黄色肉芽肿性肾盂肾炎的超声特征
黄色肉芽肿性肾盂肾炎1例并文献复习

【关键词】 黄色肉芽肿性肾盂肾炎;诊断;治疗【中图分类号】 R692.3 【文献标识码】 B 患者,女,25岁,因“左腰部疼痛1个月,加重1周”入院。
患者1个月前无明显原因出现左侧腰部疼痛,1周前左腰部疼痛加重,反复发热,伴呕吐5~6次/d,偶有寒战、盗汗,无胸闷、气促,尿色稍红,无膀胱刺激征。
就诊外院诊断为左肾结核,行抗结核治疗,疗效不佳,遂转至我院。
体格检查:T39℃,P108次/min,R20次/min,BP106/72mmHg。
双侧肋脊角无压痛,左肾区叩击痛,右肾区无叩击痛,余无异常。
血常规:WBC15.1×109/L,N81.2%,Hb100g/L;PCT0.55ng/ml,hs CRP86.17mg/L,ESR120mm/h;尿常规:RBC118×106/L,WBC2403×106/L;肝功能:ALT105.86U/L,AST144.69U/L;肾功能:BUN35.5mmol/L,SCr100.5μmol/L;PPD(-)。
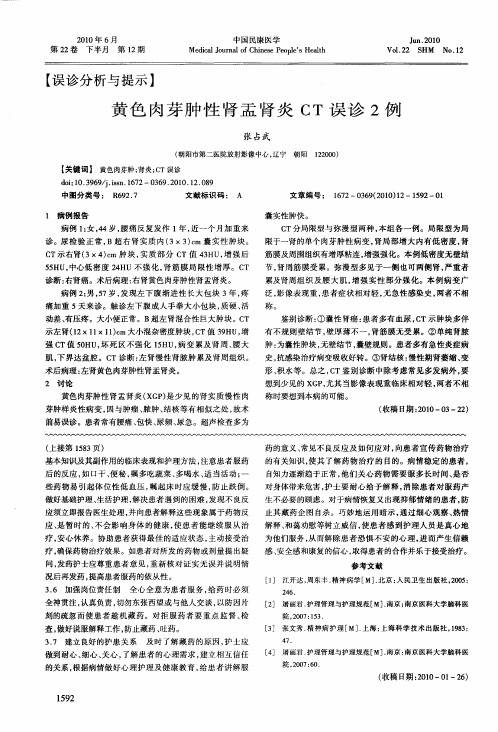
腹部CT示:左侧输尿管肾盂移行处、左肾肾区窦区可见多发结节状高密度影,较大者位于肾盂输尿管移行处,大小约1.6cm×2.5cm×3.0cm,左肾积水、体积明显增大,周围可见条絮状渗出影;左肾见不均匀强化,强化程度明显减低,肾实质内可见多处不强化呈“脓腔”样改变,腹膜后多发淋巴结增大(图1)。
入院完善相关检查,在全麻下行根治性左肾切除术。
术中见左肾明显增大,肾脏表面呈结节状,见左输尿管明显增厚,且输尿管与周围组织紧密粘连。
术后病理示:肾实质结构破坏,被炎性肉芽肿组织替代,其内可见含有大量脂质的巨噬细胞、中性粒细胞、淋巴细胞、浆细胞和成纤维细胞等,肾盂黏膜周围可见大量中性粒细胞和坏死碎屑,偶可见异物巨细胞,诊断为黄色肉芽肿性肾盂肾炎(图2)。
术后予哌拉西林他唑巴坦和替硝唑抗感染治疗,康复出院。
术后1周、6个月复查腹部增强CT及泌尿系超声未见异常,患者恢复可,未诉不适。
黄色肉芽肿性膀胱炎的超像图表现

中华超声影像学杂 志 2 0 年 5月第 】 卷第 5 02 l 期 C i J  ̄ ng . y20 . h Ut o orMa 2 n L r 0
1. o5 1 N
3 9 ・ 1
认真分析 。其鉴别 点为 : ①子宫 角 部妊 娠 的孕 囊与 宫腔相 通 ; 间质部妊娠孕囊 与宫腔不 相通 。② 前者囊胚 光环 周 围有 完整 的肌层壁包 绕 : 后者孕 囊光环接近浆膜 层 , 薄层肌 肉围绕 , 有 但 其外上方肌 层不完全或缺 失 。③前 者仔 细检察有 时可测 及子 宫原韧带 . 肛囊位于子宫 原韧带 的 内侧 方 为子宫角 部妊娠 而 后者的胚囊位于原韧带 的外 上方 ④结 台病史 . 子宫角妊娠 因 胚胎种植处 蜕膜发 育不 良. 易发 生流 产 , 临床 出现 或多 或步 的 阴道流血 : 闻质部妊娠 的胚胎 向官腔外 ( 输卵管 方向 ) 生长 . 多
行 超 声 检 查 , 给 临床 的诊 断和 处 理 提 供 可 靠 依 据 。 可
( 收稿 B期 :0 20 —0 2 0 .21 )
・
病 例 报 告 ・
飞 李鸿 曹繁 茂 鄣 玲
彩色血流信号 ( 2 。频谱 多普勒呈高阻 型动脉频谱。超声诊 图 ) 断: 膀胱实性 占位病变 ( 炎性 病变可能性大) 。排泄性屎 路造 影 : 双 肾排泄功能正常 ; 膀胱右侧壁有不规则充盈缺损 . 措右侧壁 向 内突 , 左侧 壁光滑 。提 示 : 胱右侧 壁 占位 性病 变 . 质待 查 。 膀 性 手术所 见 : 膀胱右侧壁 及顶部 见一广基 葡萄 样隆 起物 . 8叽 约 ×8Ⅱ n大小 . nx3Ⅱ 表面水 肿 . 暗红色 , 呈 切除肿物 , 面深 层 剖 呈灰黄色 。病理诊断 : 黄色肉芽肿性 膀胱炎 = 讨论
急慢性肾盂肾炎的影像诊断与鉴别诊断

女性,64Y,右侧腰背部疼痛2周。
鉴别诊断肾结核
• 主要继发于肺结核,其中25%的病人有明确肺结核病史。 • 20-40岁青壮年,男性多于女性。 • 约90%为单侧。 • 临床表现:全身症状:发热、盗汗、消瘦等典型结核症状、尿频、尿
急、尿痛、终末血尿、脓尿。 • 实验室检查:尿常规:脓尿、血尿、蛋白尿(晨尿);尿涂片:抗酸
病理
• 肾脏体积增大,表面散在脓肿。 • 肾盂黏膜充血水肿,散在小出血点。 • 显微镜下:间质水肿、炎性细胞浸润、多发微小脓肿形成。 • 感染区之间存在正常的肾组织,正常组织与病变相间为特征性
表现。
影像表现
• 平片:多数正常,少数弥漫性 肾肿胀。
• 排泄性尿路造影:肾脏体积增
大,肾脏及肾盏显影延迟(排
率高于Ⅱ型);Ⅱ型:气体影,液体集聚。
双侧气肿性肾盂肾炎。
I型
II型
小结
• 急性肾盂肾炎:女性,症状明显,肾体积增大,实质内水肿/ 出血/脓肿,楔形低强化区,肾盂肾盏壁增厚并不均匀强化。
• 慢性肾盂肾炎:女性,病程长,肾体积缩小,皮质变薄,表面 多发切迹,肾盂肾盏扩张积水。
• 黄色肉芽肿性肾盂肾炎:女性,肾体积增大,实质内多发低密 度灶,肾盂结石,肾周蔓延。
养:阳性。
病理表现
• 肉眼见肾脏体积缩小或肾萎缩,表面可见深浅不一瘢痕凹陷。 • 镜下皮髓质见间质慢性炎症、纤维化及部分肾小管萎缩。 • 肾内血管可发生硬化,造成肾缺血及肾功能减退。
影像表现CT
• 单侧或双侧肾脏体积缩小,或呈局部变小。 • 病变仅累及一侧肾脏时,对侧肾可代偿性增大。 • 肾皮质变薄,表面多个切迹,呈分叶状、局限性凹陷。 • 肾窦脂肪组织增多,肾脂肪囊相对较大。 • 肾盂肾盏变形,扩张或积水。 • 增强扫描示肾功能减弱。 • 尿路造影。 • 肾小盏变形呈杵状(瘢痕收缩-肾乳头收缩,肾盏失去正常锐
黄色肉芽肿性肾盂肾炎2例误诊分析

查亦难以确诊 。C T检 查对 X P的诊 断 帮助 很 大。弥漫 型 G
C T表 现 为 。 不 规则 增 大 , 实 质 被 多 个 囊 状 占位 取 代 , 肾脏 肾 增 强后囊状肿块呈不 均匀或 环形 强化 , 功能 明显损 害 , 内 肾 肾
见结石影 ; 局灶型 C T表 现为 肾实质 内见单发 或局 限 的囊 状 肿 块 , 强 后 病 变 壁 见 环 形 强 化 , 应 处 肾 盂 、 盏 受 压 移 增 相 肾
8版 . 京 : 民 卫 生 出 版社 ,9 87 8 . 北 人 19 :7— 9
[ ] 龙 风 宜 , 红 . 殖 器 官 发 育 异 常 与 闭 经 [ ] 中 国 实 用 妇 科 7 徐 生 J. 与 产 科 杂 志 ,0 8,4 1 )90—92 20 2 ( 2 :0 0.
