Ultrasound-Guided Regional Anesthesia for Procedures of the Upper Extremity
英语角

沿着已知的神经行走方向滑动 超声探头,短轴切面经常是看 见神经从的形成图像的最好方 式。
4.Successful local anesthetic injections clarify the border of the nerve and track along the nerve path and its branches.
超声也可以提供针尖位置和药 物注射情况的实时图像。
3.Sliding the ultrasound transducer along the known course of a nerve with it viewed in short axis is often the best way of visualizing fascicles to confirm nerve identity. visualize [ˈvɪʒuəˌlaɪz] vt. 形成思维图像;设 想;使可见; fascicle[ˈfæsɪkəl] n. 肌束;(花、叶等的) 束;簇;丛
potential[pəˈtɛnʃəl] adj. 潜在的,有可能 的n. 潜力,潜能;
在神经位置的解剖变异是阻滞 失败的潜在原因,这是可以( 在超声上)直接看见的。
6.Ultrasound imaging can prevent and
detect critical events such as intravascular or intraneural injection, which may improve safety during regional anesthesia procedures. intravascular[ˌɪntrəˈvæskjəlɚ] adj. 血管 内的; intraneural[ ɪntræn'jʊərəl ]adj. 神经内的
超声引导下腘窝上坐骨神经阻滞在胫腓骨骨折术后镇痛的应用
超声引导下腘窝上坐骨神经阻滞在胫腓骨骨折术后镇痛的应用发表时间:2018-08-31T15:05:40.697Z 来源:《医药前沿》2018年8月第23期作者:刘松彬王华婴(通讯作者) [导读] 超声引导下腘窝上坐骨神经阻滞镇痛效果确切,可以为胫腓骨骨折手术患者提供安全有效地术后镇痛。
(复旦大学附属中山医院闵行分院/复旦大学附属闵行医院/上海市闵行区中心医院上海 201199)【摘要】目的:探讨超声引导下腘窝上坐骨神经阻滞在胫腓骨骨折术后镇痛的效果。
方法:选择择期行胫腓骨骨折手术患者60例,性别不限,ASAⅠ或Ⅱ级,年龄22~72岁,BMI:18~30kg/m2。
根据电脑随机表格分为二组,腘窝上坐骨神经阻滞组(P组)、对照组(C 组),每组各30例。
记录患者术后3、6、12h疼痛VAS评分,当VAS评分大于3分且单次剂量10min后无明显改善,给予静脉注射凯纷50mg 补救镇痛,并记录补救镇痛率。
术后12小时患者镇痛效果的满意度,进行10分制评分(0分,非常不满意;10分,非常满意)。
结果:P组患者术后3h和6h的VAS评分显著低于C组(P<0.05),二组术后12h的VAS评分差异无统计学意义。
P组患者术后补救镇痛率显著低于C组(P<0.05)。
P组患者术后镇痛满意度评分显著高于C组(P<0.05)。
结论:超声引导下腘窝上坐骨神经阻滞镇痛效果确切,可以为胫腓骨骨折手术患者提供安全有效地术后镇痛,提高患者术后镇痛满意度。
【中图分类号】R614 【文献标识码】A 【文章编号】2095-1752(2018)23-0174-02 近年来临床麻醉中超声引导神经阻滞技术得到迅速发展,腘窝上坐骨神经阻滞是减轻膝关节以下手术麻醉疼痛的有效措施。
胫腓骨骨折手术是临床常见的手术,术后患者疼痛较剧烈。
本研究拟探讨超声引导下腘窝上坐骨神经阻滞在胫腓骨骨折术后镇痛的效果,为临床应用提供参考。
1.资料与方法1.1 一般资料选择择期行胫腓骨骨折手术患者60例,性别不限,ASAⅠ或Ⅱ级,年龄22~72岁,BMI:18~30kg/m2。
超声引导下腹横肌平面阻滞复合喉罩全身麻醉在腹腔镜胆囊切除患者中的应用
超声引导下腹横肌平面阻滞复合喉罩全身麻醉在腹腔镜胆囊切除患者中的应用张建林① 纪伟① 陈永军① 李树杰① 【摘要】 目的:观察超声引导下腹横肌平面阻滞(TAPB)复合喉罩全身麻醉在腹腔镜胆囊切除患者中的应用效果。
方法:选取2019年10月-2021年10月在北京市昌平区中医医院接受腹腔镜胆囊切除术的100例患者作为研究对象,采用随机数字表法分为观察组和对照组,各50例。
对照组术中采用喉罩全身麻醉,观察组采用超声引导下TAPB复合喉罩全身麻醉,两组均于术后采用自控静脉镇痛。
比较两组麻醉诱导后5 min(T1)、切皮时(T2)、胆囊切除时(T3)、术毕时(T4)的心率(HR)、平均动脉压(MAP);比较两组麻醉苏醒后6 h(T5)、12 h(T6)、24 h(T7)、48 h(T8)时疼痛程度[视觉模拟评分法(VAS)];比较两组麻醉药物使用剂量及术后48 h内不良反应发生情况。
结果:两组T2、T3、T4的HR 均较T1加快,MAP均较T1升高,并且T3、T4的HR、MAP均高于T2,差异均有统计学意义(P<0.05);观察组T2、T3、T4的HR均较对照组慢,MAP均较对照组低,差异均有统计学意义(P<0.05)。
两组VAS 评分在T6~T8处于升高阶段,与T5比较,T6、T7、T8的VAS评分均较高,T7、T8的VAS评分均高于T6,T8的VAS评分高于T7,差异均有统计学意义(P<0.05);观察组T6~T8的VAS评分均低于对照组,差异均有统计学意义(P<0.05)。
观察组丙泊酚、瑞芬太尼、舒芬太尼使用剂量均少于对照组,差异均有统计学意义(P<0.05)。
两组不良反应总发生率比较,差异无统计学意义(P>0.05)。
结论:超声引导下行TAPB并复合喉罩全身麻醉用于腹腔镜胆囊切除患者中可减轻应激反应,利于维持血流动力学稳定,还可减轻术后疼痛,减少麻醉药物使用剂量。
超声引导下胸椎旁神经阻滞复合全身麻醉在单侧多发

超声引导下胸椎旁神经阻滞复合全身麻醉在单侧多发【摘要】目的:探讨超声引导下胸椎旁神经阻滞(TPVB)复合全身麻醉在单侧多发肋骨骨折手术及术后镇痛中的应用效果。
方法:选择收治单侧多发肋骨骨折手术患者60例,所有患者均于2017年1月至2019年5月在我院接受治疗,按照随机数字表法分为实验组(n=30)和常规组(n=30)。
常规组患者实施全身麻醉后手术,实验组患者常规全身麻醉后实施超声引导下TPVB再手术,术后两组病人都静脉滴注氟比洛芬酯镇痛。
观察两组病人术中平均动脉压、心率、术后疼痛评分、不良反应发生率。
结果:切皮前两组心率、平均动脉压对比差异无统计学意义(P>0.05)。
切皮后实验组患者心率(70.0±7.1)次/min、平均动脉压(79.5±4.6)mmHg,均低于常规组的(87.8±11.2)次/min、(102.3±10.4)mmHg(P<0.05)。
术后1小时实验组静息VAS评分(0.2±0.1)分、活动VAS评分(0.3±0.2)分,均显著低于常规组的(0.7±0.5)分、(1.8±0.8)分(P<0.05)。
术后12小时实验组静息VAS评分(1.6±0.5)分、活动VAS评分(1.7±0.6)24小时实验组静息VAS评分(1.2±0.4)分、活动VAS评分(1.4±0.5)分,均显著低于常规组的(2.9±0.8)分、(3.1±0.9)分(P<0.05)。
实验组不良反应发生率和常规组对比差异无统计学意义(P<0.05)。
结论:在单侧多发肋骨骨折手术中实施超声引导下TPVB联合全身麻醉,对血流动力学指标影响较小,能够明显减轻术后疼痛,不增加不良反应发生率。
【关键词】单侧多发肋骨骨折;超声引导下TPVB;疼痛;心率;平均动脉压;不良反应[Abstract] objective:to investigate the application effect of ultrasound-guided thoracic paraspinal nerve block(TPVB)combined with general anesthesia in the operation of unilateral multiple rib fractures and postoperative analgesia. Methods:60 patients with unilateral multiple rib fractures were selected for treatment. All patients received treatment in our hospital from January 2017 to May 2019,and were divided into experimental group(n=30)and conventional group(n=30)according to the random number table method. Patients in the conventional group underwent surgery after general anesthesia,while patients in the experimental group underwent ultrasound-guided TPVB reoperation after general anesthesia. After surgery,patients in both groups received intravenous infusion of flurbiprofen ester for analgesia. The mean intraoperative arterial pressure,heart rate,postoperative pain score and incidence of adverse reactions were observed in the two groups. Results:there was no significant difference in heart rate and mean arterial pressure between the two groups before skin resection(P>0.05). Heart rate(70.0±7.1)times /min and mean arterial pressure(79.5±4.6)mmHg were lower in the experimental group than in the conventional group(87.8±11.2)times /min and(102.3±10.4)mmHg(P<0.05). VAS scores at rest(0.2±0.1)and at activity(0.3±0.2)in the experimental group at 1 hour after surgery were significantly lower than those in the conventional group(0.7±0.5)and(1.8±0.8)(P<0.05). VAS scores at 12 hours after surgery(1.6±0.5)at rest and(1.7±0.6)at 24 hours were significantly lower than those at 2.9±0.8 and 3.1±0.9 in the conventional group(P<0.05). There was no significant difference in the incidence of adverse reactions between the experimental group and the conventional group(P<0.05). Conclusion:ultrasound-guided TPVB combined with general anesthesia in the operation of unilateral multiple rib fractures has little effect on hemodynamic indexes and can significantly reduce postoperative pain without increasing the incidence of adverse reactions.【Key words 】 unilateral multiple rib fractures;TPVB guided by ultrasound;The pain;Heart rate;Mean arterial pressure;Adverse reactions胸椎旁神经阻滞(TPVB)是外周神经阻滞的一种,通过向椎旁间隙处注射局麻药物,形成同侧邻近多个节段躯体及交感神经阻滞,最终发挥区域性镇痛作用[1]。
超声引导下股神经阻滞联合全身麻醉对全膝关节置换患者疼痛及炎症反应的影响

- 61 -①福建中医药大学附属宁德中医院 福建 宁德 352100超声引导下股神经阻滞联合全身麻醉对全膝关节置换患者疼痛及炎症反应的影响郑锦平①【摘要】 目的:探究超声引导下股神经阻滞联合全身麻醉对全膝关节置换患者疼痛及炎症反应的影响。
方法:选择2021年1月—2022年12月福建中医药大学附属宁德中医院收治的100例全膝关节置换患者。
根据随机数表法分为对照组和观察组,各50例。
对照组进行全身麻醉干预,观察组则进行超声引导下股神经阻滞联合全身麻醉干预。
比较两组的不良反应发生率、手术前后的疼痛评分[视觉模拟评分法(VAS)评分]、机械疼痛阈值、疼痛因子[血清P 物质(SP)、前列腺素E 2(PGE 2)]及炎症反应指标[血清C 反应蛋白(CRP)及肿瘤坏死因子-α(TNF-α)]。
结果:两组各项不良反应发生率比较,差异无统计学意义(P >0.05)。
术前,两组静息及运动状态下VAS 评分、机械疼痛阈值、疼痛因子及炎症反应指标比较,差异无统计学意义(P >0.05);术后2 h、6 h、12 h 及24 h,观察组静息及运动状态下VAS 评分显著低于对照组,机械疼痛阈值显著高于对照组,差异有统计学意义(P <0.05);术后12 h、24 h 及48 h,观察组SP、PGE 2、CRP、TNF-α显著低于对照组,差异有统计学意义(P <0.05)。
结论:超声引导下股神经阻滞联合全身麻醉可有效控制全膝关节置换患者的疼痛程度,且可显著改善疼痛及炎症反应。
