骨肿瘤分期
骨肉瘤的分期与预后评估

论文题目:骨肉瘤的分期与预后评估1. 引言骨肉瘤是一种高度恶性的骨肿瘤,其分期与预后评估对于制定有效的治疗方案和预测患者生存率至关重要。
本文将综述目前常用的骨肉瘤分期系统及其与预后的关系,以及影响预后的相关因素。
2. 分期系统2.1 Enneking分期系统Enneking分期系统是最早应用于骨肉瘤的分期系统之一,根据肿瘤的生长方式和侵袭程度将骨肉瘤分为三个阶段:●Enneking I期:良性生长,未突破骨膜。
●Enneking II期:局部侵袭,未扩散至周围组织。
●Enneking III期:已扩散至周围组织,具有较高的转移风险。
2.2 AJCC分期系统美国癌症学会(AJCC)分期系统是目前临床上广泛应用的分期系统,将骨肉瘤分为四个阶段:●Ⅰ期:肿瘤局限于原发部位。
●Ⅱ期:肿瘤侵犯局部组织,但尚未扩散至远处。
●Ⅲ期:肿瘤扩散至周围组织或淋巴结。
●Ⅳ期:肿瘤转移到远处器官或骨髓。
3. 预后评估因素3.1 临床特征●年龄:年轻患者通常预后较好。
●肿瘤位置:肿瘤在颅骨或四肢的预后较好。
●肿瘤大小:肿瘤越大,预后越差。
3.2 病理特征●组织学类型:高分化或低分化肿瘤的预后不同。
●组织学分级:分级越高,预后越差。
●細胞型態:几型細胞型態会导致不同的预后。
3.3 分子生物学特征●基因突变:某些基因突变与预后密切相关,如TP53、RB1等。
●分子标志物:如Ki-67、P53等。
4. 预后评估预后评估通过结合临床特征、病理学特征和分子生物学特征来确定患者的预后。
通常使用Kaplan-Meier生存分析、Cox比例风险模型等统计方法进行生存分析和预后评估。
5. 结论与展望骨肉瘤的分期与预后评估是临床治疗中至关重要的一环,准确的分期和预后评估可以为患者提供更合适的治疗方案,并且有助于预测患者的生存率。
随着分子生物学和基因组学研究的不断深入,预后评估将更加精准,为个性化治疗提供更多可能性。
重视骨肿瘤的活检手术
18例则因活检误诊,决定性手术未能达到恶性肿瘤所需 的手术边缘,而需第2次手术
骨肿瘤有其独特的生物学特征
正确的诊断必须依靠临床、影像学和病理三结合的原 则,而相对侧重于病理。
因此,活检术非常重要!
活检前准备
活检手术不只是以获取诊断为目的的简单手术,而是 骨肿瘤整个诊疗计划的重要部分之一。
桡骨骨干肿瘤常需用掌侧切口来切除,在活检时要考 虑这一点。
中足及以远活检切口常取背侧纵向入路,后足活检入 路常通过外侧纵向入路。
标本送检
活检手术前,应对即将获取的组织标本作好送检准备。 标本一般不少于3块,一块用于冰冻切片以明确肿瘤性
析; 一块作石蜡包埋切片的常规HE染色及免疫组化、流式
或关节。 主要的血管神经束在活检中受到污染。
活检入路
若最终手术时未切除活检通道,肿瘤局 部复发率高达38%。
MitsuyoshiG,NaitoN,KawaiA, eta.l Accurate diagnosis of musculoskeletal lesions by core needle biopsy[ J]. J Surg Onco,l 2006, 94(1): 21-27.
尤其是皮肤因巨大肿瘤压迫或放疗而致营养受损时要 特别小心。 针距要小。减少切除活检切口的困难。
活检手术常见的并发症及预防
引流。 如果考虑为恶性肿瘤,应尽量避免使用引流装置。 如果必须安装引流装置,其通道应该邻近活检切口,
并与活检切口在同一直线上,以便将来与活检通道一 起切除。
小结
活检手术虽小,但并不简单。 要杜绝没有诊疗计划的活检手术。 要确保首次活检手术对往后的诊断及治
WHO2020骨肿瘤分类介绍

WHO2020骨肿瘤分类介绍自人类医学研究以来,骨肿瘤一直是一个备受关注的领域。
随着科技和医学的不断发展,对骨肿瘤的分类也在不断完善和更新。
在2020年,世界卫生组织(WHO)提出了一套更新的骨肿瘤分类,旨在更准确地描述和诊断骨肿瘤的各个亚型。
一、概述骨肿瘤是一类发生在骨组织中的肿瘤,它可以来源于骨骼本身的组织,也可以是骨骼周围的软组织扩展到骨内。
对骨肿瘤的准确分类是为了更好地了解其发病机制、提供精准的治疗方案以及预测病情发展。
在此背景下,WHO于2020年发布了最新的骨肿瘤分类。
二、WHO 2020骨肿瘤分类体系新的骨肿瘤分类体系将骨肿瘤分为两大类别:骨肿瘤原发性和骨肿瘤继发性。
1. 骨肿瘤原发性(Primary Bone Tumors)原发性骨肿瘤是起源于骨骼组织的肿瘤,通常为良性病变。
根据组织学和细胞学特征,这些肿瘤可以进一步分为多个亚型,如下所示:1.1. 骨肿瘤软骨成分(Bone Tumors with Cartilage Component)这类骨肿瘤以其明显的软骨成分而闻名。
包括良性的骨软骨瘤、软骨粘液样瘤以及恶性的软骨肉瘤。
