临床检验基础(血液检查英语版)
信息专业《临床基础检验学》讲义
信息专业《临床基础检验学》讲义第一章血常规检验重点:目的抗凝剂的种类血常规项目的英文缩写RBC、WBC、PLT的正常参考值ESR、Retic的定义内容:一、检测目的二、标本采集1、末梢血采集2、静脉血采集3、标本的抗凝(1)柠檬酸钠(枸橼酸钠)(2)草酸盐(3)肝素(4)EDTA盐(乙二酸四乙酸盐)三、检测项目、正常参考值及临床意义1、红细胞(RBC)(1)成年男性:(4.0~5.5)×1012/L(2)成年女性:(3.50~5.0)×1012/L(3)新生儿:(6.0~7.0)×1012/L2、血红蛋白(1)成年男性:120~160g/L(2)成年女性:110~150g/L(3)新生儿:170~200g/L3、白细胞(1)成人:(120~160)×109/L(2)新生儿:(170~200)×109/L(3)6月~2岁:(11~12)×109/L4、血小板(100~300)×109/L5、血球压积(1)成年男性:0.40~0.50(2)成年女性:0.37~0.48(3)新生儿:0.47~0.676、白细胞分类(1)中性杆状核:1%~5%(2)中性分叶核:50%~70%(3)嗜酸粒细胞:0.5%~5%(4)嗜碱粒细胞:0%~1%(5)淋巴细胞:20%~40%(6)单核细胞:3%~8%7、红细胞有关参数(1)细胞分布宽度(RDW)(2)平均红细胞体积(MCV)(3)平均红细胞血红蛋白含量(MCH)(4)平均红细胞血红蛋白浓度(MCHC)正常参考值MCV(fl) MCH(pg) MCHC(g/L) 成人82~92 27~31 320~3601~3岁79~104 25~32 280~350新生儿86~120 27~36 250~3708、血小板有关参数(1)血小板分布宽度(PDW)(2)平均血小板体积(MPV)(3)血小板压积(PCT)四、检测方法1、手工2、血细胞分析仪(1)原理(2)报告方式五、其他血液检测项目1、血沉定义:在一定条件下,单位时间内红细胞在全血中沉降的速率,以mm/h表示。
临床检验学 英语
临床检验学英语Clinical Laboratory ScienceThe field of clinical laboratory science is a critical component of the healthcare system, providing essential information to healthcare professionals for the diagnosis, treatment, and monitoring of patient health. Clinical laboratory scientists, also known as medical laboratory scientists or medical technologists, play a pivotal role in the healthcare team, utilizing specialized knowledge and skills to perform a wide range of laboratory tests and analyses.One of the primary responsibilities of a clinical laboratory scientist is to collect, process, and analyze various biological samples, such as blood, urine, and tissue specimens. These samples are subjected to a variety of tests, including hematology, chemistry, microbiology, and immunology, to provide healthcare providers with crucial data about a patient's health status. Clinical laboratory scientists must possess a deep understanding of the principles and techniques involved in these laboratory procedures, as well as the ability to interpret the results accurately and effectively communicate their findings to the healthcare team.In the field of hematology, clinical laboratory scientists analyze the cellular components of the blood, including red blood cells, white blood cells, and platelets. They perform tests to assess the quantity and quality of these cells, as well as to detect any abnormalities that may indicate the presence of various medical conditions, such as anemia, leukemia, or coagulation disorders. By providing this information, clinical