case report
迈向SCI之路:新英格兰杂志Casereport全文解析

迈向SCI之路:新英格兰杂志Casereport全⽂解析作为医学科研狗,当你没有经费,没有数据,统计跟英语都是渣渣的时候怎么样才能发表SCI呢,除了Meta分析,病例报道(Case report)可能是你迈向SCI之门的⾸选论⽂模式。
Case report是通过对⼀两个⽣动的病例进⾏记录和描述,使抽象的⼀般性的疾病表现和诊疗过程有了具体的形象的内容,试图在疾病的表现、机理以及诊断治疗等⽅⾯提供第⼀⼿感性资料的医学报告。
总结发现,⼀篇漂亮的Case report⾄少具备三个特征:1. 临床意义⼀篇个案报道最重要的是对临床实践的指导意义,这⼀点需要明确表达出来。
2. 引⼈⼊胜⼀篇个案报道必须写成⼀个简练但引⼈⼊胜的故事,这⼀点可以借鉴别⼈已经发表的东西。
注意:每个⼈都可能有不良习惯,需要借鉴的是学术界内能被⼴泛接受的东西,不能认为 “有⼈这么写,所以我也这么写”。
3. 符合习惯个案报道的语⾔表述必须符合学术界普遍认可的基本习惯。
举例⼀位医⽣⽂章第⼀句话是:In September 13, a 56-year-old male was admitted witha history of DiscTrode radiofrequency treatment ……编辑分析第⼀句话需要把⼊院的基本原因(例如双腿肿胀/疼痛2周)写出来。
⾄于以前接受过的治疗(即使被认为是主要症状的原因),需要放在稍后去说。
今天将⽤⼤篇幅从专业⽤词、典型句式、常⽤语法结构等⽅⾯,详细解读⼀篇Case report,标题为Thinking Inside the Box,于2010年8⽉发表在新英格兰杂志(The New England Journalof Medicine, IF 51.658)第363期574-579页(获取这篇⽂献全⽂可分享此⽂到朋友圈,截图发给⼩编后(微信号mrwxiaobian)即可获得。
A 62-year-old woman presented to a community hospital with nausea, vomiting, diarrhea, and fever, all of 1 week's duration.第⼀句话:主述。
SCI之路1——Case Report篇

INTRODUCTION
引言
1、总体上介绍GIST,什么是 GIST,有什么特点,病 理特征怎么样等等。。。 2、我们在这里报道1例由于 阑尾出血而偶然诊断的 GIST。
Case ReΒιβλιοθήκη ort 病例报告1、最简单易写,但是认为 最关键,因为要引起 别人的兴趣。 2、好写在什么地方? 好比我们中文个案一 样—男,多少岁,因 为XX入院,实验室检 查。。,手术。。 3、很多话是可以“拿来” 的,好比一个填空一 样,只是个别数值需 要修改下就好。
Case Report组成
1.Abstract and Keywords(摘要和关键词) 2.INTRODUCTION(引言) 3.CASE REPORT(病例报告) 4.DISCUSSION(讨论) 5.REFERENCES(参考文献)
胃肠道间质瘤举例——GIST(上文)
这是一例关于阑尾间质瘤的病例,我之前说过胃肠 道间质瘤在胃肠道常见,阑尾罕见。
Abstract an Keywords
概述性摘要: 三步走 1、GIST是什么? 2、GIST是少见,绝大部分 位于胃肠部位,但是 位于阑尾非常罕见。 3、我们在此报道1例阑尾 GIST,由于阑尾出血 而被偶然诊断。 关键词: 一般满足要求即可。
Case Report
Case Report中注意事项
1、前面讲过,比较好写,因为很多话在任何病例中基本是一样的,A 56-year-old man was admitted to our department on an emergency basis because of a sudden onset of hematochezia.注意我划线部分, 就是所谓的可以填空的,一个56岁的男性患者因为突然开始便血 而来我院就诊,那你可以替换成因为头疼,或因为腹疼,或因为 腹泻。。。 2、写作中基本就是按照我们诊断基本的步骤而来,从体检到实验室或 者影像学检查,再到手术或者治疗,再到预后等等,限于篇幅, 但是在此之间要在相应部位插入图片,比如术前的影像学、术中 照片以及术后病理等等。。。。。。
英语病例报告作文

英语病例报告作文Title: Case Report in English。
Introduction:A case report is an important tool in medical research that documents the clinical presentation, diagnosis, and treatment of a patient. It is a detailed description of a patient's medical history, symptoms, physical examination, laboratory tests, and imaging studies. Case reports are often used to share rare or unusual cases, to describe new diseases or treatments, and to highlight diagnostic challenges or successes. In this article, we will discuss the key components of a case report and provide examples of how they are used in medical research.Case Presentation:The case presentation is the first section of a case report and provides an overview of the patient's medicalhistory, symptoms, and physical examination findings. It should include a brief summary of the patient's demographic information, medical history, and presenting symptoms. For example:A 45-year-old male with a history of hypertension and hyperlipidemia presented to the emergency department with chest pain and shortness of breath. He reported a sudden onset of severe chest pain that radiated to his left arm and jaw. He also complained of difficulty breathing and sweating profusely. On physical examination, he was found to have an elevated blood pressure and heart rate, and crackles were heard in his lungs.Diagnostic Studies:The second section of a case report is the diagnostic studies, which describe the laboratory tests, imaging studies, and other diagnostic procedures used to diagnose the patient's condition. It should include the results of any relevant laboratory tests, such as blood tests, urine tests, or imaging studies, such as X-rays, CT scans, orMRIs. For example:The patient's initial electrocardiogram (ECG) showedST-segment elevation in leads II, III, and aVF, consistent with an acute inferior myocardial infarction. A chest X-ray revealed bilateral pulmonary edema. Blood tests showed elevated troponin levels, indicating myocardial injury.Treatment and Outcome:The third section of a case report is the treatment and outcome, which describes the patient's response totreatment and their overall outcome. It should include a description of the treatment plan, any complications or adverse effects of treatment, and the patient's overall clinical course. For example:The patient was diagnosed with an acute inferior myocardial infarction and was treated with aspirin, heparin, and nitroglycerin. He underwent a cardiac catheterization, which revealed a 90% stenosis in the right coronary artery. The stenosis was successfully treated with percutaneouscoronary intervention (PCI) and a stent was placed. The patient's symptoms improved and he was discharged from the hospital on the third day after admission. He was prescribed antiplatelet and lipid-lowering medications and referred to cardiac rehabilitation.Discussion:The final section of a case report is the discussion, which provides an interpretation of the case and a review of the relevant literature. It should include a discussion of the diagnosis, treatment, and outcome of the case, as well as any relevant differential diagnoses, pathophysiology, or epidemiology. For example:Acute myocardial infarction is a common cause of chest pain and shortness of breath in middle-aged and elderly patients. The classic presentation of myocardial infarction is chest pain, which is often described as pressure or tightness and may radiate to the left arm, jaw, or back. The diagnosis of myocardial infarction is based on clinical presentation, electrocardiogram findings, and cardiacbiomarker levels. The treatment of myocardial infarction includes reperfusion therapy, which can be achieved with either PCI or thrombolytic therapy. The prognosis of myocardial infarction depends on the extent and severity of the myocardial damage and the presence of comorbidities.Conclusion:Case reports are an important tool in medical research that provide valuable insights into the diagnosis, treatment, and outcome of patients with rare or unusual conditions. They can also highlight diagnostic challenges or successes and contribute to the development of new treatments or diagnostic criteria. Writing a case report requires careful attention to detail and adherence to a standardized format. By following the key components of a case report, researchers can effectively communicate their findings and contribute to the advancement of medical knowledge.。
