《罕见病诊疗指南(2019年版)》要点6
《罕见病诊疗指南(2019年版)》要点 (1)
《罕见病诊疗指南(2019年版)》要点(1)总目录1.21-羟化酶缺乏症2.白化病3.奥尔波特综合征4.肌萎缩侧索硬化5.天使综合征6.精氨酸酶缺乏症7.窒息性胸腔失养症(热纳综合征)8.非典型溶血性尿毒症综合征9.自身免疫性脑炎10.自身免疫性垂体炎11.自身免疫性胰岛素受体病12.β-酮硫解酶缺乏症13.生物素酶缺乏症14.心脏离子通道病15.原发性肉碱缺乏症16.Castleman病17.腓骨肌萎缩症18.瓜氨酸血症19.先天性肾上腺发育不良20.先天性高胰岛素性低血糖血症21.先天性肌无力综合征22.先天性肌强直23.先天性脊柱侧凸24.冠状动脉扩张25.先天性纯红细胞再生障碍性贫血26.Erdheim-Chester 病27.法布里病28.家族性地中海热29.范科尼贫血30.半乳糖血症31.戈谢病32.全身型重症肌无力33.Gitelman 综合征34.戊二酸血症型35.糖原累积病(型、型)36.血友病37.肝豆状核变性38.遗传性血管性水肿//39.遗传性大疱性表皮松解症40.遗传性果糖不耐受症41.遗传性低镁血症42.遗传性多发脑梗死性痴呆43.遗传性痉挛性截瘫44.全羧化酶合成酶缺乏症45.高同型半胱氨酸血症46.纯合子家族性高胆固醇血症47.亨廷顿病48.HHH 综合征(高鸟氨酸血症-高氨血症-同型瓜氨酸尿症)49.高苯丙氨酸血症50.低磷酸酯酶症51.低血磷性佝偻病52.特发性心肌病53.特发性低促性腺激素性性腺功能减退症54.特发性肺动脉高压55.特发性肺纤维化56.IgG4 相关性疾病57.先天性胆汁酸合成障碍58.异戊酸血症59.卡尔曼综合征60.朗格汉斯细胞组织细胞增生症61.莱伦综合征62.Leber 遗传性视神经病变63.长链-3-羟酰基辅酶A 脱氢酶缺乏症64.淋巴管肌瘤病65.赖氨酸尿蛋白不耐受症66.溶酶体酸性脂肪酶缺乏症67.枫糖尿症68.马方综合征69.McCune-Albright 综合征70.中链酰基辅酶A 脱氢酶缺乏症71.甲基丙二酸血症72.线粒体脑肌病73.黏多糖贮积症74.多灶性运动神经病75.多种酰基辅酶A 脱氢酶缺乏症76.多发性硬化77.多系统萎缩78.强直性肌营养不良79.N-乙酰谷氨酸合成酶缺乏症80.新生儿糖尿病81.视神经脊髓炎82.尼曼匹克病83.非综合征型耳聋84.努南综合征85.鸟氨酸氨甲酰基转移酶缺乏症86.成骨不全症87.帕金森病(青年型、早发型)88.阵发性睡眠性血红蛋白尿症89.波伊茨-耶格综合征90.苯丙酮尿症91.POEMS 综合征92.卟啉病93.普拉德-威利综合征94.原发性联合免疫缺陷病95.原发性遗传性肌张力不全96.原发性轻链型淀粉样变97.进行性家族性肝内胆汁淤积症98.进行性肌营养不良99.丙酸血症100.肺泡蛋白沉积症101.囊性纤维化102.视网膜色素变性103.视网膜母细胞瘤104.重症先天性粒细胞缺乏症105.婴儿严重肌阵挛性癫痫106.镰刀型细胞贫血病107.拉塞尔-西尔弗综合征Silver-Russell syndrome108.谷固醇血症109.脊髓延髓肌萎缩症(肯尼迪病) 110.脊髓性肌萎缩症111.脊髓小脑性共济失调112.系统性硬化症113.四氢生物喋呤缺乏症114.结节性硬化症115.酪氨酸血症116.极长链酰基辅酶A脱氢酶缺乏症117.威廉姆斯综合征118.湿疹-血小板减少-免疫缺陷综合征119.X连锁肾上腺脑白质营养不良120.X连锁无丙种球蛋白血症121.X连锁淋巴增生症资料(1)资料(1)目录1.21-羟化酶缺乏症2.白化病3.奥尔波特综合征4.肌萎缩侧索硬化5.天使综合征6.精氨酸酶缺乏症7.窒息性胸腔失养症(热纳综合征)8.非典型溶血性尿毒症综合征9.自身免疫性脑炎10.自身免疫性垂体炎1. 【21-羟化酶缺乏症】概述21-羟化酶缺乏症(21-OHD)是先天性肾上腺增生症(CAH)中最常见的类型,是由于编码21-羟化酶的CYP21A2 基因缺陷导致肾上腺皮质类固醇激素合成障碍的一种先天性疾病,呈常染色体隐性遗传。
威廉姆斯综合征(罕见病诊疗指南)

概述威廉姆斯综合征(Williams syndrome,WS),又称Williams-Beuren综合征(Williams-Beuren syndrome,WBS),是一种由于7q11.23区域1.5-1.8Mb基因杂合微缺失所致的多系统异常综合征。
临床以心血管疾病、特殊面容、智力低下、生长发育障碍以及内分泌异常等为特点。
病因和流行病学染色体7q11.23区域包含28个基因,目前尚未发现该区域某一单基因是威廉姆斯综合征的致病基因。
在该区域中的弹性蛋白基因(ELN基因)所编码的弹性蛋白是各器官结缔组织中的弹性纤维的重要成分,也是血管壁结构的主要成分。
该基因缺失会导致结缔组织异常、弹性蛋白动脉病等。
威廉姆斯综合征是由染色体7q11.23区域包括ELN基因在内的相邻基因杂合性微缺失所致。
该区域两侧均为低拷贝重复序列(LCR),因此易发生非等位基因的同源重组,进而导致7q11.23区域缺失。
在95%的WS患者中,缺失范围约为1.55Mb,另外5%的患者,缺失约为1.84Mb。
威廉姆斯综合征在挪威的发病率为1/7500,中国香港活产婴儿中的发病率为1/23500,中国大陆地区暂无相关的流行病学调查报告。
临床表现1.特殊面容眶周皮下组织饱满、眶距增宽、星状虹膜、人中长、嘴唇厚、宽嘴以及小下颌。
2.心血管疾病75%~80%的患者存在弹性蛋白动脉病,可影响任何动脉。
周围型肺动脉狭窄(37%~61%)在婴儿期较常见,但随着时间的推移可有改善。
瓣上型主动脉狭窄较常见(35%~65%),并且随着时间的推移在5岁前恶化。
动脉狭窄导致左心阻力增高、心肌肥厚和心力衰竭。
同时存在周围肺动脉狭窄和主动脉狭窄(双心室流出道梗阻)的威廉姆斯综合征患者心律失常、猝死的风险增加。
另外,部分猝死患者与冠状动脉狭窄有关。
麻醉和镇静会使患者发生不良事件的风险增加,包括心脏骤停。
其他异常包括肾动脉狭窄、胸主动脉狭窄、腹主动脉狭窄、二尖瓣脱垂和主动脉瓣关闭不全、肠系膜动脉狭窄、颅内血管异常等。
国家卫生健康委员会对十三届全国人大三次会议第9853号建议的答复
国家卫生健康委员会对十三届全国人大三次会议第9853号建议的答复文章属性•【制定机关】国家卫生健康委员会•【公布日期】2020.09.18•【文号】•【施行日期】2020.09.18•【效力等级】部门规范性文件•【时效性】现行有效•【主题分类】疾病防控正文对十三届全国人大三次会议第9853号建议的答复代表您好:您提出的《关于构建可持续的罕见病治疗服务体系的建议》收悉,经商财政部、国家广电总局,国家医保局、国家药监局、中国科协,现答复如下:一、工作现状和进展情况随着我国经济社会的发展和人民生活水平的提高,特别是党中央、国务院对保障和改善民生的高度重视,罕见病越来越受到社会各界的关注。
我委高度重视罕见病管理,会同相关部门开展有关工作,不断完善政策,保障罕见病患者权益。
(一)公布了我国第一批罕见病目录。
2018年5月,我委、科技部、工业和信息化部、国家药监局和国家中医药局5部门联合印发《第一批罕见病目录》,收录121种罕见病,明确罕见病病种范围,为各部门开展罕见病管理相关工作提供了有益参考。
同时,印发《关于印发罕见病目录制订工作程序的通知》,明确罕见病目录更新的工作程序,保证罕见病目录根据罕见病管理国情进行动态调整更新。
(二)发布罕见病诊疗指南。
2019年2月,我委印发《罕见病诊疗指南(2019年版)》,对121种罕见病的诊疗方法进行详细介绍,为医务人员提高罕见病诊疗能力提供有益参考。
并依托行业在线上线下组织开展多次罕见病诊疗培训,提高医务人员诊治罕见病的规范化水平,减少罕见病的误诊、错诊、漏诊情况。
(三)建立我国罕见病诊疗协作网。
我委于2019年2月印发《关于建立全国罕见病诊疗协作网的通知》,建立全国罕见病诊疗协作网(以下简称协作网)。
协作网将建立畅通完善的协作机制,对罕见病患者进行相对集中诊疗和双向转诊,以充分发挥优质医疗资源辐射带动作用,提高我国罕见病综合诊疗能力,逐步实现罕见病早发现、早诊断、能治疗、能管理的目标。
《罕少疾病杂志》“罕见病研究”专题征稿通知

《罕少疾病杂志》“罕见病研究”专题征稿通知
无
【期刊名称】《罕少疾病杂志》
【年(卷),期】2022(29)10
【摘要】一、专题简介罕见病具有病情严重、诊断困难、误诊率高、可治愈率低等特点。
近年来随着媒体报道和传播力度的加大,社会关注度的提高,我国政府出台一系列政策支持:2018年制定了《第一批罕见病目录》,共有121种罕见病;2019年相继发布了中国《罕见病诊疗指南(2019年版)》《消除罕见病患儿诊断壁垒调查结果和建议报告》,为121种罕见病诊疗提供依据;同年,国家卫生健康委员会宣布建立全国罕见病诊疗协作网,加强我国罕见病管理,提高罕见病诊疗水平。
【总页数】1页(PF0003-F0003)
【作者】无
【作者单位】罕少疾病杂志社
【正文语种】中文
【中图分类】R73
【相关文献】
1.《罕少疾病杂志》“罕见病研究”专题征稿通知
2.《罕少疾病杂志》“罕见病研究”专题征稿通知
3.《罕少疾病杂志》“罕见病研究”专题征稿通知
4.《罕少疾病杂志》“罕见病研究”专题征稿通知
5.《罕少疾病杂志》“罕见病研究”专题征稿通知
因版权原因,仅展示原文概要,查看原文内容请购买。
《罕见病诊疗指南(2019年版)》要点 自身免疫性胰岛素受体病(AIR),(2)
《罕见病诊疗指南(2019年版)》要点自身免疫性胰岛素受体病(AIR),(2)概述自身免疫性胰岛素受体病(AIR),又称B 型胰岛素抵抗(TBIR)。
是由于胰岛素受体自身抗体(IRAs)导致的一种罕见病。
AIR 好发于非洲裔美国女性,主要临床表现为高血糖、黑棘皮征、自身免疫性疾病等,少数患者病程中会出现低血糖。
病因和流行病学由于AIR非常罕见,目前确切的患病率不详。
AIR 病因目前尚不明确。
多数人认为是由于自身免疫紊乱导致了IRAs 的产生而致病。
临床表现高血糖是AIR最常见的临床表现。
但在没有干预的情况下患者可以自发缓解而维持血糖水平正常。
AIR是自身免疫性低血糖的主要原因之一,约25%的患者在病程中会出现自发性低血糖。
约50%的患者存在黑棘皮征。
此外,多囊卵巢、高雄激素血症表现在该类患者中也不少见。
AIR患者常伴发其他的自身免疫性疾病,其中以系统性红斑狼疮最为常见,约占50%。
此外,还有原发性胆汁性肝硬化、皮肌炎、硬皮病等。
AIR还可以表现为霍奇金淋巴瘤、多发性骨髓瘤等的副肿瘤综合征表现。
辅助检查1. 胰岛素水平:对于糖耐量正常的非肥胖个体,空腹胰岛素水平超过150pmol/L 或口服葡萄糖耐量试验中峰值胰岛素水平超过1500pmol/L 提示该病。
2. 甘油三酯:AIR患者甘油三酯水平正常或偏低。
3. 脂联素:AIR患者脂联素水平升高。
4. IRAs:IRAs对诊断具有重要价值。
5. 抗核抗体谱:如怀疑合并系统性红斑狼疮、皮肌炎等,完善抗核抗体谱检查有助于诊断其他自身免疫性疾病。
诊断目前尚无特异性临床特征可用于诊断该病。
患有黑棘皮病和可疑自身免疫性疾病的患者,空腹胰岛素浓度显著升高,需考虑AIR。
每日外源性胰岛素用量>3U/kg 的非肥胖患者也需怀疑AIR。
如检测到IRAs 可确诊。
确诊为AIR 的患者需评估是否存在其他自身免疫性疾病。
反过来,如发现其他自身免疫性疾病也有助于确认AIR 诊断。
罕见病科主任的罕见病诊疗指南与病例分享

罕见病科主任的罕见病诊疗指南与病例分享罕见病,顾名思义,指的是发病率极低的疾病,其患者数量少,且往往缺乏有效的治疗方案。
由于罕见病的特殊性,许多医院并未设立相应的科室或专业团队,导致患者在就医过程中面临诊断困难、治疗缺乏等问题。
然而,在某个医院的罕见病科中,有一位主任医师却致力于罕见病的诊疗研究,并积极分享自己的经验和病例,为患者提供了宝贵的帮助。
该罕见病科主任医师,名叫李医生,他在罕见病领域已经从事了多年的临床工作。
他深知罕见病患者的困境,因此他希望通过不断的学习和研究,为患者提供更好的诊疗方案。
在他的努力下,该科室建立了一套完善的罕见病诊疗指南,以帮助医生更好地诊断和治疗这些疾病。
