进展期乳癌专家共识(英文版)
中文版NCCN指南(2015_v 2版)
T4:不论肿瘤大小,直接侵犯胸壁和/或皮肤(溃疡或 皮肤结节) N2:同侧腋窝淋巴结转移,临床表现为固定或相互融 合;或缺乏同侧腋窝淋巴结转移的临床证据,但临床 上发现有同侧内乳淋巴结转移 pN2:4~9个腋窝淋巴结转移;或临床上发现内乳淋巴 结转移,但腋窝淋巴结无转移,转移病灶>2.0 mm pN2b:临床上发现内乳淋巴结转移,但腋窝淋巴结无 转移 任何T N3:同侧锁骨下淋巴结转移伴或不伴腋窝淋巴结转移; 或临床上发现同侧内乳淋巴结转移伴腋窝淋巴结转移; 或同侧锁骨上淋巴结转移伴或不伴腋窝或内乳淋巴结 转移 N3a:同侧锁骨下淋巴结转移 N3b:同侧内乳淋巴结及腋窝淋巴结转移 N3c:同侧锁骨上淋巴结转移 pN3:≥10个腋窝淋巴结转移
原发肿瘤≤0.5 cm或 原发肿瘤微浸润 pT1, pT2,或 pT3; pN0或pN1mi(腋窝 淋巴结转移灶≤2 mm)
pN0 PN1mi
组织学类型: 导管癌 小叶癌 混合型癌 化生性癌
BINV-5
仅供内部学习使用
浸润性乳腺癌
激素受体阳性、HER-2阴性的乳腺癌患者的全身辅助治疗
原发肿瘤≤0.5 cm 或原发肿瘤微浸润 pT1, pT2,或 pT3; pN0 或 pN1mi(腋窝 淋巴结转移灶≤2 mm) 组织学类 型: 导管癌 小叶癌 混合型癌 化生性癌 pN0 PN1mi 考虑辅助内分泌治疗(2B类) 辅助内分泌治疗(2B类) ±辅助化疗(2B类)
• • •
专家普遍认为,大于10 mm的切缘属阴性(但此切缘宽度也许过大,而且可能影响美观) 小于1 mm的切缘被认为不足够 对于范围在1~10 mm之间的切缘,一般切缘越宽,局部复发率越低。但是对于位于乳腺纤维-腺分界部 位(如靠近胸壁或皮肤)的肿瘤,手术边缘不足1mm并不一定要进行再次手术,但可以对肿块切除部 DCIS-1 位进行较大剂量推量照射(2B类)。 仅供内部学习使用
乳腺癌抗体偶联药物输注管理专家共识完整版

乳腺癌抗体偶联药物输注管理专家共识完整版
近年来快速发展的抗体偶联药物(antibody-drug conjugate, ADC)靶向生物制剂,是一类由单克隆抗体经由连接分子与细胞毒类药物偶联结合而组成的新型抗肿瘤药物。
ADC药物的输注规范、不良反应的预防和管理等是保证药物疗效及安全的重要前提,2023年“中国医药教育协会乳腺癌个案管理师分会”及“靶向药物输注规范共识制定小组”共同制定了《乳腺癌抗体偶联药物输注管理专家共识》,内容包括ADC 药物的输注规范、相关不良反应的早期预防和及时管理等方面。
现对其主要内容进行解读,以期为临床实践提供更全面的指导。
一、乳腺癌ADC药物配置输注标准操作流程
1. ADC药物的配置SOP
乳腺癌ADC药物静脉输注应遵循现用现配、无菌配置原则,配置流程(见图1)。
其中,TDxd和SG配置时应避光。
2. ADC药物的输注SOP
乳腺癌ADC药物整个输注过程遵循输液流程,输注流程(见图2)。
3. ADC药物输注急性反应应急SOP(见图3)
二、乳腺癌ADC药物输注管理
(一)ADC 药物输注
1. 输液装置和输液通路的选择:
(1)输液通路选择:ADC药物建议优先选择经外周静脉置入的中心静脉导管(PICC)或输液港进行输注。
(2)配置以及输液装置选择(见表1)。
(二)ADC药物保存(见表2)
三、乳腺癌ADC药物不良反应健康教育。
乳腺癌新辅助治疗专家共识(2019年版)

乳腺癌新辅助治疗专家共识(2019年版)乳腺癌新辅助治疗专家共识 (2019年版)_______________________________________________________ ____________第一章:前言1.1 编写目的1.2 文档背景1.3 文档适用范围1.4 参考文献_______________________________________________________ ____________第二章:乳腺癌新辅助治疗概述2.1 定义2.2 新辅助治疗的目的和原则2.3 治疗选择①药物治疗②放射治疗2.4 考虑因素①乳腺癌分期②基因型分析③患者整体情况2.5 监测指标①影像学评估②病理学评估③临床评估_______________________________________________________ ____________第三章:新辅助化学药物治疗3.1 化疗药物的选择①常用化疗药物②药物剂量和给药模式3.2 治疗周期和持续时间3.3 药物治疗的评估和监测①病理学反应评估②影像学反应评估③临床反应评估3.4 毒副作用管理3.5 围手术期药物治疗_______________________________________________________ ____________第四章:新辅助放射治疗4.1 放疗适应证4.2 放疗技术选择①传统放射治疗②强度调控放疗 (IMRT)③同步放化疗④部分乳房放疗4.3 放疗计划和剂量4.4 放射治疗的监测和评估4.5 放疗后并发症管理_______________________________________________________ ____________第五章:术前评估和治疗选择5.1 术前评估内容5.2 基因型检测与预后评估5.3 辅助治疗的选择①临床分期②组织病理学分级③预后危险因素评估④综合评估_______________________________________________________ ____________第六章:术后评估和治疗调整6.1 术后评估指标①影像学评估②病理学评估③临床评估6.2 治疗调整原则6.3 术后放疗的选择①标准方法②部分乳房放疗③选择性放疗6.4 支持性疗法①心血管②内分泌③生育与保育_______________________________________________________ ____________第七章:附录7.1 附件1、乳腺癌新辅助治疗专家共识 (2019年版) 相关资料7.2 附件2、乳腺癌新辅助治疗指南 (2019年版) 相关资料7.3 附件3、其他相关附件资料_______________________________________________________ ____________注释:1.乳腺癌●乳房组织中发生的恶性肿瘤。
医学英语疾病介绍——Breast Cancer(乳腺癌)ppt课件

Causes And Risk Factors
Breast Cancer Genes
—
The genes most commonly involved in breast cancer are known as BRCA1 and BRCA2. Women with mutations( 突变) in these genes have up to an 80 percent chance of getting breast cancer at some point in life(有大于80%的几 率在其一生的某个年龄段罹患乳腺癌).
