Aplastic Anaemia
再生障碍性血(AA)临床路径
再生障碍性贫血(AA)临床路径(2016年版)一、再生障碍性贫血(AA)临床路径标准住院流程(一)适用对象。
第一诊断为AA(ICD:D61)。
(二)诊断依据。
根据《血液病诊断和疗效标准》(张之南、沈悌主编,科学出版社,2008年,第三版)、《Guidelines for the diagnosis and management of aplastic anaemia》(2009)、《再生障碍性贫血诊断治疗专家共识》(2010)。
诊断标准:1. AA:(1)外周血: 全血细胞减少,淋巴细胞比例升高,网织红细胞校正值减少; 至少符合以下三项中两项:Hb <100 g /L;BPC<50 × 109/L;中性粒细胞绝对值(ANC)<1.5×109/L。
(2)骨髓涂片:多部位(不同平面)骨髓增生减低或重度减低;小粒空虚,非造血细胞(淋巴细胞、网状细胞、浆细胞、肥大细胞等)比例增高;巨核细胞明显减少或缺如;红系、粒系细胞均明显减少。
(3)骨髓活检(髂骨):全切片增生减低,造血组织减少,脂肪组织和(或)非造血细胞增多,网硬蛋白不增加,无异常细胞。
(4)除外检查:必须除外先天性和其他获得性、继发性骨髓衰竭性疾病。
2. AA程度确定(分型):(1)重型AA诊断标准(Camitta标准):①骨髓细胞增生程度<正常的25%;如≥正常的25%但<50%,则残存的造血细胞应<30%。
②血常规:需具备下列三项中的两项:ANC<0.5 ×109/L;校正的网织红细胞<1%或绝对值<20 ×109/L;BPC<20 × 109/L。
③若ANC<0.2×109/L为极重型AA。
(2)非重型AA诊断标准:未达到重型标准的AA。
(三)治疗方案的选择。
根据《内科学》(叶任高、陆再英主编,人民卫生出版社)、《内科学》(王吉耀主编,人民卫生出版社,2010,第二版)、《Guidelines for the diagnosis and management of aplastic anaemia》(2009)、《再生障碍性贫血诊断治疗专家共识》(2010)。
系统性红斑狼疮相关性再生障碍性贫血一例并文献复习
生堡坦星痘堂盘查垫!!生垒旦箜15鲞箜垒塑gh迪』丛!女堂!!!,△四1
2Q!!,Y丛:15,照Q:璺
・短篇报道・
系统性红斑狼疮相关性再生障碍性贫血一例并文献复习
王涛李志军
陈琳洁
范晓云
系统性红斑狼疮(systemic
lupus
erythematosus,SLE)是一
临床病情进一步改善。 2方法与结果
出血。渐加重。于9月23日入我院就诊。查血常规:白细胞 0.39×109/1。、中性粒细胞0.07%、淋巴细胞0.92,血红蛋白63 g/L,血小板3xlOgL。网织红细胞计数0.005xlO-YL,网织红细 胞卣分比0.24%。C反应蛋白(CRP)150.3 mg/L,红细胞沉降 率(ESR)156989,43:136-142. Roffe C。Cahill MR,Samanta A。et a1.Aplastic temic lupus erythematosus:a cellular immune Rheumatol。199l,30:301—304. Sumimoto S,Kawai
h。血清抗核抗体定量149 U/ml,抗dsDNA
抗体定量60 U/ml,补体c3、c4均明显下降。次Et行骨髓穿刺 术,骨髓象提示:有核细胞增生重度减低。粒系增生重度减低
占1l%,比例下降,以中幼及以下各阶段细胞为主,形态结构
基本正常。红系增生重度减低占4%,比例明显下降,以晚幼 红细胞为主,形态结构基本正常。淋巴细胞比例相对升高占 72%,形态结构基本正常。巨核细胞数量减少,血小板散在少 见。大部分造血岛晕纤维网状结构,造血岛细胞明屁减少。结 论:AA。遂诊断为“SLE。AA”。给予丙种球蛋向静脉滴注(每天
C3、c4均明显下降,尿常规:蛋白+、白细胞+++、隐血++,血小 板:62xlOVL。抗Clq抗体34.44 U/ml。淋巴细胞免疫分型: CD4"/CD8+--0.3。诊断为“SLE。血液系统损害”。给于泼尼松及
血液学 ITP AA
治疗原则(三)
• 免疫抑制剂:糖皮质激素和脾切除疗效不佳, 糖皮质激素和脾切除禁忌症,与糖皮质激素合 用减少糖皮质激素的使用。 例如:VDS,CTX,硫唑嘌呤,环孢素。 • 大剂量IVIG:0.4g/kg/d*4-5d,静脉注射。机 理:封闭FC受体,抑制抗体产生,中和抗体调 节机体免疫反应。 • 达那唑:合成雄激素,300-600mg/d,2-3月, 口服。作用机制抗雌激素有关。 • 中医中药。
流行病学
• Two large, controlled, population-based studies have been conducted, the International Aplastic Anemia and Agranulocytosis Study in Europe and Israel in the 1980s and the recently completed Thai NHLBI Aplastic Anemia Study in Bangkok and a northeast rural region. • The incidence of aplastic anemia in the West is 2/million and about 2- to 3-fold higher in Asia. • 老年人较高,男、女无明显差异
• 急性型 • 发热: • 出血:紫癜性,血小板减少,严重者出现颅内出 血,〈1%。 • 贫血:除非有明显大出血,一般无。
临床表现
慢性型多见青年女性 • 起病 隐伏,无前驱症状 • 出血 皮肤黏膜出血轻而局限,月经过多较 常见,严重内脏出血少见 • 其他 可见失血性贫血,感染可加重病情
诊断要点
11
实验室检查
• • • • • • 血小板计数: 血小板形态和功能:巨大血小板。 骨髓检查:巨核细胞。 出血时间:束臂试验,凝血和纤溶机制正常。 血小板抗体:PAIgG, GPⅡb/Ⅲa等。 血小板生存时间:90%明显缩短。
阿司匹林原文
Skip navigationMartindale: The Complete Drug ReferenceSear ch I nt er act i onsHomeContents Advanced search Print Help« Previous | Next»Home> Martindale: The Complete Drug Reference> Contents> Drugs and Ancillary Substances> Analgesics Anti-inflammatory Drugs and Antipyretics > Drug MonographsAspirinSub-sections•Drug Nomenclature•Adverse Effects and Treatment•Precautions•Interactions•Pharmacokinetics•Uses and Administration•PreparationsAspirinDrug NomenclatureDate of monograph revision: 05-Aug-1997; 08-Jul-1998; 07-Mar-2000;06-Nov-2001; 30-Jul-2003; 26-May-2004; 31-May-2006; (last modified: 29-Jun-2006)Synonyms: Acetilsalicílico, ácido; Acetilsalicilo rūgštis; Acetilszalicilsav; Acetylsal. Acid; Acetylsalicylic Acid; Acetylsalicylsyra; Acidum Acetylsalicylicum; Asetyylisalisyylihappo; Kyselina acetylsalicylová; Polopiryna; Salicylic Acid AcetateBAN: AspirinChemical name: O-Acetylsalicylic acid; 2-Acetoxybenzoic acid Molecular formula: C9H8O4 =180.2CAS: 50-78-2ATC code: A01AD05; B01AC06; N02BA01Read code: y00i8 [Musculoskeletal Use]; y009L [Antiplatelet]; y0291; y08Cz [CNS Use]; y07dCChemical Structure of AspirinNOTE:The use of the name Aspirin is limited; in some countries it is a trade-mark.Compounded preparations of aspirin may be represented by the following names:Co-codaprin (BAN)—aspirin 50 parts and codeine phosphate 1 part(w/w)Co-codaprin (PEN)—aspirin and codeine phosphate. Pharmacopoeias:In Chin., Eur. (see ), Int., Jpn, Pol., US, and Viet.Ph. Eur. 5.5(Acetylsalicylic Acid; Aspirin BP 2005). White, crystalline powder or colourless crystals. Slightly soluble in water; freely soluble in alcohol. Store in airtight containers.USP 29 (Aspirin). White crystals, commonly tubular or needle-like, or white crystalline powder; odourless or has a faint odour. Is stable indry air; in moist air it gradually hydrolyses to salicylic and acetic acids. Soluble 1 in 300 of water, 1 in 5 of alcohol, 1 in 17 of chloroform, and 1 in 10 to 15 of ether; sparingly soluble in absolute ether. Store in airtight containers.Adverse Effects and TreatmentAspirin has many properties in common with the non-aspirin NSAIDs, the adverse effects of which are described on .The most common adverse effects of therapeutic doses of aspirin are gastrointestinal disturbances such as nausea, dyspepsia, and vomiting. Gastrointestinal symptoms may be minimised by giving aspirin with food. Irritation of the gastric mucosa with erosion, ulceration, haematemesis, and melaena may occur. Histamine H2-antagonists, proton pump inhibitors, and prostaglandin analogues such as misoprostol may be used in the management of aspirin-induced mucosal damage (see under Peptic Ulcer Disease, ). Slight blood loss, which is often asymptomatic, may occur in about 70% of patients; it is not usually of clinical significance but may, in a few patients, cause iron-deficiency anaemia during long-term therapy. Such occult blood loss is not affected by giving aspirin with food but may be reduced by use of enteric-coated or other modified-release tablets, H2-antagonists, or high doses of antacids. Major upper gastrointestinal bleeding occurs rarely.Some persons, especially those with asthma, chronic urticaria, or chronic rhinitis, exhibit notable hypersensitivity to aspirin (see also ), which may provoke reactions including urticaria and other skin eruptions, angioedema, rhinitis, and severe, even fatal, paroxysmal bronchospasm and dyspnoea. Persons sensitive to aspirin often exhibit cross-sensitivity to other NSAIDs.Aspirin increases bleeding time, decreases platelet adhesiveness, and, in large doses, can cause hypoprothrombinaemia. It may cause other blood disorders, including thrombocytopenia.Aspirin and other salicylates may cause hepatotoxicity, particularly in patients with juvenile idiopathic arthritis or other connective tissue disorders. In children the use of aspirin has been implicated in some cases of Reye's syndrome, leading to severe restrictions on the indications for aspirin therapy in children. For further details see under Reye's Syndrome, .Aspirin given rectally may cause local irritation; anorectal stenosis has been reported.Mild chronic salicylate intoxication, or salicylism, usually occurs only after repeated use of large doses. Salicylism can also occur following excessive topical application of salicylates. Symptoms include dizziness, tinnitus, deafness, sweating, nausea and vomiting, headache, and confusion, and may be controlled by reducing the dosage. Tinnitus can occur at the plasma concentrations of 150 to 300 micrograms/mL required for optimal anti-inflammatory activity; more serious adverse effects occur at concentrations above 300 micrograms/mL. Symptoms of more severe intoxication or of acute poisoning following overdosage include hyperventilation, fever, restlessness, ketosis, and respiratory alkalosis and metabolic acidosis. Depression of the CNS may lead to coma; cardiovascular collapse and respiratory failure may also occur. In children drowsiness and metabolic acidosis commonly occur; hypoglycaemia may be severe.In acute oral salicylate overdosage the UK National Poisons Information Service recommends that repeated doses of activated charcoal be given by mouth if the patient is suspected of ingesting more than 120 mg/kg of salicylate within 1 hour of presentation. Activated charcoal not onlyprevents the absorption of any salicylate remaining in the stomach but also aids the elimination of any that has been absorbed.Measurement of plasma-salicylate concentration should be carried out in patients who have ingested more than 120 mg/kg of salicylate, although the severity of poisoning cannot be estimated from plasma concentrations alone. Absorption of aspirin can be delayed by reduced gastric emptying, formation of concretions in the stomach, or as a result of ingestion of enteric-coated preparations. In consequence, plasma concentrations should be measured at least 2 hours (symptomatic patients) or 4 hours (asymptomatic patients) after ingestion and repeated 2 hours later. Patients who overdose with enteric preparations require continual monitoring of plasma concentrations.Fluid and electrolyte management is essential to correct acidosis, hyperpyrexia, hypokalaemia, and dehydration. Intravenous sodium bicarbonate is given to enhance urinary salicylate excretion if plasma salicylate concentrations exceed 500 micrograms/mL (350 micrograms/mL in children under 5 years). Haemodialysis or haemoperfusion are also effective methods of removing salicylate from the plasma. The BNF considers haemodialysis the method of choice in severe poisoning; it should be seriously considered when the plasma salicylate concentration is more than 700 micrograms/mL or if there is severe metabolic acidosis. Vulnerable patients such as children or the elderly may require dialysis at an earlier stage.References to salicylate toxicity and its management.1. Notarianni L. A reassessment of the treatment of salicylate poisoning. Drug Safety 1992; 7: 292–303. PubMed2. Woods D, et al. Acute toxicity of drugs: salicylates. Pharm J 1993; 250: 576–8.3. Collee GG, Hanson GC. The management of acute poisoning. Br J Anaesth 1993; 70: 562–73. PubMed4. Watson JE, Tagupa ET. Suicide attempt by means of aspirin enema. Ann Pharmacother 1994; 28: 467–9. PubMed5. Dargan PI, et al. An evidence based flowchart to guide the management of acute salicylate (aspirin) overdose. Emerg Med J 2002; 19: 206–9. PubMedEffects on the blood.Although it has beneficial effects on platelets, aspirin can cause adverse blood effects. An indication of this toxicity is given by an early reference1 to reports submitted to the UK CSM. There were 787 reports of adverse reactions to aspirin reported to the CSM between June 1964 and January 1973. These included 95 reports of blood disorders (17 fatal) including thrombocytopenia (26; 2 fatal), aplastic anaemia (13; 7 fatal), and agranulocytosis or pancytopenia (10; 2 fatal). Aspirin has also been associated with haemolytic anaemia in patients with G6PD deficiency.21. Cuthbert MF. Adverse reactions to non-steroidal antirheumatic drugs. Curr Med Res Opin 1974; 2: 600–9. PubMed2. Magee P, Beeley L. Drug-induced blood dyscrasias. Pharm J 1991; 246: 396–7. Effects on the cardiovascular system.Salicylate poisoning may result in cardiovascular collapse but details of such cases have not been widely reported. In 2 patients with salicylate intoxication asystole developed after intravenous diazepam.1 It was suggested that diazepam-induced respiratory depression affected the acid–base balance so that the concentration of non-ionisedmembrane-penetrating fraction of salicylate was increased. For referenceto the effects of aspirin on blood pressure compared with other NSAIDs, see .1. Berk WA, Andersen JC. Salicylate-associated asystole: report of two cases. Am J Med 1989; 86: 505–6. PubMedEffects on the gastrointestinal tract.Clinical and epidemiological evidence suggests that aspirin produces dose-related gastrointestinal toxicity1,2 that is sometimes, but rarely, fatal.2Meta-analysis3suggests that the risk of gastrointestinal bleeding is not significantly lowered with the use of low-dose aspirin (less than 300 mg daily). A systemic review4of observational epidemiologic studies also concurred with this finding. Although it was suggested that very small doses of aspirin can produce prophylactic benefits in cardiovascular disease without the risk of gastrointestinal toxicity,5 others have reported gastric injury even with doses of 10 mg daily.6There appears to be no convincing evidence that the