Divided Pretreatment to Targets and Intentions for Query Recommendation
pretreatment翻译

pretreatment翻译pretreatment的翻译是:预处理。
用法:pretreatment是一个名词,用于描述对某物进行预先处理的过程。
在科学、工业和医学领域,pretreatment常用于指代在实验、生产或治疗之前对样品、原料或病情进行预先处理的步骤。
预处理的目的可以是去除杂质、减少干扰、改善反应效果、提高效率等。
例句:1. The pretreatment of the soil sample involves removing debris and contaminants.土壤样品的预处理包括清除杂物和污染物。
2. For this experiment, the pretreatment of the testtubes includes sterilization and rinsing.在这个实验中,试管的预处理包括消毒和冲洗。
3. The pretreatment of the wastewater before treatmentwith a chemical agent is essential for optimal results.在用化学剂处理废水之前的预处理对于获得最佳结果至关重要。
4. Pretreatment of the raw material is necessary to ensure the quality of the final product.对原料进行预处理是为了确保最终产品的质量。
5. The pretreatment of the patient's condition involves conducting diagnostic tests and assessing medical history.对患者病情的预处理包括进行诊断检查和评估病史。
6. The pretreatment of the fabric involves washing and drying to remove any impurities.对面料的预处理包括清洗和烘干以去除任何杂质。
高三现代科技前沿探索英语阅读理解20题
高三现代科技前沿探索英语阅读理解20题1<背景文章>Artificial intelligence (AI) is rapidly transforming the field of healthcare. In recent years, AI has made significant progress in various aspects of medical care, bringing new opportunities and challenges.One of the major applications of AI in healthcare is in disease diagnosis. AI-powered systems can analyze large amounts of medical data, such as medical images and patient records, to detect diseases at an early stage. For example, deep learning algorithms can accurately identify tumors in medical images, helping doctors make more accurate diagnoses.Another area where AI is making a big impact is in drug discovery. By analyzing vast amounts of biological data, AI can help researchers identify potential drug targets and design new drugs more efficiently. This can significantly shorten the time and cost of drug development.AI also has the potential to improve patient care by providing personalized treatment plans. Based on a patient's genetic information, medical history, and other factors, AI can recommend the most appropriate treatment options.However, the application of AI in healthcare also faces some challenges. One of the main concerns is data privacy and security. Medicaldata is highly sensitive, and ensuring its protection is crucial. Another challenge is the lack of transparency in AI algorithms. Doctors and patients need to understand how AI makes decisions in order to trust its recommendations.In conclusion, while AI holds great promise for improving healthcare, it also poses significant challenges that need to be addressed.1. What is one of the major applications of AI in healthcare?A. Disease prevention.B. Disease diagnosis.C. Health maintenance.D. Medical education.答案:B。
英语1
The binding of certain ligands (ˈliɡənd)to their receptors may cause receptor-mediated internalization, which is often necessary if nanocarriers are to release drugs inside the cell16-18 . For example, a more significant therapeutic outcome was achieved whenimmunoliposomes targeted to human blood cancer (B-cell lymphoma) were labelled with an internalizing anti-CD19 ligand rather than a non-internalizing anti-CD20 ligand 19. In contrast, targeting nanocarriers to non-internalizing receptors may sometimes be advantageous in solid tumours owing to the bystander effect, where cells lacking the target receptor can be killed through drug release at the surface of the neighbouring cells, where carriers can bind结合特定的配体及其受体可能导致受体介导的内在,这往往是必要的,如果纳米是释放药物在cell16-18。
比如,一个更重要的治疗结果是实现时免疫针对人类血液癌症(B淋巴瘤)标记的内在抗CD19配体而不是一个非内部抗CD 20配体19。
生物分离工程的英语

生物分离工程的英语Biological Separation Engineering is a specialized field that focuses on the isolation and purification of biological products. It plays a crucial role in the pharmaceutical, food, and biotechnology industries, where the extraction ofbioactive compounds from natural sources is essential.The process typically begins with the selection of an appropriate feedstock, which could be anything from plant material to microorganisms. Once the feedstock is identified, it undergoes a series of steps to separate the desired components. These steps may include:1. Pre-treatment: This involves breaking down the complex structure of the feedstock to release the target molecules. Techniques such as mechanical disruption, enzymatic digestion, or chemical treatment may be used.2. Extraction: The target molecules are then extractedfrom the pre-treated material. This can be done using solvent extraction, where a solvent is used to dissolve the desired compounds, or by using methods like supercritical fluid extraction, which employs high-pressure gases to extract the compounds.3. Concentration: After extraction, the solution is often diluted and needs to be concentrated to increase the concentration of the target molecules. This can be achievedthrough evaporation, membrane filtration, or centrifugation.4. Purification: The concentrated solution may still contain impurities, so further purification is necessary. Chromatography is a common technique used at this stage, which separates molecules based on their affinity to the stationary phase.5. Polishing: The final step is to polish the purified product to ensure it meets the required specifications. This may involve additional rounds of purification or the use of specific techniques to remove any remaining impurities.Biological separation engineering is a complex process that requires a deep understanding of both the properties of the target molecules and the various separation techniques available. Advances in this field are continually improving the efficiency and selectivity of these processes, making it possible to produce high-quality biological products for a wide range of applications.。
染色质结构和功能的多面修饰物

SUMO:A Multifaceted Modifierof Chromatin Structure and FunctionCaelin Cuben˜as-Potts1and Michael J.Matunis1,*1Department of Biochemistry and Molecular Biology,Bloomberg School of Public Health,Johns Hopkins University,Baltimore,MD21205,USA*Correspondence:mmatunis@/10.1016/j.devcel.2012.11.020A major challenge in nuclear organization is the packaging of DNA into dynamic chromatin structures that can respond to changes in the transcriptional requirements of the cell.Posttranslational protein modifications,of histones and other chromatin-associated factors,are essential regulators of chromatin dynamics.In this Review,we summarize studies demonstrating that posttranslational modification of proteins by small ubiq-uitin-related modifiers(SUMOs)regulates chromatin structure and function at multiple levels and through a variety of mechanisms to influence gene expression and maintain genome integrity.IntroductionThe discovery of the nucleosome,the discovery of the iconic ‘‘beads on a string,’’andfinally the realization that there are higher-order chromatin-packing structures have made it clear that DNA is intricately organized.Since this time,significant prog-ress has been made in identifying the proteins responsible for higher-order DNA packaging and in understanding how regula-tion of these proteins affects chromatin structure.A major theme that has emerged is the important role of posttranslational protein modifications in modulating the functional accessibility of DNA. Of particular interest,recent global proteomic and genetic studies have linked modification by the small ubiquitin-related modifier(SUMO)to many processes involving chromatin, including transcriptional activation and repression,DNA replica-tion and repair,and chromosome segregation(Golebiowski et al., 2009;Makhnevych et al.,2009).Here,we review the current knowledge of how SUMO modification(sumoylation)of chro-matin-associated proteins regulates chromatin structure and function and thereby controls these essential cellular processes. After introducing the sumoylation pathway and general connections between SUMO and chromatin,we will discuss the complex role of sumoylation in both euchromatin and hetero-chromatin environments.First,the multiple mechanisms by which sumoylation modulates gene expression through effects on DNA methylation,histones,and transcriptional regulators will be reviewed.Subsequently,the functional role of sumoyla-tion in repetitive DNA structures,including ribosomal DNA (rDNA),telomeres,and centromeres will be discussed.We will highlight the unique functions of sumoylation within each of these domains,as well as its common role as a protector of genomic integrity.Several emerging themes will be reiterated throughout the Review.First,sumoylation often functions as a signal to facilitate protein-protein interactions on chromatin.These interactions may be simple heterodimeric associations,but they can also involve assembly of very large multiprotein complexes.Second, sumoylation also specifies multiple other fates,including effects on enzyme activity and changes in protein subcellular localiza-tion.And lastly,although in many cases sumoylation is linked to heterochromatin and gene inactivation,a growing number of studies indicate that sumoylation also plays important roles in enhancing chromatin accessibility and gene activation.Thus, the effects of sumoylation are dichotomous and often context dependent.SUMO Modification and FunctionMechanistically,sumoylation occurs through an enzyme cascade very similar to ubiquitylation(Figure1A).The SUMO paralogs are synthesized as precursor proteins that are cleaved by a family of SUMO isopeptidases referred to as SENPs (Mukhopadhyay and Dasso,2007).Mature SUMO is subse-quently activated by a heterodimeric E1activating enzyme (Aos1/Uba2),transferred to an E2conjugating enzyme(Ubc9), andfinally transferred to lysine residues in target proteins. This last step may be facilitated by the action of E3ligases, which,in addition to enhancing rates of sumoylation,are also believed to contribute to specificity(Gareau and Lima,2010; Johnson,2004).Substrate specificity in the sumoylation path-way,however,still remains poorly understood,because only a single E2enzyme and relatively few E3ligases have been iden-tified.Sumoylation is,however,highly dynamic and can be reversed by the action of desumoylating enzymes.In vertebrates, these isopeptidases include a family of six SENPs defined by a conserved cysteine protease domain,distinct subcellular locali-zations,and nonredundant functions(Mukhopadhyay and Dasso,2007).In addition,several unique desumoylating en-zymes have more recently been identified,including the metallo-protease Wss1,the PPPDE-domain-containing proteins DeSI-1 and DeSI-2,and the ubiquitin-specific protease-like protein1 (USPL1)(Mullen et al.,2010;Schulz et al.,2012;Shin et al., 2012).Sumoylation of individual proteins is likely to be regulated by afine-tuned balance between conjugation and deconjugation (Gareau and Lima,2010).Consistent with this,and as outlined below,both SUMO-conjugating and SUMO-deconjugating enzymes are important effectors of chromatin structure. Sumoylation of proteins can affect protein stability or enzy-matic activity,alter localization,or mediate novel protein-protein interactions with other proteins containing SUMO-interacting motifs(SIMs)(Figure1B)(Geiss-Friedlander and Melchior,2007; Kerscher,2007).In many instances,sumoylation may play arole Developmental Cell24,January14,2013ª2013Elsevier Inc.1in facilitating the assembly of large multiprotein complexes between proteins that are covalently modified by SUMO and/or contain SIMs,as exemplified by promyelocytic leukemia (PML)nuclear bodies.In these subnuclear structures,SUMO acts as a scaffold to mediate interactions between the PML protein and other associated factors (Matunis et al.,2006;Shen et al.,2006).Although multiple effects of sumoylation on proteins have been discovered,the ability of SUMO to promote the assembly of multiprotein complexes is an especially prominent theme.The diverse effects of sumoylation may be explained in part through the generation of functionally distinct signals.Although invertebrates express only a single SUMO,vertebrates express four paralogs (SUMO-1,SUMO-2,SUMO-3,and SUMO-4),each with the potential to act as unique signals by interacting with distinct downstream factors (Kerscher,2007).SUMO-2and SUMO-3share $97%identity with each other and probably represent redundant signals and are thus referred to as SUMO-2/3.However,they share only $50%identity with SUMO-1(Gareau and Lima,2010).SUMO-4shares $86%identity with SUMO-2/3,but questions exist about its ability to be conjugated to other proteins (Owerbach et al.,2005;Wei et al.,2008).The ability of SUMOs to form polymeric chains provides an additional opportunity for signal diversification (Figure 1B)(Kerscher,2007).Currently,the best-studied functional role for polymeric SUMO chains involves their recognition by SUMO-targeted ubiquitin E3ligases containing tandem SIMs (Perry et al.,2008).Other functional distinctions between paralogs and polymers remain to be fully understood.Finally,the diverse effects of sumoylation can also be explained through intersections with other posttranslational modification pathways (Figure 1B).For example,both phosphorylation and acetylation affect interac-tions between SUMO and downstream SUMO-binding proteins (Chang et al.,2011;Ullmann et al.,2012).General Connections among Sumoylation,Chromatin,and TranscriptionAssociations between sumoylation and chromatin structure have been well documented through numerous immunofluores-cence microscopy studies.All three SUMO paralogs,for example,are detected in the heterochromatin XY bodies of rat pachytene spermatocytes (La Salle et al.,2008;Rogers et al.,2004;Vigodner,2009;Vigodner et al.,2006),and SUMO-1is associated with long stretches of constitutive heterochromatin in human spermatocytes (Metzler-Guillemain et al.,2008).In mitotic cells,SUMO-2/3has been observed at the inner centro-mere of chromosomes and also along the length of chromosome arms as cells progress from metaphase through telophase (Ayaydin and Dasso,2004;Azuma et al.,2005;Zhang et al.,2008).Associations between SUMO and mitotic chromosomes are also detected in Saccharomyces cerevisiae (Biggins et al.,2001)and in Drosophila melanogaster using polytene chromo-some spreads (Lehembre et al.,2000),suggesting that sumoyla-tion of chromatin-associated proteins has a conserved and fundamentally important function.Associations between SUMO and chromatin are further sup-ported by biochemical studies,including chromatin immunopre-cipitation experiments (ChIP).In Schizosaccharomyces pombe ,for example,ChIP experiments revealed that the SUMO E2conjugating enzyme Ubc9is chromatin bound and specifically enriched in regions of heterochromatin (Shin et al.,2005).Simi-larly,fractionation of Xenopus laevis egg extracts demonstrated interactions between PIAS E3ligases and chromatin (Azuma et al.,2005).Surprisingly,a comprehensive genome-wide ChIP analysis to detect the precise association of SUMO or SUMO-modified proteins with chromatin has not yet been reported.However,more targeted studies link SUMO or SUMO pathway enzymes to distinct chromatin domains,including pericentric heterochromatin,PcG bodies,the nucleolus,telomeres,and centromeres,as reviewed in detail below.Studies related to the involvement of sumoylation in control-ling transcription regulation provide the strongest evidence for functional links between SUMO and chromatin.Genetic approaches have revealed a general causal relationship between sumoylation and gene repression.Inducing hypersu-moylation by targeting SUMO and/or Ubc9to specific gene promoters primarily induces gene repression (Chupreta etal.,Figure 1.The SUMO Pathway and Molecular Consequences of Sumoylation(A)SUMO is synthesized as a precursor,processed to a mature form by SUMO-specific isopeptidases and covalently conjugated to protein substrates via an E1,E2,and E3enzyme cascade.Sumoylated protein substrates are demodified by SUMO-specific isopeptidases.(B)The molecular consequences of sumoylation (S)include protein targeting,alteration of protein or enzyme function,effects on protein stability,and effects on protein-protein interactions.Sumoylation can promote or antagonize protein stability by either blocking ubiquitylation of lysine residues or by promoting ubiq-uitylation (Ub)upon recognition by SUMO-targeted ubiquitin ligases (STUbL).Effects on protein-protein interactions may be modulated at multiple levels,including polymeric chain formation and intersection with other posttranslational modifications such as phosphorylation (P).2Developmental Cell 24,January 14,2013ª2013Elsevier Inc.2005;Shiio and Eisenman,2003).Consistently,inducing hypo-sumoylation by overexpressing SUMO isopeptidases or by depleting cells of Ubc9or SUMO enhances ectopic gene expression (Ouyang et al.,2009;Poulin et al.,2005;Spektor et al.,2011).These effects are mediated at multiple levels,including direct effects on transcription factor activities (Gill,2005).Transcription factors and coregulators make up one of the most abundant classes of SUMO-modified proteins.Although clearly able to mediate transcriptional repression,sumoylation is not simply a negative regulator of transcription.The dichotomous role of SUMO in gene regulation is demon-strated by the observations that sumoylation of certain transcrip-tion factors,including Ikaros,enhances their transcriptionalactivity (Figure 2E)(Go´mez-del Arco et al.,2005).Studies in yeast also provide a striking example of the complexities of sumoylation as both an activator and repressor of transcription.ChIP analysis in S.cerevisiae reveals the pres-ence of sumoylated proteins at the promoters of constitutively active genes and the recruitment of Ubc9and SUMO to promoters of inducible genes in response to activation (Rosonina et al.,2010).Surprisingly,sumoylation is required not only for optimal transcriptional activation of constitutive genes,but also for repression and timely inactivation of inducible genes.At constitutively active genes,sumoylation enhances transcription by promoting RNA polymerase II recruitment (Figure 2F).However,at inducible promoters,sumoylation functions down-stream of transcription initiation.Specifically,sumoylation of the transcription factor Gcn4promotes its removal from pro-moters and its degradation,thereby limiting transcription reinitia-tion (Rosonina et al.,2010,2012).Another elegant example of the subtle and complex effects of sumoylation on transcription is illustrated by phenotypes in mice expressing a mutant form of the SF-1transcription factor that cannot be sumoylated.Although studies in cultured cells indi-cate that sumoylation negatively regulates SF-1transcriptional activity,mice expressing nonsumoylatable SF-1fail to pheno-copy a constitutively active SF-1(Lee et al.,2005,2011).Thus,sumoylation does not function as a simple on-off switch,but rather enhances the functional diversity of SF-1,adding a layer of regulation for fine-tuning gene expression during development.The utility of sumoylation as a mechanism to fine-tune tran-scription can be explained in part on its broad effects on chro-matin modifications and structure.This is illustrated by studies of a well-characterized SUMO-1modified transcription factor,Sp3.In cells expressing specific mutant isoforms of Sp3that cannot be sumoylated,transcription activation and chromatin modifications at Sp3-targeted promoters are dramatically different from those observed at the same promoters in cells ex-pressing wild-type Sp3.For instance,levels of both DNA and histone methylation are reduced at promoters in cells expressing mutant Sp3and,concomitantly,levels of histone methyltrans-ferases,heterochromatin protein 1(HP1),and two ATP-depen-dent chromatin remodelers are also reduced (Ross et al.,2002;Stielow et al.,2008a ,2008b ,2010).These findings provide a relatively simple view of how sumoylation of just one transcrip-tion factor exerts multiple effects—some direct and others indi-rect—to alter chromatin structure.However,even in the case of Sp3,the situation is not so simple,as evidenced through addi-tional studies demonstrating that the effects of sumoylationareFigure 2.Sumoylation Functions as an Activator and a Repressor of Gene Expression(A)Sumoylation represses gene expression by promoting DNA methylation (yellow dots)through DNMT1activation.(B)Sumoylation represses gene expression by facilitating assembly of repressive complexes on methylated DNA and at promoters.Sumoylation also inhibits the activities of transcription factors (TFs)and affects HDAC recruitment and function.(C)Sumoylation promotes the assembly of repressive PcG bodies.(D)Sumoylation promotes DNA demethylation and gene activation through mechanisms involving the SUMO-targeted ubiquitin E3ligase activity of RNF4.(E)Sumoylation facilitates the assembly of complexes on chromatin that promote transcription.