文拉法辛说明书
文拉法辛的功能主治和副作用

文拉法辛的功能主治和副作用功能主治文拉法辛是一种非处方药,主要用于缓解疼痛和发热症状。
它属于非甾体抗炎药物(NSAIDs),具有镇痛、退热和抗炎作用。
以下是文拉法辛常见的功能主治:1.缓解头痛:文拉法辛是一种有效的缓解头痛的药物,可以被用来治疗由紧张、偏头痛或偏头痛等引起的疼痛。
2.缓解关节疼痛:文拉法辛可用于治疗由关节炎或关节损伤引起的关节疼痛和炎症。
它可以减轻关节肿胀和疼痛。
3.降低发热:文拉法辛具有退热的功效,可用于降低因感冒、流感或其他病毒感染引起的发热。
4.缓解肌肉酸痛:文拉法辛可以缓解肌肉酸痛和炎症,可用于治疗由肌肉劳损、过度使用或其他肌肉受伤引起的疼痛。
5.缓解牙痛:文拉法辛在牙科领域中也有应用,可用于缓解由牙龈炎、智齿或其他牙齿问题引起的牙痛。
副作用尽管文拉法辛是一种常见且通常较安全的非处方药,但它仍可能引起一些副作用。
与其他非甾体抗炎药物类似,使用文拉法辛时应注意以下副作用:1.胃肠道不良反应:文拉法辛可引起胃肠道不适,如胃痛、恶心、呕吐和腹泻。
长期或高剂量使用可能导致胃溃疡或消化道出血。
2.高血压:文拉法辛可能导致血压升高,特别是在高风险人群中。
如果您已经有高血压或心血管疾病,应避免过量使用文拉法辛。
3.肾脏损伤:长期或高剂量使用文拉法辛可能损伤肾脏。
如果您有肾脏疾病或肾功能受损,应避免使用文拉法辛。
4.过敏反应:个别人可能对文拉法辛过敏,表现为皮疹、荨麻疹、呼吸困难、喉咙肿胀等症状。
如果出现过敏反应,应立即停止使用文拉法辛。
5.其他副作用:文拉法辛还可能引起头晕、嗜睡、视觉模糊、耳鸣等症状。
如果出现这些副作用,应减少剂量或停止使用。
注意:以上所列的副作用并不是究竟全部,如有任何不适症状,请咨询医生或药师。
使用注意事项除了了解文拉法辛的功能主治和副作用外,还应注意以下几点:1.建议在医生或药剂师的指导下使用文拉法辛。
根据个人情况,剂量和用法可能有所不同。
2.不要将文拉法辛与其他含有相同类型药物的产品一起使用,以避免剂量过高或重复用药。
文拉法辛缓释片结构式
文拉法辛缓释片结构式文拉法辛缓释片是一种用于治疗中度至重度疼痛的药物。
它主要成分是文拉法辛,一种鸦片类止痛药物。
与传统的口服药物相比,文拉法辛缓释片具有更长的药效持续时间和更好的疼痛控制效果。
文拉法辛缓释片的结构式如下所示:文拉法辛缓释片的结构式包含了药物的化学结构信息。
通过分析结构式,我们可以了解到文拉法辛缓释片的分子组成和结构特点,从而更好地理解药物的药理作用和药效持续时间。
文拉法辛缓释片的主要作用机制是通过与大脑中的鸦片受体结合,从而减少疼痛信号的传递。
文拉法辛缓释片透过皮肤缓慢释放药物,使药物能够持续地进入血液循环系统,实现长时间的止痛效果。
文拉法辛缓释片的使用方法非常简便。
患者只需将片剂贴在干净、无毛发的皮肤上,通常选择胸部、上臂或大腿内侧作为贴药部位。
贴药后,药物会逐渐通过皮肤渗透进入血液循环系统。
患者每7天更换一次贴药片即可。
文拉法辛缓释片的剂量由医生根据患者疼痛的严重程度和个体差异进行调整。
一般情况下,开始剂量为每天5微克/小时,根据需要逐渐增加。
然而,为了避免过量使用,患者应严格按照医生的指导进行用药。
文拉法辛缓释片具有许多优点。
首先,它能够提供持续的疼痛缓解效果,减少患者频繁服药的需求。
其次,贴片的使用方式方便简单,不需要注射或口服。
此外,贴片可以减少药物在胃肠道的代谢,降低对肝脏的负担。
然而,文拉法辛缓释片也存在一定的注意事项。
首先,患者需要注意贴药部位的清洁和干燥,避免汗水、油脂等物质影响药物吸收。
其次,对于孕妇、哺乳期妇女和儿童等特殊人群,应在医生的指导下使用。
最后,患者在使用文拉法辛缓释片期间应避免饮酒,以免增加药物的镇静和呼吸抑制效果。
文拉法辛缓释片是一种有效的治疗疼痛的药物。
通过贴片的方式,药物能够持续地释放,提供长时间的止痛效果。
然而,在使用文拉法辛缓释片时,患者需要严格按照医生的指导进行用药,并注意贴药部位的清洁和干燥。
只有在医生的监督下合理使用,才能最大程度地发挥文拉法辛缓释片的治疗效果。
文拉法辛的用法用量
文拉法辛的用法用量
文拉法辛是一种强效利尿剂,通常用于治疗心力衰竭和高血压等疾病。
其用法和用量应根据患者的具体情况而定,应严格遵守医师的处方和建议进行。
一般情况下,成人一次口服文拉法辛的剂量为20毫克,一天最多不超过80毫克。
对于肾功能不良、年龄较大或有其他基础疾病的患者,剂量应减少或调整。
通常将文拉法辛在早晨或中午饭后口服,以便在正常睡眠时避免夜间尿频的麻烦。
必要时,医生可能会建议调整用药时间以获得最佳效果。
在使用文拉法辛期间,患者需要密切监测自己的体重、血压和尿量等指标,并及时向医生汇报任何异常。
同时,遵循医生的建议,避免饮酒、吃含钠、钾高的食物,以及注意饮食和生活方式的调整,有助于提高治疗效果。
盐酸文拉法辛胶囊说明书

盐酸文拉法辛胶囊说明书通用名:盐酸文拉法辛胶囊生产厂家: 山东鑫齐药业有限公司批准文号:国药准字H20214040药品规格:25mg*20s药品价格:¥48元【通用名称】盐酸文拉法辛胶囊【商品名称】盐酸文拉法辛胶囊【英文名称】VenlafaxineHydrochlorideCapsules【拼音全码】YanSuanWenLaFaXinJiaoNang【主要成份】盐酸文拉法辛。
化学名:±-1-[2-二甲胺基-1-4-甲氧苯基乙基]-环已醇盐酸盐分子式:C17H27NO2·HCl分子量:313.87【性状】盐酸文拉法辛胶囊为胶囊剂,内容物为白色粉末。
【适应症/功能主治】各种类型抑郁症,包括伴有焦虑的抑郁症及广泛性焦虑症。
【规格型号】25mg*20s【用法用量】口服,开始剂量为一次25mg,一日23次,数周后逐渐增至一日75mg225mg,分23次口服。
高量为一日350mg。
可与食物同时服用。
【不良反应】可有胃肠道不适如恶心、厌食、腹泻等。
亦可出现头痛、不安、无力、嗜睡、失眠、头晕或震颤等。
少见不良反应有过敏性皮疹及性功能减退。
可引起血压升高,且与剂量呈正相关。
大剂量时可诱发癫痫。
突然停药可见撤药综合症如失眠、焦虑、恶心、出汗、震颤、眩晕或感觉异常等。
【禁忌】对盐酸文拉法辛胶囊过敏者及正在服用单胺氧化酶抑制剂的患者禁用。
【注意事项】1.闭角型青光眼、癫痫患者慎用。
2.严重心脏疾患、高血压、甲状腺疾病、血液病患者慎用。
3.肝肾功能不全者慎用或减少用量。
4.用药过程中应监测血压,血压升高应减量或停药。
5.停用时应逐渐减少剂量,已应用盐酸文拉法辛胶囊6周或更长时间者,应在2周内逐渐减量。
6.患者出现有转向躁狂发作倾向时应立即停药。
7.用药期间不宜驾驶车辆、操作机械或高空作业。
【儿童用药】慎用。
【老年患者用药】慎用。
【孕妇及哺乳期妇女用药】慎用。
【药物相互作用】1.与选择性5-羟色胺再摄取抑制剂或与单胺氧化酶抑制剂合用时,可引起高血压、僵硬、肌阵挛、不自主运动、焦虑不安、意识障碍乃至昏迷和死亡。
文拉法辛说明书 英文
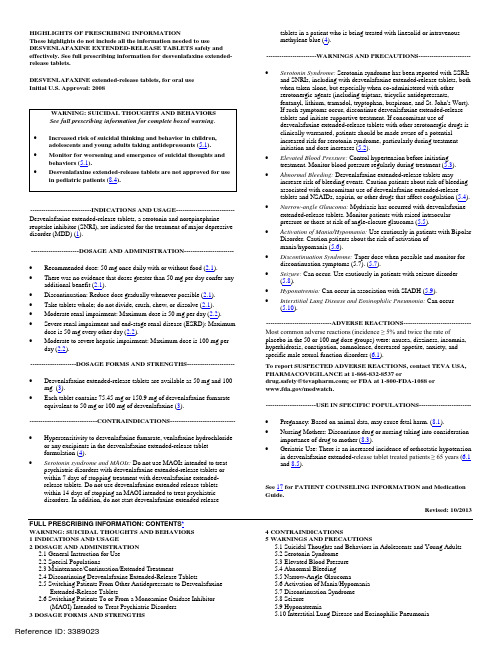
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use DESVENLAFAXINE EXTENDED-RELEASE TABLETS safely and effectively. See full prescribing information for desvenlafaxine extended-tablets in a patient who is being treated with linezolid or intravenousmethylene blue (4).-----------------------WARNINGS AND PRECAUTIONS-----------------------release tablets.DESVENLAFAXINE extended-release tablets, for oral useInitial U.S. Approval: 2008WARNING: SUICIDAL THOUGHTS AND BEHAVIORSSee full prescribing information for complete boxed warning.•••Increased risk of suicidal thinking and behavior in children, adolescents and young adults taking antidepressants (5.1). Monitor for worsening and emergence of suicidal thoughts and behaviors (5.1).Desvenlafaxine extended-release tablets are not approved for use in pediatric patients (8.4).----------------------------INDICATIONS AND USAGE---------------------------Desvenlafaxine extended-release tablets, a serotonin and norepinephrine reuptake inhibitor (SNRI), are indicated for the treatment of major depressive disorder (MDD) (1).----------------------DOSAGE AND ADMINISTRATION----------------------•Recommended dose: 50 mg once daily with or without food (2.1). •There was no evidence that doses greater than 50 mg per day confer any additional benefit (2.1).•Discontinuation: Reduce dose gradually whenever possible (2.1). •Take tablets whole; do not divide, crush, chew, or dissolve (2.1). •Moderate renal impairment: Maximum dose is 50 mg per day (2.2). •Severe renal impairment and end-stage renal disease (ESRD): Maximum dose is 50 mg every other day (2.2).•Moderate to severe hepatic impairment: Maximum dose is 100 mg per day (2.2).---------------------DOSAGE FORMS AND STRENGTHS---------------------• Desvenlafaxine extended-release tablets are available as 50 mg and 100 mg (3).• Each tablet contains 75.45 mg or 150.9 mg of desvenlafaxine fumarate equivalent to 50 mg or 100 mg of desvenlafaxine (3).-------------------------------CONTRAINDICATIONS-----------------------------• Hypersensitivity to desvenlafaxine fumarate, venlafaxine hydrochloride or any excipients in the desvenlafaxine extended-release tabletformulation (4).• Serotonin syndrome and MAOIs: Do not use MAOIs intended to treat psychiatric disorders with desvenlafaxine extended-release tablets orwithin 7 days of stopping treatment with desvenlafaxine extended-release tablets. Do not use desvenlafaxine extended release tabletswithin 14 days of stopping an MAOI intended to treat psychiatricdisorders. In addition, do not start desvenlafaxine extended release FULL PRESCRIBING INFORMATION: CONTENTS*WARNING: SUICIDAL THOUGHTS AND BEHAVIORS1 INDICATIONS AND USAGE2 DOSAGE AND ADMINISTRATION2.1 General Instruction for Use2.2 Special Populations2.3 Maintenance/Continuation/Extended Treatment2.4 Discontinuing Desvenlafaxine Extended-Release Tablets2.5 Switching Patients From Other Antidepressants to DesvenlafaxineExtended-Release Tablets2.6 Switching Patients To or From a Monoamine Oxidase Inhibitor(MAOI) Intended to Treat Psychiatric Disorders3 DOSAGE FORMS AND STRENGTHS •Serotonin Syndrome: Serotonin syndrome has been reported with SSRIs and SNRIs, including with desvenlafaxine extended-release tablets, both when taken alone, but especially when co-administered with otherserotonergic agents (including triptans, tricyclic antidepressants,fentanyl, lithium, tramadol, tryptophan, buspirone, and St. John's Wort).If such symptoms occur, discontinue desvenlafaxine extended-releasetablets and initiate supportive treatment. If concomitant use ofdesvenlafaxine extended-release tablets with other serotonergic drugs is clinically warranted, patients should be made aware of a potentialincreased risk for serotonin syndrome, particularly during treatmentinitiation and dose increases (5.2).•Elevated Blood Pressure: Control hypertension before initiating treatment. Monitor blood pressure regularly during treatment (5.3). •Abnormal Bleeding: Desvenlafaxine extended-release tablets may increase risk of bleeding events. Caution patients about risk of bleeding associated with concomitant use of desvenlafaxine extended-releasetablets and NSAIDs, aspirin, or other drugs that affect coagulation (5.4). •Narrow-angle Glaucoma: Mydriasis has occurred with desvenlafaxine extended-release tablets. Monitor patients with raised intraocularpressure or those at risk of angle-closure glaucoma (5.5).•Activation of Mania/Hypomania: Use cautiously in patients with Bipolar Disorder. Caution patients about the risk of activation ofmania/hypomania (5.6).•Discontinuation Syndrome: Taper dose when possible and monitor for discontinuation symptoms (5.7). (5.7).•Seizure: Can occur. Use cautiously in patients with seizure disorder(5.8).•Hyponatremia: Can occur in association with SIADH (5.9). •Interstitial Lung Disease and Eosinophilic Pneumonia: Can occur(5.10).------------------------------ADVERSE REACTIONS------------------------------Most common adverse reactions (incidence ≥ 5% and twice the rate of placebo in the 50 or 100 mg dose groups) were: nausea, dizziness, insomnia, hyperhidrosis, constipation, somnolence, decreased appetite, anxiety, and specific male sexual function disorders (6.1).To report SUSPECTED ADVERSE REACTIONS, contact TEVA USA, PHARMACOVIGILANCE at 1-866-832-8537 ordrug.safety@; or FDA at 1-800-FDA-1088 or/medwatch.-----------------------USE IN SPECIFIC POPULATIONS-----------------------• Pregnancy: Based on animal data, may cause fetal harm. (8.1).• Nursing Mothers: Discontinue drug or nursing taking into consideration importance of drug to mother (8.3).