围手术期静脉血栓栓塞(VTE)的防治
围手术期VTE预防与管理

1、围手术期VTE预防——评估 Caprini风险评估:筛查作用——预防措施
• VTE中高危风险的患者,同时存在较高的大出血风险或出血并发 症:
• 推荐应用机械预防
• 如出血风险降低,改用药物预防或与机械预防联用。
2、围手术期VTE预防——措施
• (一)基本预防 • 1.常规进行静脉血栓相关知识的患者教育。(宣教) • 2.积极的活动可以减少VTE的发生。对于VTE风险为低危的内科
险,且不增加肺栓塞事件的发生率。 • 机械性方法可减少部分患者发生DVT的危险,但疗效逊于抗凝药物,其最大优势
在于没有出血并发症。 • 单独使用机械性预防措施仅适用于合并凝血异常疾病、有高危出血风险的患者 • 极高危患者单独应用疗效差,推荐与有效的抗凝治疗联合应用。
2、围手操作:麻醉方式/时间、手术方式/时间、止血 • 术后处理:术后何种提问进行术后休息;重要指标、引流管的监
测和管理;术后饮食/补液、康复处理等诸多方面。
2、血栓性疾病
• 1.静脉血栓栓塞性疾病:即静脉血栓栓塞症(VTE); 包括:肺血栓栓塞症(PTE)和深静脉血 栓形成(DVT)
• 2.动脉血栓栓塞性疾病: 包括:急性冠状动脉综合征(ACS)、心房颤动、动脉缺血发作、脑卒
3、围手术期VTE预防——时机
1、术中预防VTE的措施
使用 GRADE方法 对证据的质量和推荐意见的强度进行分级(表1 ,2)
3、围手术期VTE预防——时机
2、关节置换手术:【推荐意见】
3、围手术期VTE预防——时机
3、髋部骨折手术:【推荐意见】
(1) 对于髋部骨折患者 ,推荐使用 LMWH、磺达肝癸钠、低剂量普通 肝素 (LDUH)预防 VTE【1B】。 (2) 建议在术前即开 始进行 VTE预防【2B】,不推荐手术前后 4 h 内应用 抗凝药物【1B】。 (3)推荐药物预防或机械预防应用 10-14 d ,建议延长至术后 28 -35 d 【1B】。 (4) 建议在住院期间联合应用机械预防与药物预防【2C】。 对出血风险较 高的患者 ,建议使用机械预防【2C】
胸外科围术期静脉血栓栓塞症知识科普

胸外科围术期静脉血栓栓塞症知识科普静脉血栓栓塞症(venous thromboembolism,后文简称VTE),这类疾病主要分为下肢深静脉血栓(deep vein thrombosis,后文简称DVT)和肺栓塞(pulmonary embolism,后文简称PE)两种,接受外科手术治疗的患者在术后常会发生这类疾病,属于外科手术术后常见的一种并发症。
患者术后若是发生了VTE就会延长治疗时间,不仅影响患者的恢复也增加了患者再次手术的风险。
国外对此类并发症已经提出了大量的临床预防方案,但我国对这类并发症的防治措施还不够完善,本文就为广大胸外科患者来详细阐述围术期VTE相关知识和预防措施。
1.静脉血栓栓塞症的临床表现与诊断VTE主要分为DVT、PE两种症状,两种症状的主要表现和常用检测方法如下所示:①下肢深静脉血栓(DVT)DVT患者临床的主要表现通常为下肢发生肿胀和疼痛,且患肢的两侧皮肤会变成暗紫色,而属于腓静脉型的DVT的患者则可能不会产生上述这些临床表现,有一半左右出现了以上症状的患者血栓可向近端发生延展。
通常胸外科患者在入院后临床医师都会对患者进行一个DVT临床可能性评估,该评估主要是初步预测患者在术后产生DVT的风险,Wells是很多临床医师会选择用到的评估表,其评估方式和得分情况如下表所示。
表1 Wells评分表患者具体表现、既往病史分值曾有过DVT临床病史1下肢瘫痪或近期下肢石膏制动1四周内卧床超过三日,或者四周内曾接受过大型手术1下肢有明显肿胀情况1深静脉走行会产生局部压痛感1可作出非深静脉血栓形成的其他诊断-2两侧胫骨结节下游10cm外周径只差大于3cm1进展期癌症1患肢两侧小腿产生指陷性水肿1临床医师一般会根据我们的Wells得分情况制定手术方案,得分小于2分的患者术后发生DVT的几率非常小,而大于2分或者2分的患者在术后就有很大的风险会发生DVT。
针对一些临床没有很明显表现的患者,医师一般都会选择静脉加压超声或者是多普勒超声对患者进行检查,90%以上的患者可直接通过多普勒超声检查出静脉血栓形成情况,而一些静脉血栓形成位置较为深入的患者,可能无法通过多普勒超声检查进行诊断,这时通常就会运用到加压超声对其进行探查,据相关医学调查报告显示,加压超声探查方法诊断准确率可达97%。
