头孢他啶说明书
注射用头孢他啶 说明书1g
中、重度肾功能损害者本品的消除半衰期延长,当内生肌酐清除率≤2ml/分钟时,消除半衰期可延长至14~30小时。在新生儿中的半衰期稍延长(平均4~5小时)。本品可通过血液透析清除。
5、临床检验结果的改变:发生短暂性的血清氨基转移酶、乳酸脱氢酶、碱性磷酸酶、血尿素氮、血肌酐值的轻度升高;白细胞、血小板减少及嗜酸性粒细胞增多、淋巴细胞增多等。
【禁忌】
对本品或其它头孢菌素类抗生素过敏者禁用。
【注意事项】
1.交叉过敏反应:对一种头孢菌素或头霉素(cephamycin)过敏者对其他头孢菌素或头霉素也可能过敏。对青霉素类、青霉素衍生物或青霉胺过敏者也可能对头孢菌素或头霉素过敏。对青霉素过敏病人应用头孢菌素时发生过敏反应者达5%~10%;如作过敏试验,则对青霉素过敏病人对头孢菌素过敏者达20%。
注射用头孢他啶
【药品名称】
【通用名称】
注射用头孢他啶
【商品名】
【英文名】
Ceftazidime for Injection
【汉语拼音】
Zhusheyong Toubaotading
【成份】
【化学名称】
(6R,7R)-7-[[(2-氨基-4-噻唑基)-[(1-羧基-1-甲基乙氧基)亚氨基]乙酰基]氨基]-2-羧基-8-氧代-5-硫杂-1-氮杂双环[4.2.0]辛-2-烯-3-甲基吡啶鎓内盐五水合物
5.同其他抗生素一样,长期使用本品可导致非敏感菌过度生长。应注意监察二重感染的发生并采取相应措施。
6.对重症革兰氏阳性球菌感染,本品为非首选品种。
7.对诊断的干扰:应用本品的病人直接抗球蛋白(Coombs)试验可出现阳性;本品可使硫酸铜尿糖试验呈假阳性;血清丙氨酸氨基转移酶(ALT)、门冬氨酸氨基转移酶(AST)、碱性磷酸酶、血尿素氮和血清肌酐皆可升高。
注射用头孢他啶说明书
注射用头孢他啶说明书请仔细阅读说明书并在医师指导下使用【药品名称】通用名称:注射用头孢他啶英文名称:Ceftazidime for Injection汉语拼音:Zhusheyong Toubaotading【成份】本品活性成份为头孢他啶,化学名称:(6R, 7R)-7-[[(2-氨基-4-噻唑基)-[(1-羧基-1-甲基乙氧基)亚氨基]乙酰基]氨基]-2-羧基-8-氧代-5-硫杂-1-氮杂双环[4.2.0]辛-2-烯-3-甲基吡啶鎓内盐五水合物。
化学结构式:分子式:C22H22N6O7S2·5H2O分子量:辅料:碳酸钠。
【性状】本品为白色或类白色结晶性粉末。
【适应症】用于敏感革兰氏阴性杆菌所致的败血症、下呼吸道感染、腹腔和胆道感染、复杂性尿路感染和严重皮肤软组织感染等。
对于由多种耐药革兰氏阴性杆菌引起的免疫缺陷者感染、医院内感染以及革兰氏阴性杆菌或铜绿假单胞菌所致中枢神经系统感染尤为适用。
【规格】1.0g(按头孢他啶计)【用法用量】静脉注射或静脉滴注。
剂量依感染的严重程度、微生物敏感性及患者机体状态而定。
成人:1. 败血症、下呼吸道感染、胆道感染等,一日4~6g,分2~3次静脉滴注或静脉注射,疗程10~14日。
2. 泌尿系统感染和重度皮肤软组织感染等,一日2~4g,分2次静脉滴注或静脉注射,疗程7~14日。
对于轻度尿路感染,每12小时~1g即已足够。
3. 对于某些危及生命的感染、严重铜绿假单胞菌感染和中枢神经系统感染,可酌情增量至一日~0.2g/kg,分3次静脉滴注或静脉注射。
儿童:2个月以上婴幼儿常用剂量为一日30~100mg/kg,分2~3次静脉滴注。
对新生儿至2个月婴儿临床经验有限。
肾功能损害患者:因头孢他啶主要经肾脏排泄,对肾功能损害患者应减量使用。
可根据肌酐清除率来计算合适的给药剂量。
透析后患者应重复适当维持剂量。
配制方法:5ml注射用水加入0.5g装瓶中或10ml注射用水加入1g或2g装瓶中,使完全溶解后,于3~5分钟静脉缓慢推注。
使用注射用头孢他啶需要注意哪些事项
使用注射用头孢他啶需要注意哪些事项
注射用头孢他啶为第三代头孢菌素类抗生素。
目前,注射用头孢他啶
用于敏感革兰阴性杆菌所致的败血症、下呼吸道感染、腹腔和胆道感染、复杂性尿路感染和严重皮肤软组织感染等。
对于由多种耐药革兰
阴性杆菌引起的免疫缺陷者感染、医院内感染以及革兰阴性杆菌或铜
绿假单胞菌所致中枢神经系统感染尤为适用。
那么,使用注射用头孢他啶需要注意哪些事项?
说明书介绍,注射用头孢他啶的注意事项主要有交叉过敏反应:对一
种头孢菌素或头霉素(cephamycin)过敏者对其他头孢菌素或头霉素也
可能过敏。
对青霉素类、青霉素衍生物或青霉胺过敏者也可能对头孢
菌素或头霉素过敏。
对青霉素过敏病人应用头孢菌素时发生过敏反应
者达5%~10%;如作免疫反应测定时,则对青霉素过敏病人对头孢菌素
过敏者达20%。
对青霉素过敏病人应用本品时应根据病人情况充分权衡利弊后决定。
有青霉素过敏性休克或即刻反应者,不宜再选用头孢菌素类。
有胃肠道疾病史者,特别是溃疡性结肠炎、局限性肠炎或抗生素相关
性结肠炎(头孢菌素类很少产生假膜性结肠炎)者应慎用。
肾功能不全者应减量并慎用。
用药期间应进行尿液化验,如果损及肾
功能,则应停药。
本品可引起血象改变,严重时应立即停药。
本品溶解后应立即使用,否则药液色泽会变深。
对诊断的干扰:使用本品期间,用碱性酒石酸铜试液进行尿糖实验时,可有假阳性反应;直接抗球蛋白(Coombs)试验可出现假阳性反应。
以生理盐水,5%葡萄糖注射液或乳酸钠稀释成的静脉注射液(20mg/ml)在室温存放不宜超过24小时。
注射用头孢他啶说明书

亲爱的朋友,很高兴能在此相遇!欢迎您阅读文档注射用头孢他啶说明书,这篇文档是由我们精心收集整理的新文档。
相信您通过阅读这篇文档,一定会有所收获。
假若亲能将此文档收藏或者转发,将是我们莫大的荣幸,更是我们继续前行的动力。
注射用头孢他啶说明书注射用头孢他啶又叫复达欣是一种白色至淡黄色的粉剂。
下面是我们整理的,希望对大家有所帮助!注射用头孢他啶商品介绍通用名:注射用头孢他啶生产厂家:葛兰素史克制药(苏州)有限公司批准文号:药品规格:1g/瓶药品价格:¥78元注射用头孢他啶又叫复达欣是一种白色至淡黄色的粉剂。
每克含钠近52mg,116mg的头孢他啶五水合物相等于100mg的头孢他啶游离酸。
药代动力学肌注给药500mg和1g后,可迅速达到高血药浓度18mg/L和37mg/L,静脉注射500mg、1g和2g,5分钟后平均血浓度为46mg/L,87mg/L和170mg/L。
肌注或静注8-12小时后,血中有效浓度仍然存在,血清半衰期约为1.8小时。
复达欣的血清蛋白结合率较低,约为10%左右。
头孢他啶在体内不代谢,以其原形经肾小球滤过而排泄,在24小时内,将近80-90%的剂量从尿中排出,少于1%的剂量通过胆汁排泄,故明显地限制了进入肠道的药量。
复达欣在组织中,如骨骼、心脏、胆汁、痰液、房水、滑囊液、胸膜液及腹膜液中可达到MIC的浓度。
头孢他啶易于通过胎盘,但难于通过正常的血脑屏障,在无炎症的情况下,脑脊髓液中药物浓度很低,当脑膜有炎症时,脑脊液中的药物浓度可达4-20mg/L或以上。
用法用量成人一般给予1g/次,每日3次或2g/次,每日2次肌注或静注。
严重感染可增至2g/次,每日2-3次。
囊性纤维化的成人100-150mg/kg体重/日,分3次给药,大剂量9g。
2个月以上的儿童30-100mg/kg体重/日,分2-3次给药,严重感染时给予50mg/kg体重/次,每8小时一次,大剂量为6g/日。
2个月以下的婴儿和新生儿25-60mg/kg体重/日,分2次给药。
注射用头孢他啶(复达欣)使用说明书

大约浓度 (mg/ml) 210 90 260 90 260 90 170 40# 170 40#
注: * 溶液的加入应分为两步。 # 使用0.9%的氯化钠注射液、5%葡萄糖注射液或其他批准使用的稀释液(见 药物【注意事项】)因为注射用水在此浓度产生低渗溶液。 所有瓶装的复达欣®注射剂均是经过减压的。药品溶解时会释放二氧化碳,因而 产生正压力。为方便使用,推荐采用下列调制技术: 250mg肌肉或静脉注射,500mg肌肉或静脉注射,1g肌肉或静脉注射,2g 或3g静脉推注: 1、将注射器针头插入药瓶封口,注入推荐剂量的稀释液,真空将使得稀释液进 入瓶中,拔出针头。 2、摇动至溶解,释放出二氧化碳,1-2分钟后成澄清的溶液。 3、将瓶倒置,把注射器针芯推到头后,将针头插入药瓶封口,全部的溶液就被 吸入注射器(瓶中的压力会促使溶液吸入),保持针头在溶液内。溶液中的细小 二氧化碳气泡可不予理会。 这些溶液可直接注入静脉或当病人接受肠胃外液体时, 可直接投入给药的 管子里。头孢他啶可与常用的静脉注射溶液配伍。 供应复达欣®注射剂的小瓶经过减压。在调制时由于释放二氧化碳会产生 正压。 瓶装的复达欣®注射剂不含任何防腐剂,因此只能用作单次剂量。 为了符合制剂的管理要求,最好使用新配制的复达欣®注射液。如果不能 实现,存放在2~8oC冰箱中保存24小时可保持药效。(当稀释液为注射用水BP或 任何以下所列的注射液)
<5
3
调制指导:需加稀释液量及溶液浓度见下表,需要采用部份剂量时,该表可能有 用。 溶液的调制: 瓶量 250mg肌肉注射 250mg静脉注射 500mg肌肉注射 500mg静脉注射 1g肌肉注射 1g静脉注射 2g静脉推注 2g静脉滴注 3g静脉推注 3g静脉滴注
需加稀释液量 (ml) 1.0 2.5 1.5 5.0 3.0 10.0 10.0 50.0* 15.0 75.0*
头孢他啶说明书
头孢他啶说明书【通用名】:头孢他啶【英文名】:Ceftazidime【汉语拼音】:Toubaotading【化学名】:(6R ,7R)-7-[[(2-氨基-4-噻唑基)-[(1-羧基-1-甲基乙氧基)亚氨基]乙酰基]氨基]-2-羧基-8-氧代-5-硫杂-1-氮杂双环[4.2.0]辛-2-烯-3-甲基吡啶鎓内盐五水合物【理化性质】:本品为白色或类白色结晶性粉末【药理毒理】本品为第三代头孢菌素类抗生素。
抗菌谱广,对多数革兰氏阳性菌和阴性菌有效。
对大肠埃希菌、肺炎杆菌等肠杆菌科细菌和流感嗜血杆菌、铜绿假单胞菌等有高度抗菌活性。
对硝酸盐阴性杆菌、产碱杆菌等亦有良好抗菌作用。
对于细菌产生的大多数β-内酰胺酶高度稳定,故其对上述革兰阴性杆菌中多重耐药菌株仍可具抗菌活性。
肺炎球菌、溶血性链球菌等革兰阳性球菌对本品高度敏感,但本品对葡萄球菌仅具中度活性,肠球菌和耐甲氧西林葡萄球菌则往往对本品耐药。
本品对消化球菌和消化链球菌等厌氧菌具一定抗菌活性,但对脆弱拟杆菌抗菌作用差。
本品为杀菌药,作用机制为与细菌细胞膜上的青霉素结合蛋白(PBPs)结合,使转肽酶酰化,影响细胞壁粘肽成分的交叉连结,抑制细菌细胞壁的合成,使细胞分裂和生长受到抑制,最后溶解和死亡。
急性毒性:对小鼠给与5.81g/kg,相当于成人用量的97倍,未见本品对动物生育力和生殖有明显影响。
按3.6g/kg,1.8g/kg,9g/kg进行大鼠长期毒性试验,各组大鼠均未见异常反应。
【药代动力学】成人单次静脉滴注和静脉注射头孢他啶1g后,血药峰浓度(Cmax)分别可达70~72mg/L和120~146mg/L,血液药物消除半衰期(t1/2β)约为1.5~2.3小时。
给药后在骨、心、胆汁、痰、眼房水、滑膜液、胸膜液及腹膜液等多种组织和体液中分布良好,易透过胎盘,少量可透过血-脑脊液屏障,脑膜有炎症时,脑脊液内药物浓度可达同期血浓度的17%~30%。
血浆蛋白结合率低,约为5%~23%。
头孢他啶-阿维巴坦201502版说明书
12 CLINICAL PHARMACOLOGY
2.5 Storage of Constituted Solutions
12.1 Mechanism of Action
3 DOSAGE FORMS AND STRENGTHS
12.2 Pharmacodynamics
4 CONTRAINDICATIONS
7.2 Drug/Laboratory Test Interactions
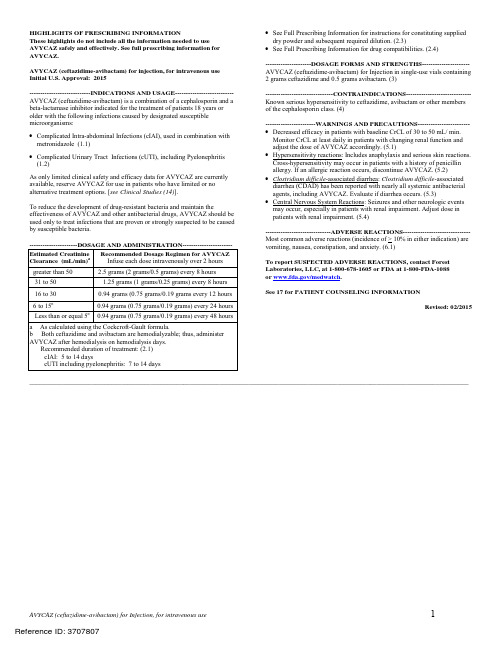
1.1 Complicated Intra-Abdominal Infections (cIAI)
8 USE IN SPECIFIC POPULATIONS
1.2 Complicated Urinary Tract Infections (cUTI), including
AVYCAZ (ceftazidime-avibactam) for Injection, for intravenous use
1
Reference ID: 3707807
FULL PRESCRIBING INFORMATION: CONTENTS*
7.1 Probenecid
1 INDICATIONS AND USAGE
Clearance of 30 to 50 mL/min
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