Staging 分期 Treatment 治疗 Expectations 预后 Prevention 预防
Summary 综述
Breast Cancer Today — In America
Breast cancer today is not what it was 20 years ago. Survival rates are climbing, thanks to greater awareness, more early detection, and advances in treatment. (归功于更多的关注,更早的监测和更先进的 治疗技术) For roughly 200,000 Americans who are diagnosed with breast cancer each year(每年约有二十万美国人被诊断为乳腺癌), there are plenty of reasons to be hopeful.
In America, About 1 out of 8 women are diagnosed with breast cancer every year.(在美国,一年统计数据表明,大约每八个女性中有 一个会罹患乳腺癌)
早期乳腺癌治疗:St. Gallen国际专家共识
今年St.?Gallen会议的主题是乳腺癌治疗的“加减法”(escalation?and?de-escalation),相关专家共识也已陆续发布。
早期乳腺癌治疗的相关共识发表在2017年第8期《Annals?of?Oncology》上,肿瘤资讯为大家编译介绍如下。
导管原位癌如果切缘可以达标,则保乳手术后放疗仍是导管原位癌的标准治疗。
关于切缘距离,专家组成员大部分赞同最近由美国肿瘤外科学会(SSO)、美国临床肿瘤学会(ASCO)、美国肿瘤放疗学会(ASTRO)提出的≥2mm;少数成员认为某些病例切缘距离可以更窄,如“墨染切缘无导管原位癌”。
芳香化酶抑制剂或他莫昔芬辅助治疗用于降低导管原位癌复发风险可能有效。
早期乳腺癌的手术治疗专家组强烈赞同只要手术切缘阴性、术后进行放疗,则多灶性及多象限病变也可进行保乳手术。
专家组再次重申了“墨染切缘无瘤”的原则,并建议无论肿瘤生物学亚型如何均可按照此原则处理。
即使有1-2枚前哨淋巴结阳性也可保乳手术后进行全乳放疗及系统辅助治疗,且这类病例行标准的“切线野”或“高切线野”均可。
行乳腺切除术且前哨淋巴结活检证实1-2枚有宏转移者,建议对腋窝处进一步治疗:术后放疗或腋窝清扫均可。
新辅助治疗后手术专家组建议根据残余肿瘤的范围确定乳腺手术的范围,没必要对最初的瘤床进行完全切除。
专家组赞同新辅助治疗后仍以“墨染切缘无肿瘤”作为手术切缘的标准,不过,很多专家认为多灶性残余者可以选择更加宽一些的切缘。
新辅助治疗后乳晕区无肿瘤累及时,可以选择保留乳头的乳腺切除术。
新辅助治疗后腋窝手术专家组强烈赞同临床检查腋窝淋巴结阴性者进行新辅助治疗后对前哨淋巴结进行活检。
临床检查腋窝淋巴结阳性、且新辅助治疗后转为阴性而临床分期下调的患者,也应进行前哨淋巴结活检:如果三枚及以上前哨淋巴结阴性则可以不必进行淋巴结清扫。
如新辅助治疗后临床检查腋窝淋巴结仍阳性、或前哨淋巴结检查有宏转移,建议进行腋窝淋巴结清扫。
乳腺癌英文版

乳腺癌英文版Breast Cancer: Understanding and Overcoming the ChallengeIntroductionBreast cancer is a prevalent and life-changing disease that affects millions of individuals worldwide, regardless of gender. In recent years, there have been significant advancements in medical research and treatment options, improving survival rates and overall quality of life for patients. This article aims to provide a comprehensive overview of breast cancer, its causes, symptoms, diagnosis, treatment, and prevention.Understanding Breast CancerBreast cancer refers to the uncontrolled growth of abnormal cells in the breast tissue. While the exact cause remains unknown, certain risk factors have been identified. These include age, gender, family history, genetic mutations, hormonal factors, and environmental influences. It is essential to highlight that men can also develop breast cancer, although it is relatively rare compared to women.Symptoms and DiagnosisDetecting breast cancer at an early stage plays a vital role in successful treatment. While symptoms may vary, common signs include a lump or thickening in the breast or underarm area, changes in breast size or shape, nipple discharge, or skin changes, such as redness, dimpling, or puckering. Regular self-examinations and mammograms are recommended as