PTV serotype is confirmed if the titre of the isolated virus in the presence of that antiserum is at least 103 lower than that virus incubated with negative serum.c) Ind irect fluorescent antibod y test for the confirmation of porcineteschovirus antigen in cellsThe IFA test is based on the reaction of the antigens in infected cells with specific antibodies in positive serum (13). The reaction is visualised by a fluorescein isothiocyanate (FITC)-conjugated antiglobulin, using a microscope with a UV or a blue light source. The antigen is detectable in cells 12 hours after the infection with PTV, i.e. before the development of CPE. Polyclonal antisera often show cross-reactivity with different PTV types, which can confuse the interpretation of results.proce d ureo Testi) Monolayers of porcine kidney cells on cover-slips are inoculated with the suspected material. Positiveand negative controls should be processed in parallel with the test specimens.ii) After incubation for 12–16 hours, the cover-slips are removed, washed twice in PBS, air-dried and fixed in cold acetone for 5–15 minutes.iii) The cover-slips are placed into a wet box and flooded with rabbit or pig hyperimmune anti-PTV serum optimally diluted 1/10 with PBS or with PTV-specific monoclonal antibody at working dilution.iv) The wet box is closed and incubated at 37°C for 60 minutes.v) The cover-slips are removed and washed three times in PBS, then flooded with FITC-conjugated anti-rabbit or anti-pig goat serum, at a previously assessed working dilution, and incubated at 37°C for30 minutes.vi) The cover-slips are then washed three times with PBS, air-dried and mounted in 0.1 M Tris-buffered glycerol, pH 8.6.After processing, the cover-slips are examined microscopically. The control slides are examined first to confirm that the fluorescence observed is specific. The fluorescence is apple green in colour and occurs in the cell cytoplasm and at the periphery of the nucleus. Instead of cover-slips, multispot slides or multiwell plates can also be used.d) Reverse-transcription polymerase chain reactionThe reverse-transcription polymerase chain reaction (RT-PCR) provides a method for detection and differentiation of specific gene regions of porcine teschoviruses (12, 19). The nested RT-PCR with specific primer sets has been used to differentiate between PTVs and PEVs (19). PCR is more rapid and less laborious than virus isolation by tissue culture technique and serotyping. However, the PCR technique is currently restricted to specialised laboratories.3. Serological testsBecause the seroprevalence of PTV-1 may exceed 60% in healthy pig populations in some countries of Central Europe, and identical clinical signs may be caused by other viruses – including other serotypes of PTV – a single serological test for PTV-1 giving positive results does not indicate that neurological signs observed are actually caused by PTV-1. A four-fold rise in titre together with typical signs should be considered to be an indication that PTV-1 infection caused clinical disease. Another reason that paired serum samples are needed for confirmation of the significance of titres is that cross-reactions have been reported with orphan teschoviruses.Pigs that have recovered from disease, or those with inapparent disease, produce specific antibodies. Several serological methods are available for their detection, of which the microtitre VN test using pig kidney cell cultures is the most useful (10). An ELISA has been developed that is more sensitive and rapid (3).For serological diagnosis it is necessary to have standard strains of PTV serotypes propagated in cell cultures and hyperimmune serum monospecific for PTV types.o Standard strains of porcine teschovirusesCharacteristics: Following long experience, the strain ‘Zabreh’, isolated in Czechoslovakia during the period of peak incidence of the disease, was selected as the standard strain to generate the severe form of teschovirus encephalomyelitis. The pathogenicity of the strain is maintained by intracerebral passages in healthy, colostrum-deprived piglets. The virus produces typical signs of teschovirus encephalomyelitis after an incubation period of 5–7 days. For serological diagnosis, the following strains of PTV serotypes should be used as standard strains: type 1: Talfan, type 2: T80, type 3: O2b, type 4: PS36, type 5: F26, type 6: PS37, type 7: F43, type 8: UKG/173/74, type 9: Ger-2899/84, type 10: Ger-460/88, type 11: Dresden.Stock virus: Standard strains are propagated on monolayers of cell culture either from primary porcine kidney or testes or on an established cell line, for example PK-15. A 10% suspension in PBS, pH 7.4, is prepared from the brain and spinal cord of piglets infected experimentally with PTV. Some types are isolated from faeces. The suspension is centrifuged and the supernatant is used for the inoculation of cell cultures. The procedure for the cultivation of PTV in cell cultures is as follows:The growth medium is removed from the cell culture and after rinsing with buffered saline, cells are inoculated with the virus suspension at 37°C. The size of the inoculum should be equal to 10% of the growth medium. After 1 hour of incubation at 37°C, the inoculum is decanted, the culture vessel is rinsed with buffered saline, and the cells are overlayed with the appropriate volume of serum-free medium supplemented with antibiotics. CPE is apparent within 48 hours, and the monolayer disintegrates more or less completely during the next 48–72 hours. In the subsequent three to five passages in cell culture, the development of the CPE accelerates and the concentration of virions increases. Titration of the virus is performed in tube cultures or on microtitre plates. A cell-adapted strain usually reaches TCID50 (50% tissue culture infective dose) titres of 106–107 per ml.The fluid harvest is checked for specificity using known specific hyperimmune antiserum. Treatment with 5% chloroform and cultivation in human and bovine cell cultures and chicken embryos is used to exclude contamination with other viruses. PTV is chloroform resistant and multiplies only in cultures of swine origin. Immunofluorescent antibody staining is useful to detect possible contaminants that are also chloroform resistant and propagate on cells of swine origin (e.g. parvovirus), or that are non-cytopathic. The stock virus should be dispensed into small aliquots and preserved at –60°C. Frozen virus retains its properties for several years. For stock virus that is to be used in the neutralisation test, a constant dose of 100 TCID50 is recommended.o Specific hyperimmune serumSpecific hyperimmune serum is obtained by repeated immunisation of guinea-pigs, rabbits or colostrum-deprived piglets with PTV. Although the animals are selected from specific pathogen free breeds, they are nonetheless tested before immunisation for absence of antibodies against PTV. The standard strains should be used. Rabbitsare immunised either intravenously, using virus suspension alone, or subcutaneously or intraperitoneally, using the virus suspension with 10% oil adjuvant. Good results may be obtained by administering three doses of 2 ml of virus suspension plus 0.2 ml oil adjuvant, at intervals of 2 weeks. The rabbits are bled 10 days after the last immunisation. Piglets are immunised in the same way. The harvested sera are clarified by centrifugation and stored in small aliquots at –20°C. The sera are titrated using a neutralisation test and constant antigen. Only sera with an antibody titre of at least 1/256 can be used for the identification of the virus.a) Virus neutralisation test in microtitre platesThe test is performed in flat-bottomed cell culture microtitre plates, using low passage porcine kidney or testes cells or cell lines derived from porcine cells. Stock virus is grown in cell monolayers. The virus harvested from cell cultures is clarified by centrifugation and stored in aliquots at –20°C. Culture medium, such as Eagle’s complete medium or LYH (Hanks balanced salt solution with yeast extract, lactalbumin and antibiotics), is used as diluent. The virus harvested from cell cultures is clarified by centrifugation and stored in aliquots at –70°C or as 50/50 mixture with glycerol and can be stored at –20°C.proce d ureo Testi) Inactivate swine sera for 30 minutes at 56°C.ii) The sera to be tested are diluted in cell culture medium in twofold steps from 1/2 to 1/64, four wells per dilution and 50 µl volumes per well.iii) Controls include positive and negative sera, cells and medium control.iv) Add to each well 50 µl of virus stock previously diluted in culture medium to provide 100 TCID50.v) Incubate for 1 hour at 37°C with the plates covered. The residual virus stock is also incubated.vi) Make back titrations of the residual virus stock in four tenfold dilution steps using 50 µl per well and four wells per dilution.vii) Add 50 µl of porcine kidney cell suspension at 5 × 105 cells per ml.viii) After further shaking, lids are put on and the plates are incubated at 37°C in a 5% CO2 atmosphere for 2–3 days or longer, to a maximum of 8 days.ix) Examine the plates microscopically for CPE. The test should be validated by checking the back titration of virus and titration of positive control serum. Virus should give a value of 100 TCID50 with a permissible range of 30–300. The standard positive serum should give a titre within 0.3 log10 units fromits predetermined mean. A negative