医学病例报道case report文章英语用词用句
case report范文

case report范文Title: A Miraculous Recovery: A Case ReportIntroduction:In this case report, we present the extraordinary journey of Mr. Smith, a 62-year-old man who experienced a life-threatening medical condition. This report aims to provide a comprehensive overview of his case, including the initial presentation, diagnostic workup, treatment interventions, and the remarkable recovery that followed. Mr. Smith's case highlights the importance of timely medical intervention, multidisciplinary collaboration, and the resilience of the human spirit.Clinical Presentation:Mr. Smith presented to the emergency department with severe chest pain, shortness of breath, and profuse sweating. His symptoms were suggestive of a myocardialinfarction, commonly known as a heart attack. Upon arrival, he appeared pale, diaphoretic, and in distress. His vital signs were unstable, with a blood pressure of 80/50 mmHgand a heart rate of 120 beats per minute. The gravity ofhis condition necessitated immediate resuscitative measures. Diagnostic Workup:An electrocardiogram (ECG) revealed ST-segmentelevation in leads II, III, and aVF, confirming the diagnosis of an inferior myocardial infarction. Further investigations, including cardiac enzyme markers and echocardiography, supported the diagnosis and provided valuable information regarding the extent of myocardial damage. Additionally, coronary angiography revealed acritical stenosis in the right coronary artery.Treatment Interventions:Given the severity of Mr. Smith's condition, a multidisciplinary team consisting of cardiologists, interventional radiologists, and cardiac surgeonscollaborated to devise an optimal treatment plan. Initially, he was stabilized with intravenous fluids, oxygen supplementation, and pain relief. Subsequently, he underwent emergent percutaneous coronary intervention (PCI) to restore blood flow in the occluded coronary artery. A drug-eluting stent was successfully placed, effectively resolving the stenosis.Recovery and Rehabilitation:Following the successful PCI, Mr. Smith's condition gradually improved. He was closely monitored in theintensive care unit for the first few days to manage potential complications and ensure optimal recovery. Physical therapy and cardiac rehabilitation were initiated early to enhance his cardiovascular fitness and prevent deconditioning. With each passing day, Mr. Smith's strength and endurance improved, and he regained his independence.Psychological Impact:While the physical recovery was remarkable, it isimportant to acknowledge the psychological impact that such a traumatic event can have on patients. Mr. Smith experienced anxiety, fear, and a sense of vulnerability during his hospitalization. A multidisciplinary team, including psychologists and social workers, provided emotional support, counseling, and education to help him cope with the psychological aftermath of the myocardial infarction. This holistic approach played a crucial role in his overall recovery.Conclusion:Mr. Smith's case demonstrates the critical importance of timely intervention, collaborative care, and comprehensive rehabilitation in achieving a successful recovery from a life-threatening medical condition. It also highlights the resilience and determination of individuals in overcoming adversity. By sharing this case report, we hope to inspire healthcare professionals to continue providing compassionate care and innovative interventions that can transform lives and restore hope.。
病历汇报英文演讲稿范文
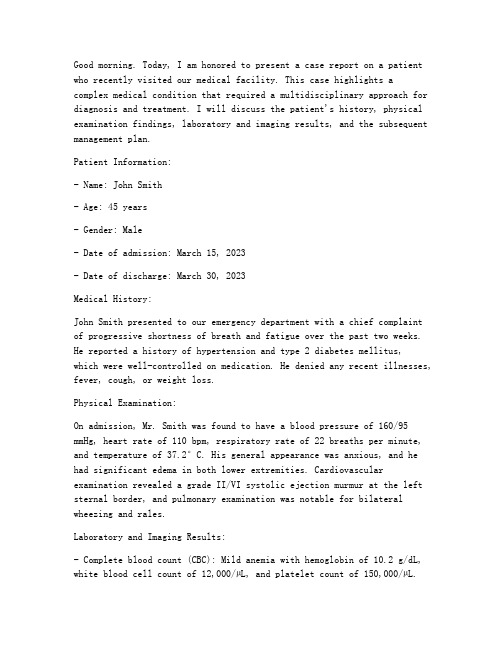
Good morning. Today, I am honored to present a case report on a patient who recently visited our medical facility. This case highlights a complex medical condition that required a multidisciplinary approach for diagnosis and treatment. I will discuss the patient's history, physical examination findings, laboratory and imaging results, and the subsequent management plan.Patient Information:- Name: John Smith- Age: 45 years- Gender: Male- Date of admission: March 15, 2023- Date of discharge: March 30, 2023Medical History:John Smith presented to our emergency department with a chief complaint of progressive shortness of breath and fatigue over the past two weeks. He reported a history of hypertension and type 2 diabetes mellitus,which were well-controlled on medication. He denied any recent illnesses, fever, cough, or weight loss.Physical Examination:On admission, Mr. Smith was found to have a blood pressure of 160/95 mmHg, heart rate of 110 bpm, respiratory rate of 22 breaths per minute, and tempera ture of 37.2°C. His general appearance was anxious, and he had significant edema in both lower extremities. Cardiovascular examination revealed a grade II/VI systolic ejection murmur at the left sternal border, and pulmonary examination was notable for bilateral wheezing and rales.Laboratory and Imaging Results:- Complete blood count (CBC): Mild anemia with hemoglobin of 10.2 g/dL, white blood cell count of 12,000/µL, and platelet count of 150,000/µL.- Electrolytes, renal function tests, and liver function tests were within normal limits.- Serologic tests for HIV, hepatitis B, and hepatitis C were negative.- Chest X-ray: Bilateral pulmonary edema and cardiomegaly.- Echocardiogram: Severe left ventricular dysfunction with an ejection fraction of 25%.- CT scan of the chest: Pulmonary embolism involving the left main pulmonary artery.Diagnosis:Based on the clinical presentation, laboratory findings, and imaging results, the patient was diagnosed with acute pulmonary embolism (PE) with secondary pulmonary hypertension and left ventricular dysfunction.Management Plan:- Anticoagulation therapy with heparin and apixaban was initiated to prevent further thromboembolic events.- Mechanical ventilation was required due to severe respiratory distress.- Inotropic support was provided to manage hypotension and improve cardiac output.- Treatment for secondary pulmonary hypertension included diuretics, nitrates, and inhaled bronchodilators.- Antibiotics were prescribed for a suspected lower respiratory tract infection.- The patient was also started on a low-sodium diet and received education on fluid management.Outcome:After a week of intensive care, Mr. Smith's clinical status improved significantly. His respiratory distress resolved, and he was able to beweaned off mechanical ventilation. His blood pressure stabilized, and the inotropic support was discontinued. By the time of discharge, his ejection fraction had improved to 30%, and he was discharged on apixaban and hydrochlorothiazide to manage his hypertension and diabetes.Conclusion:This case report illustrates the importance of early diagnosis and treatment of pulmonary embolism, which can be a life-threatening condition. The multidisciplinary approach, including emergency medicine, cardiology, pulmonology, and critical care, was crucial in managing this complex case. Mr. Smith's recovery demonstrates the potential for successful outcomes with appropriate medical intervention.Thank you for your attention, and I would be happy to answer any questions you may have.。