5.2 Hypersensitivity Reactions
As only limited clinical safety and efficacy data for AVYCAZ are currently available, reserve AVYCAZ for use in patients who have limited or no alternative treatment options. [see Clinical Studies (14)].
头孢他啶用法用量是什么?有没有不良反应?

头孢他啶用法用量是什么?有没有不良反应?头孢他啶是一种常见的抗生素,常用于治疗各种细菌感染。
正确的使用方法和用量对于疗效的发挥至关重要,同时也需要了解可能出现的不良反应,以便及时处理。
本文将介绍头孢他啶的用法用量及可能的不良反应。
用法用量头孢他啶可以以口服或静脉注射的方式使用,具体的用法用量如下:1.口服:–对于成人和儿童,通常建议每日分2-4次口服,每次剂量为250-500毫克,根据感染情况和医生的建议进行调整。
–严重感染时,剂量可能会增加,但不应超过每日4克。
–头孢他啶可用空腹或饭后服用,但应尽量保持规律服药,避免漏服。
2.静脉注射:–静脉注射头孢他啶通常用于严重感染或无法口服的情况下。
–剂量和给药频率应根据感染的类型和严重程度进行调整,建议在医护人员的指导下进行。
在使用头孢他啶时,应根据医生的建议严格遵循用药指导,不可自行增减剂量或中止用药。
不良反应虽然头孢他啶是一种常见的抗生素,但也存在一些不良反应,包括但不限于以下情况:1.消化系统反应:–可能出现恶心、呕吐、腹泻等消化不良症状。
–在用药过程中如果出现严重腹泻或胃肠道不适,应及时就医。
2.过敏反应:–个别患者对头孢他啶可能产生过敏反应,表现为皮疹、荨麻疹、药疹等。
–严重过敏反应可能引起呼吸困难、过敏性休克等危急情况,需立即就医处理。
3.其他不良反应:–头孢他啶还可能引起头晕、头痛、胃肠道不适、黄疸等不良反应,需密切观察病情并及时就医。
在使用头孢他啶期间,如出现任何不良反应或疑似过敏现象,应立即停止用药,并就医寻求帮助。
结语综上所述,头孢他啶是一种常用的抗生素药物,正确的使用方法和用量对于疗效的发挥至关重要。
同时,了解可能出现的不良反应并及时处理,可以减少并发症的发生,提高治疗效果。
在使用头孢他啶时,务必遵循医生的指导,严格按照药物说明书上的用药要求进行用药,并在必要时就医咨询。
头孢他啶英文说明书

1PRODUCT INFORMATIONCEPTAZ®2(ceftazidime for injection)3L-arginine formulation45For Intravenous or Intramuscular Use678DESCRIPTION: Ceftazidime is a semisynthetic, broad-spectrum, beta-lactam antibiotic forparenteral administration. It is the pentahydrate of pyridinium, 1-[[7-[[(2-amino-4-thiazolyl)[(1-910carboxy-1-methylethoxy)imino]acetyl]amino]-2-carboxy-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-11en-3-yl]methyl]-, hydroxide, inner salt, [6R-[6α,7β(Z)]]. It has the following structure:12131415The empirical formula is C22H32N6O12S2, representing a molecular weight of 636.6.CEPTAZ is a sterile, dry mixture of ceftazidime pentahydrate and L-arginine. The L-arginine1617is at a concentration of 349 mg/g of ceftazidime activity. CEPTAZ dissolves without the18evolution of gas. The product contains no sodium ion. Solutions of CEPTAZ range in color from 19light yellow to amber, depending on the diluent and volume used. The pH of freshly constituted 20solutions usually ranges from 5 to 7.5.2122CLINICAL PHARMACOLOGY: After intravenous (IV) administration of 500-mg and 1-g doses of ceftazidime over 5 minutes to normal adult male volunteers, mean peak serum2324concentrations of 45 and 90 mcg/mL, respectively, were achieved. After IV infusion of 500-mg, 251-g, and 2-g doses of ceftazidime over 20 to 30 minutes to normal adult male volunteers, mean peak serum concentrations of 42, 69, and 170 mcg/mL, respectively, were achieved. The average2627serum concentrations following IV infusion of 500-mg, 1-g, and 2-g doses to these volunteers28over an 8-hour interval are given in Table 1.2930Table 1Ceftazidime Serum Concentrations (mcg/mL)IV Dose 0.5 h 1 h 2 h 4 h 8 hmg 42 25 12 6 2 500g 60 39 23 11 31g 129 75 42 13 523132The absorption and elimination of ceftazidime were directly proportional to the size of the33dose. The half-life following IV administration was approximately 1.9 hours. Less than 10% of 34ceftazidime was protein bound. The degree of protein binding was independent of concentration.There was no evidence of accumulation of ceftazidime in the serum in individuals with normal3536renal function following multiple IV doses of 1 and 2 g every 8 hours for 10 days.37Following intramuscular (IM) administration of 500-mg and 1-g doses of ceftazidime to38normal adult volunteers, the mean peak serum concentrations were 17 and 39 mcg/mL,39respectively, at approximately 1 hour. Serum concentrations remained above 4 mcg/mL for 6 and 408 hours after the IM administration of 500-mg and 1-g doses, respectively. The half-life of41ceftazidime in these volunteers was approximately 2 hours.42The presence of hepatic dysfunction had no effect on the pharmacokinetics of ceftazidime in 43individuals administered 2 g intravenously every 8 hours for 5 days. Therefore, a dosage44adjustment from the normal recommended dosage is not required for patients with hepatic45dysfunction, provided renal function is not impaired.46Approximately 80% to 90% of an IM or IV dose of ceftazidime is excreted unchanged by the 47kidneys over a 24-hour period. After the IV administration of single 500-mg or 1-g doses,approximately 50% of the dose appeared in the urine in the first 2 hours. An additional 20% was4849excreted between 2 and 4 hours after dosing, and approximately another 12% of the doseappeared in the urine between 4 and 8 hours later. The elimination of ceftazidime by the kidneys5051resulted in high therapeutic concentrations in the urine.52The mean renal clearance of ceftazidime was approximately 100 mL/min. The calculated53plasma clearance of approximately 115 mL/min indicated nearly complete elimination of54ceftazidime by the renal route. Administration of probenecid before dosing had no effect on the 55elimination kinetics of ceftazidime. This suggested that ceftazidime is eliminated by glomerular 56filtration and is not actively secreted by renal tubular mechanisms.57Since ceftazidime is eliminated almost solely by the kidneys, its serum half-life is significantly 58prolonged in patients with impaired renal function. Consequently, dosage adjustments in such59patients as described in the DOSAGE AND ADMINISTRATION section are suggested.60Ceftazidime concentrations achieved in specific body tissues and fluids are depicted in61Table 2.62Table 2: Ceftazidime Concentrations in Body Tissues and Fluids 63Tissue or Fluid Dose/ RouteNo. ofPatientsTime ofSamplePostdoseAverage Tissueor Fluid Level(mcg/mL