『ቤተ መጻሕፍቲ ባይዱ] 孔秋英 , 8 谢红宁. 妇产科影像诊断与介入治疗 学[ . M] 北京 : 人
『 ] R e A,hmpo D T id 2 okJ T 0 snJ . eLn e妇 科 手 术 学 [ . 来 春 , M] 杨 段
华 妇 产 科 杂 志 ,0 2 3 ( :1 2 0 ,7 4)2 7—29 1.
涛, 朱关珍译. 济南 : 山东科学技术 出版社 ,0 3:4 20 6 3—6 8 7. 『 ] D h m yA 现代妇产科疾病诊 断及治疗 [ . 3 cC e e H. M] 刘新 民译.
『] 谢志红 , 安生 , 5 黄 肖红 , . rdr 型 女 性 假 两性 畸 形 矫 治 术 等 Pa eV 1 分析 [] 8例 J .中 国 实 用 妇 科 与 产 科 杂 志 , 05, 1( : 20 2 8)
肾囊性病变CT诊断

21
肾结核 (renal tuberculosis)
肾结核早期在乳头部或髓质锥体的深部形成结核结节 或肉芽肿,中心发生干酪坏死,随着病变扩展与肾盏相通, 坏死物质经肾盏排出,形成空洞,病变进一步扩展可自一 个肾盏至一组肾盏,成为肾盂结核。
根据病情的发展不一样,形态学可分为:结节型,囊 肿型,积水型,积脓型,萎缩型,钙化型,混合型。
增强扫描可表现为边缘环形强化并内部分隔 明显强化。静止期或寄生虫死亡时可出现钙化。 治疗及预后:
手术治疗是最有效的治疗方法。
精选ppt课件
29
(a) 平扫右肾复杂性囊性肿块 (b) 增强CT扫描病变环形强化伴分隔明显强化
精选ppt课件
30
精选ppt课件
31
肾小球囊肿病 (glomerulocystic kidney disease, GCKD)
精选ppt课件
19
精选ppt课件
20
肾脓肿 ( renal abscesses )
肾实质感染所致广泛的化脓性病变,或输尿管梗阻后 肾盂肾盏积水、感染而形成的一个集聚脓液的囊腔。
早期肾实质内略低密度影,轻度不 规则强化。
成熟期为类圆形均匀低密度影,增 强呈低密度影周围伴环形强化。
成熟期脓肿
精选ppt课件
男性单侧发病较多;女性则以双侧发病较多,且往往 左肾受累更明显。
精选ppt课件
38
患肾呈不规则分 叶的多发囊肿或 呈葡萄状,几乎 看不到肾实质。
精选ppt课件
39
肾脏多发葡萄串样囊变,囊肿间有互不相通的分隔, 分隔或少量实体部分可强化。
精选ppt课件
40
获得性肾囊性疾病 (acquired cystic kidney disease,ACKD)
泌尿系统影像诊断学

一、单选题(每题只有一个正确答案,共65道题)1、KUB系指泌尿系统影像学检查中的√A、X线平片B、排泄性尿路造影C、静脉性肾盂造影D、逆行性肾盂造影E、尿路造影2、正常成人肾脏上下径相当于同一个体A、2个腰椎椎体与其间椎间隙高度之和B、2个腰椎椎体与2个椎间隙高度之和√C、3个腰椎椎体与2个椎间隙高度之和D、3个腰椎椎体与3个椎间隙高度之和E、4个腰椎椎体与3个椎间隙高度之和3、前后位X线平片上,正常肾脊角为A、0°~10°B、5°~15°C、10°~20°√D、15°~25°E、20°~30°4、肾小盏分为A、漏斗部和颈部B、尖部、峡部和基底部√C、漏斗部和穹隆部D、穹隆部、颈部和基底部E、尖部、峡部和基底部5、正常腹段输尿管走行在A、腰方肌前缘√B、腰大肌前缘C、腰椎横突前缘D、腰小肌前缘E、腰椎椎体前缘6、排泄性尿路造影时,正常输尿管直径为A、1~5mmB、2~6mm√C、3~7mmD、4~8mmE、5~9mm7、关于尿路造影,以下哪一种描述是错误的√A、排泄性尿路造影常发生肾盂肾回流B、排泄性尿路造影可显示肾实质C、逆行肾盂造影易产生输尿管痉挛D、逆行肾盂造影不能显示肾实质E、逆行肾盂造影可发生肾盂肾回流8、关于正常肾脏CT平扫表现,以下描述错误的是A、肾实质呈软组织密度√B、肾窦脂肪密度高于肾盂密度C、不能分辨肾皮质与髓质D、肾实质密度高于肾窦脂肪密度E、肾实质密度高于肾盂密度9、关于正常肾脏增强对比三期表现,以下描述正确的是A、皮质期,肾实质均匀强化√B、皮质期,肾皮质明显强化,髓质呈较低密度C、实质期,肾髓质强化仍低于皮质D、实质期,能清楚分辨肾皮质与髓质E、排泄期,肾盏肾盂明显强化,肾实质强化仍呈上升趋势10、关于正常肾脏MRI平扫检查表现,以下描述正确的是√A、T1WI上,肾皮质信号强度高于髓质B、T2WI上,肾皮质信号强度低于髓质C、T1WI上,肾皮质与髓质信号强度相同D、预饱和脂肪抑制T1WI上,肾皮质信号强度低于髓质E、T2WI上,肾皮质信号强度高于髓质11、泌尿系统X线平片上,不发生钙化灶的病变是A、肾结核B、肾细胞癌C、肾囊肿√D、肾血管平滑肌脂肪瘤E、肾动脉瘤12、尿路造影检查时,不出现肾盏肾盂破坏的病变是A、肾结核B、肾细胞癌C、肾盂癌√D、肾囊肿E、黄色肉芽肿性肾盂肾炎13、尿路造影检查时,不造成肾盂、输尿管和膀胱腔内充盈缺损的是A、肿瘤B、结石√C、细胞管型D、血块E、气泡14、肾动脉造影检查,肾动脉偏心性狭窄的病因为√A、动脉粥样硬化B、大动脉炎C、动脉发育不良D、纤维肌肉发育不良E、结节性多动脉炎15、肾脏乎扫CT检查时,关于肾脏肿块密度的描述,不准确的是A、圆形水样密度肿块,边缘光滑,见于肾单纯性囊肿√B、混杂密度肿块仅见于肾恶性肿瘤C、含脂肪密度的混杂密度肿块为肾血管平滑肌脂肪D、高密度肿块可为出血性囊肿和部分肾细胞癌E、肿块内钙化在良、