【求助】kappa值的意义
一致性检验KAPPA检验详细解读
一致性检验(Kappa检验)诊断试验的一致性检验经常用在下列两种情况中:一种是评价待评价的诊断实验方法与金标准的一致性;另一种是评价两种化验方法对同一个样本(化验对象)的化验结果的一致性或两个医务工作者对同一组病人的诊断结论的一致性或同一医务工作者对同一组病人前后进行两次观察作出的诊断的一致性等等。
Kappa值即内部一致性系数(inter-rater,coefficient of internal consistency),是作为评价判断的一致性程度的重要指标。
取值在0~1之间。
Kappa≥0.75两者一致性较好;0.75>Kappa≥0.4两者一致性一般;Kappa<0.4两者一致性较差。
操作方法:单击【Statistics钮】,在弹出的Statistics对话框中选择Kappa 复选框。
计算Kappa值。
如果选择Risk复选框,则计算OR值(比数比)和RR值(相对危险度)。
病例对照研究(case control study)是主要用于探索病因的一种流行病学方法。
它是以某人群内一组患有某种病的人(称为病例)和同一人群内未患这种病但在与患病有关的某些已知因素方面和病例组相似的人(称为对照)作为研究对象;调查他们过去对某个或某些可疑病因(即研究因子)的暴露有无和(或)暴露程度(剂量);通过对两组暴露史的比较,推断研究因子作为病因的可能性:如果病例组有暴露史者或严重暴露者的比例在统计学上显著高于对照组,则可认为这种暴露与患病存在统计学联系,有可能是因果联系。
究竟是否是因果联系,须根据一些标准再加以衡量判断。
所谓联系(associatiom)是指两个或更多个变量间的一种依赖关系,可以是因果关系,也可以不是。
例如,对一组肺癌病人(病例组)和一组未患肺癌但有可比性的人(对照组)调查他们的吸烟(暴露)历史(可包括现在吸烟否,过去吸过烟否,开始吸烟年龄,吸烟年数,最近每天吸烟支数;如已戒烟则为戒烟前每日吸烟支数,已戒烟年数,等等)。
kappa study

用这些新的信息,另一组交叉表格被开发出来, 用这些新的信息,另一组交叉表格被开发出来,用以将每个 评价人与基准判断比较。 评价人与基准判断比较。 A与基准判断交叉表 与基准判断交叉表
B与基准判断交叉表 与基准判断交叉表
C与基准判断交叉表 与基准判断交叉表
同时计算出Kappa值以确定每个评价人与基准判断一致的程度 值以确定每个评价人与基准判断一致的程度。 同时计算出Kappa值以确定每个评价人与基准判断一致的程度。 计算
计算测量系统的有效性
三次同时 符合基准 的次数
有效率 = 正确判断的数量 / 判断的机会总数
Kappa Study
学习目标
什么是Kappa ? 为什么要学习Kappa? 如何进行kappa 计算和分析?
Kappa :大样分析法或交叉分析法
step1
• 不同评价人对同一目标评价值的一致程 度 • 每个评价人与基准判断一致的程度
step2
step3
Hale Waihona Puke • 计算测量系统的有效性Kappa是评价人之间一致性的测量值。 Kappa值越高越好。关于具体数值表示的强度, 各家意见不一致。一般认为kappa 值在 0.4~0.75为中、高度一致,≥0.75为优良好的 一致性, <0.4为极差。 如果Kappa值为0.9或更高,那么测量系统是 优秀的
Kappa 计算方法
注:“1”为合格;“0”为不合格。
通过以上表格得出评价人之间交叉数据分析
=30×32.0/150.0
A是0,B也 是 , 也 是0的情况次 的情况次 数
上面计算了评价人间的Kappa值后,小组得到下表: 值后,小组得到下表: 上面计算了评价人间的 值后 目的: 目的:分析不同评价人对同一目标评价值的一致程度
Kappa 分析摘要
Kappa 分析摘要一般把Kappa值列为非参数统计(检验)方法参数统计:在统计推断中,如总体均数的区间估计、两个或多个均数的比较、相分析和回归系数的假设检验等,大都是假定样本所来自的总体分布为已知的函数形式,但其中有的参数为未知,统计推断的目的就是对这些未知参数进行估计或检验。
这类统计推断方法称为参数统计。
在许多实际问题中,总体分布函数形式往往不知道或者知道的很少,例如只知道总体分布是连续型的或离散型的,这时参数统计方法就不适用,此时需要借助另一种不依赖总体分布的具体形式的统计方法,也就是说不拘于总体分布,称为非参数统计或分布自由统计。
参数统计:样本来自的总体分布型是已知的(如正态分布),在这种假设基础上,对总体参数进行估计或检验。
若总体非正态,则样本例数必须充分多,或经过各种变换(对数、开方、角度……)非参数统计:未知研究总体的分布,或已知总体分布与检所要求的条件不符时,称非参数统计。
优点:①不受总体分布的限定,适用范围广,对数据的要求不像参数检验那样严格,不论研究的是何种类型的变量。
②包括那些难以测量,只能以严重程度优劣等级、次序先后等表示的资料,或有的数据一端或两端是不确定数值,例如“>50mg”,或“0.5mg以下”等。
③易于理解和掌握。
④缺点:①比起参数估计来显得比较粗。
②对适宜参数分析方法的资料若用非参数法处理,常损失部分信息、降低效率。
③虽然许多非参法计算简便,但不少方法计算仍繁杂。
非参数适用于:①检验假设中没有包括总体参数。
②资料不具备参数方法所需条件。
③计算简单实验未结束,急需知道初步结果。
④用于等级资料或某些计数资料。
非参数统计方法:一、Ridit分析 (relative to an indentified distribution)二、秩和检验: N-[Ri-(N+1)/2]2三一致性检验:Kappa临床试验研究中把重复观察的一致性分为:(1)(2) 两个及两个以上医务者对同一对象进行观察。
检验员检验能力鉴定-Kappa分析
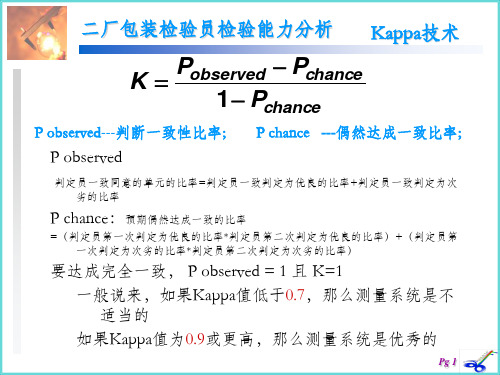
要达成完全一致, P observed = 1 且 K=1 一般说来,如果Kappa值低于0.7,那么测量系统是不 适当的 如果Kappa值为0.9或更高,那么测量系统是优秀的
肖宽鸿 10 5 50.00 (18.71, 81.29)
晋健 10 5 50.00 (18.71, 81.29)
王鲁 10 9 90.00 (55.50, 99.75)
梁延 10 6 60.00 (26.24, 87.84)
石兰 10 4 40.00 (12.16, 73.76)
杨松 10 7 70.00 (34.75, 93.33)
文远秀 10 4 40.00 (12.16, 73.76)
1、检查员与标准之 一致性比率; 2、95%之一致性置 信区间;
≧90%
# 相符数: 检验员在多次试验中的评估与已知标准一致。
Pg 18
Attribute Agreement Analysis
评估不一致
#1
#0
检验员 / 0 百分比 / 1 百分比 # Mixed 百分比
1 0.34066 0.316228 1.07726 0.1407
2、每一检查员Kappa 分析
1、每一检查ห้องสมุดไป่ตู้Kappa值
≦0.7:不适合 ≧0 .9:优秀
Pg 17
Attribute Agreement Analysis
评估一致性
3、检查员与标准一致性分析
#检 #相
95 % 置信区间
检验员 验数 符数 百分比
一二次次次次次次次次次次一二次次一二次次次次一二一二标
一致性检验kappa
大家应该也有点累了,稍作休息
大家有疑问的,可以询问和交流
12有序分类资料一致性Fra bibliotek析❖ R×C表可以分为双向无序、单向有序、双向 有序属性相同与双向有序属性不同4类。
❖ 双向无序R×C表 R×C表中两个分类变量皆 为无序分类变量,对于该类资料:①若研究目得 为多个样本率(或构成比)得比较,可用行×列 表资料得2检验;②若研究目得为分析两个分 类变量之间有无关联性以及关系得密切程度 时,可以用行×列表资料得2检验以及 Pearson列联系数进行分析。
二分类资料一致性分析
❖ 前面我们已经介绍四格表资料得2检验,本节 需要介绍得就是Kappa检验。那么Kappa检 验与配对2检验有什么区别呢?Kappa检验 重在检验两者得一致性,配对2检验重在检验 两者间得差异。对同一样本数据,这两种检验 可能给出矛盾得结论。主要原因就是两者对 所提供得有统计学意义得结论要求非常严格 所致。
KAPPA值得计算及检验
❖ 在诊断试验得研究中,数据资料多为双向有序 得列联表资料,即两个变量都就是有序变量,而 且属性相同。属性相同分为三种情况,一种情 况就是属性、分级水平数与分级水平都完全 相同。如甲医生与乙医生都把病人得检查结 果分为1、2、3、4四个等级。此时可直接作 Kappa检验。当这两个变量都只有2个水平时, 就成为配对设计得四格表资料,可使用配对χ2 检验,即McNemar检验。
Kappa
Po Pe 1 Pe
,
Po
a
n
d
,
Pe
(a
b)(a
c) (c n2
d )(b
d
)
❖ P0为实际一致率,Pe为理论一致率。
KAPPA值得计算及检验
❖ Kappa就是一个统计量,也有抽样误差,其渐进 标准误(ASE)。由于u=Kappa/ASE近似服从 标准正态分布,故可借助正态分布理论。 H0:Kappa=0,H1:Kappa≠0。如果拒绝H0认 为两种方法具有较高得一致性。
Kappa系数:一种衡量评估者间一致性的常用方法
•Biostatistics in psychiatry (25)•Kappa coefficient: a popular measure of rater agreementWan TANG 1*, Jun HU 2, Hui ZHANG 3, Pan WU 4, Hua HE 1,51 Department of Biostatistics and Computational Biology, University of Rochester, Rochester, NY , United States2College of Basic Science and Information Engineering, Yunnan Agricultural University, Kunming, Yunnan Province, China 3Department of Biostatistics, St. Jude Children’s Research Hospital, Memphis, TN, United States 4Value Institute, Christiana Care Health System, Newark, DE, United States 5Center of Excellence for Suicide Prevention, Canandaigua VA Medical Center Canandaigua, NY , United States *correspondence: wan_tang@A full-text Chinese translation of this article will be available at /cn on March 25, 2015.Summary: In mental health and psychosocial studies it is often necessary to report on the between-rater agreement of measures used in the study. This paper discusses the concept of agreement, highlighting its fundamental difference from correlation. Several examples demonstrate how to compute the kappa coefficient – a popular statistic for measuring agreement – both by hand and by using statistical software packages such as SAS and SPSS. Real study data are used to illustrate how to use and interpret this coefficient in clinical research and practice. The article concludes with a discussion of the limitations of the coefficient. Keywords: interrater agreement; kappa coefficient; weighted kappa; correlation [Shanghai Arch Psychiatry . 2015; 27(1): 62-67. doi: 10.11919/j.issn.1002-0829.215010]1. IntroductionFor most physical illnesses such as high blood pressure and tuberculosis, definitive diagnoses can be made using medical devices such as a sphygmomanometer for blood pressure or an X-ray for tuberculosis. However, there are no error-free gold standard physical indicators of mental disorders, so the diagnosis and severity of mental disorders typically depends on the use of instruments (questionnaires) that attempt to measure latent multi-faceted constructs. For example, psychiatric diagnoses are often based on criteria specified in the Fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV)[1], published by the American Psychiatric Association. But different clinicians may have different opinions about the presence or absence of the specific symptoms required to determine the presence of a diagnosis, so there is typically no perfect agreement between evaluators. In this situation, statistical methods are needed to address variability in clinicians’ ratings.Cohen’s kappa is a widely used index for assessing agreement between raters.