颈静脉孔的解剖及临床应用
颈静脉孔的解剖及临床应用

颈静脉孔的解剖及临床应用颈静脉孔的解剖及临床应用摘要:颈静脉孔由于位置深,解剖结构复杂,比较难理解,手术也难到达(5.6.7)。
因其在大小和形态在不同颅骨的差异,在同一颅骨上两侧的不同,同一孔道颅内端与颅外端的不同,以及其形态不规则行程曲折、由两块颅骨构成,有诸多的颅神经和静脉管穿行其间,所以很难将其概念化。
1 颈静脉孔的位置形态颈静脉孔是位于测颅底的枕、颞之间较大的不规则裂隙,外形和大小变异较大。
由颞、枕骨共围成,位于颅底枕髁的外侧,左右各一,呈不规则的椭圆形。
其内有后组脑神经和颈内静脉穿行,该孔为颅底最低点,有利于颅内静脉引流至颈内静脉。
颞骨岩部下面有一深窝,为颈静脉窝,构成颈静脉孔的前内界及外界,窝内容纳颈静脉球。
枕骨颈静脉突的前缘有一深而宽的切迹,为颈静脉切迹,构成颈静脉孔的后内界。
在孔的外侧壁,有乳突小管存在,迷走神经耳支穿过此管。
在其前缘有鼓室小管开口,舌咽神经鼓室支经此入鼓室。
颈静脉孔内存在颞骨和枕骨向孔内突出的颈静脉内突,分别称为颞突和枕突,部分融合成骨桥。
骨桥在影像学检查中具有一定意义。
2 颈静脉孔的结构毗邻颈静脉孔外口的前方为颈动脉管外口,外侧为茎突、茎乳孔,再向后外侧为乳突。
内侧为舌下神经管、枕髁和枕骨茎突。
茎突是咽旁间隙的中心解剖标志,能保护其深面的颈内动脉、静脉和后组颅神经。
颈静脉孔内口前内侧部的前外上方为内耳门,后内下方为舌下神经管,三者连线近乎一条直线。
其后外侧为前庭导水管外口,后内侧可出现髁管。
颈静脉孔前内侧部有岩下窦沟从颞骨岩尖向下沿岩枕裂延伸,其内有岩下窦至颈静脉孔注入颈内静脉。
颈静脉孔后外侧部则有乙状窦沟从横窦外端沿颞骨乳突部延伸。
颈静脉孔与周围结构的距离,与其本身的大小有关,主要与颈静脉窝的大小有关,颈静脉窝较大时,顶部与鼓室仅隔一层很薄的骨板。
3 颈静脉孔内结构颈静脉孔内口前内侧部的前外上方为内耳门,后下方为舌下神经管,三者连线近乎成一直线。
其后侧为前庭导水管外口,后内侧可出现髁管。
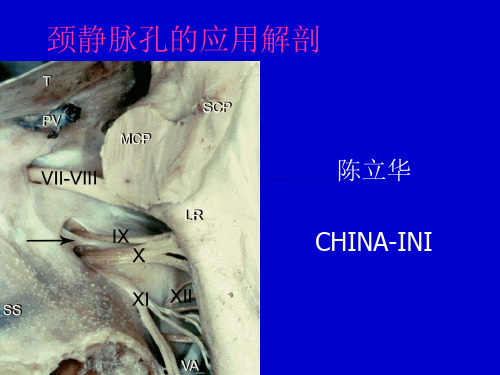
颈静脉孔的应用解剖及其在外科手术中的应用

s e s o f a d u l t s k u l l s( 1 2 6 s i d e s ) w e r e o b s e r v e d a n d me a s u r e d f r o m s h a p e , d i a m e t e r s i z e o f t h e j u g u l a r f o r a m e n a n d a d j a c e n t r e l a t i o n s h i p .Re —
静脉孔 内外 口的 口径大小和毗邻关系进行观察和测量 。结果
孔 内外 口间差异显著 ( P< 0 . 0 5 ) ; 毗邻关系左右无 明显差异 ( P> 0 . 0 5 ) 。结论
疗 中应加 以注意。 [ 关键词 ]颈静脉孔 ; 应用 解剖 ; 外科手术
[ 中图分类号 ]R 3 2 3 . 1 ; 1 1 5 4 3 . 4; R 6 5 1 . 1 1 [ 文献标识码 ]A [ 文章编号 ]1 6 7 2 — 5 0 4 2 ( 2 0 1 3 ) 0 1 4 3 0 5 8 - 0 2
d i f f e r e n c e b e t w e e n i n s i d e a n d o u t s i d e t h e m o u t h o f t h e j u g u l a r  ̄ r a me n ( P< 0 . 0 5 ) , nd a he t r e w a s n o s i g n i i f c nt a d i f f e r e n c e b e t w e e n l e f t nd a
A p p l i e d a n a t o my o f t h e j u g u l a r f o r a me n a n d i t s a p p l i c a t i o n i n s u r g e r y
颈静脉孔的应用解剖学

#应用解剖#颈静脉孔的应用解剖学肖 明, 丁 炯, 韩群颖, 王鹤鸣, 左国平(南京医科大学解剖学教研室,江苏南京210029) =摘要>目的:为与颈静脉孔相关的影像诊断和临床治疗提供解剖学资料。
方法:从颅底内、外面,对80具成年颅骨的颈静脉孔进行观测;并对20具成人尸头进行解剖,观察该区域神经血管解剖关系。
结果:¹62.3%右侧颈静脉孔较左侧大,15.9%左侧较大,21.8%两侧大小一致;º14.38%的颈静脉孔有骨桥,85.62%无骨桥;»颈静脉孔内、外侧缘距正中矢状面两侧的平均距离颅外均较颅内大:颅外分别为26.11mm 和33.41mm,颅内分别为22.29mm 和27.52mm 。
¼Ù脑神经多沿颈静脉孔前上缘,Ú、Û脑神经沿内侧缘出颅,两者被纤维索(占87.5%)或骨桥(占12.5%)隔开。
½Ù脑神经多经颈静脉孔外口前上缘向前下越过颈内动脉表面;Ù脑神经经颈内静脉深面(占57.5%)或其浅面(42.5%)行向后下。
结论:右侧颈静脉孔通常较左侧大,左右不对称;影像学观测该区域血管、神经应选择恰当的层面。
=关键词>颈静脉孔; 颈内静脉; 脑神经; 应用解剖学=中图分类号>R323.1 =文献标识码>A =文章编号>1001-165X(2001)02-0159-03Applied anatomy of jugular foramen XIAO Ming,DING J ong ,HAN Qun -ying,et al.De p a rtment o f A natom y ,Nan j ing Medical University ,Nan j ing 210029,China=Abstract >Objective:To provide anatomic data for imaging diagnosis and microsurgical treatment of jugular fora -men (JF)lesions.Methods:The JF was observed and measured from internal and external aspects in 80adult skulls.The anatomic relationships between the nerves and vessles in this region were observed i n detail by dissecting 20adult cephalic specimens.Results:¹In 62.3%of all these cases the right JF was larger than the left.In 15.9%the left was larger and in 21.8%they were equal in size.