Detection of TIMI-3 Flow Before Mechanical Reperfusion With Ultrasonic Tissue Characterizat
tim3抗体的判读标准

tim3抗体的判读标准TIM-3抗体(也称为T细胞免疫球蛋白和粘蛋白域包含蛋白3抗体)的判读标准通常基于实验的具体设计和目的,以及所使用的检测方法的特性。
以下是一些常见的考虑因素和标准:1.阳性与阴性对照:实验中应包含适当的阳性和阴性对照,以帮助解释结果。
阳性对照可以是已知表达TIM-3的细胞或组织,而阴性对照可以是已知不表达TIM-3的细胞或组织。
2.信号强度:通过比较样品与对照的信号强度,可以判断样品中TIM-3的表达水平。
信号强度可以使用荧光强度、酶活性、化学发光等参数进行量化。
3.表达模式:观察TIM-3在细胞或组织中的表达模式也很重要。
例如,TIM-3可能主要表达在某些类型的T细胞上,如CD4+辅助T 细胞1(Th1)和CD8+细胞毒性T细胞。
通过观察表达模式,可以了解TIM-3在特定细胞类型或组织中的功能。
4.定量与定性分析:根据实验需求,可以选择定量分析(如测量TIM-3表达水平的具体数值)或定性分析(如判断TIM-3是否表达)。
5.统计分析:对于大量样品或需要比较不同组之间的差异时,使用适当的统计方法进行分析是很重要的。
常见的统计方法包括t 检验、方差分析(ANOVA)等。
需要注意的是,具体的判读标准可能因实验设计、所用抗体和检测方法的差异而有所不同。
在设计和解释实验时,应参考相关文献、抗体说明书和实验方法指南,以确保准确和可靠地解读TIM-3抗体的结果。
此外,TIM-3抗体在肿瘤免疫治疗中具有潜在的应用价值。
一些临床前数据显示,TIM-3抗体与PD-1抗体联合作用可能具有比单独使用PD-1抗体更好的效果。
研究TIM-3抗体在肿瘤免疫治疗中的应用也是当前的研究热点之一。
人腺样囊性癌细胞系体外NT-3分泌水平的测定

A C2细胞培养上清液中 N - C- T3的分泌水平与 阴性对 照组 比较有 显著统计 学意义 ( 0 0 ) M S 4及 L 2 P< . 1 ; P 9 9细胞 培养上清液中 N 一 T3的分 泌水 平与 阴性 对照 组 比较 无显 著统 计学 意义 ( P>00 ) C . 5 。A C的两 个细 胞系 A CM、 C.
孙 沫逸 李志进 李 建虎 王磊 杨耀 武 张 圃
【 摘要 】 目的 研究体外培养 的 A C 胞系 中神 经营养 素一(err h -,T3 的分泌情 况。方法 应 C 细 3 nu tpi3 N -) oo n
用酶联免疫吸附测定法检测 N - A C细胞 系体外 的分泌水平 。收集 A CM、 C -、 s ,L 2 T3在 C C . A C2 M,P 、 994个细胞系无 血清培养的上清液 , E IA法检 测上 清液 中 N - 用 LS T3的含 量 。将 各组 细胞 培养 上 清液 中 N - T3的分 泌水 平采 用
Li Ⅳ a 删 , v e, G Yo z G
Me i l U ies y 6 1 d c nv ri . n 7 伽 a t
Dp r etfoa a dm xl ail ugr So ao gclC lg , eat n o l n a io c re tm tl i o ee m r lf a S y, o a l
2. h n C ia
F u hMitr o r la t iy
【 b t c】 Obet e o net a e ert no nuo p i- i C e snvt. to s S pra n A s at r jc v T vsgt t ce o ert hn3 nA Ccl ioMeh d u ent t i i i eh s i f o r li r a
地表水氨氮含量测定过程中的注意事项
5 000 mL 。
实验室根据采集水样的多少自行选择规格。
采集少量的水样通常选用2 500 mL 的规格。
下面就在湖泊某一指定深度采集三个平行水样为例来阐述有机玻璃采水器的使用注意事项。
采集水样根据要求是不能取湖面上方浮层,也不能将湖底的泥沙采集,所以一般是在湖深的1/2处进行取样。
当然取样前要用湖水将采水器和盛水器进行三次润洗,然后依次采集三个平行样。
有个问题很值得讨论:采水深度的确定。
根据有机玻璃采水器的工作原理即水是从采水器的下端进入的,所以采水深度确定时,要从采水器的底部算起。
在今年的工业分析与检验国赛试点赛上,多数参赛队对于采水深度的确定是错误的,他们没有搞清楚有机玻璃采水器的工作原理,直接从采水器上方开始算深度。
2 现场空白注意事项采集地表水检测氨氮含量时,通常空白是用无氨水来完成的。
要求把无氨水带到采集现场后,再进行空白取样,并且所加保护剂要和其他三个平行样所加的保护剂品种和量要尽可能一致。
采集空白样品要在现场完成,主要是为了使得空白和现场所处的温度,湿度完全一致,才能排除环境因素带来的误差。
3 保护剂的选择采集水样时,对于所加保护剂的要求是:经济并且对测定无干扰和无不良影响。
不同水样和不同的测定项目使用的保护剂要求是不一样的。
这里对于保护的使用级别是有严格要求的,为了避免系统误差,要求保护剂的纯度尽可能高,即保护剂0 引言地表水指的是陆地表面动态水和静态水的总称,主要包括液态水和固态水,主要有河流、湖泊、沼泽、冰川等[1]。
地表水是目前人类生活用水的主要来源之一,也是世界各国水资源的主要组成部分之一。
水溶液中的氨氮是游离的氮或离子氮,水中氨氮主要来源于天然水中的含氮物质的降解过程,还有目前另一个主要来源就是生活污水和工业废水。
氨氮在一定条件下可以转换成亚硝酸盐,生活中如果长期饮用含有氨氮的水,那么水中的亚硝酸盐会和人体内的蛋白质结合形成亚硝胺,是一种致癌物质,对人体的健康会造成很大的危害。
应用级联分类器检测安瓿内弱小运动目标
应用级联分类器检测安瓿内弱小运动目标秦垚;王伯雄;李伟;杨春毓【摘要】An inspection algorithm based on cascade classifiers is presented for detecting small moving foreign substances with low Signal and Noise Ratio (SNR) and low contrast in sequential images. The algorithm obtains three features of absolute difference, local difference contrast and neighborhood correlation from the sequential images of an ampoule. Each feature corresponds to a classifier, and small foreign substances are inspected by using three-layer cascade classifiers. The first layer corresponds to a traditional frame differencing method, which is used to remove the background and detect the large moving foreign substances. The next two layers are used to inspect small foreign substances and remove the noises generated by optical flow and the stain of bottle. Experiment results show that compared with the traditional frame differencing method, this algorithm has higher detection precision and higher anti-interference ability in inspecting small substances with the interference of a complex background, and the detection rate of small foreign substance is 99. 3%. This algorithm can meet the requirement of real-time detection of ampoules for medicine production.%针对序列图像内具有低信噪比和低对比度特征的运动目标,提出了一种基于级联分类器的弱小目标检测算法.该算法从安瓿瓶序列图像内提取绝对差分值、局部差分对比度和局部相关系数3个图像特征.每个图像特征对应一个分类器,通过三层级联形式实现序列图像中的小目标检测.第一个节点与传统帧间差分法类似,主要去除大量背景图像并检测出大颗粒运动目标,后两个节点则用于检测弱小目标、排除光流和瓶身污渍产生的噪声点.实验结果显示,相对于传统的帧间差分法,本文算法具有高检测精度和高抗干扰能力等特点,不仅可以检测出图像中弱小运动目标,同时也消除了复杂背景下的噪声影响,弱小目标的检出率达到99.3%,并且满足安瓿在线检测的实时性要求.【期刊名称】《光学精密工程》【年(卷),期】2012(020)001【总页数】7页(P190-196)【关键词】级联分类器;帧间差分法;小目标检测;序列图像【作者】秦垚;王伯雄;李伟;杨春毓【作者单位】清华大学精密仪器与机械学系精密测试技术及仪器国家重点实验室,北京100084;清华大学精密仪器与机械学系精密测试技术及仪器国家重点实验室,北京100084;清华大学精密仪器与机械学系精密测试技术及仪器国家重点实验室,北京100084;清华大学精密仪器与机械学系精密测试技术及仪器国家重点实验室,北京100084【正文语种】中文【中图分类】TP391.411 引言低信噪比和低对比度下检测出位置和速度都未知的运动小目标是基于机器视觉的医药制剂在线检测系统中的一项关键技术。
胰腺癌中人RUNT相关转录因子3基因启动子区甲基化及其临床意义

上海交通大学学报(医学版)Journal of Shanghai Jiaotong University (Medical Science )Vol.32No.8Aug.2012[基金项目]福建省自然科学基金(2009J01326)(Natural Science Foundation of Fujian Province ,2009J01326)。
[作者简介]林志川(1976—),男,主治医师,硕士;电子信箱:linzhichuan1976@163.com 。
[文章编号]1674-8115(2012)08-1034-04·论著·胰腺癌中人RUNT 相关转录因子3基因启动子区甲基化及其临床意义林志川,陈谭根,李建国(福建医科大学附属漳州市医院普外一科,漳州363000)[摘要]目的检测胰腺癌人RUNT 相关转录因子3(RUNX3)基因启动子的甲基化情况并探讨其临床意义。
方法采用甲基化特异性聚合酶链式反应(MSP )检测56例胰腺癌组织及癌旁组织、14例正常胰腺组织、3株人胰腺癌细胞株(PANC1、CFPAC-1、SW1990)、1株正常肝细胞株(HL-7702)中RUNX3基因启动子区CpG 岛甲基化状态。
检测用甲基化抑制剂5-氮杂-2'-脱氧胞苷(5-Aza-cdR )处理前后胰腺癌细胞株RUNX3mRNA 的表达。
分析RUNX3异常甲基化与胰腺癌临床特征的关系。
结果56例胰腺癌组织中,51.79%(29/56)存在RUNX3基因启动子区CpG 岛的异常甲基化,癌旁胰腺组织有10.7%(6/56)存在异常甲基化,而正常胰腺组织中未检测到RUNX3基因异常甲基化。
RUNX3基因异常甲基化与患者病理分化程度(r =0.314,P =0.018)、淋巴结转移(r =0.370,P =0.005)显著相关。
在5-Aza-cdR 处理前,胰腺癌细胞株PANC1、CFPAC-1、SW1990的RUNX3mRNA 无表达或低表达,经5-Aza-cdR 处理后各胰腺癌细胞株RUNX3mRNA 恢复表达。
不明原因复发性流产患者母胎界面Tim--3的表达开题报告

不明原因复发性流产患者母胎界面Tim--3的表达开题报告一、研究背景复发性流产是指女性在孕期前三个月内先后两次或以上发生自然流产的一种常见的妊娠并发症。
目前复发性流产的病因尚不明确,但研究表明母胎免疫耐受的破坏是其主要机制之一。
母胎免疫耐受指的是孕妇体内的免疫系统和胎儿之间的相互作用,使得胎儿在母体中不被免疫系统攻击。
然而,一旦这种免疫耐受被破坏,就会导致免疫攻击胎儿,从而引起流产。
Tim-3(T细胞免疫球蛋白领家)是一种可通过与Galectin-9(Gal-9)相互作用来抑制免疫细胞活性的膜表面受体,在许多自身免疫性疾病和某些感染中发挥了重要作用。
目前研究发现,Tim-3在母胎界面的表达可能会影响母胎免疫耐受,但其在复发性流产的发生中的作用尚不明确。
因此,本研究旨在探讨不明原因复发性流产患者母胎界面Tim-3表达的情况及其与复发性流产的关系,为治疗该疾病提供新的思路和方法。
二、研究目的1.探究不明原因复发性流产患者母胎界面Tim-3表达的特点。
2.研究母胎界面Tim-3表达与复发性流产的关系。
三、研究方法1.研究对象:选择50例不明原因复发性流产患者及50例健康产妇作为对照组,采集其胎盘组织样本。
2.实验方法:采用免疫荧光染色法检测胎盘中Tim-3的表达情况,并通过统计学方法分析不同组别之间的差异和相关性。
四、研究意义本研究可以深入了解复发性流产的发病机制,为临床治疗提供新的思路和方法。
通过探讨母胎界面Tim-3的表达情况及其与复发性流产的关系,有助于我们更好地认识这种患者免疫系统的特点,为制定个性化的治疗方案提供依据。
血流向量成像技术定量评估慢性肾脏病患者左室功能的临床价值

·临床研究·血流向量成像技术定量评估慢性肾脏病患者左室功能的临床价值王伟白晖周金玲常青王岳恒摘要目的应用血流向量成像(VFM)技术分析慢性肾脏病患者左室能量损耗(EL)变化,探讨其评估慢性肾脏病患者左室功能受损的临床价值。
方法选取慢性肾脏病患者61例,其中左室射血分数(LVEF)≥50%者42例(A组),LVEF<50%者19例(B组),另选取38例健康成人为正常对照组。
应用VFM技术获取各组左室充盈早期、左房收缩期、等容收缩期及射血期平均EL(E-EL-ave、A-EL-ave、I-EL-ave及Ej-EL-ave)。
比较各组上述参数的差异,绘制受试者工作特征曲线分析其诊断不同程度左室功能受损的诊断效能,分析各时相EL与常规超声参数的相关性。
结果与正常对照组比较,A组各时相EL均升高,B组A-EL-ave升高,Ej-EL-ave降低,差异均有统计学意义(均P<0.05)。
Ej-EL-ave在正常对照组、A组、B组表现为双相变化趋向。
Ej-EL-ave对慢性肾脏病患者早期左室功能受损及LVEF< 50%均有良好的诊断效能(曲线下面积分别为0.907、0.861,均P<0.001)。
慢性肾脏病患者Ej-EL-ave与LVEF呈正相关(r=0.636,P<0.01)。
结论VFM技术所测参数Ej-EL-ave可以作为评估慢性肾脏病患者左室泵功能效率的潜在新指标,有一定的临床应用价值。