[2] Although similar in appearance, agreement is a fundamentally different concept from correlation. To illustrate, consider an instrument with six items and suppose that two raters’ ratings of the six items on a single subject are (3,5), (4,6), (5,7), (6,8), (7,9) and (8,10). Although the scores of the two raters are quite different, the Pearson correlationcoefficient for the two scores is 1, indicating perfect correlation. The paradox occurs because there is a bias in the scoring that results in a consistent difference of 2 points in the scores of the two raters for all 6 items in the instrument. Thus, although perfectly correlated (precision), there is quite poor agreement between the two raters. The kappa index, the most popular measure of raters’ agreement, resolves this problem by assessing both the bias and the precision between raters’ ratings.In addition to its applications to psychiatric diagnosis, the concept of agreement is also widely applied to assess the utility of diagnostic and screening tests. Diagnostic tests provide information about a patient’s condition that clinicians’ often use when making decisions about the management of patients. Early detection of disease or of important changes in the clinical status of patients often leads to less suffering and quicker recovery, but false negative and false positive screening results can result in delayed treatment or in inappropriate treatment. Thus when a new diagnostic or screening test is developed, it is critical to assess its accuracy by comparing test results with those from a gold or reference standard. When assessing such tests, it is incorrect to measure the correlation of the results of the test and the gold standard, the correct procedure is to assess the agreement of the test results with the gold standard.2. ProblemsConsider an instrument with a binary outcome, with ‘1’ representing the presence of depression and ‘0’ representing the absence of depression. Suppose two independent raters apply the instrument to a random sample of n subjects. Let and denote the ratings on the n subjects by the two raters for i =1,2,...,n . We are interested in the degree of agreement between the two raters. Since the ratings are on the same scale of two levels for both raters, the data can be summarized in a 2×2 contingency table.To illustrate, Table 1 shows the results of a study assessing the prevalence of depression among 200 patients treated in a primary care setting using two methods to determine the presence of depression;[3] one based on information provided by the individual (i.e., proband) and the other based on information provided by another informant (e.g., the subject’s family member or close friend) about the proband. Intuitively, we may think that the proportion of cases in which the two ratings are the same (in this example, 34.5% [(19+50)/200]) would be a reasonable measure of agreement. But the problem with this proportion is that it is almost always positive, even when the rating by the two methods is completely random and independent of each other. So the proportion of overall agreement does not indicate whether or not two raters or two methods of rating are in agreement.by chance. This chance agreement must be removed in order to provide a valid measure of agreement. Cohen’s kappa coefficient is used to assess the level ofagreement beyond chance agreement.depressed 5065115total11684200For example, suppose that two raters with no training or experience about depression randomly decide whether or not each of the 200 patients has depression. Assume that one rater makes a positive diagnosis (i.e., considers depression present) 80% of the time and the other gives a positive diagnosis 90% of the time. Based on the assumption that their diagnoses are made independently from each other, Table 2 represents the joint distribution of their ratings. The proportion that the two raters give the same diagnosis is 74% (i.e., 0.72+0.02), suggesting that the two raters are doing a good job of diagnosing the presence of depression. But this level of agreement is purely by chance, it does not reflect the actual degree of agreement between the two raters. This hypothetical example shows that the proportion of cases in which two raters give the sameratings on an instrument is inflated by the agreementnegative 0.180.02 0.20total0.900.101.003. Kappa for 2×2 tablesConsider a hypothetical example of two raters giving ratings for n subjects on a binary scale, with ‘1’ representing a positive result (e.g., the presence of a diagnosis) and ‘0’ representing a negative result (e.g., the absence of a diagnosis). The results could be reported in a 2x2 contingency table as shown in Table 3. By convention, the results of the first rater are traditionally shown in the rows (x values) and the results of the second rater are shown in the columns (y values). Thus, n ij in the table denotes the number of subjects who receive the rating of i from the first rater and the rating j from the second rater. Let Pr(A) denote the probability of event A; then p ij =Pr(x=i,y=j) represent the proportion of all cases that receive the rating of i from the first rater and the rating j from the second rater, p i+=Pr(x=i) represents the marginal distribution of the first rater’s ratings, and p +j =Pr(y=j) represents themarginal distribution of the second rater’s ratings.11101+0 (negative)n 01n 00n 0+totaln +1n +0nIf the two raters give their ratings independently according to their marginal distributions, the probability that a subject is rated 0 (negative) by chance by both raters is the product of the marginal probabilities p 0+ and p +0. Likewise, the probability of a subject being rated 1 (positive) by chance by both raters is the product of the marginal probabilities p 1+ and p +1. The sum of these two probabilities (p 1+*p +1 + p 0+*p +0) is the agreement by chance, that is, the source of inflation discussed earlier.After excluding this source of inflation from the total proportion of cases in which the two raters give identical ratings (p 11 + p 00), we arrive at the agreement corrected for chance agreement, (p 11+p 00 – (p 1+*p +1 + p 0+*p +0)). In 1960 Cohen [1] recommended normalizing this chance-adjusted agreement as the Kappa coefficient (K ):(1)This normalization process produces kappa coefficients that vary between −1 and 1, depending on the degree of agreement or disagreement beyond chance. If the two raters completely agree with each other, then p 11+p 00=1 and K =1. Conversely, if the kappa coefficient is 1, then the two raters agree completely. On the other hand, if the raters rate the subjects in a completely random fashion, then the agreement is completely due to chance, so p 11=p 1+*p +1 and p 00=p 0+*p +0 do (p 11+p 00 – (p 1+*p +1 + p 0+*p +0))=0 and the kappa coefficient is also 0. In general, when rater agreement exceeds chance agreement the kappa coefficient is positive, and when raters disagree more than they agree the kappa coefficient is negative. The magnitude of kappa indicates the degree of agreement or disagreement.The kappa coefficient can be estimated by substituting sample proportions for the probabilities shown in equation (1). When the number of ratings given by each rater (i.e., the sample size) is large, the kappa coefficient approximately follows a normal distribution. This asymptotic distribution can be estimated using delta methods based on the asymptotic distributions of the various sample proportions.[4] Based on the asymptotic distribution, calculations of confidence intervals and hypothesis tests can be performed. For a sample with 100 or more ratings, this generally provides a good approximation. However, it may not work well for small sample sizes, in which case exact methods may be applied to provide more accurate inference.