首先,李医生强调了罕见病的早期诊断的重要性。
由于罕见病的发病率极低,很多患者在初期往往被误诊为其他常见病,导致耽误了最佳治疗时机。
因此,李医生提醒医生们在面对病情复杂、症状不明显的患者时,要保持警惕,积极进行全面的检查和鉴别诊断,以尽早确定罕见病的可能性。
其次,李医生强调了多学科团队的重要性。
罕见病的诊断和治疗通常需要多个学科的专家共同参与,而不仅仅是一个医生的努力。
李医生鼓励医生们与其他学科的专家进行密切合作,共同制定治疗方案,以提高治疗效果。
他还组织了定期的多学科讨论会,让各位专家分享自己的经验和观点,共同解决难题。
此外,李医生还通过病例分享的方式,向医生们传授罕见病的诊疗经验。
他每周都会选取一到两个有代表性的病例,详细介绍病情、诊断过程和治疗方案,并与大家进行深入的讨论。
这种病例分享的方式,不仅让医生们学到了宝贵的经验,也提高了他们对罕见病的认识和理解。
在李医生的带领下,该罕见病科的诊疗水平得到了显著提升。
越来越多的患者选择来这里就医,希望能够得到更好的治疗效果。
李医生不仅仅是一个医生,更是患者们的希望之光。
他用自己的专业知识和医术,为患者提供了新的希望。
在这里,我想分享一个真实的病例,展示李医生的医术和治疗效果。
《罕见病诊疗指南(2019年版)》要点 (1)
《罕见病诊疗指南(2019年版)》要点(1)总目录1.21-羟化酶缺乏症2.白化病3.奥尔波特综合征4.肌萎缩侧索硬化5.天使综合征6.精氨酸酶缺乏症7.窒息性胸腔失养症(热纳综合征)8.非典型溶血性尿毒症综合征9.自身免疫性脑炎10.自身免疫性垂体炎11.自身免疫性胰岛素受体病12.β-酮硫解酶缺乏症13.生物素酶缺乏症14.心脏离子通道病15.原发性肉碱缺乏症16.Castleman病17.腓骨肌萎缩症18.瓜氨酸血症19.先天性肾上腺发育不良20.先天性高胰岛素性低血糖血症21.先天性肌无力综合征22.先天性肌强直23.先天性脊柱侧凸24.冠状动脉扩张25.先天性纯红细胞再生障碍性贫血26.Erdheim-Chester 病27.法布里病28.家族性地中海热29.范科尼贫血30.半乳糖血症31.戈谢病32.全身型重症肌无力33.Gitelman 综合征34.戊二酸血症型35.糖原累积病(型、型)36.血友病37.肝豆状核变性38.遗传性血管性水肿//39.遗传性大疱性表皮松解症40.遗传性果糖不耐受症41.遗传性低镁血症42.遗传性多发脑梗死性痴呆43.遗传性痉挛性截瘫44.全羧化酶合成酶缺乏症45.高同型半胱氨酸血症46.纯合子家族性高胆固醇血症47.亨廷顿病48.HHH 综合征(高鸟氨酸血症-高氨血症-同型瓜氨酸尿症)49.高苯丙氨酸血症50.低磷酸酯酶症51.低血磷性佝偻病52.特发性心肌病53.特发性低促性腺激素性性腺功能减退症54.特发性肺动脉高压55.特发性肺纤维化56.IgG4 相关性疾病57.先天性胆汁酸合成障碍58.异戊酸血症59.卡尔曼综合征60.朗格汉斯细胞组织细胞增生症61.莱伦综合征62.Leber 遗传性视神经病变63.长链-3-羟酰基辅酶A 脱氢酶缺乏症64.淋巴管肌瘤病65.赖氨酸尿蛋白不耐受症66.溶酶体酸性脂肪酶缺乏症67.枫糖尿症68.马方综合征69.McCune-Albright 综合征70.中链酰基辅酶A 脱氢酶缺乏症71.甲基丙二酸血症72.线粒体脑肌病73.黏多糖贮积症74.多灶性运动神经病75.多种酰基辅酶A 脱氢酶缺乏症76.多发性硬化77.多系统萎缩78.强直性肌营养不良79.N-乙酰谷氨酸合成酶缺乏症80.新生儿糖尿病81.视神经脊髓炎82.尼曼匹克病83.非综合征型耳聋84.努南综合征85.鸟氨酸氨甲酰基转移酶缺乏症86.成骨不全症87.帕金森病(青年型、早发型)88.阵发性睡眠性血红蛋白尿症89.波伊茨-耶格综合征90.苯丙酮尿症91.POEMS 综合征92.卟啉病93.普拉德-威利综合征94.原发性联合免疫缺陷病95.原发性遗传性肌张力不全96.原发性轻链型淀粉样变97.进行性家族性肝内胆汁淤积症98.进行性肌营养不良99.丙酸血症100.肺泡蛋白沉积症101.囊性纤维化102.视网膜色素变性103.视网膜母细胞瘤104.重症先天性粒细胞缺乏症105.婴儿严重肌阵挛性癫痫106.镰刀型细胞贫血病107.拉塞尔-西尔弗综合征Silver-Russell syndrome108.谷固醇血症109.脊髓延髓肌萎缩症(肯尼迪病) 110.脊髓性肌萎缩症111.脊髓小脑性共济失调112.系统性硬化症113.四氢生物喋呤缺乏症114.结节性硬化症115.酪氨酸血症116.极长链酰基辅酶A脱氢酶缺乏症117.威廉姆斯综合征118.湿疹-血小板减少-免疫缺陷综合征119.X连锁肾上腺脑白质营养不良120.X连锁无丙种球蛋白血症121.X连锁淋巴增生症资料(1)资料(1)目录1.21-羟化酶缺乏症2.白化病3.奥尔波特综合征4.肌萎缩侧索硬化5.天使综合征6.精氨酸酶缺乏症7.窒息性胸腔失养症(热纳综合征)8.非典型溶血性尿毒症综合征9.自身免疫性脑炎10.自身免疫性垂体炎1. 【21-羟化酶缺乏症】概述21-羟化酶缺乏症(21-OHD)是先天性肾上腺增生症(CAH)中最常见的类型,是由于编码21-羟化酶的CYP21A2 基因缺陷导致肾上腺皮质类固醇激素合成障碍的一种先天性疾病,呈常染色体隐性遗传。
罕见病诊疗指南

Key Considerations in Using Real-World Evidence to Support Drug Development(Draft for Public Review)Center for Drug Evaluation, NMPAMay, 2019Table of Contents1.INTRODUCTION (1)1.Background and Purpose (1)2.Progress in the development of related regulations or guidelines by domestic and foreign regulatory agencies (3)2.Relevant Definitions of Real-World Research (4)1.Real-World Data (5)2.Real-World Evidence (9)3.Scenarios where real-world evidence supports drug development and regulatory decisions (9)1.Treatment for rare diseases (9)2.Revision of indications or drug combination labeling (10)3.Post-marketing evaluation (11)4.Clinical development of traditional Chinese medicine hospital preparations (12)5.Guiding clinical trial design (13)6.Identify the target population (14)4.The Basics of Real-World Research Design (14)1.Pragmatic clinical trials (14)2.Single-arm trial using real world data as control (15)3.Observational studies (16)5.Evaluation of Real-World Evidence (16)1.Real world evidence and the scientific questions it supports (17)2.How to transform real-world data to real-world evidence (17)References (19)Appendix 1: Glossary (21)Appendix 2: Common Statistical Methods for Real-World Research (24)Appendix 3: Chinese-English Vocabulary (42)Key Considerations in Using Real-World Evidence 1to Support Drug Development231.INTRODUCTION41.Background and Purpose5Randomized Controlled Trials (RCTs) are considered the "gold 6standard" for evaluating drug efficacy and are widely used in clinical 7trials. With strictly controlled trial eligibility criteria and the utilization of 8randomization, RCTs minimize the impact of factors that potentially 9affect the causal inference, and hence result in more definitive 10conclusions and derive more reliable evidence. However, RCTs also have 11limitations: stringent entry criteria may reduce the representativeness of 12the trial population to the target population, the standard trial 13interventions used may not be completely consistent with real world 14clinical practice, the limited sample size and short follow-up time leads to 15insufficient evaluation of rare adverse events. These limitations bring 16challenges when extrapolating the RCT conclusions to real world clinical 17practice. In addition, for some rare and major life-threatening diseases 18that lack effective treatments, conventional RCTs may be difficult to 19implement, require substantial time costs, or raise ethical issues.20Therefore, how to use real-world evidence (RWE) during drug R&D, 21especially as complementary evidence to RCTs in evaluating the efficacy 22and safety of drugs, has become a common and challenging question for 23global regulatory agencies, the pharmaceutical industry and academia.24First, we need to clarify the definition and scope of real-world 25evidence on a conceptual level.26Secondly, can and how will real-world data (RWD), as the 27fundamental basis of real-world evidence, provide