关键词血流向量成像;心室功能,左;能量损耗;肾脏病,慢性[中图法分类号]R540.45;R692.9[文献标识码]AQuantitative assessment of left ventricular function in patients with chronickidney disease by vector flow mappingWANG Wei,BAI Hui,ZHOU Jinling,CHANG Qing,WANG YuehengDepartment of Cardiac Ultrasound,the Second Hospital of Hebei Medical University,Shijiazhuang050000,ChinaABSTRACT Objective To analyze the change characteristics of left ventricular energy loss(EL)in chronic kidney disease by vector flow mapping(VFM)technique,and to explore the clinical value of EL in quantitative evaluating left ventricular function in patients with chronic kidney disease.Methods Sixty-one patients with chronic kidney disease were selected in this study,including42patients with left rentricular ejection fraction(LVEF)≥50%in group A,19patients with LVEF<50%in group B,38healthy adults were enrolled as control group.Left ventricle average EL in early filling phase(E-EL-ave),atrial filling phase(A-EL-ave),isovolumic contraction period(I-EL-ave),and ejection phase(Ej-EL-ave)were acquired and calculated by VFM technique,and the differences of above parameters in each group were compared.Receiver operating characteristic curve was drawn to analyze the diagnostic efficacy of different degrees of left ventricular dysfunction.The relationship between EL in each phase and conventional ultrasound parameters were analyzed.Results Compared with the control group,EL in all phases of group A were increased,A-EL-ave was increased in group B,and Ej-EL-ave was decreasedin group B.The differences were statistically significant(all P<0.05).Ej-EL-ave showed a biphasic trend in the control group,group A and group B.Ej-EL-ave had good diagnostic efficacy for early left ventricular function impairment and LVEF<50%in patients with chronic kidney disease(area were0.907,0.861,respectively,both P<0.001).Ej-EL-ave was positively correlated with LVEF in the patients with chronic kidney disease(r=0.636,P<0.01).Conclusion The parameter of Ej-EL-ave measured by VFM technique can be used as a potential new indicator to evaluate the efficiency of left ventricular pump function in patients with chronic kidney disease,which has certain clinical value.KEY WORDS Vector flow mapping;Ventricular function,left;Energy loss;Kidney disease,chronic基金项目:河北省卫生健康委青年科技课题(20210496)作者单位:050000石家庄市,河北医科大学第二医院心脏超声科通讯作者:王岳恒,Email:*****************慢性肾脏病是冠状动脉粥样硬化性心脏病、慢性心力衰竭等常见心血管疾病的独立危险因素[1]。
检测细胞凋亡的三种流式方法
三种流式方法检测细胞凋亡1、检测形态学及细胞膜完整性的Hoechs-PI双染色法细胞发生凋亡时,其细胞膜的通透性也增加,但其程度介于正常细胞和坏死细胞之间,利用这一特点,被检测细胞悬液用荧光素染色,采用流式细胞仪测量细胞悬液中细胞荧光强度来区分正常细胞、坏死细胞和凋亡细胞。
常用Hoechs-PI染色法,正常细胞对染料有拒染性,荧光着色很浅,凋亡细胞主要摄取hoechs-PI染料,呈现强蓝色荧光,而坏死细胞主要摄取碘化丙啶(PI)而呈红色荧光。
2、DNA片段原位标记凋亡细胞DNA片段原位末端检测技术是指在细胞(或组织)结构保持不变的情况下,用荧光素、地高辛或生物素标记的脱氧尿三磷酸(deoxyuridinetriphate,UDTP)和末端脱氧核苷酸转移酶(terminal deoxynucleotidy1 transferase,TdT)相反应与凋亡细胞裂解后3'的羟基(-OH)端相结合经显色反应后检测DNA裂解点的技术。
DNA片段原位标记法有两种(1)原位缺口转移(in situ nick-translation,ISNT)技术,该技术是1994年由Fehsel等提出,它是利用DNA多聚酶I将标记的核苷酸接到断裂的3'-OH端(2)原位缺口末端原位标记技术(in situ end labelling technique,ISEL),该技术即TUNEL法,于1993年由Wijsman等提出,它是利用TdT将标记DUTP接到3'-OH端。
研究证明,TUNEL的敏感性远高于尤其对早期凋亡的检出TUNEL更为适用。
其原因可能是凋亡发生时DNA大多是双链同时断裂而单链断裂少见。
ISNT是依赖DNA多聚酶I的单链修复反应,故阳性率较低。
细胞凋亡时DNA断裂早于形态学改变及DNA含量减少。
因此该法较前述各法具有更高的灵敏性,但环死细胞亦有DNA裂点形成。
因此环死亦可呈TUNEL阳性反应。
沉默AQP3基因表达对结直肠癌细胞增殖、凋亡和化疗敏感性的影响
沉默AQP3基因表达对结直肠癌细胞增殖、凋亡和化疗敏感性的影响作者:郑斯鑫周春华孔文成尹光来源:《中国现代医生》2021年第31期[摘要] 目的探討沉默水通道蛋白3(AQP3)基因表达对结直肠癌细胞增殖、凋亡和化疗敏感性的影响。
方法体外培养结直肠癌细胞LoVo,采用梯度浓度诱导法建立紫杉醇耐药细胞株LoVo/Taxol。
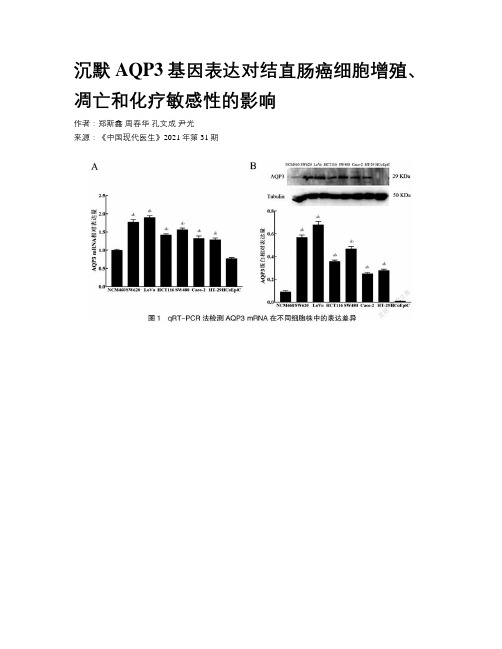
将LoVo细胞和LoVo/Taxol细胞分别分为空白对照组(细胞不做任何特殊处理)、阴性对照组(转染阴性对照质粒)、shAQP3组(沉默AQP3表达),逆转录-聚合酶链反应(qRT-PCR)和Western blot法检测AQP3 mRNA和蛋白表达。
CCK-8实验检测细胞的增殖能力,流式细胞术检测细胞的凋亡情况。
四唑化合物(MTS)检测紫杉醇的细胞毒性。
结果人结肠癌细胞LoVo中AQP3 mRNA相对表达量和蛋白表达量均高于人正常结肠上皮细胞NCM460和HCoEpiC,差异有统计学意义(P<0.05)。
敲低AQP3表达后,shAQP3组LoVo细胞增殖活性(OD值)较空白对照组和阴性对照组降低,同时凋亡率升高,差异有统计学意义(P<0.05)。
成功构建LoVo/Taxol耐药细胞,对紫杉醇、5-Fu、阿霉素的耐药指数分别为(31.97±1.78)、(17.97±2.14)、(104.80±5.53)。
而shAQP3组LoVo/Taxol细胞对紫杉醇、5-Fu、阿霉素的耐药指数分别为(6.06±0.25)、(5.57±0.20)、(21.23±0.27),较空白对照组和阴性对照组明显降低,差异有统计学意义(P<0.05)。
结论沉默AQP3基因表达能够抑制结直肠癌细胞增殖,促进结直肠癌细胞凋亡并增强LoVo/Taxol耐药细胞的化疗敏感性。
[关键词] AQP3;结直肠癌;增殖;凋亡;化疗敏感性[中图分类号] R735.3 [文献标识码] A [文章编号] 1673-9701(2021)31-0006-06[Abstract] Objective To explore the effect of silencing aquaporin 3 (AQP3) gene expression on the proliferation, apoptosis, and chemosensitivity of colorectal cancer cells. Methods LoVo colorectal cancer cells were cultured in vitro, and the LoVo/Taxol paclitaxel-resistant cell lines were established by gradient concentration induction method. The LoVo cells and LoVo/Taxol cells were divided into the blank control group (no special treatment), the negative control group (negative control plasmid transfection), and the shAQP3 group (silencing AQP3 expression). Reverse transcription-polymerase chain reaction (qRT-PCR) and Western blot method were used to detect AQP3 mRNA and protein expression. CCK-8 experiment was used to detect cell proliferation ability, and flow cytometry was used to detect cell apoptosis. Tetrazolium compound (MTS) was used to detect the cytotoxicity of paclitaxel. Results The AQP3 mRNA relative expression and protein expression in human colon cancer cells LoVo were higher than those in human normal colonic epithelial cells NCM460 and HCoEpiC,the difference was statistically significant (P<0.05). After knocking down the AQP3 expression, the proliferation activity (OD value) of LoVo cells in the shAQP3 group was lower than those in the blank control group and the negative control group, and the apoptosis rate was higher than those in the blank control group and the negative control group,the difference was statistically significant(P<0.05). The LoVo/Taxol resistant cells were successfully constructed, and the resistance indexes to paclitaxel, 5-Fu and adriamycin were (31.97±1.78),(17.97±2.14),(104.80±5.53), respectively. The resistance indexes of LoVo/Taxol cells to paclitaxel, 5-Fu and adriamycin in the shAQP3 group were (6.06±0.25),(5.57±0.20),(21.23±0.27), respectively, which were significantly lower than those in the blank control group and the negative control group,the difference was statistically significant(P<0.05). Conclusion Silencing AQP3 gene expression can inhibit the proliferation of colorectal cancer cells, promote the apoptosis of colorectal cancer cells, and enhance the chemosensitivity of LoVo/Taxol resistant cells.[Key words] AQP3; Colorectal cancer; Proliferation; Apoptosis; Chemosensitivity2018年,中国结直肠癌发病率占世界的24.3%,病死率占世界的22.9%,且逐渐呈现年轻化趋势[1]。
依托咪酯调节AMPK
广东药科大学学报Journal of Guangdong Pharmaceutical University Mar.2024,40(2)依托咪酯调节AMPK/NLRP3信号通路对急性心肌梗死大鼠心肌损伤的影响张化,王艳萍(郑州大学第一附属医院麻醉与围术期医学部,河南郑州450000)摘要:目的探究依托咪酯调节腺苷酸活化蛋白激酶(AMPK)/核苷酸结合寡聚化结构域样受体蛋白3(NLRP3)信号通路对急性心肌梗死(AMI)大鼠心肌损伤的影响。
方法取SD大鼠通过结扎左冠状动脉前降支建立AMI模型,随机分为模型组、依托咪酯组、Dorsomorphin组、依托咪酯+Dorsomorphin组,每组12只,另取12只大鼠作为假手术组开胸后不结扎,分组处理后检测各组大鼠心功能、心肌组织病理损伤及纤维化、血清乳酸脱氢酶(LDH)、肌酸磷酸激酶(CPK)、白细胞介素(IL)-1β、IL-6、超氧化物歧化酶(SOD)与丙二醛(MDA)水平、心肌组织IL-1β、IL-6、SOD与MDA水平、心肌组织AMPK/NLRP3通路相关蛋白表达。
结果与假手术组相比,模型组大鼠心肌组织呈严重病理损伤,左室舒张末期内径(LVDD)、左室收缩末期内径(LVDS)、心肌胶原容积分数(CVF)、血清LDH、CPK、IL-1β及IL-6水平、心肌组织IL-1β、IL-6及MDA水平、心肌组织NLRP3蛋白表达明显升高(P<0.05),左室射血分数(EF)、血清及心肌组织SOD水平、心肌组织p-AMPK/AMPK明显降低(P<0.05)。
与模型组相比,依托咪酯组大鼠心肌组织病理损伤减轻,LVDD、LVDS、心肌CVF、血清LDH、CPK、IL-1β及IL-6水平、心肌组织IL-1β、IL-6及MDA水平、心肌组织NLRP3蛋白表达均降低(P<0.05),EF、血清及心肌组织SOD水平、心肌组织p-AMPK/AMPK升高(P<0.05);Dorsomorphin组大鼠各指标变化趋势与依托咪酯组相反,且Dorsomorphin可减弱依托咪酯对模型组大鼠各指标的作用。
defuse3研究入组标准

defuse3研究入组标准
DEFUSE 3是一项多中心、随机、开放标签、盲法评价结局的临床研究,旨在明确距最后正常时间6-16小时的大血管(ICA或M1)闭塞患者,是否可以从取栓治疗中获益。
该研究的入组标准如下:
1. 年龄:年龄中位数为70岁(四分位间距:59\~80岁)。
2. 症状出现时间:距最后正常时间6\~16小时。
3. 血管闭塞位置:大血管(ICA或M1)闭塞。
4. 其他标准:需要满足一定的医学条件,例如无取栓禁忌症、符合影像学标准等。
具体来说,该研究排除了SWIFT-PRIME和REVASCAT研究中80岁以上的患者,以及年龄超过90岁的患者。
血管内治疗组的获益随着年龄的增加而明显下降,而对照组的预后受年龄影响较小。
无论患者年龄小于还是等于80岁,还是大于80岁,血管内治疗均有获益。
以上内容仅供参考,具体情况可能会随临床研究和医疗技术的发展而变化。
具体的入组标准还应以医生和医疗研究机构的要求为准。
基于微流控技术的癌症筛查技术研究
基于微流控技术的癌症筛查技术研究癌症是全球最常见的死亡原因之一,每年有数百万人因癌症去世。
有效的癌症筛查与早期诊断是预防癌症死亡的关键,因为早期诊断可以提高患者的生存率。
然而,传统的癌症筛查方法通常需要大量的检测样本并消耗大量的时间和资源。
因此,开发在早期诊断和预测癌症方面具有高准确性且简便快捷的技术是非常重要的。
