case-report写作PPT课件
CaseReport病例报告的书写
2021/4/13
实用文档
15
1. …were/appeared/showed/revealed (ab)normal/ , (but…)
·The right renal artery and branch arteries appeared normal without evidence of occlusion or stenosis from intrinsic vascular disease.
condition is rare, no standard
treatment regimen has been
estab实lis用h文e档d …”
8
After the problem is described, many authors close the introduction section by describing in one sentence the patient who represents the case.
“ This case report describes
clinical characteristics of a 67-year old man with small carcinoma of the prostate.”
This creates a smooth
transition to the next section,
The introduction is a brief overview of the larger problem addressed by the case. The overlying message of the section is, “ X is important to understand because…” For example:
case report 写作顺序 -回复
case report 写作顺序-回复中括号内的主题:Case Report写作顺序一. 引言(Introduction)在引言中,应该包括以下内容:1. 简要介绍研究背景和目的2. 引出研究中涉及的特定病例/患者3. 概述与病例相关的问题或挑战二. 疾病描述(Clinical Presentation)在这一部分,应该提供以下信息:1. 病例的基本信息,如年龄、性别和基本健康状况2. 患者的病情描述,包括主要症状、持续时间和程度3. 其他相关临床表现,如实验室检查和影像学结果三. 诊断过程(Diagnostic Workup)在这一部分,应该描述以下内容:1. 医生对患者进行的各种临床检查和实验室检查2. 各种诊断方法的结果和证据,包括影像学、实验室和生理学测试3. 与其他可能诊断进行鉴别的过程和依据四. 治疗方案(Management)在这一部分,应该包含以下信息:1. 研究中使用的治疗方法,如药物治疗、手术和其他非药物治疗2. 治疗的效果,包括患者的病情改善情况、副作用和并发症3. 如果有的话,与其他治疗方法进行比较的结果五. 结果(Outcome)在这一部分,应该描述以下内容:1. 患者的治疗结果,包括病情改善情况和复发率2. 对治疗效果的评估和效果的量化指标3. 如果有的话,与类似病例的比较结果六. 讨论(Discussion)在讨论部分,应该提供以下信息:1. 对病例的主要发现进行详细解释和分析2. 分析研究的局限性和可能的偏差3. 将研究结果与现有文献和临床实践进行比较4. 提出对进一步研究的建议七. 结论(Conclusion)在结论部分,应该总结研究结果的主要发现并提出对临床实践的意义八. 致谢(Acknowledgments)在致谢部分,应该感谢对本研究有重要贡献的人员、机构或资金来源九. 参考文献(References)在参考文献部分,应该列出所引用的文献,按照指定的引用格式排列这样一来,你的Case Report文章就有了清晰的结构和流程,并且每个部分都具有其独特的目的和要求。
casereports:病例报告

Life-threatening hypokalaemia from abuseof Nurofen PlusA Paul Lambert PhD Colin Close MDJ R Soc Med2005;98:21Non-steroidal anti-inflammatory drugs are widely available as over-the-counter preparations.Adverse effects of these drugs include nephrotoxicity.1CASE HISTORYA woman aged45came to hospital in a drowsy state,with headache.For three months her mood had been low and she had been prescribedfluoxetine20mg/day.She was thin (body mass index17kg/m2)and normotensive.Investi-gations revealed a serum potassium of 2.6mmol/L (reference range 3.5–5.0)and a serum creatinine of 56m mol/L(60–120).She recovered spontaneously,but at discharge48hours later her potassium concentration had fallen to2.8mmol/L.Six months before,serum potassium had been4.5mmol/L.She had two further admissions in the next six weeks with drowsiness and general weakness, on each occasion with profound hypokalaemia(potassium 2.0and1.7mmol/L,respectively).On the third admission, further investigation revealed an arterial pH of7.4(7.35–7.45)with pCO24.0kPa(4.5–6.1),serum bicarbonate 19mmol/L(24–32)and chloride110mmol/L(96–105) (anion gap18mmol/L).She had a normal serum magnesium,0.9mmol/L(0.7–1.0).Urine pH was7.0 and24h urine potassium excretion was120mmol,giving a transtubular potassium gradient of7.3mmol/L.Renal tubular acidosis with renal potassium wasting was diagnosed and she was treated with oral sodium bicarbonate6g/day and oral potassium2.8g(72mmol)per day.Potassium rose to4.3mmol/L and bicarbonate to29mmol/L.A urine drug screen was positive for ibuprofen, paracetamol,opioids and benzodiazepines,and she was subsequently readmitted after self-poisoning with Nurofen Plus(ibuprofen600mg,codeine phosphate12.8mg; Crookes Healthcare Ltd,Nottingham,UK).From another source we learned that herflat was littered with empty Nurofen Plus packets,and she later described regularly consuming28g/day of MENTAcute renal failure and interstitial nephritis are well documented adverse effects of non-steroidal anti-inflamma-tory drugs.However,we have found only two reports ofeffects of these drugs on renal tubular acidification.In both, overdose of ibuprofen was reported as causing type2 proximal renal tubular acidosis.2,3We believe this is an important issue to raise,because in the present case and thatof Chetty et al.3the ibuprofen was an over-the-counter preparation.Abuse of such agents can easily escape notice.Acknowledgment We thank Dr RE Ferner(West MidlandsCentre for Adverse Drug Reporting,City Hospital, Birmingham B187QH,UK)for his help in the preparationof this report.REFERENCES1British Medical Association,Royal Pharmaceutical Society of Great Britain.British National Formulary.London:BMA/RPS,2003:479–812Gaul C,Heckmann JG,Druschky A,Schocklmann H,Naundorfer I, Erbguth F.Renal tubular acidosis with severe hypokalemic tetraparesisafter ibuprofen intake.Dtsch Med Wochenschr1999;124:483–63Chetty R,Baoku Y,Mildner R,Banerjee A,Vallance D,Haddon A, Labib M.Severe hypokalemia and weakness due to Nurofen1misuse.Ann Clin Biochem2003;40:422–3Myocardial infarction afteraspirin treatmentDavid J Fox MB MRCP Timothy P Gray MB MRCPFarzin Fath-Ordoubadi MD MRCPJ R Soc Med2005;98:21–23Aspirin has been reported to cause coronary spasm as wellas bronchospasm,but never acute myocardial infarction.CASE HISTORYA woman of55attended the emergency department aftersix hours of left-sided chest pain.She was a smoker. Previously she had beenfit and well apart from mild asthma.There was no history of illicit drug use.She didreport an‘allergy’to aspirin but was vague about how this showed itself.On examination she was haemodynamicallystable and the onlyfinding of note was mild expiratoryCASEREPORTS21J O U R N A L O F T H E R O Y A L S O C I E T Y O F M E D I C I N E V o l u m e98J a n u a r y2005Division of Medicine,Taunton and Somerset Hospital,Musgrove Park,Taunton TA15DA,UKCorrespondence to:Dr Paul LambertE-mail:********************.uk Manchester Heart Centre,Manchester Royal Infirmary,Oxford Road, Manchester M139WL,UKCorrespondence to:Dr David FoxE-mail:**********************by guest on February 14, 2016 Downloaded fromwheeze.Baseline investigations