【关键词】 超声引导下股神经阻滞 全身麻醉 全膝关节置换 疼痛 炎症反应 doi:10.14033/ki.cfmr.2024.10.015 文献标识码 B 文章编号 1674-6805(2024)10-0061-05 Influence of Ultrasound-guided Femoral Nerve Block Combined with General Anesthesia for Pain and Inflammatory Reactions of Patients with Total Knee Arthroplasty/ZHENG Jinping. //Chinese and Foreign Medical Research, 2024, 22(10): 61-65 [Abstract] Objective: To explore the effects of ultrasound-guided femoral nerve block combined with general anesthesia on pain and inflammation in patients with total knee replacement. Method: A total of 100 total knee replacement patients admitted to Ningde Hospital of Traditional Chinese Medicine Affiliated to Fujian University of Traditional Chinese Medicine from January 2021 to December 2022 were selected. They were divided into control group and observation group according to random number table method, with 50 cases in each group. The control group received general anesthesia intervention, and the observation group received ultrasound-guided femoral nerve block combined with general anesthesia intervention. The incidence of adverse reactions, pain scores [visual analogue score (VAS)], mechanical pain threshold, pain factors [serum substance P (SP), prostaglandin E 2 (PGE 2)] and inflammatory response indicators [serum C-reactive protein (CRP), tumor necrosis factor-α (TNF-α)] before and after surgery were compared between the two groups. Result: There were no significant differences in the incidence of adverse reactions between the two groups (P >0.05). Before surgery, there were no significant differences in VAS score at rest and exercise, mechanical pain threshold, pain factor and inflammatory response index between the two groups (P >0.05). At 2 h, 6 h, 12 h and 24 h after surgery, the VAS score at rest and exercise in the observation group were significantly lower than those in the control group, and the mechanical pain threshold were significantly higher than those in the control group, the differences were statistically significant (P <0.05). At 12 h, 24 h and 48 h after surgery, SP, PGE 2, CRP and TNF-α in observation group were significantly lower than those in control group, the differences were statistically significant (P <0.05). Conclusion: Ultrasound-guided femoral nerve block combined with general anesthesia can effectively control the pain degree of patients with total knee replacement, and can significantly improve the pain and inflammation response. [Key words] Ultrasound-guided femoral nerve block General anesthesia Total knee arthroplasty Pain Inflammatory response First-author's address: Ningde Hospital of Traditional Chinese Medicine Affiliated to Fujian University of Traditional Chinese Medicine, Ningde 352100, China 全膝关节置换是骨科常见术式,其可有效改善患者的膝关节功能,是临床应用率不断提升的一类治疗方式。
超声引导下的神经阻滞用于急诊下肢截肢手术的临床观察
超声引导下的神经阻滞用于急诊下肢截肢手术的临床观察超声引导下的神经阻滞已经逐渐成为区域麻醉中的一项重要的技术,超声图像中可直接观察到神经及神经周围组织,同时可以观察到注射时局麻药的扩散,这些都可以提高神经阻滞的质量和成功率,降低并发症的发生率和严重程度[1]。
超声设备和超声介入技术在麻醉医师中的推广使得下肢完善的神经阻滞变得可能性更高。
本文采用超声引导下的神经阻滞(股神经、坐骨神经、股外侧皮神经和闭孔神经)对急诊行下肢截肢手术的患者施行麻醉,观察其临床效果和安全性。
1 资料和方法1.1 一般资料选择2010年3月至2011年5月上海市第六人民医院30例ASA Ⅰ~Ⅱ级,因下肢毁损伤急诊行下肢截肢手术的患者,分为A组(神经阻滞麻醉)和B组(硬膜外麻醉)各15例。
30例患者术前凝血酶原时间都在正常范围内。
复合有严重的颅脑外伤和其他重要器官损伤如胸腹部外伤、骨盆骨折的患者予以排除。
1.2 麻醉方法麻醉操作前所有患者予以多功能监测和开放中心静脉,部分患者给予有创动脉压监测,所有患者留置导尿管。
A组患者采用Sonosite公司的S-nerve超声仪采用高频线性探头(HFL38/ 6-13 MH Z,Sonosite)行超声引导下下肢神经阻滞(股神经、坐骨神经、股外侧皮神经和闭孔神经):患者首先取仰卧位,将超声探头平行腹股沟韧带置于腹股沟上,在股动脉的外侧看到回声较高的类似梭形的股神经截面,采用短轴平面内技术在股神经的深面注射0.5%耐乐品10 ml阻滞股神经;在髂前上棘的下缘,横行放置探头,在缝匠肌内缘和髂肌上缘之间找到股外侧皮神经,从外侧进针抵达神经注射0.5%耐乐品5 ml;在大腿内侧腹股沟水平略向头侧取得闭孔神经的短轴超声图像,以平面内技术在闭孔神经的前支和后支各注射局麻药3~5 ml[2];随后患者改侧卧位,患侧腿上置,并且屈髋、屈膝,辨认出股骨大转子和坐骨结节,在此区域内臀大肌的最深点略偏内侧找到类似三角梭形的坐骨神经,在坐骨神经的周围注射局麻药20 ml包绕神经。
超声引导颈内静脉穿刺置管术在重症创伤患者中的应用
பைடு நூலகம்
·61·
超声引导颈内静脉穿刺置管术在重症创伤患者中的应用
范 娟 ,李 宏 ,杜建 文 (1.武警 后 勤学 院 附属 医院手 术 室 ,天 津 300162;2.武 警后 勤学 院 附属 医院麻 醉科 ,天 津 300162)
Abstract Objoetivo To explore the value of ultrasound-guided puncture and catheterization of the internal jugular vein in patients with severe trauma.Methods The right internal jugular vein was identif ied with ultrasound and centered on the
FAN Juan ,LI Hong ,DU Jian—wen (1.Operating Room,Afiliated Hospital of Logistical College of CAPF,Tianjin 300162,China; 2.Department of Anesthesiology,Afiliated Hospital of Logistical College of CAPF,Tianjin 300162,China)
【摘 要】 目的 :探 讨 超 声 引导 技 术 对 严 重创 伤 患 者 行 颈 内静 脉 穿刺 置 管 的应 用 价值 。 方 法 :首先 选择 并 用超 声技 术 定 位 右 侧 颈 内静 脉 ,局 麻 后 ,超 声 引 导 直视 完 成 颈 内静 脉 穿刺 插 管。 结 果 :50例 患者 均 1次 穿刺 成 功 并 顺利 置入 中 心静 脉 导 管 ,成 功 率 100%,穿 刺 时 间 为 1~3 min;无动 脉 损 伤 、出血 、气胸 、神 经损 伤 等 并 发 症 。 结 论 :绿 色通 道 手 术 目的是 争 取 抢 救 时间 ,超 声 引导 是 提 高血 管 置 管 安 全 性 和 有 效 性 的 有 效 手段 。相 对 于传 统 的 解 剖 定 位 法 ,它可 以提 高 一针 到 位 率 、总 成 功 率 、降低 并 发 症 和 减 少 置 管 时 间 ,其 已成 为 建 立 血 管 通 路 的 有 力 工 具 .特 别 适 合 应 用 于 危 重 患者 的快 速
椎旁神经阻滞在肺癌手术中的应用进展

椎旁神经阻滞在肺癌手术中的应用进展发布时间:2022-07-24T07:22:50.166Z 来源:《医师在线》2022年3月5期作者:陈勇远秦云植[导读]陈勇远秦云植*(延边大学附属医院麻醉科;吉林延边136200)【摘要】肺癌手术因创伤大,对患者循环和呼吸系统功能干扰明显,潜在问题有术后剧烈疼痛、恶心呕吐、低氧血症、体温异常、意识障碍和血流动力学不稳定等。
胸椎旁神经阻滞( thoracic paravertebral block,TPVB)是在胸椎椎旁间隙注入麻醉药物进而产生同侧节段性躯体和交感神经阻滞的技术。
近年来,随着超声可视化技术的不断发展,胸椎旁神经阻滞得到快速发展。
TPVB镇痛效果明确,是围术期多模式镇痛可选方法之一。
此外,局麻药可降低应激反应对免疫系统的抑制作用,对肺癌患者的预后可起到一定的促进作用。
【关键词】肺癌手术;椎旁神经阻滞肺癌是我国最常见恶性肿瘤,也是我国首位恶性肿瘤死亡原因[1],现肺癌手术多在胸腔镜下进行,与传统开胸手术相比,具有创伤小、术中出血少与恢复快等优点,但仍会引起患者剧烈的疼痛与一定的应激反应,引起患者血流动力学波动、苏醒期躁动,并可能导致术后肺不张及肺部感染等并发症。
Ryungsa Kim等研究指出,手术引起的应激反应通过释放血管生成因子、抑制自然杀伤细胞和细胞介导的免疫来增强肿瘤转移,某些药物,如氯胺酮、硫喷托纳和阿片类药物等也可抑制NK细胞活性,而丙泊酚则没有[2]。
局麻药如利多卡因可增加NK细胞活性。
绝大部分研究认为以吗啡为主的阿片类药物促进了肿瘤的生长和转移。
如何减轻肺癌患者免疫功能抑制,对于预防肿瘤复发尤为重要。
巩红岩等研究发现超声引导连续胸椎旁神经阻滞能更好地抑制应激反应,并且可以减少术中全身麻醉药物的使用[3]。
1 胸椎旁间隙 thoracic pavertebral space (TPVS) 的解剖概述TPVS是临近椎体的三角形解剖结构,其内侧界由椎体和椎间盘构成,前外侧壁是壁层胸膜,后壁为肋横突韧带,不同节段的上下边界由肋骨头、肋骨颈、横突以及肋横突韧带等分隔。
超声引导下前锯肌平面阻滞预防乳腺癌术后疼痛综合征

CHINA MEDICINE AND PHARMACY Vol.11 No.9 May 2021183超声引导下前锯肌平面阻滞预防乳腺癌术后疼痛综合征刘远辉 庄彩屏 钟国城广东省惠州市中心人民医院麻醉科,广东惠州 516001[摘要] 目的 观察超声引导下前锯肌平面阻滞(SPB)超前镇痛预防乳腺癌根治术后疼痛综合征(PMPS),其原理是否与降低炎症反应有关。
方法 选择2019年4月至2020年4月在我院择期拟行乳腺癌根治术的女性患者120例,采用随机数字表法分为全身麻醉组(G 组)和前锯肌平面阻滞组(SPB 组),每组各60例。
SPB 组在术前采用超声引导下0.33%罗哌卡因行前锯肌平面阻滞,G 组不给予神经阻滞。
记录术中患者丙泊酚及瑞芬太尼的用量;比较两组在麻醉前20 min(t 0)、手术开始(t 1)、手术结束(t 2)、术后6 h(t 3)及术后24 h (t 4)血清中炎症因子表达水平的变化;评估患者术后6 h (T 1)、24 h (T 2)、48 h (T 3)、l 周(T 4)、1个月(T 5)、3个月(T 6)的视觉模拟评分(VAS);记录两组术后1、3个月慢性疼痛发生率。
结果 SPB 组术中丙泊酚和瑞芬太尼的用量低于G 组(P <0.05);在t 2~t 4时刻,SPB 组白细胞介素6(IL-6)、白细胞介素10(IL-10)水平明显低于G 组(P <0.05);SPB 组T 1~T 6的VAS 评分明显低于G 组(P <0.05)。
SPB 组术后1、3个月慢性疼痛发生率分别为42.3%、23.0%,低于G 组的62.5%、46.4%(P <0.05)。
结论 超声引导前锯肌平面阻滞在麻醉期间降低术后炎症因子水平,可为乳腺癌根治术提供良好的术后镇痛,有效预防乳腺癌术后疼痛综合征,且安全性较高。
[关键词] 乳腺癌;乳腺癌术后疼痛综合征;前锯肌平面阻滞;炎症因子[中图分类号] R614;R737.9 [文献标识码] A [文章编号] 2095-0616(2021)09-0183-04Ultrasound-guided serratus anterior plane block in prevention ofpost-mastectomy pain syndromeLIU Yuanhui ZHUANG Caiping ZHONG GuochengDepartment of Anesthesiology, Huizhou Municipal Central Hospital, Guangdong, Huizhou 516001, China[Abstract] Objective To observe whether ultrasound-guided anterior serratus muscle block (SPB) can prevent pain syndrome (PMPS) after radical mastectomy, and whether its principle is related to reducing inflammatory reaction. Methods A total of 120 female patients scheduled for radical mastectomy in our hospital from April 2019 to April 2020 were selected. They were randomly divided into the general anesthesia group (group G) and the serratus anterior plane block group (group SPB), with 60 cases in each group. In group SPB, 0.33% ropivacaine was used in ultrasound-guided SPB before operation, while in group G, no nerve block was given. The dosage of propofol and remifentanil used in patients during operation were recorded. The levels of serum inflammatory factors in the two groups were compared at 20 min before anesthesia (t 0), at the beginning of operation (t 1), at the end of operation (t 2), 6 h after operation (t 3) and 24 h after operation (t 4). The score of visual analogue scale (VAS) was evaluated at 6 h (T 1), 24 h (T 2), 48 h (T 3), 1 week (T 4), 1 month (T 5), 3 months (T 6) after operation. The incidence of chronic pain at 1 month and 3 months after operation was recorded in the two groups. Results The dosages of propofol and remifentanil were lower in group SPB than that in group G (P <0.05). The levels of IL-6 and IL-10 were significantly lower in group SPB than those in group G at t 2-t 4 (P <0.05). The VAS scores were significantly lower in group SPB than those in group G at t 1-t 6 (P <0.05). The incidence of chronic pain was 42.3% and 23.0% in group SPB, lower than 62.5% and 46.4% in group G at 1 and 3 months after operation (P <0.05). Conclusion Ultrasound-guided SPB can reduce the level of postoperative inflammatory factors during anesthesia, which can provide a good postoperative analgesia for radical mastectomy, and effectively prevent PMPS, with higher safety.[Key words] Breast cancer; Post-mastectomy pain syndrome; Serratus anterior plane block; Inflammatory factor[基金项目] 广东省惠州市医疗卫生类科技计划项目(2019Y023)乳腺癌是女性最常见的癌症之一,手术治疗是目前乳腺癌治疗的主要手段[1]。