(F)Sumoylation positively influences RNA polymerase II (RNA Pol II)recruitment to constitutively active gene promoters.Developmental Cell 24,January 14,2013ª2013Elsevier Inc.3unique for different Sp3isoforms and for different gene promoters(Ellis et al.,2006;Sapetschnig et al.,2004).An emerging view is that sumoylation sits at the intersection of multiple pathways,affecting the activities of not only transcrip-tion factors,but also other chromatin-associated proteins and chromatin-modifying enzymes.Thus,effects of sumoylation on gene expression and chromatin structure represent collective effects on multiple,context-dependent levels(Figure2).How sumoylation affects gene expression at the level of chromatin structure and accessibility,and within the context of distinct genomic subdomains,is the focus of the following sections. DNA MethylationDNA methylation of CpG dinucleotides restricts DNA accessi-bility by two mechanisms.Methylation blocks the binding of sequence-specific DNA binding proteins and/or recruits chro-matin-modifying complexes that promote a restrictive chromatin structure(Bird,2002).Multiple lines of evidence indicate that su-moylation plays important roles in regulating CpG methylation and demethylation,as well as the assembly and functions of downstream complexes recruited to methylated DNA.First,sumoylation of DNA methyltransferases(Dnmts)may alter their enzymatic activity(Figure2A).This has been demon-strated most clearly for the maintenance methyltransferase, Dnmt1,whose SUMO-1modification increases its activity toward S phase hemimethylated DNA substrates in vitro(Lee and Muller,2009).In addition,the de novo DNA methyltrans-ferases Dnmt3a and Dnmt3b are both sumoylated in vivo, although the functional consequences of their modifications remain to be fully elucidated(Kang et al.,2001;Li et al.,2007; Ling et al.,2004).Strikingly,nearly all of Dnmt3a is sumoylated in cells overexpressing SUMO-1,an effect that correlates with a disruption of Dnmt3a’s interactions with histone deacety-lases1and2(HDAC1and HDAC2)and a loss of Dnmt3a-mediated repression(Ling et al.,2004).Further studies are needed to determine whether these effects are strictly related to Dnmt3a sumoylation.In addition to regulating DNA methylation,sumoylation also promotes DNA demethylation through mechanisms mediated by RNF4,a ubiquitin E3ligase that specifically recognizes and ubiquitylates sumoylated proteins(Figure2D)(Hu et al.,2010; Perry et al.,2008).RNF4deficiency is embryonic lethal in mice. Rnf4À/Àmouse embryonicfibroblasts,however,are viable but exhibit hypermethylation of genomic DNA.Conversely,overex-pression of wild-type RNF4,but not SUMO-binding or ubiquitin ligase mutants,results in global DNA demethylation(Hu et al., 2010).Thus,SUMO and ubiquitylation are required for RNF4-mediated DNA demethylation,although the precise mechanisms of action remain unclear.Intriguingly,one favored model for DNA demethylation is based on deamination of methylcytosines to create T:G mismatches that are repaired by thymidine DNA glycosylase(TDG)and base-excision repair(BER)(Wu and Zhang,2010).TDG is known to interact with RNF4(Hu et al., 2010),and sumoylation has been proposed to play an important role in regulating TDG by enhancing its enzymatic turnover(Baba et al.,2005;Hardeland et al.,2002).Thus,ubiquitylation of sumoylated TDG or other interacting proteins could produce a signal required for DNA demethylation and possibly BER in general.Sumoylation also functions downstream of DNA methylation, affecting the assembly of methyl-CpG binding domain(MBD) proteins and other factors with methylated DNA(Figure2B) (Bogdanovi c and Veenstra,2009).SUMO-1and SUMO-2/3 both localize to heterochromatin domains enriched in MBD1, as well as heterochromatin proteins HP1and MCAF1(Uchimura et al.,2006).Formation of these heterochromatin domains is SUMO dependent,because knockdown of either SUMO-1or SUMO-2/3disrupts the colocalization of HP1and MCAF1with MBD1-containing foci(Uchimura et al.,2006).Intriguingly, MBD1and HP1are both sumoylated,whereas MCAF1binds all three SUMO paralogs(Lyst et al.,2006;Maison et al.,2011; Uchimura et al.,2006).Thus,it is tempting to speculate that MBD1-containing heterochromatin domains are organized around covalent and noncovalent SUMO interactions in a fashion similar to PML nuclear bodies(Matunis et al.,2006).In contrast with these repressive functions,however,sumoylation of MBD1also interferes with its interactions with the histone meth-yltransferase SETDB1,and might thereby limit gene inactivation (Lyst et al.,2006).Therefore,sumoylation underlies multiple mechanisms forfine-tuning the functional properties of methyl-ated DNA through effects both positive and negative,again demonstrating the dichotomous effects of SUMO on gene expression.Histones and HDACsPosttranslational modification of histones also represents a central mechanism for controlling chromatin structure and gene expression,and not surprisingly,histones are sumoylated. All four histones,as well as the H2A.Z variant,are sumoylated in S.cerevisiae(Kalocsay et al.,2009;Nathan et al.,2006),whereas only H4has been shown to be modified in mammalian cells(Shiio and Eisenman,2003).The functional significance of histone sumoylation is surprisingly not well understood.ChIP experi-ments involving exogenously expressed SUMO-histone fusion proteins in yeast reveal enrichment at subtelomeric regions,an area of the genome where SUMO is generally thought to antag-onize transcriptional repression(Nathan et al.,2006;Xhemalce et al.,2004;Zhao and Blobel,2005).In contrast,expression of SUMO-histone fusion proteins represses transcriptional reporters in both mammalian cells and in yeast at least in part through recruitment of HDACs and HP1(Nathan et al.,2006; Shiio and Eisenman,2003).Suchfindings suggest that histone sumoylation functions as a signal to recruit proteins to chromatin (Figure2B).Consistent with this general concept,recruitment of the transcription corepressor complex,LSD1/CoREST1/HDAC to chromatin is dependent on an SIM in CoREST1(Ouyang et al.,2009).Whether CoREST1recognizes sumoylated histones and/or other sumoylated factors,however,remains to be determined.In addition to histones,multiple studies have identified HDACs as another important effector of SUMO-mediated transcriptional repression.Most simply,HDACs themselves are sumoylated (Figure2B).Sumoylation of HDAC1and HDAC4is required for the full transcriptional repression activities at defined promoters (Cheng et al.,2004;David et al.,2002;Kirsh et al.,2002).Whether sumoylation directly affects HDAC activity or acts as a signal for the recruitment of other chromatin repressors,however,is a question that remains to be fully addressed.In addition to being4Developmental Cell24,January14,2013ª2013Elsevier Inc.directly modified,HDACs are also recruited to gene promoters in response to sumoylation of other factors,including transcription factors and cofactors such as Elk-1and p300(Garcia-Domi-nguez and Reyes,2009;Girdwood et al.,2003;Yang and Sharrocks,2004).Thesefindings suggest that HDAC recruitment may be mediated through noncovalent interactions with SUMO, a suggestion that has been confirmed at least for HDAC1,which contains a functionally important SIM(Ahn et al.,2009).A third level of association between HDACs and sumoylation has been made based on the observations that HDACs4,5,and7 appear to function as SUMO E3ligases for certain substrates (Gao et al.,2008;Yang et al.,2011;Zhao et al.,2005).These findings are based largely on effects of HDAC overexpression, where an alternative mechanism for enhanced sumoylation might involve substrate binding and protection from isopepti-dases.In either case,HDAC interaction would provide a feed-forward mechanism for enhancing sumoylation-mediated histone deacetylation and repression.Polycomb Group BodiesPolycomb group(PcG)bodies are subnuclear structures that function as small hubs of transcriptional repression.To facilitate repression,PcG bodies cluster distant DNA promoter elements and recruit chromatin-remodeling complexes called polycomb repressive complexes(Bantignies and Cavalli,2011).Given its involvement in repression and organizing large protein complexes,it is not surprising that SUMO localizes to PcG bodies(Figure2C)(Kagey et al.,2003).In addition to SUMO, Ubc9,the SUMO isopeptidase SENP2,and the SUMO E3ligase Cbx4/Pc2all localize to PcG bodies(Kagey et al.,2003,2005; Kang et al.,2010).Because Pc2stimulates the sumoylation of many repressive proteins,including Dnmt3a,CTCF,and compo-nents of the polycomb repressive complex2,it is attractive to speculate that sumoylation regulates the dynamic recruitment and assembly of these proteins within PcG bodies in a fashion similar to PML nuclear bodies(Li et al.,2007;MacPherson et al.,2009;Matunis et al.,2006;Riising et al.,2008). Consistent with essential functions in PcG body-mediated repression,two independent studies have demonstrated links between sumoylation and expression of PcG-body regulated genes.In C.elegans,depletion of SUMO,E1,or E2conjugating enzymes results in ectopic expression of Hox genes normally controlled by PcG body recruitment(Zhang et al.,2004).The appropriate repression of Hox genes is dependent at least in part on sumoylation of the PcG protein SOP-2,which is required for the association of SOP-2with PcG bodies(Zhang et al., 2004).SUMO-dependent assembly of PcG bodies is also conserved in mammalian cells and is also critical for normal gene expression during embryonic development.In particular, assembly of the polycomb repressive complex1(PRC1)at the promoters of genes important for normal heart development is misregulated in mice deficient in the SENP2isopeptidase (Kang et al.,2010).This misregulation is due in part to hypersu-moylation of the Cbx4/Pc2SUMO E3ligase and enhanced assembly of PRC1complexes on the promoters of PcG target genes.Thesefindings illustrate the important balance between SUMO-conjugating enzymes and isopeptidases,which is a common theme in ubiquitylation(Sowa et al.,2009).Further studies are required to understand how the activities of Cbx/Pc2and SENP2are normally regulated to affect proper PcG body function.Finally,in another example of the dichotomous effects of sumoylation,assembly of the PcG protein Sex Comb on Midleg (Scm)into repressor complexes in D.melanogaster appears to be negatively regulated by its SUMO modification(Smith et al., 2011).Whether sumoylation has universally opposing effects on PcG body formation in D.melanogaster compared to other organisms remains to be determined.An alternative and more appealing scenario is that sumoylation both positively and nega-tively affects PcG body assembly,with the ultimate effects on individual protein recruitment and gene expression being influ-enced by multiple,context-dependent factors and interactions. Chromatin InsulatorsSumoylation also influences gene expression by affecting the activities of chromatin insulator complexes.This function was first revealed by studies in D.melanogaster,demonstrating that loss of the PIAS E3ligase homolog results in ablation of heterochromatin-euchromatin barriers and normal polytene chromosome banding patterns(Hari et al.,2001).Consistent with a role in regulating insulator functions,SUMO was subse-quently localized to insulator bodies in D.melanogaster,and two of the major protein components,Mod(mdg4)2.2/67.2and CP190,were found to be sumoylated(Capelson and Corces, 2006;Golovnin et al.,2012).However,the function of SUMO in organizing and regulating the function of insulators is still unclear.Enhancing sumoylation by Ubc9overexpression leads to dispersal of insulator bodies,suggesting that sumoylation may negatively affect local and/or long-range interactions between insulator complexes(Capelson and Corces,2006).In contrast,SUMO depletion or expression of a Mod(Mdg4)2.2/ 67.2mutant that cannot be sumoylated inhibits insulator body formation,arguing for a positive role in insulator assembly (Golovnin et al.,2012).Such opposingfindings indicate that insu-lator assembly and/or maintenance may rely on afinely tuned balance of sumoylation and desumoylation,as required for the association or HP1a with pericentric DNA(Maison et al.,2012). Further analysis is needed to understand the function of SUMO in insulator activity in Drosophila,and particularly in other species.CTCF,a well-characterized vertebrate insulator protein, is sumoylated in human cells,but how sumoylation affects its insulating activities remains unknown(MacPherson et al.,2009). The NucleolusThe nucleolus is a specialized subnuclear domain for ribosomal RNA(rRNA)gene expression and preribosomal particle assem-bly(Boisvert et al.,2007).Studies in both vertebrates and yeast indicate that sumoylation plays important roles in the nucleolus, including regulation of rRNA processing and preribosomal particle assembly(Castle et al.,2012;Finkbeiner et al.,2011; Panse et al.,2006;Yun et al.,2008).Consistent with this, SUMO-1and SUMO-2/3are detected within the nucleolus in vertebrate cells(Ayaydin and Dasso,2004;Takahashi et al., 2008),as are the isopeptidases SENP3and SENP5(Gong and Yeh,2006).Sumoylation also appears to have important effects on nucleolar rDNA structure and function.Thus,hyposumoyla-tion due to defects in the SUMO E3ligase Mms21,a component of the Smc5/6complex,lead to abnormal nucleolar morphology Developmental Cell24,January14,2013ª2013Elsevier Inc.5。
2012非危重住院患者的高血糖管理指南
Objective:The aim was to formulate practice guidelines on the management of hyperglycemia in hospitalized patients in the non-critical care setting.Participants:The Task Force was composed of a chair,selected by the Clinical Guidelines Subcom-mittee of The Endocrine Society,six additional experts,and a methodologist.Evidence:This evidence-based guideline was developed using the Grading of Recommendations, Assessment,Development,and Evaluation(GRADE)system to describe both the strength of rec-ommendations and the quality of evidence.Consensus Process:One group meeting,several conference calls,and e-mail communications enabled consensus.Endocrine Society members,American Diabetes Association,American Heart Association,American Association of Diabetes Educators,European Society of Endocri-nology,and the Society of Hospital Medicine reviewed and commented on preliminary drafts of this guideline.Conclusions:Hyperglycemia is a common,serious,and costly health care problem in hospital-ized patients.Observational and randomized controlled studies indicate that improvement in glycemic control results in lower rates of hospital complications in general medicine and sur-gery patients.Implementing a standardized sc insulin order set promoting the use of scheduled basal and nutritional insulin therapy is a key intervention in the inpatient management of diabetes.We provide recommendations for practical,achievable,and safe glycemic targets and describe protocols,procedures,and system improvements required to facilitate the achieve-ment of glycemic goals in patients with hyperglycemia and diabetes admitted in non-critical care settings.(J Clin Endocrinol Metab97:16–38,2012)ISSN Print0021-972X ISSN Online1945-7197Printed in U.S.A.Copyright©2012by The Endocrine Societydoi:10.1210/jc.2011-2098Received July21,2011.Accepted October13,2011.Abbreviations:BG,Blood glucose;CII,continuous insulin infusion;EN,enteral nutrition; HbA1C,hemoglobin A1C;ICU,intensive care unit;MNT,medical nutrition therapy;NPH, neutral protamine Hagedorn;NPO,nil per os(nothing by mouth);PN,parenteral nutrition; POC,point of care;SSI,sliding scale insulin;TZD,thiazolidinedione. J Clin Endocrinol Metab,January2012,97(1):16–38Summary of Recommendations1.0Diagnosis and recognition of hyperglycemia and diabetes in the hospital setting1.1We recommend that clinicians assess all patients admitted to the hospital for a history of diabetes.When present,this diagnosis should be clearly identified in the medical record.(1ԽQEEE)1.2We suggest that all patients,independent of a prior diagnosis of diabetes,have laboratory blood glucose(BG) testing on admission.(2ԽQEEE)1.3We recommend that patients without a history of diabetes with BG greater than7.8mmol/liter(140mg/dl) be monitored with bedside point of care(POC)testing for at least24to48h.Those with BG greater than7.8mmol/ liter require ongoing POC testing with appropriate ther-apeutic intervention.(1ԽQEEE)1.4We recommend that in previously normoglycemic patients receiving therapies associated with hyperglyce-mia,such as corticosteroids or octreotide,enteral nutri-tion(EN)and parenteral nutrition(PN)be monitored with bedside POC testing for at least24to48h after initiation of these therapies.Those with BG measures greater than 7.8mmol/liter(140mg/dl)require ongoing POC testing with appropriate therapeutic intervention.(1ԽQEEE)1.5We recommend that all inpatients with known diabetes or with hyperglycemia(Ͼ7.8mmol/liter)be assessed with a hemoglobin A1C(HbA1C)level if this has not been performed in the preceding2–3months. (1ԽQEEE)2.0Monitoring glycemia in the non-critical care setting2.1We recommend bedside capillary POC testing as the preferred method for guiding ongoing glycemic man-agement of individual patients.(1ԽQQEE)2.2We recommend the use of BG monitoring devices that have demonstrated accuracy of use in acutely ill pa-tients.(1ԽQEEE)2.3We recommend that timing of glucose measures match the patient’s nutritional intake and medication reg-imen.(1ԽQEEE)2.4We suggest the following schedules for POC testing: before meals and at bedtime in patients who are eating,or every4–6h in patients who are NPO[receiving nothing by mouth(nil per os)]or receiving continuous enteral feed-ing.(2ԽQEEE)3.0Glycemic targets in the non-critical care setting3.1We recommend a premeal glucose target of less than 140mg/dl(7.8mmol/liter)and a random BG of less than 180mg/dl(10.0mmol/liter)for the majority of hospital-ized patients with non-critical illness.(1ԽQQEE)3.2We suggest that glycemic targets be modified ac-cording to clinical status.For patients who are able to achieve and maintain glycemic control without hypo-glycemia,a lower target range may be reasonable.For patients with terminal illness and/or with limited life expectancy or at high risk for hypoglycemia,a higher target range(BGϽ11.1mmol/liter or200mg/dl)may be reasonable.(2ԽQEEE)3.3For avoidance of hypoglycemia,we suggest that antidiabetic therapy be reassessed when BG values fall below5.6mmol/liter(100mg/dl).Modification of glu-cose-lowering treatment is usually necessary when BG val-ues are below3.9mmol/liter(70mg/dl).(2ԽQEEE)4.0Management of hyperglycemia in thenon-critical care setting4.1Medical nutrition therapy(MNT)4.1.1We recommend that MNT be included as a component of the glycemic management program for all hospitalized patients with diabetes and hyperglycemia. (1ԽQEEE)4.1.2We suggest that providing meals with a consistent amount of carbohydrate at each meal can be useful in coordinating doses of rapid-acting insulin to carbohydrate ingestion.(2ԽQEEE)4.2Transition from home to hospital4.2.1We recommend insulin therapy as the preferred method for achieving glycemic control in hospitalized pa-tients with hyperglycemia.(1ԽQQEE)4.2.2We suggest the discontinuation of oral hypogly-cemic agents and initiation of insulin therapy for the ma-jority of patients with type2diabetes at the time of hos-pital admission for an acute illness.(2ԽQEEE)4.2.3We suggest that patients treated with insulin be-fore admission have their insulin dose modified according to clinical status as a way of reducing the risk for hypo-glycemia and hyperglycemia.(2ԽQEEE)4.3Pharmacological therapy4.3.1We recommend that all patients with diabetes treated with insulin at home be treated with a scheduled sc insulin regimen in the hospital.(1ԽQQQQ)4.3.2We suggest that prolonged use of sliding scale insulin(SSI)therapy be avoided as the sole method for glycemic control in hyperglycemic patients with history of diabetes during hospitalization.(2ԽQEEE)4.3.3We recommend that scheduled sc insulin therapy consist of basal or intermediate-acting insulin given once or twice a day in combination with rapid-or short-acting insulin administered before meals in patients who are eat-ing.(1ԽQQQE)J Clin Endocrinol Metab,January2012,97(1):16–174.3.4We suggest that correction insulin be included asa component of a scheduled insulin regimen for treatment of BG values above the desired target.(2ԽQEEE)4.4Transition from hospital to home4.4.1We suggest reinstitution of preadmission insulin regimen or oral and non-insulin injectable antidiabetic drugs at discharge for patients with acceptable preadmis-sion glycemic control and without a contraindication to their continued use.(2ԽQEEE)4.4.2We suggest that initiation of insulin administra-tion be instituted at least one day before discharge to allow assessment of the efficacy and safety of this transition. (2ԽQEEE)4.4.3We recommend that patients and their family or caregivers receive both written and oral instructions re-garding their glycemic management regimen at the time of hospital discharge.These instructions need to be clearly written in a manner that is understandable to the person who will administer these medications.(1ԽQQEE)5.0Special situations5.1Transition from iv continuous insulin infusion(CII) to sc insulin therapy5.1.1We recommend that all patients with type1and type2diabetes be transitioned to scheduled sc insulin ther-apy at least1–2h before discontinuation of CII.(1ԽQQQQ)5.1.2We recommend that sc insulin be administered before discontinuation of CII for patients without a his-tory of diabetes who have hyperglycemia requiring more than2U/h.(1ԽQQQQ)5.1.3We recommend POC testing with daily adjust-ment of the insulin regimen after discontinuation of CII. (1ԽQQQE)5.2Patients receiving EN or PN5.2.1We recommend that POC testing be initiated for patients with or without a history of diabetes receiving EN and PN.(1ԽQQQQ)5.2.2We suggest that POC testing can be discontinued in patients without a prior history of diabetes if BG values are less than7.8mmol/liter(140mg/dl)without insulin therapy for24–48h after achievement of desired caloric intake.(2ԽQEEE)5.2.3We suggest that scheduled insulin therapy be ini-tiated in patients with and without known diabetes who have hyperglycemia,defined as BG greater than7.8mmol/ liter(140mg/dl),and who demonstrate a persistent re-quirement(i.e.Ͼ12to24h)for correction insulin. (2ԽQEEE)5.3Perioperative BG control5.3.1We recommend that all patients with type1di-abetes who undergo minor or major surgical procedures receive either CII or sc basal insulin with bolus insulin as required to prevent hyperglycemia during the periopera-tive period.(1ԽQQQQ)5.3.2We recommend discontinuation of oral and non-insulin injectable antidiabetic agents before surgery with initiation of insulin therapy in those who develop hyper-glycemia during the perioperative period for patients with diabetes.(1ԽQEEE)5.3.3When instituting sc insulin therapy in the post-surgical setting,we recommend that basal(for patients who are NPO)or basal bolus(for patients who are eating) insulin therapy be instituted as the preferred approach. (1ԽQQQE)5.4Glucocorticoid-induced diabetes5.4.1We recommend that bedside POC testing be ini-tiated for patients with or without a history of diabetes receiving glucocorticoid therapy.(1ԽQQQE)5.4.2We suggest that POC testing can be discontinued in nondiabetic patients if all BG results are below7.8 mmol/liter(140mg/dl)without insulin therapy for a pe-riod of at least24–48h.(2ԽQEEE)5.4.3We recommend that insulin therapy be initiated for patients with persistent hyperglycemia while receiving glucocorticoid therapy.(1ԽQQEE)5.4.4We suggest CII as an alternative to sc insulin ther-apy for patients with severe and persistent elevations in BG despite use of scheduled basal bolus sc insulin.