[4]Example 1. Assessing the agreement between the diagnosis of depression based on information provided by the proband compared to the diagnosis based on information provided by other informants (Table 1), the Kappa coefficient is computed as follows:The asymptotic standard error of kappa is estimated as 0.063. This gives a 95% confidence interval of κ, (0.2026, 0.4497). The positive kappa indicates some degree of agreement about the diagnosis of depression between diagnoses based on information provided by the proband versus diagnoses based on information provided by other informants. However, the level of agreement, though statistically significant, is relatively weak.In most applications, there is usually more interest in the magnitude of kappa than in the statistical significance of kappa. When the sample is relatively large (as in this example), a low kappa which represents relatively weak agreement can, nevertheless, be statistically significant (that is, significantly greater than 0). The degree of beyond-chance agreement has been classified in different ways by different authors who arbitrarily assigned each category to specific cutoff levels of Kappa. For example, Landis and Koch [5] proposed that a kappa in the range of 0.21–0.40 be considered ‘fair’ agreement, kappa=0.41–0.60 be considered ‘moderate’ agreement, kappa=0.61–0.80 be considered ‘substantial’ agreement, and kappa >0.81 be considered ‘almost perfect’ agreement.4. Kappa for categorical variables with multiple levels The kappa coefficient for a binary rating scale can be generalized to cases in which there are more than two levels in the rating scale. Suppose there are k nominal categories in the rating scale. For simplicity and without loss of generality, denote the rating levels by 1,2,...,k . The ratings from the two raters can be summarized in a k ×k contingency table, as shown in Table 4. In the table, n ij , p ij , p i+, and p +j have the same interpretations as in the 2x2 contingency table (above) but the range of the scale is extended to i,j =1,…,k. As in the binary example, we first compute the agreement by chance, (the sum of the products of the k marginal probabilities, ∑ p i+*p +i for i =1,…,k ), and subtract this chance agreement from the total observed agreement (the sum of the diagonal probabilities, ∑ p ii for i =1,...,k ) before estimating the normalized agreement beyond chance:(2)11121k 1+2n 21n 22...n 2k n 2+..................k n k1n k2...n kk n k+totaln +1n +2...n +knAs in the case of binary scales, the kappa coefficient varies between −1 and 1, depending on the extent of agreement or disagreement. If the two raters completely agree with each other (∑ p ii =1, for i =1,…,k ), then the kappa coefficient is equal to 1. If the raters rate the subjects at random, then the total agreement is equal chance agreement (∑ p ii =∑ p i+*p +i , for i =1,…,k ) so thekappa coefficient is 0. In general, the kappa coefficient is positive if there is agreement or negative if there is disagreement, with the magnitude of kappa indicating the degree of such agreement or disagreement between the raters. The kappa index in equation (2) is estimated by replacing the probabilities with their corresponding sample proportions. As in the case of binary scales, we can use asymptotic theory and exact methods to assess confidence intervals and make inferences.5. Kappa for ordinal or ranked variablesThe definition of the kappa coefficient in equation (2) assumes that the rating categories are treated as independent categories. If, however, the rated categories are ordered or ranked (for example, a Likert scale with categories such as ‘strongly disagree’, ‘disagree’, ‘neutral’, ‘agree’, and ‘strongly agree’), then a weighted kappa coefficient is computed that takes into consideration the different levels of disagreement between categories. For example, if one rater ‘strongly disagrees’ and another ‘strongly agrees’ this must be considered a greater level of disagreement than when one rater ‘agrees’ and another ‘strongly agrees’.The first step in computing a weighted kappa is to assign weights representing the different levels of agreement for each cell in the KxK contingency table. The weights in the diagonal cells are all 1 (i.e., w ii =1, for all i ), and the weights in the off-diagonal cells range from 0 to <1 (i.e., 0<w ij <1, for all i ≠j ). These weights are then added to equation (2) to generate a weighted kappa that accounts for varying degrees of agreement or disagreement between the ranked categories:The weighted kappa is computed by replacing the probabilities with their respective sample proportions, p ij , p i+, and p +i . If w ij =0 for all i ≠j , the weighted kappa coefficient K w reduces to the standard kappa in equation (2). Note that for binary rating scales, there is no weighted version of kappa, since κ remains the same regardless of the weights used. Again, we can use asymptotic theory and exact methods to estimate confidence intervals and make inferences.In theory, any weights satisfying the two defining conditions (i.e., weights in diagonal cells=1 and weights in off-diagonal cells >0 and <1) may be used. In practice, however, additional constraints are often imposed to make the weights more interpretable and meaningful. For example, since the degree of disagreement (agreement) is often a function of the difference between the i th and j th rating categories, weights are typically set to reflect adjacency between rating categories, such as by w ij =f (i-j ), where f is some decreasing function satisfying three conditions: (a) 0<f (x )<1; (b) f (x )=f (-x ); and (c) f (0)=1. Based on these conditions, larger weights (i.e., closer to 1) are used forweights of pairs of categories that are closer to each other and smaller weights (i.e., closer to 0) are used for weights of pairs of categories that are more distant from each other.Two such weighting systems based on column scores are commonly employed. Suppose the column scores are ordered, say C 1≤C 2…≤C r and assigned values of 0,1,…r. Then, the Cicchetti–Allison weight and the Fleiss–Cohen weight in each cell of the KxK contingency table are computed as follows:Cicchetti-Allison weights: Fleiss-Cohen weights:Example 2. If depression is categorized into three ranked levels as shown in Table 5, the agreement of the classification based on information provided by the probands with the classification based on information provided by other informants can be estimated using the unweighted kappa coefficient as follows:Applying the Cicchetti-Allison weights (shown in Table 5) to the unweighted formula generates a weighed kappa:Applying the Fleiss-Cohen weights (shown in Table 5) involves replacing the 0.5 weight in the above equation with 0.75 and results in a K w of 0.4482. Thus the weighted kappa coefficients have larger absolute values than the unweighted kappa coefficients. The overall result indicates only fair to moderate agreement between the two methods of classifying the level of depression. As seen in Table 5, the low agreement is partly due to the fact that a large number of subjects classified as minor depression based on information from the proband were not identified using information from other informants.6. Statistical SoftwareSeveral statistical software packages including SAS, SPSS, and STATA can compute kappa coefficients. But agreement data conceptually result in square tables with entries in all cells, so most software packages will not compute kappa if the agreement table is non-square, which can occur if one or both raters do not use all the rating categories when rating subjects because ofbiases or small samples.In some special circumstances the software pack-ages will compute incorrect kappa coefficients if a square agreement table is generated despite the failure