sufficient support will 28face many questions that need to be discussed, including data sources, 29data standards, data quality, data sharing mechanism, data infrastructure 30and so on.31Third, the lack of regulatory guidance. At present, there are no 32mature and relevant regulations worldwide. Without sufficient experience, 33how to formulate guidelines that fit the reality of China's pharmaceutical 34industry requires active exploration and innovation.35Fourth, the methodologies for evaluating real-world evidence needs 36to be streamlined. Real-world evidence stems from the correct and 37adequate analysis of real-world data. The analysis methods used are 38mainly for causal inference, which often requires more complex models 39and assumptions, screening of corresponding covariates, identification of 40confounding factors, definition of intermediate variables and instrumental 41variables, etc., All these will put forward higher requirements for 42statistical analysts as well as the urgent needs for regulatory guidelines.43Fifth, the scope of real-world evidence application remains to be 44determined. The main role of real-world evidence is to complement, 45instead of substitute, the evidence provided by conventional clinical trials, 46and to form a complete and rigorous chain of evidence to further improve 47the efficiency and scientific validity of drug development. Therefore, it is 48necessary to clearly define the scope of application of real-world 49evidence according to the stage of drug development, and in the 50meanwhile adopt appropriate adjustment as the actual conditions evolve 51over time.52In light of the above, this guideline aims to provide clarity on the 53definition of real-world research, outline the use and scope of real-world 54evidence in drug R&D, explore the basic principles for the evaluation of 55real-world evidence, and consequently provide scientific and practical 56guidance for the industry to consider when utilizing real-world evidence 57to support drug development.582.Progress in the development of related regulations or guidelines 59by domestic and foreign regulatory agencies60In February 2009, the American Recovery and Reinfection Act 61played a significant role in promoting Comparative Effectiveness 62Research (CER).Accordingly, the concept of real-world research (RWR, 63or real-world study RWS) was proposed given the context of the real 64world environment of CER.65In December 2016, the United States passed the 21st Century Cures 66Act (the Act), encouraging the Food and Drug Administration (FDA) to 67accelerate the development of pharmaceutical products by conducting 68research in the use of real-world evidence. Under the support of the Act, 69during 2017-2018 the FDA issued a series of guidelines, namely "Use of 70Real World Evidence to Support Medical Device Regulatory Decisions", 71"Guidelines for the Use of Electronic Health Record Data in Clinical 72Research" and "Framework for Real World Evidence Solutions".73In 2013, the European Medicines Agency (EMA) released the 74"Qualification opinion of a novel data driven model of disease 75progression and trial evaluation in mild and moderate Alzheimer’s 76disease", discussing the technical details in using real-world observational 77data to establish disease progression models. In 2014, EMA also launched 78the Adaptive Licensing Pilot to assess the feasibility of using 79observational study data to assist decision-making. Later in 2016, the 80“Scientific Guidance on Post-authorisation Efficacy Studies”was 81released.82At the International Council for Harmonisation of Technical 83Requirements for Medicinal Products for Human Use (ICH), Japan’s 84Pharmaceuticals and Medical Devices Agency (PMDA), proposed a 85strategic approach for pharmacoepidemiology studies submitted to 86regulatory agencies to advance more effective utilization of real-world 87data.88The systematic use of real-world evidence to support drug 89development and regulatory decision-making in China is still under 90development. However, the national drug regulatory agencies have 91already begun to utilize real-world evidence in the review practices. For 92example, the extended Bevacizumab treatment regimen in combination 93with platinum-based chemotherapies was approved in 2018, using 94real-world evidence from three retrospective studies. In another case, a 95drug was further evaluated, after marketing, through a prospective, 96observational real-world study to provide additional evidence on efficacy 97and safety.982.Relevant Definitions of Real-World Research99Generally speaking, real-world research includes both research on 100natural populations and on clinical populations; the latter yields 101real-world evidence that can be used both to support medical product 102development and regulatory decisions, as well as for other scientific 103purposes. For that reason, this guidance focuses on real-world research 104that supports healthcare product development and regulatory decisions 105(see figure below).106107Figure 1 The path from RWD to RWE, which supports regulatory108decisions for medical products109We define real-world research as: collecting patient-related data