serum should give no neutralisation at the lowest dilution tested,i.e. 1/2.x) The VN results are determined by the Spearman–Kärber method as the dilution of serum that neutralised the virus in 50% of the wells.xi) Virus neutralisation titres are regarded as positive if the corresponding serum neutralises the virus at an initial serum dilution of 1/8 or higher.b) Enzyme-linked immunosorbent assayAn alternative method for the detection and titration of specific antibodies against PTV is the ELISA technique (3). The test is performed in microtitre plates using PTV grown on cell cultures as antigen. The technique can be carried out using the following steps.preparationo Antigeni) Virus is propagated on monolayers of cell culture either from primary porcine kidney or testes or on anestablished cell line, for example PK-15. The growth medium is removed from the cell culture and afterrinsing with buffered saline, cells are inoculated with virus suspension at a low multiplicity of infection.After 30 min of incubation at 37°C, cells are overlayed with the appropriate volume of serum-free medium supplemented with antibiotics. Incubation at 37°C is continued with daily microscopic observations. CPE should be apparent within 48 hours, and the monolayer disintegrates more or less completely during the next 48–72 hours. A cell-adapted strain usually reaches TCID50 (50% tissue culture infective dose) titres of 106–107 per ml.ii) The harvested virus is clarified by centrifugation at 200 g for 15 minutes, and then precipitated with a final 50% saturated (NH4)2SO4 for 120 minutes at 4°C.iii) After centrifugation at 2000 g, the resulting precipitate is suspended in TEN buffer (Tris-hydroxymethyl-methylamine [0.01 M], ethylene diamine tetra-acetic acid [1 mM] and NaCl [0.15 M]), pH 7.4, to 1/100 of the initial volume.iv) The concentrated viral suspension is extracted by shaking with freon 3/1 for 10 minutes at 4°C.v) Following further centrifugation, the supernatant is divided into two separate phases. The upper aqueous phase, containing the viral antigen, is desalinated by passage through a 2.5 × 40 cm cylinderpacked with sephadex G 25.vi) The viral solution is finally concentrated by ultracentrifugation at 160,000 g for 3 hours.vii) The pellet is suspended in TEN buffer, pH 7.4, in approximately 1000th the initial volume of virus.viii) Insoluble proteins are separated by light centrifugation, and the supernatant is used as the positive antigen in the ELISA.proce d ureo Testi) Plates are sensitised with pre-diluted antigen in phosphate buffered saline (PBS), pH 7.2, by adding100 µl to each well. The adsorption of antigen to the surface of the plate takes place overnight at 4°C.Parallel rows of the plate should be treated with negative antigen.ii) The plate is washed five times in PBS to remove excess antigen.iii) Test sera are diluted 1/20 with PBST (PBS solution containing 0.05% Tween 20). 50 µl of the diluted sera is placed into each of two wells with positive antigen and into two wells with negative antigen.(Negative antigen is prepared as described above except that the tissue culture is not inoculated withvirus and cells are disrupted by freezing.) The plate is incubated for 1 hour at 37°C.iv) The plates are washed five times with PBST.v) A predetermined dilution of horseradish peroxidase conjugated with anti-swine immunoglobulin prepared in rabbits is added in 50 µl quantities to each well. The plates are further incubated for afurther 1 hour at room temperature.vi) The plates are washed five times in PBS.vii) Substrate solution (0.1% ortho-phenylendiamine with 0.03% hydrogen peroxide in PBS, pH 6.0) is added in 100 µl quantities to each well.viii) After the addition of substrate, positive samples change colour to dark brown. When a sufficient degree of colour reaction is seen in the wells of known positive sera, the reaction is stopped by addition of50 µl of 2 M sulphuric acid to each well. The absorbance of the wells is measured at a wavelength of492 nm, preferably using an automatic multi-channel spectrophotometer with print-out mechanism.Positive and negative sera and non-infected cells should be processed as controls in parallel with thetest specimens.ix) The absorbance of a serum is the mean reading of two wells with positive antigen minus the mean reading of two wells with negative antigen. Absorbance readings of test sera that exceed by more thantwofold the mean reading of standard negative sera are regarded as positive.C. REQUIREMENTS FOR VACCINES AND DIAGNOSTIC BIOLOGICALSo Vaccines against teschovirus encephalomyelitisDuring the period of highest incidence of the disease in central Europe and Madagascar, active immunoprophylaxis was an important means for the control of this infection (15). As severe clinical disease has disappeared, vaccination has been discontinued and the vaccine is no longer being produced or used anywhere in the world.REFERENCES1. A UERBACH J.,P RAGER D.,N EUHAUS S.,L OSS U.&W ITTE K.H. (1994). Grouping of porcine enteroviruses byindirect immunofluorescence and description of new serotypes. J. Vet. Med. [B], 41, 277–282.2. B ETTS A.O. (1960). Studies on enteroviruses of the pig. VI. The relationship of the T 80 strain of a swinepolioencephalomyelitis virus to some other viruses as shown by neutralization tests in tissue cultures. Res.Vet. Sci., 1, 296–300.3. H UBSCHLE O.J.B.,R AJOANARISON J.,K OKO M.,R AKOTONDRAMARY E.&R ASOLFOMANANA P. (1983). ELISA fordetection of Teschen virus antibodies in swine serum samples. Dtsch Tierarztl. Wochenschr., 90, 86–88.4. K LOBOUK A. (1931). Encephalomyelitis enzootica suum. Zverolekarsky obzor, 24, 436–480.5. K LOBOUK A. (1933). Aetiology of the so-called Teschen disease – Encephalomyelitis enzootica suum.Zverolekarske rozpravy, 8, 85–96.6. K NOWLES N.J.&B UCKLEY L.S. (1980). Differentiation of porcine enterovirus sertoypes by complement fixation.Res. Vet. Sci., 29, 113–115.7. K NOWLES N.J.,B UCKLEY L.S.&P EREIRA H.G. (1979). Classification of porcine enteroviruses by antigenicanalysis and cytopathic effects in tissue culture: description of 3 new serotypes. Arch. Virol.,62, 201–208.8. K RUMBHOLZ A.,D AUBER M.,H ENKE A.,B IRCH-H IRSCHFELD E.,K NOWLES N.J.,S TELZNER A.&Z ELL R. (2002).Sequencing of porcine enterovirus groups II and III reveals unique features of both virus groups. J. Virol., 76, 5813–5821.9. M ADR V. (1959). Propagation of the Teschen disease virus in cell cultures. Veterinarstvi, IX, 298–301.10. M AYR A.&B IBRACK B. (1971). Demonstration of Teschen Talfan infection using a micromodification ofneutralization test. Zentralbl. Veterinarmed. [B], 18, 657–664.11. M AYR A.&S CHWOEBEL W. (1957). Propagation of the Teschen disease virus in porcine kidney cell culturesand properties of the cultured virus. 1.2.3. part. Zentralbl. Bakteriol. [I. Orig.], 168, 329–359.12. P ALMQUIST J.,M UNIR S.,T AKU A.,K APUR V.&G OYAL S.M. (2002). Detection of porcine teschovirus andenterovirus type II by reverse transcription-polymerase chain reaction. J. Vet. Diagn. Invest., 14, 476–480. 13. R OMANENKO V.F.,P RUSS O.G.,B ELYI Y U.A.&K UPNOVSKAYA L.V. (1982). Immunofluorescent diagnosis ofporcine encephalomyelitis. Veterinariia, 4, 69–72.14. S TANWAY G.,B ROWN F.,C HRISTIAN P.,H OVI T.,H YYPIÄ T.,K ING A.M.Q.,K NOWLES N.J.,L EMON S.M.,M INORP.D.,P ALLANSCH M.A.,P ALMENBERG A.C.&S KERN T. (2005). Family Picornaviridae. In: Virus Taxonomy.Eighth Report of the International Committee on Taxonomy of Viruses, Fauquet C.M., Mayo M.A., Maniloff J., Desselberger U. & Ball L.A., eds. Elsevier/Academic Press, London, UK, 757–778.15. T RAUB E. (1942). Active immunization against Teschen disease using vaccines adsorbed on aluminiumhydroxide. Arch. Tierheilkd, 77, 52–66.16. W ITTE VON K.H.,A UERBACH J.,L OSS K.U.,N EUHAUS S.&P RAGER D. (1994). Typisierung von 17 porzinenEnterovirusisolaten aus Polioenzephalomyelitisfällen der Jahre 1983–1991. DTW Dtsch. Tierarztl.Wochenschr., 101, 453–492.17. Y AMADA M.,K OZAKURA R.,I KEGAMI R.,N AKAMURA K.,K AKU Y.,Y OSHII M.&H ARITANI M. (2004). Enterovirusencephalomyelitis in pigs in Japan caused by porcine teschovirus. Vet. Rec.,155, 304–306.18. Z ELL R.,D AUBER M.,K RUMBHOLZ A.,H ENKE A.,B IRCH-H IRSCHFELD E.,S TELZNER A.,P RAGER D.&W URM R.(2001). Porcine teschoviruses comprise at least eleven distinct serotypes: molecular and evolutionary aspects. J. Virol., 75, 1620–1631.19. Z ELL R.,K RUMBHOLZ A.,H ENKE A.,B IRCH-H IRSCHFELD E.,S TELZNER A.,D OHERTY M.,H OEY E.,D AUBER M.,P RAGER D.&W URM R. (2000). Detection of porcine enteroviruses by nRT-PCR: differentiation of CPE groups I–III with specific primer sets. J. Virol. Methods, 88, 205–218.** *。
Chapter18 Hypersensitivity
• Patients with type I hypersensitivity Very high ( to 1000 μg/ml) hereditary background:IL-4 ,DRB1*1501 Bind to FcRI on
Mast cells, basophils
(III) Mast cells, basophils
IV. Common diseases caused by type I hypersensitivity
• Systemic allergy: anaphylactic shock-----drug, serum • Hypersensitivity reaction in respiratory tract allergic rhinitis, allergic asthma
Allergen: Any antigen that induces type I hypersensitivity, including plants, drugs, foods, insects, and animals. Common allergens associated with type I hypersensitivity
early phase reaction : occurs within minutes , mainly caused by histamine,PGD constriction of smooth muscle, vascular permeability. late phase reaction : occurs within hours, caused by the induced synthesis and release of mediators including LT, PAF.
