格列吡嗪片原研说明书辉瑞
格列吡嗪片 格列吡嗪胶囊 - 药物在线-快捷药物信息平台

格列喹酮片
Gelie Kuitong Pian Gliquidone Tablets
本品含格列喹酮(C H N 0 S)应为标示量的90.0%~
2 7 3 3 3 6
110. 0% 。 【性状】本品为白色片或薄膜衣片。 【鉴别】(1)取本品细粉适量(约相当于格列吡嗪 50mg) ,加二氧六环 10ml ,置水浴中加热振摇,使格列吡嗪溶 解,滤过,加0. 5% 2 2,4-二硝基氟苯的二氧六环溶液lml,煮沸
【贮藏】遮光,密封,在干燥处保存。
3分钟,溶液显亮黄色。 (2) 在 含 量 测 定 项 下 记 录 的 色 谱 图 中 , 供 试 品 溶 液 主 峰 的
本品为1-环己基-3-〔〔对-〔2-( 3 , 4- 二氢 -7- 甲氧基- 4,4- 二 甲基 -1,3- 二氧代 -2(1H)- 异喹啉基)乙基〕苯基〕磺酰基〕脲。 按 干 燥 品 计 算 , 含 C H N 0 S 为 9 8 . 0% 102. 0%。
2 7 3 3 3 6
【性状】 本品为白色结晶或结晶性粉末;无臭,无味。 本品在三氯甲垸中易溶,在丙酮中略溶,在乙醇或甲醇中 微溶,在水中几乎不溶。 熔 点 本 品 的 熔 点 ( 附 录 W C)为178 :L82°C。 【鉴别】(1)取本品约10mg,加苯肼5滴,加热至溶液变 清,放冷,加氨试液 0. 5 m l 、 1 0 % 硫 酸 镍 溶 液 0 . 5 m l 与 三 氯 甲 烷 lml ,剧烈振摇,静置,下层溶液应变成紫红色。 (2) 在 含 量 测 定 项 下 记 录 的 色 谱 图 中 , 供 试 品 溶 液 主 峰 的 保留时间应与对照品溶液主峰的保留时间一致。 (3) 本品的红外光吸收图谱应与对照的图谱(光谱集 1097 图)一致。 【检查】氯化物取本品2.0g,加水100ml,煮沸,至剩 余约50ml时,迅速放冷,滤过,滤液加水使成50ml,量取 25ml,依法检査(附录VI A ) , 与 标 准 氯 化 钠 溶 液 7 . 0 m l 制 成 的 对照液比较,不得更浓( 0.014 %)。 硫酸盐取氯化物检査项下剩余的滤液25ml,依法检査 (附录 W B) ,与标准硫酸钾溶液 2. 0ml 制成的对照液比较,不
二甲双胍格列吡嗪片说明书
二甲双胍格列吡嗪片说明书推荐文章厄贝沙坦氢氯噻嗪片说明书热度:复方硫酸双肼屈嗪片说明书热度:盐酸特拉唑嗪片说明书热度:脑益嗪片说明书热度:盐酸曲美他嗪片说明书热度:二甲双胍格列吡嗪片(立方)治疗2型糖尿病,内分泌科。
下面是店铺整理的二甲双胍格列吡嗪片说明书,欢迎阅读。
二甲双胍格列吡嗪片商品介绍通用名:二甲双胍格列吡嗪片生产厂家: 合肥立方制药股份有限公司批准文号:国药准字H20090086药品规格:12片药品价格:¥22元二甲双胍格列吡嗪片说明书【通用名称】二甲双胍格列吡嗪片【商品名称】二甲双胍格列吡嗪片(立方)【英文名称】MetforminHydrochlorideandGlipizideTablets【拼音全码】ErJiaShuangGuoGeLieBiQinPian【主要成份】二甲双胍格列吡嗪片为复方制剂,其组份为:每片含盐酸二甲双胍250mg与格列吡嗪2.5mg。
【适应症/功能主治】2型糖尿病,内分泌科。
【规格型号】12s【用法用量】二甲双胍格列吡嗪片应根据有效性和耐受性进行个体化给药,且不得超过大推荐给药剂量即每日20mg格列毗嗪2000mg二甲双胍。
二甲双胍格列吡嗪片应与食物一起服用且从较低剂量开始给药,按下述方法逐步增大剂量以避免低血糖(主要由格列毗嗪引起),减少胃肠道不良反应(主要由二甲双胍引起),并针对不同患者确定能充分控制血糖的低有效剂量。
特殊患者人群不推荐二甲双胍格列吡嗪片在妊娠期或儿童患者中使用。
由于存在肾功能降低的可能性,二甲双胍格列吡嗪片在老年患者中应采用保守的初始及维持剂量,任何剂量调整前都应该对肾功能进行评估,一般情况下,老年患者、过度疲劳以及营养不良的患者不得将剂量增大至大给药剂量以避免发生低血糖的风险。
特别在老年患者中,必须对肾功能进行监测以防止出现与二甲双胍相关的乳酸性酸中毒症(见警告)。
【不良反应】大于5%的临床不良反应有上呼吸道感染、腹泻、眩晕、高血压、恶心、呕吐。
格列吡嗪片

泰洛平(盐酸吡格列酮胶囊)【药品名称】商品名称:泰洛平通用名称:盐酸吡格列酮胶囊英文名称:Nimodipine for Injection【成份】本品主要成份为盐酸吡格列酮化学名为(±)5-[4-[2-(5-乙基-2-吡啶)乙氧基]苯甲基] -2, 4-噻唑烷二酮盐酸盐分子式:C19H20N2O3S·HCl分子量:392.90【适应症】2型糖尿病(或非胰岛素依赖性糖尿病,NIDDM)。
【用法用量】起始剂量15或30mg,最大剂量为45mg·d-1,qd。
在早餐前服用,如漏服1次,d2不可用双倍剂量。
联合治疗:磺脲:与磺脲类药物合用时,本品初始剂量可为1片或2片,每日一次。
磺脲类药物剂量可维持不变,当发生低血糖时,应减少磺脲类药物的使用。
二甲双胍:与二甲双胍类药物联合使用时,本品的初始剂量可为1片或2片,二甲双胍类药物可维持不变。
一般而言,二甲双胍无需降低剂量也不会引起低血糖。
胰岛素:与胰岛素合用时,本品的初始剂量可为1片或2片,胰岛素剂量可维持不变,当出现低血糖或血糖浓度降低至100mg/分升以下时,可降低胰岛素用量10%-25%,根据个体情况进行调整。
【不良反应】1.低血糖。
2.吡格列酮组贫血症发生率为1.0%,安慰剂组为0。
与胰岛素联合用药,吡格列酮组与安慰剂组贫血症发生率均为1.6%。
与磺酰脲类联合治疗,吡格列酮组贫血症发生率为0.3%,安慰剂组为1.6%。
与二甲双胍联合治疗,吡格列酮组贫血症发生率为1.2%,安慰剂组为0。
血红蛋白平均降低2%~4%。
3.浮肿。
4.可能引起血浆容积增加,终致前负荷诱导型心脏肥大。
5.ALT升高,吡格列酮组有0.26%(4/1526)的患者、安慰剂组有0.25(2/793)的患者ALT水平≥正常上限的3倍。
偶尔出现肌酸激【禁忌】对本品或制剂成分过敏的患者禁作。
【注意事项】1.本品只有在胰岛素存在情况下才发挥抗高血糖的作用,因此,不适用于I型糖尿病患者或糖尿病酮酸中毒的患者。
13格列吡嗪片原研处方工艺分析
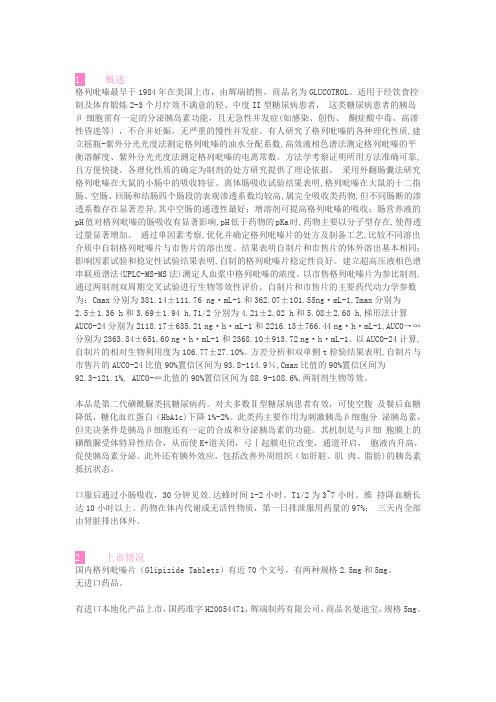
1.概述格列吡嗪最早于1984年在美国上市,由辉瑞销售,商品名为GLUCOTROL。
适用于经饮食控制及体育锻炼2-3个月疗效不满意的轻、中度II型糖尿病患者,这类糖尿病患者的胰岛β细胞需有一定的分泌胰岛素功能,且无急性并发症(如感染、创伤、酮症酸中毒、高渗性昏迷等〕,不合并妊娠,无严重的慢性并发症。
有人研究了格列吡嗪的各种理化性质,建立摇瓶-紫外分光光度法测定格列吡嗪的油水分配系数,高效液相色谱法测定格列吡嗪的平衡溶解度、紫外分光光度法测定格列吡嗪的电离常数。
方法学考察证明所用方法准确可靠,且方便快捷。
各理化性质的确定为制剂的处方研究提供了理论依据。
采用外翻肠囊法研究格列吡嗪在大鼠的小肠中的吸收特征。
离体肠吸收试验结果表明,格列吡嗪在大鼠的十二指肠、空肠、回肠和结肠四个肠段的表观渗透系数均较高,属完全吸收类药物,但不同肠断的渗透系数存在显著差异,其中空肠的通透性最好;增溶剂可提高格列吡嗪的吸收;肠营养液的pH值对格列吡嗪的肠吸收有显著影响,pH低于药物的pKa时,药物主要以分子型存在,使得透过量显著增加。
通过单因素考察,优化并确定格列吡嗪片的处方及制备工艺,比较不同溶出介质中自制格列吡嗪片与市售片的溶出度。
结果表明自制片和市售片的体外溶出基本相同;影响因素试验和稳定性试验结果表明,自制的格列吡嗪片稳定性良好。
建立超高压液相色谱串联质谱法(UPLC-MS-MS法)测定人血浆中格列吡嗪的浓度。
以市售格列吡嗪片为参比制剂,通过两制剂双周期交叉试验进行生物等效性评价。
自制片和市售片的主要药代动力学参数为:Cmax分别为381.14±111.76 ng·mL-1和362.07±101.55ng·mL-1,Tmax分别为2.5±1.36 h和3.69±1.94 h,T1/2分别为4.21±2.02 h和5.08±2.60 h,梯形法计算AUC0-24分别为2118.17±635.21 ng·h·mL-1和2216.13±766.44 ng·h·mL-1,AUC0→∞分别为2363.84±651.60 ng·h·mL-1和2368.10±913.72 ng·h·mL-1。
常顺药业格列吡嗪使用说明

常顺药业格列吡嗪【品牌】常顺药业:【用法用量】1.口服开始2.5mg,早餐前或早餐及午餐前各1次,也可1.25mg,一日3次,三餐前服,必要时7日后递增每日2.5mg。
2.一般每日剂量为5~15mg,最大剂量每日不超过20~30mg。
3.本品2.5mg作用相当甲苯磺丁脲0.5g。
4.在磺酰脲类药物中,本品胃肠吸收最快,最高药效时间与进餐后血糖升高高峰时间最一致,因此引起下餐前低血糖反应的机会较少,半衰期较短,引起严重持久的低血糖危险性在磺酰脲类药物中较小。
【注意事项】1.病人用药时应遵医嘱,注意饮食控制和用药时间。
2.下列情况应慎用:体质虚弱、高热、恶心和呕吐、有肾上腺皮质功能减退或垂体前叶功能减退症者。
3.用药期间应定期测血糖、尿糖、尿酮体、尿蛋白和肝、肾功能、血象,并进行眼科检查。
4.避免饮酒,以免引起类戒断反应。
【不良反应】1.较常见的为肠胃道症状(如恶心,上腹胀满)、头痛等,减少剂量即可缓解。
2.个别患者可出现皮肤过敏。
3.偶见低血糖,尤其是年老体弱者、活动过度者、不规则进食、饮酒或肝功能损害者。
4.亦偶见造血系统可逆性变化的报道。
【禁忌】下列患者禁用:1.对磺胺药过敏者。
2.已明确诊断的1型糖尿病患者。
3.2型糖尿病患者伴有酮症酸中毒、昏迷、严重烧伤、感染、外伤和重大手术等应激情况。
4.肝、肾功能不全者。
5.白细胞减少的病人。
