英文--肝硬化完整大病历
肝硬化 cirrhosis of liver

Company Logo
并发症
4.肝肾综合症 表现:自发性少尿、无尿、低尿钠、氮质血症、 稀释性低钠血症 5.原发性肝癌 表现:肝脏进行性肿大、血性腹水、肝区疼痛 6、电解质、酸碱平衡紊乱 低钠:与摄入不足、利尿、放腹水 低钾、低氯与代碱:与摄入不足、呕吐、腹泻、 利尿及醛固酮增多有关
门静脉 高压 肝脏功 能减退
Company Logo
临床表现
1
代偿期 :
症状轻、缺乏特异性
2
失代偿期:症状明显
肝功能减退、门静脉高压
Company Logo
代偿期
症状
乏力 消化道症状
体征
肝、脾轻度肿大
Company Logo
小结
肝硬化是一种由不同原因引起的慢性、进行性、 弥漫性肝病。我国最常见的原因是病毒性肝炎, 典型理改变是假小叶形成。 肝硬化突出的表现是肝功能减退和门脉高压。 门脉高压的表现 肝硬化的并发症 难点:腹水形成的机制
Company Logo
病因
最常见
病毒性肝炎 营养障碍 免疫紊乱 慢性酒精中毒
肝硬化
药物中毒
胆汁淤积
循环障碍 血吸虫病 代谢障碍
Company Logo
病因
肝硬化
病毒性肝炎
乙型 丙型 丁型
非病毒性肝炎
68%
32%
Company Logo
病因
first
乙醇及中 间代谢产 物乙醛的 毒性作用
second
third
酒精性肝炎
肝硬化
Company Logo
发病机制
6 5 4 3 2 1
肝硬化
5
定义
一(多)种病因
肝组织弥漫性纤维化、 肝功能损害、门脉压增
假小叶和再生结节形成 高、多种并发症
(组织学改变)
(临床表现)
慢性肝病
6
概况
各种慢性肝病的晚期阶段。
▪ 病理 — 肝脏弥漫性纤维化、假小叶形成、肝 细胞结节性再生为特征,肝逐渐变形、变硬。
▪ 临床 — 肝功能损害和门脉高压为主要表现、 晚期常出现消化道出血、肝性脑病等并发症。
凝血酶原时间: PT 18.3s (对照13.1s)
急诊胃镜:
食 道
胃 底
诊 断?
3
肝硬化
Hepatic Cirrhosis
4
目的要求:l.掌握肝硬化的临床表现、并发 症、诊断、治疗原则。
2.熟悉本病病因、发病机理及鉴别诊断
重点: 1.从病因、病理变化出发,阐述各 种症状的由来及处理原则。 2.从肝脏代谢角度来判断肝脏功能
如长期服用异烟肼、四环素、双醋酚汀、 甲基多巴、甲氨喋呤等,或长期反复接触某 些化学毒物如四氯化碳、磷、砷、氯仿等可 引起药物性或中毒性肝炎及慢性活动性肝炎, 进而发展为中毒性(药物性)肝硬化。
15
(八)自身免疫性肝炎 (AIH)
( 九 ) 血吸虫病 虫卵沉积于汇管区,导致肝脏纤维化和 窦前性门脉高压。
38
血吸虫病
窦前性 胆汁性肝硬化
门脉或脾静脉病变
窦性
病毒性肝炎 酒精性肝病 脂肪肝 细胞毒性药物:如硫唑嘌呤,等
肝小静脉闭塞病
窦后性 肝静脉、下腔静脉栓塞或畸形
心血管:缩窄性心包炎、严重右心功能不全
39
门脉高压后果
1、侧枝循环建立 引起上消出血及 肝性脑病基础
肝硬化病例

慢性乙型肝炎防治指南(2010年版). 临床肝胆病杂志 2011 , 27 (1):1-16
ALT正常或者轻度异常的患者也存在肝脏组织学改变
• 35岁以上患者炎症分级和纤维化分期均较35岁以下
患者显著升高
Shao L, Du X, Zhang Wenhong. 2011 APASL Poster P03-37
2009年4月,患者于体检时发现ALT升高 (55 IU/L),HBV DNA为8.4×107 copies/mL。患者无明显不适,但因肝功能异常 遂来就诊。
• 家族史:弟弟死于肝细胞性肝癌
实验室检查 (2009.6)
•
肝功能:ALT: 67 U/L ,AST: 45 U/L ,总胆红素: 15μmol/L , 白蛋白: 34 g/L
该患者继续拉米夫定加阿德福韦联合治疗联合治疗12个月后复查hbvdna已低于检测水平最低检测下限60copiesmlcobastaqman这个病例涉及到40岁肝功能接近正常的慢性乙肝患者是否有指证迚行治疗的问题2010乙肝指南指出1对alt大于uln且年龄40岁者也应考虑抗病毒治2对alt持续正常但年龄较大者40岁应密切随访最好迚行肝活组织检查
一例慢乙肝肝硬化代偿期患者的治疗
姓名:*** 医院:******医院
病史简介(2009.6)
• 男性, 40岁 • 主诉:发现HBsAg阳性10年,肝功能异常2月 • 现病史:
患者于10年前体检时发现HBsAg(+),当时查肝功能在正常范 围内,乙肝标志物:HBsAg (+) 、HBeAg (-) 、抗-HBe (+) , HBV DNA 3.6×107 copies/mL。未接受抗病毒等治疗。以后每年 常规检查肝功能均正常。
英文 肝硬化

Consequences of portal hypertension[II] 3. Ascites (腹水)
• • •
Theories of ascites formation Underfilling theory (灌注不足假说) Overflow theory (泛溢假说) Arterial vasodilation theory (动脉扩张假说)
Mechanisms of HRS[II]
Clinical features[I]
Compensated cirrhosis (代偿期)
Many people experience few symptoms at the onset of cirrhosis,symptoms are typically vague and nonspecific. ---Fatigue and loss of energy. ---Loss of appetite and nausea. ---Spider angiomas ---liver function is normal
degradation of matrix proteins
Pathogenesis: chronic, progressed,
diffuse • Hepatocyte injury leading to necrosis. • Chronic inflammation - (hepatitis). • Capillarization (肝窦毛细血管化) of the space of Disse is a key event. • Bridging fibrosis. • Regeneration of remaining hepatocytes proliferate as round nodules surrounded by fibrous septa. • Loss of vascular arrangement results in regenerating hepatocytes ineffective. • Cirrhosis may lead to liver failure, portal hypertension, or development of hepatocellular carcinoma
英文肝硬化完全大病历
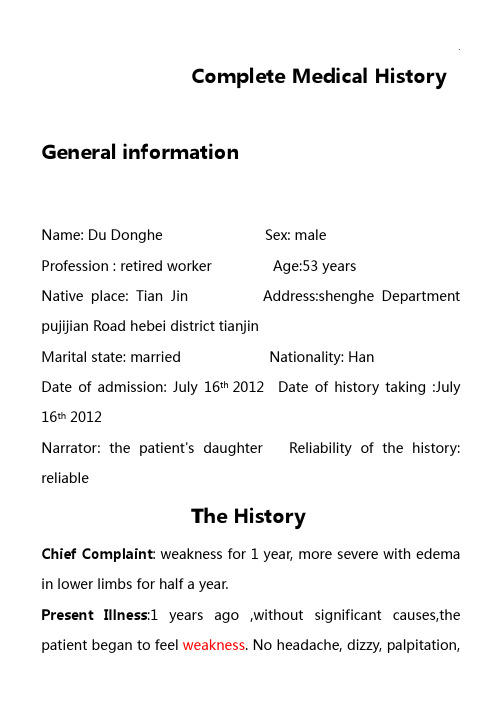