essentialtools for early detection. Diagnostic procedures may involve imaging tests, biopsies, or genetic testing to determine the presence and stage of cancer.Treatment OptionsThe treatment of breast cancer depends on several factors, including the stage of cancer, overall health, and personal preferences. Treatment modalities often include surgery, radiation therapy, chemotherapy, hormonal therapy, targeted therapy, or a combination of these. Surgery may involve a lumpectomy (removal of the tumor) or a mastectomy (removal of the breast). Radiation therapy uses high-energy rays to destroy cancer cells, while chemotherapy employs drugs to kill or prevent the growth of cancer cells throughout the body. Hormonal therapy and targeted therapy specifically target hormone receptors or specific genetic mutations within tumor cells.Support and RehabilitationCoping with breast cancer can be physically and emotionally challenging for patients and their loved ones. Alongside medical treatment, support from healthcare providers, family, friends, and support groups is crucial. The availability of psychotherapy, counseling, or support services can empower individuals to manage the psychological and emotional aspects of the disease. Additionally, rehabilitation programs and post-treatment care can help patients regain physical strength, manage side effects, and adapt to the changes brought about by their diagnosis.Importance of Awareness and PreventionEducating oneself about breast cancer is essential for early detection and prevention. Engaging in a healthy lifestyle, including regular exercise,maintaining a balanced diet, limiting alcohol consumption, and refraining from smoking, can reduce the risk of developing breast cancer. Additionally, individuals should be aware of their family history and consider genetic counseling if necessary. While breast cancer cannot always be prevented, early detection significantly improves outcomes.ConclusionBreast cancer affects individuals globally and warrants attention from both individuals and healthcare systems. Understanding the risk factors, symptoms, diagnosis, treatment options, and prevention strategies is essential for effective management of the disease. With advancements in medical technology and ongoing research, the prognosis for breast cancer patients continues to improve, bringing hope to those affected. By promoting awareness, supporting research, and fostering a supportive environment, we can collectively combat breast cancer and help individuals lead fulfilling lives beyond their diagnosis.。
2011年《St.Gallen早期乳腺癌初始治疗国际专家共识》与中国抗癌协会乳腺癌专业委员会指南之比较
测项 目。
