MEG evaluation in temporal lobe epilepsy
Myeloid-Derived Suppressor Activity Is Mediated by Monocytic Lineages Maintained by Continuous

ImmunityArticleMyeloid-Derived Suppressor Activity Is Mediated by Monocytic Lineages Maintained by Continuous Inhibition of Extrinsic and Intrinsic Death PathwaysJessica M.Haverkamp,1,2Amber M.Smith,1,2Ricardo Weinlich,2Christopher P.Dillon,2Joseph E.Qualls,1,2,9 Geoffrey Neale,3Brian Koss,4Young Kim,5Vincenzo Bronte,6Marco J.Herold,7,8Douglas R.Green,2Joseph T.Opferman,4and Peter J.Murray1,2,*1Department of Infectious Diseases2Department of Immunology3Hartwell Center for Bioinformatics and Biotechnology4Department of BiochemistrySt.Jude Children’s Research Hospital,262Danny Thomas Place,Memphis,TN38105,USA5Johns Hopkins Hospital,School of Medicine,Baltimore,MD21218,USA6Verona University Hospital and Department of Pathology,Verona,37134,Italy7Walter and Eliza Hall Institute of Medical Research,1G Royal Parade,Parkville,3052,Victoria,Australia8Department of Medical Biology,University of Melbourne,Parkville,3050,Victoria,Australia9Present address:Division of Infectious Diseases,Cincinnati Children’s Hospital Medical Center,Cincinnati OH,45229,USA*Correspondence:peter.murray@/10.1016/j.immuni.2014.10.020SUMMARYNonresolving inflammation expands a heterogeneous population of myeloid suppressor cells capable of inhibiting T cell function.This heterogeneity has confounded the functional dissection of individual myeloid subpopulations and presents an obstacle for antitumor immunity and ing genetic manipulation of cell death pathways,we found the monocytic suppressor-cell subset,but not the granulocytic subset,requires continuous c-FLIP expression to prevent caspase-8-dependent,RIPK3-independent cell death.Development of the granu-locyte subset requires MCL-1-mediated control of the intrinsic mitochondrial death pathway.Monocytic suppressors tolerate the absence of MCL-1provided cytokines increase expression of the MCL-1-related protein A1.Monocytic suppressors mediate T cell suppression,whereas their granulocytic counterparts lack suppressive function.The loss of the granulocytic subset via conditional MCL-1deletion did not alter tumor incidence implicating the monocytic compart-ment as the functionally immunosuppressive subset in vivo.Thus,death pathway modulation defines the development,survival,and function of myeloid sup-pressor cells.INTRODUCTIONNonresolving inflammation is caused by failure to eliminate a long-lived insulting entity including persisting microbes,im-planted medical devices,cholesterol and fat in atherosclerosis and obesity,and self-antigens driving chronic autoinflamma-tion(Nathan and Ding,2010).In cancer,nonresolving inflam-mation is driven by the growing malignancy and is associated with the production of large numbers of mature and immature myeloid cells from the bone marrow(BM).Circulating imma-ture myeloid cells with immunosuppressive functions are collectively called myeloid-derived suppressor cells(MDSCs), and are negatively correlated with cancer outcomes(Gabrilo-vich et al.,2012;Wu et al.,2014).MDSC expansion is related to a hematopoietic response to inflammation where growth factors such as GM-CSF and G-CSF signal to the BM to tran-siently increase cellular output.This‘‘emergency’’hematopoi-esis aids in the destruction and elimination of the insulting entity and is followed by tissue repair and resolution(Manz and Boettcher,2014).In nonresolving inflammation,the inciting agent remains and the hematopoietic cycle linked to clearance and resolution becomes dysregulated.MDSCs have attracted attention in cancer biology because they are linked with suppression of lymphocyte activation.The number and activity of cytotoxic CD8+T cells are correlated with anti-tumor immunity(Gajewski et al.,2013;Galon et al.,2013). Therapies designed to elicit antitumor T cell responses must overcome or bypass the local MDSC-mediated immune sup-pression inside the tumor microenvironment(Motz and Cou-kos,2013;Restifo et al.,2012).The current understanding of MDSC development,lifespan, and function has been limited by heterogeneity of the myeloid populations produced from the BM under inflammatory stress (Gabrilovich et al.,2007;Gabrilovich and Nagaraj,2009;Gabrilo-vich et al.,2012;Wu et al.,2014).Thus,it remains unclear which type of MDSC to target and which MDSC subpopulation(s) contributes to immunosuppression.MDSCs express combina-tions of myeloid-associated cell-surface markers and have an immature myeloid phenotype,but their hallmark functional char-acteristic is their ability to suppress T cells.(Gabrilovich et al., 2007;Peranzoni et al.,2010;Schouppe et al.,2013;Talmadge and Gabrilovich,2013;Youn et al.,2012).MDSCscomprise Immunity41,947–959,December18,2014ª2014Elsevier Inc.947heterogeneous mixtures of mature and immature granulocytes, monocyte-macrophages,and more primitive cells such as band-form granulocytic precursors(Gabrilovich et al.,2007;Ga-brilovich and Nagaraj,2009;Movahedi et al.,2008;Youn et al., 2012).So far,there is no accepted marker system to predict whether a MDSC will be suppressive without evaluating its sup-pressive function using in vitro T cell assays.However,the pres-ence of activated T cells or local inflammatory milieus engenders changes in MDSCs and alters their functional activity(Haver-kamp et al.,2011).Thus,functional dissection of MDSCs is a type of‘‘Schro¨dinger’s Cat’’scenario where suppression is monitored using an assay that induces the functional property for which it is testing(Haverkamp et al.,2011).Because the specific MDSC subpopulations required for T cell suppression remains controversial,efforts to engineer MDSCs have not yet advanced to the point at which a defined cell type is used ther-apeutically(Highfill et al.,2010;Yin et al.,2010).Similarly,inhib-iting the key suppressive subtype(s)of MDSCs to enhance T cell function might be an avenue to improve antitumor immunity via interruption of the tumor-induced immunosuppressive milieu (Gajewski et al.,2013;McAllister and Weinberg,2014;Restifo et al.,2012).In the mouse,most studies focus on the accumulation of CD11b+Gr-1+cells in the blood,spleen,and local inflammatory site,and human MDSC counterparts have been defined(Tal-madge and Gabrilovich,2013).Murine MDSCs are further subdivided by surface expression of Ly6C and Ly6G.Granulo-cytic MDSC are Ly6G+,Ly6C+,whereas monocytic MDSC (mixtures of immature monocytes,macrophages,and mono-cyte-derived dendritic cells)are Ly6G lo,Ly6C+.Based on these and other markers including F4/80,CD115,and IL-4R a,elaborate strategies have been used to separate MDSCs, and both granulocytic(referred to here as PMN-MDSC) and monocytic(Mo-MDSC)MDSCs have demonstrated immunosuppressive properties.However,further examination into the function of these cells has been impeded given that MDSC cell-surface markers have overlapping expression with other cell types and no transcription factor deficiencies have yet been described to ablate specific MDSC subpopula-tions(Gabrilovich and Nagaraj,2009;Movahedi et al.,2008; Priceman et al.,2010;Schouppe et al.,2013;Youn et al., 2012).Thus heterogeneity is an inherent hurdle toward under-standing the role of regulatory myeloid cells in chronic inflam-mation.To overcome this obstacle,we sought to define MDSC subpopulations using properties of intrinsic and extrinsic cell death pathways involved in myeloid lineage development and survival.Herein we demonstrated the hierarchy of cell death pathways required for the development,survival,and function of MDSCs,and define monocytic MDSCs as the dominant immunosuppressive subset.Further,we demon-strated that the antiapoptotic molecule c-FLIP is constitutively required for the development of Mo-MDSCs and that the in-duction of the MCL-1-related antiapoptotic A1(three closely related A1isoforms are encoded by Bcl2a1a,Bcl2a1b,and Bcl2a1c)by GM-CSF further promotes their survival.In contrast,PMN-MDSCs require a different antiapoptotic mole-cule MCL-1for development,and the loss of granulocytes through conditional MCL-1ablation does not contribute to tu-mor growth or incidence.RESULTSGenetic Manipulation of Death Pathways Skews Suppressor PopulationsImmature monocytic(Mo)and granulocytic(PMN)cells can be expanded in vitro from BM myeloid precursors with interleukin-6(IL-6)and GM-CSF(Marigo et al.,2010).Like MDSCs isolated from spleens of cancer-bearing mice(Ugel et al.,2012),BM myeloid cells grown in GM-CSF and IL-6exhibit a continuum of Ly6C and Ly6G expression(Figure1A).Hereafter we refer to in vitro-generated populations of cells expanded from the BM as‘‘myeloid suppressors’’(MS)to avoid contention with specific definitions of in vivo MDSCs accumulating in nonresolving inflammation(Gabrilovich et al.,2007;Talmadge and Gabrilo-vich,2013).We harnessed previous observations about the role of extrinsic death receptor mediated and intrinsic mitochon-drial antiapoptotic pathways in regulating the development of myeloid lineages and devised a‘‘mirror image’’genetic system to generate MS cultures dominated by either the granulocytic or monocytic populations.To generate MS depleted of granulo-cytic lineages,we used mice bearing a conditional allele of the antiapoptotic bcl-2family member Mcl1crossed to the LysM-Cre deleter(Steimer et al.,2009).These animals(referred to as MCL-1D M)have a near complete ablation of mature granulocytes in tissues and blood but retain normal numbers of monocytes and macrophages(Dzhagalov et al.,2007;Steimer et al., 2009).BM-derived MS cultures from the MCL-1D M animals pre-sented an enriched Ly6C+,Ly6GÀMo-MS fraction and reduced PMN-MS fraction relative to controls(Figure1A,see also Figures S1A and S1B available online).Deletion of MCL-1in MS cultures was efficient,as immunoblotting showed a near complete absence of MCL-1protein(Figure S1C).Therefore MCL-1abla-tion was a means to skew MS populations such that the propor-tion of Mo-MS in the cultures was increased relative to control cultures.To generate a suppressor population skewed toward PMN-MS,we used mice lacking c-FLIP(encoded by Cflar)in the late myeloid lineages again using the LysM-Cre deleter(c-FLIP D M). c-FLIP is an inhibitor of the following extrinsic death pathways controlled by death receptor(DR)signaling:caspase-8-medi-ated apoptosis,and RIPK1and RIPK3-mediated necroptosis (Green et al.,2011;Newton et al.,2014).c-FLIP D M mice have hy-perproduction of granulocytes and a relative depletion of mono-cyte-derived macrophages(Gordy et al.,2011;Huang et al., 2010)and,in our colony,die before weaning.BM cultures from c-FLIP D M mice had inverse properties from the MCL-1D M MS cultures and were enriched for Ly6G+,Ly6C+PMN-MS(Fig-ure1A;Figures S1A and S1B).Using our matched genetic systems,we investigated the suppressive capacity of c-FLIP D M and MCL-1D M MS relative to control MS by monitoring OVA-specific CD8+T(OT-I)cell prolif-eration during in vitro T cell-MS cocultures.c-FLIP D M MS had negligible suppressive activity while MCL-1D M MS were enriched for suppression on a cell-for-cell basis(Figure1B;Figure S1D). To determine whether the lack of inhibitory function of PMN-MS was caused by the loss of monocytic cells in c-FLIP D M animals,we performed experiments wherein MCL-1D M and c-FLIP D M MS were mixed immediately prior to culture with OT-I cells,at afixed suppressor cell number per well.T cellImmunity Control of Myeloid Suppressors by Death Pathways948Immunity41,947–959,December18,2014ª2014Elsevier Inc.proliferation was inhibited only in the presence of high numbers of MCL-1D M MS (Figure 1C).These data demonstrate suppres-sion is principally found in the monocytic component of the MS pool.To further evaluate MS-mediated suppression of T cell pro-liferation,we sorted Mo-MS and PMN-MS from wild-type (WT)BM cultures based on CD11b-gated Ly6G and Ly6C expression (Figure S1E).Purified Mo-MS were suppressive,with detectable inhibitory effects on T cell proliferation even when cultured at a 1:20MS:OT-I cell ratio.However,when OT-I cells were cultured with PMN-MS,proliferation was inhibited,but only at the highest ratios,and lost as the number of PMN-MS was decreased by one dilution step (Figures S1F and S1G).One explanation for the differences between Mo-MS and PMN-MS in T cell suppressive activity could have been decreased viability of the PMN-MS.We therefore evaluated the viability of both MS populations at 24hr intervals throughout the duration of the T cell suppression assay.The percentage of live cells was measured using a viability dye (V405)detecting cell-surface amine groups,a hallmark of dead and dying cells.Viability was equivalent between Mo-MS and PMN-MS atallFigure 1.Death Pathways Can Be Used to Manipulate the Population Structure and Activity of MS(A–C)BM-generated MS were grown from MCL-1D M ,C57BL/6,or FLIP D M mice.(A)Flow cytometry analysis of MS cultures.Numbers indicate the percentage of CD11b +cells.Cytospins collected from MS cultures.Data are representative of no fewer than ten independent experiments.(B)Suppressive function of MS was measured using 53105CFSE-labeled OT-I cells cultured with titrated numbers of MS from each genotype in the presence of SIINFEKL peptide.CFSE dilution in CD8+cells was evaluated by flow cytometry.Gray shaded histograms show negative control wells cultured without peptide.Plots from four independent ex-periments are shown (n =2for each experiment).(C)Representative plots from two independent experiments (n =2for each experiment)showing CFSE dilution in in CD8+cells cultured with MCL-1D M MS mixed with varying numbers of FLIP D M MS to a final number of 23105total MS (top panel)or unmixed control MCL-1D M and FLIP D M MS (bottom panels).(D)Diagram showing how genetics can be used to modulate the composition and suppressive function of MS subpopulations.ImmunityControl of Myeloid Suppressors by Death PathwaysImmunity 41,947–959,December 18,2014ª2014Elsevier Inc.949time points measured.Therefore,PMN-MS fail to suppress T cell proliferation even though they survive equally as well as the sup-pressive Mo-MS (Figure S1H).Collectively,our genetic and sort-ing strategies resolve the long-standing issue of which subset in the MS pool is responsible for suppression of T cell proliferation,identifying monocytic MS as the dominant suppressive popula-tion (Figure 1D).c-FLIP Controls the Development of Monocytic Suppressorsc-FLIP inhibits FADD-caspase-8apoptotic and RIPK1-RIPK3-mediated necroptotic pathways (Figure 2A)(Green et al.,2011).Figure 2.c-FLIP Controls Mo-MS Viability(A)Diagram showing the role of c-FLIP in the in-hibition of caspase-8-mediated apoptosis and necroptosis.(B)Flow cytometry analysis of BM-MS generated from FLIP WT ,RIPK3WT ,FADD WT and c-FLIP KO ,RIPK3KO ,FADD KO triple-deficient mice.Numbers indicate the percentage of live cells (n =3inde-pendent experiments).(C)Flow cytometry analysis of BM-MS from Cflar fl/fl;Rosa -CreERT2mice treated with 4-OH tamoxifen at d3of culture.Ethanol at the same final concentration as the 4-OH tamoxifen cultures served as the control.Numbers indicate the per-centage of live cells (n =3independent experi-ments).(D)Cflar was exogenously deleted by 4-OH tamoxifen on d5of culture using BM-MS from Cflar fl/fl;Rosa -CreERT2mice on a Ripk3+/Àor Ripk3À/Àbackground.Control cells received ethanol.On d6Mo-MS were sorted and cultured with GM-CSF (50ng/mL)for 24hr,after which viability was assessed using V405staining.