Complete Medical History General informationName: Du Donghe Sex: maleProfession : retired worker Age:53 yearsNative place: Tian Jin Address:shenghe Department pujijian Road hebei district tianjinMarital state: married Nationality: HanDate of admission: July 16th 2012 Date of history taking :July 16th 2012Narrator: the patient's daughter Reliability of the history: reliableThe HistoryChief Complaint: weakness for 1 year, more severe with edema in lower limbs for half a year.Present Illness:1 years ago ,without significant causes,the patient began to feel weakness. No headache, dizzy, palpitation,shortness, abdominal pain or diarrhea . The patient went to the hospital in his town, and checked his live function, shown the live is damaged,given liver-protecting treatment(the detail of drugs used is unclear). But the symptom is not obviously lightened. And half a year ago ,the symptom became more severe,with edema in lower limbs , abdominal distension and bulge.No headache, dizzy, palpitation, shortness, tightness, abdominal pain or diarrhea . So the patient went to the out-patient department of our hospital to check the HBV-DNA 5.410E+4copies/ml,AFP13.91mg/ml,HBsAg(+),HBsAb(+).HBsAb-Ig G(+), PreS1(+). He also had a MR scan of the upper abdomen,shown hepatic cirrhosis,splenomegaly,portal hypertention,gastric varix,umbilical vein repassing. So he was accepted in our section for advanced diagnosis and treatment. Since the disease, no changes in consciousness, appetite, body weight .and normal of stool while less of urine. Past history: the patient became blind 50 years ago.And he has a history of hepatitis B for 26years. No history of chronic diseases like hypertension, CAD and mellitus diabetics. Notuberculosis .No history of trauma, operation and blood transfusion. He was allergic to penicillin and sulfa drugs.The history of vaccination is unclear.Review of Systems:Respiratory system: no history of chronic cough , expectoration, hemoptysis , chest pain , or short of breath. Circulation system: half a year age he had the edema at the lower limbs.no history of dyspnea,palpitation or chest pain. No dizziness, headache.No history of hypertension.Digestive system: half a year age he began to have the abdominal distention and bulge.no history of anorexia, , regurgitation反流. No nausea and vomiting. No history of constipation , diarrhea ,melena .Urogenital system: no history of swollen eyelids or lumbago腰疼. No frequent micturition, urgency of micturition or urodynia. No dysuria ,hematuria or retention and incontinence of urine .no history of acute or chronic nephritis.Hemopoeltic system: 1 years ago the patient began to feel weakness and became more severe half a year ago. No pallid 苍白countenance面容,dizziness , daze头昏眼花,tinnitus耳鸣. Nohistory of bleeding and repeated infections.The MR scan shows splenomegaly..Metabolic and Endocrine system:no abnormal cold or hot feeling, hidrosis多汗,headache ,impaired vision,polyphagia 食欲过盛,polyuria ect.normal distributed hair.no change of temper and intelligence.Nervous system: No headache ,projectile vomiting . no syncope ,spasm ,impaired vision, abnormal sensation or motion. No change of personality .no mania躁狂,depression or hallucination.Motor system: No spasm, atrophy or palalysis. No joint red swollen, hot ,pain or limitation of motion. No trauma or fracture.Personal history : born in her native place and living in Tianjin. No history of exposure to radioactive poison.No habits of drinking or smoking.Marital History:. Married at 30 years old and having a son. his son and wife are both healthy.Family history: his mother had the hepatitis B.denying otherfamily history of heredity diseases ,or MD, CAD, hypertension ect.Physical Examination Temperature: 37.1C pulse rate: 101/min respiratory rate: 18/min blood pressure:130/80mmHgGeneral appearance : normal development and medium in nourished ,no abnormal consciousness, good corporation in examination. Free position.Skin and mucous membrane: No pallid , cyanosis, and