risk of major gastrointestinal bleeding associated with a 75-mg dose is reduced by using enteric-coated or modified-release formulations rather than soluble aspirin,3,4,7although individual studies have reported a reduction in acute mucosal injury with enteric coating.8All known NSAIDs have the potential for causing acute damage to the gastric mucosa (see ), and comparative studies of acute gastric mucosal damage caused by such drugs consistently associate aspirin with the most severe lesions.1 Gastric mucosal injury can occur even with cutaneous application.91. Graham DY, Smith JL. Aspirin and the stomach. Ann Intern Med 1986; 104: 390–8. PubMed2. Roderick PJ, et al. The gastrointestinal toxicity of aspirin: an overview of randomised controlled trials. Br J Clin Pharmacol 1993; 35: 219–26. PubMed3. Derry S, Loke YK. Risk of gastrointestinal haemorrhage with long term use of aspirin: meta-analysis. BMJ 2000; 321: 1183–7. PubMed4. Garcia Rodríguez LA, et al. Association between aspirin and upper gastrointestinal complications: systematic review of epidemiologic studies. Br J Clin Pharmacol 2001; 52: 563–71. PubMed5. Lee M, et al. Dose effects of aspirin on gastric prostaglandins and stomach mucosal injury. Ann Intern Med 1994; 120: 184–9. PubMed6. Cryer B, Feldman M. Effects of very low dose daily, long-term aspirin therapy on gastric, duodenal, and rectal prostaglandin levels and on mucosal injury in healthy humans. Gastroenterology 1999; 117: 17–25. PubMed7. Anonymous. Which prophylactic aspirin? Drug Ther Bull 1997; 35: 7–8. PubMed8. Cole AT, et al. Protection of human gastric mucosa against aspirin—enteric coating or dose reduction? Aliment Pharmacol Ther 1999; 13: 187–93. PubMed9. Cryer B, et al. Effects of cutaneous aspirin on the human stomach and duodenum. Proc Assoc Am Physicians 1999; 111: 448–56. PubMedEffects on hearing.Studies have indicated that tinnitus develops at serum-salicylate concentrations above 200 micrograms/mL.1 However, there appears to be considerable intersubject variation in the response of the ear to salicylate;2tinnitus may occur at lower concentrations, whereas patients with pre-existing hearing loss may not experience tinnitus despite serum-salicylate concentrations of 311 to 677 micrograms/mL.1 A graded increase in intensity of ototoxicity with increasing salicylate dose and plasma concentration has been demonstrated.2 For example, at an average total plasma-salicylate concentration of 110 micrograms/mL, the hearingloss at any given frequency was about 12 decibels; such a deficit might be relevant to patients with pre-existing hearing impairment.21. Mongan E, et al Tinnitus as an indication of therapeutic serum salicylate levels. JAMA 1973; 226: 142–5. PubMed2. Day RO, et al. Concentration-response relationships for salicylate-induced ototoxicity in normal volunteers. Br J Clin Pharmacol 1989; 28: 695–702. PubMedEffects on the kidneys.Although abuse of combined analgesic preparations containing aspirin has been implicated in the development of analgesic nephropathy, kidney damage associated with the therapeutic use of aspirin alone appears to be comparatively rare. Many studies have failed to find an increased risk of renal damage in patients taking aspirin.1-81. New Zealand Rheumatism Association Study. Aspirin and the kidney. BMJ 1974; 1: 593–6. PubMed2. Walker BR, et al. Aspirin and renal function. N Engl J Med 1977; 297: 1405. PubMed3. Akyol SM, et al. Renal function after prolonged consumption of aspirin. BMJ 1982; 284: 631–2. PubMed4. Bonney SL, et al. Renal safety of two analgesics used over the counter: ibuprofen and aspirin. Clin Pharmacol Ther 1986; 40: 373–7. PubMed5. Sandler DP, et al. Analgesic use and chronic renal disease. N Engl J Med 1989; 320: 1238–43. PubMed6. Pommer W, et al. Regular analgesic intake and the risk of end-stage renal failure. Am J Nephrol 1989; 9: 403–12. PubMed7. Dubach UC, et al. An epidemiologic study of abuse of analgesic drugs: effects of phenacetin and salicylate on mortality and cardiovascular morbidity (1968 to 1987). N Engl J Med 1991; 324: 155–60. PubMed8. Perneger TV, et al. Risk of kidney failure associated with the use of acetaminophen, aspirin, and nonsteroidal antiinflammatory drugs. N Engl J Med 1994; 331: 1675–9. PubMedEffects on the liver.Aspirin-induced hepatic injury is generally mild and manifests as a mild to moderate elevation in aminotransferase values; however, there is a risk of severe liver injury.1 One review2 reported an increase in aminotransferase values in 59 of 439 patients given aspirin; the increase was considered to be probably related to aspirin in 23. Hepatotoxicity appears to be correlated with serum-salicylate concentrations greater than 150 micrograms/mL and with active rheumatoid disease.Aspirin-induced liver injury is usually reversible on stopping the drug.2 See also under Reye's Syndrome, .1. Lewis JH. Hepatic toxicity of nonsteroidal anti-inflammatory drugs. Clin Pharm 1984; 3: 128–38. PubMed2. Freeland GR, et al. Hepatic safety of two analgesics used over the counter: ibuprofen and aspirin. Clin Pharmacol Ther 1988; 43: 473–9. PubMedEffects on the mouth.Aspirin burn (ulceration of the mucosal layer of the lips) developed in a 26-year-old woman after taking an aspirin-containing powder for a migraine.1 The woman had swallowed the powder undissolved rather than adding to water.1. Dellinger TM, Livingston HM. Aspirin burn of the oral cavity. Ann Pharmacother 1998; 32: 1107. PubMedHypersensitivity.The main clinical features of patients who have aspirin hypersensitivity include middle-age, female sex, diagnoses of asthma or rhinitis, a personal or family history of atopy, and a history of nasal polyps.1,2 Aspirin sensitivity occurring with asthma and nasal polyps has been referred to in some reports as the 'aspirin triad'. Other sensitivities often found concomitantly include allergy to food dyes such as tartrazine and to drugs such as other NSAIDs. The response to individual NSAIDs is believed to be closely linked to the extent to which they inhibit prostaglandin synthesis.3,4 There may be a dose threshold below which no detectable symptoms occur and patients who may be tolerant of regular low-dose aspirin can develop symptoms when they take larger doses.4Some4 use a formal challenge with a 300-mg dose of aspirin by mouth to confirm a diagnosis of NSAID sensitivity but others5 consider this to be a dangerous technique and use inhalation of lysine aspirin which they consider to be a safer and more predictable alternative. Intranasal challenge with lysine aspirin has also been used.61. Kwoh CK, Feinstein AR. Rates of sensitivity reactions to aspirin: problems in interpreting the data. Clin Pharmacol Ther 1986; 40: 494–505. PubMed2. Schiavino D, et al. The aspirin disease. Thorax 2000; 55 (suppl 2): S66–S69. PubMed3. Power I. Aspirin-induced asthma. Br J Anaesth 1993; 71: 619–21. PubMed4. Frew A. Selected side-effects: 13. non-steroidal anti-inflammatory drugs and asthma. Prescribers' J 1994; 34: 74–7.5. Davies BH. NSAIDs and asthma. Prescribers' J 1994; 34: 163–4.6. Casadevall J et al. Intranasal challenge with aspirin in the diagnosis of aspirin intolerant asthma: evaluation of nasal response by acoustic rhinometry. Thorax 2000; 55: 921–4. PubMedDesensitisation.Successful desensitisation has been achieved using oral aspirin challenge protocols.1,2Incremental doses of aspirin (starting at 30 mg) are given until an allergic response occurs; aspirin is readministered at the dose that caused the response and again incremental doses are given until finally a 650-mg dose is tolerated. After desensitisation, an interruption of continuous aspirin dosage results in the reappearance of sensitivity.1. Asad SI, et al Effect of aspirin in "aspirin sensitive" patients. BMJ 1984; 288: 745–8. PubMed2. Stevenson DD. Desensitization of aspirin-sensitive asthmatics: a therapeutic alternative? J Asthma 1983; 20: 31–8. PubMedHypoglycaemia.A review of the literature1on drug-induced hypoglycaemia highlighted the fact that overdosage with salicylates could produce hypoglycaemia in children. Although therapeutic doses of salicylates in adults can lower blood-glucose concentrations in diabetic and non-diabetic subjects alike, opinion on the clinical significance of this effect varies. Salicylates have been implicated in a few cases of hypoglycaemia in adults1 and some2 suggest that patients with renal impairment or those receiving large doses, such as in the treatment of rheumatoid arthritis, may be at risk. Hypoglycaemia has been reported in a patient with renal failure after excessive application of a topical preparation containing salicylic acid.31. Seltzer HS. Drug-induced hypoglycemia: a review of 1418 cases. Endocrinol Metab Clin North Am 1989; 18: 163–83. PubMed2. Pandit MK, et al. Drug-induced disorders of glucose tolerance. Ann Intern Med 1993; 118: 529–39. PubMed3. Raschke R, et al. Refractory hypoglycemia secondary to topical salicylate intoxication. Arch Intern Med 1991; 151: 591–3. PubMedReye's syndrome.Reye's syndrome is a disorder characterised by acute encephalopathy and fatty degeneration of the liver. It occurs almost exclusively in children although cases have been seen1in patients over the age of 12. Many factors may be involved in its aetiology but it typically occurs after a viral infection such as chickenpox or influenza and may be precipitated by a chemical trigger. Several large studies, as well as individual case reports, have found an association between Reye's syndrome and the prior ingestion of aspirin.2-5 The evidence for other salicylates could not be adequately evaluated.4 Although the role of aspirin and possibly other salicylates in the pathogenesis of Reye's syndrome remains to be determined, the use of aspirin and other acetylated salicylates as analgesics or antipyretics is generally considered contra-indicated in children under the age of 12 years and, in some countries, in teenagers. For example, the UK CSM has recommended that all children under 16 should not take aspirin.6(This advice superseded their earlier recommendations to avoid aspirin during fever or viral infection in children under 16 years; the Committee felt that this advice was too complex for products on general sale and, given the wide availability of other analgesic preparations, there was no need to expose this age group to any risk.) Some countries also extend these recommendations to non-acetylated salicylates. One group of workers7 who re-examined some of the original studies suggested that there might also be a link between Reye's syndrome and the use ofantiemetics, phenothiazines, and some other antihistamines, but their conclusions have been criticised.81. Hall SM, Lynn R. Reye's syndrome. N Engl J Med 1999; 341: 845–6. PubMed2. Waldman RJ, et al. Aspirin as a risk factor in Reye's syndrome. JAMA 1982; 247: 3089–94. PubMed3. Halpin TJ, et al. Reye's syndrome and medication use. JAMA 1982; 248: 687–91. PubMed4. Hurwitz ES, et al. Public health service study of Reye's syndrome and medications: report of the main study. JAMA 1987; 257: 1905–11. PubMed5. Hall SM, et al. Preadmission antipyretics in Reye's syndrome. Arch Dis Child 1988; 63: 857–66. PubMed6. Medicines and Healthcare Products Regulatory Agency. Aspirin and Reye's syndrome: questions and answers (issued 04/04/03). Available at: online (accessed 20/02/06)7. Casteels-Van Daele M, Eggermont E. Reye's syndrome. BMJ 1994; 308: 919–20. PubMed8. Hall SM. Reye's syndrome. BMJ 1994; 309: 411. PubMed。
脂联素的临床应用研究进展
脂联素的临床应用研究进展赵勇【摘要】脂肪组织已经不是普通意义上的脂肪仓库,而是一个内分泌器官。
脂联素作为脂肪组织特异分泌的一种具有重要功能的脂肪细胞因子,在能量代谢和糖脂代谢中发挥重要的调节作用。
脂联素具有广泛的生物功能,与肿瘤方面、骨代谢疾病、慢性阻塞性肺疾病、高血压、房颤、急性坏死性胰腺炎、血液病和冠状动脉粥样硬化心脏病等有一定关联。
现就其在临床中的应用进行综述。
【期刊名称】《继续医学教育》【年(卷),期】2014(000)003【总页数】3页(P49-51)【关键词】脂联素;脂联素受体;细胞因子【作者】赵勇【作者单位】天津市红桥医院检验科,天津 300131【正文语种】中文【中图分类】R364.3脂肪细胞能够分泌多种脂肪细胞因子和蛋白因子,如瘦素、脂联素、抵抗素、白细胞介素6等。
脂联素在细胞葡萄糖和脂肪酸等能量代谢过程中发挥重要的调节作用,并参与细胞增殖肥大和免疫功能的调控[1]。
脂联素具有调节体内能量平衡、糖脂代谢、抗炎症、抗动脉硬化和抗纤维化等多种作用,是一种具有广泛生物效应的细胞因子。
脂联素分泌异常与高血压,动脉粥样硬化,肝纤维化糖尿病[2]等发生密切相关,还与肿瘤、骨代谢疾病、房颤、高血压、慢性阻塞性肺疾病、急性坏死性胰腺炎、血液病和冠状动脉粥样硬化心脏病等有一定的关联。
近年来发现脂联素与前列腺癌、肾细胞癌、胃癌密切相关。
Beebe-Dimmer等[3]研究在北美男性脂联素和R1中遗传变异、与肥胖和前列腺癌的相关性。
提取DNA样本中的脂联素和脂联素受体,结果显示肥胖的脂联素受体却能预测前列腺癌的发生风险。