ormcg/g)Urine 500 mg IM 6 0-2 h 2,100.02 g IV 6 0-2 h 12,000.0Bile 2 g IV 3 90 min 36.4Synovial fluid 2 g IV 13 2 h 25.6Peritoneal fluid 2 g IV 8 2 h 48.6Sputum 1 g IV 8 1 h 9.0Cerebrospinal fluid 2 g q8h IV 5 120 min 9.8(inflamed meninges) 2 g q8h IV 6 180 min 9.4Aqueous humor 2 g IV 13 1-3 h 11.0Blister fluid 1 g IV 7 2-3 h 19.7Lymphatic fluid 1 g IV 7 2-3 h 23.4Bone 2 g IV 8 0.67 h 31.1Heart muscle 2 g IV 35 30-280 min 12.7Skin 2 g IV 22 30-180 min 6.6Skeletal muscle 2 g IV 35 30-280 min 9.4Myometrium 2 g IV 31 1-2 h 18.764Microbiology: Ceftazidime is bactericidal in action, exerting its effect by inhibition of enzymes 65responsible for cell-wall synthesis. A wide range of gram-negative organisms is susceptible to66ceftazidime in vitro, including strains resistant to gentamicin and other aminoglycosides. In67addition, ceftazidime has been shown to be active against gram-positive organisms. It is highly 68stable to most clinically important beta-lactamases, plasmid or chromosomal, which are produced 69by both gram-negative and gram-positive organisms and, consequently, is active against many 70strains resistant to ampicillin and other cephalosporins.71Ceftazidime has been shown to be active against the following organisms both in vitro and in 72clinical infections (see INDICATIONS AND USAGE).7374Aerobes,Gram-negative:Citrobacter spp., including Citrobacter freundii and Citrobacter75diversus; Enterobacter spp., including Enterobacter cloacae and Enterobacter aerogenes;76Escherichia coli; Haemophilus influenzae, including ampicillin-resistant strains; Klebsiella spp.77(including Klebsiella pneumoniae); Neisseria meningitidis; Proteus mirabilis; Proteus vulgaris;78Pseudomonas spp. (including Pseudomonas aeruginosa); and Serratia spp.79Aerobes, Gram-positive:Staphylococcus aureus, including penicillinase- and non–80penicillinase-producing strains; Streptococcus agalactiae (group B streptococci); Streptococcus 81pneumoniae; and Streptococcus pyogenes (group A beta-hemolytic streptococci).Anaerobes:Bacteroides spp. (NOTE: many strains of Bacteroides fragilis are resistant).8283Ceftazidime has been shown to be active in vitro against most strains of the following organisms; however, the clinical significance of this activity is unknown: Acinetobacter spp.,8485Clostridium spp. (not including Clostridium difficile), Haemophilus parainfluenzae, Morganella 86morganii (formerly Proteus morganii), Neisseria gonorrhoeae, Peptococcus spp.,87Peptostreptococcus spp., Providencia spp. (including Providencia rettgeri, formerly Proteus88rettgeri), Salmonella spp., Shigella spp., Staphylococcus epidermidis, and Yersinia89enterocolitica.Ceftazidime and the aminoglycosides have been shown to be synergistic in vitro against9091Pseudomonas aeruginosa and the enterobacteriaceae. Ceftazidime and carbenicillin have also 92been shown to be synergistic in vitro against Pseudomonas aeruginosa.93Ceftazidime is not active in vitro against methicillin-resistant staphylococci, Streptococcus94faecalis and many other enterococci, Listeria monocytogenes, Campylobacter spp., or95Clostridium difficile.96Susceptibility Tests:Diffusion Techniques:Quantitative methods that require measurement of 97zone diameters give an estimate of antibiotic susceptibility. One such procedure1-3 has been98recommended for use with disks to test susceptibility to ceftazidime.99Reports from the laboratory giving results of the standard single-disk susceptibility test with a 30-mcg ceftazidime disk should be interpreted according to the following criteria:100101Susceptible organisms produce zones of 18 mm or greater, indicating that the test organism 102is likely to respond to therapy.Organisms that produce zones of 15 to 17 mm are expected to be susceptible if high dosage 103104is used or if the infection is confined to tissues and fluids (e.g., urine) in which high antibiotic 105levels are attained.106Resistant organisms produce zones of 14 mm or less, indicating that other therapy should be 107selected.108Organisms should be tested with the ceftazidime disk since ceftazidime has been shown by in 109vitro tests to be active against certain strains found resistant when other beta-lactam disks are 110used.111Standardized procedures require the use of laboratory control organisms. The 30-mcg ceftazidime disk should give zone diameters between 25 and 32 mm for Escherichia coli112113ATCC 25922. For Pseudomonas aeruginosa ATCC 27853, the zone diameters should bebetween 22 and 29 mm. For Staphylococcus aureus ATCC 25923, the zone diameters should be 114115between 16 and 20 mm.116Dilution Techniques:In other susceptibility testing procedures, e.g., ICS agar dilution or the 117equivalent, a bacterial isolate may be considered susceptible if the minimum inhibitory118concentration (MIC) value for ceftazidime is not more than 16 mcg/mL. Organisms are119considered resistant to ceftazidime if the MIC is ≥64 mcg/mL. Organisms having an MIC value 120of <64 mcg/mL but >16 mcg/mL are expected to be susceptible if high dosage is used or if the 121infection is confined to tissues and fluids (e.g., urine) in which high antibiotic levels are attained. 