jaundice . no abnormal pigmentation and depigmentation . no erythma annulare, petechia and spider angioma. Normal elasticity of skin, no edema.Superficial lymph nodes: no enlargement of the superficial lymph nodes.Head and its organs:Skull: no deformity, tenderness or mass. Evenly distributed hair with black color and shine.Eyes: no drop out of eyebrow and no madarosis ,no swollen or prolapse of eyelids. No pallor, granules ,follicles pectechiae ofconjunctivae . transparent of cornea ,no nebula ,keratoleukoma, malacia, ulcer or vascularization. No exophthalmos 眼球突出or enophthalmos.free motions of the eye balls in any direction. Equal and round pupils at both sides with diameter 4mm, No light reflexes, no accommodation and convergence reflexes. Vision , visual field and eyegroud not examined.Ears:no deformity .no abnormal secretion from external canals. No red, tenderness, swollen in the mastoid. Rough tested normal hearing.Nose: no deformity. No deviation of septum nasi. No ala flutter. No edema ,abnormal secretion ,and congestion of the membrane . good ventilation. No tenderness in any paranasal sinuses.Buccal cavity: no pallid or cyanosis of lips ,also no dryness ,herpes simplex. No congestion ,petechia or ulcer in the buccal membrane . 32 teeth, no caries. No bleeding or congestion ,lead line in gums. T ongue was in midline ,with normal in motion. No redness and congestion in pharynx ,no deviation of uvulae. No edema in tonsils.Neck: symmetry . no enlargement of external jugular vein, noabnormal pulsation of carotid arteries or veins. No rigidity .no enlargement of thyroid glands ,and the trachea in the centeral position. No murmur. Negative of hepatojugular reflux. Chest: symmetry. No deformity. No barrel chest ,pigeon chest or funnel chest. No tenderness over the chest .the thoracic respiration present. R 18/min, symmetry in both sides. Symmetry and no abnormality of the 2 breasts.Lungs:Inspections: no bulges or recession of the intercostals spaces during respiration. Respiratory movement equal in both sides and regular . no dyspnea or three concave sign.Palpation: symmetry respiratory movement in the two sides, no increase or decrease of vocal fremitus. No pleural friction fremitus . no subcutaneous crepitation.Percussion: resonance in all over the lung fields . 5 cm in width of apexes ,and the lower margin of lung at 6th,8th,10th on midclavicular ,midaxillary,midcapular line respectively in both left and right side. The movements of the lower margin of the lungs are 6 cm in both left and right side. Auscultation: rough of vesicular breathing sounds all over thelung fields.fine rales are heard in bilateral subpulmonic parts.no rhonchis .normal of vocal resonance. No pleural friction sound. Heart:Inspection: no precordial bulging. Apical impulse in the 5th ICS 1cm inside of left midclavicular line with an area of 2 cm in diameter.Palpation: apical impulse and its area as that in inspection. Regular ,normal intensity. No pericardial friction rubs or thrill. Percussion: relative cardiac dullness shown as follows:The distance between the left midclvicular line and the midsternal line is 8cm.Auscultation: HR 101/min with regular rhythm, heart sounds clear and intensive . no murmurs at any auscultation area of the valvula. No pericardical friction sound.Radial arteries: pulse rate 101/min, with regular rhythm, equalin both sides, normal intensity .Perivascular signs: no capillary pulsation, water hammer pulse ,pistol-shot sounds and Duroziez’s murmur . no pulse deficit, and pulse