案例报告 Case Report Template

INSTRUCTIONS TO AUTHORSCase ReportsCASE REPORTS (Fewer than 2000 words)We receive a large number of case reports and typically accept those of exceptional teaching value.DEFINITION: Articles reporting a small number of patients (typically 1-5) patients with: (1) a diagnostic dilemma; (2) an unusual manifestation of disease processes; (3) an unusual treatment challenge; (4) an unanticipated early failure or complications of some treatment. We typically do not accept cases in which two entities are associated since conditions may occur coincidentally, rather than causally. Authors must include a comprehensive literature review if a rare event.∙ Must contain Introduction, Case Report, and Discussion. The Introduction should include the need and rationale for the new technique.∙Must use text TEMPLATE for guide: (see below).Authorship (Navigate below)We believe it important to document the adequate participation of all authors in at least three major elements of a study and report; the number of authors will generally relate to the scope of the project. For case reports we request no more than 4 authors. In all cases, however, multiple contributions of each author must be documented in our required form addressing copyright transfer, authorship, and conflicts of interest. Authors are encouraged to read “Thoughts on Authorship” Clin Orthop Rel Res 2008; 466:1002-5. Conflict of Interest statement (Navigate below)Authors of all manuscripts published in CORR must clarify any and all potential conflicts of interest. On the Title Page please note any funding or financial support or potential sources of conflict of interest:∙Consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.∙If any author has directly received research funding and/or has potential conflicts of interest, State "One or more of the authors () has received funding from" and note the source and the initials of those authors who received funding in the parentheses.∙If your institution received any sort of support state, "The institution of the authors has received funding from" and note the source.∙If you received no financial support please note, "Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article."If you or any author have received or may receive any personal payment or in-kind benefit or other professional benefits from a commercial entity (eg, serve as aconsultant), please note, "Each author certifies that he or she has or may receive payments or benefits from a commercial entity related to this work."Ethical Review Committee Statement (Navigate below)Manuscripts involving humans or human data must be accompanied by a copy of the letter from your ethical committee approving your studyREMOVE ALL INSTRUCTIONS ABOVE PRIOR TO UPLOADING FINALDRAFT TO EDITORIAL MANAGERCase ReportTITLE PAGEThis page must include the following:∙ Title (containing fewer than 80 characters including spaces)∙ Running title (containing fewer than 40 characters including spaces)∙Author name(s) and final degree(s) (must follow authorship guidelines)∙The affiliation(s), and address(es), and e-mail addresses of all author(s)∙Conflict of interest statement∙Ethical review committee statement∙ A statement of the location where the work was performed (only if authors from multiple institutions)∙Word Count (Introduction through Discussion): Limit manuscript to fewer than 2000 words.∙The Corresponding Author name and e-mail address (must be same as Corresponding Author in Editorial Manager).1Abstract: Your Abstract must be structured with the following four sections and contain 2fewer than 250 words.3∙Background4∙Case Description∙Literature Review56∙Clinical Relevance7Introduction (maximum of 500 words)89∙All manuscripts must contain an Introduction, typically three paragraphs.10∙We suggest one paragraph of background (citing but not amplifying relevant11literature), one or two of rationale, and a final paragraph only stating the purposes 12of the report.13Case Report (maximum of 250 words for each case.)14∙Describe the history, physical examination, laboratory tests and imaging, treatment, 15and followup of each case.16Discussion ( maximum of 1000 words)∙Begin with a restatement of the novelty of the case or cases.1718∙Compare and contrast your case or cases with those in the literature; when relatively few cases have been reported, provide a table comparing the key findings or1920outcomes.21∙End with a summary of the literature.AcknowledgmentsNote any nonfinancial acknowledgments. Begin with, “We thank…” and note the nature of the contribution.∙Ensure your references are complete and in alphabetical order and proper format (modified AMA style - please see our published instructions on our Website).∙In-text citations should appear before commas and periods and located in a sentence immediately after the point they are documenting.∙Provide brief legends to include the major point.∙Figure legends should be written in complete sentences.∙Illustrations with multiple figures (eg, 1A, 1B, 1C) must be labeled "A," "B," and "C"in the lower left hand corner. Each illustration requires a separate legend.∙Figures should be uploaded and separately labeled in Editorial Manager.∙Color illustrations may be used for surgical photographs, photomicrographs, complex graphics; black and white should be used for other illustrations.。
