麻醉药物基因组学研究论文
药物基因组学与阿片类镇痛药物需求个体化的研究进展

药物基因组学与阿片类镇痛药物需求个体化的研究进展药物基因组学是研究药物在个体基因组水平上的表达、变异和相互作用的学科。
随着基因组学研究的不断发展,药物基因组学逐渐成为个体化医学的重要领域之一、阿片类镇痛药物是常用的镇痛药,然而它们的疗效和副作用在不同个体间存在差异。
因此,深入研究药物基因组学与阿片类镇痛药物需求个体化的关系对个体镇痛治疗有重要意义。
研究发现,阿片类镇痛药物的作用主要是通过与μ-阿片受体相互作用来发挥的。
μ-阿片受体是阿片药物的作用靶点,它在不同个体中的表达水平和功能状态可能存在差异,导致个体对阿片类药物的反应不同。
此外,鉴于阿片类药物通过肝脏和肠道被代谢和排泄,药物代谢酶和转运体的多态性也可能对药物的药效和代谢产生影响。
通过药物基因组学研究,可以鉴定与阿片类镇痛药物需求个体化相关的基因多态性。
例如,一些基因多态性会影响阿片类药物在体内的代谢速度,进而影响药物的疗效和副作用。
临床研究表明,CYP2D6基因的多态性可以导致阿片类药物的代谢速度发生改变,从而影响药物的疗效和副作用。
此外,OPRM1基因的变异也会影响个体对阿片类药物的反应,进而影响镇痛效果。
此外,基因多态性还可能与肠道和肝脏中的转运体有关,如P玩家碱泵和乙酰化酶等。
基于药物基因组学研究的结果,可以为个体化阿片类药物治疗提供指导。
根据个体基因型,可以合理选择阿片类药物的种类、剂量和给药间隔,从而提高药物的疗效和减少不良反应。
例如,在一些患者中,由于基因变异导致药物代谢缓慢,应该减少药物剂量或延长给药间隔,以避免药物积聚导致过量和不良反应。
此外,在一些患者中,由于基因变异导致阿片受体的敏感性改变,可以酌情增加药物剂量以获得更好的镇痛效果。
总之,药物基因组学与阿片类镇痛药物需求个体化的研究为个体化阿片类药物治疗提供了重要依据。
通过鉴定与药物代谢和作用相关的基因多态性,可以合理选择药物种类、剂量和给药间隔,优化镇痛效果并减少不良反应。
药物基因组学在临床药学中的应用与研究
药物基因组学在临床药学中的应用与研究研究方案:药物基因组学在临床药学中的应用与研究一、方案内容药物基因组学是将基因组学原理与药物领域相结合,研究药物在个体基因水平上的变化和互作关系。
本研究旨在探索药物基因组学在临床药学中的应用,为临床提供有效的个体化药物治疗方式。
研究方案包括以下几个方面内容:1. 文献回顾与总结通过查阅相关文献,了解目前药物基因组学在临床药学中的应用情况,并对已有文献进行总结和分析,为后续实验或调查提供理论基础。
2. 研究对象和样本采集选择普通人群作为研究对象,采集人口学信息、生物样本等数据。
样本包括外周血、体征相关生化指标等,以便后续对药物基因组学在个体基因水平上的变化进行分析。
3. 基因组测序和分析采用高通量测序技术对研究对象的基因组进行测序,获取其基因变异信息。
通过比对与参考基因组,筛选出具有反映药物代谢、药效等的关键基因位点。
4. 药物敏感基因筛选以药物敏感为标准,根据已有研究成果进行合理的筛选,确定与药物敏感相关的基因位点。
5. 药物基因组学与临床相关性研究根据研究对象的基因组信息和药物敏感基因位点,结合已有的临床数据,对药物基因组学与临床相关性进行统计分析。
探讨个体药物治疗的精确性和有效性。
二、方案实施1. 研究对象选取从平台建立的数据库中选取普通人群作为研究对象。
通过问卷调查和筛选,保证研究对象具有合适的参与条件。
2. 样本采集与处理在符合伦理规范的前提下,采集研究对象的生物样本,包括外周血、体征相关生化指标等。
样本采集后,进行必要的处理和保存,以确保样本的稳定性和可靠性。
3. 基因组测序和分析采用高通量测序技术对研究对象的基因组进行测序,获取其基因变异信息。
利用常用的测序和比对软件,对测序结果进行分析和解读。
4. 药物敏感基因筛选根据已有的研究成果和基因数据,运用统计学方法和生物信息学工具,筛选出与药物敏感相关的基因位点。
5. 药物基因组学与临床相关性分析将基因数据与临床数据相结合,运用统计学方法对药物基因组学与临床相关性进行分析。
浅谈麻醉用药及其药物基因组学研究进展

浅谈麻醉用药及其药物基因组学研究进展摘要】目的临床麻醉中麻醉药及其辅助用药的治疗个体化差异备受关注。
目前,更多的研究在于阐明麻醉药物与转运蛋白、作用靶点和代谢酶的基因多态性之间的关系,并发现麻醉药物的药效学及药动学与相关基因多态性存在密切联系,从而为患者提供更加合理的麻醉用药使其安全平稳的度过手术期。
【关键词】麻醉药物药物基因组学基因多态性研究进展Discussion on clinical anesthesia narcotic drugs advances in Pharmacogenomics research【Abstract】 Clinical anesthesia drug concern and its auxiliary Therapeutics on individual differences of treatment. At present, more research is to clarify the narcotic drugs and transporters, target point and the relationship between gene polymorphism of metabolic enzymes and found the pharmacodynamics and pharmacokinetics of narcotic drugs and related genes polymorphisms exist in close contact, to provide anesthesia for more rational use of drugs for patients spent making it safe and smooth operation.【Key words】Anesthesia drug Pharmacogenomics gene polymorphism Research progress药物基因组学是伴随人类基因组学研究的迅猛发展而开辟的药物遗传学研究的新领域,主要阐明药物代谢、药物转运和药物靶分子的基因多态性及药物作用包括疗效和毒副作用之间关系的学科。
临床药学中的药物基因组学研究
临床药学中的药物基因组学研究标题:临床药学中的药物基因组学研究摘要:药物基因组学旨在通过分析个体的基因组信息,揭示药物与个体之间的相互作用,以实现个体化治疗的目标。
本文就临床药学中的药物基因组学研究展开探讨,包括研究问题及背景、研究方案方法、数据分析和结果呈现、结论与讨论,旨在为临床药学领域的药物个体化治疗提供理论和方法的支持。
1. 研究问题及背景临床药学中,药物个体化治疗是近年来的研究热点。
然而,药物的疗效和不良反应在不同个体中存在巨大的差异。
药物基因组学研究旨在通过分析个体基因变异与药物疗效、药物代谢和药物不良反应之间的关系,寻找临床药学中的个体化治疗策略。
2. 研究方案方法2.1 样本收集通过选择具有典型药物治疗需求的患者作为研究对象,建立大样本的研究队列,并收集其基因组信息、临床特征和药物治疗信息。
2.2 基因分型利用高通量基因检测技术,对样本中的关键基因进行分型,包括药物代谢酶基因、药物靶标基因等。
通过对基因型和表型之间的关联分析,寻找与药物疗效和不良反应相关的基因位点。
2.3 数据整合和分析将基因型、表型等数据进行整合和分析,采用统计学方法探索基因与药物反应之间的关联。
同时,结合个体基因组信息进行药物代谢动力学模拟,预测药物在个体体内的代谢过程和药物浓度变化。
3. 数据分析和结果呈现通过数据分析,识别出与药物疗效和不良反应相关的基因位点和遗传变异。
利用统计学方法评估基因变异对药物效应和代谢的影响,并通过图表等形式展示结果。
4. 结论与讨论4.1 结论药物基因组学研究为个体化药物治疗提供了理论依据,通过分析个体基因组信息,可以预测药物疗效和药物代谢水平,为合理用药提供指导。
4.2 讨论药物基因组学的研究还面临一些挑战,比如数据的获取和整合,以及样本的规模等。
同时,个体基因组信息的隐私和伦理问题也需要重视。
结论:药物基因组学作为临床药学的研究方向,为个体化药物治疗提供了理论和方法的支持。
麻醉领域的个体化用药,药物基因组学(Evan Kharasch)
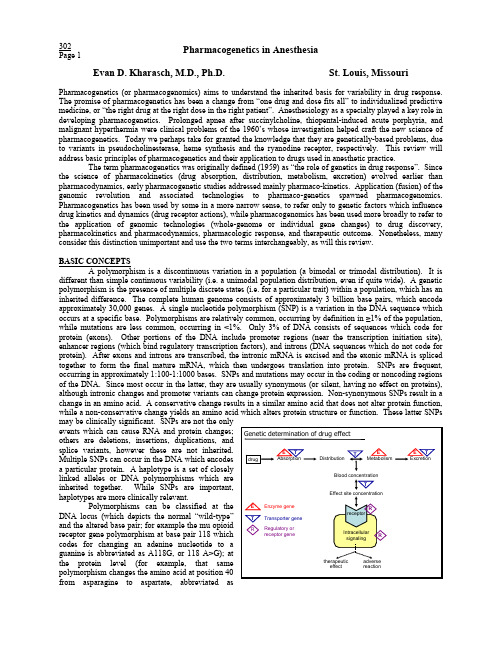
Pharmacogenetics in AnesthesiaEvan D. Kharasch, M.D., Ph.D. St. Louis, Missouri 302 Page 1Pharmacogenetics (or pharmacogenomics) aims to understand the inherited basis for variability in drug response. The promise of pharmacogenetics has been a change from “one drug and dose fits all” to individualized predictive medicine, or “the right drug at the right dose in the right patient”. Anesthesiology as a specialty played a key role in developing pharmacogenetics. Prolonged apnea after succinylcholine, thiopental-induced acute porphyria, and malignant hyperthermia were clinical problems of the 1960’s whose investigation helped craft the new science of pharmacogenetics. Today we perhaps take for granted the knowledge that they are genetically-based problems, due to variants in pseudocholinesterase, heme synthesis and the ryanodine receptor, respectively. This review will address basic principles of pharmacogenetics and their application to drugs used in anesthetic practice.The term pharmacogenetics was originally defined (1959) as “the role of genetics in drug response”. Since the science of pharmacokinetics (drug absorption, distribution, metabolism, excretion) evolved earlier than pharmacodynamics, early pharmacogenetic studies addressed mainly pharmaco-kinetics. Application (fusion) of the genomic revolution and associated technologies to pharmaco-genetics spawned pharmacogenomics. Pharmacogenetics has been used by some in a more narrow sense, to refer only to genetic factors which influence drug kinetics and dynamics (drug receptor actions), while pharmacogenomics has been used more broadly to refer to the application of genomic technologies (whole-genome or individual gene changes) to drug discovery, pharmacokinetics and pharmacodynamics, pharmacologic response, and therapeutic outcome. Nonetheless, many consider this distinction unimportant and use the two terms interchangeably, as will this review.BASIC CONCEPTSA polymorphism is a discontinuous variation in a population (a bimodal or trimodal distribution). It is different than simple continuous variability (i.e. a unimodal population distribution, even if quite wide). A