基于微流控技术的癌症筛查技术是一种新型的、高效的癌症诊断技术,其基本原理是将生物样本转移到微小通道中,使用微流控技术控制流体的移动和混合,以实现快速、高通量的细胞和分子分析。
这种技术可以通过使用单细胞分析技术来检测少量细胞的异常物质,用于早期癌症的诊断和预测。
多个研究小组已经采用微流控技术开发了各种常见癌症的筛查技术,包括前列腺癌症、乳腺癌症、卵巢癌症和肺癌症等。
这些筛查技术基于微流控芯片,通过使用经过功能化的芯片表面,可定向捕获特定的生物分子或细胞。
该技术的好处之一是可以通过单细胞的分析来检测少量的异常细胞,从而提高癌症的早期诊断率。
其中,前列腺癌症是最常见的男性恶性肿瘤之一。
传统的前列腺癌筛查方法仅基于前列腺特异性抗原(PSA)检测,因此存在误诊和过度诊断的问题。
最近开发的基于微流控技术的前列腺癌症筛查技术通过检测前列腺癌症细胞的特定蛋白质,可以提高癌症的筛查准确性。
同样地,基于微流控技术的肺癌症筛查技术可以通过检测细胞的细胞表面分子,来识别肺癌症的早期相。
此外,某些微流控技术可以用于检测环境中的致癌物质如多环芳烃。
一种常见的微流控芯片被设计成从水中捕获致癌物质的微小分子,然后将其浓缩和分析。
实验结果显示,该技术在检测环境化学污染物方面表现出良好的灵敏度和选择性。
虽然微流控技术在癌症诊断和预测上的应用前景广泛,但它们仍面临一些挑战。
首先,加速制造微流控芯片的过程并降低成本仍需进一步完善。
其次,将微流控技术转化为实际的床旁应用需要在工程、自动化和数据分析等各个方面进行深入研究。
最后,如何将微流控技术结合其他生物医学方法以进一步提高诊断准确性和影像分析的效率也是关键问题之一。
流动注射Omnion 3.0工作站菜单中英文对照表
Header&Footer
Header报表的页眉
Footer报表的页角
Calculations
计算
流动注射-流程图中文对照表
硝氮/亚硝氮
CARRIER(green)
载液-水
Sulfanilamide Color Reagent(orange)
通常不选
Calibration Weighting
重量方法
通常为「None」
AutoDilution Trigger
自动稀释
%of Hight Standard
超过浓度上限
通常为「110」
QuikChem Method
分析方法编号
Analyres-Channel
Description
Channel OFF
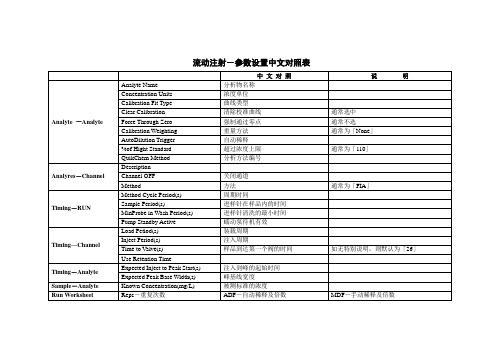
流动注射-参数设置中文对照表
中文对照
说明
Analyte-Analyte
Analyte Name
分析物名称
Concentration Units
浓度单位
Calibration Fit Type
曲线类型
Clear Calibration
清除校准曲线
通常选中
Force Through Zero
强制通过零点
磺胺显色剂
Ammonia Buffer(yellow)
氯化铵缓冲溶液
阴离子洗涤剂
Chloroform(yellow/yellow)
氯仿
Alk MB 2(gray/gray)
载液-碱性亚甲基蓝
Acidic MB(white/white)
酸性亚甲基蓝
氨氮
基于STM32植物动态离子流信号检测系统设计

基于STM32植物动态离子流信号检测系统设计张永凯;王晓冬;周航;赵建平;王成【摘要】溶液中无机盐离子的定向流动会产生微弱的电压信号,通过检测电压信号可以计算离子的浓度、植物根系吸收离子的速度,进而获取植物的生理信息;对植物动态离子流信号检测系统进行设计,采用STM32F103ZET6作为主控芯片,利用极低偏置电流放大芯片和高共模抑制比差分放大芯片,给出了信号放大、滤波处理和数据采集电路,对系统噪声来源进行分析,提出了降低噪声的方法,并通过STM32进行A/D转换,把转换数据传输到上位机;该设计实现了植物动态离子流信号的检测,得到了离子在溶液中的流速.【期刊名称】《计算机测量与控制》【年(卷),期】2016(024)003【总页数】4页(P145-148)【关键词】离子流信号;检测系统;STM32F103ZET6;信号放大;A/D转换【作者】张永凯;王晓冬;周航;赵建平;王成【作者单位】北京农业智能装备技术研究中心,北京100089;曲阜师范大学物理工程学院,山东曲阜273165;北京农业智能装备技术研究中心,北京100089;国家农业智能装备工程技术研究中心,北京100089;北京农业智能装备技术研究中心,北京100089;国家农业智能装备工程技术研究中心,北京100089;曲阜师范大学物理工程学院,山东曲阜273165;北京农业智能装备技术研究中心,北京100089;国家农业智能装备工程技术研究中心,北京100089【正文语种】中文【中图分类】TP311目前国内离子流信号检测技术大多应用在动物学领域,植物动态离子流信号的检测研究相对较少。
由于植物吸收离子产生的电压极其微弱,只有几十微伏到几百微伏,难以直接检测,需要特定的玻璃管电极把检测到的动态离子流信号转换为电信号,并进行放大与处理。
但微弱信号的检测和信号放大与处理存在一定困难,如运算放大器的零漂、噪声、外接干扰等,都将严重地影响着信号的保真与提取[1]。
TIMI危险积分与N-末端脑利钠肽前体在非ST段抬高急性冠脉综合征患者中的相关性研究

TIMI危险积分与N-末端脑利钠肽前体在非ST段抬高急性冠脉综合征患者中的相关性研究王恩荣;杨文灿【期刊名称】《山东医学高等专科学校学报》【年(卷),期】2010(032)003【摘要】目的探讨非ST段抬高急性冠脉综合征(NSTEACS)患者TIMI危险积分与血浆N-末端脑利钠肽前体(NT-ProBNP)水平的相关性.方法入选70例非ST段抬高急性冠脉综合征患者,对其进行TIMI危险评分积分,并进行危险分层,采用荧光免疫法测定血浆NT-ProBNP水平,分析其与TIMI危险积分不同层次之间的关系.结果血浆NT-ProBNP水平与TIMI危险积分呈正相关(r=0.71,P<0.05);随着TIMI 危险积分评分值增加,血浆NT-ProBNP水平亦逐渐升高,随访期主要心血管事件发生率也增多(P<0.05).结论 TIMI危险积分与NT-ProBNP水平呈正相关,并与NSTEACS预后有关,能对患者进行危险分层.【总页数】3页(P161-163)【作者】王恩荣;杨文灿【作者单位】新汶矿业集团中心医院心内科,山东新泰,271233;新汶矿业集团中心医院心内科,山东新泰,271233【正文语种】中文【中图分类】R541.4【相关文献】1.血清N-末端脑钠肽前体及脑利钠肽预测非瓣膜性房颤患者的栓塞危险性 [J], 王丽丽;刘强;赵有生;陈绮映;左辉华2.N-端脑利钠肽前体检测在心脏病患者中的应用价值分析 [J], 杨连成3.N-末端脑利钠肽前体与急性冠脉综合征的相关性研究 [J], 贺利平;赵兴胜4.GRACE危险评分与N-末端脑钠肽前体在非ST段抬高急性冠脉综合征患者中的临床研究 [J], 葛璘;陈湘5.N-端前B型利钠肽较TIMI危险积分对急性心肌梗死后死亡风险的预测价值更佳[J], Khan SO;Quinn P;Davies JE;袁志敏(摘译);刘运德(校)因版权原因,仅展示原文概要,查看原文内容请购买。
用于检测糖尿病标志物的电子鼻优化设计

用于检测糖尿病标志物的电子鼻优化设计奉轲;花中秋;伍萍辉;李彦;曾艳;王天赐;邱志磊【期刊名称】《传感技术学报》【年(卷),期】2018(031)001【摘要】人体呼气中的丙酮含量可作为糖尿病的标志物.为实现无创糖尿病诊断,设计以金属氧化物半导体气敏传感器阵列为核心的人工嗅觉系统,对完成痕量丙酮的快速检测具有重要意义.通过多个气体流量控制器MFC(Mass Flow Controller)分别配制出模拟糖尿病患者呼气样本(30×10-6丙酮)与另两种干扰气体样本(30×10-6乙醇样本、15×10-6丙酮与15×10-6乙醇混合样本)进行实验,基于BP神经网络算法对3种气体定性识别,并通过主成分分析PCA(Principal Component Analysis)算法对原始的高维特征子集进行降维优化.实验表明:PCA与BP算法相结合,可降低BP神经网络的复杂性、减少预测的误差,同时能够解决单个气体传感器交叉敏感问题,进而提高对气体的选择性.对痕量丙酮样本与另两种干扰气体样本进行分析识别,识别的结果显示:对3种样本的识别准确率为91%.该研究为准确识别糖尿病标志物实现无创诊断技术提供了理论指导.%The content of acetone in human exhalation can be used as a marker of diabetes. In order to achieve the noninvasive diagnosis of diabetes,we design a metal oxide semiconductor gas sensors array as the core of the artifi-cial olfactory system,,which is of great significance in rapid detection of trace acetone. Through multiple Mass Flow Controller(MFC),we prepared simulated diabetic patients breath samples(30×10-6 acetone)and two interference ga s samples(30×10-6 ethanol/composition of 15×10-6 acetone and15×10-6 ethanol),Three kinds of gas qualitative identifications were carried out based on BP neural network algorithm and optimization of the original high dimen-sional feature subset was achieved through PCA algorithm. The experiment shows that the combination of PCA and BP algorithm can reduce the complexity of BP neural network and reduce the error of prediction. At the same time, the cross sensitivity of individual gas sensors can be solved,thus improve the selectivity of gas d. The identification results of trace acetone and the two interference gas samples show that the accuracy of the recognition of the three gases reaches 91%. This study provides theoretical guidance for accurate identification of diabetes markers and non-invasive diagnosis.【总页数】6页(P13-18)【作者】奉轲;花中秋;伍萍辉;李彦;曾艳;王天赐;邱志磊【作者单位】河北工业大学电子信息工程学院,天津300401;河北工业大学电子信息工程学院,天津300401;天津市电子材料与器件重点实验室,天津300401;河北工业大学电子信息工程学院,天津300401;天津市电子材料与器件重点实验室,天津300401;河北工业大学电子信息工程学院,天津300401;河北工业大学电子信息工程学院,天津300401;河北工业大学电子信息工程学院,天津300401;河北工业大学电子信息工程学院,天津300401【正文语种】中文【中图分类】TP212【相关文献】1.电子鼻结合化学计量法用于检测黄酒酒龄 [J], 张振;李臻锋;宋飞虎;李静;徐晚秀2.一种用于蔬菜病害检测的电子鼻的设计 [J], 张锐敏;卢佩;周涛;钟福如3.电子鼻对非小细胞肺癌挥发性标志物检测的可行性 [J], 徐珍琴;丁露;刘虎;程杰4.用于山核桃陈化时间检测的电子鼻传感器阵列优化 [J], 徐克明;王俊;邓凡霏;韦真博;程绍明5.结合基因工程的生物电子鼻用于气味检测的研究 [J], 朱平;田玉兰;陈雅婷;陈炜;杜立萍;吴春生因版权原因,仅展示原文概要,查看原文内容请购买。
kgn细胞流式参数
kgn细胞流式参数
KGN细胞是一种人类卵巢颗粒细胞瘤细胞株,常用于研究卵泡发育和功能调控的细胞模型。
在流式细胞仪中,可以使用不同的参数来对KGN细胞进行表型和功能分析。
以下是一些常用的流式细胞参数:
1. 细胞大小(Forward Scatter,FSC):用于测量细胞的大小和形态,可以反映细胞的状态和增殖能力。
2. 细胞复杂度(Side Scatter,SSC):用于测量细胞内组分的复杂程度,如细胞器数量和大小,细胞内颗粒的含量等。
3. 细胞表面标记物(Surface Markers):通过标记特定的细胞表面蛋白,可以对KGN细胞进行表型分析。
例如,可以使用抗体标记细胞表面的受体或配体,以研究细胞的信号转导通路。
4. 细胞周期(Cell Cycle):通过染色剂如荧光素丁酸(Propidium Iodide)或霉素(BrdU)标记细胞DNA,可以对KGN细胞的细胞周期进行分析,包括细胞的G1、S、G2和M期。
5. 细胞凋亡(Apoptosis):通过染色剂如Annexin V和PI (Propidium Iodide)标记细胞膜磷脂外翻和核酸破损,可以对KGN 细胞的凋亡程度进行分析。
6. 细胞内标记物(Intracellular Markers):通过渗透染料或抗体标记
细胞内的蛋白或分子,可以对KGN细胞的内部分子水平进行定量分析。
例如,可以标记细胞内的转录因子、细胞骨架蛋白或细胞器等。
这些参数可以帮助研究者了解KGN细胞的生理状态、分子表达和功能特性,从而深入研究卵泡发育和卵巢功能调控的机制。
tff3基因名
tff3基因名
TFF3,全称为Trefoil factor 3,是一种编码蛋白质的基因。
这个基因在人类体内广泛表达,特别在消化系统中的黏膜上皮细胞中。
TFF3蛋白质主要起着维护黏膜完整性和促进伤口愈合的作用。
TFF3蛋白质在肠道黏膜细胞中的表达与许多生理和病理过程有关。
首先,它是肠道黏膜上皮细胞的保护性因子之一。
当黏膜受到损伤或炎症时,TFF3会被释放出来,形成一种保护性的黏液层,覆盖在黏膜表面,起到保护黏膜免受进一步损伤的作用。
TFF3还参与了肠道黏膜细胞的再生和修复过程。
当黏膜受损时,TFF3的表达会增加,促进黏膜上皮细胞的增殖和迁移,加速伤口的愈合。
TFF3通过与细胞表面受体结合,激活一系列信号通路和细胞因子,促进细胞增殖和迁移过程。
研究还发现TFF3在肿瘤发生和发展中也起着重要作用。
TFF3的异常表达与多种癌症的发生和预后有关,包括胃癌、结肠癌等。
TFF3通过调节细胞凋亡、增殖、迁移和转移等生物学过程,参与了肿瘤的发生和转移。
总体而言,TFF3基因编码的蛋白质在肠道黏膜细胞中发挥着重要的生物学功能。
它既是黏膜保护的关键因子,又是黏膜修复和再生的重要调节因子。
此外,TFF3还与癌症的发生和发展密切相关。
深入研究TFF3的功能和调控机制,对于理解肠道黏膜的生理与病理过
程,以及寻找新的治疗策略具有重要意义。
一种新的基于钟控浮栅MOS电路的采样保持电路