• Geriatric Use: There is an increased incidence of orthostatic hypotension in desvenlafaxine extended-release tablet treated patients ≥ 65 years (6.1 and 8.5).See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.Revised: 10/20134 CONTRAINDICATIONS5 WARNINGS AND PRECAUTIONS5.1 Suicidal Thoughts and Behaviors in Adolescents and Young Adults5.2 Serotonin Syndrome5.3 Elevated Blood Pressure5.4 Abnormal Bleeding5.5 Narrow-Angle Glaucoma5.6 Activation of Mania/Hypomania5.7 Discontinuation Syndrome5.8 Seizure5.9 Hyponatremia5.10 Interstitial Lung Disease and Eosinophilic Pneumonia6 ADVERSE REACTIONS6.1 Clinical Studies Experience6.2 Postmarketing Experience7 DRUG INTERACTIONS7.1 Monoamine Oxidase Inhibitors (MAOI)7.2 Serotonergic Drugs7.3 Drugs that Interfere with Hemostasis (e.g., NSAIDs, Aspirin, andWarfarin)7.4 Potential for Desvenlafaxine to Affect Other Drugs7.5 Other Drugs Containing Desvenlafaxine or Venlafaxine7.6 Ethanol8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.3 Nursing Mothers8.4 Pediatric Use8.5 Geriatric Use8.6 Renal ImpairmentFULL PRESCRIBING INFORMATION8.7 Hepatic Impairment9 DRUG ABUSE AND DEPENDENCE9.1 Controlled Substance10 OVERDOSAGE10.1 Human Experience With Overdosage10.2 Management of Overdosage11 DESCRIPTION12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.2 Pharmacodynamics12.3 Pharmacokinetics13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility14 CLINICAL STUDIES16 HOW SUPPLIED/STORAGE AND HANDLING17 PATIENT COUNSELING INFORMATION*Sections or subsections omitted from the full prescribing information are not listed.WARNING: SUICIDAL THOUGHTS AND BEHAVIORSAntidepressants increased the risk of suicidal thoughts and behavior in children,adolescents, and young adults in short-term studies. These studies did not show anincrease in the risk of suicidal thoughts and behavior with antidepressant use in patientsover age 24; there was a reduction in risk with antidepressant use in patients aged 65 andolder [see Warnings and Precautions (5.1)].In patients of all ages who are started on antidepressant therapy, monitor closely forworsening, and for emergence of suicidal thoughts and behaviors. Advise families andcaregivers of the need for close observation and communication with the prescriber [seeWarnings and Precautions (5.1)].Desvenlafaxine extended-release tablets are not approved for use in pediatric patients[see Use in Specific Populations (8.4)].1 INDICATIONS AND USAGEDesvenlafaxine extended-release tablets, a serotonin and norepinephrine reuptake inhibitor (SNRI), are indicated for the treatment of major depressive disorder (MDD) [see Clinical Studies (14) and Dosage and Administration (2.1)]. The efficacy of desvenlafaxine extended-release tablets has been established in four short-term (8-week, placebo-controlled studies) in adult outpatients who met DSM-IV criteria for major depressive disorder.2 DOSAGE AND ADMINISTRATION2.1 General Instruction for UseThe recommended dose for desvenlafaxine extended-release tablets is 50 mg once daily, with or without food.In clinical studies, doses of 50 mg to 400 mg per day were shown to be effective, although no additional benefit was demonstrated at doses greater than 50 mg per day and adverse reactions and discontinuations were more frequent at higher doses.When discontinuing therapy, gradual dose reduction is recommended whenever possible to minimize discontinuation symptoms [see Dosage and Administration (2.4) and Warnings and Precautions (5.7)].Desvenlafaxine extended-release tablets should be taken at approximately the same time each day. Tablets must be swallowed whole with fluid and not divided, crushed, chewed, or dissolved.2.2 Special PopulationsPatients with renal impairmentThe maximum recommended dose in patients with moderate renal impairment (24-hr creatinine clearance [CrCl] = 30 to 50 mL/min, Cockcroft-Gault [C-G]) is 50 mg per day. The maximum recommended dose in patients with severe renal impairment (24-hr CrCl less than 30 mL/min, C-G) or end-stage renal disease (ESRD) is 50 mg every other day. Supplemental doses should not be given to patients after dialysis [see Use in Specific Populations (8.6) and Clinical Pharmacology (12.3)].Patients with hepatic impairmentThe recommended dose in patients with moderate to severe hepatic impairment is 50 mg per day. Dose escalation above 100 mg per day is not recommended [see Clinical Pharmacology (12.3)].2.3 Maintenance/Continuation/Extended TreatmentIt is generally agreed that acute episodes of major depressive disorder require several months or longer of sustained pharmacologic therapy. Patients should be periodically reassessed to determine the need for continued treatment.2.4 Discontinuing Desvenlafaxine Extended-Release TabletsSymptoms associated with discontinuation of desvenlafaxine extended-release tablets, other SNRIs and SSRIs have been reported [see Warnings and Precautions (5.7)]. Patients should be monitored for these symptoms when discontinuing treatment. A gradual reduction in the dose rather than abrupt cessation is recommended whenever possible. If intolerable symptoms occur following a decrease in the dose or upon discontinuation of treatment, then resuming the previously prescribed dose may be considered. Subsequently, the physician may continue decreasing the dose, but at a more gradual rate.2.5 Switching Patients From Other Antidepressants to Desvenlafaxine Extended-Release Tablets Discontinuation symptoms have been reported when switching patients from other antidepressants, including venlafaxine, to desvenlafaxine extended-release tablets. Tapering of the initial antidepressant may be necessary to minimize discontinuation symptoms.2.6 Switching Patients To or From a Monoamine Oxidase Inhibitor (MAOI) Intended to Treat Psychiatric DisordersAt least 14 days should elapse between discontinuation of an MAOI intended to treat psychiatric disorders and initiation of therapy with desvenlafaxine extended-release tablets. Conversely, at least 7 days should be allowed after stopping desvenlafaxine extended-release tablets before starting an MAOI intended to treat psychiatric disorders [see Contraindications (4)].Use of Desvenlafaxine Extended-Release Tablets with other MAOIs such as Linezolid or Methylene BlueDo not start desvenlafaxine extended-release tablets in a patient who is being treated with linezolid or intravenous methylene blue because there is increased risk of serotonin syndrome. In a patient who requires more urgent treatment of a psychiatric condition, other interventions, including hospitalization, should be considered [see Contraindications (4)].In some cases, a patient already receiving desvenlafaxine extended-release tablet therapy may require urgent treatment with linezolid or intravenous methylene blue. If acceptable alternatives to linezolid or intravenous methylene blue treatment are not available and the potential benefits of linezolid or intravenous methylene blue treatment are judged to outweigh the risks of serotonin syndrome in a particular patient, desvenlafaxine extended-release tablets should be stopped promptly, and linezolid or intravenous methylene blue can be administered. The patient should be monitored for symptoms of serotonin syndrome for 7 days or until 24 hours after the last dose of linezolid or intravenous methylene blue, whichever comes first. Therapy with desvenlafaxine extended-release tablets may be resumed 24 hours after the last dose of linezolid or intravenous methylene blue [see Warnings and Precautions (5.2)].The risk of administering methylene blue by non-intravenous routes (such as oral tablets or by local injection) or in intravenous doses much lower than 1 mg/kg with desvenlafaxine extended-release tablets is unclear. The clinician should, nevertheless, be aware of the possibility of emergent symptoms of serotonin syndrome with such use [see Warnings and Precautions (5.2)].3 DOSAGE FORMS AND STRENGTHSDesvenlafaxine extended-release tablets are available as:50 mg, light-pink, film-coated round shaped tablets, debossed with "T" on one side of the tablet and with "N1" on the other side.100 mg, reddish-orange, film-coated round shaped tablet, debossed with "T" on one side of the tablet and with "N2" on the other side.4 CONTRAINDICATIONS• Hypersensitivity to desvenlafaxine fumarate, venlafaxine hydrochloride or to any excipients in the desvenlafaxine extended-release tablet formulation. Angioedema has been reported in patients treated with desvenlafaxine extended-release tablets [see Adverse Reactions (6.1)].• The use of MAOIs intended to treat psychiatric disorders with desvenlafaxine extended-release tablets or within 7 days of stopping treatment with desvenlafaxine extended-release tablets is contraindicated because of an increased risk of serotonin syndrome. The use of desvenlafaxine extended-release tablets within 14 days of stopping an MAOI intended to treat psychiatric disorders is also contraindicated [see Dosage and Administration (2.6) and Warnings and Precautions (5.2)].Starting desvenlafaxine extended-release tablets in a patient who is being treated with MAOIs such as linezolid or intravenous methylene blue is also contraindicated because of an increased risk of serotonin syndrome [see Dosage and Administration (2.6) and Warnings and Precautions (5.2)].5 WARNINGS AND PRECAUTIONS5.1 Suicidal Thoughts and Behaviors in Adolescents and Young AdultsPatients with major depressive disorder (MDD), both adult and pediatric, may experience worsening of their depression and/or the emergence of suicidal ideation and behavior (suicidality) or unusual changes in behavior, whether or not they are taking antidepressant medications, and this risk may persist until significant remission occurs. Suicide is a known risk of depression and certain other psychiatric disorders, and these disorders themselves are the strongest predictors of suicide. There has been a long-standing concern, however, that antidepressants may have a role in inducing worsening of depression and the emergence of suicidality in certain patients during the early phases of treatment. Pooled analyses of short-term placebo-controlled studies of antidepressant drugs (SSRIs and others) showed that these drugs increase the risk of suicidal thinking and behavior (suicidality) in children, adolescents, and young adults (ages 18 to 24) with major depressive disorder (MDD) and other psychiatric disorders. Short-term studies did not show an increase in the risk ofsuicidality with antidepressants compared to placebo in adults beyond age 24; there was a reduction with antidepressants compared to placebo in adults aged 65 and older.The pooled analyses of placebo-controlled studies in children and adolescents with MDD, obsessive compulsive disorder (OCD), or other psychiatric disorders included a total of 24 short-term studies of 9 antidepressant drugs in over 4,400 