恶性病变均可发生16、肾脏MRI检查时,关于肾脏肿块信号强度,描述正确的是A、T1WI和T2WI上均呈高信号的,为肾单纯性囊肿B、T1WI上呈高信号,T2WI呈低信号的,为肾单纯性囊肿C、T1WI和T2WI上均呈低信号的,为肾单纯性囊肿D、T1WI和T2WI上呈混杂信号的,且其中高信号部分不被预饱和抑脂技术所抑制,为肾血管平滑肌脂肪瘤的特征性表现√E、T1WI和T2WI上呈混杂信号,且其中高信号部分可被预饱和抑脂技术所抑制,为肾血管平滑肌脂肪瘤的特征性表现17、孤立肾影像学检查的最佳成像技术是A、泌尿系统X线平片B、排泄性尿路造影√C、常规CT平扫和增强检查D、CTUE、MRU18、关于异位肾,以下描述正确的是A、异位肾均高于正常位置的肾脏B、异位肾均低于正常位置的肾脏√C、异位肾可低于或高于正常位置的肾脏D、异位肾均位于腹膜腔内E、CT或MRI检查,异位肾的密度或信号强度均不同于正常位置的肾脏19、马蹄肾呈U字形,其开口通常指向√A、上方B、下方C、前方D、后方E、左或右20、驼峰肾属于肾脏形态正常变异,其易发生在A、右肾上极B、右肾下极√C、左肾上极D、左肾下极E、无易发部位21、以下关于侏儒肾的描述中,正确的是√A、侏儒肾即肾发育不全B、侏儒肾为慢性肾盂肾炎所致C、侏儒肾是由肾血管病变所致D、侏儒肾仅肾实质体积变小,而肾盏肾盂大小正常E、CT或MRI检查,侏儒肾的密度或信号强度不同于正常肾脏22、泌尿系统影像学检查时,蛇头征系指A、输尿管结石B、输尿管肿瘤C、输尿管血块√D、输尿管囊肿E、输尿管气泡23、在泌尿系统X线平片上,以下关于肾结石描述正确的是A、90%肾结石为双侧性B、绝大多数肾结石为阴性结石C、类圆形和三角形高密度钙化影为肾结石典型表现√D、分层和鹿角状高密度钙化影为肾结石典型表现E、侧位片上,肾结石位于脊柱前方24、以下关于输尿管结石的描述,正确的是A、典型临床症状为无痛性肉眼血尿B、KUB上,典型结石表现为三角形致密影√C、结石的长轴与输尿管走行一致,为其特征D、结石均可引起上方尿路明显扩张积水E、X线尿路造影检查对输尿管结石无诊断价值25、以下关于膀胱结石的描述,正确的是A、膀胱结石易发生在青年人B、膀胱结石均为肾结石或输尿管结石下降而来C、前后位X线平片上,膀胱结石位于耻骨联合下方√D、X线平片上,膀胱结石可为均匀、不均匀或分层状高密度影E、膀胱X线造影检查对膀胱结石无诊断价值26、关于肾结核,以下描述错误的是A、肾结核大多数为血源性感染所致B、肾结核早期,X线平片和排泄性尿路造影可表现正常C、肾结核晚期,排泄性尿路造影时肾盏肾盂可不显影D、肾结核晚期,逆行尿路造影显示大的不规则空腔,具有较高的诊断价值√E、肾结核晚期,CT检查不能与肾积水鉴别,故无应用价值27、肾脓肿的最佳影像学检查技术为A、KUBB、排泄性尿路造影C、逆行肾盂造影√D、CT平扫和增强检查E、MRI平扫和增强检查28、在肾脓肿成熟期,CT检查最具特征的表现是A、低密度肿块,轻度不规则强化√B、水样低密度病变并周边环状明显强化C、病变延伸至肾周间隙D、肾周脂肪密度增高E、肾筋膜增厚29、关于黄色肉芽肿性肾盂肾炎,以下描述正确的是A、黄色肉芽肿性肾盂肾炎是特发性病变,与感染无关B、病理上,形成大量成熟的脂肪组织√C、影像学检查,常可发现肾结石D、CT检查,肾窦脂肪表现正常或增加E、本病仅局限在肾内,从不累及肾周组织和结构30、肾细胞癌中最常见的组织学亚型为√A、透明细胞癌B、乳头状细胞癌C、嫌色细胞癌D、集合管癌E、未分类癌31、肾细胞癌的典型临床表现为三联症,即无痛性肉眼血尿、胁腹部痛和腹部肿块,其占肾癌患者的约√A、10%B、30%C、50%D、70%E、90%32、CT检查时,透明细胞型肾癌最具特征性的表现是A、平扫CT呈混杂密度肿块B、肿块常突向肾外,致肾轮廓发生变形C、肿块内有点状或弧线状钙化√D、三期增强检查,肿块强化呈快进快出表现类型E、发生肾静脉和下腔静脉瘤栓33、CT和MRI检查时,鉴别肾细胞癌与肾血管平滑肌脂肪瘤最可靠的依据是肿块A、大小B、形态√C、含有脂肪密度或信号灶D、增强检查的强化程度E、合并出血34、确定肾盂病变为肾盂癌的最佳影像检查技术为A、X线平片B、排泄性尿路造影C、逆行肾盂造影√D、CT检查E、MRU35、影像学检查,诊断肾肿块为肾血管平滑肌脂肪瘤的可靠依据是A、肿块较大B、肿块多发C、肿块合并出血√D、肿块含有脂肪组织E、肿块明显不均匀强化36、确定输尿管癌及其周围侵犯的最佳影像检查技术为A、排泄性尿路造影B、逆行肾盂造影√C、CT检查D、CTUE、MRU37、以下关于膀胱肿瘤的描述,错误的是A、膀胱肿瘤分为上皮性和非上皮性肿瘤√B、膀胱上皮肿瘤中大多数为良性C、膀胱非上皮肿瘤可为平滑肌瘤、嗜铬细胞瘤和淋巴瘤D、膀胱癌属于上皮性肿瘤E、膀胱癌多为移行细胞癌38、CT检查,膀胱癌侵犯精囊时,以下描述错误的是A、精囊角消失√B、精囊角增大C、精囊增大D、精囊肿块与膀胱肿块相连E、精囊结构消失39、下述肾脏的囊性病变中,最常见的类型是A、肾盂旁囊肿√B、肾单纯性囊肿C、多囊性肾病D、肾复杂性囊肿E、囊性肾细胞癌40、CT检查时,下述关于肾单纯性囊肿表现正确的是A、很少突向肾外B、囊壁清楚可见C、囊壁常有钙化√D、圆形水样低密度灶,无强化E、圆形高密度灶,无强化41、关于子宫的解剖及MRI表现,哪项不正确A、结合带是肌层的一部分,厚度为5~6mmB、肌层厚度为1~3cm√C、结合带T2WI呈明显高信号D、结合带位于子宫肌层与内膜之间E、子宫肌层T1WI呈低信号,T2WI呈略高信号42、输卵管全长为8~14cm,由内向外分为√A、间质部、峡部、壶腹部、伞部B、峡部、间质部、伞部、壶腹部C、间质部、壶腹部、峡部、伞部D、峡部、伞部、问质部、壶腹部E、伞部、间质部、峡部、壶腹部43、下列哪项不是子宫输卵管造影的禁忌证A、严重肝肾功能障碍B、清宫术后4周内C、内生殖器急性炎症√D、子宫输卵管结核E、妊娠44、宫颈正常MRI