Sikadur 42HE,part C
新概念第二册第42课课件Lesson42

C. would be warned, had not taken
D. would have been warned, had not taken
•If you had enough money, what B
?
A. will you buy
B. would you buy
C. would you have bought
•He doesn’t speak very clearly. That’s why people don’t understand
him.
•If he
more
, people
.
•That phone is too expensive, so I’m not going to buy it.
•If the phone
difference
[θrəʊ]
•必会词组: tell the difference between A and B 区分A与B
•Indian (a)印度的
•India
Part 2
Part 3
Food and talk
What happened when the snake charmer began to play jazz?
[θrəʊ]
obviously
adv.显然
obvious (a)明显的 •一个明显的错误 •一个明显的原因 •必备句型: •It is obvious that…很明显,显然 •很明显手术很成功 •It is obvious that the operation is successful •显然他后悔买了这个房子 •显然他吓了一跳(get a fright)
As we had had a long walk through one of the markets of old Delhi, we stopped at a square to have a rest. After a time, we noticed a snake charmer with two large baskets at the other side of the square, so we went to have a look at him.
新概念英语第二册Lesson42
• As soon as he saw us, he picked up a long pipe which was covered with coins and opened one of the baskets.
• When he began to play a tune, we had our first glimpse of the snake. • It rose out of the basket and began to follow the movements of the pipe.
Jazz
•a music genre that originated(起源) at the beginning of the 20th century •in the early 20th century jazz has spawned(产生) a variety of subgenres(亚种) Louis Armstrong •an American jazz trumpeter(吹小号 的人) and singer from New Orleans •in the 1960s, he was widely regarded as a profound(深切) influence on popular music in general.
• We were very much surprised when the snake charmer suddenly began to play jazz and modern pop songs. • The snake, however, continued to 'dance' slowly.
beatles
•an English rock band, formed in Liverpool in 1960 •one of the most commercially successful and critically acclaimed acts in the history of popular music
西卡214金属灌浆料说明
wTel: +86 20 82266066Fax: +86 20 82266022Page: 1 / 21.1Chemical Character: modified epoxy resin on bisphenol A.1.2Form: liquid.1.3Color: colorless1.4Odor: slight2PHYSICAL AND SAFETY DATA (Not technical specifications. Unless specified tested at 20℃. All temps quoted in ℃)2.1Changes in Physical state:2.2Density (20℃) Kg/L: 1.13 g/ml Bulk density (kg/m3 ): kg / m32.3Vapor pressure:2.4Viscosity(23℃): 550±60 mPa.s,2.5Water solubility: insoluble2.6PH Value: 62.7Flash point:2.8Ignition Temp.:2.9Explosion limits: N/A2.10Thermal decomp.: :>170℃2.11Hazardous decomposition products:2.12Hazardous reaction:2.13Further information:3TRANSPORTIMDG: UN No.: ICAO/IATA: Tremcard No.:GGVE/GGVS: RID/ADR: ADNR:Other information:4.REGULATIONS5PROTECTIVE MEASURES, STORAGE AND HANDLING5.1Technical protective measures:DO NOT TRANSFER INTO UNLABELED CONTAINERS.5.2Personal: Respiratory protection: Not applicableEye protection: Tightly fitting protecting goggles.Hand protection: Gloves, e.g. rubber.Other:5.3Industrial hygiene: EXPERTS ALWAYS WEAR THE RIGHT PROTECTIVE CLOTHING.Observe good house keeping and general hygiene guidelines.5.4Protection against fire and explosion: N / A5.5Disposal: Product: must be disposed of in a special waste disposal unit in accordance with the corresponding regulationPackaging: completely emptied packagings can be given for recycling. Packaging that cannot be cleaned shouldbe disposed of as product waste.6MEASURES IN CASE OF ACCIDENTS AND FIRES6.1After spillage: All chemical spillages must be dealt with as soon as possible to prevent contamination. Damage or stainingof the area affected (especially with liquid products). Attention is drawn to the Control of Pollution Act 1974, the provisionThe information in this safety data sheet respects the actual status of knowledge at the date of publication. They do not imply any warranty. For warranty obligations the specific product descriptions and General Status Conditions are of relativance only.of which is enforced by local authorities. Sweep up spillages. Place in polyethene bags for disposal to an authorized waste site. Wash the area with strong industrial detergent and hot water.6.2 Extinguishing media suitable: compatible with all usual extinguishing media.Not be used: N/A6.3 First aidIngestion : Do not induce vomiting. Summon a doctor immediately.Eye contact : Rinse immediately with opened eyelids under running water for 15 minutes and summon a doctorimmediately.Skin contact : Remove contaminated clothing. Wash off immediately with soap and water. Consult a doctor if skinirritation persists.Inhalation : Remove to fresh air. Give oxygen if required. In the event of symptoms take medical treatment.6.4 Further information : Sika Limited products are generally safe to use provided certain precautions normally taken whenhandling chemicals are observed. Unless specified products should not come into contact with drinking water, foodstuffs or food equipment and measures should be taken to prevent skin contact, since people with particularly sensitive skin may be affected. The use of barrier creams, goggles and industrial gloves are recommended. The skin should be cleansed at the end of each working period using a suitable industrial cleanser or warm water and soap, the use of solvents to clean the skin is not recommended. Adequate ventilation of the working area is recommended. Take careful note of all safety information on data sheets and labels.7 INFORMATION ON TOXICITYContact with eyes, skin and mucous membranes may cause slight irritation. Sensitization and allergic reaction may occur.8 INFORMATION ON ECOLOGICAL EFFECTSAddition informationDo not allow to enter waste water drain, waterways or soil.9 FURTHER INFORMATIONAll statements are based on our experience to date. Form based on DIN 52900.The information contained in this Safety Data Sheet corresponds to our level of knowledge at the time of publication. Allwarranties are excluded. Our most current General Sales Conditions shall apply. Please consult the Technical Data Sheet prior to any use and processing.SAFETY DATA SHEET Sikadur 42HE, Part A01/2007Sika Ltd., China No.96,JunDa Road, Eastern Section, GET Guangzhou, China, post code: 510530 Tel: +86 20 82266066 Fax: +86 20 82266022 Pages: 2/2。
新概念英语第二册课件Lesson42(共31页)

★pole n.(地球的)极 • the South Pole 南极 • the North Pole 北极 • Pole Star 北极星 ★explorer n. 探险家, 探测者, 探测器 • explore v.探险, 探测, 探究 • exploration n.(科研相关)探险,探求,开发 • adventure n.冒险(追求刺激) • venture n. 冒险(为了财富)
• stay in bed = lie in bed • 当我坐在篝火旁的时候,我的狗躺在我的旁边。
• While I sat by the fire, my dog lay beside me. • ③ vt. 撒谎 • tell a lie 撒谎 • You lied. = You lied to me.你骗人! 你撒谎! • You,liar! 你, 骗子! • ④ n.谎言
课文讲解
1、In 1929, three years after his flight over the North Pole, the American explorer, R.E. Byrd, successfully flew over the South Pole for the first time.