of both raters to use all rating categories. For example, suppose a scale for rater agreement has three categories, A, B, and C. If one rater only uses categories B and C, and the other only uses categories A and B, this could result in a square agreement table such as that shown in Table 6. This is a square table, but the rating categories in the rows are completely different from those represented by the column. Clearly, kappa values generated using this table would not provide the desired assessment of rater agreement. To deal with this problem the analyst must add zero counts for the rating categories not endorsed by the raters to create a square table with the right rating categories, as shown in Table 7.6.1 SASI n SAS, one may use PROC FREQ and specify thecorresponding two-way table with the “AGREE” option.B 51419total211637B 051419C 0000total211637Here are the sample codes for Example 2 using PROC FREQ:PROC FREQ DATA = (the data set for the depression diagnosis study);TABLE (variable on result using proband) * (variable on result using other informants)/ AGREE;RUN;PROC FREQ uses Cicchetti-Allison weights by default. One can specify (WT=FC) with the AGREE option to request weighted kappa coefficients based on Fleiss-Cohen weights. It is important to check the order of the levels and weights used in computing weighted kappa. SAS calculates weights for weighted kappa based on unformatted values; if the variable of interest is not coded this way, one can either recode the variable or use a format statement and sp ecify the “ORDER = FORMATTED” option. Also note that data for contingency tables are often recorded as aggregated data. For example, 10 subjects with the rating ‘A’ from the first rater and the rating ‘B’ from the second rater may be combined into one observation with a frequency variable of value 10. In such cases a weight statement “weight (the frequency variable);” may be applied to specify the frequency variable.6.2 SPSSIn SPSS, kappa coefficients can be only be computed when there are only two levels in the rating scale so it is not possible to compute weighted kappa coefficients. For a two-level rating scale such as that described in Example 1, one may use the following syntax to compute the kappa coefficient:CROSSTABS/TABLES=(variable on result using proband) BY (variable on result using other informants)/STATISTICS=KAPPA.An alternatively easier approach is to select appropriate options in the SPSS menu:1. Click on Analyze, then Descriptive Statistics, then Crosstabs.2. Choose the variables for the row and column variables in the pop-up window for the crosstab.3. Click on Statistics and select the kappa checkbox.4. Click Continue or OK to generate the output for the kappa coefficient.7. DiscussionIn this paper we introduced the use of Cohen’s kappa coefficient to assess between-rater agreement, which has the desirable property of correcting for chance agreement. We focused on cross-sectional studies for two raters, but extensions to longitudinal studies with missing values and to studies that use more than two raters are also available.[6] Cohen’s kappa generally works well, but in some specific situations it may not accurately reflect the true level of agreement between raters.[7]. For example, when both raters report a very high prevalence of the condition of interest (as in the hypothetical example shown in Table 2), some of the overlap in their diagnoses may reflect their common knowledge about the disease in the population being rated. This should be considered ‘true’ agreement, but it is attributed to chance agreement (i.e., kappa=0). Despite such limitations, the kappa coefficient is an informative measure of agreement in most circumstances that is widely used in clinical research.Cohen’s kappa can only be applied to categorical ratings. When ratings are on a continuous scale, Lin’s concordance correlation coefficient[8] is an appropriate measure of agreement between two raters,[8] and the intraclass correlation coefficients[9] is an appropriate measure of agreement between multiple raters.Conflict of interestThe authors declare no conflict of interest.FundingNone.概述:在精神卫生和社会心理学研究中,常常需要报告研究使用某一评估方法的评估者间的一致性。
Kappa分析

2015年5月27日晚,上海——潮流 界的重磅事件,众人翘首以待的联 名产品系列Kappa x CLOT Collaboration的发布活动在上海 1933老场坊展开。此次的合作在 双方彼此信任的前提下,围绕“潮 流兄弟会”这一主题,本着#信任 至上 的理念,共同打造出前所未 有的潮流联名产品。活动当天,包 括导演王岳伦、主持人孔令奇、摄 影师米原康正、DJ NOODLES等 潮流文化推手以及各行各业创意人 纷纷到场助阵,而CLOT主理人陈 冠希及潘世亨也有到场支持, Kappa和CLOT的共同好友MC Hotdog更是在After Party环节带来 了精彩的表演,以表示对Kappa x CLOT这次联名合作的支持。众嘉 宾与来自世界各地的媒体精英及潮 流人士一起,共同观看了灯光秀等 high爆全场的环节,见证了此次联 名佳作的震撼亮相。
稳固而创新
回顾国内电子商务市场近十年的发展历程,2007年可以说是一个“井喷式”的发 展时期,在这股浪潮中,Kappa也看到了中国电子商务市场的巨大潜能,在2009年决 定上线第一家线上专卖店。在当时而言,电商的市场还犹如一潭深不可测的井水,品 牌出于“探路”的心思选择了淘宝来作为试水的第一步。 在淘宝获得的成功,也更加坚定了Kappa品牌在电商领域中的继续前进,在更精 准地覆盖目标消费群体的电商平台选择中,国内知名名牌折扣网唯品会顺理成章地成 为了Kappa最为重要的合作伙伴之一。经过较长一段时间磨合,Kappa与唯品会建立 起了信任的关系,不仅展开独家网络合作,而且优惠力度也大。唯品会在11月1日推 出的Kappa男女鞋特卖专场中,男鞋2.5至3.8折以及女鞋1.8至3.6折的折扣优惠,再次 冲破了让利的最高点。而对于Kappa而言,能通过唯品会这样优质的电商平台推广品 牌的认可度,提升品牌形象就是“尝新”模式中的最大收获。
检验标准kappa

检验标准kappaKappa检验标准。
Kappa检验是一种用于评估医学诊断试验一致性的统计方法。
在医学领域,准确的诊断结果对于患者的治疗和预后至关重要。
因此,评估医学诊断试验的一致性是非常重要的。
Kappa检验可以帮助医生和研究人员评估医学诊断试验的一致性,从而提高诊断的准确性和可靠性。
Kappa检验是通过比较观察者之间的一致性来评估医学诊断试验的结果。
在医学研究中,通常会有多个观察者对同一组样本进行评估,他们可能会有不同的观点和判断。
Kappa检验可以帮助我们确定这些观察者之间的一致性程度,从而评估医学诊断试验的可靠性。
Kappa检验的结果通常是一个介于-1和1之间的数值。
当Kappa值接近1时,表示观察者之间的一致性非常高,说明医学诊断试验的结果非常可靠。
而当Kappa 值接近-1时,表示观察者之间的一致性非常低,说明医学诊断试验的结果不可靠。
当Kappa值接近0时,表示观察者之间的一致性与随机一致性相当,说明医学诊断试验的结果具有一定的随机性。
Kappa检验的结果可以帮助医生和研究人员判断医学诊断试验的可靠性,从而决定是否需要进一步改进诊断方法或者加强观察者的培训。
通过Kappa检验,我们可以及时发现医学诊断试验中存在的问题,并采取相应的措施,从而提高诊断的准确性和可靠性。
除了用于评估医学诊断试验的一致性外,Kappa检验还可以用于评估其他类型的观察者之间的一致性,比如评估医学影像的解读、评估疾病的诊断和分型等。
因此,Kappa检验在医学研究和临床实践中具有非常重要的意义。
总之,Kappa检验是一种用于评估医学诊断试验一致性的重要方法。
通过Kappa检验,我们可以及时发现医学诊断试验中存在的问题,提高诊断的准确性和可靠性。
因此,在医学研究和临床实践中,我们应该充分利用Kappa检验,从而提高医学诊断的水平,为患者的治疗和预后提供更好的支持。
Kappa系数

多分类测量结果的一致性检验
审核医生判定 无效 0 20 39 59
合计 109 264 45 418
转换成SPSS待分析样式
步骤: 创建三个变量,执行医生(1-显效、 2-有效、3-无效),审核医生(1-显 效、2-有效、3-无效)和例数
Kappa计算之SPSS实现 步骤略
多分类测量结果的一致性检验
Kappa值一致性评价
评价分类结果一致性和信度的一种重要指标……
概念
Kappa值记作κ 是评价分类结果一致性和信度的一种重要指标
公式
两次观察的一致性 两次观察的机遇一致性
Kappa值的实质是实际一致性与非机遇一致性之比
Kappa取值范围
Kappa值的取值范围是 |κ |≤1
1
表3 两次测定的一致性情况
审核医生判定 显效 105 24 有效 4 220 无效 0 20 执行医生判定 显效 有效 合计 109 264
无效
合计
0
129
6
230
39
59
45
418
计算 结果
两名医生判定结果有较 高度的一致性
Kappa计算之SPSS实现
执行医生判定 显效 有效 无效 合计 显效 105 24 0 129 有效 4 220 6 230
本例结果
Kappa值
甲乙两名医生诊断有较 高度的一致性
Kappa计算之SPSS实现
二分类测量结果的一致性检验
甲医生 +
乙医生 + 26(a) 6(b)
合计 32(a+b)
合计
4(c)
30(a+c)
28(d)
34(b+d)
Kappa值
➢ 分析结论:根据推荐的判断准则得出所有的评价人之间 一致性好。
9
进一步分析--评价人与基准判断交叉法
对评价人A/B/C 与基准判断的比较 1)A与基准比较 P(A0)=50 P(A1)=100 P( J0)=48 P( J1)=102
P(A0J0)×150=(50/150)×(48/150)×150=16 P(A1J1)×150 =(100/150)×(102/150)×150 =68 P(A0J1)×150 =(50/150)×(102/150)×150 =34 P(A1J0)×150 =(100/150)×(48/150)×150 =32
评价人A与评价人C交叉表
0.00 计算
期望值的计算
A 1.00
计算
期望值的计算
总计
计算 期望值的计算
C
0.00
1.00
43
7
17.0
33.0
8
92
34.0
66.0
51
99
51.0
99.0
总计
50 50.0 100 100.0 150 150.0
7
计算A与C的Kappa值
对角线单元观测值总和 P0=(43+99)/150=0.9(A与C判断一致 的概率) 对角线单元期望值总和 Pe=(17+66)/150=0.55 代入公式:
2)计算B与C的K值 P(B0)=47/150 P(C0)=51/150 P(B1)=103/150 P(C1)=99/150
P(B0C0)×150=(47/150)×(51/150)×150=16 P(B1C1) ×150 =(103/150)×(99/150)×150 =68 P(B0C1)×150 =(47/150)×(99/150)×150 =31.02 P(B1C0)×150 =(103/150)×(51/150)×150 =35.02
KAPPA点滴

我们怎样才能知道, 我们怎样才能知道,自己生产出的零件 是否合格?那就一定要经过检测,当你 是否合格?那就一定要经过检测, 所生产的零件被检测时, 所生产的零件被检测时,你一定希望检 测的结果是公平的, 测的结果是公平的,即通过相应量具检 测出的结果是正确的, 测出的结果是正确的,能真正反映你的 加工水平。 加工水平。 那么,现在请回答, 那么,现在请回答,哪些因素会影响 检测结果……… 检测结果
什么ቤተ መጻሕፍቲ ባይዱ Kappa?