【适应症】适用于经饮食控制及体育锻炼2~3个月疗效不满意的轻、中度2型糖尿病患者,这类糖尿病患者的胰岛β细胞需有一定的分泌胰岛素功能,且无急性并发症(如感染、创伤、酮症酸中毒、高渗性昏迷等),不合并妊娠,无严重的慢性并发症。
【药物相互作用】1.本药与双香豆素类、单胺氧化酶抑制剂、保泰松、磺胺类药、氯霉素、环磷酰胺、丙磺舒、水杨酸类药合用可增加其降血糖作用。
2.与肾上腺素、肾上腺皮质激素、口服避孕药、噻嗪类利尿剂合并使用时,可降低其降血糖作用。
3.与β-阻断药并用时应谨慎。
二甲双胍格列吡嗪片有效性及安全性评价
【结构式】
分子式:C21H33N5O4S 分子量:451.5828
【适应症】 中度或较重度的2型糖尿病患 【开发商】 辉瑞制药有限公司
第6页,共46页。
格列吡嗪
【简介】 本品属第二代磺酰脲类药物,由辉瑞制药有限公司研制,现在国内 已有公司生产。本品口服吸收迅速,1小时血药浓度达峰。肝脏代谢,代谢物无 活性,经肾排泄。降糖作用仅次于格列本脲,但因不易积蓄,较为安全。适用 于中度或较重度的2型糖尿病及老年患者,特别是餐后血糖控制不佳者。
第13页,共46页。
Company LOGO
实验方法
4、色谱条件 色谱柱:C18(4.6nun*250mm,sum,Dikma公司); 流动相:甲醇-0.01mol/ L磷酸二氢胺缓冲液(以磷酸调PH 值至3.5)(60 :40); 流速:1.2 mL / min;
检测波长:λ=275nm;
柱温:室温; 进样:20μL
第31页,共46页。
Company 任何在人体(病人或健康志愿者)进行药 物的系统性研究,以证实或揭示试验药物的作用、不良 反应及/或试验药物的吸收、分布、代谢和排泄,目的是 确定试验药物的疗效与安全性。
第32页,共46页。
Company LOGO
临床试验一般分为I、II、III和Ⅵ期临床试验
第3页,共46页。
二甲双胍
【通用名】 Metformin Hydrochloride
【商品名】 Metformin Hydrochloride Sustained-
Release Tablets
【化学名】 11,1-Dimethylbiguanide hydrochloride
【CAS登录号】 1115-70-4 (15537-72-1)
格列吡嗪片说明书

核准日期: 2008年05月09日修改日期: 2009年07月08日;2010年10月01日格列吡嗪片说明书请仔细阅读说明书并在医师指导下使用【药品名称】通用名称:格列吡嗪片商品名称:曼迪宝英文名称:Glipizide Tablets汉语拼音:Geliebiqin Pian【成份】本品主要成份为格列吡嗪。
化学名称:5-甲基-N-[2-[4-[[[(环己氨基)羰基]氨基]磺酰基]苯基]乙基]-吡嗪甲酰胺。
化学结构式:分子式:C 21H 27N 5O 4S分子量:445.54【性状】本品为白色片。
【适应症】 非胰岛素依赖型糖尿病。
仅用于单用饮食控制无满意效果的轻、中度非胰岛素依赖型糖尿病(2型),并且无严重糖尿病并发症的患者。
【规格】5mg【用法用量】 N N NH S NH N H H 3O O O O口服。
剂量因人而异,餐前30分钟服用。
单用饮食疗法失败者:起始剂量一日2.5~5.0mg,以后根据血糖和尿糖情况增减剂量,每次增减2.5~5.0mg,一日最大剂量不超过20~30mg,分2~3次餐前服用。
已使用过口服磺脲类降糖药治疗者:停用其他磺脲药3天,复查血糖后开始服用本品。
从5mg起逐渐加大剂量,直至产生理想的疗效。
最大日剂量不超过30mg。
【不良反应】与其它磺脲类药相似。
较常见的为胃肠道症状(如上腹涨满感)头痛等,减少剂量即可缓解。
个别患者可出现皮肤过敏、皮疹。
使用本品偶见能引起低血糖,尤其是年老体弱者、活动过度者、不规则进食、饮酒或肝肾功能损害者。
此外亦偶见造血系统可逆性变化的报道,如粒细胞、血小板减少等。
【禁忌】胰岛素依赖型糖尿病、糖尿病酮症、糖尿病昏迷前期或昏迷者、孕妇、有严重肝肾功能不全、肾上腺功能不全及对本品过敏者禁用。
对磺胺过敏者禁用。
在手术时、外伤及严重感染时禁用。
【注意事项】病人用药时应遵医嘱,注意饮食和用药时间。
如漏服一次要尽快补上,如已接近下次服药时间不要加倍用药。
治疗中注意早期出现的低血糖症状:头痛、兴奋、失眠、震颤和大量出汗,以便及时采取措施,严重者应静滴葡萄糖液。
格列吡嗪控释片的功能主治

格列吡嗪控释片的功能主治1. 什么是格列吡嗪控释片格列吡嗪控释片是一种口服药物,其主要成分是格列吡嗪。
格列吡嗪是一种非嗜铬降糖药物,属于二甲双胍类药物。
它通过降低肝脏的糖原合成、抑制肠道对葡萄糖的吸收以及提高外周组织对葡萄糖的利用等作用,能够有效降低血糖水平,用于控制糖尿病患者的血糖。
2. 格列吡嗪控释片的主要功能格列吡嗪控释片的主要功能是降低血糖水平,控制糖尿病患者的血糖。
具体功能主治如下:2.1 控制血糖格列吡嗪通过抑制肝脏的糖原合成,减少肝脏释放葡萄糖到血液中;同时抑制肠道对葡萄糖的吸收,降低葡萄糖的入血速度;此外,格列吡嗪还能增加外周组织对葡萄糖的利用能力,促进细胞对葡萄糖的摄取和利用。
这些作用都能够有效降低血糖的水平。
2.2 延缓糖尿病进展格列吡嗪不仅能够降低血糖水平,还能够改善胰岛功能,增强胰岛素的分泌能力。
胰岛素是调节血糖的重要激素,能够促进细胞对葡萄糖的摄取和利用。
通过增强胰岛素的分泌,格列吡嗪能够更好地控制血糖,并延缓糖尿病的进展。
2.3 降低胰岛素抵抗胰岛素抵抗是糖尿病的主要病理特征之一,也是导致高血糖的原因之一。
格列吡嗪具有降低胰岛素抵抗的作用,能够减少细胞对胰岛素的抵抗程度,从而提高胰岛素的效果。
通过降低胰岛素抵抗,格列吡嗪能够更好地控制血糖水平。
2.4 保护心脏血管糖尿病患者往往伴有心血管并发症的风险增加。
格列吡嗪能够通过改善胰岛素抵抗、调节血脂和减少血小板聚集等作用,保护心脏血管,降低心血管事件的风险。
3. 注意事项使用格列吡嗪控释片时需要注意以下事项:•请按医生的建议使用药物,不要随意更改剂量或停药。
•如果出现药物不良反应如恶心、腹泻、头痛等,请及时告知医生。
•药物治疗期间需要定期监测血糖水平和肝肾功能。
•药物使用过程中需注意饮食控制和合理运动,以配合药物的降糖效果。
•不适合孕妇、哺乳期妇女和严重肝肾功能不全患者使用。
4. 总结格列吡嗪控释片是一种用于控制糖尿病患者血糖的药物。
格列吡嗪片(灭特尼)的说明书

格列吡嗪片(灭特尼)的说明书糖尿病是世界上慢性疾病当中最为严重的疾病之一,每年因为糖尿病而失去生命的人不在少数。
血糖升高会影响人体的各种器官发生病变,严重的会堵塞血管直接导致人体死亡。
因此治疗刻不容缓,目前治疗糖尿病的药物当中有一种叫做格列吡嗪片(灭特尼)的药物,它对于糖尿病的治疗效果特别显著,患者无需担心副作用等问题。
【药品名称】通用名称:格列吡嗪片商品名称:格列吡嗪片(灭特尼)拼音全码:GeLieBiQinPian(MieTeNi)【适应症/功能主治】适用于经饮食控制及体育锻炼2~3个月疗效不满意的轻、中度2型糖尿病者,这类糖尿病患者的胰岛细胞需有一定的分泌胰岛素功能,且无急性并发症(如感染、创伤、酮症酸中毒、高渗性昏迷等),不合并妊娠,无严重【规格型号】5mg*48s【用法用量】口服剂量因人而异,一般推荐剂量2.5~20mg/日,早餐前30分钟服用。
日剂量超过15mg,宜在早、【不良反应】1.较常见的为肠胃道症状(如恶心,上腹胀满)、头痛等,减少剂量即可缓解。
2.个别患者可出现皮肤过敏。
3.偶见低血糖,尤其是年老体弱者、活动过度者、不规则进食、饮酒或肝功能损害者,4.亦偶见造血系统可逆性变化的报道。
【注意事项】1.病人用药时应遵医嘱,注意饮食控制和用药时间。
2.治疗中注意早期出现的低血糖症状:头痛、兴奋、失眠、震颤和大量出汗,以便及时采取措施,严重者应静滴葡萄糖液。
对有创伤、术后感染或发热的病人应给予胰岛素,以维持正常血糖代谢。
3.避免饮酒,以免引起类戒断反应。
【有效期】24 月【批准文号】国药准字H10983110【生产企业】珠海联邦制药股份有限公司中山分公司【英文名】Glipizide Tablets【商品名】灭特尼【通用名】格列吡嗪片【主要成份】格列吡嗪。
【性状】本品为白色片,在水中迅速崩解。
【规格】5mg【剂型】片剂【药理作用】本品是第二代磺酰脲类口服降糖药。
能促进胰岛β细胞分泌胰岛素、增强胰岛素对靶组织的作用;亦能刺激胰岛α细胞使胰高血糖素分泌受抑制,尚有抑制肝糖原分解,促进肌肉利用和消耗葡萄糖的作用。
格列吡嗪片的作用与功效

格列吡嗪片的作用与功效格列吡嗪片是一种广泛使用的药物,被用来治疗多种不同的疾病和症状。
本文将详细介绍格列吡嗪片的作用与功效。
格列吡嗪片的学名为Glibenclamide,是一种二磺胺类口服降糖药物,也被称为磺脲类降糖药物。
它被用来治疗糖尿病,特别是2型糖尿病。
格列吡嗪片的主要作用机制是通过增强胰岛素的释放来降低血糖水平。
格列吡嗪片的作用机制是通过作用于胰岛β细胞上ATP敏感的钾通道,阻断钾离子的外流,使得细胞内钾离子浓度升高,从而引发胰岛细胞体膜上的钙离子通道开放,促使胰岛素释放。
格列吡嗪片还可以增加胰岛素的灵敏性,增强胰岛素的作用,降低外周组织对胰岛素的耐受性,从而达到减少血糖水平的效果。
格列吡嗪片的主要功效是降低血糖水平,控制糖尿病症状。
格列吡嗪片可以通过减少肝糖异生,增加胰岛素的释放和减少外周耐糖激素的影响来降低血糖水平。
通过控制血糖水平,格列吡嗪片还可以预防和缓解与高血糖相关的并发症,如糖尿病视网膜病变、糖尿病肾病、糖尿病神经病变等。
除了降低血糖水平,格列吡嗪片还具有其他一些功效。
首先,格列吡嗪片可以改善胰岛素的代谢和吸收,提高胰岛素的利用率。
其次,格列吡嗪片还可以促进糖原合成和储存,增加肝脏和肌肉对糖的储存能力,从而减少高血糖发生的可能性。
此外,格列吡嗪片还可以抑制胰高血糖素的分泌,降低血糖水平。
最后,格列吡嗪片还具有保护胰岛细胞和改善β细胞功能的作用,有助于慢性糖尿病的治疗和预防。
除了上述常见的糖尿病治疗外,格列吡嗪片还可以用于其他一些疾病和症状。