musical
adj. 精通音乐的
market
n. 市场,集市
snake charmer 玩蛇者(通常借音乐控
制)
pipe
n. (吹奏的)管乐器
tune
n. 曲调
glimpse
n. 一瞥
snake
n. 蛇
movement
n. 动作
continue
v. 继续
dance
v. 跳舞
Sikadur 42HE
Sikadur® 42 HE
环氧树脂灌浆料
简介
一种高强度的灌浆料,无溶剂型,三组份,主要用于固定大型设备、往复式机床等震动
剧烈设备的基础,环氧灌浆料无收缩、微膨胀、高强度,固化快,具有良好的流动性。
* 作为自流平树脂灌浆料,应用于:混凝土、石头面、砂浆、抹灰层、钢、铝板、石棉
组份 A:
1.13±0.05
组份 B:
1.0±0.05
组份 C:
1.75±0.05
组份 A+B+C:
2.00±0.05
粘度(20°C) 适用期(5公斤)
普通型
缓慢型
30°C
25分钟
35°C
20分钟
20°C
45分钟;
20°C
60分钟
10°C
90分钟
Sikadur® 42 1/2
受限 粘贴强度 强度
最低基面温度:+5°C(普通型)和+20°C (缓慢型)
容许的最高基面温度:+40°C
每次灌浆的最高厚度为:4cm(20°C 时)
新混凝土的最低保龄期:3-6周(与气候有关)
普通型和缓慢型均可施工在湿的基面上。
混凝土 20°C 约4牛顿/平方毫米
普通型
缓慢型
抗压强度
20°C
80Mpa
35°C
抗弯强度
20°C
30Mpa
30°C
抗压弹性模模量20°C:2000Mpa
热膨胀系数20°C-60°C:5 310¯5
抗压
普通型:
80Mpa 80Mpa
缓慢型;
注意
关于西卡产品的应用和最终使用的建议,均基于西卡对于正常条件下储存、处理和使用西卡 产品时的知识和经验所善意提供的。鉴于实际使用中的物料、底层和工地存在各种差异,所 以本信息,或者任何书面建议,或者任何其他建议,并不意味着对商品性或者任何特定目的 适用性的担保,也不意味着任何法律责任的承担。应尊重第三方财产权。所有定单均须遵循 西卡当前的销售及交付条款。使用者应当始终参考相关产品技术说明书中最适合的条款,如 有要求,西卡公司非常乐意提供。
新概念二第42课课件

different
adj. 不同的
be different from 与......不同
exercise
1.We human are _d_i_f_fe_r_e_n_t from animal. We have a big d_i_f_f_er_e_n_c_e. (不同) 2.It was _o_b_vi_o_us_ (明显)that the snack could not tell the _d_if_f_er_e_n_c_e (不同)between Indian music and jazz!
2.Some of the fans had waited 24 hours outside the hotel to catch a _g_l_im_p_s_e_ of their heroine.
7.movement
movement n. 动作 move + ment → movement
v. + n.后缀 → n.
Chinese at Beijing University.
A. Indian; English
B. Indians; English
C. Indians; Englishmen D. Indian; Englishmen
Grammar
have一词多义
1. He owns a new house.
我的朋友要来徐州。我将会在机场接他。
接某人
I picked up a lot of English while I was in England.
我在英国期间,学会了很多英语。
偶然学会
pick out
There are so many beautiful cards on display, I can’t pick out the ones I like best.
M.Hauser et al. J. European Psychiatry 22 (2007) 92-98--Early recognition of bipolar disorder
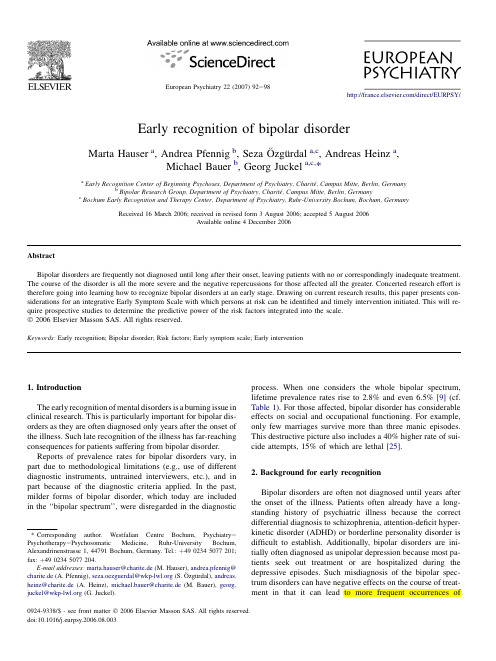
Early recognition of bipolar disorderMarta Hauser a ,Andrea Pfennig b ,Seza O ¨zgu ¨rdal a ,c ,Andreas Heinz a ,Michael Bauer b ,Georg Juckel a ,c ,*aEarly Recognition Center of Beginning Psychoses,Department of Psychiatry,Charite ´,Campus Mitte,Berlin,GermanybBipolar Research Group,Department of Psychiatry,Charite ´,Campus Mitte,Berlin,GermanycBochum Early Recognition and Therapy Center,Department of Psychiatry,Ruhr-University Bochum,Bochum,GermanyReceived 16March 2006;received in revised form 3August 2006;accepted 5August 2006Available online 4December 2006AbstractBipolar disorders are frequently not diagnosed until long after their onset,leaving patients with no or correspondingly inadequate treatment.The course of the disorder is all the more severe and the negative repercussions for those affected all the greater.Concerted research effort is therefore going into learning how to recognize bipolar disorders at an early stage.Drawing on current research results,this paper presents con-siderations for an integrative Early Symptom Scale with which persons at risk can be identified and timely intervention initiated.This will re-quire prospective studies to determine the predictive power of the risk factors integrated into the scale.Ó2006Elsevier Masson SAS.All rights reserved.Keywords:Early recognition;Bipolar disorder;Risk factors;Early symptom scale;Early intervention1.IntroductionThe early recognition of mental disorders is a burning issue in clinical research.This is particularly important for bipolar dis-orders as they are often diagnosed only years after the onset of the illness.Such late recognition of the illness has far-reaching consequences for patients suffering from bipolar disorder.Reports of prevalence rates for bipolar disorders vary,in part due to methodological limitations (e.g.,use of different diagnostic instruments,untrained interviewers,etc.),and in part because of the diagnostic criteria applied.In the past,milder forms of bipolar disorder,which today are included in the ‘‘bipolar spectrum’’,were disregarded in the diagnosticprocess.When one considers the whole bipolar spectrum,lifetime prevalence rates rise to 2.8%and even 6.5%[9](cf.Table 1).For those affected,bipolar disorder has considerable effects on social and occupational functioning.For example,only few marriages survive more than three manic episodes.This destructive picture also includes a 40%higher rate of sui-cide attempts,15%of which are lethal [25].2.Background for early recognitionBipolar disorders are often not diagnosed until years after the onset of the illness.Patients often already have a long-standing history of psychiatric illness because the correct differential diagnosis to schizophrenia,attention-deficit hyper-kinetic disorder (ADHD)or borderline personality disorder is difficult to establish.Additionally,bipolar disorders are ini-tially often diagnosed as unipolar depression because most pa-tients seek out treatment or are hospitalized during the depressive episodes.Such misdiagnosis of the bipolar spec-trum disorders can have negative effects on the course of treat-ment in that it can lead to more frequent occurrences of*Corresponding author.Westfalian Centre Bochum,Psychiatry e Psychotherapy e Psychosomatic Medicine,Ruhr-University Bochum,Alexandrinenstrasse 1,44791Bochum,Germany.Tel.:þ4902345077201;fax:þ4902345077204.E-mail addresses:marta.hauser@charite.de (M.Hauser),andrea.pfennig@charite.de (A.Pfennig),seza.oezguerdal@ (S.O ¨zgu ¨rdal),andreas.heinz@charite.de (A.Heinz),michael.bauer@charite.de (M.Bauer),georg.juckel@ (G.Juckel).0924-9338/$-see front matter Ó2006Elsevier Masson SAS.All rights reserved.doi:10.1016/j.eurpsy.2006.08.003European Psychiatry 22(2007)92e98/direct/EURPSY/episodes (e.g.,rapid cycling)with increased age.In addition,longer duration of the untreated illness leads to greater chro-nicity of the illness in that residual symptoms that were ini-tially absent from healthy periods do persist and the patient does not experience a full remission in between episodes any more,which also leads to more social impairment.A misdiagnosis and,consequently,inadequate treatment can have a far-reaching negative impact on the subsequent course of the disease,particularly in cases of patients present-ing with unipolar depression.Studies indicate that treatment with antidepressants in the presence of an undetected bipolar disorder can lead to an increased risk of suicide [10]and can,particularly in patients with a genetic risk for bipolar dis-order,trigger manic symptoms [24]or strong mood swings [16].These findings are especially significant given that stud-ies show that 20e 40%of adolescents experiencing a depres-sive episode will be diagnosed with bipolar disorder within the next five years.Similar numbers are presented by the American Academy of Child and Adolescent Psychiatry,which reflects the situation of approximately 1.1million chil-dren and adolescents in the USA alone.Fig.1shows a graphic representation of the time lost between an initially mistaken diagnosis and a final correct di-agnosis.In order to prevent these debilitating consequences for the patients,it is imperative that bipolar disorders are diag-nosed correctly and treated as early as possible.One promising approach is the use of diagnostic instruments for early recog-nition of the illness and consequently provision of early inter-ventions.Such instruments have been successfully used for schizophrenia disorders for several years now [18].Research on the schizophrenic ‘‘Basic Symptoms’’has produced a short version of the ‘‘Bonn Scale for Assessment of Basic Symp-toms’’(BSABS-P,Schultze-Lutter andKlosterko ¨tter,Ko ¨ln).It was shown to have satisfactory predictive power,a relatively low false-positive prediction rate and appears to be particu-larly useful in the early recognition of very earlyschizophrenic prodromes [17].Research conducted in order to establish the definition for the prodromal phase of schizo-phrenia disorders in the DSM-III-R led to the development of critical criteria,which today are also used for the assess-ment of pre-psychotic prodromes [27].This kind of specific early recognition is not yet within reach for bipolar illness.The goal for future research must be to establish specific early symptoms and criteria,which can be used for the definition and assessment of the bipolar prodrome.This paper presents first considerations and research approaches.3.Integrating previous research on early recognition of bipolar disorders to an Early Symptoms Scale 3.1.At what age should early recognition begin?For anyone inquiring about the topic of early recognition,age of onset is one of the first questions posed.In retrospective studies patients reported that the first signs of bipolar disorder were usually noticed between the ages of 15and 19years (Table 2).If those persons who report that signs of their illness were observed even before this age,i.e.in childhood,are taken into account,then the number increases to 59%,which means that over half experience early signs of the illness before the age of 19.Considering these results,it seems that a diagnosis of bi-polar disorder in adulthood,during which time the illness is generally diagnosed,is much too late,and thus the prospect of recognizing bipolar disorders in adolescence is very prom-ising.Consequently,this also points to the need for collabora-tion with child psychiatrists.Nevertheless other findings indicate later onset of bipolar disorders outside the USA;for example,the results of the Stanley Foundation Bipolar Network find the age of 24to be the mean age of onset in a naturalistic follow-up study among German Centers [14].Furthermore,Amminger et al.