2010年Chou等[4]使用免疫组织化学研究了R1和R2与肾细胞癌的关系,证实脂联素受体在肾细胞癌中的存在。
证实R1在肥胖相关性肿瘤中的表达高于非肥胖相关性肿瘤R1的表达更多。
2011年Tsukada等[5]通过免疫组织化学、Western blotting方法检测R1和R2在胃癌细胞株(MKN45、TMK-1、NUGC3和NUGC4)中的表达,结果显示在胃癌中,脂联素通过R1抑制细胞的增殖,促进细胞凋亡,同时R1可能成为治疗胃癌的新靶标。
医学英语术语
部分医学常用术语的英文表达Acidosis 酸中毒Adams-Stokes syndrome 亚-斯氏综合症alcoholism, alcoholic intoxication 酒精中毒alkalosis 碱中毒anaphylaxis 过敏症anemia 贫血iron deficiency anemia 缺铁性贫血megaloblastic anemia 巨幼红细胞性贫血aplastic anemia 再生障碍性贫血angiitis 脉管炎angina pectoris 心绞痛arteriosclerosis 动脉硬化apoplexy 中风auricular fibrillation 心房纤颤auriculo-ventricular block 房室传导阻滞bronchial asthma 支气管哮喘bronchitis 支气管炎bronchiectasis 支气管扩张bronchopneumonia 支气管肺炎carcinoma 癌cardiac arrhythmia 心律紊乱cardiac failure 心力衰竭cardiomyopathy 心肌病cirrhosis 肝硬化coronary arteriosclerotic heart disease 冠状动脉硬化性心脏病Crohn disease 克罗恩病Cushing's syndrome 库欣综合症diabetes 糖尿病diffuse intravascular coagulation 弥散性血管凝血dysentery 痢疾enteritis 肠炎gastric ulcer 胃溃疡gastritis 胃炎gout 痛风hepatitis 肝炎Hodgkin's disease 霍奇金病hyperlipemia 高脂血症,血脂过多hyperparathyroidism 甲状旁腺功能亢进hypersplenism 脾功能亢进hypertension 高血压hyperthyroidism 甲状腺功能亢进hypoglycemia 低血糖hypothyroidism 甲状腺功能减退infective endocarditis 感染性心内膜炎influenza 流感leukemia 白血病lobar pneumonia 大叶性肺炎lymphadenitis 淋巴结炎lymphoma 淋巴瘤malaria 疟疾malnutrition 营养不良measles 麻疹myeloma 骨髓瘤myocardial infarction 心肌梗死myocarditis 心肌炎nephritis 肾炎nephritic syndrome 肾综合症obstructive pulmonary emphysema 阻塞性肺气肿pancreatitis 胰腺炎peptic ulcer 消化性溃疡peritonitis 腹膜炎pleuritis 胸膜炎pneumonia 肺炎pneumothorax 气胸purpura 紫癜allergic purpura 过敏性紫癜thrombocytolytic purpura 血小板减少性紫癜pyelonephritis 肾盂肾炎renal failure 肾功能衰竭rheumatic fever 风湿病rheumatoid arthritis 类风湿性关节炎scarlet fever 猩红热septicemia 败血症syphilis 梅毒tachycardia 心动过速tumour 肿瘤typhoid 伤寒ulcerative colitis 溃疡性结肠炎upper gastrointestinal hemorrhage 上消化道血Neurology 神经科brain abscess 脑脓肿cerebral embolism 脑栓塞cerebral infarction 脑梗死cerebral thrombosis 脑血栓cerebral hemorrhage 脑出血concussion of brain 脑震荡craniocerebral injury 颅脑损伤epilepsy 癫痫intracranial tumour 颅内肿瘤intracranial hematoma 颅内血肿meningitis 脑膜炎migraine 偏头痛neurasthenia 神经衰弱neurosis 神经官能症paranoid psychosis 偏执性精神病Parkinson's disease 帕金森综合症psychosis 精神病schizophrenia 精神分裂症Surgery 外科abdominal external hernia 腹外疝acute diffuse peritonitis 急性弥漫性腹膜炎acute mastitis 急性乳腺炎acute pancreatitis 急性胰腺炎acute perforation of gastro-duodenal ulcer急性胃十二指肠溃疡穿孔acute pyelonephritis 急性肾盂肾炎anal fissure 肛裂anal fistula 肛瘘anesthesia 麻醉angioma 血管瘤appendicitis 阑尾炎bleeding of gastro-duodenal ulcer 胃十二指肠溃疡出血bone tumour 骨肿瘤breast adenoma 乳房腺瘤burn 烧伤cancer of breast 乳腺癌carbuncle 痈carcinoma of colon 结肠炎carcinoma of esophagus 食管癌carcinoma of gallbladder 胆囊癌carcinoma of rectum 直肠癌carcinoma of stomach 胃癌cholecystitis 胆囊炎cervical spondylosis 颈椎病choledochitis 胆管炎cholelithiasis 胆石症chondroma 软骨瘤dislocation of joint 关节脱位erysipelas 丹毒fracture 骨折furuncle 疖hemorrhoid 痔hemothorax 血胸hypertrophy of prostate 前列腺肥大intestinal obstruction 肠梗阻intestinal tuberculosis 肠结核lipoma 脂肪瘤lithangiuria 尿路结石liver abscess 肝脓肿melanoma 黑色素瘤osseous tuberculosis 骨结核osteoclastoma 骨巨细胞瘤osteoporosis 骨质疏松症osteosarcoma 骨质疏松症osteosarcoma 骨肉瘤Paget's disease 佩吉特病perianorecrtal abscess 肛管直肠周围脓肿phlegmon 蜂窝织炎portal hypertension 门静脉高压prostatitis 前列腺炎protrusion of intervertebral disc 椎间盘突出purulent arthritis 化脓性关节炎pyogenic ostcomyclitis 化脓性骨髓炎pyothorax 脓胸rectal polyp 直肠息肉rheumatoid arthritis 类风湿性关节炎rupture of spleen 脾破裂scapulohumeral periarthritis 肩周炎tenosynovitis 腱鞘炎tetanus 破伤风thromboangiitis 血栓性脉管炎thyroid adenocarcinoma 甲状腺腺癌thyroid adenoma 甲状腺腺瘤trauma 创伤urinary infection 泌尿系感染varicose vein of lower limb 下肢静脉曲张Paediatrics 儿科acute military tuberculosis of the lung 急性粟粒性肺结核acute necrotic enteritis 急性坏死性结肠炎anaphylactic purpura 过敏性紫癜ancylostomiasis 钩虫病ascariasis 蛔虫病asphyxia of the newborn 新生儿窒息atrial septal defect 房间隔缺损birth injury 产伤cephalhematoma 头颅血肿cerebral palsy 脑性瘫痪congenital torticollis 先天性斜颈convulsion 惊厥Down's syndrome 唐氏综合症glomerulonephritis 肾小球肾炎hemophilia 血友病infantile diarrhea 婴儿腹泻intracranial hemorrhage of the newborn 新生儿颅内出血intussusception 肠套叠necrotic enterocolitis of newborn 新生儿坏死性小肠结膜炎neonatal jaundice 新生儿黄疸nutritional iron deficiency anemia 营养性缺铁性贫血nutritional megaloblastic anemia 营养性巨幼细胞性贫血patent ductus arteriosis 动脉导管未闭poliomyelitis 骨髓灰质炎premature infant 早产儿primary tuberculosis 原发性肺结核progressive muscular dystrophy 进行性肌肉营养不良pulmonary stenosis 肺动脉狭窄purulent meningitis 化脓性脑膜炎rickets 佝偻病sepsis of the newborn 新生儿败血症tetanus of the newborn 新生儿破伤风tetralogy of Fallot 法洛四联症thrush 鹅口疮,真菌性口炎varicella 水痘ventricular septal defect 室间隔缺损viral encephalitis 病毒性脑炎viral myocarditis 病毒性心肌炎Gynecology and Obstetrics 妇,产科abortion 流产adenomyosis 子宫内膜异位症amniotic fluid embolism 羊水栓塞Bartholin's cyst 巴氏腺囊肿carcinoma of cervix 子宫颈癌carcinoma of endometrium 子宫内膜癌carcinoma of ovary 卵巢癌cervicitis 宫颈炎chorio-epithelioma 绒毛膜上皮癌corpora luteum cyst 黄体囊肿dystocia 难产eclampsia 子痫edema-proteinuria-hypertension syndrome水肿蛋白尿高血压综合征(妊娠高血压综合征)endometriosis 子宫内膜异位症extrauterine pregnancy 子宫外孕hydatidiform mole 葡萄胎hyperemesis gravidarum 妊娠剧吐infertility 不育症irregular menstruation 月经失调lochia 恶露monilial vaginitis 念珠菌性阴道炎multiple pregnancy 多胎妊娠myoma of uterus 子宫肿瘤oligohydramnios 羊水过少ovarian tumour 卵巢肿瘤pelvic inflammatory disease 盆腔炎placenta previa 前置胎盘placental abruption 胎盘早期剥离pregnancy-hypertension syndrome 妊娠高血压综合症premature birth 早产premature rupture of membrane 胎膜早破postpartum hemorrhage 产后出血puerperal infection 产褥感染rupture of uterus 子宫破裂trichomonas vaginitis 滴虫性阴道炎uteroplacental apoplexy 子宫胎盘卒中vulvitis 外阴炎Ophthalmology and Otorhinolaryngology 五官科amblyopia 弱视amygdalitis, tonsillitis 扁桃体炎astigmatism 散光carcinoma of nasopharynx鼻咽癌carcinoma of larynx 喉癌cataract 白内障tinnitus 耳鸣chalazion 霰粒肿,脸板腺囊肿colour blindness 色盲deflection of nasal septum 鼻中隔偏曲deafness 聋furuncle of nasalvestibule 鼻前庭疖glaucoma 青光眼heterotropia 斜视hyperopia 远视injury of cornea 角膜损伤ceruminal impaction 耵聍嵌塞iritis 虹膜炎keratitis 角膜炎labyrinthitis 迷路炎,内耳炎laryngitis 喉炎mastoiditis 乳突炎myopia 近视nasal sinusitis 鼻窦炎otitis media 中耳炎obstruction of larynx 喉梗阻peritonsillar abscess 扁桃体中脓肿pharyngitis 咽炎rhinitis 鼻炎Dermatoloty 皮科acne 痤疮carcinoma of skin 皮肤癌bed sore 褥疮decubitus ulcer 褥疮性溃疡drug eruption 药皮疹eczema 湿疹herpes simplex 单纯疱疹herpes zoster 带状疱疹lupus erythematosis 红斑狼疮psoriasis 牛皮癣urticaria 荨麻疹wart 疣英语词汇分类19:疾病英语词汇Disease 疾病anemia, anaemia 贫血angina pectoris心绞痛appendicitis 阑尾炎arthritis 关节炎bronchitis 支气管炎cancer 癌catarrh 卡他,粘膜炎chicken pox, varicella 水痘cholera 霍乱cold 感冒,伤风,着凉(head) cold患感冒diabetes糖尿病diphtheria 白喉eczema 湿疹epilepsy癫痫erysipelas 丹毒gangrene 坏疽German measles, rubella 风疹gout痛风headache 头痛hemiplegy, hemiplegia 偏瘫,半身不遂icterus, jaundice黄疸indigestion 消化不良influenza, flu 流感insanity 精神病leukemia 白血病malaria 疟疾malnutrition 营养不良Malta fever 马耳他热,波状热measles 麻疹migraine, splitting headache 偏头痛miocardial infarction 心肌梗塞mumps 流行性腮腺炎neuralgia 神经痛neurasthenia神经衰弱paralysis 麻痹peritonitis腹膜炎pharyngitis 咽炎phtisis 痨病, 肺结核pneumonia 肺炎poliomyelitis 脊髓灰质炎rabies 狂犬病rheumatism 风湿病rickets, rachitis 佝偻病scabies, itch疥疮scarlet fever猩红热sciatica 坐骨神经痛sclerosis 硬化septicemia, septicaemia败血病sinusitis 窦炎smallpox 天花swamp fever沼地热syncope 晕厥syphilis 梅毒tetanus 破伤风thrombosis 血栓形成torticollis, stiff neck 斜颈tuberculosis 结核病tumour,tumor 瘤typhus 斑疹伤寒urticaria, hives 荨麻疹whooping cough百日咳yellow fever 黄热病zona, shingles 带状疮疹医学medical science; medical service; medicine: 医学medical book: 医书medical skill; art of healing: 医术medical matters: 医务clinic: 医务所medical science; medicine: 医学forensic medicine; legal medicine: 法医学preclinical medicine: 基础医学preventive medicine: 预防医学Doctor of Medicine: 医学博士academy of medical sciences: 医学科学院medical literature: 医学文献Bachelor of Medicine: 医学学士medical heritage: 医学遗产college of medicine: 医学院medical witness: 医学证人medicine : 医药general medical knowledge: 医药常识medical expenses: 医药费medical kit; medicine chest: 药箱first-aid kit: 急救药箱property of a medicine: 药性pharmaceutical college: 药学院dipping vat: 药浴池medicated soap: 药皂drug rash; drug eruption: 药疹assistant pharmacy: 药剂士pharmaceutics; pharmacy: 药剂学medicinal liquor: 药酒pharmacology: 药理学efficacy of a drug: 药力absorbent cotton: 药棉医院hospital: 医院hospital for infectious diseases:传染病医院children's hospital: 儿童医院obstetrics and gynecology hospital:妇产医院tuberculosis hospital: 结核病医院stomatological hospital: 口腔医院army hospital: 陆军医院field hospital: 野战医院hospital of chinese medicine: 中医医院tumor hospita;: 肿瘤医院general hospital: 综合性医院mental hospital: 精神病院hospital for lepers;leprosarium: 麻风病院sanatorium: 疗养院clinic: 诊疗所first-aid station: 急救站quarantine station: 防疫站laboratory technician: 化验员nurse: 护士head nurse: 护士长anesthetist: 麻醉师pharmacist; druggist: 药剂师out-patient: 门诊病人emergency case: 急诊病人cure; treat; heal: 医治healing of burns: 医治烧伤fail to respond to any medical treatment: 医治无效doctor's advice: 医嘱take medicine according to doctor's orders:遵照医嘱服药assistant doctor: 医助医生doctor; physician: 医生medical officer; surgeon: 军医cure; treat: 医治cure ** of his illness: 医好某人的病give ** medical treatment: 给某人医病take stopgap measures: 头痛医头,脚痛医脚still<knowledge>of a doctor:医道medical ethics: 医德medical courses in general; medicine: 医科principles of medical science; medical knowledge: 医理medical treatment: 医疗public health services: 公费医疗medical team: 医疗队medical establishment: 医疗机构medicament; drug: 药剂pharmacist; druggist: 药剂师unskillful and faulty medical or surgical treatment; malpractice: 医疗事故malpractice insurance: 医疗事故保险medico-athletics: 医疗体育medical and health work: 医疗卫生工作medical station; health center: 医疗站doctor; medical man: 医生obstetrician: 产科医生pediatrician: 儿科医生ENT(ear-nose-throat)doctor: 耳鼻喉科医生radiologist: 放射科医生gynecologist: 妇科医生orthopedist: 骨科医生urologist: 泌尿科医生physician: 内科医生dermatologist: 皮肤科医生intern: 实习医生surgeon: 外科医生dentist; dental surgeon: 牙科医生oculist; eye-doctor: 眼科医生plastic surgeon: 整形外科医生oncologist: 肿瘤科医生doctor in charge: 主治医生resident doctor: 住院医生medical report: 医生检查报告书medical evidence: 医生提供的证据practitioner with secondary medical school education: 医士科室medical department; department of internal medicine:内科surgical deparment;department of surgery: 外科pediatrics department: 小儿科obstetrics and gynecology department: 妇产科ophtalmology department: 眼科dental department: 牙科ENT(ear-nose-throat)department: 耳鼻喉科urology department: 泌尿科dermatology department; skin department:皮肤科orthopedic surgery department: 矫形外科traumatology department: 创伤外科plastic surgery: 整形外科anesthesiology department: 麻醉科pathology department: 病理科cardiology department: 心脏病科psychiatry department: 精神病科orthopedics department: 骨科department of cardiac surgery: 心脏外科department of cerebral surgery: 胸外科neurology department: 神经科neurosurgery department: 神经外科thoracic surgery department: 脑外科department of traditional Chinese medicine:中医科registration office: 挂号处out-patient department: 门诊部in-patient department: 住院部nursing department: 护理部consulting room: 诊室waiting room: 候诊室emergency room: 急诊室admitting office: 住院处operation room: 手术室X-ray department: 放射科blood bank: 血库dispensary; pharmacy: 药房ward: 病房laboratory: 化验室药物medicine; drug; remedy: 药sleeping pill: 安眠药contraceptive drugs: 避孕药tonic: 补药a medicine for colds: 感冒药expectorant: 化痰药anti-cancer drugs; cancer-fighting drugs: 抗癌药anti-tuberculous drug: 抗结核药oral contraceptive; pill: 口服避孕药good medicine; a good remedy:良药laxative: 轻泻药antipyretic: 退热药for oral administration: 内服药specific medicine; specific: 特效药for external use: 外用药preventive medicine; prophylactic: 预防药sedative: 镇静药take medicine: 服药change dressings:换药decoct herbal medicine: 煎药fill a prescripttion: 配药have a prescripttion made up(filled):(患者)抓药medicinal materials; crude drugs: 药材medicinal herbs: 药草tablet: 药片medicines and chemical reagents: 药品medicine bottle: 药瓶remedies: 药石liquid medicine; medicinal liquid: 药水lotion: 洗液pill: 药丸bolus: 大药丸herbal medicines in a prescripttion: 药味(中药方中的药)flavor of a drug: 药味(药的味道或气味)medicines; pharmaceuticals; medicaments: 药物heal with drugs: 药物医治drug allergy: 药物过敏materia medica: 药物学drug poisoning: 药物中毒(medicinal)powder: 药粉ointment; salve: 药膏apply a plaster: 上药膏其他medical apparatus and instruments: 医疗器械pharmaceutical factory: 药厂drugstore; chemist's shop; pharmacy: 药店pharmacopeia: 药典prescripttion: 药方write out a prescripttion: 开药方drugstore; chemist's shop; pharmacy: 医药商店hospital pharmacy; dispensary: 医院或诊所里的药房expenses for medicine; charges for medicine: 药费a pot for decocting herbal medicine: 药罐子chronic invalid: 药罐子(经常生病的人)apothecaries'measure or weight: 药衡medicinal herb collector; herbalist 药农herbal medicine shop: 药铺。
上海市崇明区2022届高三高考一模英语试题(含听力)(练习版)