(2ԽQEEE)6.0Recognition and management of hypoglycemia in the hospital setting6.1We recommend that glucose management proto-cols with specific directions for hypoglycemia avoidance and hypoglycemia management be implemented in the hospital.(1ԽQQEE)6.2We recommend implementation of a standardized hospital-wide,nurse-initiated hypoglycemia treatment protocol to prompt immediate therapy of any recognized hypoglycemia,defined as a BG below3.9mmol/liter(70 mg/dl).(1ԽQQEE)6.3We recommend implementation of a system for tracking frequency of hypoglycemic events with root cause analysis of events associated with potential for patient harm.(1ԽQQEE)7.0Implementation of a glycemic control program in the hospital7.1We recommend that hospitals provide administra-tive support for an interdisciplinary steering committee18Umpierrez et al.Hyperglycemia Guidelines in Hospitalized Patients J Clin Endocrinol Metab,January2012,97(1):16–38targeting a systems approach to improve care of inpatients with hyperglycemia and diabetes.(1ԽQQQE)7.2We recommend that each institution establish a uniform method of collecting and evaluating POC testing data and insulin use information as a way of monitoring the safety and efficacy of the glycemic control program. (1ԽQEEE)7.3We recommend that institutions provide accurate devices for glucose measurement at the bedside with on-going staff competency assessments.(1ԽQEEE)8.0Patient and professional education8.1We recommend diabetes self-management educa-tion targeting short-term goals that focus on survival skills:basic meal planning,medication administration, BG monitoring,and hypoglycemia and hyperglycemia de-tection,treatment,and prevention.(1ԽQEEE)8.2We recommend identifying resources in the com-munity to which patients can be referred for continuing diabetes self-management education after discharge. (1ԽQEEE)8.3We recommend ongoing staff education to update diabetes knowledge,as well as targeted staff education whenever an adverse event related to diabetes manage-ment occurs.(1ԽQEEE)Method of Development of Evidence-Based Clinical Practice GuidelinesThe Clinical Guidelines Subcommittee of The Endocrine Society deemed the management of hyperglycemia in hos-pitalized patients in a non-critical care setting a priority area in need of practice guidelines and appointed a Task Force to formulate evidence-based recommendations.The Task Force followed the approach recommended by the Grading of Recommendations,Assessment,Develop-ment,and Evaluation(GRADE)group,an international group with expertise in development and implementation of evidence-based guidelines(1).A detailed description of the grading scheme has been published elsewhere(2).The Task Force used the best available research evidence to develop some of the recommendations.The Task Force also used consistent language and graphical descriptions of both the strength of a recommendation and the quality of evidence.In terms of the strength of the recommenda-tion,strong recommendations use the phrase“we recom-mend”and the number1,and weak recommendations use the phrase“we suggest”and the number2.Cross-filled circles indicate the quality of the evidence,such that QEEE denotes very low quality evidence;QQEE,low quality;QQQE,moderate quality;and QQQQ,high qual-ity.The Task Force has confidence that persons who re-ceive care according to the strong recommendations will derive,on average,more good than harm.Weak recom-mendations require more careful consideration of the per-son’s circumstances,values,and preferences to determine the best course of action.Linked to each recommendation is a description of the evidence and the values that panelists considered in making the recommendation;in some in-stances,there are remarks,a section in which panelists offer technical suggestions for testing conditions,dosing, and monitoring.These technical comments reflect the best available evidence applied to a typical person being treated.Often this evidence comes from the unsystematic observations of the panelists and their values and prefer-ences;therefore,these remarks should be considered suggestions.The prevalence of diabetes has reached epidemic pro-portions in the United States.The Centers for Disease Con-trol and Prevention recently reported that25.8million people,or8.3%of the population,have diabetes(3).Di-abetes represents the seventh leading cause of death(4) and is the fourth leading comorbid condition among hos-pital discharges in the United States(5).Approximately one in four patients admitted to the hospital has a known diagnosis of diabetes(6,7),and about30%of patients with diabetes require two or more hospitalizations in any given year(7).The prevalence of diabetes is higher in el-derly patients and residents of long-term-care facilities,in whom diabetes is reported in up to one third of adults aged 65–75yr and in40%of those older than80yr(8,9).The association between hyperglycemia in hospitalized patients(with or without diabetes)and increased risk for complications and mortality is well established(6,10–14).This association is observed for both admission glu-cose and mean BG level during the hospital stay.Although most randomized controlled trials investigating the im-pact of treating hyperglycemia on clinical outcomes have been performed in critically ill patients,there are extensive observational data supporting the importance of hyper-glycemia management among non-critically ill patients admitted to general medicine and surgery services.In such patients,hyperglycemia is associated with prolonged hos-pital stay,increased incidence of infections,and more dis-ability after hospital discharge and death(6,15–19).This manuscript contains the consensus recommendations for the management of hyperglycemia in hospitalized patients in non-critical care settings by The Endocrine Society and other organizations of health care professionals involved in inpatient diabetes care,including the American Diabe-tes Association(ADA),American Heart Association, American Association of Diabetes Educators(AADE),Eu-ropean Society of Endocrinology,and the Society of Hos-J Clin Endocrinol Metab,January2012,97(1):16–19pital Medicine.The central goal was to provide practical, achievable,and safe glycemic goals and to describe pro-tocols,procedures,and system improvements needed to facilitate their implementation.This document is ad-dressed to health care professionals,supporting staff,hos-pital administrators,and other stakeholders focused on improved management of hyperglycemia in inpatient settings.1.0Diagnosis and recognition of hyperglycemia and diabetes in the hospital setting Recommendations1.1We recommend that clinicians assess all patients admitted to the hospital for a history of diabetes.When present,this diagnosis should be clearly identified in the medical record.(1ԽQEEE)1.2We suggest that all patients,independent of a prior diagnosis of diabetes,have laboratory BG testing on ad-mission.(2ԽQEEE)1.3We recommend that patients without a history of diabetes with BG greater than7.8mmol/liter(140mg/dl) be monitored with bedside POC testing for at least24to 48h.Those with BG greater than7.8mmol/liter require ongoing POC testing with appropriate therapeutic inter-vention.(1ԽQEEE)1.4We recommend that in previously normoglycemic patients receiving therapies associated with hyperglyce-mia,such as corticosteroids or octreotide,EN and PN be monitored with bedside POC testing for at least24to48h after initiation of these therapies.Those with BG measures greater than7.8mmol/liter(140mg/dl)require ongoing POC testing with appropriate therapeutic intervention. (1ԽQEEE)1.1–1.4EvidenceIn-hospital hyperglycemia is defined as any glucose value greater than7.8mmol/liter(140mg/dl)(20,21). Hyperglycemia occurs not only in patients with known diabetes but also in those with previously undiagnosed diabetes and others with“stress hyperglycemia”that may occur during an acute illness and that resolves by the time of discharge(20,22,23).Observational studies report that hyperglycemia is present in32to38%of patients in community hospitals(6,24),41%of critically ill patients with acute coronary syndromes(13),44%of patients with heart failure(13),and80%of patients after cardiac sur-gery(25,26).In these reports,approximately one third of non-intensive care unit(ICU)patients and approximately 80%of ICU patients had no history of diabetes before admission(6,13,27–30).The ADA Clinical Practice Recommendations endorse the initiation of glucose monitoring for both those with diabetes and those without a known history of diabetes who are receiving therapies associated with hyperglyce-mia(31).We agree with these recommendations but also suggest that initial glucose measurement on admission by the hospital laboratory is appropriate for all hospitalized patients,irrespective of the presence of preexisting diabe-tes history or exposure to obvious hyperglycemia induc-ers.The high prevalence of inpatient hyperglycemia with associated poor outcomes and the opportunity to diag-nose new diabetes warrants this approach(6,24,32,33). Because the duration of care is frequently brief in the in-patient setting,the assessment of glycemic control needs to be performed early in the hospital course.Bedside POC testing has advantages over laboratory venous glucose testing.POC testing at the“point of care”allows identi-fication of patients who require initiation or modification of a glycemic management regimen(20,21).POC moni-toring has been demonstrated to be essential in guiding insulin administration toward achieving and maintaining desired glycemic goals as well as for recognizing hypogly-cemic events(16,21,34,35).Most currently used bedside glucose meters,although designed for capillary whole-blood testing,are calibrated to report results compatible to plasma,which allows for reliable comparison to the laboratory glucose test(16,22,36,37).1.1–1.4Values and preferencesOur recommendations reflect consideration of the face validity of soliciting and communicating the diagnosis of diabetes or hyperglycemia to members of the care team. The risk-to-benefit of glucose testing and documenting a history of diabetes favors this approach despite the lack of randomized controlled trials.Recommendation1.5We recommend that all inpatients with known di-abetes or with hyperglycemia(Ͼ7.8mmol/liter)be as-sessed with an HbA1C level if this has not been performed in the preceding2–3months.(1ԽQEEE)1.5EvidenceWe support the ADA recommendation of using a lab-oratory measure of HbA1C both for the diagnosis of di-abetes and for the identification of patients at risk for diabetes(31).The ADA recommendations indicate that patients with an HbA1C of6.5%or higher can be iden-tified as having diabetes,and patients with an HbA1C between5.7and6.4%can be considered as being at risk for the development of diabetes(31).Measurement of an HbA1C during periods of hospi-talization provides the opportunity to identify patients with known diabetes who would benefit from intensifi-20Umpierrez et al.Hyperglycemia Guidelines in Hospitalized Patients J Clin Endocrinol Metab,January2012,97(1):16–38cation of their glycemic management regimen.In patients with newly recognized hyperglycemia,an HbA1C may help differentiate patients with previously undiagnosed diabetes from those with stress-induced hyperglycemia (32,38).It is important to note that there are no random-ized trials demonstrating improved outcomes using HbA1C levels to assist in the diagnosis of diabetes in in-patients with new hyperglycemia or to assist in tailoring the glycemic management of inpatients with known dia-betes.Our recommendations reflect consensus opinion and the practical utility of this strategy.Clinicians must keep in mind that an HbA1C cutoff of 6.5%identifies fewer cases of undiagnosed diabetes than does a high fasting glucose(38).Several epidemiological studies have reported a low sensitivity(44to66%)but a high specificity(76to99%)for HbA1C greater than6.5% in an outpatient population(39,40).Among hospitalized hyperglycemic patients,an HbA1C level above6.0%was reported to be100%specific and57%sensitive for the diagnosis of diabetes,whereas an HbA1C below5.2% effectively excluded a diagnosis of diabetes(41).Glucose and HbA1C values,together with the med-ical history,can be used to tailor therapy and assist in discharge planning(42,43).Discharge planning,edu-cation,and care transitions are discussed in more detail in Section4.4.Briefly,the discharge plan optimally includes the diagnosis of diabetes(if present),recommendations for short-and long-term glucose control,follow-up care,a list of educational needs,and consideration of appropriate screen-ing and treatment of diabetes comorbidities(30,42,44).There are limitations to the use of an HbA1C for diagnosis of diabetes in an inpatient population.These include the relatively low diagnostic sensitivity and potential altered values in the presence of hemoglobi-nopathies(hemoglobin C or SC disease),high-dose sa-licylates,hemodialysis,blood transfusions,and iron deficiency anemia(45).When HbA1C is used for es-tablishing a diagnosis of diabetes,analysis should be performed using a method certified by the National Gly-cohemoglobin Standardization Program(31),because POC HbA1C testing is not sufficiently accurate at this time to be diagnostic.2.0Monitoring glycemia in the non-critical care settingRecommendations2.1We recommend bedside capillary POC testing as the preferred method for guiding ongoing glycemic man-agement of individual patients.(1ԽQQEE)2.2We recommend the use of BG monitoring devices that have demonstrated accuracy of use in acutely ill pa-tients.(1ԽQEEE)2.3We recommend that timing of glucose measures match the patient’s nutritional intake and medication reg-imen.(1ԽQEEE)2.4We suggest the following schedules for POC testing: before meals and at bedtime in patients who are eating,or every4–6h in patients who are NPO or receiving con-tinuous enteral feeding.(2ԽQEEE)2.1–2.4EvidenceMatching the timing of POC testing with nutritional intake and the diabetes medication regimen in the hospital setting is consistent with recommendations for the outpa-tient setting.POC testing is usually performed four times daily:before meals and at bedtime for patients who are eating(16,21).Premeal POC testing should be obtained as close to the time of the meal tray delivery as possible and no longer than1h before meals(46–48).For patients who are NPO or receiving continuous EN,POC testing is rec-ommended every4–6h.More frequent glucose monitor-ing is indicated in patients treated with continuous iv in-sulin infusion(49,50)or after a medication change that could alter glycemic control,e.g.corticosteroid use or abrupt discontinuation of EN or PN(48,51,52),or in patients with frequent episodes of hypoglycemia(16,28).Capillary BG data facilitate the ability to adjust insulin therapy based in part on calculation of total correction insulin doses over the preceding24h.Consistent sampling sites and methods of measurement should be used because glucose results can vary significantly when alternating be-tween finger-stick and alternative sites,or between sam-ples run in the laboratory vs.a POC testing device(53).As in the outpatient setting,erroneous results can be obtained from finger-stick samples whenever the BG is rapidly ris-ing or falling(53).Quality control programs are essential to meet Food and Drug Administration(FDA)requirements and to maintain the safety,accuracy,and reliability of BG testing (21).The FDA requires that the accuracy of glucose ana-lyzers in the central lab be within10%of the real value, whereas POC meters are considered acceptable within 20%(21,37);however,recent reports have advocated improvement or tightening of POC meter accuracy stan-dards(37).Using meters with bar coding capability has been shown to reduce data entry errors in medical records (37).Capillary BG values can vary between POC meters, especially at high or low hemoglobin levels,low tissue perfusion,and with some extraneous substances(36,53). Although patients can bring their own glucose meter de-vice to the hospital,personal meters should not be used for documentation or for treatment of hyperglycemia.Hos-pital meters should follow regulatory and licensing quality control procedures to ensure accuracy and reliability ofJ Clin Endocrinol Metab,January2012,97(1):16–21results.Hospital systems with data management programs can transfer results into electronic records to allow evalua-tion of hospital-wide patterns of glycemic control(54).Health care workers should keep in mind that the ac-curacy of most hand-held glucose meters is far from op-timal(53).There are potential inaccuracies of POC testing including intrinsic issues with the technology and vari-ability between different lots of test strips,inadequate sampling site,varying hemoglobin concentrations,and other interfering hematological factors in acutely ill pa-tients(37,55,56).One study from the Centers for Dis-ease Control(CDC)of five commonly used glucose me-ters showed mean differences from a central laboratory method to be as high as32%and a coefficient of vari-ation of6to11%with a single trained medical tech-nologist(37).Recent studies suggest that continuous BG monitoring devices may be helpful in reducing incidences of severe hypoglycemia in acute care(57,58).More studies,how-ever,are needed to determine the accuracy and reliability of continuous BG monitoring devices in hospitalized pa-tients.Although promising,continuous BG monitoring has not been adequately tested in acute care and therefore cannot be recommended for hospitalized patients at this time.3.0Glycemic targets in the non-critical care setting Recommendations3.1We recommend a premeal glucose target of less than 140mg/dl(7.8mmol/liter)and a random BG of less than 180mg/dl(10.0mmol/liter)for the majority of hospital-ized patients with non-critical illness.(1ԽQQEE)3.2We suggest that glycemic targets be modified ac-cording to clinical status.For patients who are able to achieve and maintain glycemic control without hypogly-cemia,a lower target range may be reasonable.For pa-tients with terminal illness and/or with limited life expec-tancy or at high risk for hypoglycemia,a higher target range(BGϽ11.1mmol/liter or200mg/dl)may be rea-sonable.(2ԽQEEE)3.3For avoidance of hypoglycemia,we suggest that antidiabetic therapy be reassessed when BG values fall below5.6mmol/liter(100mg/dl).Modification of glu-cose-lowering treatment is usually necessary when BG val-ues are below3.9mmol/liter(70mg/dl).(2ԽQEEE)3.1–3.3EvidenceThe Task Force commissioned systematic reviews and meta-analyses of observational and randomized trials to evaluate the effect of intensive glycemic control on mor-bidity and mortality in patients hospitalized in non-critical care settings.Data were available for analysis from nine randomized controlled trials and10observational studies (59).Intensive glycemic control was associated with re-duction in the risk of infection(relative risk,0.41;95% confidence interval,0.21–0.77).There was a trend for increased risk of hypoglycemia(relative risk,1.58;95% confidence interval,0.97–2.57)that was most common in surgical studies.There was no significant effect on death, myocardial infarction,or stroke.The definition of“inten-sive control”varied across studies but was generally con-sistent with BG targets in the ADA/American Association of Clinical Endocrinologists Practice Guideline(20,21). That guideline recommended a premeal glucose of less than140mg/dl(7.8mmol/liter)and a random BG of less than10.0mmol/liter(180mg/dl)for the majority of non-critically ill patients treated with insulin(21).To avoid hypoglycemia(Ͻ3.9mmol/liter),the total basal and pran-dial insulin dose should be reduced if glucose levels are between3.9mmol/liter and5.6mmol/liter(70–100mg/ dl).In contrast,higher glucose ranges may be acceptable in terminally ill patients or in patients with severe comor-bidities,as well as in those in patient-care settings where frequent glucose monitoring or close nursing supervision is not feasible(20,21,31).In such patients,however,it is prudent to maintain a reasonable degree of glycemic con-trol(BGϽ11.1mmol/liter or200mg/dl)as a way of avoiding symptomatic hyperglycemia.4.0Management of hyperglycemia in thenon-critical care settingRecommendations4.1Medical nutrition therapy4.1.1We recommend that MNT be included as a com-ponent of the glycemic management program for all hos-pitalized patients with diabetes and hyperglycemia. (1ԽQEEE)4.1.2We suggest that providing meals with a consistent amount of carbohydrate at each meal can be useful in coordinating doses of rapid-acting insulin to carbohydrate ingestion.(2ԽQEEE)4.1.1–4.1.2EvidenceMNT is an essential component of inpatient glycemic management programs.MNT is defined as a process of nutritional assessment and individualized meal planning in consultation with a nutrition professional(31,60).The goals of inpatient MNT are to optimize glycemic control, to provide adequate calories to meet metabolic demands, and to create a discharge plan for follow-up care(16,60–64).Although the majority of non-critically ill hospital-ized patients receive nutrition support as three discrete22Umpierrez et al.Hyperglycemia Guidelines in Hospitalized Patients J Clin Endocrinol Metab,January2012,97(1):16–38。
美国应对细菌耐药国家行动计划