patients. The pooled analyses of placebo-controlled studies in adults with MDD or other psychiatric disorders included a total of 295 short-term studies (median duration of 2 months) of 11 antidepressant drugs in over 77,000 patients. There was considerable variation in risk of suicidality among drugs, but a tendency toward an increase in the younger patients for almost all drugs studied. There were differences in absolute risk of suicidality across the different indications, with the highest incidence in MDD. The risk differences (drug vs. placebo), however, were relatively stable within age strata and across indications. These risk differences (drug-placebo difference in the number of cases of suicidality per 1000 patients treated) are provided in Table 1.Table 1Drug-Placebo Difference in Number of Cases of Suicidality per 1,000Patients TreatedAge RangeIncreases Compared to Placebo< 18 14 additional cases18 to 24 5 additional casesDecreases Compared to Placebo25 to 64 1 fewer case≥ 65 6 fewer casesNo suicides occurred in any of the pediatric studies. There were suicides in the adult studies, but the number was not sufficient to reach any conclusion about drug effect on suicide.It is unknown whether the suicidality risk extends to longer-term use, i.e., beyond several months. However, there is substantial evidence from placebo-controlled maintenance studies in adults with depression that the use of antidepressants can delay the recurrence of depression.All patients being treated with antidepressants for any indication should be monitored appropriately and observed closely for clinical worsening, suicidality, and unusual changes in behavior, especially during the initial few months of a course of drug therapy, or at times of dose changes, either increases or decreases.The following symptoms, anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness, impulsivity, akathisia (psychomotor restlessness), hypomania, and mania, have been reported in adult and pediatric patients being treated with antidepressants for major depressive disorder as well as for other indications, both psychiatric and nonpsychiatric. Although a causal link between the emergence of such symptoms and either the worsening of depression and/or the emergence of suicidal impulses has not been established, there is concern that such symptoms may represent precursors to emerging suicidality.Consideration should be given to changing the therapeutic regimen, including possibly discontinuing the medication, in patients whose depression is persistently worse, or who are experiencing emergent suicidality or symptoms that might be precursors to worsening depression or suicidality, especially if these symptoms are severe, abrupt in onset, or were not part of the patient’s presenting symptoms.If the decision has been made to discontinue treatment, medication should be tapered, as rapidly as is feasible, but with recognition that abrupt discontinuation can be associated with certain symptoms [see Dosage and Administration (2.4) and Warnings and Precautions (5.7) for a description of the risks of discontinuation of desvenlafaxine extended-release tablets].Families and caregivers of patients being treated with antidepressants for major depressive disorder or other indications, both psychiatric and nonpsychiatric, should be alerted about the need to monitor patients for the emergence of agitation, irritability, unusual changes in behavior, and the other symptoms described above, as well as the emergence of suicidality, and to report such symptoms immediately to healthcare providers. Such monitoring should include daily observation by families and caregivers.Prescriptions for desvenlafaxine extended-release tablets should be written for the smallest quantity of tablets consistent with good patient management, in order to reduce the risk of overdose.Screening patients for bipolar disorderA major depressive episode may be the initial presentation of bipolar disorder. It is generally believed (though not established in controlled studies) that treating such an episode with an antidepressant alone may increase the likelihood of precipitation of a mixed/manic episode in patients at risk for bipolar disorder. Whether any of the symptoms described above represent such a conversion is unknown. However, prior to initiating treatment with an antidepressant, patients with depressive symptoms should be adequately screened to determine if they are at risk for bipolar disorder; such screening should include a detailed psychiatric history, including a family history of suicide, bipolar disorder, and depression. It should be noted that desvenlafaxine extended-release tablets are not approved for use in treating bipolar depression.5.2 Serotonin SyndromeThe development of a potentially life-threatening serotonin syndrome has been reported with SNRIs and SSRIs, including desvenlafaxine extended-release tablets, alone but particularly with concomitant use of other serotonergic drugs (including triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, tryptophan, buspirone, and St. John's Wort), and with drugs that impair metabolism of serotonin (in particular, MAOIs, both those intended to treat psychiatric disorders and also others, such as linezolid and intravenous methylene blue).Serotonin syndrome symptoms may include mental status changes (e.g., agitation, hallucinations, delirium, and coma), autonomic instability (e.g., tachycardia, labile blood pressure, dizziness, diaphoresis, flushing, hyperthermia), neuromuscular symptoms (e.g., tremor, rigidity, myoclonus, hyperreflexia, incoordination), seizures, and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea). Patients should be monitored for the emergence of serotonin syndrome.The concomitant use of desvenlafaxine extended-release tablets with MAOIs intended to treat psychiatric disorders is contraindicated. Desvenlafaxine extended-release tablets should also not be started in a patient who is being treated with MAOIs such as linezolid or intravenous methylene blue. All reports with methylene blue that provided information on the route of administration involved intravenous administration in the dose range of 1 mg/kg to 8 mg/kg. No reports involved the administration of methylene blue by other routes (such as oral tablets or local tissue injection) or at lower doses. There may be circumstances when it is necessary to initiate treatment with a MAOI such as linezolid or intravenous methylene blue in a patient taking desvenlafaxine extended-release tablets. Desvenlafaxine extended-release tablets should be discontinued before initiating treatment with the MAOI [see Contraindications (4) and Dosage and Administration (2.6)]. If concomitant use of desvenlafaxine extended-release tablets with other serotonergic drugs, including triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, buspirone, tryptophan, and St. John's Wort is clinically warranted, patients should be made aware of a potential increased risk for serotonin syndrome, particularly during treatment initiation and dose increases.Treatment with desvenlafaxine extended-release tablets and any concomitant serotonergic agents should be discontinued immediately if the above events occur and supportive symptomatic treatment should be initiated.5.3 Elevated Blood PressurePatients receiving desvenlafaxine extended-release tablets should have regular monitoring of blood pressure since increases in blood pressure were observed in clinical studies [see Adverse Reactions (6.1)]. Pre-existing hypertensionshould be controlled before initiating treatment with desvenlafaxine extended-release tablets. Caution should be exercised in treating patients with pre-existing hypertension, cardiovascular, or cerebrovascular conditions that might be compromised by increases in blood pressure. Cases of elevated blood pressure requiring immediate treatment have been reported with desvenlafaxine extended-release tablets.Sustained blood pressure increases could have adverse consequences. For patients who experience a sustained increase in blood pressure while receiving desvenlafaxine extended-release tablets, either dose reduction or discontinuation should be considered [see Adverse Reactions (6.1)].5.4 Abnormal BleedingSSRIs and SNRIs, including desvenlafaxine extended-release tablets, may increase the risk of bleeding events. Concomitant use of aspirin, nonsteroidal anti-inflammatory drugs, warfarin, and other anticoagulants may add to this risk. Case reports and epidemiological studies (case-control and cohort design) have demonstrated an association between use of drugs that interfere with serotonin reuptake and the occurrence of gastrointestinal bleeding. Bleeding events related to SSRIs and SNRIs have ranged from ecchymosis, hematoma, epistaxis, and petechiae to life-threatening hemorrhages. Patients should be cautioned about the risk of bleeding associated with the concomitant use of desvenlafaxine extended-release tablets and NSAIDs, aspirin, or other drugs that affect coagulation or bleeding.5.5 Narrow-Angle GlaucomaMydriasis has been reported in association with desvenlafaxine extended-release tablets; therefore, patients with raised intraocular pressure or those at risk of acute narrow-angle glaucoma (angle-closure glaucoma) should be monitored.5.6 Activation of Mania/HypomaniaDuring all MDD 2 and phase 3 studies, mania was reported for approximately 0.02% of patients treated with desvenlafaxine extended-release tablets. Activation of mania/hypomania has also been reported in a small proportion of patients with major affective disorder who were treated with other marketed antidepressants. As with all antidepressants, desvenlafaxine extended-release tablets should be used