T2WI表现,下列哪项不正确A、自内向外有四层信号B、高信号的宫颈管内黏液C、中等信号的宫颈黏膜皱襞√D、低信号的中央基质(其与宫体JZ连续)E、中等信号宫颈肌层(其与宫体子宫肌外层相续)45、关于卵巢良性畸胎瘤,错误的是A、可见骨骼,牙齿或骨组织B、CT有时可见到脂-液面C、MRI上呈混杂信号√D、可累及膀胱、直肠E、CT上呈混杂密度46、关于子宫内膜癌,错误的是A、是子宫内膜最常见的恶性肿瘤B、多为腺癌√C、CT扫描是子宫内膜癌的主要诊断方法D、发病高峰年龄为55~65岁E、宫腔常增大或呈分叶状47、确定宫颈癌局部侵及范围,首选影像学检查是A、CTB、USG√C、MRID、血管造影E、子宫输卵管造影48、关于子宫肌瘤,下列描述哪项不对A、是子宫最常见的良性肿瘤B、T1WI,肌瘤为中等信号C、子宫单发或多发肿块D、瘤内可有出血、坏死、囊变、钙化√E、T2WI,肌瘤实体部分为较高信号49、关于正常子宫输卵管造影表现,下列描述哪项不对A、正位观察,子宫腔呈倒置三角形√B、输卵管一般呈连续充盈状C、子宫角与输卵管相通D、壶腹部末端呈漏斗状扩大,为伞端E、注入碘油后24小时或注入水溶性碘剂后1~2小时摄片,显示输卵管内对比剂全部排空并进入腹腔,呈多发弧线状或波浪状致密线影50、关于正常盆腔动脉造影表现,下述哪项正确A、可见子宫动脉由髂外动脉分出B、子宫动脉沿盆壁向内上走行√C、子宫动脉发出宫颈、阴道支供应子宫颈和阴道D、卵巢动脉起于髂内主动脉E、子宫动脉三个终支分别为子宫边缘支、输卵管支和卵巢支51、CT平扫子宫呈√A、横置梭形或椭圆形软组织密度影B、倒置三角形软组织密度影C、正置三角形软组织密度影D、圆形软组织密度影E、椭圆形低密度影52、CT扫描A、在育龄期正常卵巢不能显示B、在育龄期正常卵巢均能显示√C、正常卵巢位于子宫侧壁与髋臼内壁之间D、排卵期,卵巢密度均匀E、可以显示输卵管53、下述哪项不是正常宫颈的MRI表现A、可见高信号的宫颈管内黏液B、可见中等信号的宫颈黏膜皱襞√C、可见低信号的联合带D、可见低信号的宫颈纤维基质E、可见中等信号宫颈肌层54、输卵管僵硬、狭窄、扩张和(或)不通的常见原因是√A、结核B、良性肿瘤C、恶性肿瘤D、细菌感染E、非特异性炎症55、女性生殖系统病变首选和主要的影像检查方法是A、子宫输卵管造影B、CTC、核素扫描D、MRI√E、USG56、常见子宫畸形的类型不包括A、单角子宫B、双子宫C、双角子宫√D、后位子宫E、纵隔子宫57、关于慢性输卵管炎,子宫输卵管造影表现,不正确的是A、病变多为双侧性B、输卵管粗细不均,但仍较柔软C、可表现为梗阻近端输卵管管腔扩大,复查显示对比剂未进入腹腔√D、输卵管积水,表现梗阻远侧输卵管明显扩张E、宫腔受累则形态不规整58、关于子宫平滑肌瘤,哪项不正确A、是女性生殖系统中最常见的良性肿瘤B、可发生玻璃样变性、黏液样变性、脂肪样变性C、可有钙化√D、T2WI上,典型子宫平滑肌瘤呈稍高信号E、MRI是发现和诊断子宫肌瘤的最敏感方法59、关于子宫内膜癌分期,正确的是A、Ⅰ期,肿瘤限于子宫内膜B、Ⅱ期,肿瘤侵犯阴道C、Ⅲ期,肿瘤侵犯至宫外,有远处转移√D、Ⅳ期,肿瘤侵犯膀胱、肠管或发生远隔性转移E、Ⅲ期,肿瘤侵犯至宫外,范围超过真盆腔60、关于子宫内膜异位症,不正确的是A、常位于卵巢、子宫的韧带、直肠阴道隔、子宫直肠隐窝、输卵管、大肠、膀胱、子宫颈以及盆腔腹膜B、CT通常表现为盆腔内囊性肿块并囊腔内积血C、多数病灶轮廓不清D、MRI可表现为短T1长T2信号、长T1长T2信号或混杂信号√E、增强扫描,子宫内膜异位症形成的囊肿周围粘连带和腔内分隔无强化61、CT可测量肾上腺大小,肾上腺增大的诊断标准是A、侧支厚度大于5mm,面积大于150mm2B、侧支厚度大于10mm,面积大于50mm2√C、侧支厚度大于10mm,面积大于150mm2D、侧支厚度大于10mm,面积大于500mm2E、侧支厚度大于5mm,面积大于50mm262、以下关于肾上腺嗜铬细胞瘤的描述,正确的是√A、超声上,肿块呈实性低回声或中等回声B、CT平扫检查,密度类似于水C、CT增强检查,肿块强化且廓清迅速D、T1WI上,肿块信号强度高于肝实质E、T2WI上,肿块信号强度类似肝实质63、关于BPH描述正确的是A、良性前列腺增生好发于周围区,并压迫尿道引起梗阻√B、多见于老年人,由前列腺腺体、结缔组织和平滑肌不同程度增生引起C、增大的前列腺可突向膀胱颈部,膀胱壁不规则增厚D、最佳影像学检查技术是CT平扫及增强扫描E、首选影像学检查方法是MRI平扫及增强扫描64、男,70岁,半年前出现尿频、尿急、尿流缓慢、尿流中断和排尿不尽,无血尿。
黄色肉芽肿性肾盂肾炎CT误诊2例
4 7.
做到耐心 、 细心 、 关心 , 了解患者 的心理需求 , 建立 相互信任 的关系 , 根据病情做好 心理护理 及健康 教育 , 给患者讲 解服
[ ] 屠丽君 . 4 护理管理与护理规范[ . M]南京 : 南京 医科大学脑科医
院 ,0 76 20 :0.