[1]foundTable 1Prevalence rates of bipolar disorder by diagnostic criteria (modified according to [6])AuthorsCountry Lifetime prevalence (%)Narrow definitions of bipolar disorderKessler et al.,1994USA 1.6Regier et al.,1988USA1.2Weissmann et al.,1996Cross national 0.3e 1.5Broader definitions of bipolar disorderLevinsohn et al.,1995USA 5.7Szadoczky et al.,1998Hungary 5.0Angst et al.,1998Switzerland2.8Age 19,323,128,428,834,136,1of a doctorfirsttreatment with ADwith Mood stabilizerdisorderFig.1.Extended time axis of a late recognized bipolar disorder (adapted from [16]).93M.Hauser et al./European Psychiatry 22(2007)92e 98that an early age of onset (before age 18)was the best predic-tor to distinguish between affective and non-affective psycho-sis with non-affective psychoses showing later onset.Thus,considerations towards an early recognition in fact should es-timate juvenile adolescents as well,especially as long as we do not know much about the natural course of the bipolar pro-drome.Nevertheless,clinicians especially outside the United States should also consider older adolescents as persons at risk for bipolar disorder with later onset.3.2.Early symptoms of bipolar disorderAccording to the National Depressive and Manic-Depres-sive Association,depressive symptoms are with 47%the pre-dominant early signs of bipolar illness (Fig.2).This is consistent with other investigations (for a review see,e.g.,[9]),which showed that the course of bipolar disorders usually begins with a depressive and not with a manic episode.However,depressive symptoms are also the most commoninitial symptoms of many other psychiatric disorders,are therefore not specific to bipolar disorders,and consequently not a reliable indicator of bipolar illness.This presents a big problem for the assessment and early recognition of bipolar disorders,whose main characteristic is the disturbance of af-fect.Therefore,such symptoms naturally have to be taken into account when diagnosing bipolar disorders.The Personal Assessment and Crisis Evaluation Clinic in Melbourne,Australia (PACE),a center for the early recogni-tion of psychoses,presents first indications as to the nature of the prodromal phase of bipolar disorders that do not come from retrospective studies on patients with bipolar disor-der or from prospective following of offspring but from a pro-spective following of symptomatic patients within an Early Recognition Center.Thompson et al.[26]report on three pa-tients (average age 21years)who came to the Early Recogni-tion Center seeking clarification of a psychotic prodrome,which within the course of the following year manifested as a bipolar disorder (I and II).These patients initially showed predominantly depressive and anxiety symptoms,eating disor-ders,and substance abuse as comorbid disorders,only one of them against the background of a family history of bipolar dis-order.Two of these patients also presented with racing thoughts and mood swings.The presence of attenuated posi-tive symptoms in all three cases,i.e.psychotic symptoms not severe enough to meet diagnostic criteria for schizophre-nia,was considered by the authors to be attributable to a patient selection particular to the nature of the Early Recogni-tion Center and does not necessarily represent a typical characteristic of a prodromal phase of bipolar disorder,in par-ticular because it was initially indistinguishable from a schizo-phrenic prodrome.More findings from other prospective followings within Early Recognition Centers,namely from the Recognition And Prevention Program (RAP)at the Zucker Hillside Hospital,New York,also lead to indicators of the bi-polar prodrome,which are to be investigated in an Early Rec-ognition Scale (Correll et al.2006,personal communication).Consequently,depressive mood appears to be a basic fea-ture of the bipolar prodrome,which for purposes of early rec-ognition should be a prerequisite symptom.To allow for a reliable prediction,additional criteria with high predictive power must be included.In the search for these additional cri-teria,just as is the case with attenuated positive symptoms ac-companying the pre-psychotic schizophrenic prodrome,we might be able to find certain bipolar symptoms lurking subclin-ically just below the threshold of severity so that a diagnosis of bipolar disorder is not yet warranted.This would mean that alongside the sub-threshold depressive mood,sub-threshold (hypo-)manic symptoms would be present.Bipolar disorder risk studies singled out mood dysregula-tion d ‘‘frequent ups and downs’’d as the strongest known risk factor.An examination [4]of 591individuals from the Zurich cohort study using logistic regression analyses showed that mood regulation has a greater influence as a risk factor for bipolar disorder than does family history of bipolar disorder or a personality exhibiting ‘‘emotional and vegetative lability’’.However,the same result was found for (unipolar)depressiveTable 2Age at first signs of bipolar illness (adapted from [19])Age in years %Absolute number Under 55255to 9125910to 14147115to 192814020to 24157725to 2994730and older108147%Fig.2.Most common initial symptoms (adapted from [19]).94M.Hauser et al./European Psychiatry 22(2007)92e 98disorders,which according to the authors might be explained by the presence of individuals in the study with not yet recog-nized bipolar disorders.In our own sample of >20bipolar pa-tients investigated up to now,nearly all of them did not report‘‘ups and downs’’as initial symptoms (O ¨zgu ¨rdal et al.2006,unpublished).They rather experienced mood swings prior to the first manic episodes that followed the first manifestation of depression.Interestingly the patients described themselves mostly as ‘‘good humored’’persons until they suffered a de-pressive mood for the first time,which lasted longer and was more intensive than they had known it from ‘‘normal sad-ness’’.An 11-year prospective study by Akiskal et al.[8]also found mood dysregulation as the most powerful predictor for the transition from a unipolar to a bipolar disorder and ‘‘en-ergy activity’’as well as ‘‘daydreaming’’to be of additional predictive power [7].3.3.Difficulties in determining affective symptoms as specific risk factors for the bipolar prodromeIt is imperative for further research of early recognition to define the exact temporal and qualitative properties of the ‘‘ups and downs’’,i.e.the nature of the dysregulation,for it is the best predictive characteristic of the bipolar prodrome known so far.Existing definitions of the typical ‘‘ups and downs’’of bipolar disorder are inadequate.The study by Angst et al.[4]operationalized the concept with the general question ‘‘Would you say you were one of those people who have frequent ups and downs?’’.It is surprising that on this ba-sis healthy controls reported to hardly ever have ‘‘ups and down’’(3.8%);however,patients reported experiencing fre-quent rapid mood swings in the form of brief sub-diagnostic depressive episodes (46.6%),which made the control group easily distinguishable from the group with affective disorders.In addition,in the study by Akiskal et al.