ARDS最佳peep设定
【讨论】ARDS患者的5种床旁PEEP选择方法详解

【讨论】ARDS患者的5种床旁PEEP选择方法详解转自中国呼吸治疗大伙日常在进行机械通气的过程中总会有关于PEEP选择的疑惑,特别是针对ARDS的患者,由于ARDS肺部变化的不均一性,一个快速而有效的PEEP选择显得尤为重要。
阿T通过本期《文献》内容的引申,为大伙介绍一下目前常用的5种床旁最佳PEEP的选择方法,仅供大伙参考。
首先是由ARDS net发布的关于利用PEEP-FiO2表格选择,有低PEEP高FiO2选择和高PEEP低FiO2选择两种方式,例如当FiO2为50%时,若根据低PEEP高FiO2,其PEEP的选择在8-10cmH2O,若根据高PEEP低FiO2选择,PEEP水平在16-20cmH2O。
根据PEEP-FiO2表格选择的优点是方便快捷,但似乎不够个体化,很多人并不喜欢,但也有研究认为其与肺复张的相关性较强。
第二种方法是根据监测食道压设置最佳PEEP 。
在患者没有自主呼吸努力时,分别通过吸气屏气和呼气屏气测量食道内压力,一般设置PEEP 使跨肺压维持0-10cmH2O 防止肺泡塌陷,调整潮气量使跨肺压平台压力<25cmH2O 防止过度膨胀。
食道压测量选择PEEP 目的是达到合适的跨肺压,特别是ARDS 患者跨肺压经常被低估,食道压监测是知道局部可变性最好的方法。
但跨肺压在不同位置数值是不同的,并不是一个均值,所以判断最佳监测位置非常困难,而且目前仍然缺乏证据证明根据食道压设置的PEEP 是可以改善预后的。
第三种床旁最佳PEEP 设置被叫做快速法(Express method )。
在容控模式下设置6ml/kg 理想体重的潮气量,不断增加PEEP 水平(每次增加2-5cmH2O ),每增加一次,利用吸气屏气法测量一次平台压,直到测得的平台压达到28-30 cm H2O ,这个时候的PEEP 即为最佳PEEP 。
若患者顺应性较好,PEEP 最高增加到20cmH2O 时,平台压还没有达到以上目标,将不再继续增加PEEP 。
急性中毒试题库
1百草枯中毒给氧的原则是A、任何时候均应给氧。
,B、出现缺氧表现,动脉血氧分压<40 mmHg时,给予低流量吸氧。
C、始终不能给氧,D、应高流量给纯氧。
正确答案:B2(单选)哪些场所不产生CO?A、枯井、储菜窖、谷仓、地下坑道、密闭船仓B、火灾现场、含碳物质不完全燃烧的场所C、内燃机工作又通风不良的场所D、高炉煤气泄露的场所正确答案:A3(单选)哪一项不是窒息性气体?A、甲烷、乙烷、乙烯B、CO、一氧化氮、苯的氨基硝基化合物C、氰化氢、硫化氢D、氨气、氯气、光气正确答案:D4(单选)重度CO中毒时,下列哪项实验室检查变化是错误的A、PaO2 明显降低B、SaO2 明显下降。
C、HbCO 明显升高。
D、WBC 变化不大。
正确答案:A5(单选)在急性群体化学品中毒患者的分级管理中,重度中毒患者应当转往哪里?A、区域中毒救治基地。
B、二级以上医疗机构。
C、就近医疗机构。
D、社区医疗机构。
正确答案:A6(单选)现场按伤分类可以将患者分成三类,哪一类具有优先救治权?A、不管他们获得何种治疗,都有可能存活。
B、不管他们获得何种治疗,都有可能死亡。
C、给予即刻救治能够显著改善预后。
D、不管何种类型,按顺序救治。
正确答案:C7(单选)急性食物中毒事件中样本的选择与采集哪一条是错误的?A、可疑食品的剩余部分、半成品和原料。
B、患者的呕吐物及腹泻患者的大便。
C、对发热患者和可疑化学性食物中毒患者应注意采取血液和尿液。
D、无剩余可疑食物时就不必采集。
正确答案:D8(单选)化学物中毒的特点哪一条是不正确的?A、化学物中毒是一种全身损害性疾病。
B、不同的毒物中毒可有不同的靶器管。
C、凡是多系统、多器管损害就是中毒。
D、在同一环境中,同时或短时间内相继发生的类同综合症,要想到中毒的可能。
正确答案:C9(单选)以下哪项不是中毒性肝衰竭降低血氨的治疗方法A、口服乳果糖B、口服新霉素C、口服微生态制剂D、2%肥皂水灌肠E、食醋保留灌肠正确答案:D10(单选)下列哪项不会导致中毒性肝病的发生:A、四氯化碳中毒B、百草枯中毒C、毒蕈中毒D、抗结核药物E、硫化氢中毒正确答案:E11(单选)中毒性肝病依据临床特点,不包括下列哪种类型?A、多系统损害型B、隐匿型C、肝病型D、慢性中毒性肝病E、肾损害型正确答案:E12(单选)突发中毒事件卫生应急处置的工作报告主要分为:A、首次报告、进程报告、结案报告B、事前报告、事中报告、事后报告C、总结报告D、事件处置报告及个案救治报告正确答案:A13(单选)中毒控制的内容不包括:A、生应急体系建设B、中毒控制网络C、人员物质保障D、实验室建设正确答案:D14(单选)下列描述错误的是:A、维生素K是抗凝血类灭鼠剂的拮抗剂。
【专题笔谈】急性呼吸窘迫综合征:如何选择最佳呼气末正压

【专题笔谈】急性呼吸窘迫综合征:如何选择最佳呼气末正压展开全文点击标题下「蓝色微信名」可快速关注ARDS是一种常见的呼吸危重症,2012年柏林标准[1]定义为临床发病或呼吸系统症状新发或加重后1周内出现双肺致密影,无法用胸腔积液、肺叶/肺不张或结节解释,也无法用心力衰竭或体液过负荷(需要客观评估来除外静水压升高引起的肺水肿)来完全解释的呼吸衰竭,其氧合指数(PaO2/FiO2)不超过300 mmHg(1 mmHg=0.133 kPa),且呼气末正压或持续气道正压≥5 cmH2O(1 cmH2O=0.098 kPa)。
这一定义分别从发病时间、胸部影像学、引起肺水肿的原因和氧合状态4个方面对ARDS重新进行了定义,并基于氧合指数对ARDS的严重程度进行了轻、中、重度分级,病情的严重程度与病死率直接相关[2],重度ARDS病死率甚至高达45%[1]。
机械通气是改善ARDS氧合状态的主要手段之一,早在1998年就有学者提出小潮气量、限制平台压的通气策略可以降低病死率[3],目前这种保护性肺通气策略已经得到广泛认可,但另一主要通气参数——呼气末正压(positive end-expiratory pressure, PEEP)的选择却仍存在争议。
一、ARDS的病生理改变与使用PEEP的目的二、ARDS机械通气时PEEP的选择三、临床常用的PEEP滴定法不同,并不尽如人意。
1.FiO2-PEEP关联表:ARDSnet提出的FiO2-PEEP关联表(表1)是一简单可行地选择PEEP的方法,方法是根据患者的目标动脉血氧分压(55~80 mmHg)或指尖氧饱和度(88%~95%)来选择吸入氧浓度和PEEP水平。
临床操作简便,使用广泛。
2.肺开放法:是使用小潮气量避免肺泡过度扩张,同时选择一个PEEP使肺泡得到最大复张以减少反复开闭引起的肺损伤。
一项研究结果证实,在传统小潮气量策略的基础上,限制平台压在30 cmH2O以内和在40 cmH2O以内,住院期间的全因病死率和气压伤的发生率并无差别,而高平台压组的平均PEEP更高、氧合改善更充分,低氧相关合并症的发生率有所降低[7]。
ARDS患者的管理
七、脱机与拔管
拔管后观察
1. 拔管后注意呼吸、心率、 SaO2 等生命体征的 情况。 2. 拔管后患者床边仍应放置必要的抢救器材, 呼吸机仍应放置于床边24h。
3. 注意患者的一般状况、咳嗽及痰液的性状、 有无喘鸣及呼吸困难、声音有无嘶哑、进食有 无呛咳等,对患者出现的情况进行分析并进行 针对性的处理。
(筛孔数目、湿化瓶高度)、
气流速度有关
三、人工气道温湿化、雾化
一次性吸氧装
无菌湿化 无噪音湿化
过滤性湿化
均匀湿化
三、人工气道温湿化、雾化