(E)Cflar was exogenously deleted by 4-OH tamoxifen in the presence or absence of QVD (20m M)on d5of culture using BM-MS from Cflar fl/fl;Rosa -CreERT2mice.Control cells received ethanol and DMSO.On d6Mo-MS were sorted and cultured with GM-CSF (50ng/mL)in the presence or absence of QVD (20m M)for 24hr.Viability was assessed using V405staining.Therefore if c-FLIP regulates Mo-MS sur-vival as predicted from the c-FLIP D M results,ablation of FADD and RIPK3should rescue Mo-MS even in a complete c-FLIP-deficient background.Unlike c-FLIP D M MS cultures (Figure 1A),BM from mice lacking c-FLIP,FADD,and RIPK3had Mo-MS (Figure 2B).Thus c-FLIP is important for the viability of Mo-MS through development in vitro but dispensable for PMN-MS.We confirmed this conclusion by depleting c-FLIP using tamoxifen-mediated Cre-deletion in Cflar fl/fl;Rosa-CRE-ERT2BM MS cultures (Figure 2C).Mo-MS were absent from the tamoxifen-treated,but not from vehicle control cultures,while PMN-MS werepresent in all conditions,arguing that c-FLIP is dispensable for PMN-MS but continuously required for Mo-MS.Because c-FLIP is required to inhibit both necroptosis and Caspase-8-mediated apoptosis,we next tested whether one or both pathways were involved in the viability of Mo-MS.We generated Cflar fl/fl;Rosa-CRE-ERT2mice on a RIPK3-deficient background.Following tamoxifen-mediated Cre-deletion,Mo-MS died,even in GM-CSF,arguing that viability of Mo-MS is controlled by c-FLIP inhibiting caspase-8-mediated apoptosis rather than RIPK1-RIPK3necroptosis (Figure 2D).Concurrent treatment of MS cultures with the pan-caspase inhibitor QVD at the time of tamoxifen-mediated Cflar ablation reduced cellImmunityControl of Myeloid Suppressors by Death Pathways950Immunity 41,947–959,December 18,2014ª2014Elsevier Inc.death(Figure2E).Therefore the viability of Mo-MS is controlled by c-FLIP inhibition of caspase-8mediated apoptosis rather than RIPK1-RIPK3necroptosis.Suppressors Are Dependent on the MCL-1–A1Axis Genetic experiments have shown that nearly all cells in the body have an absolute requirement for MCL-1(Opferman et al.,2003, 2005;Wang et al.,2013;Weber et al.,2010).Monocytic cells are an exception,because they seem to develop normally in the absence of MCL-1.However,MCL-1D M Mo-MS were more sen-sitive to death compared to control Mo-MS within BM MS and T cell cocultures(Figure3A,B).Therefore,we hypothesized expression of another antiapoptotic protein was being induced to compensate for the loss of MCL-1.We performed gene-expression studies in human and mouse MDSCs and observed high mRNA expression of the MCL-1-related factor A1(Figures S2A–S2D).Like MCL-1,A1is inhibited by the BH3-only protein NOXA and couples to the BAX-BAK mitochondrial intrinsic death pathway(Figure3C).A1gene expression is regulated by NF-k B, and the short half-life of A1protein is controlled posttranslation-ally(Lee et al.,1999;Wang et al.,1999).We therefore reasoned induction of A1might sustain Mo-MS viability in the absence of MCL-1and investigated what factors promoted A1expression. GM-CSF was a strong inducer of A1protein relative to TNF,IL-1a,or IL-1b(Figure3D)and rescued the viability of MCL-1D M Mo-MS(Figure3E).Therefore,GM-CSF is a key factor sustaining A1expression and regulates the viability of Mo-MDSCs in the absence of MCL-1.The Absence of MCL-1Primes Mo-MS for DeathOur data raised the possibility that the viability of MCL-1D M Mo-MS might be compromised when A1inducing factors were limiting.Therefore we determined whether sustained A1 expression was required to maintain the suppressive function of Mo-MS in the absence of MCL-1.When we sorted MCL-1D M or control C57BL/6Mo-MS from BM cultures,we found that MCL-1D M Mo-MS were more sensitive to death in the absence of cytokines compared to control Mo-MS(Figure3F; Figure S2E).Viability was rescued only in the presence of GM-CSF,presumably due to induction of A1(Figure3D;Figures S2E and S2F).When MCL-1D M Mo-MS were used in T cell suppression assays,we noted a striking reduction in their ability to block CD8+proliferation compared to control Mo-MS(Fig-ure3G)or the unsorted MCL-1D M Mo-MS cultures(Figure1). The mechanism involved rapid loss of viability of MCL-1D M Mo-MS during T cell suppression assay(Figure3A)causing an apparent decrease in suppressive function.Therefore,MCL-1D M Mo-MS require continuous exposure to cytokines to sustain A1expression.These data also provide an explanation for the survival of monocyte-lineage cells in the MCL-1D M mice,where high circulating amounts of GM-CSF are likely enforcing A1 expression(Steimer et al.,2009).In control Mo-MS cells‘‘constitutive’’MCL-1expression should be‘‘dominant’’to the effects of cytokine-regulated A1. In other words,the absence of A1alone should not affect Mo-MS viability.To test this,we used a Vav-regulated shRNA system to simultaneously deplete all three murine A1isoforms in mouse MDSC cultures(Ottina et al.,2012).As expected,A1-deficient Mo-MS retained their suppressive effects,arguing that A1is required for sustaining the viability of MO-MDSCs,but not for their suppressive function(Figures S2G and S2H). Requirement for c-FLIP in Mo-MS Cannot Be Bypassed A prediction from the experiments described above is Mo-MS survive because they express sufficient c-FLIP and require either MCL-1or exogenous stimulation(GM-CSF)to induce A1.What is the factor inducing c-FLIP?At multiple stages dur-ing development,DR signaling induces c-FLIP as a regulatory mechanism to suppress Caspase-8and RIPK3death.A candi-date DR ligand regulating Mo-MS survival is TNF(Hu et al., 2014;Sade-Feldman et al.,2013;Zhao et al.,2012).We there-fore asked whether TNF induced the expression of c-FLIP in Mo-MS.TNF and GM-CSF-treated Mo-MDSCs had increased expression of c-FLIP and maintained A1amounts similar to GM-CSF-treated cells(Figure4A).TNF+GM-CSF-treated PMN-MDSCs expressed c-FLIP and MCL-1and did not ex-press A1(Figure S3).Given that TNF+GM-CSF treatment induced both A1and c-FLIP in Mo-MS,we next sought to determine whether A1in the absence of c-FLIP could maintain Mo-MDSC viability in response to GM-CSF.To test this,we again used tamoxifen-mediated Cre-deletion of c-FLIP in MS cultures using Cflarfl/fl; Rosa-CRE-ERT2mice(Figures4B and4C).In the absence of c-FLIP,the viability of Mo-MS could not be restored by GM-CSF(Figures4B and4C).Thus,in Mo-MS,A1induction by GM-CSF to inhibit the intrinsic death pathway cannot bypass the absolute requirement for c-FLIP to inhibit the extrinsic Caspase-8death pathway.Together these data demonstrate c-FLIP is the dominant survival factor for Mo-MS develop-ment.However,development of Mo-MS also requires sufficient expression of either MCL-1or A1to ensure their survival (Figure4).Death Signaling and Immunosuppressive Function of MDSCs in CancerWe next sought to determine whether the death pathways con-trolling in vitro-generated MS similarly regulated the survival of MDSCs in malignancy.MDSCs accumulate in spleen,blood, and local site of tissue damage as inflammation increases(Ga-brilovich and Nagaraj,2009;Gabrilovich et al.,2012;Ugel et al.,2012).Several studies have demonstrated MDSCs have different functional properties based on the tissue site they are recovered from,and it is now clear that different signals control MDSC development or expansion and acquisition of immuno-suppressive function.However,an unexplored mechanism to account for the role that different organ sites play in MDSC func-tion is the acquisition of survival signaling.We therefore tested how the anatomical site influences the suppressive function and expression of death signaling inhibitors in MDSCs during tumor growth.Bulk populations of splenic MDSC from control or MCL-1D M mice bearing EG7tumors were enriched for Mo-MDSC and had stronger suppressive activity relative to controls (Figures5A and5B).When the suppressive activity of MDSC subsets isolated from the spleens(Figure5C)or tumors(Fig-ure5D)of EG7tumor bearing C57BL/6mice was evaluated we found suppressive activity was principally found in the Mo-MDSC fraction(Figures5C and5D).Expression of death inhibitors in Mo-MDSC isolated from spleens and tumors wasImmunityControl of Myeloid Suppressors by Death PathwaysImmunity41,947–959,December18,2014ª2014Elsevier Inc.951Figure 3.A1and MCL-1Are Needed to Maintain the Survival of Mo-MS(A and B)BM-MS were grown from C57BL/6or MCL-1D M mice.The percentage of cell death was measured by V405staining of control or MCL-1D M Mo-MS at d6of BM-MS culture (top)or after 24hr T cell suppression assay coculture (bottom).(B)Quantification of V405+cells from the experiments representative in (A).Data expressed as the mean ±the SD and are representative of two independent experiments.Statistical analysis with unpaired t tests was performed;*p %05,**p %005.(C)Diagram showing the role of A1and MCL-1in inhibiting the mitochondrial death pathway.(D)Lysates from C57BL/6MS cultures were subjected to immunoblotting for A1following 24hr stimulation with the cytokines shown,all at 50ng/mL.GRB2($26kDa)was used as the loading control.(E)The percentage of nonviable V405+Mo-MS after stimulation with cytokines (50ng/mL)is shown.Data expressed as the mean ±SD and are representative of no less than three independent experiments (n =2samples for each experiment).Statistical analysis with unpaired t tests was performed;****p %0.0001.(legend continued on next page)ImmunityControl of Myeloid Suppressors by Death Pathways952Immunity 41,947–959,December 18,2014ª2014Elsevier Inc.evaluated by immunoblotting.MCL-1was expressed in both spleen and tumor resident MDSCs,while c-FLIP and A1expres-sion were predominantly found in Mo-MDSCs isolated from the tumor site (Figure 5E).Therefore,Mo-MDSC expressed the high-est amount of antideath molecules at the tumor site,and consti-tutive expression of c-FLIP and A1distinguishes suppressive tumor resident Mo-MDSC from their splenic counterparts (Fig-ures 5C–5E).Our data using the EG7model demonstrate that Mo-MDSC are the principle immunosuppressive MDSC population during tumor growth.However,MDSC expansion and population structure can be affected by the source of the primary tumor (Gabrilovich et al.,2012).Therefore,we next asked whether Mo-MDSC were the dominant immunosuppressive population of MDSCs in other transplantable tumor models.Mice bearing Lewis lung carcinoma (LLC)or B16melanoma (B16)tumors had expanded populations of Mo-and PMN-MDSC in the spleen and tumor (Figures S4A and S4B).Mo-MDSCs isolated from EG7,LLC,and B16tumors strongly inhibited T cell prolif-eration whereas PMN-MDSCs isolated from EG7or LLC tumors failed to inhibit T cell proliferation (Figures 5D and 5F;Fig-ure S4C).Evaluation of PMN-MDSC from B16tumors was not possible given the low number of PMN-MDSCs infiltrating these tumors (Figure S4B).Further,tumor-resident Mo-MDSCs,but not PMN-MDSCs,inhibited polyclonal T cell activation in vitro (Figure 5G).Taken together,these data identify Mo-MDSC as the principle immunosuppressive population of MDSCs during cancer.(F)The percentage of nonviable V405+Mo-MS was evaluated by V405staining after 24hr stimulation with the indicated cytokines (ng/mL)(n =3independent experiments).Quantification of data,expressed as the mean ±SD from one independent experiment.Statistical analysis with unpaired t tests was performed;**p %0.005.(G)Suppressive function of MS was measured using 53105CFSE-labeled OT-I cells cocultured with titrated MS in the presence of SIINFEKL peptide.CFSE dilution was evaluated by flow cytometry after 72hr.Data are compiled from three independent experiments and are presented as mean ±SD.Figure 4.Exogenous Regulation of A1Partially Rescues c-FLIP Loss(A)BM-MS were grown from C57BL/6mice.Mo-MS cell lysates were subjected to immunoblotting for the indicated targets following 24hr stimulation with the cytokines shown (ng/mL).GRB2($26kDa)was used as the loading control.Protein lysates from FLIP D M MS served as a specificity control for c-FLIP expression.(B and C)BM-MS cultures from Cflar fl/flRosa-Cre-ERT2+or Cflar fl/flRosa-Cre-ERT2Àmice were treated with tamoxifen or ethanol as a control on D5of BM culture.(B)On day 6,Mo-MS were sorted and cultured with cytokines for 24hr:GM-CSF (50ng/mL),TNF (5ng/mL).Viability was measured by V405staining.Representative histograms are gated on Ly6C +cells.(C)Mo-MS were sorted and cultured with the indicated cytokines for 24hr.The percentage of nonviable V405+cells in Mo-MS cultures was measured by flow cytometry.Data are expressed as the mean ±SD from one independent experiment and are representative of two independent experiments (two mice per group).Statistical analysis with unpaired t tests was performed;****p %0.0001.ImmunityControl of Myeloid Suppressors by Death PathwaysImmunity 41,947–959,December 18,2014ª2014Elsevier Inc.953。
扎伊尔埃博拉病毒糖蛋白泛MHC Ⅱ限制性表位预测及验证

308细胞与分子免疫学杂志(Chin J Cell M ol Immunol)2021,37(4)•论著•文章编号:1007-8738(2021 )04>0308"07扎伊尔埃博拉病毒糖蛋白泛m h c n限制性表位预测及验证刘洋1A,孙昊1△,陆振华2,兰明福、许家豪、孙报增\姜东伯杨琨W(空军军医大学,基础医学院免疫学教研室,2军事预防医学系军队防疫与流行病学教研室,陕西西安710032)[摘要]目的生物信息学预测获得埃博拉病毒(E B0V)糖蛋白泛主要组织相容性复合体n(MHC I I)限制性优势表位,分析 其特征并筛选鉴定可用于疫苗研制的候选对象。
方法通过IEDB分析预测EBOV糖蛋白的优势表位,并对优势表位进行聚类 分析,保守性分析和分子对接。
同时,利用编码糖蛋白DNA的质粒PVAX-GP免疫小鼠,酶联免疫斑点试验(ELISpot)验证预测 获得的表位。
结果在构成人群覆盖率达99%的人类白细胞抗原n(HLA I I)超家族限制性15表位肽预测中筛选获得19个优 势表位,H-2筛选获得13个优势表位。
ELISpot结果显示PVAX-GP可诱导小鼠脾细胞产生针对合成优势表位的细胞免疫反应,其中表位LFLRATTELRTFSIL和GYYSTTIRYQATGFG在C3H小鼠体内具有显著激活细胞免疫反应的效果。
保守性分析结果中 存在种间和种内均保守的优势表位,不存在种内不保守而种间保守的优势表位。
分子对接显示实验鉴定的两条优势表位可在 人HLA II类超家族分子中均可获得良好的对接分数,进一步肯定其在人群免疫中应用的可行性。
结论多肽LFLRATTELRTFSIL 和GYYSTTIRYQATGFG 可作为EB0V 表位疫苗的候选表位。
[关键词]扎伊尔埃博拉病毒(EB0V);泛主要组织相溶性复合体II (pan-MHC II )限制性表位;表位预测;保守性分析;分子对接 [中图分类号]R373.9, R392. 1[文献标志码]APrediction and verification of pan-MHC II restricted epitopes in the glycoprotein of Zaire Ebola virusLIU Yang I A,SUN Hao1A ,LU Zhenhua', Lan Mingfu' ,XU Jiahao1,SUN Baozeng' ,JIANG Dongbo1*, YANG Kun'*1 Department of Immunology, School of Basic Medicine, 2Department of Epidemiology, School of Public Health, Air Force Medical University, X i’an 710032,China* Corresponding authors, E-mail:*******************.cn;**************************[A b s tra c t] Objective To analyze the characteristics of pan-MHC n restricted dominant epitopes of Ebola virus glycoprotein and identify candidate epitopes for vaccine development by bioinformatic prediction and downstream analysis. Methods The dominant epitopes of Zaire Ebola virus glycoprotein were predicted by using lEDB-recommended prediction tool and analyzed by cluster analysis, conservation analysis, and molecular docking. Mice were immunized with the plasmid pVAX-GP encoded glycoprotein DNA, and the predicted epitopes were verified by ELISpot assay. Results There were 19 and 13 dominant epitopes obtained from the prediction of restricted 15-mer epitopes binding to the HLA n superfamily with 99% population coverage and the H-2, respectively. ELISpot assay showed that pVAX-GP induced mouse spleen cells to produce cellular immune responses against synthetic dominant epitopes, among which epitopes LFLRATTELRTFSIL and GYYSTTIRYQATGFG significantly activated cellular immune response in C3H mice. The results of conservation analysis showed that there were dominant epitopes of inter-species conservation and intra-species conservation, yet there were no dominant epitopes of inter-species conservation but no intra-species conservation. Molecular docking showed that the two dominant epitopes identified in the experiment obtained good docking scores in binding to HLA n superfamily molecules, which further confirmed the feasibility of their application in human immunity. Conclusion The polypeptides LFLRATTELRTFSIL and GYYSTTIRYQATGFG can be used as candidates for the Ebola virus epitope vaccine.[Key words] Zaire Ebola virus (EBOV) ;pan-MHC II restricted epitope;epitope prediction;conservation analysis;molecular ctocking收稿日期:2021 >014)3;接受日期:202(M)3-10基金项目:国家自然科学基金(82073154, 81772763)作者简介:刘洋(丨996-),女,陕西西安人,硕士研究生T el:155****0301;E-mail:844702157@A同为第一作者* 通讯作者,杨現,E-mail: yangkunkun@fm m ;姜东伯,E-mail: **************************4期刘洋,等.扎伊尔埃博拉病毒糖蛋白泛M HC n限制性表位预测及验证309扎伊尔埃博拉病毒(Zaire Ebola virus)通常称为 埃博拉病毒(£1)〇13^〇«,£80¥),是一种非节段负链RNA病毒。
下颌前牙根根管系统解剖及临床意义

参考文献
〔1〕J ahn R , Schiebler W , Quimet C , et al . A 380002Dalton membrane p rotein ( P38 ) p resent in synaptic vesicles[J ] . Proc Nail Acad Sci U SA , 1985 , 82 (12 ) :4137 - 4141.