[8]the construct of emotional dysregulation was elicited as a factor using various personality questionnaires.Angst et al.suggest a ‘‘new bipolar spectrum’’[2,3]which includes the ‘‘softer’’criteria for hypomania,dysthymic epi-sodes as well as recurring brief depressive episodes as indica-tors for the presence of a bipolar II disorder.However,it seems very difficult to distinguish between these syndromes,so that the prodrome of a bipolar disorder seems to be part of the ex-tended spectrum of bipolar disorders.The question arises of how one can define the ‘‘up’’-phases of the ‘‘ups and downs’’risk factor,considering that the definition of hypomania in the extended bipolar spectrum does not include any necessary minimal duration or social impairment.Furthermore it is dif-ficult to distinguish between the mild-bipolar II disorder,as defined by the previous mentioned mild hypomania and brief recurrent dysthymic,disorder and the bipolar prodrome in terms of episode frequency.Besides the above mentioned syndromes,the prodrome of bipolar disorder must also be differentiated from cyclothymia.Cyclothymia is characterized by numerous depressive and hy-pomanic episodes over a two-year period,and if a bipolar pro-drome,similar to the schizophrenic prodrome,occurs several years before the manifestation of the illness,it would almost be impossible to distinguish between cyclothymia and the bi-polar prodrome in terms of the time criterion and a definition of episodes.Table 3is an attempt to present the difficulties en-countered in delineating the conceptualizations of symptoms of a bipolar prodrome,cyclothymia and bipolar II disorder ac-cording to the extended criteria.Another difficulty is the differential diagnosis between the bipolar prodrome and a cyclothymic temperament [7].Follow-ing the assumption that affective disorders are on a continuum,and that a particular type of temperament could be the basis for the development of a affective disorder later in life,bipolar dis-order could develop from a cyclothymic temperament,whereby a particular clinical picture does not necessarily have to corre-spond to the underlying temperament.Akiskal et al.[7],there-fore,prefer to speak of temperament when dealing with subclinical forms of an affective illness.A cyclothymic temper-ament,for example,can be measured by the TEMPS-A Scale.Some of the items on the questionnaire come very close to a pos-sible definition of the risk factor ‘‘frequent ups and downs’’for a bipolar prodrome (Items 23,24,29,30,34,38).However,if a cyclothymic temperament is the basis for later bipolar disor-der,and if similar items are used to measure the best predictive risk factor,namely the ups and downs/emotional dysregulation,the question arises of what additional factors point to a transition into the manifestation of bipolar illness.This is particularly rel-evant,in particular considering that the prodromal phase,as well as the cyclothymic temperament,can remain stable for years.Recent studies have compared persons with a family risk for bipolar disorder with persons diagnosed with bipolar disor-der,persons diagnosed with a unipolar depressive disorder asTable 3Symptom conceptualizations for bipolar prodrome,cyclothymia and extended bipolar II disorderPotential bipolar ProdromeCyclothymiaExtended Definition of a Bipolar II DisorderSymptomatologyDepressive and anxious mood Episodes of mild depression Dysthymic episodes or brief recurring depressive episodes Frequent ups and downsEpisodes of slightly elated moodHypomania in the sense of asyndrome with no minimal duration requirement and no social consequences Frequent switches of these episodes Onset AdolescenceLate adolescence or early adulthood Possible at any ageDuration Several months or yearsAt least 2years95M.Hauser et al./European Psychiatry 22(2007)92e 98well as persons with cyclothymic temperament.The results showed differences among these patient groups,which can be evaluated in terms of risk,but provided no specific risk fac-tors.A comparison with the above-mentioned TEMPS-A Tem-perament Scale between healthy individuals with a family history for bipolar illness,bipolar patients in remission and healthy controls showed that the values for cyclothymic tem-perament for healthy individuals with family risk were lower than the ones for bipolar patients in remission,but higher than the ones for individuals without family risk for bipolar disorder[20].A similar investigation of cyclothymic temperament yielded a continuum between healthy individuals without any risk,healthy individuals with a family risk of an unspec-ified affective disorder and healthy individuals with a positive family history of bipolar disorder[13].Meyer and Hautzinger [22]established a connection between high values on the Hy-pomanic Personality Scale and more frequent patient reports of manic and hypomanic episodes in the subsequent clinical interview.However,this connection did not pertain to other mental disorders,which the authors viewed as an indication for the validity of the scale for bipolar disorders.Yet another difficulty for the diagnosis of a bipolar pro-drome comes from different symptomatology corresponding with the wide range of ages of onset.For example,childhood bipolar disorders are characterized by slightly different symp-toms of manic and depressive episodes than the ones in adult-hood;whereas the symptomatology of adolescent and adult bipolar disorders is quite similar.Manic episodes in children show a more frequentfluctuation of symptoms and often in-clude mixed states.The euphoria often found in adults is miss-ing in children,and is replaced by increased irritability.The depressive syndrome manifests itself more with vegetative symptoms such as headaches,abdominal pains and increased tiredness.Additionally childhood bipolar disorder is character-ized by higher frequency of manic and depressive episodes than adult bipolar disorder.Moreover,in contrast to studies which showed that depressive episodes are thefirst to occur at the development of bipolar disorders,Faedda et al.[15] found depressive symptoms in pediatric bipolar disorder to be reported least often by parents as symptoms at onset.Par-ents rather reported dysphoric-mania or mixed states.Chang et al.[12]singled out mood dysregulation and disruptive be-havior as characteristic for the risk of bipolar disorder in offspring.Thus symptomatic changes and developments over time can complicate the assessment and diagnosis of the bipolar prodrome considerably.Nevertheless,it has to be considered that pediatric bipolar disorder may be a different clinical and neurobiological entity than bipolar disorder in adulthood and accordingly the bipolar prodrome,so that the characteristics in children do not necessarily give infor-mation about the nature of the bipolar prodrome in adolescence.In addition to the number of psychiatric syndromes that may develop during adolescence and early adulthood and that consti-tute similar unspecific symptomatology as the bipolar syndrome (e.g.,schizophrenia,unipolar depression,personality disorders,neurotic maladaptations,etc.),it also has to be differentiated from‘‘normal’’pubertal or adolescent crises.3.4.Further potential risk factorsAccording to Angst et al.[4]a positive family history of mania was another independent,though weaker factor than the‘‘ups and downs’’,contributing to the risk for bipolar dis-order.It is known that children of one bipolar parent have a15e30%increased risk for bipolar disorder.The risk in-creases to50e75%for children whose parents both have bipo-lar disorder.Taking another approach,Angst et al.[5]conducted a pro-spective study in which they looked at specific characteristics of individuals who moved from a diagnosis of unipolar depres-sion to bipolar disorder as opposed to those who did not.Male gender and early onset of the illness were the resulting risk factors for the transition into bipolar I disorder.For the transi-tion to bipolar II disorder,being female,a later onset of the illness and a family history of mania were found to be the main risk factors.On the other hand Birmaher et al.