泊沙康唑Noxafilposaconazole静脉注射剂
泊沙康唑国内外临床研究介绍(1)

Cornely OA et al. N Engl J Med. 2007;356:348-359.
12
结论
对于因急性髓性白血病/骨髓异常增生综合症而接受化疗的 患者,泊沙康唑较伊曲康唑或氟康唑能更好的预防侵袭性 真菌感染的发生,并且泊沙康唑的使用可以改善上述患者 总体的生存率。
Cornely OA et al. N Engl J Med. 2007;356:348-359.
设计 开放性、前瞻、对照、多中心 13 岁;预计出现粒缺 (绝对中性粒细胞数 ≤500 cells/mm3) 7 天;因新诊断或复发的AML/MDS使用了密集化疗方案 N=602 泊沙康唑口服混悬液 200 mg TID 氟康唑口服混悬液 400 mg QD 伊曲康唑 口服混悬液 200 mg BID
严重不良事件泊沙康唑与标准唑类相当
*不良事件的统计是从患者随机化至最后一次用药后30天。由于部分患者出现上述不良反 应不止一次,因此不良反应的统计仅按照病例数而非不良事件发生的次数. †该表中包括了本次研究中所有的严重不良反应.
9
Cornely OA et al. N Engl J Med. 2007;356:348-359.
26
治疗失败率泊沙康唑低于氟康唑
因接受系统性抗真菌治疗/临床诊断及确诊IFI导致的治疗失败,泊沙康唑组 显著低于氟康唑组。
Yang Shen et al.International Journal of Clinical Pharmacology and Therapeutics. 2013,51(9):738-745
24
治疗期泊沙康唑组临床诊断/确诊IFI 发生率低于氟康唑
9.4%
3.42%
11/117
4、伏立康唑、泊沙康唑、艾沙康唑抗真菌药物对比
艾沙康唑是新型唑类抗真菌药,临床使用的 是硫酸艾沙康唑。 艾沙康唑通过变为前药的设计极大地提高了 溶解度,避免使用环糊精,无需考虑该赋形 剂在肾损患者中蓄积而导致的肾毒性,同时 也带来更好的生物利用度。
02
药动学特征
02 药动学特征
氟康唑 伊曲康唑
吸收
Oral Bioavailability: >90% IV与po剂量相同; 吸收不受食物影响
《2016 IDSA临床实践指南:曲霉病的诊 断和管理》中指出推荐使用伏立康唑作为 侵袭性曲霉病的一线疗法,替代疗法包括 脂质体两性霉素B、艾沙康唑,或其他脂 质制剂的 AmB
3.3 指南推荐-泊沙康唑
欧洲毛霉病指南(2019)
国内外多个权威指南明确指出,急性白血病 (包括 MDS)初次 诱导或挽救化疗患者、预期粒细胞缺乏持续>10d、伴有严重 粒细胞缺乏等高危因素的患者应进行预防治疗,药物首选泊 沙康唑,其次为氟康唑、伊曲康唑及伏立康唑等。 allo-HSCT 及 伴 GVHD等高危因素的患者应进行预防治疗,且 药物首选泊沙康唑,其次为米卡芬净、氟康唑、伊曲康唑等。 在毛霉病的初始治疗和挽救治疗中,建议泊沙康唑作为两性 霉素B类抗真菌药物的备选药物。
++
++
++
++
克柔念珠菌
-
+
++
++
葡萄牙念珠菌
++
++
++
++
烟曲霉菌
-
+
++
++
新型隐球菌
泊沙康唑使用指南
泊沙康唑使用指南
药物说明
泊沙康唑是一种治疗真菌感染的药物。
它能抑制真菌细胞膜的生长,达到抑制菌丝伸长和繁殖的效果,从而抑制真菌的增殖。
使用方法
泊沙康唑的使用方法如下:
1. 用药前请确保患处已经干燥。
2. 取适量泊沙康唑药膏涂于患处。
3. 患处每日使用2-3次,每次使用间隔至少6个小时。
4. 使用药物的时间视确诊的真菌感染病情决定,一般建议至少使用2-4周。
使用注意事项
使用泊沙康唑的过程中需要注意以下事项:
1. 切勿将药物接触到眼睛或口腔黏膜。
2. 请勿使用泊沙康唑治疗其他皮肤病。
3. 患者在使用泊沙康唑过程中注意个人卫生,不易交叉感染。
不良反应
尽管泊沙康唑是一种常用的治疗真菌感染的药物,但是在使用过程中仍然可能引起不良反应,如瘙痒,烧灼感,红斑等皮肤过敏症状。
如果您使用泊沙康唑期间出现不适症状,请及时停药并咨询医师。
总结
泊沙康唑是一种治疗真菌感染的药物,在使用泊沙康唑药物的过程中需要注意使用方法和注意事项,以避免不必要的不良反应,同时也能更好地发挥泊沙康唑的疗效。
泊沙康唑(posaconazole)

泊沙康唑(posaconazole)
刘晓平;胡春
【期刊名称】《中国药物化学杂志》
【年(卷),期】2007(17)4
【总页数】2页(P266-267)
【关键词】泊沙康唑;Plough公司;三唑类抗真菌药;FDA批准;曲霉菌病;真菌感染;药物耐药;镰刀菌病
【作者】刘晓平;胡春
【作者单位】沈阳药科大学
【正文语种】中文
【中图分类】R519
【相关文献】
1.三唑类广谱抗真菌新药——泊沙康唑 [J], 江丽;马道铭;刘维达
2.三唑类抗真菌新药泊沙康唑和伏立康唑简介 [J], 刘洁;胡小平;刘伟
3.三唑类抗真菌药物泊沙康唑注射液无菌检查方法研究 [J], 陈青连;姚振;万超
4.FDA批准抗真菌新药泊沙康唑(posaconazole) [J],
因版权原因,仅展示原文概要,查看原文内容请购买。
泊沙康唑 美国说明书
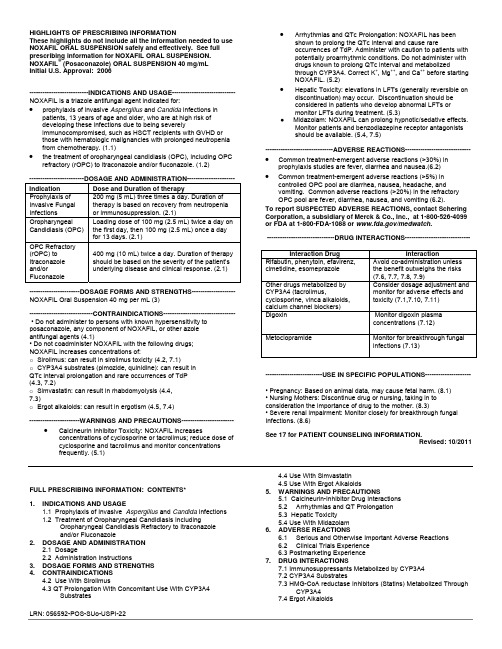
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use NOXAFIL ORAL SUSPENSION safely and effectively. See full prescribing information for NOXAFIL ORAL SUSPENSION. NOXAFIL® (Posaconazole) ORAL SUSPENSION 40 mg/mLInitial U.S. Approval: 2006---------------------------INDICATIONS AND USAGE----------------------------- NOXAFIL is a triazole antifungal agent indicated for: •prophylaxis of invasive Aspergillus and Candida infections in patients, 13 years of age and older, who are at high risk ofdeveloping these infections due to being severelyimmunocompromised, such as HSCT recipients with GVHD orthose with hematologic malignancies with prolonged neutropenia from chemotherapy. (1.1)•the treatment of oropharyngeal candidiasis (OPC), including OPC refractory (rOPC) to itraconazole and/or fluconazole. (1.2)-------------------------DOSAGE AND ADMINISTRATION---------------------- Indication Dose and Duration of therapyProphylaxis of Invasive Fungal Infections 200 mg (5 mL) three times a day. Duration of therapy is based on recovery from neutropenia or immunosuppression. (2.1)Oropharyngeal Candidiasis (OPC) Loading dose of 100 mg (2.5 mL) twice a day on the first day, then 100 mg (2.5 mL) once a day for 13 days. (2.1)OPC Refractory(rOPC) to Itraconazole and/or Fluconazole 400 mg (10 mL) twice a day. Duration of therapy should be based on the severity of the patient’s underlying disease and clinical response. (2.1)-----------------------DOSAGE FORMS AND STRENGTHS-------------------- NOXAFIL Oral Suspension 40 mg per mL (3)-----------------------------CONTRAINDICATIONS--------------------------------- • Do not administer to persons with known hypersensitivity to posaconazole, any component of NOXAFIL, or other azoleantifungal agents (4.1)• Do not coadminister NOXAFIL with the following drugs;NOXAFIL increases concentrations of:o Sirolimus: can result in sirolimus toxicity (4.2, 7.1)o CYP3A4 substrates (pimozide, quinidine): can result inQTc interval prolongation and rare occurrences of TdP(4.3, 7.2)o Simvastatin: can result in rhabdomyolysis (4.4,7.3)o Ergot alkaloids: can result in ergotism (4.5, 7.4)-----------------------WARNINGS AND PRECAUTIONS------------------------ •Calcineurin Inhibitor Toxicity: NOXAFIL increasesconcentrations of cyclosporine or tacrolimus; reduce dose ofcyclosporine and tacrolimus and monitor concentrationsfrequently. (5.1)•Arrhythmias and QTc Prolongation: NOXAFIL has beenshown to prolong the QTc interval and cause rareoccurrences of TdP. Administer with caution to patients withpotentially proarrhythmic conditions. Do not administer withdrugs known to prolong QTc interval and metabolizedthrough CYP3A4. Correct K+, Mg++, and Ca++ before startingNOXAFIL. (5.2)•Hepatic Toxicity: elevations in LFTs (generally reversible ondiscontinuation) may occur. Discontinuation should beconsidered in patients who develop abnormal LFTs ormonitor LFTs during treatment. (5.3)● Midazolam: NOXAFIL can prolong hypnotic/sedative effects.Monitor patients and benzodiazepine receptor antagonistsshould be available. (5.4, 7.5)-------------------------------ADVERSE REACTIONS------------------------------•Common treatment-emergent adverse reactions (>30%) inprophylaxis studies are fever, diarrhea and nausea.