例如,格列吡嗪片可以用于治疗妊娠期糖尿病,妊娠期糖尿病是指妊娠期间发生的糖尿病。
此外,格列吡嗪片还被用于处理继发于某些胰岛细胞瘤的低血糖症。
胰岛细胞瘤是一种罕见的胰岛细胞肿瘤,会导致胰岛素过度分泌,从而引起低血糖。
然而,格列吡嗪片也有一些不良反应和禁忌症。
常见的不良反应包括低血糖、恶心、呕吐、腹泻等胃肠道反应。
罕见但严重的副作用包括过敏反应、肝功能损害、血细胞减少等。
格列吡嗪说明书
【药物名称】中文通用名称:格列吡嗪英文通用名称:Glipizide其他名称:安达、吡磺环己脲、吡磺环乙脲、迪沙、格迪、格列甲嗪、格列匹散得、减糖尿、捷贝、蓝绿康、力达美、利糖妥、洛厄尔巴、麦林格、美吡达、美迪宝、泌乐得、灭糖尿、灭特尼、秦苏、瑞易宁、思东克、思乐克、唐贝克、天糖尿、依必达、怡平、优哒灵、元坦、智唐、Digrin、Glibenese、Glibense、Glidiab、Glipizid、Glipizidum、Glipzide、Glutrol、Glydiazinamide、Lanokan、Meibida、Meibide、Melizid、Mindiab、Minidiab、Ministab、Minodiab、Mitoneu、Ozidia。
【临床应用】用于经饮食控制及体育锻炼疗效不满意的轻、中度2型糖尿病患者。
【药理】1.药效学本药为第二代磺酰脲类口服降血糖药,对胰岛β细胞有一定胰岛素分泌功能的2型糖尿病患者有效。
作用机制参见“格列本脲”的“药效学”。
2.药动学在磺酰脲类药物中,本药胃肠吸收较快,最高药效时间与进餐后血糖达高峰的时间较一致。
主要经肝脏代谢,代谢产物无药理活性。
普通片:口服后1-2.5小时达血药峰浓度(C),消除半衰期为3-7小时。
65%-80%max的药物经尿液排出,10%-15%从粪便排出,第1日排出97%,第2日全部排出。
[约为(1.38±0.20)μg/ml],半分散片:健康成人口服10mg,约2.5小时达Cmax衰期约为(9.95±1.04)小时。
控释片:口服后2小时开始稳定地释放有效成分,可维持稳定释放约8小时。
以后释放速度逐渐下降,至服药后约16小时释放完毕。
服药后24小时内可保持较稳定的血药浓度。
一次口服5mg后,24小时平均血药浓度可达50ng/ml以上。
消除半衰期为2.5-4小时。
服药5日后,血药浓度达稳态,老年患者达稳态时间需6-7日。
二甲双胍格列吡嗪片
二甲双胍格列吡嗪片【药品名称】通用名称:二甲双胍格列吡嗪片英文名称:Metformin Hydrochloride and Glipizide Tablets【成份】格列吡嗪2.5mg/ 盐酸二甲双胍250mg【适应症】单独使用本品,建议联合饮食及运动疗法,达到控制非胰岛素依赖型(2型)糖尿病血糖的作用。
本品还可和磺脲类降糖药或胰岛素合并用以控制2型。
【用法用量】2型糖尿病使用本品治疗高血糖时没有固定的剂量。
在不超过最大推荐剂量,即2000毫克/日的情况下,剂量根据作用和耐受必须个体化。
本品通常随晚餐单次服药,为了减少胃肠道并发症的发生,也为了使用最小剂量的药物使患者的血糖足以控制,应从小剂量开始服用,逐渐增加剂量。
治疗开始和调整剂量期间(见推荐的服药计划),测定空腹血糖可用于确定本品治疗反应,以及确定患者最小的有效剂量。
此后,应每隔三月测定糖化血红蛋白,无论是单独使用,还是与磺脲类药物及胰岛素联合使用,治疗的目标都是使用最低的有效剂量使空腹血糖和糖化血红蛋白水平降至正常或接近正常水平。
监测血糖和糖化血红蛋白可以确定原发失效和继发失效,前者是指服用最大推荐剂量的药物仍不能有效降低血糖,而后者是指经过最初一段有效期后而丧失满意的降糖作用。
对于通常单纯饮食控制血糖良好而暂时血糖升高的患者,短期服用本品是有效的。
推荐服药计划成人- 通常,低于1500毫克/日的剂量时,临床上没有明显的反应。
但是为了减少胃肠道不良反应,建议从小量开始服用,逐渐增加剂量。
通常盐酸二甲双胍缓释片的起始剂量为500毫克,1次/日随晚餐服用。
每周剂量增加500毫克,最大剂量至2000毫克,1次/日随晚餐服用。
如果用至2000毫克,1次/日,血糖仍没控制满意,可以考虑改用1000毫克,2次/日试验性治疗。
如果还需要更大量的二甲双胍,应当使用盐酸二甲双胍片2550毫克/日的最大剂量,分次服用。
一项由使用盐酸二甲双胍片治疗转变为盐酸二甲双胍缓释片治疗的随机实验,结果提示,接受盐酸二甲双胍片治疗的患者可以安全的以相同剂量转换为盐酸二甲双胍缓释片1次/日的治疗,最高至2000毫克,1次/日,转变后要严密监测血糖,并相应调整剂量。
二甲双胍格列吡嗪片有效性与安全性评价

实验结果
3、非房室模型解析 采用统计矩的原理对体内血药浓度时曲线进 行非模型化解析,结果如表5,6所示,将两 制剂因素间各个非房室模型药动学参数进行 方差分析,结果表明:试验制剂与参比制剂 相比,两制剂得的体内平均滞留时间十分相 似,无显著性差异(P>0.1),说明二者具有
实验结果
4、相对生物利用度计算
实验方法
3、给药方案 3只Beagle犬采用双周期交叉试验,一组服用对照制剂5mg x l片, 一组服用实验制5mg x l粒,一周后进行交叉试验。采血时间均为: 0、1、2、3、4、5、6、8、10、12、16、24、36、48h。 分别取后肢静脉血2.5mL,于肝素化试管中,离心,分离血浆。血 浆预处理后,进HPLC分析,将所得的二甲双胍格列吡嗪与蔡普生 钠的色谱峰面积比值代入标准曲线,计算血药浓度值。
目录
二、有效性评价
1、类似2型糖尿病的动物模型的建立方法 2、二甲双胍格列吡嗪片在Beagle犬体内的药动 学研究 3、临床研究
类似2型糖尿病的动物模型的建立方法:
1、实验性肥胖及糖尿病大鼠模型 2、肥胖性胰岛素抵抗MSG动物模型 3、自发性乙型糖尿病动物
有五类动物,分别为:肥胖小鼠;糖尿病小鼠;KK小鼠(轻度肥胖型 糖尿病动物);NZO小鼠(表现为超体重、轻度高血糖及高胰岛素水平,早 期有胰岛素抵抗);Zucker fa/fa 大鼠(常染色体隐形基因的名称为fa) 。
糖尿病现状
盐酸二甲双胍和格列吡嗪是两种使用广泛、疗效好的口服降糖药,两 者联合用药,具有协同降糖作用。二甲双胍格列吡嗪片适用于患有高 血糖症而又不能单纯依赖食物和运动获得满意治疗的2型糖尿病人的初 步治疗;还适用于经食物、运动和单用磺酰脲类或二甲双胍初步治疗 均不能取得血糖过多适当控制的2 型糖尿病人的二线治疗。
格列吡嗪片

消渴灵片
【药品名称】
通用名称:消渴灵片
【成份】
地黄、黄芪、枸杞子、天花粉、麦冬、红参、茯苓、石膏、黄连、五味子、牡丹皮
【功能主治】
益气养阴,清热泻火,生津止渴。
用于气阴两虚所致的消渴病,症见多饮、多食、多尿、消瘦、气短乏力;2型轻型、中型糖尿病见上述证候者。
【用法用量】
口服。
一次8片,一日3次。
【不良反应】
偶见腹胀,一般不影响继续治疗。
【禁忌】
孕妇忌服。
【注意事项】
忌食辛辣。
【药物相互作用】
尚未明确
【药理作用】
具有降血糖、降血脂作用。
对实验性高血糖、高血脂家兔本品能降低其血清中糖、脂含量,对糖尿病高血糖小鼠,本品能保护β胰岛细胞,促进β细胞修复和再生,促进β细胞释放胰岛素。
【贮藏】
密闭,在凉暗处保存。
【批准文号】
国药准字Z22022016
【生产企业】
企业名称:吉林敖东洮南药业股份有限公司生产地址:吉林省洮南市团结东路16号。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
----------GLUCOTROL -glipizide tablet RoerigGLUCOTROL ®(glipizide)TABLETSFor Oral UseDESCRIPTIONGLUCOTROL (glipizide) is an oral blood-glucose-lowering drug of the sulfonylurea class.The Chemical Abstracts name of glipizide is 1-cyclohexyl-3-[[p-[2-(5-methylpyrazine-carboxamido)ethyl]phenyl]sulfonyl]urea. Themolecular formula is C21H 27N 5O 4S; the molecular weight is 445.55; the structural formula is shown below: Glipizide is a whitish, odorless powder with a pKa of 5.9. It is insoluble in water and alcohols, but soluble in 0.1N NaOH; it is freely soluble in dimethylformamide. GLUCOTROL tablets for oral use are available in 5 and 10 mg strengths.Inert ingredients are: colloidal silicon dioxide; lactose; microcrystalline cellulose; starch; stearic acid.CLINICAL PHARMACOLOGYMechanism of ActionThe primary mode of action of GLUCOTROL in experimental animals appears to be the stimulation of insulin secretion from the beta cells of pancreatic islet tissue and is thus dependent on functioning beta cells in the pancreatic islets. In humans GLUCOTROL appears to lower the blood glucose acutely by