122As with standard diffusion methods, dilution procedures require the use of laboratory control 123organisms. Standard ceftazidime powder should give MIC values in the range of 4 to 16 mcg/mL 124for Staphylococcus aureus ATCC 25923. For Escherichia coli ATCC 25922, the MIC range125should be between 0.125 and 0.5 mcg/mL. For Pseudomonas aeruginosa ATCC 27853, the MIC 126range should be between 0.5 and 2 mcg/mL.127128INDICATIONS AND USAGE: CEPTAZ is indicated for the treatment of patients with129infections caused by susceptible strains of the designated organisms in the following diseases: 1301.Lower Respiratory Tract Infections, including pneumonia, caused by Pseudomonas131aeruginosa and other Pseudomonas spp.; Haemophilus influenzae, including132ampicillin-resistant strains; Klebsiella spp.; Enterobacter spp.; Proteus mirabilis; Escherichiacoli; Serratia spp.; Citrobacter spp.; Streptococcus pneumoniae; and Staphylococcus aureus 133134(methicillin-susceptible strains).1352.Skin and Skin-Structure Infections caused by Pseudomonas aeruginosa; Klebsiella spp.; 136Escherichia coli; Proteus spp., including Proteus mirabilis and indole-positive Proteus;137Enterobacter spp.; Serratia spp.; Staphylococcus aureus (methicillin-susceptible strains); and 138Streptococcus pyogenes (group A beta-hemolytic streptococci).1393. Urinary Tract Infections, both complicated and uncomplicated, caused by Pseudomonas140aeruginosa; Enterobacter spp.; Proteus spp., including Proteus mirabilis and indole-positive 141Proteus; Klebsiella spp.; and Escherichia coli.4.Bacterial Septicemia caused by Pseudomonas aeruginosa, Klebsiella spp., Haemophilus142143influenzae, Escherichia coli, Serratia spp., Streptococcus pneumoniae, and Staphylococcusaureus (methicillin-susceptible strains).1441455. Bone and Joint Infections caused by Pseudomonas aeruginosa,Klebsiella spp., Enterobacter 146spp., and Staphylococcus aureus (methicillin-susceptible strains).1476.Gynecologic Infections, including endometritis, pelvic cellulitis, and other infections of the 148female genital tract caused by Escherichia coli.1497.Intra-abdominal Infections, including peritonitis caused by Escherichia coli, Klebsiella spp.,and Staphylococcus aureus (methicillin-susceptible strains) and polymicrobial infections150151caused by aerobic and anaerobic organisms and Bacteroides spp. (many strains of Bacteroides 152fragilis are resistant).1538.Central Nervous System Infections, including meningitis, caused by Haemophilus influenzae 154and Neisseria meningitidis. Ceftazidime has also been used successfully in a limited number of 155cases of meningitis due to Pseudomonas aeruginosa and Streptococcus pneumoniae.156Specimens for bacterial cultures should be obtained before therapy in order to isolate and157identify causative organisms and to determine their susceptibility to ceftazidime. Therapy may be 158instituted before results of susceptibility studies are known; however, once these results become 159available, the antibiotic treatment should be adjusted accordingly.CEPTAZ may be used alone in cases of confirmed or suspected sepsis. Ceftazidime has been 160161used successfully in clinical trials as empiric therapy in cases where various concomitant162therapies with other antibiotics have been used.163CEPTAZ may also be used concomitantly with other antibiotics, such as aminoglycosides, 164vancomycin, and clindamycin; in severe and life-threatening infections; and in the165immunocompromised patient (see COMPATIBILITY AND STABILITY). When such166concomitant treatment is appropriate, prescribing information in the labeling for the otherantibiotics should be followed. The dosage depends on the severity of the infection and the167168patient's condition.169170CONTRAINDICATIONS: CEPTAZ is contraindicated in patients who have shown171hypersensitivity to ceftazidime or the cephalosporin group of antibiotics.172173WARNINGS: BEFORE THERAPY WITH CEPTAZ IS INSTITUTED, CAREFUL INQUIRY 174SHOULD BE MADE TO DETERMINE WHETHER THE PATIENT HAS HAD PREVIOUS 175HYPERSENSITIVITY REACTIONS TO CEFTAZIDIME, CEPHALOSPORINS,176PENICILLINS, OR OTHER DRUGS. IF THIS PRODUCT IS TO BE GIVEN TOPENICILLIN-SENSITIVE PATIENTS, CAUTION SHOULD BE EXERCISED BECAUSE 177178CROSS-HYPERSENSITIVITY AMONG BETA-LACTAM ANTIBIOTICS HAS BEENCLEARLY DOCUMENTED AND MAY OCCUR IN UP TO 10% OF PATIENTS WITH A 179180HISTORY OF PENICILLIN ALLERGY. IF AN ALLERGIC REACTION TO CEPTAZ181OCCURS, DISCONTINUE THE DRUG. SERIOUS ACUTE HYPERSENSITIVITY182REACTIONS MAY REQUIRE TREATMENT WITH EPINEPHRINE AND OTHER183EMERGENCY MEASURES, INCLUDING OXYGEN, IV FLUIDS, IV ANTIHISTAMINES, 184CORTICOSTEROIDS, PRESSOR AMINES, AND AIRWAY MANAGEMENT, AS185CLINICALLY INDICATED.186Pseudomembranous colitis has been reported with nearly all antibacterial agents,187including ceftazidime, and may range in severity from mild to life threatening. Therefore, it is important to consider this diagnosis in patients who present with diarrhea subsequent to 188189the administration of antibacterial agents.Treatment with antibacterial agents alters the normal flora of the colon and may permit190191overgrowth of clostridia. Studies indicate that a toxin produced by Clostridium difficile is one 192primary cause of "antibiotic-associated colitis."After the diagnosis of pseudomembranous colitis has been established, appropriate therapeutic 193194measures should be initiated. Mild cases of pseudomembranous colitis usually respond to drug195discontinuation alone. In moderate to severe cases, consideration should be given to management196with fluids and electrolytes, protein supplementation, and treatment with an antibacterial drug197clinically effective against Clostridium difficile colitis.198Elevated levels of ceftazidime in patients with renal insufficiency can lead to seizures,encephalopathy, coma, asterixis, neuromuscular