围手术期深静脉血栓肺动脉血栓栓塞症的诊断、预防与治疗专家共识(全文)
围手术期深静脉血栓/肺动脉血栓栓塞症的诊断、预防与治疗专家共识(全文)目录一、前言二、深静脉血栓/肺动脉血栓栓塞症的定义/诊断三、围手术期静脉血栓栓塞症(VTE)风险的评估及预防四、附件:GRADE分级标准一、前言围手术期深静脉血栓(deep venous thrombosis,DVT)/肺动脉血栓栓塞症(pulmonary thrombo-embolism,PTE)是围手术期患者的常见并发症和重要死亡原因之一,多见于骨科、妇产科、血管外科和胸外科手术患者,以骨科手术最为常见。
我国每年接受全髋关节置换术、全膝关节置换术和髋部周围骨折手术等骨科大手术的数百万病例中,有近50%患者形成DVT,其中20%出现有症状的肺栓塞(pulmonaary embolism,PE)。
美国1988年调查结果提示大约17%的孕产妇死亡是由于静脉血栓栓塞所致;另外,大面积烧伤等也是诱发DVT的高危因素。
因此,对手术患者围手术期静脉血栓栓塞症(venous thrombo-embolism,VTE)及早诊断,并进行有效的预防和治疗不仅可以降低发生PE的风险,降低患者死亡率,还可有效地减少医疗费用。
二、深静脉血栓/肺动脉血栓栓塞症的定义/诊断(一)定义静脉血栓栓塞(VET):是指血液在深静脉腔内不正常凝结,阻塞静脉腔,导致静脉回流障碍。
可发生于全身各部位静脉,以下肢深静脉为多,常见于骨科大手术后。
下肢近端(腘静脉或其之近侧部位)DVT是肺栓塞血栓栓子的主要来源,预防DVT可降低发生PTE的风险。
肺动脉血栓栓塞症(PTE):指内源性或外源性栓子堵塞肺动脉主干或其分支引起肺循环障碍和呼吸障碍的临床综合征。
包括PTE、脂肪栓塞、羊水栓塞和空气栓塞等。
其中PTE为PE的最常类型,通常所说的PE即指PTE。
围手术期的PTE多见于静脉系统的栓子脱落,偶见心房纤颤者心房栓子脱落,是围手术期患者死亡的主要原因之一。
(二)诊断可根据其临床表现,结合物理、化验检查,做出较明确诊断。
静脉血栓栓塞症(VTE)防治管理制度

1.目的为规范住院患者静脉血栓栓塞症(VTE)的评估、预防、诊断、治疗、随访、质控的全流程管理, 降低VTE的发生率和致残率、致死率, 最大限度保障患者安全,特制定本办法。
2.目标规范管理。
3.适用范围全院临床、医技科室4.名词定义5.静脉血栓栓塞症(venous thromboembolism, VTE)是包括深静脉血栓形成(deep venous thromboembolism, DVT) 和肺血栓栓塞症( pulmonary thromboembolism, PTE)在内的一组血栓栓塞性疾病, 是遗传性和获得性等多种危险因素共同作用的全身性疾病。
6.内容5.1组织架构5.1.1 院内VTE防治管理委员会。
职责: 制定院内 VTE 防治管理规章制度并监督实施;制定院内 VTE 防治管理实施方案及防治工作手册;制定院内 VTE 防治的关键数据指标、监测指标及考核指标;制定院内 VTE 防治的计划, 定期进行总结、考核和评价;明确各有关部门、人员在防治工作中的责任;建立 VTE 救治绿色通道;定期召开 VTE 专题培训和教育; 8每季度召开 VTE 防治管理委员会会议。
5.1.2 院内VTE防治管理办公室。
职责: 负责医院内 VTE 防治工作的具体执行, 对医院内 VTE 防治落实情况进行检查和指导;对 VTE 防治管理进行监测、分析和反馈, 提出改进措施并指导实施, 并根据反馈情况进行不断的评议和改进;定期评价改进后的效果;对医务人员和管理人员进行医院内 VTE 防治培训并考核。
5.1.3科室VTE防治管理小组:职责:各科主任作为科室第一责任人, 全面负责本科室 VTE 防控管理的各项工作;对本科室的发生的 VTE 病例及 VTE 防控环节进行监测, 采取有效措施, 降低本科室 VTE 发病率;发生院内 VTE 时, 及时采取措施, 将危害降低到最低, 24小时内填写院内VTE 事件上报表报送医务处和护理部, 并组织分析;对本科室医护人员医院 VTE 防治知识培训;每月对本科室人员落实 VTE 防治工作情况进行抽查、考核和持续改进。
静脉血栓栓塞症(VTE)的预防与健康宣教
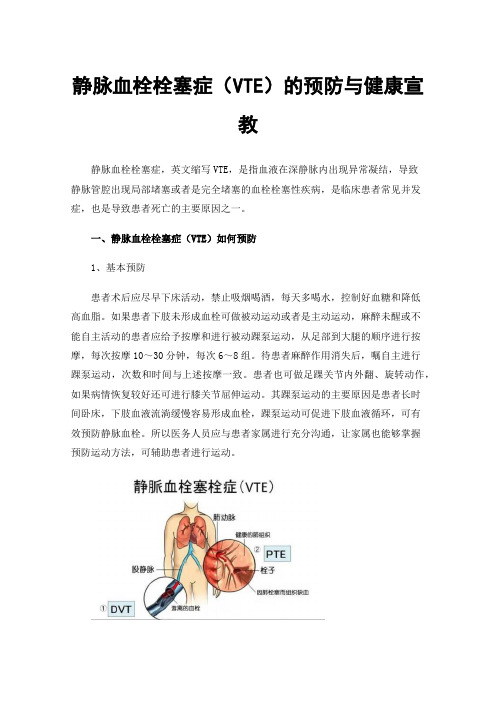