C. He doesn’t want to drive anymore.
D. The road to Bridgeport has just been opened.
5.【此处可播放相关音频,请去附件查看】
A. The ticket was expensive.B. He didn’t buy the ticket.
B. He didn’t need any support from the government.
C. His project’s financial problem has been solved.
D. He has already stopped his project halfway.
Section B
听下面一段独白,回答以下小题。【此处可播放相关音频,请去附件查看】
11
A. Many leaders are anxious about their team’s productivity.
B. Employees are happier when they work from home.
C. More and more people prefer to work at home now.
Directions: After reading the passage below, fill in the blanks to make the passage coherent and grammatically correct. For the blanks with a given word, fill in each blank with the proper form of the givenword; for the other blanks, use one word that best fits each blank.
氯吡格雷引起纯红细胞再生障碍性贫血 1 例

氯吡格雷引起纯红细胞再生障碍性贫血 1 例杨雅薇; 章伟; 秦永文; 马丽萍; 樊民【期刊名称】《《国际心血管病杂志》》【年(卷),期】2019(046)005【总页数】3页(P315-317)【作者】杨雅薇; 章伟; 秦永文; 马丽萍; 樊民【作者单位】200080 上海中医药大学附属岳阳中西医结合医院心血管内科; 200433 上海第二军医大学附属长海医院心血管内科【正文语种】中文1 病例简介患者男性,70岁,因“反复胸痛5年余,胸闷乏力2周余”入院,患者5年余前有反复胸痛,诊断为冠状动脉粥样硬化性心脏病(冠心病),3个月前行介入治疗,置入EXCEL支架3枚,术后予阿司匹林(100 mg/d)、氯吡格雷(150 mg/d)、美托洛尔、阿托伐他汀、单硝酸异山梨酯等药物治疗,氯吡格雷服用2周后减量为75 mg/d。
既往体健,无其他基础疾病及药物服用史。
入院2周余前患者出现活动后胸闷、乏力。
入院查体:心率90次/min,律齐,血压120/80 mmHg,呼吸18次/min,神志清,精神尚可,皮肤黏膜苍白,无黄染,无出血点,心界无扩大,各瓣膜听诊区未闻及杂音,双下肢无凹陷性水肿。
入院后查血常规示:红细胞(RBC)2.46×1012/L,血红蛋白(Hb)78 g/L,平均红细胞血红蛋白量(MCH)31.7 pg,平均红细胞体积(MCV)91.1 fL,平均红细胞血红蛋白浓度(MCHC)348 g/L,白细胞、血小板等均在正常范围内。
贫血原因考虑可能为双联抗血小板治疗引起的上消化道出血,给予维持循环血容量、补充红细胞悬液、保护胃黏膜等治疗后症状缓解,复查血常规示Hb 98 g/L。
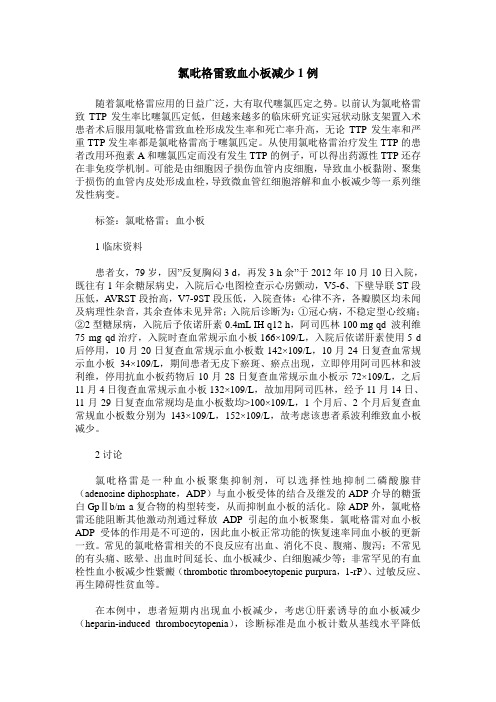
之后Hb进行性下降,2周内从98 g/L降至62 g/L(见图1)。
进一步查血清铁67.78 μmol/L,总铁结合力73 μmol/L,转铁蛋白饱和度92.8%,铁蛋白822.58 μg/L,凝血功能、自身免疫抗体、肿瘤标志物、尿常规等均未见异常,多次查粪隐血、粪转铁蛋白阴性。
甲砜霉素对肉鸡睾丸组织结构的影响
甲砜霉素对肉鸡睾丸组织结构的影响摘要:将152只4日龄雄性aa+肉鸡随机分为4组,每组38只,分别在饲料中添加0(对照组)、500(试验ⅰ组)、1 000(试验ⅱ组)、1 500 mg/kg(试验ⅲ组)的甲砜霉素,自由采食,试验期2周,对睾丸进行病理形态学观察。
2周后测量体重、睾丸重、睾丸脏器系数,并作睾丸石蜡切片测量曲精细管面积和观察甲砜霉素对肉鸡睾丸的病理组织学影响。
结果表明,各试验组肉鸡体重和曲精细管面积以及试验ⅱ、ⅲ组试验鸡的睾丸重极显著低于对照组(p 综上所述,营养缺乏可能是引起试验组肉鸡体重降低、睾丸重量改变、组织结构损伤的原因之一。
同时,甲砜霉素可显著损伤肾脏,使血清蛋白随尿液流失;显著损伤肝脏,使肝脏合成蛋白质减少,从而导致试验组肉鸡出现水肿或细胞水疱变性[8]。
另外,由于甲砜霉素能阻断造血干细胞的线粒体合成,导致造血干细胞的增生分裂停止,引起细胞的呼吸链电子传递障碍[9],使atp合成减少,从而使精原细胞和睾丸支持细胞发生水疱变性,甚至坏死。
由于精原细胞具有增值分化为精母细胞的潜能;睾丸支持细胞具有营养生精细胞,合成雄激素蛋白、促进精子发生等功能,且同神经细胞一样没有增殖分裂的潜力,因此一旦受损甚至死亡,所有生殖细胞都会死亡,因此上述两种细胞的变性死亡必然导致精原细胞分裂受阻,曲精小管中生精细胞的数量减少,曲精小管变小,结缔组织增生。
本试验结果与maita等[6]关于甲砜霉素能影响生精细胞发育的研究结果一致,但与其关于睾丸支持细胞未受损伤的结果相反,可能与试验周期和药物剂量大小不同有一定关系。
本试验中,甲砜霉素对肉鸡睾丸的影响与其对肉鸡生产性能的影响基本一致。
有报道显示,血清中雄激素的水平与肉鸡的生长发育有密切联系[12],甲砜霉素是否对睾酮的分泌有显著的影响还需进一步试验来证实。
参考文献:[1] 孟志敏,牛小飞,李连缺,等.甲砜霉素可溶性粉对人工感染鸡大肠杆菌病的药效学研究[j].湖北农业科学,2012,51(1):120-122.[2] 孙彬,徐益斌,徐连均.雏鸡沙门氏菌的分离、鉴定以及药敏试验[j].北京农业,2008(30):32-34.[3] 彭措扎西.禽霍乱病原菌的分离鉴定及药敏试验[j].养殖与饲料,2010(8):18-20.[4] turton j a,havard a c,robinson s,et al. an assessment of chloramphenicol and thiamphenicol in the induction of aplastic anaemia in the balb/c mouse[j]. food and chemical toxicology,2000,38(10):925-938.[5] maita k,kuwahara m,kosaka t,et al. time-course change of testicular toxicity with thiamphenicol in malesprague-dawley rats[j].journal of toxicologic pathology,2003,16(1):67-75.[6] maita k,kuwahara m,kosaka t,et al.the effect oftestosterone propionate supplement on testicular toxicity with thiamphenicol in male sprague-dawley rats[j]. the journal of toxicological science,2004,29(3):187-193.[7] 唐海蓉.甲砜霉素对鲤鱼危害的病理学研究[d].四川雅安:四川农业大学,2003.[8] 唐海蓉,陈仕均,王选年,等.试验性甲砜霉素中毒对肉鸡血液生化指标的影响[j].中国兽医学报,2010,30(6):833-836.[9] 唐海蓉,陈仕均,银梅,等.甲砜霉素中毒对肉仔鸡免疫器官损伤的病理学影响[j].中国兽医学报,2010,30(1):85-90.[10] 谢恺舟,姚宜林,徐东,等.甲砜霉素在鸡蛋中的残留消除规律[j].畜牧兽医学报,2011,42(1):116-123.[11] 章明,施祖灏,高玉时,等.鸡肉中甲砜霉素和氟甲砜霉素残留的高效液相色谱法检测[j].中国家禽,2010,32(21):23-25.[12] 曹静,陈耀星,王子旭,等.单色光对肉鸡睾丸形态结构的影响[j].畜牧兽医学报,2007,38(9):972-976.。
再生障碍性贫血发病机制研究进展论文

再生障碍性贫血发病机制研究进展【摘要】再生障碍性贫血(aplastic anaemia,aa)以全血细胞减少和骨髓造血功能衰竭为特征,以贫血、出血和感染为主要症状,其发病机制纷繁复杂,本文就其发病机制近年来的研究进展做一综述。
【关键词】再生障碍性贫血;发病机制;进展【中图分类号】r 556.5 【文献标识码】a 【文章编号】1004- 7484(2012)05- 0450- 01aa发病机制十分复杂,目前多数学者认为aa是一种异质性疾病,发病机制包括造血干/祖细胞内在增殖缺陷(“种子”学说)、造血微环境支持功能缺陷(“土壤”学说)、异常免疫损伤造血干细胞(“虫子”学说)、遗传易感性等[1]。
实际上,免疫异常已成为aa近年研究最活跃的领域之一。
1 发病机制1.1 造血干/祖细胞内在增殖缺陷研究证实所有aa患者都存在不同程度的造血干/祖细胞量的减少和质的缺陷。
aa患者不仅骨髓中的祖细胞总数减少,而且集落形成细胞及cd34较正常人显著减少,减少程度与病情相关。
经同基因骨髓移植成功后,正常造血功能很快恢复,表明aa发病机制主要是造血干细胞缺乏或异常[2]。
1.2 免疫异常现已积累了大量的实验证据,支持aa是一种t细胞异常活化,以骨髓为靶组织的自身免疫病。
第46届美国血液学年会明确提出aa是自身免疫性疾病[3]。
1.2.1 t细胞异常已发现的细胞免疫异常包括cd4+/cd8+倒置、th1/th2平衡向th1漂移、th1细胞因子增多和cd8+ cd28-寡克隆扩增等[4,5]。
近年来研究发现,aa患者的细胞免疫异常还包括调节性t细胞缺陷、t细胞t-bet蛋白升高、自然杀伤t细胞异常及t细胞共刺激信号改变等[6]。
尽管还有很多问题有待阐明,但可以认为aa患者的细胞毒性t细胞发生异常活化引起一系列免疫攻击,最终导致造血干/祖细胞凋亡和造血衰竭。
1.2.2 细胞因子多数造血正调控因子(包括epo、gm-csf、il-3)在aa患者中水平明显升高,一些造血负调控因子(包括il-2、tnf-α、ifn-γ)也显著升高[7]。
1例极重型再生障碍性贫血合并多重感染患者的护理体会
中西医结合护理Chinese Journal of Integrative Nursing2024 年第 10 卷第 2 期Vol.10, No.2, 20241例极重型再生障碍性贫血合并多重感染患者的护理体会武珂君, 李昕砾(中国医学科学院血液病医院 中国医学科学院血液学研究所 实验血液学国家重点实验室 国家血液系统疾病临床医学研究中心 细胞生态海河实验室 贫血诊疗中心, 天津, 300020)摘要: 极重型再生障碍性贫血(VSAA )是一种非常罕见的、严重的造血系统疾病,表现为骨髓造血功能持续受损,导致全血细胞中的三大类细胞(红细胞、白细胞和血小板)数量不足。
本文总结1例极重型再生障碍性贫血合并多重感染的患者的护理体会。
根据患者临床症状,明确护理重点,积极控制感染,加强病情观察,做好跌倒及出血风险评估和防控,针对性开展心理护理,疏导患者情绪,提高患者治疗依从性,促进早期康复。
关键词: 极重型再生障碍性贫血; 感染; 护理风险评估; 跌倒; 出血; 心理护理中图分类号: R 473.5 文献标志码: A 文章编号: 2709-1961(2024)02-0180-04Nursing of a patient with very severe aplastic anemiacomplicated with multiple infectionsWU Kejun ,LI Xinli(Center for Anaemia Diagnosis and Treatment , Hematology Hospital Chinese Academy of Medical Sciences and Peking Union Medical College , Institute of Hematology and Blood Diseases Hospital and Peking Union Medical College , Chinese Academy of Medical Sciences , State Key Laboratory of Experimental Hematology , NationalClinical Research Center for Blood Diseases , Haihe Laboratory of Cell Ecosystem , Tianjin , 300020)ABSTRACT : Very severe aplastic anemia is a very rare and serious disease of hematopoietic sys⁃tem , which is characterized by continuous impairment of hematopoietic function of bone marrow , resulting in insufficient number of three types of cells (red blood cells , white blood cells and plate⁃lets ) in whole blood cells. This paper summarized the nursing management of a patient with se⁃vere aplastic anemia complicated with multiple infections. According to the patient's existing symptoms , key issues of nursing were clarified including infection prevention and control , illness condition monitoring , risk assessment and prevention of falls and bleeding. In addition to routine personalized care psychological care was carried out to improve the patients ’ treatment adherence.KEY WORDS : very severe aplastic anemia ; multiple infection ; nursing risk assessment ; falls ; bleeding ; psychological care 极重型再生障碍性贫血(VSAA )是一种非常罕见的、严重的造血系统疾病,表现为骨髓造血功能持续受损,导致全血细胞中的三大类细胞(红细胞、白细胞和血小板)[1]数量不足。
常见病痛的英文说法