stimulating the release of insulin from the pancreas, an effect dependent uponfunctioning beta cells in the pancreatic islets. The mechanism by which GLUCOTROL lowers blood glucose during long-termadministration has not been clearly established. In man, stimulation of insulin secretion by GLUCOTROL in response to a meal isundoubtedly of major importance. Fasting insulin levels are not elevated even on long-term GLUCOTROL administration, but the postprandial insulin response continues to be enhanced after at least 6 months of treatment. The insulinotropic response to a meal occurs within 30 minutes after an oral dose of GLUCOTROL in diabetic patients, but elevated insulin levels do not persist beyond the time of the meal challenge. Extrapancreatic effects may play a part in the mechanism of action of oral sulfonylurea hypoglycemic drugs.Blood sugar control persists in some patients for up to 24 hours after a single dose of GLUCOTROL, even though plasma levels have declined to a small fraction of peak levels by that time (see Pharmacokinetics below). Some patients fail to respond initially, or gradually lose their responsiveness to sulfonylurea drugs, including GLUCOTROL. Alternatively, GLUCOTROL may be effective in some patients who have not responded or have ceased to respond to other sulfonylureas.Other Effects It has been shown that GLUCOTROL therapy was effective in controlling blood sugar without deleterious changes in the plasma lipoprotein profiles of patients treated for NIDDM. In a placebo-controlled, crossover study in normal volunteers, GLUCOTROL had no antidiuretic activity, and, in fact, led to a slight increase in free water clearance. PharmacokineticsGastrointestinal absorption of GLUCOTROL in man is uniform, rapid, and essentially complete. Peak plasma concentrations occur 1–3 hours after a single oral dose. The half-life of elimination ranges from 2–4 hours in normal subjects, whether given intravenously or orally. The metabolic and excretory patterns are similar with the two routes of administration, indicating that first-pass metabolism is not significant. GLUCOTROL does not accumulate in plasma on repeated oral administration. Total absorption and disposition of an oral dose was unaffected by food in normal volunteers, but absorption was delayed by about 40 minutes. Thus GLUCOTROL was more effective when administered about 30 minutes before, rather than with, a test meal in diabetic patients. Protein binding was studied in serum from volunteers who received either oral or intravenous GLUCOTROL and found to be 98–99% one hour after either route of administration. The apparent volume of distribution of GLUCOTROL after intravenous administration was 11 liters, indicative of localization within the extracellular fluid compartment. In mice no GLUCOTROL or metabolites were detectable autoradiographically in the brain or spinal cord of males or females, nor in the fetuses of pregnant females. In another study, however, very small amounts of radioactivity were detected in the fetuses of rats given labelled drug.The metabolism of GLUCOTROL is extensive and occurs mainly in the liver. The primary metabolites are inactive hydroxylation products and polar conjugates and are excreted mainly in the urine. Less than 10% unchanged GLUCOTROL is found in the urine. INDICATIONS AND USAGEGLUCOTROL is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus. CONTRAINDICATIONSGLUCOTROL is contraindicated in patients with:1. Known hypersensitivity to the drug.2. Type 1 diabetes mellitus, diabetic ketoacidosis, with or without coma. This condition should be treated with insulin.WARNINGSSPECIAL WARNING ON INCREASED RISK OF CARDIOVASCULAR MORTALITYThe administration of oral hypoglycemic drugs has been reported to be associated with increased cardiovascular mortalityas compared to treatment with diet alone or diet plus insulin. This warning is based on the study conducted by the University Group Diabetes Program (UGDP), a long-term prospective clinical trial designed to evaluate the effectiveness of glucose-lowering drugs in preventing or delaying vascular complications in patients with non-insulin-dependent diabetes. The study involved 823 patients who were randomly assigned to one of four treatment groups (Diabetes, 