genetic polymorphism is the presence of multiple discrete states (i.e. for a particular trait) within a population, which has an inherited difference. The complete human genome consists of approximately 3 billion base pairs, which encode approximately 30,000 genes. A single nucleotide polymorphism (SNP) is a variation in the DNA sequence which occurs at a specific base. Polymorphisms are relatively common, occurring by definition in ≥1% of the population, while mutations are less common, occurring in <1%. Only 3% of DNA consists of sequences which code for protein (exons). Other portions of the DNA include promoter regions (near the transcription initiation site), enhancer regions (which bind regulatory transcription factors), and introns (DNA sequences which do not code for protein). After exons and introns are transcribed, the intronic mRNA is excised and the exonic mRNA is spliced together to form the final mature mRNA, which then undergoes translation into protein. SNPs are frequent, occurring in approximately 1:100-1:1000 bases. SNPs and mutations may occur in the coding or noncoding regions of the DNA. Since most occur in the latter, they are usually synonymous (or silent, having no effect on proteins), although intronic changes and promoter variants can change protein expression. Non-synonymous SNPs result in a change in an amino acid. A conservative change results in a similar amino acid that does not alter protein function, while a non-conservative change yields an amino acid which alters protein structure or function. These latter SNPs may be clinically significant. SNPs are not the onlyevents which can cause RNA and protein changes; others are deletions, insertions, duplications, andsplice variants, however these are not inherited.Multiple SNPs can occur in the DNA which encodesa particular protein. A haplotype is a set of closely linked alleles or DNA polymorphisms which are inherited together. While SNPs are important, haplotypes are more clinically relevant.Polymorphisms can be classified at the DNA locus (which depicts the normal “wild-type” and the altered base pair; for example the mu opioid receptor gene polymorphism at base pair 118 which codes for changing an adenine nucleotide to aguanine is abbreviated as A118G, or 118 A>G); atpolymorphism changes the amino acid at position 40Asn40Asp); or at the allele level of whole gene or protein (for example, the second variant of the wild-type P450 (CYP) enzyme CYP2C9*1, is CYP2C9*3). Individuals may be homozygous or heterozygous for a particular allele (i.e. CYP2C9*1/*1 or CYP2C9*1/*3). Typically, function is altered more in homozygotes than in heterozygotes. APPLIED CONCEPTSPharmacogenetic variability may influence drug disposition, drug transport, receptor structure and function, cell signaling, and the myriad of downstream responses which ultimately produce a therapeutic effect or adverse reaction. The figure schematically depicts the role of genes in determining drug pharmacokinetics and pharmaco-dynamics. It is important to remember that causes of interindividual variability include genetics, as well as age, disease, environment (diet, smoking, ethanol), and interactions with drugs and herbals.1. PharmacokineticsThis section will focus on the polymorphic proteins responsible for human drug disposition, and the role of genetic variability in metabolism and response. Although transport proteins do not catalyze metabolism per se, they influence drug absorption and bioavailability, act in concert with enzymes of biotransformation, and influence effect site concentrations, and will be discussed in this section.1A. MetabolismMetabolism converts lipophilic (fat soluble) drugs to more polar (water soluble) molecules more amenable to excretion. Phase I reactions introduce or uncover a functional group that increases drug polarity and prepares it for a Phase II reaction. Phase II reactions link the drug or metabolite with a highly polar molecule which renders the conjugate water soluble and thus excreted. Although considered mainly as a route of drug inactivation, phase I and II reactions can convert an inactive prodrug to an active metabolite (i.e. oxidation of inactive codeine to the more active metabolite morphine); an active drug to an active metabolite (morphine conversion to morphine-6-glucuronide); an active drug to an inactive metabolite (morphine to normorphine); or an active drug to a toxic metabolite (meperidine to normeperidine, which can cause seizures).Phase I EnzymesCytochrome P450 (CYP): CYPs are a superfamily of drug metabolizing enzymes. The individual CYPs are classified according to their sequence evolution. CYPs that share >40% sequence homology are grouped in a family (designated by an Arabic number, i.e. CYP2), those with >55% homology are grouped in a subfamily (designated by a letter, i.e. CYP2A), and individual CYPs are identified by a third number (i.e. CYP2A6). Allelic variants are designated by an asterisk and number following the protein identifier (i.e. CYP2A6*1). The majority of drugs are metabolized in humans by CYPs 1, 2 and 3 (mainly CYPs 2C, 2D6 and 3A). Some, but not all P450s exhibit pharmacogenetic variability.CYP2B6: CYP2B6 is expressed mainly in liver; also in intestine, brain and kidney. Initially considered to be expressed in only some individuals (~20%), in very low levels, and thus not important, CYP2B6 is now known to be expressed in greater amounts, in all/most individuals, and metabolizes many drugs. It is the main enzyme responsible for methadone N-demethylation, propofol hydroxylation, and (R)- and (S)-ketamine N-demethylation. Many drugs thought previously to be metabolized mainly by CYP3A, may instead (or also) be metabolized by CYP2B6. CYP2B6 is one of the most