( 收稿 日期 :0 0—0 —2 ) 21 1 6
对身体带来危害 , 护士要 耐心给予 解释 , 除患者对 服药产 消 生不必要 的顾虑 。对于病情恢复又出现抑郁情绪 的患者 , 防 止其 藏药企 图 自杀。巧妙地运 用暗示 , 通过 细心观察 、 热情 解释 、 和蔼劝慰 等树 立威信 , 患者感 到护理 人员是 真心地 使 为他们服务 , 而解 除患者恐 惧不 安的心 理 , 而产生 信赖 从 进 感、 安全感 和康复 的信心 , 取得患者 的合作并乐于接受治疗。
张 占武
( 朝阳市第二医院放射影像 中心 , 辽宁 朝阳 12 0 ) 2 0 0
【 关键词 】 黄色肉 芽肿; 炎;T误诊 肾 c
di1 .9 9 jin 17 o:0 3 6/. s .6 2—0 6 .0 0 1 .8 s 3 9 2 1 .2 0 9 中图 分 类 号 : R 9 . 6 27 文献 标 识 码 : A 文 章 编 号 : 17 —0 6 (0 0 1 6 2 39 2 1 )2—19 0 5 2— 1
参考文献
[ ] 江开达 , 1 周东丰 . 精神病学 [ . M]北京 : 民卫生 出版社 ,0 5 人 20 :
2 6. 4
应 、 暂 时的、 是 不会影 响身 体 的健康 , 使患 者能 继续服 从 治 疗, 安心休养 。协 助患者获得 最佳 的适应状 态 , 主动接受 治
黄色肉芽肿性肾盂肾炎7例CT误诊分析
痛 阈提高 ,局麻 药 的半 衰期 延长 ,以减 轻疼 痛 , 使镇 痛 时 间延 长 。 综上所 述 ,超声技术 引导下连续 肌间沟臂丛
病变形态特征 、 病灶密度及强化形式 , 伴发结石或钙化以及肾周受累情况 。结果
C T平扫加增强扫描 ,5 例发生于左侧 ,2 例发 生于右侧 。弥漫型累及全 肾 ,。 肾影增 大 ,肾盂肾
DO :1 . 6/maJsn10 — 2 52 1 .70 3 I 03 0c .is.0 7 14 . 00 .2 7 . 0
t e f ev l k d [ . u A a s h s l 2 0 i re o a eJ E r n et ei , 0 1, m on b c ] J o
地塞米 松广泛用 于治疗 各种慢性疼 痛有一定 [] Wiim R ,C o iadP,A c n e a . l a 2 la s l S h un r ra d G, t 1 U t — r 的疗 效 。将地 塞米松加人 罗哌卡 因 、利 多卡 因混 s u d u d n es e d e u ina di r v s eq a— o n ia c e s x c t n g p e o mp o e h u l t
l 7) 4 — 5 . 8( : 2 5 8 5
合液 以施行 臂丛阻滞麻醉 ,也证实术后镇 痛时间
i f u rcaiua lc[ .n s A ag,2 0 , t o palvclr okJA et nl y s b ] h 03
明显延长 ,即使疼痛 已恢 复 ,其疼痛强度 也 明显 9 ( 1 1 —1 2 . 7 2 5 8 5 3 减轻 ,地塞米松 可减轻术后 恶心 、呕 吐发 生率和 [] 陈亚 丽 ,申新 ,程红侠 ,等. 3 罗比卡因硬膜 外术 后 自控镇痛 在老年病 人 的应用 … . 临床麻醉 学杂志 , 术后疼 痛【。其 中枢抗 呕 吐机 制可 能是激 动大脑 5 _
有图有真相:4种肾脏炎性病变的CT表现

有图有真相:4种肾脏炎性病变的CT表现肾盂肾炎是下尿路感染逆行累及肾脏所致,依病程和病理变化不同而分为急性和慢性。
1. 主要病理改变急性肾盂肾炎:表现为间质水肿、炎性细胞浸润及微小脓肿形成。
慢性肾盂肾炎:病理特点为肾脏体积变小并不规则疤痕形成而于表面出现多发深浅不同的凹陷,严重者双肾萎缩。
2. CT 表现急性肾盂肾炎:平扫大多数表现正常,少数可见肾脏增大;增强扫描早期由于肾血管分支痉挛,表现多个楔形低密度区。
慢性肾盂肾炎:平扫可见肾体积变小,肾实质变薄,肾表面有多发深浅不等切迹,不宜增强扫描。
图 1 急性肾盂肾炎图 2 慢性肾盂肾炎肾脓肿肾脓肿的 CT 表现因病情而异。
1. 早期炎症期:表现肾实质内略低密度肿块,增强检查可有轻度不规则强化。
2. 脓肿成熟期:表现为类圆形均一低密度病变,增强检查病变周边(脓肿壁)呈环状明显强化,中心脓腔低密度无强化。
3. 感染蔓延期:肾周脂肪密度增高;并有脓肿时,表现肾周和肾旁脂肪间隙消失,代之以混杂密度肿块,内可有小气泡影,增强检查表现为规则或不规则单发或多发环状强化。
图 3 肾脓肿黄色肉芽肿性肾盂肾炎(XGP)占肾脏感染0.6%~1.4%,是一种罕见的、严重的慢性肾脏炎症,可产生弥漫性肾实质破坏,中年女性好发,单侧肾脏受累多见。
临床表现大多为肾区疼痛及反复发作的尿路感染、发热、不适等。
常合并有尿路结石。
CT 表现分弥漫型和局灶型:1. 弥漫型:肾脏体积增大,轮廓不规整;集合系统可见结石影;肾实质内多发囊性占位,多以肾盂、肾盏为中心;肾周受累。
2. 局灶型:局限性囊状病灶(坏死、出血),增强扫描可见脓肿壁强化,可有结石,常伴肾周受累(此型需要与肾肿瘤、肾结核、肾脓肿鉴别)。
图 4 黄色肉芽肿性肾盂肾炎肾结核患者免疫力低,结核杆菌量大,经过肾小球过滤到达肾髓质引起结节增生和组织破坏。
结核结节互相融合,中心坏死形成干酪样病变。
干酪样物质液化肾盏肾盂形成空洞,与之想通的肾盏出现不同程度的变形。
中级卫生专业资格病理学主治医师中级模拟题2020年(23)_真题-无答案
中级卫生专业资格病理学主治医师(中级)模拟题2020年(23)(总分44,考试时间120分钟)一、A2型题1. <span class="RankNumStr">1.</span>男孩,6岁。
1周前患上呼吸道感染,经治疗好转。
近来出现大量蛋白尿、水肿、低蛋白血症和高胆固醇血症。
肾脏穿刺检查结果:肾小球和肾小管均未见明显病变,免疫荧光染色均为阴性,本例最有可能是A. 急性弥漫性增生性肾小球肾炎B. 膜性肾小球病C. 膜增生性肾小球肾炎D. 微小病变性肾小球病E. 系膜增生性肾小球肾炎2. <span class="RankNumStr">2.</span>男性患者,65岁。
1周前其左后腰部曾被人推挤过,之后腰部一直感觉不适,2天后出现无痛性肉眼血尿,同时患者有发热,近日明显消瘦、乏力。
查体:超声和CT显示左肾上极一个直径约3cm的占位病变,内有钙化。
本例最有可能是A. 肾血管平滑肌脂肪瘤B. 肾母细胞瘤C. 肾结核D. 肾细胞癌E. 婴儿型多囊肾3. <span class="RankNumStr">3.</span>男性患者,40岁,近来出现高度水肿、大量蛋白尿,检查其血脂增高,低蛋白血症。
肾穿刺病理检查,光镜下见弥漫性肾小球体积增大,肾小球毛细血管基底膜弥漫性增厚,嗜银染色显示基底膜的钉状突起,无明显细胞增生及炎性细胞浸润;电镜观察,基底膜不同程度地增厚,肾小球脏层上皮细胞下多数排列有序的电子致密物沉积,该病最大可能是A. 膜增生性肾小球肾炎B. 膜性肾小球病C. 微小病变性肾小球病D. 局灶性节段性肾小球硬化E. 系膜增生性肾小球肾炎‘4. <span class="RankNumStr">4.</span>男性患者,54岁,5年前体检时腹部B超发现左肾一个孤立性占位病变,呈囊状,当时未给予任何治疗。
超声诊断黄色肉芽肿性肾盂肾炎4例

[ ] 杨 通 , 莹 莹 , 炼 图 , . 胺 O荧 光 染 色法 在 病 理 特 殊 染 4 顾 何 等 金
( 接 第 13页 ) 细胞 而 呈黄 色 肉芽肿 , 后 形 成 上 3 噬 最
脓 肿 。根 据病 变范 围 ,o r m 把黄 色 肉芽 肿性 肾 Sl n 【 oo J 盂 肾炎 分为弥 漫 型 (5 ~9 %) 8% 0 和局 限型 (0 ~ 1%
形杆 菌 _ ; 尿涂 片 找泡 沫细 胞 , 6晨 虽然 阳性 率不 高 , 但也 是本病 的特 异 性诊 断 ,0 8%晨 尿 离心 沉 渣 图 片 可找 到泡 沫 细胞 。本 组 3例 找 到 泡 沫 细 胞 。鉴 别 仍 有 困难 时 , 行 B超引 导下 细针 穿 刺 活检 以获 建议
rn lgatrcpe t ea a o rf eiin .Am d e i,19 ll JKiny Ds 9 7,3 8 6 0:4
声表 现 多 发囊状 病 灶 1 , 例 多发 结节 状 杂乱 回声 灶
与 囊状 病灶混 合 伴轻 度 积 水 1例 , 2例 局灶 型超 声 表现 为局部不 均质 混合 性肿块 。文献 报道 7 %X . 9 G P 合并 肾结 石 或输 尿 管 结 石 l 。本 组 2例合 并 肾 N l 3 j
清 , 整个 肾脏 回声 显著 紊 乱 , 使 不均 肾盏 积水并 存 。 本 病临床 、 像 征 象 缺 乏 特 异 性 , 断 比较 困 影 诊 难, 误诊 率较 高 。作 者认 为对 有上 尿 路结 石 、 阻 , 梗 有反复 感染症 状 , 痛 、 部包 块 者 , 腰 腰 尤其 是 中年 女
其 是在气 温 较高时 如 无法 及 时检 测 则应 避 光冷 藏 ,
以免 造成假 阴性 。
肾盂癌影像表现
肾盂壁的不规则增厚,或呈扁平状肿块 增强扫描:肾盂壁局限性不规则增厚,异常强化,部分可呈结节状,
排泄期肾盂肾盏不规则充盈缺损,可导致肾积水。 ➢ MR:T2可见肾盂高信号尿液周围见锯齿状或波浪状等信号增厚肾盂壁
35Hu 62Hu
37Hu
男,64岁,反复排肉眼血 尿3个月 病理: 肾上极肾盂浸润性 低级别尿路上皮癌(T3)
间隙中 ➢ 肾盏截断:阻塞后积水继发肾功能差或肿瘤浸润肾盏
影像表现
➢ CT分型: Ⅰ型:肾盂内肿块型(大多采用KSS) Ⅱ型:肿块浸润肾实质型(大多采用RUN) Ⅲ型:肾盂壁增厚型
➢ 增强:乏血供,轻中度强化。 ➢ 肾积水:与疾病晚期和高危的病理类型有关 ➢ 肿块内低密度灶:可能提示恶性程度升高的病理,钙化罕见。 ➢ 肾功能减低:引流区域肾实质强化减弱
影像表现
肿块浸润肾实质型: ➢ CT:
肾盂-肾实质内软组织肿块,边界模糊,较大时密度不均 肾窦脂肪间隙消失 肾脏轮廓存在,无明显外突或凹陷 增强扫描:轻中度强化,肾血管无明显增粗,且肾静脉及下腔静脉很少受累 可累及或同时发生输尿管及膀胱的尿路上皮癌 ➢ MR:信号较不均匀,T1WI混杂低信号、T2WI混杂高信号
女,60岁,右侧腰背部疼痛2周。 病理:符合黄色肉芽肿性肾盂肾炎改变
治疗:
UTUC
低危(包含以下所有)
➢ 单发病灶 ➢ 肿瘤大小小于2cm ➢ 低级细胞学 ➢ 输尿管镜活检为低级别 ➢ CTU上没有侵入性特征
保肾手术(KSS)
高危(任意一个)
➢ 多发病灶 ➢ 肿瘤大小大于2cm ➢ 肾盂积水 ➢ 影像学怀疑浸润性上尿路癌 ➢ 高级细胞学或组织学变异 ➢ 输尿管镜活检为高级别 ➢ 既往有膀胱癌根治性切除术
肾脏占位性病变的影像学诊断
肾脏占位性病变的影像学诊断杨宁刚;王海燕;王绍平;王奎【摘要】肾脏占位性病变种类多,临床表现不典型,鉴别良恶性病变较困难,尤其一些不常见的病变,如集合管癌、内分泌癌等更是给临床诊断和治疗带来了难度.目前主要采用B 超、CT、MRI 等检查手段确定诊断,随着技术和设备的不断革新升级,一些新的观点和理念的出现,如超声造影、术中超声定位、增强螺旋CT 及MRI 动态增强扫描和弥散加权等,三者的各自优势越发凸显,但他们的临床利用价值说法不一.主要表现在三个方面:一是影像学检查的模式;二是确定诊断的首选方法;三是性价比.本文就B 超、CT、MRI 在肾脏占位性病变诊断中的作用进行对比说明,综述如下.【期刊名称】《中国医药科学》【年(卷),期】2011(001)011【总页数】3页(P67-69)【关键词】肾脏占位性;诊断;B 超;CT;MRI【作者】杨宁刚;王海燕;王绍平;王奎【作者单位】兰州市第一人民医院泌尿外科,甘肃兰州,730050;兰州市第一人民医院泌尿外科,甘肃兰州,730050;兰州市第一人民医院泌尿外科,甘肃兰州,730050;兰州市第一人民医院泌尿外科,甘肃兰州,730050【正文语种】中文【中图分类】R737.111 B超的筛选作用B超在实质性、囊性和混合性肿物的鉴别方面是一种简单有效的方法,在早期肾肿瘤和普查时对小肾癌发现和诊断方面起了重要作用。
据统计2/3的早期病变经B超偶然发现[1]。
Jamis报道[2]小肾癌发现率由13%上升到48%,徐朝霞等[3]报道小肾癌诊断准确率提高到70%以上。
肾脏占位性病变B超的典型表现是肿物处的肾结构不甚清楚,肾脏局部隆起,边缘毛糙不清,可发现低回声阴影,回声常不均匀。
因肿瘤出血、液化、钙化等原因,可出现液性暗区或回声增强等表现。