19, supp. 2: 747–830, 1970). UGDP reported that patients treated for 5 to 8 years with diet plus a fixed dose of tolbutamide (1.5 grams per day) hada rate of cardiovascular mortality approximately 2½ times that of patients treated with diet alone. A significant increasein total mortality was not observed, but the use of tolbutamide was discontinued based on the increase in cardiovascular mortality, thus limiting the opportunity for the study to show an increase in overall mortality. Despite controversy regarding the interpretation of these results, the findings of the UGDP study provide an adequate basis for this warning. The patient should be informed of the potential risks and advantages of GLUCOTROL and of alternative modes of therapy.Although only one drug in the sulfonylurea class (tolbutamide) was included in this study, it is prudent from a safety standpoint to consider that this warning may also apply to other oral hypoglycemic drugs in this class, in view of their close similarities in mode of action and chemical structure.PRECAUTIONSGeneralMacrovascular OutcomesThere have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with GLUCOTROL or any other anti-diabetic drug.Renal and Hepatic DiseaseThe metabolism and excretion of GLUCOTROL may be slowed in patients with impaired renal and/or hepatic function. If hypoglycemia should occur in such patients, it may be prolonged and appropriate management should be instituted. HypoglycemiaAll sulfonylurea drugs are capable of producing severe hypoglycemia. Proper patient selection, dosage, and instructions are important to avoid hypoglycemic episodes. Renal or hepatic insufficiency may cause elevated blood levels of GLUCOTROL and the lattermay also diminish gluconeogenic capacity, both of which increase the risk of serious hypoglycemic reactions. Elderly, debilitatedor malnourished patients, and those with adrenal or pituitary insufficiency, are particularly susceptible to the hypoglycemic actionof glucose-lowering drugs. Hypoglycemia may be difficult to recognize in the elderly, and in people who are taking beta-adrenergic blocking drugs. Hypoglycemia is more likely to occur when caloric intake is deficient, after severe or prolonged exercise, when alcohol is ingested, or when more than one glucose-lowering drug is used.Loss of Control of Blood GlucoseWhen a patient stabilized on any diabetic regimen is exposed to stress such as fever, trauma, infection, or surgery, a loss of control may occur. At such times, it may be necessary to discontinue GLUCOTROL and administer insulin.The effectiveness of any oral hypoglycemic drug, including GLUCOTROL, in lowering blood glucose to a desired level decreases in many patients over a period of time, which may be due to progression of the severity of the diabetes or to diminished responsiveness to the drug. This phenomenon is known as secondary failure, to distinguish it from primary failure in which the drug is ineffective in an individual patient when first given.Laboratory TestsBlood and urine glucose should be monitored periodically. Measurement of glycosylated hemoglobin may be useful.Information for PatientsPatients should be informed of the potential risks and advantages of GLUCOTROL and of alternative modes of therapy. They should also be informed about the importance of adhering to dietary instructions, of a regular exercise program, and of regular testing of urine and/or blood glucose.The risks of hypoglycemia, its symptoms and treatment, and conditions that predispose to its development should be explained to patients and responsible family members. Primary and secondary failure should also be explained.Physician Counseling Information for PatientsIn initiating treatment for type 2 diabetes, diet should be emphasized as the primary form of treatment. Caloric restriction and weight loss are essential in the obese diabetic patient. Proper dietary management alone may be effective in controlling the blood glucose and symptoms of hyperglycemia. The importance of regular physical activity should also be stressed, and cardiovascular risk factors should be identified and corrective measures taken where possible. Use of GLUCOTROL or other antidiabetic medications must be viewed by both the physician and