cough 咳嗽asthma 哮喘pneumonia 肺炎heart disease 心脏arrhythmia 心律不齐indigestion 消化不良gastritis 胃炎appendicitis 盲肠炎hepatitis 肝炎dermatitis皮炎freckle/ephelis 痣,雀斑acne 粉刺flu 流感diarrhoea 痢疾quarantine 检疫vaccinate 打疫苗endemic 水土不服relapse 复发症casualty急症stupor 昏迷sprain 扭伤scaldinggraze 擦伤scratch 搔挠trauma 外伤bruise 淤伤fracture骨折dislocation 脱臼tinnitus 耳鸣trachoma 沙眼colour blindness 色盲nearsightedness/myopia近视astigmatism 散光gingivitis 牙龈炎cavity 龋齿fever 发烧discomfort/disorder 不适malnutrition 营养不良incubation 潜伏期asthenia 虚弱poisoning 中毒fatigue 疲劳heat stroke 中暑itching 发痒ache/pain 痛tetanus 破伤风night sweat 盗汗chill 打冷颤pale 脸色发白shuddering 发抖inflammation 炎症acute 急症chronic 慢性病congenital 先天性病nausea恶心vomit 呕吐哮喘asthma扁桃体tonsil扁桃体炎tonsillitis糖尿病diabetes头痛headache感冒cold咳嗽cough肺炎pneumonia肝炎hepatitis脑膜炎brain fever/meningitis膀胱炎cystitis急性胃炎acute gastritis胃炎gastritis气管炎trachitis支气管炎bronchitis阑尾炎appendicitis胃肠炎gastroenteritis乳腺炎mastitis肿瘤tumor癌症cancer禽流感bird flu/avian influenza非典SARS(Severe Acute Respiratary Syndrome)疯牛病mad cow disease黑死病black death白血病leukemia爱滋病AIDS(Acquired Immune Deficiency Syndrome) 流感influenza白内障cataract狂犬病rabies中风stroke冠心病coronary heart disease糖尿病diabetes肺癌lung cancer肝癌liver cancer肺结核pulmonary tuberculosis肝硬化hepatocirrhosis慢性病chronic肺气肿emphysema胃癌cancer of stomach胃病stomach trouble心脏病heart disease发烧fever心脏病heart disease糖尿病sugar diabetes心脑血管疾病cardiovascular and cerebrovascular disease 小儿麻痹症infantile paralysis癌症cancer狂犬病hydrophobia肺结核pulmonary tuberculosis艾滋病AIDS=Acquired Immure Deficiency Syndrome乙型肝炎hepatitis B白内障cataractInternal Medicine 内科Acidosis 酸中毒Adams-Stokes syndrome 亚-斯氏综合症alcoholism, alcoholic intoxication 酒精中毒alkalosis 碱中毒anaphylaxis 过敏症anemia 贫血iron deficiency anemia 缺铁性贫血megaloblastic anemia 巨幼红细胞性贫血aplastic anemia 再生障碍性贫血angiitis 脉管炎angina pectoris 心绞痛arteriosclerosis 动脉硬化apoplexy 中风auricular fibrillation 心房纤颤auriculo-ventricular block 房室传导阻滞bronchial asthma 支气管哮喘bronchitis 支气管炎bronchiectasis 支气管扩张bronchopneumonia 支气管肺炎carcinoma 癌cardiac arrhythmia 心律紊乱cardiac failure 心力衰竭cardiomyopathy 心肌病cirrhosis 肝硬化coronary arteriosclerotic heart disease 冠状动脉硬化性心脏病Crohn disease 克罗恩病Cushing's syndrome 库欣综合症diabetes 糖尿病diffuse intravascular coagulation 弥散性血管凝血dysentery 痢疾enteritis 肠炎gastric ulcer 胃溃疡gastritis 胃炎gout 痛风hepatitis 肝炎Hodgkin's disease 霍奇金病hyperlipemia 高脂血症,血脂过多hyperparathyroidism 甲状旁腺功能亢进hypersplenism 脾功能亢进hypertension 高血压hyperthyroidism 甲状腺功能亢进hypoglycemia 低血糖hypothyroidism 甲状腺功能减退infective endocarditis 感染性心内膜炎influenza 流感leukemia 白血病lobar pneumonia 大叶性肺炎lymphadenitis 淋巴结炎lymphoma 淋巴瘤malaria 疟疾malnutrition 营养不良measles 麻疹myeloma 骨髓瘤myocardial infarction 心肌梗死myocarditis 心肌炎nephritis 肾炎nephritic syndrome 肾综合症obstructive pulmonary emphysema 阻塞性肺气肿pancreatitis 胰腺炎peptic ulcer 消化性溃疡peritonitis 腹膜炎pleuritis 胸膜炎pneumonia 肺炎pneumothorax 气胸purpura 紫癜allergic purpura 过敏性紫癜thrombocytolytic purpura 血小板减少性紫癜pyelonephritis 肾盂肾炎renal failure 肾功能衰竭rheumatic fever 风湿病rheumatoid arthritis 类风湿性关节炎scarlet fever 猩红热septicemia 败血症syphilis 梅毒tachycardia 心动过速tumour 肿瘤typhoid 伤寒ulcerative colitis 溃疡性结肠炎upper gastrointestinal hemorrhage 上消化道血Neurology 神经科brain abscess 脑脓肿cerebral embolism 脑栓塞cerebral infarction 脑梗死cerebral thrombosis 脑血栓cerebral hemorrhage 脑出血concussion of brain 脑震荡craniocerebral injury 颅脑损伤epilepsy 癫痫intracranial tumour 颅内肿瘤intracranial hematoma 颅内血肿meningitis 脑膜炎migraine 偏头痛neurasthenia 神经衰弱neurosis 神经官能症paranoid psychosis 偏执性精神病Parkinson's disease 帕金森综合症psychosis 精神病schizophrenia 精神分裂症Surgery 外科abdominal external hernia 腹外疝acute diffuse peritonitis 急性弥漫性腹膜炎acute mastitis 急性乳腺炎acute pancreatitis 急性胰腺炎acute perforation of gastro-duodenal ulcer急性胃十二指肠溃疡穿孔acute pyelonephritis 急性肾盂肾炎anal fissure 肛裂anal fistula 肛瘘anesthesia 麻醉angioma 血管瘤appendicitis 阑尾炎bleeding of gastro-duodenal ulcer 胃十二指肠溃疡出血bone tumour 骨肿瘤breast adenoma 乳房腺瘤burn 烧伤cancer of breast 乳腺癌carbuncle 痈carcinoma of colon 结肠炎carcinoma of esophagus 食管癌carcinoma of gallbladder 胆囊癌carcinoma of rectum 直肠癌carcinoma of stomach 胃癌cholecystitis 胆囊炎cervical spondylosis 颈椎病choledochitis 胆管炎cholelithiasis 胆石症chondroma 软骨瘤dislocation of joint 关节脱位erysipelas 丹毒fracture 骨折furuncle 疖hemorrhoid 痔hemothorax 血胸hypertrophy of prostate 前列腺肥大intestinal obstruction 肠梗阻intestinal tuberculosis 肠结核lipoma 脂肪瘤lithangiuria 尿路结石liver abscess 肝脓肿melanoma 黑色素瘤osseous tuberculosis 骨结核osteoclastoma 骨巨细胞瘤osteoporosis 骨质疏松症osteosarcoma 骨质疏松症osteosarcoma 骨肉瘤Paget's disease 佩吉特病perianorecrtal abscess 肛管直肠周围脓肿phlegmon 蜂窝织炎portal hypertension 门静脉高压prostatitis 前列腺炎protrusion of intervertebral disc 椎间盘突出purulent arthritis 化脓性关节炎pyogenic ostcomyclitis 化脓性骨髓炎pyothorax 脓胸rectal polyp 直肠息肉rheumatoid arthritis 类风湿性关节炎rupture of spleen 脾破裂scapulohumeral periarthritis 肩周炎tenosynovitis 腱鞘炎tetanus 破伤风thromboangiitis 血栓性脉管炎thyroid adenocarcinoma 甲状腺腺癌thyroid adenoma 甲状腺腺瘤trauma 创伤urinary infection 泌尿系感染varicose vein of lower limb 下肢静脉曲张Paediatrics 儿科acute military tuberculosis of the lung 急性粟粒性肺结核acute necrotic enteritis 急性坏死性结肠炎anaphylactic purpura 过敏性紫癜ancylostomiasis 钩虫病ascariasis 蛔虫病asphyxia of the newborn 新生儿窒息atrial septal defect 房间隔缺损birth injury 产伤cephalhematoma 头颅血肿cerebral palsy 脑性瘫痪congenital torticollis 先天性斜颈convulsion 惊厥Down's syndrome 唐氏综合症glomerulonephritis 肾小球肾炎hemophilia 血友病infantile diarrhea 婴儿腹泻intracranial hemorrhage of the newborn 新生儿颅内出血intussusception 肠套叠necrotic enterocolitis of newborn 新生儿坏死性小肠结膜炎neonatal jaundice 新生儿黄疸nutritional iron deficiency anemia 营养性缺铁性贫血nutritional megaloblastic anemia 营养性巨幼细胞性贫血patent ductus arteriosis 动脉导管未闭poliomyelitis 骨髓灰质炎premature infant 早产儿primary tuberculosis 原发性肺结核progressive muscular dystrophy 进行性肌肉营养不良pulmonary stenosis 肺动脉狭窄purulent meningitis 化脓性脑膜炎rickets 佝偻病sepsis of the newborn 新生儿败血症tetanus of the newborn 新生儿破伤风tetralogy of Fallot 法洛四联症thrush 鹅口疮,真菌性口炎varicella 水痘ventricular septal defect 室间隔缺损viral encephalitis 病毒性脑炎viral myocarditis 病毒性心肌炎Gynecology and Obstetrics 妇,产科abortion 流产adenomyosis 子宫内膜异位症amniotic fluid embolism 羊水栓塞Bartholin's cyst 巴氏腺囊肿carcinoma of cervix 子宫颈癌carcinoma of endometrium 子宫内膜癌carcinoma of ovary 卵巢癌cervicitis 宫颈炎chorio-epithelioma 绒毛膜上皮癌corpora luteum cyst 黄体囊肿dystocia 难产eclampsia 子痫edema-proteinuria-hypertension syndrome水肿蛋白尿高血压综合征(妊娠高血压综合征)endometriosis 子宫内膜异位症extrauterine pregnancy 子宫外孕hydatidiform mole 葡萄胎hyperemesis gravidarum 妊娠剧吐infertility 不育症irregular menstruation 月经失调lochia 恶露monilial vaginitis 念珠菌性阴道炎multiple pregnancy 多胎妊娠myoma of uterus 子宫肿瘤oligohydramnios 羊水过少ovarian tumour 卵巢肿瘤pelvic inflammatory disease 盆腔炎placenta previa 前置胎盘placental abruption 胎盘早期剥离pregnancy-hypertension syndrome 妊娠高血压综合症premature birth 早产premature rupture of membrane 胎膜早破postpartum hemorrhage 产后出血puerperal infection 产褥感染rupture of uterus 子宫破裂trichomonas vaginitis 滴虫性阴道炎uteroplacental apoplexy 子宫胎盘卒中vulvitis 外阴炎Ophthalmology and Otorhinolaryngology 五官科amblyopia 弱视amygdalitis, tonsillitis 扁桃体炎astigmatism 散光carcinoma of nasopharynx鼻咽癌carcinoma of larynx 喉癌cataract 白内障tinnitus 耳鸣chalazion 霰粒肿,脸板腺囊肿colour blindness 色盲deflection of nasal septum 鼻中隔偏曲deafness 聋furuncle of nasalvestibule 鼻前庭疖glaucoma 青光眼heterotropia 斜视hyperopia 远视injury of cornea 角膜损伤ceruminal