〔2〕Wiedenmann B , Franke WW. Identification and localization of syn2 aptop hysin , an integral membrane gly ~ op rotein of Mr 38 , 000 characteristic of p resynaptic vesicles[J ] . Cell , 1985 ,41 (3) :1017 1028.
© 1994-2009 China Academic Journal Electronic Publishing House. All rights reserved.
·44 ·
SICHUAN JOURNAL OF ANATOMY VOL. 14 NO. 3 2006
43 33 327 327 65. 44 0 21. 1 3. 36 7. 65 2. 45
945 947 74. 97 2. 32 9. 19 4. 96 7. 18 1. 37
21 2 侧副根管检出率 ,见表 2 。下颌尖牙根管侧支检 出率为 22. 94 % ,其余侧副根管检出率均较低。下颌切 牙侧副根管检出率均较低 ,中切牙未检出管间吻合。
根管治疗中图分类号r3231文献标识码a熟悉牙根管的形态了解根管系统的点是提高根管治疗成功率的先决条件本实验采用真空负压吸人美兰染色的透明牙用体视显微镜对945颗下颌前牙牙根根管系统进行了检测
大三医学资料神经系统-英文

灰质gray matter皮质cortex 神经核nucleus白质white matter髓质medulla 纤维束fasciculus 神经结ganglion网状结构reticular formation脊髓spinal cord颈膨大cervical enlargem ent腰骶膨大lumbosac ral enlargem ent脊髓圆锥conus medullari终丝filum terminale马尾cauda equina中央管central canal中间带intermedi ate zone灰质连合gray commissu re前索anterior funiculus外侧索lateral funiculus后索posterior funiculus后角posterior horn后角边缘核posterom arginal nucleus胶状质substantia gelatinos后角固有核nucleus proprius胸核nucleus thoracicus前角anterior horn侧角lateral horn中间外侧核intermedi olateral nucleus骶副交感核sacral parasymp athetic nucleus背外侧束dorsolater al fasciculus薄束fasciculus gracilis楔束fasciculus cuneatus脊髓小脑后束posterior spinocere bllar tract脊髓小脑前束anterior spinocere bllar tract脊髓丘脑束spinothal amic tract皮质脊髓束corticospi nal tract端脑Telencep halon间脑Dienceph alon小脑Cerebellu m脑干Brain stem中脑Midbrain 脑桥Pons延髓Medulla oblongat a锥体Pyramid锥体交叉Decussati on of pyramid前外侧沟Anterolat eral橄榄Olive橄榄后沟Retrooliva ry sulcus薄束结节Gracile tubercle楔束结节Cuneate tubercle小脑下脚Inferior cerebellar peduncle脑桥小脑三角Pontocer ebellar triagone小脑中脚Middle cerebellar peduncle延髓脑桥沟Bulbopon tine基底沟Basilar sulcus小脑上脚Superior cerebellar peduncle上髓帆Superior medullary velum中脑Midbrain脚间窝Interpedu ncular fossa上丘Superior colliculus下丘Inferior colliculus菱形窝Rhomboi d fossa正中沟Median sulcus界沟Sulcus limitans髓纹Striae medullare s舌下神经三角Hypoglos sal triangle迷走神经三角Vagal triangle闩Obex脑室ventricle一般躯体运动核General somatic motor nuclei动眼神经核oculomot or滑车神经核trochlear nucleus展神经核abducent nucleus舌下神经核hypogloss al nucleus特殊内脏运动核 Special visceral motor nuclei三叉神经运动核motor nucleus of trigeminal面神经核facial nucleus疑核nucleus ambiguus副神经核 spinal accessory nucleus一般内脏运动核General visceral motor nuclei动眼神经副核accessory oculomot or上泌涎核superior salivatory nucleus下泌涎核 inferior salivatory nucleus迷走神经背核 dorsal nucleus of vagus一般、特殊内脏感觉核Visceral sensory nuclei ( general and special )孤束核nucleus of solitary tract一般躯体感觉核General somatic sensory nuclei三叉神经中脑核mesencep halic nucleusof trigeminal三叉神经脑桥核pontine nucleus of trigeminal三叉神经脊束核spinal nucleus of trigeminal特殊躯体感觉核Special somatic sensory nuclei蜗神经核cochlear nuclei前庭神经核vestibular nuclei薄束核gracile nucleus楔束核cuneate nucleus下橄榄核inferior olivary nucleus脑桥核pontine nucleus红核red nucleus黑质substantia nigra上丘superior colliculus下丘inferior colliculus内侧丘系Medial lemniscus脊髓丘脑束Spinothal amic tract三叉丘系Trigemina l lemniscus外侧丘系Lateral lemniscus脑桥被盖Tegment um of基底部Basis Pontis延髓内侧综合征medical medullary syndrome延髓外侧综合征lateral medullary syndrome脑桥基底部综合征basal pontine syndrome脑桥背部综合征dorsal pontine syndrome大脑脚底综合征peduncul ar syndrome本尼迪克特综合征Benedikt syndrome小脑Cerebellu m小脑半球cerebellar hemisphe re小脑蚓vermis小脑扁桃体Tonsil of cerebellu m前叶anterior lobe后叶posterior lobe绒球小结叶flocculon odular小脑脚Cerebellar peduncles小脑皮质cerebellar cortex原小脑Archicere bellum旧小脑Paleocere bellum新小脑Neocereb ellum间脑Dienceph alon背侧丘脑Dorsal thalamus后丘脑Metathala mus上丘脑Epithalam us底丘脑Subthala mus下丘脑Hypothal amus视交叉optic chiasma灰结节tuber cinereum漏斗Infundibul um垂体hypophys is乳头体mamillary body视上核Supraopti c nucleus室旁核Paraventri cular nucleus第三脑室Third ventricle端脑Telencep halon大脑皮质Cerebral cortex沟Sulcus 回Gyrus胼胝体Corpus callosum大脑纵裂Cerebral longitudin al fissure大脑横裂Cerebral transverse fissure中央沟Central sulcus外侧沟Lateral sulcus顶枕沟Parietooc cipital sulcus额叶Frontal lobe顶叶Parietal lobe枕叶Occipital lobe颞叶Temporal lobe岛叶Insular lobe中央前沟Precentral sulcus中央前回Precentral gyrus额上沟Superior frontal sulcus额下沟Inferior frontal sulcus额上、中、下回Superior, middle and inferioe frontal Gyri顶内沟Intraparie tal sulcus中央旁小叶paracentr al lobule海马Hippoca mpus边缘叶Limbic lobe侧脑室lateral ventricle基底核basal nuclei尾状核caudate nucleus豆状核lenticular nucleus杏仁体amygdalo id连合纤维Commiss ural fibers联络纤维associatio n fibers投射纤维Projecting fibers内囊internal capsule隔区septal area硬脊膜spinal dura mater硬膜外隙epidural space硬膜下隙subdural space脊髓蛛网膜spinal arachnoid mater软脊膜spinal pia mater蛛网膜下隙subarach noid终池Terminal cistern硬脑膜Cerebral dural mater脑蛛网膜Cerebral arachnoid mater软脑膜Cerebral pia mater大脑镰cerebral falx小脑幕tentorium of cerebellu m小脑镰cerebellar falx鞍隔diaphrag ma sellae上矢状窦Superior sagittal sinus下矢状窦Inferior sagittal sinus直窦Straight sinus窦汇Confluenc e of sinus横窦Transvers e sinus乙状窦Sigmoid sinus岩上窦superior petrosal sinuses岩下窦inferior petrosal sinuses海绵窦Cavernou s sinus蛛网膜粒Arachnoi d granulatio颈内动脉internal carotid artery大脑前动脉anterior cerebral artery大脑中动脉middle cerebral artery脉络丛前动脉anterior choroidal artery椎动脉vertebral artery基底动脉basilar artery大脑后动脉posterior cerebral artery脑脊液cerebrosp inal fluid (CSF)神经元Neuron 神经胶质细胞Glial cell无髓鞘神经纤维Unmyelin ated nerve fiber有髓鞘神经纤维Myelinate d nerve fiber顺向轴浆运输Anterogra de axoplasmi c transport逆向轴浆运输Retrograd e axoplasmi c transport电突触Electrical synapse化学性突触Chemical synapse兴奋性突触后电位Excitatory postsyna ptic potential, EPSP抑制性突触后电位Inhibitory postsyna ptic potential, IPSP突触的可塑性Synaptic plasticity习惯化Habituati on敏感化Sensitizati on长时程增强Long-time potentiati on, LTP长时程抑制Long-time depressio n, LTD神经调质Neuromo dulator乙酰胆碱Acetylcho line, ACh胆碱能神经元Cholinerg ic neuron胆碱能纤维Cholinerg ic fiber非条件反射Unconditi oned reflex条件反射Condition ed reflex单线式联系Single line connectio辅散式联系Divergent connectio n聚合式联系Converge nt connectio n连锁式Chain connectio n环 式Recurrent connectio n外感受器Exterocep tors内感受器Enterocep tors本体感觉Proprioce ption触-压觉Touch-pressure sensation温度觉Warm/col d sensation内脏痛Visceral pain牵涉痛Referred pain特异感觉接替核Specific sensory relay nucleus感觉联络核Associate d nucleus简化眼Reduced eye老视presbyopi a瞳孔近反射Near reflex of the pupil瞳孔的对光反射Pupillary light眼球会聚Converge nce近视Myopia远视Hyperopi a散光Antigmati sm视杆Rod 视锥细胞Cone视紫红质Rhodopsi n视敏度Visual acuity视野Visual field听阈Hearing threshold听域Hearing span气传导Air conductio n骨传导Bone conductio n耳蜗微音器电位 cochlear micropho nic potential, CM半规管Semicircul ar canals椭圆囊Utricle 球囊Saccule眼震颤Nystagm us反射运动Reflex motor activity随意运动Voluntary motor activity节律性运动Rhythmic motor activity运动单位Motor unit脊髓休克Spinal shock姿势反射Postural reflex屈肌反射Flexor reflex对侧伸肌反射Crossed extensor reflex牵张反射Stretch reflex腱反射Tendon reflex肌紧张Muscle tonus肌梭Muscle spindle反牵张反射Inverse stretch reflex去大脑僵直Decerebr ate Rigidity易化区Inhibitory area抑制区Facilitator y area状态反射Attitudina l reflex迷路紧张反射Tonic labyrinthi ne reflex颈紧张反射Tonic neck reflex翻正反射Righting reflex巴宾斯基征Babinski sign震颤麻痹Parkinson ’s disease舞蹈病Huntingto n’s disease自主神经系统Autonomi c Nervous System(A NS)非联合型学习non-associativ e learning联合型学习associativ e learning习惯化habituatio n敏感化sensitizati on经典条件反射condition ed reflex操作式条件反射operant conditioni ng遗忘症amnesia长时程增强long-term potentiati on , LTP长时程减弱long-term depressio n,LTD鬼影细胞ghost cell单纯性神经元萎缩simple neuronal atrophy中央性尼氏小体溶解central chromatol ysisWaller变性waller degenera tion噬神经细胞现象neuronop hagia小胶质细胞结节microglial node格子细胞gitter cell 卫星现象satellitosis流行性脑脊髓膜炎Epidemic cerebrosp inal meningiti流行性脑脊髓膜炎Epidemic cerebrosp inal meningiti流行性乙型脑炎Epidemic encephali tis B阿尔茨海默病Alzheimer disease老年斑senile plaque神经原纤维缠节neurofibri llary tangles,NFTs帕金森病Parkinson 's disease,P D镇静催眠药Sedative-hypnotic Drugs地西泮diazepam苯二氮卓类benzodia zepine drugs, BZD巴比妥类barbiturat es水合氯醛chloral hydrate唑吡坦zolpidem 佐匹克隆zopiclone右佐匹克隆eszopiclo ne抗癫痫药Antiepilep tic Drugs抗惊厥药Anticonvu lsive Drugs苯妥英钠Phynotoni n Sodium卡马西平Carbmaze pine苯巴比妥Phenobar bital乙琥胺Ethosuxi mide丙戊酸钠,德巴金Sodium Valproate硫酸镁Magnesiu m Sulfate抗帕金森病药物Anti-Parkinson Drugs左旋多巴Levodopa ( L-dopa)溴隐亭Bromocri ptine卡比多巴carbidopa苯海索Trihexyph enidyl阿尔茨海默病治疗药物Drugs for Alzheimer ’s Disease多奈哌齐donepezil 他克林tacrine利斯的明,卡巴拉汀,艾斯能Rivastigmi ne加兰他敏Galantami ne石杉碱甲,双益平Huperzin e A美金刚,易倍申Memantin e占诺美林Xanomeli ne吡拉西坦,脑复康Piracetam抗精神失常药Agents Against Psychiatri c氯丙嗪chlorpro mazine氟西汀fluoxetine碳酸锂lithium carbonate三环类抗抑郁药Tricyclic Antidepre ssants (TCAs)米帕明,丙米嗪Imipramin e选择性5-HT再摄取抑制药 SSRIs黛力新Deanxit 丁螺环酮Buspirone 氯氮平Clozapine奥氮平Olanzapin e利培酮,维思通Risperido ne卡马西平Carbamaz epine镇痛药Opioid Analgesic s吗啡morphine地芬诺酯,苯乙哌啶Diphenox ylate可待因,甲基吗啡Codeine 哌替啶Pethidine 度冷丁Dolantin美沙酮Methado ne芬太尼Fentanyl喷他佐辛,镇痛新Pentazoci ne布托啡诺Butorpha nol纳洛酮Naloxone解热镇痛抗炎药Nonsteroi dal Anti-inflammat ory Drugs阿司匹林aspirin 对乙酰氨基酚, 扑热息痛Acetamin ophen布洛芬Ibuprofen吲哚美辛Indometh acin吡罗昔康Piroxicam局部麻醉药Local Anestheti cs普鲁卡因Procaine 利多卡因Lidocaine丁卡因Tetracain e布比卡因Bupivacai ne全身麻醉药General Anestheti cs吸入性麻醉药Inhaled anesthetic s静脉麻醉药Intraveno us anesthetic s最小肺泡浓度Minimum alveolarconcentra tion, MAC 恩氟烷Enflurane 异氟烷Isoflurane硫喷妥钠Pentothal Sodium 丙泊酚Propofol 氯胺酮,K粉Ketamine 麻醉前给药Premedic ation基础麻醉Basalanesthesia诱导麻醉Inductionofanesthesia低温麻醉Hypothermalanesthesia控制性降压Controlledhypotensi on神经安定镇痛术Neurolept analgesia Neurolog yIntroduc tionNeuroexa m略头痛Headache头晕Dizziness 癫痫Seizure肌无力Myasthenia 昏迷Coma 痴呆Dementi a步态障碍gaitdisorder 偏头痛Migraine紧张性头痛Tension type headach e(TTH)丛集性头痛Cluster headach e良性阵发性位置性眩晕Benign Paroxys mal Positiona l Vertigo (BPPV)前庭神经原炎Vestibula r neuroniti s(VN)后循环缺血Post-cycle ischemia( PCI)偏头痛眩晕症Migraino us vertigo( MV)自动症Automati sm短暂性脑缺血发作Transient Ischemic Attacks, TIA格林巴利综合症Guillain-Barrésyndrom e谵妄delirium 模糊vague嗜睡Somnole nce昏睡Stupor。
猪诱导多能干细胞可定向分化为前脑GABA能神经元前体

doi 10.12122/j.issn.1673-4254.2021.06.03
J South Med Univ, 2021, 41(6): 820-827
猪诱导多能干细胞可定向分化为前脑 GABA 能神经元前体
朱 缓 1,孙婷婷 2,王圆圆 2,王 铁 2,马彩云 2,王春景 2,刘长青 2,郭 俣 1 蚌埠医学院 1检验医学院,2生命科学学院,安徽 蚌埠 233000
摘A 能神经元前体的方法体系。方法 猪 iPSCs 诱导分化为 GABA 能神经元前体遵循两个阶段,第 1 阶段,猪 iPSCs 悬浮培养,第 3 天时形成类胚体,采用神经诱导培养基 NIM(SB431542、 DMH1、FGF2)继续诱导,第 12 天分化为原始神经上皮细胞。第 2 阶段,使用含 Pur、B27 的 NIM 培养基悬浮培养形成神经球,至 第 21 天时形成 GABA 能神经元前体。CM-DiI 标记后,定向移植帕金森(PD)模型大鼠黑质纹状体,检测其在宿主脑内存活、迁 移及分化状况。结果 猪 iPSCs 在饲养层细胞上稳定传代,表达多能性标记 OCT4、Nanog、SSEA1 和 TRA-160,并且核型分析显 示没有其他物种来源细胞污染。第 12 天经诱导分化获得原始神经上皮细胞能够形成玫瑰花环结构,并表达其表面标记物 (PAX6、SOX2 和 Nestin)与神经微管蛋白标志物 Tuj1。第 21 天诱导细胞高表达 GABA 能神经元前体的表面特异性抗原 NKX2.1 和前脑标志物 FOXG1。移植 8 周后,体内可分化为 GABA 能神经元与多巴胺能神经元,明显改善 PD 大鼠运动行为。 结论 结合无血清培养基筛选法逐步定向诱导猪 iPSCs 高效分化为前脑 GABA 能神经元前体,移植后能够显著改善 PD 大鼠的 运动功能障碍,为诱导 GABA 能神经元前体移植治疗神经损伤疾病奠定基础。 关键词:诱导多能干细胞,猪;细胞分化;原始神经上皮细胞;GABA 能神经元前体;帕金森模型大鼠
新型非苯二氮艹卓类镇静催眠药扎来普隆

中闺新药与临床杂志(ChinJNewDrugsCliaRem),2000年11月,19(6):495498新型非苯二氯蕈类镇静催跟药扎栗警隆李年芳,顾牛范(卜海市精神卫生中心,上海200030)e关毽诃】礼来普隆;GABA-苯并二氨革受体;催眠药和镇静药;药理学;药物动力学f摘要】失眠是一秽常见鲍癌状,镇静催隈药是主要姆治疗手提。
新莺哉来普隆与苯=氯革娄镇静催眠药不离。
它舆寄对受俸作用选择性强、起教快、不曼反应步等特点。
本文就扎采普隆的药理作用、临床应用等作一鲸述。
【中圉挣粪号】R971.3[文献标识秘】A[文章编号】1007—7669(2承J0)06.0495。
04失眠是一种常见的症状,火多数词查发现成年入中发生率在5%~45%之间H’引。
在老年人中失眠更普遍。
正因如此,人们越来越重视其治疗问题。
镇静催眠药是治疗失眠蛙常用的药物,目前用得较多的必苯二蒸蕈豢药物,这类药物作用明显,假可能会gl起一定程度的药物婊竣及寤醉症状。
近几年,新型菲苯二氮摹类镇静催眠药得到较快发曩。
已用于幅床的新药有睦吼垣(zolpidem)及佐匿壳隆(zopiclone)。
由美国惠氐医药公司开发的孛L来普隆(zalepion)为更新的一种镇静催眠药。
药理作用扎来普隆的化学名为N.{3一[3-氰基吡唑(I,5一a)噻啶一7一y1]苯1.N。
乙基己魁胺{N。
[3-3一cyanopyrazolof1,5-a)pyrimidin一7+啦】Ncthytaeimamide}。
结构式冕缀t。
在中枢神经系统,存在2种苯二氮苹(Rz)受体i亚整,即Bzl,Bz2或者埘1,嗡受体。
Bz】受体主要、位于与镇静作用有关的大脑区域,H品受体主要集中于与认知、记忆、精神运动作用有关的区域13J。
、大多数苯二氮革类药物对受体的作熙并无选择性,j这榉蘸不可避免地;l起耱秘神经系统不良反应。
掰。
型扮非苯二二氮革类镇静摧瞩药不具祷苯二氮蕈类药。
静的一些不丧蕊虚,这类药物造择髓作沼予丫_氨基、丁馥一受俸复合俸(GABk"受体复台体)上的BZ受鼙】扎来警盛的分手绪棒式体。
分子生物学常用参考书目
二十一世纪是分子生物学发展的世纪,生命科学将进 入一个新的时代——后基因组时代postgenomics
二十一世纪分子生物学发展的趋势:
1.功能基因组学 functional genomics 依附于对DNA序列的了解,应用基因组学的知识和工具
去了解影响发育和整个生物体的特征序列表达 谱。 酿酒酵母16条染色体的全部序列于1996年完成 。
…
1997
Wilmut成功获得克隆羊—Dolly诞生;
1998
Renard 克隆牛诞生(体细胞→个体);
…
2000 ,6.26 中、美、日、德、法、英6国,宣布人类基 因组草图发表。
2000 ,10月 科学家宣布将于2001年3月完 成河豚鱼的基 因组测序。
2000,12月14日英美等国科学家宣布绘出拟南芥基因组 的完整图谱。
2003年4月14日六国科学家完成了人类基因组序列图的 绘制,实现了人类基因组计划的所有目标。
二十世纪是以核酸为研究核心,带动分子生 物学向纵深发展:
•
50年代双螺旋结构
•
60年代操纵子学说
•
70年代DNA重组
•
80年代PCR技术
•
90年代DNA测序
生命科学从宏观→微观→宏观;由分析→综 合的时代。
分子生物学常用参考书 目
2024/2/1
第一章 绪 论
一、什么是分子生物学?
Instant Notes in Molecular Biology
---Turner et al.
Molecular biology seeks to explain the relationships between the structure and function of biological molecules and how these relationships contribute to the operation and control of biochemical processes.
还脑益聪方对早期认知功能障碍大鼠海马病理形态、炎症因子和氧化应激指标的影响

・
实 验研 究 ・
还脑 益聪 方对 早期认 知功 能 障碍 大 鼠海 马病 理 形态 、 炎症 因子和 氧化应 激 指标 的影 响
姚 明江 李 浩
【 摘要】 目的
赵文 明 刘剑 刚 徐立 官杰 蔡琳 琳