儿科英文病历 case report
Medical Records for AdmissonMedical Number: General informationName:Age:Sex: Female Race:Han Nationality:China Address: Parents Name:Date of admission: May 8th, 2001 Date of record: 11Am, May 8th, 2001 Complainer of history: patient’s motherReliability: ReliableChief complaint: Pharyngalgia and fever for four days.Present illness:The patient felt pharyngalgia and weak about four days ago. She ate some medicine (not clear), but it do nothing. Then she found ulcer in her mouth and fever all along, but she felt no nausea and never vomited. So her parents took her to Wuhan Children’s Hospital, there she received treatment of antibiotics, but her symptom s didn’t abate. So her parents took her to our hospital, she was adm itted with a diagnosis of “fever of unknown”Since onset, her appetite was not good, and both her spiritedness and physical energy are bad. Defecation and urination are normal.Past historyThe patient is healthy before.No history of “measles” or “pertussis” etc and no contact history with T.B or other infective diseases. No allergy history of food but she was allergy to sulfa.Personal history1.Natal: First birth born, uneventfully and on full term with birth weight2.7 Kg. The state of her at birth was good, no cyanosis, apnea, convulsionor bleeding.2.Development: Able to raise head at second month. The first tooth eruptedat 6th. She began to walk at one. Her intelligence was normal.3.Nutrition: She was only feeded with breast milk before she was 6 monthsold. Then the additives were added. She was weaned from the breast at 14th month.4.Immunization: Inoculated on schedule after birth (such as B.C.G, D.P.Tand smallpox voccination).Physical examinationT 39.5℃, P 120/min, R 30/min, BP 110/90mmHg. She is well developed and moderately nourished. Active position. The skin was not stained yellow. No cyanosis. No pigmentation. No skin eruption. Spider angioma was not seen. No pitting edema. Superficial lymph nodes were found enlarged in her neck, but no flare and tenderness.HeadCranium: Hair was black and well distributed. No deformities. No scars. No masses. No tenderness.Ear: Bilateral auricles were symmetric and of no masses. No discharges were found in external auditory canals. No tenderness in mastoid area. Auditory acuity was normal.Nose:No abnormal discharges were found in vetibulum nasi. Septum nasi was in midline. No nares flaring. No tenderness in nasal sinuses.Eye:Bilateral eyelids were not swelling. No ptosis. No entropion. Conjunctiva was not congestive. Sclera was anicteric. Eyeballs were not projected or depressed. Movement was normal. Bilateral pupils were round and equal in size. Direct and indirect pupillary reactions to light were existent.Mouth: Oral mucous membrane was not smooth, and there were ulcer can be seen. Tongue was in midline. Pharynx was congestive. Tonsils were not enlarged.Neck: Symmetric and of no deformities. No masses. Thyroid was not enlarged. Trachea was in midline.ChestChestwall: Veins could not be seen easily. No subcutaneous emphysema.Intercostal space was neither narrowed nor widened. No tenderness. Thorax: Symmetric bilaterally. No deformities.Breast: Symmetric bilaterally.Lungs:Respiratory movement was bilaterally symmetric with the frequency of 30/min. thoracic expansion and tactile fremitus were symmetric bilaterally. No pleural friction fremitus. Resonance was heard during percussion. No abnormal breath sound was heard. No wheezes. No rales.Heart:No bulge and no abnormal impulse or thrills in precordial area. The point of maximum impulse was in 5th left intercostal space inside of the mid clavicular line and not diffuse. No pericardial friction sound. Border of the heart was normal. Heart sounds were strong and no splitting. Rate 120/min. Cardiac rhythm was regular. No pathological murmurs. Abdomen:Flat and soft. No bulge or depression. No abdominal wall varicosis. Gastralintestinal type or peristalses were not seen. There was not tenderness and rebound tenderness on abdomen or renal region. Liver was touched 1.5cm under the right costal margin. Spleen was 0.5 cm under the left. No masses. Fluidthrill negative. Shifting dullness negative. Borhorygmus 5/min. No vascular murmurs.Extremities: No articular swelling. Free movements of all limbs.Neural system:Physiological reflexes were existent without any pathological ones.Genitourinary system: Not examed.Rectum: not exanedInvestigationBlood-Rt: Hb 59g/L RBC 1.90T/L WBC 0.8G/L PLT 55G/LBlood cytology: A few immature lymphocytes could be seen.History summary1.Patient was female, 13 years old2.Pharyngalgia and fever for four days.3.No special past history.4.Physical examination: T 39.5℃, P 120/min, R 30/min, BP 110/90mmHg Superficial lymph nodes were found enlarged in her neck, but no flare and tenderness. Liver was touched 1.5cm under the right costal margin. Spleen was 0.5 cm under the left. No other positive signs.5.investigation information:Blood-Rt: Hb 59g/L RBC 1.90T/L WBC 0.8G/L PLT 55G/LBlood cytology: A few immature lymphocytes could be seen.Impression: Fever of UnkownAcute Lymphocyte leukaemia?Signature:。