impaction 耵聍嵌塞iritis 虹膜炎keratitis 角膜炎labyrinthitis 迷路炎,内耳炎laryngitis 喉炎mastoiditis 乳突炎myopia 近视nasal sinusitis 鼻窦炎otitis media 中耳炎obstruction of larynx 喉梗阻peritonsillar abscess 扁桃体中脓肿pharyngitis 咽炎rhinitis 鼻炎Dermatoloty 皮科acne 痤疮carcinoma of skin 皮肤癌bed sore 褥疮decubitus ulcer 褥疮性溃疡drug eruption 药皮疹eczema 湿疹herpes simplex 单纯疱疹herpes zoster 带状疱疹lupus erythematosis 红斑狼疮psoriasis 牛皮癣urticaria 荨麻疹wart 疣neuralgia 神经痛neurasthenia 神经衰弱paralysis 麻痹peritonitis 腹膜炎pharyngitis 咽炎phtisis 痨病,肺结核pneumonia 肺炎poliomyelitis 脊髓灰质炎rabies 狂犬病rheumatism 风湿病rickets, rachitis 佝偻病scabies, itch 疥疮scarlet fever 猩红热sciatica 坐骨神经痛sclerosis 硬化septicemia, septicaemia 败血病sinusitis 窦炎smallpox 天花anemia, anaemia 贫血angina pectoris 心绞痛appendicitis 阑尾炎arthritis 关节炎bronchitis 支气管炎cancer 癌catarrh 卡他,粘膜炎chicken pox, varicella 水痘cholera 霍乱cold 感冒,伤风,着凉(head) cold 患感冒diabetes 糖尿病diphtheria 白喉eczema 湿疹epilepsy 癫痫erysipelas 丹毒gangrene 坏疽German measles, rubella 风疹gout 痛风headache 头痛hemiplegy, hemiplegia 偏瘫,半身不遂interus, jaundice 黄疸indigestion 消化不良influenza, flu 流感insanity 精神病leukemia 白血病malaria 疟疾malnutrition 营养不良Malta fever 马耳他热,波状热measles 麻疹migraine, splitting headache 偏头痛miocardial infarction 心肌梗塞mumps 流行性腮腺炎swamp fever 沼地热syncope 晕厥syphilis 梅毒tetanus 破伤风thrombosis 血栓形成torticollis, stiff neck 斜颈tuberculosis 结核病tumour 瘤(美作:tumor)typhus 斑疹伤寒urticaria, hives 荨麻疹whooping cough 百日咳yellow fever 黄热病zona, shingles 带状疮疹cough 咳嗽asthma 哮喘pneumonia 肺炎heart disease 心脏病arrhythmia 心律不齐indigestion 消化不良gastritis 胃炎appendicitis 盲肠炎hepatitis 肝炎dermatitis皮炎freckle/ephelis 痣,雀斑acne 粉刺flu 流感diarrhoea 痢疾quarantine 检疫vaccinate 打疫苗endemic 水土不服relapse 复发症casualty急症stupor 昏迷sprain 扭伤scalding烫伤graze 擦伤scratch 搔挠trauma 外伤bruise 淤伤fracture骨折dislocation 脱臼tinnitus 耳鸣trachoma 沙眼colour blindness 色盲nearsightedness/myopia 近视astigmatism 散光gingivitis 牙龈炎cavity 龋齿fever 发烧discomfort/disorder 不适malnutrition 营养不良incubation 潜伏期asthenia 虚弱poisoning 中毒fatigue 疲劳heat stroke 中暑itching 发痒ache/pain 痛tetanus 破伤风night sweat 盗汗chill 打冷颤pale 脸色发白shuddering 发抖inflammation 炎症acute 急症chronic 慢性病congenital 先天性病nausea恶心vomit 呕吐。
TNF―α,INF―γ的诊断意义

TNF―α,INF―γ的诊断意义摘要:目的为更好地为儿童急性再生障碍性贫血体内细胞因子浓度变化提供证据。
方法采再障组(46例)和对照组(48例)静脉血,用酶联免疫吸附法测定所取血样标本中肿瘤坏死因子-α(TNF-α)和干扰素-γ(INF-γ)的含量。
并用独立样本t检验分析两组外周血中细胞因子是否存在显著性差异。
结果再障组患儿外周血TNF-α和INF-γ的含量均高于对照组儿童。
结论通过对TNF-α和INF-γ的监测,可以有效的了解再障患儿疾病进展,治疗效果和预后情况。
关键词:再生障碍性贫血;肿瘤坏死因子-α;干扰素-γ再生障碍性贫血可分为急性再障和慢性再障两型。
其中急性再生障碍性贫血发病急、进展快,骨髓衰竭是其主要病理过程,常伴内脏出血、严重感染,常危及生命,预后不良。
但是现在大部分的病例被诊断为特发性免疫异常导致的再生障碍性[1]。
细胞因子失调,包括肿瘤坏死因子(TNF-α),干扰素(INF-γ),今年来研究发现在再生障碍性贫血的发病机制中起到了重要的作用[2]。
儿童再生障碍性贫血已经成为继儿童白血病之后,儿童死亡率较高的一种血液系统疾病[3]。
本研究为了给临床上提供更好的关于儿童急性再障体内细胞因子浓度变化的证据。
现报告如下:1 资料与方法1.1一般资料2010年6月~2013年6月我院诊治的46名急性再生障碍性贫血患儿。
符合我国小儿再生障碍性贫血的诊断及分型标准[4]。
患儿均为急性再生障碍性贫血发作。
其中男20例,女26例,中位年龄6.3(2~14)岁。
对照组选择同期到我院体检中心体检的正常儿童,共48例,男21例,女27例,中位年龄7(2~16)岁。
两组儿童的年龄比较和性别比例上无显著性差异,P≥0.05。
1.2方法1.2.1标本收集用肝素钠抗凝管采集静脉血5ml用于TNF-α测定。
取用无肝素采集管采集静脉血15ml用于INF-γ测定。
1.2.2TNF-α含量的测定以鼠源性的抗TNF-α单抗以每孔400ng的量,在PH值为9的碳酸-碳酸钠缓冲液中包被96孔板中,置4℃环境过夜。
第八讲 再生障碍性贫血的诊断与治疗
第八讲再生障碍性贫血的诊断与治疗再生障碍性贫血(aplastic anemia,AA)简称再障,系以外周血全血细胞减少和骨髓低增生为特征的免疫介导的骨髓造血衰竭综合征。
其年发病率在我国为0.74/10万人口,可发生于各年龄组,老年人发病率较高,男、女发病率无明显差异。
AA分为先天性和获得性两大类,以获得性AA居大多数,先天性AA甚罕见。
按临床表现分型,又可分为重型再障(SAA)和非重型再障(NSAA)。
目前认为T淋巴细胞异常活化、功能亢进造成骨髓损伤、造血细胞凋亡和造血功能衰竭在原发性获得性AA发病机制中占主要地位,新近研究显示遗传背景在AA发病及进展中也可能发挥一定作用,如端粒酶基因突变,也有部分病例发现体细胞突变。
1 AA 的诊断1.1 AA的临床表现(一)重型再生障碍性贫血起病急,进展迅速,病情重。
病初贫血常不明显,但随着病初发展呈进行性进展。
常以出血和感染/发热为首起和主要表现。
一般无肝、脾、淋巴结肿大。
大多数病人有发热,系感染所致,以呼吸道感染最常见。
几乎具有出血倾向,主要表现为消化道出血、血尿、眼底出血和颅内出血。
感染和出血互为因果,病情日益恶化。
(二)重型再生障碍性贫血起病和进展较缓慢,病情较重型轻。
以贫血为首起和主要表现;感染相对易控制;出血倾向较轻,多限于皮肤粘膜。
1.2 AA的实验室检查血常规检查示全血细胞减少,网织红细胞比例<l%,淋巴细胞比例增高。
至少符合以下三项中两项:Hb <100g/L;Plt<50×109/L;中性粒细胞(ANC)<1.5×109/L。
多部位骨髓穿刺:至少包括两处髂骨,必要时做胸骨。
提示增生减低或重度减低;小粒空虚,非造血细胞(淋巴细胞、网状细胞、浆细胞、肥大细胞等)比例增高;巨核细胞明显减少或缺如;红系、粒系细胞均明显减少。
骨髓活检:至少取2cm骨髓组织(髂骨)标本用以评估骨髓增生程度、各系细胞比例、造血组织分布情况,以及是否存在骨髓浸润、骨髓纤维化等。
氯吡格雷致血小板减少1例
氯吡格雷致血小板减少1例随着氯吡格雷应用的日益广泛,大有取代噻氯匹定之势。
以前认为氯吡格雷致TTP发生率比噻氯匹定低,但越来越多的临床研究证实冠状动脉支架置入术患者术后服用氯吡格雷致血栓形成发生率和死亡率升高,无论TTP发生率和严重TTP发生率都是氯吡格雷高于噻氯匹定。
从使用氯吡格雷治疗发生TTP的患者改用环孢素A和噻氯匹定而没有发生TTP的例子,可以得出药源性TTP还存在非免疫学机制。
可能是由细胞因子损伤血管内皮细胞,导致血小板黏附、聚集于损伤的血管内皮处形成血栓,导致微血管红细胞溶解和血小板减少等一系列继发性病变。
标签:氯吡格雷;血小板1临床资料患者女,79岁,因”反复胸闷3 d,再发3 h余”于2012年10月10日入院,既往有1年余糖尿病史,入院后心电图检查示心房颤动,V5-6、下壁导联ST段压低,A VRST段抬高,V7-9ST段压低,入院查体:心律不齐,各瓣膜区均未闻及病理性杂音,其余查体未见异常;入院后诊断为:①冠心病,不稳定型心绞痛;②2型糖尿病,入院后予依诺肝素0.4mL IH q12 h,阿司匹林100 mg qd 波利维75 mg qd治疗,入院时查血常规示血小板166×109/L,入院后依诺肝素使用5 d 后停用,10月20日复查血常规示血小板数142×109/L,10月24日复查血常规示血小板34×109/L,期间患者无皮下瘀斑、瘀点出现,立即停用阿司匹林和波利维,停用抗血小板药物后10月28日复查血常规示血小板示72×109/L,之后11月4日復查血常规示血小板132×109/L,故加用阿司匹林,经予11月14日、11月29日复查血常规均是血小板数均>100×109/L,1个月后、2个月后复查血常规血小板数分别为143×109/L,152×109/L,故考虑该患者系波利维致血小板减少。
原发性宫颈印戒细胞癌一例
bopag:aphase2study[J].Blood,2022,139(1):34-43.[10]YoshizatoT,DumitriuB,HosokawaK,etal.Somaticmutationsandclonalhematopoiesisinaplasticanemia[J].NEnglJMed,2015,373(1):35-47.[11]张㊀婷,陈㊀洋,李瑞鑫,等.再生障碍性贫血髓系肿瘤基因突变靶向测序临床研究[J].临床血液学杂志,2021,34(3):168-171.[12]SociéG,Henry⁃AmarM,BacigalupoA,etal.Malignanttumorsoccurringaftertreatmentofaplasticanemia.EuropeanBoneMarrowTransplantation⁃SevereAplasticAnaemiaWorkingParty[J].NEnglJMed,1993,329(16):1152-1157.[收稿日期㊀2023-05-13][本文编辑㊀韦㊀颖]本文引用格式顾㊀蔚,胡海波,朱㊀伟,等.再生障碍性贫血继发恶性实体肿瘤二例[J].中国临床新医学,2023,16(10):1082-1084.㊀㊀[关键词]㊀原发性;㊀宫颈印戒细胞癌;㊀分子标志物检测㊀㊀[中图分类号]㊀R737㊀[文章编号]㊀1674-3806(2023)10-1084-03㊀㊀doi:10.3969/j.issn.1674-3806.2023.10.201 病例介绍患者,女,66岁,因 反复阴道排液2个月 于2021年6月13日至长沙珂信肿瘤医院就诊㊂初诊体格检查发现宫颈上唇一直径约5cm肿块,宫颈管呈桶状增粗,质地硬,触之出血㊂血小板319ˑ109/L㊂血浆D⁃二聚体4 52μg/ml㊂血清肿瘤标志物结果示:鳞状细胞癌抗原(SCC)3 32ng/ml;糖类抗原⁃199(CA⁃199)10 48IU/ml;糖类抗原⁃125(CA⁃125)350 20IU/ml;癌胚抗原(CEA)109 30ng/ml㊂双下肢静脉彩超检查示:左侧腘静脉及双侧肌肉间静脉低回声物,考虑血栓形成㊂盆腔MRI检查示:宫颈及宫颈管巨大肿块影,大小约8 3cmˑ5 3cmˑ4 7cm,符合宫颈癌;双侧宫旁未见明显受侵(见图1)㊂宫颈人乳头瘤病毒(humanpapillomavirus,HPV)18型阳性㊂宫颈液基细胞学检查示意义不明确的非典型鳞状细胞㊂宫颈活检病理结果示(宫颈3㊁6㊁9㊁12点方位)低分化腺癌,大部分为印戒细胞癌㊂因患者病理类型特殊,且部分消化道肿瘤标志物增高,为排除消化道来源转移性恶性肿瘤,继续行电子胃镜㊁肠镜检查,胃镜下胃底息肉样赘生物,镜下活检病理结果示胃底腺息肉;肠镜下未见肠黏膜明显占位性病变㊂结合患者病史及上述检查,初步诊断为:(1)宫颈印戒细胞癌ⅠB3期;(2)双下肢静脉血栓㊂经过长沙珂信肿瘤医院多学科诊疗模式讨论认为,本例患者应积极行根治性手术治疗,且术后需补充治疗;术前可局部给予介入血管栓塞治疗阻断肿瘤血供,并同时行新辅助化疗缩小瘤体㊂患者合并下肢静脉血栓,为了降低围术期远处器官栓塞风险,术前应处理血栓㊂综合以上情况,本例患者于2021年6月17日行下腔静脉滤器植入术,术后给予低分子肝素钠皮下注射㊂于6月18日行子宫动脉造影下栓塞术+灌注化疗术(化疗为TP方案:多西他赛+顺铂)㊂在介入治疗1周后复查盆腔MRI示:宫颈肿块较前缩小,大小约6 9cmˑ4 3cmˑ4 1cm㊂患者于7月1日完成根治手术(经腹广泛性子宫切除术+双侧附件切除术+盆腔淋巴结清扫术)㊂术后大体标本可见:宫颈肿块大小为6 0cmˑ4 0cmˑ2 5cm,侵犯宫颈管及宫腔㊂术后病理结果示:宫颈㊁宫颈管低分化黏液腺癌,符合印戒细胞癌(见图2)㊂宫颈浸润深度约1 4cm(宫颈间质厚约1 5cm),宫颈管浸润深度约1 0cm(此处宫颈管深度约1 5cm),宫颈管腔面见癌组织侵犯,双侧宫旁未见癌,阴道残端未见癌㊂盆腔淋巴结均未见癌转移㊂免疫组化结果示:CDX⁃2㊁CD10㊁AFP㊁CD30㊁p40㊁Vimentin㊁ER㊁PR㊁HER⁃2均为阴性,p16(弥漫2+,见图3)㊁CK7(弥漫3+)㊁CK20(灶性+)㊁Ki⁃67(阳性指数30%)㊁CEA(2+)㊁CK⁃P(3+)㊁CK5/6(2+)㊁㊃4801㊃ChineseJournalofNewClinicalMedicine,October2023,Volume16,Number10㊀㊀p53(灶5%+)㊂四项错配修复(mismatchrepair,MMR)蛋白:MSH2(+)㊁MSH6(+)㊁MLH1(+)㊁PMS2(+),提示pMMR状态(微卫星稳定状态)㊂综上,患者术后明确诊断为宫颈低分化印戒细胞癌ⅠB3期㊂患者术后接受了1周期TC方案(多西他赛+卡铂)全身静脉化疗,拟定补充盆腔外照射放疗[临床靶体积(CTV)包括:阴道残端㊁部分阴道㊁阴道旁组织㊁原宫旁及盆腔淋巴引流区,上界L4上缘,下界双侧闭孔下缘,95%计划靶体积(PTV),46Gy:2Gy/23F]㊂患者于2021年10月18日开始放疗,由于放疗过程中反复出现 尿频㊁尿急㊁尿痛 