病例报告英文范文医护英语
病例报告英文范文医护英语Title: Case Report: Management of a Complex Surgical Case with Multi-system Involvement.Introduction:Surgical cases with multi-system involvement present unique challenges to the treating healthcare team. This case report outlines the management of a complex surgical case with involvement of multiple organ systems, highlighting the importance of interdisciplinary collaboration and comprehensive preoperative planning.Case Presentation:The patient, a 56-year-old male with a history of hypertension and type 2 diabetes, presented to the emergency department with complaints of severe abdominal pain and distension. Initial evaluation revealed a large abdominal mass with ascites. Computed tomography (CT) scanconfirmed the presence of a large, complex abdominal mass with extension into the retroperitoneum, compressing the adjacent organs and vessels.Diagnostic Workup:The patient underwent a series of diagnostic tests including blood work, imaging studies, and consultations with various specialists. The laboratory tests revealed anemia and elevated liver enzymes. The imaging studies, including CT scan and magnetic resonance imaging (MRI), demonstrated a large mass with heterogeneous enhancement, compressing the adjacent organs and vessels. The mass was suspected to be a malignant neoplasm, possibly originating from the pancreas or adrenal glands.Preoperative Planning:Given the complexity of the case and the involvement of multiple organ systems, a preoperative planning meeting was held with the surgeons, anesthesiologists, intensivists, radiologists, pathologists, and oncology team. The plan wasto perform a laparotomy with excision of the mass, followed by reconstruction of the affected organs and vessels. The anesthesiologists recommended a general anesthetic with invasive monitoring, while the intensivists recommended postoperative admission to the intensive care unit (ICU)for close monitoring.Surgical Procedure:The laparotomy was performed through a midline incision. Intraoperatively, the mass was found to be adherent to multiple organs and vessels, including the liver, spleen, kidney, and inferior vena cava. Careful dissection was performed to separate the mass from the adjacent structures, while preserving the vascular integrity. The mass was successfully excised, and the affected organs were reconstructed using sutures and patches. The patient tolerated the procedure well, and hemostasis was achieved.Postoperative Course:The patient was admitted to the ICU for closemonitoring. Postoperatively, he developed transient respiratory failure and required mechanical ventilation. He also developed wound dehiscence due to the extensive surgical dissection. The ICU team managed the patient's respiratory status and provided wound care. The patient gradually improved and was extubated on the third postoperative day. He was transferred to the general surgical floor on the fifth postoperative day and discharged home on the tenth postoperative day.Pathological Analysis:The pathological examination of the excised mass revealed a poorly differentiated adenocarcinoma, likely originating from the pancreas. The surgical margins were negative for tumor involvement. The patient was referred to the oncology team for further management, including adjuvant chemotherapy and follow-up surveillance.Conclusion:This case report demonstrates the successful managementof a complex surgical case with multi-system involvement. The interdisciplinary collaboration and comprehensive preoperative planning were essential for achieving a successful outcome. The case highlights the importance of a multidisciplinary approach in the management of complex surgical cases, ensuring optimal patient care.。
英语病例报告范文
英语病例报告范文Case Report: A Rare Case of Acute Myeloid Leukemia with Unusual Presentation。
Introduction:Acute Myeloid Leukemia (AML) is a malignant disorder characterized by the proliferation of abnormal myeloid cells in the bone marrow. It typically presents with symptoms such as fatigue, fever, and easy bruising. However, in some rare cases, AML can manifest with atypical symptoms, leading to diagnostic challenges. This report presents a unique case of AML with an unusual presentation.Case Presentation:A 45-year-old male presented to the emergency department with complaints of severe headaches, dizziness, and blurred vision. He had a history of chronic migraines and was initially treated for a severe migraine attack. However, his symptoms did not improve with standard migraine medications. On further evaluation, the patient was found to have profound anemia, with a hemoglobin level of 6 g/dL.Investigations:A complete blood count revealed severe pancytopenia, with a white blood cell count of 1.2 × 10^9/L, hemoglobin of 6 g/dL, and platelet count of 50 × 10^9/L. Peripheral blood smear examination showed blasts comprising 70% of the total nucleated cells, suggesting the possibility of acute leukemia. Bone marrow aspiration and biopsy were performed to confirm the diagnosis.Diagnosis:The bone marrow examination revealed hypercellularity with infiltration of blasts comprising more than 80% of the nucleated cells. Flow cytometry analysis showed expression of myeloid markers (CD13, CD33) and absence of lymphoid markers,confirming the diagnosis of acute myeloid leukemia. Cytogenetic analysis revealed the presence of a complex karyotype, which is associated with a poor prognosis.Treatment and Outcome:The patient was promptly started on induction chemotherapy with a combination of cytarabine and daunorubicin. He experienced severe myelosuppression and required supportive care, including red blood cell and platelet transfusions. Despite the initial response to chemotherapy, the patient developed refractory disease and relapsed within six months of completing consolidation therapy. Salvage chemotherapy and allogeneic stem cell transplantation were considered, but the patient declined further treatment due to poor prognosis and opted for palliative care.Discussion:This case highlights the importance of considering acute leukemia in the differential diagnosis of atypical presentations, even in the absence of classic symptoms. The unusual symptoms of severe headaches, dizziness, and blurred vision initially misled the clinicians to suspect migraine as the primary cause. However, the presence of profound anemia and pancytopenia raised suspicion of an underlying hematological disorder. Timely evaluation and appropriate diagnostic tests, including bone marrow examination, were crucial in establishing the correct diagnosis.Conclusion:This case report emphasizes the need for a high index of suspicion for acute leukemia, especially in patients presenting with unusual symptoms. Prompt diagnosis and initiation of appropriate treatment are essential for improving patient outcomes. Further research is warranted to better understand the underlying mechanisms of atypical presentations in AML and to develop targeted therapies for patients with poor prognostic factors.。