NAT IONA L AC T ION PL A N FOR COM BAT I NG A N T IBIOT IC-R ESISTA N TBAC TER I AM A R C H2015Table of ContentsExecutive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4Goals1 .Slow the Emergence of Resistant Bacteria and Prevent the Spread of ResistantInfections. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .112 .Strengthen National One-Health Surveillance Efforts to Combat Resistance . . . . .243 .Advance Development and Use of Rapid and Innovative Diagnostic Tests forIdentification and Characterization of Resistant Bacteria . . . . . . . . . . . . .364 .Accelerate Basic and Applied Research and Development for New Antibiotics,Other Therapeutics, and Vaccines . . . . . . . . . . . . . . . . . . . . . .405 .Improve International Collaboration and Capacities for Antibiotic-resistancePrevention, Surveillance, Control, and Antibiotic Research and Development . . . . .49 Tables1 .National Targets for Combating Antibiotic-Resistant Bacteria . . . . . . . . . . .62 .Goals and Objectives . . . . . . . . . . . . . . . . . . . . . . . . . . .93 .Antibiotic-Resistant Threats in the United States . . . . . . . . . . . . . . . .60 Appendix . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .60Executive SummaryAntibiotics have been a critical public health tool since the discovery of penicillin in 1928, saving the lives of millions of people around the world . Today, however, the emergence of drug resistance in bacteria is reversing the miracles of the past eighty years, with drug choices for the treatment of many bacterial infections becoming increasingly limited, expensive, and, in some cases, nonexistent . The Centers for Disease Control and Prevention (CDC) estimates that drug-resistant bacteria cause two million illnesses and approximately 23,000 deaths each year in the United States alone .The National Action Plan for Combating Antibiotic-resistant Bacteria provides a roadmap to guide the Nation in rising to this challenge . Developed in response to Executive Order 13676: Combating Antibiotic-Resistant Bacteria—issued by President Barack Obama on September 18, 2014—the National Action Plan outlines steps for implementing the National Strategy for Combating Antibiotic-Resistant Bacteria and addressing the policy recommendations of the President’s Council of Advisors on Science and Technology (PCAST) . Although its primary purpose is to guide activities by the U .S .Government, the National Action Plan is also designed to guide action by public health, healthcare, and veterinary partners in a common effort to address urgent and serious drug-resistant threats that affect people in the U .S .and around the world . Implementation of the National Action Plan will also support World Health Assembly resolution 67 .25 (Antimicrobial Resistance), which urges countries to take urgent action at the national, regional, and local levels to combat resistance .The goals of the National Action Plan include:1. Slow the Emergence of Resistant Bacteria and Prevent the Spread of Resistant Infections .2. Strengthen National One-Health Surveillance Efforts to Combat Resistance .3. Advance Development and Use of Rapid and Innovative Diagnostic Tests for Identification andCharacterization of Resistant Bacteria .4. Accelerate Basic and Applied Research and Development for New Antibiotics, OtherTherapeutics, and Vaccines .5. Improve International Collaboration and Capacities for Antibiotic-resistance Prevention,Surveillance, Control, and Antibiotic Research and Development .By 2020, implementation of the National Action Plan will lead to major reductions in the incidence of urgent and serious threats, including carbapenem-resistant Enterobacteriaceae (CRE), methicillin-resistant Staphylococcus aureus (MRSA), and Clostridium difficile (see Table 1) . The National Action Plan will also result in improved antibiotic stewardship in healthcare settings, prevention of the spread of drug-resistant threats, elimination of the use of medically-important antibiotics for growth promotion in food animals, and expanded surveillance for drug-resistant bacteria in humans and animals .Other significant outcomes include creation of a regional public health laboratory network, establishment of a specimen repository and sequence database that can be accessed by industrial and academic research-ers, development of new diagnostic tests through a national challenge, and development of two or moreNAT I ONAL ACT I ON P LAN FOR COMBAT I NG ANT I BI OT I C-RESISTANT BACT ERIA antibiotic drug candidates or non-traditional therapeutics for treatment of human disease . In addition, the effort to combat resistant bacteria will become an international priority for global health security . Progress towards achieving these outcomes will be monitored by the U .S .Government Task Force that developed the National Action Plan. The Task Force, which is co-chaired by the Secretaries of Defense, Agriculture, and Health and Human Services, includes representatives from the Departments of State, Justice, Veterans Affairs, and Homeland Security, as well as the Environmental Protection Agency, the United States Agency for International Development, the Office of Management and Budget, the Domestic Policy Council, the National Security Council, the Office of Science and Technology Policy, and the National Science Foundation . Additionally, the Presidential Advisory Council on Combating Antibiotic-Resistant Bacteria, created by Executive Order 13676, will provide advice, information, and recommendations to the Secretary of Health and Human Services regarding the National Action Plan’s programs and policies and their impact on the threat .Implementation of the objectives and activities in the National Action Plan requires sustained, coordi-nated, and complementary efforts of individuals and groups around the world, including healthcare providers, healthcare leaders, veterinarians, agriculture industry leaders, manufacturers, policymakers, and patients . All of us who depend on antibiotics must join in a common effort to detect, stop, and prevent the emergence and spread of resistant bacteria .IntroductionVision: The United States will work domestically and internationally to prevent, detect, and control illness and death related to infections caused by antibiotic-resistant bacteria byimplementing measures to mitigate the emergence and spread of antibiotic-resistance and ensuring the continued availability of therapeutics for the treatment of bacterial infections. Antibiotics have been a critical public health tool since the discovery of penicillin in 1928, saving the lives of millions of people around the world . Today, however, the emergence of drug resistance in bacteria is reversing the gains of the past eighty years, with many important drug choices for the treatment of bacterial infections becoming increasingly limited, expensive, and, in some cases, nonexistent . The Centers for Disease Control and Prevention (CDC) estimates that each year at least two million illnesses and 23,000 deaths are caused by drug-resistant bacteria in the United States alone .The loss of antibiotics that kill or inhibit the growth of bacteria means that we can no longer take for granted quick and reliable treatment of rare or common bacterial infections, including bacterial pneu-monias, foodborne illnesses, and healthcare-associated infections . As more strains of bacteria become resistant to an ever larger number of antibiotics, we will also lose the benefits of a range of modern medi-cal procedures—from hip replacements to organ transplants—whose safety depends on our ability to treat bacterial infections that may arise as post-surgical complications . Moreover, antibiotic-resistance also threatens animal health, agriculture, and the economy .The National Action Plan for Combating Antibiotic-resistant Bacteria provides a roadmap to guide the Nation in rising to this challenge . The National Action Plan outlines steps for implementing the National Strategy for Combating Antibiotic-Resistant Bacteria and addressing the policy recommendations of the President’s Council of Advisors on Science and Technology . Although its primary purpose is to guide activities by the U .S .Government, the National Action Plan is also designed to guide action by public health, healthcare, and veterinary partners in a common effort to address urgent and serious drug-resistant threats (Table 3) that affect people in the U .S .and around the world .Goals of the National Action PlanThe National Action Plan—informed by the guiding principles in Table 2—is organized around five goals for collaborative action by the U .S .Government, in partnership with foreign governments, individuals, and organizations aiming to strengthen healthcare, public health, veterinary medicine, agriculture, food safety, and research and manufacturing . Aggressive action will move the nation towards major reductions in the incidence of urgent and serious drug-resistant threats (Table 3), including carbapenem-resistant Enterobacteriaceae (CRE), methicillin-resistant Staphylococcus aureus (MRSA), and Clostridium difficile.•Misuse and over-use of antibiotics in healthcare and food production continue to hasten the development of bacterial drug resistance, leading to loss of efficacy of existing antibiotics .•Detecting and controlling antibiotic-resistance requires the adoption of a “One-Health” approach to disease surveillance that recognizes that resistance can arise in humans, animals, and the environment .•Implementation of evidence-based infection control practices can prevent the spread of resistant pathogens .•Interventions are necessary to accelerate private sector investment in the development of therapeutics to treat bacterial infections because current private sector interest in antibiotic development is limited .•Researchers can use innovations and new technologies—including whole genome sequencing, metagenomics, and bioinformatic approaches—to develop next-generation tools to strengthen human and animal health, including:−Point-of-need diagnostic tests to distinguish rapidly between bacterial and viral infections as well as identify bacterial drug susceptibilities;−New antibiotics and other therapies that provide much needed treatment options for those infected with resistant bacterial strains; and−Antibiotic resistance is a global health problem that requires international attention and collaboration, because bacteria do not recognize borders .1. The TB activities identified in the NAP are included as they represent critical near-term public health activities that will support progress to reduce the burden of drug-resistant TB in the U .S . Additional domestic and global activitiesto address drug-resistant TB will be provided in a companion action plan specific to TB and will be submitted to the President no later than September, 2015 . The companion action plan will build on recommendations of the Federal TB Task Force (http://www .cdc .gov/mmwr/pdf/rr/rr5803 .pdf) as well the work of the interagency USG TB working group . Those goals include:GOAL 1: Slow the Emergence of Resistant Bacteria and Prevent the Spread of Resistant Infections. Judicious use of antibiotics in healthcare and agricultural settings is essentialto slow the emergence of resistance and extend the useful lifetime of effective antibiotics .Antibiotics are a precious resource, and preserving their usefulness will require cooperationand engagement by healthcare providers, healthcare leaders, pharmaceutical companies,veterinarians, the agricultural industry, and patients . Goal 1 activities include the optimaluse of vaccines to prevent infections, implementation of healthcare policies and antibioticstewardship programs that improve patient outcomes, and efforts to minimize the develop-ment of resistance by ensuring that each patient receives the right antibiotic at the right timeat the right dose for the right duration. Prevention of resistance also requires rapid detectionand control of outbreaks and regional efforts to control transmission across community andhealthcare settings .GOAL 2: Strengthen National One-Health Surveillance Efforts to Combat Resistance. Improved detection and control of drug-resistant organisms will be achieved through an integrated,“One-Health” approach that includes the enhancement and integration of data from surveil-lance systems that monitor human pathogens—including the National Healthcare SafetyNetwork (NHSN), the Emerging Infections Program (EIP), and the National AntimicrobialResistance Monitoring System (NARMS)—with data from surveillance systems that monitoranimal pathogens—including the National Animal Health Monitoring System (NAHMS),the National Animal Health Laboratory Network (NAHLN), and the Veterinary LaboratoryInvestigation and Response Network (Vet-LIRN) . Goal 2 activities include creation of aregional public health laboratory network that provides a standardized platform for resistancetesting and advanced capacity for genetic characterization of bacteria (e .g ., through wholegenome sequencing) . Goal 2 activities will also enhance monitoring of antibiotic sales, usage,resistance, and management practices at multiple points along in the food-production chain,from farms to processing plants to supermarkets .GOAL 3: Advance Development and Use of Rapid and Innovative Diagnostic Tests for Identification and Characterization of Resistant Bacteria. Improved diagnostics fordetection of resistant bacteria and characterization of resistance patterns will help healthcareproviders make optimal treatment decisions and assist public health officials in taking actionto prevent and control disease . Improved diagnostics will also help decrease unnecessaryor inappropriate use of antibiotics . Goal 3 activities will accelerate the development of newdiagnostics and expand their availability and use to improve treatment, enhance infectioncontrol, and achieve faster response to infections and outbreaks caused by resistant bacteriain hospitals and in the community .GOAL 4: Accelerate Basic and Applied Research and Development for New Antibiotics, Other Therapeutics, and Vaccines. Despite the urgent need for new antibiotics, the number ofproducts in the drug-development pipeline is small and commercial interest remains limited .The advancement of drug development—as well as non-traditional therapeutics and vac-cines—will require intensified efforts to boost scientific research, attract private investment,and facilitate clinical trials of new drug candidates . Goal 4 activities will help accomplish theseobjectives by supporting basic and applied research, providing researchers with scientificservices (e .g ., specimens, sequence data, and regulatory guidance), and fostering public-private partnerships that strengthen the clinical trials infrastructure and reduce the risks,uncertainty, and obstacles faced by companies who are developing new antibiotics and/orother therapeutics and vaccines that can impact the use of antibiotics and the developmentof resistance .GOAL 5: Improve International Collaboration and Capacities for Antibiotic-resistance Prevention, Surveillance, Control, and Antibiotic Research and Development. Antibioticresistance is a worldwide problem that cannot be addressed by one nation in isolation . Goal5 activities include working with foreign ministries of health and agriculture, the World HealthOrganization (WHO), the Food and Agriculture Organization (FAO), the World Organizationfor Animal Health (OIE), and other multinational organizations to enhance global capacity todetect, analyze, and report antibiotic use and resistance, create incentives for the develop-ment of therapeutics and diagnostics, and strengthen global efforts to prevent and controlthe emergence and spread of antibiotic-resistance . To advance these objectives, U .S .agencieswill support development of a WHO Global Action Plan on Antimicrobial Resistance, enhanceinternational collaborations including cooperation under the European Union-United StatesTrans-Atlantic Task Force on Antimicrobial Resistance (TATFAR), and mobilize global healthresources through the Global Health Security Agenda .Development of the National Action PlanThe National Action Plan was developed in response to Executive Order 13676: Combating Antibiotic-Resistant Bacteria (Appendix 2), which was issued by President Barack Obama on September 18, 2014 in conjunction with the National Strategy for Combating Antibiotic-Resistant Bacteria.The Executive Order calls for a U .S .Government Task Force to create a five-year action plan that lays out steps and milestones for achieving the Strategy’s goals and objectives (Table 2) and addressing the PCAST recommendations . The Task Force, which is co-chaired by the Secretaries of Defense, Agriculture, and Health and Human Services, includes representatives from the Department of State, the Department of Justice, the Department of Veterans Affairs, the Department of Homeland Security, the Environmental Protection Agency, the United States Agency for International Development, the Office of Management and Budget, the Domestic Policy Council, the National Security Council staff, the Office of Science and Technology Policy, and the National Science Foundation .Development of the National Action Plan also supports World Health Assembly (WHA) resolution 67 .25 (Antimicrobial Resistance), which was endorsed in May 2014 and urges countries to develop and finance national plans and strategies and take urgent action at the national, regional, and local levels to combat resistance . The resolution urges WHA Member States to develop practical and feasible approaches to, among other actions, extend the lifespan of drugs, strengthen pharmaceutical management systems and laboratory infrastructure, develop effective surveillance systems, and encourage the development of new diagnostics, drugs, and treatment options .These recommendations are intended to inform the policy development process, and are not intended as a budget document . The commitment of resources to support these activities will be determined through the usual Executive Branch budget processes . Implementation of some of the actions in this report will require additional resources and these resources could be new or redirected from lower-priority Agency activities .Monitoring and EvaluationThe Task Force created under Executive Order 13676 is charged with providing the President with annual updates on Federal Government actions to combat antibiotic resistance, including progress made in implementing the National Action Plan, plans for addressing obstacles and challenges, and recommenda-tions for new or modified actions . The Presidential Advisory Council on Combating Antibiotic-Resistant Bacteria will provide advice, information, and recommendations to the Secretary of Health and Human Services regarding the programs and policies developed in the National Action Plan .Partnerships and ImplementationImplementation of the National Action Plan will require the sustained, coordinated, and complemen-tary efforts of individuals and groups around the world, including public and private sector partners, healthcare providers, healthcare leaders, veterinarians, agriculture industry leaders, manufacturers, policymakers, and patients . All of us who depend on antibiotics must join in a common effort to detect, stop, and prevent the emergence and spread of resistant bacteria .NAT I ONAL ACT I ON P LAN FOR COMBAT I NG ANT I BI OT I C-RESISTANT BACT ERIAGOAL 1. Slow the Emergence of Resistant Bacteria and Prevent the Spread of Resistant InfectionsJudicious use of antibiotics in healthcare and agricultural settings is essential to slow the emergence of resistance and extend the useful lifetime of effective antibiotics . Antibiotics are a precious resource, and preserving their usefulness will require cooperation and engagement by healthcare providers, healthcare leaders, pharmaceutical companies, veterinarians, the agricultural industry, and patients . Effective dissemination of information to the public is critical . Prevention of resistance also requires rapid detection and control of infections and outbreaks (see also Goal 2) and regional efforts to control transmission across community and healthcare settings .Goal 1 includes activities to foster antibiotic stewardship by improving prescribing practices across all healthcare settings, prevent the spread of drug-resistant threats in healthcare facilities and communities, and reduce and eventually eliminate the use of medically-important antibiotics for growth promotion in animals .By 2020, significant outcomes of Goal 1 will include:•Establishment of antibiotic stewardship programs in all acute care hospitals and improved antibiotic stewardship across all healthcare settings .•Reduction of inappropriate antibiotic use by 50% in outpatient settings and by 20% in inpatient settings .•Establishment of State Antibiotic Resistance (AR) Prevention (Protect) Programs in all 50 states to monitor regionally important multidrug resistant organisms and provide feedback and technical assistance to healthcare facilities .Actions taken to achieve Goal 1 will fulfill:• Executive Order 13676, Sections 5 and 7:−Improved Antibiotic Stewardship−Preventing and Responding to Infections and Outbreaks with Antibiotic-Resistant Organisms• Provisions in PCAST Recommendations #2, #6, and #7:−Effective Surveillance & Response for Antibiotic-resistance−Improving Stewardship of Existing Antibiotics in Health Care−Limit the Use of Antibiotics in Animal Agriculture•Elimination of the use of medically-important antibiotics for growth promotion in food-pro-ducing animals .•Requirement of veterinary oversight for use of medically-important antibiotics in the feed or water of food-producing animals .1.1 Implement public health programs and reporting policies that advanceantibiotic resistance prevention and foster antibiotic stewardship inhealthcare settings and the community.Perhaps the single most important action to slow the development and spread of antibiotic-resistant infections is to change the way antibiotics are used . Antibiotics are overprescribed in both human and animal settings, which makes everyone less safe . Investments in this area will be used to develop education and outreach programs to clarify and strengthen responsible, appropriate use of antibiotics in humans and animals . Efforts in this area will help greatly in slowing down the spread of resistant bacteria . This commitment to always use antibiotics appropriately and safely—to use the right antibiotic at the right time at the right dose for the right duration—is known as antibiotic stewardship.Sub-Objective 1.1.1A: Strengthen antibiotic stewardship in inpatient, outpatient, and long-term care settings by expanding existing programs, developing new ones, and monitoring progress and efficacy .The establishment and expansion of antibiotic stewardship programs will improve patient outcomes and minimize the development of resistance by ensuring judicious use of antibiotics .Milestones for provision of educational materials to enhance antibiotic stewardship in outpatient settings are provided under Sub-Objective 1 .1 .1B .MilestonesWithin one year:•The Departments of Health and Human Services (HHS), Defense (DOD), and Veterans Affairs (VA) will review existing regulations and propose new ones, as needed, requiring hospitals, ambulatory surgery centers, dialysis facilities, and other inpatient facilities to implement robust antibiotic stewardship programs that align with the CDC Core Elements. HHS, DOD, and VA will also work together to optimize standardization of stewardship programs and activities, including monitoring activities and reporting criteria .