including oxygen saturations and cardiac enzymes gave normal results;cholesterol was 4.8mmol/L.Serial12-lead electrocardiograms showed sinus rhythm and no evidence of ischaemia.She was initially managed with oxygen and sublingual glyceryl trinitrate,and when this made no difference to her pain she was given intravenous diamorphine.After10–15 minutes her symptoms had improved but as a precautionary measure the emergency team decided to administer300mg aspirin.In the next20minutes aflorid urticarial rash developed over the patient’s entire body surface,she became breathless and she reported central crushing chest pain.The electrocardiogram now showed inferior ST segment elevation of up to7mm with associated complete heart block and she was transferred for coronary angiography.Premedication was200mg intravenous hydrocortisone and10mg chlorphenamine.Gross vaso-spasm was seen in the left and the right coronary arteries, particularly near the ostium of the right coronary artery (Figure1).This abated with intracoronary nitrate injections and at the end of the procedure all the arteries appeared normal(Figure2).Intravascular ultrasound examination of the left and right coronary artery revealed no evidence of atheromatous plaque.She settled on nitrate and calcium channel blocker therapy but measurements of troponin T (0.22m mol/L)and creatine kinase1337u/L twelve hours after the procedure indicated myocardial damage.On echocardiography,inferior hypokinesia was consistent with infarction in the right coronary artery territory.She recovered without incident and was discharged afterfive days taking the antiplatelet agent clopidogrel.While she was in hospital,relatives provided some information about her aspirin allergy:she had developed a serious rash and been very unwell after taking aspirin in the past.COMMENTWe postulate that the coronary vasospasm and infarction resulted from the aspirin administration.After aspirin,her atypical pain changed to a typical crushing cardiac chest pain,and ischaemic changes developed on the electro-cardiogram.Possible mechanisms are coronary artery smooth muscle spasm1or massive catecholamine release as part of a stress response to the adverse drug reaction. Aspirin-induced coronary vasospasm has been reported previously,leading to exercise induced angina.2Also, variant angina has been suggested to be aggravated by aspirin.3In our patient the pain on admission was probably musculoskeletal;there was no evidence of cardiac ischaemia at that time.There is only one previous report of coronary spasm related to asthma4,and in this the authors suggest a link between bronchospasm and coronary spasm caused by aspirin.With cocaine,spasm leading to myocardial infarction is well recognized5but we have found no recorded case of aspirin inducing spasm severe enough to cause infarction.Patients who are suspected of having ischaemic chest pain and who report allergy to aspirin should be given an alternative antiplatelet agent such as clopidogrel.REFERENCES1Ramanuja S,Breall JA,Kalaria VG.Approach to‘aspirin allergy’in cardiovascular patients.Circulation2004;110:e1–e42Miwa K,Kambara H,Kawai C.Exercise-induced angina provoked by aspirin administration in patients with variant angina.Am J Cardiol 1981;47:1210–1422J O U R N A L O F T H E R O Y A L S O C I E T Y O F M E D I C I N E V o l u m e98J a n u a r y2005 Figure1Proximal spasm in right coronaryarteryFigure2Right coronary artery after intracoronary nitrateby guest on February 14, 2016Downloaded from3Miwa K,Kambara H,Kawai C.Variant angina aggravated by aspirin.Lancet1979;2:13824Habbab MA,Szwed SA,Haft JI.Is coronary arterial spasm part of the aspirin-induced asthma syndrome?Chest1986;90:141–35Kontos MC,Jesse RL,Tatum JL,Ornato JP.Coronary angiographic findings in patients with cocaine-induced chest pain.J Emerg Med 2003;24:9–13Splenomegaly,anaemia and pleural effusionP Kojodjojo MRCP S Chew BScK Wakeham BSc MRCP R Lancaster FRCPJ R Soc Med2005;98:23–24Most pseudocysts of the spleen cause no symptoms,but occasionally they lead to disaster.CASE HISTORYA man of71was admitted after syncope.He was on treatment for hypertension,atenolol25mg daily,with good control.Recently he had lost a few kilograms but had otherwise beenfit and well.He had not travelled abroad for many years and was teetotal.His blood pressure was133/76mmHg without postural drop,pulse78/min.On chest examination there was a small area of stony dullness at the left base,consistent with a small pleural effusion;the abdomen was distended and a very large spleen could be felt.Investigations revealed a normochromic normocytic anaemia(haemoglobin10.3g/ dL),white cell count13.76109/L(81%neutrophils,17% lymphocytes)and platelets3076109/L.Liver function tests,corrected calcium and clotting profile were normal. Blunting of the left costophrenic angle was seen on a chest radiograph,in keeping with the positive respiratory findings.Further investigations were requested including serum electrophoresis,hepatic screen,abdominal imaging and bone marrow studies.Several hours later the patient experienced presyncope on the ward and blood pressure declined to97/62mmHg, pulse74/min.Clinically,the left-sided pleural effusion was larger and the haemoglobin was now8.1g/dL.The abdomen remained non-tender and the size of the spleen had not obviously changed.A diagnostic pleural tap drew a small amount of dark blood.Central venous and urinary catheters,along with an arterial line,were inserted to monitor his haemodynamic status more closely.CT showeda large effusion almost completelyfilling the left hemithorax,associated with complete left lung collapseand mediastinal shift(Figure1).The spleen was massively enlarged,measuring23623617cm—a cyst with only athin rim of splenic tissue(Figure2).No rib fractures,otherbony injuries or lymphadenopathy were seen.His blood pressure