病例报告英语作文模板高中

病例报告英语作文模板高中Title: A Case Report: The Symptoms, Diagnosis, and Treatment of Influenza。
Introduction:Influenza, commonly known as the flu, is a contagious respiratory illness caused by influenza viruses. It can cause mild to severe illness and even lead to hospitalization or death, especially in high-risk groups. Here, we present a case report of a patient with influenza, detailing their symptoms, diagnosis, and treatment.Patient History:The patient, a 35-year-old male, presented to theclinic with complaints of fever, cough, sore throat, body aches, fatigue, and headache. The symptoms had started suddenly two days prior to the visit and had progressively worsened. The patient denied any recent travel history orcontact with sick individuals but reported exposure to crowded areas due to work.Clinical Examination:On examination, the patient appeared ill and fatigued. Vital signs revealed a temperature of 39.2°C (102.5°F), heart rate of 100 beats per minute, respiratory rate of 22 breaths per minute, and blood pressure within normal limits. Examination of the respiratory system revealed bilateral coarse crackles on auscultation.Diagnostic Evaluation:Given the patient's clinical presentation during the influenza season, a presumptive diagnosis of influenza was made. Nasopharyngeal swab specimens were collected for laboratory confirmation. Rapid influenza diagnostic tests (RIDTs) were performed, which yielded positive results for influenza A virus. Additionally, reverse transcription-polymerase chain reaction (RT-PCR) testing confirmed the presence of influenza A virus subtype H3N2.Treatment:Based on the diagnosis of influenza A, the patient was initiated on antiviral therapy with oseltamivir (Tamiflu). The treatment regimen included oral oseltamivir 75 mg twice daily for a duration of five days. In addition, supportive measures were implemented to alleviate symptoms and prevent complications. These measures included adequate hydration, rest, and over-the-counter analgesics for fever and body aches.Clinical Course:Following initiation of antiviral therapy and supportive measures, the patient's symptoms gradually improved over the course of the next week. Fever subsided within 48 hours of starting oseltamivir, and respiratory symptoms began to resolve. The patient was advised to complete the full course of antiviral therapy and to follow up if symptoms persisted or worsened.Discussion:Influenza is a common viral illness characterized by respiratory symptoms and systemic manifestations. It is typically diagnosed based on clinical presentation and confirmed by laboratory testing. Early initiation of antiviral therapy, such as oseltamivir, can reduce the severity and duration of symptoms, especially if started within 48 hours of symptom onset. Supportive measures play a crucial role in managing influenza, particularly in alleviating symptoms and preventing complications.Conclusion:This case report highlights the clinical presentation, diagnosis, and management of influenza in a young adult male. Prompt recognition of symptoms, timely diagnosis, and initiation of appropriate treatment are essential in managing influenza and preventing its spread in the community. Healthcare providers should remain vigilant during influenza season and advocate for vaccination as themost effective preventive measure against influenza infection.。
病例报告英语范文
病例报告英语范文深度解析与中文对照**[English Version]****Case Report: Unusual Manifestations of Acute Appendicitis in a Pediatric Patient****Abstract** This case report presents an unusual case of acute appendicitis in a 12-year-old male patient. The patient presented with atypical symptoms, making the initial diagnosis challenging. The aim of this report is to highlight the importance of clinical suspicion and thorough investigation in diagnosing uncommon presentations of common conditions.**Introduction** Acute appendicitis is a common surgical emergency, typically presenting with right lower quadrant abdominal pain, fever, and leukocytosis. However, atypical presentations are not uncommon, especially in pediatric patients. This case report describes an instance where the classic symptoms were absent, leading to delayed diagnosis.**Case Presentation** A 12-year-old male patient presented to the emergency department with a history ofvague abdominal discomfort for the past three days. Thepain was intermittent and located in the epigastric region, radiating to the back. The patient had no history of fever, vomiting, or changes in bowel habits. Physical examination revealed mild tenderness in the epigastric region, with no rebound tenderness or guarding. Laboratory tests were remarkable for a mildly elevated white blood cell count.Initial differential diagnosis included gastroenteritis, urinary tract infection, and pancreatitis. However, due to persistent abdominal discomfort and the presence of mild leukocytosis, the possibility of appendicitis was entertained. Abdominal ultrasound revealed a distended appendix with peri-appendiceal fluid, confirming the diagnosis of acute appendicitis.**Discussion** This case highlights the challenges in diagnosing acute appendicitis in pediatric patients, especially when the classic symptoms are absent. Clinicians must maintain a high index of suspicion, consideringatypical presentations, especially in children. Detailed history, thorough physical examination, and appropriatediagnostic testing are crucial in making an accurate diagnosis.**Conclusion** Acute appendicitis can present with atypical symptoms in pediatric patients, making diagnosis challenging. Clinicians should be aware of these presentations and utilize diagnostic tools such as ultrasound to aid in the prompt and accurate diagnosis of appendicitis. Prompt surgical intervention is essential to prevent complications and ensure patient recovery.**[Chinese Version]****病例报告:儿童急性阑尾炎的非典型表现****摘要** 本病例报告介绍了一名12岁男性患者的急性阑尾炎非典型表现。
英文病例报告作文范文