•The National Healthcare Safety Network (NHSN) will begin tracking the number of healthcare facilities with stewardship policies and programs in place .•DOD will establish a multidisciplinary group, under the purview of the Assistant Secretary of Defense for Health Affairs, to support and coordinate stewardship activities across DOD .Within three years:•All hospitals that participate in Medicare and Medicaid programs must comply with Conditions of Participation (COP) . The Centers for Medicare & Medicaid Services (CMS) will issue new COPs or revise current COP Interpretive Guidelines to advance compliance with recommendations in CDC’s Core Elements of Hospital Antibiotic Stewardship Programs. HHS, DOD, and VA will also implement policies that:−Encourage implementation of antibiotic stewardship programs as a condition for receiving Federal grants for health care delivery (e .g ., in community healthcare centers) .−Require health facilities operated by the U .S . Government to develop and implement antibiotic stewardship programs and participate in NHSN reporting (see Objective 2 .2) .•All acute care hospitals governed by the CMS COP will implement antibiotic stewardship pro-grams . CMS will expand COP requirements to apply to long-term acute care hospitals, other post-acute facilities, ambulatory surgery centers, and dialysis centers .•CMS will revise existing Interpretive Guidelines (IGs), as needed, to include antimicrobial steward-ship improvements . For example, IGs on Quality Assurance and Performance Improvement for hospitals may incorporate antibiotic-stewardship performance measures developed by the CDC, the Agency for Healthcare Research and Quality (AHRQ), or other professional organizations .•Training webinars for CMS surveyors will be updated to include information on antibiotic utilization in nursing homes, in accordance with existing IGs in the Infection Control Nursing Home regulations .•CDC, CMS, AHRQ, and other partners will issue guidance on antibiotic stewardship and best practices for ambulatory surgery centers, dialysis centers, nursing homes and other long-term care facilities, doctors’ offices and other outpatient settings, pharmacies, emergency depart-ments, and medical departments at correctional facilities .•At least 25 States, the District of Columbia, and Puerto Rico will establish or enhance antibiotic stewardship activities in inpatient healthcare delivery settings, in accordance with the CDC Core Elements . CDC will support these efforts via State AR Prevention (Protect) Programs for Healthcare (“AR Protect Programs”; see also Sub-Objective 1 .1 .2) .Within five years:•DOD will support antibiotic stewardship programs and interventions critical for maintaining quality health care throughout the Military Healthcare System (MHS) .•CDC will work with select hospital systems to expand antibiotic use reporting and steward-ship implementation, and will partner with nursing organizations to develop and implement stewardship programs and interventions in a set of nursing homes .•All states will establish or enhance antibiotic stewardship activities in healthcare delivery settings .Sub-Objective 1.1.1B: Strengthen educational programs that inform physicians, veterinari-ans, members of the agricultural industry, and the public about good antibiotic stewardship .Educational programs that promote good antibiotic stewardship in healthcare settings include:•Get Smart: Know When Antibiotics Work . Many antibiotics prescribed in doctors’ offices, clinics, and other outpatient settings are not needed . This program focuses on appropriate antibiotic prescribing and use for common illnesses in children and adults .•Get Smart for Healthcare. Many patients in hospitals, nursing homes, and other healthcare facili-ties receive antibiotics to fight infections, but these drugs are often prescribed incorrectly . This program helps clinicians prescribe the right drugs for the right patients at the right doses and times . The United States Department of Agriculture (USDA), CDC, and the Food and Drug Administration (FDA) will also continue to work with partners in the agriculture industry to advance appropriate use of antibiotics in food animals and promote collaborations among partners in medicine, veterinary medicine, and public health .Additional milestones for provision of educational materials to enhance antibiotic stewardship in agri-cultural settings are provided under Sub-Objectives 1 .2 .3 and 1 .3 .1 .MilestonesWithin one year:•CDC and VA will apply lessons learned from the CDC and VA pilot project to provide clinicians with support for making prescribing decisions based on judicious use of antibiotics and will submit a manuscript for publication describing initial research findings from this effort . Within three years:•CDC will support public health departments in establishing statewide programs for antibiotic stewardship and appropriate antibiotic use . These programs will identify healthcare facilities with high antibiotic-prescribing rates and use lessons learned from the CDC and VA pilot project (see above) and other best practices to improve antibiotic prescribing in these facilities . The success of these efforts will be assessed by measuring changes in prescribing rates and in clini-cians’ understanding of antibiotic stewardship activities and programs .•CDC will provide technical assistance to Federal facilities (e .g ., those operated by DOD, the VA, and the Indian Health Service) and other large health systems in scaling up implementation and assessment of interventions to improve outpatient antibiotic prescribing, extending effective interventions to long-term care settings, and ensuring long-term sustainability of antibiotic stewardship efforts .•DOD will initiate the planning and approval process to modify clinical decision-support interven-tions in DOD facilities in targeted regions .•CDC, CMS, and partners will propose expanded quality measures for antibiotic prescribing .。
2014 ADA指南解读(英文版)
• To test for diabetes/prediabetes, the A1C, FPG, or 2-h 75-g OGTT are appropriate B
STANDARDS OF MEDICAL CARE IN DIABETES—2014
Table of Contents
Section
ADA Evidence Grading System of Clinical Recommendations I. II. III. IV. V. VI. VII. VIII. IX. X. Classification and Diagnosis Testing for Diabetes in Asymptomatic Patients Detection and Diagnosis of Gestational Diabetes Mellitus (GDM) Prevention/Delay of Type 2 Diabetes Diabetes Care Prevention and Management of Diabetes Complications Assessment of Common Comorbid Conditions Diabetes Care in Specific Populations Diabetes Care in Specific Settings Strategies for Improving Diabetes Care
OR
Fasting plasma glucose (FPG) ≥126 mg/dL (7.0 mmol/L)
中药血清药物化学研究进展
中药血清药物化学研究进展中药血清药物化学是通过口服给药后,对血中移行成分进行鉴定分析,从而快速筛选药效物质基础及揭示复方配伍规律的有效方法。
在近20年的发展中,得到了众多学者的认可及普遍应用。
随着血清药物化学和血清药理学、药代动力学、代谢组学、网络药理学、系统生物学等学科的交叉融合,其在沟通药物体内外变化、药物之间的相互作用、药物与机体之间的相互作用等方面体现出了较强的优越性,契合了中药配伍使用、多成分、多靶点、多种作用机制的复杂性。
该文通过查阅2013—2016年CNKI Scholar 和Pubmed 2个数据库中与中药血清药物化学相关的文献,对有关的研究成果进行了统计分析,并对血清药物化学研究中供试样品制备、实验动物选择、给药方案确定、取血方式和时间、血样制备和处理、血中移行成分分析等关键技术难题及多种解决方法进行了经验性归纳,同时,展望了中药血清药物化学的拓展及综合应用,以期为该方法在中医药研究中更好的应用奠定基础。
标签:血清药物化学;血中移行成分;药效物质基础;中药复方Research progress of serum pharmacochemistry of traditional Chinese medicineMA Feixiang,XUE Peifeng*,WANG Yuanyuan,WANG Yinuo,XUE Shuyuan(College of Pharmacy,Inner Mongolia Medical University,Hohhot 010110,China)[Abstract] Serum pharmacochemistry of traditional Chinese medicine(TCM)is an effective method to rapidly screen the effective substances and reveal the compatibility law of compound by identification and analysis of constituents migrating to blood after oral administration. In the last two decades,it has been universally accepted and widely applied in the field. With the crossfusion with other disciplines,such as serum pharmacology,pharmacokinetics,metabolomics,network pharmacology and systems biology,serum pharmacochemistry shows comprehensive superiority in explaining drug changes in vivo and in vitro,interactions between drugs,interactions between drug and body,which coincides with the complexity of TCM compatibility,multicomponents,multitargets and multimechanisms. Based on the references related with the serum pharmacochemistry from CNKI scholar and Pubmed in 2013—2016,the research results of serum pharmacochemistry were statistically analyzed,and the key technical problems during the study of serum pharmacochemistry,for example,preparation of test sample,selection of experimental animal,determination of drug delivery scheme,method and time of the adoption blood,preparation and pretreatment of blood sample,as well as analysis of constituents migrating to blood,and the solving ways were empirically introduced. In addition,the development and comprehensiveapplication of serum pharmacochemistry in TCM were summarized in this paper,hoping to lay a foundation for the further application of this method in TCM research.[Key words] serum pharmacochemistry;constituents migrating to blood;effective substances;Chinese medicine compound中藥是在中医理论指导下用于预防、治疗疾病或调节人体机能的药物。
The discovery of first in class drugs origins and evolution

Since Drews and Ryser 1 published an analysis on escalating research and development (R&D) costs in the pharmaceutical industry and discussed the consequences if this increase continued, many additional studies and perspectives have been published on the trends, metrics and measures that drive R&D productivity. Several have offered possible solutions to increase R&D efficiency 2–8, but some are rather pessimistic and raise doubts about the sustainability of the current drug discovery model 9–11. In fact, the numbers are concerning. Over the past six decades the average inflationadjusted cost of bringing a new drug to market has been increasing constantly and is doubling approximately every 9 years, despite scientific discoveries and technological advances that include modern molecular biology methods, highthroughput screening, structurebased drug design, combinatorial and parallel chemistry, and the sequencing of the human genome 8. These innovations have allowed a rational, target and hypothesisdriven approach to drug discovery and were implemented with the promise of greatly enhancing the productivity of R&D. However, so far there has been little apparent impact of these advances on the number of drug approvals by the US Food and Drug Administration (FDA).An excellent recent analysis of new medicines that were approved by the FDA during the 10year period from 1999 to 2008 found that, of the first‑in‑class drugs that are small molecules, 28 were discovered through phenotypic screening , whereas 17 originated from target‑based approaches 12. Given that this was an era in which the focus and investment was heavily biased towards targetbased approaches, the apparent greater success of phenotypic screening in the discovery of innovative small‑molecule drugs raises several important questions. Has the pharmaceutical industry invested in the wrong technologies for almost three decades? Should the industry return to a ‘classical’ phenotypic approach to drug discovery, as postulated by some 13–16? What is the basis for the apparent superiority of phenotypic screening over targetbased approaches, and what are the implications for future drug discovery projects?A definition of phenotypic screeningTo try to answer these questions, we analysed the origins of the firstinclass drugs approved by the FDA between 1999 and 2013, an extension of 5 years over the previous analysis 12. We considered this extension to be important in evaluating the impact of targetbased approaches,Novartis Institutes for BioMedical Research, Fabrikstrasse 16,CH‑4002 Basel, Switzerland.Correspondence to J.E. e‑mail:joerg.eder@ doi:10.1038/nrd4336Published online 18 July 2014First‑in‑class drugsDrugs that modulate an as‑yet unprecedented drug target or biological pathway.Phenotypic screeningThe testing of a large number of — in most cases randomly selected — compounds in a systems‑based assay.T arget‑based approachesHypothesis‑based approaches that aim to manipulate a biological system by pharma‑co l og i cally modulating a specific component or target (an enzyme, receptor, and so on).The discovery of first‑in‑class drugs: origins and evolutionJörg Eder, Richard Sedrani and Christian WiesmannAbstract | Analysis of the origins of new drugs approved by the US Food and DrugAdministration (FDA) from 1999 to 2008 suggested that phenotypic screening strategies had been more productive than target-based approaches in the discovery of first-in-class small-molecule drugs. However, given the relatively recent introduction of target-based approaches in the context of the long time frames of drug development, their full impact might not yet have become apparent. Here, we present an analysis of the origins of all 113 first-in-class drugs approved by the FDA from 1999 to 2013, which shows that the majority (78) were discovered through target-based approaches (45 small-molecule drugs and 33 biologics). In addition, of 33 drugs identified in the absence of a target hypothesis, 25 were found through a chemocentric approach in which compounds with known pharmacology served as the starting point, with only eight coming from what we define here as phenotypic screening: testing a large number of compounds in a target-agnostic assay that monitors phenotypic changes. We also discuss the implications for drugdiscovery strategies, including viewing phenotypic screening as a novel discipline rather than as a neoclassical approach.ANALYSISNature Reviews Drug Discovery | AOP , published online 18 July 2014; doi:10.1038/nrd4336| Drug Discovery• Chemocentric • Chemocentric/ rational designSmall‑molecule drugsDrugs with a low molecular mass (typically <1,000 Da); this includes synthetic drugs, natural products (or derivatives) and natural substances (or derivatives).Systems‑based approachHypothesis‑agnostic assay or approach that monitors or is based on a phenotypic change in vitro or in vivo .given their relatively recent introduction in the context of the long time frames of drug discovery and development. We also realized that the conclusions that can be drawn from the data depend on a clear definition of the drug discovery approaches and on careful use of terminology. The term ‘phenotypic screening’ in particular appears to be used rather loosely and with different meanings. In the original analysis 12, and also in a subsequent paper focused on firstinclass drugs 17, phenotypic screening was considered to encompass all nontargetbased approaches to drug discovery. However, for the purpose of this analysis we define phenotypic screening more specifically as the testing of a large number of (in most cases randomly selected) compounds in asystems‑based approach using a targetagnostic assaythat monitors phenotypic changes. We believe that this is how the term is understood and used in most research laboratories today.Using this definition, it is apparent that not all systemsbased approaches to drug discovery rely on phenotypic screening. Aspirin, for example, was not discovered through phenotypic screening in this sense, but through the isolation and further derivatization of an active ingredient from a plant extract, the pharmacological activity of which was known for hundreds of years 18. In fact, before the invention of modern molecular biology (for example, in BOX 1.With the advent of gene cloning and sophisticated molecular biology techniques in the mid1980s, it was possible to work in a more hypothesisbased, rational and systematic manner on particular protein targets. Many pharmaceutical companies quickly switched to this new approach, which is typically referred to as targetbased drug discovery. Highthroughput technologies for screening large compound libraries in targetbased assays have been used to discover many new, synthetic or naturally occurring pharmacologically active compounds with low molecular mass 20. Molecular biology techniques have also enabled the development of therapeutic biologics , such as monoclonal antibodies that are specific for a particular protein target 21. For our analysis, we have therefore divided targetbased drugs into these two categories (FIG. 1a).AnalysisFirst‑in‑class drugs and their origins. Our analysis covers a time frame of 15 years (1999–2013), during which 113 firstinclass drugs were approved by the FDA (see the Drugs@FDA database). The results are shown in FIGS 2,3,4 and the data are listed in Supplementary information S1 (table). Drugs were designated as firstinclass drugs based on their modulation of an — until then — unprecedented target or biological pathway. This was considered to be independent of the mechanism of modulation; that is, if two drugs modulate the same target with the same biological consequence but bind to different sites (for example, the active site versus allostericdiscovered in a systems-based, target-agnostic manner or using a hypothesis-driven, target-based approach. Central to the discovery of systems-based drugs was either a phenotypic screen or a chemocentric approach starting from a known compound or compound class. Target-based drugs were categorized into small-molecule drugs and biologics depending on whether they were approved by the US Food and Drug Administration (FDA) under a new drug application (NDA) or biologics license application (BLA), respectively. b | The majority of first-in-class drugs were discovered through target-based approaches with slightly more small-molecule drugs than biologics. Most drugs that were discovered through systems-based approaches originated from a known compound or compound class (that is, a chemocentricapproach), and only a few were based on a phenotypic screen as defined in this article. c | There is no statistically significant trend over the 15-year period that would indicate a growing superiority of one approach over the other. However, from 2003 onwards (with two exceptions), the number of newly approved target-based first-in-class drugs exceeds that of system-based drugs, and since 1999 the level of systems-based drugs has been constantly low.Chemocentric approachesDrug discovery approaches based around a specific compound or compound class. Chemocentric approaches have made a substantial contribution both to drugs originating from systems‑based approaches and to drugs originating from target‑based approaches. Natural substance(or derivative)A chemical substance(or derivative thereof) produced by a living organism found in nature that usually has pharmacological or biological activity. For this article we arbitrarily excluded natural products from natural substances to keep the former as a separate classof compounds.BiologicsDefined here as all drugs approved under a biologics license application (BLA)by the US Food and Drug Administration (FDA); usually antibodies and other proteins. ChemotypeA family of molecules that possess the same core structure or scaffold.site of an enzyme), only the drug that was approved firsthas been categorized as firstinclass. For the purposeof our analysis, we excluded diagnostic drugs such ascontrast agents.We searched scientific publications and the patentliterature using the chemical structure of the moleculeand its mechanism of action to identify the following: theorigins of the relevant chemotype; the findings that ledto the formulation of the therapeutic hypothesis and thelink to the final indication; the methods and technologies that were used for the discovery of the drug, andthe first publication on the final drug molecule. We havedefined the starting point for drug discovery as the publication of the key finding that, at the time, enabled theinitiation of dedicated drug discovery efforts. In manycases, these key initial findings were the identificationof the target or chemotype. In our analysis, we have nottaken into account the fundamental research that ledto these key findings, which in itself often constituted aseries of important discoveries. Therefore, our definitionof the starting point arbitrarily separates the foundation ofscientific studies from drug discovery; however, in realitythey are closely linked.For example, the capacity of tumour cells to stimulate angiogenesis was discovered in 1945 (REF. 22) and thepresence of soluble tumourderived factors was demonstrated in 1968 (REF. 23). This led to the formulation of the‘antiangiogenesis’ therapeutic concept for the treatmentof tumours24. The subsequent purification of vascularendothelial growth factor (VEGF) in 1983 (REF. 25) andits cloning in 1989 (REF. 26) facilitated the discovery ofbevacizumab, the first VEGFspecific antibody27. Forour analysis, we have chosen the purification of VEGFas the starting point of drug discovery efforts. Anotherexample is the discovery of imatinib for the treatmentof chronic myelogenous leukaemia (CML)28. A chromosomal abnormality, the Philadelphia chromosome,was discovered in 1960 in white blood cells of patientswith CML29. In 1973 the Philadelphia chromosome wasshown to be a translocation between chromosomes 9 and22 (REF. 30). A series of subsequent discoveries resulted(in 1985) in the insight that the chromosomal translocation leads to the expression of the BCR–ABL fusionprotein and led to the hypothesis that its tyrosine kinaseactivity drives malignant transformation31. Imatinib wassubsequently developed as an inhibitor of the BCR–ABLkinase. Given the scope of this analysis, we selected thediscovery of the BCR–ABL fusion protein as the startingpoint for drug discovery.We also realize that what we have identified as a firstpublication might not always represent the exact startingpoint of discovery efforts towards a particular drug. Thismight pertain more to systemsbased drugs, as the firstpublication of the chemotype — which usually is also thefirst publication of such projects — may have occurredseveral years after the initiation of drug discovery activities. In addition, publication intensity was substantiallylower before the 1980s. For targetbased drugs, however,ANALYSIS| Drug DiscoveryFigure 2 | Chronology of the discovery of first‑in‑class drugs approved between 1999 and 2003. All 113 first-in-class drugs approved by the US Food and Drug Administration (FDA) between 1999 and 2013 are listed in theorder of their approval date in FIGS 2,3,4. This figure shows those approved in the 5-year period from 1999 to 2003.The colour coding for the different approaches, systems-based phenotypic screening, systems-based chemocentric, target-based small-molecule drug and target-based biologic, is defined as in FIG. 1. Other drugs are represented by grey arrows. Important points in the discovery chronology of each drug, such as the publication year of the patent covering the final drug molecule and the publication year of the final molecule, are indicated on the arrows using the symbols in the key. The first publication, usually the identification of the chemotype, target or concept, does not necessarily mark the exact starting point of discovery efforts towards a particular drug; this is symbolized by the fading at the beginning of each arrow. For details of each drug, see Supplementary information S1 (table).