(6.2)• Common treatment-emergent adverse reactions (>5%) incontrolled OPC pool are diarrhea, nausea, headache, andvomiting. Common adverse reactions (>20%) in the refractoryOPC pool are fever, diarrhea, nausea, and vomiting (6.2).To report SUSPECTED ADVERSE REACTIONS, contact ScheringCorporation, a subsidiary of Merck & Co., Inc., at 1-800-526-4099or FDA at 1-800-FDA-1088 or /medwatch.-------------------------------DRUG INTERACTIONS------------------------------Interaction Drug InteractionRifabutin, phenytoin, efavirenz,cimetidine, esomeprazoleAvoid co-administration unlessthe benefit outweighs the risks(7.6, 7.7, 7.8, 7.9)Other drugs metabolized byCYP3A4 (tacrolimus,cyclosporine, vinca alkaloids,calcium channel blockers)Consider dosage adjustment andmonitor for adverse effects andtoxicity (7.1,7.10, 7.11)Digoxin Monitor digoxin plasmaconcentrations (7.12)Metoclopramide Monitor for breakthrough fungalinfections (7.13)--------------------------USE IN SPECIFIC POPULATIONS---------------------• Pregnancy: Based on animal data, may cause fetal harm. (8.1)• Nursing Mothers: Discontinue drug or nursing, taking in toconsideration the importance of drug to the mother. (8.3)• Severe renal impairment: Monitor closely for breakthrough fungalInfections. (8.6)See 17 for PATIENT COUNSELING INFORMATION.Revised:10/2011FULL PRESCRIBING INFORMATION: CONTENTS*1.INDICATIONS AND USAGE1.1 Prophylaxis of Invasive Aspergillus and Candida Infections1.2 Treatment of Oropharyngeal Candidiasis IncludingOropharyngeal Candidiasis Refractory to Itraconazoleand/or Fluconazole2.DOSAGE AND ADMINISTRATION2.1 Dosage2.2 Administration Instructions3.DOSAGE FORMS AND STRENGTHS4.CONTRAINDICATIONS4.2 Use With Sirolimus4.3 QT Prolongation With Concomitant Use With CYP3A4Substrates4.4 Use With Simvastatin4.5 Use With Ergot Alkaloids5.WARNINGS AND PRECAUTIONS5.1 Calcineurin-Inhibitor Drug Interactions5.2Arrhythmias and QT Prolongation5.3 Hepatic Toxicity5.4 Use With Midazolam6.ADVERSE REACTIONS6.1Serious and Otherwise Important Adverse Reactions6.2Clinical Trials Experience6.3 Postmarketing Experience7.DRUG INTERACTIONS7.1 Immunosuppressants Metabolized by CYP3A47.2 CYP3A4 Substrates7.3 HMG-CoA reductase Inhibitors (Statins) Metabolized ThroughCYP3A47.4 Ergot Alkaloids7.5 Benzodiazepines Metabolized by CYP3A47.6 Anti-HIV Drugs7.7 Rifabutin7.8 Phenytoin7.9 Gastric Acid Suppressors/Neutralizers7.10 Vinca Alkaloids7.11 Calcium Channel Blockers Metabolized by CYP3A47.12 Digoxin7.13 Gastrointestinal Motility Agents7.14 GlipizideE IN SPECIFIC POPULATIONS8.1Pregnancy8.3Nursing Mothers8.4Pediatric Use8.5Geriatric Use8.6Renal Insufficiency8.7Hepatic Insufficiency8.8Gender8.9Race10.OVERDOSAGE11.DESCRIPTION12.CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.2 Pharmacodynamics12.3 Pharmacokinetics12.4 Microbiology13. NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility13.2Animal Toxicology and/or Pharmacology14. CLINICAL STUDIES14.1Prophylaxis of Aspergillus and Candida Infections14.2Treatment of Oropharyngeal Candidiasis14.3Treatment of Oropharyngeal Candidiasis Refractory toTreatment With Fluconazole or Itraconazole16.HOW SUPPLIED/STORAGE AND HANDLING17.PATIENT COUNSELING INFORMATION17.1 Administration With Food17.2 Drug Interactions17.3 Serious and Potentially Serious Adverse Reactions17.4See Accompanying FDA-Approved Patient Labeling* Sections or subsections omitted from the full prescribing information are not listed.________________________________________________________FULL PRESCRIBING INFORMATION1. INDICATIONS AND USAGE1.1 Prophylaxis of Invasive Aspergillus and Candida InfectionsNOXAFIL Oral Suspension is indicated for prophylaxis of invasive Aspergillus and Candida infections in patients, 13 years of age and older, who are at high risk of developing these infections due to being severely immunocompromised, such as hematopoietic stem cell transplant (HSCT) recipients with graft-versus-host disease (GVHD) or those with hematologic malignancies with prolonged neutropenia from chemotherapy.1.2 Treatment of Oropharyngeal Candidiasis Including Oropharyngeal Candidiasis Refractory to Itraconazole and/or FluconazoleNOXAFIL is indicated for the treatment of oropharyngeal candidiasis, including oropharyngeal candidiasis refractory to itraconazole and/or fluconazole.2. DOSAGE AND ADMINISTRATION2.1DosageIndication Dose and Duration of TherapyProphylaxis of Invasive Fungal Infections 200 mg (5 mL) three times a day. The duration of therapy is based on recovery from neutropenia or immunosuppression.Oropharyngeal Candidiasis Loading dose of 100 mg (2.5 mL) twice a day on the first day, then100 mg (2.5 mL) once a day for 13 days.Oropharyngeal Candidiasis Refractory to itraconazole and/or fluconazole 400 mg (10 mL) twice a day. Duration of therapy should be based on the severity of the patient’s underlying disease and clinical response.2.2Administration InstructionsShake NOXAFIL Oral Suspension well before use.Figure 1: A measured dosing spoon is provided, marked for doses of 2.5 mL and 5 mL.It is recommended that the spoon is rinsed with water after each administration and before storage.Each dose of NOXAFIL should be administered with a full meal or with a liquid nutritional supplement or an acidic carbonated beverage (e.g. ginger ale) in patients who cannot eat a full meal.To enhance the oral absorption of posaconazole and optimize plasma concentrations:•Each dose of NOXAFIL should be administered during or immediately (i.e. within 20 minutes) following a full meal. In patients who cannot eata full meal, each dose of NOXAFIL should be administered with a liquid nutritional supplement or an acidic carbonated beverage. For patientswho cannot eat a full meal or tolerate an oral nutritional supplement or an acidic carbonated beverage, alternative antifungal therapy should be considered or patients should be monitored closely for breakthrough fungal infections.