cautiously in patients with a history or family history of mania or hypomania.5.7 Discontinuation SyndromeDiscontinuation symptoms have been systematically and prospectively evaluated in patients treated with desvenlafaxine extended-release tablets during clinical studies in Major Depressive Disorder. Abrupt discontinuation or dose reduction has been associated with the appearance of new symptoms that include dizziness, nausea, headache, irritability, insomnia, diarrhea, anxiety, fatigue, abnormal dreams, and hyperhidrosis. In general, discontinuation events occurred more frequently with longer duration of therapy.During marketing of SNRIs (Serotonin and Norepinephrine Reuptake Inhibitors), and SSRIs (Selective Serotonin Reuptake Inhibitors), there have been spontaneous reports of adverse events occurring upon discontinuation of these drugs, particularly when abrupt, including the following: dysphoric mood, irritability, agitation, dizziness, sensory disturbances (e.g., paresthesia, such as electric shock sensations), anxiety, confusion, headache, lethargy, emotional lability, insomnia, hypomania, tinnitus, and seizures. While these events are generally self-limiting, there have been reports of serious discontinuation symptoms.Patients should be monitored for these symptoms when discontinuing treatment with desvenlafaxine extended-release tablets. A gradual reduction in the dose rather than abrupt cessation is recommended whenever possible. If intolerable symptoms occur following a decrease in the dose or upon discontinuation of treatment, then resuming the previously prescribed dose may be considered. Subsequently, the physician may continue decreasing the dose, but at a more gradual rate [see Dosage and Administration (2.4) and Adverse Reactions (6.1)].。
文拉法辛

大剂量时可能诱发癫痫。突然停药可有撤药综合征,如失眠、焦虑、恶心、出汗、震颤、眩晕或感觉异常等。 应逐渐减量而不是突然停药。如果使用文拉法辛超过6周,建议逐渐减量时间最少要多于两周。对于严重抑郁状态 患者,用药期间应密切观察病情。用药期间驾驶机动车或操纵机器患者应谨慎。
用药禁忌
各种抑郁症和广泛性焦虑症。
临床应用
口服:开始25毫克/次,2~3次/日,逐渐增至75~225毫克/日,分2~3次服用。缓释胶囊应按日剂量在固定 时间与食物一起每日一次服用。增加剂量的间隔不少于4天,每次增加75毫克/日。轻中度肾功能损伤患者,每天 给药总量降低25%~50%。轻中度肝损伤者,每日总剂量为常规用药剂量的一半或不足一半,需根据患者实际情况 个体化用药。
药物相互作用
1.与5-HT活性药物(TCAs、SSRIs、SNRIs、利奈唑胺、锂剂、圣约翰草、色氨酸、曲坦类药物、右苯丙胺、 芬氟拉明)合用,会引起5-HT综合征,故慎与这些药物合用。
2.与三氟拉嗪等抗精神病药合用可能会导致神经恶性综合征发生。与氯氮平、右美沙芬合用,均会相互作用, 导致对方血药浓度增加,而出现不良反应。本品减少氟哌啶醇代谢,两者合用应谨慎。
文拉法辛
二环类非典型抗抑郁药
01 适应证
盐酸文拉法辛缓释片说明书

常见食欲下降,便秘,恶心,呕吐,眩晕,口干,镇静,出汗(包括夜汗),虚弱/疲倦,高血压,紧张不安,呵欠,性功能异常等。 文拉法辛被突然停用、剂量降低或逐渐减少时,有报道以下的症状:轻躁狂、焦虑、激越、紧张不安、精神混乱、失眠或其它睡眠干扰、疲劳、嗜睡、感觉异常、头昏、惊厥、眩晕、头痛、耳鸣、发汗、口干、厌食、腹泻、恶心或呕吐。绝大多数的停药反应是轻度的并且无需治疗即可恢复。 按CIOMS不良反应发生率的分类,对不良反应列表如下:
【药理毒理】
非临床研究显示,文拉法辛及其活性代谢物O-去甲基文拉法辛是5-HT、NE再摄取的强抑制剂,是多巴胺的弱抑制剂。体外试验未发现文拉法辛及O-去甲基文拉法辛对M胆碱受体、H1组胺受体、α1-肾上腺素能受体有明显的亲和力。文拉法辛及O-去甲基文拉法辛无MAO抑制活性。动物试验显示,文拉法辛对醋酸、啤酒酵母【药代动力学】
文拉法辛容易吸收,主要在肝脏内代谢,O-去甲基文拉法辛(ODV)是其主要的活性代谢产物。单次口服本品后,至少有92%被吸收,其绝对生物利用度约为45%。文拉法辛及其代谢产物主要通过肾脏排泄。
常见:≥1%
少见:≥0.1%和<1%
罕见:≥0.01%和<0.1%
【禁忌】
对本品过敏者及正在服用单胺氧化酶抑制剂的患者禁用本品。
【注意事项】
闭角型青光眼、癫痫患者慎用;严重心脏疾患、高血压、甲状腺疾病、血液病患者慎用;肝肾功能不全者慎用或酌情减量;大剂量服用时应监测血压;孕妇和儿童应小心服用;患者出现有转向燥狂发作倾向时应立即停药;用药期间应尽量避免烟酒;需停药时应逐渐减少剂量,避免骤停骤加;食物对本品吸收无影响,为减少胃肠道不良反应,要求在餐中或餐后服用,避免餐前空腹服用。
盐酸文拉法辛缓释片说明书
文拉法辛原料及制剂(缓释胶囊、片、缓释片)(BP2013)
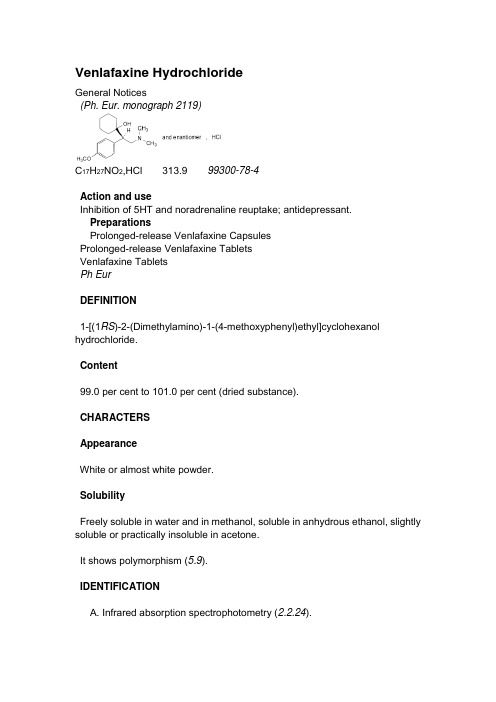
Venlafaxine HydrochlorideGeneral Notices(Ph. Eur. monograph 2119)C17H27NO2,HCl 313.9 99300-78-4Action and useInhibition of 5HT and noradrenaline reuptake; antidepressant.PreparationsProlonged-release Venlafaxine CapsulesProlonged-release Venlafaxine TabletsVenlafaxine TabletsPhEurDEFINITION1-[(1RS)-2-(Dimethylamino)-1-(4-methoxyphenyl)ethyl]cyclohexanol hydrochloride.Content99.0 per cent to 101.0 per cent (dried substance).CHARACTERSAppearanceWhite or almost white powder.SolubilityFreely soluble in water and in methanol, soluble in anhydrous ethanol, slightly soluble or practically insoluble in acetone.It shows polymorphism (5.9).IDENTIFICATIONA. Infrared absorption spectrophotometry (2.2.24).Comparison venlafaxine hydrochloride CRS.If the spectra obtained in the solid state show differences, dissolve the substance to be examined and the reference substance separately in2-propanol R, evaporate to dryness and record new spectra using the residues.B. It gives reaction (a) of chlorides (2.3.1).TESTSAcidity or alkalinityDissolve 0.20 g in carbon dioxide-free water R and dilute to 10 mL with the same solvent. Add 0.05 mL of methyl red solution R and 0.1 mL of 0.01 M hydrochloric acid. The solution is pink. Not more than 0.2 mL of 0.01 M sodium hydroxide is required to change the colour of the indicator to yellow.Related substancesLiquid chromatography (2.2.29).Test solution Dissolve 25.0 mg of the substance to be examined in the mobile phase and dilute to 25.0 mL with the mobile phase.Reference solution (a)Dilute 1.0 mL of the test solution to 10.0 mL with the mobile phase. Dilute 1.0 mL of this solution to 100.0 mL with the mobile phase.Reference solution (b)Dissolve the contents of a vial of venlafaxine for system suitability CRS (containing impurities D and F) in 1.0 mL of the mobile phase.Column:—size: l = 0.25 m, Ø = 4.6 mm;—stationary phase: end-capped octylsilyl silica gel for chromatography R (5 µm) with a pore size of 10 nm.Mobile phase Mix 510 volumes of acetonitrile R and 1490 volumes of a solution prepared as follows: dissolve 17 g of ammonium dihydrogen phosphate R in 1490 mL of water R and adjust to pH 4.4 using phosphoric acid R.Flow rate 1.2 mL/min.Detection Spectrophotometer at 225 nm.Injection20 µL.Run time10 times the retention time of venlafaxine.Relative retention With reference to venlafaxine (retention time = about 9 min): impurity D = about 0.9; impurity F = about 3.4.System suitability Reference solution (b):—resolution: minimum 1.5 between the peaks due to impurity D and venlafaxine.Limits:—impurity F: not more than the area of the principal peak in the chromatogram obtained with reference solution (a) (0.1 per cent);—unspecified impurities: for each impurity, not more than the area of the principal peak in the chromatogram obtained with reference solution (a) (0.10 per cent);—total: not more than twice the area of the principal peak in the chromatogram obtained with reference solution (a) (0.2 per cent); —disregard limit: 0.5 times the area of the principal peak in the chromatogram obtained with reference solution (a) (0.05 per cent).Heavy metals (2.4.8)Maximum 20 ppm.Dissolve 1.0 g in 20 mL of water R. 12 mL of the solution complies with test A. Prepare the reference solution using lead standard solution (1 ppm Pb) R. Loss on drying (2.2.32)Maximum 0.5 per cent, determined on 1.000 g by drying in vacuo at 80 °C for 3 h.Sulfated ash (2.4.14)Maximum 0.1 per cent, determined on 1.0 g.ASSAYDissolve 0.250 g in a mixture of 5.0 mL of 0.01 M hydrochloric acid and 50 mL of ethanol (96 per cent) R. Carry out a potentiometric titration (2.2.20), using 0.1 M sodium hydroxide. Read the volume added between the 2 points of inflexion. Carry out a blank titration.1 mL of 0.1 M sodium hydroxide is equivalent to 31.39 mg of C17H28ClNO2. IMPURITIESSpecified impurities F.Other detectable impurities (the following substances would, if present at a sufficient level, be detected by one or other of the tests in the monograph. They are limited by the general acceptance criterion for other/unspecified impurities and/or by the general monograph Substances for pharmaceutical use (2034). It is therefore not necessary to identify these impurities for demonstration of compliance. See also 5.10. Control of impurities in substances for pharmaceutical use): A, B, C, D, E, G, H.A. R = H: 2-(4-methoxyphenyl)-N,N-dimethylethanamine,B. R = CO-O-C2H5: ethyl(2RS)-3-(dimethylamino)-2-(4-methoxyphenyl)propanoate,C. R = H: 1-[(1RS)-2-amino-1-(4-methoxyphenyl)ethyl]cyclohexanol,D. R = CH3:1-[(1RS)-1-(4-methoxyphenyl)-2-(methylamino)ethyl]cyclohexanol,H. R = CH2-CH2-C6H4-p-OCH3:1-[(1RS)-1-(4-methoxyphenyl)-2-[[2-(4-methoxyphenyl)ethyl]amino]ethyl]cyclohexanol,E. (5RS)-5-(4-methoxyphenyl)-3-methyl-1-oxa-3-azaspiro[5.5]undecane,F.(2RS)-2-(cyclohex-1-enyl)-2-(4-methoxyphenyl)-N,N-dimethylethanamine,G. (2RS)-2-cyclohexyl-2-(4-methoxyphenyl)-N,N-dimethylethanamine. PhEurProlonged-release Venlafaxine CapsulesGeneral NoticesAction and useInhibition of 5HT and noradrenaline reuptake; antidepressant.Prolonged-release Venlafaxine Capsules from different manufacturers, whilst complying with the requirements of the monograph, are not interchangeable unless otherwise justified and authorised.DEFINITIONProlonged-release Venlafaxine Capsules contain Venlafaxine Hydrochloride. They are formulated so that the medicament is released over a period of several hours.PRODUCTIONA suitable dissolution test is carried out to demonstrate the appropriate release of Venlafaxine Hydrochloride. The dissolution profile reflects the performance which in turn is compatible with the dosage schedule recommended by the manufacturer.The capsules comply with the requirements stated under Capsules and with the following requirements.Content of venlafaxine, C17H27NO295.0 to 105.0% of the stated amount.IDENTIFICATIONShake a quantity of the powdered capsule contents containing the equivalent of 0.35 g of venlafaxine with 100 mL of a mixture of 30 volumes of cyclohexane and 70 volumes of dichloromethane for 30 minutes, filter the extract through anhydrous sodium sulfate and evaporate the filtrate to dryness. Wash the residue with a mixture of 30 volumes of cyclohexane and 70 volumes of dichloromethane, filter and dry the residue. The infrared absorption spectrum of the residue, Appendix II A, is concordant with the reference spectrum of venlafaxine hydrochloride (RS439).TESTSRelated substancesCarry out the method for liquid chromatography, Appendix III D, using the following solutions in the mobile phase A.