| Drug Discoverywe believe that many projects were initiated around the time of the publication of the target hypothesis, which we take as the typical starting point of such projects. In fact, some targetbased drug discovery projects might even have started later than that. Despite these uncertainties, we think that our analysis gives a clear picture of the various drug discovery approaches and chronology of events.Drug types and discovery approaches. According to our analysis and definitions, of the 113 firstinclass drugs, 33 (30%) were discovered through systemsbased approaches and 78 (70%) were discovered from targetbased approaches (FIG. 1b); the numbers discovered per year from each approach are shown in FIG. 1c . Two drugs were classified as ‘other’: aminolevulinicFigure 3 | Chronology of the discovery of first‑in‑class drugs approved between 2004 and 2008. The colour coding for the different approaches, systems-based phenotypic screening, systems-based chemocentric, target-basedsmall-molecule drug and target-based biologic, is defined as in FIG. 1. Important points in the discovery chronology of each drug are indicated on the arrows using the symbols in the key. For details of each drug, see Supplementary information S1 (table).ANALYSISNatural product (or derivative)Secondary metabolites (or derivatives thereof) that are extracted from tissues of plants, marine organisms or microorganism fermentation broths.PharmacophoreThe steric and electronic features of a ligand that are necessary to ensure optimal interactions with a biological target structure and to trigger (or to block) its biological response.acid (a precursor of protoporphyrin, which is used for photodynamic therapy) and lucinactant (a peptide that lowers alveolar surface tension, used for the treatment of respiratory distress syndrome).Targetbased drugs are divided into 45 (41%) smallmolecule drugs and 33 (30%) biologics. Biologics were typically found by screening (antibodies) or rational design. The starting points for targetbased smallmolecule drugs were derived as follows: 21 from various screening methods (18 from highthroughput screening, one from fragmentbased screening, one from in silico screening and one from lowthroughput screening); 18 from chemocentric approaches (for example, the starting points were analogues of known ligands for the target or related targets); and six from rational design, in most cases based on a known substrate.Of the 33 systemsbased drugs, 25 were smallmolecule drugs that were discovered through chemocentric approaches (which were considered as a type of phenotypic screening in the previous analysis)12. A further seven smallmolecule drugs were discovered by phenotypic screening according to the more specific definition we use: sirolimus, daptomycin, artemether–lumefantrine, fingolimod, eribulin, bedaquiline and trametinib. The other drug we classified as being discovered through a phenotypic screening approach was alemtuzumab, an antibody directed against CD52 that was discovered by raising antibodies against human peripheral blood mononuclear cells without knowledge of the target.Three of the smallmolecule drugs originating from phenotypic screening (sirolimus, fingolimod and eribulin) are natural product‑derived compounds that were found by analysing a discrete number of extracts for specific biological activity, with some prior knowledge on similar extracts (see Supplementary information S1 (table)). Interestingly, the original phenotypic activity of sirolimus and that of the fingolimod precursor myriocin were unrelated to their therapeutic activity, which only became apparent during followup studies. Of the eight drugs discovered through phenotypic screening, three are antiinfective, four are antiproliferative or cytotoxic molecules, and one — fingolimod — is an immunosuppressive drug.Target- versus systems-based approachesAt first glance, the results of our analysis appear to significantly deviate from the numbers previously published for firstinclass drugs, which reported that of the 75 firstinclass drugs discovered between 1999 and 2008, 28 (37%) were discovered through phenotypic screening, 17 (23%) through targetbased approaches,25 (33%) were biologics and five (7%) came from other approaches 12. This discrepancy occurs for two reasons. First, we consider biologics to be targetbased drugs, as there is little philosophical distinction in the hypothesisdriven approach to drug discovery for smallmolecule drugs versus biologics. Second, the past 5 years of our analysis time frame have seen a significant increase in the approval of firstinclass drugs, most of which were discovered in a targetbased fashion.With regard to the second reason, it is interesting to look at the time frame for drug discovery projects. For all the drugs in our data set, we calculated the apparent median time from the first publication of the therapeutic concept, target or chemotype to FDA approval, and found that it was 22 years. There was also a statistically significant difference in the median time frame for drugs that were discovered through systemsbased versus targetbased approaches: 25 and 20 years, respectively (Supplementary information S2 (box)). Therefore, taking into account the fact that the tools needed to efficiently discover drugs in a hypothesisdriven manner — including modern gene cloning and expression methods, highthroughput screening, crystallography and the sequencing of the human genome — have only become established or sufficiently advanced between 1985 and 2000, it is not surprising that the impact of these tools on targetbased drug discovery may only have begun to become apparent in more recent years 12.Interestingly, all but four systemsbased drugs have their beginnings before 1985, and one of those four drugs — ezetimibe — originated from a targetbased drug discovery project until it was noticed that the lead molecule had in vivo activity independently of, or in addition to, its targetbased activity 32. So, the finding that a considerable number of systemsbased drugs have been approved over the past 10 years is likely to be due in part to the length of time these projects took.The data also suggest that targetbased drug discovery might have helped reduce the median time for drug discovery and development. Closer examination of the differences in median times between systemsbased approaches and targetbased approaches revealed that the 5year median difference in overall approval time is largely due to statistically significant differences in the period from patent publication to FDA approval, where targetbased approaches (taking 8 years) took only half the time as systemsbased approaches (taking 16 years) (Supplementary information S2 (box)).The pharmaceutical industry has often been criticized for not being sufficiently innovative. We think that our analysis indicates otherwise and perhaps even suggests that the best is yet to come as, owing to the length of time between project initiation and launch, new technologies such as highthroughput screening and the sequencing of the human genome may only be starting to have a major impact on drug approvals. Targetbased drug discovery, together with modern screening technologies, has also greatly broadened the scope of pharmacophores available for medicinal chemistry 20, and increased the number of ‘tool compounds’ to use for investigating biological systems, potentially leading to new therapeuticFigure 4 | Chronology of the discovery of first‑in‑class drugs approved between 2009 and 2013. The colour coding for the different approaches, systems-based phenotypic screening, systems-based chemocentric, target-based small-molecule drug and target-based biologic, is defined as in FIG. 1. Other drugs are represented by grey arrows. Important points in the discovery chronology of each drug are indicated on the arrows using the symbols in the key. For details of each drug, see Supplementary information S1 (table).▶ANALYSIS| Drug DiscoverybTotalLow‑molecular‑mass synthetic drugLow‑molecular‑mass drugs that are not derived from natural products or natural substances.targets and/or chemical starting points for new drugs. One question that may be asked, although a rather academic one, is what course the industry would have taken in the absence of these innovations: that is, at what point in time would the industry have run out of chemotypes as starting points for the classical chemocentric approach?Molecules and target families Of the 113 firstinclass drugs, 34 (30%) are biologics, 14 (13%) are natural products or compounds derived thereof, 17 (15%) are natural substancederived molecules (including peptides, but arbitrarily excluding natural products to keep this class of compounds separate for the analysis) and 47 (42%) are other smallmolecule drugs, mainly low‑molecular‑mass synthetic compounds (FIG. 5a). Although natural substances appear to be the basis for a similar proportion of the drugs discovered by target and systemsbased approaches (17% and 12% respectively), natural products were the basis for a much more substantial proportion of systemsbased approaches. Of the 33 systemsbased drugs, 12 (35%) are derived from natural products, whereas only two (3%)of the 78 targetbased drugs are derived from natural products: orlistat, which is based on the lipase inhibitor lipstatin; and canagliflozin, which is based on phlorizin. Of the 14 natural productderived firstinclass drugs approved between 1999 and 2013, five were discovered by screening approaches (four by systemsbased phenotypic screening and one by targetbased highthroughputFigure 5 | Distribution of first‑in‑class drugs according to the molecule type and target family. a | The distribution according to molecule type (that is, the source of the drug molecule) differs between systems- and target-basedapproaches. There is a strong bias for the use of natural products for systems-based approaches over target-basedapproaches, whereas biologics have only had a major impact in the target-based space. Note that artemether–lumefantrine was counted twice as it contains two drugs. b | The distribution of drugs across target families. G protein-coupled receptors (GPCRs), kinases, proteases and ion channels constitute the major target families. Kinase and protease inhibitors are prominent in the list of target-based drugs, but under-represented or absent from that of systems-based drugs. By contrast, the fraction of drugs targeting ion channels is significantly higher among systems-based drugs. Note that memantine was counted twice as it modulates GPCRs as well as ion channels. NHR, nuclear hormone receptor.screening) and nine were discovered by chemocentric approaches. The latter includes four drugs that were found by ethnobotanical approaches through the isolation and identification of the active ingredients of plant extracts that are used in Chinese and other traditional medicines. Natural products, therefore, have been an important source of chemotypes for systemsbased drug discovery approaches and are likely to have an important role in future phenotypic screening as well as in chemocentric approaches.The distribution of firstinclass drugs across target families is similar to that previously published for all drugs33, with G proteincoupled receptors (GPCRs), kinases, proteases and ion channels being the major target families in addition to the ‘other enzymes’ category, which contains a number of smaller target families and singletons (FIG. 5b). Probably based on the lack of suitable chemotypes before the 1980s, kinase and protease inhibitors are underrepresented or absent from the list of systemsbased drugs, and were predominantly discovered by targetbased approaches. By contrast, drugs that target ion channels are overrepresented in this list, perhaps reflecting some of the difficulty and complexity in discovering such inhibitors in a targetbased, rational manner.Interestingly, for nine (26%) of the 33 systemsbased drugs, the mechanism of action is unclear or even unknown, which highlights that knowledge of the mechanism of action might be helpful but is not mandatory to successfully develop a drug. However, elucidating the mechanism of action of molecules identified through systemsbased approaches by using forward chemical genetics, chemoproteomics or other chemical biology methods could access a large untapped potential for the discovery of novel mechanisms and therapeutic principles34–37. In this way, systems and targetbased approaches are often interlinked, and what started as a systemsbased drug discovery effort might uncover important tool compounds for further targetbased approaches. The discovery of the mammalian target of rapamycin (mTOR) pathway, for example, was greatly facilitated by studies with sirolimus38, and there are numerous other examples. Phenotypic screening as a new disciplineIn the course of almost three decades of targetbased drug discovery, a number of evolutionary steps have been taken to improve its efficiency, and some initial problems have been addressed. In particular, there was a widespread trend in the field during the late 1990s and early 2000s to industrialize drug discovery using highthroughput methodologies in biology and chemistry. Consequently, this approach to candidate drug discovery was established as a linear sequence of separate steps — target identification, tool production and assay development, hit finding and validation, hittolead progression, lead optimization and preclinical development — each of which was the focus of optimization efforts with the goal of increasing the throughput and/or efficiency of each step. The assumption was that brute force and everlarger numbers of projects and highthroughput experiments would increase productivity.Today, the pharmaceutical industry has largely taken a step back from this ‘brute force’ approach, realizing that this seemed to instead hamper creativity, innovation and, ultimately, productivity39. Despite all the improvements over the past decades towards more effective drug discovery, the productivity challenge remains substantial, particularly with regard to the discovery of firstinclass drugs. In this context, phenotypic screening could be an important contribution as it offers the potential to provide important pharmacological tools to study new biology34–37 at a faster pace than classical chemocentric systemsbased approaches. We would like to emphasize that, in our view, the distinction between phenotypic screening and chemocentric drug discovery is not just a semantic one; rather, phenotypic screening as we define it here is a new discipline. A plea for more phenotypic screening in drug discovery, as has been made frequently during recent years and is being implemented in many groups40–44, should not be taken as a call to revert to the classical, chemocentric approach to drug discovery.Phenotypic screening holds the promise to uncover new therapeutic principles and molecular pathways of currently untreatable diseases45. Indeed, a number of highly encouraging recent examples of potential drugs derived from phenotypic screening46–51, such as bromodomain inhibitors50 and hepatitis C virus NS5A inhibitors51, are now in latestage clinical trials. However, so far only a few of the approved drugs were discovered through phenotypic screening, the majority of them either being antiinfective or antiproliferative compounds (see above).Reporter gene assays are a specific category of phenotypic screens, although they are somewhat artificial and have limitations52,53. Many reporter gene assays have been run in pharmaceutical companies and academic institutions over the past 20 years, with a peak in the mid to late 1990s, apparently with little success in terms of delivering drug candidates. We did not find any example of a firstinclass drug originating from such a screen, but noticed several examples of targetbased drugs that could have been identified in such assays.One of the fundamental challenges of phenotypic screening is the selection of a few interesting compounds from a large list of active substances, which typically contains thousands of compounds and is often heavily dominated by unselective or toxic compounds, substances with unwanted mechanisms of action or false positives. Usually, potency is the sole criterion by which such hit lists are sorted and compounds selected for further studies, but this criterion might be inappropriate for identifying the best chemotypes. It is important to understand that we will require new methodologies and approaches to increase the success rate of phenotypic screens. For example, many diseases today are still difficult to faithfully mirror in test plates and model organisms, and the use of stem cell technology or wholeorganism screens might enable the establishment of more physiological assay systems that better reflect the actual disease. Progress here will certainly increase the likelihood of finding diseaserelevant pathways, but it may not enableANALYSIS。
海洋放线菌

Contents 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Actinomycetes in the marine environment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Role of actinomycetes in marine environment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Rare actinomycetes and selective isolation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Molecular approaches to search for indigenous marine actinomycetes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Different genera of marine actinomycetes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Marine streptomycetes – a boundary microorganism . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Fermentation process for metabolites production . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Secondary metabolites from actinomycetes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Novel/new metabolites from marine actinomycetes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Acknowledgement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 00 00 00 00 00 00 00 00 00 00 00 00
药物筛选 英语
药物筛选英语Drug ScreeningDrug screening is a process used to identify potential drug candidates for further development. It involves testing a large number of chemical compounds to determine their efficacy and safety for use as a medication.There are several steps involved in drug screening:1. Target identification: The first step is to identify the target molecule or pathway that the drug will interact with. This could be a specific protein, enzyme, receptor, or other molecule involved ina disease process.2. Compound libraries: A library of small molecule compounds is created, which can be sourced from various chemical suppliers or synthesized in-house. These compounds will be tested to see if they have any activity against the target.3. High-throughput screening (HTS): This is a method where thousands or even millions of compounds are tested against the target in a short amount of time. It involves automated robotic systems that can quickly analyze the activity of each compound.4. Hit identification: From the HTS results, compounds that show activity against the target are identified as "hits." These hits are further tested to confirm their activity and to ensure they are not toxic.5. Lead optimization: The identified hits are then modified and optimized to enhance their potency, selectivity, and pharmacokinetic properties. This involves chemical modifications, structural modifications, and other modifications to improve the drug-likeness of the compound.6. Preclinical testing: The optimized compounds are then tested in various preclinical models, including cell-based assays and animal studies, to assess their efficacy, safety, and toxicity.7. Clinical trials: If the compound passes preclinical testing, it can proceed to clinical trials. These are conducted in humans to evaluate the safety and efficacy of the drug and determine appropriate dosage.8. Regulatory approval: If the drug demonstrates significant therapeutic benefits and an acceptable safety profile, it may be submitted for regulatory approval. Regulatory agencies, such as the FDA in the United States, review the data from clinical trials and decide whether to approve the drug for marketing.9. Post-marketing surveillance: Once a drug is approved and on the market, ongoing monitoring and surveillance are conducted to ensure its safety and effectiveness in real-world use.Drug screening is a crucial step in the drug development process, as it helps to identify potential drug candidates and guide further development. The process integrates various scientific disciplines, including chemistry, biology, pharmacology, and toxicology, to identify safe and effective medications.。
TREATTOTARGET(T2T)INRHEUMATOID:治疗目标(..

WHAT IS TREAT TO TARGET?
The treat to target (T2T) approach involves defining a treatment goal or “target” and
modifying the therapy if the target is not reached.