•Patients who have severe diarrhea or vomiting should be monitored closely for breakthrough fungal infections.•Co-administration of drugs that can decrease the plasma concentrations of posaconazole should generally be avoided unless the benefit outweighs the risk. If such drugs are necessary, patients should be monitored closely for breakthrough fungal infections [see Drug Interactions(7.6, 7.7, 7.8, 7.9, 7.13)].3. DOSAGE FORMS AND STRENGTHSNOXAFIL Oral Suspension is available in 4-ounce (123 mL) amber glass bottles with child-resistant closures (NDC 0085-1328-01) containing105 mL of suspension (40 mg of posaconazole per mL).4. CONTRAINDICATIONS4.1HypersensitivityNOXAFIL is contraindicated in persons with known hypersensitivity to posaconazole, any component of NOXAFIL, or other azole antifungal agents.4.2 Use With SirolimusNOXAFIL is contraindicated with sirolimus. Concomitant administration of NOXAFIL with sirolimus increases the sirolimus blood concentrations by approximately 9 fold and can result in sirolimus toxicity [see Drug Interactions (7.1) and Clinical Pharmacology (12.3)].4.3 QT Prolongation With Concomitant Use With CYP3A4 SubstratesNOXAFIL is contraindicated with CYP3A4 substrates that prolong the QT interval. Concomitant administration of NOXAFIL with the CYP3A4 substrates, pimozide and quinidine may result in increased plasma concentrations of these drugs, leading to QTc prolongation and rare occurrences of torsades de pointes [see Warnings and Precautions (5.2) and Drug Interactions (7.2)].4.4 Use With SimvastatinConcomitant administration of NOXAFIL with simvastatin increases the simvastatin plasma concentrations by approximately 10 fold. Increased plasma statin concentrations can be associated with rhabdomyolysis [see Drug Interactions (7.3) and Clinical Pharmacology (12.3)].4.5 Use With Ergot AlkaloidsPosaconazole may increase the plasma concentrations of ergot alkaloids (ergotamine and dihydroergotamine) which may lead to ergotism [see Drug Interactions (7.4)].5. WARNINGS AND PRECAUTIONS5.1 Calcineurin-Inhibitor Drug InteractionsConcomitant administration of NOXAFIL with cyclosporine or tacrolimus increases the whole blood trough concentrations of these calcineurin-inhibitors [see Drug Interactions (7.1) and Clinical Pharmacology (12.3)]. Nephrotoxicity and leukoencephalopathy (including isolated deaths) have been reported in clinical efficacy studies in patients with elevated cyclosporine concentrations. Frequent monitoring of tacrolimus or cyclosporine whole blood trough concentrations should be performed during and at discontinuation of posaconazole treatment and the tacrolimus or cyclosporine dose adjusted accordingly.5.2 Arrhythmias and QT ProlongationSome azoles, including posaconazole, have been associated with prolongation of the QT interval on the electrocardiogram. In addition, rare cases of torsades de pointes have been reported in patients taking posaconazole.Results from a multiple time-matched ECG analysis in healthy volunteers did not show any increase in the mean of the QTc interval. Multiple, time-matched ECGs collected over a 12-hour period were recorded at baseline and steady-state from 173 healthy male and female volunteers (18-85 years of age) administered posaconazole 400 mg BID with a high-fat meal. In this pooled analysis, the mean QTc (Fridericia) interval change from baseline was –5 msec following administration of the recommended clinical dose. A decrease in the QTc (F) interval (–3 msec) was also observed in a small number of subjects (n=16) administered placebo. The placebo-adjusted mean maximum QTc (F) interval change from baseline was <0 msec (–8 msec). No healthy subject administered posaconazole had a QTc (F) interval ≥500 msec or an increase ≥60 msec in their QTc (F) interval from baseline.Posaconazole should be administered with caution to patients with potentially proarrhythmic conditions. Do not administer with drugs that are known to prolong the QTc interval and are metabolized through CYP3A4 [see Contraindications (4.3) and Drug Interactions (7.2)]. Rigorous attempts to correct potassium, magnesium, and calcium should be made before starting posaconazole.5.3 Hepatic ToxicityHepatic reactions (e.g.,mild to moderate elevations in alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase, total bilirubin, and/or clinical hepatitis) have been reported in clinical trials. The elevations in liver function tests were generally reversible on discontinuation of therapy, and in some instances these tests normalized without drug interruption and rarely required drug discontinuation. Isolated cases of more severe hepatic reactions including cholestasis or hepatic failure including deaths have been reported in patients with serious underlying medical conditions (e.g., hematologic malignancy) during treatment with posaconazole. These severe hepatic reactions were seen primarily in subjects receiving the 800 mg daily (400 mg BID or 200 mg QID) in clinical trials.Liver function tests should be evaluated at the start of and during the course of posaconazole therapy. Patients who develop abnormal liver function tests during posaconazole therapy should be monitored for the development of more severe hepatic injury. Patient management should include laboratory evaluation of hepatic function (particularly liver function tests and bilirubin). Discontinuation of posaconazole must be considered if clinical signs and symptoms consistent with liver disease develop that may be attributable to posaconazole.5.4 Use With MidazolamConcomitant administration of NOXAFIL with midazolam increases the midazolam plasma concentrations