Medical Systems
医疗保障体系英语

医疗保障体系英语
医疗保障体系在英语中可以表达为"Healthcare System"。
以下是关于医疗保障体系的一些常见英语表达和术语:
Healthcare System: 医疗保障体系
Health Insurance: 健康保险
Universal Healthcare: 普遍医疗制度
Public Health Services: 公共卫生服务
Medical Coverage: 医疗保障
Healthcare Access: 医疗服务获取
Primary Care Physicians: 初级医疗服务提供者
Specialist Services: 专科医疗服务
Outpatient Care: 门诊医疗服务
Inpatient Care: 住院医疗服务
Prescription Medications: 处方药物
Preventive Care: 预防保健
Emergency Medical Services (EMS): 急救医疗服务
Healthcare Providers: 医疗服务提供者
Healthcare Facilities: 医疗机构
Healthcare Professionals: 医疗专业人员
Medical Expenses: 医疗费用
Patient Care: 患者护理
Telemedicine: 远程医疗
Healthcare Policy: 医疗政策
这些术语可以用于描述医疗保障体系的各个方面,从健康保险到医疗服务的不同层面。
医学领域英语词汇全集
医学领域英语词汇全集以下是医学领域常用的英语词汇全集,供参考:1. Anatomy(解剖学)- Skeleton(骨骼)- Muscles(肌肉)- Organs(器官)- Nerves(神经)2. Physiology(生理学)- Circulatory system(循环系统)- Respiratory system(呼吸系统)- Digestive system(消化系统)- Endocrine system(内分泌系统)3. Diseases(疾病)- Cancer(癌症)- Diabetes(糖尿病)- Hypertension(高血压)- Influenza(流感)4. Medical Procedures(医疗程序)- Surgery(外科手术)- Radiology(放射学)- Physical therapy(物理疗法)- Chemotherapy(化疗)5. Medications(药物)- Antibiotics(抗生素)- Analgesics(止痛药)- Antidepressants(抗抑郁药)- Antihistamines(抗组胺药)6. Medical Equipment(医疗设备)- Stethoscope(听诊器)- X-ray machine(X光机)- Ultrasound machine(超声波机)- Blood pressure monitor(血压计)7. Medical Specialties(医学专业)- Cardiology(心脏病学)- Dermatology(皮肤病学)- Gynecology(妇科学)- Pediatrics(儿科学)8. Medical Ethics(医学伦理)- Informed consent(知情同意)- Confidentiality(保密性)- Patient autonomy(患者自主权)- Non-maleficence(不伤害原则)9. Medical Research(医学研究)- Clinical trials(临床试验)- Case studies(病例研究)- Epidemiology(流行病学)- Genetic research(遗传研究)以上是医学领域常用的英语词汇全集。
医疗系统专业术语

医疗系统专业术语1. HIS(医院信息系统)HIS全称Hospital Information System。
HIS是覆盖医院所有业务和业务全过程的信息管理系统。
利用电子计算机和通讯设备,为医院所属各部门提供病人诊疗信息和行政管理信息的收集、存储、处理、提取和数据交换的能力并满足授权用户的功能需求的平台。
天健HIS系统包括:PACS、RIS、LIS、PIS、PEIS、CIS、EMR、Medvision影像工作站等。
2. LIS(检验信息系统)LIS全称Laboratory Information Management System。
LIS是专为医院检验科设计的一套实验室信息管理系统,能将实验仪器与计算机组成网络,使病人样品登录、实验数据存取、报告审核、打印分发,实验数据统计分析等繁杂的操作过程实现了智能化、自动化和规范化管理。
3. PACS(影像归档和通信系统)PACS全称Picture Archiving and munication Systems。
它是应用在医院影像科室的系统,主要的任务就是把日常产生的各种医学影像(包括核磁,CT,超声,X光机,红外仪、显微仪等设备产生的图像)通过各种接口(模拟,DI,网络)以数字化的方式海量保存起来,当需要的时候在一定的授权下能够很快的调回使用,同时增加一些辅助诊断管理功能。
它在各种影像设备间传输数据和组织存储数据具有重要作用。
DI (Digital Imaging and munications in Medicine),是医学数字成像和通信的标准。
4. RIS(放射科信息系统)RIS全称Radiology Information System。
它是医院重要的医学影像信息系统之一,它与PACS系统共同构成医学影像学的信息化环境。
放射科信息系统是基于医院影像科室工作流程的任务执行过程管理的计算机信息系统,主要实现医学影像学检验工作流程的计算机网络化控制、管理和医学图文信息的共享,并在此基础上实现远程医疗。
美国医疗系统(AmericanMedicalSystem)

美国医疗系统(American Medical System)Medical system in the United States--------------------------------------------------------------------------------There is a course on medical policy that describes the structure and functioning of the American health care system, the interaction between patients and health care providers, and the role that they play in the health care system. The United States does not currently have a national health care system, and only two Medicare and Medicaid are federally managed medical organizations. Although they are part of social welfare, the former belongs to the elderly medical care, the latter to the disabled and low-income families.The medical administration is closely related to the daily lives of the American people, affecting the patterns of medical referral, the extent of physician prescribing, and the chances that patients will receive appropriate care. In the 90s, the American Medical System plunged into a dilemma of medical waste and unequal allocation of medical resources. Some have a complete health care who accept unnecessary medical services; while others have no insurance (1996, more than 40 million Americans without health insurance or medical insurance), is not perfect, they receive the necessary medical services were deprived of their rights. Over the past few years, however, there has been a landmark change in the health care system in the United states. This major reform stems from a new concept, "Managed care"". Managed care has developed new interactions between American patients, insurance companies, and healthcare workers.Traditionally, employers for their employees to pay the medical insurance premium to the insurance company, the insurance company (the insurer) payment for medical service providers (including physicians, hospitals, home - care, nursing, home institutions or pharmacy). Under the system, the doctor decides what kind of treatment, treatment, and who should provide medical care. Medical costs are usually decided unilaterally by providers of medical services, and insurance companies simply pay medical bills. If the cost is too high, the insurance company will increase the premium for the following year (premium). Under the Managed care system, institutions that settle patient health costs will play the role of managing patient care. Employers and insurance companies don't just pay medical bills. They also decide how much medical care they should give to patients, what medical services, and who should provide them with treatment. In other words, employers and insurance companies will determine the way health care providers receive income and how they pay. Therefore, managed care can be said to be a major change in the American Medical system. In the past, medical professionals, especially physicians, decided that the rights of medical behavior were no longer. Doctors and employers, as well as insurance companies, share their decisions. This profoundly changed the doctor's role in the medical system.Payment system for medical careThere are four kinds of payment system in American Medical care:1) out - of - pocket payment,2) individual, private, insurance,3) employment - based group private insurance4) government financingThe first is the simplest payment system - just as consumers buy goods and services directly. However, based on several characteristics, medical care is different from the general consumer behavior. For example, medical care is the basic human needs, and not a luxury; so if the patient is unable to bear the medical expenses, there must be a different from the out - of - Pocket payment system to help patients to pay for medical expenses and medical needs; and expenditure cannot advance estimates and selection; and when patients receive treatment, often lack these treatment knowledge; not to mention the people do not know what time they will be hit by illness or injury.The second is private insurance - in addition to patients and medical staff, the insurance company is on the one hand to collect premiums, on the other hand, pay the patient's medical expenses to the medical institutions.The third is Employment--based group private insurance - the employer pays all or part of the medical premium for the employer. Health insurance provides a mechanism for allocating medical resources to people who really need it, not on their ability to pay medical bills. In other words, the premium fund is redistributed from the healthy person to the patient, whilethe health care system helps the person who cannot pay the medical expenses to share their expenses. However, the positive significance of health care in this respect has sometimes become its fatal injury. The original is to solve the Out - of - Pocket payment system, the patient can not afford the high medical costs will lead to control medical expenses, but the dilemma. Because under this system, patients don't have to pay for their own medical bills themselves, so virtually everyone will increase the number of visits. Together with medical institutions turning to insurance companies, they can easily raise medical costs. Therefore, based on the consideration of business competition, insurance companies have to lower their premiums to attract young, healthy or low-risk groups. By contrast, the elderly and the sick are becoming less and less able to pay high premiums. In order to cope with the new problems, there are fourth kinds of payment systems, namely Tax - financed government health insurance: Medicare and Medicaid. Medicare's services are for the elderly, funded from social security taxes, federal taxes, and premiums paid by beneficiaries. The Medicaid is run by the state government, targeting low-income people, with federal taxes and state taxes.In our impression, the United States is a country with a sound social welfare system, and the medical care system should be no exception. But in 1996, nearly 1/6 of Americans had no medical insurance. The main reason is that in the employment--based system, some employers are reluctant to insure their employees (the reason is rising year by year reduced premium and enterprise scale makes the employer cannot afford); or some people belong to non employees, or is in a state of temporary unemployment. Although these people could notafford the premiums for private health insurance, they failed to meet standards that could benefit from Medicare and Medicaid.As a result of the recent economic downturn, many people have been forced to change jobs, divorce or retire early because they have been forced to retire by lay off,Suspension or even permanent loss of coverage. But even with health insurance, most insurance companies now restrict access to the care they need. The reason is that in order to reduce