ºBone bridges could be seen in 14.38%and could not in 85.62%.»Measured from extracranial aspect,the average distance from midsagi ttal plane to the medial and lateral border of the JF (medial 26.11mm,lateral 33.41mm),was larger than those measured from intracramial aspect (medial 22.29mm,lat -eral 27.52mm).¼Ùcranial nerve made its ex i t through the anterior superior border of the JF in most cases,meanwhile Úand Ûcranial nerve through the medial border,they were distinctly separated from each other by a band of fibrous tissue (account for 87.5%)or a bone bridge (12.5%).½Jus t outside the J F,Ùcranial nerve appeared at the anter-ior border and made a loop downward and forward superficial to the internal carotid artery.Ùcranial nerve run down ward and back ward deep (account for 57.5%),or superficially (42.5%)to the internal jugular vei n.Conclusions:T he right J F is usually larger than the left,and not symmetry on both sides.The key to imaging diagnosi s of nerves and ves -sels in the JF region is to select the sectional plane correctly.=Key w ords >Jugular foramen; Internal jugular vein; Cranial nerve; Applied anatomy颈静脉孔为枕骨与颞骨岩部之间的一骨性孔道,位于岩枕缝的后端,被颈内静脉结节分为二部或三部[1]。
前世今生:颈静脉孔区入路——概述

前世今生:颈静脉孔区入路——概述颈静脉孔区手术入路,这是颅底外科界一个让人望而却步但又不得不理清的话题。
首先,颈静脉孔本身就是颅底解剖中最为复杂的一个区域,相较于仅仅涉及单一颅骨的海绵窦区(蝶骨)和枕骨大孔区(枕骨),颈静脉孔区涉及了两块颅骨——颞骨和枕骨,而它们又分别牵扯到了两个学科——颞骨是耳鼻喉(ENT)的灵魂之地,而神外对枕骨更为熟悉。
再来说手术入路,由于该区域位置深在,结构复杂,无论对于哪个学科来说,都必然经历很长的时间去完善自己的体系,这过程中就诞生了无数混乱不堪的理念和命名,这是纵向的复杂;而由于隶属于不同学科范畴,涉及不同的病变,处理的方式和理念自然有很大区别,两个学科从互不相认到发生碰撞到逐渐融合,又“杂交”出了更多的混沌,这是横向的复杂。
即使是当今世界级的中心,似乎也因受限于某一主导专业与生俱来的学科天性,在处理该区域病变时,仍是“个性鲜明”而非“海纳百川”,相应地,其发表的学术著作自然而然带上了某些印记,深入有余而广度不足。
这些都造成了开篇所说的“望而却步”。
要解决这一难题,唯有思考阅读实践。
对于实践机会严重有限的我们,借用沈李奎师兄说的一句话,“唯有阅读和思考是超越时空的捷径”。
接下来就跟随百余篇历史文献来理一理这个难题——颈静脉孔区手术入路。
概述首先需明确,颅底所有的“孔”(foramen)都不是二维的开口,而是三维的管道;贯穿颈静脉孔这一管道的,并不是颈静脉,而只有IX-XI后组颅神经。
颈静脉孔(jugular foramen)又称“后破裂孔”(posterior foramen lacerum)[1],因此同破裂孔一样,对于颈静脉而言,开口只有一个,即颅外口,其只是在颅内口的外侧“擦身而过”。
可以假想,如果在颅内面不存在颈静脉孔,对乙状窦和颈静脉球来说丝毫没有影响。
故颈静脉球和乙状窦都属于颈静脉孔内口处脑膜层以外的硬膜间结构。
图1:蓝色虚线为颈静脉孔内空间范围,红色箭头和黄色箭头为颅内口(分别进入乙状部和岩部),红色实线为颅外口,大小对比可理解下文的“别有洞天”和“管中窥豹”。
最新颈静脉孔区解剖
• posterosuperior view of the intrajugular process and ridge, which separate the sigmoid and petrosal parts of the jugular foramen
Rembrandt van Rijn (Dutch, 1606-1669). ห้องสมุดไป่ตู้his painting is called "The Anatomy Lecture of Dr. Nicolaes Tulp", painted in 1632
• the vestibular aqueduct opens onto the posterior surface of the temporal bone superolateral to the jugular foramen
• The inferior petrosal sinus extends along the petroclival fissure and enters the petrosal part of the foramen
• cochlear aqueduct opens above the petrosal part of the foramen , where the glossopharyngeal nerve enters the intrajugular part of the foramen on the medial side of the intrajugular process.