by approximately 5 fold. Increased plasma midazolam concentrations could potentiate and prolong hypnotic and sedative effects. Patients must be monitored closely for adverse effects associated with high plasma concentrations of midazolam and benzodiazepine receptor antagonists must be available to reverse these effects [see Drug Interactions (7.5) and Clinical Pharmacology (12.3)].6. ADVERSE REACTIONS6.1 Serious and Otherwise Important Adverse ReactionsThe following serious and otherwise important adverse reactions are discussed in detail in another section of the labeling: • Hypersensitivity[see Contraindications (4.1)]•Arrhythmias and QT Prolongation [see Warnings and Precautions (5.2)][see Warnings and Precautions (5.3)]• HepaticToxicity6.2 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in clinical trials of NOXAFIL cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.The safety of posaconazole therapy has been assessed in 1844 patients in clinical trials. This includes 605 patients in the active-controlled prophylaxis studies, 557 patients in the active-controlled OPC studies, 239 patients in refractory OPC studies, and 443 patients from other indications. Thisrepresents a heterogeneous population, including immunocompromised patients, e.g., patients with hematological malignancy, neutropenia post-chemotherapy, graft vs. host disease post hematopoietic stem cell transplant, and HIV infection, as well as non-neutropenic patients. This patient population was 71% male, had a mean age of 42 years (range 8-84 years, 6% of patients were ≥65 years of age and 1% was <18 years of age), and were 64% white, 16% Hispanic, and 36% non-white (including 14% black). Posaconazole therapy was given to 171 patients for ≥6 months, with 58 patients receiving posaconazole therapy for ≥12 months. Table 1 presents treatment-emergent adverse reactions observed at an incidence of >10% in posaconazole prophylaxis studies. Table 2 presents treatment-emergent adverse reactions observed at an incidence of at least 10% in the OPC/rOPC studies.Prophylaxis of Aspergillus and Candida: In the 2 randomized, comparative prophylaxis studies, the safety of posaconazole 200 mg threetimes a day was compared to fluconazole 400 mg once daily or itraconazole 200 mg twice a day in severely immunocompromised patients.The most frequently reported adverse reactions (>30%) in the prophylaxis clinical trials were fever, diarrhea and nausea.The most common adverse reactions leading to discontinuation of posaconazole in the prophylaxis studies were associated with GI disorders,specifically, nausea (2%), vomiting (2%), and hepatic enzymes increased (2%).TABLE 1: Study 1 and Study 2. Number (%) of Randomized Subjects Reporting Treatment-Emergent Adverse Reactions: Frequency of at Least 10% in the Posaconazole or Fluconazole Treatment Groups (Pooled Prophylaxis Safety Analysis)Body SystemPreferred Term Posaconazole(n=605)Fluconazole(n=539)Itraconazole(n=58)Subjects Reporting any Adverse Reaction 595 (98) 531 (99) 58 (100) Body as a Whole - General DisordersFever 274 (45) 254 (47) 32 (55) Headache 171 (28) 141 (26) 23 (40) Rigors 122 (20) 87 (16) 17 (29) Fatigue 101 (17) 98 (18) 5 (9) Edema Legs 93 (15) 67 (12) 11 (19) Anorexia 92 (15) 94 (17) 16 (28) Dizziness 64 (11) 56 (10) 5 (9) Edema 54 (9) 68 (13) 8 (14) Weakness 51 (8) 52 (10) 2 (3) Cardiovascular Disorders, GeneralHypertension 106 (18) 88 (16) 3 (5) Hypotension 83 (14) 79 (15) 10 (17) Disorders of Blood and Lymphatic SystemAnemia 149 (25) 124 (23) 16 (28) Neutropenia 141 (23) 122 (23) 23 (40) Febrile Neutropenia 118 (20) 85 (16) 23 (40) Disorders of the Reproductive System and BreastVaginal Hemorrhage* 24 (10) 20 (9) 3 (12) Gastrointestinal System DisordersDiarrhea 256 (42) 212 (39) 35 (60) Nausea 232 (38) 198 (37) 30 (52) Vomiting 174 (29) 173 (32) 24 (41) Abdominal Pain 161 (27) 147 (27) 21 (36) Constipation 126 (21) 94 (17) 10 (17) Mucositis NOS 105 (17) 68 (13) 15 (26) Dyspepsia 61 (10) 50 (9) 6 (10) Heart Rate and Rhythm DisordersTachycardia 72 (12) 75 (14) 3 (5) Infection and InfestationsBacteremia 107 (18) 98 (18) 16 (28) Herpes Simplex 88 (15) 61 (11) 10 (17) Cytomegalovirus Infection 82 (14) 69 (13) 0Pharyngitis 71 (12) 60 (11) 12 (21)Upper Respiratory Tract Infection 44 (7) 54 (10) 5 (9)Liver and Biliary System DisordersBilirubinemia 59 (10) 51 (9) 11 (19)Metabolic and Nutritional DisordersHypokalemia 181 (30) 142 (26) 30 (52)Hypomagnesemia 110 (18) 84 (16) 11 (19)Hyperglycemia 68 (11) 76 (14) 2 (3)Hypocalcemia 56 (9) 55 (10) 5 (9)Musculoskeletal System DisordersMusculoskeletal Pain 95 (16) 82 (15) 9 (16)Arthralgia 69 (11) 67 (12) 5 (9)Back Pain 63 (10) 66 (12) 4 (7)Platelet, Bleeding and Clotting DisordersThrombocytopenia 175 (29) 146 (27) 20 (34)Petechiae 64 (11) 54 (10) 9 (16)Psychiatric DisordersInsomnia 103 (17) 92 (17) 11 (19)Anxiety 52 (9) 61 (11) 9 (16)Respiratory System DisordersCoughing 146 (24) 130 (24) 14 (24)Dyspnea 121 (20) 116 (22) 15 (26)Epistaxis 82 (14) 73 (14) 12 (21)Skin and Subcutaneous Tissue DisordersRash 113 (19) 96 (18) 25 (43)Pruritus 69 (11) 62 (12) 11 (19)* Percentages of sex-specific adverse reactions are based on the number of males/females.NOS = not otherwise specified.HIV Infected Subjects With OPC: In 2 randomized comparative studies in OPC, the safety of posaconazole at a dose of ≤400 mg QD in 557 HIV-infected patients was compared to the safety of fluconazole in 262 HIV-infected patients at a dose of 100 mg QD.An additional 239 HIV-infected patients with refractory OPC received posaconazole in 2 non-comparative trials for refractory OPC (rOPC).Of these subjects, 149 received the 800-mg/day dose and the remainder received the ≤400-mg