加热湿化器(heated humiபைடு நூலகம்ifier,HH)
以物理加热的方法为干燥气体提供恰当的温度和充 分的湿度,适用于机械通气时。 输出气体的湿度至少达到30mg/L(相当于30℃时 100%的相对湿度)
四、人工气道气囊的管理
最小漏气技术(MLT)
定义:气囊充气后,在吸气时有少量气体漏出 步骤
听诊器置于气管处,向气囊内注气直到听不到漏气 声为止 然后抽出气体,每次0.1ml,直到吸气时听到少量 漏气为止
优点:减少潜在的气道损伤(与MOV相比) 缺点:易发生误吸、对潮气量有影响,导管移位
ARDS—呼吸机模式
压力调节容量控制 (Pressure regulated Volume Control) PRVC 开始呼吸序列时的第一次呼吸是容量控制通气 的尝试性呼吸,暂停时间设置为10%。所测得 的此次呼吸的暂停期压力用作下一次呼吸的压 力值。
ARDS—呼吸机模式
ARDS--最佳PEEP
六、俯卧位通气
呼吸机管理:
1.避免气管导管口被堵或移位,及时整理、检查呼 吸机管道,防止扭曲、折叠,调节呼吸机支架适应 体位改变,避免牵拉气管导管。 2.及时清理口鼻腔内大量分泌物。每30~60 min 拍背1次,以促进气体分布均匀及气体交换,促使 痰液排出。
peep的正常范围

peep的正常范围
Peep,即持续性正压呼吸(Positive End Expiratory Pressure,PEEP),是指在呼气期间维持一定的正压水平,并将此正压水平保持到下一次呼吸开始。
Peep是一种机械通气技术,常用于治疗呼吸功能不足的重症患者,例如ARDS (急性呼吸窘迫综合症)患者。
Peep的正常范围与患者的情况和通气机参数等因素有关。
以下是一些常见的Peep正常范围参考值:
1. 对于健康成人,一般Peep水平在3-5 cmH2O,而当需要机械通气支持时,Peep水平通常会增加至5-15cmH2O,具体取决于病情和需要。
2. 对于ARDS患者,Peep水平可能需要较高。
一般推荐起始Peep水平为
5-10cmH2O。
然后根据氧合和呼吸机参数调整Peep水平,一般可增加至15-
25 cmH2O。
较高Peep水平可能增加治疗效果,但也可能增加器官损伤的风险。
3. 对于其他疾病患者,Peep水平的推荐范围可能有所不同。
例如,肺水肿和慢性阻塞性肺病(COPD)患者可能需要较低的Peep水平(3-5 cmH2O),而肺挫伤或肺炎患者可能需要较高的水平(10-15 cmH2O)。
需要注意的是,Peep水平不能盲目设置,需要动态调整,根据患者情况、呼吸机参数和氧合状况进行调整。
过高或过低的Peep水平都可能对患者产生不利影响。
因此,医护人员需要仔细监测氧饱和度、呼吸频率和血气分析情况等指标,随时调整Peep水平以确保有效治疗。
不同方式滴定PEEP对中重度ARDS患者右心功能及肺动脉压影响的研究

不同方式滴定PEEP对中重度ARDS患者右心功能及肺动脉压影响的研究东南大学附属中大医院重症医学科硕士研究生:杜同跃导师:郭凤梅主任医师副教授中文摘要目的:比较ARDSnet法、EIT法和跨肺压方法选择PEEP对中重度急性呼吸窘迫综合征(Acute Respiratory Distress Syndrome, ARDS)患者右心功能及肺动脉压的影响。
方法:以2018年08月至2019年4月收住东南大学附属中大医院重症医学科符合柏林诊断标准中重度ARDS的患者为研究对象。
入组后记录患者一般资料,在PEEP=5cmH2O的条件下进行基础机械通气并记录右心功能相关指标。
以ARDSnet、EIT、跨肺压三种方法分别滴定最佳PEEP。
然后在ARDSnet、EIT、跨肺压滴定的PEEP下,分别以驱动压为15cmH2O和12cmH2O、采用压控模式下(FiO2 40-80%、I:E 1:2、RR 20次/min)进行机械通气,每个条件下机械通气前行肺复张一次(高压45cmH2O、低压30cmH2O、持续35S),每组上述条件通气持续10min,后通过经胸超声心动图(transthoracic echocardiography, TTE )测定右心功能包括:在心尖四腔心界面监测右左心室直径比值、三尖瓣环收缩期位移(tricuspid annular plane systolic excursion, TAPSE)、三尖瓣环收缩速度(tricuspid annular motion, TAM)及肺动脉压力。
实验过程中记录患者呼吸力学、血流动力学、动静脉血气。
结果:1、一般情况实验共纳入ARDS患者25例,中度14例、重度11例,排除图像质量不佳3例,共22例纳入最终研究,其中10例接受ECMO治疗。
基础PEEP 5cmH2O状态下右心室中度扩大19例(86.36%),重度扩大3例(13.63%)。
肺动脉高压1例(4.54%)。
临床peep安全有效评估设置

临床peep安全有效评估设置临床上需要设置peep的疾病主要有两类:ARDS和AECOPD,前者是呼气时部分肺泡出现塌陷,后者则是在呼气时小气道塌陷。
所以,ARDS患者设置peep的目的保持呼气时塌陷的肺泡开放,而AECOPD患者则是保持呼气时塌陷的小气道通畅。
但是,peep作为一个压力,特性就是“欺软怕硬”,其作用部位可能不会按照我们的设想进行。
对于ARDS,我们希望设置的peep尽量都作用在塌陷的肺泡,使塌陷的肺泡在呼气相保持开放,事实上这部分力会优先传导至正常的肺泡,使正常的肺泡过度膨胀。
同样,对于AECOPD患者,设置的peep不仅会作用在塌陷的气道,更可能的是通过正常的气道把压力传导至肺泡。
临床上如何评估设置的peep是否安全,其实也就是说如何避免设置的peep使肺泡出现过度膨胀造成肺损伤。
先说ARDS吧,如果设置的peep大部分是作用在塌陷的肺泡,则患者呼气末肺容积增加,顺应性改善,此时患者的驱动压和平台压下降,则此时设置的peep一定是有益的。
而如果peep增加时,平台压和驱动压也相应的增加,表明设置的peep在打开塌陷肺泡的同时也造成了正常肺泡的过度膨胀,此时peep是否有益则需要评估,而如果平台压和驱动压的增加值超过了peep的增加值,则说明此时的peep大部分作用于正常的肺泡,使正常肺泡出现了过度膨胀,有肺损伤的风险,此时的peep是不安全的,是有害的。
对于AECOPD患者,我们希望设置的peep仅作用于塌陷的气道,使呼气相塌陷的气道保持开放,减小气道阻力,呼出更多的气体,降低内源性peep。
所以,临床上如果增加peep时,peepi下降,则提示设置的peep 大部分是作用在塌陷的气道上,而如果peepi增加,则说明设置的peep 大部分是通过正常的气道传导至肺泡,使呼气末肺泡压力升高,此时的peep不安全。
由于临床上测定peepi需要把外源性peep关掉,我们可以通过测定peep 总来评估peep的安全。
ARDS机械通气中PEEP的设置方法 080519

2. 是否应用微分法还未达到一致。
3. 肺复张贯穿于P-V曲线吸气过程中陡峭的部分, 不能单独用LIP来判定最佳PEEP。
三、利用PaO2 变化率设置PEEP • 方法:绘测PEEP-PaO2 曲线。 • 优点:临床操作容易、劳动强度不大。 • 缺点:
1. 动脉氧合还依赖于心输出量,混合静脉氧饱 和度和低氧性肺血管收缩等因素。 2. 特殊情况下,在肺的不同部位,肺泡复张和 过度膨胀同时存在,氧分压的变化不能灵 敏地检测到发生肺损伤的危险。
二、低位转折点法(吸气支)
1. 传统的大注射器法(1975 年)。流速法获得静态P-V曲 线(1999年)。
P
1. 2.