polymorphic CYPs, with several mutations occurring with high frequency, particularly in African-Americans, one of which results in low CYP2B6 activity.CYP2C: The human CYP2C gene family consists of CYPs 2C8, 2C9, 2C18 and 2C19, which together account for ~one-fourth of total hepatic CYP and metabolizing 15-20% of all therapeutic drugs. The pharmacogenetically most important CYP2C enzymes are 2C9 and 2C19. Others (CYP2C8, CYP2C18) are expressed in low levels or have narrow substrate specificities, and are not polymorphically expressed.CYP2C9 is the major 2C isoform in human liver. The best known CYP2C9 substrates are (S)-warfarin, phenytoin, tolbutamide, diclofenac, and several NSAIDs. Several variant 2C9 proteins with substantially decreased activity (as low as one-fifth) have been identified. The frequency of these mutant alleles occurs more commonly in Caucasians (10-20%) than in Asians and African-Americans (<5%). Homozygotes (CYP2C9*3/*3) have very low enzyme activity (1/10 of normal) while heterozygotes (*1/*3, *2/*3 ) have moderately reduced activity (1/3-2/3 of normal) compared with wild-types (*1/*1), with correspondingly reduced clearances. Warfarin is an excellent example of pharmacogenetics and its application in modern therapeutics. Patients with CYP2C9 variants havehigher warfarin plasma concentrations, and are more susceptible to over-anticoagulation, serious or life-threatening bleeding complications, and longer hospitalizations. CYP2C9 genotyping, and correspondingly adjusted doses for CYP2C9 variants, results in more rapid attainment of proper anticoagulation, and fewer complications.CYP2C19 is a minor P450, but has been well-studied since it was one of the early CYPs for which a genetic polymorphism was identified. The prototype 2C19 reaction is S-mephenytoin hydroxylation; genetic variability was initially termed the mephenytoin polymorphism. Other substrates include barbiturates (R-mephobarbital, hexobarbital) and diazepam. Individuals are classified as extensive (EM) or poor (PM) metabolizers of S-mephenytoin, with a PM frequency of 2-5% in Caucasians, 2% in African-Americans, 18-23% in Japanese, and 15-17% in Chinese. PM is caused by an autosomal recessive mutation, and PMs do not express CYP2C19. The CYP2C19 polymorphism is important in the disposition and clinical effect of diazepam, particularly PM homozygotes. Diazepam clearance in PM is half that in EM, with dose requirements correspondingly less, and heterozygotes are intermediate. This is thought to account for lower diazepam dose requirements in Chinese.CYP2D6 metabolizes ~25% of all drugs, even though it accounts for only 2-5% of total human liver P450. It is also of historical significance, being the first identified CYP genetic polymorphism, termed the “debrisoquine/sparteine polymorphism”. The list of CYP2D6 substrates is notable for a group of opioids which undergo CYP2D6-mediated O-demethylation (codeine, dextromethorphan, dihydrocodeine, hydrocodone, oxycodone, tramadol), beta-blockers (alprenolol, bufurolol, labetolol, metoprolol, propranolol, timolol) as well as various antiarrhythmics, antipsychotics, tricyclic anti-depressants, serotonin reuptake inhibitors. and antiemetic 5-HT3 antagonists. The debrisoquine/sparteine phenotype is an autosomal recessive monogenic trait. Patients are extensive (EM, wildtype), poor (PM), or ultrarapid (UM) metabolizers. The overall PM frequency is 7-8% in Caucasians, 2% in African-Americans, and <1% in Asians. Over 20 mutant CYP2D6 alleles have been identified. Most code for inactive proteins, and homozygotes are PM. Some alleles, however, which are particularly frequent in Asians, code for a protein with reduced activity. UM are caused by gene duplication, with up to 13 copies. UMs (20% Ethiopians, 7% Spanish, 1% Scandinavians) generally require substantially higher drug doses. There is even a spectrum of CYP2D6 activity within the EMs, owing to the diversity of 2D6 alleles. Commercial assays are now available which allow for accurate CYP2D6 genotyping.The role of pharmacogenetics in interindividual variability in drug disposition and response is well illustrated by codeine, a prodrug requiring CYP2D6-mediated metabolic activation (O-demethylation) to the mu agonist morphine, and even greater bioactivation to the more potent agonist morphine-6-glucuronide. CYP2D6 deficient individuals (PMs) are poor metabolizers of codeine, have markedly diminished or absent morphine formation, and minimal if any analgesia. Conversely, individuals with CYP2D6 gene amplification and/or duplication (UM) have greater morphine formation from codeine than extensive metabolizers and poor metabolizers. Ethnic variations attributable to codeine biotransformation have also been observed. For example, Chinese produced less morphine from codeine, were less sensitive to the opioid effects of codeine, and might therefore experience reduced analgesia.CYP3A: The CYP3A family metabolizes >50% of all therapeutic drugs. In adults it is comprised of CYP3A4 (which exhibits wide variability in activity but no genetic polymorphism) and the polymorphically expressed CYP3A5. CYP3A4 is the most quantitatively abundant CYP in human liver, accounting for ~30% (but as much as 60%) of total CYP. It is also the predominant CYP in human intestine. It exhibits the broadest substrate specificity of all CYPs, including opioids, benzodiazepines, local anesthetics, calcium channel antagonists, and immunosuppressants.CYP3A5 is similar to CYP3A4, and metabolizes many but not all CYP3A4 substrates, often with diminished activity. Hepatic CYP3A5 is polymorphically expressed, and was once thought present in only 25% of human livers and at lower levels than CYP3A4. However, more recent studies suggest that hepatic