观察还脑益聪方对复合 因素所 致早期认知功 能障碍大 鼠行 为学 及海马病理形
—
( S — T 含 量 。结 果 GH S)
鼠海马神经细胞损伤 、 线粒体病 变及 胶质 细胞增 生, 降低海 马匀 浆 T F—O及 O N t X—L L含量 ( D P<
00 , 00 ) .5 P< . 1 。结 论 还 脑 益 聪 方 能 提 高 早 期 认 知 功 能 障 碍 模 型 大 鼠的 空 间 学 习 记 忆 能 力 , 可 这 能 与其 抑 制 脑 内 炎症 反 应 与 氧 化应 激 , 而 减 轻 海 马 组织 病 理 变 化 有 关 。 从
maoy f co n x d t n sr s n xo i o a usi o n t e i tr a t ra d o i ai te side fhpp c mp n c g ii mpar n asa al tg n u e y o v ime tr t te rysa ei d c d b
・
3 0・ 0
世 界 中西 医结合 杂 志 2 1 00年第 5卷第 4期
WodJunl fnert r ioa adWet M d i 2 1 , o 5 N . r orao It a dTa tnl n l g e di s m e in e c e 00 V 1 , o4 .
t nmcocp ( E w r ue ei h ahm rhl i l hne o ipcm u ; erdo m — r i so e T M) ee sdt rv wtepto o o g a cags f poa ps t aii u o r o e p oc h h m
颞叶癫痫与海马成体神经再生

颞叶癫痫与海马成体神经再生陈立颖;汪仪;陈忠【期刊名称】《浙江大学学报(医学版)》【年(卷),期】2017(046)001【摘要】Temporal lobe epilepsy (TLE) is a common and severe neurological disorder which is often intractable.It can not only damage the normal structure and function of hippocampus, but also affect the neurogenesis in dentate gyrus (DG).It is well documented from researches on the animal models of TLE that after a latent period of several days, prolonged seizure activity leads to a dramatic increase in mitotic activity in the hippocampal DG.However, cell proliferation returns to baseline levels within 3-4 weeks after status epilepticus (SE).Meanwhile, there are two major abnormalities of DG neurogenesis, including the formation of hilar basal dendrites and the ectopic migration of newborn granule cells into the polymorphic cell layer, which may affect epileptogenesis and seizure onset.However, the specific contribution of these abnormalities to seizures is still unknown.In other words, whether they are anti-epileptic or pro-epileptic is still under heated discussion.This article systematically reviews current knowledge on neurogenesis and epilepsy based on the results of studies in recent years and discusses the possible roles of neurogenesis in epileptogenesis and pathologic mechanisms, so as to provide information for the potential application of neurogenesis as a new clinical therapeutictarget for temporal lobe epilepsy.%颞叶癫痫是一种严重的慢性中枢系统疾病,难治性比例非常高,它不仅会损害海马的结构功能,还会影响海马齿状回区的成体神经再生.颞叶癫痫模型研究表明,海马齿状回区的内源性神经干细胞在癫痫持续状态后会迅速激活,神经再生水平显著提高,而在癫痫发作后期(慢性期)神经元再生水平降低至正常水平以下;另外,癫痫持续状态后产生并分化成熟的颗粒细胞会存在异常的形态和位置,并有可能异常整合到海马神经环路并对癫痫的形成和发作产生影响.然而,癫痫后的成体神经再生对于癫痫是利是弊仍存在较大争议.本文对近年来颞叶癫痫后成体神经再生的数量、形态和功能的研究进展进行综述,讨论成体神经再生在癫痫形成和病理机制中扮演的角色,为日后临床上以成体神经再生作为癫痫治疗调控的新靶点研究提供借鉴.【总页数】8页(P22-29)【作者】陈立颖;汪仪;陈忠【作者单位】浙江大学药学院, 浙江杭州 310058;浙江大学药学院, 浙江杭州310058;浙江大学药学院, 浙江杭州 310058【正文语种】中文【中图分类】R741.02;R742.1【相关文献】1.颞叶内侧癫痫手术治疗:前颞叶切除术与选择性杏仁核海马切除术 [J], 王承雄;刘定阳;杨治权;杨转移2.阿司匹林通过促进海马功能性神经再生改善颞叶癫痫慢性期小鼠的空间记忆能力[J], 朱坤;胡明;杨蓬勃;张建水;陈新林;刘建新3.前颞叶切除术与选择性海马杏仁核切除术治疗海马硬化性颞叶内侧癫痫疗效比较[J], 钱海燕;马羽;许尚臣;庞琦4.前颞叶切除术(ATL)与选择性海马杏仁核切除术(SAH)治疗海马硬化性颞叶内侧癫痫的疗效评价 [J], 吕京波;马德志;刘秋芬5.前颞叶切除术与选择性杏仁核海马切除术治疗颞叶癫痫的疗效对比 [J], 李亚飞;尹绍雅因版权原因,仅展示原文概要,查看原文内容请购买。
瘤样炎性脱髓鞘病MRI的临床意义

复长期的变化最终导致癫的激发且不断反复。
那么,颞叶癫的不断发作有可能是52HT 2C 受体含量较少的原因,同时它的反复发作加重了神经损伤,导致52HT 2C 受体含量进一步减少。
Lie w 等[5]用Positr on em issi on t omogr aphy w ith (18)F 2trans 242fluor o 2N 222[42(22m ethoxy phenyl )pipe r azin 212yl ]e thyl 2N 2(22pyridyl )cycl ohexane ca r boxa m ide (18F 2FC WA Y PET )发现,MR I正常的难治性颞叶癫患者病灶区52羟色胺(52HT )1A 受体结合率下降,也从另外一方面证实52HT 2C 受体的结合率也有可能下降,导致其含量较少。
本研究还发现短病程(<10年)的患者其52HT 2C 受体的表达高于长病程组(>10年),这可能与癫反复发作,神经损伤有关。
本实验也存在一定的缺陷,没有和正常脑组织进行比较分析,还有待进一步研究。
参 考 文 献[1] Jas eja H.Defi n iti on of ep ilep s y:sign i ficance of its revisi on on clinicalneu r ophysi ol ogical basis t o i mp rove p r ognosis and quality of li fe of patients with e p ilep s y .M ed Hypo t hes es,2009,72:7562757.[2] M idzyanovs kaya I S,Kuznets ova G D,van Luijtelaar EL,et al .The brain5HTer gic res pons e t o an acute s ound stress i n rats wit h generalized (abs ence and aud i ogeni c)epile p sy .B rai n Res B ull,2006,69:6312638.[3] Jaku s R ,GrafM ,Juhasz G,et al .52HT2C recep t o rs inhibit and 52HT1A recep t o rs acti vat e the generati on of s p ike 2wave discharges in a geneti c rat m odel of ab s ence ep ilep s y .Exp Neu r ol,2003,184:9642972.[4] B arnes ,N M.,Shar,T .A revie w of central 52HT rece p t o r and theirfuncti on.Neurop har m aco l ogy,1999,38:108321152.[5] L i ew CJ,L i m Y M ,B onwets ch R,et al .18F 2FC WAY and 18F 2F DGPET in MR I 2negative te mporal lobe ep il ep sy .Ep ilep si a,2009,50:2342239.(2009210230收稿)论 著瘤样炎性脱髓鞘病MR I 的临床意义张文洛 戚晓昆 刘建国 王 起 林 伟 赵全军 于新 【摘要】 目的 分析瘤样炎性脱髓鞘病(TI D D )临床、影像与病理特点,探讨磁共振(MR I )检查对TI D D 的诊断价值。
Cell-free nucleic acids as biomarkers in cancer patients

In 1948, Mandel and Métais 1 described the presence of cell-free nucleic acid (cfNA) in human blood for the first time. This attracted little attention in the scientific com-munity and it was not until 1994 that the importance of cfNA was recognized as a result of the detection of mutated RAS gene fragments in the blood of cancer patients 2,3 (TIMELINE). In 1996, microsatellite altera-tions on cell-free DNA (cfDNA) were shown in cancer patients 4, and during the past decade increasing atten-tion has been paid to cfNAs (such as DNA, mRNA and microRNAs (miRNAs)) that are present at high concentra-tions in the blood of cancer patients (FIG. 1). Indeed, their potential value as blood biomarkers was highlighted in a recent editorial in the journal Science 5.Detecting cfNA in plasma or serum could serve as a ‘liquid biopsy’, which would be useful for numer-ous diagnostic applications and would avoid the need for tumour tissue biopsies. Use of such a liquid biopsy delivers the possibility of taking repeated blood sam-ples, consequently allowing the changes in cfNA to be traced during the natural course of the disease or during cancer treatment. However, the levels of cfNA might also reflect physiological and pathological processes that are not tumour-specific 6. cfNA yields are higher in patients with malignant lesions than in patients without tumours, but increased levels have also been quantified in patients with benign lesions, inflammatory diseases and tissue trauma 7. The physi-ological events that lead to the increase of cfNA during cancer development and progression are still not well understood. However, analyses of circulating DNA allow the detection of tumour-related genetic and epi-genetic alterations that are relevant to cancer develop-ment and progression. In addition, circulating miRNAs have recently been shown to be potential cancer biomarkers in blood.This Review focuses on the clinical utility of cfNA, including genetic and epigenetic alterations that can be detected in cfDNA, as well as the quantification of nucleo s omes and miRNAs, and discusses the relationship between cfNA and micrometastatic cells.Biology of cfNAThe release of nucleic acids into the blood is thought to be related to the apoptosis and necrosis of cancer cells in the tumour microenvironment. Secretion has also been suggested as a potential source of cfDNA (FIG. 1). Necrotic and apoptotic cells are usually phagocytosed by macrophages or other scavenger cells 8. Macrophages that engulf necrotic cells can release digested DNA into the tissue environment. In vitro cell culture experiments indicated that macrophages can be either activated or dying during the process of DNA release 8. Fragments of cellular nucleic acids can also be actively released 9,10. It has been estimated that for a patient with a tumour that weighs 100 g, which corresponds to 3 × 1010 tumour cells, up to 3.3% of tumour DNA may enter the blood every day 11. On average, the size of this DNA varies between small fragments of 70 to 200 base pairs and large fragments of approximately 21 kilobases 12. Tumour cells that circulate in the blood, and micro-metastatic deposits that are present at distant sites, such as the bone marrow and liver, can also contribute to the release of cfNA 13,14.T umours usually represent a mixture of different cancer cell clones (which account for the genomic and epig-enomic heterogeneity of tumours) and other normal cell types, such as haematopoietic and stromal cells. Thus, during tumour progression and turnover both tumour-derived and wild-type (normal) cfNA can be released into the blood. As such, the proportion of cfNA that originates from tumour cells varies owing to the state*Institute of T umour Biology, Center of ExperimentalMedicine, University Medical Center Hamburg-Eppendorf, Hamburg 20246, Germany.‡Department of Molecular Oncology, John Wayne Cancer Institute, Santa Monica, California 90404, USA.Correspondence to K.P . e-mail:pantel@uke.uni-hamburg.de doi:10.1038/nrc3066Published online 12 May 2011microRNAsSmall non-coding RNAmolecules that modulate the activity of specific mRNA molecules by binding and inhibiting their translation into polypeptides.Cell-free nucleic acids as biomarkers in cancer patientsHeidi Schwarzenbach*, Dave S. B. Hoon ‡ and Klaus Pantel*Abstract | DNA, mRNA and microRNA are released and circulate in the blood of cancerpatients. Changes in the levels of circulating nucleic acids have been associated with tumour burden and malignant progression. In the past decade a wealth of information indicating the potential use of circulating nucleic acids for cancer screening, prognosis and monitoring of the efficacy of anticancer therapies has emerged. In this Review, we discuss these findings with a specific focus on the clinical utility of cell-free nucleic acids as blood biomarkers.and size of the tumour. The amount of cfNA is also influ-enced by clearance, degradation and other physiological filtering events of the blood and lymphatic circulation. Nucleic acids are cleared from the blood by the liver and kidney and they have a variable half-life in the circulation ranging from 15 minutes to several hours7. Assuming an exponential decay model and plotting the natural loga-rithm of cfDNA concentration against time, serial DNA measure m ents have shown that some forms of cfNA might survive longer than others. When purified DNA was injected into the blood of mice, double-stranded DNA remained in the circulation longer than single-stranded DNA15. Moreover, viral DNA as a closed ring may survive longer than linear DNA15. However, regardless of its size or configuration, cfDNA is cleared from the circulation rapidly and efficiently16. miRNAs seem to be highly stable, but their clearance rate from the blood has not yet been well studied in cancer patients owing to the novelty of this area of research. The nuclease activ-ity in blood may be one of the important factors for the turnover of cfNA. However, this area of cfNA physiology remains unclear and needs further examination. Circulating cfDNADNA content. In patients with tumours of different histo-pathological types, increased levels of total cfDNA, which consists of epigenomic and genomic, as well as mito-chondrial and viral DNA, have been assessed by different fluorescence-based methods (such as, PicoGreen stain-ing and ultraviolet (UV) spectrometry) or quantitative PCR (such as, SYBR Green and TaqMan). Although cancer patients have higher cfDNA levels than healthy control donors, the concentrations of overall cfDNA vary considerably in plasma or serum samples in both groups17–19. A range of between 0 and >1,000 ng per ml of blood, with an average of 180 ng per ml cfDNA, has been measured20–23. By comparison, healthy subjects have concentrations between 0 and 100 ng per ml cfDNA of blood, with an average of 30 ng per ml cfDNA7. However, it is difficult to draw conclusions from these studies, as the size of the investigated patient cohort is often small and the techniques used to quantify cfDNA vary. A large prospective study assessed the value of plasma DNA levels as indicators for the development of neoplastic or pulmonary disease. The concentration of plasma DNA varied considerably between the European Prospective Investigation into Cancer and Nutrition (EPIC) centres that were involved in the study. This variation was pro-posed to be due to the type of population recruited and/or the treatment of the samples24. However, the quantifica-tion of cfDNA concentrations alone does not seem to be useful in a diagnostic setting owing to the overlapping DNA concentrations that are found in healthy