静脉血栓栓塞症(VTE)的预防与健康宣教静脉血栓栓塞症,英文缩写VTE,是指血液在深静脉内出现异常凝结,导致静脉管腔出现局部堵塞或者是完全堵塞的血栓栓塞性疾病,是临床患者常见并发症,也是导致患者死亡的主要原因之一。
一、静脉血栓栓塞症(VTE)如何预防1、基本预防患者术后应尽早下床活动,禁止吸烟喝酒,每天多喝水,控制好血糖和降低高血脂。
如果患者下肢未形成血栓可做被动运动或者是主动运动,麻醉未醒或不能自主活动的患者应给予按摩和进行被动踝泵运动,从足部到大腿的顺序进行按摩,每次按摩10~30分钟,每次6~8组。
待患者麻醉作用消失后,嘱自主进行踝泵运动,次数和时间与上述按摩一致。
患者也可做足踝关节内外翻、旋转动作,如果病情恢复较好还可进行膝关节屈伸运动。
其踝泵运动的主要原因是患者长时间卧床,下肢血液流淌缓慢容易形成血栓,踝泵运动可促进下肢血液循环,可有效预防静脉血栓。
所以医务人员应与患者家属进行充分沟通,让家属也能够掌握预防运动方法,可辅助患者进行运动。
2、物理预防根据医嘱使用抗血栓弹力袜或间歇性充气加压装置,每次30分钟,每天2~4次。
使用弹力时患者需要注意以下事项:①弹力袜最佳穿戴时间为早上起床,晚上睡觉时脱下,每天必须保证弹力袜穿戴8小时以上。
②如果是在较为干燥的季节,患者要预防脚后部位皮肤皲裂,否则会对弹力袜造成损伤,同时,穿戴前检查鞋内是否存在异物、是否平整,否则会对弹力袜造成损伤。
③不能用女性弹力袜替代医用弹力袜,因为医用弹力袜有治疗压力,并且部位不同所产生的压力也不同,如果盲目替代会影响最终的穿戴效果。
④穿戴弹力袜时如果发现疼痛情况并无改善,且腿部受到的压迫明显,可能是因为弹力袜压力过大,可联系护士或者是医生更换弹力袜。
⑤弹力袜的要定期进行清洗,清洗时要使用温水,保证水温不超过40℃,切忌机洗或者是用力拧绞。
⑥洗净后不要拧干,可用手挤出多余水分,或者是用毛巾吸干,平整放置于阴凉处晾干。
3、药物预防患者应严格按照医嘱服用抗凝药物,但是由于抗凝药物作用机制的影响的,每种药物都存在注意事项和不良反应,患者服用药物前需要详细说明。
骨科大手术围术期深静脉血栓的防治策略PPT课件

恶性肿瘤妊娠和围产期雌激素治疗创伤或下肢、髋部、腹部或骨盆手术炎性肠道疾病肾病综合征脓毒血症易栓症
创伤或手术静脉穿刺术化学刺激心脏瓣膜疾病或瓣膜置换术动脉粥样硬化留置导管
房颤左心室功能障碍活动受限或瘫痪静脉机能不全或静脉曲张肿瘤、肥胖或妊娠造成的静脉闭塞
高凝状态:
血管壁损伤:
循环淤滞:
维柯氏三角(Virchow’s triad)
→
→
髋部骨折
VTE的危险因素
1、静脉内膜损伤;(创伤、手术、化学性损伤、感染性损伤等)2、静脉血流瘀滞;(既往VTE病史、术中应用止血带、瘫痪、制动等)3、高凝状态。(高龄、肥胖、全身麻醉、中心静脉插管、红细胞增多症、巨球蛋白血症、骨髓增生异常综合症、人工血管或血管腔内移植物等)
VTE的产生和形成与以下因素有关
1、预计3天后方能行手术治疗的,皮下常规剂量低分 子肝素(手术前12小时前停止),同时联合使用间 歇充气泵;2、预计1~2天行手术治疗的,仅使用间歇充气泵;3、术后12小时行皮下注射低分子肝素,维持7~14天 ,同时联合使用间歇充气泵。
展 望
未来骨科大手术DVT预防的研究方向 找出预测将发展成为有临床表现的重要的术后DVT的遗传、临床和生化特征,根据个体危险因素对病人进行分层次预防目前确定高危病例的能力有限我国骨科大手术DVT预防任重道远需要推出中国特色的骨科大手术DVT预防指南
骨科大手术围术期
深静脉血栓的防治策略
静脉血栓栓塞症(Venous Thromboem-bolism VTE):是指血液在静脉内不正常的凝结,使血管完全或不完全性阻塞,属于静脉回流障碍性疾病。 包括两种类型:深静脉血栓(DVT)和肺动脉血栓栓塞症(PTE)骨科大手术后VTE发生率较高,是患者围手术期死亡的主要原因之一。也是医院内非预期死亡的重要原因。
骨科静脉血栓栓塞症规范预防(全文)
骨科静脉血栓栓塞症规范预防(全文)静脉血栓栓塞症(VTE)是骨科手术的常见并发症,是患者围手术期主要的死亡原因之一,也是医院内非预期死亡的重要原因。
由于临床表现隐匿,VTE常被临床医生所忽视。
在过去相当长的历史时期,由于抗凝药物种类单一,剂量调整困难,变异因素较多,除专科医生外,其他临床医生掌握困难。