• larger lateral part, the sigmoid part, which receives the drainage of the sigmoid sinus, and a smaller medial part, the petrosal part, which receives the drainage of the inferior petrosal sinus
颈静脉孔区静脉窦开口的解剖学研究
颈静脉孔区静脉窦开口的解剖学研究孙慧颖高志强田旭赵杨魏兴梅奥登苏日塔于姝婷宋雯洁冯国栋*中国医学科学院北京协和医学院北京协和医院耳鼻咽喉头颈外科(北京100730)【摘要】目的探讨颈静脉孔区静脉窦开口的特点及与神经的毗邻关系。
方法统计分析30例颅骨标本中颈静脉球及近颈静脉球的乙状窦、颈内静脉内静脉窦开口的位置、数量、最长径及其与颅神经的关系。
结果全部标本均可观察到岩下窦开口,60%(18/30)为多个开口,90%(27/30)有一较大开口位于颈静脉球前内侧壁,且与第IX、X、XI颅神经关系密切。
60%(18/30)标本中可见后髁导静脉的开口,94.4%(17/18)为单个开口,常位于颈静脉球底壁或静脉球与乙状窦交界处。
颈静脉球内侧壁可见数量不等的边缘窦、枕窦及岩骨穿支静脉的开口。
结论颈静脉球及近颈静脉球的乙状窦、颈内静脉内存在多个静脉窦的开口,行此区手术时应充分止血并仔细检查各个开口,避免肿瘤残留,处理前内侧岩下窦开口时应轻柔操作,避免损伤后组颅神经(IX、X、XI)。
【关键词】颈静脉孔;静脉窦;颅神经【中图分类号】R764【文献标识码】A【文章编号】1672-2922(2019)03-296-4 An Anatomical Study of Openings of Venous Sinuses in Jugular ForamenSUN Huiying,GAO Zhiqiang,TIAN Xu,ZHAO Yang,WEI Xingmei,AO Dengsurita,YU Shuting,SONG Wenjie,FENG Guodong*Department of Otorhinolaryngology,Peking Union Hospital,Chinese Academy of Medical Sciences and Peking UnionMedical College,Beijing100730,ChinaCorresponding author:FENG Guodong Email:fengguodong2013@ 【Abstract】Objective To study the anatomical characteristics of venous sinuses openings and their relationship with cranial nerves in the jugular foramen.Methods The location,number and longest diameter of venous sinuses open-ings in the jugular foramen were measured in30temporal bones specimens.The relationship between venous sinuses openings and cranial nerves was examined.Results60%(18/30)of inferior petrosal sinus(IPS)had several openings. 90%(27/30)of IPS had the largest branch going between cranial nerves with an opening in the anteromedial wall of jug-ular bulb(JB).60%(18/30)of specimens had opening of posterior condylar emissary vein(PCEV).94.4%(17/18)of PCEV had one large opening on the floor of JB or the junction of sigmoid sinus and JB.There were several openings of marginal sinus(MS),occipital sinus(OS)or perforating branches of veins going through petrosal bone.Conclusion The venous sinuses may have several openings in the jugular foramen,requiring carefully examination for residual tumor and adequate hemostasis.Care must be taken in the management of the IPS anteromedial branch to avoid damaging the cranial nerves.【Key words】Jugular Foramen;Venous Sinuses;Cranial NervesFund program:Key Projects in the National Science&Technology Pillar Program during the Twelfth Five-year Plan Period (No.2012BAI12B01).The authors report no conflicts of interest.·侧颅底专辑·颈静脉孔区(jugular foramen,JF)是侧颅底手术中重要的解剖区域之一,其位置深在且结构复杂,是沟通颅内外的重要通道,由颞骨及枕骨构成,呈不规则裂孔状。
颈静脉孔区解剖
颈静脉孔诊断
颈静脉孔区不同性质肿瘤的生长 方式及特点,对术前正确诊断、 确定合理的治疗方案及术中保护 神经功能具重要意义
神经鞘瘤