(1) Mix with the aid of ultrasound, a quantity of the powdered capsule contents containing the equivalent of 200 mg of venlafaxine with 80 mL of a 2.4% v/v solution of orthophosphoric acid , shake for a further 30 minutes, cool, add sufficient water to produce 100 mL, mix and centrifuge; use the supernatant liquid.(2) Dilute 1 volume of solution (1) to 500 volumes.(3) 0.2% w/v of venlafaxine impurity standard BPCRS.(4) Dilute 25 volumes of solution (2) to 100 volumes. CHROMATOGRAPHIC CONDITIONS(a) Use a stainless steel column (25 cm × 4.6 mm) packed with octadecylsilyl silica gel for chromatography (5 µm) (Partisil ODS 3 is suitable).(b) Use gradient elution and the mobile phase described below.(c) Use a flow rate of 1 mL per minute.(d) Use an ambient column temperature.(e) Use a detection wavelength of 226 nm.(f) Inject 20 µL of each solution.MOBILE PHASEMobile phase A 1 volume of triethylamine, 20 volumes of acetonitrile and 80 volumes of water adjusted to pH 3.5 with orthophosphoric acid .Mobile phase B 1 volume of triethylamine, 50 volumes of acetonitrile and 50 volumes of water adjusted to pH 3.5 with orthophosphoric acid .Under the prescribed conditions, the retention time of venlafaxine is about 13 minutes.SYSTEM SUITABILITYThe test is not valid unless, in the chromatogram obtained with solution (3), the resolution factor between the peaks due to impurity D and venlafaxine is at least 1.5.LIMITSIn the chromatogram obtained with solution (1):the area of any peak corresponding to impurity D or impurity F is not greater than the area of the principal peak in the chromatogram obtained with solution (2) (0.2% of each);the area of any other secondary peak is not greater than the area of the principal peak in the chromatogram obtained with solution (2) (0.2%);the sum of the areas of all the secondary peaks is not greater than 2.5 times the area of the principal peak in the chromatogram obtained with solution (2) (0.5%).Disregard any peak with an area less than that of the principal peak in the chromatogram obtained with solution (4) (0.05%).ASSAYMix the contents of 20 capsules. Carry out the method for liquid chromatography, Appendix III D, using the following solutions in the mobile phase.(1) Shake a quantity of the capsule contents containing the equivalent of 175 mg of venlafaxine for 30 minutes with 50 mL of methanol , add sufficientmethanol to produce 100 mL, mix and filter. To 5 volumes of the filtrate add sufficient of the mobile phase to produce 100 volumes.(2) 0.01% w/v of venlafaxine hydrochloride BPCRS.(3) 0.01% w/v of venlafaxine impurity standard BPCRS.CHROMATOGRAPHIC CONDITIONS(a) Use a stainless steel column (15 cm × 4.6 mm) packed with octadecylsilyl silica gel for chromatography (5 µm) (Zorbax Rx C18 is suitable)(b) Use isocratic elution and the mobile phase described below.(c) Use a flow rate of 1 mL per minute.(d) Use an ambient column temperature.(e) Use a detection wavelength of 226 nm.(f) Inject 10 µL of each solution.MOBILE PHASE20 volumes of acetonitrile and 80 volumes of a 1% v/v solution of triethylamine previously adjusted to pH 3.0 with orthophosphoric acid .Under the prescribed conditions, the retention time of venlafaxine is about 3.5 minutes. If necessary adjust the acetonitrile content of the mobile phase.SYSTEM SUITABILITYThe test is not valid unless, in the chromatogram obtained with solution (3), the resolution factor between the peaks due to impurity D and venlafaxine is at least 1.0.DETERMINATION OF CONTENTCalculate the content of C17H27NO2 in the capsules using the declared content of C17H27NO2,HCl in venlafaxine hydrochloride BPCRS. Each mg ofC17H27NO2,HCl is equivalent to 0.884 mg of C17H27NO2.LABELLINGThe quantity of active ingredient is stated in terms of the equivalent amount of venlafaxine.IMPURITIESThe impurities limited by the requirements of this monograph include:D. 1-[(1RS)-1-(4-methoxyphenyl)-2-(methylamino)ethyl]cyclohexanol (European Pharmacopoeia impurity D);F. (2RS)-2-(cyclohex-1-enyl)-2-(4-methoxyphenyl)-N,N-dimethylethanamine (European Pharmacopoeia impurity F).Venlafaxine TabletsGeneral NoticesAction and useInhibition of 5HT and noradrenaline reuptake; antidepressant.DEFINITIONVenlafaxine Tablets contain Venlafaxine Hydrochloride.The tablets comply with the requirements stated under Tablets and with the following requirements.Content of venlafaxine, C17H27NO295.0 to 105.0% of the stated amount.IDENTIFICATIONShake a quantity of the powdered tablets containing the equivalent of 0.35 g of venlafaxine with 100 mL of a mixture of 30 volumes of cyclohexane and 70 volumes of dichloromethane for 30 minutes, filter and evaporate the filtrate to dryness. Wash the residue with a mixture of 30 volumes of cyclohexane and 70 volumes of dichloromethane, filter and dry the residue. The i nfrared absorption spectrum of the residue, Appendix II A, is concordant with the reference spectrum of venlafaxine hydrochloride (RS 439).TESTSDissolutionComply with the dissolution test for tablets and capsules, Appendix XII B1. TEST CONDITIONS(a) Use Apparatus 2, rotating the paddle at 50 revolutions per minute.(b) Use 900 mL of water, at a temperature of 37°, as the medium. PROCEDURE(1) After 45 minutes withdraw a sample of the medium and measure the absorbance of the filtered sample, suitably diluted with the dissolution mediumif necessary, to give a solution expected to contain the equivalent of about0.0025% w/v of venlafaxine, at the maximum at 274 nm, Appendix II B using water in the reference cell.(2) Measure the absorbance of a 0.0025% w/v solution of venlafaxinehydrochloride BPCRS using water in the reference cell. DETERMINATION OF CONTENTCalculate the total content of venlafaxine, C17H27NO2, in the medium from the absorbances obtained and using the declared content of C17H27NO2,HCl in venlafaxinehydrochloride BPCRS. Each mg of C17H27NO2,HCl is equivalent to 0.884 mg of C17H27NO2.LIMITSThe amount of venlafaxine released is not less than 75% (Q) of the stated amount.Related substancesCarry out the method for liquid chromatography, Appendix III D, using the following solutions in the mobile phase A.(1) Mix with the aid of ultrasound a quantity of the powdered tablets containing the equivalent of 200 mg of venlafaxine with 80 mL of a 2.4% v/v solution of orthophosphoric acid , shake for a further 30 minutes, cool, add sufficient water to produce 100 mL, mix and centrifuge; use the supernatant liquid.(2) Dilute 1 volume of solution (1) to 500 volumes.(3) 0.2% w/v of venlafaxine impurity standard BPCRS.(4) Dilute 25 volumes of solution (2) to 100 volumes. CHROMATOGRAPHIC CONDITIONS(a) Use a stainless steel column (25 cm × 4.6 mm) packed with octadecylsilyl silica gel for chromatography (5 µm) (Partisil ODS 3 is suitable).(b) Use gradient elution and the mobile phase described below.(c) Use a flow rate of 1 mL per minute.(d) Use an ambient column temperature.(e) Use a detection wavelength of 226 nm.(f) Inject 20 µL of each solution.MOBILE PHASEMobile phase A 1 volume of triethylamine, 20 volumes of acetonitrile and 80 volumes of water adjusted to pH 3.5 with orthophosphoric acid .Mobile phase B 1 volume of triethylamine, 50 volumes of acetonitrile and 50 volumes of water adjusted to pH 3.5 with orthophosphoric acid .Under the prescribed conditions, the retention time of venlafaxine is about 13 minutes.SYSTEM SUITABILITYThe test is not valid unless, in the chromatogram obtained with solution (3), the resolution factor between the peaks due to impurity D and venlafaxine is at least 1.5.LIMITSIn the chromatogram obtained with solution (1):the area of any peak corresponding to impurity D or impurity F is not greater than the area of the principal peak in the chromatogram obtained with solution (2) (0.2% of each);the area of any other secondary peak is not greater than the area of the principal peak in the chromatogram obtained with solution (2) (0.2%);the sum of the areas of all the secondary peaks is not greater than 2.5 times the area of the principal peak in the chromatogram obtained with solution (2) (0.5%).Disregard any peak with an area less than that of the principal peak in the chromatogram obtained with solution (4) (0.05%).ASSAYWeigh and powder 20 tablets. Carry out the method for liquid chromatography, Appendix III D, using the following solutions in the mobile phase.(1) Mix a quantity of the powdered tablets containing the equivalent of 50 mg of venlafaxine with 200 mL of a 0.2% v/v solution of orthophosphoric acid for 15 minutes with the aid of ultrasound and shake vigorously. Mix for a further 15 minutes with the aid of ultrasound, cool, add sufficient of a 0.2% v/v solution of orthophosphoricacid to produce 250 mL, mix and centrifuge. To 2 volumes of the supernatant liquid add sufficient of the mobile phase to produce 5 volumes.(2) 0.009% w/v of venlafaxine hydrochloride BPCRS.(3) 0.01% w/v of venlafaxine impurity standard BPCRS. CHROMATOGRAPHIC CONDITIONS(a) Use a stainless steel column (15 cm × 4.6 mm) packed with octylsilyl silica gel for chromatography (5 µm) (Zorbax C8 is suitable)(b) Use isocratic elution and the mobile phase described below.(c) Use a flow rate of 1 mL per minute.(d) Use an ambient column temperature.(e) Use a detection wavelength of 226 nm.