expenditure, the insurance company does not cover certain treatments or examinations, such as injection prevention and mammograms. They also reject the cover pre-existing disease, and limit the amount of benefit (benefit), or adopt the co payment system.Reimbursement for medical expenses (reimbursements)We mentioned different medical payment systems and the problem of high medical costs. The main reason for this problem stems from the high costs of medical and medical reimbursement (reimbursements) for physicians and hospitals. As a result, new approaches to reimbursement are being developed to stem the growth of medical costs. And these new methods are the main features of managed care. These methods include:Fee-for-service, episode, of, illness, Diem, payment, capitation, salary (or, global, budget). In the form of reimbursement for the first fee-for-service, the medical unit is paid on the basis of individual visits, EKG checks, or treatment procedures. Under the Payment per procedure system,physicians will have more perform examinations and treatment programs in order to obtain more payment. As a result, medical costs are rising and waste of medical resources. The second way is according to the Diagnosis-related group (DRGs) classification, during a disease, regardless of the amount of medical service, medical service is a sum of all payments to hospitals, such as global surgical fees and Hospital DRGs. The unit of payment is not individual treatment or examination, but case or episode. Under this system, physicians will perform more surgery and limit the number of patients postoperative visits. Because they don't get extra payment from the patient's extra visits, the risk of a rise in medical costs is partly transfer. In third Diem payment way, to accept all patients according to the sum of the day hospital service is payment unit is the number of days (i.e. whether the hospital a day for examination and treatment of patients number, it gets payment is a fixed number). The fourth is capitation, the unit is individual. Regardless of the number, degree, or degree of medical treatment each patient receives in one month or year, payment is given to the head. The reimbursement system is very close to managed care.Because you've already mentioned managed care plan, so let's explain its meaning here. Traditionally, physicians and hospitals charge fees based on individual services. In order to control costs, people joined managed care plan to change the way medical units were paid. In the Managed care organization, three main forms are: Fee-for-service, practice, with, utilization, view, preferred, provider, organizations (PPOs),和健康维护组织(HMO)。
Philips Medical Systems JETConnect 9206-0000 版本 C

DICOM 3.0CONFORMANCESTATEMENTJETConnect9206-0000, REV. C 09-20049206-0000, REV. C09-2004A D A CA Philips Medical Systems CompanyCopyright StatementPhilips Medical Systems has taken care to ensure the accuracy of this document. However, Philips Medical Systems assumes no liability for errors or omissions and reserves the right to make changes without further notice to any products herein to improve reliability, function, or design. Philips Medical Systems provides this guide without warranty of any kind, either implied or expressed, including, but not limited to, the implied warranties of merchantability and fitness for a particular purpose. Philips Medical Systems may make improvements or changes in the product(s) and/or program(s) described in this manual at any time.This document contains proprietary information which is protected by copyright. All rights are reserved.No part of this manual may be photocopied, reproduced, or translated to another language without written permission from Philips Medical Systems.Philips Medical Systems reserves the right to revise this publication and to make changes in content from time to time without obligation on the part of Philips Medical Systems to provide notification of such revision or change.DisclaimerPhilips Medical Systems DICOM software is in compliance with the ACR-NEMA DICOM 3.0 standard;however, due to the inherent nature of DICOM, the user must perform acceptance testing to verify that the Philips Medical Systems DICOM software meets the requirements for your configuration. The acceptance testing must include all representative datasets (images) that you intend to transfer, all types of transfers desired for a type of dataset, and clinical evaluation of each representative dataset on the receiving end after each desired type of transfer. For further information on conformance of this product to the DICOM 3.0 standard, please refer to the DICOM 3.0 JETConnect Conformance Statement, Philips Medical Systems.TrademarksADAC®, CPET®Imaging System, CPET®Plus Imaging System, FORTE TM, Cardio TM, CardioMD®,CardioTrac TM, Cardio TM 60, GlobalQ®, Solus TM, Vertex TM, Vertex TM Plus,Vertex TM 60, EPIC TM, Pegasys TM, Pegasys TM X, Pegasys TM MD, Pegasys TM MD+, Pegasys TM Ultra, Atlas TM, AutoQUANT®, ARGUS®, GENESYS®, AutoSPECT®, AutoSPECT®Plus, CardiaQ®, PINNACLE®, SMARTSIM®, P3IMRT®, InStill®, INSYNC TM, P3MD TM, PIXELAR TM, ALLEGRO TM, JetStream TM, DELTA PIXEL BEAM TM, SKYLight®, PETPLAN TM,APET TM, Transcam TM, SKYTable TM, Midas TM, Shadow TM, Vantage TM, ExSPECT TM, ACCESS TM, X-ACT TM, FlexLOGIC TM, TeleLOGIC TM, InteLOGIC TM, SENTRY TM, VersaTable TM, ColliMATE TM, EZX TM, CCT TM, WebView TM, MCD/AC TM and GEMINI TM are trademarks or registered trademarks of Philips Medical Systems.Adobe, the Adobe logo, Acrobat, the Acrobat logo, and PostScript are trademarks of Adobe SystemsIncorporated or its subsidiaries and may be registered in certain jurisdictions.Sun, SunView, NFS, OpenWindows, Solaris, and SPARCstation are trademarks of Sun Microsystems, Inc.SPARC is a registered trademark of SPARC International, Inc.SPARCstation is a trademark of SPARC International, Inc. licensed exclusively to Sun Microsystems, Inc.UNIX and OPEN LOOK are registered trademarks of UNIX System Laboratories, Inc.X Window System is a trademark of the Massachusetts Institute of Technology.Other brand or product names are trademarks or registered trademarks of their respective holders. Prescription Device StatementCaution: Federal law restricts this device to sale by or on the order of a physician (or properly licensed practitioner).Copyright 2004, Koninklijke Philips Electronics N.V.540 Alder Drive, Milpitas, CA, 95035, USA9206-0000, REV. C•PROPERTY OF KONINKLIJKE PHILIPS ELECTRONICS N.V.•Table of Contents T ABLE OF C ONTENTSINTRODUCTION (1)Scope (1)Important Notes (1)Why a Conformance Statement (1)Source of Information (2)How DICOM Works in JETConnect DICOM (2)Implementation Model (3)Application Data Flow Diagram (3)Functional Definitions of AE (Application Entities) (4)Sequencing of Real-World Activities (4)Network Interchange AE Specifications (4)Supported SOP Classes (4)Communication Profiles (9)Deviation Report (10)Extensions, Specialization, Privatizations (10)Support of Extended Character Sets (10)Configuration (10)Comments (10)Appendix A :GLOSSARY.......................................................................................................A-1 Acronyms and Abbreviations .........................................................................................................A-19206-0000, REV. C09-2004DICOM 3.0 Conformance Statement JETConnect■iiiTable of Contentsiv■DICOM 3.0 Conformance Statement JETConnect9206-0000, R EV. C09-2004INTRODUCTION INTRODUCTIONScopeThis document states the conformance of the JETConnect DICOM software versionAtlantis400R01.The DICOM conformance of other medical devices manufactured by Philips MedicalSystems is detailed in separate documents.Important NotesThis DICOM software is in compliance with ACR-NEMA DICOM 3.0 standard;however, due to the inherent nature of DICOM, you must perform acceptance testingto verify that the DICOM software meets requirements for your configuration.The acceptance testing must include all representative data sets (images) that youintend to transfer, all types of transfers desired for a type of data set, and clinicalevaluation of each representative data set on the receiving end after the transfer ofthe desired type.Please read the following sections carefully before you use any of the DICOMsoftware products.Why a Conformance StatementThe DICOM 3.0 standard enables vendors to configure systems in such a way that animaging device can exchange patient and image data with another imaging device ofthe same or different modality, a Radiology Information System (RIS), a HospitalInformation System (HIS), a Review/PACS station, or an archive device or a hardcopydevice over a standard network. It also permits data exchange via removable media,such as a magneto-optical disk.Because of the broadness and extensibility of the DICOM standard, each DICOM-conforming system normally supports only a subset of DICOM 3.0. Each pair ofDICOM peer devices, or Application Entities (AE), can only communicate over theintersection of commonly supported parts of DICOM. Fortunately, DICOM 3.0standard requires some minimum conformance.This conformance statement can help you understand the level of connectivitybetween JETConnect DICOM and other DICOM-compatible devices.This conformance statement