responded to blood and colloid transfusions,but before he could be transferred for exploratory thoracolaparotomy he had a cardiac arrest.After restoration of the pulse andfluid administration, insertion of an intercostal drain yielded3L of dark altered blood.At operation he was found to have a splenothoracicfistula.There was no blood in the peritoneal cavity.The spleen was removed and the left diaphragm was repaired.23J O U R N A L O F T H E R O Y A L S O C I E T Y O F M E D I C I N E V o l u m e98J a n u a r y2005Department of General Medicine,St Mary’s Hospital,London W21NY,UK Correspondence to:Pipin Kojodjojo,Waller Department of Cardiology,St Mary’s Hospital,Praed Street,London W21NY,UKE-mail:***************************.ukFigure1CT of chest showing large left pleural effusion aroundthe collapsed lung(black arrow)with associated mediastinalshiftFigure2CT of abdomen showing thin rim of splenic tissueencasing cystby guest on February 14, 2016Downloaded fromBelow is given annual work summary, do not need friends can download after editor deleted Welcome to visit againXXXX annual work summaryDear every leader, colleagues:Look back end of XXXX, XXXX years of work, have the joy of success in your work, have a collaboration with colleagues, working hard, also have disappointed when encountered difficulties and setbacks. Imperceptible in tense and orderly to be over a year, a year, under the loving care and guidance of the leadership of the company, under the support and help of colleagues, through their own efforts, various aspects have made certain progress, better to complete the job. For better work, sum up experience and lessons, will now work a brief summary.To continuously strengthen learning, improve their comprehensive quality. With good comprehensive quality is the precondition of completes the labor of duty and conditions. A year always put learning in the important position, trying to improve their comprehensive quality. Continuous learning professional skills, learn from surrounding colleagues with rich work experience, equip themselves with knowledge, the expanded aspect of knowledge, efforts to improve their comprehensive quality.The second Do best, strictly perform their responsibilities. Set up the company, to maximize the customer to the satisfaction of the company's products, do a good job in technical services and product promotion to the company. And collected on the properties of the products of the company, in order to make improvement in time, make the products better meet the using demand of the scene.Three to learn to be good at communication, coordinating assistance. On‐site technical service personnel should not only have strong professional technology, should also have good communication ability, a lot of a product due to improper operation to appear problem, but often not customers reflect the quality of no, so this time we need to find out the crux, and customer communication, standardized operation, to avoid customer's mistrust of the products and even the damage of the company's image. Some experiences in the past work, mentality is very important in the work, work to have passion, keep the smile of sunshine, can close the distance between people, easy to communicate with the customer. Do better in the daily work to communicate with customers and achieve customer satisfaction, excellent technical service every time, on behalf of the customer on our products much a understanding and trust.Fourth, we need to continue to learn professional knowledge, do practical grasp skilled operation. Over the past year, through continuous learning and fumble, studied the gas generation, collection and methods, gradually familiar with and master the company introduced the working principle, operation method of gas machine. With the help of the department leaders and colleagues, familiar with and master the launch of the division principle, debugging method of the control system, and to wuhan Chen Guchong garbage power plant of gas machine control system transformation, learn to debug, accumulated some experience. All in all, over the past year, did some work, have also made some achievements, but the results can only represent the past, there are some problems to work, can't meet the higher requirements. In the future work, I must develop the oneself advantage, lack of correct, foster strengths and circumvent weaknesses, for greater achievements. Looking forward to XXXX years of work, I'll be more efforts, constant progress in their jobs, make greater achievements. Every year I have progress, the growth of believe will get greater returns, I will my biggest contribution to the development of the company, believe inyourself do better next year!I wish you all work study progress in the year to come.。
病例汇报ppt模板

病例介绍
病例汇报P
ቤተ መጻሕፍቲ ባይዱ
性别:男
经过充分的讨论和评估,制定了以下治疗方案
病例编号:XXXXXXXXXX
患者姓名:XXX
治疗方法:XXX
用药方案:XXX
康复计划:XXX
实施上述治疗方案后,患者症状得到了明显的改善,实验室和影像学检查结果也显示病情好转。目前,患者已顺利出院,继续接受后续治疗。
04
治疗方法及过程
2. 实验室检查结果反映了患者当前身体状况,对于疾病诊断、治疗和预后评估具有重要意义。
3. 实验室检查结果对治疗方案的选择具有重要影响,医生会根据检查结果制定相应的治疗方案,确保患者得到及时、有效的治疗。
4. 实验室检查在诊断、治疗和预后评估中具有重要作用,通过检测各项指标,为医生提供准确的诊断依据,制定合理的治疗方案,并评估疾病的预后情况。
7. 并发症名称:急性心肌梗死
8. 并发症发生时间:患者入院后第5天
9. 并发症症状:胸痛、胸闷、心悸等
10. 并发症治疗:进行紧急PCI手术,植入支架一枚。
11. 治疗效果:患者急性心肌梗死得到有效治疗,生命体征稳定。
12. 预后:患者需要继续进行药物治疗和生活方式干预,以控制血压、血糖和血脂,预防再次发生并发症。同时,患者需要定期进行心电图、超声心动图等检查,以监测心脏功能。
病例汇报
XXX,35岁男性办公室职员,2023年3月1日确诊COVID-19感染,症状包括咳嗽、发热、喉咙疼痛、乏力、肌肉疼痛、头痛、流鼻涕等。经药物治疗(如口服莲花清瘟胶囊、对乙酰氨基酚等)和护理措施(如隔离、休息、饮水、补充营养等),病情好转,核酸检测转阴,康复出院。该病例提示COVID-19可发生于各个年龄段和人群,预防措施至关重要,包括戴口罩、勤洗手、少聚集、保持社交距离等。
胸外科casereport ln
Imaging diagnosis
❖ The chest CT scan shows the basal segment bronchial obstruction and a mass high density shadow, about 3.2cm in diameter and some burr on the edge of the lower lobe of right lung.
Other
❖ Personal history, marital history and family history : No special
❖ Physical examination was normal.