研究生公共英语教材阅读B第3、4、10、11、14课文原文及翻译
Unite 3 Doctor’s Dilemma: Treat or Let Die?Abigail Trafford1. Medical advances in wonder drugs, daring surgical procedures, radiation therapies, and intensive-care units have brought new life to thousands of people. Yet to many of them, modern medicine has become a double-edged sword.2. Doctor’s power to treat with an array of space-age techniques has outstripped the body’s capacity to heal. More medical problems can be treated, but for many patients, there is little hope of recovery. Even the fundamental distinction between life and death has been blurred.3. Many Americans are caught in medical limbo, as was the South Korean boxer Duk Koo Kim, who was kept alive by artificial means after he had been knocked unconscious in a fight and his brain ceased to function. With the permission of his family, doctors in Las Vegas disconnected the life-support machines and death quickly followed.4. In the wake of technology’s advances in medicine, a heated debate is taking place in hospitals and nursing homes across the country --- over whether survival or quality of life is the paramount goal of medicine.5. “It gets down to what medicine is all about, ” says Daniel Callahan, director of the Institute of Society, Ethics, and the Life Sciences in Hastings-on-Hudson, New York. “Is it really to save a life? Or is the larger goal the welfare of the patient?”6. Doctors, patients, relatives, and often the courts are being forced to make hard choices in medicine. Most often it is at the two extremes of life that these difficultyethical questions arise --- at the beginning for the very sick newborn and at the end for the dying patient.7. The dilemma posed by modern medical technology has created the growing new discipline or bioethics. Many of the country’s 127 medical s chools now offer courses in medical ethics, a field virtually ignored only a decade ago. Many hospitals have chaplains, philosophers, psychiatrists, and social workers on the staff to help patients make crucial decisions, and one in twenty institutions has a special ethics committee to resolve difficult cases.Death and Dying8. Of all the patients in intensive-care units who are at risk of dying, some 20 percent present difficult ethical choices --- whether to keep trying to save the life or to pull back and let the patient die. In many units, decisions regarding life-sustaining care are made about three times a week.9. Even the definition of death has been changed. Now that the heart-lung machine can take over the functions of breathing and pumping blood, death no longer always comes with the patient’s “last gasp” or when the heart stops beating. Thirty-one states and the District of Columbia have passed brain-death statutes that identify death as when the whole brain ceases to function.10. More than a do zen states recognize “living wills” in which the patients leave instructions to doctors not to prolong life by feeding them intravenously or by other methods if their illness becomes hopeless. A survey of California doctors showed that 20 to 30 percent were following instructions of such wills. Meanwhile, the hospicemovement, which its emphasis on providing comfort --- not cure --- to the dying patient, has gained momentum in many areas.11. Despite progress in society’s understanding of death and dying, t heory issues remain. Example: A woman, 87, afflicted by the nervous-system disorder of Parkinson’s disease, has a massive stroke and is found unconscious by her family. Their choices are to put her in a nursing home until she dies or to send her to a medical center for diagnosis and possible treatment. The family opts for a teaching hospital in New York city. Tests show the woman’s stroke resulted from a blood clot that is curable with surgery. After the operation, she says to her family: “Why did you bring me back to this agony?” Her health continues to worsen, and two years later she dies.12. On the other hand, doctors say prognosis is often uncertain and that patients, just because they are old and disabled, should not be denied life-saving therapy. Ethicists also fear that under the guise of medical decision not to treat certain patients, death may become too easy, pushing the country toward the acceptance of euthanasia.13. For some people, the agony of watching high-technology dying is too great. Earlier this year, Woodrow Wilson Collums, a retired dairyman from Poteet, Texas, was put on probation for the mercy killing of his older brother Jim, who lay hopeless in his bed at a nursing home, a victim of severe senility resul ting from Alzheimer’s disease. After the killing, the victim’s widow said: “I think God, Jim’s out of his misery. I hate to think it had to be done the way it was done, but I understand it. ”Crisis in Newborn Care14. At the other end of the life span, technology has so revolutionized newborn carethat it is no longer clear when human life is viable outside the womb. Newborn care has got huge progress, so it is absolutely clear that human being can survive independently outside the womb. Twenty-five years ago, infants weighting less than three and one-half pounds rarely survived. The current survival rate is 70 percent, and doctors are “salvaging” some babies that weigh only one and one-half pounds. Tremendous progress has been made in treating birth deformities such as spina bifida. Just ten years ago, only 5 percent of infants with transposition of the great arteries --- the congenital heart defect most commonly found in newborns --- survived. Today, 50 percent live.15. Yet, for many infants who owe their lives to new medical advances, survival has come at a price. A significant number emerge with permanent physical and mental handicaps.16. “The question of treatment and nontreatment of seriously ill newborns is not a single one,”says Thomas Murray of the Hastings Center. “But I feel strongly that retardation or the fact that someone is going to be less than perfect is not good grounds for allowing an infant to die.”17. For many parents, however, the experience of having a sick newborn becomes a lingering nightmare. Two years ago, an Atlanta mother gave birth to a baby suffering from Down’s Syndrome, a form of mental retardation; the child also had blocked intestines. The doctors rejected the parents’ plea not to operate, and today the child, severely retarded, still suffers intestinal problems.18. “Every time Melanie has a bowel movement, she cries,” explains her mother.“She’s not able to take care of herself, and we won’t live forever. I wanted to save her from sorrow, pain, and suffering. I don’t understand the emphasis on life at all costs, and I’m very angry at the doctors and the hospital. Who will take care of Melanie after we’re gone? Where will you doctors be then?”Changing Standards19. The choices posed by modern technology have profoundly changed the practice of medicine. Until now, most doctors have been activists, trained to use all the tools in their medical arsenals to treat disease. The current trend is toward nontreatment as doctors grapple with questions not just of who should get care but when to take therapy away.20. Always in the background is the threat of legal action. In August, two California doctors were charged with murdering a comatose patient by allegedly disconnecting the respirator and cutting off food and water. In 1981, a Massachusetts nurse was charged with murdering a cancer patient with massive doses of morphine but was subsequently acquitted.21. Between lawsuits, government regulations, and patients’ rights, many doctors feel they are under siege. Modern technology actually has limited their ability to make choices. More recently, these actions are resolved by committees.Public Policy22. In recent years, the debate on medical ethics has moved to the level of national policy. “It’s just beginning to hit us that we don’t have unlimited resources,” says Washington Hospital Center’s Dr. Lynch. “You can’t talk about ethics without talkingethics without talking about money.”23. Since 1972. Americans have enjoyed unlimited access to a taxpayer-supported, kidney dialysis program that offers life-prolonging therapy to all patients with kidney failure. To a number of police analysts, the program has grown out of control --- to a $1.4billion operation supporting 61,000 patients. The majority are over 50, and about a quarter have other illness, such as cancer or heart disease, conditions that could exclude them from dialysis in other countries.24. Some hospitals are pulling back from certain lifesaving treatment. Massachusetts General Hospital, for example, has decided not perform heart transplants on the ground that the high costs of providing such surgery help too few patients. Burn units --- through extremely effective --- also provide very expensive therapy for very few patients.25. As medical scientists push back the frontiers of therapy, the moral dilemma will continue to grow for doctors and patients alike, making the choice of to treat the basic question in modern medicine.1. 在特效药、风险性手术进程、放疗法以及特护病房方面的医学进展已为数千人带来新生。
五年制《医学免疫学》17.hypersensitivity (2)
Type I hypersensitivity
(immediate hypersensitivity)
Allergy(变态反应) Anaphylaxis(过敏反应)
Richet和Porteir提出了过敏反应的概念, 二人因此获1913年诺贝尔奖。
初次注射 海葵毒素
导致狗死亡
再次注射 海葵毒素
Anaphylaxis
Chapter 17
Hypersensitivity (超敏反应)
下载PPT
/qingqingwang 左下角链接:课件下载-2014-进入“2014冬ivity
Some immune responses can give rise to an excessive or inappropriate reaction, resulting in significant tissue damage or even death.
The classification: type I~IV
I型 ---- 速发型 (IgE) II型 ---- 细胞毒型(IgG,IgM) III型 ---- 免疫复合物型(IgG) IV型 ---- 迟发型(TDTH) ----------------------------------------------
1. Characteristics of Type I hypersensitivity
1. Rapid: react and disappear quickly on re-exposure to Ag
2. Dysfunction: dysfunction rather than severe tissue and cell damage occurs
Allergin is a specific IgE that gives rise to immediate hypersensitivity.
hypersensitivityDetection免疫学超敏反应
2.IC type:
Medicine (Hapten) + tissue pro → Ab →medicine again → Hapten + Ab →IC → C3b, Fc →RBC, Platelet, neutrophil
Allergic Individual过敏体质
(1) IgE↑ (2) Ach↑ (3) Th2 ↑ (4) SIgA↓ (5) C1INH ↓ (C2a ↑)
(iii) IgE-FceR+ cells
mast cell, basophil
1) Distribution: mast cell: skin and basophil: blood.