is written in accordance with Part 2 of DICOM, NEMAStandards Publication No. PS 3.2.9206-0000, REV. C09-2004DICOM 3.0 Conformance Statement JETConnect■1INTRODUCTION2■DICOM 3.0 Conformance Statement JETConnect 9206-0000, REV. C 09-2004Source of InformationDigital Imaging and Communication in Medicine (DICOM), NEMA Standards Publi-cation No. PS 3.1~3.16.NEMA, 1300 N. 17th Street Rosalyn, Virginia 22209 USAHow DICOM Works in JETConnect DICOMJETStream acquisition computers build a transparent network environment with other DICOM-compatible imaging and administrative medical devices (i.e.: PACS) through an implementation of some of the following DICOM service classes (see NEMA Standard Publication PS 3.4) and DICOM message exchange commands (see NEMA Standard Publication PS 3.7).The JETConnect DICOM software is transparent to the person using the SKYLight or Forte imaging system. The Philips Nuclear Medicine Field Service Engineer is not required to change or modify any configurations. By default the Save To field on the Protocol Information page is set to the target system (DICOM target). A Philips Nuclear Medicine Field Service Engineer configures the JETConnect DICOM software during the initial installation.Table 1 on page 2 describes the DICOM Service Classes and DICOM Commands supported by JETConnect DICOM.Table 1: DICOM Service Classes and Commands DICOM Service ClassDICOM commands (DIMSE-C/N group)Purpose VerificationC-ECHO Checks if the peer application entity is active StorageC-STORE Image data transfer Modality Worklist C-FIND Patient and Schedule dataretrievalStorage Commitment N-ActionChecks if the data transfer wassuccessful.Implementation Model9206-0000, REV. C 09-2004DICOM 3.0 Conformance Statement JETConnect ■3Implementation ModelApplication Data Flow DiagramVerificationSimple Image Transfer “Put”DICOM interface JETConnectDICOM Foreign host DICOMC-ECHO-RQ “ping”C-ECHO-RSP “echo”DICOM Interface JETConnectDICOM Foreign host DICOM Storage CommitC-STORE-RQ “put”C-STORE-RSP “acknowledge”(1) Storage of images, overlays, etcJETConnectDICOM Foreign host DICOM(2) N-Action (Request Storage Commitment)(3) N-Event-Report (Results Status)Sequencing of Real-World Activities4■DICOM 3.0 Conformance Statement JETConnect 9206-0000, REV. C 09-2004Worklist QueryFunctional Definitions of AE (Application Entities)A utility program called mc3echo performs C-ECHO to check if a remote DICOM peer is responding. The DICOM server responds to a remote C-ECHO with a C-ECHO-RSP .◆Exporting image data to a remote systemThe JETStream acquisition automates the export to the remote system.JETConnect initiates a C-STORE request and the remote DICOM server uses the SCP role of storage to receive the data.Sequencing of Real-World ActivitiesNot Applicable.Network Interchange AE Specifications Supported SOP ClassesJETConnect DICOM provides standard conformance to the following DICOM 3.0 SOP Classes.Table 2: Verification of SOP Class SOP Class NameSOP Class UID Role Verification 1.2.840.10008.1.1SCUDICOM interface JETConnectDICOM Foreign host DICOMC-FIND-RQ “request worklist”C-FIND-RSP “directories ”Supported SOP Classes9206-0000, REV. C 09-2004DICOM 3.0 Conformance Statement JETConnect ■5General Association PoliciesThis implementation generally establishes one association (connection) per SOP interaction, such as Ping-Echo and Store (“put”), Find (query for Worklist infor-mation). The association closes at the completion of each interaction. The associ-ation aborts if the SOP class is not supported.Some interactions, such as C-STORE, require a series of packet exchanges. The following are the general rules for transfer:■The association (connection) remains open until all data is transferred.■The maximum PDU (Protocol Data Unit) size is site configurable. The defaultmaximum is 28672 8-bit bytes.Number of Associations■Each SCU role client application maintains one association at a time.■You can run multiple SCU role client applications, or multiple instances of thesame application, at the same time, with each having an association.Asynchronous NatureJETConnect DICOM does not perform asynchronous operations window negotiation.Table 3: Storage SOP Class SOP Class NameSOP Class UID Role NM Image Storage 1.2.840.10008.5.1.4.1.1.20SCUTable 4: Storage Commitment Model (Push)SOP Class NameSOP Class UID Role N-Action 1.2.840.10008.1.20.2SCUTable 5: Modality Worklist SOP Class NameSOP Class UID Role Modality Worklist InformationModel-FIND 1.2.840.10008.5.1.4.31SCUNetwork Interchange AE Specifications6■DICOM 3.0 Conformance Statement JETConnect 9206-0000, REV. C 09-2004Implementation Identifying Information■The Philips IMPLEMENTATION_CLASS_UID is “1.3.46.670589.28.1.1”.■The implementation version contains the release tag of the ADACJetC software.The initial release contains the implementation version name Atlantis200R03. The implementation version value changes for each release of the ADACJetC software. An example of a potential future implementation version number is Atlantis400R01.Philips uses UID’s with an ANSI-registered <org root> numeric root.Association Initiation Policy■All of the SCU role applications attempts to initiate an association for each inter-action. These include “verification”, “put” and “find”.■You use the default port number, DICOM registered TCP port 104, unless otherwise configured.Associated Real World ActivityThe associated Real-World Activity is the attempt to send a request for:■Echo (C-ECHO request)■Sending image data (C-STORE request)■Getting patient schedule informationSupported SOP Classes9206-0000, REV. C 09-2004DICOM 3.0 Conformance Statement JETConnect■7Proposed Presentation ContextSOP Specific Conformance of SCUThe SCU role of all the SOP classes listed in Tables 1-5 in this document are provided with Standard Conformance.Table 6: Proposed Presentation Contexts for Sending Data/RequestPresentation context (SCU)Abstract Syntax Transfer SyntaxRoleExtended NegotiationSOP Name UID Name list UID listsee Tables 1-5see Tables 1-5DICOM Implicit VR Little Endian 1.2.840.10008.1.2SCUNonesee Tables 1-5see Tables 1-5DICOM Explicit VR Little Endian1.2.840.10008.1.2.1SCU NoneNetwork Interchange AE Specifications8■DICOM 3.0 Conformance Statement JETConnect9206-0000, REV. C 09-2004Table 7: Supported Query Keys/Elements for Worklist MatchingDescriptionTagTypeReturn Value RequestStudy Date 0008, 0020Required Study Time 0008, 0030Required Accession Number 0008, 0050Optional Modality0008, 0060Required Referring Physician 0008, 0090Optional Patient Name 0010, 0010Required Patient ID 0010, 0020Required Patient Birth Date 0010, 0030Optional Patient Sex0010, 0040Optional Secondary Patient ID 0010, 1000Optional Patient Age 0010, 1010Optional Patient Weight 0010, 1030Optional Patient Medical Alerts 0010, 2000Optional Patient Contrast Allergies 0010, 2110Optional Patient Pregnancy Status 0010, 21C0Optional Img Svc Requesting Physician 0032, 1032Optional Req Procedure Description 0032, 1060Optional Scheduled Contrast Agent 0032, 1070Optional Scheduled Station AE Title 0040, 0001Required Procedure Step Start Date 0040, 0002Required Procedure Step Start Time 0040, 0003Required Performing Physician0040, 0006Required Scheduled Proc Step Description 0040, 0007Optional Scheduled Procedure Step ID 0040, 0009Optional Scheduled Station Name 0040, 0010Optional Scheduled Proc Step Location 0040, 0011Optional Scheduled Pre-Medication 0040, 0012Optional Scheduled Pro Step Status 0040, 0020Optional Procedure Step Sequence 0040, 0100Optional Scheduling Comments 0040, 0400Optional Requested Procedure ID 0040, 1001Optional Reason for Requested Procedure 0040, 1002Optional Intended Recipients0040, 1010OptionalCommunication ProfilesSOP-Specific Conformance for SOP Class Storage:The Storage service class converts a JETConnect image into an appropriate DICOMimage format and exports it to a remote DICOM server. While all the importantdiagnostic information is preserved, it is not lossless or reversible.The Nuclear Medicine image is converted into corresponding DICOM NM images. Amulti-detector, energy window and/or rotation image is converted and stored intoseparate DICOM images.Communication ProfilesSupported Protocol StacksThe data transfer uses DICOM Upper Layer Protocol as defined in Part 8 of DICOMstandard, i.e., NEMA Standards Publication No. PS 3.8. Under or parallel to this layer:■TCP/IP stack is supported9206-0000, REV. C09-2004DICOM 3.0 Conformance Statement JETConnect■9Deviation ReportNetwork Media SupportThe DICOM implementation is indifferent to the physical network media. The onlyrequirement, which is completely transparent to you, is that it operates on top of theTCP/IP stack.The default connection port is the Ethernet.You can use other common network media like the following: Token Ring, FDDI,ATM, ISDN, and dedicated T1, T3, and other types of digital or digital/audio lines.These are transparently supported by DICOM but can require additionalhardware/software and expertise.Deviation ReportExtensions, Specialization, PrivatizationsThere are no extensions, specialization or privatizations in this release.Support of Extended Character SetsExtended character sets are not supported in this release. ConfigurationConfiguration files can be found in the following locations:/export/home/atlas/etc/Facility.ADAC01/systems/systems.xml/export/home/atlas/DicomJetConnect/mc3java/config/export/home/atlas/DicomJetConnect/mc3c/mc3apps/export/home/atlas/data/Facilty.ADAC01/WorklistCommentsPhilips Medical Systems’ JETConnect implementation of DICOM - is synchronizedwith the latest DICOM standard development at ACR-NEMA.10■DICOM 3.0 Conformance Statement JETConnect9206-0000, REV. C 09-2004AppendixA GLOSSARYAcronyms and Abbreviations■ACR American College of RadiologyEntity■AE Application■ANSI American National Standards Institute■ATM Async Transfer Mode■DICOM Digital Imaging and Communication in Medicine■DIMSE-C DICOM Message Service Element-Composite■DIMSE-N DICOM Message Service Element-Normalized■FDDI Fiber Distributed Data Interface■IOD Information Object Definition■ISDN Integrated Services Digital Network■ISO International Standards Organization■NEMA National Electrical Manufacturers Association■NM Nuclear Medicine■PACS Archive Communication System■PDU Protocol Data Unit■RIS Radiology Information System■SCP Service Class Provider (server)■SCU Service Class User (client)■T1 A dedicated digital communication link provided by atelephone company that offers 1.544 megabytes/sec ofbandwith, commonly used for carrying traffic to and fromprivate business networks and internet service providers.