21 0 1年 6月《 na f nooy 杂志公 布 了 A nlo cl ) s O g) 最新 版《 tG ln早 期乳 腺癌 初 始 治 疗 国际 专 家 S. ae l 共识 》 以下 简 称《 tG ln共 识 》 。 与此 同 时 , ( S. al e ) 中国抗癌 协会 乳 腺 癌 专 业 委 员会 ( B S 也 更新 CC ) 了《 乳腺癌诊治指南与规范》 以下简称《 B S指 ( CC 南》 。现 将 两部 指 南 的主要 更新 点作 一介绍 。 )
肿块 最 大 直 径 为 0 5~1 m 的 乳 腺 癌 , 有 . c 也 7 . % 的专家 投 了赞 成 票 。在 低 收入 国 家 中, 87 可 否使 用 短于 1年 的 曲妥 珠 单克 隆抗 体 治疗? 也 有 7 % 的专家投 了赞成 票 。《 B S指 南》同样 强调 1 CC
1 共 同 点
1 2 曲妥珠 单 克 隆抗体 辅助 治疗 . 对 于 肿瘤 直 径 >0 5 o 的 H R 2阳性 早 期 . n E-
乳腺癌 患者 , 两部 指 南 均推 荐 1年 的辅 助 曲妥 珠 单克 隆抗体 治疗 。短 于 1年使用 曲妥珠 单 克 隆抗 体 并 不是 最 佳 方 案 , 是 用 比 不 用 者 疗 效 好 I 但 。 21 0 1年 S.G ln会 议 上 , 10 多个 需 要 表 决 t ae l 在 0 的 问题 中 ,对 于 H R. 性早 期 乳 腺 癌 , “ E 2阳 1年 的 辅助 曲妥 珠 单 克 隆 抗 体 治疗 是 否 是 一个 治 疗 标 准” 唯 一 的 1 0 专 家 投 赞 成 票 的 问题。 对 于 是 0%
2017年第三版ESO-ESMO晚期乳腺癌国际共识(ABC3)
2017年第三版ESO-ESMO晚期乳腺癌国际共识(ABC3)
实名微信号:breastbreastMDT(内有海量最新乳腺病学专业资讯(近五千条),关注时需要提供您目前就职的省份城市名称、医院科室和姓名信息,只接受实名互粉,信息不全者,一律不回复!一律不回复!一律不回复!)
ER+/HER2-(luminal)晚期乳腺癌最重要的推荐之一是关于luminal型晚期乳腺癌的优选治疗,大多数患者应为内分泌治疗。
所有乳腺癌指南都认可这一推荐,然而真实世界研究发现,很多患者仍然将化疗作为一线治疗。
三阴性晚期乳腺癌三阴性乳腺癌仍然是晚期乳腺癌治疗中最未被满足的领域,尽管进行了广泛的研究,但目前除了化疗外仍无其他治疗方案对这类人群有效。
鉴于此原因,对于这一亚型患者,除了铂类药物用于BRCA突变患者外,指南没有给出更多特定的推荐。
2024乳腺癌抗体偶联药物输注管理专家共识
2024乳腺癌抗体偶联药物输注管理专家共识近年来快速发展的抗体偶联药物(antibody-drug conjugates , ADC ) 靶向生物制剂,是一类由单克隆抗体经由连接分子与细胞毒类药物偶联结合而组成的新型抗肿瘤药物,具有强杀伤作用和高度的靶向性,给部分乳腺癌以及多线治疗后的难治性乳腺癌患者带来了更加有效且安全的治疗方法,开启了乳腺癌分子分型精准诊疗的新时代。
目前,已经获美国食品药品监督管理局(FDA )批准上市用于治疗乳腺癌的ADC 药物有恩美曲妥珠单抗(trastuzumab emtansine , T-DM1 \ 德曲妥珠单抗(trastuzumab deru×tecan , T-DXd )和戈沙妥珠单抗(Sacituzumab govitecan , SG ) 3种,也均已获得中国国家药品监督管理局(NMPA )的批准在中国国内上市。
治疗策略和诊疗方式的改变,需要医护人员及时了解和熟悉ADC药物的输注规范和输注过程中药物的不良反应的管理,降低并发症的发生,确保ADC药物输注的安全和有效性。
基于此,本共识小组就T-DM1s T-DXd x SG这3种乳腺癌ADC药物的输注管理及输注过程中的不良事件的安全性管理展开讨论,采取专家投票方式形成共识推荐意见,为医护人员在ADC药物输注管理的临床实践中提供参考。
一、乳腺癌ADC简介1. T-DM1 : T-DM1商品名称为赫赛莱,是首个获批用于实体瘤的人类表皮生长因子受体2( HER2 )的ADC。
T-DM1将抗体的高度靶向特异性(曲妥珠单抗)和小分子毒素(DMl)的高毒性相结合,实现对肿瘤细胞的精准高效杀伤,同时具有靶向作用,T-DM1分子中的曲妥珠单抗发挥靶向作用,DM1具有强效细胞毒性作用,硫酷连接体结构稳定;T-DM1具有曲妥珠单抗和DM1双重作用机制,疗效较靶向更强、耐受性较化疗更好。
2. T-DXd : T-DXd商品名称为优赫得,又称DS-8201a ,用于治疗HER2 阳性乳腺癌。
中国进展期乳腺癌共识指南
中国进展期乳腺癌共识指南近年来,乳腺癌已成为全球范围内高发的女性恶性肿瘤之一。
在中国,每年有大量的女性被诊断为乳腺癌,其中进展期乳腺癌(ABC)患者的比例不在少数。
为了更好地规范和治疗进展期乳腺癌,中国抗癌协会乳腺专业委员会特地制定了《中国进展期乳腺癌共识指南》(以下简称《指南》)。
本文将详细介绍该《指南》的内容和特点,并针对如何更好地利用该《指南》提出一些建议。
中国进展期乳腺癌共识指南是为了提高进展期乳腺癌患者的生存率和生活质量,规范临床诊疗行为,促进医疗质量的全面提升而制定的。
该《指南》由国内权威的乳腺肿瘤专家共同讨论和制定,包含了关于进展期乳腺癌的病理学、临床诊断、治疗策略和随访等多个方面的内容,具有极高的实用性和指导意义。
中国进展期乳腺癌共识指南具有以下几个主要特点:它强调了多学科联合诊疗的重要性,要求医生们具备丰富的专业知识和临床经验,从而为患者提供更为全面的诊疗服务;它引进了国外最新的乳腺癌治疗理念和技术,并根据国内实际情况进行了调整和改进,更符合中国患者的实际情况;它注重患者的生活质量,提倡在治疗过程中尽可能地减少对患者生活质量的影响。
在《指南》中,专家们针对进展期乳腺癌的各个方面提出了许多推荐意见。
其中包括:(1)对于ABC患者,推荐使用多学科联合诊疗模式,包括外科、放疗科、化疗科、病理科和医学影像科等;(2)在制定治疗策略时,应该根据患者的病理学特征、临床分期、身体状况和生育需求等因素进行综合评估,为患者制定个性化的治疗方案;(3)对于需要接受化疗的患者,推荐使用包括紫杉类药物、曲妥珠单抗、帕博西尼等在内的多种药物联合化疗方案;(4)在放疗方面,推荐使用精准放疗技术和设备,如三维适形放疗、调强放疗等,以提高治疗效果和减少不良反应;(5)在内分泌治疗方面,根据患者的ER/PR状态和病情需要,可以选择使用他莫昔芬、来曲唑、依西美坦等内分泌药物进行治疗。