Skin tests with different allergens
2.IgE detection
V Prevention&treatment of Hypersensitivity
(i) Prevention
Identify the offending allergen,
avoid contact if possible! (找出变
2) Xenogenic serum异种动物血清
2 Allergy of respiratory tract
1) Bronchia asthma
支气管哮喘
Asthma
2)Allergic rhinitis 过敏性鼻炎
Rhinitis
3 Allergy of digestive tract 胃肠道过敏反应 4 Allergy of skin 皮肤过敏反应
ADVERSE DRUG REACTIONS

ADVERSE DRUG REACTIONS Therese I.PoirierRobert L.Maher,Jr.Duquesne University,Pittsburgh,Pennsylvania,U.S.A.INTRODUCTIONAdverse drug reactions(ADRs)are types of adverse drug events(ADEs)(1).ADEs include ADRs,medication errors,and other drug-related problems.ADEs are the negative consequences of drug misadventures.Henri Manasse defined drug misadventure as the iatrogenic hazard that is an inherent risk when drug therapy is indicated.This chapter will focus on ADRs. DEFINITIONSThe World Health Organization’s(WHO)and Karch and Lasagna’s definitions of an ADR are quite similar.An ADR is any response to a drug that is noxious and unintended,and occurs at doses used for prophylaxis, diagnosis,or therapy,excluding failure to accomplish the intended purpose(2).The Food and Drug Administration (FDA)focuses on ADRs that have unexpected reactions and/or those of more significant morbidity.These ADRs would include those where the patient outcome is death, life-threatening,hospitalization,disability,congenital anomaly,or required intervention to prevent permanent impairment or damage(3).The Joint Commission on Accreditation of Healthcare Organizations(JCAHO)is concerned with the reporting of significant ADRs.Those that result in morbidity,require additional treatment, require an increased length of stay,temporarily or permanently cause disability,or cause death must be reported to the FDA(4).The American Society of Health-System Pharmacists(ASHP)defines significant ADRs as any unexpected,unintended,undesired,or excessive response to a drug that includes the following:.Requires discontinuing the drug.Requires changing the drug therapy.Requires modifying the dose.Necessitates admission to the hospital.Prolongs stay in a health care facility.Necessitates supportive treatment.Significantly complicates diagnosis .Negatively affects prognosis or results in temporary or permanent harm,disability,or death(5)The ASHP definition does not include reactions due to drug withdrawal,drug abuse,poisoning,or drug complications.Other terms that may be included as ADRs are side effects,drug intolerance,idiosyncratic reactions,toxic reactions,allergic reactions,or hypersensitivity reactions (6).Side effects are reactions that are unintended and unwanted but are known pharmacologic effects of the drug and occur with predictable frequency.Drug intolerance is a mild reaction to a drug that results in little or no change in patient management.Idiosyncratic reaction is an unex-pected response that occurs with usual dose of a drug.Toxic reaction is a predictable response that results from greater than recommended drug dosages or drug concentration in the body.Allergic or hypersensitivity reaction is an unusual sensitivity to a drug of an immunologic nature. CLASSIFICATION SYSTEMSFour classification systems are used to describe ADRs(1,7).ADRs can be classified according to the pharmacologic effect of the drug—Type A,B,C,and D reactions.Type A reactions are exaggerated but normal pharmacologic actions of a drug.They are predictable and dose dependent.Type B reactions are not predictable given the known pharmacologic action of a drug and are not dose related.Many of these Type B reactions are hypersensitivity or immune-based.These reactions can be further subdivided into type I(IgE-mediated reaction), II(IgG or IgM-mediated cytotoxic reaction),III(IgG-mediated immune complex reactions),and IV(cell-mediated immune reaction).Type C reactions are those due to long-term use of a drug.Type D reactions are delayed drug effects,such as due to carcinogenicity or teratogenicity.ADRs can also be classified according to the dose relationship,i.e.,dose-related and non-dose-related reac-tions.Another classification system is based on the causal relationship between the reaction and the drug.One of theEncyclopedia of Pharmaceutical Technology Copyright q2002by Marcel Dekker,Inc.All rights reserved.34most widely used causality classifications is based on Naranjo’s descriptions.These categories include definite (drug is likely the true cause),probable(drug is the apparent cause),possible(drug appears to be associated), and remote(drug is not likely to be the cause).The fourth classification system is based on degree of injury or severity of reaction.There are mild reactions(temporary discomfort and tolerable),moderate(significant discom-fort),and severe(potentially life threatening or causing permanent disability or death).INCIDENCEThe frequency of ADRs in the general population is unknown.However,the reported rates of new occurrences for ADRs are noted for selected patient populations.A meta-analysis of39prospective studies reported an overall incidence of serious ADRs in hospitalized patients of6.7% and of fatal ADRs of0.32%(8).The fatality rate makes ADRs the fourth to sixth leading cause of death in the United States.Another meta-analysis of36studies indicated that approximately5%of hospital admissions are due to ADRs(9).The costs of ADRs are estimated to be$1.56–$4billion in direct hospital costs per year in the United States(10).FACTORS PREDISPOSING TO ADRSTwo major factors predispose to adverse drug reactions: the drug itself and patient factors.Factors related to the drug include its dose,dosage form and delivery system, and interactions between drugs.Patient-related factors include age,disease states,genetics,gender,nutrition, multidrug therapy use,and use of herbal therapies.Drug-Related FactorsDoseADRs may be the result of ingestion of increased amounts of a drug.Dosing issues are especially likely with narrow therapeutic index drugs.Examples of these types of drugs include digoxin,anticoagulants,anticonvulsants,antiar-rhythmics,antineoplastic agents,bronchodilators,seda-tives,and hypnotics(11).Dosage form and delivery systemMany of the ADRs related to the dosage form and delivery system are the result of local irritation or hypersensitivity reactions(12).Local irritation to the gastrointestinal(GI)tract can occur with oral dosages. For example,toxicity resulting in mouth ulcerations is associated with antineoplastic drugs.In addition,the use of certain formulations,such as sustained release preparations,can increase esophageal injury if esopha-geal transit is delayed.For example,a controlled release wax matrix of potassium chloride has been associated with significant esophageal erosions.Factors identified to predispose to esophageal injury include largefilm-coated tablets,capsules,large sustained-release preparations,rapidly dissolving formulations, and ingestion of solid oral dosage forms before bed rest with very little water intake(12).Localized tissue irritation can be seen from the intramuscular(IM)route.This is especially an issue when the formulation pH differs from the pH of the surrounding tissue or when precipitation of poorly soluble drugs occurs(12).Incorrect administration of IM injections is probably the most important factor that causes local adverse effects.Local skin irritation can also be seen with transdermal delivery systems due to the alcohols,nonionic surfactants,and adhesives.Hypersensitivity reactions can occur due to the presence of contaminants or excipients in pharmaceutical dosage forms(e.g.,outbreaks of eosinophilia-myalgia syndrome associated with oral tryptophan contaminants in various drugs)(12).Another example is the anaphylactoid reactions to the surfactant Cremaophor EL,which is used in paclitaxel(Taxol).Direct toxicity effects related to use of preservatives also has been documented.For example,severe metabolic acidosis and death in infants was attributed to the presence of benzyl alcohol,a preservative used in bacterostatic normal saline that was used toflush catheters(12).The use of specific intravenous(IV)delivery devices also can cause ADRs.For instance,use of plastic infusion sets for IV administration of nitroglycerin has resulted in subtherapeutic effects due to diffusion of the drug into the plastic tubes(12).Formulation effects,such as bioavailability differences, can cause ADRs when patients are switched to generic products.For example,significant adverse effects have occurred with anticonvulsants and thyroid prep-arations(12).Interactions between drugsIt has been estimated that6.9%of ADRs are due to drug–drug interactions(6).The most likely reason for an adverse drug interaction is the pharmacokinetic changes that result in altered metabolism or excretion of drugs,or thepharmacodynamic changes that result in synergistic or additive effects of drugs.Patient-Related FactorsAge,disease states,genetics,gender,nutrition,multidrug therapy use,and herbal therapies use are patient-related factors that influence the likelihood of adverse drug reactions.Age—geriatricsAge-related alterations in pharmacokinetics and pharma-codynamics may affect the response of elderly patients to certain medications,and may increase the susceptibility for ADRs among elderly patients(13–15)(Table1).The risk of ADRs among elderly patients is probably not due to age alone.ADRs may be related more to the degree of frailty and medical conditions of the patient(15).On average, older persons havefive or more coexisting diseases that may increase the risk of adverse events.Polypharmacy seems to be more of a common problem among the elderly. The average elderly patient takes4.5chronic medications andfills13prescriptions yearly(15).Elderly patients appear to have a decline in homeostatic mechanisms.The imbalance of homeostatic mechanisms and the decline in function reserves may put a patient at greater risk for ADEs due to decreased tolerance of medications and the ability to handle stressful situations(16).Age—pediatricsThe two factors responsible for increasing risks of ADRs in children are pharmacokinetic changes and dose delivery issues.Age-related differences in pharmacoki-netics in children are documented(17).However,the data on both efficacy and safety are often limited or not studied at all in this population.Thus,it is unclear whether an increased risk for ADRs exists in this group. However,there is a potential risk for increased ADRs if appropriate considerations are not taken into account in view of pharmacokinetic changes(18).It is important to note that only one-fourth of the drugs approved by the FDA have indications specific for use in a pediatric population(17).Medications used in adults are often given to children without FDA safety and efficacy patibility and stability issues with dosage forms intended for adults that have been altered(e.g.,dilution or reformulation)can increase risks for ADRs.Information on pediatric age-related difference in neonates,children,and adolescents may aid in prevention of pediatric ADRs(18)(Table2).Further studies of drug use in pediatrics are needed in order to prevent ADRs. Concurrent diseasesDiseases such as hepatic or renal diseases can influence the incidence of ADRs by altering the pharmacokinetics of drugs,such as absorption,distribution,metabolism,or excretion(6).Hepatic diseasePatients with liver disease have an increased susceptibility to certain drugs due to decreased hepatic clearance for drugs metabolized by the liver or due to enhanced sensitivity(6).For example,impaired hepatic metabolism can precipitate central nervous system(CNS)toxicity in patients on theophylline,phenytoin,or lidocaine;or ergot poisoning on ergotamine(19).Increased sensitivity to drugs is also encountered in liver disease(19).The use of anticoagulants increases the risk of bleeding due to the reduced absorption of vitamin K or decreased production of vitamin K-dependent clotting factors.There is an enhanced risk for respiratory depression and hepatic encephalopathy due to morphineTable1Geriatric age-related changes in pharmacokineticsPharmacokinetic phase Pharmacokinetic parametersGastrointestinal absorption Unchanged passive diffusion and no change in bioavailability for most drugs#Active transport and"bioavailability for some drugs#First-pass effect and"bioavailabilityDistribution#Volume of distribution and"concentration of water soluble drugs"Volume of distribution and"half-life for fat soluble drugs"or#free fraction of highly plasma protein-bound drugs#Clearance and"half-life for some Phase IOxidation drugs#Clearance and"half-life of drugs with high extraction ratioRenal excretion#Clearance and"half-life of renally eliminated drugs#¼Decreased;"¼Increased.or barbiturates in patients with severe liver disease. Vigorous use of diuretics can precipitate hepatic coma due to potassium loss in liver disease.There is an increased risk of hypoglycemia with sulphonylurea antidiabetic drugs due to decreased glycogenesis in liver disease.Liver disease can also cause hypoalbuminemia due to decreased liver synthesis of albumin.For drugs that are extensively bound to albumin,such as phenytoin,an enhanced risk of drug toxicity could occur because of the increase in free drug concentration.There are no useful methods to quantify the degree of liver disease that can assist in dosage adjustment.A practical approach involves checking patients for elevated prothrombin time,rising bilirubin levels,and/or falling albumin levels.In such instances,drugs that have an altered response in liver disease or cause hepatotoxicity need to be avoided.Renal diseaseImpaired renal function increases the incidence of ADRs for drugs that depend on the kidney for their elimination.Unlike liver disease,use of pharmacokinetic dosing principles can minimize the risk for adverse effects.Mechanisms responsible for enhanced ADRs in renal disease include delayed drug excretion,decreased protein binding due to hypoalbuminemia,and increased drug sensitivity(6).Delayed renal excretion is responsible for enhanced toxicity with drugs