alternant.Abdomen:Inspection: symmetry. bulge abdomen.normal abdominal respiration. No visible gastrointestinal waves. No varicosity , scar ,petechia at the abdominal Skin.Palpation: tightened abdominal wall ,no tenderness and rebounding tenderness . No palpable mass.Liver: not palpable.Gallbladder: not palpable. Negative of murphy’s sign. Kidneys: not palpable. No tenderness in the any site of kidneys or ureters.Spleen: not palpable.Appendix: no tenderness at the Mcburney’s site. Percussion: tympany in all over the abdomen, shifting dullness(+). No percussive pain of liver and spleen. The upper margin of liver at the 5th ICS in the right midcalvicular line Auscultation: normal borhorygmus, 4/min, no murmur ofvessels. No friction rubs .Anus and rectum: not examined.Spine: no lordosis, kyphosis, or scoliosis. No tenderness and punching tenderness . No Limitation of movement. No changes in the local skin.Extremities: symmetry, no deformity . free motion .muscle strength is normal.no joint redness ,swollen ,tenderness or hotness. No acropachy,koilonychia,floating patella test(-).bilateral dorsalis pedis arteries can be palpated. edema in the lower extremities(+++).Nerve system: Biceps,triceps ,radioperiosteal , and abdominal wall reflexes normal. knee jerk and Achilles jerk are also normal. babinski’s ,oppenheim’s,chaddock’s,gordon’s negative. Hoffmann sign (-). Neck tetany (-) Kernig sign (-).Brudzinski sign (-).No patellar or ankle clonus.Laboratory findings: HBsAg(+),HBsAb(+).HBsAb-IgG(+), PreS1(+). HBV-DNA 5.4 10E+4copies/ml,AFP13.91mg/ml(2012.6.29,GH)MRI : hepatic cirrhosis,splenomegaly,portal hypertention,gastric varix,umbilical vein repassing.SummaryThe patient named Du Donghe ,male ,is 53years old,admission with the chief complaint of weakness for 1 year, more severe with edema in lower limbs for half a year in July 16th 2012 .1 years ago ,without significant causes,the patient began to feel weakness.He went to the hospital in his town, and checked his live function, shown the live is damaged, given liver-protecting treatment(the detail of drugs used is unclear). But the symptom is not obviously lightened. And half a year ago ,the symptom became more severe,with edema in lower limbs , abdominal distension and bulge.So the patient went to the out-patient department of our hospital to check the HBV-DNA 5.410E+4copies/ml,AFP13.91mg/ml,HBsAg(+),HBsAb(+).HBsAb-Ig G(+), PreS1(+). He also had a MR scan of the upper abdomen,shown hepatic cirrhosis,splenomegaly,portal hypertention,gastric varix,umbilical vein repassing. So he was accepted in our section for advanced diagnosis and treatment.the patient became blind 50 years ago.And he has ahistory of hepatitis B for 26years. He was allergic to penicillin and sulfa drugs.He has no history of exposure to radioactive poison.and his mother had the hepatitis B.PE: T:37.1C ,P: 101/min R: 18/min Bp 130/80mmHg,normal development, moderately nourished, clear counsciousness. Good corporation in physical examination. rough of vesicular breathing sounds all over the lung fields.fine rales are heard in bilateral subpulmonic parts.HR101bpm,with regular rhythm. no murmurs at any auscultation area of the valvula. bulge abdomen,tightened abdominal wall ,no tenderness and rebounding tenderness. Liver and Spleen are not palpable.shifting dullness(+),edema in the lower extremities(+++)Laboratory findings: HBsAg(+),HBsAb(+).HBsAb-IgG(+), PreS1(+). HBV-DNA 5.4 10E+4copies/ml,AFP13.91mg/ml(2012.6.29,GH)MRI : hepatic cirrhosis,splenomegaly,portal hypertention,gastric varix,umbilical vein repassing.Impression: 1.HBV cirrhosisPortal hypertensiongastric varix2.HypersplenismSignature:JinDan。