excitability, and myoclonia (see199200PRECAUTIONS).201202PRECAUTIONS:203General: High and prolonged serum ceftazidime concentrations can occur from usual dosages in204patients with transient or persistent reduction of urinary output because of renal insufficiency.205The total daily dosage should be reduced when ceftazidime is administered to patients with renal206insufficiency (see DOSAGE AND ADMINISTRATION). Elevated levels of ceftazidime in thesepatients can lead to seizures, encephalopathy, coma, asterixis, neuromuscular excitability, and 207208myoclonia. Continued dosage should be determined by degree of renal impairment, severity ofinfection, and susceptibility of the causative organisms.209210As with other antibiotics, prolonged use of CEPTAZ may result in overgrowth of211nonsusceptible organisms. Repeated evaluation of the patient's condition is essential. If212superinfection occurs during therapy, appropriate measures should be taken.213Inducible type I beta-lactamase resistance has been noted with some organisms (e.g.,214Enterobacter spp.,Pseudomonas spp., and Serratia spp.). As with other extended-spectrum215beta-lactam antibiotics, resistance can develop during therapy, leading to clinical failure in some216cases. When treating infections caused by these organisms, periodic susceptibility testing should217be performed when clinically appropriate. If patients fail to respond to monotherapy, anaminoglycoside or similar agent should be considered.218219Cephalosporins may be associated with a fall in prothrombin activity. Those at risk includepatients with renal or hepatic impairment, or poor nutritional state, as well as patients receiving a 220221protracted course of antimicrobial therapy. Prothrombin time should be monitored in patients at222risk and exogenous vitamin K administered as indicated.CEPTAZ should be prescribed with caution in individuals with a history of gastrointestinal 223224disease, particularly colitis.225Arginine has been shown to alter glucose metabolism and elevate serum potassium transiently 226when administered at 50 times the recommended dose. The effect of lower dosing is not known. 227Distal necrosis can occur after inadvertent intra-arterial administration of ceftazidime.228Drug Interactions: Nephrotoxicity has been reported following concomitant administration of 229cephalosporins with aminoglycoside antibiotics or potent diuretics such as furosemide. Renal 230function should be carefully monitored, especially if higher dosages of the aminoglycosides are to 231be administered or if therapy is prolonged, because of the potential nephrotoxicity and ototoxicity of aminoglycosidic antibiotics. Nephrotoxicity and ototoxicity were not noted when ceftazidime 232233was given alone in clinical trials.Chloramphenicol has been shown to be antagonistic to beta-lactam antibiotics, including234235ceftazidime, based on in vitro studies and time kill curves with enteric gram-negative bacilli. Due 236to the possibility of antagonism in vivo, particularly when bactericidal activity is desired, this 237drug combination should be avoided.238Drug/Laboratory Test Interactions: The administration of ceftazidime may result in a239false-positive reaction for glucose in the urine when using CLINITEST® tablets, Benedict'ssolution, or Fehling's solution. It is recommended that glucose tests based on enzymatic glucose 240241oxidase reactions (such as CLINISTIX®) be used.242Carcinogenesis, Mutagenesis, Impairment of Fertility: Long-term studies in animals have not 243been performed to evaluate carcinogenic potential. However, a mouse Micronucleus test and an 244Ames test were both negative for mutagenic effects.245Pregnancy:Teratogenic Effects: Pregnancy Category B. Reproduction studies have been246performed in mice and rats at doses up to 40 times the human dose and have revealed no evidence 247of impaired fertility or harm to the fetus due to ceftazidime. CEPTAZ at 23 times the human dose 248was not teratogenic or embryotoxic in a rat reproduction study. There are, however, no adequate 249and well-controlled studies in pregnant women. Because animal reproduction studies are notalways predictive of human response, this drug should be used during pregnancy only if clearly 250251needed.252Nursing Mothers: Ceftazidime is excreted in human milk in low concentrations. It is not knownwhether the arginine component of this product is excreted in human milk. Because many drugs 253254are excreted in human milk and because safety of the arginine component of CEPTAZ in nursing 255infants has not been established, a decision should be made whether to discontinue nursing or to 256discontinue the drug, taking into account the importance of the drug to the mother.257Pediatric Use: Safety of the arginine component of CEPTAZ in neonates, infants, and children 258has not been established. This product is for use in patients 12 years and older. If treatment with ceftazidime is indicated for neonates, infants, or children, a sodium carbonate formulation should 259260be used.261262ADVERSE REACTIONS: The following adverse effects from clinical trials were considered to 263be either related to ceftazidime therapy or were of uncertain etiology. The most common were 264local reactions following IV injection and allergic and gastrointestinal reactions. No265disulfiramlike reactions were reported.266Local Effects, reported in fewer than 2% of patients, were phlebitis and inflammation at the site of injection (1 in 69 patients).267268Hypersensitivity Reactions, reported in 2% of patients, were pruritus, rash, and fever.Immediate reactions, generally manifested by rash and/or pruritus, occurred in 1 in 285 patients. 