[11]found children and adolescents with major depressive disorder to be at higher risk for the development of bipolar disorder in cases where they show psychotic features,psychomotor retardation, pharmacological induced hypomania or mania and/or family history for bipolar disorder.Meyer and Blechert[21]investigated differences in atten-tion deficit of healthy controls,individuals with a risk for uni-polar depressive disorder and individuals with a risk for bipolar disorder.The study produced an interesting group clas-sification.The group at risk for a bipolar disorder consisted of individuals who showed values in the upper10%on the Hypo-manic Personality Scale but had no further risk factors such as a positive family history for bipolar disorder.There were no general differences in attention deficit between the group of in-dividuals who were at risk for a depressive disorder and those at risk for a bipolar disorder,though lesser differences pointed to cognitive deficits in individuals with a possible risk for bi-polar disorder.4.Necessary steps toward an early diagnosis ofbipolar disordersAs the review demonstrates,more research has been done in recent years in order tofind specific features of the bipolar prodrome,i.e.the risk for developing bipolar disorder.The next step,in an effort to systemize the existing results,is to de-velop an early recognition scale and to evaluate it in prospec-tive case studies in early recognition centers as was done with the schizophrenia prodrome.The scale should encompass the following criteria,which should help identify a person who is at risk and who then should be followed,e.g.,through a pro-spective study:Considering the results of a connection between the cyclo-thymic temperament and bipolar disorder,a cut-off score on the TEMPS-A Scale should be set which indicates an96M.Hauser et al./European Psychiatry22(2007)92e98increased risk for bipolar illness.Preliminarily the cut-off score could be set according to the discriminating score for individuals with family history as found by Mendlowicz et al.[20].This score may need to be changed if prospective studies yield a more precise score.An individual meeting this requirement should be expected to also exhibit:The frequent‘‘ups and downs’’are the most powerful known predictor to date.This predictor should be exam-ined further and defined in more detail than has been the case thus far.It is possible that these‘‘ups and downs’’ex-press subjectively perceived,acute changes in the form of more frequent or more severe mood swings.Alongside the‘‘ups and downs’’,there should be identifi-able current or past distinct depressive or anxious mood episodes.Even minor symptoms pointing toward a mania such as elated mood,irritability or racing thoughts should be probed for,though paying careful attention to the age-specific symptomatology.No minimal duration for and no consequences from the symptoms are necessary in order to qualify them.To raise the probability of an actual existing risk and to allow for a better differentiation to bipolar disorder in childhood,screening for a bipolar prodrome with an early recognition scale in case of suspicion should be conducted with individuals from the age of15on,keep-ing in mind that later onset might be equally typical for the bipolar prodrome and older individuals in equal po-tential risk for bipolar disorder.Family history should be most definitely explored and taken into account as an additional predictor.A prospective follow-up of individuals presenting with such features can yield important insight into a more precise charac-terization of the risk for bipolar disorder and thus the bipolar prodrome.To better distinguish between a schizophrenic and a bipolar prodrome,it would also be beneficial to examine in-dividuals at risk for bipolar disorder with the BSABS-P(Schul-tze-Lutter and Klosterko¨tter,Ko¨ln)and the SIPS(Structured Interview for Prodromal Symptoms)[23],i.e.,to check for ba-sic symptoms and attenuated psychotic symptoms.It is rather improbable that psychosocial factors can add to the differentiation.5.Summary and future directionsCurrent efforts at early recognition of bipolar disorder are of greatest clinical relevance,especially in terms of the course of the illness.It is an enormous challenge to research that is being addressed in increasing numbers of studies.Drawing on already available results,considerations for an early recog-nition scale were presented in this paper,with which individ-uals can be identified for risk of bipolar disorder better than has been possible to date.It was suggested to assess these in-dividuals in the context of early recognition centers and follow them in order to receive detailed information about potential risk factors,so that this knowledge can be used in the development of early intervention strategies as well as preven-tion for bipolar disorders.References[1]Amminger GP,Leicester S,Yung AR,Phillips LJ,Berger GE,Francey SM.Early-onset of symptoms predicts conversion to non-affective psychosis in ultra-high risk individuals.Schizophr Res2006;84:67e76.[2]Angst G,Gamma A,Benazzi F,Ajdacic V,Eich D,Ro¨ssler W.Researchreport:Towards a re-definition of subthreshold bipolarity:epidemiology and proposed criteria for bipolar-II,minor bipolar disorders and hypoma-nia.J Affect Disord2003;73:133e46.[3]Angst G,Gamma A,Benazzi F,Ajdacic V,Eich D,Ro¨ssler W.Diagnosticissues in bipolar disorder.Eur Neuropsychopharmacol2003;13:43e50.[4]Angst G,Gamma A,Endrass J.Risk factors for the bipolar and depres-sion spectra.Acta Psychiatr Scand2003;108(Suppl.418):15e9.[5]Angst G,Sellaro R,Stassen HH,Gamma A.Research report:Diagnosticconversion from depression to bipolar disorders:results of a long-term pro-spective study of hospital admissions.J Affect Disord2005;84:149e57.[6]Akiskal HS,Bourgeois ML,Angst J,Post R,Mo¨ller HJ,Hirschfeld R.Re-evaluating the prevalence of and diagnostic composition within the broad clinical spectrum of bipolar disorders.J Affect Disord2000;59:S5e30.[7]Akiskal HS,Brieger P,Mundt C,Angst J,Marneros A.Temperament undaffektive Sto¨rungen.Die TEMPS-A-Skala als Konvergenz europa¨ischer und US-amerikanischer Konzepte.Nervenarzt2002;3:262e71.[8]Akiskal HS,Maser JD,Zeller PJ,Endicott J,Coryell W,Keller M.Switching from‘unipolar’to bipolar II.An11-year prospective study of clinical and temperamental predictors in559patients.Arch Gen Psychiatry1995;52(2):114e23.[9]Bauer M,Pfennig A.Epidemiology of bipolar disorders.Epilepsia2005;46(Suppl.4):8e13.[10]Berk M,Dodd S.Are treatment emergent suicidality and decreased re-sponse to antidepressants in younger patients due to bipolar disorder being misdiagnosed as unipolar depression?Med Hypotheses2005;65:39e43.[11]Birmaher B,Arbelaez C,Brent D.Course and outcome of child and ad-olescent major depressive disorder.Child Adolesc Psychiatr Clin North Am2002;11(3):619e37.[12]Chang K,Steiner H,Dienes K,Adleman N,Ketter T.Bipolar offspring:A window into bipolar disorder evolution.Biol Psychiatry2003;53(11):945e51.[13]Chiaroni P,Hantouche E-G,Gouvernet J,Azorin J-M,Akiskal HS.Re-search report:The cyclothymic temperament in healthy controls and familially at risk individuals for mood disorder:endophenotype for ge-netic studies?J Affect Disord2005;85:135e45.[14]Dittman S,Biedermann NC,Grunze H,Hummel B,Scha¨rer LO,Kleindienst N.The Stanley Foundation Bipolar Network:Results of the naturalistic follow-up study after2.5years of follow-up in the Ger-man centres.Neuropsychobiology2002;46(suppl.1):2e9.[15]Faedda GL,Baldessarini RJ,Glovinsky IP,Austin NB.Pediatric bipolardisorder:phenomenology and course of illness.Bipolar Disord 2004;6:305e13.[16]Ghaemi SN,Hsu DJ,Soldani F,Goodwin FK.Antidepressants in bipolardisorder.The case for caution.Bipolar Disord2003;5(6):421e33. [17]Klosterko¨tter J,Hellmich M,Steinmeyer EM,Schultze-Lutter F.Diag-nosing schizophrenia in the initial prodromal phase.Arch Gen Psychiatry 2001;58:158e64.[18]Klosterko¨tter J,Ruhrmann S,Schultze-Lutter F,Salokangas RK,Linszen D,Birchwood M,et al.The European Prediction of Psychosis Study(EPOS):integrating early recognition and intervention in Europe.World Psychiatry2005;4(3):161e7.[19]Lish JD,Dime-Meenan S,Whybrow PC,Price RA,Hirschfeld RM.TheNational Depressive and Manic-depressive Association(DMDA)survey of bipolar members.J Affect Disord1994;31(4):281e94.[20]Mendlowicz MV,Girardin J-L,Kelsoe JR,Akiskal HS.Research report:A comparison of recovered bipolar patients,healthy relatives of bipolarprobands,and normal controls using the short TEMPS-A.J Affect Disord 2005;85:147e51.97M.Hauser et al./European Psychiatry22(2007)92e98。
新概念2 lesson 42 (讲练+习题,含答案,共36张PPT)
1.If you have a A ability, you should use it. A. musical B. music C.musician D. musically