英文病例报告作文范文Case Report: Unusual Stomach Trouble.Man, 45, keeps saying his stomach hurts and he vomits sometimes. He's been like this for half a year, even after trying different meds. He hasn't changed his eating or lifestyle, so what's the problem? When we checked him out, his stomach area was a bit tender, but nothing else unusual.The lab tests showed his liver enzymes were up and he had a bit of anemia. The ultrasound of his belly showed his stomach wall was thicker than normal, like he might have chronic gastritis. But when we did an endoscopy, we saw something weird: there were little sores all over his stomach lining. It didn't look like a regular ulcer.We thought of a few other possibilities: maybe it's Crohn's disease or an autoimmune problem with his stomach. Or could it be eosinophilic gastroenteritis? Since his symptoms were so unusual and the regular treatments didn'twork, we decided to do a biopsy. And guess what? It showed there were a lot of eosinophils in his stomach lining, which means he has eosinophilic gastroenteritis.After starting him on corticosteroids, he felt much better in just two weeks. His stomach pain went away and he didn't vomit as much. When we checked his stomach again three months later, all the sores had healed up. It was a relief to see the treatment worked so well.This case really shows you can't always trust first impressions. Even if a patient's symptoms seem like a common problem, they might be something else entirely. It's always worth doing a thorough investigation to get theright diagnosis and the right treatment.。
英文版病例汇报

Chest CT
Chest CT
2015.05.28 Pelvic CT
2015.05.28 Pelvic CT
Present diagnosis
Rectal cancer after resection pT4aN0M0 ⅡB
Liver metastasis
Harbin Medical University cancer hospital
Present history
Tumor marker after Chem15.05.29
Before chemotherapy
113.2
168.2
135.3
157.7
CEA:0-5ng/ml CA199:0-37U/ml
2015.06.23
1 course later
Harbin Medical University cancer hospital
Present history
The pathologic diagnosis • Rectal: moderately differentiated adenocarcinoma and mucinous adenocarcinoma with disc protrude type • Invading wall of intestine • A negative upper margin of resection • Number of positive lymph nodes 0/22
• XELOX *1 Cycles Oxaliplatin 200mg d1 ivgtt; Capecitabine 1500mg am 2000mg pm d1-14 po; Repeated every 3 weeks
医学病例报告英语作文
医学病例报告英语作文Title: Medical Case Report A Rare Neurological Disorder。
Introduction:This case report discusses a rare neurological disorder called Moyamoya disease. The patient, a 32-year-old female, presented with recurring episodes of transient ischemic attacks (TIAs) and was diagnosed with this condition. This report aims to provide a comprehensive understanding of the disease, its clinical presentation, diagnostic procedures, treatment options, and prognosis.Clinical Presentation:The patient initially complained of frequent headaches, dizziness, and difficulty speaking. She also experienced weakness and numbness on the right side of her body. The symptoms worsened over time, leading to multiple episodesof TIAs. The patient's medical history revealed nosignificant risk factors for stroke, such as hypertension or diabetes.Diagnostic Procedures:The diagnostic workup included a detailed medical history, physical examination, and various imaging studies. Magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA) revealed bilateral stenosis of the distal internal carotid arteries and the proximal anterior cerebral arteries. These findings were consistent with Moyamoya disease.Treatment:The treatment plan for the patient involved a multidisciplinary approach. Medications, including antiplatelet agents and anticoagulants, were prescribed to prevent further TIAs and stroke. Additionally, the patient underwent surgical revascularization to improve blood flow to the affected areas of the brain. Direct and indirect bypass procedures were performed to establish collateralcirculation.Prognosis:The prognosis for patients with Moyamoya disease varies depending on several factors, including the severity of symptoms, age at diagnosis, and promptness of treatment. Early diagnosis and intervention can significantly improve outcomes and reduce the risk of stroke. Regular follow-up visits and close monitoring of the patient's condition are essential to manage any potential complications and ensure optimal long-term outcomes.Discussion:Moyamoya disease is a rare cerebrovascular disorder characterized by progressive narrowing of the internal carotid arteries and the development of collateral blood vessels. It primarily affects children and young adults, with a higher prevalence in individuals of Asian descent. The exact cause of the disease remains unknown, although genetic and environmental factors are believed to play arole.Conclusion:Moyamoya disease is a rare neurological disorder that requires early recognition and appropriate management to prevent potentially devastating complications such as stroke. This case report highlights the importance of a comprehensive diagnostic approach and multidisciplinary treatment strategies. Further research is needed to better understand the pathogenesis and develop novel therapeutic interventions for this challenging condition.。
英文病例报告作文范文
英文病例报告作文范文英文回答:Case Report:Patient History:The patient is a 45-year-old male who presented to the clinic with complaints of chest pain and shortness of breath. He reported a history of smoking and a familyhistory of heart disease. The patient also mentioned experiencing occasional dizziness and fatigue.Physical Examination:On physical examination, the patient appeared pale and diaphoretic. His blood pressure was elevated at 160/90 mmHg, and his heart rate was 110 beats per minute. Auscultation revealed a systolic murmur and crackles in the lungs.Diagnostic Tests:An electrocardiogram (ECG) showed ST-segment depression in leads V1 to V4, suggestive of myocardial ischemia. Cardiac enzymes were elevated, indicating myocardial damage.A chest X-ray revealed pulmonary congestion and cardiomegaly.Diagnosis:Based on the clinical presentation and diagnostic findings, the patient was diagnosed with acute coronary syndrome (ACS) and congestive heart failure (CHF).Treatment:The patient was admitted to the cardiac care unit and started on oxygen therapy, nitroglycerin, and aspirin. He also received intravenous diuretics for the management of pulmonary edema. Coronary angiography was performed, revealing severe stenosis in the left anterior descending artery. The patient underwent percutaneous coronaryintervention (PCI) with stent placement.Follow-Up:The patient's symptoms improved with treatment, and he was discharged on a regimen of beta-blockers, angiotensin-converting enzyme (ACE) inhibitors, and statins. He was advised to quit smoking and adopt a heart-healthy lifestyle.中文回答:病例报告:病史:患者为45岁男性,主诉胸痛和气促前来就诊。
英文病例报告作文范文

英文病例报告作文范文英文:Case Report: A Patient with Abdominal Pain。
I recently saw a patient, a 35-year-old female, who presented with severe abdominal pain. She reported that the pain had started suddenly and was located in the lowerright quadrant of her abdomen. She also reported nausea and vomiting.Upon examination, I noted that her abdomen was tender to the touch and that she had rebound tenderness in the lower right quadrant. Based on these findings, I suspected that she had appendicitis.I ordered a CT scan of her abdomen, which confirmed my suspicion. The scan showed an enlarged appendix with signs of inflammation.I immediately admitted the patient to the hospital and consulted with a surgeon. The patient underwent an appendectomy, and her recovery was uneventful.This case highlights the importance of prompt diagnosis and treatment of appendicitis. If left untreated, appendicitis can lead to serious complications, such as a ruptured appendix and peritonitis.中文:病例报告,一位患有腹痛的患者。