优点:利用弹性力学特征,比较符合病理生理。 缺点:
1. 影响顺应性的因素十分复杂,很大程度受潮气量、肺力
学干扰。
2. 某些研究发现使用更高的压力,效果更好。
四、肺牵张指数法
• 方法:监测压力——时间曲线(吸气支)。曲 线回归法算得方程P=a×timeb十c。b值即为牵 张指数。选择b=1时的PEEP值。 • 但目前该法还处于动物研究阶段。
五、顺应性法。 六、胸部CT导向的PEEP递减法。 七、最佳氧合法(PaO2 / FiO2)。
ARDS机械通气中 PEEP的设置方法
广东省人民医院 急危重症医学部 叶 珩
一、FiO2-PEEP递增法(PaO2经验法)
1. 方法:交替提高PEEP和FiO2的水平,以达到 氧合目标。 2. 优点:简单方便,临床最为常用。 3. 缺点:因为FiO2也在提高,PEEP维持肺复张 的效应如何并不明确。
3. 患病肺的P-V曲线上不一定总存在拐点。
4. P-V 曲线吸气支和呼气支是分离的。
二、低位转折点法(呼气支)
ARDS患者peep滴定方法--氧合导向
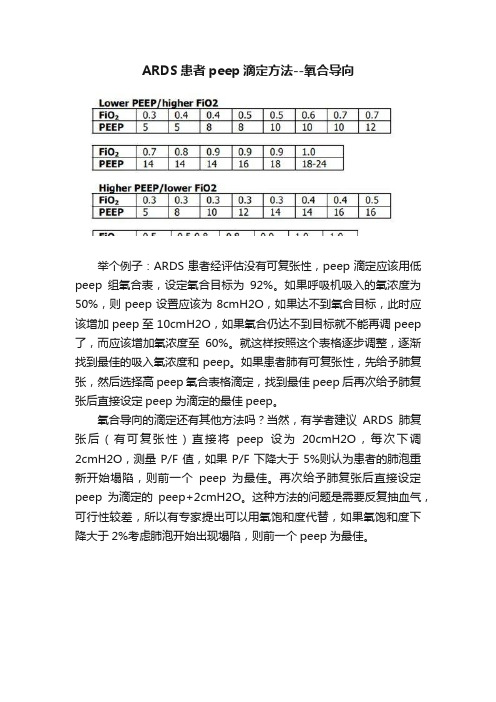
ARDS患者peep滴定方法--氧合导向举个例子:ARDS患者经评估没有可复张性,peep滴定应该用低peep组氧合表,设定氧合目标为92%。
如果呼吸机吸入的氧浓度为50%,则peep设置应该为8cmH2O,如果达不到氧合目标,此时应该增加peep至10cmH2O,如果氧合仍达不到目标就不能再调peep 了,而应该增加氧浓度至60%。
就这样按照这个表格逐步调整,逐渐找到最佳的吸入氧浓度和peep。
如果患者肺有可复张性,先给予肺复张,然后选择高peep氧合表格滴定,找到最佳peep后再次给予肺复张后直接设定peep为滴定的最佳peep。
氧合导向的滴定还有其他方法吗?当然,有学者建议ARDS肺复张后(有可复张性)直接将peep设为20cmH2O,每次下调2cmH2O,测量P/F值,如果P/F下降大于5%则认为患者的肺泡重新开始塌陷,则前一个peep为最佳。
再次给予肺复张后直接设定peep为滴定的peep+2cmH2O。
这种方法的问题是需要反复抽血气,可行性较差,所以有专家提出可以用氧饱和度代替,如果氧饱和度下降大于2%考虑肺泡开始出现塌陷,则前一个peep为最佳。
当然,还有学者研究用最佳氧供的方法滴定peep,更加复杂,不适合临床普遍应用,不再介绍。
以氧合为目标进行滴定peep,可以实现氧供最佳化,看似比较合理,但是最佳氧合的同时可能肺已经出现了过度膨胀,造成气压伤,所以也要综合评估。
好了,下一讲我们谈谈呼吸力学导向的peep滴定。
参考文献:1.NHLBI ARDS Clinical Network Mechanical Ventilation Protocol Summary2.Journal of Korean medical science 18.3 (2003): 349.。
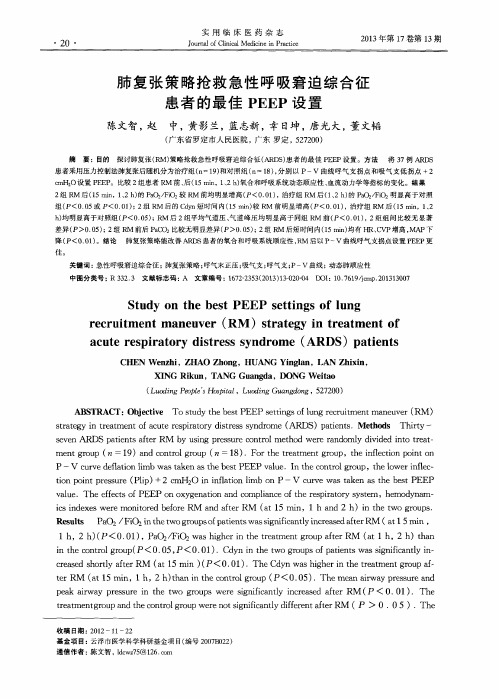
肺复张策略抢救急性呼吸窘迫综合征患者的最佳PEEP设置
2 0 ・
J o u r n 詈 a l o 用 f C 临 1 i n i 医 c a 1 M e d i 药 c i n e 母 i n 志 P r a c t i c e
2 …~… 0 1 3 年 第 1 7 … 卷 第 1 3 期
肺 复 张 策 略抢 救 急性 呼 吸窘 迫 综 合征 患 者 的最 佳 P E E P设 置
P —V c u r v e d e f l a t i o n l i mb wa s t a k e n a s t h e b e s t P EE P v a l u e .I n t h e c o n t r o l g r o u p.t h e l o we r i n f l e c —
a c u t e r e s p i r a t o r y d i s t r e s s s y n d r o me( AR DS )p a t i e n t s
CHEN We n z h i ,ZHAO Zho ng,HUANG Yi n gl a n,LAN Zhi xi n, XI NG Ri k u n,TANG Gu a ng da,DONG We i t a o
( L u o d i n g P e o p l e 5 H o s Nt a £ ,L 0 ( f 锄 G u a n g d o n g, 5 2 7 2 0 0 )
A B S T RA C T: O b j e c t i v e T o s t u d y t h e b e s t P E E P s e t t i n g s o f l u n g r e c r u i t me n t ma n e u v e r ( R M) s t r a t e g y i n t r e a t me n t o f a c u t e r e s p i r a t o r y d i s t r e s s s y n d r o me( AR D S ) p a t i e n t s . Me t h o d s T h i r t y —
如何设置PEEP

如何设置PEEP我们知道,对于ARDS患者PEEP的设置是非常重要和关键的,也是我们主要的治疗手段和措施之一。
如何设置一个最佳PEEP对ARDS 患者的预后有着非常关键的作用,今天,我们就如何设置PEEP来做一个讨论。
急性呼吸窘迫综合征(Acute Respiratory Distress Syndrome,ARDS)由各种肺内、外致病因素(心源性除外)所致的,以弥漫性肺泡-毛细血管膜损伤为病理特征的急性呼吸衰竭,临床表现为顽固性低氧血症和呼吸窘迫【1】。
参考推荐影像学与呼吸力学【徐磊】▼ Berlin定义已知诱因或新出现或原有呼吸系统症状加重后一周内发病。
影像学改变:•仍然认定双肺浸润改变诊断ARDS,可以行CT检查较胸片更准确•双肺透光度减弱,不能完全用胸腔积液、叶/肺不张或结节来解释•不能完全由心力衰竭或容量过负荷解释的呼吸衰竭•如果没有ARDS的危险因素时可行超声心动图等检查排除静水压性肺水肿参考推荐Estimation of Driving Pressure During Assisted Ventilation 【杜斌】用氧合指数来进行轻、中、重度的分型:氧合指数:200-300之间,属于轻型ARDS氧合指数:100-200之间,属于中度ARDS氧合指数:<100,属于重度ARDS对于上PEEP来说,PEEP治疗ARDS主要是在中重度的患者,轻度患者一般采用高量吸氧,或者有一些无创的机械通气。
中、重度患者,上了有创机械通气时,设置的PEEP对于患者的氧合改善也是至关重要的。
▼ AR DS病理生理改变【2】▼根据ARDS的严重程度可供选择的治疗方法参考推荐ARDS phenotypes Hyper-/hypoin flammation:Holygrail?【邱海波】PEEP概念呼气末正压:吸气由病人或呼吸机产生,而呼气末借助装在呼气端的限制气流的活瓣等装置,使气道压力高于大气压。
PEEPi指在呼气相,气道提前闭合或小气道部分萎陷,导致呼气相阻力增加,使在呼气末肺泡内压力维持正压,称自身呼气末正压或内源性呼气末正压。
ARDS最佳peep设定护理课件

定期复查相关指标,如肺功能、血气分析等,了解患者恢复情况, 及时调整治疗方案。
ARDS的康复和随访
康复训练
指导患者进行呼吸功能训练、运动康复等,促进肺功能的恢复。
健康宣教
加强患者及家属的健康宣教,提高对ARDS的认识和自我管理能 力。
定期随访
定期对患者进行随访,了解病情变化,评估治疗效果,及时调整 治疗方案。
减轻肺水肿
通过减轻肺水肿,降低肺 内分流,提高氧合。
PEEP的适用范围和限制
适用范围
适用于ARDS患者,尤其是有明显肺萎陷和氧合障碍的患者。
限制
过高的PEEP可能导致气压伤、心排血量下降、呼吸机相关肺 炎等并发症。因此,需要根据患者的具体情况选择合适的 PEEP水平。
03
ARDS最佳PEEP设定 的护理实践
THANKS
感谢观看
控制基础疾病
积极治疗和控制基础疾病,如慢性阻塞性肺疾病、糖尿病等,降低 ARDS的发病风险。
避免吸入性损伤
加强工业卫生和职业防护,减少有毒气体、粉尘等吸入性损伤,预防 ARDS的发生。
ARDS的预后评估
评估病情严重程度
根据ARDS的病情严重程度,评估患者的预后情况。
观察治疗反应
观察患者对治疗的反应,如氧合指数、呼吸频率等指标的变化,评 估病情的改善情况。
氧化应激
细胞凋亡和坏死
炎症反应和氧化应激可诱导肺部细胞 凋亡和坏死,进一步加重肺损伤。
炎症反应过程中产生的大量活性氧自 由基可导致肺部组织损伤。
ARDS的临床表现
呼吸困难
患者感到呼吸急促、费 力,严重时呼吸窘迫。
紫绀
由于低氧血症,患者口 唇、甲床出现紫绀。
肺部听诊
最佳PEEP设置在ARDS患者机械通气中的应用及护理
需求 ,把患者放在 首位 ,强化基础护理 ,整体提升 护理服务水
表 1 护理 的理念 贯穿在 心包 穿刺 引流术 的整个
过程 ,使患者 在生理 、心 理 、社会 等方 面得到满 足 ,增 强 了患
者 战胜疾病 的信心 ,提高了患者的生活质 量。
分 <20分为差 ,20—29分为 良,30—45分为优 。
一 位护理工作者将细心 、耐心 、爱心 、责任 心付诸 于护理行动
1.2.3 统计学方法 数据采 用 SPSS 13.0软件进行 统计分 之 中 J。应该从身边的每 一件事 情做起 ,大 到治疗 操作 ,小
析,采用 )(2检验 ,以 P≤0.05为差异有统计学意义。
【参考文献 】
[1] 马柳英 ,罗旭芬 ,屈平英.冠心病 患者介入治疗过程中舒适护理 的效果评价 [J].华夏医学 ,2008,21(4):784-785.
[2] 霍云英 .舒适护理 在门诊注射 治疗患 者 中的应 用 [J].中国城 乡企 业 卫 生 ,2011,(2):76-77. (2012-03—13收稿 2012- 05- 09修 回) (本 文编 辑 贡 树 基 )
到体位 的摆放 ,都要 主动满 足患者 的需求 ,使患者感到舒适 。
2 结 果
综上所述 ,舒适 护理要 以患 者为 中心 ,在思想 观念 和 医
两组患者 的满意度 比较 ,见 表 1。观察组优 良率 高于对 疗行为上 ,处 处为患者着 想 ,一切 活动都要 紧 紧围绕 患者 的
照 组 (× =19.84,P <0.01)。
急性 呼吸窘迫 综合征 (ARDS)是 以进 行性 呼吸 困难 、低 氧血症 、肺顺应性下 降为特 征的 急性呼 吸衰竭 ,病 死率高 达 50% 一70%… 。机械通气是治疗 ARDS的重要手段 之一 ,间 歇 正 压 通 气 (IPPV)+呼气 末 正 压 (PEEP)是 目前 治 疗 ARDS 的常用通气方式 J。如何控制气道峰压 、平均压 ,改善氧合 , 减少呼吸机相关性 肺损 伤 (VILI),是 目前 临床 研究 的重点 。 本研究将机械 通气 时 PEEP的 常规设 置 与通过 胸肺 顺应 性 曲线 (P.V曲线 )选择最 佳 PEEP设 置进行 比较 ,以评价其 临 床应 用 价 值 并 总结 护 理 经 验 。 1 资料与方法 1.1 一般 资料 2010年 1月 一2011年 12月我 院 ICU收治 ARDS患者 22例 ,随机分 为对 照组 (常规设 置 PEEP)和观察 组 (选 择 P—V曲线下 拐点上 l一2 em设 置 PEEP),各 11例 。 所有病 例 均 符 合 ARDS的诊 断 标 准 。对 照 组 患 者 年 龄
ARDS个性化PEEP设置