269270Toxic epidermal necrolysis, Stevens-Johnson syndrome, and erythema multiforme have also been 271reported with cephalosporin antibiotics, including ceftazidime. Angioedema and anaphylaxis 272(bronchospasm and/or hypotension) have been reported very rarely.273Gastrointestinal Symptoms, reported in fewer than 2% of patients, were diarrhea (1 in 78),274nausea (1 in 156), vomiting (1 in 500), and abdominal pain (1 in 416). The onset of275pseudomembranous colitis symptoms may occur during or after treatment (see WARNINGS). 276Central Nervous System Reactions (fewer than 1%) included headache, dizziness, and277paresthesia. Seizures have been reported with several cephalosporins, including ceftazidime. In addition, encephalopathy, coma, asterixis, neuromuscular excitability, and myoclonia have been 278279reported in renally impaired patients treated with unadjusted dosage regimens of ceftazidime (see PRECAUTIONS: General).280281Less Frequent Adverse Events (fewer than 1%) were candidiasis (including oral thrush) and 282vaginitis.Hematologic: Rare cases of hemolytic anemia have been reported.283284Laboratory Test Changes noted during ceftazidime clinical trials were transient and included: 285eosinophilia (1 in 13), positive Coombs' test without hemolysis (1 in 23), thrombocytosis (1 in 28645), and slight elevations in one or more of the hepatic enzymes, aspartate aminotransferase287(AST, SGOT) (1 in 16), alanine aminotransferase (ALT, SGPT) (1 in 15), LDH (1 in 18), GGT (1 288in 19), and alkaline phosphatase (1 in 23). As with some other cephalosporins, transient289elevations of blood urea, blood urea nitrogen, and/or serum creatinine were observed290occasionally. Transient leukopenia, neutropenia, agranulocytosis, thrombocytopenia, and291lymphocytosis were seen very rarely.292293POSTMARKETING EXPERIENCE WITH CEPTAZ PRODUCTS: In addition to theadverse events reported during clinical trials, the following events have been observed during 294295clinical practice in patients treated with CEPTAZ and were reported spontaneously. For some of 296these events, data are insufficient to allow an estimate of incidence or to establish causation.297General: Anaphylaxis; allergic reactions, which, in rare instances, were severe (e.g.,298cardiopulmonary arrest); urticaria; pain at injection site.299Hepatobiliary Tract: Hyperbilirubinemia, jaundice.300Renal and Genitourinary: Renal impairment.301Cephalosporin-Class Adverse Reactions: In addition to the adverse reactions listed above that 302have been observed in patients treated with ceftazidime, the following adverse reactions and303altered laboratory tests have been reported for cephalosporin-class antibiotics:304Adverse Reactions:Colitis, toxic nephropathy, hepatic dysfunction including cholestasis, 305aplastic anemia, hemorrhage.306Altered Laboratory Tests:Prolonged prothrombin time, false-positive test for urinary307glucose, pancytopenia.308309OVERDOSAGE: Ceftazidime overdosage has occurred in patients with renal failure. Reactions 310have included seizure activity, encephalopathy, asterixis, neuromuscular excitability, and coma. 311Patients who receive an acute overdosage should be carefully observed and given supportive312treatment. In the presence of renal insufficiency, hemodialysis or peritoneal dialysis may aid inthe removal of ceftazidime from the body.313314315DOSAGE AND ADMINISTRATION:Dosage: The usual adult dosage is 1 gram administered intravenously or intramuscularly every 8 316317to 12 hours. The dosage and route should be determined by the susceptibility of the causative 318organisms, the severity of infection, and the condition and renal function of the patient.319The guidelines for dosage of CEPTAZ are listed in Table 3. The following dosage schedule is 320recommended.321Table 3: Recommended Dosage Schedule322DoseFrequency Patients 12 years and older*Usual recommended dosage 1 gram IV or IM q8-12hUncomplicated urinary tract infections 250 mg IV or IM q12hBone and joint infections 2 grams IV q12hComplicated urinary tract infections 500 mg IV or IM q8-12hUncomplicated pneumonia; mild skin and skin- structure infections 500 mg-1 gramIV or IM q8hSerious gynecologic and intra-abdominal infections 2 grams IV q8h Meningitis 2 grams IV q8h Very severe life-threatening infections, especiallyin immunocompromised patients 2 grams IV q8hLung infections caused by Pseudomonas spp. in patients with cystic fibrosis with normal renal function†30-50 mg/kg IVto a maximumof 6 grams per day q8h* This product is for use in patients 12 years and older. If treatment with ceftazidime is323indicated for patients less than 12 years old, a sodium carbonate formulation should324be used.325†Although clinical improvement has been shown, bacteriologic cures cannot be326expected in patients with chronic respiratory disease and cystic fibrosis.327328Impaired Hepatic Function: No adjustment in dosage is required for patients with hepatic 329dysfunction.330Impaired Renal Function: Ceftazidime is excreted by the kidneys, almost exclusively by 331glomerular filtration. Therefore, in patients with impaired renal function (glomerular filtration 332rate [GFR]<50 mL/min), it is recommended that the dosage of ceftazidime be reduced to333compensate for its slower excretion. In patients with suspected renal insufficiency, an initial334loading dose of 1 gram of CEPTAZ may be given. An estimate of GFR should be made to335determine the appropriate maintenance dosage. The recommended dosage is presented in Table 4. 336。