关于三个病人病历的报告英语作文
关于三个病人病历的报告英语作文英文回答:Case 1:A 65-year-old male with a history of hypertension and hyperlipidemia presents with a chief complaint of progressive shortness of breath and fatigue. He has been experiencing exertional dyspnea for the past 6 months, which has gradually worsened over the past few weeks. He now has difficulty walking up a flight of stairs without stopping to rest. He also complains of fatigue and decreased exercise tolerance.Physical examination reveals an obese male with a blood pressure of 150/90 mmHg, a heart rate of 90 bpm, and a respiratory rate of 20 breaths per minute. Auscultation of the chest reveals bibasilar crackles.Chest X-ray shows cardiomegaly and interstitial edema.Echocardiogram demonstrates a left ventricular ejection fraction of 40% and mild mitral regurgitation.Diagnosis:Heart failure with preserved ejection fraction (HFpEF)。
英语病例报告范文

英语病例报告范文I am writing to provide a case report of a patient who presented with symptoms of chest pain and shortness of breath. The patient, a 55-year-old man, arrived at the emergency department complaining of sudden onset chest pain that radiated to his left arm. 本文将介绍一位55岁男性患者的病例报告,该患者出现胸痛和呼吸困难症状。
这位患者突然出现胸痛,疼痛向左臂放射。
Upon arrival, the patient was noted to be diaphoretic and tachypneic, with a blood pressure of 150/90 mmHg and a heart rate of 110 beats per minute. Further assessment revealed he had a history of hypertension and smoking. High-sensitivity troponin levels were elevated, indicating a possible myocardial infarction. 到达医院后,患者被发现出现出汗和呼吸急促的症状,血压为150/90mmHg,心率为每分钟110次。
进一步评估显示他有高血压和吸烟史。
高敏肌钙蛋白水平升高,提示可能发生心肌梗死。
The patient was immediately started on oxygen therapy and given aspirin and nitroglycerin for symptom relief. An ECG showed ST-segment elevations in leads II, III, and aVF, suggestive of an inferiormyocardial infarction. He was promptly taken to the catheterization lab for emergent angiography. 患者立即开始吸氧疗法,并服用阿司匹林和硝化甘油缓解症状。
写英语病例报告的作文模板

写英语病例报告的作文模板英文回答:Case Report。
Title: A Case of Acute Ischemic Stroke in a 65-Year-Old Male。
Patient Information。
Name: John Doe。
Age: 65 years。
Sex: Male。
Occupation: Retired engineer。
Chief Complaint。
Sudden onset of left-sided weakness and numbness。
History of Present Illness。
The patient awoke this morning with sudden onset of left-sided weakness and numbness. He also complained of a headache and difficulty speaking.He has no known history of hypertension, diabetes, or hyperlipidemia.He is a former smoker and drinks alcohol occasionally.Physical Examination。
Vital signs:Blood pressure: 160/90 mmHg。
Pulse: 80 beats per minute。
Respiratory rate: 16 breaths per minute。
Temperature: 98.6°F。
Neurological examination:Left-sided weakness (4/5)。
Left-sided numbness。
Aphasia。
No neglect。
Laboratory Studies。
CBC: Normal。
英语病例报告作文
英语病例报告作文Medical Case Report: A Rare Case of Acute Myeloid Leukemia in a Young Adult。
Abstract:Acute myeloid leukemia (AML) is a rare and aggressive form of cancer that affects the blood and bone marrow. Itis characterized by the rapid growth of abnormal white blood cells, which can interfere with the normal production of red blood cells, platelets, and other white blood cells. This case report presents the clinical and laboratory findings of a 25-year-old male patient who was diagnosed with AML. The patient's symptoms, diagnostic tests, treatment, and outcomes are discussed in detail.Introduction:AML is a relatively rare form of leukemia, accounting for approximately 1% of all cancer diagnoses. It typicallyoccurs in older adults, with a median age at diagnosis of 68 years. However, AML can also affect younger individuals, as demonstrated by the case of the 25-year-old male patient described in this report. The incidence of AML in young adults is low, and the disease is often more aggressive and difficult to treat in this population.Case Presentation:The patient presented to the hospital with complaints of fatigue, shortness of breath, and easy bruising. He reported a 3-month history of progressively worsening symptoms, including fever, night sweats, and weight loss. On physical examination, the patient appeared pale and had petechiae and ecchymoses on his skin. Laboratory tests revealed pancytopenia, with a white blood cell count of 1.2 × 109/L, hemoglobin level of 8.5 g/dL, and platelet count of 45 × 109/L. A peripheral blood smear showed the presence of blast cells, which raised suspicion for leukemia. Further testing, including bone marrow aspiration and biopsy, confirmed the diagnosis of AML.Treatment and Outcome:The patient was started on induction chemotherapy with a regimen of cytarabine and daunorubicin. He experienced severe myelosuppression and required supportive care with transfusions of red blood cells and platelets. Despite initial improvement in his blood counts, the patient developed febrile neutropenia and was found to have a bloodstream infection with a multidrug-resistant organism. He was treated with broad-spectrum antibiotics and antifungal agents, but his condition continued to deteriorate. Unfortunately, the patient succumbed to complications of his leukemia and infection, and he passed away 2 months after his initial presentation.Discussion:This case highlights the challenges of managing AML in young adults. The disease is often more aggressive and refractory to treatment in this population, leading to poor outcomes. In addition, the patient's susceptibility to infections due to severe myelosuppression furthercomplicated his clinical course. This case underscores the need for more effective and less toxic therapies for AML, particularly in young patients who may be more resilient to aggressive treatment approaches.Conclusion:Acute myeloid leukemia is a rare and aggressive form of cancer that can affect individuals of all ages. This case report illustrates the challenges of diagnosing andtreating AML in a young adult, and it emphasizes the needfor further research to improve outcomes in this population. Healthcare providers should be aware of the unique clinical characteristics of AML in young patients and strive to develop more effective and less toxic therapies for this challenging disease.。
case report范文