肝硬化大病历

肝硬化大病历
肝硬化是一种常见的肝脏疾病,其主要特点是肝脏组织发生不可逆性的纤维化和结缔组织增生,导致肝功能逐渐恶化,最终发展为肝功能衰竭。
下面是一位患有肝硬化的患者的病历。
患者姓名:王先生
性别:男
年龄:56岁
职业:退休工人
初诊日期:2020年7月1日
患者主诉:肝区酸痛、腹胀、乏力、食欲减退、黄疸等症状已有一年,加重一周。
既往病史:患者有高血压、糖尿病等慢性病史,多年饮酒史。
体格检查:肝区有压痛、肝大明显,腹水征阳性。
实验室检查:ALT 68 U/L(正常值<40 U/L)、AST 78 U/L(正常值<40 U/L)、总胆红素 72 μmol/L(正常值<20 μmol/L)、白蛋白 30 g/L(正常值35-55 g/L)、凝血酶原时间延长(14秒)。
影像学检查:腹部超声检查显示肝脏弥漫性回声增高,门静脉高压,脾脏肿大,胆囊壁增厚,腹水征象明显。
诊断:肝硬化,门脉高压综合征。
治疗方案:给予维持治疗,包括禁酒、低蛋白饮食、支持疗法等,同时进行症状缓解治疗,如利尿剂、肝素钠、抗感染等。
定期进行肝功能检查,观察病情变化,及时调整治疗方案。
预后:肝硬化是一种不可逆性疾病,预后与病情的严重程度和治疗的及时性有关。
患者需积极治疗,遵守医嘱,控制饮食和生活方式,早期发现和处理并发症,以延缓疾病的进展,提高生活质量。
总结:肝硬化是一种常见的肝脏疾病,患者需要积极治疗,控制病情,提高生活质量。
预防肝硬化的最好方法是戒酒,保持健康的生活方式。
及早治疗肝硬化并发症,保持规律的检查,是控制肝硬化病情的关键。
第十五章肝硬化(Cirrhosis of Liver,LC)

临床表现
重点
(Clinical features)
肝硬化的临床表现多样,起病常隐匿, 病情进展缓慢,可潜伏3~5年或10年 以上,少数因短期大片肝坏死,3~6 个月可发展成肝硬化。
临床上分为肝功能代偿期和失代偿期
代偿期
重点
症状较轻、缺乏特异性
疲乏无力、食欲减退,腹胀不适、恶心、 上腹隐痛、轻微腹泻 。间断性,因劳 累或伴发病而出现,休息或治疗后可缓 解
继发性醛固酮↑和抗利尿激素↑-对腹水的形成 和加重有促进作用
门脉高压症表现
重点
发生机制:门脉阻力增加
门脉血流量增多
临床表现
脾肿大:脾功能亢进
侧枝循环建立和开放:PVP>200mmH2O 食管静脉曲张:胃冠状V-食管V、肋间
V、奇V
腹壁静脉曲张:脐V-副脐V、腹壁V
痔静脉扩张:直肠上V-直肠中、下V
营养一般,肝轻度肿大,质地坚硬或偏 硬,无或有轻度压痛。脾轻-中度肿大
肝功能检查正常或轻度异常
失代偿期
重点
肝功能减退症状 门脉高压表现 全身多系统表现
肝功能减退的临床表现
全身症状:营养差、消瘦乏力、皮肤干枯、 肝病面容,可有不规则低热、夜盲、浮肿等
消化系症状:厌食,上腹部饱胀不适、恶心、 纳差、腹胀、腹泻、黄疸等。症状的产生与 门脉高压胃肠道淤血水肿、消化吸收障碍和 肠道菌丛失调等有关
损伤与修复反复交替
肝小叶结构改建、肝血液循环途径改建, 肝变 形、变硬
门静脉高压症、肝功能不全
病理
形态学分类
小结节性肝硬化
直径多在 3~5 mm,不超过1 cm,最常见 酒精性,血色病,肝外胆管梗阻,肝静脉输出梗阻,空回肠旁路, 小结节型肝硬化常可进展为大结节型肝硬化
肝硬化(2010)
发病机制
电镜下的肝血窦 及部分与炎性坏 死和纤维化形成 有关的间质细胞 L 为肝脏相关性 淋巴细胞 K 为Kupffer细 胞 S 为肝血窦腔
发病机制—肝纤维化形成
发病机制—腹水形成 第一、门静脉系压力增加与低蛋白血症 根据Starling平衡理论,在门静脉系的 毛细血管和组织间隙之间,液体的交换取决 于局部静水压与渗透压之差。在动脉端,静 水压大于渗透压,组织液流向组织间隙。在 静脉端,静水压小于渗透压,组织液流向血 管内。
发病机制—腹水形成 肝硬化后,肝细胞坏死和纤维化形成 ,肝脏正常结构特点被破坏使门静脉系血 流阻力增加,根据Laplace法则,阻力增 加使静水压升高。并且,肝功能损害使白 蛋白浓度减少,胶体渗透压下降。此共同 的作用使组织液不能回流到血管内,经脏 层腹膜溢入腹腔,形成腹水。
第二部分—门静脉高压表现 腹水(是漏出液!)和脾肿大
肝硬化患者因腹水所 表现的腹部高度膨隆
肝功能失代偿期临床表现
第三部分—肝脏的结构变化 多数类型的晚期肝硬化肝脏常较正常有不同程 度的缩小,肝脏触诊时肝脏常不能触及,形成“肝 小脾大”的基本腹部触诊结果,但下述等情况或肝 硬化类型可有肝脏增大。
病因
肝硬化
肝硬化是一种以肝组织弥漫性纤维化、假小 叶和再生结节形成为特征的慢性肝病。是一种不 可逆的肝脏组织结构改变。
肝硬化的外观表现 正常肝小叶 的镜下特征
假小叶
肝硬化的镜下特征
pseudolobule
病因:病毒,酒精,血吸虫, …… 病理:大结节,小结节,混合结节和不完全分隔性 临床表现:肝功能损害,门静脉高压症 肝功能损害:肝病面容,肝掌,蜘蛛痣,黄疸 门静脉高压症:侧支循环的建立与开放,腹水,脾大 并发症:出血,肝性脑病,感染,肝肾综合征,癌变, 水、电解质与酸碱平衡紊乱 实验室改变:B超:肝表面结节,腹水,门、脾静脉增宽,脾厚 胃镜:食管和/或胃底静脉曲张,门静脉高压胃病 血液:白蛋白降低,胆红素增高,PT延长,…… 诊断:病史,临床表现与实验室改变,病理学改变 鉴别诊断:上消化道出血,腹水,黄疸,肝癌,…… 治疗:腹水的治疗—限钠、水,利尿剂,…… 腹膜炎的治疗—抗生素 肝肾综合征的治疗—限水,纠偏,增容利尿, 改善肾血流 护理:护理诊断,护理措施
肝硬化病历模板

肝硬化病历模板基本信息姓名•姓名:XXX•性别:男/女•年龄:X岁•联系电话:XXXXXXXXXXX诊断日期•初次诊断时间:XXXX年X月X日•最近一次就诊时间:XXXX年X月X日主要症状•腹胀胀痛,XXX部位,X月前开始,X级别(1-10),以往有无类似症状?•厌食、腹泻、便秘、黄疸等,其他症状?就诊经过就诊医院/科室•就诊医院:XXXX医院•就诊科室:XXX科室检查结果•血常规:WBC:X,Hb:X,PLT:X•肝功能:–ALT:X,AST:X,TBil:X,DBil:X,ALP:X–凝血功能:PT:X,INR:X•影像学检查:B超、CT/MRI等(如有)–肝脏大小、形态、回声情况–肝内血流情况、门脉高压–肝硬化分级情况治疗方案•药物治疗:X药物,用药时间、剂量、疗程等•介入治疗:TIPS、肝动脉栓塞等(如有)•营养支持:口服/静脉注射营养液、饮食要求等•其他治疗方案随访记录随访时间•随访时间:XXXX年X月X日•下一次随访时间:XXXX年X月X日过去治疗效果•当前主要症状是否缓解?疼痛程度、频率、持续时间等•肝功能、凝血功能等检查结果是否有变化?•是否出现并发症、恶化情况?随访方案•继续原有治疗方案•加减药物/调整剂量/更换药物等,具体计划•补充营养、加强锻炼等建议•下一次随访时间及注意事项注意事项•饮食:低盐、低脂、易消化等•生活:避免饮酒、勿用毒品、保证充足睡眠等•孕产妇:应告知主治医生,避免用药过度造成不良影响。
英文 肝硬化
Etiology of cirrhosis(II)
6. Hepatic venous outflow obstruction(肝血液循环 障碍)
veno-occlusive disease, Budd-Chiari syndrome, constrictive pericarditis
7. Metabolic disorders (遗传代谢性疾病)
Pulmonary manifestations
Hepatic hydrothorax (肝性胸水) Hepatopulmonary syndrome (HPS, 肝肺综合征)
HRS is characterized clinically by the triad of pulmonary vascular dilatation causing arterial hypoxemia in the setting of advanced liver disease.