in a 110real-world environment (real-world data), and obtaining clinical evidence 111(real-world evidence) of the value and potential benefits or risks of the 112medical products through analysis. The primary research type is 113observational, but it can also be pragmatic clinical trials.1141.Real-World Data115(1)D efinition116Section 505F (b) of the Federal Food, Drug, and Cosmetics Act (FD&C 117Act) defines real-world data as "data regarding the usage, or the potential 118benefits or risks, of a drug derived from sources other than traditional 119clinical trials". In “Framework for FDA’s Real-World Evidence Program”120and the “Use of Real World Evidence to Support Medical Device 121Regulatory Decisions.", the FDA defines real-world data as "data relating 122to patient health status and/or the delivery of health care routinely 123collected from a variety of sources”. For example, Electronic Health 124Record (EHR) data, Electronic Medical Record (EMR) data, medical 125insurance data, product and disease registry data, patient report data 126(including home environment), and other health tests (such as mobile 127devices) data.128We define real world data as: data collected from patients’ 129medications and health status, and/or derived from various daily medical 130processes.131(2)S ource of real-world data132Common sources of real-world data in China include:1331) Health Information System (HIS): similar to EMR/HER, digital 134patient records including structured and unstructured data fields, such as 135patient demographics, clinical characteristics, diagnosis, treatment, 136laboratory tests, safety and clinical outcomes.1372) Medicare system: structured data such as basic patient 138information, medical service utilization, prescriptions, billing, medical 139claims, and planned health care.1403) Disease Registry System: a database of patients with specific 141(usually chronic) diseases, often derived from a cohort registry of the 142disease population in the hospital.1434) China ADR Sentinel Surveillance Alliance (CASSA): the use of 144electronic data from medical institutions to establish an active monitoring 145and evaluation system for the safety of drugs and medical devices.1465) Natural population cohort database: the (to be) established 147natural population cohort and special disease cohort database.1486) Omics-related databases: databases that collect information on 149the physiology, biology, health, behavior, and possible environmental 150interactions of patients, such as pharmacogenomics, metabolomics, and 151proteomics.1527) Death registration database: a database formed by death 153registries jointly confirmed by hospitals, centers for disease control and 154prevention (CDC), and department of household registration.1558) Mobile devices: mobile devices such as wearable devices that 156measure relevant data.1579) Other special data sources: databases created for special purposes, 158such as national immunization program databases.159(3)D ata Quality Evaluation160The quality of real-world data is mainly assessed by its relevance 161and reliability.1621) Relevance: Important relevant factors to assess the suitability of 163real-world data for regulatory use include, but are not limited to:164①the inclusion of important variables and information related to 165clinical outcomes, such as drug use, patient demographic and clinical 166characteristics, covariates, outcome variables, follow-up duration, sample 167size, etc.;168②whether the definition of clinical outcome is accurate and the 169corresponding clinical significance is meaningful;170③Accurate and representative definition of target population;171④The study hypothesis can be evaluated through the study 172protocol and statistical analysis plan.1732) Reliability: The reliability of real-world data is mainly evaluated 174by data integrity, accuracy, quality assurance, and quality control.175①Integrity: missing data problems are inevitable in the real-world 176setting, but the amount of missing should have a certain limit. For 177different studies, the degree of missing data may vary. When the 178proportion of missing data within a specific study exceeds a certain limit, 179there is a great deal of uncertainty about its impact on the study 180conclusion. At this time, it will be necessary to carefully assess whether 181the data can be used as real-world data that produce real-world evidence. 