近年来由于新型安全方便抗凝药的出现,骨科术后VTE得到了广泛的重视,也制定出了相应《指南》和《共识》。
但在临床实际应用中仍有不规范之处,需要加强基础理论学习。
一、亚洲人DVT的发生率并不低随着生活水平提高及生活方式改变,中国人肥胖、糖尿病、高脂血症等发生率大幅度升高,导致外周血管病变和血液动力学改变,加之生活和工作节奏加快,缺乏必要的体能锻炼,DVT发生的危险因素急剧增加。
马来西亚Dhillon[1]对髋关节置换、膝关节置换和髋部骨折88例患者静脉造影,55例(62.5%)显示DVT,其中11例发生在腘静脉和股静脉(表1)。
北京协和医院、上海瑞金医院和广州医学院一附院联合完成的有关关节置换术后DVT的研究结果显示,抗凝预防组的DVT发生率为11.8%,未预防组为30.8%[2]。
与加拿大Geerts[3]报告相比(表2),亚洲人骨科大手术后DVT的发生率与西方人相似。
二、骨科术后DVT 有其独特的原因德国Virchow在l856年首次描述血栓形成的基本要素即Virchow三联征:高凝状态、内皮损伤和静脉瘀滞。
骨科手术的VTE高发生率有其独特的原因:(1)下肢关节置换术和髋部骨折手术后,由于隐形失血[4]导致血液浓缩和血液中存组织碎片、胶原、脂肪而易发生血液凝固;(2)下肢骨折后畸形及手术操作中对血管的扭曲以及骨碎片对血管壁的损伤都会增加内皮细胞损伤的概率,老年患者血管本身已存有病变,血管内皮下组织暴露导致凝血机制激活;(3)髋部骨折后疼痛,导致肢体正常的活动减少;(4)全膝关节置换术中使用大腿止血带、膝关节屈曲时间过长,术后固定、术后局部肿胀和活动受限都会增加静脉瘀滞。
静脉血栓栓塞症(VTE)防治管理方案
静脉血栓栓塞症(VTE)防治管理方案目录一、静脉血栓栓塞症(VTE)防治工作的目的二、静脉血栓栓塞症(VTE)防治管理体系三、静脉血栓栓塞症(VTE)防治管理四、静脉血栓栓塞症(VTE)抗凝后严重出血的处理流程五、附件一、静脉血栓栓塞症(VTE)防治工作的目的静脉血栓栓塞症(VTE)是包括深静脉血栓形成(DVT)和肺血栓栓塞症(PTE)在内的一组血栓栓塞性疾病,是遗传性和获得性等多种危险因素共同作用的全身性疾病。
为了建立院内VTE防治综合管理体系,在全院开展VTE风险评估、VTE综合预防和规范化治疗等工作,指导临床科学有效进行VTE防治,达到有效降低住院患者VTE发生率,对VTE做到早期识别、早期诊断和规范治疗,提高医疗质量,保障医疗安全的目的,制定本方案。
二、静脉血栓栓塞症(VTE)防治管理体系1.成立医院静脉血栓栓塞症(VTE)防治管理组,人员组成包括院领导相关科室负责人。
职责包括建立健全院内VTE防治管理制度并监督实施;确定医院VTE防治工作流程;确定医院VTE防治重点部门、重点环节及采取的预防措施,明确各有关部门的责任;通过信息化手段推动VTE防治工作的开展;定期对院内各科各级医护人员举办VTE 知识培训;将VTE防治管理纳入科室综合管理目标,完善院内VTE预防与管理体系;其他医院VTE防治管理的重要事宜。
2.以科室质量管理小组为基础的科室VTE防治管理小组,人员组成包括科主任、护士长及科室其他人员。
职责包括科主任为科室VTE 防治管理工作第一责任人,全面负责本科室VTE防治管理的各项工作;对本科室VTE防治环节进行监测,采取有效措施,降低科室VTE发生率;发生院内VTE病例时,及时采取有效措施,将危害降到最低;定期评测分析科室内VTE防治工作效果;对本科室医护人员进行VTE防治知识培训。
三、静脉血栓栓塞症(VTE)防治管理1.对住院患者进行VTE风险评估。
具体评估内容参照外科住院患者VTE风险评估表(Caprini评分)和内科住院患者VTE风险评估表(Padua评分)。
静脉血栓栓塞疾病症候群(VTE)防治管理方案

静脉血栓栓塞疾病症候群(VTE)防治管理方案简介静脉血栓栓塞疾病症候群(Venous Thromboembolism,简称VTE)是一种临床上常见的疾病,包括深静脉血栓形成和肺栓塞两个主要部分。
本文档旨在提供一份VTE的防治管理方案,以帮助医务人员更好地预防和治疗VTE。
预防措施VTE的预防非常重要,特别是对于患有相关危险因素的患者。
以下是一些常见的预防措施:1. 患者教育:教育患者了解VTE的风险因素、症状和预防方法,并提醒他们在行动减少期间进行适当的运动和活动。
2. 动态评估:对于高危患者,需要进行动态评估,及时发现和干预潜在的血栓形成和栓塞风险。