CYP3A5 expression is more frequent, occurs at a higher level, and is more contributory to the metabolism of certain CYP3A substrates than previously appreciated. CYP3A5 may account for >50% of CYP3A in some livers. Individuals expressing CYP3A5 along with 3A4 may have greater metabolism of CYP3A drugs. CYP3A5 is also polymorphically expressed in intestine, although levels are less than CYP3A4. The clinical role of polymorphic CYP3A5 expression is under investigation.Non-P450 EnzymesCarboxylesterases have a wide tissue distribution, found in greatest amounts in the liver, and also in the gastrointestinal tract, brain, and possibly blood. They have a nonselective substrate specificity, and hydrolyze estersand amides. Two broad-substrate human liver microsomal carboxylesterases have been isolated (hCE-1 and -2). hCE-1 catalyzes the hydrolysis of cocaine to benzoylecgonine, the hydrolysis of meperidine to meperidinic acid (the major route of metabolism), and the hydrolysis of heroin (3,6-diacetylmorphine) to 6-monoacetylmorphine, the active metabolite. hCE-02 also hydrolyzes heroin to both 6-monoacetylmorphine and then to morphine. It also catalyzes the bioactivation of the anticancer drug irinotecan into its active metabolite. There are numerous polymorphisms in the hCE-02 gene, however none result in altered enzyme activity.One major human cholinesterase is plasma cholinesterase (also known as pseudocholinesterase, serum cholinesterase, butyrylcholine esterase, and nonspecific cholinesterase), found in plasma as well as liver and other tissues. Plasma cholinesterase was one of the early enzymes for which pharmacogenetic variation was elucidated, based on observed heritable variability in the response to succinylcholine. A single autosomal locus is responsible for all plasma cholinesterase variants. Plasma cholinesterase activity is evaluating by its inhibition by dibucaine. The dibucaine number is the percent inhibition; normal is 71-85, intermediate ~60, and atypical ~20. The activity of atypical cholinesterase is decreased by 70%, homozygotes are very sensitive to succinylcholine, and the frequency of this variant is about 2%. Another method for evaluating activity is inhibition by fluoride, which typically parallels dibucaine inhibition. A small number of patients (0.3%), however, express a fluoride-resistant enzyme whose activity is decreased by 60%, and who are moderately sensitive to succinylcholine. Patients with the silent variant (0.03%) have no enzyme activity. Succinylcholine hydrolysis is rapid (90% within one minute) and robust (70% reduction in enzyme activity only moderately prolongs neuromuscular blockade). Mivacurium is also hydrolyzed by plasma cholinesterase, at a rate 70-90% of that of succinylcholine. Patients with cholinesterase variants respond similarly to mivacurium and succinylcholine. Recovery of neuromuscular function can be prolonged up to 60-fold in atypical cholinesterase homozygotes. Plasma cholinesterase also metabolizes the three ester local anesthetics cocaine, procaine and chloroprocaine. Heroin undergoes extensive deacetylation in blood to 6-monoacetylmorphine, and then to morphine. The former reaction is catalyzed rapidly by plasma cholinesterase, and more slowly by erythrocyte AchE (see below), although the latter reaction accounts for most hydrolysis in vivo and only erythrocyte AchE can convert 6-monoacetylmorphine to morphine.A second major human cholinesterase is acetylcholinesterase (AChE). The major function of AChE is to hydrolyze acetylcholine at the neuromuscular junction thereby terminating synaptic transmission. However there are two other AChE forms, in erythrocytes and the brain. Like succinylcholine, esmolol and remifentanil, also undergo extensive metabolic inactivation in blood. However their metabolism is catalyzed exclusively by erythrocyte AchE, and plasma cholinesterase has no catalytic activity. Hence neither remifentanil nor esmolol elimination are altered by pseudocholinesterase deficiency.Phase II EnzymesGlucuronosyltransferase: The glucuronosyltransferases (UGT) catalyze addition of glucuronic acid to lipophilic compounds to form water soluble metabolites which are rapidly excreted. Glucuronides may be more or less pharmacologically active than their parent drugs. Human UGTs are broadly classified into the UGT1A (phenol/bilirubin) and UGT2 (steroid/bile) families. Humans express UGT1As which glucuronidate endogenous compounds and many drugs (phenols, amines, anthraquinones, flavones), and UGT2s which glucuronidate endogenous compounds and a few drugs. There are several polymorphisms in the UGT1A family, most notably in UGT1A1, which results in much lower enzyme activity and mild hyperbilirubinemia (Gilbert's syndrome). Glucuronidation is an important pathway for certain drugs used in anesthesia. Propofol glucuronidation by human UGT1A9 is the major route of systemic elimination. UGT2B7 glucuronidates many opioids such as morphine, codeine, naloxone, nalorphine, buprenorphine, oxymorphone, and hydromorphone. Morphine 6-glucuronidation is important since this metabolite is more potent than its parent drug, is thought to play a significant role in morphine analgesia, and the finding of UGT2B7 in human brain suggests that in situ formation of this metabolite may play a role in analgesia. The glucuronide of 1-hydroxymidazolam is pharmacologically active, is renally excreted, and is thought to underlie the prolonged effects of midazolam in patients with renal insufficiency when used for ICU sedation. The role of UGT polymorphisms in anesthetic metabolism and response are unknown.Glutathione-S-transferase: Glutathione-S-transferases (GST) catalyze the reaction of the tripeptide glutathione with a diverse array of drugs and