182②Accuracy: the accuracy of the data is critically important and 183needs to be identified and verified against authoritative sources of 184reference. For example, the measurement of blood pressure requires the 185use of a calibrated sphygmomanometer, for which and the measurement 186process is subject to the operating specifications; whether the endpoint 187event is determined by an independent endpoint event committee, etc.188③Quality Assurance: quality assurance refers to the prevention, 189identification, and correction of data errors that occur during the course of 190the research. Quality assurance is closely related to regulatory compliance 191and should run through every aspect of data management that needs to 192have a corresponding Standard Operating Procedures (SOPs).193④Quality Control: data collection, modification, transmission, 194storage, and archiving, as well as data processing, analysis, and 195submission, are all subject to quality control to ensure that the real-world 196data are accurate and reliable. It is necessary to develop a complete, 197normative and reliable data management process or protocol.198(4)D ata criteria199Data standards, in the form that information technology systems or 200scientific tools can use, help ensure that the submitted data are predictable 201and consistent. In order to manage real-world data from multiple sources, 202it is necessary to convert the data into a common format with a generic 203formulation (e.g., terminology, vocabulary, coding scheme, etc.).204In addition, whether the quality of real-world data can support drug 205development depend on key factors including (but not limited to): 206whether there is a clear process and qualified personnel for data 207collection; whether a common defining framework, i.e., the data 208dictionary, is used; whether the common time frame for key data points 209collection is followed; whether a study plan, protocol and/or analysis plan 210related to the collection of real-world data have been established; whether 211the technical approach used for data element capture, including 212integration of data from various sources, data records of drug use, links to 213claims data etc., is adequate; whether patient recruitment minimizes the 214bias and reflects the true target population; whether data entry and 215transfer are useable and timely; and whether adequate and necessary 216patient protection measures such as patient privacy protection and 217regulatory compliance with informed consent are in place.2182.Real-World Evidence219Real-world evidence is clinical evidence about the use and potential 220benefits or risks of medical products, obtained through the analysis of 221real-world data. This definition is not limited in concept to obtaining 222evidence through retrospective observational studies, but also allows 223prospective access to a wider range of data to form evidence, through 224particular study designs including pragmatic clinical trials (PCTs).2253.Scenarios where real-world evidence supports drug 226development and regulatory decisions227Real world evidence may support drug development through a variety of 228ways, covering pre-marketing clinical development and post-marketing 229evaluation. Any use of real-world evidence for the purpose of product 230registration will require adequate communication in advance with231regulatory authorities to ensure alignment on the study objectives and232methodology.2331.Treatment for rare diseases234In addition to the challenges in subject recruitment, clinical trials for 235rare disease also face difficulties in the choice of control arm, given the 236few or lack of treatment options. Therefore, external controls established 237based on real world data in natural disease cohorts can be considered.238External controls are primarily used for non-randomized single-arm 239trials, as a historical or in-parallel control. Historical external controls are 240based on real-world data obtained earlier; parallel external controls are 241based on data from disease registries constructed simultaneously with the 242single-arm trial. The use of external controls should take into account the 243impact of the heterogeneity and comparability of the target population on 244the corresponding real-world evidence.2452.Revision of indications or drug combination labeling246For drugs that are already marketed, long-term clinical practice may 247find it necessary to expand the indication, and RCTs are often utilized to 248support the indication expansion. When an RCT is not feasible or when 249evidence it generates is not optimal, a PCT could be a reasonable choice. 250For example, clinical practice may find that a new drug for diabetes can 251potentially benefit patients with cardiovascular diseases (such as heart 252failure). In that case the subject recruitment into an RCT will be difficult 253with potential ethical issues and therefore the use of a PCT design may be 254more feasible.255In terms of pediatrics medication, there are often cases of off-label 256usage in clinical practice. For that reason, the use of RWE in supporting 257the expansion of targeted population is also a viable strategy in drug 258development.259A typical use of real-world evidence to support the development of 260Bevacizumab, a humanized monoclonal antibody of the vascular 261endothelial growth factor (VEGF). In 2015, Bevacizumab was approved 262in China in combination with chemotherapy (carboplatin and paclitaxel) 263for the first-line treatment of late stage unresectable advanced, metastatic 264or recurrent squamous non-small cell lung cancer. However, the 265real-world use of chemotherapy with Bevacizumab also includes 266Pemetrexed in combination with platinum, Gemcitabine and Cisplatin. In 267October 2018, Bevacizumab was approved to expand the treatment 268regimen with a combination of platinum-based chemotherapy, based on 269the strong supporting evidence from three real-world