3. 弹力袜:对于有高风险的患者,建议佩戴弹力袜,以增加血液回流,减少血栓形成的可能性。
4. 药物预防:在一些需要长时间卧床或手术的患者中,可以考虑使用抗凝药物进行预防,但需要根据患者个体化情况进行判断。
诊断和治疗一旦疑似VTE,应进行及时的诊断和治疗,以避免严重并发症的发生。
以下是常见的诊断和治疗措施:1. 临床评估:通过病史、体检和相关实验室检查,进行初步的临床评估,排除其他疾病并确定VTE的可能性。
2. 影像学检查:采用超声、CT扫描等影像学技术,对深静脉血栓和肺栓塞进行定位和确认。
3. 抗凝治疗:对于已确诊的VTE患者,应尽早进行抗凝治疗,以阻止血栓的进一步发展和防止血栓栓塞的再次发作。
4. 支持治疗:在抗凝治疗的同时,对于病情较重的患者,可以考虑使用溶栓剂或进行手术治疗等支持措施。
随访和复发预防治疗完成后,需要进行随访和复发预防工作,以减少VTE的再次发作风险。
以下是相关措施:1. 定期随访:对于VTE患者,应定期进行复查和随访,观察病情变化,并及时调整治疗方案。
2. 个体化护理:根据患者的年龄、患病情况、危险因素等因素,制定个体化的复发预防计划,包括生活方式改变、药物治疗等方面。
3. 教育与指导:通过患者教育和指导,提高患者对VTE的认知和自我监测能力,以及掌握紧急处理措施。
静脉血栓栓塞症(VTE)防治工作手册

静脉血栓栓塞症(VTE)防治工作手册第一部分、住院患者VTE防治工作的意义静脉血栓栓塞症(VTE)包括深静脉血栓形成(DVT)和肺血栓栓塞症(PTE),是全球性的医疗保健问题。
医院内VTE发生的风险与患者的住院病情、手术等治疗措施以及患者并存的其他危险因素(如高龄、肥胖、卧床、合并症等)有关,常并发于其他疾病,在住院患者中发病率很高,是导致医院内患者非预期死亡及围手术期死亡的重要原因之一,已经成为医院管理者和临床医务人员面临的严峻问题。
VTE是可防可治的,针对VTE高危因素主动采取恰当的预防措施,可减少或避免发展成VTE;己经发生了VTE也要进行正确的评估,采取恰当的治疗措施,降低死亡率和致残率。
第二部分、各科室VTE防治管理小组人员组成:科室主任、护士长及指定人员或联络员。
职责:1.科主任为科室内VTE防治管理第一负责人,对科内静脉血栓栓塞症防治工作中的培训I、考核及VTE发生负有管理责任。
2.质控医生监督填报本科室院内VTE相关评估表。
3.在科主任领导下开展工作,负责本科室院内VTE防治管理的各项工作,根据科室特点制定管理制度,并组织落实。
4.协助各科室完成院内VTE防治的诊疗过程。
5.协助院内VTE防治管理委员会交办的其他工作。
第三部分、院内VTE预防院内VTE预防的基本原则1,由于VTE的发生是十分复杂的病理、生理过程,采取预防措施前必须进行个体化评估,权衡抗凝与出血的利弊,并认真研读药物及器械相关说明书;2.如预防过程中出现药物使用禁忌症或其他特殊情况,请及时邀请专业科室医生会诊;3.即使采取VTE预防措施之后,仍有可能发生VTEo 一旦发生,应采取相应治疗措施;4.预防性抗凝药物使用后可能出现出血并发症。
一旦发生出血,应采取相应治疗措施;5.各临床科室根据专业特点制定相应的预防措施,如本科室已有专业指南(如骨科),请遵循该专业指南执行。
院内VTE预防措施基本预防措施1.常规进行静脉血栓相关知识的患者教育。
骨外科患者围手术期VTE的防治

VTE药物预防
• 低分子量肝素LMWH
– 那曲肝素(速碧林)——0.6ml/支 – 依诺肝素(克赛) ——0.6ml/支 – 达肝素(法安明)
• 外科患者LMWH预防剂量
– 中危,LMWH0.2ml qd – 高危, LMWH0.4ml qd – 术前12h开始给药 – 持续7-10d或患者解除VTE危险因素
LMWH的使用
• 一般情况下无需血液学检测 • 出现异常出血时
– 血常规
• 异常血小板减少, 考虑HIT时,行PF4抗体检测(外送)
– 凝血常规 – 血栓弹力图
VTE预防
• 间接Xa抑制剂
– 磺达肝癸钠(安卓) 2.5mg, ih qd
• 直接Xa抑制剂
– 利伐沙班(拜瑞妥) 10mg~20mg qd 可和LMWH连接替换
• 中危 3-4分 • 高危 ≥5分
DVT急性期的治疗
• 溶栓
– 导管溶栓 – 系统性溶栓 – 尿激酶 – 组织纤溶酶原激活物
• 手术取栓 • 下腔静脉滤器置入?