case report 写作顺序 -回复

case report 写作顺序-回复1. 引言(Introduction)- 介绍案例背景和目的(200-300字)在引言中,作者首先应该提供一个简要的案例背景,描述患者的基本信息和相关症状。
此外,还应明确指出本次案例报告的目的,即要解决的问题或要提供的新见解。
2. 患者病史(Patient History)- 描述患者的医疗史和诊断过程(200-300字)在患者病史部分,作者应详细叙述患者就诊的时间、原因和医疗过程。
包括从患者首次就诊到最终的诊断和治疗方案的过程。
也可以包括一些重要的实验室检查结果和影像学报告。
3. 临床表现(Clinical Presentation)- 描述患者的症状和体征(200-300字)在这一部分,作者详细描述患者的临床表现,包括主诉、症状和体征。
可以根据时间顺序描述患者各个阶段的变化,并与相关文献进行对比分析。
4. 诊断过程(Diagnostic Process)- 描述患者的诊断过程和结果(200-300字)在这一部分,作者详细描述医生是如何通过不同的检查和实验室结果对患者进行诊断的。
还可以包括一些相关的影像学检查和生化检查结果。
最后,作者应明确指出最终的诊断结果。
5. 治疗过程(Treatment Process)- 描述患者的治疗过程和效果(200-300字)在治疗过程部分,作者详细描述患者接受的治疗方案以及治疗结果。
可以包括手术细节(如有),使用的药物和其他治疗方法。
同时,还应提供患者的疗效评估和随访结果。
6. 病因分析(Etiology Analysis)- 分析可能的病因和相关因素(200-300字)在这一部分,作者可以根据文献资料和自身观察,分析患者病因的可能性。
可以讨论各种可能性和其依据,并提供对每种可能性的评估和论证。
7. 讨论和结论(Discussion and Conclusion)- 对案例进行分析和总结(200-300字)在讨论和结论部分,作者可以根据已有的文献资料对患者的病情进行深入的分析和讨论。
如何写casereport97-2003文档
如何写casereport97-2003文档引言临床病例报告是描述和分析诊断和/或管理1或2 患者健康的第一线证据。
care.1,2,3病例报告已使用多年作为健康科学的方法教导学生,2,4是作者学术写作的最佳开端之一,他可以成为作者和读者共同2,5,6和宝贵的学习经验,尽管病例报告很有价值但由于各种原因许多期刊不再公布了这项研究设计。
过去的在病例报告上的侵权行为终于在一些杂志上消失。
有些期刊不再公布,一般应用中实践水平低,因为案件以证据为基础的,使得有一定的病例报告固有limitations.2,8,9,10,11有些案件增加量以科学知识体系来说太少了,这是作为一个停止出版原因cases.12其他因素,包括有限的页面空间在一本杂志,往往专注于实验研究,以及身材矮小的影响情况报告对日记??的影响评价factor.13因此,这些期刊那些继续发表个案报告他们接受更多的,如果一个人渴望看到他或她的手稿宽限期1页同行评议的杂志,它需要的高品质。
使用一案的报告发表在一份杂志并没有很困难。
许多麻烦可避免通过了解必要的属性和零件的出版物案件report15值得,16 并具有一对同侪审查和理解出版过程。
本文讨论的原因写一份报告,报告的一个可写的风格,对病例报告的局限性,达到高潮的1病例报告编制一步一步的述。
会前提交检查表被列入在写作过程中提供协助。
这是我们的打算使写作过程更愉快的新和经验丰富的作家一样。
方法这篇文章是对一个先前的文件,是更新创建使用一对文献进行全面检讨通过年中2000.17因为很多人改变的案例报告,我们的要求认为这是适当的和必要的更新上次审查。
对于当前文件,我们搜查医学,护理累积索引和联合健康文学(CINAHL资料)和索引捏脊通过文学的2000年2006年9月。
搜索范围包括以下关键词:病例报告,作者,同行评审,手稿。
检索有关手稿来源进一步审查发现有关在每个环节提供的数据库和通过审查该论文的参考阅读。
英文写作 Case Report

Case ReportCase report can divided into three parts, namely, Introduction, Case History, and Discussion.1, INTRODUCTION is used to tell content, its purpose and significance. It should be as brief, and concise as possible and in present tense.Sample 1,Isolated false aneurysms of the innominate artery resulting from penetrating trauma are rare. We present one such case that was successful managed by resection and interposition grafting and emphasize the importance of arch aortography in the management of penetrating thoracic trauma.Sample 2,Malignant disease should be remembered in the differential diagnosis of common rheumtological disorders. We present a patient whose pain proved to be due to malignant disorder and not to simple trochanteric bursitis.2, CASE HISTORY consists of the patient’s gender, age, history, symptoms, tests, diagnosis as well as treatment. Details of the normal test results, the clinical process of post-operational and medication treatment should be recorded when necessary. If more cases are to be reported they should be numbered respectively “case 1”,” case 2”…2-1, General Introduction of Case History consists of the name, sex, general conditions and complaints of the patient as well as occupation and race if necessary. The real name and residential number shouldn’t be referred to. The language should be brief and in past tense.Sample 1, a 37-year-old woman with the previously uncomplicated pregnancies was seen 5 months into her third pregnancy with a two-week history of severe lower back pain.Sample 2, two women, aged 17 and 22 years, came to the accident and emergency department early in the afternoon. They described the acute on set of a diffuse rash 15 to 30 minutes after they had lunched together in a local pub.2-2 Symptoms and Clinical treatment;1), to tell about the typical symptoms, complications, diagnosis and treatment instead of other irrelevant materials.2), to tell about special examining method as well as its result.3), to tell about medication dosage; either smaller one or bigger one should be marked.4), to tell about effects of treatment: Are the symptoms relieved? Are there any complications? Are these in expectation?5), to tell about the result of treatment: Is the patient alive or dead? What are the current conditions? What treatment is the patient to be given?Sample 1 (description of symptoms), They described the acute onset of a diffuse rash 15 to 30minutes after they had lunched together in a local pub. Both felt hot and had passed two or three bowel motions. They had no respiratory symptoms and were otherwise systematically well. Neither had ever experienced an allergic reaction and the only medical history of note was that both used occasional salbutamol for mild asthma.Sample 2 (exanimation); On examination, both had diffuse erythematous rash widely spread over the face, torso and limbs. When symptoms did not resolve she was refereed to hospital where clinical examination revealed saddle anesthesia, reduced anal tone and absent ankle reflexes bilaterally.Sample 3 (treatment); They were given intravenous chlorpheniramine, hydrocortisone and fluids. After that, they were observed for a few hours and discharged when improved. Note: passive voice should be used in this description.3, DISCUSSIONTo focus on the case and to sum up the special experience and new views from the process of diagnosis and treatment. Present tense is used to show the objectivenessSample 1; Intravenous chlorpheniramine and hydrocortisone are helpful in treatment of diffuse erythematous rash.Sample 2, Many factors contribute to back pain during pregnancy.Sample 3, Diagnosis of midlife prolapse of a disc causing cauda equine compression is particularly important since a delay in surgical intervention can lead to permanent neurological deficits.Sample 4, We recommend that in pregnant and postpartum women back pain should not be looked upon merely as a normal occurrence. Detailed history and neurological examination are essential to identify the danger signs.(from “Back Pain During Pregnancy and After Childbirth: an Unusual Cause Not to Miss)。