case report范文Case Report: A Rare Presentation of Gastrointestinal Stromal TumorIntroductionGastrointestinal stromal tumors (GISTs) are mesenchymal neoplasms that arise from the interstitial cells of Cajal or their precursors. They are relatively uncommon, accounting for less than 1% of all gastrointestinal malignancies. This case report presents an unusual case of a GIST with a rare presentation and discusses its diagnosis, management, and outcome.Case PresentationA 52-year-old male presented to our hospital with a history of abdominal discomfort and weight loss over the past three months. Physical examination revealed a palpable abdominal mass in the right upper quadrant. Laboratory tests were within normal limits. Abdominal ultrasonography showed a heterogeneous mass in the liver, suggestive of a metastaticlesion. Computed tomography (CT) scan of the abdomen revealed a large mass in the right lobe of the liver with multiple smaller lesions scattered throughout both lobes. There was also evidence of peritoneal seeding.The patient underwent a laparotomy, which revealed a large, firm, and encapsulated mass in the right lobe of the liver. The mass was resected along with a segment of the liver. Intraoperatively, there was no evidence of peritoneal metastasis. Histopathological examination of the resected specimen revealed a spindle cell neoplasm with mitoses and atypical cells. Immunohistochemistry staining was positive for CD117 (c-kit) and DOG-1, confirming the diagnosis of GIST.Postoperatively, the patient recovered well and was discharged on the seventh postoperative day. He was started on imatinib mesylate (Gleevec) as adjuvant therapy. Follow-up CT scans showed no evidence of recurrence or metastasis at six months and one year post-surgery.DiscussionGISTs can occur anywhere in the gastrointestinal tract, but they are most commonly found in the stomach (60-70%) and small intestine (20-30%). They typically present as asymptomatic masses and are often diagnosed incidentally. However, symptoms can include abdominal pain, weight loss, and gastrointestinal bleeding. Metastasis is common, and the liver is the most frequent site of involvement.The diagnosis of GIST is confirmed by histopathological examination and immunohistochemistry staining. Surgical resection is the primary treatment modality for localized GISTs. The extent of resection depends on the size and location of the tumor. Adjuvant therapy with tyrosine kinase inhibitors (TKIs) such as imatinib mesylate is recommended for patients with high-risk features, including large tumor size, high mitotic rate, and/or positive resection margins.The prognosis of GISTs varies depending on tumor size, mitotic rate, resection margins, and the presence of metastasis. Long-term survival is possible with complete resection andadjuvant therapy. Regular follow-up with CT scans is recommended to monitor for recurrence or metastasis.ConclusionThis case report highlights the importance of considering GIST in the differential diagnosis of abdominal masses. Surgical resection is the mainstay of treatment, and adjuvant therapy with TKIs improves outcomes in patients with high-risk features. Regular follow-up is crucial for early detection of recurrence or metastasis.案例报告:胃肠道间质瘤罕见病例介绍胃肠道间质瘤(GIST)是起源于卡哈尔间质细胞或其前体的间叶性肿瘤。
病例报告 英语作文
病例报告英语作文Title: A Case Report: The Diagnosis and Treatment of a Rare Medical Condition。
Abstract:This case report presents a rare medical condition of a 45-year-old patient who presented with a unique set of symptoms. The aim of this report is to describe the diagnostic process, treatment plan, and patient outcome. The case highlights the importance of a multidisciplinary approach and thorough investigation in diagnosing and managing rare medical conditions.Introduction:Rare medical conditions pose significant challenges in terms of diagnosis and treatment due to their limited prevalence and diverse clinical presentations. This case report focuses on a patient with an unusual set of symptomsthat required a comprehensive evaluation to determine the underlying cause.Case Presentation:A 45-year-old male patient presented with a three-month history of fatigue, weight loss, and intermittent fevers. The patient reported no significant medical history or family history of similar symptoms. Initial physical examination revealed enlarged lymph nodes in the neck and groin, along with hepatomegaly. Laboratory investigations showed elevated inflammatory markers and abnormal liver function tests.Diagnostic Assessment:Given the patient's symptoms and physical examination findings, a wide range of potential diagnoses were considered, including infectious, autoimmune, and neoplastic diseases. The patient underwent a series of diagnostic tests, including blood cultures, serology for infectious diseases, imaging studies, and a lymph nodebiopsy.Results:Blood cultures were negative for any bacterial orfungal growth. Serology tests ruled out common infectious diseases such as tuberculosis and HIV. Imaging studies revealed multiple enlarged lymph nodes in various regionsof the body. A lymph node biopsy was performed, and histopathological examination showed features consistentwith Castleman disease, a rare lymphoproliferative disorder. Treatment and Outcome:The patient was referred to a multidisciplinary team consisting of hematologists, oncologists, and infectious disease specialists for further management. The treatment plan included the administration of corticosteroids to alleviate symptoms and reduce inflammation. Additionally,the patient received targeted therapy with rituximab, a monoclonal antibody, to target the abnormal lymphocytes.Over the course of several months, the patient showed significant improvement in symptoms, with a reduction in lymph node size and normalization of liver function tests. Regular follow-up visits were scheduled to monitor the patient's progress and adjust the treatment plan as necessary.Discussion:Castleman disease is a rare disorder characterized by abnormal lymph node enlargement and systemic symptoms. The diagnosis of this condition requires a combination of clinical suspicion, thorough investigation, and histopathological examination. Treatment options vary depending on the subtype of Castleman disease and may include surgery, chemotherapy, or targeted therapy.Conclusion:This case report highlights the importance of a multidisciplinary approach in diagnosing and managing rare medical conditions. The successful diagnosis and treatmentof Castleman disease in this patient demonstrate the significance of thorough investigation, collaboration among healthcare professionals, and individualized treatment plans. Further research is needed to enhance our understanding of rare medical conditions and improvepatient outcomes.。
英语作文病人案例报告
英语作文病人案例报告Title: Patient Case Report: A Journey Towards Recovery。