等副反应,患者拒绝继续放疗,因此实际仅执行5次放疗,未能完成全部照射计划㊂结束治疗后患者于长沙珂信肿瘤医院规律完成复查及随访,目前生化检查及影像学资料仍无疾病进展及复发证据㊂自患者初诊至2023年4月,总随访生存时间为22个月㊂㊀图1㊀患者宫颈肿块在盆腔MRI的影像学所见图2㊀患者术后组织病理学印戒细胞癌表现图(HEˑ50)图3㊀患者p16蛋白的免疫组化染色图(HEˑ50)2㊀讨论2 1㊀宫颈癌是我国最常见的女性生殖系统恶性肿瘤之一㊂在组织病理类型上,宫颈鳞癌最为常见且预后最好,约占80%;宫颈腺癌虽仅占15% 20%,但其恶性程度高,且近年来发生率呈上升趋势[1]㊂2014年世界卫生组织将宫颈黏液性腺癌分为胃型㊁肠型及印戒细胞型3种类型,其中以原发性宫颈印戒细胞癌(primarycervicalsignet⁃ringcellcarcinoma,PCSRCC)这类型最为罕见[2⁃3]㊂印戒细胞癌常见于消化道恶性肿瘤(比如胃癌),其余部位多为转移瘤㊂也有报道自肺癌㊁乳腺癌㊁阑尾癌㊁胆管癌或卵巢癌转移[4],而PCSRCC罕见[5⁃6]㊂自1990年报道PCSRCC以来[5],目前国内外已发表的文献较少,缺乏对PCSRCC的诊断及治疗经验㊂2 2㊀病理学诊断是宫颈印戒细胞癌诊断的金标准㊂绝大部分宫颈癌患者的症状为不规则阴道流血或性交后阴道流血,其主要病理类型为鳞癌㊂除上述症状外,部分宫颈腺癌患者还可出现不规则阴道排液㊂在已报道文献中,有2例主诉为 异常阴道排液 [7⁃8]㊂本例患者主诉 不规则阴道排液2个月 就诊,符合既往文献的报道㊂除此之外,PCSRCC患者在体格检查㊁实验室检验及MRI㊁CT等影像学检查等方面,与其他病理类型的宫颈癌患者比较并无特异性差异,增加了PCSRCC诊断的难度㊂2 3㊀基于病理诊断的结果,宫颈发现的印戒细胞癌必须与其他部位来源的转移瘤相鉴别[3],除了采用内镜手段排除胃肠道原发肿瘤之外(如本例患者),检测HPV的感染和生物标记蛋白的表达可为PCSRCC的鉴别诊断提供依据[7]㊂HPV16型和18型感染与宫颈癌发生最为密切[9],以往文献报道中,大部分PCSRCC患者为HPV18型阳性[4,7,9⁃11]㊂本例患者亦为HPV18型阳性,推测HPV18型感染可能与PCSRCC的发病及进展密切相关,但还需更多样本量研究证实㊂通过免疫组化检测生物标记蛋白表达量在分子层面为PCSRCC的鉴别诊断提供了重要依据㊂文献提示p16可作为一个重要的诊断标志物[7]㊂本例患者p16表达阳性且范围弥漫,阳性程度高㊂本例患者CK20为阳性表达,ER及PR为阴性表达,与文献[4,11⁃13]报道相符合㊂有文献指出CDX⁃2在PCSRCC中为阳性表达[8,13],而本例患者CDX⁃2为阴性㊂本例患者的CK7为阳性表达,有文献指出胃转移及乳腺转移的宫颈印戒细胞癌中CK7亦为阳性表达[7],故CK7无法作为鉴别肿瘤来源的分子标志物㊂本例检测了MMR标志物(MSH2㊁MSH6㊁MLH1㊁PMS2),因PCSRCC尚无有效的治疗方案,检查微卫星稳定状态㊁PDL1表达量㊁MMR标志物及肿瘤突变负荷等基因检测十分重要,为PCSRCC患者提供可能的免疫治疗选择㊂2 4㊀PCSRCC总体预后较差,从现有报道文献来看,预后与患者国际妇产科学联合(InternationalFederationofGynecologyandObstetrics,FIGO)分期相关[14]㊂PCSRCC的治疗主要依据鳞癌㊁腺癌㊁腺鳞癌3种病理类型的方案推荐[1]㊂文献显示,晚期患者疾病进展迅速,3例㊃5801㊃㊀㊀中国临床新医学㊀2023年㊀10月㊀第16卷㊀第10期Ⅳ期患者生存期均不到3个月[10⁃11],其中1例确诊后7周内死亡[11]㊂1例ⅢC期患者在接受姑息化疗后随访生存期超过半年[15]㊂大部分早期患者都接受了手术治疗,其中3例ⅠB期患者仅接受手术并未补充放化疗[9,11,16],仅接受手术的1例患者随访期内生存时间达25个月[16]㊂有2例ⅠB期患者接受了手术,术后辅助同步放化疗,生存期超过8年(其中1例生存期长达10年)[13,17]㊂本例患者FIGO分期为ⅠB期,手术前给予介入治疗及新辅助化疗以缩小瘤体,术后计划补充同步放化疗,但由于患者无法耐受未能完成所有巩固治疗计划,截至2023年4月,随访期内生存时间达22个月㊂2 5㊀PCSRCC的恶性程度高,预后差㊂由于病例较少,治疗手段和方案尚未形成专家共识㊂通过不断累积的案例报道,笔者认为通过HPV感染状态㊁分子标志物检测等手段,可为PCSRCC的诊断及鉴别诊断提供有力的依据㊂参考文献[1]彭巧华,吕卫国.2022年第1版‘NCCN子宫颈癌临床实践指南“解读[J].实用肿瘤杂志,2022,37(3):205-214.[2]赵东奇,李㊀淼,朱继红,等.原发性宫颈印戒细胞癌1例报告[J].西南国防医药,2021,31(2):181-182.[3]LazharH,SlaouiA,RostoumS,etal.Primarysignetringcellcarci⁃nomaofthecervix:aboutanuncommoncasereport[J].IntJSurgCaseRep,2023,105:107950.[4]WashimiK,YokoseT,NoguchiA,etal.Diagnosisofprimarypuresignet⁃ringcellcarcinomaofthecervix[J].PatholInt,2015,65(7):393-395.[5]MollUM,ChumasJC,MannWJ,etal.Primarysignetringcellcar⁃cinomaoftheuterinecervix[J].NYStateJMed,1990,90(11):559-560.[6]CardosiRJ,ReedyMB,VanNagellJR,etal.Neuroendocrinesignetringcelladenocarcinomaoftheendocervix[J].IntJGynecolCancer,1999,9(5):433-437.[7]GiordanoG,PizziS,BerrettaR,etal.Anewcaseofprimarysignet⁃ringcellcarcinomaofthecervixwithprominentendometrialandmyo⁃metrialinvolvement:immunohistochemicalandmolecularstudiesandreviewoftheliterature[J].WorldJSurgOncol,2012,10:7.[8]Su rez⁃PeñarandaJM,AbdulkaderI,Barón⁃DuarteFJ,etal.Signet⁃ringcellcarcinomapresentingintheuterinecervix:reportofaprimaryand2metastaticcases[J].IntJGynecolPathol,2007,26(3):254-258.[9]BalciS,SaglamA,UsubutunA.Primarysignet⁃ringcellcarcinomaofthecervix:casereportandreviewoftheliterature[J].IntJGynecolPathol,2010,29(2):181-184.[10]CracchioloB,KuhnT,HellerD.Primarysignetringcelladenocar⁃cinomaoftheuterinecervix arareneoplasmthatraisestheques⁃tionofmetastasistothecervix[J].GynecolOncolRep,2016,16:9-10.[11]SalV,KahramanogluI,TuranH,etal.Primarysignetringcellcarci⁃nomaofthecervix:acasereportandreviewoftheliterature[J].IntJSurgCaseRep,2016,21:1-5.[12]VerasE,SrodonM,NeijstromES,etal.MetastaticHPV⁃relatedcer⁃vicaladenocarcinomaspresentingwiththromboembolicevents(trous⁃seausyndrome):clinicopathologiccharacteristicsof2cases[J].IntJGynecolPathol,2009,28(2):134-139.[13]InsabatoL,SimonettiS,DeCecioR,etal.Primarysignet⁃ringcellcarcinomaoftheuterinecervixwithlongtermfollow⁃up:casereport[J].EurJGynaecolOncol,2007,28(5):411-414.[14]PurwotoG,NuryantoKH,WibowoTA,etal.Couldcombinationofradicalhysterectomyandradiationeffectiveinthetreatmentofpri⁃marycervicalsignetringcellcarcinoma?:ararecasereport[J].IntJSurgCaseRep,2022,94:107083.[15]MoritaniS,IchiharaS,KushimaR,etal.CombinedsignetringcellandglassycellcarcinomaoftheuterinecervixarisinginayoungJapanesewoman:acasereportwithimmunohistochemicalandhistochemicalanalyses[J].PatholInt,2004,54(10):787-792.[16]MayorgaM,García⁃ValtuilleA,Fern ndezF,etal.Adenocarcinomaoftheuterinecervixwithmassivesignet⁃ringcelldifferentiation[J].IntJSurgPathol,1997,5(3⁃4):95-100.[17]LoweryWJ,DifurioMJ,SundborgMJ,etal.Cervicalsignet⁃ringcellcarcinomapresentingasasynchronousprimarycarcinomawithuterineadenocarcinoma[J].MilMed,2009,174(2):212-213.[收稿日期㊀2023-07-29][本文编辑㊀韦㊀颖]本文引用格式敖基兴,张建飞,刘国华.原发性宫颈印戒细胞癌一例[J].中国临床新医学,2023,16(10):1084-1086.㊃6801㊃ChineseJournalofNewClinicalMedicine,October2023,Volume16,Number10㊀㊀。
再生障碍性贫血继发恶性实体肿瘤二例
㊀㊀[关键词]㊀再生障碍性贫血;㊀继发;㊀恶性实体肿瘤㊀㊀[中图分类号]㊀R556 5㊀[文章编号]㊀1674-3806(2023)10-1082-03㊀㊀doi:10.3969/j.issn.1674-3806.2023.10.191 病例介绍病例1㊀女,56岁,1992年因 反复发热2周 在徐州市第一人民医院就诊㊂血常规结果示:白细胞1 5ˑ109/L,中性粒细胞0 47ˑ109/L,血红蛋白90g/L,血小板50ˑ109/L㊂骨髓细胞学示:骨髓小粒偶见,呈空架状,有核细胞量减少㊂中性粒细胞各阶段细胞比例降低,幼稚粒细胞少见,部分中性粒细胞胞浆内含有中毒性颗粒㊂淋巴细胞约占69 5%,巨核细胞全片未见,血小板少见㊂骨髓活检示:骨髓增生显著低下,仅见2个巨核细胞,未见明显异型增生及原始细胞增多㊂综合以上检查结果诊断为再生障碍性贫血(aplasticanemia,AA)㊂予以积极抗感染,环孢素A㊁十一酸睾丸酮治疗后,症状好转,病情平稳㊂2019年7月24日患者因受凉后出现咳嗽㊁咳痰再次入住徐州市第一人民医院㊂患者咳嗽阵发性发作,痰较难咳出,呈白色黏液痰,无发热㊁骨痛㊁憋喘㊁阵发性呼吸困难㊂入院前曾在当地社区医院予阿奇霉素抗感染治疗,效果不佳㊂查胸部CT示:考虑右肺下叶炎症可能;其他双肺散在少许炎症,考虑双肺尖陈旧性病变可能㊂以抗感染治疗2周后复查血常规结果示:白细胞3 33ˑ109/L,中性粒细胞1 47ˑ109/L,血红蛋白93g/L,血小板74ˑ109/L;胸部CT示炎症部位大小较前无明显改变;磷癌抗原24 89ng/ml,较正常升高㊂2019年8月19日行胸部增强CT示:右肺下叶内基底位置占位,符合肺恶性肿瘤CT表现㊂18F⁃脱氧葡萄糖(18F⁃fluorodeoxyglucose,18F⁃FDG)肿瘤全身探查示:右肺下叶病灶FDG代谢轻度增高,考虑肿瘤性病变可能㊂复查骨髓细胞学示:粒系㊁红系㊁巨核系增生活跃,血小板散在可见,未见异常肿瘤细胞㊂综合检查结果考虑患者存在肺癌可能,患者于2019年8月23日至外院行胸腔镜手术,术后病理诊断为肺腺癌㊂病例2㊀女,57岁,2013年因 反复发作头晕㊁乏力不适 ,就诊于徐州市第一人民医院血液科㊂血常规结果示:白细胞1 8ˑ109/L,中性粒细胞0 32ˑ109/L,血红蛋白90g/L,血小板36ˑ109/L㊂多部分行骨髓穿刺,骨髓细胞学示:多部位骨髓增生减低,淋巴细胞比例70%,骨髓小粒空虚㊂骨髓活检示:全切片增生减低,造血组织减少,未见异常细胞㊂综合以上检查结果诊断为AA,予间断输血支持治疗,予以口服环孢素A联合司坦唑醇等治疗,症状好转㊂2022年10月至2022年11月患者因多次黑便,出现胸闷㊁心悸症状,遂到徐州市第一人民医院就诊㊂复查血常规示:白细胞2 73ˑ109/L,血红蛋白43g/L,血小板36ˑ109/L㊂予以输注红细胞㊁血小板对症支持治疗后,复查骨髓细胞学示:骨髓增生减低,有核红细胞散在不明显灶性分布,粒系㊁巨核系增生减低㊂胃镜检查结果示:浅表性胃窦炎,伴胆汁反流;胃窦小弯侧大片增生及溃疡改变㊂胃窦病理结果:考虑低分化腺癌(印戒细胞癌)㊂予以阿伐曲泊帕口服联合输注血小板治疗,以提升血小板水平㊁改善止凝血功能,为行手术治疗创造条件㊂患者于2022年12月1日转入普外科治疗,12月2日术中发现肿瘤位于胃窦部,大小约3cmˑ2cmˑ1cm,尚未侵犯浆膜外(见图1ⓐ)㊂行胃癌根治术(毕I式),术后予以抗炎㊁补液㊁抑酸等对症支持治疗㊂术后病理示:距上切端5cm下切端3cm胃窦小弯侧浸润溃疡型低黏附性癌,部分为印戒细胞癌㊂Lauren分型:弥漫型,癌侵犯胃壁㊃2801㊃ChineseJournalofNewClinicalMedicine,October2023,Volume16,Number10㊀㊀全层达浆膜下脂肪组织内,部分侵犯间皮层,侵犯神经,脉管内见癌栓,上下切端均(-),下切端脉管内见癌栓,胃小弯淋巴结见癌转移(15/16枚),胃大弯淋巴结见癌转移(9/9枚),胃网膜组织未见癌, 吻合口 未见癌㊂CK7(+),CK20(-),Villin(+),CEA(小灶+),CDX⁃2(+),HER⁃2(1+),EGFR(部分弱+),MUC5AC(+),MUC6(少量弱+),PMS2(+),MSH2(+),MSH6(+),MLH1(+),Ki⁃67(阳性指数60%),免疫组化结果支持原诊断,并示错配修复功能完整(见图1ⓑ)㊂ⓐ胃窦病理(HEˑ10);ⓑ术后病理(HEˑ100)图1㊀病例2病理所见2㊀讨论2 1㊀AA是一种常见的骨髓造血功能衰竭性疾病,发病机制至今尚未完全明确,可能与免疫系统异常㊁造血干细胞减少㊁基因突变以及造血微环境的改变有关,以全血细胞减少为特征,主要临床表现为感染㊁出血㊁贫血[1⁃2]㊂诊断本病需要完善血常规㊁骨髓细胞形态学㊁骨髓活检㊁流式细胞术㊁染色体核型分析㊁基因检测等相关检查,以全面评估患者病情,明确有无先天性造血功能衰竭等疾病存在,并排除阵发性睡眠性血红蛋白尿以及骨髓增生异常综合征㊂临床发现本病与阵发性睡眠性血红蛋白尿相关,并可进展为骨髓增生异常综合征或急性髓系白血病[3]㊂但临床上继发恶性实体肿瘤的文献报道较少㊂2 2㊀病例1多年前在多家医院就诊,均诊断为AA,予以环孢素㊁十一酸睾丸酮治疗后,病情平稳㊂2019年7月患者因出现咳嗽㊁咳痰等呼吸道症状就诊,与肺部感染相似,经抗感染后未明显好转,行增强胸部CT㊁正电子发射计算机断层扫描检查考虑肺部恶性肿瘤可能,最终行肺病理活检,及时诊断肺部恶性肿瘤,进行早期切除,未延误病情㊂随访至2022年5月,患者病情平稳㊂2 3㊀病例2诊断AA明确,消化道出血为患者此次就诊原因,血小板减少引发出血是AA常见症状之一,但因反复消化道出血行电子内镜检查发现胃部恶性肿瘤㊂在多学科共同诊疗下,最终行胃部肿瘤切除术,延长患者生存时间同时提高患者生存质量㊂随访至2022年5月,患者病情平稳㊂AA有向恶性疾病进展或转变的风险,一方面与AA本身的发病机制有关:已知免疫异常是AA的重要发病机制之一,研究结果显示细胞毒性T淋巴细胞通过激活FAS/FASL凋亡通路或者上调肿瘤坏死因子⁃α㊁干扰素⁃γ的产生从而介导了造血干细胞免疫损伤易引起AA的发生[4],而免疫系统负责清除癌性基因,当免疫受损后抑癌作用减弱,因此容易合并肿瘤的发生㊂另一方面,AA患者长期维持治疗中需要应用免疫抑制剂[5],环孢素A或他克莫司的长期作用引发机体免疫监控失常,不能及时消灭突变的细胞;此外,环孢素A可阻碍断裂的DNA修复以及促进转化生长因子⁃β产生增高,他克莫司可增加肿瘤的侵袭性等作用促进了肿瘤的发生[6⁃7]㊂研究还发现AA存在细胞遗传学方面的异常[8⁃9]㊂研究发现,部分AA患者存在染色体异常,常见有+8㊁+6㊁13号染色体异常等,这些异常的克隆性增生占AA患者的4% 11%,而存在染色体异常或基因异常是否会发生其他肿瘤性疾病尚需进行密切观察及随访[10]㊂2 4㊀AA可与多种血液系统疾病发生转化,如AA与骨髓增生异常综合征㊁阵发性睡眠性血红蛋白尿之间可相互转化,有的最终发展成急性髓系白血病[11]㊂但AA合并恶性实体肿瘤较少见[12]㊂这类肿瘤的临床表现与AA类似,及时㊁积极进行骨髓复查等相关检查是减少临床漏诊的可行方法㊂参考文献[1]DeegHJ.Morethanoneangletotargetaplasticanemia?