1.2. 骨肿瘤成骨成分(Bone Tumors with Osteoid Component)该类别的骨肿瘤以其成骨性表现而著名。
其中包括骨纤维异常增生、成骨样软骨肉瘤、骨囊肿样骨肉瘤等。
1.3. 骨肿瘤透明细胞变异(Bone Tumors with Osteoclast-Rich Component)髓样肉瘤、透明细胞骨巨细胞瘤和漏斗状细胞巨细胞瘤等均属于这一类别。
1.4. 骨肿瘤小圆细胞成分(Bone Tumors with Small Round Cell Component)此类别的骨肿瘤主要是由小圆细胞所构成,包括了骨神经外胶质素肉瘤、骨原始神经外胶质瘤、骨肉瘤等。
1.5. 成骨细胞瘤及其他骨肿瘤(Osteoblastic Tumors and Other Bone Tumors)此类别包括了成骨细胞瘤、恶性骨肿瘤、畸形性成骨瘤等多种类型。
骨肿瘤的外科分期
骨肿瘤的外科分期
目前,治疗方案的制定已常规地按照外科分期。
外科分期将外科分级(grade,G)、外科区域(territory,T)和区域性活远处转移(metastasis,M)结合起来。
G分良性(G0)、低度恶性(G1)、和高度恶性(G2)。
G0(良性):组织学为良性细胞学表现,分化良好,细胞/基质之比为低度到中度;X线表现肿瘤为边界清楚或穿破囊壁或向软组织侵蚀;临床显示包囊完整,无卫星灶,无跳跃转移,极少远隔转移。
G1(低度恶性):组织学显示细胞分化中等;X线表现为肿瘤穿越囊壁,骨密质破坏;临床表现为生长较慢,活动性区域可向囊外生长,无跳跃转移,偶有远隔转移。
G2(高度恶性):组织学显示核分裂多见,分化极差,细胞/基质之比高;X线表现为边缘模糊,肿瘤扩散,波及软组织;临床表现为生长快,症状明显,有跳跃转移现象,常发生局部及远隔转移。
T是指肿瘤侵袭范围,以肿瘤囊和间室为分界。
T0:囊内;T1:间室内;T2:间室外。
M是转移。
M0:无转移;Ml:转移。
临床肿瘤学-骨肿瘤
第三十五章骨肿瘤第一节概论骨肿瘤包括的范围较广,凡与骨骼系统相关的组织的原发性良、恶性肿瘤或继发性肿瘤均包含其中。
此外,还包括了部分骨组织或其附属组织内的瘤样病损,这些瘤样病损严格地说不是肿瘤,或尚未确定其性质是否属于真正的肿瘤,但由于这些病损中的一部分在一定情况下也会转化为真正的肿瘤,可发生复发或恶变,加上这些瘤样病损在临床、影像和病理上有时会和一些骨肿瘤相混淆,故常合并在一起讨论。
一、外科分期Enneking提出的肌肉骨骼的外科分期是目前较为全面的评价骨肿瘤恶性程度的系统。
对肿瘤的手术选择应考虑到肿瘤的解剖部位,因为解剖学间室是预防微小肿瘤扩散的天然屏障,在长骨,这些屏障是皮质骨和关节软骨;在关节,是关节囊和关节软骨;在软组织,是大的筋膜间隔和肌腱的起止点。
这个外科分期系统是将外科病理分级(G),外科区域即肿瘤与解剖间室的关系(T)以及有无区域性或远处转移(M)结合起来,设计出G-T-M 外科分级系统,并以此作为制定治疗方案和术前选择手术方式的科学依据(表35-1)。
骨肿瘤的诊断主要依靠病理学检查,并结合临床和影象学诊断。
良性肿瘤用阿拉伯数字1、2、3表示,分别代表潜隐性,活动性和侵袭性。
恶性肿瘤用罗马字Ⅰ,Ⅱ,Ⅲ表示,Ⅰ为低度恶性,Ⅱ为高度恶性,Ⅲ表示存在区域性和转移性病损。
用G表示肿瘤的良恶性程度,G0属良性,G1属低度恶性,G2属高度恶性(表35-2)。
T表示肿瘤的侵袭范围,以肿瘤囊和间室为分界。
T0为囊内;T1为囊外但仍在间室内;T2为囊外和间室外。
转移是指有无区域转移或远处转移,用M表示。
M0为无转移,M1为转移。
表35-1 Enneking外科分期类别分期分级部位转移代号性质良性 123 G0G0G0T0T0T1~2M0M0M0~1G0T0M0G0T0M0G0T1~2M0~1迟发性活跃性侵袭性恶性ⅠAⅠBⅡA G1G1G2T1T2T1M0M0M0G1T1M0G1T2M0G2T1M0低度恶性,无转移,间室内低度恶性,无转移,间室外高度恶性,无转移,间室内ⅡB ⅢA ⅢBG2G1~2G1~2T2T1T2M0M1M1G2T2M0G1~2T1M1G1~2T2M1高度恶性,无转移,间室外低/高度恶性,有转移,间室内低/高度恶性,有转移,间室外表35-2 骨肿瘤外科病理分级良性(G0)低度恶性(G1)高度恶性(G2)骨瘤骨旁骨肉瘤典型骨肉瘤骨样骨瘤骨内骨肉瘤照射后骨肉瘤骨母细胞瘤骨软骨瘤继发性软骨肉瘤原发性软骨肉瘤内生软骨瘤去分化软骨肉瘤软骨母细胞瘤间充质软骨肉瘤骨膜性软骨瘤纤维瘤纤维肉瘤,分化良好未分化纤维肉瘤纤维瘤病恶性纤维组织细胞瘤,分化良好恶性纤维组织细胞瘤骨巨细胞瘤恶性骨巨细胞瘤未分化梭形细胞肉瘤腱鞘巨细胞瘤腱鞘巨细胞肉瘤滑膜肉瘤神经纤维瘤上皮样肉瘤神经肉瘤神经鞘瘤脊索瘤小泡细胞肉瘤脂肪瘤粘液样脂肪肉瘤多形性脂肪肉瘤血管脂肪瘤血管内皮细胞瘤血管肉瘤血管瘤血管外皮细胞瘤牙釉质瘤Ewing肉瘤平滑肌肉瘤横纹肌肉瘤二、治疗(一)治疗原则对肌肉骨骼系统肿瘤的治疗,应该采取以手术为主的联合治疗方法。