神经鞘瘤起源于舌咽神经、迷走神经、副神 经或颈交感干,沿其起源的神经生长。神经 鞘瘤因压迫性溶骨致颈静脉孔扩大,表现为 扇贝样改变而骨皮质完好。边缘常是光滑的 ,瘤边界清楚。
glossopharyngeal nerve passes forward along the medial side of the intrajugular ridge vagus and accessory nerves, on the medial side of the
medial side of the intrajugular process, intrajugular ridge extends forward along the medial side of the jugular bulb
larger lateral part, the sigmoid part, which receives the drainage of the sigmoid sinus, and a smaller medial part, the petrosal part, which receives the drainage of the inferior petrosal
CT为高密度肿瘤。
MRI缺乏象化学感受器那样的瘤内血管流空影。增强 后T1像明显强化,其程度较化学感受器瘤更为明显 ,并常可见脑膜尾征。
脑膜瘤典型的表现为“离心性”扩张和“匍匐状” 生长,并有浸润颅神经和血管外膜的倾向。其对邻 近骨质的破坏表现为广泛浸润板障而骨结构和骨密 度得以保留,颈静脉孔边缘因皮质遭破坏而不规则 。边缘往往有骨质增生或硬化的表现。
前世今生:颈静脉孔区入路(中篇)
前世今生:颈静脉孔区入路(中篇)三、“转”(1980s初~1990s末)1980s年代,CT和脑血管造影成为颈静脉孔区病变的必备检查,球囊闭塞试验和内分泌检查也开始成为术前常规。
80s末MRI(最早1977)的引入,更填补了MRI、CT、DSA BOT影像学诊断体系的最后一环。
1979年Delgado第一次进行了术中面神经电生理监测。
这些辅助技术的进步,促使ENT在Fisch入路体系基础上,对颈静脉球瘤手术的思考“转”向两个方向:1、颅内部分肿瘤的更好切除;2、更好的功能保护(面神经、听力)。
神外方面,80s~90s年代迎来了颅底亚专业的大爆发,虽然起步晚于ENT,但随着颅底内侧面的“三座大山”(前床突、岩骨嵴和颈静脉结节)一一被攻克,通向海绵窦、岩斜区和枕骨大孔的道路前所未有的敞亮,来自颅底内面观的神外入路终于与来自颅底外面观的ENT入路胜利会师。
聚焦到颈静脉孔区,神外也出现了巨大“转”变:视角终于不再是局限于CPA,而是将其纳入了枕骨大孔/颅颈交界区入路体系,发展出了后外下视角的“髁旁入路”。
由于两个学科的“转”在时间和形式上都相互交错重叠,若仍然以编年史的形式来记录就会比较混乱,因此将从上述三大“转”变分别记录。
文中标识:下划线:历史上的第一次橙色:命名相关绿色:ENT相关蓝色:神外相关紫色:分级系统灰色:长期随访报告红色:大事件粗体:重要手术入路或技术参考文献和图例序号均接《上篇》1、关于肿瘤颅内扩展(intracranialextension,ICE)•1979 Kinney:着重从ENT角度讨论颈静脉球瘤累及颅内部分处理的早期文献,强调了与神外的合作,联合神外的乙状窦后入路,选择性地对如下病例行一期切除:肿瘤后颅窝部分较局限,且未向前方延伸而位于颈内动脉后方。
处理颞骨时,保留外耳道,面神经前移位从第二膝开始(短程),强调保留与二腹肌后腹的附着以保护面神经,对下鼓室的暴露经扩大面神经隐窝,并强调了对内听道下壁下方鼓骨的切除。
颈静脉孔区薄层断层解剖学研究

37
中国耳鼻咽喉颅底外科杂志
第8卷
两侧颧弓点, 作垂直于横断面的冠状切面; 平行于此 冠状平面 , 过乳突后缘作另一冠状平面 ; 再作一正中 矢状切面, 最后得到一包含颈静脉孔区及相邻组织 结构在内的组织块, 一共取 9 个组织块。 1. 2 生物塑化标本的制作 采用生物塑化技术, 将上述 9 例组织块分别制 成塑化薄层连续断面标本, 横断、 冠状、 矢状每个方 位各 3 套, 片间距 1. 5mm, 其中片厚 1. 2mm, 锯路损 耗0. 3mm 。断层标本 逐一用肉眼、 手术显 微镜、 光 学显微镜观察和测量 , 分片记录。 2 结果 2. 1 横断断面 颈静脉孔位于颞骨岩部 ( P ) 与枕骨 ( Oc) 之间 ,
颈静脉孔( JF) 是颅底重要解剖结构 , 位置较深 , 有舌咽神经、 迷走神经、 副神经及血管结构穿过 , 神 经与血管之间相互关系复杂。尽管对颈静脉孔区的 显微解剖已有较多研究
[ 1, 2]
t ion)
[ 5]
, 重点进行了颈 静脉孔区的供详细的断层 解剖学依据。 1 材料与方法
[ 1, 2]
邱明国 , 等 : 颈静脉孔区薄层断层解剖学研究
第1期
血管部两个部分 , 神经部为第 为第
脑神经占据, 血管部
静脉孔及相关神经、 血管能够连续显示并准确分辨, 与 HRCT 、 MRI 图象有良好的对应关系, 对颈静脉 孔及相关结构的正常断层解剖研究有较高的价值, 可以为临床颈静脉孔区的影像学诊断提供较准确的 断层解剖学资料。 ( 本文图 1~ 6 见插页第 2 页 )
突小房。舌下神经管( HC) 位于乙状窦的内下方 , 管 内有大量的静脉结构。在面神经垂直段层面 , 颈静 脉球顶部位于颞骨下部的颈静脉窝内, 其上方紧邻 后半规管下脚 , 外上方为鼓窦 , 外侧为 面神经垂直 段 , 内侧部有舌咽神经束、 迷走神经束、 副神经束进 入。颈静脉孔内下方为舌下神经管( 图 3) 。在茎突 根部层面 , 颈静脉孔上方为前庭及面神经垂直段的 起始部 , 舌咽神经束、 迷走神经束、 副神经束沿枕骨 表面进入颈静脉孔 , 位于颈静脉孔的内下方, 沿颈内 静脉向前下走行。在颈静脉孔内口处可见岩下窦由 内上向外下走行, 位于神经束的前内侧, 进入颈静脉 孔后, 逐渐向下走行, 在颈静脉孔外口处与颈静脉球 交汇 , 开口于颈静脉球的内侧壁。同时可见舌下神 经向外下伴随舌咽神经束、 迷走神经束、 副神经束走 行( 图 4) 。在前庭窗层面 , 颈内静脉位于颈内动脉 的外侧 , 上方为鼓室的下壁 , 仍可见岩下窦于颈内动 脉的后方汇入颈内静脉。此层面可清楚显示颈内静 脉、 颈内动脉、 颈静脉孔及颞骨内结构的相互关系。 2. 3 矢状断面 颈静脉孔10~ 11层面显示, 其中 6~ 7 个层面可 显示内外口及管道全程。管道前上壁为颞骨岩部构 成 , 后下壁由枕骨构成。颈静脉球与乙状窦的移行 部可全程显示 , 两者几乎成直角。颈静脉球向下延 续为颈内静脉。颈静脉窝成光滑的穹隆状 , 其上方 有前庭( Vs) 、 耳蜗 ( Co) 等结构, 内耳道内面神经、 前 庭神经 ( VN) 及蜗神经 ( CoN) 可清楚显示。颈静脉 孔的前方为颈内动脉, 在颈内动脉的前方可见棘孔、 卵圆孔及下颌神经等结构。颈静脉孔内神经结构在 矢状断面难以观察, 仅在颈静脉孔内口处可见舌咽 神经束、 迷走神经束、 副神经束呈上下方向排列, 位 于脉络膜丛的前下方( 图 5, 6) 。 3 讨论