individuals with those in patients with benign and malignant disease. The assessment of cfDNA concentration might prove to be useful in combination with other blood tumour bio-markers. Following surgery, the levels of cfDNA in cancer patients with localized disease can decrease to levels that are observed in healthy individuals25. However, when the cfDNA level remains high, it might indicate the presence of residual tumour cells17. Further studies are needed for the repeat assessment of quantitative cfNA in large cohorts of patients with well-defined clinical parameters. Such investigations will be crucial if we are to use cfDNA as a prognostic biomarker, as will the isolation and processingof cfNA to defined standards (discussed below).cfDNA is composed of both genomic DNA (gDNA) and mitochondrial DNA (mtDNA). Interestingly, the levels of cell-free mtDNA and gDNA do not correlate in some tumour types26,27, indicating the different nature of circulating mtDNA and gDNA. In contrast to two copies of gDNA, a single cell contains up to several hundred copies of mtDNA. Whereas gDNA usually circulates in a cell-free form, circulating mtDNA in plasma exists in both particle-associated and non-particle-associated forms28. Diverging results have been reported regarding whether cell-free mtDNA levels are increased and clinically relevant in cancer patients.The cfDNA can also include both coding and non-coding gDNA that can be used to examine microsatellite instability, loss of heterozygosity (LOH), mutations, poly-morphisms, methylation and integrity (size). In recent years, considerable attention has been paid to non-coding DNA, particularly repetitive sequences, such as ALU (which is a short interspersed nucleic element (SINE)) and as long interspersed nucleotide elements such as LINE1 (REFS 29–31) (discussed below). ALU and LINE1 are dis-tributed throughout the genome and are known to be less methylated in cancer cells compared with normal cells32. Tumour-specific LOH. Genetic alterations found in cfDNA frequently include LOH that is detected using PCR-based assays13,18,33–38(TABLE 1). Although similar plasma- and serum-based LOH detection methods have been used, a great variability in the detection of LOH in cfDNA has been reported. Despite the concordance between tumour-related LOH that is present in cfDNA in blood and LOH that is found in DNA isolated from matched primary tumours, discrepancies have also been found7. These contradictory LOH data that have been derived from blood and tumour tissue and the low incidence of LOH in cfDNA have partly been explained by technical problems and the dilution of tumour-associated cfDNA in blood by DNA released from normal cells11,39–41. Moreover, the abnormal proliferation of benign cells, owing to inflammation or tissue repair processes, for example, leads to an increase in apoptotic cell death, the accumulation of small, fragmented DNA in blood and the masking of LOH42.Alternative approaches, such as the detection of tumour-specific deletions are needed to better address the inherent problems of LOH analyses.Tumour-specific gene mutations.The analysis of cfDNA for specific gene mutations, such as those in KRAS and TP53, is desirable because these genes have a high mutation frequency in many tumour types and contribute to tumour progression43. Additionally, clini-cally relevant mutations in BRAF, epidermal growth factor receptor (EGFR) and adenomatous polyposis coli (APC) have now been studied in cfDNA. Several thera-peutic agents in clinical trials target the KRAS, BRAF, EGFR or p53 pathways44,45, and require the identifica-tion of the mutation status of the patient’s tumour to predict response to treatment. In this regard, cfDNA provides a unique opportunity to repeatedly monitor patients during treatment. In particular, in stage IV cancer patients, biopsies are not possible or repeat sam-pling of primary tumour and metastatic samples is not practical or ethical.The major problem with this approach has been assay specificity and sensitivity. Assays targeting cfDNA mutations require that the mutation in the tumour occurs frequently at a specific genomic site.A major drawback of cfDNA assays is the low frequency of some of the mutations that occur in tumours. In general, wild-type sequences often interfere with cfDNA muta-tion assays. This is due to the low level of cfDNA mutations and the dilution effect of DNA fragments and wild-type DNA in circulation. In PCR-based assays technological design can significantly limit the assay sensitivity and specificity. An example is the KRAS muta-tion tissue assay that can frequently detect mutations in tumour tissues, such as the pancreas, colon and lung;Quantitative real-time clamp PCR assayA technique that uses a peptide nucleic acid clamp and locked nucleic acid probes, which are DNA synthetic analogues that hybridize to complementary DNA and are highly sensitive and specific for recognizing single base pair mismatches.however, cfDNA mutation assays using blood sam-ples have not yet been concordantly successful46–48.New approaches are needed, such as cfDNA sequenc-ing. The BRAF mutation V600E, which is present in>70% of metastatic melanomas, can be detectedin cfDNA and has been shown to be useful in monitor-ing patients with melanoma who are receiving ther-apy49. This mutation has been detected in differentstages of melanoma (according to the American JointCommittee on Cancer (AJCC) Cancer Staging Manual)using a quantitative real-time clamp PCR assay, with thehighest levels found in the more advanced stages49. Thisis one of the first major studies to demonstrate thatcfDNA mutation assays have the sensitivity to monitorpatient responses before and after treatment. The util-ity of a cfDNA BRAF mutation assay has gained moreimportance, as new anti-BRAF drugs, such as PLX4032(Roche)50 and GSK2118436 (GlaxoSmithKline)51, haveshown substantial responses in patients in early clinicaltrials. EGFR mutations that occur in a specific subset ofpatients with lung cancers52–54 make these tumours sen-sitive to EGFR-targeted therapies; however, the detec-tion of EGFR mutations in cfDNA has not been welldeveloped owing to issues with sensitivity and specifi-city. Patients whose tumours have a specific gene muta-tion would be strong candidates for monitoring of theircfDNA in blood for the respective specific mutation.However, sensitivity, specificity and validation needto be carried out in multicentre settings to determinetrue clinical utility. Alternatively, cfDNA assays mightbe more appropriate when used with other biomarkerassays, and this might be applicable to personalizedmedicine, rather than diagnostic screens that can beused across a wide group of cancer patients.DNA integrity. Another assay that is applicable to cfDNAthat has gained interest in recent years is the integrityof non-coding gDNA, such as the repeat sequences ofALU and LINE1. The ALU and LINE1 sequences havebeen referred to as ‘junk DNA’; however, in recentyears evidence has indicated their importance invarious physiological events, such as DNA repair,transcription, epigenetics and transposon-based activ-ity55,56. Approximately 17–18% of the human genomeconsists of LINE1. In normal cells LINE1 sequencesare heavily methylated, restricting the activities ofthese retrotransposon elements and thus preventinggenomic instability. LINE1 sequences are moderatelyCpG-rich, and most methylated CpGs are locatedin the 5′ region of the sequence that can function asan internal promoter23. These forms of DNA can bedetected as cfDNA of different sizes, but also as methyl-ated and unmethylated DNA. Studies on these types ofcfDNA are still in their infancy; however, recent studieshave shown potential prognostic and diagnostic util-ity23,29–31. The assays are based on the observation thatcommon DNA repeat sequences are preferentiallyreleased by tumour cells that are undergoing non-apoptotic or necrotic cell death, and these fragmentscan be between 200 bp and 400 bp in size. The ALU andLINE1 sequences are well interspersed throughout thegenome on all chromosomes, so although specificity understood; tumour burden and tumour cell proliferation rate may have a substantial role in these events. Individual tumour types can release more than one form of cfDNA.for an individual cancer type is lost in these assays, sen-sitivity is enhanced. Using a PCR assay, the integrity of cfDNA ALU sequences in blood has been shown to be sensitive for the assessment of the early stages of breast cancer progression, including micro m etastasis30. DNA integrity cfDNA assays have also been used in testicular, prostate, nasopharyngeal and ovarian cancer31,57–59. These assays are still in their infancy and address an important challenge of whether a ‘universal’ blood biomarker for multiple cancers can be of clinical utility. Further validation of these assays will also determine their clinical utility in specific cancers.Table 1 |Detection of cfDNA and its alterations in patients with different tumour types*cancers in both males and females182. This table is not meant to be comprehensive and is based on our own view of studies that offer substantial clinical insight. cfDNA, cell-free DNA.Epigenetic alterations. Epigenetic alterations can have a substantial effect on tumorigenesis and progression (BOX 1). Several studies have revealed the presence of methylated DNA in the serum or plasma of patients with various types of malignancy (TABLE 1). The detection of methylated cfDNA represents one of the most promising approaches for risk assessment in cancer patients. Assays for the detection of promoter hypermethylation may have a higher sensitivity than microsatellite analyses, and can have advantages over mutation analyses. In gen-eral, aberrant DNA methylation, which seems to be com-mon in cancer, occurs at specific CpG dinucleotides60. The acquired hypermethylation of a specific gene can be detected by sodium bisulphite treatment of DNA, which converts unmethylated (but not methylated) cytosines to uracil. The modified DNA is analysed using either methylation-specific PCR, with primers that are specific for methylated and unmethylated DNA, or DNA sequenc-ing61. Nevertheless, to improve the assay conditions and the clinical relevance, the selection of appropriate tumour-related genes from a long list of candidate genes that are known to be methylated in neoplasia is essential. Although epigenetic alterations are not unique for a single tumour entity, there are particular tumour suppressor genes that are frequently methylated and downregulated in certain tumours62,63. For example, important epigenetic events in carcinogenesis include the hypermethylation of the promoter region of the genes pi-class glutathione S-transferase P1 (GSTP1) and APC, which are the most common somatic genome abnormalities in prostate and colorectal cancer, respectively62,63. Other important methylated genes that have shown prognostic utility using cfDNA assays in significant numbers of patients include RAS association domain family 1A (RASSF1A), retinoic acid receptor-b (RARB), septin 9 (SEPT9), oestrogen receptor-a (ESR1)and cyclin-dependent kinase inhibitor 2A (CDKN2A) (TABLE 1). The first commercial real-time PCR plasma test for the detection of early colorectal cancer (developed by Epigenomics AG and Abbott Molecular) is for the detection of SEPT9. This biomarker is still under-going validation, but it demonstrates the potential diag-nostic screening utility of methylated tumour-related cfDNA to differentiate cancer patients from healthy individuals and to identify the tumour type.It is also possible to detect tumour-related alterations in histone modifications in the blood. By monitoring changes in the circulating histones and DNA methylation pattern, the antitumour effects of histone deacetylase and histone methyltransferase inhibitors may be evalu-ated and consequently allow a better screening of cancer patients64,65.Circulating nucleosomes.Circulating gDNA that is derived from tumours seems to predominantly exist as mononucleosomes and oligonucleosomes, or it is bound to the surface of blood cells by