除了指南推荐外,《指南》还为临床实践提供了以下建议:(1)在诊治患者过程中,应注重与患者的沟通和交流,充分了解其病情和需求,增强患者的信任感和依从性;(2)在制定治疗方案时,应充分考虑患者的实际情况和意愿,合理选择治疗手段和药物,尽可能地提高治疗效果和生活质量;(3)在放疗和化疗过程中,应注重观察和评估患者的反应和副作用,及时调整治疗方案和药物剂量,减少不良反应的发生;(4)在内分泌治疗过程中,应根据患者的ER/PR状态和病情变化,及时调整药物种类和剂量,以达到最佳治疗效果。
中国早期乳腺癌卵巢功能抑制临床应用专家共识(2024年版)
中国早期乳腺癌卵巢功能抑制临床应用专家共识(2024年版)中国抗癌协会乳腺癌专业委员会;胡夕春;吴炅;任国胜;江泽飞;张瑾;张剑【期刊名称】《中国癌症杂志》【年(卷),期】2024(34)3【摘要】中国乳腺癌患者发病年龄较轻,60%的女性患者在诊断时为绝经前。
与绝经后相比,未绝经女性卵巢功能旺盛,可持续大量分泌雌激素、促进乳腺癌细胞增殖。
卵巢功能抑制(ovarian function suppression,OFS)已用于乳腺癌临床治疗数十年,大量循证证据表明,单用OFS和加用OFS均可降低未绝经女性乳腺癌的复发风险并改善生存。
部分OFS研究的长期随访数据(SOFT/TEXT研究12和13年随访、STO-5研究20年随访、亚裔人群的ASTRRA研究8年随访)近期陆续公布,进一步证实对于早期乳腺癌患者加用OFS可显著降低10年以上的复发风险,提高治愈可能。
monarchE和NATALEE研究显示,部分CDK4/6抑制剂叠加在绝经前早期乳腺癌患者含有药物去势[促性腺激素释放激素类似物(gonadotropin releasing hormone analog,GnRHa)]的辅助内分泌治疗方案时仍可进一步增加生存获益。
中国抗癌协会乳腺癌专业委员会召集了国内乳腺癌治疗领域的临床专家,在2021年版的基础上共同商讨编制了《中国早期乳腺癌卵巢功能抑制临床应用专家共识(2024年版)》。
本共识建议,GnRHa仍作为绝经前激素受体阳性早期乳腺癌OFS方式的首选。
GnRHa联合内分泌治疗基础上添加特定CDK4/6抑制剂的激素受体阳性绝经前乳腺癌获益人群包括:淋巴结阳性,淋巴结阴性且满足任一条件[G3,G2伴Ki-67增殖指数≥20%,G2伴多基因检测(21基因评分、Prosigna PAM50、MammaPrint、EndoPredict)高危]。
本共识也认可将2023年St.Gallen共识中有化疗指征的风险因素作为OFS适用判定标准之一。
中国早期乳腺癌卵巢功能抑制临床应用专家共识
中国早期乳腺癌卵巢功能抑制临床应用专家共识乳腺癌是中国女性中最常见的恶性肿瘤之一,而早期乳腺癌的治疗方案一直备受关注。
近年来,一种新的治疗方法——卵巢功能抑制(Ovarian Function Suppression, OFS)在早期乳腺癌患者中得到了广泛的应用。
为了统一临床实践,一群中国乳腺癌专家在探讨和总结国内外相关研究的基础上,制定了中国早期乳腺癌卵巢功能抑制临床应用的专家共识,为临床医生提供了重要的指导。
OFS是通过抑制卵巢功能来达到治疗乳腺癌的目的。
根据研究,卵巢功能抑制可以降低雌激素水平,从而减少肿瘤生长所需的雌激素供应,延缓病情进展并减少复发的风险。
在早期乳腺癌的治疗中,OFS常常与内分泌治疗相结合,以提高疗效。
根据专家共识的指导,早期乳腺癌患者可以选择手术切除肿瘤后进行卵巢功能抑制。
抑制卵巢功能的方法包括手术切除卵巢、放射治疗和药物治疗等。
在选择治疗方法时,应综合考虑患者的肿瘤分子特征、年龄、生育需求以及相关不良反应等因素。
对于未停经的患者,手术切除卵巢是一种较为常见的选择;而对于已停经的患者,放射治疗和药物治疗则是更为合适的选择。
专家共识还进一步明确了乳腺癌患者在进行OFS治疗时的监测方法和注意事项。
监测方法主要包括雌激素水平的测定、相关不良反应的评估以及骨密度的检查等。
及时监测可以帮助医生了解患者的治疗效果和身体状况,从而作出相应的调整和治疗措施。
此外,专家强调,OFS治疗也可能导致一些副作用,如骨质疏松、心血管疾病和女性生殖系统的不良反应等,因此患者在进行治疗时需要密切与医生沟通,及时报告任何身体不适。
与此同时,专家共识还探讨了OFS治疗在不同乳腺癌亚型中的应用。
根据乳腺癌的分子特征和表型,乳腺癌可以分为雌激素受体(ER)阳性、HER2阳性和三阴性乳腺癌等不同亚型。
根据不同亚型的特点和治疗需求,专家共识提供了相应的治疗指导。
例如,在ER阳性乳腺癌患者中,OFS治疗可作为内分泌治疗的首选,而在HER2阳性和三阴性乳腺癌患者中,OFS治疗则往往与其他治疗方式相结合,以达到最佳治疗效果。
HER2阳性乳腺癌诊疗专家共识

456 418
风险患者数
40
0
1
2
3
4
5
随机化时间 3025495-13
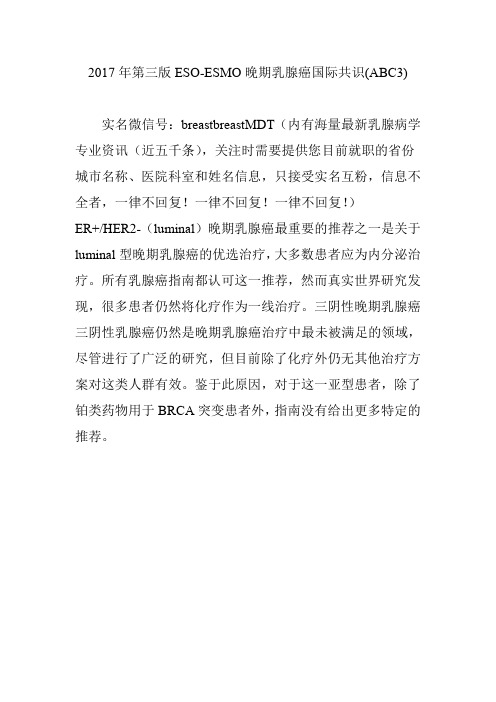
序贯组 (B组) vs 联合治疗组 (C组) 无病生存率
N9831
结果: 无病生存率 联合分析 (N9831/B31) ~中位数为3年的随访1
100
80
60
40
20
0
0
6
12
18
24
30
48
36
42
随机化后月
1698 1703
1564 1619
1440 1552
1363 1485
1297 1414
1240 1352
712 854
1180 1280
992 1020
风险患者数
事件 458 369
4年 DFS 72.2 78.6
HR 0.76
多西紫杉醇75 mg/m2,卡铂 AUC 6, 每 21天一疗程共6周期, 同时曲妥珠单抗周疗, 化疗结束后曲妥珠单抗6 mg/kg,三周一次,至1年
标准化疗后单用曲妥珠单抗治疗 1年
曲妥珠单抗治疗方案为 6 mg/kg,(首剂 8 mg/kg) 每 3周方案,治疗时间为1年
HERA 2008中期分析: 曲妥珠单抗2 年 vs 1 年治疗组目前无结论
*
NCCTG 9831
1年曲妥珠单抗
4 x AC
12 x
紫杉醇
80 mg/m2
Breast InterGroup
HERA
HER2 +
允许的化疗
AC, EC, FAC, FEC,
ET, AT, CMF
中国进展期乳腺癌共识指南_CABC2015_.