根据密度特点,B超分为两种类型:(1)强回声型:表现为肿瘤区密度细小而增强回声,远端可伴有信号衰减,多见于小型肾细胞癌;(2)弱回声型:肿瘤区表现为密度细小的点状回声,其强度与肾皮质回声近似,多见于中等大小肾癌。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Ultrasonographic Features of Focal Xanthogranulomatous PyelonephritisJongchul Kim, MDObjective.T o analyze the ultrasonographic features of focal xanthogranulomatous pyelonephritis.Methods.Ultrasonographic features of 15 patients with pathologically proved focal xanthogranulo-matous pyelonephritis were retrospectively analyzed by 2 radiologists who reached a consensus, in terms of the location, margin, size, and echo texture of the mass, associated calculi, lymphadenopa-thy, or local extension, in comparison with computed tomographic and clinical findings. Results.At ultrasonography, 12 (80%) of 15 masses were well circumscribed. The maximal sizes of the masses ranged from 2.5 to 5.8 (mean, 3.8) cm. Thirteen solid masses (87%) were hyperechoic (n = 7), hypoe-choic (n = 4), or isoechoic (n = 4) to the renal cortex, and the preoperative diagnosis was either renal cell carcinoma (n = 11) or Wilms tumor (n = 2). The preoperative diagnosis of the other 2 cystic lesions (13%) was renal abscess. Renal calculi were found in 1 case, but lymphadenopathy or local extension was not depicted. Clinical inflammatory signs were found in 11 of 15 patients. Conclusions.There were no specific ultrasonographic features that allow for the distinction between focal xanthogranu-lomatous pyelonephritis and renal tumors or abscesses. Focal xanthogranulomatous pyelonephritis should be considered when there are clinical signs of infection or inflammation and a focal solid mass is seen on ultrasonography. Key words:inflammation; kidney; ultrasonography.Received September 2, 2003, from the Department of Diagnostic Radiology, College of Medicine,Chungnam National University, Daejeon, South Korea. Revision requested September 15, 2003.Revised manuscript accepted for publication September 24, 2003.Address correspondence and reprint requests to Jongchul Kim, MD, Department of Diagnostic Radiology, Chungnam National University Hospital,640 Daesa-dong, Jung-ku, Daejeon 301-721, South Korea.E-mail: jckim@cnuh.co.kr.AbbreviationsCT , computed tomography; ESR, erythrocyte sedimenta-tion rate; MR, magnetic resonance; RCC, renal cell car-cinoma; XGP , xanthogranulomatous pyelonephritisanthogranulomatous pyelonephritis (XGP) is a relatively uncommon form of renal granuloma-tous inflammatory disease characterizedhistopathologically by the presence of lipid-laden macrophages (xanthoma cells), as well as other inflammatory cells, including plasma cells, leukocytes,and histiocytes.1T wo forms of XGP , a diffuse form (85%)and a focal (localized, segmental) form (15%), are well known, and the latter is sometimes referred to as the “tumefactive” form of XGP because the findings are more easily confused with a renal tumor.1–8The definitive diag-nosis of focal XGP is most often recognized after histolog-ic examination of the surgical specimen.9Although surgery is considered the only effective treatment of focal XGP , a high index of suspicion of XGP may prevent radical nephrectomy.10Therefore, it may be helpful and useful in© 2004 by the American Institute of Ultrasound in Medicine • J Ultrasound Med 23:409–416, 2004 • 0278-4297/04/$3.50Xclinical fields to know whether there are any characteristic imaging findings more favorable to focal XGP rather than, for example, renal tumors. Ultrasonography is commonly used in the diag-nosis of renal lesions as a primary imaging tool. The purpose of this study was to analyze the ultrasonographic features of focal XGP. Materials and MethodsBetween January 4, 1986, and June 28, 2003, 15 cases of pathologically proved focal XGP were collected at our hospital and at other associated institutions. After clinical examination with imaging studies by ultrasonography, the patients underwent total (n = 13) or partial (n = 2) nephrectomy. In the latter 2 patients, an area of focal disease was identified as an abnormality on ultrasonography, which was confirmed as XGP by biopsy, and a limited resection was performed to remove the focal area of inflammation. Renal ultrasonography was performed with 3.5- and 5-MHz transabdominal probes of an SL-2 system (Siemens Medical Solutions, Erlangen, Germany), a D RF 400 system (D iasonics, Milpitas, CA), and SSD-630, SSD-650, and SSD-280 systems (Aloka Co, Ltd, T okyo, Japan); 3.5-and 4-MHz transducers of Acuson 128XP and Sequoia systems (Siemens Medical Solutions); a 4- to 7-MHz convex probe of an Ultramark 9 HDI system (Philips Medical Systems, Bothell, WA); and a 2- to 4-MHz curved probe of an HDI 3000 system (Philips Medical Systems). Computed tomography (CT) was also performed in all patients with a HiSpeed Advantage CTi Standard system (GE Medical Systems, Milwaukee, Wisconsin) or a Somatom Plus VD30 system (Siemens Medical Solutions). After precontrast abdominal CT, postcontrast CT scanning with an 8- to 10-mm slice interval was done by bolus injection of iopromide (Ultravist 300; Schering AG, Berlin, Germany; 0.6234 g/mL, 140–150 mL). The ultrasonographic features of the 15 patients were retrospectively analyzed by 2 radi-ologists who reached a consensus. Renal lesions were retrospectively evaluated in terms of their location, margin based on the degree of demar-cation from surrounding renal parenchyma, maximal size, echogenicity based on comparison with the renal cortex, signs of perinephric involvement, signs of metastatic disease such as lymphadenopathy or venous invasion, and asso-ciated calculi or hydronephrosis.The hospital records of all patients were retro-spectively examined in detail, and the patients were checked for clinical symptoms and signs. ResultsThere were 13 adults and 2 children younger than 15 years and 10 male and 5 female patients (age range, 6–57 years; mean age, 39 years). The right kidney was affected in 8 (53%) of the 15 patients.On review of hospital records, the positive find-ings on initial clinical and laboratory examina-tions were found to be flank pain in 10 patients, fever in 11, leukocytosis in 9, pyuria in 8, anemia in 9, a raised erythrocyte sedimentation rate (ESR) in 10, and positive urine culture results in 5. Of the 5 patients with positive urine