proteins that harbour specific nucleic acid-binding properties66. A nucleosome consists of a histone octamer core wrapped twice by a 200 bp-long DNA strand. Under physiological condi-tions these complexes are packed in apoptotic particles and engulfed by macrophages67. However, an excess of apoptotic cell death, as occurs in large and rapidly pro-liferating tumours or after chemotherapy treatment, can lead to a saturation of apoptotic cell engulfment and thus increased nucleosome levels in the blood68. The detection of circulating nucleosomes that are associ-ated with cfDNA suggests that DNA in blood retains at least some features of the nuclear chromatin during the process of release.Enzyme-linked immunosorbent assays (ELISAs) have been developed to quantify circulating nucleosomes. As increased concentrations are found in both benign and malignant tumours, high nucleosome levels in blood are not indicators of malignant disease69. However, the observed changes in apoptosis-related deregulation of proteolytic activities along with the increased serum levels of nucleosomes have been linked to breast cancer progression70. As typical cell-death products, the quan-tification of circulating nucleosomes seems to be valu-able for monitoring the efficacy of cytotoxic cancer therapies71. For example, platinum-based chemotherapy induces caspase-dependent apoptosis of tumour cells and an increase in circulating nucleosomes in the blood of patients with ovarian cancer17. Moreover, the outcome of therapy can be indicated by nucleosome levels during the first week of chemotherapy and radiotherapy in patients with lung, pancreatic and colorectal cancer, as well as in patients with haematological malignancies71.Viral DNA. Viral cfDNA can also be detected in some tumour types. Viruses, such as human papillomavirus (HPV), hepatitis B virus (HBV) and Epstein–Barr virus (EBV), are aetiological factors in various malignancies, such as nasopharyngeal, cervical, head and neck, and hepatocellular cancer and lymphoma72–75. Their specific DNA may have the potential to be used as molecular biomarkers for neoplastic disease. Associations between circulating viral DNA and disease have been reported for EBV with Hodgkin’s disease, Burkitt’s lymphoma and nasopharyngeal carcinoma; for HBV with some forms of hepatic cell carcinoma; and for HPV with head and neck, cervical and hepatocellular cancers (TABLE 1). The clinical utility of EBV cfDNA in diagnosis and prognosis of nasopharyngeal carcinoma has been demonstrated in multiple studies with large cohorts of patients76–80, and the use of this cfDNA has became one of the leading cfDNA blood tests for the assessment of nasopharyngeal carci-noma progression in Hong Kong, Taiwan and China, where this cancer is highly prevalent77,78,81. The limitationof most viral cfNA assays is that benign viral infections that are caused by the same viruses can complicate the interpretation of results, particularly in diagnostic screen-ing. Establishing clinically meaningful cut-off levels is important to move these screens into the clinic. Genometastasis.The genometastasis hypothesis describes the horizontal transfer of cell-free tumour DNA to other cells that results in transformation. If true, metastases could develop in distant organs as a result of a transfection-like uptake of dominant oncogenes that are released from the primary tumour82. García-Olmo et al.83 showed that plasma isolated from patients with colon cancer is able to transform NIH-3T3 cells and that these cells can form carcinomas when injected into non-obese diabetic-severe combined immunodeficient mice83. Whether this biological function of circulating DNA has relevance in human blood is an aspect to be considered in the future.cfDNA assay issuesOne of the problems in evaluating cfNA is the standard-ization of assays, such as isolation technologies, standards, assay conditions, and specificity and sensitivity7. It remains controversial whether plasma or serum is the optimal sampling specimen. The diversity of protocols and reagents currently in use impedes the comparison of data from different laboratories.The pre-analytical phases of cfDNA analysis such as blood collection, processing (plasma and serum), storage, baseline of patients, diurnal variations and accurate clinical conditions need to be better defined before comparisons and clinical utility can be validated84.A major technical issue that hampers consistency in all the cfDNA assays is the efficacy of the extraction pro-cedures, with only small amounts of DNA obtained from plasma and serum. Another key issue is quanti-fication before assessment on specific assay platforms. Improvement is needed in these aspects for cfDNA analysis to be more robust, consistent, comparative and informative. Extraction of cfDNA can be carried out in accordance with many methods; for example, commer-cial kits, company in-house procedures or individual laboratory protocols. To date no approach has been truly developed that is consistent, robust, reproduc-ible, accurate, and validated on a large-scale patient and normal donor population. If these issues were solved a better universal standardization for the comparison of results would be provided and the clinical utility of the assays could be addressed. The development of a direct DNA assay without extraction would override many of these problems30. As new approaches in the assessment of cfDNA, such as next-generation sequencing, are being developed, the issue of extraction of DNA will continue to complicate cfDNA biomarker assay development and regulatory group approval.The other major issue for cfDNA assessment is that after DNA extraction, different platform assays are used for analysis. This can vary owing to the type of cfDNA being analysed, assay sensitivity and specificity, and ana-lytical approach. These variables are important and need to be standardized for consensus analysis and reporting. The development of PCR-based assay standardization is needed in order to report clinical and prognostic biomarker results that are similar to those outlined in the recent minimal information for the publication of quantitative real-time PCR guidelines85. However, this may take time to reach an international consensus, as has been apparent with the standardization of other cancer blood biomarkers. Unfortunately, the rate of approval of new cancer blood biomarkers over the past decade has been very slow. New regulatory guidelines, such as those listed for tumour biomarkers in clinical practice by the National Academy of Clinical Biochemistry (NACB USA)84, should help to resolve some of these issues. The NACB website provides up-to-date informative detailed guidelines with references of pre-analytical and post- analytical phases, assay validation, internal quality controls, proficiency and requirements for minimiz-ing the risk of method-related errors for biomarkers. Nevertheless, as with other types of biomarkers, new reg-ulatory guidelines mean that developing cfNA biomarkers will be more time-consuming and costly. Circulating cfRNAmRNA content. Besides the quantification of cfDNA, cir-culating gene transcripts are also detectable in the serum and plasma of cancer patients. It is known that RNA released into the circulation is surprisingly stable in spite of the fact that increased amounts of RNases circulate in the blood of cancer patients. This implies that RNA may be protected from degradation by its packaging into exosomes86, such as microparticles, microvesicles or multivesicles, which are shed from cellular surfaces into the bloodstream87. The detection and identification of RNA can be carried out using microarray technologies or reverse transcription quantitative real-time PCR88. Serum thyroglobulin levels are a specific and sensi-tive tumour marker for the detection of persistent or recurrent thyroid cancer. Levels of thyroglobulin change during thyroid hormone-suppressive therapy, as well as after stimulation with thyroid-stimulating hormone, and the levels correlate well with disease progression. The measurement of mRNA levels of thyroid-specific tran-scripts might be useful in the early detection of tumour relapse89. However, another study has shown that the detection of circulating thyroglobulin mRNA one year after thyroidectomy might be of no use in the prediction of early and midterm local and distant recurrences of this disease90.In patients with breast cancer, levels of CCND1 mRNA (encoding cyclin D1) identified patients with poor overall survival in good-prognosis groups and patients who were non-responsive to tamoxifen91. Nasopharyngeal carcinoma has been associated with disturbances in the integrity of cell-free circulating RNA, suggesting that the measurement of plasma RNA integrity may be a useful biomarker for the diagnosis and monitoring of malignant diseases92. Several groups have tried to detect human telo-merase reverse transcriptase (TERT) mRNA in plasma, and have not found any association between the pres-ence of this mRNA and clinicopathological parameters7.。
中国10个全面性癫痫伴热性惊厥附加症家系的临床特征分析

论 著中国10个全面性癫痫伴热性惊厥附加症家系的临床特征分析林 华 王玉平 王梦阳 吴立文 【摘要】目的 探讨中国全面性癫痫伴热性惊厥附加症(gene ra lized epilep s y with febrile se i zure plus,GEFS+)家系的临床特征。
方法 通过门诊就诊、个人访视、电话等方式,对10个GEFS+家系所有成员进行详细临床资料收集,包括家系图谱、有无发作、发作形式以及检查结果等。
结果 10个家系共有140名成员接受了调查(其中3名去世,由亲属提供病史),发现受累者80例,其中74例符合G EFS+临床发作谱,2例为特发性全面性癫痫,4例不能明确分类。
其中有两个家系较为特殊(家系I和家系H),2个家系受累者绝大部分仅表现为热性惊厥(febrile seizure,FS),每个家系仅有先症者1人表现为热性惊厥附加症(febril e s e izureplus,FS+)。
此外还发现3例FS+伴局灶性发作,2例为FS+伴儿童良性癫痫伴中央颞部棘波,1例为FS+伴颞叶癫痫。
结论 GEFS+是一种常见的、儿童时期起病的遗传性癫痫综合征,GEFS+最常见的表型为FS和FS+,其次是FS+伴局灶性发作、FS伴IG E、FS+伴失神发作以及FS+伴肌阵挛发作,我们的10个GEFS+家系中未发现FS+伴失张力发作、肌阵挛站立不能性癫痫和婴儿严重肌阵挛癫痫,说明这些表型为临床少见表型;此外我们还发现了GEFS+合并IGE以及在FS遗传背景上仅个别患者为FS+的较特殊家系,这些将进一步扩展G EFS+的概念。
【关键词】 癫痫;全面性;热性惊厥;突变分析中图分类号:R742.1 文献标识码:A 文章编号:1006-351X(2009)01-0005-04C li n ica l cha ra cter i stics of ten ped i gr ees with genera li zed ep i lep s y with febr il e se i zur es plus i n C h i n a L I NHua,WAN G Yu2pi ng,WANG M eng2yang,WU L i2wen.Depa rt m ent of Neur o l ogy,Xuanwu Hos p ital of Cap ita lMedicalUniversity,Be ijing100053,China.【Abstra c t】 O bjec ti ve T o de s c ribe the c linical cha racte ristics of ten China fam ili e s with gene ra lized epilep2s y with febrile se izure plus(GEFS+).M ethods The deta iled c linical da ta of a ll mem bers of ten GEFS+we re in2vestigated by visiting c linic service,indi vidual interview,telephone ca ll.The se data inc lude t he fa m ily pedi gree,sei2zure or no,type s of seizure s,re s ult of exa m i nati on,and so on.Resu lts 140members of ten fam ilies we re investi2gated and80pers ons a re affected individua l,which74pa tients me t the c riterion of G EFS+,2pa tients me t the diag2nosis of idi opathic generalized epilepsy(I GE),4pa tients were unclassified according t o their seizures.T wo G EFS+fa m ilies(fa m il y I and fam ily H)we re unusua l,which most of affected individua ls p re s ented febril e s e izure(FS),onlyproband of t w o fam ilies wa s febrile seizu re p lus(FS+).In additi on we still found three of FS+with focal seizure,t w o of FS+wit h benig n epilepsy with centro-tempora l s p ikes,one of FS+wit h tempora l l obe epilep s y.C onclu si on Our da t a support t he vie w that GEFS+is a co mmon he redit ory ep ilep tic syndro m e which is onset in childhood.Themost co mmon phenotypes of GEFS+are FS and FS+,next are FS+with focal s e izure,FS with foca l seizure,FS+with absence se i zure and FS+with m y oc l onic seizure.The re is not FS+wit h atonic se izure,m y oclonic2astatic ep i2l epsy and severe m y oc l oni c ep ilep sy of infancy,which i ndi ca te these phenoty p es are infrequent i n GEFS+.In the tenfa m ilies of GEFS+,we find GEFS+with I GE,t wo s pecia l fam ilie s tha t only one pers on present FS+in t he gene ticbackground of FS.The s e data will further extend the concept of GEFS+.【Key wor d s】 ep ilepsy;g enera lized;febrile s e izure;muta ti on ana lysis基金项目:中国博士后基金一等资助项目((2006039122)作者单位53 北京,首都医科大学宣武医院神经科(林华、王玉平);北京协和医院神经科(王梦阳、吴立文)通信作者吴立文,6@y 全面性癫痫伴热性惊厥附加症(GEFS+)是儿童期发病的常染色体显性遗传病,2001年国际抗癫痫联盟将“G FS+”作为一种新的综合征列入癫痫综合征分类中[]。
海马电刺激在癫(癎)治疗中的进展