QD dose.In the OPC/rOPC studies, the most common adverse reactions were fever, diarrhea, nausea, headache, and vomiting.The most common adverse reactions that led to treatment discontinuation of posaconazole in the Controlled OPC Pool included respiratory insufficiency (1%) and pneumonia (1%). In the refractory OPC pool, the most common adverse reactions that led to treatment discontinuation of posaconazole were AIDS (7%) and respiratory insufficiency (3%).TABLE 2: Treatment-Emergent Adverse Reactions With Frequency of at Least 10% in OPC Studies (Treated Population)Number (%) of SubjectsControlled OPC Pool Refractory OPC PoolPosaconazole Fluconazole PosaconazoleBody SystemPreferred Term n=557 n=262 n=239356 (64) 175 (67) 221 (92)Subjects Reporting any AdverseReaction*Body as a Whole – General DisordersFever 34 (6) 22 (8) 82 (34)Headache 44 (8) 23 (9) 47 (20)Anorexia 10 (2) 4 (2) 46 (19)Fatigue 18 (3) 12 (5) 31 (13)Asthenia 9 (2) 5 (2) 31 (13)Rigors 2 (<1) 4 (2) 29 (12)Pain 4 (1) 2 (1) 27 (11)Disorders of Blood and Lymphatic SystemNeutropenia 21 (4) 8 (3) 39 (16)Anemia 11 (2) 5 (2) 34 (14)Gastrointestinal System DisordersDiarrhea 58 (10) 34 (13) 70 (29)Nausea 48 (9) 30 (11) 70 (29)Vomiting 37 (7) 18 (7) 67 (28)Abdominal Pain 27 (5) 17 (6) 43 (18)Infection and InfestationsCandidiasis, Oral 3 (1) 1 (<1) 28 (12)Herpes Simplex 16 (3) 8 (3) 26 (11)Pneumonia 17 (3) 6 (2) 25 (10)Metabolic and Nutritional DisordersWeight Decrease 4 (1) 2 (1) 33 (14)Dehydration 4 (1) 7 (3) 27 (11)Psychiatric DisordersInsomnia 8 (1) 3 (1) 39 (16)Respiratory System DisordersCoughing 18 (3) 11 (4) 60 (25)Dyspnea 8 (1) 8 (3) 28 (12)Skin and Subcutaneous Tissue DisordersRash 15 (3) 10 (4) 36 (15)Sweating Increased 13 (2) 5 (2) 23 (10)OPC=oropharyngeal candidiasis; SGOT=serum glutamic oxaloacetic transaminase (same as AST);SGPT=serum glutamic pyruvic transaminase (same as ALT).* Number of subjects reporting treatment-emergent adverse reactions at least once during the study,without regard to relationship to treatment. Subjects may have reported more than 1 event.Adverse reactions were reported more frequently in the pool of patients with refractory OPC. Among these highly immunocompromised patients with advanced HIV disease, serious adverse reactions (SARs) were reported in 55% (132/239). The most commonly reported SARs were fever (13%) and neutropenia (10%).Less Common Adverse Reactions: Clinically significant adverse reactions reported during clinical trials in prophylaxis, OPC/rOPC or other trials with posaconazole which occurred in less than 5% of patients are listed below:•Blood and lymphatic system disorders: hemolytic uremic syndrome, thrombotic thrombocytopenic purpura, neutropenia aggravated •Endocrine disorders: adrenal insufficiency•Nervous system disorders: paresthesia•Immune system disorders: allergic reaction [see Contraindications (4.1)]•Cardiac disorders: Torsades de pointes [see Warnings and Precautions (5.2)]•Vascular disorders: pulmonary embolism•Liver and Biliary System Disorders: bilirubinemia, hepatic enzymes increased, hepatic function abnormal, hepatitis, hepatomegaly, jaundice, SGOT Increased, SGPT Increased•Metabolic and Nutritional Disorders: Hypokalemia•Platelet, Bleeding, and Clotting Disorders: Thrombocytopenia•Renal & Urinary System Disorders: Renal Failure AcuteClinical Laboratory Values: In healthy volunteers and patients, elevation of liver function test values did not appear to be associated with higher plasma concentrations of posaconazole. The majority of abnormal liver function tests were minor, transient, and did not lead to discontinuation of therapy.For the prophylaxis studies, the number of patients with changes in liver function tests from Common Toxicity Criteria (CTC) Grade 0, 1, or 2 at baseline to Grade 3 or 4 during the study is presented in Table 3.TABLE 3: Study 1 and Study 2. Changes in Liver Function Test Results From CTC Grade 0, 1, or 2 at Baseline to Grade 3 or 4Number (%) of Patients With Change*Study 1Laboratory Parameter Posaconazolen=301Fluconazolen=299AST 11/266 (4) 13/266 (5)Number (%) of Patients With Change*ALT 47/271 (17) 39/272 (14) Bilirubin 24/271 (9) 20/275 (7) Alkaline Phosphatase 9/271 (3) 8/271 (3)Study 2Laboratory Parameter Posaconazole(n=304)Fluconazole/Itraconazole(n=298)AST 9/286 (3) 5/280 (2)ALT 18/289 (6) 13/284 (5)Bilirubin 20/290 (7) 25/285 (9)Alkaline Phosphatase 4/281 (1) 1/276 (<1)* Change from Grade 0 to 2 at baseline to Grade 3 or 4 during the study.These data are presented in the form X/Y, where X represents the numberof patients who met the criterion as indicated, and Y represents the numberof patients who had a baseline observation and at least one post-baselineobservation.CTC = Common Toxicity Criteria; AST= Aspartate Aminotransferase;ALT= Alanine Aminotransferase.The number of patients treated for OPC with clinically significant liver function test (LFT) abnormalities at any time during the studies is provided in Table 4. (LFT abnormalities were present in some of these patients prior to initiation of the study drug).TABLE 4: Clinically Significant Laboratory Test Abnormalities Without Regard to Baseline ValueControlled RefractoryPosaconazole Fluconazole PosaconazoleLaboratory Test n= 557(%) n=262(%) n=239(%)ALT > 3.0 x ULN 16/537 (3) 13/254 (5) 25/226 (11)AST > 3.0 x ULN 33/537 (6) 26/254(10)39/223 (17)Total Bilirubin > 1.5 x ULN 15/536 (3) 5/254 (2) 9/197 (5)Alkaline Phosphatase > 3.0 x ULN 17/535 (3) 15/253 (6) 24/190 (13)ALT= Alanine Aminotransferase; AST= Aspartate Aminotransferase.6.3 Postmarketing ExperienceNo clinically significant postmarketing adverse reactions were identified that have not previously been reported during clinical