[J].Cancer,2018,124(21):4165-4167.[2]FurlongE,CarterT.Aplasticanaemia:currentconceptsindiagnosisandmanagement[J].JPaediatrChildHealth,2020,56(7):1023-1028.[3]ClucasDB,FoxLC,WoodEM,etal.Revisitingacquiredaplasticanaemia:currentconceptsindiagnosisandmanagement[J].InternMedJ,2019,49(2):152-159.[4]ScheinbergP.Acquiredsevereaplasticanaemia:howmedicaltherapyevolvedinthe20thand21stcenturies[J].BrJHaematol,2021,194(6):954-969.[5]PeslakSA,OlsonT,BabushokDV.Diagnosisandtreatmentofaplasticanemia[J].CurrTreatOptionsOncol,2017,18(12):70.[6]徐小明,张㊀岩,徐自强,等.肾移植受者并发恶性肿瘤34例临床分析[J].中华移植杂志(电子版),2012,6(2):97-104.[7]张强弩.他克莫司代替环孢素治疗对肝移植受者新发肿瘤发病率的影响[J].中华移植杂志(电子版),2013,7(4):225-226.[8]常光妮,王绪栋,孙㊀燕,等.儿童重型再生障碍性贫血合并多发性骨软骨瘤1例[J].现代医药卫生,2022,38(5):898-900.[9]PatelBA,GroarkeEM,LotterJ,etal.Long⁃termoutcomesinpatientswithsevereaplasticanemiatreatedwithimmunosuppressionandeltrom⁃㊃3801㊃㊀㊀中国临床新医学㊀2023年㊀10月㊀第16卷㊀第10期bopag:aphase2study[J].Blood,2022,139(1):34-43.[10]YoshizatoT,DumitriuB,HosokawaK,etal.Somaticmutationsandclonalhematopoiesisinaplasticanemia[J].NEnglJMed,2015,373(1):35-47.[11]张㊀婷,陈㊀洋,李瑞鑫,等.再生障碍性贫血髓系肿瘤基因突变靶向测序临床研究[J].临床血液学杂志,2021,34(3):168-171.[12]SociéG,Henry⁃AmarM,BacigalupoA,etal.Malignanttumorsoccurringaftertreatmentofaplasticanemia.EuropeanBoneMarrowTransplantation⁃SevereAplasticAnaemiaWorkingParty[J].NEnglJMed,1993,329(16):1152-1157.[收稿日期㊀2023-05-13][本文编辑㊀韦㊀颖]本文引用格式顾㊀蔚,胡海波,朱㊀伟,等.再生障碍性贫血继发恶性实体肿瘤二例[J].中国临床新医学,2023,16(10):1082-1084.㊀㊀[关键词]㊀原发性;㊀宫颈印戒细胞癌;㊀分子标志物检测㊀㊀[中图分类号]㊀R737㊀[文章编号]㊀1674-3806(2023)10-1084-03㊀㊀doi:10.3969/j.issn.1674-3806.2023.10.201 病例介绍患者,女,66岁,因 反复阴道排液2个月 于2021年6月13日至长沙珂信肿瘤医院就诊㊂初诊体格检查发现宫颈上唇一直径约5cm肿块,宫颈管呈桶状增粗,质地硬,触之出血㊂血小板319ˑ109/L㊂血浆D⁃二聚体4 52μg/ml㊂血清肿瘤标志物结果示:鳞状细胞癌抗原(SCC)3 32ng/ml;糖类抗原⁃199(CA⁃199)10 48IU/ml;糖类抗原⁃125(CA⁃125)350 20IU/ml;癌胚抗原(CEA)109 30ng/ml㊂双下肢静脉彩超检查示:左侧腘静脉及双侧肌肉间静脉低回声物,考虑血栓形成㊂盆腔MRI检查示:宫颈及宫颈管巨大肿块影,大小约8 3cmˑ5 3cmˑ4 7cm,符合宫颈癌;双侧宫旁未见明显受侵(见图1)㊂宫颈人乳头瘤病毒(humanpapillomavirus,HPV)18型阳性㊂宫颈液基细胞学检查示意义不明确的非典型鳞状细胞㊂宫颈活检病理结果示(宫颈3㊁6㊁9㊁12点方位)低分化腺癌,大部分为印戒细胞癌㊂因患者病理类型特殊,且部分消化道肿瘤标志物增高,为排除消化道来源转移性恶性肿瘤,继续行电子胃镜㊁肠镜检查,胃镜下胃底息肉样赘生物,镜下活检病理结果示胃底腺息肉;肠镜下未见肠黏膜明显占位性病变㊂结合患者病史及上述检查,初步诊断为:(1)宫颈印戒细胞癌ⅠB3期;(2)双下肢静脉血栓㊂经过长沙珂信肿瘤医院多学科诊疗模式讨论认为,本例患者应积极行根治性手术治疗,且术后需补充治疗;术前可局部给予介入血管栓塞治疗阻断肿瘤血供,并同时行新辅助化疗缩小瘤体㊂患者合并下肢静脉血栓,为了降低围术期远处器官栓塞风险,术前应处理血栓㊂综合以上情况,本例患者于2021年6月17日行下腔静脉滤器植入术,术后给予低分子肝素钠皮下注射㊂于6月18日行子宫动脉造影下栓塞术+灌注化疗术(化疗为TP方案:多西他赛+顺铂)㊂在介入治疗1周后复查盆腔MRI示:宫颈肿块较前缩小,大小约6 9cmˑ4 3cmˑ4 1cm㊂患者于7月1日完成根治手术(经腹广泛性子宫切除术+双侧附件切除术+盆腔淋巴结清扫术)㊂术后大体标本可见:宫颈肿块大小为6 0cmˑ4 0cmˑ2 5cm,侵犯宫颈管及宫腔㊂术后病理结果示:宫颈㊁宫颈管低分化黏液腺癌,符合印戒细胞癌(见图2)㊂宫颈浸润深度约1 4cm(宫颈间质厚约1 5cm),宫颈管浸润深度约1 0cm(此处宫颈管深度约1 5cm),宫颈管腔面见癌组织侵犯,双侧宫旁未见癌,阴道残端未见癌㊂盆腔淋巴结均未见癌转移㊂免疫组化结果示:CDX⁃2㊁CD10㊁AFP㊁CD30㊁p40㊁Vimentin㊁ER㊁PR㊁HER⁃2均为阴性,p16(弥漫2+,见图3)㊁CK7(弥漫3+)㊁CK20(灶性+)㊁Ki⁃67(阳性指数30%)㊁CEA(2+)㊁CK⁃P(3+)㊁CK5/6(2+)㊁㊃4801㊃ChineseJournalofNewClinicalMedicine,October2023,Volume16,Number10㊀㊀。
再生障碍性贫血英文ppt课件
• 2.Generally,without the liver and spleen enlargement. • 3.At least one area of hypoplasia in bone marrow. Non-
SAA laboratory criteria
To define SAA there must be at least two of the following: (1) absolute neutrophil count less than 0.5 × 109/L, (2) platelet count less than 20 × 109/L,
3.Bone marrow smear
• The bone marrow is usually readily aspirated but dilute on smear, and the fatty biopsy specimen may be grossly pale on withdrawal; In severe aplasia the smear of the aspirated specimen shows only red cells, residual lymphocytes, and stromal cells.
C. Normal bone marrow aspirate smear. The marrow is normally 30–70% cellular, and there is a heterogeneous mix of myeloid, erythroid, and lymphoid cells.
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Therapy:
Renew of the seed Bone marrow transplantation
fertilize the soil Growth factors
kill the worms
Immunosuppressive treatment
Thank You For Your Attention!
Hematopoietic stem cell.
Pathogenesis
Primary defect or damage to hematopoietic stem cells
Flow cytometry shows that the CD34-cell population,which contain the the stem cells is substantially reduced Date from in vitro colony-culture assays suggest profound functional loss of the hematopoietic progenitors
These cells produce inhibitory cytokines,such as gammarinterferon and tumor necrosis factor, these cytokines suppress hemotopoiesis by affecting the mitotic cycle and cell killing by inducing Fas-mediated apoptosis)
Aplastic Anemia
Li Fuxing Tongji Hospital of Tongji University.
Outline
• Definition
• Pathogenesis
• Clinical features
• Treatment
• summary
Definition
Aplastice anemia Failure of the bone marrow stem cells to produce mature cells and normal marrow is replaced by fat cells. Character Peripheral blood pancytopenia (anemia, reduced WBC and platelet count)
Seed Soil Worm
Clinical Features.
Low WBC count Low platelets Anemia recurrent infections. bruising/bleeding. tiredness/palpitation
Marrow Biopsy
Treatment
Renew of the
Restoration of marrow activity
Bone marrow/stem cell transplantation
Fertilize the soil
Supportive -Growth factors
G-CSF,EPO,IL-11
Kill the worms
Pathogenesis
possible Immunological attack on stem cells
Expanded popultion of the cytotoxic T lymphocytes: CD8,HLA-DR+,which are detectable in both the blood and the bone marrow of patients with aplastic anemia.
Abnormal cells are not found.
Normal Hematopoiesis.
• • • • Red cell life span 120 days. Platelet life span 6 days. Granulocyte life span < 24 hours. Constant marrow activity needed to replace dead cells.
Pathogenesis
Defective microenvironment
Bone marrow stromal defect low G-CSF ,IL-11 and so on
Pathogenesis
The seed soil and worm theory seed Stem cell defect Soil microenvironment disorder Worm Immunological attack on stem cells
Immunosuppressive treatment
Antilymphocyte glob ,Cyclosporin, Prednisolone
summary
Pathogenesis:The seed soil and worm theory
seed Stem cell defect Soil microenvironment disorder Worm Immunological attack on stem cells