The chest CT 2017.10.17
The chest CT 2017.10.17
胸外科casereport ppt课件
Name:guangbo sun Age: 61 years old Sex:male Chief complaint:chest pain for 15 days
History of present illness
Past history
He have underwent Interventional surgery of left coronary artery at our hospital in 2015, now oral aspirin intestinal solution 100milligram qd , atorvastatin 20milligram qd , metopolol 25milligram qd.
Other Supplementary Examination
❖ Pulmonary function test showed(2017ory volume in one second(FEV1):2.85L
case report of XXX(英文病例汇报)PPT参考幻灯片
Marital status: Unmarried Date of admission: Nov 11th, 2015 Date of record: 8Pm, Nov 11th, 2015 Complainer of history: patient’s father and himself Reliability: Reliable
15
Present illness:
The endoscopic examination showed he had duodenal ulcers and reflux esophagitis.And the pathological report of the ulcers was chronic inflammation with proliferation of lymphocytes.Then the Rabeprazole which had show a curative effect was given to him.
12
Chief complaint: Reduplicated nausea and vomit for six and a half months.
13
Present illness:
The patient felt sudden nausea and vomited the food he took in with no recognizable cause about six and a half months ago. He didn’t pay attention to it and thought he had ate something wrong.
17
Present illness:
case_report_of_某(英文病例汇报)
The Third Section of The Department of Gastroenterology
Present illness:
The endoscopic examination showed he had duodenal ulcers and reflux esophagitis.And the pathological report of the ulcers was chronic inflammation with proliferation of lymphocytes.Then the Rabeprazole which had show a curative effect was given to him.
Present illness:
The patient felt sudden nausea and vomited the food he took in with no recognizable cause about six and a half months ago. He didn’t pay attention to it and thought he had ate something wrong.
The Third Section of The Department of Gastroenterology
Chief complaint: Reduplicated nausea and vomit for six and a half months.
The Third Section of The Department of Gastroenterology
Case report
The Third Ward of The Department of GastroenterologyCompany
case report
Case ReportSubacute delayed ascending myelopathy after low spine injury:case report and evidence of a vascular mechanismBJ Schmidt1,*1Section of Neurology,Departments of Internal Medicine and Physiology,Faculty of Medicine,University of Manitoba, Winnipeg,MB,CanadaStudy design:Case report of a patient with subacute delayed myelopathy after an acute lowthoracic spine injury.Objectives:To draw awareness to a rarely described complication with potential to adddevastating neurological insult to the original spinal cord injury,and to discuss evidencesupporting a vascular mechanism.Setting:Health Science Centre,Winnipeg,Manitoba,Canada.Case report:A35-year-old woman developed clinical and MRI evidence of ascendingmyelopathy,extending up to C5,16days after a T11/12fracture dislocation.The distribution ofMRI signal abnormality,MRI evidence of prominent venous markings,and association withupright mobilization and the wearing of a thoraco-lumbo-sacral orthosis,suggest that elevatedspinal venous pressure in conjunction with low arterial pressure may have induced impairedspinal cord vascular perfusion.Conclusion:After recent spinal cord injury,factors exacerbating spinal venous hypertensionand/or arterial hypotension may in some patients lead to impaired spinal cord perfusion.Thesefactors should be considered and corrected if symptoms or signs of progressive myelopathyemerge in thefirst few days or weeks after injury.Spinal Cord advance online publication,20September2005;doi:10.1038/sj.sc.3101801Keywords:ascending myelopathy;post-traumatic;spinal cord ischemia;venousIntroductionSeveral types of neurological deterioration,not directly attributable to ongoing mechanical instability of the spine,may occur after acute spinal cord injury.During thefirst few hours and days,neurological deterioration may result from edema and other secondary changes involving one or two spinal cord segments adjacent to the original site of trauma.After a period of neurological stability,late delayed complications,such as progressive post-traumatic cystic myelopathy(syr-ingomyelia)1–3or progressive post-traumatic myeloma-lacic myelopathy,4,5may produce new ascending neurological symptoms months,years,or even decades after the original injury.In addition to acute phase progression and late delayed syndromes,myelopathic deterioration may present during thefirst few weeks after spinal cord injury.Although several mechanisms have been postu-lated,the exact cause of subacute delayed post-traumatic myelopathy is unknown.Case reportA35-year-old woman suffered a hyperflexion injury of the lower thoracic spine resulting in complete loss of sensation and voluntary movement below T11.On admission,the cervical spine was cleared and she had no neck puterized axial tomography(CT) demonstrated a fracture-dislocation;the T11vertebral body was displaced anteriorly by50%on the T12 vertebral body,resulting in marked stenosis of the central canal and severe spinal cord compression (Figure1).She was treated with intravenous methyl-prednisilone30mg/kg bolus followed by5.4mg/kg/h for 23h.At4days after admission,she underwent open reduction and internalfixation from T9to L1,without complication,and was started on low molecular weight heparin,5000units daily.On postinjury day14,she began to wear a thoraco-lumbo-sacral orthosis(TLSO)and sit at451for brief periods,during which time she experienced light-head-edness.Her routine daily blood pressures,recorded in the supine position,ranged from92/48to106/60mmHg. During postinjury days16and17,the level of numbness ascended,insidiously,to her mid chest.She also*Correspondence:BJ Schmidt,Section of Neurology,Health Sciences Centre,820Sherbrook St,Winnipeg,MB,Canada R3A1R9Spinal Cord(2005),1–4&2005International Spinal Cord Society All rights reserved1362-4393/05$30.00 /screported pain in the back,chest,and low-neck regions.Neurological examination confirmed that the sensory level had risen to the T5level by postinjury day 17.A magnetic resonance imaging (MRI)study of the cervical and thoracic spine on postinjury day 18showed increased T2-weighted signal from C5to T9(Figure 2a;artefact from spinal instrumentation obscured visualiza-tion of cord segments caudal to T9).The abnormal signal,and cord swelling,was most intense in the lower cervical and upper thoracic segments.Axial sections demonstrated that the signal abnormality was located in the posterior cord region (Figure 2b and c).There was no gadolinium enhancement.Prominent vascular mark-ings were noted in the thecal sac in the thoracic region (Figure 3),suggesting elevated venous pressure.Thor-acic and abdominal aortograms,as well as selective injections of the spinal arteries from T8to L2showed no evidence of thrombosis,vascular anomaly,or dural arteriovenous fistula to account for evidence of dis-tended vascular markings noted on MRI.Plain radio-graphs of the thoracolumbar spine showed no change in the spine alignment