Pobserved − Pchance K= 1 − Pchance P observed
判定员一致判定产品为良与不良的比率=判定员一致 判定为良品的比率+判定员一致判定为不良的比率
P chance
预期偶然达成一致的比率=(判定员A判定为优良的比 率*判定员B判定为优良的比率)+(判定员A判定为不 良的比率*判定员B判定为不良的比率) 注意: 上述等式适用于两类分析,即良或不良
属性测量系统指导
如果你的类别超过2种,其中一类是良品, 其它类别是不同的缺陷不良品,那么你 至少应该选择大约50%的良品和和每种 缺陷至少占10%的不良品 这些分类应该互相排斥,否则它们应该 合并起来
分级员内部/可重复性考虑
让每个检查员至少两次判定同一单元 为每个检查员建立独立的Kappa表,计算他们的 Kappa值
首先, 要有合适的量具, 举例说明, 首先, 要有合适的量具, 举例说明,我们要准确的测量一张 铁的厚度, 要选择千分尺, 而不是格尺; 铁的厚度, 要选择千分尺, 而不是格尺; 要有合适和统一的测量方法,即在测量之前,要先规定怎么测 要有合适和统一的测量方法,即在测量之前, 而且保证大家均采用统一的方法测量; 量,而且保证大家均采用统一的方法测量; 要有大家公认的检测员,他有能力反映真实的测量结果; 要有大家公认的检测员,他有能力反映真实的测量结果; 如果你所生产的部件,经过如上的检测,你是否觉得公平, 如果你所生产的部件,经过如上的检测,你是否觉得公平,放心 满意
《致性检验kappa》课件

分类标准要明确且稳定
kappa值是基于分类标准进行计算的,因此 分类标准的明确性和稳定性对kappa值的结 果有重要影响。
在实际应用中,需要提前制定明确的分类标 准,并确保分类标准在试验过程中保持一致
Scott's Pi
总结词
Scott's Pi用于衡量多个评价者对同一组数 据的一致性程度。
详细描述
Scott's Pi的计算公式为:(pi = frac{P_o}{P_o + P_e}),其中(P_o)是实际 一致的观察频数,(P_e)是期望一致的频数 ,但每个评价者的期望一致频数不同。
03
kappa值的应用场景
自然语言处理
文本分类
在自然语言处理中,kappa值可用于评估文本分类算法 的性能。通过比较算法分类出的文本和实际文本的类别 ,可以计算出kappa值,从而了解分类结果的准确性和 一致性。
信息抽取
在信息抽取任务中,kappa值可用于评估实体识别和关 系抽取的性能。通过比较算法抽取出的实体和关系与实 际实体和关系的相似度,可以计算出kappa值,从而了 解抽取结果的准确性和一致性。
详细描述
F1分数是准确率和召回率的调和平均数,它综合考虑了模型的精度和召回率。而kappa值则更注重类别间的平衡 和差异性,通过计算实际分类与预测分类之间的差异来评估模型的性能。与F1分数相比,kappa值在处理类别不 平衡问题时更具优势。
06
kappa值在实际应用中 的注意事项
样本量要足够大
样本量的大小会影响kappa值的稳定性,因此在实际应用中需要保证足够的样本量。样本量过小可能导致kappa值不稳定, 从而影响结果的可靠性。
Kappa值

分析结论:根据推荐的判断准那么得出所有的评价 9
进一步分析--评价人与基准判断穿插法
对评价人A/B/C 与基准判断的比较 1〕A与基准比较 P(A0)=50 P(A1)=100 P( J0)=48 P( J1)=102
P(A0J0)×150=〔50/150〕×〔48/150〕×150=16 P(A1J1)×150 =〔100/150〕×〔102/150〕×150 =68 P(A0J1)×150 =〔50/150〕×〔102/150〕×150 =34 P(A1J0)×150 =〔100/150〕×〔48/150〕×150 =32
1
1
0
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
0
0
0
1
1
1
1
1
1
1
0
0
0
评价人B
B-1 B-2 B-3
1
1
1
1
1
1
0
0
0
0
0
0
0
0
0
1
1
0
1
1
1
1
1
1
0
0
0
1
1
1
1
1
1
0
0
0
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Kappa系数:一种衡量评估者间一致性的常用方法
Kappa系数:一种衡量评估者间一致性的常用方法Biostatistics in psychiatry (25)?Kappa coefficient: a popular measure of rater agreementWan TANG 1*, Jun HU 2, Hui ZHANG 3, Pan WU 4, Hua HE 1,51 Department of Biostatistics and Computational Biology, University of Rochester, Rochester, NY , United States 2College of Basic Science and Information Engineering, Yunnan Agricultural University, Kunming, Yunnan Province, China 3Department of Biostatistics, St. Ju de Children’s Research Hospital, Memphis, TN, United States 4Value Institute, Christiana Care Health System, Newark, DE, United States 5Center of Excellence for Suicide Prevention, Canandaigua VA Medical Center Canandaigua, NY , United States *correspondence:***********************.eduA full-text Chinese translation of this article will be available at /cn on March 25, 2015.Summary: In mental health and psychosocial studies it is often necessary to report on the between-rater agreement of measures used in the study. This paper discusses the concept of agreement, highlighting its fundamental difference from correlation. Several examples demonstrate how to compute the kappa coefficient – a popular statistic for measuring agreement – both by hand and by using statistical software packages such as SAS and SPSS. Real study data are used to illustrate how to use and interpret this coefficient in clinical research and practice. Thearticle concludes with a discussion of the limitations of the coefficient. Keywords: interrater agreement; kappa coefficient; weighted kappa; correlation [Shanghai Arch Psychiatry . 2015; 27(1): 62-67. doi: 10.11919/j.issn.1002-0829.215010]1. IntroductionFor most physical illnesses such as high blood pressure and tuberculosis, definitive diagnoses can be made using medical devices such as a sphygmomanometer for blood pressure or an X-ray for tuberculosis. However, there are no error-free gold standard physical indicators of mental disorders, so the diagnosis and severity of mental disorders typically depends on the use of instruments (questionnaires) that attempt to measure latent multi-faceted constructs. For example, psychiatric diagnoses are often based on criteria specified in the Fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV)[1], published by the American Psychiatric Association. But different clinicians may have different opinions about the presence or absence of the specific symptoms required to determine the presence of a diagnosis, so there is typically no perfect agreement between evaluators. In this situation, statistical methods are needed to address variability in clinicians’ ratings.Cohen’s kappa is a widely used index for assessing agreement between raters.[2] Although similar in appearance, agreement is a fundamentally different concept from correlation. To illustrate, consider an instrument with six items and suppose that two raters’ ratings of the six items on a single subject are (3,5), (4,6), (5,7), (6,8), (7,9) and (8,10). Although the scores of the two raters are quite different, the Pearson correlationcoefficient for the two scores is 1, indicating perfectcorrelation. The paradox occurs because there is a bias in the scoring that results in a consistent difference of 2 points in the scores of the two raters for all 6 items in the instrument. Thus, although perfectly correlated (precision), there is quite poor agreement between the two raters. The kappa index, the most popular measure of rate rs’ agreement, resolves this problem by assessing both the bias and the precision between raters’ ratings.In addition to its applications to psychiatric diagnosis, the concept of agreement is also widely applied to assess the utility of diagnostic and screening tests. Diagnostic tests provide information about a patient’s condition that clinicians’ often use when making decisions about the management of patients. Early detection of disease or of important changes in the clinical status of patients often leads to less suffering and quicker recovery, but false negative and false positive screening results can result in delayed treatment or in inappropriate treatment. Thus when a new diagnostic or screening test is developed, it is critical to assess its accuracy by comparing test results with those from a gold or reference standard. When assessing such tests, it is incorrect to measure the correlation of the results of the test and the gold standard, the correct procedure is to assess the agreement of the test results with the gold standard.2. ProblemsConsider an instrument with a binary outcome, with ‘1’ representing the presence of depression and ‘0’ representing the absence of depression. Suppose two independent raters apply the instrument to a random sample of n subjects. Let and denote the ratings on the n subjects by the two raters for i =1,2,...,n . We are interested in the degree of agreement between the two raters. Since the ratings are on the same scale of two levels for both raters, the data can be summarized in a 2×2 contingency table.To illustrate, Table 1 shows the results of a study assessing the prevalence of depression among 200 patients treated in a primary care setting using two methods to determine the presence of depression;[3] one based on information provided by the individual (i.e., proband) and the other based on information provided by another informant (e.g., the subject’s family member or close friend) about the proband. Intuitively, we may think that the proportion of cases in which the two ratings are the