■T3 A dedicated digital communication link provided by atelephone company that offers 44.75 megabytes/sec ofbandwith, commonly used for carrying traffic to and fromprivate business networks and internet service providers.■TCP/IP Transmission Control Protocol/Internet Protocol■SOP Service Object Pair■UID Unique Identification9206-0000, REV. C09-2004DICOM 3.0 Conformance Statement JETConnect ■ A–1A–2 ■ DICOM 3.0 Conformance Statement JETConnect 9206-0000, REV. C 09-2004。
医疗器械类英语及其缩写
医疗器械类英语及其缩写DC (direct current)直流电DAMPER 阻尼器DGC (degaussing coil)消磁线圈DL (delay line ) 延时线DRIVE 激励、推动DRIVE TRANSF 推动变压器DY (deflection yoke)偏转线圈EHT (extra —high tension)极高压EMERGENCY-急停装置ERROR AMP (error amplifier) 误差电压放大器E—W CORRECTION(east — west correction) 东西向校正FBT (fly back transformer) 逆程变压器FILTER 滤波器FLIP FLOP 双稳态触发器FIYEACK BLANKING 回扫消隐FOCUS 焦点FOCUS VR (focus variable rheostat) 聚焦电位器f。
(fuse) (fuse)保险丝GANTRY-机架G (green)绿色的GND (ground) 接地GREEN CUT OFF 绿枪截止调节GREEN OUT 绿色输出GREY 灰度G - Y MATRIX (G - Y )矩阵H。
BLK (horizontal blanking)行消隐H.DY (horizontal deflection yoke) 行偏转线圈HFC (high frequency choke) 高频扼流圈H.HOLD (horizontal hold) 行同步调节H (L).DRIVE (horizontal driver)行推动放大器HLIN (horizontal linearity)行线性H(L)OUT BOARD 行输出板H 。
M(module)厚膜电路HOR AFC (horizontal automatic frequency control) 行自动频率控制HOR DRIVE TRANS 行激励变压器HORIZONTAL 行(水平)扫描部分HORIZ O/P (horizontal out put ) 行脉冲输出H.OSC(horizontal oscillator) 行振荡器H。
医疗器械类英语及其缩写

医疗器械类英语及其缩写(—) 医疗器械类英语及其缩写(-)急诊室Emergency Room医院Hospital内科病房MedicalWard外科病房SurgicalWard儿科病房PediatricWard接生房Labor andDelivery手术室OperationRoom (OR)心脏重症室CoronaryCare Unit (CCU)重症室IntensiveCare Unit (ICU)内科重症室MedicalIntensive Care Unit (MICU)初生婴儿重症室NeonatalIntensive Care Unit (NICU)儿科重症室PediatricIntensive Care Unit (PICU)外科重症室SurgicalIntensive Care Unit (SICU)末期护理Hospice 末期病患者照料居家健康服务HomeHealth Service 药疗、物理治疗等化验所Laboratory 进行化验研究门诊手术中心OutpatientSurgical Center 一般非严重性手术Health Care Provider 医疗服务Physician 医生Acupuncture 针灸Allergy and Immunology 过敏性专科Anesthesiology 麻醉科Cardiology 心脏科Cardio—Thoracic Surgery 心胸外科Chiropractic 脊椎神经科Colorectal Surgery 结肠直肠外科Dentistry 牙科Dermatology 皮肤科Endocrinology 内分泌科Family Practice 家庭科Gastroenterology 肠胃科General Practice 普通全科General Surgery 普通外科Geriatrics 老人病专科Hematology 血液科Hepatology 肝病专科Infectious Disease 传染病科Internal Medicine 内科Nephrology 肾脏科Neurology 神经科Neurosurgery 神经外科Obstetrics—Gynecology 妇产科Oncology 癌症专科Ophthalmology 眼科Optometry 验光科Orthopedic Surgery 骨外科Osteopathy 整骨疗科Otolaryngology (ENT)耳鼻喉科Pathology 病理科Pediatrics 小儿科Plastic surgery 整形外科Podiatry 足科Psychiatry 精神治疗科Physiatry 物理康复科Physical Medicine and Rehabilitation 物理疗法及恢复正常生活护理Pulmonary Medicine 肺科Radiation Oncology 癌症放射疗科Radiology X光科Urology 泌尿科Vascular Surgery 血管外科Other Health Care Professionals 其它医疗专业人员Audiologist 听觉学专家Dental Assistant 牙医助理Dietitian 饮食指导员Genetic Counselor 遗传病辅导员Health Technician 健康技员Laboratory Technician 化验技员Medical Assistant 医务助理Medical Technologist 医学技师Nurse 护士Home Visiting Nurse 家访护士Nurse Midwife 接生护士Nutritionist 营养专家Pharmacist 药剂师Pharmacologist 药理学专家Physical Therapist 物理治疗员Physicians Assistant 医生助手Psychologist 心理学专家Psychologic Counselor 心理辅导员Respiratory Therapist 呼吸治疗员ABSS 自动(磁带)空白部分扫描ABL(automatic bright limiting)自动亮度限制ABL ON OFF 自动黑电平开/关ABL SW ON 自动黑电平开关接通ABO 自动电子束最佳化ABO ADJ 自动电子束最佳化调整ABO VIDEO 自动电子束最佳化视频ABO VIDEO ADJ 自动电子束最佳化视频调整ABO VIDEO IN 自动电子束最佳化视频输入AC (alternating current) 交流电AC IN 交流输入AC MOTOR 交流电机AC MOTOR SWAC 交流电机开关AC 自动色(饱和度)控制AC mains input 交流电输入ACC AMP ACC放大ACC AMP (REC)ACC放大录制ACC/APC BURST FLAG 自动色度控制/自动相位控制旗脉冲ACC (automatic chrominance control)自动色度控制ACC AMP (automatic chrominance controlamplifier)自动色度控制ACC BF PHASE 自动控制旗脉冲相位ACC LEVEL 自动色度控制电平ACC LEVEL SW 自动色度控制电平开关ACC BURST GATE ACC色同步选通门ACC DC AMP ACC直流放大ACC DET 自动消色放大ACTION 作用ADAPTOR适配器ADC(automatic degaussing circuit)自动消磁电路ADD CIRUIT 相加电路ADD RESSING 寻址ADJ (ADJUSTMENT)调整ADV (一桢一桢)步进AERIAL 天线AFC (automatic frequency control)自动频率控制AFC BALANCN 自动频率控制平衡调节AFC CENTER AFC中心AFC DC 自动频率控制(AFC)直流AFC DC BIAS AFC直流偏置AFC (DC)OUT 自动频率控制(DC)输出AFC DRIVE 自动频率控制推动AFC ERROR 自动频率控制误差信号AFC ERROR BUFFER AFC误差缓冲AFC FH TUNING AFC行频调谐AFC FH TUNING AMP AFC行频调谐放大AFC GAIN AFC增益AFC GATE 自动频率控制门AFC IN 自动频率控制输入AFC OUT AFC输出AFC PULSE AMP 自动频率控制脉冲放大AFC SET 自动频率控制设定AFC VCO AFC压控振荡器AFC VCO FREQ AFC压控振荡器频率AFPC (automatic frequency phase control) 自动频率相位控制AFS(automatic frequency stabilization)自动频率稳定AFTER CLOCK 时钟后AFTER CLOCK PULSE 时钟脉冲之后AGC 自动增益控制AGC AMP AGC放大AGC DETECTOR 自动增益控制检测AGC ERROR BUFFER 自动增益控制误差缓冲器AGC PROT AGC保护AH(AUDIO/CTLHEAD) AH(音频控制磁头) ALARM TONE BURST 告警音频缓冲ALT 行交替ALT PULSE 行交替脉冲ALTERNATEDSC 交替的副载波ALU 运算器AMP(amplifier)放大器AMPLIFIER DETECTOR 放大器/检波器AMPLITUED LIMIER 限幅器ANALOG SWITCH 模拟开关ANODE 阳极ANC 自动消噪电路ANTENNA 天线APC(automatic phase control)自动相位控制APC BF INV APC 旗脉冲倒相APC 自动相位控制(检波)ARC(automatic resolution control)自动清晰度控制AT(Ampere turns)安(培)匝数ATT (ATTENUATOR) 衰减器AUTOMATIC地自动B(blue)蓝色B(brightness)亮度BA(buffer amplifier)缓冲放大器BALANCE平衡BALUN 平衡-不平衡转换器BRIGHT 亮度BRIGHTNESS 亮度调节BLLE OUT OFF蓝枪截止调节BLUE OUT 蓝色输出BURST 色同步信号BURST GATE 色同步选通电路BURST PHASE 色同步信号相位CURRENT LIMITTER 电流限制器CEN 中心CHROMA 色度CHROMA AMP 色度放大器CHROMA BURST AMP 色度、色同步信号放大器CHROMA BOARD 色通道板CHROMA FILTER 色度滤波器CHROMINANCE 色度通道CLAMPER 钳位器CMOS (complementary metal -oxide-semiconductor)互补型金属-氧化物半导体COLOUR CONT(color controller) 彩色控制器COLOUR DIFFERENCE 色差COLOUR SYNC 彩色同步调节COLORKILLER 消色器COLORTONE 色调CONT 对比度、控制CONTRAST 对比度CONTROL 控制CONSOLE—控制柜CPT (color picture tube)彩色显像管CPT BOARD 彩色显像管座板CRT (cathode - ray tube)阴极射线管(显像管)CRT DRIVE BOARD 显像管激励电路板。
一、医学系统缩略语

一医学系统縮略语:CDA clinical document architecture 临床结构化文档CDC change data capture 变化数据捕获CDR clinical data repository 推临床数据仓库CHIS community health information system 社区卫生服务信息系统CIS clinical information system临床信息系统DICOM digital imaging and communications in medicine 数字影像和通讯标准DM data-mart 数据集市DW data warehouse数据仓库EHR electronic heath record电子健康档案EMPI enterprise master patient index 患者主索引EMR electronic medical record电子病历GCP good clinical practice药物临床试验管理HIAL heath information access layer区域信息交换层HIS hospital information system医院信息系统HIT healthcare information technology 医疗卫生信息技术HL7 health level7卫生信息交换标准HRP hospital resource planning system医院资源规划HSB hospital server bus医院服务总线1CD/1ICD 10 international classification of diseases 国际疾病分类编码IHE integrating the healthcare enterprise医疗信息系统集成技术规范/集成医疗环境LIS laboratory information system实验室信息系统NIS nurse information system 护理信息系统CDR operation data repository运营数据仓库ODS operational data store操作数据存储PACS Picture archiving and communication systems医学影像存储与传输系统PHR personal health record 个人健康记录PIVAS pharmacy intravenous admixture services 静脉药物配置中心PIX patient identifier cross referencing integration profile患者标识交叉索引集成规范RDR research data repository 科研数据仓库RHIN regional health information network区域医疗信息网络RIS radiology information system放射信息系统XDS/XDS- 1 cross enterprise document sharing跨机构文共享技术框架。
精选医学专业英语词汇大全
精选医学专业英语词汇大全1. Anatomy (解剖学)- Abdomen: 腹部- Brain: 大脑- Heart: 心脏- Kidney: 肾脏- Liver: 肝脏- Lungs: 肺- Stomach: 胃- Spine: 脊柱2. Physiology (生理学)- Blood pressure: 血压- Digestion: 消化- Respiration: 呼吸- Circulation: 循环- Metabolism: 新陈代谢- Hormones: 激素- Nervous system: 神经系统- Immune system: 免疫系统3. Diseases and Conditions (疾病与病况) - Diabetes: 糖尿病- Cancer: 癌症- Asthma: 哮喘- Hypertension: 高血压- Arthritis: 关节炎- Depression: 抑郁症- Obesity: 肥胖症- Pneumonia: 肺炎4. Medical Procedures (医疗程序)- Surgery: 手术- X-ray: X射线- MRI (Magnetic Resonance Imaging): 磁共振成像- Blood test: 血液检查- Vaccination: 疫苗接种- Dialysis: 透析- Chemotherapy: 化疗5. Medical Specialties (医学专科) - Cardiology: 心脏病学- Dermatology: 皮肤科- Gastroenterology: 胃肠病学- Neurology: 神经学- Psychiatry: 精神病学- Obstetrics and Gynecology: 妇产科- Orthopedics: 骨科- Pediatrics: 儿科6. Medical Instruments (医疗器械) - Stethoscope: 听诊器- Thermometer: 温度计- Sphygmomanometer: 血压计- Scalpel: 解剖刀- Syringe: 注射器- Electrocardiograph: 心电图仪- Ultrasound machine: 超声波机- Endoscope: 内窥镜以上是一份精选医学专业英语词汇大全,涵盖了解剖学、生理学、疾病与病况、医疗程序、医学专科和医疗器械等方面的词汇。
介入耗材相关资料品牌推荐
美国Medtronic Inc 德国 BIOTRONIK SE & Co. KG
第十六大类:消化内窥镜耗材
序 号 品种目录
进口品牌
1
斑马导丝
美国 Cook Incorporated Boston Scientific Corporation
2
肠镜胶
Optimum Medical Solutions
3
美国Medtronic Inc 美国 Medtronic Inc.