骨肿瘤分期

外科分级──G
G0 ──良性病变
临床:肿瘤边界清,有完整包膜,极少远处转移 X线表现:肿瘤界清,囊内生长呈膨胀性,罕见 穿破囊壁者 组织学表现:细胞分化良好,基质细胞比例正常, 核分裂相极少见
IUCC(International Union Against Cancer) 国际推广
外科分期目的
治疗的要求:手术时机、手术方法、切除范围的 选择;辅助治疗方法的选择
预后判断
标准化的要求:统一标准、有利于治疗资料和疗 效的交流(interinstitutional and interdisciplinary communication)
with C-arm guidance ,CT-guided biopsy 切取活检 切除活检
影像学:X-ray Lodwick 放射学分 级
Grade 1A, 1B, and 1C lesions represent benign lesions with edge characteristics ranging from well defined to poorly defined. Grade 2 lesions are low-grade malignant lesions with invasive features, particularly those with total penetration of the cortex. Grade 3 lesions are high-grade malignant lesions with invasive, permeative, and destructive features
骨肿瘤外科分期的肿瘤学意义
然而在不 同的专 家之间 ,保 肢治疗的方法却存 在相 当大 的差 异 。这是 由于专 家们 不同 的个人观点所 造成的 ,这些 观点大 多来源于他们个 人的经验而不是来 源于理论或临床 的研 究 。 积 累临床证据最好 的方式 是先 对手术 标本 的外科 边界 进行 分 析 ,然后 通过随访得 出结 论 。 目前 ,最现 实 的问题是 需要 根据理论结果确定 哪种手术方式效 果最好 ,但 又没 有足够可
山东医药 2009年第 49卷第 朝
骨肿 瘤外 科 分 期 的肿 瘤 学 意义
· 述 评 ·
牛 晓辉 (北京积 水 潭 医院 ,北京 100035)
[关键词 ] 骨肿瘤 ;恶性 ;外科分期 ;复发 ;转 移 [中图分类号 ] R738.1 [文献标 识码 ] A [文章编 号] 1002-266X(2009)08-0001-02
动系统功能病损 。普通 骨科 医生最 常犯 的错误 是 过分 地重 靠 的数据积 累来 提供 支持 。因为在几乎 所有的临床记 录中 ,
视肢体功能 的保 留及重建 ,而 忽略 了肿瘤 地治 疗 ,即 以牺牲 对 外科边界 的描 述多是 不确定 的 。造 成这 种情况 的原 因之
肿瘤治疗 的外科边界为代价 ,保 留维持 良好 功能所需 的组织 一 是缺 乏 已被证实有 效的外科边界评价标 准 ,另外 就科 学的范畴 。实 际上 , 骨肿瘤学所涉及 的内容 不仅 是骨科学 ,很重要而常常 又被忽 视的是其 同时属 于肿瘤学 范畴 的意 义 。因此 ,对 于骨肿 瘤 , 需要考虑肿瘤 的生长 方式 、侵袭性 、累及范 围、对运动 系统功 能的影响程度等多方 面内容。具体到恶性骨肿瘤 的治疗 ,医 生需要考虑彻底切 除肿瘤 …及 重建 因切 除肿瘤 所造成 的运
WHO骨肿瘤分类

恶性骨肿瘤
1 2 3
骨肉瘤
骨肉瘤是一种高度恶性的肿瘤,由恶性肉瘤和恶 性骨组织组成,通常在青少年期发病,生长迅速 ,容易发生转移。
尤因肉瘤
尤因肉瘤是一种低度恶性的肿瘤,由小圆形细胞 组成,通常在儿童和青少年期发病,生长速度较 慢,但容易发生转移。
骨髓瘤
骨髓瘤是一种恶性浆细胞肿瘤,通常在老年期发 病,生长速度较慢,但容易发生转移。
WHO骨肿瘤分类
汇报人:可编辑 2024-01-10
• 引言 • 骨肿瘤分类 • 骨肿瘤的症状和诊断 • 治疗和预后 • 预防和日常注意事项
01 引言
目的和背景
骨肿瘤分类是病理学领域的重要分支,用于对骨肿瘤进行科学、准确的诊 断和分类,为临床治疗提供依据。
随着医学技术的不断发展,骨肿瘤分类也在不断更新和完善,以适应新的 认识和需求。
恶性骨肿瘤的治疗
手术切除
手术切除是恶性骨肿瘤的主要治疗方法,包括根治性切除和保肢 手术。手术的目标是彻底切除肿瘤,同时尽量减少肿瘤复发的风
险。
化疗
对于某些恶性骨肿瘤,如骨肉瘤和尤因肉瘤,化疗是重要的辅助 治疗手段。化疗药物通过口服或静脉注射给予,以杀死癌细胞并