%
肺栓塞 Pulmonary embolism, PE
血友病患者的手术
• 血友病患者大多数可以安全手术
– 血友病A –血液病B – 遗传性XI因子缺乏症
VTE预防
• 维生素K拮抗剂
– 华法林, 2.5mg~3mg po qd; – 维持INR在2-3之间; – 术前应用华法林的患者,建议围手术期改用 LMWH抗凝 – LMWH转回华法林时,需重叠应用5-7d
抗凝药物的禁忌症
• 是否有活动性出血 • 是否有活动性消化道溃疡(A期) • 是否有凝血功能障碍
• 详细、充分的凝血因子补充方案和预案必 不可少
小结
骨科手术患者围手术期VTE风险评估及预防

VTE是骨科手术患者常见的并发 症,可导致肺栓塞、下肢功能障 碍等严重后果,甚至危及生命。
因此,对骨科手术患者进行围手 术期VTE风险评估及预防至关重
要。
VTE的定义和危害
VTE是指血液在静脉内不正常地凝结,阻塞管腔, 导致静脉回流障碍的一系列病症,包括深静脉血栓 形成(DVT)和肺血栓栓塞(PTE)。
淤积。
早期活动
鼓励患者术后早期进行下肢肌肉收 缩及踝泵运动,促进下肢血液循环。
抬高下肢
适当抬高下肢,减轻下肢静脉压力, 促进血液回流。
药物预防措施
01
02
03
低分子量肝素
通过注射的方式给予低分 子量肝素,抑制血栓形成。
华法林
口服华法林等抗凝药物, 降低血液凝固性,预防血 栓形成。
其他抗凝药物
根据患者的具体情况,选 择其他适当的抗凝药物进 行预防。
03
促进患者康复
术后血栓形成不仅可能导致肢体功能障碍,还可能引发肺 栓塞等严重并发症,威胁患者的生命安全。通过VTE风险 评估及预防,可以促进患者的康复进程,缩短住院时间, 提高患者的生活质量。
骨科手术患者围手术期VTE风险评估及预防的实践建议
完善术前评估
术中预防措施
术后康复指导
定期随访与监测
在手术前,应对患者的VTE 风险进行全面评估,包括患 者的年龄、性别、基础疾病 、家族史等。根据评估结果 ,制定个性化的预防方案。
治疗方案。
THANKS
04
VTE风险评估及预防的最新研 究进展
VTE风险评估的研究进展
遗传因素研究
近年来,越来越多的研究关注遗 传因素在VTE风险评估中的作用, 发现某些基因突变与VTE的发生
普通外科围手术期血栓预防和管理指南

普通外科围手术期血栓预防和管理指南引言随着人口老龄化程度的不断进展、心血管疾病发病率的逐年上升,血栓栓塞性疾病的防治和处理逐渐受到各学科的关注和重视。
静脉血栓栓塞症(venous thromboembolism,VTE)包括肺血栓栓塞症(pulmonary thromboembolism,PE)和深静脉血栓形成(deep vein thrombosis,DVT)。
PE 与 DVT是同一疾病发展的不同阶段和其在不同部位的两种临床表现,二者统称为 VTE。
外科患者术前活动量减少、术中制动、术后长期卧床均使静脉血流速度明显减慢;麻醉及手术创伤促使组织因子释放,并直接激活外源性凝血系统,导致高凝状态或血栓形成;患者自身因素,如高龄、肥胖、恶性肿瘤等,均可使VTE发生的风险增加。
此外,越来越多的患者在接受普通外科手术的同时使用抗栓药物,常见的如机械瓣膜置换术后、慢性心房颤动、冠心病支架置入后等心脏疾病及周围血管疾病患者。
对于长期服用抗栓药物并需要进行普通外科手术的患者,外科医师应该对患者实施评估,并根据评估结果决定围手术期的抗栓药物管理。
为了规范和推动全国范围内外科围手术期患者的血栓管理实践,2015年11月,由中华医学会外科学分会牵头,依据现有的循证医学证据,参考相关学科专家的意见和已有的工作基础[1],制定普通外科围手术期血栓预防和管理指南,希望对国内广大临床医师有所帮助。
第一部分:围手术期静脉血栓栓塞症的预防一、概述(一)普通外科患者VTE发生率VTE是外科手术患者常见的并发症,如无预防措施,普通外科手术患者DVT发生率为10%~40%[2]。
大型手术患者同时具有多种VTE风险因素(年龄>40岁、VTE病史、肿瘤等)时,致死性PE发生率高达5%[3]。
亚洲人群中,普通外科未进行抗凝预防的手术患者DVT发生率为13%,症状性PE发生率为1%[4]。
日本调查结果显示,腹部大手术患者仅使用弹力袜或弹力绷带预防,静脉造影检出的VTE发生率为24.3%[5]。
围手术期VTE预防

预防并发症
加强皮肤护理,预防压疮等并发症的发生。
患者教育与心理支持
健康宣教
心理疏导
向患者及家属讲解VTE的相关知识、治疗方 案及护理措施,提高患者的认知度和依从 性。
关注患者的心理变化,给予积极的心理疏 导和支持,帮助患者树立战胜疾病的信心 。
康复指导
出院指导
指导患者进行康复锻炼,如下肢肌肉收缩 、关节活动等,促进下肢静脉回流,减轻 肿胀和疼痛。
THANK YOU
。
02
围手术期VTE评估
评估工具与流程
VTE风险评估量表
采用国际通用的VTE风险评估量表,如Caprini评分、Padua评分等,患者入院时、手术前、手术后及出院前的评估 ,确保患者得到及时有效的预防。
患者因素评估
年龄与性别
高龄、女性患者VTE风险相对较高。
基础疾病
合并高血压、糖尿病、冠心病等基础 疾病的患者VTE风险增加。
生活习惯
长期卧床、缺乏运动等不良生活习惯 会增加VTE风险。
既往史
有VTE病史或家族史的患者应高度重 视。
手术因素评估
1 2
手术类型
不同手术类型对VTE风险的影响不同,如骨科大 手术、盆腔手术等VTE风险较高。
手术时间
手术时间长、术后卧床时间久的患者VTE风险增 加。
处理措施
针对不同并发症采取相应治疗措施,如抗凝、溶栓、手术等,同时加强患者护理 和康复指导。
05
围手术期VTE治疗与护理
治疗方案选择与实施
药物治疗
根据患者病情和手术类型,选择 合适的抗凝药物,如普通肝素、 低分子肝素等,预防血栓形成。
机械性预防措施
应用间歇性充气加压装置、梯度 压力袜等,增加下肢静脉血流速 度,减少血液淤积。
2023年静脉血栓栓塞防治的专家共识

2023年静脉血栓栓塞防治的专家共识
简介
本文档旨在总结2023年静脉血栓栓塞(VTE)防治方面的专
家共识。
根据最新的研究和临床实践,以下是一些关键观点和建议。
1. VTE的定义和分类
- VTE是指静脉系统内发生的血栓形成和血栓栓塞的病理过程。
- VTE可分为深静脉血栓形成(DVT)和肺血栓栓塞(PE)两