动脉覆膜支架 36
动脉覆膜支架
美国Medtronic Inc 美国 Cook Incorporated
37
球囊压力注射器
Boston Scientific Corporation
血管缝合器 38
血管缝合器
Synovis Micro Companies Alliance, Inc 美国 Abbott Laboratories Abbott Vascular Inc.
下腔静脉滤器 10
下腔静脉滤器
爱尔兰 Cordis Cashel 美国Bard Peripheral Vascular,Inc
PTC针 11
PTC针
美国Argon Medical Devices, Inc 意大利GALLINI S.R.L.
引流套管 12
引流套管
丹麦PBN Medicals Denmark A/S 美国 Cook Incorporated
三联三通板 20
三联三通板
美国 Smiths Medical ASD,Inc 美国 B.Braun Medical Inc.
弹簧圈 21
弹簧圈
美国 Cook Incorporated 美国库克公司 Cook Incorporated
MRS原理

肌醇(mI) • 位于3.56 ppm,只在短TE时显示 • 胶质细胞的标记物,位于星形细胞中 • 最重要的渗透压或细胞容积调节剂 • 有研究认为,在低级星形细胞瘤中,mI含量多较高
Castillo, et al. Am J Nuroradiol, 2000;21:1645-1649
g MRS临床应用
g MRS临床应用
胆碱(Cho) • 位于3. 20 ppm附近;
GE GE Medical Medical Systems Systems Training Training in in Partnership Partnership
• 磷脂代谢的成分,细胞膜转换的标记物,反应细胞增
殖
• 评价脑肿瘤的重要共振峰之一
ω= γB ω= γ(1- σ)B
GE Medical Systems Training in Partnership
• 质子进动频率取决于外加磁场强度(B)和原子核的旋磁比(γ) (Larmor Equation) • 由于质子周围电子的磁屏蔽作用,Larmor Equation应修正为: • 处于不同化合物中的同一种原子核,由于所受磁屏蔽作用的程度不同 (即σ不同),具有不同的共振频率,这就是所谓的化学位移现象
GE Medical Systems Training in Partnership
确定MRS扫描的感兴趣区,保证局部磁场的绝对均匀 被检查病变的大小
g 水抑制的重要性
GE GE Medical Medical Systems Systems Training Training in in Partnership Partnership
– 评价病灶的范围 – 可以获得对侧或未被病变累及区域的波谱,从而提供 某一已知代谢物的图形
综合医院建筑设计.ppt何瑞清
医疗管 理
病案、 统计
住院管 理
门诊管 理
感染控 制
基地选择
综合医院选址,应符合当地城镇规划、区域卫生规划和环 保评估的要求。
① 应符合规划和医疗卫生网点布局要求,最好设于服务范围的中 心。
② 交通便利,宜两侧面临道路(不宜临主干道)。 ③ 环境安静,远离污染源、危险区,不要临近少年儿童活动密集场
总平面设计
总平面设计应符合下列要求: ① 功能分区明确;洁污、内外、隔离与非隔离流线清楚, 避免或减少交叉感染。 ② 医疗用房安排卫生条件好的地段;病房楼应有最佳朝 向,住院部、手术室等房间环境安静。 ③ 交通组织便捷安全;出入口不少于二处,废弃物出入 口单设。门诊部、急诊部入口附近应设停车场。 ④注意传染病区、太平间、病理解剖室、焚毁炉的设置位 置。 ⑤职工住宅不得建在医院基地内。 ⑥充分利用环境布置庭院绿化和康复活动场地等设施。 ⑦应留有改、扩建余地。
住院部由出入院、住院病房及各科病房组成。病房有普内 科、普外科、儿科、妇科、产科、神经内科、神经外科、 泌尿科、皮肤科、消化科、肿瘤科、眼科、五官科、心血 管科等,还有传染科、整形外科病房,供需要住院治疗的 病人在此卧床诊断和治疗。此外,还有针对特殊人群或病 程设置的病房,如康复病房,以接待高级干部、外宾为主 的特优病房等。
急救中心的规划布点——应考虑交通方便,位置适中,起城市服 务半径(国内学者)认为4~6km较为理想,郊野以15分钟内救护 车或直升机能到达为原则。日本东京急救反应时间平均为4分40秒, 大阪为5分30秒,法国巴黎15分钟,北京急救中心16分钟。(国际 上用以衡量急救水平的重要标志)
急诊部分析
急诊部组成 诊查用房:包括急诊、
后勤部或称医疗辅助部门,如中心供应、营养厨房、中心 仓库、洗衣房、蒸汽站、中心供氧站、中心吸引、医疗器 械秀丽,汽车库、动物房、太平间、污水处理站、编配电 站、空调机房及其他设备用房等。有一些医院则将中心供
医疗英语词汇

医疗英语词汇医疗英语词汇医疗英语词汇内科系统medicine systems 外科系统surgery systems医技科室medical laboratory血液病科hematology department普外(肝胆)general surgery临床检验clinical laboratory输血科blood bank内分泌科endocrinology department胸外科thoracic surgery病理科pathology deparment脑电图室ecg laboratory消化内科digestive system department心外科cardial surgery传统放射科traditional radiology department肺功能室lung function laboratory心血管内科vasculocardiology deparment泌尿外科urology surgerymr室mr laboratory胃镜室dndoscope laboratory神经内科neurology department肿瘤外科oncological surgerysct室sct laboratory人工肾室hemodialyses room介入科invasive technology department神经外科neurological surgery超声诊断科uitrasonic diagnosis deparment dsa室dsa room呼吸科pneumology department骨科orthopedics department超声多谱勒室uitrasonic doppler laboratory血液净化室laminar airflow (laf) room肾内科urology department小儿外科pediatric surgery核医学科isotopic laboratory高压氧仓室hyperbaric chamber小儿科pediatrics department整形科plastic surgeryect 室ect laboratory院内感染监控室nosocomial infection monitory 中医科traditional chinese medicine department 烧伤科department of burn供应室supply house血液成份分离室cytopheresis laboratory高干病房senior officials inpatient ward妇产科obstetric and gynecologic department营养室nutrition house体外反搏室counter extropulsative room华侨病房overseas chinese ward口腔科stomatological department康复科rehabilitation department保健科medical care department for personnel眼科ophthalmologic department针灸科acupuncture and moxibustion de-parment耳鼻喉科otorhinolaryngologic department理疗科physiotherapy deparment痔疮科hemorrhoids deparment按摩科massage department皮肤科dermatology department麻醉科anesthesia department省级重点学科key subjects at the provincial level血液病、内分泌疾病、肝胆外科、胸心外科hematology, endocrinology, genneral surgery and cardio-thoracic surgery 省级医疗领先特色专业the leading subjects of medicine atthe provincial level心内科、烧伤科、儿科心理学cardiology, department of b urn , pediatric psychology医院特色专科characteristic professional subjects of union hospital消化内科、普外、肿瘤、泌尿、神经、整形、耳鼻喉科、介入、影像digestive system diseases, generalsurgery, oncology, urology, neurology, plastic surgery,otorhinolary, invasive department and medical imagery医疗英语词汇相关内容:。
FFR-动脉生理检测仪中文说明书
生理学鉴定界面动脉生理检测仪使用说明书产品名称:动脉生理检测仪(商品名:RadiAnalyzer Xpress)规格型号:12711生产商:Radi Medical Systems AB地址:Palmbladsgatan 10, SE-754 50 Uppsala, Sweden电话:+46 (0) 18 16 10 00注册证号:国食药监械(进)字2008第3213570号(更)产品标准号:YZB/SWE 4995-2008售后服务机构:圣犹达医疗用品(上海)有限公司售后服务机构地址:上海市外高桥保税区富特西一路439号01号楼1层邮编:200130电话:(86)21-2306-7588传真:(86)21-6422-4838RadiAnalyzer XpressRoHS有毒有害物质或元素部件名称铅(Pb) 汞(Hg)镉(Cd)六价铬(Cr(VI))多溴联苯(PBB)多溴二苯醚(PBDE)主板X O O O O OPC-104X O O O O O绝缘材料,红色O O X O O O PIN针O O X O O O PIN针O(X)O O O O内部线缆红色X O O(X; Cr) O O内部线缆红色O O O O(X; Br) (X; Br) 塑料部件O O O O(X; Br) (X; Br) 螺钉O O-(X;Cr)O OO:表示该有毒有害物质在该部件所有均质材料中的含量均在SJ/T11363-2006 标准规定的限量要求以下。
Pb,Hg,Cr(VI),PBB,PBDE的浓度极限:1000ppmCd的浓度极限:100ppmX:表示该有毒有害物质至少在该部件的某一均质材料中的含量超出SJ/T11363-2006 标准规定的限量要求。
(X):表示被提及的元素在定期系统中的含量符号说明有毒有害物质依据RoHS含量额外的产品标签内容1.产品的描述1.1使用者的适应症 (6)1.2禁忌症 (6)1.3警告和警惕 (6)1.4清洗和维护 (8)1.5RADIAnalyzer® Xpress的界面 (9)1.6使用者的绘图界面 (11)2.遵从法规要求2.1遵从的标准和导则 (18)2.2仪器外表上的标志 (20)3.RADIAnalyzer® Xpress的安装3.1安装设备 (22)3.2连接到电源 (23)3.3连接到实验室监测系统 (23)3.4连接到打印机RADIView TM..(选配) (23)3.5连接到RADIView TM(选配) (24)4.开始一个程序4.1打开系统 (26)4.2使RADIAnalyzer® Xpress和心脏介入检查室监测系统平衡 (26)4.3校准AO (27)4.4校准PressureWire® 传感器 (27)4.5输入病人的ID号 (28)4.6自动的开始顺序 (29)4.6.1平衡RADIAnalyzer® Xpress和心脏介入检查室监测系统 (29)4.6.2校准AO (29)4.6.3校准PressureWire® 传感器 (30)5.分次的流量测量5.1验证合适的压力信号 (32)5.2使Pa和Pd的压力均衡 (32)5.3使远端的位置传感器狭窄 (32)5.4诱导最大极限的充血 (32)5.5压力记录 (33)5.6停止记录并显示FFR (33)5.7使用指标器来确认FFR的价值 (33)5.8返回测量模式 (34)5.9断开PressureWire® 传感器 (34)6.测量传感器顶端的温度(选配)要求RADIAnalyzer® Xpress安装Thermo Option (34)7.测量冠状动脉血流储备,CFR(选配)要求RADIAnalyzer® Xpress安装Thermo Option (34)8.记录库8.1查看储存的记录 (36)8.2转移记录到RADView TM(选配) (36)8.3打印记录(选配) (36)8.4删除储存的记录 (36)9.仪器的设定9.1平均的压力计算结果 (38)9.2曲线图的扫描速度 (38)9.3曲线图的刻度 (39)9.4系统定时间 (39)9.5系统定日期 (39)9.6样本模式 (40)9.7Pd/Pa的曲线趋势 (40)9.8自动的开始顺序 (41)9.9监视器输出的敏感性 (41)10.维护10.1一年一次的检修 (43)10.2遥控装置电池 (43)10.3系统的备用电池 (43)10.4清洗 (43)10.5其他的维修/修理 (43)10.6一次性用品 (43)11.故障排除11.1屏幕信息 (44)12.规格12.1 技术规格 (45)担保声明:Radi Medical Systems AB拒绝所有的担保,不论操作者或者其他人明确的或者是含蓄的保证,包括但是不局限于对有销路的或者是适当的任何含蓄的担保。
Philips Medical Systems SpO2 监测 了解脉搏血氧仪 SpO2 概念说明书
Philips Medical Systems SpO2 Monitoring Understanding Pulse Oximetry SpO2 ConceptsContents1Introduction1What is SpO2?How Does Pulse Oximetry Work?SpO2 SensorsAbsorption at the Sensor SiteOxyhemoglobin Dissociation Curve5How Do I Use SpO2?Choosing a Sensor7Using SpO28Considerations When Using Pulse Oximetry8Effects of Non-functional Hemoglobin on Oxygen SaturationMeasurementsOther SituationsCommon Problems with Pulse Oximetry13GlossaryIntroductionThe body's need for oxygen is certain. Its availability at a tissue level is some-times in doubt. Blood gas measurements provide critical information regard-ing oxygenation, ventilation, and acid-base status.However, these measurements only provide a snapshot of the patient's condi-tion taken at the time that the blood sample was drawn. It is well known that oxygenation can change very quickly. In the absence of continuous oxygen-ation monitoring, these changes may go undetected until it is too late. Pulse oximeters measure blood oxygen saturation noninvasively and continu-ously.What is SpO2?A blood-oxygen saturation reading indicates the percentage of hemoglobin molecules in the arterial blood which are saturated with oxygen. The reading may be referred to as SaO2. Readings vary from 0 to 100%. Normal readings in a healthy adult, however, range from 94% to 100%.The term SpO2 means the SaO2 measurement determined by pulse oximetry. As explained in the section "Considerations When Using Pulse Oximetry," under some circumstances pulse oximetry gives different readings, and the use of a different term indicates this.1SpO2 Concepts2How Does Pulse Oximetry Work?Within the Sp02 sensor, light emitting diodes shine red and infrared light through the tissue. Most sensors work on extremities such as a finger, toe or ear. The blood, tissue and bone at the application site absorb much of the light. However, some light passes through the extremity. A light-sensitive detector opposite the light source receives it.Figure 1: SpO 2 SensorSpO2 SensorsMost sensors work on extremities such as a finger, toe or ear. The sensor mea-sures the amount of red and infrared light received by the detector and calcu-lates the amount absorbed. Much of it is absorbed by tissue, bone and venous blood, but these amounts do not change dramatically over short periods of time.The amount of arterial blood does change over short periods of time due to pulsation (although there is some constant level of arterial blood). Because the arterial blood is usually the only light absorbing component which is changing over short periods of time, it can be isolated from the other compo-nents.Red and Infrared Diodes3Absorption at the Sensor SiteThe amount of light received by the detector indicates the amount of oxygen bound to the hemoglobin in the blood. Oxygenated hemoglobin (oxyhemo-globin or HbO 