Individualized PEEP Setting in Subjects With ARDS:A Randomized Controlled Pilot StudyMaría-Consuelo Pintado MD PhD,Rau´l de Pablo MD PhD,María Trascasa, Jose´-María Milicua,Santiago Rogero,Martín Daguerre,Jose´-Andre´s Cambronero, Ignacio Arribas MD PhD,and Miguel Sa´nchez-García MD PhDBACKGROUND:Low-tidal-volume ventilation may be associated with repetitive opening and closing of terminal airways.The use of PEEP is intended to keep the alveoli open.No method of adjusting the optimal PEEP has shown to be superior or to improve clinical outcomes.We con-ducted a pilot study to evaluate the effect of setting an individualized level of PEEP at the highest compliance on oxygenation,multiple-organ-dysfunction,and survival in subjects with ARDS. METHODS:Subjects with ARDS ventilated with low tidal volumes and limitation of airway pres-sure to30cm H2O were randomized to either a compliance-guided PEEP group or an F IO2-guidedgroup.RESULTS:Of the159patients with ARDS admitted during the study period,70met the inclusion criteria.Subjects in the compliance-guided group showed nonsignificant improvements inP aO2/F IO2during the first14days,and in28-day mortality(20.6%vs.38.9%,P؍.12).Multiple-organ-dysfunction-free days(median6vs20.5d,P؍.02),respiratory-failure-free days(median7.5 vs14.5d,P؍.03),and hemodynamic-failure-free days(median16vs22d,P؍.04)at28days were significantly lower in subjects with compliance-guided setting of PEEP.CONCLUSIONS:In ARDS subjects,protective mechanical ventilation with PEEP application according to the highest com-pliance was associated with less organ dysfunction and a strong nonsignificant trend toward lower Number NCT01119872.Key words:ARDS;mechanical ventilation;tidal volume;multiple organ dysfunction.[Respir Care2013;58(9):1416–1423.©2013Daedalus Enterprises]IntroductionARDS is characterized by the acute onset of hypoxemia and bilateral infiltrates that are consistent with pulmonary edema,without evidence of left heart failure.1Mechanical ventilation is potentially lifesaving in patients with ARDS, but may cause ventilator-associated lung injury.Lung-protective ventilation strategies seek to prevent ventilator-associated lung injury by using low tidal volume(V T)to avoid overdistention,and PEEP to prevent repetitive alve-olar collapse and reopening.2-4S EE THE R ELATED E DITORIAL ON P AGE1552 The application of PEEP improves gas exchange and lung function.The main effect of increasing PEEP is to maintain the recruitment of alveolar units that were pre-viously collapsed.Thus,since the V T is distributed to more alveoli,peak airway pressure is reduced and compliance is increased.5However,the pressure needed to open and re-cruit some alveoli may overdistend others,which may direct blood perfusion away from these areas,thereby in-creasing dead space,pulmonary vascular resistance,andDr Pintado,Dr de Pablo,Ms Trascasa,Mr Milicua,Mr Rogero, Mr Daguerre,Dr Cambronero,and Dr Sa´nchez-García are affiliated with the Intensive Care Unit;and Dr Arribas is affiliated with the Foundation for Biomedical Research,Hospital Universitario Príncipe de Asturias, Alcala´de Henares,Madrid,Spain.Drs Pintado and de Pablo are co-first authors.Supplementary material related to this paper is available at http:// .Correspondence:María-Consuelo Pintado MD PhD,Intensive Care Unit, Hospital Universitario Príncipe de Asturias,Carretera Alcala´-Meco, SN E-28805,Alcala´de Henares,Madrid,Spain.E-mail:consuelo pintado@yahoo.es.DOI:10.4187/respcare.02068mean hydrostatic pressure,and thus increase lung dam-age.6The preferred method of adjusting the PEEP is still controversial.7,8The amount of potentially recruitable lung tissue has best been evaluated using computed tomogra-phy,9but this approach is usually not readily available in ICUs for routine assessment of ventilator settings.Some have suggested that lung mechanics are a better surrogate than gas exchange for bedside assessment of lung recruitment,10and that the PEEP should be chosen individually.10-12In fact,several studies have shown im-proved survival when PEEP is set above the lower in-flection point on the pressure-volume curve,the steepest portion of the curve,a sign of increase of functional re-sidual capacity.12-15Unfortunately,all these studies also compared low versus high V T ventilation,which hinders evaluation of the effect directly attributable to PEEP.Re-cently,2studies compared different methods of PEEP setting.One study,based on individual maximum alveolar recruitment,failed to demonstrate a reduction in mortality,although they observed significant improvements in oxy-genation 16and lung function.17We conducted an open,randomized controlled pilot study to test the hypothesis that individualized PEEP set based on highest compliance would improve oxygenation,com-pared to setting PEEP based on F IO 2.18MethodsThis study was conducted in a 14-bed mixed medical-surgical ICU in Spain,over a time period of 60months.The study protocol was approved by our institution’s Ethics and Clinical Trials Committee,and registered at (NCT01119872).Written informed consent was required for inclusion,and obtained from the nearest relatives.No commercial entities had any role in any aspect of this study.We screened all patients with ARDS according to the American-European consensus conference definition,1who maintained ARDS criteria after 24hours of mechanical ventilation,in order to confirm ARDS and exclude other causes of hypoxemia and pulmonary infiltrates,since me-chanical ventilation parameters can affect oxygenation and whether the patient meets the ARDS definition.19We ex-cluded patients who were younger than 18years,pregnant,or had neuromuscular disease,intracranial hypertension,head trauma,left ventricular dysfunction (on echocardiog-raphy),Ͼ72hours of mechanical ventilation,or baro-trauma.Patients with end-stage conditions (death expected within 90days)were also excluded.We defined baro-trauma as the presence of air outside the tracheobronchial tree,resulting from presumed alveolar rupture,and man-ifested as interstitial emphysema,pneumothorax,pneumo-mediastinum,pneumoperitoneum,or subcutaneous emphy-sema.20Patients who developed barotrauma during thefirst 24hours of observation prior to randomization were also excluded,because it was not feasible to measure pla-teau pressure.In subjects excluded after randomization,the respiratory protocol was not applied,although protec-tive lung ventilation was maintained,and they were kept in their assigned study groups for outcome analysis.Study DesignAll patients who met ARDS criteria were ventilated during 24hours with low V T (6–8mL/kg predicted body weight [PBW]),an inspiratory plateau pressure Ͻ30cm H 2O,a breathing frequency of 30breaths/min,adjusted to maintain a pH between 7.30and 7.45,and limited to a maximum of 35breaths/min,F IO 2that kept arterial oxygen saturation at 88–95%or P aO 2at 55–80mm Hg,and PEEP adjusted to achieve the best oxygenation with the lowest F IO 2while avoiding adverse hemodynamic effects.If the plateau pressure was Ͼ30cm H 2O with a V T of 6mL/kg PBW,a stepwise V T reduction of 1mL/kg PBW to as low as 4mL/kg/PBW was allowed,in which case the plateau pressure limit was set at 35cm H 2O.After 24hours,subjects who met the inclusion criteria were randomized to either F IO 2-guided PEEP (control group)or compliance-guided PEEP.Randomization was performed in blocks of 10,using sealed envelopes.In the control group,PEEP was set based on the sub-ject’s F IO 2,as applied in the ARDS Network study.18In the compliance-guided group,PEEP was set daily,according to the method described by Suter et al.12Static compliance was measured at increasing levels of PEEP and at constant PEEP.Static compliance was calculated as V T divided by the pressure difference at end of inflation hold (2s),and PEEP was increased in steps of 2cm H 2O,beginning at 5cm H 2O,without an upper PEEP titration limit.The highest static compliance was considered to be the best PEEP.If at 2different PEEPs the static compliance wasidentical,we chose the one with the lower plateau pressure (see the respiratory protocol in the supplementary materi-als at ).All subjects received sedatives and opioids at the time of PEEP setting.Neuro-muscular blocking agents were used as required for low-V T ventilation,although not for the measurement of intrinsic PEEP or plateau pressure.According to the study group,PEEP was adjusted once daily during the morning shift,until the weaning phase started.Intrinsic PEEP was measured before and after ev-ery change of applied PEEP,and the inspiratory/expiratory ratio was changed accordingly to prevent intrinsic PEEP. All other ventilator parameters were set in the same way in both study groups,following the protocol applied for 24hours before randomization.18The weaning protocol was identical for both groups. Weaning was begun if the cause of respiratory failure hadresolved,P aO2wasϾ60mm Hg,F IO2wasՅ0.4,andPEEP was below6cm H2O.In the compliance-guided group,PEEP was lowered by steps of2cm H2O.In the control group we applied the protocol described in the ARDS Network study18(see the supplementary materials at ).Subjects were monitored with a pulmonary artery cath-eter for at least the first72hours after randomization,to study the hemodynamic effects of PEEP.Therapy other than mechanical ventilation was prescribed at the discre-tion of the attending physicians not involved in the study. Our local protocols were applied to guide sedation,hemo-dynamic support,and other standard interventions.End points were assessed at28days.The primaryend point was P aO2/F IO2.Secondary end points were mor-tality,ventilator-free days,ICU and hospital stay,multiple-organ-dysfunction(MOD)free days,and respiratory and hemodynamic parameters.MeasurementsData collected from each subject included demograph-ics,risk factors for ARDS,routine laboratory measure-ments,Acute Physiology and Chronic Health Evaluation II score21at ICU admission,daily Lung Injury Score,22 Sepsis-Related Organ Failure Assessment score,23MOD score,24days on mechanical ventilation,ICU and hospital outcomes and stay,28-day mortality,pulmonary mea-surements,physiologic measurements,ventilatory mea-surements,cardiovascular measurements,adverse events, extrapulmonary organ failures,sedation,and daily chest x-ray.All measurements and data were recorded at study inclusion,at6hours after inclusion,and between6:00AM and8:00AM on days1,2,3,4,7,14,21,and28. Organ failure was defined as a Sepsis-Related Organ Failure Assessment score23Ͼ2,and MOD requiresՆ2 organ an-dysfunction-free days were de-fined as days alive and free of any organ dysfunction,15,17 and ventilator-free days were defined as days of unassisted breathing,both calculated at28days(all deaths oc-curring prior to day28were considered as zero organ-dysfunction-free or ventilator-free days).18Subjects were followed until hospital discharge or death.Statistical AnalysisNormality of data distribution was assessed using the Kolmogorov-Smirnov test.Quantitative variables with nor-mal distribution are expressed as meanϮSD,and were compared using the Student t test.Non-normal distribution variables are shown as medians and interquartile ranges, and were compared using the Mann-Whitney test.Quali-tative variables are shown as percentages,and were com-pared with the chi-square test.Kaplan-Meier analysis with log-rank test was applied to compare survival at28days between groups.Statistical significance was set at PϽ.05, and results are expressed with their95%confidence inter-vals.Statistical analysis was performed using statistics soft-ware(SPSS15.0,SPSS,Chicago,Illinois).ResultsA total of159patients met the criteria for ARDS during the study period,70of whom were randomized toeither Fig.1.Screening and enrollment.compliance-guided (n ϭ34)or F IO 2-guided PEEP adjust-ment (n ϭ36)(Fig.1).No patients were excluded after randomization or discharged from hospital earlier than 28days.The main cause of ARDS was infection (n ϭ50,71.4%)(detailed causes of ARDS per study group are shown in the supplementary materials at ).There were no significant differences in subject character-istics between study groups at randomization,except for the high incidence of MOD in the compliance-guided group (Table 1).Physiological MeasurementsThere was no difference in median PEEP at study entry (Fig.2).Figure 3shows the ventilatory parameters over the 28-day study period.There was no significant