or position of the fixation hardware.An MRI of the brain,chest radiograph,lung scan,abdominal CT and sonogram,and duplex venous sonogram of both legs were normal.Blood tests included a normal complete blood cell count,INR,PTT,sedimentation rate,C-reactive protein,antipho-spholipid antibody screen,and antinuclear antibody screen.Pain subsided over several days without specific treatment.Repeat MRI of the cervical and thoracic spine on postinjury day 22showed substantial decrease of the T2-weighted signal abnormality.By 7months postinjury,MRI of the cervical cord was normal,however,marked atrophy of the thoracic cord caudal to T5was noted;clinically a T5sensory level persisted.DiscussionDelayed neurological deterioration during the first month after lower spinal cord injury has been rarely reported.In 1969,Frankel described eight patients with post-traumatic ascending myelopathy starting 2–11days after injury and progressing for 2–12days.6They all had fractures of the lower thoracic spine,except one patient with a T5fracture.More recently,Belanger et al ,7reported ascending neurological deficit in three patients with spine injuries,starting 7–13days after injury.7Similar to the present patient,one of their cases hadaFigure 1CT sagittal reconstruction of the spine showing a fracture dislocation.The T11vertebral body is displaced anteriorly by approximately 50%on the T12vertebralbodyFigure 2MRI of the spinal cord on postinjury day 18.(a )T2-weighted sequence shows increased signal and swelling in the cervical and upper thoracic spinal cord.(b )Axial T2-weighted image shows increased signal in the central and posterior cord region.(c )T1-weighted image shows decreased signal in the central and posterior cordregionSubacute delayed ascending myelopathyBJ Schmidt2Spinal Cordlow spinal injury (L1level)and showed increased T2-weighted MRI signal in the central cord region extending to the mid cervical level.Also,very similar to the present patient,is the 30-year-old woman with a fracture dislocation at T11/12described by Aito et al.8Low baseline blood pressures were noted in their patient,and on postinjury day 12,she developed scapular pain and paresthesia in the upper limbs whenever she sat upright for physiotherapy.Two days later her sensory level ascended to the T3level and an MRI showed increased T2-weighted signal between C3and T1.Visocchi et al 9reported two patients with post-traumatic ‘descending’myelopathy,which they attrib-uted to spinal venous thrombosis in one patient and anterior spinal artery occlusion (secondary to disk herniation)in the other patient.Unlike the distinctly rare occurrence of subacute delayed myelopathy after low spinal injury,early delayed deterioration is noted more frequently (6–10%)in patients with acute cervical spine trauma.10,11In the series by Harrop et al ,10approximately half of the patients who deteriorated developed new symptoms within the first 24h of injury,in association with halo vest placement or cervical spine traction immobilization.Most of the other patients deteriorate 1–7days after cervical trauma;the mechanism was unknown but the authors suggested the possibility of cord ischemia secondary to sustained hypotension and/or venous insufficiency.To date,most patients with lower spine trauma and delayed ascending myelopathy,including our patient,were injured near the thoraco-lumbar junction.This part of the spine corresponds to the region most frequently entered by the Great Artery of Adamkiewicz (GAA),the largest single medullary artery supplying the spinal cord.12Thus,post-traumatic thrombus of the GAA was considered by Aito et al ,8among other etiologies,as a possible cause of early delayed ascending myelopathy.However,a spinal angiogram was not performed on their patient.Angiographic study of the present patient,as well as the patient with an L1injury reported by Belanger et al ,7showed no evidence of thrombus in the GAA.Impaired venous drainage of the cord after injury may contribute to early delayed myelopathy.8,10After spinal cord injury,68%of patients demonstrate reversal of the normal hemodynamic gradient which in healthy subjects causes blood to flow from the paravertebral venous plexus to the inferior vena cava.13The gradient reversal is thought to be due to increased vena caval pressure which,in turn,produces retrograde elevation of pressure and decreased venous flow in the valveless paravertebral system.13Although variable in distribution,venous stasis and infarction involves predominantly central and posterior cord regions in autopsied cases.14,15Lesions produced by experimental occlusion of the dorsal spinal vein of the rat 16and monkey 17are confined to the posterior columns.These observations,in conjunction with the central posterior cord distribution of MRI signal abnormality in the present patient and the presence of distended venous markings in the thecal sac,suggests that elevated venous pressures causing venous stasis and ischemia,may have contributed to the subacute delayed myelopathy.However,if increased spinal venous pressure and stasis is relatively common among patients with spinal cord injury,13why is early delayed myelopathy only rarely reported?Other factors must be important.One consideration is the effect of mobilization after injury.The present patient,and the patient described by Aito et al ,8developed symptoms when they began to sit upright.Increased intraabdominal pressure associated with sitting,and wearing a TLSO,may further impair venous return from the paravertebral plexus.Sitting may also induce an orthostatic drop in blood pressure,including spinal arterial pressure,especially in patients with spinal cord patible with this mechan-ism,Cybulski,and D’Angelo described four patients who underwent laminectomy for nontraumatic cervical spondylosis and postoperatively developed myelopathy in association with hypotensive episodes (50–60mmHg systolic)evoked while attempting to sit.18The combination of decreased spinal arterial pressure and increased spinal venous pressure,potentially ag-gravated by sitting and the use of a TLSO,may impair cord perfusion sufficient to produce an ischemic insult.Consistent with this hypothesis,a combination of decreased spinal arterial pressure (secondary to transient moderate hypotension)and elevated vertebralvenousFigure 3MRI of the spinal cord on postinjury day 18shows prominent vascular markings in the thecalsacSubacute delayed ascending myelopathy BJ Schmidt3Spinal Cordpressure (associated prone positioning and use of chest rolls)was previously proposed as the cause of transient cervical myelopathy in four patients who underwent elective laminectomy for myeloradiculopathy.19In conclusion,the observations suggest that factors exacerbating spinal venous hypertension and/or arterial hypotension may in some instances lead to impaired spinal cord perfusion.These factors should be promptly considered and corrected if symptoms or signs of progressive myelopathy emerge during the first few days or weeks after spinal cord