颈静脉孔区的显微解剖学对策.pdf

1、JF后壁2、颈突3、枕髁4、枕骨大孔5、舌下神经管外口6、斜坡下部(基底部)7、髁管外口图1枕骨底面观l、JF后内侧缘2、乙状窦末段3、颈静脉结节4、舌下神经管内口5、斜坡6、小脑窝7、枕内嵴8、枕内隆突9、横窦沟图2枕骨内面观颞骨以外耳门为中心分三部。
前上方、呈鳞片状的鳞部。
内有脑膜中动脉沟、颧突、下颌窝、关节结节等结构;从前、下、后三面围绕外耳道的弯曲骨片称鼓部;岩部也称锥部,尖指向前内对着蝶骨体。
岩举成JF的前外侧边。
’结构见图3,图41、内耳门2、蜗水管外口3、锥形窝4、颞突5、乙状窦沟6、乳突孔7、顶切迹8、岩上窦沟9、弓状隆起10、岩浅大神经沟11、脑膜中动脉沟12、前庭水管外口13、三叉神经压迹图3颞骨的内面观31、乳突孔2、二腹肌沟3、乳突4、鼓乳裂5、外耳门6、岩鼓裂7、下颌窝8、颧突9、茎乳孔10、颈动脉管11、颈静脉窝图4颞骨的底面观JF位于颅底枕髁的前外侧和岩骨的后内侧,左右各一。
从颅内看,JF位于颞骨岩部外1/3的后面,岩枕裂的后端,岩部与枕骨结合处(图7)。
从颅外看,JF位于颈动脉管外口、茎突和枕髁3点连线形成的三角区内,居颈动脉管外口之后,茎突的前讷侧,枕骨髁的外‘侧。
和咽旁间隙相对应(图8)。
2.JF形态和大小JF位于后颅窝,+既不是严格的矢状位,也不是严格冠状位,其长轴由后外至前内。
它。
的后外侧部分较大,而前内侧部较小,JF外口呈不规则的三角形,偏向外侧。
内口位于后颅窝的中部斜坡的两侧,形似鸟状,头部相当于前内侧部,腹部相当于后外侧部,两端分别连与与鞍区相连的岩下窦沟和与横窦沟相连的乙状窦沟。
内口和外口之间是膨大的一形状不规则深窝,称颈静脉窝,内容纳颈静脉球(jugIllarbulk,JB)(图9.2)。
镜下对每个标本测量JF的长径、前内侧部的最大横径及后外侧部的最大横径,然后以三径之和作为比较的指标,比较JF左右侧的大小。
见表1表1JF左右侧的大小比较3.分型颞骨岩部和枕骨在发育过程中向JF’各发出大小不等骨性突起,称颈静脉内突(intrajugularpress,uP),其中发自颞骨岩部的称颞突,发自枕骨的称枕突,前者细长、后者短粗,二者发育程度的不同可形成几种情况:1、枕突和颞突均明显发育,伸向JF内(图5,图9·1);2、颞突发育明显,并向颈静脉孔外口方向延伸,形成颈静脉窝部分内侧壁,枕突不发育(图7);3、枕突发育明显,伸向颈静脉孔内,颞突不明显。
颈静脉孔区解剖课件

04
术后护理:预 防感染、保持 1 诊断方法:CT、MRI、超声等影像学检 查
02 治疗方法:药物治疗、手术治疗、介入治 疗等
03 颈静脉孔区病变的临床表现:头痛、头晕、 耳鸣、视力下降等
04 颈静脉孔区病变的预防:保持良好的生活 习惯,避免长时间低头、颈部受凉等。
03
颈内静脉的主 要功能是收集 头部和颈部的 血液,并将其 输送到心脏
04
颈内静脉在颈 部的位置和走 行与颈动脉相 似,但比颈动 脉更靠近中线
迷走神经
01
02
03
04
迷走神经损伤可能导致心脏、 呼吸、消化等功能障碍,需 要及时治疗。
迷走神经在颈静脉孔区与颈 动脉、颈静脉等血管紧密相 邻,容易受到损伤。
热等症状
颈静脉孔区损伤: 如外伤、手术损 伤等,可引起局 部出血、神经损
伤等症状
颈静脉孔区畸形: 如先天性颈静脉 孔区畸形、颈静 脉孔区发育不良 等,可引起局部 畸形、功能障碍
等症状
颈静脉孔区的手术
01
手术目的:治 疗颈静脉孔区 病变,如肿瘤、 畸形等
02
手术方式:微 创手术、开放 手术等
03
手术风险: 损伤神经、 血管等
颈静脉孔是颈部的重要结构,位于颈部前外 侧,是颈部血管、神经和淋巴管的通道。
颈静脉孔是颈部血管的重要通道,包括颈内 静脉、颈外静脉和颈总动脉。
颈静脉孔是颈部神经的重要通道,包括颈神 经、臂神经和胸神经。
颈静脉孔是颈部淋巴管的重要通道,包括颈 淋巴管、臂淋巴管和胸淋巴管。
颈静脉孔区的神经 血管
颈内动脉
谢谢
颈静脉孔区解剖课件
演讲人
目录
01
颈静脉孔区解剖结 构
颈静脉孔区的应用解剖学研究

颈静脉孔区的应用解剖学研究**颈静脉孔区的应用解剖学研究***引言*颈静脉孔区是颈部解剖学中一个重要而复杂的区域,涉及到颈动脉、颈静脉等多个血管和神经结构。
对颈静脉孔区进行深入的应用解剖学研究,对于理解颈部血管循环、神经分布以及手术操作等方面具有重要的临床意义。
本文将从颈静脉孔区的解剖结构、应用价值以及研究方法等方面展开讨论,旨在全面呈现颈静脉孔区的应用解剖学研究。
*一、颈静脉孔区的解剖结构*颈静脉孔区位于颈部的后三角区域,是一个由多个解剖结构组成的区域。
主要包括颈静脉、颈动脉、神经丛等多个重要结构。
颈静脉孔区内的结构相互交错,密集的血管和神经网络构成了一个复杂的解剖学区域。
详细了解这些结构的位置、走向和相互关系,对于在临床实践中进行准确的解剖和操作具有重要的指导价值。
1. **颈静脉**:颈静脉是颈部最重要的静脉之一,负责将头颈区域的血液输送至上腔静脉。
其在颈静脉孔区的走向以及与其他血管的关系直接影响到手术操作的安全性和效果。
2. **颈动脉**:颈动脉是颈部主要的动脉之一,通过颈静脉孔区向上供应大脑血液。
对颈动脉在颈静脉孔区的分支、变异以及与周围结构的关系进行深入研究,有助于在手术中避免不必要的损伤。
3. **神经丛**:颈静脉孔区包含丰富的神经丛,其中既有迷走神经,也有来自交感神经系统的神经纤维。
了解这些神经的分布情况,对于手术操作中的神经保护和功能维持具有关键性的作用。