Clinical features[II]
---Tendency to hemorrhage(出血倾向) and anaemia(贫血): Due to reduced synthesis of coagulation factors (II,V,VII,IX,X), hypersplenism(脾亢), low platelet count, poor absorption,gastrointestinal bleeding. ---Hormonal abnormalities gynecomastia(男性乳房发育), telangiectases (毛细血管扩张症), spider nevi(蜘蛛痣), palmar erythema(肝掌) ---Jaundice(黄疸)
肝硬化-Cirrhosis-of-liver
氨对脑组织的毒性作用:
抑制丙酮酸脱氢酶→乙酰辅酶A减少→ 影响三羧酸循环; 氨的清除需要消耗α-酮戊二酸、ATP等物质→影响能量代谢; 直接作用于神经膜→ 突触后抑制。
Ammonia neurotoxicity hypothesis
Factors of influence ammonia neurotoxicity: Excessive dietary protein(饮食中蛋白过量) Hypoxia & Dehydration(缺氧或脱水) GI hemorrhage(消化道出血) Constipation(便秘) Infection(感染)
Uremia(尿毒症)/Azotemia(氮质血症) Sedatives, benzodiazepines(镇静剂, 苯二氮卓类) Gastrointestinal bleeding(消化道出 Barbiturates (巴比妥类药物) 血)
Tab 1.Clinical Factors that may precipitate hepatic enceph
表 4-1.慢性肝性脑病的分期
分期 前驱期 主要神经精神表现 轻度性格改变、 举止反常 神经系体征 多无扑翼震颤 常出现扑翼震颤、腱 反射亢进、肌张力增 高、锥体束征(一) 可引出扑翼需震颤 深昏迷时不能引出扑 翼震颤、反射消失 脑电图 无明显异常, 波的频率可减少 常出现异常的慢波 (θ波) 明显异常的θ波和 三相慢波 出现δ波
Hypoglycemia(低血糖)
……
False neurotransmitter hypothesis
表2. 两大类神经递 质 兴奋性神经递质 抑制性神经递质
去甲肾上腺素 鱆胺
乙酰胆碱
肝硬化,双语
5 HRS诊断标准 HRS诊断标准 主要标准: 主要标准: (1) GFR↓ , 血 肌 酐 > 132 . 6umol⁄L( 等 于 15mg⁄L) 24小时肌酐清除率 40ml⁄min mg⁄L)或 小时肌酐清除率< 15mg⁄L)或 24小时肌酐清除率<40ml⁄min 排除其他病因如休克、 感染、 (2) 排除其他病因如休克 、 感染 、 肾毒药物或液 体丢失等 停利尿剂及扩容治疗(输液1500ml) 1500ml (3) 停利尿剂及扩容治疗(输液1500ml)后无 改善。 改善。 尿蛋白低于500mg⁄d、 500mg⁄d (4) 尿蛋白低于500mg⁄d、超声波检查肾及尿路 无梗阻与肾实质损害等异常。 无梗阻与肾实质损害等异常。 次要标准: 次要标准: 尿量<500ml⁄d (1) 尿量<500ml⁄d 尿钠< 10mmol⁄L (2) 尿钠< 10mmol⁄L (3) 尿渗透压>血浆渗透压; 尿渗透压>血浆渗透压; RBC<50⁄HP ⁄HP; (4) 尿RBC<50⁄HP; Na<130mmol⁄L (5) 血Na<130mmol⁄L
肝硬化(hepatic 肝硬化(hepatic cirrhosis)
湘雅医院消化科 冯莉娟
Definition
Chronic disease of the liver characterized by : fibrosis regenerating nodules of hepatocytes disorganization of the lobular and vascular architecture
Signs
•
• • • •
Spider nevi, palmar erythema parotid and lacrimal gland enlargement nail changes Gynecomasia,testicular atrophy hepatosplenomegaly
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Complete Medical History General informationName: Du Donghe Sex: maleProfession : retired worker Age:53 yearsNative place: Tian Jin Address:shenghe Department pujijian Road hebei district tianjinMarital state: married Nationality: HanDate of admission: July 16th 2012 Date of history taking :July 16th 2012 Narrator: the patient's daughter Reliability of the history: reliableThe HistoryChief Complaint: weakness for 1 year, more severe with edema in lower limbs for half a year.Present Illness:1 years ago ,without significant causes,the patient began to feel weakness. No headache, dizzy, palpitation, shortness, abdominal pain or diarrhea . The patient went to the hospital in his town, and checked his live function, shown the live is damaged,given liver-protecting treatment(the detail of drugs used is unclear). But the symptom is not obviously lightened. And half a year ago ,the symptom became more severe,with edema in lower limbs , abdominal distension and bulge.No headache, dizzy, palpitation, shortness, tightness, abdominal pain or diarrhea . So the patientwent to the out-patient department of our hospital to check the HBV-DNA 5.4 10E+4copies/ml,AFP13.91mg/ml,HBsAg(+),HBsAb(+).HBsAb-IgG(+), PreS1(+). He also had a MR scan of the upper abdomen,shown hepatic cirrhosis,splenomegaly,portal hypertention,gastric varix,umbilical vein repassing. So he was accepted in our section for advanced diagnosis and treatment. Since the disease, no changes in consciousness, appetite, body weight .and normal of stool while less of urine.Past history: the patient became blind 50 years ago.And he has a history of hepatitis B for 26years. No history of chronic diseases like hypertension, CAD and mellitus diabetics. No tuberculosis .No history of trauma, operation and blood transfusion. He was allergic to penicillin and sulfa drugs.The history of vaccination is unclear.Review of Systems:Respiratory system: no history of chronic cough , expectoration, hemoptysis , chest pain , or short of breath.Circulation system: half a year age he had the edema at the lower limbs.no history of dyspnea,palpitation or chest pain. No dizziness, headache.No history of hypertension.Digestive system: half a year age he began to have the abdominal distention and bulge.no history of anorexia, , regurgitation反流. No nausea andvomiting. No history of constipation , diarrhea ,melena .Urogenital system: no history of swollen eyelids or