(f) Inject 20 µL of each solution.MOBILE PHASE25 volumes of acetonitrile and 75 volumes of a 1% v/v solution of triethylamine,previously adjusted to pH 3.0 with orthophosphoric acid .Under the prescribed conditions, the retention time of venlafaxine is about 5 minutes, if necessary adjust the acetonitrile content of the mobile phase. SYSTEM SUITABILITYThe test is not valid unless, in the chromatogram obtained with solution (3), the resolution factor between the peaks due to impurity D and venlafaxine is at least 1.0.DETERMINATION OF CONTENTCalculate the content of C17H27NO2 in the tablets using the declared content of C17H27NO2,HCl in venlafaxine hydrochloride BPCRS. Each mg ofC17H27NO2,HCl is equivalent to 0.884 mg of C17H27NO2.LABELLINGThe quantity of active ingredient is stated in terms of the equivalent amount of venlafaxine.IMPURITIESThe impurities limited by the requirements of this monograph include:D. 1-[(1RS)-1-(4-methoxyphenyl)-2-(methylamino)ethyl]cyclohexanol (European Pharmacopoeia impurity D);F. (2RS)-2-(cyclohex-1-enyl)-2-(4-methoxyphenyl)-N,N-dimethylethanamine (European Pharmacopoeia impurity F).Prolonged-release Venlafaxine TabletsGeneral NoticesAction and useInhibition of 5HT and noradrenaline reuptake; antidepressant.Prolonged-release Venlafaxine Tablets from different manufacturers, whilst complying with the requirements of the monograph, are not interchangeable unless otherwise justified and authorised.DEFINITIONProlonged-release Venlafaxine Tablets contain Venlafaxine Hydrochloride. They are formulated so that the medicament is released over a period of several hours.PRODUCTIONA suitable dissolution test is carried out to demonstrate the appropriate release of Venlafaxine Hydrochloride. The dissolution profile reflects the performance which in turn is compatible with the dosage schedule recommended by the manufacturer.The tablets comply with the requirements stated under Tablets and with the following requirements.Content of venlafaxine, C17H27NO295.0 to 105.0% of the stated amount.IDENTIFICATIONShake a quantity of the powdered tablets containing the equivalent of 0.35 g of venlafaxine with 100 mL of a mixture of 30 volumes of cyclohexane and 70 volumes of dichloromethane for 30 minutes, filter the extract through anhydrous sodium sulfate and evaporate the filtrate to dryness. Wash the residue with a mixture of 30 volumes of cyclohexane and 70 volumes of dichloromethane, filter and dry the residue. The infrared absorption spectrum of the residue, Appendix II A, is concordant with the reference spectrum of venlafaxine hydrochloride (RS439).TESTSRelated substancesCarry out the method for liquid chromatography, Appendix III D, using the following solutions.(1) Mix, with the aid of ultrasound, a quantity of the powdered tablets containing the equivalent of 200 mg of venlafaxine with 80 mL of a 2.4% v/v solution of orthophosphoric acid , shake for a further 30 minutes, cool, add sufficient water to produce 100 mL, mix and centrifuge; use the supernatant liquid.(2) Dilute 1 volume of solution (1) to 100 volumes with mobile phase A, further dilute 1 volume of this solution to 5 volumes with mobile phase A.(3) 0.2% w/v of venlafaxine impurity standard BPCRS in mobile phase A.(4) Dilute 25 volumes of solution (2) to 100 volumes with mobile phase A. CHROMATOGRAPHIC CONDITIONS(a) Use a stainless steel column (25 cm × 4.6 mm) packed with octadecylsilyl silica gel for chromatography (5 µm) (Partisil ODS 3 is suitable).(b) Use gradient elution and the mobile phase described below.(c) Use a flow rate of 1 mL per minute.(d) Use an ambient column temperature.(e) Use a detection wavelength of 226 nm.(f) Inject 20 µL of each solution.MOBILE PHASEMobile phase A 1 volume of triethylamine, 20 volumes of acetonitrile and 80 volumes of water previously adjusted to pH 3.5 with orthophosphoric acid . Mobile phase B 1 volume of triethylamine, 50 volumes of acetonitrile and 50 volumes of water previously adjusted to pH 3.5 with orthophosphoric acid .When the chromatograms are recorded under the prescribed conditions, the retention time of venlafaxine is about 13 minutes. Retention times relative to venlafaxine are: impurity D, about 0.8; impurity F, about 1.7.SYSTEM SUITABILITYThe test is not valid unless, in the chromatogram obtained with solution (3), the resolution factor between the peaks due to impurity D and venlafaxine is at least 1.5.LIMITSIn the chromatogram obtained with solution (1):the area of any peak corresponding to impurity D or impurity F is not greater than the area of the principal peak in the chromatogram obtained with solution (2) (0.2% of each);the area of any other secondary peak is not greater than the area of the principal peak in the chromatogram obtained with solution (2) (0.2%);the sum of the areas of all the secondary peaks is not greater than 2.5 times the area of the principal peak in the chromatogram obtained with solution (2) (0.5%).Disregard any peak with an area less than that of the principal peak in the chromatogram obtained with solution (4) (0.05%).ASSAYWeigh and powder 20 tablets. Carry out the method for liquid chromatography, Appendix III D, using the following solutions in the mobile phase.(1) Shake a quantity of the powdered tablets containing the equivalent of 175 mg of venlafaxine for 30 minutes with 50 mL of methanol , add sufficient methanol to produce 100 mL, mix and filter. Dilute 1 volume of the filtrate to 20 volumes with mobile phase.(2) 0.01% w/v of venlafaxine hydrochloride BPCRS.(3) 0.01% w/v of venlafaxine impurity standard BPCRS.CHROMATOGRAPHIC CONDITIONS(a) Use a stainless steel column (15 cm × 4.6 mm) packed with octadecylsilyl silica gel for chromatography (5 µm) (Zorbax Rx C18 is suitable)(b) Use isocratic elution and the mobile phase described below.(c) Use a flow rate of 1 mL per minute.(d) Use an ambient column temperature.(e) Use a detection wavelength of 226 nm.(f) Inject 10 µL of each solution.MOBILE PHASE20 volumes of acetonitrile and 80 volumes of a 1% v/v solution of triethylamine previously adjusted to pH 3.0 with orthophosphoric acid .Under the prescribed conditions, the retention time of venlafaxine is about 3.5 minutes. If necessary, adjust the acetonitrile content of the mobile phase.SYSTEM SUITABILITYThe test is not valid unless, in the chromatogram obtained with solution (3), the resolution factor between the peaks due to impurity D and venlafaxine is at least 1.0.DETERMINATION OF CONTENTCalculate the content of C17H27NO2 in the tablets using the declared content of C17H27NO2,HCl in venlafaxine hydrochloride BPCRS. Each mg ofC17H27NO2,HCl is equivalent to 0.884 mg of C17H27NO2.LABELLINGThe quantity of active ingredient is stated in terms of the equivalent amount of venlafaxine.IMPURITIESThe impurities limited by the requirements of this monograph include:D. 1-[(1RS)-1-(4-methoxyphenyl)-2-(methylamino)ethyl]cyclohexanol (European Pharmacopoeia impurity D);F. (2RS)-2-(cyclohex-1-enyl)-2-(4-methoxyphenyl)-N,N-dimethylethanamine (European Pharmacopoeia impurity F).。
文拉法辛

化学信息 CA登录号 登录号99300-78-4 登录号 分子式C17H28ClNO2 分子式 化学名Cyclohexanol, 1-[2化学名 (dimethylamino)-1-(4methoxyphenyl)ethyl]-, hydrochloride [CAS] • 结构式 • • • •
• • • • • • • •
知识产权状况 专利优先权国家专利号专利申请日英国;UKGB22277431989年02月 专利优先权国家专利号专利申请日 01日 行政保护 药品名称申请人状态PDF链接 链接Efexor缓释胶囊(venlafaxine 药品名称申请人状态 链接 hydrochloride)AHP制药有限公司保护相关文档 基本药物 药品名称剂型版本文拉法辛(盐酸盐)胶囊剂、缓释胶囊剂2004 药品名称剂型版本 医保情况 药品名称剂型医保类别版本文拉法辛口服常释剂型乙类2004文拉法辛 药品名称剂型医保类别版本 口服常释剂型乙2009版文拉法辛缓释控释剂型乙类2004文拉法辛缓 释控释剂型乙2009版
药品概况 药品名称 英文通用名中文通用名状态状态进程venlafaxine 英文通用名中文通用名状态状态进程 hydrochloride盐酸文拉法辛上市上市 异名中文名:文拉法辛,盐酸文拉法辛,盐酸文拉法辛 异名 胶囊,盐酸文拉法辛胶囊(原名为盐酸万拉法新胶囊) 英文名:venlafexine,Dobupal Retard,Wy-45655,Wy45030,Trevilor,Dobupal,Effexor,Efectin,Efexor,Wy45651,Efexor Depot,venlafaxine hydrochloride,venlafaxine
• 药品标准 • 药品名称标准号出处文拉法辛WS1-(X-006)药品名称标准号出处 2002Z新药转正标准(第28册)盐酸文拉法辛胶囊 WS1-(X-007)-2002Z新药转正标准(第28册) • 国外企业开发和许可信息 • 原创企业国家进程 原创企业国家进程Pfizer美国;USA上市 • 许可企业国家进程 许可企业国家进程Almirall西班牙;Spain上市 • 治疗信息 • 治疗类别代码治疗类别进程 治疗类别代码治疗类别进程P04A抗焦虑药上市 P01A抗抑郁药上市
【药品名】文拉法辛
【药品名】文拉法辛【英文名】Venlafaxine【别名】万法拉新;文拉法新;博乐欣;万拉法辛;凡拉克辛;顽发克星;Effexor;WY-45030【剂型】片剂:25mg,37.5mg,50mg,75mg,100mg。
【药理作用】本品为苯乙胺衍生物,对5-HT和去甲肾上腺素的重摄取具有抑制作用,对多巴胺的再摄取也有微弱的抑制作用。
对毒蕈碱、组胺能或α-肾上腺素能受体几乎没有亲和力。
【药动学】口服后快速被吸收。
在肝内主要广泛首过代谢物为活性代谢物O-去甲文拉法辛。
原药和代谢物的血药峰值分别于2h和4h达到。
原药和代谢物的蛋白结合率很低。
两者的平均消除t约为5和11h。
主要以代谢物随尿排出,见于粪便中者仅2%。
【适应症】抗抑郁症。
【禁忌症】对本品过敏者、哺乳者禁用。
【注意事项】1.肝肾功能不全、不稳定型心绞痛或有心梗病史的患者慎用。
2.有轻度躁狂、躁狂症和癫痫病史者慎用。
【不良反应】1.最常见者有恶心、头痛、头晕、失眠、嗜睡、口干、便秘、虚弱、出汗和神经过敏。
2.偶见直立性低血压。
3.其他还有厌食、消化不良、腹痛、焦虑、性功能障碍、视力障碍、血管扩张、呕吐、震颤、感觉异常、寒战、心悸、体重增加、激动和皮疹。
还有发生惊厥的报道。
4.肝酶可见可逆性升高,血胆固醇水平改变。
5.有些患者出现与剂量有关的血压升高。
轻躁狂和躁狂症偶有发生。
6.可能出现低钠血症,尤其是老年人。
7.超剂量的表现有嗜睡、昏睡、心电图改变、心律失常和癫痫发生。
【用法用量】成人:开始剂量每天口服75mg,2~3次分服,与食物同进,如必要,几周后可加量至每天150mg。
严重而住院者,开始给予150mg,如必要,每2~4天增加75mg,最大剂量可达375mg;接着,剂量必须逐渐减少。
【药物相互作用】西咪替丁可抑制本品原药的代谢,但对其活性代谢物无作用,因此,当本品合用西咪替丁时,对老年患者、肝功能不全者或有高血压史者应进行临床监测。
【专家点评】抗抑郁作用较其他抗抑郁剂出现的快、副作用较丙咪嗪小,而效果优于丙咪嗪、其疗效与曲唑酮相当。
文拉法辛的功能主治
文拉法辛的功能主治一、什么是文拉法辛文拉法辛(Vimlafaxine)是一种常用的抗抑郁药物,属于选择性血清素和去甲肾上腺素再摄取抑制剂(SNRI)。
它通过抑制神经递质的再摄取来提高血浆中的血清素和去甲肾上腺素水平,以达到调节情绪和改善抑郁症状的作用。
二、文拉法辛的功能文拉法辛具有以下功能:1.抗抑郁作用:文拉法辛通过调节血浆中的血清素和去甲肾上腺素水平,可以改善抑郁症状,提高患者的情绪状态。
2.缓解焦虑:文拉法辛在治疗抑郁症的同时,也可以缓解患者的焦虑症状,减轻紧张和不安感。
3.提升注意力和警觉性:文拉法辛能够改善患者的注意力和警觉性,使其更加专注和集中注意力。
4.改善睡眠质量:文拉法辛可以调节患者的睡眠模式,改善睡眠质量,缓解失眠和嗜睡等问题。
5.减少疼痛感知:文拉法辛在一些情况下可以用作镇痛剂,减轻患者的疼痛感知。
三、文拉法辛的主治疾病文拉法辛主要用于以下疾病的治疗:1.抑郁症:文拉法辛是一种常用的抗抑郁药物,可以改善抑郁症状,提高患者的情绪状态。
2.焦虑症:文拉法辛不仅可以治疗抑郁症,还可以缓解焦虑症状,减轻紧张和不安感。
3.适应障碍:文拉法辛也可以用于治疗适应障碍,帮助患者更好地适应环境和情境的改变。
4.失眠症:由于文拉法辛可以改善睡眠质量,因此在治疗失眠症方面也有一定的作用。
5.神经性疼痛:文拉法辛可以减少疼痛感知,因此在神经性疼痛的治疗中也有一定的应用价值。
四、文拉法辛的用法和注意事项•用法:通常建议口服用药,一般每日一次,剂量根据患者的具体情况进行调整。
•注意事项:–在使用文拉法辛时,应该密切关注患者的心理状态和体征变化,及时与医生沟通。
–不得随意更改剂量或停用文拉法辛,以免影响疗效或产生不良反应。
–在服用文拉法辛期间,避免同时使用其他药物,尤其是与其相互作用的药物,以免出现药物不良反应。
–孕妇、哺乳期妇女、儿童等特殊人群在使用文拉法辛之前应咨询医生。
五、副作用和禁忌症1.常见副作用包括恶心、呕吐、乏力、失眠、头痛和食欲减退等,多数患者可以适应并耐受这些副作用。
【上市新药】 抗抑郁药 琥珀酸去甲文拉法辛(desvenlafaxine succinate)
本 品 用 于 MDD 的 初 始 治 疗 , 推 荐 剂 量 为 一 日 1 次 5 , 与 或 不 与食 物 同服 。应 在 每 天 同 一 时 间服 用 。 片剂 0mg 应 随 液 体 整 片 吞 咽 ,不 能 分 开 、压 碎 、咀 嚼 或 溶 解 。 轻 度 肾 损 害 患 者 无 需 调 整 起 始 剂 量 ; 中度 肾损 害 患 者 , 推 荐 剂量 为一 日 1 5 :严 重 肾损 害或 终 末 期 肾 病 患 者 , 次 0 mg
【 市新药 】 上
抗抑 郁 药 琥 珀 酸 去 甲 文 拉 法 辛 (evnaa i ciae d se l xn s c t) f eu n
良反 应 的停 药 率 为 8 %。 导 致 停 药 的 最 常 见 不 良反 应 有 恶 . 7 心 、头 晕 、头 痛 和 呕 吐 。 7 注 意 事 项 对 本 品 、盐 酸 文 拉 法 辛 或 任 一 组分 过 敏 者 禁 用 。
■
譬
g
9
厶
本 品 为 选 择 性 5 羟 色 胺 和 去 甲肾 上 腺 素 再 摄 取 抑 制 剂 .