超声引导与传统解剖定位行臂丛神经阻滞的麻醉效果比较

超声引导与传统解剖定位行臂丛神经阻滞的麻醉效果比较目的探討超声引导与传统解剖定位行臂丛神经阻滞的麻醉效果。
方法方便选取2017年1月—2018年1月间在该院进行上肢手术的患者150例,ASAⅠ-Ⅲ级,随机分为两组,每组75例,超声引导组(U组)与传统方法组(T组)。
U组采用超导定位下的臂丛神经阻滞,T组采用传统解剖定位臂丛神经阻滞。
观察并记录两组神经阻滞麻醉起效时间、操作完成时间以及不良反应和并发症发生率。
结果U组患者的麻醉起效时间、操作完成时间分别为(3.19±0.21)min,(3.59±0.16)min,T组分别为(5.98±0.11)min,(4.98±0.26)min,U组显著低于T组,差异有统计学意义(t=111.650、43.194,P<0.05),U组患者并发症发生率、不良反应发生率分别为0.00%、1.33%,T组分别为5.33%、9.33%,U 组显著低于T组,两组比较,差异有统计学意义(χ2=4.109、4.754,P<0.05)。
结论超声引导与传统解剖定位行臂丛神经阻滞相比较,超声引导臂丛神经阻滞操作时间更短、麻醉起效时间更短,麻醉效果更加完善,并具有较高的安全性,值得在临床大力推广。
[Abstract] Objective To investigate the anesthetic effects of brachial plexus block with ultrasound guidance and traditional anatomical positioning. Methods A total of 150 patients undergoing upper extremity surgery in the hospital from January 2017 to January 2018 were convenient selected and classified as ASA I-III and randomly divided into two groups (n=75). Ultrasound-guided group (U group)and traditional methods Group (T group). In the U group,the brachial plexus block was performed with superconducting localization. In the T group,the brachial plexus block was positioned with traditional anatomy. Observe and record the onset time,operation completion time,incidence of adverse reactions and complications in the two groups of nerve block anesthesia. Results The onset time and operation completion time of group A were(3.19±0.21)min and (3.59±0.16)min,respectively. The T group was (5.98±0.11)min and (4.98±0.26)min respectively. The U group was significantly lower than the T group. The difference was significant. Statistical significance (t=111.650,43.194,P<0.05). Incidence of complications and incidence of adverse reactions were 0.00% and 1.33% in group U,and 5.33% in group T,respectively.9.33%,U group was significantly lower than T group,the difference between the two groups was statistically significant (χ2=4.109,4.754,P<0.05). Conclusion Ultrasound-guided brachial plexus block compared with traditional anatomical positioning,ultrasound-guided brachial plexus block more short operation time,shorter onset of anesthesia,better anesthetic effect,and higher safety,it is worth clinical promotion.[Key words] Ultrasound guidance;Traditional anatomical location;Brachial plexus block;Anesthetic effect 臂丛神经阻滞是一项传统麻醉技术,常用于上肢手术[1]。
超声引导下神经阻滞的标准

超声引导下神经阻滞的标准Ultrasound-guided nerve blockade is a standard technique used in regional anesthesia to provide targeted pain relief during surgical procedures or for postoperative pain management. This procedure involves the use of ultrasound imaging to visualize the nerves and surrounding structures, allowing for precise needle placement and accurate delivery of local anesthetic agents. The following paragraphs will discuss the importance of ultrasound guidance in nerve blockade from various perspectives.From a patient's perspective, ultrasound-guided nerve blockade offers several advantages. Firstly, it enhances the safety of the procedure by minimizing the risk of complications such as accidental puncture of blood vessels or neighboring organs. The real-time visualization provided by ultrasound allows the anesthesiologist to accurately identify the target nerve and avoid potential hazards. This reduces the likelihood of adverse events and improves patient outcomes.Furthermore, ultrasound guidance improves the efficacyof nerve blockade. By visualizing the nerves andsurrounding tissues, the anesthesiologist can precisely target the nerve of interest and ensure optimal needle placement. This results in more effective anesthesia, leading to improved pain control and patient satisfaction. Additionally, ultrasound guidance allows for the deposition of local anesthetic agents in close proximity to the nerve, reducing the required dosage and minimizing systemic side effects.From the perspective of the anesthesiologist,ultrasound-guided nerve blockade offers increased accuracy and confidence during the procedure. Traditionally, nerve blocks were performed using landmark-based techniques,which relied on anatomical landmarks and palpation. However, these techniques are often imprecise and can lead to inconsistent results. With ultrasound guidance, the anesthesiologist can directly visualize the nerve, needle, and local anesthetic spread, ensuring accurate placementand optimal distribution of the anesthetic agent.Moreover, ultrasound guidance allows for real-time adjustments and refinements during the procedure. If the initial needle placement does not result in the desired spread of local anesthetic, the anesthesiologist can modify the approach and redirect the needle under direct visualization. This dynamic process ensures that the nerve blockade is performed with precision and adaptability, maximizing the chances of success.From a healthcare system perspective, ultrasound-guided nerve blockade has the potential to reduce healthcare costs. By improving the accuracy and efficacy of nerve blocks, ultrasound guidance can lead to better pain control and reduced reliance on systemic analgesics. This not only improves patient comfort but also decreases the length of hospital stays and the need for additional interventions. Additionally, the reduction in complications associatedwith nerve blockade performed without ultrasound guidance can result in cost savings by avoiding the need for subsequent treatments or interventions to address these complications.In conclusion, ultrasound-guided nerve blockade has become the standard technique for regional anesthesia due to its numerous benefits. From the patient's perspective, it enhances safety and improves pain control, leading to better outcomes and increased satisfaction. For the anesthesiologist, ultrasound guidance provides accuracy, confidence, and the ability to make real-time adjustments. From a healthcare system standpoint, ultrasound-guided nerve blockade has the potential to reduce costs by improving pain management and minimizing complications. Overall, this technique has revolutionized the field of regional anesthesia and continues to be a valuable tool in providing effective and safe pain relief.。
腹横肌平面阻滞技术在腹部手术后镇痛中的应用

腹横肌平面阻滞技术在腹部手术后镇痛中的应用王国湘;王凯元【期刊名称】《山东医药》【年(卷),期】2014(000)014【总页数】3页(P98-100)【关键词】腹横肌平面阻滞;镇痛;腹部手术【作者】王国湘;王凯元【作者单位】蓟县人民医院,天津301900;天津医科大学肿瘤医院【正文语种】中文【中图分类】R614术后疼痛治疗是腹部手术术后管理重要的组成部分。
良好的镇痛可以减少术后并发症发生,缩短住院时间,有利于患者恢复。
腹部手术的疼痛主要来自腹壁切口,传统的静脉自控镇痛或硬膜外镇痛虽然镇痛效果确切,但存在术后恶心、呕吐、过度镇静甚至呼吸抑制等风险。
腹横肌平面(TAP)阻滞是一种区域阻滞方法,即将局部麻醉药注入腹内斜肌和腹横肌之间的筋膜平面以阻断腹壁前侧的神经支配[1],从而减轻皮区腹部切口疼痛,其优点是作用确切,对呼吸、循环及植物神经系统影响小,安全性高[2]。
随着超声技术的引进以及肋缘下穿刺技术的发展,TAP阻滞已经成为腹部手术术后疼痛或前腹壁慢性疼痛综合征的一种诊断工具及治疗手段。
现对TAP在腹部手术术后镇痛中的应用概述如下。
1 TAP阻滞方法1.1 穿刺方法1.1.1 Petit三角盲穿法患者仰卧位,麻醉科医师位于阻滞侧对面,触诊Petit三角,即背阔肌前缘、腹外斜肌后缘和髂嵴共同组成的三角区。
该区域内针尖朝向髂嵴进针,由浅入深穿刺有两次突破感。
第一次突破说明当针尖到达腹外斜肌筋膜及腹内斜肌筋膜之间,第二个突破感说明穿刺针进入TAP平面。
仔细回抽无血后,给予适量局麻药,对侧以同样的方法操作。
1.1.2 超声引导穿刺法超声引导下TAP阻滞需了解不同层面结构回声特点,即脂肪为低回声,腹外斜肌、腹内斜肌及腹横肌为低回声及高回声条带,而目标区域TAP为高回声带。
根据髂嵴与第12肋之间腋前线水平区域患者腹壁进行扫描,获得TAP图像。
探头的纵轴中位线进针,进针过程中保持针身与超声探头纵轴中位线在同一平面,进针回抽无血无气注射局部麻醉药。
超声引导下星状神经节阻滞加快胃癌根治术患者术后胃肠功能恢复

胃癌现居全球癌症发病谱的第5位与死因谱的第4位[1],手术是目前治疗胃癌最有效的、最主要的方法。