studies. These 270studies retrospectively analyzed patient data from three hospitals and 271showed that the combination of Bevacizumab with platinum-based 272chemotherapy significantly prolonged PFS and OS compared with 273chemotherapy alone, and no new safety issues were identified. This 274finding was consistent with global population data. In addition, relevant 275real-world studies have also provided data in different patient subgroups 276such as those with EGFR mutations or brain metastases, confirming the 277efficacy and safety of Bevacizumab combination therapy from multiple 278perspectives.2793.Post-marketing evaluation280Due to factors such as limited sample size, short study duration, 281strict enrollment criteria, and standardization of intervention, drugs 282approved based on RCTs usually have limited safety information, lack of 283generalization of efficacy conclusions, less optimal drug regimen, and 284insufficient health economic benefits. As a result, there is a need to use 285real-world data for more comprehensive assessment of these aspects of 286the approved drugs, and to refine the decision making based on the 287real-world evidence from natural populations on a continuous basis.288For example, a drug for cardiovascular diseases has been approved 289in more than 50 countries/regions worldwide. In the multi-regional 290clinical trials that supported it approval, small number of Chinese 291subjects resulted in limited number of cardiovascular events and short 292drug exposure in the Chinese subgroup. This has led to greater variability 293in the efficacy results in the Chinese population. As an overseas marketed 294drug with clinically urgent needs in China, to further evaluate the efficacy 295of this compound in Chinese patients, the applicant plans to conduct a 296prospective, observational, post-marketing real-world study to evaluate 297the combination of the compound with standard treatment versus standard 298treatment alone, in the prevention of major adverse cardiovascular events 299(MACE) in Chinese patients with cardiovascular disease.3004.Clinical development of traditional Chinese medicine hospital 301preparations302Traditional Chinese medicine prepared and used in hospitals have 303been widely used clinically for a long time without being approved for 304marketing. This is a unique phenomenon in China. For the clinical 305research and development of such drugs, if real-world research and 306randomized controlled clinical trials can be combined, scientific and 307feasible clinical R&D and regulatory decision-making pathways can be 308further explored.309For the development of traditional Chinese medicine hospital 310preparation, there exist multiple R&D strategies that utilize real-world 311evidence. Figures 2 and 3 outline two potentially possible pathways. The 312pathway that combines observational studies and RCTs is illustrated in 313Figure 2. Specifically, stage 1 starts with retrospective observational 314studies. At this stage effort should be made to collect as much as possible 315existing real-world data related to the use of the product including all 316possible covariates, develop data cleaning rules, identify possible controls, 317assess data quality, and conduct comprehensive and detailed analyses 318using appropriate statistical methods. If the retrospective observational 319studies show that the drug has potential benefits for patients in clinical 320use, it may proceed to the next stage of the development, otherwise the 321process should be terminated. In stage 2, prospective observational 322studies can be conducted. Based on the stage 1 research, this second stage 323can be more carefully designed in terms of several aspects, including data 324acquisition and its system, data quality control, data cleaning rules, and 325clearer definition of controls. Once this stage 2 prospective observational 326research has progressed to certain phase, and if the data are consistent 327with the results of stage 1 retrospective observational studies by 328continuing to show clinically meaningful benefits, a third stage of RCT 329can be conducted in parallel. If needed, a pilot RCT may be conducted 330first to acquire sufficient information to support the design of the primary 331RCT. However, if existing evidence from previous observational studies 332is deemed sufficient, a confirmatory RCT may be designed and 333conducted directly. In terms of timing, the duration of the RCT may be 334covered by the stage 2 prospective observational studies, which can be 335completed at the same time as the RCT or extended for some time after 336the end of the RCT, depending on the maturity of the real-world 337evidence.338339Figure 2 Potential development pathway for traditional Chinese medicine 340hospital preparations341Another potentially possible pathway, which combines observational 342studies with PCTs, is outlined in Figure 3. In the first stage, retrospective 343observational studies are conducted first. If it is concluded that the drug 344has potential benefits in clinical practice, it may proceed to the second 345stage, otherwise the process should be terminated. The second offstage 346consists of a