种类型。
2. 预防措施
- 对于高风险患者,如手术患者、长期卧床患者以及有其他相
关危险因素的患者,应采取积极的预防措施,包括使用抗凝药物、
弹力袜等。
- 在药物预防方面,常用的药物包括肝素、华法林、新型口服
抗凝药物等。
3. 诊断和治疗
- 在临床症状和体征提示VTE的情况下,应及时进行相关检查,包括超声波、放射学影像和实验室检查等。
- 对于DVT的治疗,常用的方法包括抗凝治疗、静脉溶栓和手
术取栓等。
- 对于PE的治疗,根据患者的病情和全身状况,可选择抗凝治疗、溶栓治疗和介入手术等。
4. 长期管理和后续随访
- 对于VTE患者,应进行长期的抗凝治疗,时间因个体情况而异。
- 必须密切监测治疗效果和患者的安全性。
- 随访时注意VTE的复发和并发症的产生。
以上是2023年静脉血栓栓塞防治的专家共识的简要总结。
具
体内容还需根据最新研究和临床指南进行详细制定和解释。
VTE防治及护理

VTE防治及护理VTE(静脉血栓栓塞)是一种由血液凝块形成的疾病,常见的类型包括深静脉血栓(DVT)和肺栓塞(PE)。
VTE的预防和护理是非常重要的,因为它可以导致严重的并发症甚至危及生命。
本文将详细介绍VTE的预防和护理措施。
预防VTE的方法包括以下几个方面:1.早期行动:对于长期卧床或手术患者,需要尽早进行活动,包括卧床患者的主动翻身和进行肢体练习,手术患者则需要尽早下床活动。
2.引导使用弹性袜:对于高危人群,如年龄较大、手术后、长时间旅行或患有其他可独立危险因素的患者,可以使用医生指导下的弹性袜,来减少静脉回流的压力。
3.使用抗凝剂:对于高危人群,如卧床不动或长时间坐立的患者,医生可能会考虑使用抗凝剂来延长凝血时间,减少血栓形成的风险。
4.饮食调整:限制摄入高盐食物和高胆固醇食物,增加蔬菜、水果和全谷物的摄入,保持健康的体重和饮食习惯,以降低患血栓的风险。
VTE的护理措施主要包括以下几个方面:1.定期监测:对于已经确诊的VTE患者,需要进行定期的血液检测,包括凝血功能、D-二聚体和其他相关指标的监测,以评估病情的发展和治疗效果。
2.药物治疗:抗凝治疗是VTE患者的常用方法,常用药物包括肝素和华法林。
患者需要遵循医生的指导,按时、按量服用药物,并定期进行血液检测。
3.外科治疗:对于严重的VTE患者,如合并出血或肺功能受损者,可能需要进行外科手术治疗,如置入血栓取出器或过滤器来去除或阻止血栓形成。
4.运动锻炼:合适的运动锻炼可以减少血液在静脉中滞留的时间,并促进静脉回流,减少血栓形成的风险。
患者可以进行适度的有氧运动,如散步、游泳或骑自行车等。
5.饮食管理:建议患者保持均衡的饮食,避免摄入过多的高盐食物和高胆固醇食物,增加纤维素的摄入,并避免饮食过量和饮食过度。
对于VTE患者和高危人群,还有一些值得注意的事项:1.定期复查:定期复查包括凝血功能、D-二聚体、超声检查和病情评估等,以确保病情的稳定和治疗效果的评估。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
5 Points
Stroke (< 1 mo)
Hip, pelvis, or leg fracture
Elective arthroplasty
Acute spinal cord injury (< 1 mo)
Caprini风险评分
危险因素 得分:1分
年龄41-60岁 小手术
BMI>25 kg/㎡ 下肢水肿 严重肺部疾病,包括肺 炎(1个月内) 妊娠期或产后 不能解释或二次自然流 产病史 需要卧床休息的患者
Active bleeding Previous major bleeding Known, untreated bleeding disorder Severe renal or hepatic failure Thrombocytopenia Acute stroke Uncontrolled systemic hypertension Lumbar puncture, epidural, or spinal anesthesia within previous 4 h or next 12 h Concomitant use of anticoagulants, antiplatelet therapy, or thrombolytic drugs
3 Points
Age ≥ 75 y History of VTE Family history of VTE Factor V Leiden Prothrombin 20210A Lupus anticoagulant Anticardiolipin Antibodies Elevated serum Homocysteine Heparin-induced thrombocytopenia Other congenital or acquired thrombophilia
low-molecular-weight heparin(LMWH) (2B), low-dose unfractionated heparin(LDUH) (2B),or mechanical prophylaxis, preferably with IPC (2C) mechanical prophylaxis, preferably with IPC (2C)
危险因素 得分:5分
脑卒中(1个月内) 髋关节、骨盆或下肢骨折
VTE家族史 因子V Leiden 阳性 凝血酶原20210A阳性
择期关节置换术
急性脊柱损伤(1个月内)
VTE Risk For General Surgery
VTE Risk
Very low Low Moderate High
Caprini Score
very low risk
no specific pharmaclogic (1B) or mechanical (2C) prophylaxis be used other than early ambulation
low risk
moderate risk
mechanical prophylaxis, preferably with intermittent pneumatic compression (IPC) (2C)