culture results, Proteus mirabilis grew in 2, Escherichia coli grew in 2, and a mixture of these 2 bacteria grew in the remaining patient. Ultrasonography depicted that 12 (80%) of 15 masses were well circumscribed (Figures 1–3) and were confined within the renal outline. Eight masses were based in the cortex (Figures 1 and 3), and the other 7 were based more centrally near the renal sinus (Figure 2). The maximal sizes of the masses ranged from 2.5 to 5.8 (mean, 3.8) cm. Of 15 masses, 13 (87%) were solid, and 2 were cystic. The predominant echogenicity of the solid lesions was hypere-choic to the renal cortex in 7, hypoechoic in 4, and isoechoic in 4. There were no masses that were as echogenic as renal sinus fat. The 13 solid masses included 10 (77%) with inner hypoe-choic or anechoic foci and 3 without inner hypoechoic or anechoic foci, and the preopera-tive clinical diagnoses were renal cell carcinoma (RCC) in 11 cases (Figure 1) and Wilms tumor (Figure 2) in 2 cases. Ultrasonography depicted no evidence of perirenal or vascular (eg, renal vein and inferior vena cava) involvement or local or distant lymphadenopathy in any case. In the other 2 cystic masses, ultrasonography depicted mainly anechoic renal lesions with thick and irregular walls, suggesting the preop-erative diagnosis of renal abscess (Figure 3). A focal bulge of renal contour adjacent to the mass was not noted in any case except 1 large mass of 5.8 cm in maximal diameter. Renal cal-culi were found as highly echogenic foci with clean posterior acoustic shadowing in the periphery of the solid mass in 1 case.410J Ultrasound Med 23:409–416, 2004 Focal Xanthogranulomatous PyelonephritisOn noncontrast abdominal CT , the density of the 13 solid masses compared with surrounding normal renal parenchyma was slightly lower in 2J Ultrasound Med 23:409–416, 2004411KimCA412J Ultrasound Med 23:409–416, 2004Focal Xanthogranulomatous PyelonephritisBA DCJ Ultrasound Med 23:409–416, 2004413KimBAquent peritumoral halo, intratumoral cyst, and calcification in small RCC,1the infrequency of these findings in our focal XGP cases may play a certain role in the differentiation of these 2 renal parenchymal lesions. Most Wilms tumors are expansile masses with well-circumscribed peripheral margins due to the formation of a sur-rounding pseudocapsule composed of fibrous tissue and compressed adjacent normal parenchyma. Occasionally, an infiltrative pattern of growth is seen. A Wilms tumor is typically a predominantly solid but heterogeneous tumor on ultrasonography. The echogenicity is variable; in tumors with areas of necrosis, hypoechoic and anechoic areas may be seen. Calcification or invasion of the renal vein and inferior vena cava may also occur.13Absence of perirenal involve-ment, local or distant lymphadenopathy, distant metastases, a focal renal contour bulge, and vas-cular invasion in our focal XGP cases may also suggest some hints to differentiate a large focal XGP from a large RCC or Wilms tumor. In our study, the predominant echogenicity of the solid lesions was hyperechoic (n = 7), hypoechoic (n = 4), or isoechoic (n = 4) to the renal cortex, and there were no masses that were as echogenic as renal sinus fat. The classification of the predomi-nant echogenicity of the solid lesions of XGP was not found in other reports describing ultrasono-graphic features of focal XGP.6,10,12In our study, however, focal XGP appeared as very nonspecific masses, and there was extensive overlap between the ultrasonographic features of focal XGP and those of renal tumors or abscesses.Co mputed tomography, which is considered the imaging modality of choice, reveals the XGP lesion, but differential diagnosis from hydronephrosis or pyonephrosis, malako-plakia, lymphoma, and especially renal neo-plasms is sometimes difficult.11Computed tomographic features that have been consid-ered characteristic of (but not pathognomonic for) XGP (especially in th e diffuse form) are renal enlargement, strands in perinephric fat, thicken-ing of the Gerota fascia, and thick enhancing septa in the hypodense areas in renal parenchy-ma.12Round or egg-shaped areas of water densi-ty representing dilated calyces and abscess cavities with pus and debris in diffuse XGP may be described as the “bear paw sign.”12Computed tomography usually depicts focal XGP as a clear-ly or poorly defined localized intrarenal mass with fluidlike attenuation,1,3,13as in our cases.There are not many data about magnetic reso-nance (MR) imaging findings in the focal form of XGP,3,4,13,15and we have no experience with MR imaging in XGP. According to a report by Cakmakci et al,3the focal mass had slightly low signal intensity on transverse relaxation time–weighted imaging (probably because of fluid with very high protein content) and was isointense with the renal parenchyma on longi-tudinal relaxation time–weighted imaging. They found that the findings of absent high signal intensity on transverse relaxation time–weight-ed imaging and long-standing low signal inten-sity compared with the renal cortex during the whole course of the dynamic MR imaging study were useful in the differentiation of XGP from RCC. The different signal intensity of the solid component of XGP on longitudinal relaxation time–weighted imaging, compared with the renal parenchyma, seems to depend on the amount of xanthoma cells involved in the granu-lomatous process.4None of our patients, howev-er, underwent MR imaging.The treatment of focal XGP is still controversial. Partial nephrectomy, however, has been tried in the treatment of focal XGP.12–14Quinn et al12said that, “In the relatively rare cases where the focal form of XGP is found, which involves only a sin-gle pole of the kidney, it might be possible to carry out a partial nephrectomy. It is generally accepted that once the diseased