PCT research, which provides evidence that can be used to 347support the evaluation of the drug’s clinical efficacy and safety.348349Figure 3 Potential development pathway for traditional Chinese medicine 350hospital preparations3515.Guiding clinical trial design352Compared with other potential applications, using real-world 353evidence to guide clinical trial design has more practical utilization. For 354example, the two potential pathways for the development of 355hospital-prepared traditional Chinese medicines described in the previous 356section have used the real-world evidence generated by retrospective 357observational studies, including for example the disease natural history, 358the disease prevalence in the target population, the effectiveness of 359standardized treatments, and the distribution and variation of key related 360covariates, to provide a basis for the next stage study design. More 361generally, real-world evidence can provide valid reference for inclusion 362and exclusion criteria, parameters for sample size estimation, and 363determination of non-inferiority margins, etc.3646.Identify the target population365Precision medicine aims to better predict the therapeutic benefits and 366risks of drugs to specific populations (subgroups), and real-world 367evidence based on real-world data provides the possibility for the 368development of precision medicine. For example, due to the limited 369sample size, regular clinical trials often ignore or have limited power to 370consider subgroup effects in the research plan. This prevents important 371information on potential treatment responders or high-risk populations 372with serious side effects from being fully recognized. Through a thorough 373analysis of real-world data, the treatment benefits and risks in different 374subgroups can be more adequately assessed, and hence real-world 375evidence can be obtained to support more precise identification of the 376target population.377The identification of biomarker is critical for preclinical and early 378clinical studies of targeted therapies. Using real-world information such 379as omics data, public gene bank information, and related clinical data in 380population cohorts, real-world evidence can be generated through various 381contemporary data mining techniques such as machine learning, which 382can in consequence support the precise identification of population for 383targeted therapies.3844.The Basics of Real-World Research Design3851.Pragmatic clinical trials386Pragmatic Clinical Trials (PCT), also known as practical clinical 387trials, refer to clinical trials that are designed and conducted in an 388environment close to the real-world clinical practice. They represent a 389type of study between RCTs and observational studies. Unlike RCTs, 390PCT interventions can be either standardized or non-standardized; 391subjects in the PCTs can be randomized or allocated per pre-defined 392criteria; the inclusion criteria for the subjects are often less restrict and 393considered more representative of the target population, and the 394evaluation of intervention outcomes may not be limited to clinical 395。
2019罕见病诊疗指南-非典型溶血性尿毒症综合征
非典型溶血性尿毒症综合征概述溶血性尿毒症综合征是指临床表现为微血管病性溶血性贫血、血小板减少和急性肾损伤的一组临床综合征。
由产志贺毒素的大肠埃希菌所致者,称典型溶血性尿毒症综合征;其他病因所致者称非典型溶血性尿毒症综合征(atypicalhemolyticuremicsyndrome,aHUS)。
主要病因为先天性或获得性补体旁路异常,特别是补体旁路调节蛋白的异常。
病因和流行病学aHUS的发病机制主要包括存在补体蛋白基因突变或补体蛋白抗体的易感个体,经触发事件(如感染或妊娠),引起补体替代途径不可抑制的持续激活,从而导致膜攻击复合物形成,进而导致肾脏内皮损伤、凝血级联活化和肾小动脉微血栓形成,继而引起微血管病性溶血性贫血、血小板减少及急性肾功能衰竭等临床表现。
已知相关的致病基因包括补体旁路调节基因(如补体因子H、补体因子I或CD46)的功能丧失性突变,或效应基因(如补体因子B 或C3)的功能获得性突变。
在已知与aHUS相关的补体相关因子基因突变中,以补体因子H(complementfactorH,CFH)基因突变最为常见,占所有突变的20%~30%;其他常见补体相关因子基因突变,包括CD46、补体因子I(complementfactorI,CFI)、补体因子3(complementfactor3,C3)、补体因子B(complementfactorB,CFB)和血栓调节蛋白(thrombomodulin,THBD)等。
相当一部分aHUS 患者存在1种以上的补体蛋白基因突变。
不过,由于该病的外显率较低,携带与aHUS患者相同突变基因的家庭成员中出现疾病表现者不到一半。
此外,8%~10%的aHUS患者中存在补体因子H的自身抗体。
aHUS患病率约为7/100万。
多数aHUS存在补体相关因子的基因突变,6%~10%的患者病因涉及补体蛋白抗体。
患者可能同时存在基因突变和补体蛋白抗体。
临床表现典型的临床表现包括微血管病性溶血性贫血、血小板减少及急性肾功能衰竭三联征。
罕见病诊疗指南(2019年版):血友病
罕见病诊疗指南(2019年版):血友病概述血友病(hemophilia)是一种X染色体连锁的隐性遗传性出血性疾病。
可分为血友病A(hemophilia A,HA)和血友病B (hemophilia B,HB)两种。
前者为凝血因子Ⅷ(FⅧ)缺乏,后者为凝血因子Ⅸ(FⅨ)缺乏,均由相应的凝血因子基因突变引起。
病因和流行病学编码FⅧ和FⅨ的基因均位于X染色体,女性常是携带者(46;XX),而男性是患者(46;XY),女性患者极为罕见(通常是由2个FⅧ或者FⅨ基因同时发生缺陷,或者是X染色体非随机失活所致)。
在FⅧ和FⅨ基因中点突变、缺失、插入和重排/倒位均可见,点突变是最常见的基因缺陷,约在90%的患者中存在。
HA中45%的重型患者为重现性的基因倒位突变;而HB患者中无重现性突变。
血友病的发病率没有种族或地区差异。
在男性人群中,血友病A 的发病率约为1/5000,血友病B的发病率约为1/25 000。
所有血友病患者中,血友病A占80%~85%,血友病B占15%~20%。
女性血友病患者极其罕见。
由于经济等各方面的原因,血友病的患病率在不同国家甚至同一国家的不同时期都存在很大的差异。
我国1986—1989年期间在全国24个省的37个地区进行的调查结果显示,我国血友病的患病率为2.73/100 000人口。
临床表现HA和HB的临床表现相似。
主要表现为关节、肌肉和深部组织出血,也可表现为胃肠道、中枢神经系统等内部脏器出血等。
若反复出血,不及时治疗可导致关节畸形和(或)假肿瘤形成,严重者可危及生命。
外伤或手术后延迟性出血是本病的特点。
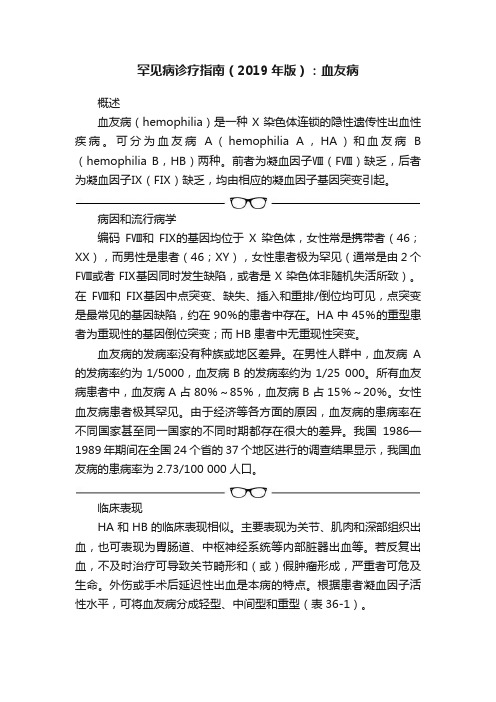
根据患者凝血因子活性水平,可将血友病分成轻型、中间型和重型(表36-1)。
辅助检查1. 筛选试验包括进行血小板计数排除血小板异常导致的出血;凝血检查中仅活化部分凝血活酶时间(APTT)延长,凝血酶原时间(PT)、凝血酶时间(TT)、纤维蛋白原(Fbg)均正常。
2. 纠正试验血友病患者若无抑制物存在,其延长的APTT(即刻或37℃孵育2小时)可以被等量的正常人混合血浆所纠正。
2019罕见病诊疗指南:肯尼迪病(Kennedy’sDisease)

2019罕见病诊疗指南:肯尼迪病(Kennedy’sDisease)论坛导读:为提高我国罕见病规范化诊疗水平,保障医疗质量和医疗安全,维护罕见病患者健康权益,根据2018年国家卫计委等5部门印发的《第一批罕见病目录》,国家卫生健康委罕见病诊疗与保障专家委员会办公室(中国医学科学院北京协和医院)牵头制定了本罕见病诊疗指南(2019年版)。