differ-ence in P aO 2/F IO 2.There was a trend toward better oxy-genation in the compliance-guided group over the first 2weeks of study (see Fig.3and the supplementary ma-terials at ).In the compliance-guided group there was also a nonsignificantly higher pul-monary compliance and lower airway pressure (see Fig.3and the supplementary materials at ).There were no differences in pH,V T ,intrinsic PEEP,or breathing frequency (see the supplementary materials at ).In a post-hoc analysis we found that 80%of the subjects in the compliance-guided group would have had a differ-ent PEEP if set according to the F IO 2/PEEP table.There were no limitations in daily PEEP changes,rather than the measurement frequency of PEEP.Clinical OutcomesThe compliance-guided group had significantly more MOD-free days at day 28(Table 2),in spite of a higher baseline incidence (see Table 1),as well as more ventila-tor-free days and hemodynamic failure-free days.Twelve subjects developed barotrauma after randomiza-tion:6per study group (see Table 2).A total of 9episodesTable 1.Baseline Characteristics of Subjects at Study InclusionF IO 2-Guided PEEP(n ϭ36)Compliance-Guided PEEP(n ϭ34)Male,no.(%)29(80.55)20(58.82)Age,y54.1Ϯ2.955.6Ϯ3.1APACHE II score 20.53Ϯ1.3318.71Ϯ1.02SOFA score8.86Ϯ0.619.38Ϯ0.66Multiple-organ-dysfunction score 8.36Ϯ0.528.50Ϯ0.57Lung Injury Score,median (IQR)3(2.5–3.25)3(2.5–3.25)Percentage of patients with multiple-organ-dysfunction syndrome*77.897.1P aO 2/F IO 2,mm Hg133.15Ϯ5.88146.33Ϯ6.19PEEP pre-randomization,median (IQR)cm H 2O 10(8–14)10(8–12)Tidal volume,mL/kg predicted body weight 6.61Ϯ0.87 6.66Ϯ1.01Peak pressure,cm H 2O 38.10Ϯ1.1138.22Ϯ1.33Plateau pressure,cm H 2O31.87Ϯ1.5628.24Ϯ1.22Breathing frequency,breaths/min 23Ϯ125Ϯ1Minute ventilation,L/min 12.1Ϯ0.412.9Ϯ0.4pH7.34Ϯ0.017.33Ϯ0.01P aCO 2,mm Hg43.28Ϯ1.2742.11Ϯ1.01Values are mean ϮSD unless otherwise indicated.*There were no significant differences between the groups at study randomization,except percentage of patients with multiple-organ-dysfunction syndrome:P ϭ.02.APACHE ϭAcute Physiology and Chronic Health Evaluation SOFA ϭsepsis-related organ failureassessmentFig.2.PEEP in the first 28days.of barotrauma occurred during the first week:5in the compliance-guided group,and 4in the F IO 2-guided group.One subject in the compliance-guided group and 2in F IO 2-guided group developed barotrauma in the second week of study.Global 28-day mortality was 30%(21subjects),with a hospital mortality of 42.8%(30subjects).28-day mortality was 20.6%(n ϭ7)in the compliance-guided group and 38.9%(n ϭ14)in the F IO 2-guided group (P ϭ.12)(Fig.4).The main causes of death were multi-organ failure (n ϭ50,71.4%)and refractory hypoxemia (n ϭ10,14.3%).Sub-jects who died had a higher Sepsis-Related Organ Failure Assessment score 23at inclusion (11.4Ϯ0.7vs 8.1Ϯ0.5,P ϭ.01),as well as lower P aO 2/F IO 2(126.4Ϯ9.6mm Hgvs 145.1Ϯ4.3mm Hg,P ϭ.04)and a higher Lung Injury Score 22(3.25[2.50–3.50]vs 3.00[2.50–3.25],P ϭ.04).There were no significant differences in hemodynamic variables or sedative dosage between the groups (see the supplementary materials at ).There were no complications associated with insertion of the pulmonary artery catheter.DiscussionIn subjects with ARDS,ventilated with low V T and airway pressure limited to 30cm H 2O,compliance-guided PEEP adjustment,compared to F IO 2-guided PEEP adjust-ment,had no significant effect on oxygenation,althoughitFig.3.P aO 2/F IO 2,static compliance,peak pressure,and plateau pressure.Table 2.Clinical OutcomesF IO 2-Guided PEEP(n ϭ36)Compliance-Guided PEEP(n ϭ34)P 28-day mortality,no.(%)14(38.9)7(20.6).12Multiple-organ-dysfunction-free days at 28days 6(0–23.75)20.5(0–26).02Respiratory-failure-free days at 28days 7.5(0–19)14.5(0–22.5).03Hemodynamic failure-free days at 28days 16(0–23.75)22(0–25).04Renal-failure-free days at 28days28(0–28)28(0–28).39Hematological-failure-free days at 28days 25.5(0–28)28(0–28).52Hepatic-failure-free days at 28days 28(0–28)28(0–28).08ICU stay,d20(12–29)21(15–46).24Hospital stay,mean ϮSD d 32Ϯ355Ϯ7.01ICU-free days at 28days0(0–11)0(0–14).84Ventilator-free days at 28days 0(0–15.75)1(0–18).16Barotrauma,no.(%)6(16.7)6(17.6).99Values are median (IQR)unless otherwise indicated.was associated with a significant reduction of the duration of MOD.To our knowledge,static-compliance-guided PEEP has not previously been studied in a large group of subjects under lung-protective ventilation.25Interestingly,there was no significant difference in the mean PEEP applied to the 2groups.In previous studies PEEP was higher if set ac-cording to“compliance.”13,17,26Although mean PEEP was similar,our post-hoc analysis showed that80%of the compliance-guided subjects would have received different PEEP than did the control group.Hypothetically,subjects with customized PEEP might have been on higher or lower PEEP than those prescribed PEEP according to thePEEP/F IO2table.Thus,the similar mean PEEP value,inour opinion,does not exclude the possibility that individ-ual compliance-guided PEEP might be distributed over a wider range and might be associated with less ventilator-induced lung injury.We also found that subjects on compliance-guided PEEP had nonsignificantly lower plateau pressures over the first 21days of study(see Fig.3).This could be explained by improved alveolar recruitment,since other respiratory pa-rameters were set according to the same protocol in both groups,but this needs to be confirmed in a larger study. In previous studies,lower plateau pressure has been asso-ciated with lower mortality,18and,similar to our findings, shorter duration of MOD.17,18There have been only3randomized controlled clinical trials in which PEEP set according to the pressure-volume curve was compared with other methods of setting PEEP.13-15Those studies compared higher