patient as a treatment in addition to diet and not as a substitution or as a convenient mechanismfor avoiding dietary restraint. Furthermore, loss of blood glucose control on diet alone may be transient, thus requiring only short-term administration of GLUCOTROL or other antidiabetic medications. Maintenance or discontinuation of GLUCOTROL or other antidiabetic medications should be based on clinical judgment using regular clinical and laboratory evaluations.Drug InteractionsThe hypoglycemic action of sulfonylureas may be potentiated by certain drugs including nonsteroidal anti-inflammatory agents, some azoles, and other drugs that are highly protein bound, salicylates, sulfonamides, chloramphenicol, probenecid, coumarins, monoamine oxidase inhibitors, and beta adrenergic blocking agents. When such drugs are administered to a patient receiving GLUCOTROL, the patient should be observed closely for hypoglycemia. When such drugs are withdrawn from a patient receiving GLUCOTROL, the patient should be observed closely for loss of control. In vitro binding studies with human serum proteins indicate that GLUCOTROL binds differently than tolbutamide and does not interact with salicylate or dicumarol. However, caution must be exercised in extrapolating these findings to the clinical situation and in the use of GLUCOTROL with these drugs.Certain drugs tend to produce hyperglycemia and may lead to loss of control. These drugs include the thiazides and other diuretics, corticosteroids, phenothiazines, thyroid products, estrogens, oral contraceptives, phenytoin, nicotinic acid, sympathomimetics, calcium channel blocking drugs, and isoniazid. When such drugs are administered to a patient receiving GLUCOTROL, the patient should be closely observed for loss of control. When such drugs are withdrawn from a patient receiving GLUCOTROL, the patient should be observed closely for hypoglycemia.A potential interaction between oral miconazole and oral hypoglycemic agents leading to severe hypoglycemia has been reported. Whether this interaction also occurs with the intravenous, topical, or vaginal preparations of miconazole is not known. The effectof concomitant administration of DIFLUCAN® (fluconazole) and GLUCOTROL has been demonstrated in a placebo-controlled crossover study in normal volunteers. All subjects received GLUCOTROL alone and following treatment with 100 mg of DIFLUCAN as a single daily oral dose for 7 days. The mean percentage increase in the GLUCOTROL AUC after fluconazole administration was 56.9% (range: 35 to 81).Carcinogenesis, Mutagenesis, Impairment of FertilityA twenty month study in rats and an eighteen month study in mice at doses up to 75 times the maximum human dose revealed no evidence of drug-related carcinogenicity. Bacterial and in vivo mutagenicity tests were uniformly negative. Studies in rats of both sexes at doses up to 75 times the human dose showed no effects on fertility.PregnancyPregnancy Category CGLUCOTROL (glipizide) was found to be mildly fetotoxic in rat reproductive studies at all dose levels (5–50 mg/kg). This fetotoxicity has been similarly noted with other sulfonylureas, such as tolbutamide and tolazamide. The effect is perinatal and believed to be directly related to the pharmacologic (hypoglycemic) action of GLUCOTROL. In studies in rats and rabbits no teratogenic effects were found. There are no adequate and well controlled studies in pregnant women. GLUCOTROL should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.Because recent information suggests that abnormal blood glucose levels during pregnancy are associated with a higher incidence of congenital abnormalities, many experts recommend that insulin be used during pregnancy to maintain blood glucose levels as close to normal as possible.Nonteratogenic EffectsProlonged severe hypoglycemia (4 to 10 days) has been reported in neonates born to mothers who were receiving a sulfonylurea drug at the time of delivery. This has been reported more frequently with the use of agents with prolonged half-lives. If GLUCOTROL is used during pregnancy, it should be discontinued at least one month before the expected delivery date.Nursing MothersAlthough it is not known whether GLUCOTROL is excreted in human milk, some sulfonylurea drugs