toxins, and are primarily a defensive system for detoxification. There isconsiderable polymorphism in GST expression, however this enzyme is of little relevance to anesthesia (except in the metabolism of the sevoflurane degradation product ‘compound A’).N-acetyl-transferase: N-Acetylation by N-acetyl-transferases (NAT1 & NAT2) is a common Phase II reaction, and can result in drug inactivation (isonizaid), an active therapeutic metabolite (N-acetylprocainamide) or an active toxic metabolite (carcinogens). NAT is of great historical significance, since it was the first drug metabolizing enzyme for which a genetic polymorphism was discovered (fast- and slow isoniazid N-acetylation). Slow acetylators show a greater therapeutic response than fast acetylators to several drugs (i.e. isoniazid, hydralazine, dapsone), and the latter group may require a greater dose. In contrast, slow acetylators may be more susceptible to the side effects of drugs mediated by acetylated metabolites, such as isoniazid hepatotoxicity and lupus-like syndrome after hydralazine or procainamide. There are NAT1 polymorphisms, but NAT2 polymorphisms cause the slow-acetylator phenotype (50-60% in Caucasians, 40% in African-Americans, 20% in Chinese, 8% in Japanese.1B Transport ProteinsP-glycoprotein (P-gp) is a plasma membrane efflux pump that actively transports a structurally diverse array of compounds out of the interior of several cell types. It is also known as the multidrug resistance protein (MDR1) because it was first associated with cancer cell resistance. P-gp is expressed on the apical (luminal) surface of epithelial cells, including the brush border of intestinal cells, hepatocyte biliary canalicular cell membranes, and the luminal surface of renal proximal tubular cells. In the gut, it actively pumps drugs from the intracellular milieu against a concentration gradient back into the intestinal lumen, actively countering intestinal drug absorption, and thereby limiting oral drug absorption. P-gp plays a major role in the intestinal absorption, first-pass elimination, and bioavailability of many drugs. P-gp is also expressed on the luminal surface of brain capillary endothelial cells, where it is an intrinsic part of the blood brain barrier and limits CNS access of drugs. Thus P-gp can be a major determinant of drug pharmacodynamics. There is considerable interindividual variability in human P-gp expression, and numerous polymorphisms and haplotypes in humans have been identified.Of particular potential significance in anesthesia is that opioids may be substrates for P-gp, both in the intestine and the brain. Morphine, the best-characterized opioid, is extruded by P-gp in blood-brain barrier brain capillary endothelial cells in rodents, actively limiting morphine access to the CNS. Alfentanil is also thought to be a brain P-gp substrate in rodents. Although P-gp is a major determinant of analgesic opioid CNS access and analgesia in animals, its role in humans is presently unknown. The role of P-gp polymorphisms in anesthetic transport and response is also unknown.A second subfamily of transporters are the multidrug resistance-associated proteins, also known as the multispecific organic anion transporter. The first protein to be discovered in this family was MRP1, whose overexpression is responsible for the majority of non-P-gp mediated multidrug resistance. Because MRPs were only recently discovered, little is known about their significance in anesthetic transport and clinical effects.2. PharmacodynamicsPharmacodynamic polymorphisms are generally attributable to variants in cell surface receptors or intracellular signaling pathways Compared with genetic influences on drug disposition, less information is currently available about genetic influences on pharmacodynamics. There are however several notable examples. Malignant hyperthermia is due to polymorphism in the skeletal muscle calcium release channel (ryanodine receptor) gene.Of considerable interest in anesthesiology is the occurrence and potentialA clinical significance in opioid receptor polymorphisms. The best studied SNP is the A118G mu opioid receptor polymorphism. Nevertheless, it is a confusing picture. Some but not all studies show decreased A118G mu receptor affinity for ß-endorphin and morphine. Some have shown a 2- to 3 fold decrease in the potency of morphine and morphine-6-glucuronide, while others have shown no difference. Some have shown a 1.5 to 2-fold increase in postop morphine PCA requirements in A118G homozygotes (but not heterozygotes), while othes suggest no major difference. If there is a major difference among A118G carriers, it is small.Several nonsynonymous polymorphisms in adrenergic receptors have been identified, although their functional significance awaits full determination. Some ß-adrenergic receptor polymorphisms have been implicated in the response to asthma therapy, and speculated to be involved in the response to drugs used for hypertension and congestive heart failure.SummaryPharmacogenetics is a rapidly evolving science. Genetic polymorphisms have been identified which alter drug metabolism, bioavailability, clearance, receptor binding, clinical effect, and toxicity. The ultimate clinical utility and cost-effectiveness of pharmacogenetic testing remains to be determined.ReferencesA. General references on pharmacogenetics1.Dervieux T: Pharmacogenetic testing: proofs of principle and pharmacoeconomic implications. Mutat Res2005;573:180-942.Lesko LJ, Woodcock J: Translation of pharmacogenomics and pharmacogenetics: a regulatory perspective. NatRev Drug Discov 2004;3:763-93.Ma JD: Genetic polymorphisms of cytochrome P450 enzymes and the effect on interindividual,pharmacokinetic variability in extensive metabolizers. J