3. Let the rainwater run through this pipe.
让雨水从这个管道中流过去。
2. The stock market turned down sharply. 股票市场行情急转直下。
raise a subject 提出一个问题 raise one’s voice 提高嗓门 raise a family 养家糊口 raise money 筹款 raise price 提高价格 raise one’s spirits 打起精神
Practice: 1. It _r_o_s_e_out of the basket and began to follow the movements of the pipe. 2. _R_a_is_e_ your hands if you like listening to music.
当耍蛇人突然又吹奏起爵士乐和现代流行乐曲时,我们 感到非常惊奇。
Note: ①很少用very much 放在一起修饰surprise, 一般用very surprised 或 most surprised
Text analysing
Indian印度
The snake, however, continued to 'dance' slowly. It obviously could not tell the difference between Indian music and jazz!
随着音乐跳舞 (固定搭配,用“to”)
八年级英语上册Unit42课件
I ride the bicycle.
It takes me about 10 minutes.
I walk to school. It takes me 20 minutes.
I take the car. It takes me about 5 minutes.
Can you say the numbers?
take the train
How does he get to school? He rides the bike.
•
How do they get to school? They take a taxi.
How does he go to work? He takes the car.
How does she get to school? She takes a bus.
Conversation:
A: How do you get to school?
A: How long does it take?
How does she get to school? She takes a bus. How long does it take? It takes 25 minutes.
Make a survey:
Interview three of your classmates ,then give a report about it.
90 ninety 258 two hundred and fifty-eight
100 one hundred
A :How do you get to school ? B :I ride my bike.
take a bus take a subway ride a bike
西卡214金属灌浆料说明
wTel: +86 20 82266066Fax: +86 20 82266022Page: 1 / 21.1Chemical Character: modified epoxy resin on bisphenol A.1.2Form: liquid.1.3Color: colorless1.4Odor: slight2PHYSICAL AND SAFETY DATA (Not technical specifications. Unless specified tested at 20℃. All temps quoted in ℃)2.1Changes in Physical state:2.2Density (20℃) Kg/L: 1.13 g/ml Bulk density (kg/m3 ): kg / m32.3Vapor pressure:2.4Viscosity(23℃): 550±60 mPa.s,2.5Water solubility: insoluble2.6PH Value: 62.7Flash point:2.8Ignition Temp.:2.9Explosion limits: N/A2.10Thermal decomp.: :>170℃2.11Hazardous decomposition products:2.12Hazardous reaction:2.13Further information:3TRANSPORTIMDG: UN No.: ICAO/IATA: Tremcard No.:GGVE/GGVS: RID/ADR: ADNR:Other information:4.REGULATIONS5PROTECTIVE MEASURES, STORAGE AND HANDLING5.1Technical protective measures:DO NOT TRANSFER INTO UNLABELED CONTAINERS.5.2Personal: Respiratory protection: Not applicableEye protection: Tightly fitting protecting goggles.Hand protection: Gloves, e.g. rubber.Other:5.3Industrial hygiene: EXPERTS ALWAYS WEAR THE RIGHT PROTECTIVE CLOTHING.Observe good house keeping and general hygiene guidelines.5.4Protection against fire and explosion: N / A5.5Disposal: Product: must be disposed of in a special waste disposal unit in accordance with the corresponding regulationPackaging: completely emptied packagings can be given for recycling. Packaging that cannot be cleaned shouldbe disposed of as product waste.6MEASURES IN CASE OF ACCIDENTS AND FIRES6.1After spillage: All chemical spillages must be dealt with as soon as possible to prevent contamination. Damage or stainingof the area affected (especially with liquid products). Attention is drawn to the Control of Pollution Act 1974, the provisionThe information in this safety data sheet respects the actual status of knowledge at the date of publication. They do not imply any warranty. For warranty obligations the specific product descriptions and General Status Conditions are of relativance only.of which is enforced by local authorities. Sweep up spillages. Place in polyethene bags for disposal to an authorized waste site. Wash the area with strong industrial detergent and hot water.6.2 Extinguishing media suitable: compatible with all usual extinguishing media.Not be used: N/A6.3 First aidIngestion : Do not induce vomiting. Summon a doctor immediately.Eye contact : Rinse immediately with opened eyelids under running water for 15 minutes and summon a doctorimmediately.Skin contact : Remove contaminated clothing. Wash off immediately with soap and water. Consult a doctor if skinirritation persists.Inhalation : Remove to fresh air. Give oxygen if required. In the event of symptoms take medical treatment.6.4 Further information : Sika Limited products are generally safe to use provided certain precautions normally taken whenhandling chemicals are observed. Unless specified products should not come into contact with drinking water, foodstuffs or food equipment and measures should be taken to prevent skin contact, since people with particularly sensitive skin may be affected. The use of barrier creams, goggles and industrial gloves are recommended. The skin should be cleansed at the end of each working period using a suitable industrial cleanser or warm water and soap, the use of solvents to clean the skin is not recommended. Adequate ventilation of the working area is recommended. Take careful note of all safety information on data sheets and labels.7 INFORMATION ON TOXICITYContact with eyes, skin and mucous membranes may cause slight irritation. Sensitization and allergic reaction may occur.8 INFORMATION ON ECOLOGICAL EFFECTSAddition informationDo not allow to enter waste water drain, waterways or soil.9 FURTHER INFORMATIONAll statements are based on our experience to date. Form based on DIN 52900.The information contained in this Safety Data Sheet corresponds to our level of knowledge at the time of publication. Allwarranties are excluded. Our most current General Sales Conditions shall apply. Please consult the Technical Data Sheet prior to any use and processing.SAFETY DATA SHEET Sikadur 42HE, Part A01/2007Sika Ltd., China No.96,JunDa Road, Eastern Section, GET Guangzhou, China, post code: 510530 Tel: +86 20 82266066 Fax: +86 20 82266022 Pages: 2/2。
lesson 42课件(共24张PPT) 冀教版英语八年级上册
Jenny and I joined the club. So did most of our classmates ቤተ መጻሕፍቲ ባይዱ Please write back to me soon. I miss you!
Love, Brian
Vocabulary
real adj. 真正的;确实的 support v.& n. 支持;拥护;鼓励 daily adv. 每日;每天 adj. 每日的;日常的
Let’s do it!
1. Read the lesson and answer the questions.
1. What is Jenny’s hobby? Jenny’s hobby is gardening.
2. What does Brian’s teacher say about gardening? The teacher says that gardening is enjoyable and easy to learn.
4. We can work in it daily and take good care of it. 我们可以每天在里面工作并好好照顾它。
◉ daily在此做副词,意为“每日;每天”;take care of意为“照顾, 照料”。
※ We need to take care of our bodies. 我们需要照顾好自己的身体。
那些是真花吗?