lumbago腰疼. No frequent micturition, urgency of micturition or urodynia. No dysuria ,hematuria or retention and incontinence of urine .no history of acute or chronic nephritis.Hemopoeltic system: 1 years ago the patient began to feel weakness and became more severe half a year ago. No pallid 苍白countenance面容,dizziness ,daze头昏眼花,tinnitus耳鸣. No history of bleeding and repeated infections.The MR scan shows splenomegaly..Metabolic and Endocrine system:no abnormal cold or hot feeling, hidrosis多汗,headache ,impaired vision,polyphagia 食欲过盛,polyuria ect.normal distributed hair.no change of temper and intelligence.Nervous system: No headache ,projectile vomiting . no syncope ,spasm ,impaired vision, abnormal sensation or motion. No change of personality .no mania躁狂 ,depression or hallucination.Motor system: No spasm, atrophy or palalysis. No joint red swollen, hot ,pain or limitation of motion. No trauma or fracture.Personal history : born in her native place and living in Tianjin. No history of exposure to radioactive poison.No habits of drinking or smoking.Marital History:. Married at 30 years old and having a son. his son and wife are both healthy.Family history: his mother had the hepatitis B.denying other family history of heredity diseases ,or MD, CAD, hypertension ect.Physical Examination Temperature: 37.1C pulse rate: 101/min respiratory rate: 18/min blood pressure:130/80mmHgGeneral appearance : normal development and medium in nourished ,no abnormal consciousness, good corporation in examination. Free position. Skin and mucous membrane: No pallid , cyanosis, and jaundice . no abnormal pigmentation and depigmentation . no erythma annulare, petechia and spider angioma. Normal elasticity of skin, no edema.Superficial lymph nodes: no enlargement of the superficial lymph nodes. Head and its organs:Skull: no deformity, tenderness or mass. Evenly distributed hair with black color and shine.Eyes: no drop out of eyebrow and no madarosis ,no swollen or prolapse of eyelids. No pallor, granules ,follicles pectechiae of conjunctivae . transparent of cornea ,no nebula ,keratoleukoma, malacia, ulcer or vascularization. No exophthalmos 眼球突出or enophthalmos.free motionsof the eye balls in any direction. Equal and round pupils at both sides with diameter 4mm, No light reflexes, no accommodation and convergence reflexes. Vision , visual field and eyegroud not examined.Ears:no deformity .no abnormal secretion from external canals. No red, tenderness, swollen in the mastoid. Rough tested normal hearing.Nose: no deformity. No deviation of septum nasi. No ala flutter. No edema ,abnormal secretion ,and congestion of the membrane . good ventilation. No tenderness in any paranasal sinuses.Buccal cavity: no pallid or cyanosis of lips ,also no dryness ,herpes simplex. No congestion ,petechia or ulcer in the buccal membrane . 32 teeth, no caries. No bleeding or congestion ,lead line in gums. Tongue was in midline ,with normal in motion. No redness and congestion in pharynx ,no deviation of uvulae. No edema in tonsils.Neck: symmetry . no enlargement of external jugular vein, no abnormal pulsation of carotid arteries or veins. No rigidity .no enlargement of thyroid glands ,and the trachea in the centeral position. No murmur. Negative of hepatojugular reflux.Chest: symmetry. No deformity. No barrel chest ,pigeon chest or funnel chest. No tenderness over the chest .the thoracic respiration present. R 18/min, symmetry in both sides. Symmetry and no abnormality of the 2breasts.Lungs:Inspections: no bulges or recession of the intercostals spaces during respiration. Respiratory movement equal in both sides and regular . no dyspnea or three concave sign.Palpation: symmetry respiratory movement in the two sides, no increase or decrease of vocal fremitus. No pleural friction fremitus . no subcutaneous crepitation.Percussion: resonance in all over the lung fields . 