基于钟控神经元MOS管的新型采样保持电路杭国强1,2, 李锦煊1, 王国飞1(1. 浙江大学信息与通信工程研究所, 浙江杭州310027; 2. 浙江省综合信息网技术重点实验室, 浙江杭州310027)摘要:提出一种新的采样保持电路,该电路采用钟控神经元MOS管. 电路引入了阈值补偿单元,克服了单管神经元MOS管跟随电路输出电压和输入电压有一个阈值电压损失这一缺点,提高了采样保持电路的精度. 由于引入阈值补偿技术,电路可以采用1.5V的低电压供电,并且由于采用具有高功能度的钟控神经元MOS管,电路的结构和功耗都比传统的采样保持电路有了很大的改良. 采用TSMC 0.35μm 双层多晶硅CMOS工艺参数的HSPICE模拟结果验证了所提出设计方案的正确性. 最后对仿真结果与已有的采样保持电路方案进行了分析与比较.关键字:浮栅MOS;钟控神经元MOS;采样保持A novel S/H circuit based on the clock-controlledneuron-MOS transistorHANG Guo-qiang1,2, LI Jin-xuan1, WANG Guo-fei1(1. Institute of Information and Communication Engineering, Zhejiang University , Hangzhou, 310027, China; 2. Zhejiang Provincial Key Laboratory of Information Network Technology,Zhejiang University , Hangzhou, 310027,China)Abstract:Keyword: floating-gate MOS; clock-controlled neuron-MOS; S/H1引言采样保持电路是实现连续时间信号转变为离散时间信号的关键部件. 对于高速高精度的ADC来说,要求采样保持电路具有较高的采样精度和采样频率. 而对一些结构庞大,精度要求相对不苛刻的系统(如神经网络,匹配滤波器等),简化采样保持电路结构以及降低功耗更具实际意义. 传统的采样保持电路,是通过运算放大器和电容来实现的,采样精度越高,要求运算放大器的放大倍数越高,电路的结构也越复杂. 多输入浮栅MOS器件或称神经元MOS(neuron-MOS)器件是近年来提出的一种具有功能性强、阈值控制灵活等特点的新型器件[1], 基于该器件设计的采样保持电路,具有结构简单、功耗低等特点.文献[2,3]采用浮栅器件构造了一个模拟反相器,在此基础上设计了一个采样保持电路,实现了简化电路结构,降低电路功耗等目的. 然而,这个电路的性能与反相器输入输出特性曲线在工作点附近的斜率有关,斜率越大,性能越好. 实际电路中, 这个斜率不可能达到无限大,因此不可避免地会引入一些误差,对接近于0或者电源电压的输入信号,存在较大的误差. 该设计方案不具备轨到轨的输出特点. 本文提出一种新的采用钟控神经元MOS管的采样保持电路,该电路实现了轨到轨的输出,具有更高的精度和更低的功耗. 采用HSPICE在TSMC 0.35um的工艺下对所设计电路进行了模拟,并给出了与以往设计的性能比较.2 钟控神经元MOS 管钟控神经元MOS 管和普通的神经元MOS 管一样,各个输入信号通过耦合电容耦合输入,在浮栅上面耦合出一个加权的电压之和,加权值由对应的耦合电容值来决定. 两者的不同之处,就是普通神经元MOS 管有一个浮置的栅极,而钟控神经元MOS 管的浮栅是通过一个开关接到一个参考电压,从而可以对浮栅的初始电压进行设置. 钟控神经元MOS 管的结构图如图1所示:……Vin V 1V nφ图1钟控神经元MOS 管的结构图Fig.1 structure of the clock-controlled neuron-MOS transistor钟控神经元MOS 管的工作分为两个阶段:预充电阶段和评估阶段. 在预充电阶段,各个输入电容耦合端接到电容输入预置电压V iREF 上面,开关信号φ为高电平,开关闭合,浮栅输入电压V in 与浮栅连通,将浮栅钳位. 在评估阶段,开关信号φ为低电平,开关断开,浮栅浮置,相应地,输入电容耦合端切换到各自的输入信号V i . 此时,浮栅的电压由φ从高跳到低时V in 的瞬间值(记为V INREF )、输入电容耦合端预置电压V iREF 和输入端电压V i 共同决定.根据以上描述,在预充电阶段,浮栅接到浮栅输入电压V in ,浮栅输入电压对浮栅充电,因此,有1FG in V V = (1) 在预充电阶段切换到评估阶段的瞬间,V in 的值记为V INREF ,用作评估阶段浮栅电压的计算. 在评估阶段,因为浮栅浮置,浮栅上的电荷不会改变,可以算得此时电压为:12()n i i iREF i FG INREF TOT C V V V V C =-=+∑ (2) 式中,1n TOT iGD GS GB OX i C C C C C C ==++++∑ ,V INREF 是浮栅预置电压,V iREF 是输入预置电压. 令开关信号φ,当开关闭合时,φ= VDD ,当开关断开时,φ=0. 综合(1)(2)两式可得[4,5]:1()(1)n i i iREF i FG INREF DD TOTC V V V V V C φ=-=+-∑ (3) 3 采用钟控神经元MOS 管的采样保持电路基于钟控神经元MOS 管的采样保持电路以其具有结构简单,功耗低等优点被提出来,基本结构[6]如图2所示:V inoutφ图2基于钟控神经元MOS 管的采样保持电路基本结构Fig.2 The basic structure of a S/H circuit based on the clock-controlled neuron-MOS transistor此采样保持电路分为采样、保持、跟随三个阶段. 在采样阶段,开关信号1φ为高电平,开关信号2φ为低电平,输入电平V in 对浮栅充电,等到浮栅充电完成时,浮栅电压和输入电压V in 一致. 在保持阶段,开关信号1φ变为低电平,此时浮栅浮置,浮栅上的电荷不会改变,并且可以长期保存. 在跟随阶段,2φ变为高电平,V out 跟随浮栅的电压输出.这个结构的跟随电路,浮栅电压和最后的输出电压V out 之间会有一个nMOS 管阈值电压的损失. 由于这个阈值电压损失的存在,大大降低了跟随电路的精确度,并且,电源电压不可能降得很低,否则,损失的值会产生很大的影响.而另一个基于准浮栅MOS 管的采样保持电路[2,3],采用一个模拟反相器,并且用一个电容,将输出电压反馈回反相器的输入端,从而构造一个采样保持电路,电路结构如图3所示. 当SAMPLE 信号为高电平时,是采样阶段,当SAMPLE 信号为低电平时,是保持阶段. 这个采样保持电路的性能,是基于反相器输入输出曲线的特性的. 反相器的输入输出曲线在工作点的斜率越大,采样保持电路的性能越好,当反相器的斜率达到无限大时,采样保持电路的输出电压无限接近于输入电压. 但是,实际中反相器的输入输出曲线斜率不可能无限大,因此,就会引入误差,降低了采样保持电路的线性度,并且使采样保持电路不具有轨到轨的特性.Vout图3基于准浮栅MOS 管的采样保持电路Fig.3 A S/H circuit based on the semi-floating-gate MOS transistor为了降低电源电压,提高跟随器的精度,本文提出了一种新的采样保持电路,电路结构如图4所示. 采样阶段,1φ为高电平,2φ、3φ为低电平,这样,M1的漏端会被上拉到一个比较高的电压值,浮栅被输入电压V in 充电,浮栅电压和输入电压V in 一致.V in图4基于钟控神经元MOS 管的新型采样保持电路Fig.4 A new S/H circuit based on the clock-controlled neuron-MOS transistor保持阶段,1φ、2φ为低电平,3φ为高电平. 这样,浮栅浮置,浮栅上的电荷不会改变,而M1的漏极电压会固定在M1的阈值电压值,并通过耦合电容,耦合叠加在浮栅上,此时,根据式(2),浮栅上的电压为:1*th FG INREF INREF th TOT C V V V V V C =+≈+ (4) 式中,11TOT GD GS GB OX C C C C C C C =++++≈,th V 是M1的阈值电压,INREF V 是浮栅预置电压,也就是1φ跳变之前V in 的值.跟随阶段,只要2φ变为高电平,就可以让V out 跟随浮栅电压输出,此时的输出电压'OUT FG th V V V =-,其中,'th V 是钟控神经元MOS 管的阈值电压. 因为钟控神经元MOS 管跟随器的损失电压为一个nMOS 管的阈值电压,并且因为采用一样的工艺和参数,所以,钟控神经元MOS 管的阈值电压值和M1的阈值电压值一样,即'th th V V =. 这样就可以让输出电压V out 精确等于输入电压V in ,实现精确跟随的效果. 实际应用中,跟随阶段和保持阶段可以合并,保持的同时实现跟随输出,这样,采样保持的过程只需要两个步骤.由于消除了阈值电压的损失,这个采样保持电路降低了对电源电压的要求,可以采用1.5V 的低电源电压供电. 整个电路只包括一个钟控神经元MOS 管,两个普通的MOS 管和若干辅助开关,所用的元器件非常少,可以大大减小电路芯片的面积. 因为采用了低电源电压,并且结构简单,所以电路的功耗非常低.4 模拟结果与比较图2所示采样保持电路与图4所示采样保持电路的差别就是,图2所示的电路,输出电压和输入电压存在一个阈值损失,而图4所示电路则带有一个阈值补偿电路,不存在阈值损失. 两电路的仿真对比波形如图5所示.图5原始结构与新型结构的采样保持电路仿真结果比较Fig.5 Compare of the S/H circuits between the original structure and the new structure上图分别是图2所示电路和图4所示电路的仿真对比图,采用的是TSMC 0.35um 工艺,wn/ln=2.625/0.35um , wp/lp=7.875/0.35um ,nMOS 阈值电压是0.464V ,pMOS 阈值电压是-0.706V. 输入信号是频率为0.67M 的正弦信号,采样时钟频率是20M. 从上图可以看出,对于图2所示电路,输出和输入电压有约为一个nMOS 管阈值电压的差值,并且,当输入电压小于阈值电压时,输出电压就变成0,不能继续对输入电压进行正确采样. 而对于图4所示的电路,因为引入了阈值补偿电路,输入和输出电压基本一致,不存在阈值损失,并且即使输入信号电压小于nMOS 管的阈值电压,采样保持电路也可以很好地对输入信号进行采样保持的操作.图3所示电路,是基于模拟反相器的采样保持电路,其性能取决于反相器的输入输出特性曲线在工作点的斜率,斜率无限大时,采样保持电路的性能最好. 这个电路的工作点总是在/2VDD 附近,即浮栅电压总能保持在/2VDD 左右. 但是,反相器在输入电压为/2VDD 时,输入输出特性曲线的斜率并不是无限大的,这样,采样保持电路就会产生误差,斜率越小,产生的误差就越大. 这个电路中,当输入电压为0或者VDD 的时候,电路的误差最大. 反相器的输入输出特性曲线如图6所示.工作点偏离VDD 越大,误差就越大. 图3所示电路和图4所示电路的仿真结果对比图如图7所示.图6反相器的输入输出曲线Fig.6 The input-output curve of the inverter图7 基于反相器的结构和新型结构的采样保持电路仿真结果比较Fig.7 The simulation results Compare between the structure based on the converter and thenew structure两电路都是采用TSMC 0.35um 工艺参数,输入信号是频率为0.67M 的正弦信号,采样时钟频率是20M. 上面是图3所示电路的波形,采用的是2V 的电源电压,当输入为2V 时,输出为1.87V ,误差约为6.5%左右. 输入为0时,输出为0.092V. 下面是图4所示电路的波形,采用的是1.5V 的电源电压,输入为1.5V 时,输出为1.48V ,误差约为1.3%左右. 输入为0时,输出为0.067V ,误差也比图3所示电路要小30%左右.图8 采用1.5V电源电压的图3所示电路仿真波形当把图3所示电路的电源电压降低成1.5V时,波形如图8所示.对于20M的采样频率,在保持阶段,此电路输出数据不能稳定,性能大大下降.功耗方面,图2所示电路不存在直流功耗,并且结构最简单,因而功耗也最低,其平均功耗只有0.0059mw. 图3所示电路,分为反相器部分和非反相器部分,其中,因为浮栅VDD附近,所以,反相器部分一直都存在直流功耗. 而非反相器部分,采电压一直都在/2样阶段,不存在直流功耗,保持阶段,存在直流功耗. 这个采样保持电路的平均功耗为0.203mw. 图4所示电路,浮栅MOS管部分电路,一直不存在直流功耗. 对于阈值提取部分电路,采样阶段存在直流功耗,保持阶段不存在直流功耗. 整个电路平均功耗为0.147mw. 各电路的结构复杂度和功耗情况具体如表1所示:表1各种基于浮栅MOS的采样保持电路结构和功耗对比Tab.1 The structure and power consumption compare among the different kinds of S/H5总结传统的采样保持电路是通过运算放大器和电容来实现的,放大器的放大倍数越高,得到的精度也越高. 但是,那需要制作高放大倍数的放大器,需要复杂的电路结构,并且,功耗会比较大. 例如一个同样采用0.35um CMOS工艺的采样保持电路[7],总共需要34个MOS 管,以及大量的输入输出端口和电容,在3.3V电源电压下,功耗是27mw. 然而,在某些应用场合,电路的复杂度和功耗的大小往往比精度要求更苛刻,例如在手机终端的匹配滤波器,或者是结构庞大的神经网络,等等,这些电路中,电路的结构和功耗的大小成了主要的考虑因素. 而本文提出的基于钟控神经元MOS管的新型采样保持电路,比之前提出的基于浮栅器件的采样保持电路具有更高的精度,并且可以有效地降低电源电压,功耗也只有0.147mw,整个电路只需要一个钟控神经元MOS管和2个普通MOS管,加上若干辅助开关,结构非常简单,这些特点使它更适合于高精度、低复杂度和低功耗的应用场合.参考文献:[1] SHIBA TA T; OHMI T. A functional MOS transistor featuring gate-level weighted sum and thresholdoperations[J], Electron Devices, 1992,39(6) :1444 - 1455.[2] BERG Y; AUNET S; MINNOTAHARI O; et al. Novel recharge semi-floating-gate CMOS logic formultiple-valued systems[C]// Proceedings of the 2003 International Symposium on Circuits and Systems.[S. l.]: [s. n.], 2003: V-193 - V-196 vol.5[3] JENSEN R; BERG Y; LOMSDALEN J G. Semi floating-gate S/H circuits[C]// NORCHIP Conference. [S. l.]:[s. n.], 2005: 176 – 179[4] 曹亚明,汤玉生. 钟控神经MOS晶体管的建模及其电路仿真[J] 固体电子学研究与进展,2003,23(1):89-95CAO Ya-ming, TANG Yu-sheng. Modeling of Clock-controlled NeuMOS and Simulation of Clock-controlled NeuMOS IC[J], Research & Progress of Solid State Electronics, 2003,23(1):89-95[5] 杨媛,高勇,余宁梅,等. 钟控神经元MOS晶体管的改进HSPICE宏模型[J] 固体电子学研究与进展,2007.8,27(3):301-304YANG Yuan, GAO Yong, YU Ning-mei, et al. Modified HSPICE Macro-model of Clock-controlled Neuron-MOS, Research & Progress of Solid State Electronics, 2007.8,27(3):301-304[6] 杨媛. 神经元MOS及其应用电路的研究[D],西安:西安理工大学,2004:80-81.Yang Yuan. Research of Neuron-MOS and Its Application Circuits[D], Xi’an: Xi'an University of Technology, 2004: 80-81.[7] 潘星,王永禄,裴金亮. 一种高性能采样/保持电路的设计[J] 微电子学, 2008.6, 38(3):442-444PAN Xing, WANG Yong-lu, PEI Jin-liang. Design of a High-Performance Sample-and-Hold Circuit.MICROELECTRONICS, 2008.6, 38(3):442-444。
第十届泰迪杯B题电力分析
第⼗届泰迪杯B题电⼒分析
本次代码有机器学习、LSTM神经⽹络、MK突变检验
突变时间确定代码,通过MK突变检验以及Pettitt检验确定突变时间,本次分享包括检验的资料以及完整代码,导⼊数据直接运⾏即可。
mk检验是曼-肯德尔法,⼜称Mann—Kenddall 检验法,是⼀种⽓候诊断与预测技术,应⽤Mann-Kendall检验法可以判断⽓候序列中是否存在⽓候突变,如果存在,可确定出突变发⽣的时间。
Mann-Kendall检验法也经常⽤于⽓候变化影响下的降⽔、⼲旱频次趋势检测。
本次赛题为长序列时间序列预测任务,该Baseline对数据进⾏了处理与特征提取,基于5折LightGBM全流程运⾏时间⼀般在2分钟内。
本次代码⾸先对数据进⾏可视化,其次对数据进⾏特征⼯程,最后通过机器学习catboost、xgboost、lightgbm进⾏预测,⽂中包括数据清洗、特征⼯程、模型预测以及后期优化策略。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