Clin Pharmacology 2004;44:447-564.Wilkinson GR: Drug metabolism and variability among patients in drug response. N Engl J Med 2005; 352:2211-215.Need AC: Priorities and standards in pharmacogenetic research. Nat Genet 2005; 37: 671-816.Williams JA: So many studies, too few subjects: establishing functional relevance of genetic polymorphisms onpharmacokinetics. J Clin Pharmacol 2006; 46: 258-647.Leschziner GD: ABCB1 genotype and PGP expression, function and therapeutic drug response: a criticalreview and recommendations for future research. Pharmacogenomics J 2007; 7: 154-79B. Pharmacogenetics and anesthesia8.Belfer I: Candidate gene studies of human pain mechanisms: methods for optimizing choice of polymorphismsand sample size. Anesthesiology 2004; 100:1562-72.9.Bukaveckas BL: Pharmacogenetics as related to the practice of cardiothoracic and vascular anesthesia. JCardiothorac Vasc Anesth 2004;18:353-65.10.Freeman BD: Challenges of implementing pharmacogenetics in the critical care environment. Nat Rev DrugDiscov 2004; 3: 88-9311.Iohom G: Principles of pharmacogenetics--implications for the anaesthetist. Br J Anaesth 2004; 93:440-5012.Palmer SN: Pharmacogenetics of anesthetic and analgesic agents. Anesthesiology 2005;102:663-7113.Zaugg M: Genetic modulation of adrenergic activity in the heart and vasculature: implications for perioperativemedicine. Anesthesiology 2005; 102:429-4614.Ziegeler S: Influence of genotype on perioperative risk and outcome. Anesthesiology 2003;99:212-915.Samer CF: Individualizing analgesic prescription Part I: pharmacogenetics of opioid analgesics. PersonalizedMedicine 2006; 3: 239-6916.Lötsch J: Current evidence for a genetic modulation of the response to analgesics. Pain 2006; 121: 1-517.Kharasch ED: Influence of CYP3A5 genotype on the pharmacokinetics and pharmacodynamics of alfentaniland midazolam. Clin Pharmacol Ther. 2007 in pressC. WebsitesGlossary of Genetic Terms /10002096AMA overview /ama/pub/category/2306.htmlNCBI pharmacogenomic primer /about/primer/pharm.htmlHuman Genome Project /sci/techresources/Human_Genome/home.shtml Haplotype map (HapMap) project /NIH pharmacogenetics research network http://www.nigms。
药物基因组学在临床用药决策中的实践研究
药物基因组学在临床用药决策中的实践研究1.引言药物基因组学是研究个体基因对药物代谢、药效和毒性反应等影响的学科,其发展为临床用药决策提供了重要的依据。
随着基因测序技术的进步和生物信息学的发展,药物基因组学成为临床医学中一个备受关注的领域。
本文将重点探讨药物基因组学在临床用药决策中的实践研究。
2.药物基因组学的理论基础药物基因组学的理论基础主要包括药物代谢酶基因的遗传多态性、药物靶点基因的遗传变异、药物相互作用相关基因等。
药物代谢酶基因的遗传多态性导致个体对药物代谢速率的差异,从而影响药物的疗效和毒性反应。
药物靶点基因的遗传变异会影响药物的结合能力和作用效果。
而药物相互作用相关基因则是影响药物在体内代谢时相互作用的基因。
3.药物基因组学在药物选择上的应用药物基因组学在药物选择上的应用主要包括以下几个方面:(1)基因型对药物代谢的影响:通过检测患者的药物代谢酶基因型,可以明确患者对某些药物的代谢速率,从而选择更合适的药物剂量;(2)个体基因变异对药物疗效的影响:一些药物的疗效会受到个体基因的影响,因此在选择药物时需要考虑个体的遗传变异情况;(3)个体基因变异对药物毒性反应的影响:有些药物在一些个体中会引发严重的毒性反应,而在另一些个体中则不会,这与个体基因的变异有关,因此在用药时需要根据患者的基因型进行评估。
4.药物基因组学在药物调整上的应用药物基因组学在药物调整上的应用主要包括以下几个方面:(1)基因型对药物剂量的调整:根据患者的基因型,可以确定合适的药物剂量,避免药物过量或过少导致的不良反应;(2)基因型对药物疗效和毒性反应的监测:监测患者的基因型,可以及时发现药物疗效不佳或毒性反应增加的情况,及时调整药物治疗方案;(3)基因型对药物相互作用的监测:一些药物在体内会相互作用,影响药物的代谢和效果,因此需要根据患者基因型对药物相互作用进行监测。
5.实践研究中的挑战和未来发展药物基因组学在临床用药决策中的实践研究面临一些挑战,如基因检测技术的标准化、数据解释的一致性、社会伦理等方面的问题。
麻醉药物基因组学研究论文
麻醉药物基因组学研究论文近年来,基因组学已经成为临床医学研究的重要领域之一。
在医学研究中,基因组学的应用可以帮助我们更好地理解疾病的发病机制,并且为临床诊疗提供指导。
在此背景下,麻醉药物基因组学研究逐渐受到研究者们的关注。
麻醉药物基因组学研究,旨在通过研究患者体内的基因型信息和药物代谢酶等代谢酶的表达情况,为临床麻醉药物剂量和种类的选择提供帮助,从而提高麻醉安全性、减少术后并发症的发生率。
首先,我们需要了解一下基因组学中的一些基本概念。
人类基因组由数千万个碱基对组成,这些碱基对构成了基因的DNA序列。
每个人都会在其DNA序列中携带着数百万个不同的基因型,其中包括一部分影响药物代谢酶水平的基因。
这些基因可以影响机体对于麻醉药物的代谢速率和药效,进而影响药物在体内的清除速度和药效持续时间。
因此,我们可以理解为,这部分基因决定了每个人对同一剂量药物的反应差异。
近年来的研究发现,同样剂量的麻醉药物在不同人的体内代谢速率不同,导致药效差异很大。
这样,对于既要满足药效,又要避免副作用发生的复杂需求下,麻醉剂量选择不得不更具针对性。
因此,我们需要进行基因表达分析,找到与麻醉药物代谢相关的基因,以此来选择最合适的药物剂量。
例如,一项名为“Genome-wide association study of intraoperative awareness risk in ~80000 Veterans Administration patients implicates genetic variants in the beta 2 subunit of thenicotinic acetylcholine receptor”(J Anesth. 2015)的研究就尝试从基因层面分析围手术期患者的清醒风险。
这项研究对来自美国退伍军人局的80,000名患者进行了全基因组关联分析,用于评估基因与麻醉遗忘和清醒之间的关联。
基因组学在药物方面的研究进展
基因组学在药物方面的研究进展摘要:药物基因组学可以说是基因功能学与分子药理学的有机结合,在很多方面这种结合是非常必要的。
药物基因组学区别于一般意义上的基因学,它不是以发现人体基因组基因为主要目的,而是相对简单地运用已知的基因理论改善病人的治疗。
也可以这么说,药物基因组学以药物效应及安全性为目标,研究各种基因突变与药效及安全性的关系[1]。
正因为药物基因组学是研究基因序列变异及其对药物不同反应的科学,所以它是研究高效、特效药物的重要途径,通过它为患者或者特定人群寻找合适的药物,药物基因组学强调个体化;因人制宜,有重要的理论意义和广阔的应用前景。
关键词:基因组学;药物;进展;基因多态性;SNP概述:同一种药物对患有相同疾病的不同患者疗效不同是临床上常见的一种现象,以往的观点认为这是由于药代动力学的差异造成的。
最近的研究表明,药效学原因所产生的差异更为广泛和显著,而药效学差异大多源于基因的差异。
为此,提出了“药物基因组学”这个全新的概念[2]。
药物基因组学以基因多态性为基础,而基因多态性是指群体中正常个体的基因在相同位置上存在差别(如单碱基差别,或单基因、多基因以及重复序列数目的差别),这种差别出现的频率大于1%。
药物基因组学研究药物效应的个体间差异,针对不同个体基因型进行个性化治疗。
其研究内容包括药物效应的基因型预测和基因组学在医药上的应用,在分子水平上证明和阐述药物疗效、药物作用的靶位、作用模式和毒副作用[3]。
药物基因组学不是以发现新的基因和探索疾病的发生机理为主要目标,而是以探讨药物作用的遗传分布,确定药物作用靶点来满足临床上最佳的药物效应及安全性为目标。
药物基因组学除了具有药物遗传学研究的遗传多样性引起对药物或有毒物质反应的差异外,还研究基因多样性与药效的关系,以及个体差异与同种药物不同作用靶点的关系等[4]。
药物基因组学涉及的研究大体可分为个阶段:首先检测一些候选基因,寻找等位缺失以及造成的生物学后果;其次借助现有分子遗传学等技术,同时进行更多候选基因的研究;最后进行基因组水平的关联分析[5]。
与麻醉相关的基因研究
与麻醉药物作用相关的基因及基因表达调控因子何艳2011106 皖南医学院随着人类全基因测序工作的完成,特别是药物基因组学的发展,越来越多的研究发现不同人种及个体间由于基因变异而导致药物的效能异常,进而影响麻醉药物的作用。
由于基因的多态性,导致不同人群及个体对相同药物产生不同的反应。
本文对目前某些基因与麻醉的相互作用做综述如下。
1.阿片受体 (MOR)的相关基因MOR是与Gi蛋白耦联的受体,其细胞内途径是通过兴奋Gj,抑制腺苷酸环化酶,使cAMP合成减少。
目前已知MOR基因有多个突变位点,与镇痛相关的有N40D、R260H、R265H和$268P。
最早报道的突变是 s268P(T802C),使受体产生脱敏及G蛋白耦联信号减弱,导致吗啡和B一内啡肽的作用强度大大下降,不过此突变频率比较低(<1%)。
而AI18G(N40D)突变则是最常见的,I临床资料显示带有Gl18等位基因的患者阿片类的镇痛作用明显下降[1]。
也有资料发现Gl 18等位基因的携带者在M6G所致的困倦、呼吸抑制等副作用也较Al18等位基因的携带者轻[2]。
然而,最近Romberg等[3]用健康志愿者实验认为G1 18突变只降低阿片药物的镇痛作用,但不减轻其困倦、呼吸抑制、恶性、呕吐等副作用。
故MOR基因Gl18突变降低阿片类药物的镇痛作用已形成共识,但对是否减轻阿片药物的副作用仍存争论。
有些MOR基因的变异与药瘾形成有关,Szeto等在华人海洛因成瘾者中发现C17T联同AII8G、C691G 变异的频率较非药瘾者要高。
在印度的海洛因成瘾者中也发现A1 18G的频率明显比对照组高[1]。
2.RYR1(Ryanodine receptor)RYR1基因表达骨骼肌肌浆网膜上的电压门控钙离子通道的主要部分,此部分是促使钙离子释放引起骨骼肌收缩的关键结构,它的变异是临床发生恶性高热(malignant hyperthermia MH)的根本原因,至今已发现超过50个不同的RYR1基因突变位点,认为可能跟发生MH有关[4]。
药物基因组学在精准医疗中的应用与挑战

药物基因组学在精准医疗中的应用与挑战摘要:药物基因组学是一种将基因组学知识应用于药物治疗个体化的新兴学科,为精准医疗的发展提供了重要支持。