Chinese Guideline for Advanced Breast Cancer 2015(CABC 2015)
China Medical Women′s Association of Clinical Oncology Chinese Anti-Cancer Association of Breast Cancer
在 乳 腺 癌 患 者 的 治 疗 领 域 中 ,早 期 诊 断 技 术
和 新 药 研 发 都 出 现 了 蓬 勃 发 展 的 态 势 ,尤 其 是 一 系 列 新 药 的 出 现 ,更 让 乳 腺 癌 的 治 疗 得 到 了 前 所 未 有 的 进 步 ,即 便 是 进 展 期 乳 腺 癌 包 括 的 原 发 局 部晚期乳腺癌(即诊断时不能 R0 切除)、局部复发 乳 腺 癌 和 转 移 性 乳 腺 癌(metastatic breast cancer, MBC)仍 然 有 很 多 方 法 可 以 治 疗 。 目 前 进 展 期 乳 腺癌患者的中位生存时间为 2~4 年[4-5],但不同亚 型和不同转移部位的结果完全不同。有文献报道 并分析了 544 例乳腺癌患者的资料,其中位生存 时间为 33 个月(13.6~53.4 个月)[6];另一篇文献则 报道,146 例单纯骨转移的乳腺癌患者中,激素受 体(HR)阳 性 患 者 的 中 位 生 存 时 间 为 65 个 月 ,人 表皮生长因子受体(HER2)阳性和三阴性(ER 阴
Key words: advanced breast cancer; experts consensus; guideline; China Prog Oncol, 201年 升 高 ,这 部 分 患 者 的 治 疗越来越受乳腺肿瘤科医生的重视。在新发乳腺 癌患者中,有 6%~7%的患者初次诊断即为进展 期乳腺癌(advanced breast cancer,ABC)[1],而最初 诊 断 为 早 期 乳 腺 癌 的 患 者 在 接 受 辅 助 治 疗 后 ,其 中有 30%的患者最终会出现复发转移[2-3],这就意 味 着 在 今 后 的 几 年 内 ,我 国 进 展 期 乳 腺 癌 的 比 例 也会增加,并会出现一个较大的群体。目前认为, 进 展 期 乳 腺 癌 还 不 能 被 治 愈 ,但 可 以 被 治 疗 ;所 以 ,治 疗 是 以 延 缓 疾 病 进 展 、改 善 生 活 质 量 、延 长 生存为目的的。进展期乳腺癌虽然没有绝对的标 准治疗方案,但仍有一定的规律可循(附 1)。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Table 1Levels of evidence grading systemGrade of Recommendation /Description Benefit vs. Risk andBurdensMethodological Quality of SupportingEvidenceImplications1A/Strong recommendation, high quality evidence Benefits clearly outweighrisk and burden, or viceversaRCTs without important limitations oroverwhelming evidence from observationalstudiesStrong recommendation, can apply tomost patients in most circumstanceswithout reservation1B/Strong recommendation, moderate quality evidence Benefits clearly outweighrisk and burdens, or viceversaRCTs without importantlimitations(inconsistent results,methodological flaws, indirect, or imprecise)or exceptionally strong evidence fromobservational studiesStrong recommendation, can apply tomost patients in most circumstanceswithout reservation1C/Strong recommendation, low quality evidence Benefits clearly outweighrisk and burdens, or viceversaObservational studies or case series Strong recommendation, but maychange when higher quality evidencebecomes available2A/Weak recommendation, high quality evidence Benefits closely balancedwith risk and burdenRCTs without important limitations oroverwhelming evidence from observationalstudiesWeak recommendation, best actionmay differ depending on circumstancesor patients’ or societal values2B/Weak recommendation, moderate quality evidence Benefits closely balancedwith risk and burdenRCTs with important limitations(inconsistentresults, methodological flaws, indirect, orimprecise) or exceptionally strong evidencefrom observational studiesWeak recommendation, best actionmay differ depending on circumstancesor patients’ or societal values2C/Weak recommendation, low quality evidence Benefits closely balancedwith risk and burdenObservational studies or case series Very weak recommendation, otheralternative may be equally reasonableTable 2General guideline.Guideline statement LoE ABC Consensus CABC Consensus1) The management of ABC is complex and, therefore, involvement of allappropriate specialties in a multidisciplinaryteam (including but not restricted tomedical, radiation, surgical oncologists, imaging experts,pathologists,gynaecologists, psycho-oncologists, social workers, nurses andpalliative care specialists), is crucial.Expert opinion 100% Yes (29 voters) 100% Yes (20 voters)2) From the time of diagnosis of ABC, patients should be offered appropriatepsychosocial care, supportive care,and symptom-related interventions as aroutine part of their care. The approach must be personalized tomeet the needsof the individual patient.Expert opinion 100% Yes (30 voters) 100% Yes (20 voters)3) Following a thorough assessment and confirmation of MBC, the potential treatment goals of care should bediscussed. Patients should be told that MBC is incurable but treatable, and women can live with MBC for extendedperiods of time (many years in some circumstances). This conversation should be conducted in accessible language,respecting patient privacy and cultural differences, and whenever possible, written information should be provided. Expert opinion 97% (29) Yes 3% (1)Abstain (30 voters)95% (18) Yes(19 voters)4) Patients (and their families, caregivers or support network, if the patient agrees) should be invited to participate inthe decision-making process at all times. When possible, patients should be encouraged to be accompanied bypersons who can support them and share treatment decisions (e.g. family members, caregivers, support network) Expert opinion 100% Yes (30 voters) 75% (15) Yes 15% (3)Abstain (20 voters)Table 3Assessment guidelines.Guideline statement LoE ABC Consensus CABC Consensus8) Minimal staging workup for MBC includes a history and physical examination, haematology and biochemistry tests,and imaging of chest, abdomen and bone. 2 C 67% (20) Yes 3% (1)Abstain (30 voters)100% Yes (19 voters)9) Brain imaging should not be routinely performed in asymptomatic patients. This approach is applicable to all patientswith MBC including those patients with HER-2þ and/or TNBC MBC. Expertopinion 94% (30) Yes(32 voters)45% (9) Yes(20 voters)10) The clinical value of tumour markers is not well established for diagnosis or follow-up after adjuvant therapy,but their use (if elevated) as an aid to evaluate response to treatment, particularly in patients with non-measurablemetastatic disease, is reasonable. A change in tumour markers alone should not be used to initiate a change in treatment. 