*二、颈静脉孔区的应用价值*深入研究颈静脉孔区的解剖学结构,不仅有助于提高手术的安全性和成功率,还对多个临床领域具有广泛的应用价值。
1. **外科手术导航**:颈静脉孔区的解剖结构研究可为颈部外科手术提供重要的导航信息。
在颈部肿瘤切除、颈动脉瘤修复等手术中,深入了解颈静脉孔区的结构有助于外科医生更准确地定位和操作。
2. **介入治疗**:对颈静脉孔区的解剖学研究有助于指导介入性治疗,如颈静脉导管插入、球囊扩张术等。
准确地了解血管结构和神经分布,可以最大程度地避免并发症。
颈静脉孔区显微解剖研究

颈静脉孔区显微解剖研究[摘要] 目的研究颈静脉孔区显微解剖,为手术入路的选择提供形态学资料。
方法手术显微镜(15倍)下对15个头颅标本,30侧颈静脉孔进行显微解剖和观察。
结果颈静脉孔分为三部,即岩部、神经部、乙状部。
岩部为接收岩下窦、舌下神经管静脉、岩斜裂静脉和椎静脉丛分支的静脉窦;神经部由位于结缔组织鞘中的舌咽、迷走、副神经所组成,行于颈静脉球上方的内侧,舌咽神经位于最前方,神经间被纤维或骨性结构隔开;乙状部接收乙状窦血流。
结论颈静脉孔区结构复杂,熟悉颈静脉孔区的显微解剖有利于手术中保护重要的神经和血管。
[关键词]颈静脉孔显微解剖The Mieroanatomical Study of the Jugular ForamenWang Lu, Ruan CaiLian, Han ZhenkuiAbstract:Objective To provide morphological basis for the selection of operation approach by studying the microanatomy of jugular forainen. Methods 30 jugular foramens of 15 specimenswere studied under the microscope.Results The jugular foramen was divided into three parts, the petrosa part, the neutral part and the sigmoid part. The jugular bulb and adjacent part of jugular vein received drainage from the sigmoid and inferior petrosal sinuses,the vertebral venous plexus,the venous plexus of the hypoglossal canal,the condylar emissary vein,and the vein coursing along the inferior aspect of the petroclival fissure. Conclusion The jugular foramen is a complex area. The vital nerves and vascular structures can be protected in operation if the microsurgical anatomy of the jugular foramen is familiarized by the doctor.Key words: jugular foramen;microanatomy颈静脉孔(iugular foramen,JF) 在颅底各孔中结构复杂,位置深在,内容物多,差异较大[1]。
颈静脉孔区解剖

颈静脉孔区解剖
HELLO NOVEMBER
颈静脉孔由枕骨基底部和颞骨岩部下面围成,近似呈尖向前内的三角形,内侧壁为枕骨基底部,后外侧壁为颈静脉窝,前外侧壁为颈静脉内突和颈动脉管内侧壁。
内主要有岩下窦、颅神经及乙状窦等重要结构。
Hovelague将颈静脉孔分为两部分:前内侧部较小,内含有舌咽神经,也叫作神经部;后外侧部较大,内含有颈静脉球体、迷走神经和副神经,叫作静脉部。
这两部分通常被纤维桥或骨桥分隔。
在颈静脉孔上覆盖有硬脑膜,在硬脑膜上有两个孔洞,一个孔为舌咽神经经过的通路,此神经经孔进入神经部;另一个是迷走神经孔,迷走神经和副神经由此孔进入静脉部。
上述诸结构在颈静脉孔内的位置与相互毗邻关系, 国内外有关文献描术不一。
岩下窦在颈静脉孔注入颈内静脉。
舌咽神经、迷走神经及副神经经颈静脉孔出颅。
乙状窦经颈静脉孔延续为颈内静脉。
颈静脉孔区的应用解剖学研究

颈静脉孔区的应用解剖学研究摘要:颈静脉孔区是颈部重要的解剖结构,其解剖特点对颈部肿瘤、血管外科手术、神经外科手术等领域具有重要的临床应用价值。
本文主要对颈静脉孔区的解剖结构、生理功能、临床应用及相关问题进行综述,以期为临床医生提供参考。
关键词:颈静脉孔区;解剖结构;生理功能;临床应用一、简介颈静脉孔区是颈部重要的解剖结构之一,位于颈部胸锁乳突肌和斜角肌之间,是颈部血管、神经、淋巴等结构的交汇处。
其解剖特点对颈部肿瘤、血管外科手术、神经外科手术等领域具有重要的临床应用价值。
本文主要对颈静脉孔区的解剖结构、生理功能、临床应用及相关问题进行综述。
二、颈静脉孔区的解剖结构颈静脉孔区是由胸锁乳突肌、斜角肌、颈内静脉、迷走神经、副神经、颈部淋巴结等组成的一个三角形结构,其顶部为胸锁乳突肌,底部为斜角肌,内侧为颈内静脉,外侧为颈部淋巴结。
颈静脉孔区的大小和形状因人而异,但一般为椭圆形或三角形,其面积约为2-3平方厘米。
(一)胸锁乳突肌胸锁乳突肌是颈部肌肉中的重要肌肉之一,其起点为胸骨和锁骨,止点为颈椎横突和第一肋骨,属于颈肩部肌肉。
胸锁乳突肌在颈静脉孔区的位置较高,其上缘为颈静脉孔区的顶部。
(二)斜角肌斜角肌是颈部肌肉中的重要肌肉之一,起点为胸锁乳突肌和第一肋骨,止点为颈椎横突和第二肋骨。
斜角肌在颈静脉孔区的位置较低,其下缘为颈静脉孔区的底部。
(三)颈内静脉颈内静脉是颈部重要的血管之一,起点为颅内静脉窦,止点为锁骨下静脉汇合处。
颈内静脉在颈静脉孔区内穿过斜角肌和胸锁乳突肌之间的裂隙,进入胸腔。
(四)迷走神经迷走神经是颈部神经中的重要神经之一,起点为延髓,止点为胃肠道。
迷走神经在颈静脉孔区内从颈内静脉的外侧穿过,进入胸腔。
(五)副神经副神经是颈部神经中的重要神经之一,起点为延髓和颈髓,止点为肌肉和腺体。