same (in this example, 34.5% [(19+50)/200]) would be a reasonable measure of agreement. But the problem with this proportion is that it is almost always positive, even when the rating by the two methods is completely random and independent of each other. So the proportion of overall agreement does not indicate whether or not two raters or two methods of rating are in agreement.by chance. This chance agreement must be removed in order to provide a valid measure of agreement. Coh en’s kappa coefficient is used to assess the level ofagreement beyond chance agreement.depressed 5065115total11684200For example, suppose that two raters with no training or experience about depression randomly decide whether or not each of the 200 patients has depression. Assume that one rater makes a positive diagnosis (i.e., considers depression present) 80% of the time and the other gives a positive diagnosis 90% of the time. Based on the assumption that their diagnoses are made independently from each other, Table 2 represents the joint distribution of their ratings. The proportion that the two raters give the same diagnosis is 74% (i.e., 0.72+0.02), suggesting that the two raters are doing a good job of diagnosing the presence of depression. But this level of agreement is purely by chance, it does not reflect the actual degree of agreement between the two raters. This hypothetical example shows that the proportion of cases in which two raters give the sameratings on an instrument is inflated by the agreementnegative 0.180.02 0.20total0.900.101.003. Kappa for 2×2 tablesConsider a hypothetical example of two raters giving ratings for n subjects on a binary scale, with ‘1’ representing a positive result (e.g., the presence of a diagnosis) a nd ‘0’ representing a negative result (e.g., the absence of a diagnosis). The results could be reported in a 2x2 contingency table as shown in Table 3. By convention, the results of the first rater are traditionally shown in the rows (x values) and the results of the second rater are shown in the columns (y values). Thus, n ij in the table denotes the number of subjects who receive the rating of i from the first rater and the rating j from the second rater. Let Pr(A) denote the probability of event A; then p ij =Pr(x=i,y=j) represent the proportion of all cases that receive the rating of i from the first rater and the rating j from the second rater, p i+=Pr(x=i) represents the marginal distribution of the first rater’s ratings, and p +j =Pr(y=j) represents themarginal distribution of the second rater’s ratings.11101+0 (negative)n 01n 00n 0+totaln +1n +0nIf the two raters give their ratings independently according to their marginal distributions, the probability that a subject is rated 0 (negative) by chance by both raters is the product of the marginal probabilities p 0+ and p +0. Likewise, the probability of a subject being rated 1 (positive) by chance by both raters is theproduct of the marginal probabilities p 1+ and p +1. The sum of these two probabilities (p 1+*p +1 + p 0+*p +0) is the agreement by chance, that is, the source of inflation discussed earlier.After excluding this source of inflation from the total proportion of cases in which the two raters give identical ratings (p 11 + p 00), we arrive at the agreement corrected for chance agreement, (p 11+p 00 –(p 1+*p +1 + p 0+*p +0)). In 1960 Cohen [1] recommended normalizing this chance-adjusted agreement as the Kappa coefficient (K ):(1)This normalization process produces kappa coefficients that vary between ?1 and 1, depending on the degree of agreement or disagreement beyond chance. If the two raters completely agree with each other, then p 11+p 00=1 and K =1. Conversely, if the kappa coefficient is 1, then the two raters agree completely. On the other hand, if the raters rate the subjects in a completely random fashion, then the agreement is completely due to chance, so p 11=p 1+*p +1 and p 00=p 0+*p +0 do (p 11+p 00 – (p 1+*p +1 + p 0+*p +0))=0 and the kappa coefficient is also 0. In general, when rater agreement exceeds chance agreement the kappa coefficient is positive, and when raters disagree more than they agree the kappa coefficient is negative. The magnitude of kappa indicates the degree of agreement or disagreement.The kappa coefficient can be estimated by substituting sample proportions for the probabilities shown in equation (1). When the number of ratings given by each rater (i.e., the samplesize) is large, the kappa coefficient approximately follows a normal distribution. This asymptotic distribution can be estimated using delta methods based on the asymptotic distributions of the various sample proportions.[4] Based on the asymptotic distribution, calculations of confidence intervals and hypothesis tests can be performed. For a sample with 100 or more ratings, this generally provides a good approximation. However, it may not work well for small sample sizes, in which case exact methods may be applied to provide more accurate inference.[4]Example 1. Assessing the agreement between the diagnosis of depression based on information provided by the proband compared to the diagnosis based on information provided by other informants (Table 1), the Kappa coefficient is computed as follows:The asymptotic standard error of kappa is estimated as 0.063. This gives a 95% confidence interval of κ, (0.2026, 0.4497). The positive kappa indicates some degree of agreement about the diagnosis of depression between diagnoses based on information provided by the proband versus diagnoses based on information provided by other informants. However, the level of agreement, though statistically significant, is relatively weak.In most applications, there is usually more interest in the magnitude of kappa than in the statistical significance of kappa. When the sample is relatively large (as in this example), a low kappa which represents relatively weak agreement can, nevertheless, be statistically significant (that is, significantly greater than 0). The degree of beyond-chance agreement has been classified in different ways by different authors who arbitrarily assigned each category to specific cutoff levels of Kappa. For example, Landis and Koch [5] proposed that a kappa in the range of 0.21–0.40 be considered ‘fair’ agreement, kappa=0.41–0.60 be c onsidered ‘moderate’ agreement, kappa=0.61–0.80 be considered ‘substantial’ agreement, and kappa >0.81 be considered ‘almost perfect’ agreement.4. Kappa for categorical variables with multiple levels The kappa coefficient for a binary rating scale can be generalized to cases in which there are more than two levels in the rating scale. Suppose there are k nominal categories in the rating scale. For simplicity and without loss of generality, denote the rating levels by 1,2,...,k . The ratings from the two raters can be summarized in a k ×k contingency table, as shown in Table 4. In the table, n ij , p ij , p i+, and p +j have the same interpretations as in the 2x2 contingency table (above) but the range of the scale is extended to i,j =1,…,k. As in the binary example, we first compute the agreement by chance, (the sum of the products of the k marginal probabilities, ∑ p i+*p +i for i =1,…,k ), and subtract this chance agreement from the total observed agreement (the sum of the diagonal probabilities, ∑ p ii fo r i =1,...,k ) before estimating