抑制其生长。
放疗
放疗可以用于缩小肿瘤、缓解疼痛或控制转移病灶。放疗通过 高能射线破坏癌细胞的DNA,从而抑制其生长和繁殖。
其他骨肿瘤
非骨化性纤维瘤
非骨化性纤维瘤是一种良性肿瘤 ,由成熟的纤维组织构成,通常 在青少年期发病,生长速度较慢 ,但容易复发。
动脉瘤样骨囊肿
动脉瘤样骨囊肿是一种良性肿瘤 ,由充满血液的囊状结构组成, 通常在青少年期发病,生长速度 较慢,但容易复发。
03 骨肿瘤的症状和诊断
骨髓瘤分期标准

骨髓瘤分期标准国际骨髓瘤工作组(IMWG)的分期标准主要是根据患者的临床特征和实验室检查结果来进行评估。
它将患者分为三个阶段,Ⅰ期、Ⅱ期和Ⅲ期。
Ⅰ期患者通常具有以下特征,血红蛋白水平较高(≥10.5g/dL)、血钙水平正常或轻度升高(≤12mg/dL)、骨骼损害较轻或无骨折、血清肌酐水平正常或轻度升高(≤2mg/dL)。
Ⅱ期患者通常具有介于Ⅰ期和Ⅲ期之间的特征。
而Ⅲ期患者通常具有以下特征,血红蛋白水平较低(≤8.5g/dL)、血钙水平较高(>12mg/dL)、严重的骨骼损害或多次骨折、血清肌酐水平较高(>2mg/dL)。
另一个常用的分期系统是国际分期系统(ISS),它主要是根据血清白蛋白水平和β2微球蛋白水平来进行评估。
ISS将患者分为三个阶段,Ⅰ期、Ⅱ期和Ⅲ期。
Ⅰ期患者的血清白蛋白水平较高(≥3.5g/dL)、β2微球蛋白水平较低(≤3.5mg/L);Ⅱ期患者的血清白蛋白水平介于Ⅰ期和Ⅲ期之间;Ⅲ期患者的血清白蛋白水平较低(<3.5g/dL)、β2微球蛋白水平较高(>5.5mg/L)。
对于骨髓瘤的治疗,分期是非常重要的,因为它可以帮助医生选择最合适的治疗方案。
一般来说,对于Ⅰ期和Ⅱ期的患者,常常可以选择局部治疗或化疗等方法进行治疗;而对于Ⅲ期患者,通常需要采取更加积极的治疗手段,如干细胞移植、靶向治疗等。
因此,对于骨髓瘤患者来说,及早进行分期评估,并选择合适的治疗方案是非常重要的。
总之,骨髓瘤的分期对于患者的治疗和预后具有非常重要的意义。
国际骨髓瘤工作组(IMWG)和国际分期系统(ISS)是目前广泛采用的骨髓瘤分期标准,它们可以帮助医生对患者的病情进行准确评估,并选择最合适的治疗方案。
因此,对于骨髓瘤患者来说,及早进行分期评估是非常重要的,可以帮助他们获得更好的治疗效果和生存质量。
WHO2020骨肿瘤分类介绍
WHO2020骨肿瘤分类介绍骨肿瘤是一类罕见但严重的疾病,影响着全球范围内的许多人。
世界卫生组织(WHO)在2020年发布了一份全面介绍骨肿瘤分类的报告,该报告对骨肿瘤进行了分类和描述。
本文将对该报告的内容进行介绍和总结。
首先,骨肿瘤是指发生在骨骼中的良性或恶性肿瘤。
骨肿瘤可分为原发性和继发性两类。
原发性骨肿瘤是起源于骨组织的肿瘤,而继发性骨肿瘤是由其他器官的肿瘤扩散到骨骼引起的。
根据WHO的分类标准,原发性骨肿瘤可以分为骨肉瘤、骨髓瘤和骨膜瘤等主要类型。
其中,骨肉瘤是最常见的骨肿瘤,通常在10至25岁的年轻人中发生,且多数发生在长骨中。
骨肉瘤通常是一种高恶性程度的肿瘤,早期症状不明显,发展到晚期时常出现骨痛、肿胀和活动受限等症状。
骨髓瘤是一种良性原发性骨肿瘤,多数发生在40岁以上的人群中。
它通常起源于骨骼中的浆细胞,骨髓瘤患者可出现贫血、骨痛和易骨折等症状。
虽然骨髓瘤是一种良性病变,但在部分患者中可能会演变为恶性肿瘤,称为浆细胞骨髓瘤。
骨膜瘤是一种较为罕见的原发性骨肿瘤,多发生在中老年人中。
它通常起源于骨膜,即覆盖在骨骼表面的薄膜。
骨膜瘤多数为良性肿瘤,但在少数患者中也可能会恶变。
此外,继发性骨肿瘤也是骨肿瘤分类中的一个重要部分。
肺癌、乳腺癌和前列腺癌等常见的恶性肿瘤常会扩散到骨骼并形成继发性骨肿瘤。
继发性骨肿瘤的临床表现通常与原发性骨肿瘤不同,患者可能会出现骨痛、骨折和骨质疏松等症状。
除了按照病理类型进行分类,WHO还对骨肿瘤进行了分期。
分期是评估和描述肿瘤扩散程度及预后的重要指标。
在骨肿瘤分类中,分期可从骨骼组织内的肿瘤扩散程度、深度和潜在风险等方面进行评估。
总结起来,WHO在2020年发布的骨肿瘤分类报告为我们提供了一个全面了解骨肿瘤的工具。
通过对原发性骨肿瘤和继发性骨肿瘤的分类和描述,我们可以更好地理解不同类型骨肿瘤的特点和发展规律。
此外,通过对骨肿瘤的分期,我们可以对患者的疾病状态和预后进行更为准确的评估。
第二十八章 骨与软组织肿瘤的临床分期
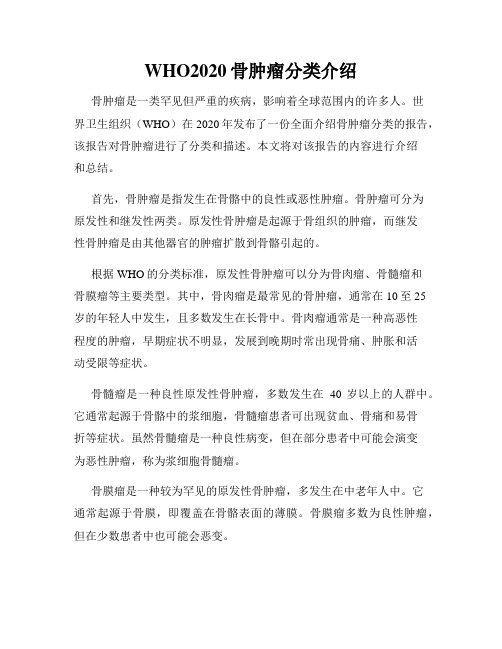
第二十八章骨与软组织肿瘤的临床分期骨肿瘤的临床治疗取决于病变的类型、组织学分期以及在宿主体内局部发展的程度。
评估以上情况的过程称为肿瘤分期。
美同肿瘤联合委员会(AJCC)提出的肿瘤-淋巴-转移瘤(TNM)分期标准在骨肿瘤的应用方面具有一定的局限性(表28-1)。