2) absorbs more infrared light than red light. Deoxygenated hemoglobin (Hb) absorbs more red light than infrared light. By comparing the amounts of red and infrared light received, the instrument can calculate the SpO 2 reading.Figure 2: AbsorptionOxyhemoglobin Dissociation CurveYou may have used oxygen partial pressure (PaO 2) to judge oxygen saturation. SpO 2 is related to PaO 2 in a complex way, as shown in Figure 3, the Oxyhe-moglobin Dissociation Curve.At very high SpO 2 levels, PaO 2 values can vary widely without producing a significant change in SpO 2 levels. Because of this, SpO 2 readings cannot be used to warn of high PaO 2 levels.Many variables can affect hemoglobin’s affinity for oxygen, and thus the posi-tion of the curve. Decreasing concentrations of hydrogen ions, PaCO 2 and 2,3DPG, increase hemoglobin’s affinity for oxygen and shift the curve to the left. Absorption due to:Timetissue and bonevenous bloodpulse-added volume ofarterial blood arterial bloodSpO2 Concepts4An increase in the variables shifts the curve to the right. Fetal hemoglobin, which binds more readily with oxygen than adult hemoglobin, also affects the curve, as does temperature.The relationship between SpO2 and PaO2 is not simple, so judging one mea-surement from the other should only be attempted with caution.Figure 3: Oxyhemoglobin Dissociation Curve0 Partial Pressure of Oxygen (mmHG) 100%OxygenSaturation Decreased Affinityof Hemoglobin for OxygenIncreased Affinityof Hemoglobinfor Oxygen100%5How Do I Use SpO 2?Using pulse oximetry is fairly simple. Many questions may be answered by referring to your instrument’s Instructions for Use .Choosing a SensorThere are some general guidelines to choosing the right sensor. The ideal application site has good perfusion, does not generate movement artifact, is comfortable for the patient and allows easy application.The size of the application site determines what size sensor to use. The age of the patient is not a factor.If a sensor is too big or too small, the light emitting diode and the light detec-tor may not line up. This could cause a false reading or an alarm.If a finger sensor is too large, it may slip partway off so that the light source partly covers the finger. This condition, called optical bypass, causes incorrect readings.Figure 4:Pediatric Finger SensorIf a finger is inserted too far into the sensor it may be squeezed by the sensor, which causes venous pulsation. The pulse oximeter recognizes arterial blood only by its pulsing motion, so in this case it also measures venous blood. This causes readings which are falsely low.SpO2 Concepts6Since motion between the sensor and the application site may cause move-ment artifacts, adhesive sensors may be better than non-adhesive sensors. Neonates tend to have movement artifact in their fingers, so choose a toe or foot sensor.Figure 5: Neonate Foot SensorDo not apply the sensor too tightly in an attempt to reduce movement arti-facts. Not only does this not reduce movement artifacts, it may lead to venous pulsation and necrosis.Check all sensors regularly and move them if necessary. Refer to the sensor documentation for recommended times for checking and replacing the sen-sor. If the patient’s skin cannot breathe or is subjected to sustained pressure, he or she may suffer from skin necrosis, particularly if the patient has poor microcirculation.The preferred application site for newborns immediately after birth is the right hand. SpO2 values on the right hand (pre-ductal) are more representa-tive for brain oxygenation.Pre and post-ductal SpO2 in preterm neonates with hyaline membrane disease or persistent ductus arteriosus (PPHN/PDA) may differ as high as 25%. It is important to place the sensor at the site relevant to the ductus arteriosus (right hand = pre-ductal; left hand, feet = post-ductal).Using SpO2Because pulse oximetry provides continuous monitoring and is noninvasive, it may be useful in several clinical situations.Surgery and Post Anesthetic Care UnitsSince pulse oximetry provides a means of continuously assessing of the oxy-genation of the patient, many require it. If ventilation fails, an alarm sounds. Additionally, SpO2 is noninvasive so it is safer and more pleasant for the patient than invasive methods of oxygen analysis.Neonatal Care and NICUBlood-oxygen saturation levels taken immediately after birth, preferably on the right hand, (within five minutes) are a good guide to the neonate's general state of health. Levels below 75% may indicate abnormalities. T ogether with Apgar scores, blood-oxygen saturation readings are very useful. Both too little or too much oxygen is dangerous for the neonate, particularly for the prema-ture neonate.Oxygen partial pressure (PaO2) is most critical for the neonate. Although blood-oxygen saturation and PaO2 are related, there are too many other fac-tors involved to convert easily between the two measurements. Refer to the “Oxyhemoglobin Dissociation Curve” on page3 for more details. Emergency CareIn emergent care situations, both in and out of the hospital, patients may need ECG monitoring, SpO2 monitoring, pacing and defibrillation at a moment's notice.Noninvasive Transcutaneous PacingPulse oximetry, as integrated into Philips’ defibrillator/monitors, provides a tool to help determine whether pacing is effective.You can use the SpO2 measurements in addition to the patient's ECG signal as shown on the monitor to verify that mechanical capture has been achieved.SpO2 ConceptsWhen the patient is being successfully paced, the pulse rate derived from thepulse oximeter, the ECG heart rate derived from the ECG monitor and thepacing rate should all be about the same. In addition, there should be signs ofimproved cardiac output.Recorded strips provide a printed record of SpO2 measurements and SpO2alarm violations during pacing.Considerations When Using Pulse OximetryBlood oxygen saturation is a measure of the amount of oxygen carried byhemoglobin in the blood stream. It is usually expressed as a percentage ratherthan an absolute reading. Pulse oximeters define this percentage in a differentway than other instruments. These subtle, but important differences, aredescribed in the following section.Effects of Non-functional Hemoglobin onOxygen Saturation MeasurementsIn order to judge a patient’s condition, ideally you would like to have bloodoxygen saturation expressed as a percentage of the total hemoglobin that issaturated with oxygen. Under many circumstances, that is the reading you getfrom pulse oximeters. However, if the patient has a large amount of non-functional hemoglobin, the reading is not accurate. Non-functional hemo-globin is defined as hemoglobin which is incapable of carrying oxygen, butdoes include carboxyhemoglobin (HbCO) and methemoglobin (METHb).Functional hemoglobin is defined as hemoglobin capable of carrying oxygen.It includes oxygenated hemoglobin (HbO2) and deoxygenated hemoglobin(Hb).In other words, the ideal blood saturation measurement is:100HbO2Hb HbO2HbCO METHb other non-functioning hemoglobins ++++------------------------------------------------------------------------------------------------------------------------------------------------------------------------------¥where Hb is hemoglobin, HbO 2 is oxygenated hemoglobin, HbCO is carbox-yhemoglobin, and METHb is methemoglobin. This is also referred to as frac-tional saturation.Pulse oximeters usually assume there are no non-functioning hemoglobins in the arterial blood and measure the blood oxygen saturation as:When the amount of non-functioning hemoglobin (represented above by HbCO + METHHb + other non-functioning hemoglobins) is very small, both readings are nearly the same.When the patient has large amounts of non-functioning hemoglobin, these measurements vary widely. Several situations can lead to such large amounts of non-functioning hemoglobin. Carbon monoxide poisoning and even heavy smoking increase the amount of carboxyhemoglobin, a non-functioning hemoglobin.Other SituationsPulse oximetry is a very useful technology, but there are situations where you must be careful in applying it. Keep the following in mind when you use a pulse oximeter.AnemiaDamage to red blood cells may cause anemia, a lack of red blood cells and thus hemoglobin in the blood. An anemic patient may not have enough function-ing hemoglobin in the blood to oxygenate the tissues. The small amount of functioning hemoglobin in the blood may be well saturated with oxygen, so the patient may have a normal SpO 2 reading, but the patient may not have enough oxygen going to the tissues.100HbO 2Hb HbO 2+-----------------------------¥SpO2 ConceptsDyesSome surgical procedures, especially in cardiology and urology, call for theinjection of dyes into the blood in order to trace blood flow.These dyes affect light transmission through the blood. They directly influ-ence the pulse oximeter and lead to wrong readings.If the patient’s blood contains any of the following dyes, you cannot use pulseoximetry to measure