laboratory scientists play a vital role in the early detection and management of these conditions.The chemistry laboratory is another critical area of focus for clinical laboratory scientists. Here, they analyze various chemical components of the body, such as electrolytes, enzymes, and hormones, to evaluate the overall metabolic function and organ health of the patient. These tests can help identify imbalances or abnormalities that may be indicative of conditions like diabetes, kidney disease, or liver dysfunction. The accurate interpretation of these results is essential for healthcare providers to make informed decisions regarding treatment and patient care.In the field of microbiology, clinical laboratory scientists are responsible for identifying and characterizing infectious agents, such as bacteria, viruses, and fungi, that may be present in a patient's sample. They use a variety of techniques, including culture, staining, and molecular-based methods, to detect and identify these microorganisms. This information is crucial for the diagnosis andappropriate treatment of infectious diseases, as well as for monitoring the effectiveness of antimicrobial therapies.The immunology laboratory is another important area of clinical laboratory science, where scientists analyze the body's immune system and its response to various stimuli. They perform tests to measure the levels of specific antibodies, proteins, and other markers that can provide insight into the functioning of the immune system. This information is particularly valuable in the diagnosis and management of autoimmune disorders, allergies, and other conditions that involve the immune system.In addition to their technical expertise, clinical laboratory scientists must also possess strong critical thinking and problem-solving skills. They often encounter complex or ambiguous situations that require them to analyze data, identify potential sources of error, and make informed decisions to ensure the accuracy and reliability of their results. Furthermore, they must be able to effectively communicate their findings to healthcare providers, who rely on this information to make crucial decisions regarding patient care.Clinical laboratory science is a dynamic and constantly evolving field, with new technologies, techniques, and discoveries constantly emerging. As such, clinical laboratory scientists must be dedicated to ongoing learning and professional