ISSN: 1524-4539Copyright © 2003 American Heart Association. All rights reserved. Print ISSN: 0009-7322. Online72514Circulation is published by the American Heart Association. 7272 Greenville Avenue, Dallas, TXDOI: 10.1161/01.CIR.0000074228.53741.722003;107;3159-3164; originally published online Jun 9, 2003;Circulation Tadashi Kuroda, Koji Tanaka, Tohru Masuyama, Masatsugu Hori and Kenshi FujiiKatsuomi Iwakura, Hiroshi Ito, Shigeo Kawano, Atsushi Okamura, Katsuaki Asano,Infarction Tissue Characterization in Patients With Anterior Wall Acute MyocardialDetection of TIMI-3 Flow Before Mechanical Reperfusion With Ultrasonic/cgi/content/full/107/25/3159located on the World Wide Web at:The online version of this article, along with updated information and services, is/reprints Reprints: Information about reprints can be found online atjournalpermissions@ 410-528-8550. E-mail:Fax:Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters/subscriptions/Subscriptions: Information about subscribing to Circulation is online atDetection of TIMI-3Flow Before Mechanical Reperfusion With Ultrasonic Tissue Characterization in Patients With Anterior Wall Acute Myocardial Infarction Katsuomi Iwakura,MD;Hiroshi Ito,MD;Shigeo Kawano,MD;Atsushi Okamura,MD;Katsuaki Asano,MD;Tadashi Kuroda,MD;Koji Tanaka,MD;Tohru Masuyama,MD;Masatsugu Hori,MD;Kenshi Fujii,MDBackground—Spontaneous coronary reperfusion with TIMI-3flow is associated with favorable clinical outcomes in patients with acute myocardial infarction(AMI).We investigated the ability of analyzing cardiac cycle-dependent variation of myocardial integrated backscatter(IBS)for predicting spontaneous reperfusion in anterior AMI. Methods and Results—We recorded IBS images on admission in104patients with first anterior wall AMI and subsequently performed coronary angiography and coronary intervention.We measured the cyclic variation of IBS within the infarct zone and expressed its magnitude as phase-corrected magnitude(PCM)by giving positive and negative values when it showed synchronous and asynchronous contraction,respectively.Twenty-three patients showing TIMI-3flow at the initial coronary angiography had smaller peak creatine kinase value than57patients with initial TIMI-0/1flow(864Ϯ961versus2358Ϯ1757IU/L;Pϭ0.0002)and better percent wall thickening within risk area(36.1Ϯ15.1%)than those with TIMI-2(16.7Ϯ12.8%,PϽ0.0001)or TIMI-0/1(5.1Ϯ11.6,PϽ0.0001).The patients withinitial TIMI-3had higher PCM(2.7Ϯ1.3dB)than those with TIMI-2(Ϫ0.3Ϯ2.2dB,PϽ0.0001)or those with TIMI-0/1 (Ϫ1.1Ϯ2.4dB,PϽ0.0001).Using PCMϭ1.0dB as the cutoff point,PCM detected TIMI-3flow with95.7%sensitivity and90.1%specificity.Multivariable logistic regression analysis revealed that only PCM is an independent predictor for spontaneous reperfusion among the hemodynamic,echocardiographic,and electrocardiographic variables. Conclusions—Analysis of myocardial IBS could detect spontaneous reperfusion noninvasively in the emergent stage of anterior AMI.(Circulation.2003;107:3159-3164.)Key Words:echocardiographyⅢmyocardial infarctionⅢreperfusionE arly achievement of Thrombolysis in Myocardial Infarc-tion trial(TIMI)grade3flow in infarct related artery plays a crucial role to obtain favorable outcomes after acute myocardial infarction(AMI).1,2The patients with spontane-ous TIMI-3flow show better functional and clinical out-comes after percutaneous coronary intervention(PCI)than those without it.3,4Thus,patency of infarct related artery at the early stage of AMI has an impact on the clinical course after reperfusion.The interaction between ultrasound and tissue has been studied to characterize the histological state of tissue as the ultrasonic tissue characterization.Measuring quantitated in-tegrated backscatter(IBS)from unprocessed radiofrequency signal,which is usually processed and displayed on the traditional echocardiographic images,is a unique approach to assess coronary perfusion and myocardial viability.Myocar-dial IBS shows cardiac cycle-dependent variation(CV),5,6 and it blunts during coronary occlusion and recovers much faster than wall motion after coronary reperfusion.7–9We previously reported that the synchronous CV after coronary reperfusion implies adequate tissue perfusion and viable myocardium in the patients with AMI.10,11In the present study,we investigated whether analyzing CV of IBS could detect spontaneous reperfusion in the patients with first, anterior wall AMI before angiography.MethodsStudy PopulationBetween January2000and July2001,122consecutive patients were admitted to our hospital within24hours of the symptom onset and diagnosed as having first anterior wall AMI.Diagnosis of AMI was made if the patient showed at least2of the following:prolonged chest pain(Ͼ30minutes),ST segment elevationՆ2mm in at least 2precordial electrocardiographic leads,andՆ3-fold increase in serum creatine kinase(CK)-MB level.Location of infarct area was confirmed with ECG or with echocardiography in each patient. Eighteen patients were excluded because of inadequate echocardio-Received December9,2002;revision received March25,2003;accepted March26,2003.From the Division of Cardiology,Sakurabashi Watanabe Hospital,and Department of Internal Medicine and Therapeutics,Graduate School of Medicine(T.M.,M.H.),Osaka University,Osaka,Japan.Correspondence to Hiroshi Ito,MD,Division of Cardiology,Sakurabashi Watanabe Hospital,2-4-32Umeda,Kita-ku,Osaka530-0001,Japan.E-mail itomd@osk4.3web.ne.jp©2003American Heart Association,Inc.Circulation is available at DOI:10.1161/01.CIR.0000074228.53741.72graphic image(13patients)or severe heart failure(5patients). Therefore,the final study population consisted of104patients.The study protocol was approved by the hospital ethics committee.Each patient gave written informed consent before cardiac catheterization. ProtocolAfter the admission,we recorded a12-lead ECG and monitored the multiplane echocardiograms with a commercially available echocar-diograph(SONOS5500,Philips Medical Systems).We determined the risk segments as myocardial segments showing dyskinesia, akinesia,or severe hypokinesia in this baseline study.Then we recorded2D IBS images of the short-axis view at the mid-papillary muscle level using acoustic densitometry package and stored con-secutive60frames(30frames/s)on the magnetic optical disc.10,11 All of these examinations were completed within15minutes after admission.Aspirin(243mg)was orally given at least30minutes before coronary angiography(CAG),and heparin(100U/kg)was intrave-nously administrated just before CAG.We recorded ECG again and measured hemodynamic data with Swan-Ganz catheter just before CAG.We performed CAG using the right femoral approach within 1hour after echo examination and recorded images at15frames/s. We performed PCI on culprit lesion using appropriate sized balloon.We repeated angioplasty or implanted stent to reduce the residual diameterϽ50%.We defined in-hospital complications as arrhythmia such as ventricular tachycardia,ventricular fibrillation and atrial fibrillation, congestive heart failure lastingՆ4days after reperfusion,reinfarc-tion,or cardiac death.We performed echocardiography at a mean of 4months later in all the patients except2who died in hospital