trials experience.7. DRUG INTERACTIONSPosaconazole is primarily metabolized via UDP glucuronidation and is a substrate of p-glycoprotein efflux. Therefore, inhibitors or inducers of these clearance pathways may affect posaconazole plasma concentrations. Posaconazole is also a strong inhibitor of CYP3A4. Therefore, plasma concentrations of drugs predominantly metabolized by CYP3A4 may be increased by posaconazole [see Clinical Pharmacology (12.3)].7.1 Immunosuppressants Metabolized by CYP3A4Sirolimus: Concomitant administration of posaconazole with sirolimus increases the sirolimus blood concentrations by approximately 9 fold and can result in sirolimus toxicity. Therefore, posaconazole is contraindicated with sirolimus [see Contraindications (4.2) and Clinical Pharmacology (12.3)].Tacrolimus: Posaconazole has been shown to significantly increase the C max and AUC of tacrolimus. At initiation of posaconazole treatment, reduce the tacrolimus dose to approximately one-third of the original dose. Frequent monitoring of tacrolimus whole blood trough concentrations should be performed during and at discontinuation of posaconazole treatment and the tacrolimus dose adjusted accordingly [see Warnings and Precautions (5.1) and Clinical Pharmacology (12.3)].Cyclosporine: Posaconazole has been shown to increase cyclosporine whole blood concentrations in heart transplant patients upon initiation of posaconazole treatment. It is recommended to reduce cyclosporine dose to approximately three-fourths of the original dose upon initiation of posaconazole treatment. Frequent monitoring of cyclosporine whole blood trough concentrations should be performed during and at discontinuation of posaconazole treatment and the cyclosporine dose adjusted accordingly [see Warnings and Precautions (5.1) and Clinical Pharmacology (12.3)].7.2 CYP3A4 SubstratesConcomitant administration of posaconazole with CYP3A4 substrates such as pimozide and quinidine may result in increased plasma concentrations of these drugs, leading to QTc prolongation and rare occurrences of torsades de pointes. Therefore, posaconazole is contraindicated with these drugs. [see Contraindications (4.3), and Warnings and Precautions (5.2)].。
评价泊沙康唑预防血液系统疾病患者粒细胞缺乏期侵袭性真菌病的效果

评价泊沙康唑预防血液系统疾病患者粒细胞缺乏期侵袭性真菌病的效果徐宵寒;张路;段明辉【摘要】目的评价泊沙康唑作为血液系统疾病患者粒细胞缺乏期侵袭性真菌病(IFD)预防用药的疗效和安全性.方法通过回顾性分析北京某院2014-2015年18例血液系统疾病患者在粒细胞缺乏期应用泊沙康唑单药预防IFD的病历,评价其疗效和安全性.结果 18例患者中,预防用药期间无1例出现临床诊断或确诊IFD,无1例因严重不良反应停用泊沙康唑.2例急性髓系白血病(AML)患者因肺部感染死亡,其中1例在预防用药第12天痰培养出嗜麦芽窄食单胞菌,另1例在预防用药第14天痰培养出大肠埃希菌.其余患者均坚持预防用药至粒细胞计数恢复,随访至预防用药100 d后无死亡.预防用药期间最低外周血中性粒细胞计数为(0.00~0.27)×109/L,中位数为0.02×109/L;泊沙康唑预防用药持续时间为8~27 d,中位数为16 d;无IFD突破以及合并全身性使用其他抗真菌药者,100日内全因死亡2例(11.1%);未出现2级及以上肝功能异常、2级及以上肾功能异常以及QTc延长等不良反应.结论应用泊沙康唑预防该组血液系统疾病患者粒细胞缺乏期IFD有效,也未出现严重不良反应.%Objective To evaluate the prophylactic efficacy and safety of posaconazole against invasive fungal disease(IFD)in hematologic patients with neutropenia.Methods Medical records of 18 hematologic patients with neutropenia received posaconazole for preventing IFD in a Beijing hospital between 2014 and 2015,the efficacy and safety was evaluated.Results There was no clinical diagnosis or confirmed diagnosis of IFD among 18 patients during posaconazole prophylaxis period,none of patients stopped posaconazole due to severe adverse reaction.Twopatients with acute myeloid leukemia(AML) died of pulmonary infection,1 of whom isolated Stenotrophomonas maltophilia from sputum culture on the 12th day of posaconazole prophylaxis,the other isolated Escherichia coli from sputum culture on the 14th day of posaconazole prophylaxis.Other patients all adherence to posaconazole prophylaxis until granulocyte count recovered,patients were followed up until 100 days medication,no death occurred.The lowest peripheral neutrophil count was(0.00-0.27) x 109/L during posaconazole prophylaxis period,with the median of 0.02 x 109/L;the duration of posaconazole prophylaxis was 8-27days,with the median of 16 days;among patients without IFD breakthrough or received systemic use of other antifungal agents,there were 2 (11.1%) all-cause death within 100 days;there were no adverse reaction,such as liver function abnormalities≥grade 2 and kidney function abnormalities≥grade 2,as well as QTc prolongation.Conclusion Posaconazole is effective for preventing IFD in hematologic patients with neutropenia,adverse reaction is rare.【期刊名称】《中国感染控制杂志》【年(卷),期】2017(016)001【总页数】5页(P32-35,57)【关键词】泊沙康唑;急性白血病;再生障碍性贫血;粒细胞缺乏;侵袭性真菌病;预防用药【作者】徐宵寒;张路;段明辉【作者单位】中国医学科学院北京协和医院,北京100730;中国医学科学院北京协和医院,北京100730;中国医学科学院北京协和医院,北京100730【正文语种】中文【中图分类】R519;R733侵袭性真菌病(invasive fungal disease,IFD)是血液系统疾病患者粒细胞缺乏(外周血中性粒细胞计数<0.5×109/L)期的主要并发症和致死原因之一[1],且近年来发生率呈升高趋势[2],IFD发生率与粒细胞缺乏期的持续时间以及宿主的免疫抑制程度相关[3],所以粒细胞缺乏期较长是IFD发生的高危因素,如急性白血病(acute leukemia,AL)诱导治疗期患者和重型再生障碍性贫血(severe aplastic anemia,SAA)患者。
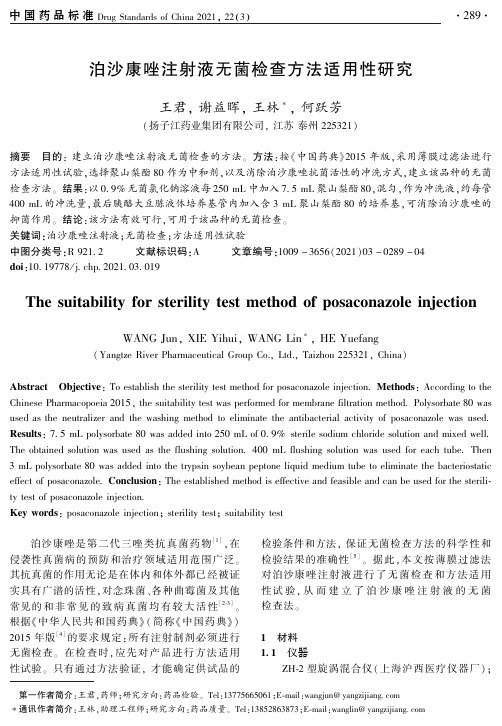
泊沙康唑注射液无菌检查方法适用性研究
67
白色念珠菌(Candida albicans)
50
黑曲霉(Aspergillus niger)
平均
1
(average)
57
62
60
40
77
75
60
61
62
65
51
51
表 2 培养基灵敏度检查结果
Tab 2 The sensitivity test results of culture medium
1 3 试验用菌种( 第 4 代)
[6]
金黄色葡萄球菌 CMCC( B)26003ꎬ枯草芽孢杆
菌 CMCC( B) 63501ꎬ大肠埃希菌 CMCC ( B) 44102ꎬ
菌、铜绿假单胞菌、生孢梭菌各 2 支ꎬ另 1 支不接种
的胰酪大豆胨液体培养基 7 支ꎬ分别接种 1 mL 小于
100 cfumL - 1 的枯草芽孢杆菌、白色念珠菌、黑曲
0 9% 无菌氯化钠溶液 ( 批号:17082841 ) 为扬
分别接种 1 mL 小于 100 cfumL - 1 的金黄色葡萄球
聚山梨酯 80( 批号:SH1 ̄19040404) ꎬ 由国药集
作为空白对照ꎬ30 ~ 35 ℃ 培养培养 3 dꎻ取每管 9 mL
子江药业集团有限公司自制ꎮ
团化学试剂有限公司提供ꎮ
400 mL 的冲洗量ꎬ最后胰酪大豆胨液体培养基管内加入含 3 mL 聚山梨酯 80 的培养基ꎬ可消除泊沙康唑的
抑菌作用ꎮ 结论:该方法有效可行ꎬ可用于该品种的无菌检查ꎮ
关键词:泊沙康唑注射液ꎻ无菌检查ꎻ方法适用性试验
中图分类号:R 921 2 文献标识码:A 文章编号:1009 - 3656(2021)03 - 0289 - 04
2014年上半年美国FDA批准药物简介

改变患者群
Upsher鄄Smith Laboratories
癫痫发作
依索拉唑(esomeprazole)
新非处方剂型
Pfizer
胃灼热
混合花粉变应原提取物
新生物制品
Stallergenes S.A.