(NR ) S I ,适 用 于 MD 的治 疗 。 D
4 药 理
本 品 是 一种 强效 S / NR ,其 抗抑 郁 效 果 与 文 拉 法 辛 相 似 。
在 一 日 10~ 6 0mg的剂 量 范 围 内 ,本 品 的 药 动 学 呈 0 0
( 责任 编辑 :赵绪 韬 )
中 根 据 临 床 总 体 印象 . 善 量 表 ( G . 改 C I )判 断 的症 状 改 善情 I
盐酸文拉法辛胶囊
盐酸文拉法辛胶囊【药品名称】通用名称:盐酸文拉法辛胶囊英文名称:Venlafaxine Hydrochloride Capsules【成份】盐酸文拉法辛。
分子式:C17H27NO2·HCl分子量:313.87【适应症】本品适用于各种类型抑郁症,包括伴有焦虑的抑郁症,及广泛性焦虑症。
【用法用量】起始剂量为75mg/日,分两次或三次,进餐时服用。
根据病情和耐受性可以逐渐增加剂量,一般情况最高剂量为225mg/日,分三次口服。
增加的剂量达75mg/天,至少应间隔4天。
对于严重的抑郁症患者,可增加到375mg/日。
【不良反应】通常在治疗早期发生,部分存在剂量相关性,常见不良反应有恶心、呕吐、头痛、虚弱、出汗、嗜睡、失眠、头晕、神经质、口干、焦虑、厌食、体重下降、皮疹、男性射精异常或阳萎。
较少发生的不良反应有心动过速、血压升高及肾功能异常、血清胆固醇轻度升高、视力模糊、可逆性骨髓抑制。
【禁忌】对本品过敏者及正在服用单胺氧化酶抑制剂的患者禁用。
【注意事项】1.有躁狂史和癫痫的患者应慎用本品。
癫痫发作应停用本品。
2.有心脏病、高血压及甲状腺疾病、血液病患者应慎用本品。
3.有中等肝硬化的患者,应降低50%的剂量,有轻度到中度肾损害的病人,每日剂量降低25%。
4.18岁以下及老年患者服用本品应小心。
5.目前尚无有关和电休克联合治疗的经验。
6.用药期间避免饮酒。
7.停药时应逐渐减小剂量,已应用本品6周或更长时间,应在两周内逐渐减量。
8.妊娠和哺乳期:动物研究表明,本品无任何至畸性,也无胚胎毒性,但妊娠期服用本品的安全性尚未确定。
因此妊娠期或哺乳期妇女不宜服用,除非医生认为利大于弊时方可使用。
9.驾驶/操纵机器:临床证明,服用本品,对认知功能或精神活动没有影响,然而与所有精神类药物一样,病人在驾车或操纵机器时,小心谨慎。
10.药物相互作用:本品与单胺氧化酶抑制剂合用将产生严重的甚至是致命的副作用。
文拉法辛

文拉法辛概述文拉法辛(Venlafaxine)为苯乙胺衍生物,是二环类非典型抗抑郁药。
本品及其活性代谢物O-去甲基文法拉辛(ODV)能有效低拮抗5-HT和NA的再摄取,对DA的再摄取也有一定的作用,具有抗抑郁作用。
镇静作用较弱。
口服吸收良好,进食不影响药物的吸收。
在肝脏内广泛代谢,主要代谢产物是ODV,并主要通过肾脏排泄,亦可从乳汁中泌出。
二适应证适用于各种抑郁症和广泛性焦虑症。
三临床应用口服:开始25毫克/次,2~3次/日,逐渐增至75~225毫克/日,分2~3次服用。
缓释胶囊应按日剂量在固定时间与食物一起每日一次服用。
增加剂量的间隔不少于4天,每次增加75毫克/日。
轻中度肾功能损伤患者,每天给药总量降低25%~50%。
轻中度肝损伤者,每日总剂量为常规用药剂量的一半或不足一半,需根据患者实际情况个体化用药。
四不良反应不良反应少。
可有恶心、嗜睡、发汗、眩晕、性功能障碍、高血压、焦虑、口干、头昏、便秘等。
多在治疗初始阶段发生,随着治疗的进行,这些症状逐渐减轻。
五注意事项肝肾功能不全、心脏病、高血压、血液病、青光眼、甲状腺功能亢进或低下、双相情感障碍、有癫痫病史者慎用。
儿童、老年人、孕妇、哺乳期妇女慎用。
大剂量时可能诱发癫痫。
突然停药可有撤药综合征,如失眠、焦虑、恶心、出汗、震颤、眩晕或感觉异常等。
应逐渐减量而不是突然停药。
如果使用文拉法辛超过6周,建议逐渐减量时间最少要多于两周。
对于严重抑郁状态患者,用药期间应密切观察病情。
用药期间驾驶机动车或操纵机器患者应谨慎。
六用药禁忌对本药过敏者禁用。
七药物相互作用1.与5-HT活性药物(TCAs、SSRIs、SNRIs、利奈唑胺、锂剂、圣约翰草、色氨酸、曲坦类药物、右苯丙胺、芬佛拉明)合用,会引起5-HT综合征,故慎与这些药物合用。
2.与三氟拉嗪等抗精神病药合用可能会导致神经恶性综合征发生。
与氯氮平、右美沙芬合用,均会相互作用,导致对方血药浓度增加,而出现不良反应。
盐酸文法拉辛缓释片(博乐欣)说明书

核准日期:2007年12月11日修改日期:2008年03月14日2009年06月19日盐酸文拉法辛缓释片说明书请仔细阅读说明书并在医师指导下使用警示语自杀倾向和抗抑郁药物对抑郁症(MDD)和其它精神障碍的短期临床试验结果显示,与安慰剂相比,抗抑郁药物增加了儿童、青少年和青年(<24岁)患者自杀的想法和实施自杀行为(自杀倾向)的风险。
任何人如果考虑将盐酸文拉法辛缓释片或其它抗抑郁药物用于儿童、青少年或青年(<24岁),都必须在其风险和临川需求之间进行权衡。
短期的临床试验没有显示出,与安慰剂相比年龄大于24岁的成年人使用抗抑郁药物会增加自杀倾向的风险;而在年龄65岁及以上的成年人中,使用抗抑郁药物后,自杀倾向的风险有所降低。
抑郁和某些精神障碍本身与自杀风险的增加有关,必须密切观察所有年龄患者使用抗抑郁药物治疗开始后的临床症状的恶化、自杀倾向、行为的异常变化。
应建议家属和看护者必须密切观察并与医生进行沟通。
盐酸文拉法辛缓释片为被批准用于儿童患者(见[注意事项])-警告,临床症状的恶化和自杀风险,[注意事项]-患者用药信息,和[儿童用药]。
【药品名称】通用名称:盐酸文拉法辛缓释片英文名称:Venlafaxine Hydrochloride Sustained-Release Tablets汉语拼音Yansuan Wenlafaxin Huanshi Pian【成分】主要组成成分盐酸文拉法辛。
化学名称:(±)-1-[2-(二甲胺基)-1-(4-甲氧苯基)乙基]-环己醇盐酸盐。
化学结构式:分子式:C17H27NO2·HCl分子量:313.87【性状】本品为白色或类白色片剂,表面有一小孔,除去包衣后显白色或类白色。
【适应症】本品适用于各种类型抑郁症(包括伴有焦虑的抑郁症)及广泛性焦虑症。
【规格】(1)37.5mg;(2)75mg(以文拉法辛计)【用法用量】盐酸文拉法辛缓释片应该在早晨或晚间一个相对固定时间和食物同时服用,每日一次,用水送服。
文拉法辛——抗抑郁药物

一、化学结构
文拉法辛为苯乙胺衍生物, 其化学结构如图所示,是二 环类非典型抗抑郁药。 文拉法辛具有NE和5-HT双重 摄取抑制作用,有普通型制 剂和缓释型制剂2种。
二、药理作用
本品为苯乙胺衍生物,是二环类非典型抗抑郁药,文拉法辛具有NE和 5-HT双重摄取抑制作用,还有轻度DA再摄取抑制作用,3种递质的 再摄取抑制作用与药物剂量相关
五、最新研究
该药物的最新进展:文拉法辛联合使用治疗脑卒中抑郁患者 参考文献: [1]朱慧敏.文拉法辛联合心理治疗对脑卒中后抑郁患者抑郁症状的改善[J].
心理月刊,2021,16(06):72-73. [2]陶珍,郭洪伟,高丽,赵磊,程明,宋景贵.乌灵胶囊联合文拉法辛配合针灸治
疗脑卒中后抑郁的疗效观察[J].中国医院用药评价与分析,2020,20(06):678681. [3]谢顺利,王洪.渝东南地区文拉法辛治疗脑卒中后抑郁的临床疗效分析[J]. 世界复合医学,2020,6(05):168-170.