development, staying up-to-datewith the latest advancements in the field and continuously honing their skills and knowledge. This commitment to lifelong learning is essential for ensuring the delivery of high-quality, evidence-based laboratory services that support the overall healthcare system.In conclusion, the field of clinical laboratory science is a vital component of the healthcare industry, providing essential information and support to healthcare providers and their patients. Clinical laboratory scientists play a crucial role in the diagnosis, treatment, and monitoring of various medical conditions, utilizing their specialized knowledge and skills to perform a wide range of laboratory tests and analyses. As the healthcare landscape continues to evolve, the demand for skilled and knowledgeable clinical laboratory scientists will only continue to grow, making this a dynamic and rewarding career path for those interested in the intersection of science, technology, and patient care.。
临床检验基础复习资料.doc

㈤名词解释1.核左移(shift to the left)外周血中杆状核粒细胞增多并出现晚幼粒、中幼粒甚至早幼粒细胞时称为核左移。
核左移常伴中毒颗粒、空泡、核变性等毒性变化。
最常见于急性化脓性感染,急性中毒、急性溶血时也可见到。
4.核右移(shift to the right)外周血中5叶核以上的中性粒细胞>3%时称为核右移。
核右移常伴有白细胞总数的减少,属造血功能衰退的表现。
是因缺乏造血物质、DNA合成减少或骨髓造血功能减退所致。
主要见于营养性巨幼细胞性贫血及恶性贫血。
在炎症的恢复期,可出现一过性的核右移。
在患病进展期突然出现核右移则提示预后不良。
12.类白血病反应(leukemoid reaction)指机体对某些刺激因素所产生的类似白血病表现的血象反应。
外周血中白细胞总数大多明显增高,并可有数量不等的幼稚细胞出现,但红细胞和血小板一般无改变。
骨髓增生但很少达到白血病的程度,当病因去除后,类白血病反应也逐渐消失。
引起类白血病反应的病因很多,以感染和恶性肿瘤最多见,其次还有急性中毒、外伤、休克、急性溶血或出血、大面积烧伤及过敏等。
1.血细胞体积分布直方图(histogram)血细胞分析仪根据检测结果,以细胞体积大小为横座标,细胞相对频率为纵座标所获得表示细胞群体分布情况的曲线图形,称作血细胞直方图。
它为检验人员监控仪器工作状态及检测结果提供了直观的图形。
2.血小板平均体积(MPV)是指血液中血小板的平均体积,单位用飞升(fl)表示3.血小板分布体积宽度(platelet distribution width, PDW)是反映血小板体积大小异质性的参数,用血小板积的变异系数来表示(CV),主要用于血小板异常疾病的辅助诊断与鉴别诊断。
4.网织红细胞成熟指数(RMI)RMI=(MFR+HFR)/LFRX100,为全自动网织红细胞分析仪提供的新参数,是反映幼稚网织红细胞变化较敏感的指标。
对贫血的诊断、骨髓移植术和白血病疗效观察有非常重要意义。
临床常规检验项目及英文缩写
临床常规检验项目及英文缩写一、血液检验项目及英文缩写1. 血红蛋白(Hemoglobin,Hb):血红蛋白是红细胞内的一种蛋白质,负责携带氧气到身体各部位。
2. 红细胞计数(Red Blood Cell Count,RBC):用于评估患者的红细胞数量,匡助诊断贫血等疾病。
3. 血小板计数(Platelet Count,PLT):用于评估患者的血小板数量,匡助诊断出血倾向等疾病。
4. 白细胞计数(White Blood Cell Count,WBC):用于评估患者的白细胞数量,匡助诊断感染等疾病。
5. 血小板压积(Plateletcrit,PCT):用于评估患者血液中血小板的比例,匡助诊断出血倾向等疾病。
6. 血小板平均体积(Mean Platelet Volume,MPV):用于评估患者血小板的平均大小,匡助诊断出血倾向等疾病。
7. 血小板分布宽度(Platelet Distribution Width,PDW):用于评估患者血小板的大小分布范围,匡助诊断出血倾向等疾病。
8. 血沉(Erythrocyte Sedimentation Rate,ESR):用于评估患者红细胞在一定时间内沉降的速度,匡助诊断炎症等疾病。
9. 糖化血红蛋白(Glycated Hemoglobin,HbA1c):用于评估患者血糖操纵情况,匡助诊断糖尿病等疾病。