这篇casereport终于发表了,谈下个人感受
这篇casereport终于发表了,谈下个人感受作者:sci论文发表今天终于收到了接受信,也松了口气。
这是我第一篇case report,投了4次,前三次都拒绝了,最后这个IF2.3的杂志接收了。
没什么经验,谈下感受吧:1. case report病历报告上一定要详细、全面反映你的病历,同时重点突出你的新颖独特之处,突出和其他人不同的地方。
虽然和我病历类似的报告已有2篇,但我的资料更详细,更细致,也更别致。
所以鼓起勇气写了出来。
2.讨论部分需要重点分析这个病历的特点,给人们的启示,以及重点指出和其他报告的区别。
3.写好后,要屡投屡改,屡改屡投,不要怕失败。
相信总有杂志要的,我一直这样坚信---是不是有点固执?4.不要胆怯杂志影响因子多么多么高。
我就喜欢投那些影响因子高的,反正不要投稿费。
虽然都被拒绝了,但也过了瘾。
附接受信Dear ##:The reviewers and the Editorial Team have re-evaluated your revised manuscript.We are pleased to inform you that your manuscript has been accepted for publication in ##.Manuscript ID: ##Title: A case of ##We are currently reviewing it for style and we may be in touch with you again to ask for specific information.The comments of the reviewerMoon who reviewed your manuscript are included at the foot of this letter.Thank you for your fine contribution. On behalf of the Editors of the ##, we look forward to your continued contributions to the Journal.。
case report 写作顺序 -回复
case report 写作顺序-回复中括号内的主题:Case Report写作顺序一. 引言(Introduction)在引言中,应该包括以下内容:1. 简要介绍研究背景和目的2. 引出研究中涉及的特定病例/患者3. 概述与病例相关的问题或挑战二. 疾病描述(Clinical Presentation)在这一部分,应该提供以下信息:1. 病例的基本信息,如年龄、性别和基本健康状况2. 患者的病情描述,包括主要症状、持续时间和程度3. 其他相关临床表现,如实验室检查和影像学结果三. 诊断过程(Diagnostic Workup)在这一部分,应该描述以下内容:1. 医生对患者进行的各种临床检查和实验室检查2. 各种诊断方法的结果和证据,包括影像学、实验室和生理学测试3. 与其他可能诊断进行鉴别的过程和依据四. 治疗方案(Management)在这一部分,应该包含以下信息:1. 研究中使用的治疗方法,如药物治疗、手术和其他非药物治疗2. 治疗的效果,包括患者的病情改善情况、副作用和并发症3. 如果有的话,与其他治疗方法进行比较的结果五. 结果(Outcome)在这一部分,应该描述以下内容:1. 患者的治疗结果,包括病情改善情况和复发率2. 对治疗效果的评估和效果的量化指标3. 如果有的话,与类似病例的比较结果六. 讨论(Discussion)在讨论部分,应该提供以下信息:1. 对病例的主要发现进行详细解释和分析2. 分析研究的局限性和可能的偏差3. 将研究结果与现有文献和临床实践进行比较4. 提出对进一步研究的建议七. 结论(Conclusion)在结论部分,应该总结研究结果的主要发现并提出对临床实践的意义八. 致谢(Acknowledgments)在致谢部分,应该感谢对本研究有重要贡献的人员、机构或资金来源九. 参考文献(References)在参考文献部分,应该列出所引用的文献,按照指定的引用格式排列这样一来,你的Case Report文章就有了清晰的结构和流程,并且每个部分都具有其独特的目的和要求。
SCI写作攻略(7): Case Report
SCI写作攻略(7):Case Report 当你一无所有,没有资源、没有数据、不会统计、英语很差,怎么开始你的第一篇SCI 呢?可以考虑做一个Case report(病例报道)。
作为一位医生,你可能没有时间做大样本的回顾,没有课题支持,没有经费可用,没有人手帮忙。
而且,在你有足够数量的SCI论文前,这些也绝不会有。
万事开头难。
怎样在你一无所有的时候开始你的第一篇SCI呢?作为一个中国医生,Case Report是一个很好的选择。
在我国,医生的优势就是患者量实在太大,千奇百怪的病例足够多。
只要这个病例够特别,而且你能够拿到这个病例完整的资料,那么这篇Case就可以写。
一个完整的Case Report包括以下几个部分:1. Abstract2. Introduction3. Case presentation4. Discussion5.References让我们以一个例子来说明。
这是一例关于肺腺癌患者中EGFR基因和EML-ALK基因共同突变的Case。
EGFR基因和EML-ALK基因是互斥的,极少共同突变,这个病例的特殊性,成为它可以发表的亮点。
1. Abstract六句话:第一句:关于肺癌;第二句:关于EGFR;第三句:EGFR基因与肺癌;第四句:关于EML4-ALK;第五句:EML4-ALK与肺癌;第六句:EGFR与EML4-ALK关系2. Introduction写两个部分:第一部分:逻辑上与摘要相同,只是展开一些讲,每一点用2-3句话,重点部分用4-6句话(本例就是:EGFR与EML4-ALK互斥,很少同时在同一患者肿瘤组织中发现。
同时陈述支持这一观点的几个重要文献和数据)。
第二部分:套话。
我们在这里报道EGFR与EML4-ALK同时positive的一例肺腺癌患者。
3. Case presentation这部分是文章的主体,最关键。
但却是全文最好写的部分。
为什么?因为你只需要陈述这个病例的全部情况就可以,女,45岁,因为XX入院,实验室检查发现……,手术发现……,病理提示……,免疫组化提示……而且,很多话是可以“拿来”的,好比一个填空一样,只是个别数值需要修改下就好。
Acasereport:一例报告

1www.onk.ns.ac.yu/Archive August 10, 2004Primary non-Hodgkin's lymphoma of the uterine cervix:A case reportMilica ®ivaljeviæ, Tamara Vujkov, Darjana Jovanoviæ, Aljo¹a Mandiæ, Olgica Mihajloviæ,Mladen Prvuloviæ, Bratislav StojiljkoviæABSTRACTPrimary uterine cervical non-Hodgkin's lymphomas (NHL) are rare. Limited experience dictates careful pretherapy evaluation and multidisciplinary approach in treatment planning. A 53-year-old woman pre-sented with postmenopausal bleeding and PAP smear IIIb. Cervical biopsy and endocervical curettage biopsy revealed NHL of the uterine cervix. Abdominal hysterectomy with bilateral adnexectomy was fol-lowed by pelvic lymphadenectomy due to lymph node metastasis, 21 months after the primary opera-tion. Subsequently, the patient received postoperative chemotherapy. Seven years after the onset of NHL she is alive with no evidence of disease recurrence.KEY WORDS: Cervix Neoplasms; Lymphoma, Non-HodgkinInstitute of Oncology Sremska Kamenica, Institutski put 4,21204 Sremska Kamenica, Serbia & Monetengero;Address correspondence to: Dr Milica ®ivaljeviæ, Institute of Oncology Sremska Kamenica, Institutski put 4, 21204Sremska Kamenica, Serbia & Monetengero; E-mail:*****************,Themanuscriptwasreceived:26.06.2004, Provisionally accepted: 05.07.2004, Accepted for publication: 19.07.2004©2004, Institute of Oncology Sremska Kamenica, Serbia &MontenegroCASE REPORTUDC: 618.126-006:616-006.44:616-089.8:615-085the cervix. After consulting a medical oncologist, no further therapy was planned.The patient was put on close follow-up every 3 months. She was doing well for 21 months after the operation, when gynecological examination revealed right iliac node enlargement and abdominal ultrasound showed hydronephrosis of the right kidney. MRI of the pelvis Figure1.Low-grade B cell non-HodgkinÕs lymphoma, invaded stroma of the uterine cervix under the normal squamocellular epithelium of the exocervixSeven years after the first operation the patient is doing well, without evidence of disease recurrence.DISCUSSIONMalignant NHLs of the uterine cervix are so rare, that less than 100 cases are described in the literature, with the largest data coming from 38 cases from English literature (2). Our patient presented with slight postmenopausal bleeding and abnormal PAP smear. According to the majority of authors, abnormal vaginal bleeding (54%), vaginal mass (12%) and dyspareunia (5%) are the most common clinical features (8). Abnormal cervical smear is only rarely found (9). The pathogenesis of cervical NHL is unclear and they are usually classified in the MALT-oma category (mucosa-associated lymphoiod tissue) because of relatively low malignancy, good prognosis and localized growth (2,5). Individual approach should be used in treatment decision. There are no internationally accepted recommenda-tions, due to lack of experience because of the rarity of this condition. Stroh et al., in ana-lyzing 16 cases, recommend combination of chemotherapy and irradiation (6). Chinese authors prefer combination of surgery and chemotherapy (9). Holweg et al. recommend radiation after surgical staging (10). According to our modest experience, hysterectomy with pelvic lymphadenectomy is the first step in therapy. Lymph node status dictates fur-ther chemotherapy and/or radiotherapy.CONCLUSIONMalignant NHL of the uterine cervix is a rare entity and it should be treated and followed-up by a multidisciplinary team. As a systemic disease, interdisciplinary intervention, including radical surgery, systemic chemotherapy and radiation therapy should be considered.REFERENCES1.Hempling ER in Piver MS: Cervical cancer. Handbook of Gynecologic Oncology, 2nd ed. Boston:Little, Brown and Co.; 1996. p. 103-30.2.Muntz HG, Ferry JA, Flynn D, Fuller AF, Tarraza HM. Stage IE primary malignant lymphomas ofthe uterine cervix. Cancer 1991;68(9):2023-32.3.Vang R, Medeiros LJ, Ha CS, Dearers M. Non - Hodgkin lymphomas involving the uterus: a clin-icopathologic analysis of 26 cases. Med Pathol 2000;13(1):19-28.4.Agrawal A, Ofili G, Allan TL, Mann BS: Malignant lymphoma of uterus: a case report with areview of the literature. Aust N Z J Obstet Gynacol 2000;40(3):358-60.5.el Omari-Alaoui H, Kebdani T, Benjaafar N, el Ghazi E, Erriahni H, el Gueddari BK. Non-Hodgkin'slymphoma of the uterus: apropos of 4 cases and review of the literature. Cancer Radiother 2002;6(1):39-45.6.Stroh EL, Besa PC, Cox JD, Fuller LM, Cabanillas FF. Treatment of patients with lymphomas of theuterus or cervix with combination chemotherapy and radiation therapy. Cancer 1996;75: 239 -9.7.Bollermann C, Reuter t, Weber FW, Schwenzer T. Immunoblastic highly malignant lymphoma ofthe uterine cervix. Zentralbl Gynakol,1996;118:673 - 5.8.DiSaia JPh, Creasmann TW. Invasive cervical cancer In: Clinical Gynecologic Oncology, 5th ed.St. Louis: Mosby-Year Book, Inc; 1997. p. 51-106.9.Sun M, Cao J, Zhang G. Ten case report on primary cervical lymphoma. Abstract. Chung Liu TsaChih 1997;19(3):206-8.10.Holweg M, Kopp A, Stegner HE, Loning T, Jonat W. Primary lymphoma of the cervix uteri - 2case reports. Source Geburtshilfe Frauenheilkd 1995;55:171-2.®ivaljeviæ M. et al.2www.onk.ns.ac.yu/Archive August 10, 2004Figure 2.MR tomography of pelvis. Axial section in T1w sequence before and after the application of paramagnetic contrast medium. At the level of cervix and involving fornix and ishmus, paramedianly left, an ovoid formation dia. 2 cm slightly hypertense in T1w sequence (A), moderate post contrast signal intensity (B)Figure 3.Sagittal sectin in T1w sequence. Tumor formation is relatively homogenous and well defined in relation to postcervical mass. No enlarged lymph nodes are observed。
病例报告与系列病例研究
主讲教师:周 波一、病例报告与系列病例研究(一)概念p病例报告(case report)针对临床实践中发现的单个病例或10个以下病例进行的详尽临床报告,包括临床表现(症状、体征和实验室检查结果)、治疗、治疗后的反应及结局,最后是作者对病因的分析及治疗的经验p系列病例研究(case series)与病例报告相似,但报告病例较多,多在10例以上,有时是对多年积累的病例的一种总结(二)原理p从新发现的“异常病例”中提出假设•异常病例:出现的频率和分布异常,临床表现异常、实验室检查结果异常及对治疗的反应异常等p分析出现异常的原因(三)步骤明确选题:依据临床观察和资料报道查阅相关文献,明确拟研究问题的价值阅读主要病例记录,了解主要信息的记载情况(确定信息的完整性、真实性和研究的可行性)设计简要调查表,收集病例资料描述性分析讨论病例的独特性及启示(四)特征p不需累计样本,第一时间报告p临床医生较常用,特别是基层医院的医生p用于分析某种疾病的临床表现和治疗效果p回顾性研究,不设立对照组p没有严格的设计及分析p论证强度较弱,只提供线索和参考,属于低级别证据(五)用途p发现和研究新发病例、罕见病例及药物不良反应等p只为临床研究提供线索•高度选择研究对象——偏倚•缺乏对照——局限性p仍有重要意义•例:20世纪70年代出现未明原因脑膜炎,1982年浙江医大报道了4例服用咪唑类驱虫药发生脑炎病例,使该脑炎病因研究方向正确(六)优点和缺点p优点:Ø资料容易收集,统计分析方法简单易行,易被临床医生接受Ø可充分利用临床资料Ø及时发现问题,提高医疗质量Ø为深入研究提供线索,指明方向p缺点:Ø资料缺乏完整性和标准化,可比性差Ø没有对照组Ø偏倚较大且又无法控制Ø研究结论缺乏外推性主讲教师:周 波病例报告与系列病例研究。
如何撰写和发表病例报告

如何撰写和发表病例报告病例报告(case report)是对一例或数例病案诊断处理的描述和分析,在医学刊物上发表的病例报告实际上是开始从事医学写作的最好的方法之一、病例报告可以为未来的患者诊治提供一丝线索,能从临床上帮到医生很多。
作为一种记录临床观察的方法之一,病例报告能及时提供有价值的信息,特别是关于罕见疾病的信息。
它们向医务专业人员展示了同行在类似情况下是如何行动的,从而通过分享最佳做法来帮助决策过程。
它们不仅对知识库做出了重大贡献,而且还有助于为研究人员自己的出版履历加分。
然而,写出一个好的病例报告需要的不仅仅是一个吸引人的病例。
病例报告的撰写,首先要做好题目的选择,肯定要选择与自己专业有关的临床工作,并能提出你认为是很感兴趣的,在概念上、临床上以及理论上存在的棘手问题。
那么,病例报告应该怎么写呢?今天和大家分享一些撰写和发表具有高影响力的病例报告的技巧。
如何撰写临床病例报告?万变不离其宗。
病例报告一般包括四大部分:摘要、前言、病例介绍、讨论。
DO应该这么做1.把案例报道当做故事来讲写病例报告的最好方法是讲故事。
可以按时间顺序排列事件,具体说明你的诊断考虑因素,阐明你的临床决策过程的论据,让你的读者可以跟随病例的每一个发展,并了解为什么你在治疗期间进行了特定的测试或作出一些决定的原因。
2.注意细节清楚描述导致鉴别诊断的相关症状和体征,无论是正面的还是负面的信息,以便为读者提供你做出决定的背景。
你也可以在你的病例报告中写出包括血液检测结果的实际值、处方药的详细剂量或其他应根据情况结果考虑的变量。
3.关联的情况下尽量使用图片俗话说得好,一张图片胜过千言万语,尤其是对于能够通过图像清晰有效地说明检查结果的病例报告而言。
但是,如果没有正当理由,请避免使用图片-只有当他们具备关联时才这样做。
例如,一个新鉴定的致病微生物的宏观和微观图像是必不可少的,而你在文中其他地方已经清楚地解释了模型的图片可能是过度的。
case report of XXX(英文病例汇报)

The Third Section of The Department of Gastroenterology
Present illness:
The abdominal CT,MRI and M RCP all showed the dilatation of the bile ducts(both the intrahepatic and extrahepatic bile ducts)and the pancreatic ducts. Besides,the abdominal CT showed the enlargement of pancreas with the probability of pancreatic divisum.Then he was diagnosed as pancreatitis and the sy mptomatic treatment was applie d but the effect was not comfortable.