Introduction:In this report, we delve into the case of a patient who presented with a complex medical condition, requiring comprehensive care and management. The patient's journey towards recovery showcases the collaborative efforts of healthcare professionals and highlights the importance of individualized treatment plans.Case Presentation:Mr. X, a 45-year-old male, was admitted to our hospital with complaints of severe abdominal pain, fatigue, and unintentional weight loss over the past six months. Upon initial assessment, Mr. X appeared pale and fatigued, with signs of dehydration. Laboratory investigations revealed elevated inflammatory markers and abnormal liver functiontests.Medical History:Mr. X had a significant medical history, including chronic hepatitis B infection and a previous diagnosis of ulcerative colitis. He had been non-compliant with his prescribed medications and follow-up appointments, which likely contributed to the exacerbation of his conditions.Diagnostic Workup:A series of diagnostic tests were conducted to further evaluate Mr. X's condition. Imaging studies, including abdominal ultrasound and CT scans, revealed evidence of liver cirrhosis and colonic inflammation consistent with ulcerative colitis. Additionally, serological tests confirmed active hepatitisB infection.Treatment Plan:Given the complexity of Mr. X's condition, amultidisciplinary team comprising gastroenterologists, hepatologists, and infectious disease specialists was convened to develop a comprehensive treatment plan. The goals of therapy were to manage his symptoms, control inflammation, and prevent disease progression.Mr. X was initiated on a regimen of oral andintravenous medications, including corticosteroids for ulcerative colitis flare, antiviral therapy for hepatitis B, and supportive measures to address nutritional deficiencies and fluid imbalance. Close monitoring of liver function,viral load, and disease activity was instituted to guide treatment adjustments.Clinical Course:Throughout his hospitalization, Mr. X demonstrated gradual improvement in his symptoms and biochemical parameters. His abdominal pain subsided, and his energy levels improved with adequate hydration and nutritional support. Serial imaging studies showed stabilization ofliver cirrhosis and resolution of colonic inflammation.However, Mr. X's progress was not without challenges. He experienced adverse effects from some medications, including corticosteroid-induced hyperglycemia and electrolyte disturbances, which required promptintervention and adjustment of therapy. Moreover, addressing his non-adherence to treatment and follow-up remained a significant concern for long-term management.Outcome:After an extended hospital stay and intensive medical management, Mr. X was discharged with a tailored treatment plan and comprehensive follow-up arrangements. He was counseled extensively on the importance of medication adherence, lifestyle modifications, and regular monitoring to optimize his health outcomes.Follow-Up:In the months following discharge, Mr. X continued to be followed closely by his healthcare team. He demonstratedsustained improvement in his clinical condition, with well-controlled disease activity and stable liver function. Through ongoing education and support, efforts were made to empower Mr. X to take an active role in managing his health and preventing disease complications.Conclusion:The case of Mr. X underscores the intricate interplay of medical, social, and behavioral factors in the management of complex medical conditions. By employing a multidisciplinary approach and individualized treatment strategies, significant progress can be achieved in improving patient outcomes and quality of life. Moving forward, continued efforts are needed to address barriers to care and promote patient engagement in their health journey.[word count: 561]。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
出生/妊娠情况∙was the first child born to unrelated healthy parents after a full-term pregnancy.∙The patient was born after a full-term pregnancy by caesarean section because of premature rupture of the membranes足月、剖腹产、胎膜早破∙she spontaneously breathed and cried.∙The proposita, a 15-year-old girl, was the product of the fifth full-term pregnancy.∙Polyhydramnios was present in the third trimester. 晚期妊娠羊水过多∙Anthropometrical data recorded at birth were: weight 1700g ( < 3rd centile) and height 40cm ( < 3rd centile).∙He was the first child of a nonconsanguineous 非近亲结婚Turkish couple born at term by normal spontaneous vaginal delivery. 顺产∙This 13-year-old boy was born to non-consanguineous Pakistani parents by Caesarean section and weighed 3.6 kg (50th centile) at birth.∙She was delivered by Cesarean for failure to progress 停育at 37 weeks’ gestation.∙Pregnancy was characterized by intrauterine growth retardation宫内发育迟缓, nuchal thickness, and turbidity of amniotic fluid requiring a caesarean birth at the 39th week of gestation.∙short femora 股骨短家人情况∙Her younger sister is healthy.∙ A 13-year-old girl was the second child born to a 42-yearold mother and an unrelated 43-year-old father∙There was no family history of short stature, mental deficiency or congenital anomalies∙He is the only affected member in his pedigree∙At the time of his birth, his father was 35 year-old, 170 cm tall, his mother was32 year-old, 157 cm tall and obese.∙He had two brothers; one was obese but had neither learning difficulties nor visual impairment.生长发育∙Her developmental milestones were normal∙At 11.5 years of age, her height was 129 cm ( – 3 SD), weight 29 kg ( – 1.5 SD), and occipitofrontal circumference 49 cm ( – 2.75 SD).∙Along with her cognitive profile, she showed difficulty in mathematics, reading and writing. 学习困难∙His height and weight have remained markedly below the 3rd percentile∙His height and weight have always been below the 3rd percentile∙Stature (115 cm, 10–25th centile) was disproportionate to the weight (30 kg, 97th centile)∙病情发现∙We call attention to∙Soon after birth, were noted.∙She attained menarche at∙The patient exhibited a full MS phenotype of the clinical and radiological criteria reported in MS, including∙Multiple/ Several congenital anomalies were noted at birth including cleft lip and palate唇腭裂, left facial paralysis左面部瘫痪, systolic heart murmur左面部瘫痪, pilonidal dimple, hypospadias with meatal stricture尿道下裂, congenital phimosis先天性包茎, right crytorchidism右隐睾and inguinal hernia腹股沟疝.∙Hypertension was documented at age 1 1 years∙Marked hyperopia was found on an ophthalmologic examination at age 21 years ∙At age 1 year he was felt to be developmentally delayed∙From infancy the mother noticed the existence of hearing-loss which remained untreated until adolescence.∙He has hypernasal speech because of adenoid hypertrophy.∙From age 3 years he frequently refused to walk complaining of painful legs.就诊原因∙She was referred to us for investigating her short stature at the age of 10 years ∙He was admitted to a state institution for the mentally retarded at age 30 years with ∙He was first referred to a pediatric nutritionist at the age of seven years for the exploration and management of polyphagia and obesity.