injury.References1Quencer RM,Green BA,Eismont FJ.Post-traumatic spinal cord cysts:clinical features and characterization with metrizamide computed tomography.Radiology 1983;146:415–423.2Rossier AB et al.Posttraumatic cervical syringomyelia.Brain 1985;108:439–461.3Vernon JD,Silver JR,Ohry A.Post-traumatic syringo-myelia.Paraplegia 1982;20:339–354.4Falcone S et al.Progressive posttraumatic myelomalacic myelopathy:Imaging and clinical features.Am J Neuror-adiol 1994;15:747–754.5Gebarski SS et al.Posttraumatic progressive myelopathy.Radiology 1985;157:379–385.6Frankel HL.Ascending cord lesions in the early stages following spinal injury.Paraplegia 1969;7:111–118.7Belanger E et al.Subacute posttraumatic ascending myelopathy after spinal cord injury.J Neurosurgery 2000;93:294–299.8Aito S et al.Ascending myelopathy in the early stage of spinal cord injury.Spinal Cord 1999;37:617–623.9Visocchi M,Di Rocco F,Meglio M.Subacute clinical onset of posttraumatic myelopathy.Acta Neurochir 2003;145:799–804.10Harrop JS et al.The cause of neurological deterioration after acute cervical spinal cord injury.Spine 2001;26:340–346.11Yablon IG et al.Acute ascending myelopathy of the spine.Spine 1989;14:1084–1089.12Sliwa JA,Maclean IC.Ischemic myelopathy:a review of spinal vasculature and related clinical syndromes.Arch Phys Med Rehab 1992;73:365–372.13Cassar-Pullicino VN et al.Hemodynamic alterations in the paravertebral venous plexus after spinal injury.Radiology 1995;197:659–663.14Hughes JT.Venous infarction of the spinal cord.Neurol-ogy 1971;21:794–800.15Kim RC et al.Nonhemorrhagic venous infarction of the spinal cord.Ann Neurol 1984;15:379–385.16Zhang Z et al.Circulatory disturbance of rat spinal cord induced by occluding ligation of the dorsal spinal vein.Acta Neuropathol 2001;102:335–338.17Doppman JL,Girton M,Popovsky MA.Acute occlusion of the posterior spinal vein.J Neurosurg 1979;51:201–205.18Cybulski GR,D’Angelo CM.Neurological deterioration after laminectomy for spondylotic cervical myeloradiculo-pathy:the putative role of spinal cord ischaemia.J Neurol Neurosurg Psychiatry 1988;51:717–718.19Bhardwaj A et al.Neurological deficits after cervical laminectomy in the prone position.J Neurosurg Anesthesiol 2001;13:314–319.Subacute delayed ascending myelopathyBJ Schmidt4Spinal Cord。
Case report

功能与分子医学影像学(电子版) 2020年7月第9卷第3期 Funct Mol Med Imaging (Electronic Edition), Jul 2020, V ol. 9, No.31913Case reportLiu Kaili•英文病例•1 HistoryA 57-year-old male with a mass detected in the abdomen for 1 month.2 Image FindingsUnenhanced CT-scan shows a round-like mass measured 8.7 cm × 7.3 cm with clear boundary in the para-aortic region. The lesion shows uneven density, lower density shadow was observed inside, without obvious calcification. On contrast enhanced images, the mass shows obviously heterogeneous enhancement, and is persistent enhanced at venous phase. There is no significant enhancement in the cystic area, and the capsule is intact. CTA showed the mass was supplied by a branch of left renal artery.3 Key Signs(1)A low-density mass with clear boundary in the para-aortic region, without calcification.(2)Enhanced CT-scan shows obviously hetero-geneous enhancement, and persistent enhancement at venous phase.(3)No significant enhancement in the cystic area, and the capsule is intact.(4)Supplied by a branch of left renal artery.4 Final Diagnosis5 Differential Diagnosis(1)Schwannoma It’s the most common retroperitoneal benign tumors, which derived from Schwann cell. Mostly located in the course region of the retroperitoneal nerve trunk. No gender difference. It can be divided into three types, cystic, mixed and solid. The characteristic imaging features include progressive delayed heterogeneous enhancement and no vascular invasion.(2)Leiomyosarcoma Leiomyosarcoma is the third common of the malignant retroperitoneal tumor. It was derived from smooth muscle tissue. The characteristic imaging features is heterogeneous enhancement, cystic degeneration and necrosis were seen frequently, calcification is rare. The solid components enhanced moderately to obviously, partial delayed enhancement.(3)Lymphoma Lymphoma is a malignant tumor originating from lymph nodes or lymphoid tissue. The clinical symptoms are not specific, including painless lymphadenectasis, splenomegaly, epatomegaly and fever. The characteristic imaging features is retroperitoneal multiple lymph nodes,partially fused into a mass. The lymphadenopathy displaced and surrounded adjacent vessels, shows the vascular submergence sign. On enhanced CT-scan, the mass shows slight homogeneous enhancement, cystic degeneration, necrosis and hemorrhage are rare.6 CommentParaganglioma is an extra-adrenal pheochro-mocytoma, derived from neural crest cells in sympathetic ganglions. It’s mostly located in the para-aortic region between the level of renal artery to aortic bifurcation. The ratios of male-to-female is three to two, and mostly in 30 ~ 50 years old. The majority areParaganglioma功能与分子医学影像学(电子版) 2020年7月第9卷第3期 Funct Mol Med Imaging (Electronic Edition), Jul 2020, V ol. 9, No.3 1914benign tumors.Nonfunctional paragangliomas may be asymptomatic. Functional paragangliomas may present with typical sympathetic symptoms of excessive release of catecholamines, such as paroxysmal hypertension, headache, palpitation, diaphoresis.The characteristic imaging features: this tumor shows round-like well-defined mass in the para-aortic region with heterogeneous density and capsule. There is abundant blood supply, obvious enhancement at arterial phase, the degree of enhancement is similar to that of the vascular, and persistent enhancement at venous phase.Due to uneven blood supply, hemorrhage, necrosis, cystic degeneration are common.7 Interactive Activities(1)Question: List the common types of primary tumors located in retroperitoneum.Answer:①Paraganglioma.②Schwannoma.③Lymphoma.④Liposarcoma.⑤Leiomyosarcoma.(2)Question: What are the distinguishing points between paraganglioma and schwannomaAnswer: Table 1.(收稿日期:2020-05-28)(本文编辑:何梅)Figure 1a ~ e Pre-contrast images a:Show a low-density mass with cystic degeneration; b ~ d:The septations shows obviously heterogeneous enhancement, while the cystic region have no enhancement; e:CTA shows the mass be supplied by a branch of left renal arteryTable 1 The distinguishing points between paraganglioma and schwannomaClinical Features Imaging FeaturesParaganglioma30 ~ 50 year Located in the para-aortic regionMale︰Female = 3︰2Obvious enhancement Sympathetic symptoms Hemorrhage, necrosis, cystic degenerationSchwannoma20 ~ 50 year Located in the course region of the retroperitoneal nerve trunk No gender difference Progressive delayed heterogeneous enhancementNo obvious symptoms Necrosis, cystic degeneration are more commonNo vascular invasion。
CaseReport病例报告的书写
26.03.2021
“ Small cell carcinoma of the
prostate is extremely rare. When
it does occur, it is usually in
concordance with prostatic
adenocarcinoma… Because this
2) An unexpected event in the course of observing or treating
a patient.