such as aminoglycosides, digoxin,vancomycin,chlorpropamide,H2-antagonists, allopurinol,lithium,insulin,and methotrexate(20).For some drugs,the accumulation of a toxic metabolite during renal failure is responsible for ADRs.This is the case with meperidine,where a toxic metabolite,normeperidine, accumulates in renal failure(20).Patients with accumulation of uremic toxins have increased sensitivity to certain drugs.There may be an enhanced response to CNS depressants(such as barbitu-rates and benzodiazepines),hemorrhagic effects from aspirin or warfarin,and other bleeding effects from antibiotics that inhibit platelet aggregation,such as carbenicillin,ticarcillin,and piperacillin.Other diseasesOn theoretical grounds,other diseases associated with hypoalbuminemia could predispose patients to adverse reactions and to altered responses to drugs that are highly protein bound(21)(Table3).The presence of other diseases can influence the risk for ADRs.Many of these adverse effects are related to an extension of the pharmacologic effects of the drug in the presence of certain pathophysiology.Numerous examples are given in Table4(6).Patients who have had a previous reaction to drugs are also more likely to experience an ADR(22).Patients with history of allergic diseases also have an increased risk due to a genetically related ability to form immunoglobulin E. Genetic factorsGenetic factors account for some ADRs due to either altered pharmacokinetics or by altering tissue responsive-ness.Altered metabolism of drugs occurs due toTable2Pediatric age-related risk factors and causes of ADRsNeonates:Placental transfer of drug before birthDiffering drug actionAltered pharmacokineticsIncreased percutaneous absorptionDecreased renal/hepatic functionDecreased plasma protein bindingUse of multiple drugsLimited information on drug action in critically ill and prematureneonatesChildren:Paradoxical effect of medications(excitability rather thansedation from antihistamines)Excipients of liquid dosage formsSugar as sweetenersPropylene glycol as solventLarge volume intravenous solutionsTreatment of viral infections with antibioticsDisruption of neurologic and somatic developmentAdolescents:Autonomy seekingUse and misuse of devices(e.g.,tampons)Use and misuse of prescription and nonprescription medicationsPoor compliance with instructionsUse of multiple medicationsRecreational use of alcohol and illicit drugsEffects of changing hormone levels on drugs(From Ref.7.)Table3Conditions associated with hypoalbuminemiaAging Liver diseaseBurns Nephrotic syndromeCancer Nutritional deficiencyCardiac failure PregnancyProtein-losing enteropathy Renal failureInflammatory diseases SepsisInjury StressImmobilization Surgerydifferences in hydrolysis,acetylation,and hepatic oxidation of drugs.Altered pharmacodynamic reactions could be either an exaggerated response or a qualitative response.These types of reactions are unpredictable. Examples of altered drug response due to genetic factors are found in Table5(6).GenderA higher incidence of ADRs has been reported for women in comparison to men(6).One reason for this observation is that women take more drugs than men.Yet,no sex-linked differences in drug pharmacokinetics have been documented.Other reports have not supported a higher incidence of ADRs in women as compared to men.Thus, sex alone is unlikely to be a major determinant of ADRs. NutritionNutritional factors are also responsible for ADRs.These factors include the interaction of drugs and nutrients,and altered pharmacokinetics related to nutritional status.One study reported a very low incidence(0.4%)of clinically significant drug–nutrient interactions in a teaching hospital(23).Three mechanisms postulated for drug–nutrient interactions are interference with drug absorption,alteration of drug excretion,and affecting drug activity.For example,the absorption of tetracycline is reduced by chelation with iron,calcium,and magnesium. Foods that acidify or alkalinize the urine can affect drug excretion.Foods that contain a large amount of vitamin K can inhibit the activity of warfarin.A listing of important drug–nutrient interactions is found in Table6(23).A review article on drug–food interactions in clinical practice is found in Ref.24.Drug–nutrient interactions may be more highly significant in renal failure patients.A review article of drug–nutrient interactions in renal failure has been published(25).Nutritional status can affect drug pharmacokinetics. Malnutrition states can cause the following:1)the liver and kidneys changes affect drug elimination;2)GI system changes affect drug absorption;3)changes in the heart affect bloodflow;4)hormone changes affect metabolic enzymes and drug binding proteins;5)plasma,tissue proteins,and body composition changes affect protein binding and elimination;6)mineral and electrolyte changes affect drug metabolism and protein binding;and 7)tissue changes affect uptake of drugs and drug–receptor interactions(26).Multidrug useAccording to several epidemiological studies,multiple drug use has a strong association in the causality of ADRs.It has been suggested that the more medications used,the higher the risk for ADRs(27).Consistent drug regimen reviews by healthcare providers in order to reduce polypharmacy may decrease the risk of ADRs.Herbal therapies useThe use of herbal therapies increased dramatically during the1990s.Herbal therapy sales are estimated to be$4billion a year,with sales increasing at20%per year since the early1990s(28).Patients often mistakenly believe that since these products are natural, they do not possess the potential harm as in prescription medications.Since herbal medications are sold and marketed without stringent FDA approval and guidelines,limited evidence-based data on efficacy, adverse effects,and drug interactions exist.Recently, two review articles examined available data on ADRs for the most common herbal medications(28,29). Many of these available reports fall short on documentation of temporal relationship with the specific ADR and the herbal drug.For most conditions,herbal products are not a replacement for proven prescription or nonprescription drugs.Patients should be aware that health care practitioners cannot guarantee the safety and consistency of herbal products.Patients should start with the recommended effective doses and report any unusual side effects to their health care practitioner.Patients should always consult with their pharmacist for possible drug–herbal interactions.Side effects and possible drug interactions for the ten most commonly used herbals are listed in Table7.ADVERSE DRUG REACTIONREPORTING SYSTEMSThe WHO,the FDA,the JCAHO,and the Health Care Financing Administration(HCFA)have all addressed and mandated the need for health care institutions to implement an ADE detection and reporting system. Detection systems are instrumental in postmarketing surveillance of ADRs.The JCAHO requires all accredited health care institutions to have an ongoing drug surveillance program(4).The goals of ADR detecting and reporting systems are to aid in postmarketing surveillance of FDA approved medi-cations and to identify ways to decrease ADR risks. The main focus of all of these reporting systems is to aid in promoting improvements in the medication use process.Adverse Drug Reactions39ADR Screening MethodsThe best methodology for screening for ADRs has not been determined.However,several screening methods have been proposed.In particular,the literature has highlighted five screening methods using clinical data(30–34).The five include screening for:1)“tracer drugs,”e.g.,antidotes such as vitamin K and diphenhydramine;2)“narrow therapeutic range drugs,”e.g.,follow-up of computer lab values for warfarin and digoxin;3)change in medications, e.g.,documentation of discontinued medications or decreased dose;4)diagnosed ADRs documented in the medical record,e.g.,chart review or reviewing ICD-9CM (International Classification of Diseases,Ninth Revision, Clinical Modification)codes;and5)ADR computer report tracking systems.Although each of these ADR screening methods has been described in detail,limited data are available on the productivity of these screens.Systems for Pharmaco-epidemiologic StudiesPharmacoepidemiology is used to detect ADRs(35,36). Several types of systems use pharmacoepidemiologic methods.These include spontaneous reporting,studies of therapeutic classes,and studies of specific medical syndromes.Spontaneous reportingSpontaneous reporting is currently the major backbone for the detection of ADRs(37).It occurs in one of three ways: 1.Reporting to the FDA as part of clinical trials;2.Reporting by practitioners to medical journals;or3.Patients’self-reporting to either manufacturers or theFDA(38).Clinical trials in new drug development cannot detect all the possibilities for drug safety.Limitations in Phase III clinical trials include a relatively small sample size,short duration of the trial,restricted populations(e.g.,geriatrics and pediatrics),uncomplicated patients,(e.g.,limited disease states),and limited power for adverse drug reaction detection(30).Thus,the FDA relies heavily on spontaneous reporting of suspected ADRs(39).Spon-taneous reporting is important in early market history of the drug to determine previously unidentified drug reactions.This has been particularly true in the last few years because of numerous new medications that have entered the market and now carry a black box warning.For example,Rezulin w and Trovan w are associated with hepatotoxicity and carry black box warnings.Additional advantages of spontaneous reporting sys-tems include the detection of extremely rare ADRs and ability to identify at-risk subgroups.In order to enhance the spontaneous reporting system approach,the FDA developed the MedWatch form.This form can be faxed to the agency(1-800-FDA-1078)or called in(1-800-FDA-1088)(40).The forms also can be obtained by the “MedWatch Online”internet-based website(http://www. /medwatch/).Limitations of FDA spontaneous reporting include both under-reporting and over-reporting.An example of over-reporting occurs with recently approved drugs.This is partly due to enhanced publicity about these drugs.Table6Important drug-nutrient interactionsDrug Nutrient InteractionPhenytoin Alcohol Enhanced metabolism of phenytoinEnteral feedings Decreased phenytoin absorption Tetracycline Dairy products Impaired drug absorption Theophylline Caffeine Potential for toxic effects Warfarin Foods high in vitamin K Decreases anticoagulant response Chlorpropamide,tolbutamide,tolazamide,acetohexamide,metronidazoleAlcohol Disulfiram-like reaction Trancylcypromide Foods high in tyramine Hypertensive crisisDisulfiram Alcohol Nausea,blurred vision,chest pain,dizziness,fainting Spironolactone Foods high in potassium Hyperkalemia(Adapted from Ref.23.)Studies of therapeutic classesObservational cohort or case control designs have been used to determine ADR relationships with specific therapeutic classes(36,41).Medical claims data are often used in these studies and caution should be warranted due to lack of definite confirmation of drug exposure and the potential for confounding variables(38).However, these studies have been beneficial in determining risk of ADRs with specific classes(e.g.,NSAIDs and the risk of peptic ulcer disease)(42).Studies of specific medicalsyndromesObservational cohort or case control designs can also be useful to study possible causality relationships of specific medical conditions or syndromes due to drug exposure(36, 41).These types of studies have been particularly useful in examining ADRs in a specific population,such as geriatric or pediatric patients.These groups of patients are often excluded in Phase III trials.However,a disadvantage of these studies is that they also often use administrative data. These data can warrant risk of problems in determining causality due to potential confounding variables(38). Assessing Adverse DrugReactionsAfter detection of a possible ADE,causality assessment needs to be performed.It is important to be able to rank the likelihood of an ADR as unlikely,possible,probable,or definite.A major problem with determining causality is that confounding variables can contribute to the complexity of causality assessment(43).In order to determine causality, several important points of data are required.These include the nature of the adverse event,name of the putative drug, other potential causes,and the temporal relationshipTable7ADRs for the top ten herbal medicinesHerbal Common use Side effects and interactionsEchinacea Treatment and prevention of upperrespiratory infections,common cold Rash,pruritis,dizziness,unclear long-term effects on the immune system.St.John’s wort Mild to moderate depression Gastrointestinal upset,photo-sensitivity.Mild serotonin syndrome with the followingmedications:paroxetine,trazodone,sertraline,andnefazodone.May decrease digoxin levels.May decrease cyclosporine serum concentrations.Combined oral contraceptives—breakthrough bleeding. Gingko biloba Dementia Mild gastrointestinal distress,headache,mayaffect warfarin(increase INR).Interaction with aspirin(spontaneous hyphema) Garlic Hypertension,hypercholesterolemia Gastrointestinal upset,gas,reflux,nausea,allergic reactions,and antiplatelet effects.May effect warfarin(increase INR)Saw palmetto Benign prostatic hyperplasia UncommonGinseng General health promotion,sexual function,athletic ability,energy,fertility High doses may cause diarrhea, hypertension,insomnia,nervousness,may affect warfarin(decreased INR)Goldenseal Upper respiratory infections,common cold Diarrhea,hypertension,vasoconstrictionAloe Topical application for dermatitis,herpes,wound healing,and psoriasis,orallyfor constipation May delay wound healing aftertopical application.Diarrhea,and hypokalemia with oral useSiberian ginseng Similar to ginseng May raise digoxin levels.May affect warfarin(increased INR)Valerian Insomnia,anxiety Fatigue,tremor,headache,paradoxical insomnia(not advised with other sedative-hypnotics)。
药理学医学英语词汇.