10. 血型(Blood Type):用于确定患者血液类型,匡助输血和器官移植等医疗操作。
二、尿液检验项目及英文缩写1. 尿常规(Urinalysis,UA):用于评估患者尿液的物理性质和化学成份,匡助诊断泌尿系统疾病等。
2. 尿白细胞计数(Urinary White Blood Cell Count,UWBC):用于评估患者尿液中白细胞的数量,匡助诊断尿路感染等疾病。
3. 尿红细胞计数(Urinary Red Blood Cell Count,URBC):用于评估患者尿液中红细胞的数量,匡助诊断泌尿系统疾病等。
血液分析仪检验临床检验基础

检测项目 M;M#;E#;E;B;B#;未成熟白细胞 NRBC;RET;IPF
01
代表仪器 SF-3000血细胞分析仪、EXCELTM22血细胞分析仪等。
02
仪器性能的评价
影响直方图变化的因素
仪器类型和特点
仪器方法学评价
仪器类型和特点 单纯电阻抗法三分群血液分析仪特点
检测参数:约20项左右。
P94
分析仪检测Hb 的原理: 被稀释的血液加入溶血剂后,红细胞溶解,释放血红蛋白,后者与溶血剂结合形成Hb衍生物,在特定波长(530~550nm)下比色,吸光度的变化与液体中Hb含量成比例。
P96
四、分光光度法
血红蛋白
血红蛋白 衍生物
吸光度
Hb浓度
λ=540nm
溶血剂
血液分析仪检测参数原理
白细胞分类:只能对白细胞进行三分群。
直方图:3种直方图。
报警功能: 以文字和(或)图标提示 异常检测结果的信息。
(一)仪器类型和特点
(一)仪器类型和特点
2.综合光学和电学等技术血液分析仪特点 (1)检测参数:约20至40项左右 (2)白细胞分类:能对白细胞进行五分类。 (3)直方图和散点图:3种直方图和散点图。 (4)报警功能: 以文字和(或)图标显示 异常检测结果的信息。 注意:各类型血液分析仪不具备识别异常细胞 形态的能力,故不能完全代替镜检。
血细胞直方图
1 血细胞直方图概念: 在细胞通过小孔计数时,感应器收集脉冲 的大小及数量,转换为相应的细胞体积和数量, 并在坐标上表示出来。坐标的横轴(x)代表体积 (FL),纵轴(Y)代表相对数量,将各点用光滑的 曲线相连,就是直方图。即直方图是可以表示 出细胞群体体积分布情况的图形。
关于准确度和精密度的注意点
临床血液学检验中英文名词(1)

临床血液学检验中英文名词(1)临床血液学检验中英文名词1. MICM 细胞形态学,免疫学,细胞遗传学,分子生物学P.2542.EH 髓外造血P.133.HIM 造血微环境P.134.TSC 全能干细胞P.105.HSC 造血干细胞P.106.HPC 造血祖细胞P.137.EPO 促红细胞生成素P.318.PCD 凋亡(Ⅰ型程序性细胞死亡)P.339.HbF 胎儿血红蛋白(抗碱血红蛋白)P.1010.SCF干细胞因子P.1411.ESC 胚胎干细胞P.912.MSC 骨髓间充质干细胞P.1713.MPO 髓过氧化物酶P.2714.CSF 集落刺激因子P.3115.TPO 血小板生成素P.3116.TNF 肿瘤坏死因子P.3317.IFN 干扰素P.3318.CK 趋化因子P.3319.G/E 粒红比值P.8620.ANC 有核细胞百分比P.25521.NEC 非红系细胞百分比P.25522.PV 真性红细胞增多症P.21923.IDA 缺铁性贫血P.22324.ID 贮存铁缺乏P.22425.IDE 缺铁性红细胞生成P.22426.SF 血清铁蛋白P.22627.SI 血清铁P.22628.TIBC 总铁结合力P.22629. UIBC 未饱和铁结合力P.14930.TS 转铁蛋白饱和度P.22631.sTf 血清转铁蛋白P.15032.sTfR 血清转铁蛋白受体P.15033.MA 巨幼细胞性贫血P.22834.IF 内因子P.15235.PAS 糖原染色,过碘酸-希夫反应P.10336.AA 再生障碍性贫血P.23237.FA 范科尼贫血(先天性再障)P.23238.NAP 碱性磷酸酶染色P.10539.PNH 阵发性睡眠型血红蛋白尿症P.165 40.HA 溶血性贫血P.14441.HS 遗传性球形红细胞增多症P.23842.HE 遗传性椭圆形红细胞增多症P.23943.G-6-PD 葡萄糖-6-磷酸脱氢酶P.24144.PK 丙酮酸激酶P.24345.AIHA 自身免疫性溶血性贫血P.24346.CAS 冷凝集素综合征P.24447.PCH 阵发性冷性血红蛋白尿症P.24448.AGLT 酸化甘油溶血试验P.15449.NADPH 还原性辅酶ⅡP.15650.MHb-RT 高铁血红蛋白还原试验P.15751.AGT 抗球蛋白试验P.15952.HPLC 高效液相色谱法P.18453.AL 急性白血病P.25454.MRL 微量残留白血病P.135/doc/dc13532528.html,SL 中枢神经系统白血病P.27956.LSCs白血病干细胞P.26057.B-ALL/LBL B淋巴母细胞白血病/淋巴瘤P.27658.T-ALL/LBL T淋巴母细胞白血病/淋巴瘤59.EL 红白血病P.27460.PEL 纯红血病P.27461.PPO 血小板髓过氧化物酶P.4662.AML 急性髓系白血病P.24263.ALL 急性淋巴细胞白血病P.25464.NHL非霍奇金淋巴瘤P.28065.HD 霍奇金病P.28366.HL 霍奇金淋巴瘤P.25867.NLPHL结节性淋巴细胞为主型霍奇金淋巴瘤P.28368.CHL 经典型霍奇金淋巴瘤P.28369.CLL 慢性淋巴细胞白血病P.28570.SLL 小淋巴细胞淋巴瘤P.28571.HCL 多毛细胞白血病P.28672.ATLL 成人T细胞白血病/淋巴瘤P.28773.PLL 幼淋巴细胞白血病P.28874.LGL 