2 C 89% (24) Yes 4% (1)Abstain (27 voters)86% (18) Yes 10% (2)Abstain (21 voters)11) Evaluation of response to therapy should generally occur every 2e4 months for ET or after 2-4 cycles for CT,depending on the dynamics of the disease, the location and extent of metastatic involvement, and type of treatment.Imaging of a target lesion may be sufficient in many patients. In certain patients, such as those with indolent disease,less frequent monitoring is acceptable. Additional testing should be performed in a timely manner, irrespective of theplanned intervals, if PD is suspected or symptoms appear. Thorough history and physical examination must alwaysbe performed. Expert opinion 81% (25) Yes 10% (3)Abstain (31 voters)100% Yes (18 voters)Table 4Treatment general guidelines.Guideline statement LoE ABC Consensus CABC Consensus15) Treatment choice should take into account at least these factors: HR &HER-2 status; previous therapies andtheir toxicities; disease-free interval; tumourburden (defined as number and site of metastases); physiologicage; performancestatus; co-morbidities (including organ dysfunctions); menopausal status (for ET);need fora rapid disease/symptom control; socio-economic and psychologicalfactors; available therapies in the patient’s country and patient preference.Expert opinion 100% Yes (30 voters) 100% Yes (19 voters)16) The age of the patient should not be a reason to withhold effective therapy. 1 B 94% (28) Yes 3% (1)Abstain (30 voters)100% Yes (15 voters)17) A small but very important subset of patients with MBC, for example those with oligo-metastatic disease,can achieve complete remission and a long survival. A multimodal approach should be considered for theseselected patients.A prospective clinical trial addressing this specific situation is needed. Expertopinion 96% (25) Yes (26voters)100% Yes (17 voters)18) The true value of the removal of the primary tumour in patients with stage IVbreast cancer is currentlyunknown. However, it can be considered in selectedpatients. Of note, some studies suggest that surgery isonly valuable if performedwith the same attention to detail (e.g. attaining clear margins and addressingdisease in the axilla) as in patients with early stage disease. Prospective clinicaltrials to confirm the valueof this approach, the best candidates and timing arecurrently ongoing.2 B 100% Yes (29 voters) 100% Yes (19 voters)Table 5ER +/HER-2 negative ABC.Guideline statement LoE ABC Consensus CABC Consensus19) Endocrine therapy (ET) is the preferred option for hormone receptor positive disease, even in the presence ofvisceral disease, unless there is concern or proof of endocrine resistance or there is disease needing a fast response. 1 A 100% Yes (29 voters) 75% (12) Yes 6% (1)Abstain (16 voters)20) For pre-menopausal women, ovarian suppression/ablation combined with additional endocrine therapy is the first choice. 1 A 97% (29) Yes (30voters)93% (14) Yes (15voters)21) The additional endocrine agent should be tamoxifen unless tamoxifen resistance is proven.An AI is also a viable option, but absolutely mandates the use of ovarian suppression/ablation. 1 B 97% (29) Yes (30voters)88% (14) Yes 6% (1)Abstain (16 voters)22) The preferred 1st line ET for postmenopausal patients is an aromatase inhibitor; however, tamoxifen remains aviable option in selected patients. Type and duration of adjuvant ET must be taken into account. 1 A 94% (29) Yes 6% (2)Abstain (32 voters)100% Yes (16 voters)23) Optimal post-aromatase inhibitor treatment is uncertain. Available options include, but arenot limited to, tamoxifen, another AI (with a different mechanism of action), fulvestrant, and megestrol acetate. 1 A 97% (30) Yes 3% (1)Abstain (30 voters)100% Yes (15 voters)24) The addition of everolimus to an AI has shown favourable results in patients with acquired endocrine resistance. However, themajority of the panel believes that additional data/studies are needed before this strategy can be recommended as standardof care. At this time, everolimus is not approved for use in this setting by EU/US regulatory authorities. Expertopinion 48% (15) Yes 13% (4)Abstain (31 voters)93% (14) Yes (15voters)Table 6HER-2-positive ABC.Guideline statement LoE ABC Consensus CABC Consensus27) Anti-HER-2 therapy should be offered early to all patients with HER-2þ MBC, except inthe presence of contra-indications to the use of such therapy. 1 A 91% (30) Yes 3% (1)Abstain (33 voters)100% Yes (16 voters)28) For patients with ER+/HER-2+ MBC for whom ET was chosen over CT, anti-HER-2therapy + ET should be considered with the initiation of endocrine therapy (providedthat further anti-HER-2 therapy is available) since anti-HER-2 therapy (either trastuzumabor lapatinib) in combination with ET has shown substantial PFS benefit (i.e., “time without CT”)1 A 90% (27) Yes 10% (3)Abstain (30 voters)100% Yes (12 voters)29) Patients progressing on an anti-HER-2 therapy combined with a cytotoxic orendocrine agent should be offered additional anti-HER-2 therapy with subsequenttreatment since it is beneficial to continue suppression of the HER-2 pathway. 1 B 97% (29) Yes (30voters)100% Yes (15 voters)30) It is currently unknown if the best option for patients progressing after receiving one line oftrastuzumab þ cytotoxic agent is to continue trastuzumab in conjunction with anothercytotoxic agent or to change to lapatinib in combination with capecitabine. Therefore, both options are viable. 1 A 90% (26) Yes 10% (3)Abstain (29 voters)100% Yes (16 voters)31) In patients with HER-2þ MBC who relapse after adjuvant anti-HER-2 therapy, the best option remains unclear,but all such patients should be considered for further anti-HER-2 therapy. The choice of the anti-HER2 agent willdepend on country-specific availability, the specific anti-HER2 therapy that was administered, and therelapse free interval. 