For more information, to order copies of this and other brochures, or to become a Member, visit our website:
捕食螨天敌昆虫产品开发策略
捕食螨天敌昆虫产品开发策略英文回答:Developing a strategy for the production of predatory mite insect products requires careful planning and consideration. Here are some steps that can be taken to develop an effective strategy:1. Market Research: The first step is to conduct thorough market research to identify the demand for predatory mite insect products. This involves analyzing the target market, understanding customer needs and preferences, and identifying potential competitors. For example, I can conduct surveys or interviews with potential customers to gather insights into their requirements.2. Product Development: Once the market research is complete, it is important to focus on product development. This involves identifying the specific species of predatory mites that are most effective in controlling pests, anddeveloping a product line that includes these species. For instance, I can collaborate with entomologists and researchers to identify the most efficient predatory mite species for different types of pests.3. Production and Quality Control: After identifying the species of predatory mites, the next step is to establish a production process. This involves setting up breeding facilities, ensuring optimal conditions for mite reproduction, and implementing quality control measures to ensure the production of healthy and effective mites. For example, I can establish a breeding facility withcontrolled temperature and humidity to ensure the optimal growth of predatory mites.4. Packaging and Marketing: Packaging plays a crucial role in attracting customers and conveying the effectiveness of the product. It is important to design attractive and informative packaging that highlights the benefits of using predatory mite insect products. Additionally, effective marketing strategies, such as online advertising, trade shows, and partnerships with pestcontrol companies, can help reach a wider audience. For instance, I can collaborate with graphic designers to create visually appealing packaging that clearly communicates the advantages of using predatory mite insect products.5. Distribution and Sales: Developing a distribution network is essential to ensure that the products reach the target market effectively. This involves identifying potential distributors, establishing partnerships, and implementing efficient logistics systems. For example, I can partner with agricultural supply stores, online marketplaces, and pest control professionals to ensure widespread availability of the products.中文回答:制定捕食螨天敌昆虫产品的开发策略需要认真的规划和考虑。
Tollip在左前降支结扎的心肌梗死小鼠模型心肌细胞凋亡中的作用及其机制
Tollip 在左前降支结扎的心肌梗死小鼠模型心肌细胞凋亡中的 作用及其机制
周姝1 卜法芹1 常巧玉2 陈红伟3 赵舒才1 李娜4 韩红强1 王岩1 (1 新乡市中心医院心内二科ꎬ河南 新乡 453000ꎻ2 河南医学组织再生重点实验室ꎻ新乡市中心医院 3 CCUꎻ4 彩超室)
9 Marano FꎬHussain SꎬRodrigues ̄Lima Fꎬet al. Nanoparticles:molecu ̄ lar targets and cell signalling 〔 J 〕 . Arch Toxicolꎬ 2011ꎻ 85 ( 7 ) : 733 ̄41. 〔2018 ̄09 ̄17 修回〕
Tollip 是 一 种 内 源 性 的 Toll 样 受 体 家 族 抑 制 剂ꎬ表达于心脏且在心脏发育调控中具有重要作用ꎮ Tollip 可抑制压力负荷诱导的心肌肥厚ꎬ表明 Tollip 可能与心脏疾病的发生发展有关ꎬ但针对 Tollip 在 急性心肌梗死( AMI) 中的作用研究目前国内外暂无 报道〔1ꎬ2〕 ꎮ 为探索 Tollip 在 AMI 中的作用及其相关 机制ꎬ本文利用转基因小鼠建立 AMI 动物模型ꎬ并 通过分析心脏相关的结构和功能方面的参数来解释 Tollip 基因对 AMI 进程的影响ꎮ
〔 摘 要〕 目的 研究 Tollip 在左前降支结扎的心肌梗死( AMI) 小鼠模型的作用及可能机制ꎮ 方法 将实验动物分 4 组ꎬNTG 对照( NTG ̄Sham) 组、NTG AMI( NTG ̄MI) 组、TG 对照( TG ̄Sham) 组、TG AMI( TG ̄MI) 组ꎮ AMI 组永久性结扎左冠状动 脉前降支ꎬSham 组分离出左前降支但只做挂线不结扎ꎮ 术后 4 w 先后采用超声( Echo) 和右颈总动脉内插管检测血流动力学 (PV) 的方法评价小鼠的心脏功能ꎮ 小鼠心脏样本中ꎬ病理取材用于石蜡包埋切片ꎬ苏木素 ̄伊红( HE) 染色评价 AMI 面积ꎬ免 疫荧光( IF) 染色观察炎症反应ꎬ分生样本则用于分子生物学、凋亡和信号通路相关蛋白检测ꎮ 结果 与 NTG ̄MI 组比较ꎬTG ̄ MI 组心 脏 梗 死 面 积 显 著 扩 大ꎬ 心 功 能 紊 乱 更 严 重ꎮ 与 NTG ̄MI 组 比 较ꎬ TG ̄MI 组 Mac ̄1、 LY6G、 CD3 阳 性 率 显 著 增 加 ( P<0������ 05) ꎮ与 NTG ̄MI 组比较ꎬTG ̄MI 组抗凋亡 Bcl ̄2、含半胱氨酸的天冬氨酸蛋白水解酶( Caspase)3 蛋白水平显著降低ꎬ促凋 亡基因 Bax、活化的( Cleaved) Cacpase3 蛋白水平显著升高( P<0������ 05) ꎮ 与 NTG ̄MI 组比较ꎬTG ̄MI 组丝裂原活化蛋白激酶激酶 ( MEK)1 / 2ꎬ丝裂原活化蛋白激酶( ERK)1 / 2ꎬc ̄Jun 氨基末端激酶( JNK)1 / 2 和 P38 的磷酸化水平与总水平差异无统计学意义 ( P>0������ 05) ꎻ与 NTG ̄MI 组比较ꎬTG ̄MI 组 Akt、mTOR、GSK3β、S6 和叉头框蛋白( FOX) O1 的磷酸化水平明显降低( P<0������ 05) ꎮ 结论 Tollip 可通过抑制 Akt 信号通路促进炎性细胞浸润、加重危险区或缺血区的心肌细胞凋亡ꎬ导致 AMI 面积扩大、心脏功 能紊乱加重ꎮ
SURROGATES FOR TARGETS AND IMPROVED REFERENCE PANE

专利名称:SURROGATES FOR TARGETS ANDIMPROVED REFERENCE PANELS发明人:KAUVAR, Lawrence, M.,VILLAR, Hugo, O.申请号:EP95906754.7申请日:19950105公开号:EP0738390B1公开日:20030402专利内容由知识产权出版社提供摘要:A method to determine reactivity of a candidate compound with a target which method does not require the physical presence of the target is disclosed. By providing a formula for treating data obtained from a reference set of target substitutes which formula is predictive of reactivity with the target, the compound to be tested can be physically assessed with respect to the reference panels, the formula applied, and reactivity with the actual target may be predicted. Panels which consist of individual members, said members comprising proteins, wherein at least one of the members of the panel is a protein other than an immunoglobulin (Ig) or fragment thereof and wherein the presence of said non-Ig protein enriches the panel are described. These panels can be tested for reactivity with an analyte to create a profile. Such profiles can be used in pattern matching, analysis of samples and other analyses.申请人:TELIK INC地址:US国籍:US代理机构:Goldin, Douglas Michael更多信息请下载全文后查看。
硅微粉改性工艺流程

硅微粉改性工艺流程英文回答:Silicon micro powder modification process can be divided into several steps: pretreatment, surface modification, and post-treatment.In the pretreatment stage, the raw silicon micro powder needs to be cleaned and dried to remove impurities and moisture. This can be done through processes such as washing, filtering, and drying.After pretreatment, the surface modification process begins. This involves treating the silicon micro powder with various modifiers to improve its properties. The choice of modifier depends on the desired outcome. For example, if we want to enhance the dispersibility of the silicon micro powder, we can use a surfactant as the modifier. The silicon micro powder is mixed with the surfactant and then subjected to a high-speed shearingprocess to ensure uniform distribution of the surfactant on the surface of the particles.In addition to surfactants, other modifiers such as coupling agents, silane agents, or polymers can be used to modify the surface of the silicon micro powder. These modifiers can improve the compatibility of the silicon micro powder with different matrices, enhance its adhesion properties, or increase its thermal stability.Once the surface modification process is complete,post-treatment is carried out to further improve the performance of the modified silicon micro powder. This can involve processes such as drying, sieving, and packaging.Overall, the silicon micro powder modification process requires careful consideration of the desired properties and the choice of appropriate modifiers. It is important to optimize each step of the process to ensure the desired outcome is achieved.中文回答:硅微粉的改性工艺流程可以分为几个步骤,预处理、表面改性和后处理。
Photoelectrochemical DNA Biosensors
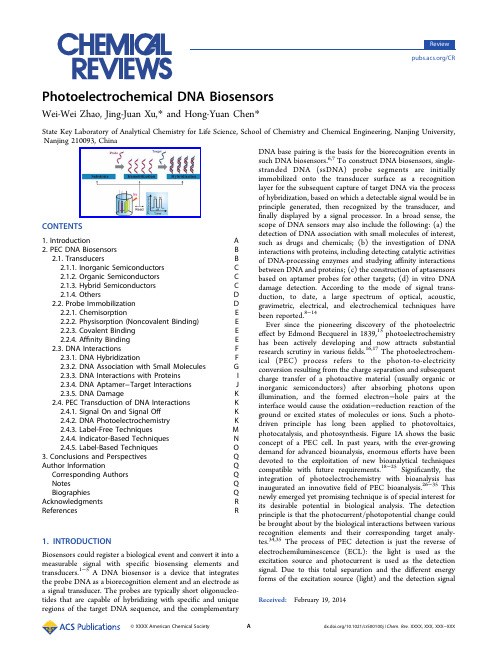
A
/10.1021/cr500100j | Chem. Rev. XXXX, XXX, XXX−XXX
Chemical Reviews
Review
articles about the DNA biosensors that are based on different techniques such as electrochemical method have been published,8,9 whereas to date there have been no efforts addressing specifically the survey of this dynamically developing area of PEC DNA biosensors. Given the pace of advances in this area, the PEC routes for monitoring the DNA biorecognition events are the subject of the present review. In more detail, for the first time, this review surveys the methodology related to the PEC DNA biosensor construction, the interactions to be addressed, and the inventive detection principles. The recent progress, current directions, and future prospects in this area are also evaluated and discussed, with the aim to provide an accessible introduction to PEC DNA biosensors for any scientistchemical DNA Biosensors
联合降压药物治疗英文版

ASH Position ArticleCombination therapy in hypertensionAlan H.Gradman,MD a,*,Jan N.Basile,MD b,Barry L.Carter,PharmD c,andGeorge L.Bakris,MD d,on behalf of the American Society of Hypertension Writing Groupa The Western Pennsylvania Hospital,Pittsburgh,Pennsylvania and Temple University School of Medicine,Philadelphia,PA,USA;b Ralph H.Johnson VA Medical Center,Medical University of South Carolina,Charleston,SC,USA;c Roy J.and Lucille A.Carver College of Medicine,University of Iowa,Iowa City,IA,USA;andd The University of Chicago Pritzker School of Medicine,Chicago,IL,USAManuscript received February5,2010and accepted February5,2010AbstractThe goal of antihypertensive therapy is to abolish the risks associated with blood pressure(BP)elevation without adversely affecting quality of life.Drug selection is based on efficacy in lowering BP and in reducing cardiovascular(CV)end points including stroke,myocardial infarction,and heart failure.Although the choice of initial drug therapy exerts some effect on long-term outcomes,it is evident that BP reduction per se is the primary determinant of CV risk reduction.Available data suggest that at least75%of patients will require combination therapy to achieve contemporary BP targets,and increasing emphasis is being placed on the practical tasks involved in consistently achieving and maintaining goal BP in clinical practice.It is within this context that the American Society of Hypertension presents this Position Paper on Combination Therapy for Hypertension.It will address the scientific basis of combination therapy,present the pharmacologic rationale for choosing specific drug combinations, and review patient selection criteria for initial and secondary use.The advantages and disadvantages of single pill(fixed)drug combinations,and the implications of recent clinical trials involving specific combination strategies will also be discussed.J Am Soc Hypertens2010;4(1):42–50.Ó2010American Society of Hypertension.All rights reserved.Keywords:Hypertension;combination therapy;drug therapy;angiotensin converting enzyme inhibitor;angiotensin receptor blocker;beta blockers diuretic; calcium channel blocker.IntroductionThe goal of antihypertensive therapy is to abolish the risks associated with blood pressure(BP)elevation without adversely affecting quality of life.Epidemiologic studies and clinical trials have been used to define individual risk and set appropriate BP targets,1–3recognizing that these targets reflect expert consensus based on available data and are subject to revision as additional evidence is obtained.4 Drug selection is based on efficacy in lowering BP and in reducing cardiovascular(CV)end points including stroke, myocardial infarction,and heart failure.Although the choice of initial drug therapy exerts some effect on long-term outcomes,it is evident that BP reduction per se is the primary determinant of CV risk reduction.As a result,there has been a progressive lowering of BP targets in large segments of the hypertensive population,including diabetics and patients with established renal or vascular disease.1–3,5At the same time,increasing emphasis is being placed on the practical tasks involved in consistently achieving and maintaining goal BP in clinical practice.It is within this context that the American Society of Hypertension presents this Position Paper on Combination Therapy for Hypertension.It will address the scientific basis of combination therapy,present the pharmacologic rationale for choosing specific drug combinations,and review patient selection criteria for initial and secondary use.The advantages and disadvantages of single pill(fixed) drug combinations(SPC)and the implications of recent clinical trials involving specific combination strategies will also be discussed.Combination Therapy:A Practical NecessityThe ability to maintain constant or near-constant BP in response to various stressors is central to homeostasis,and*Corresponding author:Dr.Alan H.Gradman,The WesternPennsylvania Hospital,Department of Medicine,4800FriendshipAvenue,Pittsburgh,PA15224.Tel:412-721-4915.E-mail:gradmanmd@1933-1711/10/$–see front matterÓ2010American Society of Hypertension.All rights reserved. doi:10.1016/j.jash.2010.02.005Journal of the American Society of Hypertension4(1)(2010)42–50the human organism has redundant physiologic mechanisms for regulating arterial pressure.BP is determined primarily by three factors:renal sodium excretion and resultant plasma and total body volume,cardiac performance,and vascular tone.6These factors control intravascular volume,cardiac output,and systemic vascular resistance,which are the imme-diate hemodynamic determinants of BP.Both the sympathetic nervous system and the renin-angiotensin-aldosterone system (RAAS)are intimately involved in adjusting these parameters on a real-time basis.In addition,genetic makeup,diet,and environmental factors influence BP in individual patients. Although it is occasionally possible to identify a specific cause for hypertension in some patients,BP elevation is usually multifactorial,making it very difficult,if not impos-sible,to normalize pressure by interfering with only a single pressor mechanism.In addition,drug therapy directed at any one component routinely evokes compensatory(counterre-gulatory)responses that reduce the magnitude of response, even if it was accurately directed at the predominant patho-physiologic mechanism.As a consequence,limited BP reduction is seen with all available antihypertensive agents. In a recent meta-analysis by Law et al of354randomized, double-blind trials,the mean placebo-corrected reduction in BP with monotherapy was only9.1/5.5mm Hg.7There was little difference in this regard between a diuretic, b-blocker,angiotensin-converting enzyme(ACE)inhibitor, angiotensin receptor blocker(ARB),or calcium channel blocker(CCB).Similar results were found in the Treatment of Mild Hypertension study,in which comparable BP reduc-tion was observed after long-term treatment with a diuretic, b-blocker,CCB,a-blocker,and ACE inhibitor.8Clinical trials document that achieving BP targets is usually not possible with a single agent.In the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial, only26%of patients achieved goal BP with monotherapy—despite the fact that the target BP for diabetics(36%of the patient population)was<140/90mm Hg rather than the <130/80mm Hg mandated by current guidelines.9In the Hypertension Optimal Treatment trial,33%of patients achieved their(diastolic only)BP target with monotherapy, 45%required two drugs,and22%needed three or more agents.10Systolic BP at the end of the study averaged141 mm Hg,indicating that even a higher percentage would have required combination therapy according to current treatment standards.In the Losartan Intervention for Endpoints trial,in which treatment to goal(<140/90mm Hg)was aggressively pursued in patients with left ventricular hypertrophy and a mean baseline BP of175/98mm Hg,more than90%required at least two antihypertensive agents.11The importance of blocking multiple physiologic path-ways is underscored by studies using a treatment strategy known as‘‘sequential monotherapy.’’This approach is based on the observation that BP response to different antihyperten-sive medications is often quite variable,and BP control should be more readily achieved with monotherapy if patients are exposed to multiple drugs and then treated with the most effective agent.12In the Strategies in Treatment of Hypertension study,treatment initiated with a low-dose combination was compared with a monotherapy arm in which patients werefirst treated with a b-blocker but could be switched to an ACE inhibitor or a CCB if BP remained >140/90mm Hg.At the end of9months,a significantly higher percentage of patients randomized to the low-dose combination achieved target BP compared with those receiving sequential monotherapy(62%vs.49%,P¼.02).13 The aggregate of available data suggests that at least75% of patients will require combination therapy to achieve contemporary BP targets.This estimate reflects the results of previous studies,the lower BP targets now in place for large segments of the hypertensive population,and the rapidly increasing prevalence of obesity.The latter is impor-tant as the presence of obesity further elevates pretreatment BP and increases the magnitude of BP reduction needed to achieve therapeutic targets.14The importance of achieving goal BP in individual patients cannot be overemphasized.In major clinical trials,small differences in on-treatment BP frequently translate into major differences in clinical event rates.Recent data also suggest that inadequate BP control is itself an independent risk factor for the development of diabetes in hypertensive patients.15 Combination Therapy:Theoretical ConsiderationsEfficacyRational combination therapy is based on the deliberate coadministration of two or more carefully selected antihy-pertensive agents.Inclusion of drugs known to reduce the long-term incidence of CV end points is highly preferred.A fundamental requirement of any combination is evidence that it lowers BP to a greater degree compared with mono-therapy with its individual components.This is achieved by combining agents that either interfere with distinctly different pressor mechanisms or effectively block counter-regulatory bining two drugs may result in partial or complete additivity of their BP-lowering effects, depending on the degree to which their pharmacologic effects are distinct and complimentary.Fully additive combinations are more effective in terms of BP reduction. In general,combining drugs from complementary classes is approximatelyfive times more effective in lowering BP than increasing the dose of one drug.16Another important requirement of a combination is pharmacokinetic compati-bility(ie,combined drug administration results in smooth and continuous BP reduction throughout the dosing interval).17These principles apply regardless of whether agents are included in an SPC or are coadministered as separate drugs.43A.H.Gradman et al./Journal of the American Society of Hypertension4(1)(2010)42–50TolerabilityImproving the overall tolerability of treatment is a key element in designing rational drug combinations.This beneficial effect will occur whenever side effects associated with a particular agent are neutralized by the pharmaco-logic properties of an added drug.17Because most antihy-pertensive agents produce dose-dependent side effects, high-dose monotherapy may lead to adverse events.In this circumstance,a lower dose of the initial agent in combination with another antihypertensive may be prefer-able to minimize dose-dependent side effects even if no additional BP reduction is achieved.An example is the use of a low-dose combination of an ACE inhibitor and a dihydropyridine CCB in a patient who develops edema at a higher CCB dose.In this instance,reducing the CCB dose and adding an ACE inhibitor will produce comparable BP reduction,but will generally do so without the side effects previously observed.18AdherenceLong-term adherence to treatment is necessary to control BP,and combination regimens can facilitate this objective, both in reducing the number of medications and the frequency of dosing required.A recent study of w85,000 patients from Kaiser Permanente found that adherence was inversely related to the number of medications prescribed. In this study,antihypertensive medication adherence levels were77.2%,69.7%,62.9%,and55%in subjects receiving one-,two-,three-,or four-drug regimens.19Other studies have found that adherence drops even more dramatically with increasing number of doses taken per day from71% with once-daily dosing to61%,50%,and31%with two, three,or four daily doses of antihypertensive medication.20 In many patients,SPCs promote adherence by reducing pill burden and simplifying the treatment regimen.In a meta-analysis of nine studies comparing administration of SPCs or their separate components,the adherence rate was improved by26%in patients receiving SPCs.21It should be emphasized that simplification of the treat-ment regimen is only one strategy for improving adherence. For many patients,cost is a critical issue.Branded combina-tions that are not available generically are often more expensive and can,in some cases,result in significant copays that adversely affect medication adherence.It should be noted that many SPCs that combine an ACE inhibitor with a diuretic are generic,as is one ACE inhibitor/ CCB combination.Physicians should be aware of these generic preparations and use them when necessary.They should not assume that an SPC improves adherence in every situation,particularly if its use increases direct patient expenditure or does not significantly reduce pill burden because the patient is receiving multiple other medications.Specific Drug CombinationsThere are seven major classes of antihypertensive drugs and multiple members of each class;therefore,the number of possible combinations is quite large.In this position paper,two-drug combinations involving classes of pharma-cologic agents that reduce CV end points(diuretics,CCBs, ACE inhibitors,ARBs,b-blockers)are emphasized. Combinations of three or more drugs are not reviewed. Specific combinations are designated as preferred or acceptable based on the considerations outlined previously. Combinations that are less effective on the basis of efficacy, safety,or tolerability concerns are also identified. RAAS InhibitorþDiureticThe combination of an ACE inhibitor,ARB,or direct renin inhibitor with a low-dose,thiazide-type diuretic results in fully additive BP reduction.22–26Diuretics initially reduce intravascular volume and activate the RAAS,leading to vasoconstriction as well as salt and water retention.In the presence of a RAAS inhibitor,this counterregulatory response is attenuated.Addition of a RAAS inhibitor to a thiazide-type diuretic also improves its safety profile by ameliorating diuretic-induced hypokalemia,27but can result in hyperkalemia in susceptible patients.Based on their safety, efficacy,and favorable performance in long-term trials, combinations of an ACE inhibitor or an ARB with a low-dose diuretic are classified as preferred.Most FDCs contain-ing a diuretic use hydrochlorthiazide(HCTZ).Because chlorthalidone is more effective than