and determined the wall motion recovery within the risk area. Analysis of Echocardiographic DataTwo independent observers blinded to patients’data evaluated wall motion in echocardiogram on admission and at the follow-up study. Percent systolic wall thickening(%SWT)within risk area and at remote normal segments was determined on short-axis image as difference in the wall thickness at end systole and at end diastole divided by end diastolic thickness.Analysis of IBS DataTwo experienced echocardiographers blinded to patients’data ana-lyzed IBS images according to a procedure described elsewhere.10,11 We used a special software package(Acoustic Densitometry)in-stalled on SONOS5500.This system is capable of providing2D images in which gray level is displayed proportional to ultrasonic backscatter amplitude as the IBS image.To analyze it,we placed the ovoid region of interest at the center of the segments at risk and in the remote normal region in each patient at each examination(Figure 1).We used the largest region of interest possible that did not include endocardial and epicardial reflectors.We manually adjusted the location of the site on a frame-by-frame basis to keep it within mid-wall throughout a cardiac cycle and constructed a curve of IBS versus time.We determined the magnitude(in decibels)of cyclic variation of IBS as the difference between the minimal and maximal values in a cardiac cycle averaged over at least2consecutive beats. Because the regional contraction in the infarct zone may not be necessarily synchronized exactly with global contraction,we cor-rected the magnitude of cyclic variation with respect to the phase of regional contraction.The interval from the upstroke of QRS complex to the nadir of the cyclic variation was divided by QT interval to determine the normalized delay to ventricular contraction(unitless) (Figure1).We previously determined a mean of the normalized delay in the normal segment as1.0Ϯ0.1.10Therefore,if normalized delay value in the normal segment wasϾ1.2(meanϮ2SD of normal),we considered it indicative of delayed contraction or passive stretching and multiplied the magnitude byϪ1.0(phase-corrected magnitude[PCM]).This is an approximation of the phase-weighted amplitude.7,8If the normalized delay value was Յ1.2,the phase-corrected magnitude is the same as the measured magnitude value.Analysis of Coronary AngiographyTwo experienced interventional cardiologists blinded to patients analyzed CAG and determined patency of culprit lesion before PCI with TIMI flow grade.If TIMI flow gradeՆ2was observed in left anterior descending coronary artery(LAD),TIMI frame count was determined as the frame count required for dye to first opacify a standard distal landmark.12Collateral channels were graded accord-ing to the report by Rentrop,13and good collateral was defined as grade2or3.Analysis of ElectrocardiographyAn experienced cardiologist blinded to patients’data analyzed ECG recorded on hospital admission and just before CAG.Resolution of more than70%of ST elevation in the precordial leads was consid-ered as the electrographic signs of spontaneous reperfusion. Reproducibility of DataWe determined intraobserver and interobserver variability of mea-suring the magnitude and normalized delay value of cyclic variation of IBS by measuring the2variables in a randomly selected10 records twice by the same observer and by2independent observers, respectively.Intraobserver and interobserver variabilities of the magnitude were 4.2Ϯ4.0%and 5.1Ϯ4.2%(absolute difference), respectively.Intraobserver and interobserver variabilities of normal-ized time delay were4.2Ϯ3.2%and4.7Ϯ2.4%(absolute difference), respectively.StatisticsAll data are expressed as meanϮSD.We made multiple comparisons by one-way ANOVA,and significance of difference was calculated with Scheffe’s F test.To analyze predictive value of variables,we constructed receiver operating characteristic curves and determined the suitable cutoff point where sensitivity is as nearly equal to specificity as possible.Multivariate logistic regression analysis was used to identify independent predictors for spontaneous recanaliza-tion.Differences were considered significant at PϽ0.05.Statistical analysis was performed with StatView5.0(SAS Institute).ResultsPatients’CharacteristicsAmong the104study patients(mean age,63Ϯ12years; range,40to91years),78patients were men.Theculprit Figure1.Analysis of IBS images.Left,The ovoid region of interest(Arrow)was placed at the center of the segments at risk to reconstruct a curve of IBS versus time.Right,The magnitude of cyclic variation of IBS was determined as the difference between the minimal and maximal values in a cardiac cycle(A). The interval from the upstroke of QRS complex to the nadir of the cyclic variation(B)was divided the value by QT interval(C) to determine the normalized delay.3160Circulation July1,2003lesion was at the proximal portion of LAD in58patients (55.8%)and at the middle portion in46patients.The mean time from the symptomatic onset to CAG was7.4Ϯ5.4hours, and peak creatine kinase level was2142Ϯ1581IU/L. Initial TIMI Flow GradeAmong the104study patients,23patients(22.1%)showed TIMI-3flow at the initial CAG.TIMI-2was observed in18 patients(17.3%),TIMI-1in6patients(5.8%),and TIMI-0in 57patients(54.8%).TIMI frame count in TIMI-3flow was significantly smaller than that in TIMI-2flow(16Ϯ4versus 37Ϯ10frames,respectively;PϽ0.0001).The initial TIMI-3 and TIMI-2groups had significantly lower pulmonary capil-lary wedge pressure(PCWP)than the TIMI-0/1group,but no differences were observed between these2subsets(Table1). We performed PCI in all patients except for1patient with initial TIMI-2flow and6with initial TIMI-3and obtained successful coronary recanalization in all but2patients.After PCI,TIMI-3flow was observed in47of63patients(74.6%) with initial TIMI-0/1,in15of18patients(83.3%)with initial TIMI-2,and in all patients(100%)with initial TIMI-3flow (Pϭ0.03among the3subsets)(Table1).Patients with initial TIMI-3or TIMI-2flow had signifi-cantly lower peak CK and CK-MB values than those with TIMI-0/1(Table1),whereas there were no significant differ-ences between the TIMI-3and the TIMI-2groups.The patients with initial TIMI-3flow also had higher%SWT within risk area than the others.At the follow-up study,the initial TIMI-3group showed significantly higher%SWT within risk area(36.1Ϯ15.1%)than the initial TIMI-2 (16.7Ϯ12.8%,PϽ0.0001)or TIMI-0/1groups(5.1Ϯ11.6, PϽ0.0001).The incidence of in-hospital complications was lower in patients with initial TIMI-3(4.3%)than those with initial TIMI-2(27.8%)and with initial TIMI-0/1(36.5%), although the difference did not reach the statistical signifi-cance.Two patients who died during hospital stay showed initial TIMI-0flow.Prediction of Spontaneous Coronary Reperfusion Figure2shows waveforms of CV on admission.CV within the infarct zone shows synchronous contraction in the patient with initial TIMI-3flow(left).In the patients with initial TIMI-0,CV showed its nadir in diastole,implying asynchro-nous contraction(right).Twenty-three patients with initialTABLE1.Clinical Characteristics of the Study PatientsTIMI Flow Grade at Initial CAGAll Patients TIMI-0/1TIMI-2TIMI-3PNo.of patients104631823Age,y63Ϯ1263Ϯ1264Ϯ1465Ϯ130.72Gender,male/female78/2645/1813/520/30.32Risk factorsDiabetes mellitus,%48.746.061.143.50.60Hypertension,%59.661.955.656.50.82Hyperlipidemia,%26.931.727.813.00.46Smoking,%53.850.861.153.80.81Hemodynamic dataSystolic blood pressure,mm Hg130Ϯ23132Ϯ23127Ϯ23128Ϯ240.54Heart rate,bpm84Ϯ1586Ϯ1580Ϯ160.47PCWP,mm Hg12Ϯ614Ϯ610Ϯ7*8Ϯ5‡0.002Cardiac index,L/min per m2 3.6Ϯ0.8 3.6Ϯ0.9 3.5Ϯ0.2 3.6Ϯ1.00.90Symptom to CAG time,h7.7Ϯ6.07.9Ϯ6.6 4.8Ϯ2.39.4Ϯ5.70.20Proximal culprit,%55.858.750.052.20.75Stent implantation,%45.246.044.443.50.98TIMI-3flow after PCI,%81.774.683.31000.03Peak CK,IU/L1855Ϯ16262358Ϯ17571361Ϯ1016†864Ϯ961‡0.0002Peak CK-MB,IU/L166Ϯ128206Ϯ13097Ϯ67‡86Ϯ97‡ʈ0.0001In-hospital complications,%17.336.527.8 4.30.12Echocardiographic study%SWT:risk area 2.2Ϯ6.40.6Ϯ4.70.04Ϯ1.18.1Ϯ9.0*‡§ʈϽ0.0001%SWT:normal area46.0Ϯ21.246.7Ϯ23.141.2Ϯ12.547.5Ϯ21.30.57PCM:risk area,dBϪ0.1Ϯ2.6Ϫ1.1Ϯ2.4Ϫ0.4Ϯ2.2 2.7Ϯ1.3‡ʈϽ0.001PCM:normal area,dB 5.7Ϯ2.2 5.7Ϯ2.4 5.6Ϯ1.6 5.6Ϯ1.90.91%SWT at follow-up study12.7Ϯ17.0 5.1Ϯ11.616.7Ϯ12.8*‡36.1Ϯ15.1‡ʈϽ0.0001P values for the differences among the TIMI-0/1,Ϫ2andϪ3groups.