kidney has been removed the future prognosis for the affected child is excellent.” Anezinis et al13insisted that focal XGP could appear as a pseudotumoral cys-tic lesion, suggesting that XGP in such cases might be useful to the surgeon to plan an organ-sparing procedure. Osca et al14insisted that,“When focal XGP is diagnosed, local excision such as partial nephrectomy is recommended, since relapse in the affected kidney is unusual.”There also are reports of a few patients who recovered from the disease after administration of antibiotic therapy.10,16Thus, although surgery is considered as the only effective treatment of this disease, a high index of suspicion on the basis of clinical and imaging findings may pre-vent radical nephrectomy.Our retrospective study has some limitations. The number of cases, 15, is not sufficient to be statistically significant. There were no patients who underwent MR imaging. Because our 15 cases were collected not only from our hospital but also from many other associated institutions,414J Ultrasound Med 23:409–416, 2004 Focal Xanthogranulomatous Pyelonephritisultrasonographic imaging standards and tech-niques were not constant among the many oper-ators performing ultrasonography.The characteristics of the condition that might help in a preoperative diagnosis of dif-fuse or focal XGP include the following: the disease is usually unilateral (although very rare bilateral cases have been reported); renal func-tion is absent or grossly impaired on the involved side, especially in diffuse XGP; large, often numerous, renal calculi, including staghorn calculi, with or without hydronephro-sis are present, especially in diffuse XGP; and anemia, a raised ESR, and leukocytosis are often present.12Usually, typical solid tumors of the kidney such as RCC or Wilms tumor would not present with infection. However, if inflam-matory signs are few or absent and a history of urinary tract infection or a stone is absent, the preoperative diagnosis of XGP as differentiated from typical solid renal tumors may be very dif-ficult. Accurate diagnosis of the XGP is usually not achieved preoperatively because symp-toms are not specific and pathognomonic lab-oratory tests are not available. Although the diagnosis of XGP is mainly achieved histologi-cally, a suggestive preoperative diagnosis and determination of the extent of the lesion by ultrasonography, CT, MR imaging, or any com-bination could allow less radical surgery in selected focal XGP cases. D espite the protean clinical and imaging manifestations of focal XGP, awareness of the possibility of this condi-tion occurring in adults and children may allow early recognition and possible treatment.In conclusion, there are no specific ultra-sonographic features that allow for the distinc-tion between the solid form of focal XGP and renal tumors, and there is no way to distin-guish the cystic form of focal XGP from a renal abscess. Focal XGP should be considered when there are clinical signs of infection or inflammation and a focal solid mass is seen on ultrasonography.References1.Dunnick NR, Sandler CM, Amis ES Jr, Newhouse JH.Renal inflammatory disease. In: Dunnick NR, Sandler CM, A mis ES Jr, Newhouse JH (eds). T extbook of Uroradiology. 2nd ed. Baltimore, MD: Williams & Wilkins; 1997:163–189.2.Zorzos I, Moutzouris V, Petraki C, Katsou G.Xanthogranulomatous pyelonephritis: the “great imitator” justifies its name. Scand J Urol Nephrol 2002; 36:74–76.3.Cakmakci H, Tasdelen N, Obuz F, Yilmaz E,Kovanlikaya A. Pediatric focal xanthogranulomatous pyelonephritis: dynamic contrast-enhanced MRI find-ings. Clin Imaging 2002; 26:183–186.4.Verswijvel G, Oyen R, Van Poppel H, Roskams T.Xanthogranulomatous pyelonephritis: MRI findings in the diffuse and the focal type. Eur Radiol 2000;10:586–589.5.Zia-Ul-Miraj M, Cheema MA. Xanthogranulomatouspyelonephritis presenting as a pseudotumor in a 2-month-old boy. J Pediatr Surg 2000; 35:1256–1258.6.Özcan H, Akyar S, Atasoy C. An unusual manifesta-tion of xanthogranulomatous pyelonephritis: bilater-al focal solid renal masses. A JR A m J Roentgenol 1995; 165:1552–1553.7.Kim JC. US and CT findings of xanthogranulomatouspyelonephritis. Clin Imaging 2001; 25:118–121. 8.Tiu CM, Chou YH, Chiou HJ, et al. Sonographic fea-tures of xanthogranulomatous pyelonephritis. J Clin Ultrasound 2001; 29:279–285.9.Perez LM, Netto JM, Induhara R, Mroczek-MusulmanE. Xanthogranulomatous pyelonephritis in an infantwith an obstructed upper pole renal moiety. Urology 1999; 54:744.10.Raziel A, Steinberg R, Kornreich L, et al.Xanthogranulomatous pyelonephritis mimicking malignant disease: is preservation of the kidney pos-sible? Pediatr Surg Int 1997; 12:535–537.11.Youngson GG, Gray ES. Neonatal xanthogranuloma-tous pyelonephritis. Br J Urol 1990; 65:541–542. 12.Quinn FMJ, Dick AC, Corbally MT, McDermott MB,Guiney EJ. Xanthogranulomatous pyelonephritis in childhood. Arch Dis Child 1999; 81:483–486.13.A nezinis P, Prassopoulos P, Daskalopoulos G,Mavromanolakisa E, Gourtsoyiannis N, Cranidis A.MRI and CT features in 2 unusual cases of xan-thogranulomatous pyelonephritis. Eur J Radiol 1998;28:98–101.14.Osca JM, Peiro MJ, Rodrigo M, Martinez-JabaloyasJM, Jimenez-Cruz JF. Focal xanthogranulomatous pyelonephritis: partial nephrectomy as definitive treatment. Eur Urol 1997; 32:375–379.J Ultrasound Med 23:409–416, 2004415KimFocal Xanthogranulomatous Pyelonephritis15.Pickhardt PJ, Lonergan GJ, Davis CJ Jr, Kashitani N,Wagner BJ. Infiltrative renal lesions: radiologic-patho-logic correlation. Radiographics 2000; 20:215–243.16.Ramboer K, Oyen R, Verellen S, Vermeersch S, BaertA L, Verberckmoes R. Focal xanthogranulomatouspyelonephritis mimicking a renal tumor: CT and MRfindings and evolution under therapy. Nephrol DialTransplant 1997; 12:1028–1030.416J Ultrasound Med 23:409–416, 2004。