胃癌手术破坏了胃肠道的生理解剖和腹腔植物神经系统,引发机体强烈的应激反应,胃肠激素调节失衡也会加剧胃肠道功能的抑制[2]。
因此,降低胃癌患者术后应激反应,稳定胃肠激素水平意味着患者有更好的治疗结局,同时也符合ERAS 理念。
研究表明,神经调节可有效调节围术期应激和胃肠道功能[3]。
交感神经通过抑制平滑肌收缩,粘膜分泌和增强血管收缩而对胃肠道产生抑制作用[4]。
星状神经节阻滞(SGB )作为一种交感神经阻滞术,目前已安全广泛应用于临床[5]。
SGB 能够增强机体免疫功能,稳定手术引起的应激反应[6,7]。
胃肠Ultrasound-guided stellate ganglion block accelerates postoperative gastrointestinal function recovery following laparoscopic radical gastrectomy for gastric cancerLI Xiaoyu,JIANG Yuyu,GU Cuifang,MA Shasha,CHENG XiangyangDepartment of Anesthesiology,First Affiliated Hospital of Bengbu Medical College,Bengbu 233000,China摘要:目的探究超声引导下星状神经节阻滞(SGB )对腹腔镜下胃癌根治术患者围术期应激反应、胃肠激素和术后胃肠功能恢复的影响。
方法择期行腹腔镜胃癌根治术患者60例,性别不限,年龄35~75岁,BMI 18.5~26kg/m 2,ASA 分组Ⅱ~Ⅲ级。
采用随机数字表法将其分为实验组和对照组,各30例。
实验组于麻醉诱导前15min 行超声引导下右侧C 6水平SGB 操作,注入0.5%罗哌卡因7mL 。
超声引导下对门诊病人的区域麻醉(双语)

Local Anesthetics and Adjuvants 局部麻醉剂和佐剂
Local anesthetic (LA) agents should be chosen according to the desired duration of action and the required degree of motor blockade. 局部麻醉剂选 用应根据所需阻滞的持续时间和所需的运动神经阻滞深度, An insensate extremity in a patient whose procedure may not produce much postoperative discomfort may be at risk for injury secondary to the loss of protective reflex to pain, or place the patient at risk secondary to a loss of proprioception本体感 觉—blocks of the longest possible duration are not always the wisest choice. 对一个手术后可能不会有什么不适的病人让其 肢体没有感觉,可能有继发损伤的风险,由于 疼痛保护性反射消失或失去本体感觉,最长阻 滞时间并不总是最明智的选择。
introduction
• Specifically, orthopedic patients are the group of ambulatory patients with the highest incidence (16.1%) of pain in the PACU. • 具体来说,在PACU中骨科病人是门诊病人中疼痛发生率最高 的 • Peripheral nerve blocks (PNBs) offer predictable intraoperative anesthesia, as well as provide analgesia into the postoperative period, the opportunity to bypass Phase I recovery, and the avoidance of airway manipulations. • 外周神经阻滞(PNBs)提供可预测的术中麻醉,还提供术后镇痛, 绕过复苏第一阶段,避免了气道处理。
椎管内麻醉不同给药方法在剖宫产术中的效果

椎管内麻醉不同给药方法在剖宫产术中的效果椎管内麻醉(spinal anesthesia)是一种广泛应用于剖宫产手术的麻醉方法。
它通过将药物注射到脊髓腔(spinal space)中,使患者下半身及腰以下部位失去感觉和运动功能。
椎管内麻醉的效果和安全性取决于许多因素,如给药方法,药物剂量和药物种类等。
本文旨在探讨椎管内麻醉不同给药方法在剖宫产术中的效果。
为了解决这些问题,一些新的椎管内麻醉技术被发明,如微创椎管内麻醉(microcatheter spinal anesthesia)和超声引导下椎管内麻醉(ultrasound-guided spinal anesthesia)。
微创椎管内麻醉是将一根软管插入硬膜外腔,然后通过软管将药物注入脊髓腔中。
这种方法相对于传统椎管内麻醉方法来说有以下优点:(1)注射过程中针头不会与硬膜外层和蛛网膜直接接触,不会产生“空气”现象。
(2)药物注射可以在较长时间内进行,从而更好地控制麻醉深度。
(3)对于有针道技术难度的患者,可以减少并发症的发生。
超声引导下椎管内麻醉是一种新的椎管内麻醉技术,可以通过超声仪器直接观察到患者解剖结构,从而根据患者不同的解剖结构选择最佳的穿刺部位。
这种方法相对于传统椎管内麻醉方法来说有以下优点:(1)穿刺过程更加准确,能够避免硬膜外腔或神经结构受损的风险。
(2)可以更好的控制药物注射的速度和剂量。
(3)可以提高患者的手术满意度和安全性。
总的来说,不同的椎管内麻醉给药方法在剖宫产手术中都能够达到良好的麻醉效果。
传统的椎管内麻醉方法操作简单,作用迅速,但存在一些不足之处。
微创椎管内麻醉和超声引导下椎管内麻醉相对于传统椎管内麻醉方法有更多的优点,可以减少并发症的发生,提高手术效果和患者的手术满意度。
对于患者来说,选择最合适的椎管内麻醉方法是非常重要的。
医生应根据患者的具体情况,选择最佳的椎管内麻醉给药方法。
超声引导下椎旁神经阻滞复合全身麻醉在胸腔镜下肺癌根治术中的麻
超声引导下椎旁神经阻滞复合全身麻醉在胸腔镜下肺癌根治术中的麻醉效果观察发表时间:2019-10-31T16:50:58.303Z 来源:《医药前沿》2019年26期作者:谭栎樊雅玲李照刚[导读] 超声引导下椎旁神经阻滞复合全身麻醉可以有效的促进血流动力学的稳定,减少术中麻醉用药量,苏醒拔管时间较短,是一种理想的胸科手术麻醉方法。
(乐山市人民医院四川乐山 614000)【摘要】目的:观察超声引导下椎旁神经阻滞(PVB)复合全身麻醉在胸腔镜下肺癌根治术的应用效果。
方法:筛取2017年5月—2018年5月我院接受治疗的肺癌患者90例,随机分为对照组和实验组,各45例。
实验组采用超声引导下PVB复合全身麻醉的方法,对照组则是采用静吸复合全身麻醉的方法,比较两组患者手术中特定时间血流动力学变化、手术中用药情况、苏醒拔管时间。
结果:实验组血流动力学相对平稳,麻醉用药量相对较少,苏醒拔管时间较短,两组差异具有统计学意义(P<0.05)。
结论:超声引导下椎旁神经阻滞复合全身麻醉应用效果显著[1]。
【关键词】超声引导;椎旁神经阻滞;全身麻醉;胸腔镜;肺癌根治术【中图分类号】R730.5 【文献标识码】A 【文章编号】2095-1752(2019)26-0026-02Application of ultrasound-guided paravertebral nerve block combined with general anesthesia in thoracoscopic radical resection of lung cancerTan Li, Fan Yaling, Li ZhaogangThe People's Hospital of Leshan,Leshan,Sichuan 614000,China【Abstract】Objective To study the effect of ultrasound-guided paravertebral nerve block combined with general anesthesia in thoracoscopic radical mastectomy, and analyze its clinical effects. Methods 90 patients with lung cancer who were treated in our hospital from May 2017 to May 2018 were screened and divided into two groups, 45 patients in the control group and the experimental group.The experimental group was treated with thoracic paravertebral nerve block combined with general anesthesia,while the control group was treated with general anesthesia with intravenous inhalation.The two groups were observed and compared between the two groups. Flow dynamics,medication during surgery, and time to recovery from anesthesia.Results The hemodynamics of the experimental group was relatively stable, the dose of anesthesia was relatively small, and the recovery time after anesthesia was shorter. The difference between the two groups was statistically significant (P<0.05). Conclusion Ultrasound-guided paravertebral nerve block combined with general anesthesia has a significant effect, which is worthy of further exploration for clinical promotion.【Key words】Ultrasound guidance; Paravertebral nerve block; General anesthesia; Thoracoscopy; Radical mastectomy现如今,超声医学作为一种新兴的医学诊断技术以其效率高、作用速度快、精确度高在临床中逐渐被使用,又由于其患者易接受,医生诊断时间缩短因而很快被众多医院应用。
超声引导下肢神经阻滞
Christian R. Falyar, CRNA, DNAP
Objectives
• Discuss the patient and surgical indications for ultrasound-guided regional anesthesia (UGRA) of the lower extremity
• Explain potential side-effects and complications related to regional anesthesia
Indications
• The choice to use UGRA is determined by many factors such as patient comorbidities, suitability of the technique for the proposed surgery, provider comfort in performing the procedure, as well the mental status of the patient. UGRA has many indications, including:
• The femoral nerve lies lateral to the femoral artery and deep to the fascia lata and iliaca, and superior to the ilopsoas muscle
• The lateral approach is the most common method when using ultrasound
超声引导前锯肌平面阻滞复合全麻对乳腺癌改良根治术患者围手术期免疫功能的影响
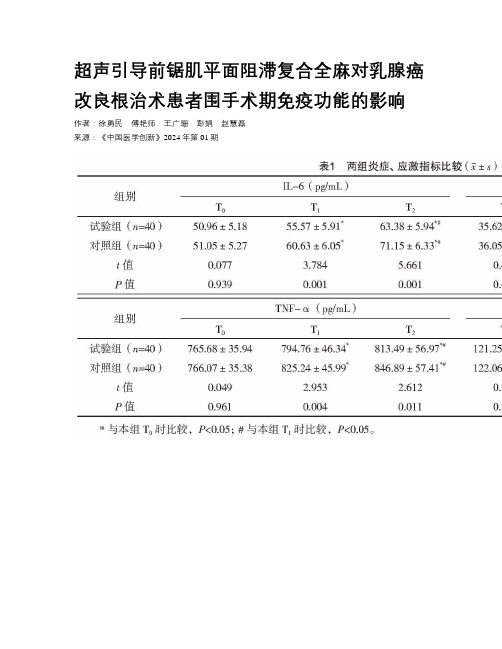
超声引导前锯肌平面阻滞复合全麻对乳腺癌改良根治术患者围手术期免疫功能的影响作者:徐勇民傅艳师王广珊彭娟赵慧磊来源:《中国医学创新》2024年第01期【摘要】目的:探究超声引导前锯肌平面阻滞(SAPB)复合全麻对行乳腺癌改良根治术患者围手术期免疫功能的影响。
方法:选取2020年4月—2022年7月南昌市第三医院收治的80例行乳腺癌改良根治术(MRM)患者,随机分为对照组(n=40)、试验组(n=40)。
对照组在单纯全麻下手术,试验组在超声SAPB复合全麻下手术;于麻醉前30 min(T0)、术中(T1)、术毕时(T2)时,比较两组炎症指标[白细胞介素(IL)-6、IL-8、肿瘤坏死因子-α(TNF-α)]、血清皮质醇(Cor);于术前、术后24 h,比较两组免疫功能(T淋巴细胞亚群);于术后6、12、24、48 h,比较两组疼痛感[视觉模拟评分法(VAS)]。
结果:T1、T2时,两组炎症、应激指标水平较T0时逐渐上升,且试验组各时点IL-6、IL-8、TNF-α、Cor水平均低于对照组(P<0.05)。
术后24 h,两组CD4+均较术前显著下降,CD8+显著升高,但试验组CD4+高于对照组,CD8+低于对照组(P<0.05)。
术后6、12、24、48 h,两组VAS评分逐渐下降,且试验组均低于对照组(P<0.05)。
结论:超声引导SAPB复合全麻应用于MRM 患者中,能够减轻患者应激及炎症反应,缓解疼痛程度,且有一定免疫保护作用。