the normalized agreement beyond chance:(2)11121k 1+2n 21n 22...n 2k n 2+..................k n k1n k2...n kk nk+totaln +1n +2...n +knAs in the case of binary scales, the kappa coefficient varies between ?1 and 1, depending on the extent of agreement or disagreement. If the two raters completely agree with each other (∑ p ii =1, for i =1,…,k ), then the kappa coefficient is equal to 1. If the raters rate the subjects at random, then the total agreement is equal chance agreement (∑ p ii =∑ p i+*p +i , for i =1,…,k ) so thekappa coefficient is 0. In general, the kappa coefficient is positive if there is agreement or negative if there is disagreement, with the magnitude of kappa indicating the degree of such agreement or disagreement between the raters. The kappa index in equation (2) is estimated by replacing the probabilities with their corresponding sample proportions. As in the case of binary scales, we can use asymptotic theory and exact methods to assess confidence intervals and make inferences.5. Kappa for ordinal or ranked variablesThe definition of the kappa coefficient in equation (2) assumes that the rating categories are treated as independent categories. If, however, the rated categories are ordered or ranked (for example, a Likert scale with categories such as ‘strongly disagree’, ‘disagree’, ‘neutral’, ‘agree’, and ‘strongly agree’), then a weighted kappa coefficient is computed that takes into consideration the different levels of disagreement between categories. For example, if one rater‘strongly disagrees’ and another ‘strongly agrees’ this must be considered a greater level of disagreement than when one rater ‘agrees’ and another ‘strongly agrees’.The first step in computing a weighted kappa is to assign weights representing the different levels of agreement for each cell in the KxK contingency table. The weights in the diagonal cells are all 1 (i.e., w ii =1, for all i ), and the weights in the off-diagonal cells range from 0 to <1 (i.e., 0<="" degrees="" disagreement="" equation="" for="" generate="" i="" ij="" kappa="" of="" or="" p="" ranked="" that="" the="" then="" these="" to="" varying="" weighted="" weights="" ≠j=""> The weighted kappa is computed by replacing the probabilities with their respective sample proportions, p ij , p i+, and p +i . If w ij =0 for all i ≠j , the weighted kappa coefficient K w reduces to the standard kappa in equation (2). Note that for binary rating scales, there is no weighted version of kappa, since κ remains the same regardless of the weights used. Again, we can use asymptotic theory and exact methods to estimate confidence intervals and make inferences.In theory, any weights satisfying the two defining conditions (i.e., weights in diagonal cells=1 and weights in off-diagonal cells >0 and <1) may be used. In practice, however, additional constraints are often imposed to make the weights more interpretable and meaningful. For example, since the degree of disagreement (agreement) is often a function of the difference between the i th and j th rating categories, weights are typically set to reflect adjacency between rating categories, such as by w ij =f (i-j ), where f is some decreasing function satisfying three conditions: (a) 0<="" larger="" on="" p="" these="" to="" used="" weights="">weights of pairs of categories that are closer to each other and smaller weights (i.e., closer to 0) are used for weights of pairs of categories that are more distant from each other.Two such weighting systems based on column scores are commonly employed. Suppose the column scores are ordered, say C 1≤C 2…≤C r and assigned values of 0,1,…r. Then, the Cicchetti–Allison weight and the Fleiss–Cohen weight in each cell of the KxK contingency table are computed as follows: Cicchetti-Allison weights: Fleiss-Cohen weights:Example 2. If depression is categorized into three ranked levels as shown in Table 5, the agreement of the classification based on information provided by the probands with the classification based on information provided by other informants can be estimated using the unweighted kappa coefficient as follows:Applying the Cicchetti-Allison weights (shown in Table 5) to the unweighted formula generates a weighed kappa: Applying the Fleiss-Cohen weights (shown in Table 5) involves replacing the 0.5 weight in the above equation with 0.75 and results in a K w of 0.4482. Thus the weighted kappa coefficients have larger absolute values than the unweighted kappa coefficients. The overall result indicates only fair to moderate agreement between the two methods of classifying the level of depression. As seen in Table 5, the low agreement is partly due to the fact that a large number of subjects classified as minor depression based on information from the proband were not identified using information from other informants.6. Statistical SoftwareSeveral statistical software packages including SAS, SPSS, and STATA can compute kappa coefficients. But agreement dataconceptually result in square tables with entries in all cells, so most software packages will not compute kappa if the agreement table is non-square, which can occur if one or both raters do not use all the rating categories when rating subjects because ofbiases or small samples.In some special circumstances the software pack-ages will compute incorrect kappa coefficients if a square agreement table is generated despite the failure of both raters to use all rating categories. For example, suppose a scale for rater agreement has three categories, A, B, and C. If one rater only uses categories B and C, and the other only uses categories A and B, this could result in a square agreement table such as that shown in Table 6. This is a square table, but the rating categories in the rows are completely different from those represented by the column. Clearly, kappa values generated using this table would not provide the desired assessment of rater agreement. To deal with this problem the analyst must add zero counts for the rating categories not endorsed by the raters to create a square tablewith the right rating categories, as shown in Table 7.6.1 SASI n SAS, one may use PROC FREQ and specify thecorresponding two-way table with the “AGREE” option.B 51419total211637B 051419C 0000total211637Here are the sample codes for Example 2 using PROC FREQ:PROC FREQ DATA = (the data set for the depression diagnosis study);TABLE (variable on result using proband) * (variable on result using other informants)/ AGREE;RUN;PROC FREQ uses Cicchetti-Allison weights by default. One can specify (WT=FC) with the AGREE option to request weighted kappa coefficients based on Fleiss-Cohen weights. It is important to check the order of the levels and weights used in computing weighted kappa. SAS calculates weights for weighted kappa based on unformatted values; if the variable of interest is not coded this way, one can either recode the variable or use a format statement and sp ecify the “ORDER = FORMATTED” option. Also note that data for contingency tables are often recorded as aggreg ated data. For example, 10 subjects with the rating ‘A’ from the first rater and the rating ‘B’ from the second rater may be combined into one observation with a frequency variable of value 10. In such cases a weight statement “weight (the frequency variab le);” may be applied to specify the frequency