协同作用 治疗效应 治疗指数 阈浓度 毒性反应
Chapter 3 Pharmacokinetics
英文 absorption active transport apparent volume of distribution(vd) bioavailability biotransformation blood-brain-barrier clearance, cl distribution drug transport rate elimination enzyme inducer enzyme inhibitor first order kinetics first-pass effect half life( t1/2) hepatoenteral circulation maintenance dose metabolism one-compartment model passive diffusion peak concentration (cmax ) placental barrier redistribution of drugs steady state concentration(css ) Plateau concentration time-concentration curve two-compartment model zero order kinetics
中文 卡巴胆碱 胆碱酯酶抑制剂 胆碱受体激动剂 调节麻痹 调节痉挛 加兰他敏 新斯的明 毒扁豆碱 毛果芸香碱 有机磷酸酯类 胆碱酯酶复活剂
Chapter 7 Cholinoceptor blocking drugs
英文
anisodamine
atropine
homatropine
pirenzepine
Chapter 13 - Review
Chapter 13 - Review
Which
of the following electron configurations is the most stable? 4d55s1 or 4d45s2 Stable electron configurations are likely to contain _____.
Chapter 13 - Review
What
is the approximate frequency of a photon having an energy of 5 x 10-24 J? (h = 6.6 x 10-34 J.s)
Chapter 13 - Review
The
lowest energy state of an atom is called the ______. What is the approximate mass of a particle having a wavelength of 1 x 10-7 m, and a speed of 1 m/s? (h = 6.6 x 10-34 J.s)
Chapter 13 - Review
In
order to occupy the same orbital, two electrons must have _____. According to the Aufbau principle, electrons enter orbitals of _____ energy first.
Chapter 13 - Review
What
statement says that no more than two electrons can occupy an atomic orbital, and that two electrons in the same orbital have opposite spins?
适应性免疫应答

2.通常起抗原提呈作用的靶细胞上无/少协同刺激 分子,CD8+CTL细胞需要活化CD4+Th1细胞分泌的 IL-2、 IFN-γ的作用作为活化第二信号才能活化 并表达 IL-12 等细胞因子受体。
3.通过交叉提呈作用被活化的CD4+Th细胞,可诱
活化Tc增殖、分化成效应细胞/记忆细胞 Tc脱颗粒作用,颗粒内含穿孔素、使靶细胞溶解死亡 Tc分泌蛋白毒素,使靶细胞内DNA降解酶活化,靶细胞凋亡 Tc表达FASL与靶细胞表面FAS结合,诱导靶细胞凋亡
思考题
固有免疫应答与适应性免疫应答的主要特点 有哪些不同?
CTL细胞怎样发挥细胞毒作用?
抗原肽-MHC II类分子复合物相互作用
产生Th细胞活化第一信号。
• 3.B细胞通过表面B7和ICAM-1共刺激分子
与CD4+Th细胞表面相应的CD28和LFA-1共刺
激分子结合,产生Th细胞活化第二信号。
4.活化Th细胞可表达CD40L(gp39)和多种细胞
因子受体,同时分泌IL-2、4、5及 IFN- γ 等细胞因子,参与免疫调节,促进T/B细胞活 化、增殖和分化。
导靶细胞表达共刺激分子,从而能使与同一靶
细胞结合后只获得第一活化信号的CD8+CTL细胞
获得B7分子刺激,产生第二活化信号,CD8+CTL 活化并表达 IL-12 等CK受体。
(二)CD8+效应CTL细胞的形成及作用 1. 活化CD8+CTL细胞在IL-12、IL-2、 IFNγ 协同作用下,增殖分化为具有杀伤作用 的效应性CD8+CTL细胞。
3、免疫应答过程中淋巴细胞之间相互作用
Firmagon (degaralix) 使用指南说明书

Firmagon® (degaralix)Document Number: IC-0044 Last Review Date: 10/31/2017Date of Origin: 01/01/2012Dates Reviewed: 03/2012, 06/2012, 09/2012, 12/2012, 03/2013, 06/2013, 09/2013, 12/2013, 03/2014, 02/2015, 1/2016, 10/2016, 10/2017I.Length of AuthorizationCoverage will be provided for twelve months and may be renewed.II.Dosing LimitsA.Quantity Limit (max daily dose) [Pharmacy Benefit]:∙Loading Doseo Firmagon 120 mg vial powder for injection: 2 vials first 28 days∙Maintenance Doseo Firmagon 80 mg powder for injection: 1 vial every 28 daysB.Max Units (per dose and over time) [Medical Benefit]:∙Loading Doseo240 units one time∙Maintenance Doseo80 units every 28 daysIII.Initial Approval CriteriaCoverage is provided in the following conditions:Advanced Prostate cancer ††FDA Approved Indication(s)IV.Renewal CriteriaCoverage can be renewed based upon the following criteria:∙Tumor response with stabilization of disease or decrease in size of tumor or tumor spread;ANDAbsence of unacceptable toxicity from the drug. Examples of unacceptable toxicity includethe following: prolongation of the QT-interval, severe hypersensitivity, etc.V.Dosage/AdministrationVI.Billing Code/Availability InformationJcode:J9155– Injection, degarelix, 1 mg: 1 billable unit = 1 mgNDC:∙Firmagon 80 mg powder for injection Maintenance Dose Kit: 55566-8303-xx∙Firmagon 120 mg vial (2) powder for injection Starter Dose Kit: 55566-8403-xxVII.References1.Firmagon [package insert]. Parsippany, NJ; Ferring Pharmaceuticals, Inc; July 2016.Accessed September 2017.2.Referenced with permission from the NCCN Drugs & Biologics Compendium (NCCNCompendium®) for Degaralix. National Comprehensive Cancer Network, 2017. TheNCCN Compendium® is a derivative work of the NCCN Guidelines®. NATIONALCOMPREHENSIVE CANCER NETWORK®, NCCN®, and NCCN GUIDELINES® aretrademarks owned by the National Comprehensive Cancer Network, Inc.” To view the mostrecent and complete version of the Compendium, go online to . AccessedSeptember 2017.Appendix 1 – Covered Diagnosis CodesAppendix 2 – Centers for Medicare and Medicaid Services (CMS)Medicare coverage for outpatient (Part B) drugs is outlined in the Medicare Benefit Policy Manual (Pub.100-2), Chapter 15, §50 Drugs and Biologicals. In addition, National Coverage Determination (NCD) and Local Coverage Determinations (LCDs) may exist and compliance with these policies is required where applicable. They can be found at: /medicare-coverage-database/search/advanced-search.aspx. Additional indications may be covered at the discretion of the health plan. Medicare Part B Covered Diagnosis Codes (applicable to existing NCD/LCD):N/A。
2013超敏反应
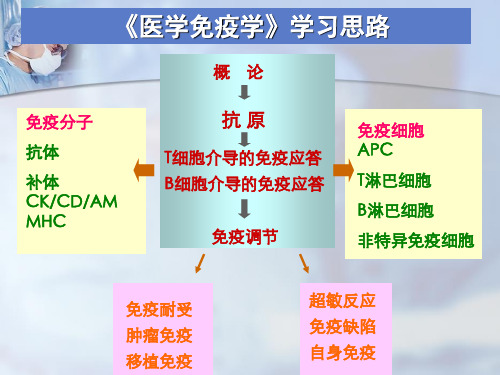
IgE的合成受许多因素的调节
Ⅰ型超▲敏反遗应传常因表素现为的家影族响易感性。与正常人相比,易
感家族成员血清IgE水平明显升高,肥大细胞数较多,且
胞膜上Ig▲E受接体触也较变多应。原此的与机相会关基因活跃有关。
★查明变应原,避免再次接触
◆询问过敏性疾病的病史
★◆脱变敏应原、皮减肤敏试治验 疗
◆异血种清免特疫异血性清脱Ig敏E疗检法测
★应药用:物抗防毒素治皮试阳性但又必须使用时
方法:小剂量、短间隔、多次注射
机◆抑制制:生体物内活致性敏介靶质细合胞成分与批释分放期的脱药敏物如
◆◆特生异物性活变性应介原质减拮敏抗疗剂法;
→释放细胞因子 IL-2 IFN-γ TNF IL-3 GM-CSF等 →以单核细胞及淋巴细胞浸润为主的免疫损伤
CD8+ CTL细胞 介导的细胞毒作用
→释放穿孔素和颗粒酶 直接杀伤靶细胞 →通过Fas/FasL途径→靶细胞凋亡
三、临床常见疾病
传染性迟发型超敏反应 接触性皮炎 结核
四型超敏反应与临床疾病
种血清等
抗
IgG和IgM为主;少数为 IgA
体
二、发生机制
免疫复合物
形成 沉积 致病
2:1
3:2
4:6
小分子
滤过排出
中分子
沉 积
致病
大分子
吞噬清除
免疫复合物的形成和沉积的影响因素
血管活性胺类物质的作用
胺类活性物质的释放
IC直接与血小板表面FcγR结合
→释放组胺等
补体活性片段作用于肥大细胞、嗜碱细胞、血小板
研究生学术综合英语Units1-6课文及翻译

Unit 1 Presenting a speech(做演讲)Of all human creations, language may be the most remarkable. Through在人类所有的创造中,语言也许是影响最为深远的。
我们用语言language we share experience, formulate values, exchange ideas, transmit来分享经验,表达(传递?)价值观,交换想法,传播知识,knowledge, and sustain culture. Indeed, language is vital to think itself.传承文化。
事实上,对语言本身的思考也是至关重要的。
[Contrary to popular belief], language | does not simply mirror reality butalso helps to create our sense of reality [by giving meaning to events].和通常所认为的不同的是,语言并不只是简单地反映现实,语言在具体描述事件的时候也在帮助我们建立对现实的感知。
——语序的调整。
Good speakers have respect for language and know how it works. Words are the tools of a speaker’s craft. They have special uses, just like the tools of any other profession. As a speaker, you should be aware of the meaning of words and know how to use language accurately, clearly,vividly,and appropriately.好的演讲者对语言很重视,也知道如何让它发挥更好的效果。
IntelectIFC和IntelectTENS产品说明书
ContentsChapter Page 1INTRODUCTION1.1General information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1 1.2 Cautions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1 1.3Indications for use . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1 1.4Warnings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1-2 1.5Precautions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2-3 1.6 Adverse Reactions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .32PRODUCT DESCRIPTIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4-63STIMULATION MODES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7-84INSTRUCTIONS FOR USE4.1Check Battery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9 4.2Connect electrodes to lead wires . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9 4.3Connect lead wires to unit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .10 4.4Place electrodes on skin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11 4.5Select the electrode numbers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11Chapter Page 4.6 Select the mode . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11 4.7Adjust the Rate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12 4.8 Adjust Channel Amplitude . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12 4.9 T urn Unit Off . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12 4.10 Portability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13 4.11 Battery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13 4.12 Care of Electrodes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .14 4.13 Care of Electrode Cords . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .145HANDLING AND STORAGE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .156SPECIFICATION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .157ACCESSORIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .168TROUBLESHOOTING . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .179WARRANTY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .181. INTRODUCTION1.1 General information:This interferential (IFC) device is a lightweight and portable medical device which can help to reduce pain and discomfort. It utilizes the low electric-current to stimulate muscle nerves to achieve the symptomatic relief of chronic intractable pain, post-traumatic pain, and post-surgical pain.1.2 CautionsFederal law (USA) restricts this device to sale by or on the order of practitioners licensed by the State in which they practice to use or order the use of the device.1.3 Indications for use:This device is used in symptomatic relief of chronic intractable pain, post-traumatic and post-surgical pain.1.4 Warnings:1.4.1 The long-term effects of chronic electrical stimulation are unknown.1.4.2 Stimulation should not be applied over the carotid sinus nerves, particularly in patients with a knownsensitivity to the carotid sinus reflex.1.4.3 Stimulation should not be applied over the neck or mouth. Severe spasm of the laryngeal and pharyngealmuscles may occur and the contractions may be strong enough to close the airway or cause difficulty inbreathing.1.4.4 Stimulation should not be applied transthoracically in that the introduction of electrical current into theheart may cause cardiac arrhythmias.11.4.5 Stimulation should not be applied over swollen, infected, or inflamed areas or skin eruptions, e.g., phlebitis,thrombophlebitis, varicose veins, etc.1.4.6 Stimulation should not be applied over, or in proximity to, cancerous lesions.1.4.7 For external use only.1.4.8 Do not use IFC on the eye area.1.4.9 This device should be used only under the continued supervision of a licensed medical practitioner.1.4.10 Safety of IFC devices for use during pregnancy or delivery has not been established.1.4.11 Electronic equipment such as ECG monitors and ECG alarms may not operate properly when IFC is in use.1.4.12 Apply the electrodes to clean, dry, and unbroken skin only.1.4.13 This device should not be used while driving, operating machinery, or during any activity in whichinvoluntary muscle contractions may put the user at undue risk of injury.1.4.14 This device should be kept out of the reach of children.1.4.15 Keep electrodes separate during treatment. Electrodes in contact with each other could result in improperstimulation or skin burns.1.5 Precautions:1.5.1 Caution should be used for patients with suspected or diagnosed heart problems.1.5.2 Caution should be used for patients with suspected or diagnosed epilepsy.21.5.3 Caution should be used in the presence of the following:(a)When there is a tendency to hemorrhage following acute trauma or fracture(b)Following recent surgical procedures when muscle contraction may disrupt the healing process.(c)Over the menstruating or pregnant uterus(d)Over areas of the skin which lack normal sensation.1.5.4 Some patients may experience skin irritation or hypersensitivity due to the electrical stimulation orelectrical conductive medium. The irritation can usually be reduced by using an alternate conductivemedium, or alternate electrode placement.1.5.5 Electrode placement and stimulation settings should be based on the guidance of the prescribingpractitioner.1.5.6 This device should be used only with the leads and electrodes recommended for use by the manufacturer.1.5.7 Isolated cases of skin irritation may occur at the site of the electrode placement following long-termapplication.1.5.8 Effectiveness is highly dependent upon patient selection by a person qualified in the management of painpatients.1.5.9 If the stimulation levels are uncomfortable or become uncomfortable, reduce the stimulation amplitude to acomfortable level and contact your physician if problems persist.1.6 Adverse Reactions:1.6.1 Possible skin irritation or electrode burn under the electrodes may occur.1.6.2 Possible allergic skin reaction to tape or gel may occur.34A panel covers the controls. Y our medical professional may ask to set these controls for you and request you leave the cover in place.Amplitude Control:It controls the "INTENSITY" level of stimulating pulses. The control located at the right top of the unit regulates the amplitude, or intensity, of the stimulation and is the ON/OFF CONTROL. The power indicator will light up with green color when the unit is working.Caution: If the stimulation levels are uncomfortable or become uncomfortable, reduce the stimulation intensity to a comfortable level and contact your physician if problems persist.Rate ControlAdjust Frequency from 1 Hz to 150 Hz by turning the control. The control is located at the left top of the unit. Electrode SwitchT o select for using two electrode pads or four electrode pads.Mode SelectorSet C, 1/1, 8/8, 10/10 mode56789NOTE: Always read this instruction manual before use.PREPARATION FOR USE4.1 Check Battery:Insert a fresh 9V alkaline or rechargeable battery into the battery compartment. Makesure that you are installing the battery properly. The battery is inserted in the casing onthe foot of the stimulator unit.BE SURE TO MATCH THE POSITIVE AND NEGATIVE ENDS OF THEBATTERY TO THE MARKINGS IN THE BATTERY COMPARTMENT OFUNIT .CONNECTING THE STIMULATOR4.2 Connect electrodes to lead wires:Insert the lead wire connector into electrodes connector (standard 0.08 inch femaleconnection).MAKE SURE THAT NO BARE METAL OF THE PINS IS EXPOSEDCaution: Always use the electrodes with the requirements of the EN60601-1 and EN60601-2, such as withCE mark, or which are legally marketed in the US under 510(K) procedure.4. INSTRUCTIONS FOR USEAngle"L"-shapeplugSelf-adhesiveElectrodes Pads104.4 Place electrodes on skin:Apply electrodes to the exact site indicated by your physician following the instruction included with the electrodes labeling. Before applying electrodes, be sure the skin surface over which electrodes are placed is thoroughly cleaned and dried. Make sure the electrodes are placed firmly to skin and make good contact between the skin and the electrodes. Place the electrodes over the skin; attach them properly, firmly and evenly. ADJUSTING THE CONTROLS4.5 Select the electrode numbersShift to the left when applying one pair of electrodes (the "two electrodes" position). Shift the switch to the right when applying two pairs of electrodes (the "four electrodes" position). No stimulation is delivered from "Channel 1" when one pair of electrodes is utilized and the electrode switch is set in the "two electrodes" position.4.6 Select the mode:Shift "MODE" switch to set the stimulation mode recommended by your physician or therapist. For details about stimulating sequences, refer to Sec. 3 "Stimulation Modes ".114.7 Adjust the Rate:The rate is adjustable 1~150Hz.T urn Rate Control to adjust Rate to the setting recommended by your medicalprofessional.4.8 Adjust Channel Amplitude:T urn Amplitude knob clockwise. Slowly turn the Amplitude control until you reach thesetting recommended by your prescribing medical practitioner.Caution: If the stimulation levels are uncomfortable or become uncomfortable, reduce the stimulationintensity to a comfortable level and contact your physician if problems persist.4.9 T urn Unit Off:T urn Channel Amplitude control to OFF. Unplug the electrode lead wires, grasping themby the plug, not the cord. If treatment will be resumed shortly, the electrodes may be left on the skin. When the electrodes are removed, clean the skin thoroughly with mild soap and water. If there is skin irritation, consult your medical professional.12CARE AND MAINTENANCE4.10 Portability:Y our unit is portable and may be clipped to a belt, shirt pocket, bra or other clothing.4.11 Battery:T o replace the battery, open the lid cover and extract the battery. Replace it with a 9 V alkaline or similar rechargeable battery. Make sure you insert the battery correctly.13144.12 Care of Electrodes:T o avoid skin irritation and ensure good contact with skin, clean silicone rubber electrodes with soap and water frequently. The electrodes must be dried completely before using.