3. Many classmates supported the idea. 很多同学都支持这个想法。
◉ suppot作动词时意为“支持;拥护”,作名词时意为“支持;支撑; 证据”,其常见搭配为: suppot sb./sth. in sth.在某事上支持某人或 某物。
新概念英语第二册听力及翻译Lesson 42
新概念英语第二册听力及翻译Lesson 42Lesson 42 Not very musical 并非很懂音乐First listen and then answer the question.听录音,然后回答以下问题。
What happened when the snake charmer began to play jazz?As we had had a long walk through one of the markets of Old Delhi,we stopped at a square to have a rest. After a time, we noticed a snake charmer with two large baskets at the other side of the square, so we went to have a look at him. As soon as he saw us, he picked 5 up a long pipe which was covered with coins and opened one of the baskets. When he began to play a tune, we had our first glimpse of the snake. It rose out of the basket and began to follow the movementsof the pipe. We were very much surprised when the snake charmer suddenly began to play jazz and modern pop songs. The snake, however, continued to ‘dance’slowly. It 10 obviously could not tell the difference between Indian music and jazz!New words and expressions 生词和短语musical adj. 精通音乐的snake n. 蛇market n. 市场,集市movement n.动作snake charmer 玩蛇者 (通常借音乐控制)continue v. 继续dance v. 跳舞pipe n.(吹奏的)管乐器obviously adv.显然tune n. 曲调difference n.差别glimpse n. 一瞥Indian adj.印度的Notes on the text 课文注释1 Not very musical 是指蛇并不那样“懂”音乐。
新概念英语第二册Lesson42Notverymusical课件
glimpse & glance
glance “一眼,看一眼”。粗略地匆匆看一眼。强调动作过 程,常常用give / take a glance at。 e.g. The man gave me a glance。
glimpse n “一瞥,瞥见”。无意识地一看,所见并不一定 全面。强调动作结果,常用catch / get a glimpse of 。 e.g. I caught a glimpse of the beautiful house as train train went by.
NCE 2 LESSON 42
Not very musical
并非很懂音乐
text
As we ______________________one of the markets of Old Delhi, we stopped at a square ________________. After a time, we _______ a snake-charmer ___________________________at __________________the square, so we went to have a look at him. _______________he saw us, he _____________a long pipe _______ was covered with coins and opened one of the baskets. When he began to __________________, we had our first glimpse of the snake. It _______________________and began to __________________ of the pipe. We were very much surprised when the snake charmer suddenly __________________and modern pop songs. The snake, however, _____________'dance' slowly. It _________ could not __________________between Indian music and jazz!
托福听力tpo42 section2 对话讲座原文+题目+答案+译文
托福听力tpo42section2对话讲座原文+题目+答案+译文Conversation2 (2)原文 (2)题目 (3)答案 (5)译文 (5)Lecture3 (6)原文 (6)题目 (8)答案 (10)译文 (10)Lecture4 (12)原文 (12)题目 (15)答案 (17)译文 (17)Conversation2原文NARRATOR:Listen to a conversation between a student and a university activities coordinator.MALE ACTIVITIES COORDINATOR:I understand your problem,but the upper level of the student center isn’t available for the time being.FEMALE STUDENT:But my dance group has a performance coming up.MALE ACTIVITIES COORDINATOR:I've been talking with people all day long who are in the exact same situation.There are at least a dozen dance and drama groups on campus,and they're all scrambling for rehearsal space right now.FEMALE STUDENT:But I made this reservation last June,before leaving for the summer.No one said anything about construction...MALE ACTIVITIES COORDINATOR:That's because no one knew that the remodeling was going to run over into the beginning of the school year.The builders are just way behind schedule.For a while,we weren't even sure that the dining hall on the lower level would be ready for the start of the semester.So,it could've been a lot worse.FEMALE STUDENT:So when will…MALE ACTIVITIES COORDINATOR:The whole upper level will be ready in six weeks: the rehearsal rooms,the game room,the computer center…FEMALE STUDENT:Six weeks?That's not going to help me.Our performance is in five weeks.MALE ACTIVITIES COORDINATOR:Ah,are you part of the program they planned for Parents'Weekend?FEMALE STUDENT:Yeah.The thing is we're a tap dancing group,and we need to practice on hard floors,preferably wood.We can practice on carpet at first,but...It'simportant for us to be able to hear our feet hit the floor.MALE ACTIVITIES COORDINATOR:Interesting.Uh,because of the rhythm,huh? FEMALE STUDENT:Yeah,because the tapping becomes part of the music.MALE ACTIVITIES COORDINATOR:…so the floors are very important.FEMALE STUDENT:Exactly.And just about everywhere on campus has carpeting.MALE ACTIVITIES COORDINATOR:Well,there's always the stage at the student theater.Though it's a long shot.We can look at the schedule.There might be some odd hours free.FEMALE STUDENT:What about in town?Do you think the university could help us rent a rehearsal space in a commercial dance studio in town,given the situation?MALE ACTIVITIES COORDINATOR:That's not really my call.I can reserve rehearsal and performance spaces on campus for you,but,uh...off campus…FEMALE STUDENT:So who would I talk to?The dance department?MALE ACTIVITIES COORDINATOR:Look,let's check the theater schedule first.题目1.Why does the student go to see the man?A.To register her group to perform for Parents'WeekendB.To change the date when her dance group will give a performanceC.To complain about the floor in a newly built rehearsal roomD.To find out when a room she reserved will be available2.Why is the student's group unable to rehearse in the student center?A.The rehearsal space was overbooked.B.The building is being renovated.C.The rehearsal space was replaced by a game room.D.The group did not reserve a rehearsal room.3.What two points do the speakers make about tap dancing?[Click on2answers.]A.Tap dancing is becoming a popular form of entertainment on campus.B.Tap dancing classes have always been offered at the university.C.Tap dancing requires a certain type of flooring.D.Tap dancing creates sounds that are important to the performance.4.What does the man imply about the student theater?A.It is almost always booked.B.It has not been renovated in a long time.C.It is too small to accommodate the student's dance group.D.It is rarely used for dance performances.5.What does the man imply when he says this:(MALE ACTIVITIES COORDINATOR)That's not really my call.I can reserve rehearsal and performance spaces on campus for you,but,uhh…off campus...A.He is not sure what kind of rehearsal space the student needs.B.He does not know of any rehearsal space off campus.C.He is unable to reserve rehearsal space off campus.D.He will call a dance studio in town.答案D B CD A C译文旁白:接下来你会听到一段某个学生和大学活动协调员之间的对话。
新概念英语 第二册 lesson42 课文讲解

Lesson 42 Not very musical一、阅读课文As we had had a long walk through one of the markets of old Delhi, we stopped at a square to have a rest. After a time, we noticed a snake charmer with two large baskets at the other side of the square, so we went to have a look at him. As soon as he saw us, he picked up a long pipe which was covered with coins and opened one of the baskets. When he began to play a tune, we had our first glimpse of the snake. It rose out of the basket and began to follow the movements of the pipe. We were very much surprised when the snake charmer suddenly began to play jazz and modern pop songs. The snake, however, continued to ‘dance’ slowly. It obviously could not tell the difference between Indian music and jazz! (142 words)二、单词解析1. musical [ˈmjuːzɪkl]adj. 音乐的,有音乐天赋的She’s very musical. 她极具音乐天赋。
【大学英语专业教材】高级英语(张汉熙主编)第四册课文及习题详解
u the thesis ----“ All colonial empires are founded upon this fact”
u the author's central idea
uColonializa on is based on the fact that people are very poor.
un l it is needed.
u= store
ustowst –ow away = hide
u 土豆要在阴凉避光处储藏。 u Potatoes must be stowed in a cool dark place.
u stow away:
u My jewellery is safely stowed away in the bank. u The hungry boy stowed away all the food on the table.