该分期系统中,T1期指局限于皮质内的肿瘤,T2期指皮质外肿瘤,发生在骨表面而并不侵犯骨内部的肿瘤准确分期。
在骨肿瘤中没有Ⅲ期肿瘤,Ⅰ、Ⅱ、Ⅳ期肿瘤属于转移性肿瘤。
此外,该分期系统中的淋巴标准很难用于骨肉瘤,因为后者很少通过淋巴转移。
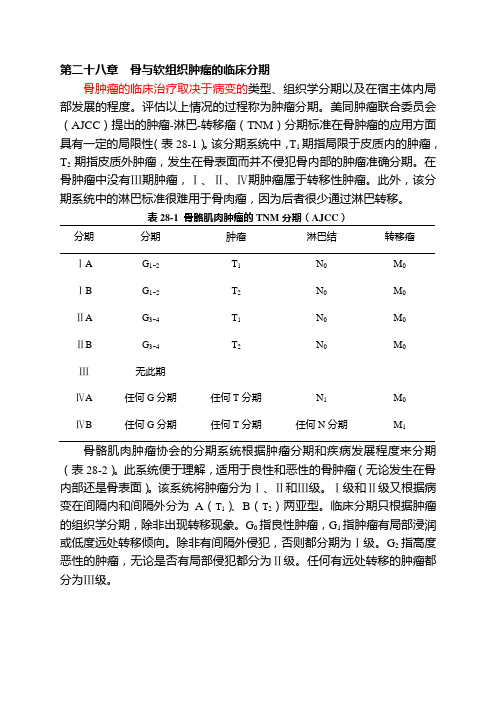
表28-1 骨骼肌肉肿瘤的TNM分期(AJCC)分期分期肿瘤淋巴结转移瘤ⅠA G1~2T1N0M0ⅠB G1~2T2N0M0ⅡA G3~4T1N0M0ⅡB G3~4T2N0M0Ⅲ无此期ⅣA 任何G分期任何T分期N1M0ⅣB 任何G分期任何T分期任何N分期M1骨骼肌肉肿瘤协会的分期系统根据肿瘤分期和疾病发展程度来分期(表28-2)。
此系统便于理解,适用于良性和恶性的骨肿瘤(无论发生在骨内部还是骨表面)。
该系统将肿瘤分为Ⅰ、Ⅱ和Ⅲ级。
Ⅰ级和Ⅱ级又根据病变在间隔内和间隔外分为A(T1)、B(T2)两亚型。
临床分期只根据肿瘤的组织学分期,除非出现转移现象。
G0指良性肿瘤,G1指肿瘤有局部浸润或低度远处转移倾向。
除非有间隔外侵犯,否则都分期为Ⅰ级。
G2指高度恶性的肿瘤,无论是否有局部侵犯都分为Ⅱ级。
任何有远处转移的肿瘤都分为Ⅲ级。
表28-2 骨骼肌肉肿瘤的Enneking分期系统分期分期部位良性G0ⅠA G1T1ⅠB G1T2ⅡA G2T1ⅡB G2T2Ⅲ转移(任何G分期)转移(任何T分期)。
骨肿瘤(长征医院

连续性
中断性
肿瘤基质
大致判断肿瘤类型
结合其他征象
结合其他影像方法
类骨基质
弥漫均匀,呈烟雾状、云朵 状或象牙状钙化。
纤维源性基质
均匀透亮、较少钙化。 网织骨或纤维骨造成毛玻璃状改 变或高达骨样密度。
软骨基质
点状、絮状、环状或孤状钙
化。
软组织肿块
X线提供的诊断信息
病变的部位 病变的边缘 破坏的类型 骨膜反应 肿瘤基质 侵犯软组织的范围及其性质。
骨肿瘤X线检查方法
常规正侧位片,加摄斜位、切线位、点 片 放大摄影或体层摄影检查:早期或细节 高仟伏和钼靶软组织照片:肿瘤内部和 软组织肿块。 CR:可扩大影像的信息内容 血管造影:显示血供和肿瘤染色
边缘模糊
生物活性高,见于巨细胞瘤、骨肉瘤、 软骨肉瘤、纤维肉瘤、恶性纤维组织细 胞瘤,常提示为恶性
骨质破坏
肿瘤细胞直接作用
破骨细胞反应性活动增加
肿瘤周围组织的活动性充血
皮质骨破坏出现较早 松质骨破坏晚(矿物质含量丧失70% 以后)
骨质破坏的类型
与肿瘤的生长速度有关。
不是任何一种肿瘤的特征。
幼年骨
软骨母
成熟骨
骨软骨瘤
骨内腱 鞘囊肿
巨细胞瘤恶纤 组
骨肉瘤
骨囊肿 ABC或软骨黏液纤维瘤
骨膜软骨瘤 内生软骨瘤
纤维肉瘤
骨髓瘤
骨样骨瘤
骨母细胞瘤 尤文氏肉瘤 纤维结构不良 纤维结构不良 骨化性纤维瘤
造釉细胞瘤 转移瘤 骨瘤 淋巴瘤
骨肉瘤的分型

骨肉瘤的分型
骨肉瘤是一种恶性肿瘤,常发生在长骨的干骺端或近干骺端,是
儿童和青少年时期最常见的骨肿瘤之一。
根据肿瘤的组织学特征,骨
肉瘤可分为多种类型。
1. 骨原性骨肉瘤
骨原性骨肉瘤是最常见的一种骨肉瘤。
这种骨肉瘤通常起源于干
骺端的骨组织,具有明显的浸润性和转移能力。
常见症状有骨痛、可
触及的肿块和关节疼痛。
治疗方案主要包括手术切除、化疗和放疗。
2. 软骨母细胞型骨肉瘤
软骨母细胞型骨肉瘤是一种罕见的骨肉瘤,起源于软骨组织或其
前体细胞,通常发生在长骨的干骺端。
与骨原性骨肉瘤相比,此类型
骨肉瘤的预后较好。
常见症状是慢性关节疼痛和可触及的软组织肿块。
治疗方案包括手术切除和化疗。
3. 少见的骨肉瘤类型
除了上述两种较为常见的骨肉瘤类型外,还有一些罕见的骨肉瘤
类型,例如纤维型骨肉瘤、软骨瘤样骨肉瘤、小圆细胞型骨肉瘤等。
这些骨肉瘤类型发生的部位和症状差异较大,但治疗方案通常包括手
术切除、化疗和放疗。
总体来说,骨肉瘤是一种常见的骨肿瘤,且分类繁多。
医生要通
过临床症状和影像学检查来确诊,并根据不同类型的骨肉瘤采取不同
的治疗方案。
早期发现和及时治疗可以提高治愈率,对于骨肉瘤患者来说,注意保持良好的营养状态和积极心态也是至关重要的。
骨肿瘤分期

骨肿瘤分期
良性肿瘤分期:
1级:静止性肿瘤,有完整的包囊;
2级:生长活跃,仍位于囊内或者为自然屏障所阻挡;
3级:具有侵袭性,可穿破皮质或者间隔;
分级(G):根据肿瘤的生长速度及侵袭性,良性肿瘤G0,低度恶性为G1,高度恶性G2 外科部位(T):完整的纤维组肿囊或者反应骨包绕T0;肿瘤位于囊外间隔内(肌间隔或者骨旁间隔及潜在的间隔内)T1;间隔外,肿瘤位于囊外,超过肿瘤的间隔或者起源于分界不清的间隔T2
转移(M):包括局部淋巴结转移和远处转移,无局部及远处转移为M0,有局部及远处转移为M1
恶性肿瘤分期:
IA(G1,T1,M0):低度恶性,间室内病变,无转移;