本文旨在探讨药物基因组学在精准医疗中的应用和挑战,分析其在个体化用药、疾病治疗、药物研发等方面的意义和局限性,并展望其未来发展趋势。
关键词:药物基因组学,精准医疗,个体化用药,疾病治疗,药物研发一、介绍药物基因组学是研究基因和药物相互作用的学科,旨在揭示个体基因变异对药物反应的影响,实现药物治疗的个体化和精准化。
随着基因组学技术的发展和成本的降低,药物基因组学逐渐成为精准医疗的重要组成部分。
本文将探讨药物基因组学在精准医疗中的应用与挑战,旨在深入探讨其意义和发展前景。
二、药物基因组学在精准医疗中的应用1.个体化用药药物基因组学通过分析个体的基因型和表现型,可以预测个体对特定药物的代谢情况、疗效和毒副作用。
例如,CYP2D6和CYP2C19等基因在药物代谢中发挥重要作用,个体对这些基因的变异可能导致药物疗效和安全性的差异。
通过对这些基因进行检测和分析,可以实现个体化用药,为患者选择最适合的治疗方案,提高治疗效果并减少不良反应。
2.疾病治疗药物基因组学还可以帮助医生确定患者的疾病风险和治疗方案。
例如,某些基因变异可能增加患某种疾病的风险,通过检测这些基因变异,可以及早发现高风险人群并采取预防措施。
同时,药物基因组学也可以指导疾病治疗方案的选择,个体化用药可以提高治疗效果,减少治疗时间和剂量,并减少不必要的药物试验。
3.药物研发药物基因组学在药物研发领域也发挥着重要作用。
通过研究基因变异对药物反应的影响,可以设计更具靶向性和个体化的药物,提高新药的疗效和安全性。
同时,药物基因组学还可以帮助研究人员预测药物的药代动力学和药效动力学,加快药物的开发速度和降低开发成本。
三、药物基因组学在精准医疗中的挑战1.技术挑战药物基因组学依赖于高通量测序技术和生物信息学分析工具,这些技术的发展和应用仍存在一些挑战。
药物基因组学在临床药学中的应用与实践
药物基因组学在临床药学中的应用与实践引言药物基因组学作为一门新兴的交叉学科,在临床药学中扮演着越来越重要的角色。
通过研究患者基因变异对药物代谢、疗效和不良反应的影响,药物基因组学为个体化药物治疗提供了重要依据,促进了临床药学的发展。
本文将探讨药物基因组学在临床药学中的应用及实践,以期为未来的临床药物治疗提供指导。
药物基因组学的基本原理药物基因组学是研究基因对药物代谢、疗效和不良反应的影响的学科,其基本原理是个体的遗传变异会影响其对药物的反应。
这些遗传变异可能包括单核苷酸多态性(SNPs)、基因重复、基因突变等。
这些变异会导致药物在体内的代谢途径发生改变,从而影响药物的疗效和安全性。
药物基因组学在临床药学中的应用1. 个体化用药药物基因组学为个体化用药提供了理论基础。
通过分析患者的遗传变异信息,医生可以根据患者的基因型来选择最适合的药物种类和剂量,从而提高治疗效果,减少不良反应。
例如,对于华法林这种存在明确基因药代动力学联系的药物,根据患者的CYP2C9和VKORC1基因型可以调整剂量,减少出血风险。
2. 药物安全性评估药物基因组学可以帮助评估药物的安全性。
某些基因型会使个体对某些药物产生不良反应,例如药物代谢酶基因CYP2D6的多态性会影响抗抑郁药帕罗西汀的代谢,从而引起毒性反应。
通过对患者基因型的检测,可以预测患者对某些药物的代谢情况,从而提前预防不良反应的发生。
3. 药物疗效评估药物基因组学也可以帮助评估药物的疗效。
有些药物的疗效受到基因型的影响,例如抗癫痫药卡马西平对CYP2C9基因型为突变型的患者的疗效较差。
通过对患者基因型的分析,可以预测患者对某些药物的疗效,从而选择更有效的治疗方案。
4. 药物开发药物基因组学也在药物研发领域得到广泛应用。
通过研究患者基因型和药物反应之间的关系,可以帮助制药公司设计更有效的药物,减少不良反应的发生。
例如,对于HER2阳性乳腺癌患者,靶向药曲妥珠单抗可以提高疗效,而对于HER2阴性患者则无效,基因检测可以准确筛选患者,提高治疗效果。
药物基因组学对个体化用药影响的研究现状探讨论文

药物基因组学对个体化用药影响的研究现状探讨论文药物基因组学对个体化用药影响的研究现状探讨论文药物基因组学(pharmacogenomics)又称为基因组药理学或基因组药物学,主要研究基因组或基因变异对药物在人体内吸收、代谢、疗效及不良反应产生的影响及其作用机制,进而更好地指导新药研发及合理用药,它是药理学或基因组学一个重要的分支。
药物基因组学的提出为个体化用药提供了坚实的理论基础和明确的发展方向。
1 药物基因组学的发展现状药物基因组学是建立在药物遗传学基础上发展起来的新兴学科。
通过对患者个体基因型(genotype)的识别预测药物反应的表型(phenotype),从而达到个性化治疗的目的。
而新的疾病基因的发现将会提供新的药物靶点。
药物基因组学通过研究影响药物代谢等个体差异的基因特性,以及基因变异所导致的患者对药物的反应,提高药物的疗效及安全性。
为开发新药、指导合理用药、提高药效、减少不良反应、降低开发成本提供信息平台,进而提高各种疾病的临床治疗质量。
2 个体化治疗的意义任何药物都具备两重性,既能“治病”,也能“致病”。
而且,在很多情况下,最佳用药剂量对于每个个体也是不同的。
由于用药过量带来的不良反应及用药不足导致的疗效欠佳都是治疗失败的重要原因。
个体化用药是要充分、全面地考虑每个患者的遗传因素(药物代谢基因类型)、身体因素(性别、年龄、体质量)、病情因素(病理生理特征、正在服用的其他药物)等基础上,综合制定全面、安全、合理、有效、经济的药物治疗方案。
遵循“以人为本、因人而异”的原则,予以“适当的患者,适当的给药,适当的.剂量和适当的时间”,才能充分发挥药物的效应,减少不良反应及降低医疗费用。
据世界卫生组织统计结果显示,全球约有三分之一的患者由于不合理用药导致死亡。
因而,推行个体化用药不仅势在必行,而且迫在眉睫。
3 药物基因组学与个性化治疗合理用药的核心是个体化给药,目前最主要的方法是:测定药物的体液浓度,以药代动力学原理计算药代动力学参数,设计个体化给药方案,这对于血药浓度与药效相一致的药物是可行的,但对于血药浓度与药效不一致的药物,如何达到个体化给药,目前并没有比较可靠的方法。
基于药物基因组学的药物设计研究
基于药物基因组学的药物设计研究随着科技的飞速发展以及对医学的不断研究,药物基因组学已成为一项热门的医学研究领域。
使用药物基因组学技术可以为设计个性化的治疗方案提供重要的依据。
药物基因组学研究是将基因组信息,包括基因表达和DNA序列等,与药物代谢过程相关的基因进行分析,通过了解药物在不同人群中的代谢过程差异,以实现更有效的药物治疗效果,减少药物不良反应的发生。
药物的作用原理是通过干预生物体内的生化反应来治疗疾病。
每个人对于药物反应的不同都是由其遗传基因的因素决定的。
药物基因组学研究通过分析人体代谢药物的基因,可以知道药物对每个人的作用效果,预测治疗疾病的方式和治疗效果,从而为治疗提供依据。
药物基因组学的应用可以追溯到20世纪80年代,当时研究人员发现前列腺素合成酶基因的突变与非甾体消炎药对于减轻疼痛的效果有关。
通过日益增强的生物技术和计算技术,使得药物基因组学在未来发展的前景更加广阔。
药物基因组学的发展将可以改变药物设计的方式,让药物更加准确地满足患者的特殊需求。
一些创新型药物公司已经开始使用药物基因组学的技术来新开发药物。
同时,药物基因组学将为临床医学提供重要信息,帮助医生更精确地预测治疗效果,减少药物的副作用。
利用药物基因组学进行药物设计时,必须通过大量的生物信息学分析和统计学建模等机器学习方法来分析研究数据。
与传统的药物研发模式相比,这种方法具有更高的效率和更大的准确性。
通过了解人体代谢药物的基因、酶以及通路,提高对于治疗疾病的认识,这样就可以直接开发更加有效的药物。
药物基因组学还可以在药物治疗后的监测中起着重要的作用。
通过监测受试者的基因组信息,可以解释药物的不良反应。
制定包括基因组学数据的治疗方案成为了一种常见的方法,这些方案不仅可以提高个体药物治疗的效果,还可以减少药物不良反应的发生。
在药物基因组学的发展中,外部因素对基因组的影响依然是一个重要的研究领域。
这些外部因素包含药物作用时对于生物体的影响以及环境因素、生活方式以及基因表观遗传信息等。
药物基因组学的研究与应用
药物基因组学的研究与应用药物治疗是现代医学中最为常见的一种治疗方式之一,它通过使用化学物质来调节人体的生理功能,从而达到治疗疾病的效果。
但是,每个人的身体特征不同,也会导致同样一种药物对不同的人有不同的反应。
药物基因组学的研究与应用,就在探寻人们身体与药物之间的联系,从而实现个性化医疗,提高疗效与安全性。
药物基因组学是一个交叉学科,它将基因组学、转录组学、蛋白质组学,以及实验药理学、临床药理学等多个领域结合起来,以个体基因差异为出发点和研究对象,探究了基因与药物之间的相互作用,以期以个人化的方式决定药物治疗方案。
药物基因组学实现个性化用药人体内有许多基因都与药物代谢、药物作用相关。
比如,CYP450酶群就是人体中非常重要的药物代谢酶之一,能够代谢70%以上的信任成分,对药物代谢能力的提高和降低都是有影响的。
在临床上,一些药物过度积累会导致毒副作用,而另一些药物则被代谢过快,无法起到治疗作用。
此时,通过检测患者的CYP450基因变异情况,可以根据个体的代谢情况,定制个性化的用药方案,进而增加疗效,并减少毒副作用的发生。
药物基因组学应用于药物疗效预测不同基因型的患者对同种药物的疗效也有所不同。
在临床上,应用药物基因组学技术,可以根据患者的基因型判断对于某些药物的疗效,并选择最合适的治疗方案。
比如,考虑到乙肝病毒是一种存在转录变异的病毒,目前的药物治疗方案则是在阻止病毒复制的基础上,通过治疗和预防的方法来防止肝硬化和肝癌等疾病的发生。
因为每个患者对于病毒的反应是不确定的,因此,在药物治疗中应用药物基因组学技术,预测每个患者对于药物的反应,从而针对性的选择最佳的药物治疗方案,提高治疗效果,并减少毒副作用的发生。
药物基因组学在药品临床研究中的应用基因组学技术为药物临床研究带来了新的机会和挑战。
在药物研究之前,结合基因组学技术可以预测试验对象的药物反应,选择试验对象,减少临床研究的成本和周期。
在药物研究中,可以通过基因组学技术望着靶点和药物中间物的表达方式,掌握更全面的药物信息,进而设计更加合理的药物分子。
药物基因组学在个体化治疗中的应用与研究
药物基因组学在个体化治疗中的应用与研究研究方案:药物基因组学在个体化治疗中的应用与研究引言:随着基因组学研究的快速发展,人们开始认识到基因与药物反应之间的关系对于个体化治疗的重要性。
药物基因组学的研究旨在探索个体基因变异对药物治疗效果和不良反应的影响,以实现个体化用药,提高药物治疗效果并减少患者的不良反应。
本研究方案将探索药物基因组学在个体化治疗中的应用,并提出新的观点和方法,以解决实际临床中的问题。
一、研究目的:本研究的目的是探索药物基因组学在个体化治疗中的应用,重点研究个体基因变异对药物治疗效果和不良反应的影响,并提出新的观点和方法,为解决实际临床问题提供有价值的参考。
二、研究方法:1. 数据采集选择一定数量的患者作为样本,对其进行基因组测序,获取个体基因数据。
同时收集患者的临床信息,包括病例资料、疾病类型及相关检测结果。
2. 实验设计根据药物基因组学的研究目的,选取若干药物进行研究。
将药物按照其作用机制分为不同类别,每类药物选取一种作为研究对象。
对于每种药物,将样本分为两组:药物治疗组和对照组。
药物治疗组给予药物治疗,对照组给予安慰剂。
治疗过程中监测患者的疗效和不良反应。
3. 数据采集和整理根据实验设计,采集患者的临床观察结果,包括药效评估和不良反应记录。
将基因组测序数据与临床观察结果进行关联分析,以确定个体基因变异与药物治疗效果和不良反应之间的关系。
4. 数据分析对采集到的数据进行统计学分析和生物信息学分析。
采用适当的统计学方法,比较药物治疗组和对照组之间的差异,判断药物治疗的有效性和安全性。
通过生物信息学分析,挖掘基因组数据中的潜在规律,识别与药物治疗效果和不良反应相关的基因位点。
三、预期结果与讨论:本研究预计将通过药物基因组学的研究手段,探索个体基因变异对药物治疗效果和不良反应的影响。
通过分析研究结果,预期能发现个体基因变异与药物治疗效果和不良反应之间的关联关系,并发现新的治疗靶点和治疗策略。
曲马多的药物基因组学相关研究进展