5 cm in width of apexes ,and the lower margin of lung at 6th,8th,10th on midclavicular ,midaxillary,midcapular line respectively in both left and right side. The movements of the lower margin of the lungs are 6 cm in both left and right side.Auscultation: rough of vesicular breathing sounds all over the lung fields.fine rales are heard in bilateral subpulmonic parts.no rhonchis .normal of vocal resonance. No pleural friction sound.Heart:Inspection: no precordial bulging. Apical impulse in the 5th ICS 1cm inside of left midclavicular line with an area of 2 cm in diameter.Palpation: apical impulse and its area as that in inspection. Regular ,normalintensity. No pericardial friction rubs or thrill.Percussion: relative cardiac dullness shown as follows:Right (cm) ICS Left (cm)2 Ⅱ 22 Ⅲ 43 Ⅳ 6Ⅴ7The distance between the left midclvicular line and the midsternal line is 8cm.Auscultation: HR 101/min with regular rhythm, heart sounds clear and intensive . no murmurs at any auscultation area of the valvula. No pericardical friction sound.Radial arteries: pulse rate 101/min, with regular rhythm, equal in both sides, normal intensity .Perivascular signs: no capillary pulsation, water hammer pulse ,pistol-shot sounds and Duroziez’s murmur . no pulse deficit, and pulse alternant. Abdomen:Inspection: symmetry. bulge abdomen .normal abdominal respiration. No visible gastrointestinal waves. No varicosity , scar ,petechia at the abdominal Skin.Palpation: tightened abdominal wall ,no tenderness and rebounding tenderness . No palpable mass.Liver: not palpable.Gallbladder: not palpable. Negative of murphy’s sign.Kidneys: not palpable. No tenderness in the any site of kidneys or ureters. Spleen: not palpable.Appendix: no tenderness at the Mcburney’s site.Percussion: tympany in all over the abdomen, shifting dullness(+). No percussive pain of liver and spleen. The upper margin of liver at the 5th ICS in the right midcalvicular lineAuscultation: normal borhorygmus, 4/min, no murmur of vessels. No friction rubs .Anus and rectum: not examined.Spine: no lordosis, kyphosis, or scoliosis. No tenderness and punching tenderness . No Limitation of movement. No changes in the local skin. Extremities: symmetry, no deformity . free motion .muscle strength is normal.no joint redness ,swollen ,tenderness or hotness. No acropachy,koilonychia,floating patella test(-).bilateral dorsalis pedis arteries can be palpated. edema in the lower extremities(+++).Nerve system: Biceps,triceps ,radioperiosteal , and abdominal wall reflexesnormal. knee jerk and Achilles jerk are also normal. babinski’s ,oppenheim’s,chaddock’s,gordon’s negative. Hoffmann sign (-). Neck tetany (-) Kernig sign (-).Brudzinski sign (-).No patellar or ankle clonus.Laboratory findings: HBsAg(+),HBsAb(+).HBsAb-IgG(+), PreS1(+). HBV-DNA 5.4 10E+4copies/ml,AFP13.91mg/ml(2012.6.29,GH)MRI: hepatic cirrhosis,splenomegaly,portal hypertention,gastric varix,umbilical vein repassing.SummaryThe patient named Du Donghe ,male ,is 53years old,admission with the chief complaint of weakness for 1 year, more severe with edema in lower limbs for half a year in July 16th 2012 .1 years ago ,without significant causes,the patient began to feel weakness.He went to the hospital in his town, and checked his live function, shown the live is damaged,given liver-protecting treatment(the detail of drugs used is unclear). But the symptom is not obviously lightened. And half a year ago ,the symptom became more severe,with edema in lower limbs , abdominal distension and bulge.So the patient went to the out-patient department of our hospital to check the HBV-DNA 5.4 10E+4copies/ml,AFP13.91mg/ml,HBsAg(+),HBsAb(+).HBsAb-IgG(+),PreS1(+). He also had a MR scan of the upper abdomen,shown hepatic cirrhosis,splenomegaly,portal hypertention,gastric varix,umbilical vein repassing. So he was accepted in our section for advanced diagnosis and treatment.the patient became blind 50 years ago.And he has a history of hepatitis B for 26years. He was allergic to penicillin and sulfa drugs.He has no history of exposure to radioactive poison.and his mother had the hepatitis B.PE: T:37.1C,P: 101/min R: 18/min Bp 130/80mmHg,normal development, moderately nourished, clear counsciousness. Good corporation in physical examination. rough of vesicular breathing sounds all over the lung fields.fine rales are heard in bilateral subpulmonic parts.HR101bpm,with regular rhythm. no murmurs at any auscultation area of the valvula. bulge abdomen,tightened abdominal wall ,no tenderness and rebounding tenderness. Liver and Spleen are not palpable.shifting dullness(+),edema in the lower extremities(+++)Laboratory findings: HBsAg(+),HBsAb(+).HBsAb-IgG(+), PreS1(+). HBV-DNA 5.4 10E+4copies/ml,AFP13.91mg/ml(2012.6.29,GH)MRI: hepatic cirrhosis,splenomegaly,portal hypertention,gastric varix,umbilical vein repassing.Impression: 1.HBV cirrhosisPortal hypertensiongastric varix2.HypersplenismSignature:Jin Dan。