【关键词】乳腺癌改良根治术全麻前锯肌平面阻滞免疫功能[Abstract] Objective: To investigate the effect of ultrasound guided serratus anterior plane block (SAPB) combined with general anesthesia on immune function in the perioperative period of modified radical mastectomy for breast cancer patients. Method: A total of eighty patients with breast cancer undergoing modified radical mastectomy (MRM) from April 2020 to July 2022 in Nanchang Third Hospital were selected, were randomly divided into control group (n=40) and experimental group (n=40). The control group was operated under simple general anesthesia, and the experimental group was operated under ultrasound guided SAPB combined general anesthesia; at 30 min before anesthesia (T0), intraoperative (T1), and at the end of operation (T2),the inflammatory indicators [interleukin (IL)-6, IL-8, and tumor necrosis factor-α (TNF-α)], serum cortisol (Cor) of the two groups were compared; the immune function (T lymphocyte subsets) of the two groups were compared before and 24 h after operation; at 6, 12,24 and 48 h after operation, the pain sensation [visual analogue scale (VAS)] of the two groups was compared. Result: At T1 and T2, the levels of inflammation and stress indicators in the two groups were gradually increased compared with those at T0, and IL-6, IL-8, TNF-α and Cor in the experimental group at various time points were lower than those in the control group (P<0.05). At 24 h after operation, CD4+ decreased significantly and CD8+ increased significantly in the two groups compared to those preoperative, but CD4+ in the experimental group was higher than that in the control group, and CD8+ was lower than that in the control group (P<0.05). At 6, 12,24, 48 h after operation, the VAS scores of the two groups decreased gradually, and those in the experimental group were lower than those in the control group (P<0.05). Conclusion: The application of ultrasound guided SAPB combined with general anesthesia in MRM patients can alleviate stress and inflammatory reactions, alleviate pain levels, and have a certain degree of immune protection.[Key words] Modified radical mastectomy for breast cancer General anesthesia Serratus anterior plane block Immune function乳腺癌改良根治术(MRM)是根治乳腺癌的主要手段,能够将病变组织彻底切除,但手术创伤较大,涉及乳腺及腋窝区,围手术期会引起应激反应,释放大量炎症细胞因子,加剧患者疼痛感,不利于术后恢复[1-2]。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Hindawi Publishing CorporationAnesthesiology Research and PracticeVolume2011,Article ID579824,6pagesdoi:10.1155/2011/579824Review ArticleUltrasound-Guided Regional Anesthesia forProcedures of the Upper ExtremityFarheen Mirza and Anthony R.BrownCollege of Physicians and Surgeons,Columbia University,New York,NY10027,USACorrespondence should be addressed to Anthony R.Brown,arb6@Received24December2010;Accepted7April2011Academic Editor:Attila BondarCopyright©2011F.Mirza and A.R.Brown.This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use,distribution,and reproduction in any medium,provided the original work is properly cited.Anesthesia options for upper extremity surgery include general and regional anesthesia.Brachial plexus blockade has several advantages including decreased hemodynamic instability,avoidance of airway instrumentation,and intra-,as well as post-operative analgesia.Prior to the availability of ultrasound the risks of complications and failure of regional anesthesia made general anesthesia a more desirable option for anesthesiologists inexperienced in the practice of regional anesthesia.Ultrasonography has revolutionized the practice of regional anesthesia.By visualizing needle entry throughout the procedure,the relationship between the anatomical structures and the needle can reduce the incidence of complications.In addition,direct visualization of the spread of local anesthesia around the nerves provides instant feedback regarding the likely success of the block.This review article outlines how ultrasound has improved the safety and success of brachial plexus blocks.The advantages that ultrasound guidance provides are only as good as the experience of the anesthesiologist performing the block.For example,in experienced hands,with real time needle visualization,a supraclavicular brachial plexus block has changed from an approach with the highest risk of pneumothorax to a block with minimal risks making it the ideal choice for most upper extremity surgeries.1.General Anesthesia versusRegional AnesthesiaAnesthesia options for upper extremity surgery include gen-eral anesthesia,regional anesthesia,or a combination of the two.In the past general anesthesia was frequently the method of choice for upper extremity surgery due to lack of training and experience with regional anesthesia as well as fear of complications including vascular puncture,local anesthetic toxicity,pneumothorax,and patient discomfort[1].Needle placement utilizing the paresthesia technique or peripheral nerve stimulator could be a time-consuming process leading to operating room delays and patient discomfort.However, the advantages of general anesthesia,including control of the airway and familiarity of the technique by the majority of anesthesiologists are overshadowed by the clear benefits of regional anesthesia.These include intraoperative,as well as postoperative analgesia[2,3].In addition,regional anes-thesia results in excellent muscle relaxation during surgery, decreased opioid requirements and their potential side effects,greater hemodynamic stability,increased efficiency in the operating room by avoiding the time required to awaken and extubate the patient,reduced PACU stay,a decrease in unplanned hospital admission for pain control,as well as greater patient satisfaction[2,3].The most significant advantage of regional anesthesia for surgery of the upper extremity is the prolonged postoperative analgesia that a nerve block can provide.The pain relief following brachial plexus blockade with long-acting local anesthetics such as bupivacaine,ropivacaine and levobupivacaine has resulted in patients being discharged home on the day of surgery as opposed to a planned or unplanned overnight admission [3,4].2.Brachial Plexus AnatomyThompson and Rorie performed cadaveric studies to map out the brachial plexus anatomy[5].Thefifth through eighth cervical andfirst thoracic nerve exit through theintervertebral foramina and travel along the groove formed by the transverse processes of their corresponding vertebrae. After exiting the transverse processes the roots of the brachial plexus travel between the anterior and the middle scalene muscles,identified as the interscalene groove[1].The authors reported that the brachial plexus is confined by a continuous fascial sheath formed by the deep cervical fascia and that the fascia is continuous from emergence of the nerve roots to the axilla.Distally the fascia folds inwards to form separate compartments for each nerve.For example,at the cord level,local anesthetic injected around the posterior cord may not spread to include the lateral or medial cords[6–8]whereas an axillary brachial plexus block is performed by identifying the individual nerves and blocking each one separately[9–11].While an interscalene block is performed by means of a single injection technique,the more distal approach to the brachial plexus,the less likely that a single injection technique will result in complete blockade of the upper extremity[12–14].3.Basics of UltrasoundUltrasound probes(transducers)act as both a transmitter and receiver of sound waves.The probes are classified as either high(10–15MHz),midrange(5–10MHz),or low (<5MHz)frequency.High-frequency probes provide high-resolution images but lack depth of penetration compared to low-frequency probes[15].Both frequency types are available with a wide or a narrow footprint.High-resolution linear transducers are most suitable for imaging superficial structures such as the brachial plexus in the interscalene, supraclavicular,and axillary regions.The lower frequency curved transducer is preferable when the anatomical struc-tures are deeper than4cm,for example,when performing an infraclavicular block[16].Prior to the use of ultrasound, block needle placement was achieved using a blind approach with the nerve stimulation or paresthesia technique.Ultra-sound imaging has revolutionized the practice of regional anesthesia in that the operator can visualize and identify nerves and blood vessels as well as the needle during its passage through the tissues.Abnormal anatomy can also be recognized[17].In