草花粉诱发过敏性鼻炎
盐酸纳洛酮(naloxone)
新剂型
Kaleo
可疑阿片过量
达比加群酯(dabigatran etexilate) 新适应证
新剂型
Teva
多发性硬化症
他美替胺(tasimelteon)
新分子实体 2
Vanda Pharmaceuticals
偏头痛
依罗替尼(ibrutinib)
新适应证
East Hanover
套细胞淋巴瘤
α鄄埃洛硫酸酯酶(elosulfase alfa) 新生物制品 4
BioMarin Pharmaceutical
新缓释剂型 新静脉注射剂 新剂型或制造商
Upsher鄄Smith Laboratories
Merck Pierre Fabre Dermatologi
癫痫发作 预防侵袭性曲霉 婴幼儿血管瘤
阿哌沙班(apixaban) 米替福新(miltefosine) 阿普斯特(apremilast)
新适应证 新分子实体 2,3 新分子实体
色瑞替尼(ceritinib)
新分子实体 1,2,5
Novartis
肺癌
vorapaxar
新分子实体
Merck
心脏病发作和卒中
维多珠单抗(vedolizumab)
新重组蛋白
Takeda Pharmaceutical
溃疡结肠炎或克罗恩病
新型抗真菌药简介

新型抗真菌药简介当前真菌感染治疗面临很多挑战,侵袭性真菌感染死亡率居高不下、抗真菌药物的耐药性逐渐上升、多重耐药和高致死率的“超级真菌”的出现、抗真菌治疗疗程长、可选用的联合治疗方案有限以及抗真菌药物的安全性及药物相互作用问题等等。
再加上抗真菌药物的可及性相对较差,新型抗真菌药物具有巨大市场需求。
抗真菌药物近些年来有较好的发展,全球范围内新作用机制及新型抗真菌药物不断出现。
王明贵教授谈到,在中国,近年上市或即将上市的抗真菌药物也相对较多。
近年中国上市的抗真菌新药原研泊沙康唑在2022年之前的适应证为预防真菌感染,其混悬液、片剂和注射剂分别于2013、2018和2021年上市。
2022年3月原研泊沙康唑的片剂及注射剂被批准用于治疗侵袭性曲霉菌病。
国产泊沙康唑于2021年4月上市了片剂和注射剂,用于预防曲霉及念珠菌感染。
原研艾沙康唑胶囊于2021年12月被批准上市,用于治疗侵袭性曲霉病、毛霉病。
注射用艾沙康唑也于2022年6月获批上市。
除了艾沙康唑,毛霉病也可选择两性霉素B类进行药物治疗。
两性霉素B去氧胆酸盐不良反应较大,两性霉素B含脂制剂可使与输注相关的不良反应和肾毒性明显减少。
国产两性霉素B胆固醇硫酸酯复合物(ABCD)于2021年3月正式上市,用于治疗各类真菌病,同年该药进入医保国谈品种。
除此之外,原研脂质体两性霉素B(L-AMB)目前也处于审批当中。
正在进行或即将开展Ⅲ期临床试验的抗真菌新药目前也有一些其他药物在中国正在进行或者即将进入Ⅲ期临床试验中。
Rezafungin属于棘白菌素类药物,在国内的临床试验已经开展一段时间。
Ibrexafungerp(艾瑞芬净,IBX)作为首个全新三萜类结构的糖原合成酶抑制剂,其虽然为棘白菌素的衍生物,但IBX也可视为新作用机制的第四代抗真菌类药物。
IBX治疗念珠菌阴道炎疗效好,复发率低。
Fosmanogepix是一种新作用机制的抗真菌药物,对于曲霉病和毛霉病都可起到治疗效果,未来也将在中国开展临床试验。
泊沙康唑预防和治疗侵袭性真菌病

47(1-2): p. 40-6.
毛霉菌感染
• 毛霉菌分布极为广泛,土壤、空气、食物中均较常见。 毛霉菌易感者主要是白血病及恶性肿瘤化疗所致中性粒 细胞减少的患者。
• 美国一项人群监测项目报告在1992年至1993年间毛霉菌 的发病率为1.7/100万人 [1] 。
• 欧洲的2004年SEIFEM数据调查表明毛霉病病死率在血液 肿瘤病人中接近65% [2]。
细胞色素P450同工酶的抑制剂或诱导剂 --- 三唑类之间存在很大差异
泊沙康唑仅仅作为CYP3A4的抑制剂与P450酶系统存在相互作用
Dodds Ashley ES, CID 2006; 43: S28-39
泊沙康唑: 可能的药物相互作用
• 泊沙康唑主要以原型形式排泄
• 仅抑制CYP3A4,不抑制其他的同工酶1 • 不是CYP酶的底物,因此不会受到这些酶的诱导剂或者抑制
Time, h
3. Courtney R, Wexler D, Radwanski E, et al. Br J Clin Pharmacol.
2004;57:218–222.
26
可编辑
唑类的与细胞色素P450酶的相互作用
• 泊沙康唑不是CYP酶系统底物11 • 仅抑制CYP3A412
11. Drug interactions. Med Letter. 2003;45(W1158B):46–48. 12. Wexler D, et al. Eur J Pharm Sci. 2004;21:645-653.
泊沙康唑Noxafil(posaconazole)静脉注射剂

“Noxafil静脉剂型特别适用于需要静脉给药或者不能口服用药的患者。而且,部分患者可在初始治疗时选用Noxafil注射剂,之后逐渐转为口服剂型等。”Merck传染病研究室执行董事Nicholas Kartsonis表示。
Noxafil的获批,是基于一项药代动力学研究。该项研究是一项非对照、多中心临床研究,在已发生或预期将发生显著中性粒细胞减少(neutropenia)的急性髓性系白血病(AML)或骨髓增生异常综合症(MDS)患者、以及已接受造血干细胞移植(HSCT)同时正接受免疫抑制治疗以预防移植物抗宿主病(GVHD)的患者中开展中,评价了Noxafil的药代动力学、安全性和耐受性。
Merck的三唑抗真菌药泊沙康唑(posaconazole,Noxafil)静脉注射剂获得美国食品和药物管理局(FDA)批准。
此前,Noxafil的缓释片剂型已于2013年11月获FDA批准。目前有两种剂型,分别为100mg缓释片和40mg/ml口服混悬液。据了解,缓释片和口服混悬液剂型适用于13岁以上患者,而使用新的静脉用剂型患者要在18岁以上。
OPC耐火材料(ROPC),以伊曲康唑和/或氟康唑400毫克(10毫升),每日两次。治疗持续时间,应根据患者的潜在疾病的严重性和临床反应。
【如何购买】
美国是医药分开的国家,药房全部实行严格的处方药与非处方药分类管理。对处方药的销售,必须凭美国医生(电子/纸质)处方。如今国内患者可以依托科技,通过好医友国际医疗平台实现远程的病历交互,由美国医生根据患者病情开具电子处方,以正规渠道在好医友美国药房购买到处方药。
【禁忌】
·切勿管理与已知的过敏泊沙康唑, Noxafil的任何组件或其他唑类抗真菌药人。
·请勿共同使用Noxafil与下列药物; Noxafil增加浓度:
泊沙康唑临床应用专家共识

属于第二代三唑类抗真菌药物,其抗菌谱和药物代
代氯,同时侧链进行羟基化,一系列结构改造使其
谢过程有别于其他三唑类药物,口服混悬液、肠溶
和真菌亲和 力 更 强,稳 定 性 更 高,细 胞 毒 性 增 加,
片和注射剂分别于 2005、2013 和 2014 年经美国食
品药品监督管理局批准先后上市。在我国,泊沙康
片多中 心 PK 研 究 (n =65,AML/MDS) 显 示,
[ ]
泊沙康唑在预防和治疗肺真菌病时,虽然血药浓度
泊沙 康 唑 在 体 内 消 除 缓 慢, 半 衰 期 为 27~