Sex: Male
Race: Han Nationality: China
father and himself
Reliability: Reliable
Address: XinYang,Henan.
Occupation: Excavator driver
The Third Section of The Department of Gastroenterology
amination report of the duodenal wall showed he was diagnosed T lymphoma.
The Third Section of The Department of Gastroenterology
case report范文

case report范文Case Report: A Rare Presentation of Gastrointestinal Stromal TumorIntroductionGastrointestinal stromal tumors (GISTs) are mesenchymal neoplasms that arise from the interstitial cells of Cajal or their precursors. They are relatively uncommon, accounting for less than 1% of all gastrointestinal malignancies. This case report presents an unusual case of a GIST with a rare presentation and discusses its diagnosis, management, and outcome.Case PresentationA 52-year-old male presented to our hospital with a history of abdominal discomfort and weight loss over the past three months. Physical examination revealed a palpable abdominal mass in the right upper quadrant. Laboratory tests were within normal limits. Abdominal ultrasonography showed a heterogeneous mass in the liver, suggestive of a metastaticlesion. Computed tomography (CT) scan of the abdomen revealed a large mass in the right lobe of the liver with multiple smaller lesions scattered throughout both lobes. There was also evidence of peritoneal seeding.The patient underwent a laparotomy, which revealed a large, firm, and encapsulated mass in the right lobe of the liver. The mass was resected along with a segment of the liver. Intraoperatively, there was no evidence of peritoneal metastasis. Histopathological examination of the resected specimen revealed a spindle cell neoplasm with mitoses and atypical cells. Immunohistochemistry staining was positive for CD117 (c-kit) and DOG-1, confirming the diagnosis of GIST.Postoperatively, the patient recovered well and was discharged on the seventh postoperative day. He was started on imatinib mesylate (Gleevec) as adjuvant therapy. Follow-up CT scans showed no evidence of recurrence or metastasis at six months and one year post-surgery.DiscussionGISTs can occur anywhere in the gastrointestinal tract, but they are most commonly found in the stomach (60-70%) and small intestine (20-30%). They typically present as asymptomatic masses and are often diagnosed incidentally. However, symptoms can include abdominal pain, weight loss, and gastrointestinal bleeding. Metastasis is common, and the liver is the most frequent site of involvement.The diagnosis of GIST is confirmed by histopathological examination and immunohistochemistry staining. Surgical resection is the primary treatment modality for localized GISTs. The extent of resection depends on the size and location of the tumor. Adjuvant therapy with tyrosine kinase inhibitors (TKIs) such as imatinib mesylate is recommended for patients with high-risk features, including large tumor size, high mitotic rate, and/or positive resection margins.The prognosis of GISTs varies depending on tumor size, mitotic rate, resection margins, and the presence of metastasis. Long-term survival is possible with complete resection andadjuvant therapy. Regular follow-up with CT scans is recommended to monitor for recurrence or metastasis.ConclusionThis case report highlights the importance of considering GIST in the differential diagnosis of abdominal masses. Surgical resection is the mainstay of treatment, and adjuvant therapy with TKIs improves outcomes in patients with high-risk features. Regular follow-up is crucial for early detection of recurrence or metastasis.案例报告:胃肠道间质瘤罕见病例介绍胃肠道间质瘤(GIST)是起源于卡哈尔间质细胞或其前体的间叶性肿瘤。
case report 写作顺序

case report 写作顺序
(原创实用版)
目录
1.引言
2.case report 的定义和作用
3.case report 的写作顺序
4.案例分析
5.结论
6.参考文献