are known to be excreted in human milk. Because the potential for hypoglycemia in nursing infants may exist, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother. If the drug is discontinued and if diet alone is inadequate for controlling blood glucose, insulin therapy should be considered.Pediatric UseSafety and effectiveness in children have not been established.Geriatric UseA determination has not been made whether controlled clinical studies of GLUCOTROL included sufficient numbers of subjects aged65 and over to define a difference in response from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal or cardiac function, and of concomitant disease or other drug therapy.ADVERSE REACTIONSIn U.S. and foreign controlled studies, the frequency of serious adverse reactions reported was very low. Of 702 patients, 11.8% reported adverse reactions and in only 1.5% was GLUCOTROL discontinued.HypoglycemiaSee PRECAUTIONS and OVERDOSAGE sections.GastrointestinalGastrointestinal disturbances are the most common reactions. Gastrointestinal complaints were reported with the following approximate incidence: nausea and diarrhea, one in seventy; constipation and gastralgia, one in one hundred. They appear to bedose-related and may disappear on division or reduction of dosage. Cholestatic jaundice may occur rarely with sulfonylureas: GLUCOTROL should be discontinued if this occurs.DermatologicAllergic skin reactions including erythema, morbilliform or maculopapular eruptions, urticaria, pruritus, and eczema have been reported in about one in seventy patients. These may be transient and may disappear despite continued use of GLUCOTROL; if skin reactions persist, the drug should be discontinued. Porphyria cutanea tarda and photosensitivity reactions have been reported with sulfonylureas.HematologicLeukopenia, agranulocytosis, thrombocytopenia, hemolytic anemia, aplastic anemia, and pancytopenia have been reported with sulfonylureas.MetabolicHepatic porphyria and disulfiram-like reactions have been reported with sulfonylureas. In the mouse, GLUCOTROL pretreatment did not cause an accumulation of acetaldehyde after ethanol administration. Clinical experience to date has shown that GLUCOTROL has an extremely low incidence of disulfiram-like alcohol reactions.Endocrine ReactionsCases of hyponatremia and the syndrome of inappropriate antidiuretic hormone (SIADH) secretion have been reported with this and other sulfonylureas.MiscellaneousDizziness, drowsiness, and headache have each been reported in about one in fifty patients treated with GLUCOTROL. They are usually transient and seldom require discontinuance of therapy.Laboratory TestsThe pattern of laboratory test abnormalities observed with GLUCOTROL was similar to that for other sulfonylureas. Occasional mild to moderate elevations of SGOT, LDH, alkaline phosphatase, BUN and creatinine were noted. One case of jaundice was reported. The relationship of these abnormalities to GLUCOTROL is uncertain, and they have rarely been associated with clinical symptoms.OVERDOSAGEThere is no well documented experience with GLUCOTROL overdosage. The acute oral toxicity was extremely low in all species tested (LD50 greater than 4 g/kg).Overdosage of sulfonylureas including GLUCOTROL can produce hypoglycemia. Mild hypoglycemic symptoms without loss of consciousness or neurologic findings should be treated aggressively with oral glucose and adjustments in drug dosage and/or meal patterns. Close monitoring should continue until the physician is assured that the patient is out of danger. Severe hypoglycemic reactions with coma, seizure, or other neurological impairment occur infrequently, but constitute medical emergencies requiring immediate hospitalization. If hypoglycemic coma is diagnosed or suspected, the patient should be given a rapid intravenous injection of concentrated (50%) glucose solution. This should be followed by a continuous infusion of a more dilute (10%) glucose solution at a rate that will maintain the blood glucose at a level above 100 mg/dL. Patients should be closely monitored for a minimum of 24 to 48 hours since hypoglycemia may recur after apparent clinical recovery. Clearance of GLUCOTROL from plasma would be prolonged in persons with liver disease. Because