副神经在颈静脉孔区内从颈内静脉的内侧穿过,进入胸腔。
(六)颈部淋巴结颈部淋巴结是颈部淋巴系统的重要组成部分,位于颈部的深浅两层,与颈动脉、颈静脉、迷走神经、副神经等结构密切相关。
颈静脉孔区的应用解剖学研究

颈静脉孔区的应用解剖学研究
颈静脉孔区是指颈静脉在咽鼓管入口处存在的一种狭窄现象,这
种狭窄多发生在中老年人身上,主要是由于老化所致。
它是由粘膜覆
盖的颈静脉出口引起,它们中间可能存在一个或多个狭窄的群体,且
容易受到外界的影响,有的时候会收紧或扩张。
因此,研究颈静脉孔
区的应用解剖学具有重要的意义。
颈静脉孔区的应用解剖学研究主要包括以下几个方面。
首先,探
讨颈静脉孔区的解剖特点,比如它的大小、形状、位置、粘膜厚度等。
此外,研究还可以分析颈静脉孔区内或周围部位肿瘤或其他疾病的分
布情况以及影响因素。
此外,研究还可以针对颈静脉孔区开展功能性
研究,比如考察它是否会影响血流量和血液循环,或者它是否会影响
呼吸等等。
此外,颈静脉孔区的应用解剖学研究还可以探讨其临床治疗价值。
比如,可以通过测定颈静脉孔区的尺寸来预测患者的血流量,从而为
临床制定定制化的治疗方案。
另外,可以通过研究颈静脉孔区的状况
来准确判断患者的健康状况,以便对患者采取有效的治疗措施。
总而言之,颈静脉孔区的应用解剖学研究具有重要的意义,它可
以准确判断患者健康状况,帮助更好地管理患者,并有助于更好地制
定治疗方案。
颈静脉孔区静脉窦开口的解剖学研究

颈静脉孔区静脉窦开口的解剖学研究孙慧颖高志强田旭赵杨魏兴梅奥登苏日塔于姝婷宋雯洁冯国栋*中国医学科学院北京协和医学院北京协和医院耳鼻咽喉科(北京100730)【摘要】目的探讨颈静脉孔区静脉窦开口的特点及与神经的毗邻关系。
方法统计分析30例颅骨标本中颈静脉球及近颈静脉球的乙状窦、颈内静脉内静脉窦开口的位置、数量、最长径及其与颅神经的关系。
结果全部标本均可观察到岩下窦开口,60%(18/30)为多个开口,90%(27/30)有一较大开口位于颈静脉球前内侧壁,且与第IX、X、XI颅神经关系密切。
60%(18/30)标本中可见后髁导静脉的开口,94.4%(17/18)为单个开口,常位于颈静脉球底壁或静脉球与乙状窦交界处。
颈静脉球内侧壁可见数量不等的边缘窦、枕窦及岩骨穿支静脉的开口。
结论颈静脉球及近颈静脉球的乙状窦、颈内静脉内存在多个静脉窦的开口,行此区手术时应充分止血并仔细检查各个开口,避免肿瘤残留,处理前内侧岩下窦开口时应轻柔操作,避免损伤后组颅神经(IX、X、XI)。
【关键词】颈静脉孔;静脉窦;颅神经【中图分类号】R764【文献标识码】A【文章编号】1672-2922(2019)03-296-4 An Anatomical Study of Openings of Venous Sinuses in Jugular ForamenSUN Huiying,GAO Zhiqiang,TIAN Xu,ZHAO Yang,WEI Xingmei,AO Dengsurita,YU Shuting,SONG Wenjie,FENG Guodong*Department of Otorhinolaryngology,Peking Union Hospital,Chinese Academy of Medical Sciences and Peking UnionMedical College,Beijing100730,ChinaCorresponding author:FENG Guodong Email:fengguodong2013@ 【Abstract】Objective To study the anatomical characteristics of venous sinuses openings and their relationship with cranial nerves in the jugular foramen.Methods The location,number and longest diameter of venous sinuses open-ings in the jugular foramen were measured in30temporal bones specimens.The relationship between venous sinuses openings and cranial nerves was examined.Results60%(18/30)of inferior petrosal sinus(IPS)had several openings. 90%(27/30)of IPS had the largest branch going between cranial nerves with an opening in the anteromedial wall of jug-ular bulb(JB).60%(18/30)of specimens had opening of posterior condylar emissary vein(PCEV).94.4%(17/18)of PCEV had one large opening on the floor of JB or the junction of sigmoid sinus and JB.There were several openings of marginal sinus(MS),occipital sinus(OS)or perforating branches of veins going through petrosal bone.Conclusion The venous sinuses may have several openings in the jugular foramen,requiring carefully examination for residual tumor and adequate hemostasis.Care must be taken in the management of the IPS anteromedial branch to avoid damaging the cranial nerves.【Key words】Jugular Foramen;Venous Sinuses;Cranial NervesFund program:Key Projects in the National Science&Technology Pillar Program during the Twelfth Five-year Plan Period (No.2012BAI12B01).The authors report no conflicts of interest.·侧颅底专辑·颈静脉孔区(jugular foramen,JF)是侧颅底手术中重要的解剖区域之一,其位置深在且结构复杂,是沟通颅内外的重要通道,由颞骨及枕骨构成,呈不规则裂孔状。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