Prevention and Treatment of Perioperative Venous Thromboembolism (VTE)
Gordon H. Guyatt, et al. Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. CHEST 2012; 141(2)(Suppl):7S–47S.
Acute myocardial infarction
Congestive heart failure (< 1 mo) History of inflammatory bowel disease Oral contraceptives or hormone replacement
Immobilizing plaster cast Central venous access
Recommendations are classified as strong (Grade 1) or weak (Grade 2), according to the balance between benefits, risks, burden, and cost, and the degree of confidence in estimates of benefits, risks, and burden. Quality of evidence are classified as high (Grade A), moderate (Grade B), or low (Grade C) according to factors that include the risk of bias, precision of estimates, the consistency of the results, and the directness of the evidence.
Prevention of VTE in General and Abdominal-pelvic Surgical Patients
Risk Prophylaxis for normal paitients Prophylaxis for patients at high risk for major bleeding complications pharmacologic prophylaxis with LMWH (1B) or LDUH (1B), mechanical prophylaxis with elastic stockings (ES) or IPC should be added to pharmacologic prophylaxis (2C) extended-duration pharmacologic prophylaxis (4 weeks) with LMWH (1B) mechanical prophylaxis, preferably with IPC, until the risk of bleeding diminishes and pharmacologic prophylaxis may be initiated (2C)
Risk Factors for Major Bleeding Complications Procedure-specific risk factors
Байду номын сангаас
Abdominal surgery Male sex, preoperative hemoglobin level < 13 g/dL, malignancy, and complex surgery defined as two or more procedures, difficult dissection, or more than one anastamosis Pancreaticoduodenectomy Sepsis, pancreatic leak, sentinel bleed Hepatic resection Number of segments, concomitant extrahepatic organ resection, primary liver malignancy, lower preoperative hemoglobin level, and platelet counts
Risk Factors for Major Bleeding Complications Procedure-specific risk factors
Cardiac surgery Use of aspirin Use of clopidogrel within 3 d before surgery BMI > 25 kg/m2, nonelective surgery, placement of five or more grafts, older age Older age, renal insufficiency, operation other than CABG, longer bypass time Thoracic surgery Pneumonectomy or extended resection
Pulmonary Embolism (PE)
Deep Venous Thrombosis (DVT)
VTE-related deaths
200,000 per year in US 1/3 occur following surgery
2~3-fold for cancer patients
Prophylaxis?
VTE ↓71% Death ↓46% Major bleeding ↑103% Wound hematoma ↑ 88%
VTE
Bleeding
Mismetti P, et al. Meta-analysis of low molecular weight heparin in the prevention of venous thromboembolism in general surgery .Br J Surg . 2001 ; 88 ( 7 ): 913 - 930 .
Risk Factors for Major Bleeding Complications