注射用头孢他啶 Ceftazidime for Injection-详细说明书及重点
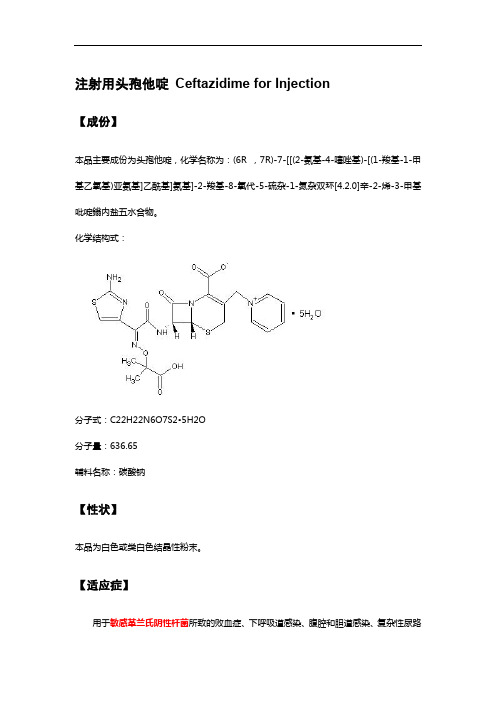
注射用头孢他啶Ceftazidime for Injection【成份】本品主要成份为头孢他啶,化学名称为:(6R ,7R)-7-[[(2-氨基-4-噻唑基)-[(1-羧基-1-甲基乙氧基)亚氨基]乙酰基]氨基]-2-羧基-8-氧代-5-硫杂-1-氮杂双环[4.2.0]辛-2-烯-3-甲基吡啶鎓内盐五水合物。
化学结构式:分子式:C22H22N6O7S2•5H2O分子量:636.65辅料名称:碳酸钠【性状】本品为白色或类白色结晶性粉末。
【适应症】用于敏感革兰氏阴性杆菌所致的败血症、下呼吸道感染、腹腔和胆道感染、复杂性尿路感染和严重皮肤软组织感染等。
对于由多种耐药革兰氏阴性杆菌引起的免疫缺陷者感染、医院内感染以及革兰氏阴性杆菌或铜绿假单胞菌所致中枢神经系统感染尤为适用。
【规格】按C22H22N6O7S2计算1.0g【用法用量】静脉注射或静脉滴注。
1.败血症、下呼吸道感染、胆道感染等,一日4~6g,分2~3次静脉滴注或静脉注射,疗程10~14日。
2.泌尿系统感染和重度皮肤软组织感染等,一日2~4g,分2次静脉滴注或静脉注射,疗程7~14日。
3.对于某些危及生命的感染、严重铜绿假单胞菌感染和中枢神经系统感染,可酌情增量至一日0.15~0.2g/kg,分3次静脉滴注或静脉注射。
4.婴幼儿常用剂量为一日30~100mg/kg,分2~3次静脉滴注。
【不良反应】本品的不良反应少见而轻微。
少数患者可发生皮疹、皮肤瘙痒、药物热;恶心、腹泻、腹痛;注射部位轻度静脉炎;偶可发生一过性血清氨基转移酶酶、血尿素氮、血肌酐值的轻度升高;白细胞、血小板减少及嗜酸性粒细胞增多等。
【禁忌】对头孢菌素类抗生素过敏者禁用。
【注意事项】1.交叉过敏反应:对一种头孢菌素或头霉素(cephamycin)过敏者对其他头孢菌素或头霉素也可能过敏。
对青霉素类、青霉素衍生物或青霉胺过敏者也可能对头孢菌素或头霉素过敏。
对青霉素过敏病人应用头孢菌素时发生过敏反应者达5%~10%;如作过敏试验,则对青霉素过敏病人对头孢菌素过敏者达20%。
注射用头孢他啶
注射用头孢他啶【适应症】头孢他啶适用于由敏感细菌所引起的单一感染及由二种或二种以上的敏感菌引起的混合感染。
全身性的严重感染;呼吸道感染;耳、鼻和喉感染;尿路感染;皮肤及软组织感染;胃肠、胆及腹部感染;骨骼及关节感染;与血透和腹膜透析及不卧床之延续腹膜透析(CAPD)有关的感染。
对于脑膜炎,推荐在得知敏感试验结果后,单独应用头孢他啶治疗。
头孢他啶可用于耐其它抗生素包括氨基糖苷类和多数头孢菌素的感染。
如果合适,可联同氨基糖苷类或其它b-内酰胺类抗生素使用,例如在严重中性粒细胞减少时,或在怀疑是脆弱拟杆菌感染时,与另一抗厌氧菌抗生素合用。
另外,头孢他啶还可用于经尿道前列腺切除手术的预防治疗。
细菌学:头孢他啶的药效是杀菌性的,通过抑制细菌的细胞壁合成而发挥作用。
在体外,广谱的与医院获得性感染有关的病原菌株和分离株都对头孢他啶敏感,包括耐庆大霉素和其他氨基糖苷类的菌株。
其对绝大多数临床上重要的革兰氏阳性及革兰氏阴性细菌所产生的b-内酰胺酶都具高度的稳定性,因而对很多耐氨苄青霉素及头孢噻吩的菌株都有效。
头孢他啶于体外显示高度的固有活性,在较窄的最低抑制浓度范围内便对绝大多数的菌属有效,且于不同的接种水平下其最低抑菌浓度亦改变极微。
在体外,头孢他啶已证实对下列细菌有效:革兰氏阴性菌:绿脓杆菌及其它假单胞菌属,肺炎克雷伯杆菌及其它克雷伯杆菌属,奇异变形杆菌,普通变形杆菌,摩根摩氏菌(以前的摩根变形杆菌),雷特格氏变形杆菌,普罗威登斯杆菌,大肠杆菌,肠杆菌属,枸橼酸菌属,沙雷菌属,沙门氏菌属,志贺氏菌属,小肠结肠炎耶氏菌,多杀巴斯德氏菌,不动杆菌属,淋病奈瑟氏菌,脑膜炎奈瑟氏菌,流感嗜血杆菌(包括耐氨苄青霉素的菌株),副流感嗜血杆菌(包括耐氨苄青霉素的菌株)。
革兰氏阳性菌:金黄色葡萄球菌(对甲氧西林敏感的菌株),和表皮葡萄球菌(对甲氧西林敏感的菌株),微球菌属,化脓链球菌(A群b-溶血性链球菌),B簇链球菌,肺炎链球菌,缓症链球菌,链球菌属(粪肠球菌除外)。
头孢他啶如何用药?用法用量是多少?

头孢他啶如何用药?用法用量是多少?头孢他啶是一种广谱抗生素,属于头孢菌素类药物。
它可用于治疗各种感染症,如上呼吸道感染、下呼吸道感染、皮肤和软组织感染等。
头孢他啶的用药剂型有口服片剂、颗粒剂、注射剂等,具体的用法和用量如下:1. 口服片剂和颗粒剂:- 成人:一般建议每次口服125-500毫克,每日2-4次。
根据感染的严重程度和个体差异,医生可能会调整剂量和用药频率。
- 儿童:通常建议每日口服剂量为30-50毫克/千克,分2-4次服用。
2. 注射剂:- 成人:一般建议每次肌肉注射250-500毫克头孢他啶,每日2-4次。
对于严重感染,医生可能会调整剂量和给药频率,并进行静脉注射。
- 儿童:每次肌肉注射剂量一般为25-100毫克/千克,每日2-4次。
对于严重感染,医生可能会调整剂量和给药频率,并进行静脉注射。
用药的具体使用方法和注意事项如下:1. 口服片剂和颗粒剂:- 可以随餐服用,也可空腹服用。
- 服用头孢他啶前后应用适量的水冲服,以确保药物充分吸收。
- 若遇到胃肠道不适,可考虑与食物一同服用,以减轻不良反应。
- 用药过程中要坚持按照医生的指示进行,不得擅自改变剂量和用药频率。
- 用药时间一般为7-14天,要按疗程进行,不可提前停药。
2. 注射剂:- 由专业医生或医护人员进行静脉注射或肌肉注射。
- 可以通过静脉滴注或缓慢注射进行给药,注射速度不可过快。
- 使用前应先检查药品的外观,如有异样请勿使用。
- 用药期间注意用药器具的无菌性,并注意药液是否清晰无混悬物。
- 一般情况下,感染得到控制后3-5天可以改用口服制剂。
需要注意的是,使用头孢他啶时,应根据具体情况,结合病原学检查和药敏试验结果,以及患者的年龄、体重、肝肾功能等因素进行个体化治疗。
同时,使用抗生素需要注意以下几点:1. 遵医嘱:药物使用必须在医生的指导下进行,严格按照医嘱的剂量和用药频率使用药物。
2. 完成疗程:即使症状减轻或消失,也不能随意停药。
头孢他啶阿维巴坦药品说明书
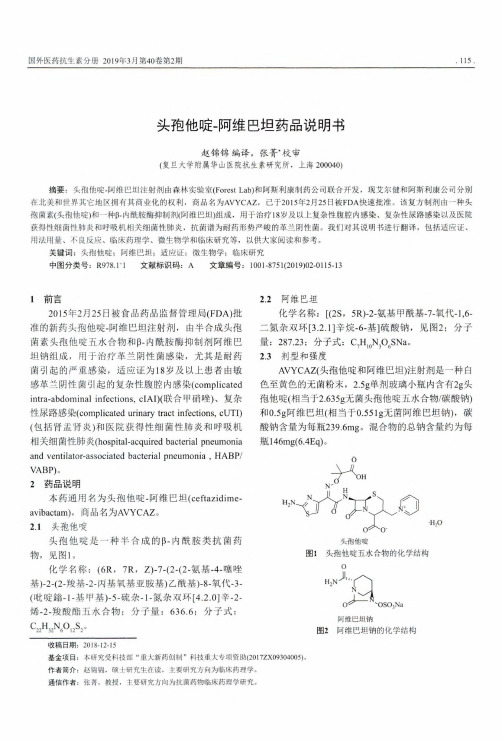
头胞他唳-阿维巴坦药品说明书赵锦锦编译,张菁•校审(复旦大学附属华山医院抗生素研究所,上海200040)摘要:头抱他喘-阿维巴坦注射剂由森林实验室(Forest Lab)和阿斯利康制药公司联合开发,现艾尔健和阿斯利康公司分别在北美和世界其它地区拥有其商业化的权利,商品名为AVYCA 乙已于2015年2月25日被FDA 快速批准。
该复方制剂由一种头 抱菌素(头抱他喘)和一种卜内酰胺酶抑制剂(阿维巴坦)组成,用于治疗18岁及以上复杂性腹腔内感染、复杂性尿路感染以及医院 获得性细菌性肺炎和呼吸机相关细菌性肺炎,抗菌谱为耐药形势严峻的革兰阴性菌。
我们对其说明书进行翻译,包括适应证、用法用量、不良反应、临床药理学、微生物学和临床研究等,以供大家阅读和参考。
关键词:头抱他喘;阿维巴坦;适应证;微生物学;临床研究中图分类号:R978.1-1 文献标识码:A 文章编号:1001-8751(2019)02-0115-131前言2015年2月25日被食品药品监督管理局(FDA)批 准的新药头抱他噪-阿维巴坦注射剂,由半合成头抱菌素头抱他噪五水合物和卜内酰胺酶抑制剂阿维巴坦钠组成,用于治疗革兰阴性菌感染,尤其是耐药 菌引起的严重感染,适应证为18岁及以上患者由敏感革兰阴性菌引起的复杂性腹腔内感染(complicatedintra-abdominal infections, cIAI)(联合甲硝呼)、复杂 性尿路感染(complicated urinary tract infections, cUTI)(包括肾盂肾炎)和医院获得性细菌性肺炎和呼吸机相关细菌性肺炎(hospital-acquired bacterial pneumoniaand ventilator-associated bacterial pneumonia , HABP/VABP)…2药品说明本药通用名为头抱他噪-阿维巴坦(ceftazidime-avibactam),商品名为AVYCAZ 。
注射用头孢他啶阿维巴坦钠的介绍

研发过程与技术难点
研发背景:为了 解决头孢他啶和 阿维巴坦钠的耐 药性问题
研发团队:由多 家制药企业和研 究机构共同组成
研发过程:包括 药物筛选、药理 毒理研究、临床 试验等阶段
技术难点:如何 保持药物的稳定 性和生物利用度 ,以及如何解决 药物的耐药性问 题
成果转化与产业化进程
研发背景:为了 解决抗生素耐药 性问题,提高治 疗效果
安全性:注射用 头孢他啶阿维巴 坦钠的安全性较 高,不良反应较 少,但可能会引 起过敏反应、胃
肠道反应等。
相互作用:与其 他药物合用时, 可能会发生相互 作用,需要谨慎
使用。
用法与用量
儿童:静脉注射,每次按体 重10mg/kg,每日2次, 疗程7-14天
成人:静脉注射,每次 1.5g,每日2次,疗程714天
市场趋势:随着对头孢他啶阿维 巴坦钠研究的深入,未来市场有 望进一步扩大。
添加标题
添加标题
添加标题
添加标题
竞争格局:目前,头孢他啶阿维 巴坦钠市场主要由几家大型制药 企业占据,竞争较为激烈。
挑战与机遇:虽然市场竞争激烈, 但头孢他啶阿维巴坦钠作为新型 抗生素,具有较大的市场潜力和 机遇。
政策环境与产业政策
作用机制:通过抑制细菌细胞壁的合成,导致细菌死亡
耐药性:对某些细菌可能产生耐药性,需要根据实际情况调整用药方案
耐药性及敏感菌株
头孢他啶阿维巴 坦钠对耐药菌株 具有较强的抗菌 活性
头孢他啶阿维巴 坦钠对敏感菌株 具有较高的抗菌 活性
头孢他啶阿维巴 坦钠对耐药菌株 的抗菌活性与敏 感菌株的抗菌活 性相比,具有更 高的抗菌活性
头孢他啶:一种抗生素,用于治 疗敏感菌引起的感染
添加标题
临床头孢他啶药物常规用药、剂量调整、给药说明、贮藏、药物警戒、不良反应、禁忌症、注意事项、药物监控及
临床头胞他口定药物常规用药、剂量调整、给药说明、贮藏、药物警戒、不良反应、禁忌症、注意事项、药物监控及药物过量常规用药头抱他咤是用于肠胃外给药的半合成、广谱、B-内酰胺类抗菌药物。
可用于敏感微生物引起的单一或多重感染。
成人常用剂量头抱他咤可用于治疗由敏感微生物引起的单一或多重感染,具体如下:♦全身性重度感染:由假单胞菌属(包括铜绿假单胞菌)、流感嗜血杆菌(包括氨茉西林耐药菌株)、克雷伯菌属(包括克雷伯菌)、肠杆菌属、变形杆菌属、大肠埃希菌、沙雷氏菌属、枸椽酸杆菌属、肺炎链球菌和金黄色葡萄球菌(甲氧西林敏感菌株)引起的全身性重度感染,例如:败血症、菌血症、腹膜炎、免疫抑制患者的感染和重症监护患者的感染(如烧伤感染)。
♦下呼吸道感染(包括肺炎):由假单胞菌属(包括铜绿假单胞菌)、流感嗜血杆菌(包括氨苇西林耐药菌株)、克雷伯菌属(包括肺炎克雷伯菌)、肠杆菌属、奇异变形杆菌、大肠埃希菌、沙雷氏菌属、枸檬酸杆菌属、肺炎链球菌和金黄色葡萄球菌(甲氧西林敏感菌株)引起。
♦耳鼻喉感染:由假单胞菌属(包括铜绿假单胞菌)、流感嗜血杆菌(包括氨苇西林耐药菌株)、肺炎链球菌、金黄色葡萄球菌(甲氧西林敏感菌株)和酿脓链球菌(A族B溶血性链球菌)引起。
变形杆菌属(包括奇异变形杆菌和口引跺阳性变形杆菌)、克雷伯菌属和大肠埃希菌引起。
♦皮肤和软组织感染:由铜绿假单胞菌、克雷伯菌属、大肠埃希菌、变形杆菌属(包括奇异变形杆菌和呵喙阳性变形杆菌)、肠杆菌属、沙雷氏菌属、金黄色葡萄球菌(甲氧西林敏感菌株)和酿脓链球菌(A族B溶血性链球菌)引起。
♦骨和关节感染:由铜绿假单胞菌、克雷伯菌属、肠杆菌属和金黄色葡萄球菌(甲氧西林敏感菌株)引起。
♦妇科感染:包括子宫内膜炎、盆腔蜂窝组织炎和其他由大肠埃希菌引起的女性生殖道感染。
♦胃肠道、胆道和腹部感染:包括由大肠埃希菌、克雷伯菌属和金黄色葡萄球菌(甲氧西林敏感菌株)引起的腹膜炎,以及由需氧和厌氧微生物以及拟杆菌(注意:许多脆弱拟杆菌菌株具有耐药性)引起的多种微生物感染。
注射用头孢他啶说明书