*PϽ0.05,†PϽ0.02,and‡PϽ0.01vsTIMI-0/1;§PϽ0.05,ʈPϽ0.01vs TIMI-2.Iwakura et al Ultrasonic Assessment of Spontaneous Reperfusion in AMI3161TIMI-3flow showed significantly higher PCM (2.7Ϯ1.3dB)than those with initial TIMI-2(Ϫ0.3Ϯ2.2dB,P Ͻ0.0001)and those with initial TIMI-0/1(Ϫ1.1Ϯ2.4dB,P Ͻ0.0001)(Table 1).There were no significant differences in PCM between the initial TIMI-2and the TIMI-0/1groups.Among the 81patients with initial TIMI-0/1/2,there was no significant difference in PCM between the 26(32.1%)patients with good collaterals and those without it (Ϫ0.5Ϯ3.0versus Ϫ1.1Ϯ1.9dB,P ϭ0.29).No collateral channel was observed in CAG in the patients with initial TIMI-3.PCM within risk area as well as that within remote normal segments showed weak but significant correla-tions with %SWT of the corresponding area (R ϭ0.40,P Ͻ0.0001,and R ϭ0.21,P ϭ0.04,respectively)(Figure 3).However,PCM values ranged from Ϫ4.2to 3.8dB (mean,Ϫ0.3Ϯ1.8db)even in the 42segments with %SWT ϭ0.In the patients with initial TIMI Ն2flow,TIMI frame count in LAD also showed a significant correlation with PCM within risk area (R ϭ0.65,P Ͻ0.0001;Figure 4).Moreover,PCM was also correlated with TIMI frame count in the 19patients with both TIMI Ն2flow and %SWT ϭ0(R ϭ0.59,P ϭ0.02).These results suggested that PCM somehow reflected coronary flow independently from residual wall motion.PCM within risk area also showed a significant but weak correlation with PCWP before CAG (R ϭ0.29,P ϭ0.004).Although a better correlation was observed in the initial TIMI-3group (R ϭ0.46,P ϭ0.04),no correlation was ob-served in patients with TIMI-2(R ϭ0.004,P ϭ0.98)or in those with TIMI-0/1(R ϭ0.14,P ϭ0.30).No correlations were observed between PCM and other hemodynamic fac-tors.Also there was no correlation between PCM and the elapsed time from symptom onset to CAG.The receiver-operating characteristic analysis indicated that PCM ϭ1.0dB was the suitable cutoff point to detect initial TIMI-3flow (Figure 5).Among 30patients with PCM Ͼ1.0dB,22patients (73.3%)showed TIMI-3flow,whereas only 1(1.4%)of 74patients with PCM Ͻ1.0dB showed TIMI-3flow.Thus,PCM Ͼ1.0dB before CAG predicted TIMI-3flow with 95.7%sensitivity and 90.1%specificity.Patients with PCM Ͼ1.0db showed lower peak CK value (1250Ϯ1377versus 2537Ϯ1657IU/L,P ϭ0.0017)andbetterFigure 2.The cyclic variation of inte-grated backscatter in the area at risk (anterior septum)and in the normal zone (posterior wall)on hospital admission in the patients with anterior AMI.In the patients showing spontaneous TIMI-3reperfusion,integrated backscatter from the anterior septum showed cyclic varia-tion synchronized with that in the poste-rior wall (left).On the other hand,the integrated backscatter within risk area showed asynchronous cyclic variation with its nadir in diastole (right)in the patient with total occlusion (TIMI flow grade 0)inLAD.Figure 3.Relation between %SWT and PCM.The relations between %SWT (hor-izontal bar)and PCM (vertical bar)within area at risk (left)and within the remote normal segments (right)were demon-strated.PCM showed weak but signifi-cant correlations with %SWT in both areas.3162Circulation July 1,2003%SWT on follow-up study (29.6Ϯ17.1versus 6.7Ϯ12.3,P Ͻ0.001)than those with PCM Յ1.0db.ST resolution was observed on ECG in 7of 23patients with the initial TIMI-3(30.4%)and in 10of 81patients with initial TIMI-0/1/2(12.3%,P ϭ0.04),indicating ECG assessed spontaneous TIMI-3reperfusion with only 30.4%sensitivity and 87.7%specificity.We performed multivariate logistic regression analysis to determine the independent predictive factors for spontaneous TIMI-3reperfusion using PCM,peak CK-MB,PCWP,%SWT within risk area,and ST resolution as variables.Among these variables,PCM was the only independent predictor for spontaneous coronary reperfusion (Table 2).DiscussionWe investigated the effects of spontaneous coronary reperfu-sion on functional and clinical outcomes after AMI and the potential of myocardial IBS for predicting spontaneous reper-fusion in the 104patients with first,anterior wall AMI.Patients showing spontaneous reperfusion with TIMI-3flow had lower peak CK value and better functional recovery thanthose with initial TIMI Յ2.The patients with initial TIMI-3had higher PCM in the infarct zone than those showing TIMI-0/1/ing 1.0dB as the cutoff point,PCM detected TIMI-3spontaneous reperfusion with 95.7%sensi-tivity and 90.1%specificity.Multivariate logistic regression analysis indicated that PCM is only an independent predictor of spontaneous recanalization among echocardiographic and ECG variables.Cyclic Variation of IBS at the Early Stage of AMIRecently,Hancock et al 14reported that CV of IBS measured 90minutes after thrombolysis detects successful coronary reperfusion in the patients with AMI.The present study demonstrated that spontaneous reperfusion with TIMI-3flow also could elicit similar quick recovery of CV,whereas TIMI-2flow was not enough for the recovery of CV.The mechanism of CV of IBS has not been fully understood yet.Prior studies indicated that CV of IBS recovers after ischemia before wall motion recovery.7–10In the present study,PCM showed weak but significant correlation with %SWT (Figure 3).However,CV was observed even in some of the 42segments showing no visible wall motion.These results implied that PCM somehow reflects wall motion itself,but it is not the only mechanism of recovery of CV.The lower PCWP in the initial TIMI-3group and a weak but significant correlation between PCWP and PCM suggested that PCWP also might affect CV,although its effect might be very limited.The significant correlation between PCM and TIMI frame count in LAD in the patients with initial TIMI Ն2flow implied that PCM also could somehow reflect coronary perfusion,though CV could be observed even in some patients with total coronary occlusion.The other possible explanation of presence of CV is that it could reflect intrinsic contraction of sarcomere that might not be enough for visible wall thickening.The recent study reported that magnitude of CV without phase correction could detect successful reperfusion after thrombolysis.14However,some segments within risk area showed asynchronous contraction or passive