3) Findings that shed new light on the possible pathogenesis
of a disease or an adverse effect.
The introduction is a brief overview of the larger problem addressed by the case. The overlying message of the section is, “ X is important to understand because…” For example:
“ This case report describes clinical characteristics of a 67-year old man with small carcinoma of the prostate.”
26.03.2021
.
6
Writing: Case report
Structure of a case report:
1. Introduction 2. Case Presentation 3. Discussion 4. References
case report
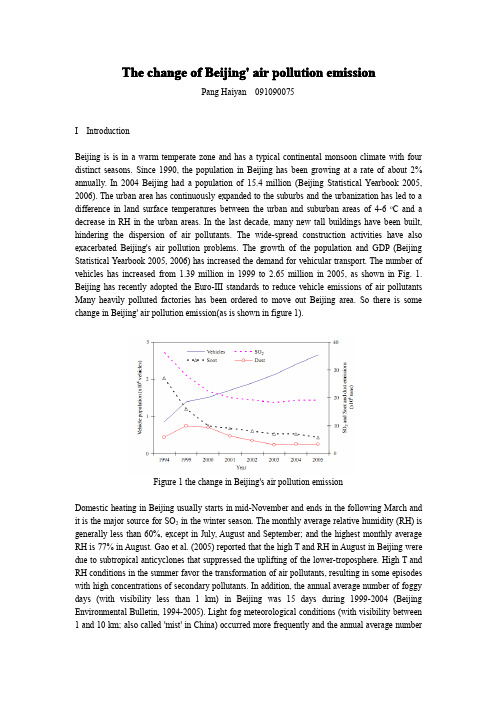
The change of Beijing'air pollution emissionPang Haiyan091090075I IntroductionBeijing is is in a warm temperate zone and has a typical continental monsoon climate with four distinct seasons.Since1990,the population in Beijing has been growing at a rate of about2% annually.In2004Beijing had a population of15.4million(Beijing Statistical Yearbook2005, 2006).The urban area has continuously expanded to the suburbs and the urbanization has led to a difference in land surface temperatures between the urban and suburban areas of4-6o C and a decrease in RH in the urban areas.In the last decade,many new tall buildings have been built, hindering the dispersion of air pollutants.The wide-spread construction activities have also exacerbated Beijing's air pollution problems.The growth of the population and GDP(Beijing Statistical Yearbook2005,2006)has increased the demand for vehicular transport.The number of vehicles has increased from1.39million in1999to2.65million in2005,as shown in Fig.1. Beijing has recently adopted the Euro-III standards to reduce vehicle emissions of air pollutants Many heavily polluted factories has been ordered to move out Beijing area.So there is some change in Beijing'air pollution emission(as is shown in figure1).Figure1the change in Beijing's air pollution emissionDomestic heating in Beijing usually starts in mid-November and ends in the following March and it is the major source for SO2in the winter season.The monthly average relative humidity(RH)is generally less than60%,except in July,August and September;and the highest monthly average RH is77%in August.Gao et al.(2005)reported that the high T and RH in August in Beijing were due to subtropical anticyclones that suppressed the uplifting of the lower-troposphere.High T and RH conditions in the summer favor the transformation of air pollutants,resulting in some episodes with high concentrations of secondary pollutants.In addition,the annual average number of foggy days(with visibility less than1km)in Beijing was15days during1999-2004(Beijing Environmental Bulletin,1994-2005).Light fog meteorological conditions(with visibility between 1and10km;also called'mist'in China)occurred more frequently and the annual average numberof light foggy days was180days during1999-2004.Foggy conditions promote atmospheric chemical reactions.Hydrophilic aerosols can be cloud condensation nuclei,leading to the formation of fogs.The prevailing wind in Beijing is from the north and the northwest,particularly, in the winter and the spring,respectively.The concentrations of air pollutants generally decrease with increasing wind speed.However,the strong northwestern wind carries dust from the Gobi desert to Beijing in the spring and leads to low visibility and high PM10concentrations.II Facts about the change in Beijing's air pollution emission1SO2As reported in the Beijing Environmental Bulletin,SO2emissions decreased from3.62×105tons in1994to1.91×105tons in2005as shown in Fig.2.The local emissions inventory shows that the three major contributors of SO2are power plants,domestic heating,and industrial sources; accounting for49%,26%and24%of the total emissions,respectively,in1999(Hao et al.,2005). When no external transport of SO2to Beijing was considered,Hao et al.(2005)estimated that 39%and36%of the ground SO2concentrations in Beijing were,respectively,from domestic heating and industrial area sources using the ISCST3model with the local emissions inventory. The power plant and industrial point emissions contributed only8%and4%to the ground SO2 concentrations,respectively,due to their emissions at high elevations(460m).More than20%of the ground SO2concentration in Beijing was estimated to be transported from external sources.2NO xNO2is mainly from local on-road vehicle emissions in Beijing.Strengthening the local NO2 emissions regulations from on-roadvehicles would alleviate ambient NO2pollution.NO x (NO2+NO)emissions in1995in Beijing were2.37×105tons and there was no significant increase in the total NO x emissions in1998(2.39×105tons)(Hao et al.,2000).In Fig.2,the constant NO x concentrations in Beijing from1998to2005suggest that there is no significant increase in NO x emissions in Beijing.Hao et al.