35h,其中仅 约 的 药 物 在 肝 脏 转 化 为 多 种 形
式的 葡 萄 苷 酸 化 衍 生 物 经 肾 脏 排 泄, 而 大 部 分
s
sn 1673
436X 2020 04 001
近年来,随 着 各 类 免 疫 缺 陷 人 群 及 危 重 疾 患
的增多, 侵 袭 性 真 菌 病 (
i
nva
s
i
vef
unga
ld
i
s
e
a
s
e,
[
1
5]
, 且 非 白 念 珠 菌、
IFD)的整体发病 率 逐 年 上 升
曲霉及毛霉等 真 菌 感 染 的 比 例 在 血 液 科、 呼 吸 科、
范围广泛。本共识对泊沙康唑的 临 床 药 理 特 性、 现 有 临 床 研 究 资 料 以 及 编 写 组 专 家 的 临 床 应 用
经验进行了系统的复习和总结, 在 此 基 础 上 对 其 临 床 应 用 做 出 了 全 面 建 议, 这 些 建 议 涉 及 了 泊
沙康唑在预防和治疗侵袭性真 菌 病 中 的 临 床 应 用 原 则、 在 特 殊 人 群 中 的 使 用 原 则、 治 疗 药 物 监
泊沙康唑化学结构式

泊沙康唑化学结构式
泊沙康唑是一种广谱抗真菌药物,常用于治疗真菌感染疾病。
它的化学结构式如下:
C17H13ClN4
泊沙康唑的分子式为C17H13ClN4,它是一种白色晶体粉末,在水中溶解度较低。
泊沙康唑属于三唑类抗真菌药物,通过抑制真菌细胞壁合成的酵母菌色素14α-脱甲基酶,从而阻断真菌细胞壁酵母菌色素的合成,最终导致真菌细胞死亡。
泊沙康唑具有广谱的抗真菌活性,可以有效治疗多种真菌感染疾病,包括念珠菌属、白念珠菌属、皮肤癣菌属等引起的感染。
它可以通过口服或外用的方式使用,用于治疗口腔念珠菌感染、阴道念珠菌感染、皮肤癣等疾病。
泊沙康唑的药理作用机制是通过抑制真菌的细胞壁合成,阻断真菌的生长和繁殖。
它与真菌细胞内的酵母菌色素14α-脱甲基酶结合,干扰酵母菌色素的合成过程,导致真菌细胞壁的合成受阻,最终导致真菌细胞死亡。
泊沙康唑在临床上的应用非常广泛,它可以治疗口腔念珠菌感染、阴道念珠菌感染、皮肤癣等常见真菌感染疾病。
在使用泊沙康唑治疗真菌感染时,需要根据病情和患者的具体情况确定剂量和疗程。
泊沙康唑作为一种抗真菌药物,虽然效果显著,但也有一定的不良反应。
常见的不良反应包括恶心、呕吐、腹泻、头痛等。
在使用泊沙康唑治疗时,应遵医嘱,注意药物的正确使用和剂量控制,以减少不良反应的发生。
总的来说,泊沙康唑是一种广谱抗真菌药物,可以有效治疗多种真菌感染疾病。
它通过抑制真菌细胞壁合成的酵母菌色素14α-脱甲基酶,从而阻断真菌细胞壁酵母菌色素的合成,最终导致真菌细胞死亡。
在使用泊沙康唑治疗真菌感染时,需要根据病情和患者的具体情况确定剂量和疗程,并注意药物的不良反应。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
泊沙康唑Noxafil(posaconazole)静脉注射剂
Merck的三唑抗真菌药泊沙康唑(posaconazole,Noxafil)静脉注射剂获得美国食品和药物管理局(FDA)批准。
此前,Noxafil的缓释片剂型已于2013年11月获FDA批准。
目前有两种剂型,分别为100mg缓释片和40mg/ml口服混悬液。
据了解,缓释片和口服混悬液剂型适用于13岁以上患者,而使用新的静脉用剂型患者要在18岁以上。
“Noxafil静脉剂型特别适用于需要静脉给药或者不能口服用药的患者。
而且,部分患者可在初始治疗时选用Noxafil注射剂,之后逐渐转为口服剂型等。
”Merck传染病研究室执行董事Nicholas Kartsonis表示。
Noxafil的获批,是基于一项药代动力学研究。
该项研究是一项非对照、多中心临床研究,在已发生或预期将发生显著中性粒细胞减少(neutropenia)的急性髓性系白血病(AML)或骨髓增生异常综合症(MDS)患者、以及已接受造血干细胞移植(HSCT)同时正接受免疫抑制治疗以预防移植物抗宿主病(GVHD)的患者中开展中,评价了Noxafil 的药代动力学、安全性和耐受性。
附药品部分重点处方资料:
【适应症】
Noxafil是一种三唑类抗真菌药表示为:
·侵袭性曲霉菌和念珠菌感染的患者中,13岁及以上,谁在发展这些感染,由于受到严重免疫功能低下,如造血干细胞移植受者移植物抗宿主或那些与恶性血液病与化疗延长中性粒细胞减少高风险预防。
·治疗口咽念珠菌病(OPC),包括OPC耐火材料(ROPC),伊曲康唑和/或氟康唑。
【剂型和规格】
每毫升Noxafil口服混悬液40毫克。
【剂量与用法】
适应症剂量和治疗时间
侵袭性真菌感染的预防200毫克(5毫升),一天三次。
治疗持续时间是基于来自嗜中性白血球或免疫抑制的恢复。
口咽念珠菌病(OPC)装载的100毫克(2.5毫升)的剂量每天两次的第一天,然后100毫克(2.5毫升),每日一次,连续13天。
OPC耐火材料(ROPC),以伊曲康唑和/或氟康唑400毫克(10毫升),每日两次。
治疗持续时间,应根据患者的潜在疾病的严重性和临床反应。
【如何购买】
美国是医药分开的国家,药房全部实行严格的处方药与非处方药分类管理。
对处方药的销售,必须凭美国医生(电子/纸质)处方。
如今国内患者可以依托科技,通过好医友国际医疗平台实现远程的病历交互,由美国医生根据患者病情开具电子处方,以正规渠道在好医友美国药房购买到处方药。
【禁忌】
·切勿管理与已知的过敏泊沙康唑,Noxafil的任何组件或其他唑类抗真菌药人。
·请勿共同使用Noxafil与下列药物;Noxafil增加
浓度:
·西罗莫司:可导致雷帕霉素毒性。
·CYP3A4底物(匹莫齐特,奎尼丁):可能导致QT间期延长和TdP的罕见事件。
·辛伐他汀:可导致横纹肌溶解症。
·麦角生物碱:可导致麦角中毒。
【警告和注意事项】
·钙调磷酸酶抑制剂毒性:环孢素或他克莫司Noxafil浓度增加;经常减少环孢素和他克莫司和监控浓度的剂量。
·心律失常及QT间期延长:Noxafil已经显示出延长QT间期和心动过速引起的罕见事件。
管理慎用给患者带来潜在的致心律失常的条件。
不管理与已知延长QT间期,并通过CYP3A4代谢的药物。
正确的K +,镁+ +和Ca + +开始Noxafil之前。
·肝毒性:在海拔肝功(一般是可逆的停药)可能发生。
应停药谁在治疗期间出现肝功异常或监测肝功能试验的患者可以考虑。
·蓝精灵:Noxafil能延长催眠/镇静作用。
监测病人和苯二氮受体拮抗剂应该可用。
【不良反应】
·常见的治疗出现不良反应(>30%)的预防研究是发热,腹泻和恶心。
·常见的治疗出现不良反应(>5%)控制的OPC游泳池腹泻,恶心,头痛,呕吐等。
常见的不良反应(>20%)在耐火材料的OPC池有发热,腹泻,恶心,呕吐。
【药物相互作用】
利福布汀,苯妥英,依非韦伦,西咪替丁,奥美拉唑避免联合用药,除非胜过风险的利益。
由CYP3A代谢的其他药物(他克莫司,环孢霉素,长春花生物碱类,钙通道阻滞剂)考虑调整剂量并监测不良反应和毒性。
地高辛监视器高辛血药浓度。
霉菌感染胃复安监控。
【特殊人群中使用】
·妊娠:根据动物数据,可能对胎儿造成伤害。
·哺乳母亲:请停止药物或哺乳期,同时在考虑到药物的重要性母亲。
·严重肾功能损害:密切留意突破真菌感染。