颈静脉孔的解剖及临床应用
颈静脉孔的解剖及临床应用
摘要:颈静脉孔由于位置深,解剖结构复杂,比较难理解,手术也难到达(5.6.7)。
因其在大小和形态在不同颅骨的差异,在同一颅骨上两侧的不同,同一孔道颅内端与颅外端的不同,以及其形态不规则行程曲折、由两块颅骨构成,有诸多的颅神经和静脉管穿行其间,所以很难将其概念化。
1 颈静脉孔的位置形态
颈静脉孔是位于测颅底的枕、颞之间较大的不规则裂隙,外形和大小变异较大。
由颞、枕骨共围成,位于颅底枕髁的外侧,左右各一,呈不规则的椭圆形。
其内有后组脑神经和颈内静脉穿行,该孔为颅底最低点,有利于颅内静脉引流至颈内静脉。
颞骨岩部下面有一深窝,为颈静脉窝,构成颈静脉孔的前内界及外界,窝内容纳颈静脉球。
枕骨颈静脉突的前缘有一深而宽的切迹,为颈静脉切迹,构成颈静脉孔的后内界。
在孔的外侧壁,有乳突小管存在,迷走神经耳支穿过此管。
在其前缘有鼓室小管开口,舌咽神经鼓室支经此入鼓室。
颈静脉孔内存在颞骨和枕骨向孔内突出的颈静脉内突,分别称为颞突和枕突,部分融合成骨桥。
骨桥在影像学检查中具有一定意义。
2 颈静脉孔的结构毗邻
颈静脉孔外口的前方为颈动脉管外口,外侧为茎突、茎乳孔,再向后外侧为乳突。
内侧为舌下神经管、枕髁和枕骨茎突。
茎突是咽旁间隙的中心解剖标志,能保护其深面的颈内动脉、静脉和后组颅神经。
颈静脉孔内口前内侧部的前外上方为内耳门,后内下方为舌下神经管,三者连线近乎一条直线。
其后外侧为前庭导水管外口,后内侧可出现髁管。
颈静脉孔前内侧部有岩下窦沟从颞骨岩尖向下沿岩枕裂延伸,其内有岩下窦至颈静脉孔注入颈内静脉。
颈静脉孔后外侧部则有乙状窦沟从横窦外端沿颞骨乳突部延伸。
颈静脉孔与周围结构的距离,与其本身的大小有关,主要与颈静脉窝的大小有关,颈静脉窝较大时,顶部与鼓室仅隔一层很薄的骨板。
3 颈静脉孔内结构
颈静脉孔内口前内侧部的前外上方为内耳门,后下方为舌下神经管,三者连线近乎成一直线。
其后侧为前庭导水管外口,后内侧可出现髁管。
颈静脉孔前内侧部有岩下窦从颞骨岩尖部向下沿岩枕裂延伸,其内的岩下窦与展神经一同通过Dorello管。
岩下窦向外下方引流至颈内静脉。
颈静脉孔后外侧部则有乙状窦沟从横窦沟外端沿颞骨乳突部延伸。
乙状窦与乳突小房仅隔一层薄骨板,乳突手术时不要误伤。
岩上窦位于颞骨岩部的上缘,将海绵窦的血液引入横窦延伸为乙状窦处。
颈静脉孔外口的前方为颈动脉管外口,外侧为茎突、茎乳孔以及稍远处的乳突,内侧为舌下神经管、枕髁和枕骨大孔,后方枕骨茎突。
茎突是咽旁间隙的中心解剖标志,能保护其神面的颈内动、静脉和后组颅神经。
颈静脉神经部有舌咽神经和岩下窦通过。
少数舌咽神经经神经部之前独立的骨管出颅。
覆盖颈静脉孔的硬脑膜有2个持征性的穿孔。
分别形成漏斗状的舌咽神经道相筛网状的迷走神经道,前者有舌咽神经穿过。
后者有迷走神经和副神经穿过;由于吞咽、迷走神经起点邻近.且常有蛛网膜粘连,因而在脑干附近或蛛网膜下腔很难将二者确切分开,唯有在舌咽神经道与迷走神经道间的硬膜隔处方可分辨。
乙状窦进入颈静脉孔的静脉部后延续为颈静脉球。
岩下窦接纳斜坡区的血液,形成单一或多个静脉道,在舌咽—迷走神经间,或舌咽神经前,或迷走神经后.或迷走—副神经间穿过。
汇入颈静脉球内侧壁。
4 颈静脉孔与临床应用
颈静脉孔发生病变时,较大颈静脉孔的症状出现相对较晚,然而较大的颈静脉孔血流量大,处理横窦时并发症相对较多。
由于颈静脉孔大小的不同,可推断两侧颈静脉球的大小及血流量的多少。
因此,术前骨窗CT显示颈静脉孔大小有助于推断两侧颈静脉血流量的多少。
(1)
颈静脉孔临床综合征:为颈静脉孔发生病变时可出现的第IX、X、XI脑神经麻痹症候群。
IX、X麻痹可致同侧软腭、咽部感觉障碍,舌后1/3部味觉缺失;声带和软腭麻痹致声音嘶哑,病侧咽反射消失。
XI麻痹出现病侧胸锁乳突肌和斜方肌麻痹和萎缩,临床表现为不能
向对侧转颈,不能耸肩。
偶可出现耳鸣、耳聋和面神经麻痹等症状。
villaret`s、Horner`s 、ver net`s 综合征与IX---XII神经有关;sicard 、Jackson`s 、sieben mann`s 和vernet`s为颈静脉孔周围颅内区域受影响导致;而schmiedt`s是由于第X和XI颅外区域受影响导致。
参考文献
[1]陈立华、陈凌、袁贤瑞主编,实用颅底显微外科[M].中国科
学技术出版社,2010:198-205
[2]德.Johannes Lang著,孙为群、滕良珠译,颅底与相关结构临床解剖图谱[M].山东科学技术出版社,2002:267-274
[3]刘庆良、王忠诚、于春江,颈静脉孔区显微解剖(J).中华
神经外科杂志,2004,20:10-13
[4]美.Albert L.Rhoton Jr.著,刘庆良主译,颅脑解剖与手术
入路[M]中国科学技术出版社,2010:699-716
[5]Dichio G Fischer RL,Nelson KB:The jugular foramen.J
Neurosurg 21:447-460,1964.
[6]Hovelacque A:Osteologie.Paris,G Doin and Cie,1967,vol 2,ppp
155-156
[7]Kveton JF,Cooper MH:Microsurgical anatomy of the jugular foramen region.Am J Otol 9:109-112,1998.
------------最新【精品】范文。