upome --- apple
ugranate ---- uhaving many seeds
chant ---words repeated in a monotonous tone of voice
u 1. a word or group of words that is repeated over and over again, usually by more
ufrenTzhieedre – isa daj . warp in her nature. ufull of uncontrolled excitement
u那狗狂吠著跳起扑向闯进来的人. uThe dog jumped at the intruder with frenzied barks. u--- make frenzied efforts
新概念第四册Lesson42Recordinganearthquake
新概念第四册Lesson 42 Recording anearthquakeLesson 42Recording an earthquake记录地震First listen and then answer the following question.听录音,然后回答以下问题。
What does a pen have to do to record on paper the vibrations generated by an earthquake?An earthquake comes like a thief in the night, without warning ・It was necessary, therefore, to invent instruments that neither slumbered nor slept・ Some devices were quite simple. One, for instance, consisted of rods of various lengths and thicknesses which would stand up on end like ninepins・ When a shock came, it shook the rigid table upon which these stood・ If it were gentle, only the more unstable rods fel1. If it were severe, they all fel1. Thus the rods, by falling, and by the direction in which they fell, recorded for the slumbering scientist the strength of a shock that was too weak to waken him, and the direction from which it came ・But instruments far more delicate than that were needed if any really serious advance was to be made・ The ideal to be aimed at was to devise an instrument that could record with a pen on paper, the movements of the ground or of the table as the quake passed by. While I write my pen moves, but the paper keeps stil1・ With practice, no doubt, I could in time learn to write by holding thepen still while the paper moved. That sounds a silly suggestion, but that was precisely the idea adopted in some of the early instruments (seismometers) for recording earthquake waves・ But when table, penholder and paper are all moving, how is it possible to write legibly?The key to a solution of that problem lay in an everyday observation ・ Why does a person standing in a bus or train tend to fall when a sudden start is made? It is because his feet move on , but his head stays stil1. A simple experiment will help us a littie further ・ Tie a heavy weight at the end of a long piece of string・ With the hand held high in the air, hold the string so that the weight nearly touches the ground・Now move the hand to and fro and around but not up and down・ It will be found that the weight moves but slightly or not at all. Imagine a pen attached to the weight in such a way that its point rests upon a piece of paper on the floor ・ Imagine an earthquake shock shaking the floor, the paper, you and your hand・ In the midst of all this movement, the weight and the pen would be still. But as the paper moved from side to side under the pen point, its movement would be recorded in ink upon its surface・It was upon this principle that the first instruments were made, but the paper was wrapped round a drum which rotated slowly. As long as all was still, the pen drew a straight line, but while the drum was being shaken, the line that the pen was drawing wriggled from side to side. The apparatus thus described, however, records only the horizontal component of the wave movement, which is, in fact, much more complicated. If we could actually see the path described by a particle, such as a sand grain in the rock, it would be more like that of a bluebottle buzzing round the room; it would be up and down, to and fro and from side to side. Instruments have been devised and can be so placed that all three elements can be recorded in different graphs・When the instrument is situated at more than 700 miles from the earthquake centre, the graphic record shows three waves arriving one after the other at short intervals・The first records the arrival of longitudinal vibrations・ The second marks the arrival of transverse vibrations which travel more slowly and arrive several minutes after the first. These two have travelled through the earth・ It was from the study of these that so much was learnt about the interior of the earth・ The third, or main wave, is the slowest and has travelled round the earth through the surface rocks・H. H, SWINNERTON The Earth beneath UsNew words and expressions 生词与短语earthquaken.地震slumberV.睡眠ninepinn.九柱戏中的木柱rigidadj.坚硬的delicate adj.灵感的seismometer n.地震仪penholdern.笔杆legiblyadv.字迹清楚地drumn.鼓状物wriggleV.扭动bluebottien.绿头苍蝇graphn.图表graphicadj.图示的longitudinal adj.纵向的transverseadj.横向的木文参考译文地震就像夜间的小偷,不打招呼就来了。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Guangzhou, China, post code: 510530 Tel: +86 20 82266066 Fax: +86 20 82266022 Page: 1 / 2
1.1 Chemical Character: filler 1.2 Form: powder 1.3 Color: grey
1.4 Odor: odourless
2 PHYSICAL AND SAFETY DATA (Not technical specifications. Unless specified tested at 20℃. All temps quoted in ℃) 2.1 Changes in Physical state:
2.2 Density (20℃) Kg/L: 1.7 Bulk density (kg/m 3 ): kg / m 3 2.3 Vapor pressure: 2.4 Viscosity:
2.5 Water solubility: 2.6 PH Value: 12 2.7 Flash point: 2.8 Ignition Temp.:
2.9 Explosion limits: N/A 2.10 Thermal decomp.: :
2.11 Hazardous decomposition products: 2.12 Hazardous reaction: 2.13 Further information: 3 TRANSPORT IMDG: UN No.: ICAO/IATA: Tremcard No.: GGVE/GGVS: RID/ADR: ADNR: Other information: 4. REGULATIONS (C.P.L Parts IV & V “Approved List”, also EEC Directive - Dangerous Substances 67/548EEC). 5 PROTECTIVE MEASURES, STORAGE AND HANDLING 5.1 Technical protective measures:
DO NOT TRANSFER INTO UNLABELED CONTAINERS. 5.2 Personal: Respiratory protection: dust mask
Eye protection: Safety glasses
Hand protection: Butyl rubber/nitrile rubber gloves. Other:
5.3 Industrial hygiene: EXPERTS ALWAYS WEAR THE RIGHT PROTECTIVE CLOTHING.
Observe good house keeping and general hygiene guidelines. 5.4 Protection against fire and explosion: N / A
5.5 Disposal: Product: must be disposed of in a special waste disposal unit in accordance with the corresponding regulation
Packaging: completely emptied packagings can be given for recycling. Packaging that cannot be cleaned should be disposed of as product waste.
6 MEASURES IN CASE OF ACCIDENTS AND FIRES
6.1 After spillage: All chemical spillages must be dealt with as soon as possible to prevent contamination. Damage or
staining of the area affected (especially with liquid products). Attention is drawn to the Control of Pollution Act 1974, the
The information in this safety data sheet respects the actual status of knowledge at the date of publication. They do not imply any warranty. For warranty obligations the specific product descriptions and General Status Conditions are of relativance only.
provision of which is enforced by local authorities. Sweep up spillages. Place in polyethene bags for disposal to an authorized waste site. Wash the area with strong industrial detergent and hot water. 6.2 Extinguishing media suitable: N/A
Not be used: 6.3 First aid
Ingestion : Do not induce vomiting. Summon a doctor immediately.
Eye contact : Rinse immediately with plenty of water for 15 minutes and summon a doctor immediately.
Skin contact : Remove contaminated clothing. Wash off immediately with soap and water. Consult a doctor if skin
irritation persists..
Inhalation : Remove to fresh air. Give oxygen if required. In the event of symptoms take medical treatment.
6.4 Further information : Sika Limited products are generally safe to use provided certain precautions normally taken when
handling chemicals are observed. Unless specified products should not come into contact with drinking water, foodstuffs or food equipment and measures should be taken to prevent skin contact, since people with particularly sensitive skin may be affected. The use of barrier creams, goggles and industrial gloves are recommended. The skin should be cleansed at the end of each working period using a suitable industrial cleanser or warm water and soap, the use of solvents to clean the skin is not recommended. Adequate ventilation of the working area is recommended. Take careful note of all safety information on data sheets and labels.
7 INFORMATION ON TOXICITY
8 INFORMATION ON ECOLOGICAL EFFECTS
Addition information
Do not allow to enter waste water drain, waterways or soil.
9 FURTHER INFORMATION
All statements are based on our experience to date. Form based on DIN 52900.
The information contained in this Safety Data Sheet corresponds to our level of knowledge at the time of publication. All
warranties are excluded. Our most current General Sales Conditions shall apply. Please consult the Technical Data Sheet prior to any use and processing.
SAFETY DATA SHEET
Sikadur 42HE,Part C
01/2007
Sika Ltd., China
No.96,JunDa Road, Eastern Section, GET
Guangzhou, China, post code: 510530 Tel: +86 20 82266066
Fax: +86 20 82266022 Pages: 2/2。