variable.6.2 SPSSIn SPSS, kappa coefficients can be only be computed when there are only two levels in the rating scale so it is not possible to compute weighted kappa coefficients. For a two-level rating scale such as that described in Example 1, one may use the following syntax to compute the kappa coefficient:CROSSTABS/TABLES=(variable on result using proband) BY (variable on result using other informants)/STATISTICS=KAPPA.An alternatively easier approach is to select appropriate options in the SPSS menu:1. Click on Analyze, then Descriptive Statistics, then Crosstabs.2. Choose the variables for the row and column variables in the pop-up window for the crosstab.3. Click on Statistics and select the kappa checkbox.4. Click Continue or OK to generate the output for the kappa coefficient.7. DiscussionIn this paper we introduced the use of Cohen’s kappa coefficient to assess between-rater agreement, which has the desirable property of correcting for chance agreement. We focused on cross-sectional studies for two raters, but extensions to longitudinal studies with missing values and to studies that use more than two raters are also available.[6] Cohen’s kappa generally works well, but in some specific situations it may not accurately reflect the true level of agreement between raters.[7]. For example, when both raters report a very high prevalence of the condition of interest (as in the hypothetical example shown in Table 2), some of the overlap in their diagnoses may reflect their common knowledge about the disease in the population being rated. This should be considered ‘true’ agreement, but it is attributed to chance agreement (i.e., kappa=0). Despite such limitations, the kappa coefficient is an informative measure of agreement in most circumstances that is widely used in clinical research.Cohen’s kappa can only be applied to categorical ratings. When ratings are on a continuous scale, Lin’s concordance correlation coefficient[8] is an appropriate measure of agreement between two raters,[8] and the intraclass correlation coefficients[9] is an appropriate measure of agreement between multiple raters.Conflict of interestThe authors declare no conflict of interest.FundingNone.概述:在精神卫生和社会心理学研究中,常常需要报告研究使用某一评估方法的评估者间的一致性。
kappa统计值与分类精度的对应关系(举例说明)
遥感图像分类的精度评价精度评价是指比较实地数据与分类结果,以确定分类过程的准确程度。
分类结果精度评价是进行土地覆被/利用遥感监测中重要的一步,也是分类结果是否可信的一种度量。
最常用的精度评价方法是误差矩阵或混淆矩阵(Error Matrix )方法(Congalton ,1991;Richards ,1996;Stehman ,1997),从误差矩阵可以计算出各种精度统计值,如总体正确率、使用者正确率、生产者正确率(Story 等,1986),Kappa 系数等。
误差矩阵是一个n ×n 矩阵(n 为分类数),用来简单比较参照点和分类点。
一般矩阵的行代表分类点,列代表参照点,对角线部分指某类型与验证类型完全一致的样点个数,对角线为经验证后正确的样点个数(Stehman ,1997)。
对分类图像的每一个像素进行检测是不现实的,需要选择一组参照像素,参照像素必须随机选择。
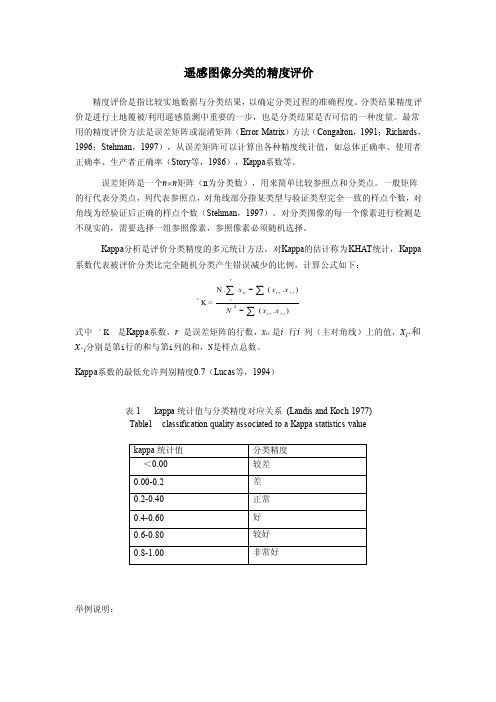
Kappa 分析是评价分类精度的多元统计方法,对Kappa 的估计称为KHAT 统计,Kappa系数代表被评价分类比完全随机分类产生错误减少的比例,计算公式如下:2N.(.)K =(.)rii i i ii i x x x Nx x ++∧++--∑∑∑式中 K ∧ 是Kappa 系数,r 是误差矩阵的行数,x ii 是i 行i 列(主对角线)上的值,x i +和x +i 分别是第i 行的和与第i 列的和,N 是样点总数。
Kappa 系数的最低允许判别精度0.7(Lucas 等,1994)表1 kappa 统计值与分类精度对应关系 (Landis and Koch 1977) Table1 classification quality associated to a Kappa statistics value举例说明:。
kappa值
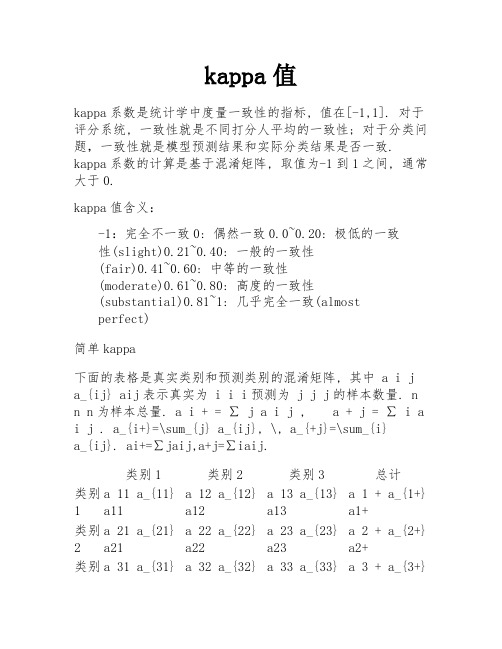
kappa值kappa系数是统计学中度量一致性的指标, 值在[-1,1]. 对于评分系统, 一致性就是不同打分人平均的一致性; 对于分类问题,一致性就是模型预测结果和实际分类结果是否一致. kappa系数的计算是基于混淆矩阵, 取值为-1到1之间, 通常大于0.kappa值含义:-1:完全不一致0: 偶然一致0.0~0.20: 极低的一致性(slight)0.21~0.40: 一般的一致性(fair)0.41~0.60: 中等的一致性(moderate)0.61~0.80: 高度的一致性(substantial)0.81~1: 几乎完全一致(almostperfect)简单kappa下面的表格是真实类别和预测类别的混淆矩阵, 其中 a i j a_{ij} aij表示真实为 i i i预测为 j j j的样本数量. n n n为样本总量. a i + = ∑ j a i j , a + j = ∑ i a i j . a_{i+}=\sum_{j} a_{ij}, \, a_{+j}=\sum_{i}a_{ij}. ai+=∑jaij,a+j=∑iaij.类别1类别2类别3总计类别1a 11 a_{11}a11a 12 a_{12}a12a 13 a_{13}a13a 1 + a_{1+}a1+类别2a 21 a_{21}a21a 22 a_{22}a22a 23 a_{23}a23a 2 + a_{2+}a2+类别a 31 a_{31} a 32 a_{32} a 33 a_{33} a 3 + a_{3+}类别1类别2类别3总计3a31a32a33a3+总计a + 1 a_{+1}a+1a + 2 a_{+2}a+2a + 3 a_{+3}a+3n n nkappa系数的数学表达: k = p o − p e 1 − p ek=\frac{p_o-p_e}{1-p_e} k=1−pepo−pe其中, p o p_o po为预测的准确率, 也可理解为预测的一致性, p o = ∑ i = 1 3 a i i n p_o=\frac{\sum_{i=1}^{3} a_{ii} } {n} po=n∑i=13aii. p e p_e pe表示偶然一致性, p e = ∑ i = 1 3 a i + ∗ a + i n 2p_e=\frac{\sum_{i=1}^{3} a_{i+}*a_{+i} } {n^2} pe=n2∑i=13ai+∗a+i.其实, 本人以为同用频(概)率来表示, 形式更加简洁.记 p i j = a i j / n p_{ij}=a_{ij}/ n pij=aij/n, p i + = a i + / n p_{i+}=a_{i+}/ n pi+=ai+/n, p + j = a + j / n p_{+j}=a_{+j} / n p+j=a+j/n, 则kappa系数为p o = ∑ i = 1 3 a i i n = ∑ i = 1 3 p i i , p_o=\frac{\sum_{i=1}^{3} a_{ii} }{n}=\sum_{i=1}^{3} p_{ii}, po=n∑i=13aii=i=1∑3pii, p e = ∑ i = 1 3 a i + ∗ a + i n 2 = ∑ i = 1 3 p i + ∗ p + i . p_e=\frac{\sum_{i=1}^{3} a_{i+}*a_{+i} } {n^2}=\sum_{i=1}^{3} p_{i+}*p_{+i}. pe=n2∑i=13ai+∗a+i=i=1∑3pi+∗p+i.kappa值 2对于一些有序关系的级别得分, 使用上面简单的计算方法存在一些问题. 比如在疾病预判时, 假设病人是无病的, 一个医生预测为得病且特别严重, 另一个医生预测为得病且中度. 很明显, 第一个医生的预测结果更加不可接受. 所以, 我们要在计算kappa值时加入权重的概念, 以区分这种预测结果的后果程度.设有 m m m个类别, 记 w i j w_{ij} wij表示真实为 i i i预测为 j j j的权重. 加权kappa的数学计算公式为 k = p o − p e 1 − p e = ∑ i = 1 m ∑ j = 1 m w i j p ij − ∑ i = 1 m ∑ j = 1 m w i j p i + p + j 1 − ∑ i = 1 m ∑ j = 1 m w i j p i + p + j k=\frac{p_o-p_e}{1-p_e}=\frac{ \sum_{i=1}^{m} \sum_{j=1}^{m} w_{ij}p_{ij} - \sum_{i=1}^{m} \sum_{j=1}^{m} w_{ij}p_{i+} p_{+j} } { 1- \sum_{i=1}^{m} \sum_{j=1}^{m} w_{ij}p_{i+}p_{+j} } k=1−pepo−pe=1−∑i=1m∑j=1mwijpi+p+j∑i=1m∑j=1mwijpij−∑i=1m∑j=1mwijpi+p+j一般地, w i i = 1w_{ii}=1 wii=1. 若当 i , j i,j i,j不同时, w i j = 0w_{ij}=0 wij=0, 就退化为上面简单的kappa.下面介绍几种常用的权重计算方法:设得分有序为 c 0 < c 1 < ⋯ < c m − 1 c_0<c_1<\cdots< c_{m-1} c0<c1<⋯<cm−1, 取值为 c i = i c_i=i ci=i.•线性权重 w i j = 1 − ∣ i − j ∣ m − 1 ,w_{ij}=1-\frac{|i-j|}{m-1}, wij=1−m−1∣i−j∣,•二次权重 w i j = 1 − ( i − j m − 1 ) 2 .w_{ij}=1-(\frac{i-j}{m-1})^2. wij=1−(m−1i−j)2.参考文献[1] dandelion的博客一致性检验– kappa 系数[2] 唐万,胡俊,张晖,吴攀,贺华.kappa系数:一种衡量评估者间一致性的常用方法[j].上海精神医学,2015,27(01):62-67.。
科恩卡帕系数

科恩卡帕系数
科恩卡帕系数是一种用于测量两个分类者一致性的统计方法。
该系数
可用于评估医生、研究员、教育者、调查员等分类者在对同一事物进
行分类时的一致性。
科恩卡帕系数在研究中具有广泛的应用,例如在
医疗诊断、心理测量、教育评估和市场调研等领域得到了广泛的应用。
科恩卡帕系数可用以下公式计算:
$$ \kappa =\frac{P(A)-P(E)}{1-P(E)} $$
其中,$P(A)$ 表示分类者之间的实际协议率,$P(E)$ 是预期协议率。
预期协议率的计算方式取决于所使用的测量方法。
科恩卡帕系数的取
值范围为 -1 到 1,其解释如下:
- $\kappa=1$:完全一致,分类者完全一致。
- $\kappa=0$:随机一致,分类者与随机选择的一致程度相同。
- $\kappa=-1$:完全不一致,分类者完全不一致。
科恩卡帕系数的优点在于可以对两个分类者的一致性进行评估,不考
虑分类者是否正确。
因此,该系数可以帮助评估分类者的一致性程度,而不仅仅是准确性。
此外,该系数还可以用于比较两种不同的分类方
法。
然而,科恩卡帕系数也有其局限性。
例如,该系数可能过于敏感,因为它代表实际和理论的差异。
此外,在样本容量较小或分类变量具有很少种类的情况下,科恩卡帕系数也可能不够稳定和精确。
总之,科恩卡帕系数是一种用于评估分类者一致性的重要方法。
该系数可以帮助评估分类者的一致性程度,而不考虑其准确性。
然而,使用科恩卡帕系数也需要注意其局限性。
对于不确定的情况,需要使用其他方法来评估分类者的一致性。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Kappa value range from 0-1,from no agreement to absolute agreement.
It is not unusual for a high r value to indicate a clear association between groups of measurements when the kappa value for the same data is low, indicating little agreement among the individual measurements (Altman 1994 Jerosch-Herold 2005) and therefore limited ability of one test to predict the results of the others.
话说能不能举个例子,就是很相关,但是kappa值,就是不一致性低的内容。
话说最近在看一本相关统计学方面的书,这个书上的有个内容部太理解,现摘录如下:
其实核心就是理解统计学相关性的kappa量。
丁香园上搜索到这个信息:Kappa 值越大,表明一致性越好。一般来说,若Kappa 值≥0.75 , 说明一致性较好;若Kappa 值<0.40, 说明一致程度不够理想。否则一致程度中等。
该文段原文是这样的:to measure the actual agreement between two sets of observations, one must calculate the kappa value, a chance-corrected measured of proportional agreement(Altman,1994), The kappa value is often weighted to take into reement between measurements, Alternatively, an intrerclass correlation coefficient (ICC) may be used.