正文
【引言】
在医学和科研领域,case report 是一种重要的学术论文形式,主要用于描述某个特定病例的详细情况,以及对该病例的分析和研究。
case report 不仅能够为医学界提供宝贵的实践经验,还能够推动医学科学的发展。
【case report 的定义和作用】
case report,即病例报告,是医学科研论文的一种形式,主要描述某个特定病例的详细情况,包括病情、诊断、治疗和结果等。
case report 的作用主要有两点:一是为医学界提供实践经验,二是推动医学科学的发展。
【case report 的写作顺序】
case report 的写作顺序通常包括以下几个部分:引言、病例介绍、病例分析、结论和参考文献。
【案例分析】
以某个具体病例为例,详细介绍了病例的诊断、治疗和结果,并对病例进行了深入分析。
【结论】
通过对这个病例的研究,得出了什么结论,这些结论对于医学实践和科研有何意义。
【参考文献】
列出了在写作这篇 case report 时引用的所有参考资料。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
病例分析
a a.正畸治疗前牙合面观 b.植入微螺钉后 c.粘结远移磨牙装置后
b
c
2014-11-6
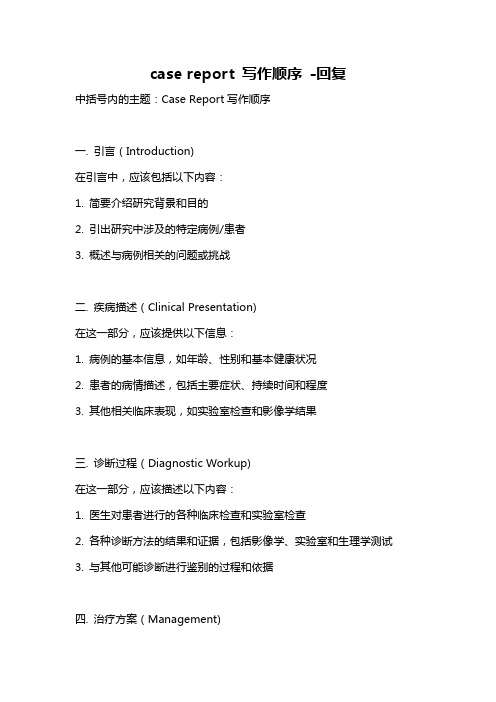
影像表现
a
b
ห้องสมุดไป่ตู้
c
a.放置微螺钉后X片 b.上颌右侧切牙根尖透射影像 c.根管治疗术后 注:箭头所示根部损害
2014-11-6
影像表现
a
b
c
a.b.c分别为3、6、10个月后的随访X片 箭头示牙骨质沉积
病例报告
上橡皮障,开髓,去髓,测工作长度,用逐步后退法由 15-40号K锉逐步根管预备,同时不断地用次氯酸钠液和 EDTA液交替冲洗,无菌纸捻干燥,氢氧化钙封入根管, 暂封。2周后,该牙无症状,窦道闭合,去除氢氧化钙, 用牙胶尖和AH-plus糊剂侧压充填根管,玻璃离子粘结剂 垫底,复合树脂修复。术后拍片随访,3和6个月后,可看到 骨修复,10个月后,根尖部有牙骨质沉积,软组织健康。 随后,患者于正畸科继续正畸治疗。
2014-11-6
总结
1.在行正畸治疗时,要注意微螺钉种植体的位置,尤 其是当种植体与根尖靠的很近的时候。 2.放置微种植体前要有详细的计划,充分考虑牙根形 态的个体差异,3DCT 的应用会有很大的帮助。 3.即便采取了必要的预防措施,根部损害也有可能发 生,在术前务必告知患者可能的风险。 4.对由微螺钉种植体损伤引起的根尖周病损,可成功 进行根管治疗。在除去种植体后,牙根和牙周膜再生 是完全可能的。
病例报告
学习要点:1.此案例阐明了在行正畸治疗时,要注意微螺钉种植体的位置, 尤其是当种植体与根尖靠的很近的时候。 2.对由微螺钉种植体损伤引起的根尖周病损成功进行了根管治疗。 关键词: 正畸微螺钉种植体,根尖周病损,根部损害
简介:支抗是指抵抗位移的解剖结构,支抗的控制是决定正畸治疗成功与否的 要素之一。然而传统的支抗控制方法中很难提供绝对稳定的支抗,支抗 不足是限制正畸治疗的重要因素。近几年,微螺钉种植体逐渐广泛用于 临床,因为它尺寸小,操作简单,植入部位灵活。但其局限性在于有损 伤邻接牙齿牙根的危险,即使采取预防性的措施,比如术前拍根尖周 X片 根部损伤也可发生。它的植入对牙髓的损伤会带来不可逆的作用,往往 需要进行牙髓治疗或者将患牙拔出。
References
Bae SM, Kyung HM (2006) Mandibular molar intrusion with miniscrew anchorage. Journal of Clinical Orthodontics 40, 107–8. Brisceno CE, Rossouw PE, Carrillo R, Spears R, Buschang PH (2009) Healing of the roots and surrounding structures after intentional damage with miniscrew implants. American Journal ofOrthodontics and Dentofacial Orthopedics 135, 292–301. Chen F, Terada K, Hanada K, Saito I (2006) Anchorage effect of osseointegrated vs nonosseointegratedpalatal implants. Angle Orthodontist 76, 660–5. Costa A, Raffainl M, Melsen B (1998) Miniscrews as orthodontic anchorage: a preliminary report.International Journal of Adult Orthodontics and Orthognathic Surgery 13, 201–9.Deguchi T, Nasu M, Murakami K, Yabuuchi T, Kamioka H, Takano-Yamamoto T (2006) Quantitative evaluation of cortical bone thickness with computed tomographic scanning for orthodontic implants.American Journal of Orthodontics and Dentofacial Orthopedics 129, e7–12. Gelgo¨ r IE, Karaman AI, Bu¨ yu¨ kyılmaz T (2007) Comparison of 2 distalization syste supported by intraosseous screws. American Journal of Orthodontics and Dentofacial Orthopedics 131, e1–8. Hembree M, Buschang PH, Carrillo R, Spears R, Rossouw PE (2009) Effects of intentiona damage of the roots and surrounding structures with miniscrew implants. American Journa of Orthodontics and Dentofacial Orthopedics 135, e1–9.
摘要:患者女,22岁,诊断为骨性II类2分类错颌畸形,伴有 双侧II类磨牙及尖牙关系。治疗计划是推双侧上颌第一磨牙向 远中,随后固定矫治器治疗。为了推磨牙向远中,设计应用了 微螺钉种植体支抗系统。两个月后,患者来诊,诉上颌右侧侧 切牙区疼痛。口内检查见上颌右侧颊沟和腭部有窦道,X光下 见右上颌侧切牙根部周围有界限清楚的大的透射性损害。 随后对该牙行根管治疗,用牙胶尖和AH-plus糊剂侧向加压充填, 最后用复合树脂修复。10个月之后复诊,牙齿无症状,影像学显 示损害修复,无需再行后续治疗。
病例报告
患者,女,22岁,主诉上前牙舌倾、不齐,伴深覆合。 诊断为骨性II类2分类错颌畸形,伴双侧II类磨牙及尖牙关系。 治疗计划是推双侧上颌第一磨牙向远中,随后固定矫治器治疗。 在此应用了微螺钉种植体支抗系统,在侧切牙和尖牙之间双侧 植入了直径1.5mm,长10mm的微螺钉种植体,与腭中缝保持 有安全距离。嘱患者每隔四周复诊,2个月后,患者来诊, 诉上颌右侧侧切牙区疼痛。口内检查见上颌右侧颊沟和腭部有窦道, 遂决定将矫治器连同右侧的微螺钉一起拆除,经详细检查,X光下 见上颌右侧切牙根部周围有界限清楚的大的透射性损害。右上侧切 牙叩(—),冷(—),电测(—),I度松动,诊断为慢性根尖脓肿 遂行根管治疗术。
多彩的世界
Embrace the world
子夜
K. Er, M. Bayram& T. Tas¸ demir
---International Endodontic Journal
题目
对因放置正畸微螺钉种植体意外损伤 根部引起的根尖周病损的根管治疗 ----病例报告
病例报告
目的:展示对一颗上颌侧切牙成功进行牙髓治疗,此牙因 放置正畸微螺钉种植体意外损伤根部而引起了根尖周病变。
病例报告
PPT
YUN
Case Report
Root canal treatment of a periradicular lesion caused by unintentional root damage after orthodontic miniscrew placement: a case report