addition,direct visualization of the spread of local anesthetic decreases the risk of intravascular injection,local anesthetic toxicity,pneumothorax,and a failed block[18].It is important to remember,however, that the success of an ultrasound-guided block is dependent upon the skill and experience of the anesthesiologist.Anes-thesiologists performing brachial plexus anesthesia under ultrasound guidance mustfirst become comfortable with identifying anatomical structures as well as visualizing the needle during the block performance.In experienced hands, the benefits of performing a peripheral nerve block with real-time ultrasound imaging of needle placement and local anesthesia spread include decreased performance as well as onset time,a decreased dose of local anesthetic required to achieve a successful block,and an increase in block success rate[19–24].In a systematic review and meta-analysis of ran-domized controlled trials comparing ultrasound guidance with electrical neurostimulation for peripheral nerve blocks, Abrahams et al.confirmed these aforementioned benefits of ultrasound.However,the authors concluded that larger studies are needed to determine whether ultrasound can decrease the number of complications[25].4.Patient PreoperativeEvaluation and EducationThe success of a regional anesthesia program is dependent on patient education and the support of the surgical team. T o put a patient at ease it is desirable for the surgeon to inform the patient about the possibility of receiving a brachial plexus block for his or her surgery prior to the day of surgery.A patient that has been informed beforehand is often more amenable to accepting regional anesthesia.In addition,the training,education,and skill of the individual performing the block are of paramount importance.T o this end,both the American as well as the European Society of Regional Anesthesia(ASRA and ESRA)hold annual meetings as well as numerous workshops throughout the year to educate and train individuals in the art of regional anesthesia[26].There are few absolute contraindications to a brachial plexus block.These include patient refusal, local anesthetic allergy,infection at the site of needle entry, and the presence of infected lymph nodes in the axilla or supraclavicular region[7,27].Deep blocks,for example,an infraclavicular approach,as well as blocks in the vicinity of a noncompressible artery(e.g.,supraclavicular)should not be performed in coagulopathic patients[6,7].A patient that is unable to cooperate secondary to decreased mental status is also an absolute contraindication.Regional anesthesia is not contraindicated in patients that have a pre-existing stable neurological deficit or chronic neurological disease provided that the condition is well documented[28,29]. It is up to the anesthesiologist to decide,based on each individual patient’s risk benefit ratio whether performance of a peripheral nerve block in the presence of pre-existing nerve damage is indicated[30].An informed cooperative patient is an essential factor in ensuring safe and effective regional anesthesia.Following a brachial plexus block,it is essential that the affected extremity be immobilized and protected until loss of sensation and proprioception have resolved.Patients and family members should receive clear instructions regarding the anticipated duration of the block and how to transition to oral analgesia at home to avoid the sudden onset of pain.5.Anesthetic TechniquesDe Andres and Sala-Blanch state that it is essential to under-stand both the topographic anatomy and cross-sectional anatomy of each anatomic zone of the brachial plexus[15]. They describe the brachial plexus as being divided into three zones:the supraclavicular region in the posterior triangle of the neck,the infraclavicular region deep to the pectoralis muscles in the anterior chest,and the axillary region.The level of needle entry in one of these zones will determine theextent,limitations,and potential complications of a brachial plexus block.Prior to the use of ultrasound,the likelihood of encountering the spinal cord,the lung,and major vessels such as the subclavian and vertebral arteries with the more proximal approaches(interscalene and supraclavicular)was a concern[31].Ultrasound has minimized these risks provided that the needle tip as well as the spread of local anesthetic is constantly visualized throughout performance of the block[20,32].The choice of which technique to use is dependent on the surgical procedure,the comfort and expertise of the anesthesiologist,and patient-associated factors such as sepsis in the axilla.In the latter case a more proximal approach is desirable[30].6.Interscalene BlockThe interscalene approach to the brachial plexus is the technique of choice for surgical procedures of the shoulder. It is inappropriate for surgeries involving the medial aspect of the upper extremity due to inconsistent blockade of the lower trunk(C8and T1)[33,34].At the level of the cricoid cartilage the brachial plexus trunks appear as three distinct hypoechoic areas between the anterior and middle scalene muscles[1,35].It should be emphasized that the large doses of local anesthetic traditionally used for an interscalene block with the neurostimulation technique result in a100%inci-dence of ipsilateral phrenic nerve paralysis due to blockade of the3rd,4th,and5th cervical nerve roots.This may decrease the patient’s FRC by25%[36]and may therefore not be suitable for patients with emphysema and other chronic lung diseases with decreased pulmonary reserve.Ultrasound imaging improves the interscalene approach primarily by being able to visualize the spread of local anesthetic within the fascia surrounding the trunks.This direct visualization decreases the amount of local anesthetic needed to provide surgical anesthesia[37,38].Decreasing the volume of local anesthetic to10mL or5mL resulted in a significant decrease in the incidence of hemidiaphragmatic paresis[37,39,40]. Kapral et al.report that ultrasound guidance improves both the quality of the nerve block and shortens the time of onset of sensory blockade[22].7.Supraclavicular BlockThe supraclavicular block was traditionally performed for surgeries of the upper extremity below the shoulder.Liu et al.,however,recently reported that ultrasound-guided supraclavicular blocks are effective and safe for shoulder arthroscopy[41].The supraclavicular approach has several advantages over the more distal approaches including rapid onset of the block,more complete blockade of the nerves supplying the upper extremity(with the exception of the intercostobrachial nerve)due to the compact arrangement of the trunks of the brachial plexus at this level[32,42].Prior to the use of ultrasound the supraclavicular approach was frequently avoided,particularly in ambulatory surgeries,due to the increased risk of pneumothorax and,to a lesser extent,direct vascular puncture of the subclavian,superficial(trans-verse)cervical,suprascapular,or dorsal scapular arteries with subsequent local anesthetic toxicity and cardiovascular collapse[43,44].Ultrasound has improved the safety of a supraclavicular block as the anesthesiologist can now visualize the subclavian artery,thefirst rib,as well as the dome of the lung.Placement of the needle and spread of the local anesthetic can now be seen in real-time resulting in resurgence in