概述肯尼迪病,又称脊髓延髓肌萎缩症(spinal bulbar muscular atrophy,SBMA),是一种X连锁隐性遗传的神经系统变性病。
患者表现为不同程度的下运动神经元损害、感觉障碍及内分泌系统异常,后者包括男性乳房发育、不育以及糖尿病等。
该病是由染色体Xq11-12上的雄激素受体(androgen receptor,AR)基因第1号外显子CAG重复序列异常扩增所致,具体发病机制尚不十分明确。
病因和流行病学肯尼迪病的致病基因是位于Xq11-12上的雄激素受体基因,因其第1号外显子N端的一段CAG重复序列异常增多而致病。
文献报道该CAG重复序列在肯尼迪病患者平均为46次。
在肯尼迪病中,CAG的重复次数具有遗传的相对不稳定性,其与起病年龄和疾病的严重程度呈负相关;但也有不同结果的报道。
发病机制尚未完全清楚。
肯尼迪病主要在成年男性中发病,女性携带者一般无明显症状。
在美国,肯尼迪病的发生率为男性中1/40 000,但芬兰西部和意大利报道的发病率更高。
尚缺乏肯尼迪病在中国人群中发病率等流行病学数据。
临床表现男性发病,起病隐匿,常见发病年龄为30~60岁。
患者常以痛性痉挛、震颤、双下肢无力等症状起病,逐渐出现双上肢无力、延髓部和面部的肌肉萎缩、肌束颤动、构音障碍、吞咽困难、呼吸困难等。
可伴有男性乳房发育、生殖功能降低等雄激素受体不敏感表现。
约超过50%的患者存在感觉异常。
部分女性基因突变携带者有轻度临床症状,可仅出现痉挛,电生理检查所示慢性失神经改变多轻微。
该病进展缓慢,患者通常在病程晚期才出现行走不能,仅有部分患者需要辅助通气,对生存期无显著影响。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
《罕见病诊疗指南(2019年版)》要点6概述丙酸血症(PA)又称丙酰辅酶A羧化酶缺乏症、酮症性高甘氨酸血症或丙酸尿症。
是一种常染色体隐性遗传的有机酸血症。
PA由编码线粒体多聚体酶丙酰辅酶A羧化酶(PCC)基因PCCA或PCCB缺陷所致。
PCC缺乏可导致体内丙酰辅酶A转化为甲基丙二酰辅酶A 异常、丙酸及其相关代谢物异常蓄积,导致有机酸血症,并造成一系列生化异常、神经系统和其他脏器损害症状。
病因和流行病学PA致病基因分别为PCCA和PCCB。
PA总患病率在国外不同人种之间为1/100 000~100/100 000,我国0.6/100 000~0.7/100 000。
临床表现主要为高血氨、脑损伤和心肌病等。
1. 新生儿起病型出生时正常,开始哺乳后出现呕吐、嗜睡、肌张力低下、惊厥、呼吸困难、高血氨、酮症、低血糖、酸中毒、扩张性心肌病、胰腺炎等异常,病死率高。
2. 迟发型常因发热、饥饿、高蛋白饮食和感染等诱发,表现为婴幼儿期喂养困难、发育落后、惊厥、肌张力低下等。
由于丙酸等有机酸蓄积,许多患者的认知能力及神经系统发育受到损害,脑电图慢波增多或见癫痫波;一些患者可有骨折,X线见骨质疏松;还常造成骨髓抑制,引起粒细胞减少、贫血、血小板减少。
也可有心脏损害,如心肌病、心律失常、QT间期延长、心功能减弱等。
肾功能损害较为少见。
辅助检查1. 实验室常规检查:2. 血氨基酸和酯酰肉碱谱分析甘氨酸水平增高,丙酰肉碱(C3)、丙酰肉碱/乙酰肉碱比值(C3/C2)增高。
3. 尿有机酸分析3-羟基丙酸和甲基枸橼酸增高高度提示此病。
4. 头部MRI/CT可表现为脑萎缩、脑室增宽及基底节区异常信号。
5. 基因诊断PCCA或PCCB检出2个等位基因致病突变有确诊意义。
诊断新生儿生后数小时到1周内出现拒乳、呕吐、嗜睡、肌张力低下、惊厥、呼吸困难、高血氨、酮症、低血糖、酸中毒等异常;婴幼儿不明原因反复呕吐、惊厥、意识障碍,严重的酸中毒、高血氨,伴有特殊的影像学异常及血液系统损害者,特别是有类似/不明原因死亡家族史时,应考虑到本病。
鉴别诊断1. 甲基丙二酸血症该病患者也有血中丙酰肉碱、丙酰肉碱与游离肉碱比值增高,但同时伴有尿液中的甲基丙二酸、甲基枸橼酸异常增加,而PA患者尿中的甲基丙二酸水平正常。
2. 多种羧化酶缺乏症(包括生物素酶缺乏症、全羧化酶合成酶缺乏症)患者尿中的3-羟基丙酸、甲基巴豆酰甘氨酸及丙酰甘氨酸增高,与PA类似;但血酰基肉碱谱的3-羟基异戊酰肉碱增高,而PA 患者的该指标正常。
3. 糖尿病酮症酸中毒、乳酸性酸中毒或其他有机酸血症等可通过血尿代谢物的质谱分析鉴别诊断。
治疗1. 急性期治疗以补液,纠正酸中毒、低血糖和电解质紊乱为主,同时限制天然蛋白质摄入,供给足量热量。
可予静脉滴注左卡尼汀促进酸性物质的代谢和排出。
如出现高氨血症,可予精氨酸静脉滴注,口服促肠蠕动剂、氨甲酰谷氨酸等。
若高氨血症或代谢性酸中毒难以控制时,还需通过腹膜透析或血液透析去除毒性代谢物。
2. 长期治疗(1)饮食控制:(2)药物治疗(3)肝移植:100. 【肺泡蛋白沉积症】概述肺泡蛋白沉积症(PAP)是以肺泡表面活性物质在肺泡腔内大量沉积为特征的疾病,其原因是肺泡巨噬细胞清除表面活性物质障碍或是异常的表面活性物质产生所致。
病因和流行病学PAP的分子病理机制尚不清楚。
PAP是呼吸系统罕见病,患病率为0.36/1 000 000~3.7/1 000 000。
临床表现PAP的临床表现常没有特异性,隐匿起病。
可出现咳痰、消瘦、乏力等症状。
继发感染时可有发热、咳脓性痰,也可出现胸痛、咯血。
少数患者可无症状,可以没有阳性体征。
部分患者可以出现爆裂音,重症患者可有发绀,少数患者可见杵状指。
PAP的临床表现常比胸部影像受累的程度轻,这种症状和影像不一致的表现也是PAP的一个特征。
aPAP和遗传性PAP 的患者很少出现肺外表现。
但如果是继发于血液系统疾病或是感染等导致的PAP,患者常有原发病的相应表现。
辅助检查1. 实验室检查2. 肺功能检查3. 影像学检查4. 病理诊断诊断目前国际上并无统一的诊断标准,可以参照以下标准进行诊断:1. 临床症状主要表现为程度不等的呼吸困难,少数患者可无明显症状。
2. 查体可出现发绀、肺部啰音和杵状指,也可无阳性体征。
3. 影像学检查4. 肺泡灌洗液检测5. 肺组织病理学6. aPAP7. 先天性PAP8. 继发性PAP鉴别诊断PAP应与以下疾病相鉴别:间质性肺炎;侵袭性黏液腺癌;粟粒性肺结核;病毒性肺炎;耶氏肺孢子菌肺炎;肺水肿等。
治疗治疗目标是清除沉积在肺泡腔内的脂蛋白样物质。
1. 全肺灌洗术近年来,用双腔气管插管进行大容量全肺灌洗(WLL)可获得较好疗效。
2. 经支气管镜行分次肺段灌洗术3. 针对抗GM-CSF抗体异常雾化吸入或皮下注射粒细胞-巨噬细胞集落刺激因子(GM-CSF)目前被证实有效,临床常用雾化吸入方法。
4. 对于PAP的其他治疗选择比较有限5. 继发性PAP以治疗原发病为主6. 抗感染101. 【囊性纤维化】概述囊性纤维化(CF)是由囊性纤维化跨膜传导调节因子(CFTR)基因突变导致的多系统疾病。
以反复的呼吸道感染、咳嗽、咳痰和呼吸困难为特征,还可以出现鼻窦炎、生长发育障碍、脂肪泻和男性不育等症状,是高加索人种最常见的遗传疾病之一。
病因和流行病学CF为常染色体隐性遗传,其致病基因CFTR位于7q,CF在我国尚处于初步认识阶段,其确切的发病率并不清楚,但由于诊断意识和能力的提高,目前我国诊断的CF病例在迅速增加。
临床表现CF患者常在婴幼儿或青少年期起病,男女比例大致相等。
CF是由于CFTR 蛋白异常导致氯离子通道功能障碍,引起呼吸道、胰腺和胆道等上皮细胞的分泌物含水量减低,分泌物变黏稠而难以清除。
肺脏是最常见的受累器官,CF患者呼吸道出现慢性细菌感染及病原体的定植,最初常为流感嗜血杆菌和金黄色葡萄球菌,最终出现铜绿假单胞菌或洋葱克雷伯杆菌的慢性定植和(或)感染。
一旦出现感染,中性粒细胞被大量募集到肺组织中,并释放弹性蛋白酶,从而造成肺组织的破坏,导致支气管扩张形成。
患者的支气管扩张常在幼年起病,且常从上叶起病,与多数感染后形成的支气管扩张症主要位于中、下肺不同。
辅助检查1. 实验室检查(1)一般检查:(2)汗液氯离子测定:(3)鼻黏膜电位差:(4)肠电流测定:(5)胰腺外分泌功能:2. 肺功能检查3. 影像学检查4. 呼吸道病原体检查5. 生殖系统检查6. 基因诊断诊断至少一个器官存在CF的典型表现以及存在以下至少一种CFTR基因功能异常的证据:1. 两个部位汗液氯离子测定超过60mmol/L;2. 等位基因上存在两个CFTR 致病突变;3. 鼻黏膜电位差异常。
鉴别诊断需要与以下疾病相鉴别:感染后支气管扩张,弥漫性泛细支气管炎,α-1 抗胰蛋白酶缺乏(AAT),原发性纤毛运动障碍(PCD),变应性支气管肺曲霉菌病(ABPA),低丙种球蛋白血症,胃食管反流病等可以导致弥漫性支气管扩张的疾病。
治疗1. 综合治疗目前仍然没有治愈CF的方法。
常见的治疗建议包括:(1)促进气道分泌物的清除(2)抗生素治疗:(3)支气管扩张剂:(4)抗炎治疗:(5)改善营养:(6)肺移植:2. 特异性治疗方法102. 【视网膜色素变性】概述视网膜色素变性(RP)是一组以进行性视网膜光感受器细胞凋亡和色素上皮变性为主要特征的遗传性视网膜变性疾病,具有显著临床及遗传异质性。
病因和流行病学RP是最常见的遗传性致盲眼病,世界范围内患病率为1/7000~1/3000,在我国约为1/3784。
临床表现大多RP患者青少年时期起病,首先是视杆细胞逐渐丧失,随后出现视锥细胞受累,视网膜色素上皮细胞死亡。
因此通常以夜盲为首发症状(但城市化后部分患者常以视力下降为首发症状),而且夜盲出现得越早,患者的病情往往越严重。
虽然周边视野缺损也发生较早,但患者通常意识不到,很少以此作为疾病早期的主诉。
病情逐渐发展为中心视力下降,视野进一步缩窄,多数在40岁之前就成为法定盲人。
辅助检查OCT 常表现为椭圆体带消失、RPE 层变薄,但中心凹下的椭圆体带通常能保留到疾病晚期;ERG 可表现为不同程度的视杆、视锥细胞反应下降,其中以视杆细胞反应下降为主,疾病晚期可表现为熄灭型。
视野(VF)可表现为不同程度的视野缺损,晚期通常为管状视野。
诊断诊断标准:有典型眼底改变者即可直接诊断;对于眼底改变不典型者,需要ERG检查确诊。
鉴别诊断1. 锥杆细胞营养不良2. Leber先天黑矇(LCA)3. 早发视网膜变性4. 无脉络膜症(CHM)治疗近年来,随着对RP发病机制认识的不断深入,不同类型的治疗方式在积极研究中,包括神经保护、基因治疗、干细胞治疗以及人工视网膜等。
基因治疗的进展是近年来成果最为显著的。
103. 【视网膜母细胞瘤】概述视网膜母细胞瘤(RB)是儿童最常见的原发性眼内恶性肿瘤,起源于原始视网膜干细胞或视锥细胞前体细胞。
分遗传型和非遗传性型。
遗传型大约占45%,其中主要是双眼患者或有家族史者(大约10%的RB有家族史),还有部分单眼患者以及三侧性RB患者(双眼RB合并松果体瘤);大多数单眼患者属非遗传型。
遗传型RB临床上呈常染色体显性遗传,子代有大约50%遗传该肿瘤的风险。
病因和流行病学视网膜母细胞瘤由RB1 基因纯合或复杂合突变所致。
我国每年新增患者约为1 100 人,且84%为晚期高风险患者。
临床表现RB最常见的临床表现是白瞳症,俗称“猫眼”,即瞳孔可见黄白色反光。
患眼可因肿瘤位于后极部,视力低下,而发生失用性斜视。
临床上依据RB 是否局限在眼内可分为眼内期、青光眼期、眼外期以及全身转移期四期。
也可从发病部位分为单侧性、双侧性及三侧性RB。
辅助检查1. B超2. CT3. MRI4. 病理5. 基因检测诊断RB的诊断依靠眼底表现和辅助检查。
如果可以在眼底镜下观察到肿瘤组织的结构,大多可以做出明确的诊断,B超和CT检查是重要的诊断和鉴别诊断方法。
鉴别诊断1. 转移性眼内炎2. Coats病3. 早产儿视网膜病变4. 原始玻璃体持续增生症5. 增殖性玻璃体视网膜病变、Norrie氏病或相关疾病治疗目前RB的治疗目的不再仅为挽救生命,还应尽可能保留眼球保存视力,以提高患儿的生活质量。
临床上依据IIRC和TNM分期,合理选用现有治疗方法,进行个体化治疗,以期取得满意的疗效。
1. 眼内RB(cT~cT3N0M0)2. 眼外RB(T4N1M1)104. 【重症先天性粒细胞缺乏症】概述重症先天性中性粒细胞缺乏症(SCN)是一种以低水平粒细胞(<200/mm3)为特征的免疫缺陷,不伴有相关的淋巴细胞缺陷。
病因和流行病学目前已知的发病机制是髓系细胞凋亡增加。