大颗粒淋巴细胞P.28975.MDS 骨髓增生异常综合征P.29076.RCUD 难治性血细胞减少伴单系发育异常P.29177.RA 难治性贫血P.29178.RN 难治性中性粒细胞减少P.29179.RT 难治性血小板减少P.29180.RARS 难治性贫血伴环形铁粒幼细胞P.29281.RCMD 难治性血细胞减少伴多系发育异常P.29382.RAEB 难治性贫血伴原始细胞增多P.29483.MPN 骨髓增殖性肿瘤P.29584.CML 慢性髓细胞白血病P.29585.PV 真性红细胞增多症P.29886.ET 原发性血小板增多症P.29987.Ph染色体费城染色体P.29588.PMF 原发性骨髓纤维化P.30089.CEL,NOS慢性嗜酸性粒细胞,非特指型P.30290.MD-MPN骨髓增生异常-骨髓增殖性肿瘤P.30391.CMML 慢性粒-单核细胞白血病P.30392.αCML,BCR/ABL1-不典型慢性髓细胞白血病,BCR/ABL阴性P.30493.JMML幼年型粒-单细胞白血病P.30594.MM 多发性骨髓瘤P.30695.PCL 浆细胞白血病P.30896.MGUS 意义未定的单克隆免疫球蛋白病P.30997.LR 类白血病反应P.31198.IM 传染性单核细胞增多症P.31299.NPD 尼曼-匹克病P.316 100.HPS 嗜血细胞综合征P.317 101.HLH 嗜血细胞性淋巴细胞组织细胞增多症P.317 (100=101)102.ITP 原发性血小板减少性紫癜P.326 103.TTP 血栓性血小板减少性紫癜P.327 104.GT 血小板无力症P.327 105.PF3 血小板第三因子P.328 106.vWD血管性血友病P.330 /doc/dc13532528.html, 狼疮抗凝物质P.334 108.DIC 弥散性血管内凝血P.335 109.AMI 急性心肌梗死P.337 110.CAD 冠状动脉粥样硬化性心脏病P.337 111.PTE 肺栓塞P.338 112.PI 肺梗死P.338 113.DVT 深静脉血栓形成P.338。
实验诊断血液一般检查
2.血红蛋白测定 determining the concentration of hemoglobin
• 方法method
氰化高铁血红蛋白法
hemiglobincyanide (HiCN)method
Hemoglobin Structure
实验诊断血液一般检查
THE NORMAL HUMAN HEMOGLOBENS
20ul血液 数
充池、静止
镜下计
实验诊断血液一般检查
Neubauer计数盘
实验诊断血液一般检查
WBC
3mm
WBC
WBC
WBC
1mm 计算:WBC/L=N/4×10×106×20 实验诊断血液一般检查
(2)自动血液分析仪automated
hematology analyzer,AHA
• 电阻抗法血细胞分析仪的原理
ICSH分为4型:正常周围血Ⅲ型网织红细胞约为0.2~0.3,IV 型约0.7~0.8,但骨髓红系明显增生时,可出现I型和II型网 织红细胞。
实验诊断血液一般检查
检测方法:
1)普通光学显微镜法 用活体染色(煌焦油
蓝等染液)方法显示红细胞内网状结构
2)网织细胞计数仪法 用荧光染料(如吖
啶橙、派若宁-Y、噻唑橙)使含RNA的网织红 细胞着色,用流式细胞仪(flow cytometry, FCM)计数并计算出网织红细胞的百分比。
实验诊断血液一般检查
实验诊断血液一般检查
病理性变化
(1)红细胞和血红蛋白量减少:在临床最 常见于各种原因的贫血anemia。
①急性、慢性红细胞丢失过多:如各种原因的 出血。 ②红细胞寿命缩短:如各种原因的溶血 ③造血原料不足 ④骨髓造血功能减退
血液常规检验
血常规检验(一)血红蛋白检验1.英文或缩写:Determinatiom of Hemoglobin in Blood,Hb 或 HGB。
2.标本采集:静脉抽取血0.5-1ml 迅速注入含有20μl 的E DTA-K2 抗凝剂内,混匀送检。
3.正常参考值:男:120-160g/L;女:110-150g/L;新生儿:170-200g/L。
4.临床意义:升高:(1)生理性升高,如新生儿、高原居民住者。
(2)病理性升高,真性红细胞增多症,代偿性红细胞增多症(如先天性青紫性心脏病、慢性肺心病、脱水)。
降低:各种贫血、白血病、产后、手术后、大量失血。
5. 注意事项:末梢采血切忌用力挤压,以免流入大量组织液,使血液稀释,影响检验结果,且血液易凝固。
为避免血液浓缩,用止血带压迫时间不能过长,最好不超过半分钟。
不得随意增加抗凝剂量,若末梢采血,最好先将试管内抗凝剂涂壁烤干再用。
(二)红细胞检验红细胞计数1.英文或缩写:Erythrocyte Count in Blood,RBC。
2.标本采集:同H GB。
3.正常参考值:男:(4-5.5)×1012/L;女:(3.5-5.0)×1012/L;新生儿:(6-7) ×1012/L。
4.临床意义:一般情况红细胞与血红蛋白之间成正比例关系,但在部分患者,同时检验二项对贫血诊断和鉴别诊断有帮助。
5.注意事项:注射器和容器均须清洁干燥,防止溶血;抽血速度不能过快,以免产生大量泡沫;抽血后应先拔去针头,再将血液缓缓注入标本容器,否则易造成溶血。
血细胞比容检验1.英文或缩写:Hematiocrit in Blood,HCT。
2.标本采集:同H GB。
3.正常参考值:男:0.42-0.49L/L;女:0.37-0.43L/L。
4.临床意义:增高:大面积烧伤.各种原因引起的红细胞与血红蛋白增多、脱水等。
降低:各类贫血时随红细胞数的减少而有不同程度的降低。
临床检验基础_血液学一般检验

肾脏有实质性损伤的依据 问:tumor?