✽If you are using self-adhesive electrodes, disregard this procedure.✽Always use the electrodes with the requirements of the EN60601-1 and EN60601-2, such as with C E mark, or which are legally marketed in the US under 510(K) procedure.4.13 Care of Electrode cords:Clean the electrode cords by wiping them with damp cloth. Coating them lightly with talcum powder will reduce tangles and prolong the life.5. HANDLING AND STORAGEKeep this device in the carrying case and store at room temperature.6. SPECIFICATIONransportation Humidity Range*All values have10% tolerance.7. ACCESSORIESSelf-Adhesive Electrodes 4 PCS.9 V Battery 1 PC.Lead Wires 2 PCS.Instruction Manual 1 PC. ArrayAC Adapter 1 PC.168. TROUBLESHOOTING17•The power indicator lights up, butunit does not function properly.•"On" and "Battery Light" are dim.•None of indicators light up.1. Check all control settings. Are they set to values prescribed byyour medical professional?2. Are electrodes in proper position?3. Check lead wires. Be sure allconnectors are firmly sealed.4. Replace cord set with another tocheck for broken wires.1. Replace battery with a new one.1. Replace battery with a new one.If your unit does not seem to operate correctly, refer to the chart below to determine what may be wrong. If none of these measures correct the problem, the unit should be serviced.9. WARRANTY* Unit: One year (12 months) from the date of the original consumer purchase.* Accessories (consisting of lead wire, AC adapter, electrodes, carrying case, and belt clip): 90 days from the date of original consumer purchase.T o obtain service from Chattanooga Group or the selling dealer under this warranty, a written claim must be made within the warranty period to Chattanooga Group or the selling dealer.Chattanooga Group shall not be held liable in any event for incidental or consequential damages. Some states do notallow exclusion or limitation of incidental or consequential damages so the above limitation or exclusion may notapply to you.18。
一型超敏反应

5, Type I hypersensitivity: mechanisms
(1), Sensitization stage: IgE
5, Type I hypersensitivity: mechanisms
(2), excitation stage:
5, Type I hypersensitivity: mechanisms
Cytokines: TNF, IL-4, IL-6, and others
attract neutrophiles and basophiles, promote inflammation
6, Type I hypersensitivity: disease
Systemic anaphylaxis (anaphylactic shock)
Histamines Bradykinin
-adrenaline
–Bronchodialators
Prevent mast cell degranulation
– sodium,
Cortisone, theophylline, aspirin
(3), Immunotherapy
(3),
Prostaglandin D2:
kinins - vascular permeability, vasodilatation, edema
platelet activating factor PAF:
platelet aggregation, microthrombi formation, heparin release
2, Type I hypersensitivity: feature
Kalbitor(ecallantide)(SQ形式)商品说明书

NDC: Kalbitor 10 mg – 47783-0101-xx (Dyax Corp)
Max Units (per dose and over time):
Male
360 billable units per 28 days
Female
360 billable units per 28 days
I. Medication Description: Kalbitor (ecallantide) is a selective, reversible human plasma kallikrein inhibitor. Ecallantide binds to plasma kallikrein and blocks its binding site, inhibiting the conversion of HMW kininogen to bradykinin. By directly inhibiting plasma kallikrein, ecallantide reduces the conversion of HMW kininogen to bradykinin and thereby treats symptoms of the disease during acute episodic attacks of HAE.
VII. Centers for Medicare and Medicaid Services (CMS): Medicare coverage for outpatient (Part B) drugs is outlined in the Medicare Benefit Policy Manual (Pub. 100-2), Chapter 15, §50 Drugs and Biologicals. In addition, National Coverage Determination (NCD) and Local Coverage Determinations (LCDs) may exist and compliance with these policies is required where applicable. They can be found at: /medicare-coverage-database/search/advanced-search.aspx. Additional indications may be covered at the discretion of the health plan.
高一英语科幻小说阅读理解20题
高一英语科幻小说阅读理解20题1<背景文章>In the classic science - fiction novel "Dune", the world is set in a far - flung future. The technology level is a complex mix. On one hand, there are advanced spaceships that can traverse the galaxy, powered by a mysterious energy source known as the Spice. This Spice is not only crucial for space travel but also has a profound impact on human abilities. It can expand the mind, allowing some to gain prescient visions.The society is highly stratified. There are noble houses that hold great power and wealth. These noble houses are in a constant struggle for control over the Spice - rich planet Arrakis. Beneath the nobles are the common people, who live in a more subservient role. There are also the Bene Gesserit, a powerful all - female order. They have trained their minds and bodies to extraordinary levels through years of discipline.Regarding the relationship with alien life, there are no obvious extraterrestrial intelligent beings in the traditional sense. However, the sandworms on Arrakis can be considered a unique form of "alien" life. These gigantic creatures are native to the desert planet. They are both feared and revered, as they are the source of the Spice. The people on Arrakis have to co - exist with these massive and dangerous creatures, andthe entire ecosystem of the planet revolves around them.1. What is the most important thing for space travel in the world of "Dune"?A. Advanced spaceshipsB. The SpiceC. Prescient visionsD. The Bene Gesserit答案:B。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
• Histamines have many functions in the body, among them the dilation (or opening up) of capillaries and contraction (or tightening up) of muscles, both of which contribute to intense itching.
• 局部性反应 多在注射后数小时,在注射局部出 现肿胀、热痛,数天后有波动感,穿刺流出黄红 色液体。
• 防治措施 用药过程中应注意观察,如出现 变态反应,立即停止用药并对症治疗。严 重的及时静脉注射0.1%肾上腺素5mL或 10%葡萄糖酸钙200—300mg(马、牛); 也可用可的松类、氨茶碱、抗组胺药等。 全身性过敏,一般经20—30分钟可康复, 但禁止再次注射青霉素,局部过敏只要不 再注射青霉素多能自愈。
• Each exposure to the allergen causes a new reaction, and if not treated, the pet has no choice but to scratch or chew at the inflamed area, causing further inflammation, welts(raised marker on skin), and sores - even ear infections.
• Allergens enter your pet's body via inhalation, ingestion, injection, parasites, or touch. When animals have allergies, they tend to sneeze, have watery eyes, and a runny nose. Dogs and cats are more likely to excessively scratch or lick themselves instead.
12-2 Antibody-dependent cytotoxic hypersensitivity(type II)
• Blood transfusion • IgM, IgG • Complement, Fc receptor
Antibody-Dependent Cellular Cytotoxicity(ADCC)
How does an allergen create allergies?
• When your pet is first exposed to the potential allergen, such as grass pollen, his immune system develops antibodies to the pollen, though there will be no noticeable outward symptoms during this initial exposure.
《中国兽药杂志》2004 年10 月38 卷10 期
12-1 Hypersensitivity Type I
• 各种家畜对青霉素都可发生过敏反应,严 重的可出现过敏性休克,甚至引起死亡。 所以在临床应用时,应注意观察家畜的反 应。家畜青霉素过敏有两种,即全身性过 敏和局部性反应。
• 全身性过敏 在注射青霉素后立即或经过15-25分 钟后出现过敏反应,表现为全身出汗,肌肉震颤, 体温升高,脉搏加速,呼吸急促,结膜潮红或发 绀,呆立不动,强迫其运动则步态不稳,或突然 倒地,角弓反张,瞳孔散大,视力障碍,粪尿失 禁,反射减弱或消失。病猪多鸣叫不安,呕吐, 出现皮疹。
新生马驹溶血病
Aa-negative mare
Aa-positive foal
Hemolytic disease
12-3 Immune Complex-Mediated Hypersensitivity(Type III)
• Excessive antigen + antibody=Complex • Macrophage FcγReceptor + Complex→
Proinflammatory cytokines, IL-1, TNF-α • Complement
Immted(Delayed-Type) Hypersensitivity(Type IV)
• Bacteria, viruses and fungi • CD4+ T cells-mediated, macrophage
12 Hypersensitivity
Four Types of Hypersensitivity Reaction
病例分析
用庆大霉素200万单位加入500 mL葡萄糖 溶液中给病牛静脉注射,奶牛发生疑似过敏反 应,及时注射盐酸肾上腺素5 mL,并将氟美 松30 mg加入500 mL生理盐水中静脉注射,至 次日患牛恢复正常。
Mechanism of Type I Hypersensitivity
结缔组织型肥大细胞 黏膜型肥大细胞
What is an allergy?
• An allergy is a reaction to an allergen, a substance capable of inducing a hypersensitive reaction in animals. An allergen can be almost any natural or man-made substance in the environment such as grass, pollen, flea saliva, dust, or even fabric.
• The next time your pet comes in contact with this allergen, the antibodies go into hyperaction. They send out signals to the immune system to produce a protein called Immunoglobulin E (IgE) that binds to cells called mast cells in the skin and causes a chemical called histamine to be released.
activation, and then release inflammatory cytokines. • CD8+ T cells-mediated, killing target cells, and mediating inflammation