IB(G1,T2,M0):低度恶性,间室外病变,无转移;
IIA(G2,T1,M0):高度恶性,间室内病变,无转移;
IIB(G2,T2,M0):高度恶性,间室外病变,无转移;
IIIA(G1,T1,M1):间室内病变伴有转移的恶性肿瘤;
IIIB(G1或G2,T1或T2,M1):间室外病变伴有转移的恶性肿瘤。
骨肿瘤的分类

骨肿瘤的分类骨肿瘤是指发生在骨骼系统中的肿瘤,根据其性质和发生部位的不同,可以将骨肿瘤分为多种类型。
本文将就骨肿瘤的分类进行详细介绍。
一、原发性骨肿瘤原发性骨肿瘤是指起源于骨骼系统的肿瘤,不是由其他部位的恶性肿瘤转移至骨骼系统所致。
根据肿瘤的良性或恶性性质,原发性骨肿瘤可分为良性骨肿瘤和恶性骨肿瘤。
1. 良性骨肿瘤良性骨肿瘤是指生长缓慢、不具有侵袭性和转移性的骨肿瘤。
常见的良性骨肿瘤包括骨母细胞瘤、骨骺瘤、骨囊肿等。
良性骨肿瘤多数不需要立即治疗,但有些病例需要手术切除或其他治疗手段。
2. 恶性骨肿瘤恶性骨肿瘤是指能够侵入周围组织、破坏骨骼结构并发生转移的骨肿瘤。
最常见的恶性骨肿瘤是骨肉瘤,其他还包括骨源性肉瘤、骨巨细胞瘤等。
恶性骨肿瘤需要积极治疗,一般采取手术切除、放疗和化疗等综合治疗方法。
二、继发性骨肿瘤继发性骨肿瘤是指由其他部位的原发性肿瘤转移至骨骼系统所致的肿瘤。
常见的原发性肿瘤有乳腺癌、肺癌、前列腺癌等。
转移至骨骼系统的肿瘤多数为恶性肿瘤,且具有侵袭性和转移性。
继发性骨肿瘤的治疗主要是针对原发性肿瘤进行治疗,如手术切除、放疗、化疗等。
三、良性骨囊肿良性骨囊肿是一种常见的骨肿瘤,通常发生在骨骼的长骨中,如股骨、胫骨等。
骨囊肿是由骨骼内的液体积聚形成的囊性病变,其内部充满液体。
大多数骨囊肿无症状,被发现时已经长大。
治疗骨囊肿的方法主要有手术切除、骨填充物填充和硬化治疗等。
四、骨肉瘤骨肉瘤是一种高度恶性的骨肿瘤,多见于发育期的儿童和青少年。
骨肉瘤常见于长骨的近端,如股骨、胫骨等。
其主要症状包括局部疼痛、肿胀和活动受限。
治疗骨肉瘤的方法包括手术切除、放疗和化疗等。
早期发现和积极治疗对提高患者生存率具有重要意义。
五、骨巨细胞瘤骨巨细胞瘤是一种常见的良性骨肿瘤,常见于长骨的骨骺和骨干部位。
骨巨细胞瘤的症状包括局部疼痛、肿胀和活动受限。
治疗骨巨细胞瘤的方法主要有手术切除、介入治疗和放疗等。
骨肿瘤可分为原发性骨肿瘤和继发性骨肿瘤,原发性骨肿瘤又可细分为良性骨肿瘤和恶性骨肿瘤。
bcs分类标准
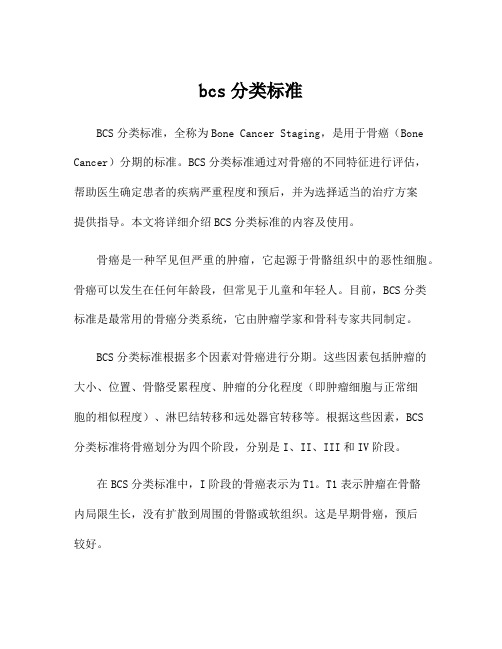
bcs分类标准BCS分类标准,全称为Bone Cancer Staging,是用于骨癌(Bone Cancer)分期的标准。
BCS分类标准通过对骨癌的不同特征进行评估,帮助医生确定患者的疾病严重程度和预后,并为选择适当的治疗方案提供指导。
本文将详细介绍BCS分类标准的内容及使用。
骨癌是一种罕见但严重的肿瘤,它起源于骨骼组织中的恶性细胞。
骨癌可以发生在任何年龄段,但常见于儿童和年轻人。
目前,BCS分类标准是最常用的骨癌分类系统,它由肿瘤学家和骨科专家共同制定。
BCS分类标准根据多个因素对骨癌进行分期。
这些因素包括肿瘤的大小、位置、骨骼受累程度、肿瘤的分化程度(即肿瘤细胞与正常细胞的相似程度)、淋巴结转移和远处器官转移等。
根据这些因素,BCS分类标准将骨癌划分为四个阶段,分别是I、II、III和IV阶段。
在BCS分类标准中,I阶段的骨癌表示为T1。
T1表示肿瘤在骨骼内局限生长,没有扩散到周围的骨骼或软组织。
这是早期骨癌,预后较好。
II阶段的骨癌表示为T2。
T2表示肿瘤扩散到周围骨骼,但尚未扩散到远处器官。
这是局部进展的骨癌,预后较I阶段差。
III阶段的骨癌表示为T3。
T3表示肿瘤扩散到远离原位的骨骼区域,但仍然限制在一个特定的区域。
这是进一步扩散的骨癌。
最后,IV阶段的骨癌表示为T4。
T4表示骨癌已经扩散到远处器官,如肺、肝或其他骨骼。
这是晚期骨癌,预后最差。
除了T分期外,BCS分类标准还包括N分期和M分期。
N分期表示淋巴结转移的情况,M分期表示远处器官转移的情况。
根据N分期和M分期的不同组合,骨癌可以进一步划分为N0、N1、M0和M1四个子分期。
N0表示没有淋巴结转移,N1表示有淋巴结转移。
M0表示没有远处器官转移,M1表示有远处器官转移。
根据这些子分期的不同组合,可以更准确地确定骨癌的预后和治疗方案。
BCS分类标准的使用有助于医生对骨癌进行系统评估,并为患者制定个体化的治疗方案。
早期骨癌通常可以通过手术切除和放疗进行治疗。
骨肿瘤【61页】
骨巨细胞瘤X线特点
溶骨性 偏心性 膨胀性 皂性改变
骨巨细胞瘤
骨巨细胞瘤的手术治疗
骨巨细胞瘤
骨巨细胞瘤目前存在的问题
肿瘤分级与复发、转移的关系? 骨巨细胞瘤放疗后是否导致恶变?