oxygenation:• Methylene blue• Indiocyanine green• IndiocarmineBilirubin, a breakdown product from red blood cells, does not affect readingsfrom pulse oximeters.PerfusionSpO2 is always measured at one of the body’s peripheral sites: a finger, toe orear. The site chosen for the SpO2 measurement must be adequately perfusedwith blood.ShockThe body reduces blood supply to the limbs and extremities as a response toinjury, or even the fear of injury, to maintain the blood supply to vital organseven in the event of severe blood loss. Because of this reduced perfusion,pulse oximeters may give misleading readings on patients in severe shock.HypothermiaThe body reduces the heat lost by the skin by constricting the peripheralblood vessels.Cold is a common problem, often seen with car accident victims and patientsundergoing brain or open heart surgery during which body temperature islowered. Cold also causes shivering, which can lead to movement artifacts.MedicationMany kinds of medication, nerve blockers in particular, can lead to the con-striction of peripheral blood vessels.Common Problems with Pulse OximetryAlthough a pulse oximeter is easy to use, there are common problems associ-ated with the use of oximeters.Light InterferenceSometimes external light sources may cause inaccurate readings. If you suspect that a light may be causing interference, try covering the site with an opaque material and see if the reading changes. If so, keep the site covered. Movement ArtifactsMovement artifacts, such as shivering, have been overcome with the latest SpO2 algorithms, such as Philips FAST-SpO2. However, unusually strong movement may cause movement artifact in the pulse. Apply the sensor to a less susceptible site if possible.Sensor applicationThe sensor should fit the application site snugly. If it is too tight, it might cause venous pulsation. If it is too loose, the light issuing from the emitters may not pass completely through the site and may cause erroneous readings. If adhesive sensors are not the right size, the emitter and detector may not line up correctly. Make sure you use the correct sensor for the patient to get the most accurate reading.Inadequate Blood FlowBlood pressure cuffs, tight clothing or restraints may interfere with blood flow. Use another application site or loosen clothing.SpO2 ConceptsNail PolishSome nail polish and false fingernails may cause false readings. If possible,switch to an unpolished nail, or consider another application site.GlossaryBlood-oxygen SaturationThe amount of oxygen bound to hemoglobin in the blood, expressed as a percentage. Functioning HemoglobinHemoglobin which is capable of carrying oxygen. Functioning hemoglobin includes oxygenated hemoglobin (HbO2) and deoxygenated hemoglobin (Hb).Movement ArtifactsMotion of the blood caused by patient motion instead of pulsation.Non-functioning HemoglobinHemoglobin which is not capable of carrying oxygen. Non-functioning hemoglobin includes carboxyhemoglobin (HbCO) and methemoglobin (METHb).Pulse OximetryThe technique of measuring oxyhemoglobin saturation by shining red and infrared light through a peripheral site, such as a finger, toe, or nose.SaO2A measurement of oxygen saturation in arterial blood.SpO2Oxygen saturation in arterial blood as measured by a pulse oximeter. SaO2 and SpO2 readings differ because pulse oximetry measures the oxygen saturation of only func-tional hemoglobin. SaO2 readings indicate the saturation of both functional and non-functional hemoglobin.SpO2 ConceptsSpO2 ConceptsPhilips Medical Systems is partof Royal Philips ElectronicsInterested?Would you like to know more about our imaginative products? Please do not hesitate to contact us. We would be happy to provide specific information about our products and services, or put you on our mailing list for news about new product developments, upcoming events or for our clinical journal, Medicamundi. We would be glad to hear from you.On the webVia e-mail*******************By postal servicePlease write to us at the following address:Philips Medical SystemsGlobal Information CenterI.B.R.S./C.C.R.I. Numéro 110885600 VC EindhovenPays-Bas/The Netherlands(no stamp required)CORPORATE HEADQUARTERS Philips Medical SystemsNederland B.V.Postbus 10.0005680 DA BestNetherlandsUNITED STATESPhilips Medical Systems3000 Minuteman RoadAndover, MA 01810(800) 225-0230CANADAPhilips Medical Systems281 Hillmount RoadMarkham, Ontario L6C 2S3(800) 291-6743EUROPE, MIDDLE EAST AND AFRICA Philips Medizinsysteme Böblingen GmbH Cardiac and Monitoring Systems Hewlett-Packard Str. 271034 BöblingenGermanyFax:(+49) 7031 463 1552LATIN AMERICAPhilips Medical Systems1550 Sawgrass Corporate Parkway#300Sunrise, FL 33323(954) 835-2600ASIA PACIFICPhilips Medical SystemsAsia Pacific Regional Centre30/F Hopewell Centre17 Kennedy RoadWanchai, Hong Kong(+852) 2821-5888© 2002 Philips Electronics North America Corporation. All rights are reserved. Reproduction in whole or in part is prohibited without the prior written consent fo teh copyright holder.Printed in United StatesJanuary 1, 20035990-0684EN。
医疗体制英语作文

医疗体制英语作文The Medical System。
The medical system is a crucial part of any society, as it is responsible for providing healthcare services to the population. A well-functioning medical system is essential for maintaining the health and well-being of the people, as well as for promoting economic and social development. In this essay, we will discuss the importance of the medical system, its key components, and the challenges it faces.First and foremost, the medical system plays a vital role in maintaining the health of the population. It provides a wide range of healthcare services, including preventive care, treatment of illnesses and injuries, and rehabilitation. These services are essential for preventing diseases and promoting a healthy lifestyle, as well as for treating and managing various health conditions. Without a well-functioning medical system, the population would be at risk of suffering from poor health and reduced lifeexpectancy.In addition to maintaining the health of the population, the medical system also contributes to economic and social development. A healthy population is more productive andcan actively participate in the workforce, which in turn contributes to economic growth. Furthermore, a well-functioning medical system reduces the burden of disease on the society, leading to lower healthcare costs andincreased productivity. Moreover, access to quality healthcare services is a fundamental human right, and awell-functioning medical system can contribute to social equity and justice.The medical system is composed of various key components, including healthcare facilities, healthcare professionals, medical equipment and technology, and healthcare financing and administration. Healthcare facilities, such as hospitals, clinics, and nursing homes, are essential for providing healthcare services to the population. Healthcare professionals, including doctors, nurses, and other healthcare workers, are responsible fordelivering care and treatment to patients. Medical equipment and technology, such as diagnostic tools and treatment devices, are essential for diagnosing andtreating health conditions. Finally, healthcare financing and administration are crucial for funding and managing the medical system.Despite its importance, the medical system faces several challenges that need to be addressed. One of the main challenges is the increasing cost of healthcare, which puts a strain on healthcare financing and administration. This is due to various factors, including the rising cost of medical technology, the aging population, and the increasing prevalence of chronic diseases. Another challenge is the shortage of healthcare professionals, especially in rural and underserved areas. This shortage is exacerbated by the increasing demand for healthcare services and the aging workforce. Additionally, the medical system also faces challenges related to access to healthcare services, quality of care, and patient safety.In conclusion, the medical system is a crucial part ofany society, as it is responsible for providing healthcare services to the population. A well-functioning medical system is essential for maintaining the health and well-being of the people, as well as for promoting economic and social development. However, the medical system faces several challenges that need to be addressed in order to ensure that it can continue to fulfill its important role. By addressing these challenges, we can build a stronger and more resilient medical system that can meet the healthcare needs of the population.。
VARISEED放射性粒子植入治疗计划系统-VarianMedicalSystems
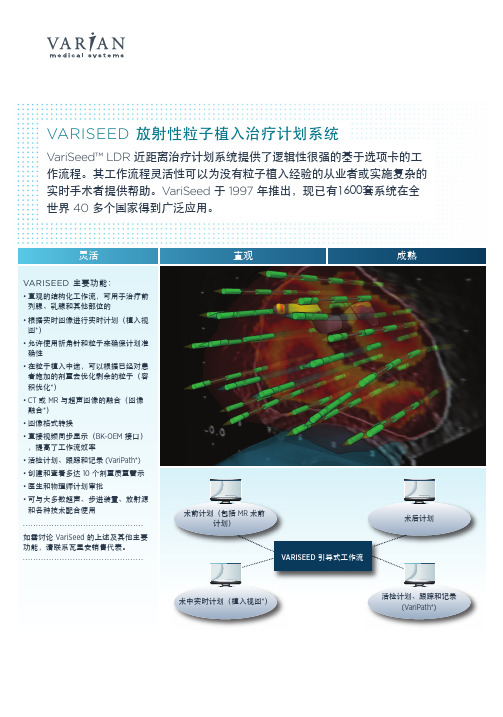
一步的支持 • 提供的源数据经过相关的 QA 检查 • 使用 TG43 剂量计算体系,并支持各向异性常数、系数和
函数计算
通过两次单击保存或返回情景设置
VariPath™ 活检模块* VariPath 活检模块支持经会阴以模板为基础的活检, 以便实时计划活检位置并进行跟踪。计划的针芯可以 移动,与活检针一起倾斜,并标记为已采样。
.............................................. 如需讨论 VariSeed 的上述及其他主要 功能,请联系瓦里安销售代表。 ..............................................