the use of this block[17,45].Chan et al. examined the supraclavicular region in40patients and reported that in all cases the nerves of the brachial plexus appeared as hypoechoic nodules in clusters lateral,posterior, and cephalad to the subclavian artery[46].The authors also concluded that if the needle is seen at all times and not inserted beyond thefirst rib,then the risk of a pneumothorax in a supraclavicular block is essentially eliminated.Williams found that supraclavicular nerve blocks were performed faster with ultrasound guidance when compared with nerve stimulation(5versus10min)[20].Ultrasound guidance has increased the safety profile of the supraclavicular approach so that in experienced hands this may be the block of choice for most upper extremity surgeries below the shoulder.8.Infraclavicular BlockThe infraclavicular approach is indicated for surgeries of the arm and pared to the supraclavicular approach, the risk of pneumothorax is significantly reduced and is virtually eliminated with the use of ultrasound.In addition, the phrenic nerve is not blocked with this approach[47]. Compared to the axillary approach,the infraclavicular block targets the brachial plexus at the level of the cords which surround the second part of the axillary artery and are proximal to the takeoffof the musculocutaneous,axillary, and medial brachial cutaneous nerves.This may result in a higher success rate of complete blockade with a single injection technique[48].The infraclavicular anatomy may, however,be more difficult to visualize under ultrasound guidance particularly in obese patients.Perlas et al.found that compared to the interscalene,supraclavicular,axillary, and midhumeral approaches in which the brachial plexus was visualized100%of the time,in only27%of patients were they able to visualize the infraclavicular brachial plexus[1, 49].This difficulty is due to the relative depth of the brachial plexus in the infraclavicular approach compared to all other approaches to the brachial plexus.A low-frequency probe with its greater tissue penetration may facilitate performance of this block[47].In an ultrasound-guided infraclavicular block the lateral,posterior,and medial cords are seen in close proximity to the axillary artery and vein.The posterior cord is usually blockedfirst.If the spread of local anesthetic does not surround the lateral and medial cords,then all three cords must be blocked individually to obtain complete block-ade of the upper extremity.As with the supraclavicular and axillary approaches,the intercostobrachial nerve will have to be blocked separately in the axilla to achieve anesthesia of the inner aspect of the upper arm.9.Axillary BlockAxillary blocks are performed for procedures of the elbow, distal arm,and hand.Prior to the use of ultrasound,the axillary approach was the most common approach to the brachial plexus due to the safety of this technique.As with the infraclavicular block,the risk of phrenic nerve paresis is avoided and the risk of pneumothorax is eliminated.The high success rate without respiratory compromise makes this block desirable in patients with reduced lung capacities and chronic pulmonary diseases[50].Contraindications to the axillary approach include inability to abduct the arm to the position necessary to perform the block,localized infection in the axilla,or enlarged axillary lymph nodes[51].A major advantage of using ultrasound in an axillary approach is the ability to confirm blockade of the musculocutaneous nerve[52].Because of the anatomical variance of the musculocutaneous nerve in relation to the axillary artery, failure to block this nerve with a perivascular approach in not uncommon[53].At the axillary level,the terminal branches of the brachial plexus(median,ulnar,and radial nerves)are situated close to the axillary artery and veins with the two axillary veins situated medial to the artery.There is,however, a great deal of variation in the distribution of these three nerves in relation to the artery[54].The four nerves are easily visualized utilizing ultrasonography.The ultrasound guided axillary approach has been shown to both decrease block failure rate and time of onset of sensory blockade compared to the transarterial technique[14].The success of US guided axillary blocks depends on the multiple needle approach in which each nerve is identified individually and spread of local anesthetic is observed around the median,ulnar,radial,and musculocutaneous nerves.10.Distal Upper Extremity BlocksIndividual terminal nerve blocks can be performed at the midhumeral,elbow,forearm,or wrist either by design or as a rescue block[7].These more peripheral nerve blocks may be performed to achieve postoperative analgesia while at the same time maintaining more proximal control of the upper extremity.11.Postoperative Pain ControlPostoperative pain and nausea are the leading causes of unplanned hospital admission after ambulatory surgery[55]. Orthopedic upper extremity surgery is reported as having a high incidence of severe pain[56].One of the clear benefits of regional anesthesia over general anesthesia for upper extrem-ity surgery is the postoperative pain relief a long-acting local anesthetic can provide.The choice of local anesthetic is determined by the duration of surgery,necessity of motor blockade,urgency of neurological assessment after surgery, and the anticipated requirement for postoperative analgesia. In brachial plexus nerve blocks short-,intermediate-,and long-acting local anesthetics can be chosen.Bupivacaine, ropivacaine,and levobupivacaine are equally effective in surgeries in which extended postoperative analgesia would be beneficial.In comparison to bupivacaine,however,ropiva-caine and levobupivacaine are the long-acting local anes-thetics of choice due to their decreased cardiotoxicity[57–59].It is important for the patient to be informed of the anticipated duration of the local anesthetic so that he or she will not be concerned about the length of time it takes for the block to wear off.It is also essential that patients be instructed regarding protection of the extremity until sensation has completely returned.Finally,patients should be instructed to take their prescribed oral analgesics at the earliest sign of pain to mitigate against the analgesic gap that may otherwise develop.Additional methods to improve and or prolong postoperative analgesia include insertion of a brachial plexus catheter to provide continuous regional analgesia[51,60]as well as the use of multimodal analgesia. In the multimodal approach use of a long-acting peripheral nerve block in combination with acetaminophen,NSAIDs (when not contraindicated),and oral opioid analgesics will minimize the total opioid requirements and their resulting side effects[61,62].12.ConclusionThe various approaches to the brachial plexus afford the anesthesiologist the ability to provide both excellent intra-operative anesthesia as well as postoperative analgesia with minimal complications and increased patient satisfaction following upper extremity surgery.The advantages over general anesthesia are numerous when performed in skilled hands.Ultrasound guidance with real-time needle visual-ization in relation to anatomic structures and target nerves makes regional anesthesia safer and more successful.With ultrasound guidance in experienced hands,brachial plexus blockade can lead to decreased block performance and onset time,increased success rate and decreased rate of com-plications.These advantages result in increased operating room efficiency,as well as increased patient and surgeon satisfaction.References[1]A.Perlas,V.W.S.Chan,and M.Simons,“Brachial plexusexamination and localization using ultrasound and electrical stimulation:a volunteer study,”Anesthesiology,vol.99,no.2, pp.429–435,2003.