电刺激参数选择的研究
对于最佳电刺激频率的选择问题上,仍然没有 达成共识.一部分研究者倾向于选择低频电刺激模 式(O.1—25 Hz),另一部分研究者倾向于选择高频 电刺激模式(130 Hz)。Barbarosie等用低频刺激
(0.25—1.5 Hz)在离体海马一内嗅皮质脑片上灌流无
镁人工脑脊液和4一氨基吡啶(4一AP)两种癫瘌模型, 剪断CA,和cA。问的联系后予低频电刺激(O.25~
万方数据
神经病学与神经康复学杂志2009年12月第6卷第4期J
Neuml Neuromhabil,December 2009,V01.6,No.4
要进一步的观察。一般认为主要的不良反应与DBs
适应证的研究
临床上DBS研究的人选病例都是药物控制不 好、外科手术禁忌的患者,对于具体的适应证不是很 明确。Velasco等长期致力于将DBS应用于难治性 癫痫的临床研究,在他们早期的一项临床试验中对 16例复杂部分发作的颞叶癫痢患者进行了海马电刺 激治疗。结果显示在电刺激的亚急性期(3—4周 内),在对临床发作频率和发作间期棘波个数的控制 方面要优于前颢叶切除术,而且经显微镜检查分析, 电刺激海马组织与未刺激海马组织相比较,没有显 示出病理异常;慢性期(3—4 m)能持续地抑制癫疴 发作的产生,并不伴对近记忆的影响;他们又用电生 理方法检测发现电刺激后海马组织产生了抑制效 应,这可能是其抗癫痫作用的机制之一¨“。Velasco 等对9例复杂部分性发作的患者进行了海马电刺激 治疗,并进行18个月的随访,MRI显示5例患者海马 正常,4例患者有海马硬化,治疗前发作次数为10— 50次/月;治疗后,5例海马正常的患者没有再发,4例 海马硬化的患者仍有少数发作;因此他们认为DBS技 术可能更适用于MRI正常的难治性癫痫患者¨“。 其他一些临床研究结果也都提示,海马电刺激 可能对起源于双侧、无硬化迹象的难治性颞叶癫痢 疗效要好。
《2024年MHR、NPAR、SII对进展性缺血性脑卒中发生预测价值的研究》范文

《MHR、NPAR、SII对进展性缺血性脑卒中发生预测价值的研究》篇一一、引言进展性缺血性脑卒中是一种常见的神经系统疾病,其发病机制复杂,病程进展迅速,给患者带来极大的健康风险。
因此,准确预测其发生对于制定有效的治疗方案和改善患者预后具有重要意义。
近年来,随着医学研究的深入,MHR(Mean Hematocrit Ratio,平均血细胞比容比)、NPAR(Neurological Parameters of Acute Stroke,急性卒中神经学参数)和SII(Systemic Immune-Inflammation Index,全身免疫炎症指数)等指标在缺血性脑卒中的预测和评估中逐渐受到关注。
本文旨在探讨MHR、NPAR、SII 对进展性缺血性脑卒中发生的预测价值,以期为临床诊断和治疗提供参考依据。
二、研究方法本研究采用回顾性分析方法,收集了某医院近三年内收治的缺血性脑卒中患者的临床数据。
纳入标准为年龄≥18岁、诊断为缺血性脑卒中、有完整的MHR、NPAR和SII等指标数据。
排除标准为患有其他严重神经系统疾病或恶性肿瘤等影响研究结果的患者。
根据患者病情发展情况,将患者分为进展性缺血性脑卒中组和非进展性组。
采用统计学方法比较两组患者在MHR、NPAR、SII等指标上的差异,并分析这些指标对进展性缺血性脑卒中发生的预测价值。
三、研究结果1. 患者基本情况本研究共纳入200例缺血性脑卒中患者,其中进展性组80例,非进展性组120例。
患者年龄、性别、基础疾病等方面无明显差异。
2. MHR与进展性缺血性脑卒中的关系研究结果显示,进展性组患者的MHR值明显高于非进展性组(P<0.05)。
进一步分析表明,MHR值越高,患者发生进展性缺血性脑卒中的风险越大。
3. NPAR与进展性缺血性脑卒中的关系NPAR指标在进展性组和非进展性组之间也存在显著差异(P<0.05)。
与MHR类似,NPAR值越高,患者发生进展性缺血性脑卒中的风险也越大。
布托啡诺在无痛胃镜中的应用及研究进展
- 160 -blood urea nitrogen (BUN) can predict mortality in acute pancreatitis: comparative study between BISAP Score, APACHE-Ⅱ, and other laboratory markers-a prospective observational study[J].Can J Gastroenterol Hepatol,2021,22:6643595.[37] DAI M,FAN Y,PAN P,et al.Blood urea nitrogen as aprognostic marker in severe acute pancreatitis[J].Dis Markers,2022,29:7785497.[38] WU B U,BAKKER O J,PAPACHRISTOU G I,et al.Bloodurea nitrogen in the early assessment of acute pancreatitis: an international validation study[J].Arch Intern Med,2011,171(7):669-676.[39]罗博文,邓德海,韦慧芬,等.早期液体复苏终点指标对急性胰腺炎容量评估的价值[J].临床肝胆病杂志,2020,36(12):2777-2781.[40] MUDDANA V,WHITCOMB D C,KHALID A,et al.Elevatedserum creatinine as a marker of pancreatic necrosis in acute pancreatitis[J].Am J Gastroenterol,2009,104(1):164-170.[41]耿金婷,王瑞峰,杨宁,等.血尿素氮、血肌酐、C-反应蛋白质对急性胰腺炎严重程度及预后的预测价值[J].中国临床医生杂志,2021,49(8):956-958.[42] WIESE M L,URBAN S,VON RHEINBABEN S,et al.Identification of early predictors for infected necrosis in acute pancreatitis[J].BMC Gastroenterol,2022,22(1):405.(收稿日期:2023-10-30) (本文编辑:陈韵)*基金项目:滨州医学院附属医院科研项目(滨附行发[2020]31号)①滨州医学院附属医院麻醉科 山东 滨州 256603通信作者:张全意布托啡诺在无痛胃镜中的应用及研究进展*孙瑶芮① 张全意① 【摘要】 近年来,我国胃肠道疾病的发病率逐渐增加,无痛胃镜检查则是最可靠、最常用的诊断方法。
儿童热性惊厥发病机制相关研究进展
Advances in Clinical Medicine 临床医学进展, 2023, 13(3), 3731-3735 Published Online March 2023 in Hans. https:///journal/acm https:///10.12677/acm.2023.133535儿童热性惊厥发病机制相关研究进展代 琛,贾鲲鹏*延安大学附属医院儿科,陕西 延安收稿日期:2023年2月13日;录用日期:2023年3月9日;发布日期:2023年3月16日摘要 惊厥是一种严重危害儿童身体健康甚至危及生命安全的危急重症,尽管对于儿童时期来说惊厥绝大多数预后是比较好的,但仍有部分呈反复发作,甚至会导致成人期的癫痫发作及认知功能障碍等神经系统后遗症。
惊厥的发作机制及病因复杂,儿童反复发生惊厥可能对神经系统遗留不同程度的后遗症,甚至发展为癫痫,因此成为目前国内外研究热点。
惊厥从发病至一次病情痊愈的过程中,给患儿、家庭及社会造成很大负担。
随着医学科学研究的不断进步,惊厥越来越引起学者们的关注,并较多地对病因、危险因素、发病机制、预测惊厥复发指标及预后方面的规律进行了研究,使临床医师对该类疾病的诊治有了更多认识,现对儿童时期发生惊厥的发病机制与血清学指标的改变相关研究进展作一综述。
关键词儿童惊厥,发病机制,热性惊厥,良性惊厥,中枢神经系统感染Advances in Research Related to the Pathogenesis of Febrile Convulsions in ChildrenChen Dai, Kunpeng Jia *Department of Paediatrics, Affiliated Hospital of Yan’an University, Yan’an Shaanxi Received: Feb. 13th , 2023; accepted: Mar. 9th , 2023; published: Mar. 16th , 2023AbstractConvulsion is a critical illness that seriously endangers children’s health and even life safety. Al-though the vast majority of convulsions in children have a good prognosis, some still have recur-*通讯作者。
影响因子10分以上的关于代谢产物的文章

影响因子10分以上的关于代谢产物的文章
以下是几篇关于代谢产物的影响因子(Impact Factor)大于10的文章的示例:
1. Ganna, A., et al. (2019). Large-scale GWAS reveals insights into the genetic architecture of same-sex sexual behavior. Science, 365(6456), eaat7693. Impact Factor: 41.037.
2. Chen, M., et al. (2018). Metabolomics reveals metabolite changes in coronary artery disease patients with myocardial infarction. Metabolomics, 14(4), 47. Impact Factor: 4.502.
3. Lawton, K. A., et al. (2008). Identification of a β-d-glucosidase in flax (Linum usitatissimum) involved in the biosynthesis of secoisolariciresinol diglucoside. Plant Journal, 54(3), 419-433. Impact Factor: 5.895.
请注意,这些文章只是作为示例提供,并且参考期刊的影响因子可能会随时间变化。
建议您使用学术数据库(如Web of Science、PubMed 等)来搜索特定领域的权威期刊和相关文章,以获取最新的高影响因子的代谢产物研究文章。
《2024年急诊PCI的STEMI患者PAB、Lp-PLA2与Zwolle评分的关系》范文
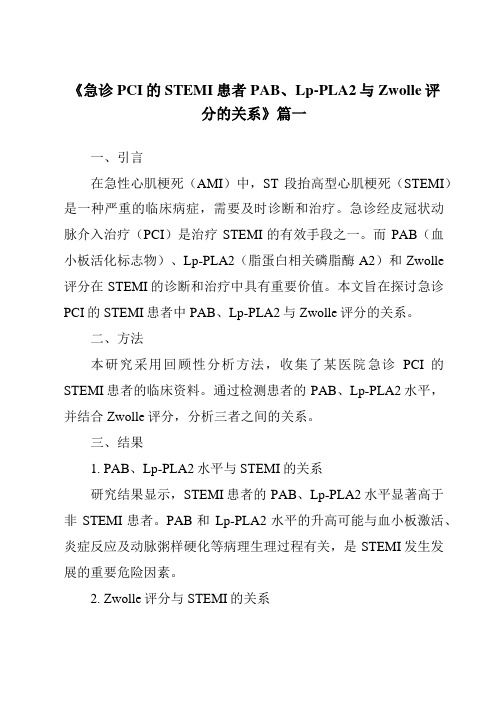
《急诊PCI的STEMI患者PAB、Lp-PLA2与Zwolle评分的关系》篇一一、引言在急性心肌梗死(AMI)中,ST段抬高型心肌梗死(STEMI)是一种严重的临床病症,需要及时诊断和治疗。
急诊经皮冠状动脉介入治疗(PCI)是治疗STEMI的有效手段之一。
而PAB(血小板活化标志物)、Lp-PLA2(脂蛋白相关磷脂酶A2)和Zwolle 评分在STEMI的诊断和治疗中具有重要价值。
本文旨在探讨急诊PCI的STEMI患者中PAB、Lp-PLA2与Zwolle评分的关系。
二、方法本研究采用回顾性分析方法,收集了某医院急诊PCI的STEMI患者的临床资料。
通过检测患者的PAB、Lp-PLA2水平,并结合Zwolle评分,分析三者之间的关系。
三、结果1. PAB、Lp-PLA2水平与STEMI的关系研究结果显示,STEMI患者的PAB、Lp-PLA2水平显著高于非STEMI患者。
PAB和Lp-PLA2水平的升高可能与血小板激活、炎症反应及动脉粥样硬化等病理生理过程有关,是STEMI发生发展的重要危险因素。
2. Zwolle评分与STEMI的关系Zwolle评分是一种用于评估AMI严重程度的评分系统。
本研究发现,Zwolle评分越高,STEMI患者的病情越严重。
Zwolle评分与患者的年龄、性别、心血管病史、心肌梗死部位及范围等因素有关。
3. PAB、Lp-PLA2与Zwolle评分的关系本研究还发现,PAB、Lp-PLA2水平与Zwolle评分之间存在正相关关系。
即PAB、Lp-PLA2水平越高,Zwolle评分越高,患者的病情越严重。
这提示我们,PAB、Lp-PLA2水平可以作为评估STEMI患者病情严重程度的重要指标。
四、讨论PAB是一种血小板活化标志物,其水平升高可能与血小板激活、血栓形成等有关。
Lp-PLA2是一种炎症标志物,参与动脉粥样硬化和血栓形成的过程。
两者在STEMI的发生发展过程中起着重要作用。
《2024年丁苯酞预处理对脑缺血再灌注大鼠皮质神经元超微结构和白介素-1β的影响》范文

《丁苯酞预处理对脑缺血再灌注大鼠皮质神经元超微结构和白介素-1β的影响》篇一一、引言脑缺血是一种常见的神经系统疾病,其病理过程涉及神经元损伤和炎症反应的复杂交互。
近年来,丁苯酞作为一种神经保护剂在脑缺血治疗中引起了广泛关注。
本实验旨在研究丁苯酞预处理对脑缺血再灌注大鼠皮质神经元超微结构和白介素-1β(IL-1β)的影响,以期为临床治疗提供理论依据。
二、材料与方法1. 实验动物与分组本实验选用健康成年SD大鼠,随机分为四组:正常对照组、缺血再灌注组、丁苯酞预处理组及假手术组。
2. 模型建立与药物处理采用线栓法建立大鼠脑缺血再灌注模型,丁苯酞预处理组在缺血前进行丁苯酞药物注射。
3. 观察指标通过透射电镜观察皮质神经元的超微结构变化,同时检测IL-1β的表达水平。
三、实验结果1. 神经元超微结构观察透射电镜结果显示,与正常对照组相比,缺血再灌注组大鼠皮质神经元出现明显的超微结构损伤,如线粒体肿胀、内质网扩张等。
而丁苯酞预处理组的大鼠皮质神经元超微结构损伤程度明显减轻。
2. IL-1β表达水平检测与正常对照组相比,缺血再灌注组大鼠IL-1β表达水平显著升高。
而丁苯酞预处理组大鼠IL-1β表达水平较缺血再灌注组明显降低。
四、讨论本实验结果表明,丁苯酞预处理能够减轻脑缺血再灌注大鼠皮质神经元的超微结构损伤,同时降低IL-1β的表达水平。
这可能与丁苯酞的抗炎和神经保护作用有关。
在脑缺血过程中,炎症反应是导致神经元损伤的重要机制之一,而IL-1β是一种重要的炎症介质。
丁苯酞可能通过抑制炎症反应,减轻神经元损伤,从而发挥神经保护作用。
此外,丁苯酞还可能通过改善线粒体功能、调节内质网应激等途径,进一步保护神经元超微结构。
五、结论本实验结果表明,丁苯酞预处理能够减轻脑缺血再灌注大鼠的神经元超微结构损伤和炎症反应,降低IL-1β的表达水平。
这为丁苯酞在脑缺血治疗中的应用提供了理论依据,为临床治疗脑缺血提供了新的思路和方法。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
MEG evaluation in temporal lobe epilepsy E. Pataraia, G. Lindinger, L. Deecke, and C. BaumgartnerUniversity Clinic of Neurology, Vienna, Austria1 IntroductionTemporal lobe epilepsies represent the most frequent form of focal epilepsies [1]. The seizures are frequently difficult to control with antiepileptic medication and eventually 30-50% of patients have to be considered as medically refractory. Epilepsy surgery can be considered as a valuable treatment option for these patients rendering 70-90% of them seizure-free [2]. Thus, exact localization of both the epileptogenic zone and essential brain regions which can only be accomplished during a thorough presurgical work-up is crucial for a successful surgical treatment and the improvement of non-invasive methods is clinically warranted. Magnetoencephalography (MEG) could improve the non-invasive evaluation of temporal lobe epilepsy patients for several reasons.First, MEG provides a superior spatial resolution as compared to scalp-EEG because magnetic fields are far less distorted than electric fields by the resistive properties of the skull and scalp measured [3]. Second, the advent of whole-head MEG systems represented a major breakthrough because simultaneous recordings from the entire brain can be obtained which is critical for the assessment of spontaneous brain activity.Thus, magnetic field generated by epileptic activity can be mapped in a single shot without repositioning the MEG probe inevitable with previous multichannel MEG systems [4].While numerous MEG studies in human temporal lobe epilepsy have been published [5-11], only few studies systematically assessed the merit of MEG in clearly defined temporal lobe syndromes [12,13] and its impact as well as practicability in a clinical setting [14]. We therefore assessed the following questions concerning MEG in temporal lobe epilepsy:1. What is the diagnostic yield of MEG intemporal lobe epilepsy? Are there differencesin diagnostic yield for the various subgroupsof temporal lobe epilepsy?2. What is the role of MEG for the evaluationof specific temporal lobe epilepsysyndromes, i.e. mesial TLE, non-lesionalTLE and lesional TLE? 2 Methods2.1 PatientsWe studied a total of 49 patients suffering from medically refractory temporal epilepsy who were evaluated in our epilepsy monitoring unit for possible epilepsy surgery. 26 patients suffered from mesial temporal lobe epilepsy (mesial TLE). 15 patients were diagnosed as non-lesional temporal lobe epilepsy (non-lesional TLE). Finally, in 8 patients structural lesions within the temporal lobes could be identified on MRI. As clinical seizure semiology, interictal spikes and ictal EEG changes proved that the lesions were responsible for the patients’ seizures, these patients were classified as lesional temporal lobe epilepsy (lesional TLE).All patients underwent an extensive presurgical work-up including intensive video-EEG-monitoring, high resolution MRI-scan, interictal SPECT, formal neuropsychological testing and an intracarotid sodium amytal test.2.2 MEGrecordingsMEG recordings were performed in all patients for a duration of 2-3 hours. MEG was performed with a 143 channel whole-head MEG (CTF Systems Inc., Port Coquitlam, B.C. Canada) in a large magnetically shielded room (Vacuumschmelze GmbH, Hanau, Germany). The MEG system consisted of an array of 143 first order axial gradiometers with 2 cm diameter and 5 cm baseline, uniformly distributed in a helmet-shaped liquid helium dewar. The average coil center separation was 3.2 cm covering the head down to an extent of 130 degrees from the vertex [15]. Scalp-EEG was recorded simultaneously from 23-26 gold-disk electrodes placed according the International 10-20 System with additional basal temporal electrodes. MEG signals were amplified, filtered (bandpass 1-70 Hz), analog-to-digital converted (sampling frequency = 250 Hz, 12 bits) and stored digitally for off-line data analysis.We used spontaneous spikes for dipole analysis in order to avoid introducing artificial time delays byaveraging variable spike populations. After visual inspection of the data and artifact rejection, we first calculated isofield maps using spherical spline interpolation. We then applied dipole modeling to calculate backwards unto the neuronal sources underlying the epileptic spike complex. We assumed a single equivalent current dipole as neural source and a spherical head model as volume conductor. The goal of the program was to find which combination of dipole location and orientation parameters most closely reproduced the data using a non-linear least squares minimization procedure.In order to correlate source localizations with anatomical structures on MRI, head position with respect to the sensing gradiometers was monitored by tracking 3 small coils placed at anatomical landmarks of the head, i.e. the nasion, the right and left pre-auricular points, defining a head based coordinate system during the MEG recording session [15]. Subsequently, MRI scans were performed with lipid-filled capsules placed at these fiducial points.3 Results3.1 Diagnostic yield of MEGDuring the MEG recordings interictal spikes could be recorded in 11 out of 26 patients with mesial TLE (= 42.3%), in 11 of 15 patients with non-lesional TLE (= 73.3%) and in 4 out of 8 patients with lesional TLE (= 50.0%; p=0.154). Although in most cases, interictal spikes could be identified both on scalp-EEG and MEG, in some instances spikes were visible on scalp-EEG but not on MEG, while the reverse, i.e. MEG spikes without EEG spikes