∙He presented to endocrine clinic at age 11 for short stature and precocious puberty (onset at age 10), and had elevated FSH, and an enlarged left testis.∙特殊面容Craniofacial features/ Craniofacial features∙She had a flat wide facies with prominent prognathism, blepharophimosis, anda narrow mouth with a thin vermilion of the upper lip∙She had a short stature and an unusual square-shaped body habitus with horizontal position of the clavicles and shoulders along with a short neck∙flat wide facies with upward slanting palpebral fissures, blepharophimosis, and a flat nasal bridge with hypoplastic left nares and flat maxillary regions.∙She had a muscular build肌肉身材, brachycephaly短头畸形, frontal bossing 额部隆起, hypertelorism眼距过宽, a broad and prominent nasal bridge宽鼻梁, deep-set eyes 凹眼with short palpebral fissures短睑裂, midfacial hypoplasia面中部发育不良, small external ears小外耳, a short philtrum短人中, a narrow mouth窄嘴, a thin upper lip上嘴唇薄, downturned corners to the mouth嘴角向下翘, hypoplastic teeth发育不全的牙齿, a high palate高上腭, prognathism凸颚, a short neck短颈, Tanner III breast development and external genitalia, short upper limbs 短上肢(rhizo-acromelic shortening), cubitus valgus肘外翻, brachydactyly of the hands and feet手脚短指, clinodactyly of the fifth fingers指过弯, generalized nail dysplasia指甲发育不良, and normal skin and joint movements∙Facial dysmorphism indicative of Myhre syndrome included short palpebral fissures with ptosis, a flat face with mid-face hypoplasia, prognathism and a high arched palate∙Facial and limb morphology further suggested the diagnosis of MS检查∙Audiological examination revealed mixed conductive and sensorial hearing loss∙Radiological examination revealed a thick calvarium, mandibular protrusion,, shortening of the tubular bones, and large pedicles and thick neural arches, resulting in a narrow spinal canal.∙MRI showed thick basilar bone and large and thick clivus.∙The patient underwent a provocative test by insulin-induced hypoglycemia (ITT), thyrotropin-releasing hormone (TRH), and luteinizing hormone-releasing hormone (LHRH)∙Radiographic studies (Fig. 2) showed∙the peak GH response was∙the serum IGF-1 level was appropriate for a pubertal girl∙Physical findings at age 24 years (Fig. I) revealed/ showed a height of 140 cm, weight of 45 kg and a head circumference of 56 cm.∙On physical exam/ examination at age 18 years he had a height of 146 cm, a weight of 50.5 kg and a head circumference of 54.7 cm∙The skeletal survey showed multiple abnormalities∙His muscle mass and strength werc increased 升高∙The skeletal survey demonstrated multiple skeletal ab normalities identical to those pictiired in Case 1∙Psychological evaluation showed an IQ of 48∙ A muscle biopsy revealed fascicles of normal looking muscle fibres∙Gene sequencing analysis was carried out of all 11 coding exons of SMAD4 using the MiSeq next-generation sequencing platform∙Musculoskeletal examination revealed generalised stiff muscles, limited phalangeal extension∙Neurological examination was normal apart from clumsy gait with toe walking. ∙he was normotensive (120/65 mm Hg) 血压正常∙he had mild learning difficulties that necessitated additional educational support. 特殊教育∙Dermatological assessment of the proband revealed keratosis pilaris with a clinical impression of thickened skin. 皮肤病学Skin biopsy findings confirmed∙Three additional clinical genetics evaluations failed to identify a unifying diagnosis.∙检查结果正常∙Results of the routine biochemical studies were within the normal ranges.∙Results of the screening tests for metabolic defects, including analysis of urinary mucopolysaccharides and blood amino acids were normal.∙Routine karyotyping (G-bands) showed 46,XX, and the results of the array CGH (Agilent SurePrint G3 60K) were also negative∙EMG showed no abnormalities.∙Endocrinological studies (basalthyroid profile,LH, FSH, estradiol, cortisol, and IGF-1 serum determinations,thyroid profile) showed normal results.∙No signs of polycystic ovary syndrome were identified.∙The histology of a striated muscle biopsy was normal.∙Cardiovascular evaluations began at age 3 years when a twodimensional echocardiogram showed mild valvar pulmonic stenosis, and clinical follow-up suggested resolution∙Sequencing for Kabuki and Rubinstein–Taybi syndromes, (MLL2, CREBBP, and EP300) was normal∙Psychomotor development was normal 智力,精神发育正常被诊断∙She was diagnosed with∙We propose that∙The thick calvarium and thick and stiff skin were clues to the diagnosis of MS ∙She fulfilled the clinical criteria reported for MS.∙This finding indicated that her GH secretion was not defective.∙Gonadotropin responses were not excessive or inappropriate for an early pubertal girl.治疗∙necessitating hormone replacement therapy.∙The patient was diagnosed with skeletal dysplasia of unknown origin and treated for this condition for several years∙He required surgery for right cryptorchidism at the age of 1.5 years.∙The prednisone dose was raised (1 mg/kg/day) with a good clinical response ∙mycophenolate-mofetil (500 mg twice/day) was added for two months to the prednisone therapy.∙The starting dosage of anakinra was 1 mg/kg/day, subcutaneously. 皮下注射∙年龄At the age of 15,测序∙Direct sequence analysis of the coding lesions led to the identification of three missense mutations in the region ofSMAD4 coding for the MH2 domain∙No likely pathological copy number variants (CNVs) were detected in either case 1 or his mother on a 180 K oligo array CGH报道发病情况∙All cases have been sporadic and an autosomal dominant inheritance was suggested because of advanced paternal age.青春期∙These findings suggest that endocrinological abnormalities related to the hypothalamus–hypophysis feedback may be part of the syndrome. This has been proven at least in one male patient (Case 2, Burglen et al., 2003).∙the abnormal onset of puberty observed in three of our cases, two showing early onset (before the age of 9 years) and another one showing delayed puberty with hypergonadotrophic hypogonadism. Although these phenotypic manifestations are discordant, they may point to a disturbance in the hypothalamohypophyso-gonadal axis that should be investigated in further cases.疾病∙Myhre syndrome is a rare, distinctive syndrome due to specific gain-of-function mutations in SMAD4∙The characteristic phenotype includes∙Cardiomyopathy and pericardial abnormalities distinguish Myhre syndrome from other disorders caused by mutations in the TGF-b signaling cascade (Marfan, Loeys–Dietz, or Shprintzen–Goldberg syndromes)∙Major facial features were病例报道∙We report four newly described patients with typical features of Myhre syndrome who had∙To our knowledge, the severely shortened distal phalanges, shortened third metacarpals, and shortened proximal phalanges of digit 5 have not yet been reported elsewhere as being associated with BDA1 据我们所知,在其他地方尚未报道严重缩短远端指骨,缩短第三掌骨和缩短指骨5位与BDA1相关不明were not recorded。