other diuretics in reducing BP over24hours28and was the agent used in all but one large US-based hypertension outcome trial,some authorities favor its use over HCTZ.Because it is not currently aligned in any SPC with an ACE inhibitor or ARB,it can be administered as a separate agent.RAAS InhibitorþCCBThe combination of an ACE inhibitor or ARB with a CCB results in fully additive BP reduction.29–31Addition of either of these two RAAS inhibitors significantly improves the tolerability profile of the CCB.Through their antisympa-thetic effects,RAAS inhibitors blunt the increase in heart rate that may accompany treatment with a dihydropyridine-type CCB.In addition,RAAS inhibitors partially neutralize the peripheral edema,which is a dose-limiting side effect of these CCBs.32The cause of the edema is believed to be arteriolar dilation,resulting in an increased pressure gradient across capillary membranes in dependent portions of the body.RAAS blockers are thought to counteract this effect through venodilation.The Avoiding Cardiovascular events through Combina-tion therapy in Patients Living with Systolic Hypertension trial tested whether initialfixed-dose combination therapy44 A.H.Gradman et al./Journal of the American Society of Hypertension4(1)(2010)42–50with an ACE inhibitor and CCB differs from initial fixed-dose combination therapy with an ACE inhibitor and diuretic on clinical outcomes in high-risk hypertensive patients.Despite comparable BP reduction,the ACE inhibitor/CCB combination reduced the combined end point of cardiovascular death,myocardial infarction,and stroke by20%compared with the ACE inhibitor/diuretic combination.33Of note,60%of patients were diabetic, and a large percentage had evidence of underlying ischemic heart disease.34These results suggest the superiority of a CCB over a diuretic when used in conjunction with a RAAS blocker in this high-risk population.ACE inhib-itor/CCB combinations are classified as preferred.In view of end point studies demonstrating comparability between ACE inhibitors and ARBs,ARB/CCB combinations are considered to be equivalent.35Renin InhibitorþARBsThe combination of a renin inhibitor with an ARB produces partially additive BP reduction and is well-tolerated.In a study in which maximum approved doses of valsartan and aliskiren were combined,a30%additional BP response was observed compared with either monother-apy.36The side effect profile of this acceptable combination was comparable with placebo.There are no cardiovascular outcome data with this combination to date.CCBsþDiureticsThe combination of a diuretic and a CCB results in partially additive BP reduction.37,38Presumably,this partial effect reflects overlap in the pharmacologic properties of the two Bs increase renal sodium excretion,albeit not to the same extent as diuretics.Moreover,long-term treat-ment with both classes is associated with vasodilation,given that volume depletion does not occur with diuretics.From an endpoint perspective,this combination performed well in the Valsartan Antihypertensive Long-term Use Evaluation trial in which HCTZ was added as a second step in patients randomized to amlodipine.39As opposed to ACE inhibitor/ CCB or ARB/CCB combinations,the CCBþdiuretic has no favorable effect on either drug’s side effect profile.These combinations are classified as acceptable.b-BlockersþDiureticsAlthough b-blockers reduce CV end points in placebo-controlled trials,meta-analyses(based primarily on the performance of atenolol)suggest that they are less effective than diuretics,ACE inhibitors,ARBs,and CCBs.40–42The antihypertensive effects of b-blockers are mediated through reduction in cardiac output and suppression of renin release.43 As with the ACE inhibitors and ARBs,b-blockers attenuate the RAAS activation that accompanies the use of thiazide diuretics,and their combination results in fully additive BP reduction.44–46Addition of diuretics also improves the effec-tiveness of b-blockers in blacks and others with low renin hypertension.47These combinations are classified as accept-able,recognizing that their use is associated with increased risk of glucose intolerance,fatigue,and sexual dysfunction. Thiazide DiureticsþPotassium-sparingDiureticsHypokalemia is an extremely important dose-related side effect of thiazide diuretics.By attenuating hypokalemia, the combination of HCTZ with a potassium-sparing diuretic such as triamterene,amiloride,or spironolactone improves its safety profile.48Because of the risk of hypokalemia that can lead to cardiac arrhythmias,and sudden death,HCTZ 50mg and chlorthalidone25mg should generally be used in combination with a potassium-sparing agent(or an inhib-itor of the RAAS).Given the latest data demonstrating the importance of aldosterone blockade in obese patients and the efficacy of aldosterone blockade in helping achieve BP goals,the spironolactone/HCTZ combination is particularly well-suited in such individuals.49The addition of amiloride to HCTZ reduces hypokalemia and results in variable BP reduction.50,51These combinations are classified as accept-able in people with relatively well-preserved kidney function (ie,estimated glomerularfiltration rate>50mL/min/1.73 m2).At glomerularfiltration rate levels below this,the risk for hyperkalemia increases and the diuretic efficacy of HCTZ starts to diminish.52CCBsþb-BlockersThe pharmacologic effects of these two drug classes are complementary,and their combination results in additive BP reduction.In one study,a low-dose combination of felodipine ER and metoprolol ER produced BP reduction comparable to maximum doses of each agent with an inci-dence of edema similar to placebo.53,54The combination of a b-blocker and a dihydropyridine CCB is acceptable. b-blockers should not generally be combined with nondihy-dropyridine CCBs such as verapamil or diltiazem because their additive effects on heart rate and A-V conduction may result in severe bradycardia or heart block.Less Effective CombinationsACE InhibitorsþARBsAlthough sometimes useful for proteinuria reduction and in the treatment of symptomatic patients with heart failure, the combination of an ACE inhibitor and an ARB is not recommended for the treatment of hypertension.ACE/ ARB combinations produce little additional BP reduction compared with monotherapy with either agent alone.In the Ongoing Telmisartan Alone and in Combination with45A.H.Gradman et al./Journal of the American Society of Hypertension4(1)(2010)42–50Ramipril Global Endpoint Trial,patients receiving the ACE inhibitor/ARB combination showed no improvement in cardiovascular end points despite additional BP reduction averaging2.4/1.4mm Hg.35There were also more side effects with the combination than with individual agents. These combinations are classified as less effective. RAAS Inhibitorþb-BlockerThese drug classes are both cardioprotective and are frequently coadministered to patients with coronary heart disease or heart failure.When these agents are combined, however,they produce little additional BP reduction compared with either monotherapy.55For this reason,they constitute a less effective combination when BP reduction is the principal goal.They can,however,be used together in patients with coronary artery disease or heart failure when outcome improvement is the primary objective.b-BlockersþCentrally Acting Agentsb-blockers and centrally acting agent(eg,clonidine, a-methyldopa)interfere with the sympathetic nervous system.The degree to which they produce additive BP reduc-tion has not been studied.When used together,their combi-nation may result in severe bradycardia or heart block.In addition,when discontinued abruptly,patients receiving these drugs in combination may exhibit severe rebound hypertension.56For this reason,they constitute a less effec-tive combination.Clinical ApplicationPatient Selection:Initial TherapyBecause most patients with hypertension will require two to three drugs to achieve BP control,the pivotal questions for initial therapy are as follows.Should treatment be started with monotherapy ora combination?If two drugs are initiated,should they be administered as single entities or an SPC?Although there is limited scientific evidence to answer these questions definitively,several considerations support the use of initial combination therapy in most patients with hypertension.Initiation of multiple drugs targets multiple physiologic pathways,making it more likely that those making a significant contribution to BP elevation will be inhibited.By beginning with combination therapy,counter-regulatory responses will be reduced.The result is an increase in the percentage of responders as well as increased magnitude of response in any population of hypertensive patients.Recent studies also suggest an important correlation between the time taken to achieve goal BP and clinical outcome.In the Valsartan Antihypertensive Long-term Use Evaluation trial,a post hoc analysis indicated that subjects who reached target BP within6months of entering the protocol demonstrated substantially better outcomes throughout the5-year duration of the study,regardless of assigned treatment.57Likewise,in the International Verap-amil SR-Trandolapril study,lower CV risk was documented in patients who spent a larger fraction of the time with BP <140/90mm Hg.58,59It is therefore prudent to adopt therapeutic approaches designed to achieve goal BP within several months whenever possible.Several studies have documented that BP control is achieved more rapidly using an initial combination strategy.Weir et al compared the time to achieve goal BP withfixed doses of the ARB,valsartan,alone and in combination with HCTZ in a meta-analysis of nine randomized trials that included subjects with either stage1or stage2hypertension.After8weeks of treatment,48%of patients begun on monotherapy with the usual starting dose of valsartan achieved their Joint National Committee on Prevention,Detection,Evaluation,and Treat-ment of High Blood Pressure(JNC)-7target compared with 75%begun on a combination of HCTZ with the same dose of valsartan.60In the Avoiding Cardiovascular events through Combination therapy in Patients Living with Systolic Hyper-tension study,thefirst major end point trial in which treatment was initiated with an SPC,BP was reduced to<140/90mm Hg in73%of patients after6months.61The Simplified Treatment Intervention to Control Hypertension study compared the effectiveness of a treatment algorithm using an initial SPC (ACEI/HCTZ or ARB/HCTZ)to a guideline-based approach that included initial monotherapy in45Canadian family prac-tices.In this‘‘real-world’’study,the proportion of subjects who achieved target BP within6months was65%in those initiated with the SPC compared with53%receiving guideline-based treatment.Patients initiated on the SPC experienced no addi-tional side effects.62Current guidelines suggest that two drugs be used for initial therapy if there is a20/10mm Hg elevation in BP above goal(BP is>160/100mm Hg for patients with uncom-plicated hypertension or>150/90for those with diabetes and other comorbid conditions).1–3For patients with stage1 hypertension,it is often reasonable to start with monother-apy.Recent data,however,suggest that the advantages of initial combination treatment may extend to stage1hyper-tension.In the meta-analysis by Weir,the magnitude of effect in terms of time-specific achievement of goal BP was greater in the stage1compared with the stage2subgroup.Among patients who were stage1,72%achieved their JNC-7target by week8if initiated on valsartan160mg monotherapy vs. 92%who received initial therapy with the same dose of valsartan in combination with HCTZ.60With regard to tolerability,the percentage of patients complaining of dizzi-ness was higher in the combination treatment group,but the number who discontinued therapy from adverse events was similar.46 A.H.Gradman et al./Journal of the American Society of Hypertension4(1)(2010)42–50SPCsSingle pill combinations may be used:as initial treatment in a patient in whom multidrug therapy is likely to be needed, as the‘‘second step’’in a patient partially controlled on monotherapy,or as a substitute for independently titrated doses of individual components.Convenience is the major advantage of using an SPC.It is easier for the patient to comply with a regimen that includes fewer pills.63In addi-tion,it takes less time for a physician to achieve BP control in a group of patients using a combination that is known to be safe,effective,and well-tolerated.62,64On the other hand,SPCs may significantly increase the cost to the patient compared with adding individual generic drugs and may affect the pharmacokinetics of administered agents.The same or better control rates and medication costs as SPCs can be achieved through the use of a labor intensive, knowledge-based approach.For example,in the Collabora-tive Management of Hypertension study,a physician/ pharmacist team achieved an89%BP control rate within9 months using such an approach.65Although some form of combination treatment is a necessity,similar treatment results are achievable with or without the routine use of SPCs.The choice can be made based on the individual practice setting and the resources available to both patient and physician. Combination Therapy:Partially Treated PatientsIn patients who are taking antihypertensive therapy but do not have their BP controlled,additional treatment is indicated.The selection of specific combinations should be made from those that are listed as preferred or accept-able in the Table;less effective combinations should generally be avoided or used with caution.The choice of specific combinations will be dictated by individual patient considerations including demographics,comorbid condi-tions,response to previous treatments,and cost,as well as physician preference.The goal is always cost-effective, long-term treatment which controls BP using agents that are safe,effective,and well-tolerated.Summary RecommendationsUse combination therapy routinely to achieve BP targetsUse only preferred or acceptable two-drug combinations (Table)Initiate combination therapy routinely in patients who require 20/10mm Hg BP reduction to achieve target BPInitiate combination therapy in stage1patients(at the physician’s discretion),especially when the second agent will improve the side effect profile of initial therapyUse SPCs rather than separate individual agents in circumstances where convenience outweighs other considerationsAcknowledgmentsThis article was reviewed by Raymond R.Townsend, MD,and Matthew R.Weir,MD.The American Society of Hypertension Writing Group Steering Committee:Barry J.Materson,MD,MBA,Chair; Henry R Black,MD;Joseph L.Izzo,Jr.,MD;Suzanne Oparil,MD;and Michael A.Weber,MD.References1.Chobanian A V,Bakris GL,Black HR,Cushman WC,Green LA,Izzo JL Jr,et al.National High Blood Pressure Education Program Coordinating Committee: Seventh Report of the Joint National Committee on Prevention,Detection,Evaluation,and Treatment of High Blood Pressure.Hypertension2003;42:1206–52.2.The Task Force for the Management of Arterial Hyper-tension of the European Society of Hypertension(ESH) and of the European Society of Cardiology(ESC):2007 Guidelines for the management of arterial hypertension.J Hypertens2007;25:1105–87.3.Williams B,Poulter NR,Brown MJ,et al.Guidelines forthe management of hypertension:report of the fourth working party of the British Hypertension Society, 2004–BHSIV.J Hum Hypertens2004;18:139–85.4.Mancia G,Laurent S,Agabati-Rosei E,et al.Reap-praisal of European guidelines on hypertension management:a European Society of Hypertension Task Force document.J Hypertens2009;27:2121–58.TableDrug Combinations in Hypertension:Recommendations PreferredACE inhibitor/diuretic*ARB/diuretic*ACE inhibitor/CCB*ARB/CCB*Acceptableb-blocker/diuretic*CCB(dihydropyridine)/b-blockerCCB/diureticRenin inhibitor/diuretic*Renin inhibitor/ARB*Thiazide diuretics/Kþsparing diuretics*Less effectiveACE inhibitor/ARBACE inhibitor/b-blockerARB/b-blockerCCB(nondihydropyridine)/b-blockerCentrally acting agent/b-blockerARB,angiotensin receptor blocker;ACE,angiotensin-converting enzyme;CCB,calcium channel blocker.*Single pill combinations available in the United States.47A.H.Gradman et al./Journal of the American Society of Hypertension4(1)(2010)42–50。
见微知著:漫谈阿片类镇痛药物——地佐辛
见微知著:漫谈阿片类镇痛药物——地佐辛谢克亮;王国林【摘要】地佐辛作为混合阿片受体激动/拮抗剂,镇痛效果好,不良反应少,得到临床医师的认可,近几年在临床中广泛应用.地佐辛可与其他μ受体阿片药物合用,增强镇痛效果;该药不仅在术后镇痛中应用,还可以在围术期应用.本文通过总结近年地佐辛在作用机制和临床应用方面的相关研究,重点阐述该药在术后镇痛、手术麻醉中和手术室外的应用,为临床用药提供依据.【期刊名称】《广东医学》【年(卷),期】2018(039)001【总页数】3页(P10-12)【关键词】地佐辛;术后;镇痛;加速康复【作者】谢克亮;王国林【作者单位】天津医科大学总医院麻醉科,天津300052;天津医科大学总医院麻醉科,天津300052【正文语种】中文国际疼痛学会(International Association for the Study of Pain,IASP)定义疼痛是一种令人不快的感觉和情绪上的主观感受,伴有现存的和潜在的组织损伤。
在临床工作中,疼痛已成为继体温、脉搏、呼吸、血压4大生命体征之后的第5生命体征,并日益得到重视。
有效的治疗和控制围术期疼痛,可直接影响手术患者的预后和转归。
围术期疼痛管理是加速康复外科(enhanced recovery after surgery,ERAS)的重要组成部分。
随着患者的对围术期舒适度要求的不断提升,越来越多的疼痛治疗药物被不断的研发生产。
阿片类药物是医学疼痛治疗中的基石,也在不断创新研发之中。
1952年吗啡经美国食品药品管理局(FDA) 批准上市[1],1982年哌替啶上市,1984年芬太尼上市[2],1986—1996年舒芬太尼、阿芬太尼、雷米芬太尼相继上市[3]。
这些阿片类药物为围术期临床麻醉与镇痛提供了良好的选择,但是强阿片类药物在提供镇痛作用的同时,也存在相关不良反应,其发生的耐受、依赖及滥用也给临床医师和患者带来了困扰。
阿片受体激动-拮抗剂是在寻找更少不良反应和滥用的强效镇痛剂中发展起来的。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
1
IntrodBiblioteka ctionQuery Recommendation is an information retrieval technology to recommend identical or related queries for a particular query. Its core mission is to understand user’s query intention through machine learning, mine the expressional forms of query with similar intentions, and finally realize mutual recommendation of the synonymous or associated queries. The ultimate purpose is to use the synonymous or associated queries as medium to share and mutually recommend better search results. Currently, the main research form of query recommendation is to express user’s potential query intention with the correlation information within the framework of information retrieval and outside the query such as relevant or pseudo-relevant text content or click and browsing retrieval behaviors, then measure query semantic consistency and intention association, and recommend approximate or related queries finally. However, we ignore to analyze or understand the intention from query itself because of sparse information, fuzzy structural relations and optional component forms.It is often used as a medium to auxiliarily mine external reference resources which contain richer and potential intention informations. Therefore, query itself was long considered “be unrefined” for intention analysis and query recommendation.
Divided Pretreatment to Targets and Intentions for Query Recommendation
Yangyang Kang, Yu Hong*, Li Yu, Jianmin Yao, and Qiaoming Zhu School of Computer Science & Technology, Soochow University No.1 Shizi Street, Canglang District, Suzhou City, Jiangsu Province, 215006 tianxianer@
*
Corresponding author.
M. Zhou et al. (Eds.): NLPCC 2012, CCIS 333, pp. 199–212, 2012. © Springer-Verlag Berlin Heidelberg 2012
200
Y. Kang et al.
However, query is a direct intention expression of user, which describes real and appropriate meaning of intention. At the same time, query itself contains less noisy informations when semantic ambiguity and misspelling is ignored. In contrast, using external resources associated with the query for intention analysis will introduce a lot of noise which will mislead intention analysis and calculation. So, if there is an effective measure of expansion and disambiguation, the direct use of query itself can achieve the mining of correlation intention and query recommendation from the perspective most closed to user as well as intention expressed in behavior. Therefore, we propose a query recommendation method based on divided pretreatment to query targets and query intentions. This method includes three basic steps. ─ Classifying and recognizing the words of query which describe the target and the intention. ─ Clustering the words of query intention to mine consistent or similar intention. ─ Using intention cluster to realize a simple substitution of peer intentions to form query recommendation. Query target refers to the target entity, behavior or status which user retrieves. Query intention refers to the operations of intention or the motivations of retrieval which impose on the query target. For Example 1, there is a query “Where is the No. 18 bus station?”..Its query target is “No. 18 bus station” and query intention is “where”. We can effectively overcome the sparsity and ambiguity of the query informations, through classifying and recognizing the targets and intentions of query with largescale query samples. As the sparsity of the information which describes the intention, we can expand by different intention words with common target. There are queries such as “How to get to the 18 bus station?”, “Where is the location of the 18 bus station” and “Where is the position of the 18 bus station” with common target “18 bus station” in large-scale query samples. We expand the intention “where” in example 1 to {“where”, “how to get to”, “location”, “position”} to enrich the description of original query intention. As description of target can cause ambiguity possibility, we can take different targets pointed to by same intention to disambiguate. For example 2, there is a query “Apple Quote” which query target is “Apple” and query intention is “Quote”. The target “Apple” is ambiguous because it may refers to the electronic product or fruit. So, we gather the queries with consistent intention words such as “Iphone Quote”, “Ipod Quote”, “Computer Quote”, “Mainboard Quote”. By extracting the description of targets, the lexical meanings {“Iphone”, “Ipod”, “Computer”, “Mainboard”} of target “Apple” in original query are formed to disambiguate effectively. While, “Fruit” is often gone with the word “Price”, such as “Banana Price” rather than “Banana Quote”. In the rest of the paper, we will first introduce the related work in Section 2. Then, we give the framework of a new query recommendation method based on divided pretreatment to targets and intentions in Section 3. Section 4 will show the modeling process of classifying and recognizing the targets and intentions of query. The method of intention cluster will be given in Section 5. We present and discuss the experimental results in Section 6. Finally, we conclude the paper in Section 7.