核准日期: 年 月 日注射用头孢他啶说明书请仔细阅读说明书并在医师指导下使用【药品名称】通用名称:注射用头孢他啶英文名称:Ceftazidime for Injection汉语拼音:Zhusheyong Toubaotading【成份】本品活性成份为头孢他啶,化学名称:(6R , 7R )-7-[[(2-氨基-4-噻唑基)-[(1-羧基-1-甲基乙氧基)亚氨基]乙酰基]氨基]-2-羧基-8-氧代-5-硫杂-1-氮杂双环[4.2.0]辛-2-烯-3-甲基吡啶鎓内盐五水合物。
化学结构式:分子式:C 22H 22N 6O 7S 2·5H 2O分子量:辅 料:碳酸钠。
【性状】本品为白色或类白色结晶性粉末。
【适应症】用于敏感革兰氏阴性杆菌所致的败血症、下呼吸道感染、腹腔和胆道感染、复杂性尿路感染和严重皮肤软组织感染等。
对于由多种耐药革兰氏阴性杆菌引起的免疫缺陷者感染、医院内感染以及革兰氏阴性杆菌或铜绿假单胞菌所致中枢神经系统感染尤为适用。
【规格】1.0g(按头孢他啶计)【用法用量】静脉注射或静脉滴注。
剂量依感染的严重程度、微生物敏感性及患者机体状态而定。
成人:1. 败血症、下呼吸道感染、胆道感染等,一日4~6g ,分2~3次静脉滴注或静脉注射,疗程10~14日。
2. 泌尿系统感染和重度皮肤软组织感染等,一日2~4g ,分2次静脉滴注或静脉注射,疗程7~14日。
对于轻度尿路感染,每12小时~1g即已足够。
3. 对于某些危及生命的感染、严重铜绿假单胞菌感染和中枢神经系统感染,可酌情增量至一日~0.2g/kg,分3次静脉滴注或静脉注射。
儿童:2个月以上婴幼儿常用剂量为一日30~100mg/kg,分2~3次静脉滴注。
对新生儿至2个月婴儿临床经验有限。
肾功能损害患者:因头孢他啶主要经肾脏排泄,对肾功能损害患者应减量使用。
可根据肌酐清除率来计算合适的给药剂量。
透析后患者应重复适当维持剂量。
配制方法:5ml注射用水加入0.5g装瓶中或10ml注射用水加入1g或2g装瓶中,使完全溶解后,于3~5分钟静脉缓慢推注。
注射用头孢他啶说明书
注射用头孢他啶说明书核准日期: 年 月 日注射用头孢她啶说明书请仔细阅读说明书并在医师指导下使用【药品名称】通用名称:注射用头孢她啶英文名称:Ceftazidime for Injection汉语拼音:Zhusheyong Toubaotading【成份】本品活性成份为头孢她啶,化学名称:(6R , 7R )-7-[[(2-氨基-4-噻唑基)-[(1-羧基-1-甲基乙氧基)亚氨基]乙酰基]氨基]-2-羧基-8-氧代-5-硫杂-1-氮杂双环[4.2.0]辛-2-烯-3-甲基吡啶鎓内盐五水合物。
化学结构式:H 3CH 3C OH O,5H 2O S N N +N-NH 2O分子式:C 22H 22N 6O 7S 2·5H 2O分子量:636.65辅 料:碳酸钠。
【性状】本品为白色或类白色结晶性粉末。
【适应症】用于敏感革兰氏阴性杆菌所致的败血症、下呼吸道感染、腹腔和胆道感染、复杂性尿路感染和严重皮肤软组织感染等。
对于由多种耐药革兰氏阴性杆菌引起的免疫缺陷者感染、医院内感染以及革兰氏阴性杆菌或铜绿假单胞菌所致中枢神经系统感染尤为适用。
【规格】1.0g(按头孢她啶计)【用法用量】静脉注射或静脉滴注。
剂量依感染的严重程度、微生物敏感性及患者机体状态而定。
成人:1. 败血症、下呼吸道感染、胆道感染等,一日4~6g,分2~3次静脉滴注或静脉注射,疗程10~14日。
2. 泌尿系统感染和重度皮肤软组织感染等,一日2~4g,分2次静脉滴注或静脉注射,疗程7~14日。
对于轻度尿路感染,每12小时0.5~1g即已足够。
3. 对于某些危及生命的感染、严重铜绿假单胞菌感染和中枢神经系统感染,可酌情增量至一日0.15~0.2g/kg,分3次静脉滴注或静脉注射。
儿童:2个月以上婴幼儿常见剂量为一日30~100mg/kg,分2~3次静脉滴注。
对新生儿至2个月婴儿临床经验有限。
肾功能损害患者:因头孢她啶主要经肾脏排泄,对肾功能损害患者应减量使用。
注射用头孢他啶 复达欣 使用说明书

核准日期:2006年12月29日修改日期:2011年9月5日2013年9月7日2014年10月18日注射用头孢他啶使用说明书请仔细阅读说明书并在医师指导下使用。
【药品名称】通用名称:注射用头孢他啶商品名称:复达欣®英文名称:Ceftazidime for Injection汉语拼音:Zhusheyong Toubaotading【成份】化学名称:(6R,7R)-7(〔(2-氨基-4-噻唑基)-〔(1-羧基-1-甲基乙氧基)亚氨基〕乙酰基〕氨基〕-2-羧基-8-氧代-5-硫杂-1-氮杂双环[4.2.0]辛-2-烯-3-甲基吡啶鎓内盐五水合物化学结构式:分子式:C22H22N6O7S2·5 H2O分子量:636.65辅料:无水碳酸钠【性状】白色或类白色结晶性无菌粉末,供配制成注射液。
【适应症】头孢他啶适用于由敏感细菌所引起的单一感染及由二种或二种以上的敏感菌引起的混合感染。
全身性的严重感染;呼吸道感染;耳、鼻和喉感染;尿路感染;皮肤及软组织感染;胃肠、胆及腹部感染;骨骼及关节感染;与血液透析和腹膜透析及持续腹膜透析(CAPD)有关的感染。
对于脑膜炎,仅在得到敏感试验结果后,才能应用单一的头孢他啶治疗。
头孢他啶可用于耐其它抗生素包括氨基糖苷类和多数头孢菌素的感染。
如果合适,可联同氨基糖苷类或其它β-内酰胺类抗生素使用,例如在严重中性粒细胞减少时,或在怀疑是脆弱拟杆菌感染时,与另一种抗厌氧菌抗生素合用。
另外,头孢他啶还可用于经尿道前列腺切除手术的预防治疗。
头孢他啶的敏感性存在差异,应该咨询可适用的地理、时间和当地敏感性数据(见【药理毒理】部分)。
【规格】每瓶含1g头孢他啶(五水合物形式),及118mg碳酸钠。
【用法用量】头孢他啶是肠道外给药,剂量依感染的严重程度、敏感性、感染种类及病人的年龄、体重和肾功能而定。
成人:头孢他啶的成人剂量范围是每天1g至6g,分每8小时或每12小时作静脉注射或肌肉注射给药。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
头孢他啶说明书
头孢他啶
Ceftazidime,Fortum
别名:、头孢塔齐定、噻甲酸肟头孢菌素、凯复定、复达欣、CAZ。
中文名称头孢他啶
中文别名 6R,7R-7-[[2Z-2-2-氨基-1,3-噻唑-4-基-2-1-羟基-2-甲基-1-氧代丙烷-2-基氧亚氨乙酰]氨基]-8-氧代-3-吡啶-1-鎓-1-基甲基-5-硫杂-1-氮杂双环[4.2.0]辛-2-烯-2-甲酸
英文名称 Ceftazidime
英文别名 Ceftazidime anhydrous; 1-6r,7r-7-2z-2-amino-4-thiazolyl1-carboxy-1-methylethoxyimino acetyl amino-2-carboxy-8-oxo-5-thia-1-azabicyclo4.2.0
oct-2-en-3-ylmethylpyridinum hydroxide inner salt;
6R,7R-7-{2Z-2-2-amino-1,3-thiazol-4-yl-2-[1-carboxy-1-methylethoxyimino]acetyl}amino-8-oxo-3-pyridinium-1-ylmethyl-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylate;
6R,7R-7-{2Z-2-2-amino-1,3-thiazol-4-yl-2-[1-carboxy-1-methylethoxyimino]acetyl}amino-8-oxo-3-pyridinium-1-ylmethyl-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylate pentahydrate;
6R,7R-7-[3Z-3-2-aminothiazol-4-yl-3-2-hydroxy-1,1-dimethyl-2-oxo-ethoxyimino-2-oxo-propyl]-8-oxo-3-pyridin-1-ium-1-ylmethyl-5-thia-1-azabicyclo[4.2.0]oct-2-ene-2-carboxylate
EINECS 276-715-9
分子式 C22H22N6O7S2
【性状】无色或微黄色粉末,加水即泡腾溶解生成澄明药液。
因浓度的不同,药液可由浅黄色至琥珀色。
新制备液的pH为6~8。
【作用与用途】
该品为第三代头孢菌素类抗生素,抗菌活力较强,抗菌谱较广,对革兰阳性或阴性菌均具有较强作用。
对革兰阳性菌、阴性菌产生的β内酰胺酶具有高度的稳定性,该品对绿脓杆菌、大肠杆菌、克雷白杆菌、变形杆菌、沙门菌、志贺菌、淋病奈瑟菌、脑膜炎奈瑟菌、金葡菌、溶血性链球菌、肺炎球菌及产气杆菌等具有强的抗菌活性,特别是对于绿脓杆菌作用最强抗生素。
可用于治疗单纯的感染或由两种以上敏感菌引起的混合感染。
临床上主要用于败血症、菌血症、支气管炎、肺炎、胸膜炎、腹膜炎、肾盂肾炎、尿路感染、前列腺炎、膀胱炎、
耳鼻咽喉感染、皮肤和软组织感染、骨和关节感染、盆腔炎及烧伤等。
属于新型农村合作医疗报销基本药物目录中药物。
作用机制
头孢他啶的抗菌作用机制为影响细菌细胞壁的合成。
与其它头孢菌素类药相似,该品
能抑制转肽酶在细胞壁合成的最后一步交叉连接中的转肽作用,使交叉连接不能形成,从
而影响细胞壁合成,导致细菌溶菌死亡。
用法用量
静脉注射或静脉滴注。
剂量依感染的严重程度、微生物敏感性及患者机体状态而定。
成人:
1.败血症、下呼吸道感染、胆道感染等,一日4~6g,分2~3次静脉滴注或静脉注射,疗程10~14日。
2.泌尿系统感染和重度皮肤软组织感染等,一日2~4g,分2次静脉滴注或静脉注射,疗程7~14日。
对于轻度尿路感染,每12小时0.5~1g即已足够。
3.对于某些危及生命的感染、严重铜绿假单胞菌感染和中枢神经系统感染,可酌情增
量至一日0.15~0.2g/kg,分3次静脉滴注或静脉注射。
儿童:2个月以上婴幼儿常用剂量为一日30~100mg/kg,分2~3次静脉滴注。
对新
生儿至2个月婴儿临床经验有限。
肾功能损害患者:因头孢他啶主要经肾脏排泄,对肾功能损害患者应减量使用,可根
据肌酐清除率来计算合适的给药剂量。
透析后患者应重复适当维持剂量。
配制方法:5ml注射用水加入0.5g装瓶中或10ml注射用水加入1g或2g装瓶中,使
完全溶解后,于3~5分钟静脉缓慢推注。
也可将上述溶解后的药液含1~2g用5%葡萄糖
或生理盐水100ml稀释后静脉滴注20-30分钟。
【药品名称】
通用名称:注射用头孢他啶
英文名称:Ceftazidime for Injection
拼音名称:Zhusheyong Toubatading
【成份】本品成分为头孢他啶
【性状】本品为白色或类白色结晶性粉末。
【抗菌作用】头孢他啶对大肠杆菌、肺炎克雷伯氏杆菌等肠杆菌科细菌和流感杆菌、绿脓杆菌等有较好的抗菌活性,本品对硝酸盐阴性杆菌、产碱杆菌等亦有良好抗菌作用。
本品对于细菌产生的大多数β-内酰胺酶高度稳定,故其对上述革兰氏阴性杆菌中多
重耐药菌株仍可具抗菌活性。
肺炎球菌、溶血性链球菌等革兰氏阳性球菌对头孢他啶高度敏感,但本品对葡萄球菌
仅具中度活性,肠球菌和耐甲氧西林葡萄球菌则往往对本品耐药。
本品对消化球菌和消化链球菌等厌氧菌具一定抗菌
【适应症】本品适用于由敏感菌所致的呼吸道感染、泌尿道感染、皮肤及软组织感染、胃肠、胆及腹部感染、骨和关节感染、透析有关血和腹膜透析及不卧床之延续腹膜透析而
并发的感染、感染的预防治疗,以及败血症、菌血症、腹膜炎、脑膜炎、免疫受抑制的病
人之感染和感染性烧伤。
【规格】1.0g/支1.0g C22H22N6O7S2 + 0.118g Na2CO3。
【用法用量】成人:
泌尿道或较轻的感染:每日1~2克,分2次静滴或静注;
大多数感染:每日2~4克,分2~3次静滴或静注;
非常严重的感染:每日4~6克,分2~3次静滴或静注。
疗程:7~14天。
婴幼儿出生2个月以上:常用剂量为每日30~100mg/kg,分2~3次静脉滴注。
【不良反应】1.胃肠道: 恶心、腹泻、呕吐、腹痛等;
2.过敏反应:皮疹、荨麻疹、皮肤搔痒、嗜酸细胞增多;
3.中枢神经系统:头痛、眩晕、味觉异常;
4.其他:血清肝酶、BUN、肌酐增高。
【禁忌】对本品或头孢菌素类过敏者禁用。
【注意事项】
1.对青霉素过敏者、肾功能严重损伤者、孕妇及哺乳妇女慎用。
2.与氨基糖甙类抗生素或速尿等强利尿剂合用时需严密观察肾功能情况。
【贮藏】避光、密闭,在凉暗处保存。
【有效期】暂定24个月半。
【执行标准】本品成分为头孢他啶
头孢他啶的副作用
1 过敏反应,主要是红斑及荨麻疹、瘙痒、药物热,偶有血管性水肿、气喘和低血压。
2 恶心、呕吐及腹泻等胃肠道反应。
3 血清丙氨酸氨基转移酶可轻度升高。
4 局部肌注部位可引起疼痛,静注可引起静脉炎或血栓性静脉炎。
5 少有头痛、眩晕感觉失常等神经系统反应。
6 对头孢菌素类抗生素有过敏的病人禁用。
感谢您的阅读,祝您生活愉快。