低剂量时以DA为主,兼有轻度的5-HT作用,中等剂量以5-HT和NE作用 为主,高剂量时则对NE的再摄取抑制作用最强,具有抗抑郁作用
镇静作用较弱
三、适应焦虑障碍 适用于强迫症和慢性疼痛 起效较快是其特点,治疗剂量疗效与TCAs、氟西汀的疗效相当,对重
国家卫生和计划生育委员会“十三五”规划教材 全国高等医药教材建设研究会“十三五”规划教材 全国高等学校教材
供精神医学等专业用
主 编 刘吉成 艾静 副主编 吕路线 王传跃 时杰
现不良反应 本品减少氟哌啶醇代谢,两者合用应谨慎 与酒精合用可能增加中枢神经系统抑制 酮康唑、西咪替丁、利托那韦等可减少本品的代谢,增加本品的毒性。 本品是CYP2D6的作用底物与弱抑制剂,与通过该酶代谢的TCAs药物合用时,
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
【中文名称】:文拉法辛[1]【拼音名】:Wenlafaxin【英文名称】:Venlafaxine【英文别名】:(RS)-1-[2-(dimethylamino)-1-(4-methoxyphenyl)ethyl]cyclohexanol hydrochloride; Venlafaxine HCl; EFFEXOR; D,L-VENLAFAXINE; D,L-VENLAFAXINE, HYDROCHLORIDE; 1-[2-(DIMETHYLAMINO)-1-(4-METHOXYPHENYL)ETHYL]CYCLOHEXANOL, HCL; 1-[2-(DIMETHYLAMINO)-1-(4-METHOXYPHENYL)ETHYL]CYCLOHEXANOL HYDROCHLORIDE; (+/-)-1-(alpha-((dimethylamino)methyl)-p-methoxybenzyl)cyclohexanol hydrochloride; AKOS 92111【所属类别】:抗抑郁药【别名】R/S)-1-[2-(二甲胺)-1-(4-甲氧苯基)乙基]环己醇盐酸盐;盐酸文拉法新;盐酸维拉法辛;文拉法辛盐酸盐【外文名】Venlafaxine HCl,Efexor XR2用法【适应症】各种类型抑郁症,包括伴有焦虑的抑郁症及广泛性焦虑症。
【不良反应】常见的不良反应为:胃肠道不适(恶心、口干、厌食、便秘和呕吐)、中枢神经系统异常(眩晕、嗜睡、梦境怪异、失眠和紧张)、视觉异常、打哈欠、出汗和性功能异常(阳痿、射精异常、性欲降低)。
偶见不良反应为:无力、气胀、震颤、激动、腹泻、鼻炎。
不良反应多在治疗的初始阶段发生,随着治疗的进行,这些症状逐渐减轻。
文拉法辛没有明显的药物依赖倾向。
【用法用量】起始推荐剂量为75 mg/天,每天1次。
如有必要,可递增剂量至最大为225 mg/天(间隔时间不少于4天。
每次增加75 mg/ 天)。
肝功能损伤病人的起始剂量降低50%,个别病人需进行剂量个体化。
肾功能损伤病人,每天给药总量降低25- 50%。
老年病人按个体化给药,增加用药剂量时应格外注意。
如果用文拉法辛治疗6周以上,建议逐渐停药,所需的时间不少于2周。
用药须知该品缓释胶囊应在每天相同的时间与食物同时服用,每天1次,用水送服。
注意不得将其弄碎、嚼碎后服用或化在水中服用。
3注意事项编辑【注意事项】1.在服用本品过程中不宜饮酒。
2.与西米替丁合用可使文拉法辛清除率降低,因此对老年病人、高血压患者和肝功能障碍的病人应慎用。
3.与氟哌啶醇合用可增加氟哌啶醇的血药浓度,最大血药浓度可增加88%,但清除半衰期不变。
4.本品对细胞色素P450-IID6、P450-3A4二酶的药物同时使用时,应慎用.5.本品与丙咪嗪合用可使去甲丙咪嗪的血药峰浓度和血药谷浓度增加35%。
6.本品与中枢神经系统活性药物联合应用时,应慎用。
7.有报道与氯氮平合用出现氯氮平血药浓度升高的短暂性不良反应,如癫痫。
8.据报道,接受华法林治疗的病人服用文拉法辛后出现凝血酶原时间、部分促凝血酶原激酶时间或INR增大。
9..对该品过敏及正在服用单胺氧化酶抑制剂的患者禁用该品。
某些病人服用文拉法辛后会出现血压持续高,对服用该品的病人,应定期监测血压。
若出现血压持续升高,应减小剂量或停药。
【规格】75 mg本药为桃色胶囊,囊体上印有"75",囊帽上印有"W"。
150 mg本药为深桔色胶囊,囊体上印有"150",囊帽上印有"W"。
【不良反应防治】⑴对该品过敏者禁用。
闭角型青光眼、癫痫患者慎用。
⑵严重心脏疾患、高血压、甲状腺疾病、血液病患者慎用。
⑶肝肾功能不全者慎用或减少用量。
⑷用药过程中应监测血压,血压升高应减量或停药。
⑸停用时应逐渐减少剂量,已应用该品6周或更长时间者,应在2周内逐渐减量。
⑹患者出现有转向躁狂发作倾向时应立即停药。
⑺用药期间不宜驾驶车辆、操作机械或高空作业。
4药理作用编辑抗抑郁作用该药主要通过同时阻断NE和5-HT的再摄取,升高NE和5-HT浓度而发挥双重抗抑郁作用,对多巴胺(DA)的重摄取,仅有轻微的抑制作用。
对M胆碱受体,肾上腺素α1、α2、β受体,组胺H1受体几乎无亲和力。
其活性代谢产物0-去甲基文拉法辛亦可抑制5-HT和NE 的重摄取,活性比原形药低。
有研究表明,该品小剂量时主要抑制5-HT的再摄取,大剂量时对5-HT和NE的再摄取均有抑制作用。
该药对5-HT再摄取的抑制作用弱于选择性5-HT重摄取抑制剂(SSRI);对NE再摄取的抑制作用也弱于某些三环类抗抑郁药(TCA)或选择性NE再摄取抑制药。
但该品单次或多次给药均可降低由异丙肾上腺素刺激大鼠松果体产生的cAMP浓度,引起肾上腺素β受体的快速下调,而TCA则需长期给药才有此效应。
现认为文拉法辛对肾上腺素β受体的快速下调作用与其起效快有关。
有研究表明,此药可使正常人注意力集中,增强记忆力,加快反应速度,改善智力,且对主要驾驶参数(横向偏离水平)及一系列精神运动均无明显影响,但影响警觉。
对于抑郁病人,一般用药1~2周后(也有4天内)即可出现明显抗抑郁作用,比TCA起效快。
对睡眠的影响文拉法辛该药可使总的睡眠时间减少,觉醒时间增加,总的快波睡眠时间(REM)缩短。
阻断抑郁病人REM睡眠可产生缓慢而持久的症状改善,故此药对睡眠的影响可能参与抗抑郁作用。
镇痛作用腹腔注射此药可提高小鼠的痛阈,半数有效量(ED50)为46.7mg/kg。
这种作用可被纳洛酮(naloxone)明显抑制,但不被βFNA或naloxonazine所抑制。
肾上腺素α2受体阻断药育亨宾(yohimbine)能削弱其镇痛作用,而肾上腺素α2受体激动剂可乐定(clonidine)可增强其作用。
提示阿片κ、δ受体,肾上腺素α2受体与这种作用有关。
但其临床镇痛作用仍待研究。
对体温的影响一般认为文拉法辛不升高正常体温,但能拮抗利血平(reserpine)和阿扑吗啡(apomorphine)对小鼠的降温作用。
但最近有文拉法辛治疗引起情感性精神障碍患者发热感的报道,并认为文拉法辛在50~75mg/d的剂量时仍有拟NE能作用,故可增加糖原及脂肪的分解,从而增强代谢引起全身发热感。
心血管系统有报道称该药可使血压轻度升高,特别是舒张压,血压的轻度上升可能就是因为文拉法辛引起的,这与文拉法辛有很大的关系。
5临床应用编辑治疗抑郁症多项比较文拉法辛疗效的研究均认为该品治疗抑郁症疗效显著。
Thase收集了关于文拉法辛与5-HT再摄取抑制剂(SSRIs)比较的8项双盲对照研究,其中4项研究还与安慰剂进行对照[5]。
8项研究共有2045例研究对象,其中服用文拉法辛者85l例,SSRIs者748例,安慰药者446例。
经分析后得出文拉法辛组的痊愈率高于SSRIs组,痊愈出现更快,且该结论与患者年龄性别无关。
金卫东等对16项对照研究的Meta分析亦得出相似的结论。
与TCA相比,因文拉法辛较叔胺类三环抗抑郁药的不良反应少,故可耐受剂量范围更大,缓解率亦更高。
此外,该品起效时间与米氮平差异无显著性;转躁率与舍曲林相似。
另有人运用药物经济学成本-效果分析方法比较氟西汀、文拉法辛和阿米替林的经济效果后认为文拉法辛成本-效果比较低,显效率较高。
有研究表明该药对某些特定抑郁人群仍有效。
该品可升高5-HT能,故具抗焦虑和抑郁双向作用,亦能治疗产后抑郁。
开放研究表明,文拉法辛治疗l5例产后抑郁症病人,8周时80% 的病人缓解[11]。
此外,对老年人的激越性或焦虑性抑郁的8周缓解率比SSRIs高(40%~55%;31%~37%,P<0.05)。
亦可治疗卒中后抑郁状态,利于患者神经功能康复,提高生活能力,减少并发症。
亦有报道该品可用于难治性抑郁。
治疗焦虑症文拉法辛的抗焦虑效应较复杂,具有拟5-HT能,可激动5-HT1A受体抗焦虑,亦可激动5-HT2A 受体致焦虑。
故其作用取决于患者对哪种受体更敏感,以抗焦虑为多见。
Kate等汇集了5项安慰剂对照试验,发现文拉法辛治疗广泛性焦虑症的有效率比安慰剂高,在年轻人为67%:44%(P<0.001),在年长成人为66%:41% (P<0.001)。
文拉法辛治疗强迫症文拉法辛治疗强迫症有效。
包括曾经接受过选择性5-HT再摄取抑制剂治疗无效的患者。
其抗强迫作用可能有两方面原因:一是强迫症发生的机制是脑内5-HT功能低下,而去甲肾上腺素的功能变化对之有影响;二是文拉法辛可同时抑制5-HT和NE的再摄取。
可同时调整二者的功能变化。
故其抗强迫效应稍胜SSRIs。
研究表明,一种SSRI足量足程(12周)无效后,可换成另一种SSRI、氯丙咪嗪或文拉法辛,有效率可升至70%。
治疗社交恐怖症社交恐怖症的5-HT1A受体正常,5-HT2受体超敏。
文拉法辛可能是通过增加5-HT能,使5-HT2受体逐渐脱敏,达到治疗社交恐怖症的目的。
但因该品有拟NE能,故目前不作为该症的一线药物。
治疗精神创伤精神创伤激活蓝斑引起创伤后应激障碍(PTSD)症状。
文拉法辛通过阻断5-HT回吸收而激活背部缝际-蓝斑5-HT通路,抑制蓝斑NE能,改善PTSD症状。
对照试验表明,PTSD患者用文拉法辛缓释剂、舍曲林和安慰剂治疗l2周后发现,文拉法辛的PTSD缓解率比安慰剂为高(31%:20%,P<0.05),而舍曲林的缓解率与安慰剂无差异(24%:20%P>0.05)[16],提示文拉法辛治疗PTSD比舍曲林有效。
文拉法辛治疗多动症研究表明,ADHD患者脑内NE能递质功能不足,至少是NE能递质功能不平衡。
故文拉法辛通过NE能作用可改善注意力,通过5-HT能作用可抑制冲动行为,能消除多动症的各种症状。
王文强等[17]报道有效率可达80.9%。
治疗精神分裂症近年来有多个研究表明文拉法辛与抗精神病药合用治疗精神分裂症有较好疗效,包括辅助治疗精神分裂症阴性症状。
高存友等[18]的研究还发现该药有益于改善慢性精神分裂症患者的认知障碍。
此外,有研究得出,该品结合低热卡饮食可显著降低抗精神病药引起的肥胖;延长释放本药75mg/d的剂量可改善绝经后妇女的潮热;长效制剂可缓解糖尿病人的神经性疼痛。
该品亦可用于戒酒,目前已成为新一代治疗酒依赖的抗抑郁剂。
6药动学编辑文拉法辛自胃肠道吸收,半衰期约为5小时,每日约需2~3次服药。
文拉法辛在肝脏中经细胞色素P450(CYP)酶CYP2D6代谢,至少有一种活性代谢产物,O-去甲基文拉法辛。
7适应症编辑重性抑郁症。
8用法用量编辑起始剂量为75mg/d,分2~3次服用。
一般2周以内即可见效。
9相互作用编辑西咪替丁可抑制肝脏首过消除作用,提高血浆中游离药物的浓度。