versus lower V T and found progressive improvement of oxygenation14 over the first week.13,15There were no data about the course of oxygenation beyond the first week.Those stud-ies differed from ours in that PEEP was set slightly above the lower inflection point of the quasi-static pressure-volume curve.That method correlates poorly with alveolar recruitment,and therefore with total alveolar compliance.27 We also found a nonsignificant improvement in oxygen-ation in the compliance-guided group during the first 2weeks,but this effect was not observed at later stages. Unlike in previous studies,improved oxygenation,if con-firmed,may be attributed to the method of PEEP deter-mination,since this was the only difference between the 2study parisons of oxygenation data are methodologically very difficult because of important dif-ferences in clinical course and how death and weaning should statistically be accounted for.In addition,in later stages of ARDS,with increased lung fibrosis,28,29the use of the pressure-volume curve may be less effective in achieving alveolar recruitment and,consequently,in im-proving oxygenation.We observed that customizing PEEP to the individual subject was associated with shorter duration of MOD at 28days.It is reasonable to assume that this effect is the cause for the strong trend toward lower mortality in this study group.Previous studies have been criticized for similar results because subjects were ventilated with high V T,which is associated with higher mortality.18A meta-analysis30of3studies13-15showed significantly lower mor-tality if PEEP was determined according to the pressure-volume curve.This effect on duration of MOD may be related to a reduced release of inflammatory cytokines. Several clinical studies have confirmed that an array of inflammatory cytokines is released into the systemic cir-culation as a consequence of high V T or high PEEP,which correlates with higher morbidity and mortality.14,18,31,32 Other studies have compared methods of setting PEEP. The Express study17showed that,compared to a fixed and low PEEP,an individualized PEEP set at the highest value allowing a plateau pressure of28–30cm H2O is associ-ated with significant increase of MOD-free days at28days, without improving survival.Talmor et al26compared the application of fixed PEEP according to the ARDS Net-work standard-of-care recommendations,18with an indi-vidualized method based on transpulmonary pressure at end-expiration.They found improved oxygenation,as well as a trend toward lower mortality in the customized PEEP group.It is interesting to note that,as in our study,Talmor et al found that the respiratory-system compliance appeared to be higher in their esophageal-pressure-guided group.26 Unlike in our study,however,they determined PEEP dec-rementally after a recruitment maneuver,which has been demonstrated to influence the evaluation of lung compli-ance according to the pressure-volume curve.27,33 Grasso et al34found that,compared to the ARDS Net-work protocol,18in subjects with a focal pattern of loss of aeration,PEEP is lower if set according to stress index and that the application of the ARDS Network protocol18in-Fig.4.Kaplan-Meier curves for survival.duces alveolar hyperinsufflation and increases cytokineplasma levels.The LOVs16study found a lower incidenceof refractory hypoxemia and need for rescue therapies as-sociated with the application of PEEP according to F IO2 after a40-second,40cm H2O airway pressure recruitmentmaneuver,compared to the ARDS Network protocol18without previous recruitment maneuver,although withouta statistically significant difference in rates of all-causehospital mortality or barotrauma.In our study12subjects(17%)developed barotrauma.The incidence of barotrauma in ARDS has been reportedto range between0andϾ76%,35although recent studiesshow reduced incidences between6%and10%.16,17,36,37Risk factors for barotrauma included high peak airwaypressure,large V T,and the level of acute lung injury.38The slightly higher incidence of barotrauma in our studymay be explained by the high Lung Injury Score,22as largeV T and high peak airway pressure were avoided.The in-cidence of barotrauma was similar in our2study groups.Previous studies have not found differences in the inci-dence of barotrauma according the different levels or meth-ods of PEEP applied.16,17,36,37Our study has several limitations.Being a pilot studywith the aim to provide a basis for a future multicenterstudy,it had a small sample size and its results requireconfirmation.The study was carried out in a single center,and included only44%of subjects who met the inclusioncriteria.Although randomized,the study was unblinded,and bias cannot be excluded.Some difficulties in settingPEEP at best compliance became apparent during the study.At times,several time-consuming attempts were requiredto find the best PEEP in the compliance group,includingthe need for muscle relaxants,or the study procedures hadto be interrupted to allow for endotracheal suctioning.Wealso did not measure inflammatory cytokines to supportthe findings on MOD.ConclusionsIn conclusion,this randomized controlled pilot trialshowed that individualized PEEP selection based on thebest static compliance in subjects with ARDS treated withlow V T and limited plateau pressure did not improveoxygenation,but was associated with a significant increasein organ-dysfunction-free days and a strong trend towardlower mortality at rger,randomized,multicentertrials are necessary to validate this approach as an integralpart of lung-protective strategy.REFERENCES1.Bernard GR,Artigas A,Brigham KL,Carlet J,Falke K,Hudson L,et al.The American-European Consensus Conference on ARDS.Definitions,mechanisms,relevant outcomes,and clinical trial coor-dination.Am J Respir Crit Care Med1994;149(3Pt1):818-824.2.Diaz JV,Brower R,Calfee CS,Matthay MA.Therapeuticstrategies for severe acute lung injury.Crit Care Med2010;38(8): 1644-1650.3.Gattinoni L,Protti A,Caironi P,Carlesso E.Ventilator-induced lunginjury:the anatomical and physiological framework.Crit Care Med 2010;38(10Suppl):S539-S548.4.Pipeling MR,Fan E.Therapies for refractory hypoxemia in acuterespiratory distress syndrome.JAMA2010;304(22):2521-2527. 