直观
成熟
术前计划(包括 MR 术前 计划)
详细的活检报告列出了已采样的针芯,每个异常针芯 记为针芯的百分比或扇区。根据异常针芯的严重性和 位置创建肿瘤体积。异常针芯位置和/或肿瘤体积可与 图像和任何其他结构一起导出,如 DICOM RT 组织结 构。然后可将这些资料导入其他兼容系统,以便进行 记录或计划设计。
可选配的模块
Twister 三维图像 采集
。提供新的情景设置,可存储视图设置,并可通过两次单 击从一个视图设置切换到另一个。 • 显示光标处的剂量
• 剂量体积直方图 (DVH) 和连续容积分析 (CVA),可用于确 定剂量覆盖范围和均匀性
• 病例总结报告 – 打印或导出可配置的剂量质量参数 • 通过打开 VariSeed 多实例选项并排查看两个计划
像和组织结构 − DICOM RT 导出图像、组织结构、放射源和剂量信息 • 与 BK 的接口免除了 VariSeed 内的超声图像校准,改进了 工作流和图像质量。无需干预便可传输在超声图像上勾绘 的轮廓并自动补偿图像缩放带来的分辨率变化。 • 基于模板的角度或超声波的角度重新生成 CT 或 MR 图像 ,以便创建术前计划
GE CT操作
定位扫描3
z Scan type 扫描类型 z Start Loc 开始位置 z End Loc 结束位置 z Scout Plane 定位平面 z Azimuth 角度(0,90,180,270)
GE Medical Systems
轴扫/螺旋扫描设定1
Image Area
GE Medical Systems
操作程序3
Exam Pg/Series Pg检查资料系列资料 Hide/Show graphics隐去/显示图形 Erase 删除注释和光标 Screen Save 屏幕保存 Back 退出
GE Medical Systems
测量1
z Measurements
轴扫/螺旋扫描设定7
Add Group 追加扫描组合 Spilt Current group分割当前组合 Delete Selected group 删除当前组合
GE Medical Systems
轴扫/螺旋扫描设定8
Biopsy Rx 活体检查扫描 Smart Prep选择最佳扫描时机 Preview 预览
GE Medical Systems
设定管理
z 设定管理包括两个功能,一是自 动声音录制,二是扫描设定管理.
Auto voice record 设 定自动声音 ProtocolManagement 设定扫描参数
GE Medical Systems
管理设定1
z 单击[Protocol Management] 进入下一屏幕
轴扫/螺旋扫描设定4
Recon 重建参数
DFOV:显示视野(96-430mm) A/P Center:前/后重建中心 Image Filters:图象滤波器 Motion Correct:体动补偿修正
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
50
2004
120
2003
65
2002
南部 北部 西部 东部
50
2001
0
20
40
60
80
100
120
140
3 Sept. 2008 NEUSOFT SECRET
Column chart
130
2005
50
2004
120
2003
65
2002
南部 北部 西部 东部
50
2001
0
20
40
60
80
3 Sept. 2008 NEUSOFT SECRET
Chart
Text here Text here Text here Text here Text here Text here TextSkills Shared values Staff
Column chart
400 350 300 250
130 120
200 150
60
65 50
46.9 45.9
45 34.6
南部 北部 西部 东部
45
50
43.9
100 50 30.6 20.4 0 2001
38.6 27.4 2002
90
120 31.6 20.4 2004 2005
2003
Department Name Name
Department Name Name
Department Name Name
Department Name Name
Department Name Name
Department Name Name
Department Name Name
Department Name Name
Label 2
Label 3
Label 4
Label 5
3 Sept. 2008 NEUSOFT SECRET
Chart
Series Label 1 Label 2
20 45
Series
90
Series
50
100%= 000 000
80
40
Label 3
30
70
30
000
Label 4
40
60
20
80
40
3 Sept. 2008 NEUSOFT SECRET
Column chart
140 50 45 120 40 100 35 30 25 60 20 15 10 20 5 0 2001 2002 2003 2004 2005 0 东部 北部 南部 西部
80
40
3 Sept. 2008 NEUSOFT SECRET
000
Label 5
50
50
10
000
3 Sept. 2008 NEUSOFT SECRET
Chart
Group/Department Name
Department Name Name
Department Name Name
Department Name Name
Department Name Name
Department Name Name
Department Name Name
Department Name Name
Department Name Name
Department Name Name
Department Name Name
3 Sept. 2008 NEUSOFT SECRET
Chart
3 Sept. 2008 NEUSOFT SECRET
Column chart
450 400 350 300 250
130 120
200 150
65 50 50
东部 南部 北部 西部 东部
100 50 0 2001
2002
2003
2004
2005
3 Sept. 2008 NEUSOFT SECRET
color palette
R G B
0 162 180
65 195 200
175 220 220
205 235 230
218 240 240
153 51 102
153 204 0
240 210 80
255 204 153
255 255 150
0 0 0
51 51 51
102 102 102
153 153 153
100
120
140
3 Sept. 2008 NEUSOFT SECRET
Pie chart
20.4 20.4 20.4
2001 2003 2005 2007 2008 2010
20.4
27.4 100
3 Sept. 2008 NEUSOFT SECRET
Pie chart
20.4
20.4 20.4 20.4
Title主标题,英文: Frutiger 65 Bold 40pt ; 中文:黑体简 加粗 40pt
Speaker Name 演讲人 Title职位 英文:Frutiger 55 Roman 20pt;中文: 黑体简 20pt
3 Sept. 20082008 By Neusoft Corporation All rights reserved Copyright © NEUSOFT SECRET
Maximize shareholder value
Adopt sound financing approach
Grow through cultural initiative
Grow through acquisition and/or merger
3 Sept. 2008 NEUSOFT SECRET
140
130 120
120
100
80
65
60
50
50
东部 西部 北部 南部
40
20
0 2001 2002 2003 2004 2005
3 Sept. 2008 NEUSOFT SECRET
Column chart
140
130 120
120
100
80
65
60
50
50
东部 西部 北部 南部
40
20
0 2001 2002 2003 2004 2005
3 Sept. 2008 NEUSOFT SECRET
Text, 英文:Frutiger 55 Roman 36pt;中文:黑体简36pt
Text, 3 Sept. 2008 NEUSOFT SECRET 英文:Frutiger 55 Roman 36pt;中文:黑体简36pt
Text, 英文:Frutiger 55 Roman 36pt;中文:黑体简36pt
Systems
3 Sept. 2008 NEUSOFT SECRET
Staff Systems Style
Text here Text here Text here Text here Text here Text here Text here =
Shared Text here Text here Structure Values Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here
2001 2003 2005 2007 2008 2010
27.4 100
3 Sept. 2008 NEUSOFT SECRET
Column chart
140 50 45 120 40 100 35 30 25 60 20 15 10 20 5 0 2001 2002 2003 2004 2005 0 东部 北部 南部 西部
Label 5
3 Sept. 2008 NEUSOFT SECRET
Chart
000 000 000 000 000 Series Series Series Series
20 20 20 20 20 20 30 40 50 60 20 20 20 40 30 20 20 25 50 30
Label 1
230 230 230
255 255 255
Mini palette
Text on the palette
text
text
text
text
text
text
text
text
text
text
text
text
text
text
text
text
3 Sept. 2008 NEUSOFT SECRET
Column chart
Chart
Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Text here Strategy Skills