(2005)estimated that the emissions from vehicles, power plants,and industries in1999accounted for35%,27%and26%in the total local NOx emissions respectively.They found that74%of the ground NO x was due to vehicular emissions while powe plants and industrial sources only contributed2%and13%,ing Models-3/CMAQ with the local emissions inventory,Xu J.M.et al(2005)predicted ground-level NO2concentration that agree well the measured values.3PM10PM10is a criteria pollutant in the National Ambient Air Pollutant Standards,but PM2.5is not.Thus, routine measurements at the local government air quality monitoring stations include PM10but not PM2.5.Although TSP is still in the current standard,but Environment Bulletin in China does not report TSP after2001.TSP is particularly affected when dust storms hit Beijing.We return to TSP when we discuss dust storm events.The annual average of PM10decreased from180μgm-3in 1999to142μgm-3in2005in Beijing as shown in Fig.2.The annual average of PM10was almost constant from2003to2005,and was about40%higher than the Chinese Grade-II standards and seven times the latest WHO Air Quality Guidelines(WHO,2005).In2005,the PM10 concentration in urban areas and the southern suburban areas was almost spatially uniform but thePM10concentration in the northern suburban areas was about30%lower than the PM10 concentration in urban areas(Beijing Environmental Bulletin,2005).Zhang Y.H.et al.(2004)also reported that the daily average PM10concentrations were sometimes higher than100μgm-3at the rural sites of Ming Tomb and Yongledian in Beijing in2000.The high background concentrations suggest the importance of regional sources of PM10in Beijing.Figure2the change in SO2,NO2,PM10emission4O3The control of O3is a complicated problem due to the nature of the non-linear formation of O3.In this paper,O3episodes are events with hourly O3concentrations larger than240μgm-3(the Grade-II standards),if not specified otherwise.O3episodes are frequently observed during the summer in Beijing.For example,the maximum hourly O3concentration in2005reached424μgm-3,which was2.7times the Grade-II standards and also higher than the maximum concentration of384μgm-3in1998().Zheng X.et al.(2005a)observed O3episodes in a rural area(the Ming Tombs)in September2001when the air mass was transported from Beijing's urban areas to the site.In addition,the hours of O3concentrations exceeding the Grade-II standards unexpectedly increased after2002.NO x-VOC photochemical reactions are commonly believed to generate O3in the atmosphere.Alkenes contribute75%of the atmospheric VOC reactivity;and C4 and C5alkenes are particularly important,although alkenes only account for15%of VOC by mass. Alkenes also mainly from vehicular emissions and solvents.Figure3the change in O3emission。
CASE REPORTS
Case Discussion
All choices are potentially correct, but as is often the case, the pathologist has the last word.
• In contrast to pneumonia, colonization of the airway with Candida species and/or contamination of the respiratory secretions with oropharyngeal material are extremely common. • Unfortunately, a positive culture from respiratory secretions is frequently used as an indication to initiate antifungal therapy in febrile patients who have no other evidence of invasive disease."
• Despite the rarity of Candida pulmonary infections, there are occasional cases of pulmonary mycetomas caused by Candida, often in patients with underlying medical problems such as cancer and diabetes. • Candida can also cause formation of masses in other organs, with the renal collecting system perhaps being the most common.
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Case Report组成
1.Abstract and Keywords(摘要和关键词) 2.INTRODUCTION(引言) 3.CASE REPORT(病例报告) 4.DISCUSSION(讨论) 5.REFERENCES(参考文献)
2021
2、写作中基本就是按照我们诊断基本的步骤而来,从体检到实验室或 者影像学检查,再到手术或者治疗,再到预后等等,限于篇幅, 但是在此之间要在相应部位插入图片,比如术前的影像学、术中 照片以及术后病理等等。。。。。。
2021
Case Report
图片
Case Report的精彩部分在 于图片,所以尽可能有详 细的资料。
参考文献
这个没什么好说的,跟一 般中文要求没太大差别, 但是要注意各杂志的要求
2021
总结
限于篇幅,没能讲得很好
1、模仿写——尤其是Case report部分。 2、注意医学术语——比如入院admitted to。。。。。。 3、准备好的资料,尤其是图片资料。。。。。。 4、平时多看文献,或者写Case之前 多看看别人是怎么写Case的,看的
2021
INTRODUCTION
引言
1、总体上介绍GIST,什么是 GIST,有什么特点,病 理特征怎么样等等。。。
2、我们在这里报道1例由于
阑尾出血而偶然诊断的 GIST。
2021
Case Report
2021
病例报告
1、最简单易写,但是认为 最关键,因为要引起 别人的兴趣。
2、好写在什么地方?
多了,慢慢也就会了!
2021
2021
DISCUSSION
讨论
1、讨论部分一般而言比较 难写,但是这个不同于 论著,主要是针对文献 进行讨论。
2、讨论中要参插本例病例 的特点,与其他的病例 或以往病例进行比较,
3、基本的思路就是从临床 特点、影像学检查、治 疗方法以及术后病理等 方面讨论,有点类似综 述的样子。。。
2021
References
2021
胃肠道间质瘤举例——GIST(上文)
这是一例关于阑尾间质瘤的病例,我之前说过胃肠 道间质瘤在胃肠道常见,阑尾罕见。
2021
Abstract an Keywords
概述性摘要: 三步走 1、GIST是什么? 2、GIST是少见,绝大部分
位于胃肠部位,但是 位于阑尾非常罕见。 3、我们在此报道1例阑尾 GIST,由于阑尾出血 而被偶然诊断。 关键词: 一般满足要求即可。
好比我们中文个案一 样—男,多少岁,因 为XX入院,实验室检 查。。,手术。。
3、很多话是可以“拿来” 的,好比一个填空一 样,只是个别数值需 要修改下就好。
Case Report
Case Report中注意事项
1、前面讲过,比较好写,因为很多话在任何病例中基本是一样的,A 56-year-old man was admitted to our department on an emergency basis because of a sudden onset of hematochezia.注意我划线部分, 就是所谓的可以填空的,一个56岁的男性患者因为突然开始便血 而来我院就诊,那你可以替换成因为头疼,或因为腹疼,或因为 腹泻。。。