骨肉瘤
1 骨肉瘤起发于原始间充质细胞的成 骨细胞类,故名成骨肉瘤,恶性程度非 常高。其特征为从肿瘤细胞直接形成 骨和类骨.
2 多见于10—20岁,在成人也可因放射治
疗,Paget氏病,甚至个别经久不愈的慢性骨 髓炎引起骨肉瘤。
3 好发部位 股骨、胫骨和肱骨近端 是最常见发病部位,大约有50 %- 70%骨肉瘤发生在膝关节周围
4 在组织学上可以很大的变异,表现为 肿瘤不仅可产生大量肿瘤性骨或瘤性类骨, 还或产生软骨,纤维组织,粘液样组织。
血沉和碱性磷酸酶可作为 观察骨肿瘤疗效的动态指标
病理学检查
1 常规组织学切片 2 组织化学检查 3 免疫组织化学
骨肿瘤与X线病理
有些肿瘤产生类骨或肿瘤骨称为反应骨, 在X线片上表现为高密度区。
有些骨肿瘤破骨或使骨吸收, 在X线片上表现为低密度区
骨膨胀性改变
葱皮样改变
骨肿瘤刺激骨膜是阶段性,使 骨膜阶段性形成板层状新骨,
其生物学特性为具有较强侵蚀性,采 通常的刮除法复发率较高。
少数病例可出现局部恶性变或肺转移, 属于临界性肿瘤。
骨巨细胞瘤的分级
Jaffe于1940年提出的分级主要 依据巨细胞的数量多少和基质细胞 的分化程度。
Jaffe分级的临床意义和存在的问 题最新的研究进展
骨巨细胞瘤征象
20—40成人(3/4),10岁以下儿童罕见 股骨下端最多见,其次为胫骨上端及挠骨下端, 三处占全部骨巨细胞瘤的60—70% 病灶位于骨端,邻关节面(不累及骼后的骨的巨 细胞瘤诊断基本不存立)。 病灶延伸至骨突内 。
骨肉瘤AJCC分期(TNM)
骨肉瘤AJCC分期(TNM)前言2018 年,中国临床肿瘤学会(CSCO)更新了肺癌、乳腺癌、胃癌、结直肠癌诊疗指南,新发布了肾癌、头颈肿瘤、甲状腺癌、骨肉瘤、胰腺癌、肝癌、血液肿瘤、食管癌等八个诊疗指南。
我们将经典型骨肉瘤诊疗指南中「骨肉瘤AJCC 分期(TNM)」进行了节选,方便广大病理老师们查阅与参考。
骨肉瘤的分期•美国癌症联合委员会(AJCC)骨肿瘤分期系统(第八版)(不包括淋巴瘤和骨髓瘤)•骨及软组织肿瘤外科分期系统(SSS 分期)骨肉瘤的分期策略注释1对新诊断骨肉瘤患者进行肿瘤分期是必要的,具有十分重要的意义。
不同分期的骨肉瘤的预后和治疗原则有很大差别,因此,准确而完整的分期是制定和实施有效治疗的重要基础。
分期还可提示肿瘤的恶性程度、局部受累、区域和远隔转移情况,这些与患者的肿瘤学预后密切相关。
骨肉瘤通常使用 SSS 分期系统和 AJCC 分期系统,两种分期系统具有不同的特点。
2Enneking 提出的SSS 外科分期系统是目前临床上使用最为广泛的分期系统,此分期系统与肿瘤的预后有很好的相关性,不同分期肿瘤5 年生存率有显著差异。
此分期系统被美国骨骼肌肉系统肿瘤协会(Musculoskeletal Tumor Society,MSTS)及国际保肢协会(International Society of Limb Salvage,ISOLS)采纳,又称MSTS 外科分期。
此系统根据肿瘤的组织学级别、局部累及范围和有无远隔转移对恶性骨肿瘤进行分期。
骨肉瘤完全位于骨内的称为间室内(A)肿瘤,而穿透骨皮质的称为间室外(B)肿瘤;通过影像学分期,没有转移证据的患者被归于M0,有转移者为 M1。
SSS 分期的主要特点如下:①肿瘤位于间室内或间室外能体现骨肉瘤特有的生物学行为特征,对于治疗方案的选择和肿瘤切除范围的计划有指导意义;②转移灶通常位于肺、淋巴结或髓内的“跳跃”病灶,预示着预后不良。
3美国癌症联合委员会(AJCC)分期系统是目前国际上最为通用的肿瘤分期系统,因此临床上更为肿瘤内科医生所熟悉,但在骨肿瘤中不常用。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
CT in evaluating the lungs for metastases
• More accurate than chest radiographs • May produce false-positive results
when small lung nodules are detected. • Follow-up CT scans are useful in monitoring the nodules.