1 B 85% (23) Yes 15% (4)Abstain (27 voters)100% Yes (16 voters)Table 7Chemotherapy and biological therapy.Guideline statement LoE ABC Consensus CABC Consensus34) Both combination and sequential single agent CT are reasonable options. Based on the available data, we recommendsequential monotherapy as the preferred choice for MBC. Combination CT should be reserved for patients with rapidclinical progression, life-threatening visceral metastases, or need for rapid symptom and/or disease control. 1 B 96% (25) Yes 4% (1)Abstain (26 voters)100% Yes (18 voters)35) In the absence of medical contra-indications or patient concerns, anthracycline or taxane-based regimens, preferablyas single agents, would usually be considered as first line CT for HER-2 negative MBC, in those patients who have notreceived these regimens as adjuvant treatment and for whom chemotherapy is appropriate. Other options are, however,available and effective, such as capecitabine and vinorelbine, particularly if avoiding alopecia is a priority for the patient. 1 A 71% (17) Yes 4% (1)Abstain (24 voters)100% Yes (13 voters)36) In patients with taxane-naive and anthracycline-resistant MBC or with anthracycline cumulative dose or toxicity(i.e., cardiac) who are being considered for further CT, taxane-based therapy, preferably as single agents, would usuallybe considered as treatment of choice. Other options are, however, available and effective, such as capecitabine andvinorelbine, particularly if avoiding alopecia is a priority for the patient. 1 A 59% (14) Yes 8% (2)Abstain (24 voters)88% (14) Yes 12% (2)Abstain (16 voters)37) In patients pre-treated with anthracycline and taxanes (in the adjuvant or metastatic setting) and who do not needcombination CT, capecitabine single agent is the preferred choice. 1 B 56% (15) Yes 11% (3)Abstain (27 voters)83% (10) Yes (12voters)38) If given in the adjuvant setting, a taxane can be re-used as 1st line therapy, particularly if there has been at least oneyear of disease-free survival. 1 A 92% (22) Yes 8% (1)Abstain (24 voters)77% (10) Yes 8% (1)Abstain (13 voters)39) Duration of each regimen and number of regimens should be tailored to each individual patient. Expert opinion 96% (26) Yes (27voters)100% Yes (13 voters)40) Usually each regimen should be given until progression of disease or unacceptable toxicity (unacceptable should bedefined together with the patient). 1 B 72% (21) Yes 7% (2)Abstain (29 voters)73% (8) Yes (11voters)41) Bevacizumab combined with a taxane as 1st line therapy for MBC provides only a moderate benefit in PFS and no benefitin OS. The absence of known predictive factors for bevacizumab efficacy renders recommendations on its use difficultand it is a research priority. Bevacizumab can only therefore be considered as an option in selected cases. 1 A 74% (17) Yes 17% (4)Abstain (23 voters)100% Yes (13 voters)Table 8Bone and brain metastases.Guideline statement LoE ABC Consensus CABC Consensus42) A bone modifying agent (bisphosphonate, denosumab) should be routinely used in combination with other systemictherapy in patients with MBC and bone metastases. 1 A 96% (26) Yes 4% (1)Abstain (27 voters)100% Yes (21 voters)43) Radiological assessments are required in patients with persistent and localized pain due to bone metastases todetermine whether there are impending or actual pathological fractures. If a fracture of a long bone is likely or hasoccurred, an orthopaedic assessment is required as the treatment of choice may be surgical stabilization which isgenerally followed by RT. In the absence of a clear fracture risk, RT is the treatment of choice. 1 A 96% (23) Yes 4% (1)Abstain (24 voters)100% Yes (20 voters)44) Neurological symptoms and signs which suggest the possibility of spinal cordcompression must be investigated as a matter ofurgency. This requires a fullradiological assessment of potentially affected area as well as adjacent areas ofthe spine. MRI is themethod of choice. An emergency surgical (neurosurgery ororthopaedic surgery) opinion may be required for surgicaldecompression. If nodecompression/stabilization is feasible, emergency radiotherapy is the treatmentof choice.1 B 100% Yes (24 voters) 100% Yes (21 voters)45) Patients with a single or a small number of potentially resectable brain metastasis should be treated with surgeryor radiosurgery. Radiosurgery is also an option for some unresectable brain metastases. 1 B 92% (22) Yes 4% (1)Abstain (24 voters)100% Yes (19 voters)46) If surgery/radiosurgery is performed it may be followed by whole brain radiotherapy but this should be discussedin detail with the patient, balancing the longer duration of intracranial disease control and the risk of neurocognitive effects. 1 B 72% (18) Yes 16% (4)Abstain (25 voters)100% Yes (16 voters)Table 9Supportive and palliative care.Guideline statement LoE ABC Consensus CABC Consensus47) Supportive care allowing safer and more tolerable delivery of appropriatetreatments should alwaysbe part of the treatment plan.1 A 100% Yes (26 voters) 100% Yes (20 voters)48) Expert palliative care, including effective control of pain and other symptoms,should be a priority.1 A 100% Yes (26 voters) 100% Yes (20 voters)49) Access to effective pain treatment (including morphine, which is inexpensive)is necessary for allpatients in need of pain relief.1 A 100% yes (27 voters) 100% Yes (20 voters)50) Optimally, discussions about patient preferences at the end of life should begin early in the course of metastatic disease.However, when active treatment no longer is able to control widespread and life-threatening disease, and the toxicitiesof remaining options outweigh benefits, physicians and other members of the healthcare team should initiate discussionswith the patient (and family members/friends, if the patient agrees) about end-of-life care. Expert opinion 96% (25) Yes 4% (1)Abstain (26 voters)100% Yes (21 voters)。