5.Villar J.The use of positive end-expiratory pressure in the manage-ment of the acute respiratory distress syndrome.Minerva Anestesiol 2005;71(6):265-272.6.Marini JJ.Initial management of acute hypoxemia.In:ShoemakerWC,Ayres SM,Grenvik A,Holbrook PR,eds.Textbook of Critical Care,4th ed.Philadelphia:WB Saunders;2000:1412.7.Dellinger RP,Levy MM,Carlet JM,Bion J,Parker MM,Jaeschke R,et al.Surviving Sepsis Campaign:international guidelines for man-agement of severe sepsis and septic shock:2008.Crit Care Med 2008;36(1):296-327.8.Gattinoni L,Caironi P.Refining ventilatory treatment for acute lunginjury and acute respiratory distress syndrome.JAMA2008;299(6): 691-693.9.Gattinoni L,Caironi P,Cressoni M,Chiumello D,Ranieri VM,Quintel M,et al.Lung recruitment in patients with the acute respiratory distress syndrome.N Engl J Med2006;354(17): 1775-1786.10.Gattinoni L,Carlesso E,Brazzi L,Caironi P.Positive end-expiratorypressure.Curr Opin Crit Care2010;16(1):39-44.11.Rouby JJ,Lu Q,Goldstein I.Selecting the right level of positiveend-expiratory pressure in patients with acute respiratory distress syndrome.Am J Respir Crit Care Med2002;165(8):1182-1186. 12.Suter PM,Fairley HB,Isenberg MD.Effect of tidal volume andpositive end-expiratory pressure on compliance during mechanical ventilation.Chest1978;73(2):158-162.13.Amato MB,Barbas CS,Medeiros DM,Magaldi RB,Schettino GP,Lorenzi-Filho G,et al.Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome.N Engl J Med 1998;338(6):347-354.14.Ranieri VM,Suter PM,Tortorella C,De Tullio R,Dayer JM,BrienzaA,et al.Effect of mechanical ventilation on inflammatory mediators in patients with acute respiratory distress syndrome:a randomized controlled trial.JAMA1999;282(1):54-61.15.Villar J,Kacmarek RM,Pe´rez-Me´ndez L,Aguirre-Jaime A.A highpositive end-expiratory pressure,low tidal volume ventilatory strat-egy improves outcomes in persistent acute respiratory distress syn-drome:a randomized,controlled trial.Crit Care Med2006;34(5): 1311-1318.16.Meade MO,Cook DJ,Guyatt GH,Slutsky AS,Arabi YM,CooperDJ,et al;Lung Open Ventilation Study Investigators.Ventilation strategy using low tidal volumes,recruitment maneuvers,and high positive end-expiratory pressure for acute lung injury and acute re-spiratory distress syndrome:a randomized controlled trial.JAMA 2008;299(6):637-645.17.Mercat A,Richard JC,Vielle B,Jaber S,Osman D,Diehl JL,et al;Expiratory Pressure(Express)Study Group.Positive end-expiratory pressure setting in adults with acute lung injury and acute respiratory distress syndrome:a randomized controlled trial.JAMA2008;299(6): 646-655.18.The Acute Respiratory Distress Syndrome Network.Ventilation withlower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome.N Engl J Med2000;342(18):1301-1308.19.Ferguson ND,Kacmarek RM,Chiche JD,Singh JM,Hallett DC,Mehta S,et al.Screening of ARDS patients using standardized ven-。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
©2020瑞呼吸大讲堂
PEEP滴定---牵张指数法
容控,方波; VC:6ml/Kg理想公斤体重逐步增加
PEEP观察压力—时间曲线成;
优点H:igh简单L易ow行 Right 缺点:易受胸壁顺应性的影响
©2020瑞呼吸大讲堂
PEEP滴定---peep递减法
©2020瑞呼吸大讲堂
指南怎么推荐
2017年ATC/ESCCM/SCCM联合推荐
©2020瑞呼吸大讲堂
PEEP滴定---氧合表法
优点:简单易行,无需复杂操作,依从性好; 缺点:不精准,波动范围较大;
©2020瑞呼吸大讲堂
PEEP滴定---最佳氧合法
充分肺复张; 将peep设置到较高水平比如20cmH20,每3-5min将peep降低2cmH2O,直到氧合指数
PEEP设定的方法
氧合导向:最佳氧合、最佳氧供 力学导向:最佳顺应性、驱动压导向、跨肺压导向等 循环导向:右心功能、最小分流 通气导向:最小死腔 影像学导向:CT 、超声、EIT等
©2020瑞呼吸大讲堂
指南怎么推荐
中华医学会呼吸病学会呼吸危重症学组 (2016)
美国呼吸治疗学会(AARC) (2014)
23
12
33
360ml
22
10
30
360ml
22
8
26
SPO2 92% 92% 91% 90% 87% 86% 84%
©2020瑞呼吸大讲堂
优点:个体化滴定peep,与氧供契合高; 缺点:操作稍复杂;
Respiratory Care September 2013, 58 (9) 1416-1423
©2020瑞呼吸大讲堂来自PEEP滴定—最小分流法
Qs/Qt=(CaO2-CAO2)/(CvO2-CAO2) =(SaO2-SAO2)/(SaO2-SAO2) =(1-SaO2)/(1-SvO2)
度时,驱动压增加;
优点:个体化滴定peep,真实反应肺应力; 缺点:无法去除肺外因素的影响;
©2020瑞呼吸大讲堂
PEEP滴定—最佳顺应性法
容控、方波,吸气暂停大于2秒测平台压; 静态顺应性=潮气量/(平台压-peep); Peep从5cmH2O开始,每次增加2cmH2O; 最大的顺应性为最佳的peep
根据RV功能、平台压设置适当PEEP 评估升高PEEP对肺复张和肺过度膨
胀的作用
➢ 右心功能不全→降低PEEP ➢ 无RV功能不全→升高PEEP
影像学方法
➢ CT ➢ 超声 ➢ EIT ➢…
©2020瑞呼吸大讲堂
Peep滴定方法
氧合导向:氧合表法、最佳氧合法 呼吸力学导向:最佳顺应性法、低流速PV曲线、牵张指数法、快速法、跨肺压法、 影像学导向:CT/EIT/超声/容积CO2 血流动力学导向/右心功能导向: 其他:死腔/呼末等
的降低>5% 重新肺复张,滴定的peep+2cmH2O即为最佳peep
优点:简单方便 缺点:反复查血气,临床可操作性稍差
©2020瑞呼吸大讲堂
PEEP滴定---食道压法
无自主呼吸时分别通过吸气屏气和呼气屏气测量食 道内压力;
一般设置PEEP使呼气末跨肺压维持在0~10cmH2O, 防止肺泡塌陷;
调整潮气量使吸气末跨肺压<25cmH2O,防止过度 膨胀
优点:消除胸壁的影响
缺点:微创;技术上具有一定挑战性
©2020瑞呼吸大讲堂
PEEP滴定---PV曲线法
低位平坦段:反映肺泡存在陷闭 陡直段:反映塌陷肺泡复张,肺顺应性
明显增加; 高位平坦段:提示肺泡过度膨胀 最佳peep:下拐点+2cmH2O
©2020瑞呼吸大讲堂
测试
ARDS患者,6ml/IBW,潮气量360ml,应用peep递减法,从20cmH2O每隔两分钟递减 2cmH2O,所测得结果如下,则该患者最佳peep设置
潮气量
平台压
peep
Crs
360ml
28
20
45
360ml
26
18
43
360ml
25
16
40
360ml
23
14
38
360ml
瑞呼吸大讲堂
ARDS最佳PEEP设定
迈瑞临床 李景涛
机械通过的目的
改善通气和换气
➢ 维持合理的二氧化碳分压; ➢ 改善氧分压;
肺保护
➢ 避免增加VILI(压力/容积伤、萎陷伤)
循环保护
➢ 肺不张和过度通气均会循环抑制
©2020瑞呼吸大讲堂
机械通气改善氧合的核心是--peep
PEEP是个双刃剑
操作复杂,需要漂浮导管,临床应用受限;
©2020瑞呼吸大讲堂
PEEP滴定—最小死腔法
Vd/Vt=(PaCO2-PeCO2)/PaCO2 可用呼末CO2代替PeCO2
Respiratory Care Oct 2012, 57 (10) 1578-1585;
©2020瑞呼吸大讲堂
其他方法
右心功能导向法
优点:将复张潜能和PEEP联系起来; 缺点:可能在轻度ARDS上应用高PEEP ;
©2020瑞呼吸大讲堂
PEEP滴定—驱动压导向
容控方波模式下,滴定好氧浓度后; 从5cmH2O开始,逐步增加peep,每次增加peep后测量平台压力; 驱动压力=平台压力-peep,增加peep后如果驱动压力增加的幅度明显大于peep增加的幅
容控模式,6ml/IBW ; 从高PEEP每2-3分钟减2cmH2O的PEEP 每次降低PEEP前,测量顺应性,当肺顺应
性明显下降时,前一个水平的PEEP即是最 佳PEEP
优点:更加个体化; 缺点:实施较复杂;
©2020瑞呼吸大讲堂
PEEP滴定---快速法
VC:6ml/IBW,逐渐增加PEEP(每次2~5cmH2O); 每增加一次PEEP,用吸气屏气法测量一次平台压; 直到测得平台压为28~30cmH2O,此时的PEEP为最佳;
DO2=CaO2 x CO x 10 =(1.34 x Hb x SaO2+0.003 x PaO2)x CO x 10
peep不足:肺泡塌陷,分流增加,剪切伤 peep过度:肺泡过度膨胀,死腔增加,容积伤;右负荷增 加,循环抑制; 最佳的peep:V/Q最佳,循环抑制最小,氧供最佳化
©2020瑞呼吸大讲堂