曲马多的药物基因组学相关研究进展赵琴;于锋;朱君荣【期刊名称】《药学与临床研究》【年(卷),期】2013(021)001【摘要】Tramadol is a centrally acting non-narcotic analgesic, and it is widely used for variously caused acute and chronic moderate to severe pain. Tramadol has great individual differences toward the drug response, that is to say, under-analgesia or complications may occur in patients given the same dose. Recent studies indicate that the individual variance in tramadol response is associated with gene polymorphisms influencing metabolism and action. This paper reviews the progress of the pharmacogenomics of tramadol in order to provide a reference for its individualized therapy in clinical practice.%曲马多是一种中枢性非麻醉镇痛药,广泛应用于各种原因引起的急慢性中重度疼痛.曲马多的药效个体间差异大,临床常见相同剂量的曲马多在不同患者间出现镇痛不足或胃肠道不良反应的现象.近年研究表明,曲马多个体反应的差异与其药代学和药效学相关的多个基因多态性有关.本文综述了曲马多的药物基因组学研究进展,为临床开辟曲马多个体化治疗提供参考.【总页数】6页(P56-61)【作者】赵琴;于锋;朱君荣【作者单位】南京医科大学附属南京医院临床药学室,南京210006【正文语种】中文【中图分类】R971+.1【相关文献】1.药物基因组学-指导合理用药的基因组学 [J], 张祖杰;陈慧2.中国患者华法林抗凝治疗剂量的药物基因组学相关性及药物基因组学方程的比较分析 [J], 王红娟;刘瑜;杨洁;徐斌;李泱;尹彤3.铂类联合第三代化疗药物治疗非小细胞肺癌的药物基因组学研究进展 [J], 刘姗;李兴德;宋沧桑;张阳;赖泳;张函舒4.参与非典型抗精神病药物代谢的CYP450的药物基因组学研究进展 [J], 姚燕春;魏英5.围产期心肌病基因组学相关研究进展 [J], 董婷;胡英因版权原因,仅展示原文概要,查看原文内容请购买。
麻醉药物及其辅助药物基因组学的研究进展
麻醉药物及其辅助药物基因组学的研究进展
郑卓玲;黄民;李嘉丽
【期刊名称】《中国药理学通报》
【年(卷),期】2018(34)8
【摘要】麻醉药及其辅助药物是外科手术的必备药物,然而在临床常规治疗方案下,药物反应具有明显的个体差异.遗传因素是造成个体间药代动力学、药效学反应差异的重要原因.现对国内外麻醉药及其辅助药物的基因组学研究进展进行综述,为麻醉药物的个体化用药提供参考.
【总页数】4页(P1049-1052)
【作者】郑卓玲;黄民;李嘉丽
【作者单位】中山大学药学院临床药理研究所,广东广州 510080;中山大学药学院临床药理研究所,广东广州 510080;中山大学药学院临床药理研究所,广东广州510080
【正文语种】中文
【中图分类】R-05;R394.6;R971.2;R977.3
【相关文献】
1.静脉麻醉药物的现状及其辅助药物的研究进展 [J], 韩波;王晓丹;张英俊
2.鞘内应用辅助药物复合局部麻醉药在蛛网膜下腔阻滞中的研究进展 [J], 吴佳旻; 张延卓
3.加速康复外科中麻醉与围手术期管理的药物基因组学研究进展 [J], 马黎娜;郭海云;麻玉梅;聂煌
4.麻醉药及其辅助药物基因组学的研究进展 [J], 邓婕;侯颖;宋洪涛
5.麻醉药物代谢酶CYP45O酶系基因组学研究进展 [J], 汪国香;方向明;郑汉光因版权原因,仅展示原文概要,查看原文内容请购买。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
麻醉药物基因组学研究论文本文对药物基因组学的基本概念和常用麻醉药的药物基因组学研究进展进行综述。
药物基因组学是伴随人类基因组学研究的迅猛发展而开辟的药物遗传学研究的新领域,主要阐明药物代谢、药物转运和药物靶分子的基因多态性及药物作用包括疗效和毒副作用之间关系的学科。
基因多态性是药物基因组学的研究基础。
药物效应基因所编码的酶、受体、离子通道作为药物作用的靶,是药物基因组学研究的关键所在。
基因多态性可通过药物代谢动力学和药物效应动力学改变来影响麻醉药物的作用。
基因多态性对药代动力学的影响主要是通过相应编码的药物代谢酶及药物转运蛋白等的改变而影响药物的吸收、分布、转运、代谢和生物转化等方面。
与麻醉药物代谢有关的酶有很多,其中对细胞色素-P450家族与丁酰胆碱酯酶的研究较多。
基因多态性对药效动力学的影响主要是受体蛋白编码基因的多态性使个体对药物敏感性发生差异。
苯二氮卓类药与基因多态性:咪唑安定由CYP3A代谢,不同个体对咪唑安定的清除率可有五倍的差异。
地西泮是由CYP2C19和CYP2D6代谢,基因的差异在临床上可表现为用药后镇静时间的延长。
吸入麻醉药与基因多态性:RYR1基因变异与MH密切相关,现在已知至少有23种不同的RYR1基因多态性与MH有关。
氟烷性肝炎可能源于机体对在CYP2E1作用下产生的氟烷代谢产物的一种免疫反应。
神经肌肉阻滞药与基因多态性:丁酰胆碱酯酶是水解琥珀酰胆碱和美维库铵的酶,已发现该酶超过40种的基因多态性,其中最常见的是被称为非典型的(A)变异体,与用药后长时间窒息有关。
镇痛药物与基因多态性:μ-阿片受体是阿片类药的主要作用部位,常见的基因多态性是A118G和G2172T。
可待因和曲马多通过CYP2D6代谢。
此外,美沙酮的代谢还受CYP3A4的作用。
儿茶酚O-甲基转移酶(COMT)基因与痛觉的产生有关。
局部麻醉药与基因多态性:罗哌卡因主要由CYP1A2和CYP3A4代谢。
CYP1A2的基因多态性主要是C734T和G2964A,可能影响药物代谢速度。
一直以来麻醉科医生较其它专业的医疗人员更能意识到不同个体对药物的反应存在差异。
麻醉药的药物基因组学研究将不仅更加合理的解释药效与不良反应的个体差异,更重要的是在用药前就可以根据病人的遗传特征选择最有效而副作用最小的药物种类和剂型,达到真正的个体化用药。
能够准确预测病人对麻醉及镇痛药物的反应,一直是广大麻醉科医生追求的目标之一。
若能了解药物基因组学的基本原理,掌握用药的个体化原则,就有可能根据病人的不同基因组学特性合理用药,达到提高药效,降低毒性,防止不良反应的目的。
本文对药物基因组学的基本概念和常用麻醉药的药物基因组学研究进展进行综述。
一、概述二十世纪60年代对临床麻醉过程中应用琥珀酰胆碱后长时间窒息、硫喷妥钠诱发卟啉症及恶性高热等的研究促进了药物遗传学(Pharmacogenetics)的形成和发展,可以说这门学科最早的研究就是从麻醉学开始的。
药物基因组学(Phamacogenomics)是伴随人类基因组学研究的迅猛发展而开辟的药物遗传学研究的新领域,主要阐明药物代谢、药物转运和药物靶分子的基因多态性及药物作用包括疗效和毒副作用之间的关系。
它是以提高药物的疗效及安全性为目标,研究影响药物吸收、转运、代谢、消除等个体差异的基因特性,以及基因变异所致的不同病人对药物的不同反应,并由此开发新的药物和用药方法的科学。
1959年Vogel提出了“药物遗传学”,1997年Marshall提出“药物基因组学”。
药物基因组学是药物遗传学的延伸和发展,两者的研究方法和范畴有颇多相似之处,都是研究基因的遗传变异与药物反应关系的学科。
但药物遗传学主要集中于研究单基因变异,特别是药物代谢酶基因变异对药物作用的影响;而药物基因组学除覆盖药物遗传学研究范畴外,还包括与药物反应有关的所有遗传学标志,药物代谢靶受体或疾病发生链上诸多环节,所以研究领域更为广泛[1,2,3]。
二、基本概念1.分子生物学基本概念基因是一个遗传密码单位,由位于一条染色体(即一条长DNA分子和与其相关的蛋白)上特定位置的一段DNA序列组成。
等位基因是位于染色体单一基因座位上的、两种或两种以上不同形式基因中的一种。
人类基因或等位基因变异最常见的类型是单核苷酸多态性(single-nucleotidepolymorphism,SNP)。
目前为止,已经鉴定出13000000多种SNPs。
突变和多态性常可互换使用,但一般来说,突变是指低于1%的群体发生的变异,而多态性是高于1%的群体发生的变异。
2.基因多态性的命名法:(1)数字前面的字母代表该基因座上最常见的核苷酸(即野生型),而数字后的字母则代表突变的核苷酸。
例如:μ阿片受体基因A118G指的是在118碱基对上的腺嘌呤核苷酸(A)被鸟嘌呤核苷酸(G)取代,也可写成118A/G或118A>G。
(2)对于单个基因密码子导致氨基酸转换的多态性编码也可以用相互转换的氨基酸的来标记。
例如:丁酰胆碱酯酶基因多态性Asp70Gly是指此蛋白质中第70个氨基酸-甘氨酸被天冬氨酸取代。
三、药物基因组学的研究内容基因多态性是药物基因组学的研究基础。
药物效应基因所编码的酶、受体、离子通道及基因本身作为药物作用的靶,是药物基因组学研究的关键所在。
这些基因编码蛋白大致可分为三大类:药物代谢酶、药物作用靶点、药物转运蛋白等。
其中研究最为深入的是麻醉药物与药物代谢酶CYP45O酶系基因多态性的相关性[1,2,3]。
基因多态性可通过药物代谢动力学和药物效应动力学改变来影响药物作用,对于临床较常用的、治疗剂量范围较窄的、替代药物较少的麻醉药物尤其需引起临床重视。
(一)基因多态性对药物代谢动力学的影响基因多态性对药物代谢动力学的影响主要是通过相应编码的药物代谢酶及药物转运蛋白等的改变而影响药物的吸收、分布、转运、代谢和生物转化等方面[3,4,5,6]。
1、药物代谢酶与麻醉药物代谢有关的酶有很多,其中对细胞色素-P450家族与丁酰胆碱酯酶的研究较多。
(1)细胞色素P-450(CYP45O)麻醉药物绝大部分在肝脏进行生物转化,参与反应的主要酶类是由一个庞大基因家族编码控制的细胞色素P450的氧化酶系统,其主要成分是细胞色素P-450(CYP45O)。
CYP45O组成复杂,受基因多态性影响,称为CYP45O基因超家族。
1993年Nelson等制定出能反应CYP45O基因超家族内的进化关系的统一命名法:凡CYP45O基因表达的P450酶系的氨基酸同源性大于40%的视为同一家族(Family),以CYP后标阿拉伯数字表示,如CYP2;氨基酸同源性大于55%为同一亚族(Subfamily),在家族表达后面加一大写字母,如CYP2D;每一亚族中的单个变化则在表达式后加上一个阿拉伯数字,如CYP2D6。
(2)丁酰胆碱酯酶麻醉过程中常用短效肌松剂美维库铵和琥珀酰胆碱,其作用时限依赖于水解速度。
血浆中丁酰胆碱酯酶(假性胆碱酯酶)是水解这两种药物的酶,它的基因变异会使肌肉麻痹持续时间在个体间出现显著差异。
2、药物转运蛋白的多态性转运蛋白控制药物的摄取、分布和排除。
P-糖蛋白参与很多药物的能量依赖性跨膜转运,包括一些止吐药、镇痛药和抗心律失常药等。
P-糖蛋白由多药耐药基因(MDR1)编码。
不同个体间P-糖蛋白的表达差别明显,MDR1基因的数种SNPs 已经被证实,但其对临床麻醉的意义还不清楚。
(二)基因多态性对药物效应动力学的影响麻醉药物的受体(药物靶点)蛋白编码基因的多态性有可能引起个体对许多药物敏感性的差异,产生不同的药物效应和毒性反应[7,8]。
1、蓝尼定受体-1(Ryanodinereceptor-1,RYR1)蓝尼定受体-1是一种骨骼肌的钙离子通道蛋白,参与骨骼肌的收缩过程。
恶性高热(malignanthyperthermia,MH)是一种具有家族遗传性的、由于RYR1基因异常而导致RYR1存在缺陷的亚临床肌肉病,在挥发性吸入麻醉药和琥珀酰胆碱的触发下可以出现骨骼肌异常高代谢状态,以至导致患者死亡。
2、阿片受体μ-阿片受体由OPRM1基因编码,是临床使用的大部分阿片类药物的主要作用位点。
OPRM1基因的多态性在启动子、内含子和编码区均有发生,可引起受体蛋白的改变。
吗啡和其它阿片类药物与μ-受体结合而产生镇痛、镇静及呼吸抑制。
不同个体之间μ-阿片受体基因的表达水平有差异,对疼痛刺激的反应也有差异,对阿片药物的反应也不同。
3、GABAA和NMDA受体γ-氨基丁酸A型(GABAA)受体是递质门控离子通道,能够调节多种麻醉药物的效应。
GABAA受体的亚单位(α、β、γ、δ、ε和θ)的编码基因存在多态性(尤其α和β),可能与孤独症、酒精依赖、癫痫及精神分裂症有关,但尚未见与麻醉药物敏感性有关的报道。
N-甲基-D-天门冬氨酸(NMDA)受体的多态性也有报道,但尚未发现与之相关的疾病。
(三)基因多态性对其它调节因子的影响有些蛋白既不是药物作用的直接靶点,也不影响药代和药效动力学,但其编码基因的多态性在某些特定情况下会改变个体对药物的反应。
例如,载脂蛋白E 基因的遗传多态性可以影响羟甲基戊二酸单酰辅酶A(HMG-CoA)还原酶抑制剂(他汀类药物)的治疗反应。
鲜红色头发的出现几乎都是黑皮质素-1受体(MC1R)基因突变的结果。
MC1R基因敲除的老鼠对麻醉药的需求量增加。
先天红发妇女对地氟醚的需要量增加,热痛敏上升而局麻效力减弱。
四、苯二氮卓类药与基因多态性大多数苯二氮卓类药经肝脏CYP45O代谢形成极性代谢物,由胆汁或尿液排出。
常用的苯二氮卓类药物咪唑安定就是由CYP3A代谢,其代谢产物主要是1-羟基咪唑安定,其次是4-羟基咪唑安定。
在体实验显示不同个体咪唑安定的清除率可有五倍的差异。
地西泮是另一种常用的苯二氮卓类镇静药,由CYP2C19和CYP2D6代谢。
细胞色素CYP2C19的G681A多态性中A等位基因纯合子个体与正常等位基因G纯合子个体相比,地西泮的半衰期延长4倍,可能是CYP2C19的代谢活性明显降低的原因。
A等位基因杂合子个体对地西泮代谢的半衰期介于两者之间。
这些基因的差异在临床上表现为地西泮用药后镇静或意识消失的时间延长[9,10]。
五、吸入麻醉药与基因多态性到目前为止,吸入麻醉药的药物基因组学研究主要集中于寻找引起药物副反应的遗传方面的原因,其中研究最多的是MH。
药物基因组学研究发现RYR1基因变异与MH密切相关,现在已知至少有23种不同的RYR1基因多态性与MH有关。
与MH不同,氟烷性肝炎可能源于机体对在CYP2E1作用下产生的氟烷代谢产物的一种免疫反应,但其发生机制还不十分清楚[7,11]。
六、神经肌肉阻滞药与基因多态性神经肌肉阻滞药如琥珀酰胆碱和美维库铵的作用与遗传因素密切相关。