[2]J.G.D’Alessio,M.Rosenblum,K.P.Shea,and D.G.Freitas,“A retrospective comparison of interscalene block and general anesthesia for ambulatory surgery shoulder arthroscopy,”Regional Anesthesia and Pain Medicine,vol.20,no.1,pp.62–68,1995.[3]A.R.Brown,R.Weiss,C.Greenberg, E.L.Flatow,andL.U.Bigliani,“Interscalene block for shoulder arthroscopy: comparison with general anesthesia,”Arthroscopy,vol.9,no.3,pp.295–300,1993.[4]B.M.Ilfeld and F.K.Enneking,“Continuous peripheral nerveblocks at home:a review,”Anesthesia&Analgesia,vol.100,no.6,pp.1822–1833,2005.[5]G.E.Thompson and D.K.Rorie,“Functional anatomy of thebrachial plexus sheaths,”Anesthesiology,vol.59,no.2,pp.117–122,1983.[6]C.Ootaki,H.Hayashi,and M.Amano,“Ultrasound-guidedinfraclavicular brachial plexus block:an alternative technique to anatomical landmark-guided approaches,”Regional Anes-thesia and Pain Medicine,vol.25,no.6,pp.600–604,2000. [7]N.S.Sandhu and L.M.Capan,“Ultrasound-guided infraclav-icular brachial plexus block,”British Journal of Anaesthesia, vol.89,no.2,pp.254–259,2002.[8]E.Gaertner,J.P.Estebe,A.Zamfir,C.Cuby,and P.Macaire,“Infraclavicular plexus block:multiple injection versus single injection,”Regional Anesthesia and Pain Medicine,vol.27,no.6,pp.590–594,2002.[9]S.Sia,M.Bartoli,A.Lepri,O.Marchini,and P.Ponsecchi,“Multiple-injection axillary brachial plexus block:a compar-ison of two methods of nerve localization-nerve stimulation versus paresthesia,”Anesthesia&Analgesia,vol.91,no.3,pp.647–651,2000.[10]G.Retzl,S.Kapral,M.Greher,and W.Mauritz,“Ultrasono-graphicfindings of the axillary part of the brachial plexus,”Anesthesia&Analgesia,vol.92,no.5,pp.1271–1275,2001. [11]Z.J.Koscielniak-Nielsen,H.L.Stens-Pedersen,and F.K.Lippert,“Readiness for surgery after axillary block:single or multiple injection techniques,”European Journal of Anaesthe-siology,vol.14,no.2,pp.164–171,1997.[12]W.T.Y ang,P.T.Chui,and C.Metreweli,“Anatomy of thenormal brachial plexus revealed by sonography and the role of sonographic guidance in anesthesia of the brachial plexus,”American Journal of Roentgenology,vol.171,no.6,pp.1631–1636,1998.[13]B.D.Sites,M.L.Beach,B.C.Spence et al.,“Ultrasoundguidance improves the success rate of a perivascular axillary plexus block,”Acta Anaesthesiologica Scandinavica,vol.50,no.6,pp.678–684,2006.[14]Q.H.Tran, A.Clemente,J.Doan,and R.J.Finlayson,“Brachial plexus blocks:a review of approaches and tech-niques,”Canadian Journal of Anesthesia,vol.54,no.8,pp.662–674,2007.[15]J.De Andres and X.Sala-Blanch,“Ultrasound in the practiceof brachial plexus anesthesia,”Regional Anesthesia and Pain Medicine,vol.27,no.1,pp.77–89,2002.[16]P.Marhofer,H.Willschke,and S.Kettner,“Current conceptsand future trends in ultrasound-guided regional anesthesia,”Current Opinion in Anaesthesiology,vol.23,no.5,pp.632–636, 2010.[17]A.T.Gray,“Ultrasound-guided regional anesthesia:currentstate of the art,”Anesthesiology,vol.104,no.2,pp.368–373, 2006.[18]P.Marhofer,M.Greher,and S.Kapral,“Ultrasound guidancein regional anaesthesia,”British Journal of Anaesthesia,vol.94, no.1,pp.7–17,2005.[19]B.D.Sites and R.Brull,“Ultrasound guidance in peripheralregional anesthesia:philosophy,evidence-based medicine,and techniques,”Current Opinion in Anaesthesiology,vol.19,no.6, pp.630–639,2006.[20]S.R.Williams,P.Chouinard,G.Arcand et al.,“Ultrasoundguidance speeds execution and improves the quality of supraclavicular block,”Anesthesia&Analgesia,vol.97,no.5, pp.1518–1523,2003.[21]S.S.Liu,J.E.Ngeow,and J.T.Y aDeau,“Ultrasound-guidedregional anesthesia and analgesia:a qualitative systematic review,”Regional Anesthesia and Pain Medicine,vol.34,no.1, pp.47–59,2009.[22]S.Kapral,M.Greher,G.Huber et al.,“Ultrasonographicguidance improves the success rate of interscalene brachialplexus blockade,”Regional Anesthesia and Pain Medicine,vol.33,no.3,pp.253–258,2008.[23]P.Marhofer,K.Schr¨o gendorfer,T.Wallner,H.Koinig,N.Mayer,and S.Kapral,“Ultrasonographic guidance reduces the amount of local anesthetic for3-in-1blocks,”Regional Anesthesia and Pain Medicine,vol.23,no.6,pp.584–588,1998.[24]P.Marhofer and V.W.S.Chan,“Ultrasound-guided regionalanesthesia:current concepts and future trends,”Anesthesia& Analgesia,vol.104,no.5,pp.1265–1269,2007.[25]M.S.Abrahams,M.F.Aziz,R.F.Fu,and J.L.Horn,“Ultra-sound guidance compared with electrical neurostimulation for peripheral nerve block:a systematic review and meta-analysis of randomized controlled trials,”British Journal of Anaesthesia,vol.102,no.3,pp.408–417,2009.[26]M.P.Smith,J.Sprung,A.Zura,E.Mascha,and J.E.T etzlaff,“A survey of exposure to regional anesthesia techniques in American anesthesia residency training programs,”Regional Anesthesia and Pain Medicine,vol.24,no.1,pp.11–16,1999.[27]F.J.Singelyn,S.Seguy,and J.M.Gouverneur,“Intersca-lene brachial plexus analgesia after open shoulder surgery: continuous versus patient-controlled infusion,”Anesthesia& Analgesia,vol.89,no.5,pp.1216–1220,1999.[28]J.R.Hebl,T.T.Horlocker, E.J.Sorenson,and D.R.Schroeder,“Regional anesthesia does not increase the risk of postoperative neuropathy in patients undergoing ulnar nerve transposition,”Anesthesia&Analgesia,vol.93,no.6,pp.1606–1611,2001.[29]T.T.Horlocker,R.P.Kufner,A.T.Bishop,P.M.Maxson,and D.R.Schroeder,“The risk of persistent paresthesia is not increased with repeated axillary block,”Anesthesia& Analgesia,vol.88,no.2,pp.382–387,1999.[30]A.R.Brown,“Anaesthesia for procedures of the hand andelbow,”Best Practice and Research,vol.16,no.2,pp.227–246, 2002.[31]A.Borgeat,G.Ekatodramis,F.Kalberer,and C.Benz,“Acuteand nonacute complications associated with interscalene block and shoulder surgery:a prospective study,”Anesthesiol-ogy,vol.95,no.4,pp.875–880,2001.[32]S.Kapral,P.Krafft,K.Eibenberger,R.Fitzgerald,M.Gosch,and C.Weinstabl,“Ultrasound-guided supraclavicular approach for regional anesthesia of the brachial plexus,”Anesthesia&Analgesia,vol.78,no.3,pp.507–513,1994. [33]A.P.Winnie,“Interscalene brachial plexus block,”Anesthesia&Analgesia,vol.49,no.3,pp.455–466,1970.[34]D.L.Brown,“Brachial plexus anesthesia:an analysis ofoptions,”Yale Journal of Biology and Medicine,vol.66,no.5, pp.415–431,1993.[35]V.W.S.Chan,“Applying ultrasound imaging to interscalenebrachial plexus block,”Regional Anesthesia and Pain Medicine, vol.28,no.4,pp.340–343,2003.[36]W.F.Urmey and M.McDonald,“Hemidiaphragmatic paresisduring interscalene brachial plexus block:effects on pul-monary functin and chest wall mechanics,”Anesthesia& Analgesia,vol.74,no.3,pp.352–257,1992.[37]S.Riazi,N.Carmichael,I.Awad,R.M.Holtby,and C.J.L.McCartney,“Effect of local anaesthetic volume(20vs5ml) on the efficacy and respiratory consequences of ultrasound-guided interscalene brachial plexus block,”British Journal of Anaesthesia,vol.101,no.4,pp.549–556,2008.[38]A.Al-Kaisy,G.McGuire,V.W.S.Chan et al.,“Analgesiceffect of interscalene block using low-dose bupivacaine for outpatient arthroscopic shoulder surgery,”Regional Anesthesia and Pain Medicine,vol.23,no.5,pp.469–473,1998.。