stretch,indi-cated as negative value in %SWT,and these segments showed highly delay in CV indicated as negative PCM (Figure 3).Previous studies indicated that not only the magnitude of CV but also changes in cyclic phase are important for analysis of ultrasonic tissue characterization.9,15In the original phase-weighted amplitude,negative value is given to magnitude of CV if delay of phase of cyclic variation ()is within 90to 0degrees,whereas it was multipliedwithFigure 4.Relation between TIMI frame count and PCM from area at risk in the patients with initial TIMI-2or -3flow.TIMI frame count in LAD was signi ficantly related with PCM obtained from area at risk in the 41patients with TIMI-2or -3flow in LAD on the initialCAG.Figure 5.Receiver-operating characteristic curve for determin-ing the optimal cutoff value of the PCM on hospital admission for predicting spontaneous TIMI-3reperfusion.Each actual number denotes the cutoff value for PCM.TABLE 2.Multivariable Predictors of Spontaneous Recanalization2P Odds Ratio (95%CI)PCM within risk area 6.840.009 1.77(1.15to 2.72)%SWT:risk area 3.710.054 1.16(0.99to 1.35)PCWP 0.180.670.97(0.82to 1.14)ST resolution 0.080.780.76(0.11to 5.28)Peak CK-MB1.200.270.99(0.98to 1.004)Iwakura et al Ultrasonic Assessment of Spontaneous Reperfusion in AMI3163Ϫcos(2)if0degreesՅՅ90degrees.Although this method would reflect the phase delay more accurately than PCM,it is too tedious for the clinical use.PCM is an easier way to assess both magnitude and phase delay of CV at the same time,and our previous studies demonstrated that it could be a good index for coronary reperfusion and myocar-dial viability.10,11Prediction of Spontaneous Reperfusion With PCM The early detection of spontaneous TIMI-3reperfusion could be important for clinical decision making after AMI.Al-though ST resolution in ECG has been used for the assess-ment of successful coronary reperfusion,it could detect spontaneous reperfusion with only modest accuracy in the present study.It might be because ST resolution takes some time to become apparent,as observed in the case of thrombolysis.16Spontaneous reperfusion was associated with significantly better%SWT in the present study.However, multivariate logistic regression analysis revealed that PCM could be an independent predictor for spontaneous reperfu-sion but not%SWT.As discussed above,PCM reflects not only visible myocardial contraction but also other factors related with coronary reperfusion,which might lead to more sensitive detection of spontaneous reperfusion than%SWT. Study LimitationsWe enrolled the patients who underwent PCI within24hours in the present study,and the relatively longer symptom to CAG time(7.7Ϯ6.0hours)might affect the present results. CV of IBS is dependent on the angle between fiber orienta-tion and ultrasonic beam,called anisotropy.17We measured CV only in anterior and posterior(control)wall in the short-axis view,in which myocardial fiber is oriented nearly perpendicular to the ultrasound beam,to avoid problems with anisotropy as possible.It is unclear whether the results in the present study could be applied to inferior or lateral wall infarction because of anisotropy.Measurement of CV on apical views might be also useful for detecting coronary reperfusion to reduce anisotropy.17The quality of echocar-diographic images also could affect analysis of IBS,and approximately10%of the study patients were excluded because of inadequate echocardiographic images.This method might also not be inapplicable for the patients having prior myocardial infarction,bundle branch block,paced rhythm,or cardiomyopathy.Moreover,additional prospective studies would be required to validate the cutoff value of1.0 dB to predict spontaneous recanalization in another patient population.References1.Cannon CP,Gibson CM,Lambrew CT,et al.Relationship of symptom-onset-to-balloon time and door-to-balloon time with mortality in patients undergoing angioplasty for acute myocardial infarction.JAMA.2000;283: 2941–2947.2.Berger PB,Ellis SG,Holmes DR,et al.Relationship between delay inperforming direct coronary angioplasty and early clinical outcome in patients with acute myocardial infarction:results from the global use of strategies to open occluded arteries in Acute Coronary Syndromes (GUSTO-IIb)trial.Circulation.1999;100:14–20.3.Lee CW,Hong MK,Lee JH,et al.Determinants and prognostic signif-icance of spontaneous coronary recanalization in acute myocardial infarction.Am J Cardiol.2001;87:951–954.4.Stone GW,Cox D,Garcia E,et al.Normal flow(TIMI-3)beforemechanical reperfusion therapy is an independent determinant of survival in acute myocardial infarction:analysis from the primary angioplasty in myocardial infarction trials.Circulation.2001;104:636–641.5.Wickline SA,Thomas LJ III,Miller JG,et al.A relationship betweenultrasonic integrated backscatter and myocardial contractile function.J Clin Invest.1985;76:2151–2159.6.Wickline SA,Thomas LJ III,Miller JG,et al.The dependence of myo-cardial ultrasonic integrated backscatter on contractile performance.Cir-culation.1985;72:183–192.7.Wickline SA,Thomas LJ III,Miller JG,et al.Sensitive detection of theeffects of reperfusion on myocardium by ultrasonic tissue character-ization with integrated backscatter.Circulation.1986;74:389–400.8.Vitale DF,Bonow RO,Gerundo G,et al.Alterations in ultrasonic back-scatter during exercise-induced myocardial ischemia in humans.Circu-lation.1995;92:1452–1457.9.Colonna P,Montisci R,Galiuto L,et al.Effects of acute myocardialischemia on intramyocardial contraction heterogeneity:a study performed with ultrasound integrated backscatter during transesophageal atrial pacing.Circulation.1999;100:1770–1776.10.Takiuchi S,Ito H,Iwakura K,et al.Ultrasonic tissue characterizationpredicts myocardial viability in early stage of reperfused acute myo-cardial infarction.Circulation.1998;97:356–362.11.Iwakura K,Ito H,Nishikawa N,et e of echocardiography forpredicting myocardial viability in patients with reperfused anterior wall myocardial infarction.Am J Cardiol.2000;85:744–748.12.Gibson CM,Cannon CP,Daley WL,et al.TIMI frame count:a quanti-tative method of assessing coronary artery flow.Circulation.1996;93: 879–888.13.Rentrop KP,Cohen M,Blanke H,et al.Changes in collateral channelfilling immediately after controlled coronary artery occlusion by an angioplasty balloon in human subjects.J Am Coll Cardiol.1985;5: 587–592.14.Hancock JE,Cooke JC,Chin DT,et al.Determination of successfulreperfusion after thrombolysis for acute myocardial infarction:a nonin-vasive method using ultrasonic tissue characterization that can be applied clinically.Circulation.2002;105:157–161.15.Wagner RF,Wear KA,Perez JE,et al.Quantitative assessment of myo-cardial ultrasound tissue characterization through receiver operating char-acteristic analysis of Bayesian classifier.J Am Coll Cardiol.1995;25: 1706–1711.16.De Lemos JA,Antman EM,Giugliano RP,et al.Very early risk strati-fication after thrombolytic therapy with a bedside myoglobin assay and the12-lead electrocardiogram.Am Heart J.2000;140:373–378.17.Bouki KP,Lange A,Palka P,et al.Regional variation of ultrasonicintegrated backscatter in normal and myopathic left ventricles:a new multi-view approach.Eur Heart J.1996;17:1747–1755.3164Circulation July1,2003。