of the extensive protein binding of GLUCOTROL, dialysis is unlikely to be of benefit. DOSAGE AND ADMINISTRATIONThere is no fixed dosage regimen for the management of diabetes mellitus with GLUCOTROL or any other hypoglycemic agent.In addition to the usual monitoring of urinary glucose, the patient's blood glucose must also be monitored periodically to determine the minimum effective dose for the patient; to detect primary failure, i.e., inadequate lowering of blood glucose at the maximum recommended dose of medication; and to detect secondary failure, i.e., loss of an adequate blood-glucose-lowering response after an initial period of effectiveness. Glycosylated hemoglobin levels may also be of value in monitoring the patient's response to therapy. Short-term administration of GLUCOTROL may be sufficient during periods of transient loss of control in patients usually controlled well on diet.In general, GLUCOTROL should be given approximately 30 minutes before a meal to achieve the greatest reduction in postprandial hyperglycemia.Initial DoseThe recommended starting dose is 5 mg, given before breakfast. Geriatric patients or those with liver disease may be started on 2.5 mg.TitrationDosage adjustments should ordinarily be in increments of 2.5–5 mg, as determined by blood glucose response. At least severaldays should elapse between titration steps. If response to a single dose is not satisfactory, dividing that dose may prove effective.The maximum recommended once daily dose is 15 mg. Doses above 15 mg should ordinarily be divided and given before meals of adequate caloric content. The maximum recommended total daily dose is 40 mg.MaintenanceSome patients may be effectively controlled on a once-a-day regimen, while others show better response with divided dosing. Total daily doses above 15 mg should ordinarily be divided. Total daily doses above 30 mg have been safely given on a b.i.d. basis to long-term patients.In elderly patients, debilitated or malnourished patients, and patients with impaired renal or hepatic function, the initial and maintenance dosing should be conservative to avoid hypoglycemic reactions (see PRECAUTIONS section).Patients Receiving InsulinAs with other sulfonylurea-class hypoglycemics, many stable non-insulin-dependent diabetic patients receiving insulin may be safely placed on GLUCOTROL. When transferring patients from insulin to GLUCOTROL, the following general guidelines should be considered:For patients whose daily insulin requirement is 20 units or less, insulin may be discontinued and GLUCOTROL therapy may begin at usual dosages. Several days should elapse between GLUCOTROL titration steps.For patients whose daily insulin requirement is greater than 20 units, the insulin dose should be reduced by 50% andGLUCOTROL therapy may begin at usual dosages. Subsequent reductions in insulin dosage should depend on individual patient response. Several days should elapse between GLUCOTROL titration steps.During the insulin withdrawal period, the patient should test urine samples for sugar and ketone bodies at least three times daily. Patients should be instructed to contact the prescriber immediately if these tests are abnormal. In some cases, especially when patient has been receiving greater than 40 units of insulin daily, it may be advisable to consider hospitalization during the transition period.Patients Receiving Other Oral Hypoglycemic AgentsAs with other sulfonylurea-class hypoglycemics, no transition period is necessary when transferring patients to GLUCOTROL. Patients should be observed carefully (1–2 weeks) for hypoglycemia when being transferred from longer half-life sulfonylureas (e.g., chlorpropamide) to GLUCOTROL due to potential overlapping of drug effect.HOW SUPPLIEDGLUCOTROL tablets are white, dye-free, scored, diamond-shaped, and imprinted as follows:5 mg–Pfizer 411; 10 mg–Pfizer 412.5 mg Bottles: 100's (NDC 0049-4110-66) (NDC 59012-411-66);500's (NDC 0049-4110-73) (NDC 59012-411-73);UNIT DOSE 100's (NDC 0049-4110-41) (NDC 59012-411-41).10 mg Bottles: 100's (NDC 0049-4120-66) (NDC 59012-412-66);500's (NDC 0049-4120-73) (NDC 59012-412-73);UNIT DOSE 100's (NDC 0049-4120-41) (NDC 59012-412-41).RECOMMENDED STORAGEStore below 86°F (30°C).Rx onlyLAB-0114-2.4September 2008。