室内
间室内── T1
• 皮质骨内,未穿破骨膜和骨髓腔 • 关节内,未穿破关节囊
• 骨旁间隙内,未进入骨皮质,未穿破骨膜
侵犯肌、筋膜
间室外── T2
• 间室内病变穿破解剖学间室:
肿块本身穿出 反应带超出原发间室 意外创伤和不恰当的手术切除污染多个间室 病变或其反应带临近或侵犯主要血管、神经束者 一些缺乏阻止肿瘤扩散的内在屏障的解剖学部位, 如腹股沟等
sharply demarcated from the surrounding healthy tissue. Malignant lesions are typically more extensive and involve surrounding tissue to a greater extent than do benign lesions. MRI signal intensity alone is not reliable in distinguishing benign tumors and malignant tumors.
骨肿瘤的外科分期 Surgical Staging of Bone Tumors
中山医院骨科 姜南春
Enneking-Musculoskeletal Tumor Staging System
骨与软组织肿瘤TNMG分期系统
• AJCC(American Joint Committee on
Cancer) 提出
影像学:X-ray Lodwick 放射学分 级
• Grade 1A, 1B, and 1C lesions represent •
•
benign lesions with edge characteristics ranging from well defined to poorly defined. Grade 2 lesions are low-grade malignant lesions with invasive features, particularly those with total penetration of the cortex. Grade 3 lesions are high-grade malignant lesions with invasive, permeative, and destructive features
1期(G0T0M0)
1期(G0T0M0)
• 复杂,对手术治疗无指导价值 • 很少使用
肌肉骨骼系统肿瘤的外科分期 (MTS分期系统)
• 佛罗里达大学,Enneking,1977 • MTS(Musculoskeletal Tumor Society)试
用 • Clinical Orthopedics and Related Research,1980 • AJC(American Joint Committee)修订 • IUCC(International Union Against Cancer) 国际推广
• Radionuclide bone scans • Ultrasonography • Angiography • Positron Emission Tomography
外科分级──G
• G0 ──良性病变
临床:肿瘤边界清,有完整包膜,极少远处转移 X线表现:肿瘤界清,囊内生长呈膨胀性,罕见穿破 囊壁者 组织学表现:细胞分化良好,基质细胞比例正常, 核分裂相极少见
外科分级──G
• G1 ──低度恶性病变
临床:肿瘤可向囊外生长,但生长速度较慢,可有 软组织肿块,偶有远处转移 X线表现:肿瘤界欠清,呈侵袭性生长 组织学表现:细胞分化中等,基质细胞较多,可见 核分裂相但较少
外科分级──G
G2 ──高度恶性病变
临床:症状明显,肿瘤生长快,有跳跃性生长和软组织 肿块,常早期就发生局部和远处转移
排除范围
• 来源于骨髓、网状内皮组织的肿瘤
白血病、淋巴瘤、骨髓瘤、尤文肉瘤、未分化小圆细胞 肉瘤
• 转移性肿瘤
Enneking──G-T-M外科分期系统
• G(Histologic Grade):分级──肿瘤的外科分级 • T(Anatomic Site):肿瘤与解剖学间室的关系
• M(Metastasis):肿瘤有无转移,包括区域和远处
• •
≠组织学分级──Broder’s分级 ≠放射学分级──Lodwick’s分级 G0:良性病变;G1:低度恶性;G2:高度恶性 恶性肿瘤外科分级通常依从于组织学分级。但是, 如组织学表现偏良性而放射和临床表现为高度侵 袭性者应定为高度恶性
组织学
• 细针穿刺活检
影像引导下穿刺活检如Fluoroscopy with C-arm guidance ,CT-guided biopsy • 切取活检 • 切除活检
影像学:MRI
accurate depiction of the soft tissues allows sensitive detection of soft tissue extension and medullary involvement by tumor
MRI良恶性影像学特征
• Benign lesions are well defined and • •
MRA
• Provide additional information
regarding neurovascular bundle involvement. • Assessing peripheral vascular branches and tumor neovascularity.
其他影像学检查
影像学:CT
• Evaluation of local disease in detail • Assessing the lungs for pulmonary
metastases
CT in evaluation of local disease
Complements radiography • Assess disease in areas not easily visualized with radiography, eg, the spine and pelvis • CT is better in assessing the type of cortical destruction and the presence of matrix mineralization. • CT is also helpful in determining the internal contents of some lesions.
转移
Enneking分期
• 良性骨肿瘤
1期:潜隐性 2期:活动性 3期:侵袭性
• 恶性骨肿瘤
Ⅰ期( ⅠA ⅠB ):低度恶性 Ⅱ期( Ⅱ A ⅡB ):高度恶性 Ⅲ期( Ⅲ A ⅢB ):有局部和远处转移 A:间室内; B:间室外
外科分级──G
• 临床或外科分级 • 在恶性肿瘤反映生物学侵袭程度 • 组织学、放射和临床三结合
MRI对分期的价值
• Assessing local spread of tumor (Enneking
• •
sites T1 and T2). Accurately detecting tumor involvement of neurovascular structures, muscle compartments, growth plates, and joints. Usually accurately depicts intramedullary spread and soft tissue extension of tumor
重要的放射学征象
• Pattern of destruction (geographic or not • • •
geographic, appearance of marginal interface zone) Penetration of cortex by lesion Absence or presence of a sclerotic rim Absence or presence and extent (if present) of the expanded cortical shell
X线表现:病变侵袭破坏明显,骨膜反应,软组织肿块 组织学表现:细胞分化极差,基质细胞多,核分裂相多 见
肿瘤与解剖学间隙的关系──T
• T0:良性囊内和间室内病变 • T1:间室内病变 • T2:间室外病变
间室内── T1
• 无真性包膜,但有假包膜 • 反应带内有指状突起或卫星灶
• 原发病灶和反应带均局限在病灶的原发间
良性骨肿瘤
1期:潜隐性(latent)---G0 T0 M0
2期:活动性(active)--- G0 T0 M0 3期:侵袭性(aggressive)--- G0 T1 或T2 M0 或 M1
1期── G0T0M0 ,良性潜隐性
• 临床:无症状,无功能障碍,无意中发现,缓
• •
慢增大,有接触抑制,无骨皮质变形 放射学:平片示病灶界限清楚、形状和边界规 则,有皮质骨样反应骨包围(LodwickⅠA); CT示病灶呈均质性,无骨皮质穿破 组织学:基质成熟,分化好,细胞-基质比例 低,无恶性细胞学表现,如:细胞核深染、核 分裂相、间变、多行性;病灶被成熟的纤维组 织或皮质骨包围,极少反应性间质浸润、炎症 反应和新生血管形成