occurred less often.3.2Mesial temporal lobe epilepsyIn patients with mesial TLE all spike dipoles could be localized to the temporal lobe with a clear preponderance of its medio-basal aspects. We observed two types of dipole orientations. In 6 patients interictal spikes could be modeled by so-called ‘anterior temporal vertical dipoles’ which were oriented vertically with their positive poles directed towards the vertex and their negative poles towards the basal temporal region resulting in a magnetic field emerging from the head at the anterior temporal and frontal recording positions and re-entering the head at the posterior temporal, temporo-parietal and temporo-occipital sensor positions (Fig. 1). In the other 5 patients so-called ‘anterior temporal horizontal dipoles’ were observed which were characterized by a horizontal orientation with their positive poles oriented posterior and their negative poles oriented anterior producing a magnetic field pattern emerging from the head at the inferior temporal sensor positions and re-entering the head at the superior temporal and central sensor locations (Fig. 2).a) b)Figure 1:Mesial temporal lobe epilepsy: anterior temporal vertical dipole: a) Isofield map and b) dipole localization projected unto MRI scan.a) b)Figure 2:Mesial temporal lobe epilepsy: anterior temporal horizontal dipole: a) Isofield map and b) dipole localization projected unto MRI scan3.3 Non-lesional temporal lobe epilepsy Whereas in 5 patients dipole sources were localized to the anterior medial temporal lobe, in the other 6 patients dipole localizations were attributed to the posterior and lateral temporal lobe. Dipole orientation was vertical in all patients with the positive poles directed superior and the negative poles inferior generating a magnetic field pattern emerging from the head at the anterior temporal and frontal recording positions and re-entering the head at the posterior temporal, temporo-parietal and temporo-occipital region (Fig. 3). In 3 patients - one with a medial and two with lateral vertical dipoles - invasive recordings with chronically indwelling subdural grid electrodes were performed. Whereas the seizure onset zone was confined to the medial temporal lobe in the patient with medial MEG spikes, in the other two patients with lateral MEG spikes invasive seizure onset was more widespreadinvolving both the lateral and medial temporal contacts.a) b)Figure 3: Nonlesional temporal lobe epilepsy: posterior lateral temporal vertical dipole: a) Isofield map and b) dipole localization projected unto MRI scan 3.4Lesional temporal lobe epilepsyIn patients with lesional TLE, MEG spike dipoles could be localized within or in the immediate vicinity of the lesion. Dipole orientations were variable across patients. We also studied a patient who had undergone a prior lesionectomy of a pilocytic astrocytoma. After an initial seizure-free interval the patient continued to experience seizures. MEG localized the most active spiking zone to the lateral border of the resection (Fig. 4).a) b)Figure 4: Lesional temporal lobe epilepsy: anterior temporal horizontal dipole: a) Isofield map and b) dipole localization projected unto MRI scan.4 Discussion4.1Diagnostic yield of MEGIn our patients the diagnostic yield of MEG during a single 2-3 hour recording session was 53.1%. During intensive video-EEG monitoring on the contrary, spikes could be recorded in all patients. Interictal spikes were recorded more often in patients with non-lesional TLE (73.3%) as compared to patients with mesial (42.3%) or lesional (50%)TLE although this difference did not reach statistical significance. Thus, MEG seems to be more sensitive to detect spikes in neocortical epilepsy which also was evident in a previous study where MEG spikes could be detected in 92% of patients with neocortical epilepsy, but only in 50% of patients with mesial TLE [14].There were more EEG spikes without simultaneous MEG spikes than MEG spikes without EEG spikes which is in agreement with previous combined MEG and EEG studies [9,16]. This finding can be explained by the selective sensitivity of MEG for tangential sources, while radial sources do not produce a detectable MEG signal. 4.2Interictal spikes in mesial temporal lobeepilepsyIn mesial temporal lobe epilepsy the dipolar sources underlying the interictal spike complex could be localized to the temporal lobe with a predominance of its medio-basal aspects in all patients. However, dipole localizations have to be interpreted with respect to the basic modeling assumptions underlying source modeling.Based on orientation dipoles could be classified into two types, namely an anterior temporal vertical dipole and an anterior temporal horizontal dipole. Dipole orientations were useful to identify temporal lobe subcompartments involved in epileptic activity. Thus, our anterior temporal vertical dipole is compatible with epileptic activity in the medio-basal temporal lobe and corresponds closely to the type 1 dipoles defined by Ebersole and Wade [17,18] using spike voltage topography and single instantaneous dipole modeling on scalp-EEG.The anterior horizontal dipole can be explained by epileptic activity of the temporal tip cortex as proposed by Ebersole [13].We therefore believe that dipole orientations are more important than absolute dipole localizations for an appropriate delineation of the irritative zone from MEG recordings. 4.3Non-lesional temporal lobe epilepsyNon-lesional epilepsy poses a major challenge in presurgical epilepsy evaluation because these patients usually require invasive recordings to adequately define the seizure onset zone [1].In our 11 patients with non-lesional TLE, MEG spike dipoles were localized either to the anterior medial (n=5) or to the posterior lateral temporal lobe (n=6). Dipole orientation was vertical in all cases. In the 3 patients in whom invasive recordings were performed the invasive EEG seizure onset agreed very well with the interictal MEG dipolelocalizations. Our results thus concur with the findings of Ebersole[13].In conclusion, interictal MEG spike dipole modeling may become a useful non-invasive method to differentiate mesial from lateral temporal epileptogenic zones in patients with normal MRI scans.4.4 Lesional temporal lobe epilepsyIn our patients with lesional TLE, MEG spike dipoles could be localized adjacent to the lesions visible on MRI scans. Numerous interictal MEG studies in patients with temporal lobe structural lesions have been reported [5,10,11,14]. MEG provided useful information for the placement of invasive electrodes and the planning of surgical strategy in these patients [18]. Furthermore, MEG may help to clarify the still poorly understood relationship of discrete lesions to the generation of seizures and more specifically whether lesionectomy alone or resection of the lesion plus the adjacent epileptogenic zone should be performed in these patients [19].5 ConclusionThe introduction of whole-head MEG systems has lead to a major breakthrough of the MEG application in clinical epileptology. MEG is useful to identify subcompartments of the temporal lobe involved in epileptic activity. Dipole orientations are more important than absolute dipole localizations for an appropriate delineation of the irritative zone. Whether the two dipole types identified in mesial TLE are of prognostic significance for surgical outcome and whether their occurrence should influence the surgical strategy remains to be determined. In non-lesional TLE MEG may help to differentiate between mesial, lateral or diffuse seizure onset zones and thus could reduce the need of invasive procedures in these patients. In lesional TLE MEG can help to define the spatial relationship between the structural lesion and the irritative zone which is important for surgical planning. Especially patients with persistent seizures after lesionectomy or epilepsy surgery will benefit from MEG, because the magnetic fields are less distorted by skull and dura defects introduced by the prior operation. The sensitivity of MEG seems to be higher in lateral TLE as compared to mesial TLE which underlines its potentials for the investigation of non-lesional neocortical TLE. MEG therefore can be regarded as a useful, clinically relevant non-invasive method to better define the interictal irritative spike zone in patients with temporal lobe epilepsies. AcknowledgementsThis work was supported by the Fonds zur Förderung der wissenschaftlichen Forschung Österreichs (project P12697-MED).References1. J. Engel Jr., ”Introduction to the temporal lobeepilepsies”, Epilepsy Res26, 141-50, 1996.2. J. Engel Jr., “Surgery for seizures”, New Engl JMed334, 647-652, 1996.3. S.J. Williamson and L. Kaufman, “Magneticfields of the cerebral cortex”, in: S.N. Erne,H.D. Hahlbohm, H. Lübbig, eds. Biomagnetism.Berlin: Walter der Gruyter, pp. 353-402, 1981.4. C. Baumgartner and L. Deecke, “Magneto-encephalography in clinical epileptology andepilepsy research”, Brain Topography2, 203-219, 1990.5. D.S. Barth, W.W. Sutherling, J. Engel, andJ. Beatty, “Neuromagnetic evidence of spatiallydistributed sources underlying epileptiformspikes in the human brain”, Science223, 293-296, 1984.6. C. Baumgartner, S. Di, W.W. Sutherling, andD.S. Barth, “ Spatiotemporal neuromagneticanalysis of the human epileptic spike complex”,Epilepsia29, 672, 1988.7. C. Baumgartner, W.W. Sutherling, S. Di, andD.S. Barth, “Multiple source modeling of thehuman epileptic spike complex in themagnetoencephalogram”, in: S.J. Williamson,M. Hoke, G. Stroink, M. Kotani eds. Advancesin Biomagnetism. New York: Plenum Press, pp.299-302, 19898. D. Ko, S. Sato, K. Reese, K. Kufta, J. Gamelin,and K. Squires, “Simultaneously recorded EEGand MEG spikes: comparison of localization”,in: C. Baumgartner, L. Deecke, G. Stroink, andS.J. Williamson, eds. Biomagnetism:Fundamental Research and Clinical Applications. Amsterdam: IOS Press, pp. 32-4,1995.9. D. Ko, S. Sato, D. Scaffidi, and C. Kufta,“Source localization determined by magneto-encephalography and electroencephalography intemporal lobe epilepsy. Comparison withelectrocorticography: technical case report”,Neurosurgery42, pp. 414-21, 1998.10. H. Stefan, S. Schneider, and K. Abraham-Fuchs,“Magnetic source localization in focal epilepsy”,Brain 113, 1347-59, 1990.11. H. Stefan, S. Schneider, and H. Feistel, “Ictaland interictal activity in partial epilepsyrecorded with multichannel magnetoence-phalography: correlation of electroencephalo-graphy/ electrocorticography, magnetic resonance imaging, single photon emission computed tomography, and positron emission tomography findings”, Epilepsia 33, 874-87, 1992. 12. J.S. Ebersole, K.C. Squires, S.D. Eliashiv, and J.R. Smith, “Applications of magnetic source imaging in evaluation of candidates for epilepsy surgery”, Neuroimaging Clin N Am 5, 267-288, 1995. 13. J.S. Ebersole, “Classification of MEG spikes in temporal lobe epilepsy”, in: T. Yoshimoto, M. Kotani, S. Kuriki, H. Karibe, N. Nakasoto eds. Recent Advances in Biomagnetism . Sendai: Tohoku University Press, pp. 758-61, 1999. 14. R.C. Knowlton, K.D. Laxer, M.J. Aminoff, T. Roberts, and S. Wong, H.A. Rowley, ”Magnetoencephalography in partial epilepsy: Clinical yield and localization accuracy”, Ann Neurol 42, 622-31, 1997. 15. J. Vrba, K. Betts, and M. Burbank, “Wholecortex 64 channel system for shielded andunshielded environments”, in: C. Baumgartner, L. Deecke, G. Stroink, S.J. Williamson eds. Biomagnetism: Fundamental Research and Clinical Applications . Amsterdam: IOS Press, pp. 521-5, 1995. 16. W.W. Sutherling, P. Crandall, L.D. Cahan, andD.S. Barth, “The magnetic field of epileptic spikes agrees with intracranial localizations in complex partial epilepsy”, Neurology 38, 778-786, 1988. 17. J.S. Ebersole, “EEG dipole modeling incomplex partial epilepsy”, Brain Topography 4, 113-123, 1991. 18. W.W. Sutherling, B.N. Cuffin, and R. Hari, “Assessment: Magnetoencephalography”, Neurology 42, 1-4, 1992.19. I. Fried and G.D. Cascino, “Lesional Surgery”, in: J. Engel Jr., ed. Surgical Treatment of the Epilepsies , Second Edition. New York: Raven Press, pp. 501-509, 1993.。