2、为分析病情、观察疗效、判断预后提供依据 在疾病过程中,血液、体液、分泌物和排泄物也 会随之发生相应的变化 3、为预防疾病提供资料 如血象和肿瘤细胞学的普查等
三、临床检验的一般方法 1、目视检查 直接观察标本:颜色、透明度、性状,有无 凝块或寄生虫 液体的相对密度、血液比粘度、红细胞沉降 率、红细胞比积等病理变化 定性和定量检测标本化学成分的病理变化 观察有型成分的数量和形态
第一章 血液学一般检 验(1、2)
检验教研室
绪
论
• 一、临床检验(clinical laboratory technology or science)
又称实验诊断学,就是通过实验室的各种检 查方法,包括感官检查、理学检查、化学检 查、显微镜检查以及自动化仪器检查等,对 病人的血液、体液、分泌物和排泄物等标本 进行检查、分析,以获得病原、病理变化及 脏器功能状态等资料。
草酸钾
可使RBC缩小 可使RBC胀大 RBC形态、体积无变化 适用于测Hct。
草酸铵
草酸钾:草酸铵
5. 肝素
• 肝素能阻止凝血酶形成 和抑制血小板聚集
• 肝素具有抗凝能力强,不影响血细胞体积, 不引起溶血
• 肝素会引起白细胞聚集,使血涂片染色产 生蓝色背景,不能用于白细胞计数和分类 计数
四、血涂片的制备
• 2. 血浆成分、血浆粘 度及血流动力学等
(4)粘滞性
• 取决于血细胞比容和血浆粘度
• 健康成人: 全血粘度为生理盐水粘度的4~5倍 血浆粘度为生理盐水粘度的1.6倍左右
(5)比重和渗透浓度
• 全血比重: 男性约为1.055~1.063 女性约为1.051~1.060; 与红细胞的百分比有关
临床基础检验学血液常规检查课件

检测完的血液标本 经消毒后再集中燃烧。
思考题:
1.血浆与血清有何不同? 2.采血前应考虑哪些问题? 3.采血时应注意些什么?
1
第二章
一般血液学检验
主要内容
第一节 外周血液血细胞形态学检验 第二节 红细胞检验 第三节 白细胞检验
2、异常红细胞形态
大小异常 染色异常 形态异常 结构异常
红细胞形态变化
1.红细胞大小不一
〔1〕小红细胞 (microcyte) 指直径小于 6μm的红细胞。出现较多染色过浅的小红 细胞,提示血红蛋白合成障碍,见于缺铁 性贫血。而遗传性球形细胞增多症,其血 红蛋白充盈良好,生理性中心浅染区却消 失。
白或其他衍生物时,呈暗红色、紫黑色。
第一节 血液标本采集和抗凝剂选择
一、血液标本种类 全血:由血细胞和血浆组成,主要用于临床
血液 学检查,如血细胞计数、分类和形态学检 查. 血浆:为全血除去血细胞的局部,适合临床 生化 检查,内分泌激素测定、血栓与止血的检 查。 血清:是离体后的血液自然凝固后析出的液
方法 将肘部静脉上端用压脉带 系紧,使静脉充分暴露,局部消 毒,用注射器刺入取血;
用途 需血量较多或采用全自动血液分析仪测定 时使用; 评价 采集的血量可任意控制,但操作环节多,在 移液及丢弃注射器时可能造成环境污染位同普通法。采血器有套筒
〔2〕大红细胞 (macrocyte )指直径大于10μm的 红细胞。常见于巨幼细胞性贫血,也可见于溶血 性贫血、恶性贫血等。
〔3〕巨红细胞 (megalocyte)指直径大于15μm 的红细胞。最常见于叶酸及维生素B12缺乏所致 的巨幼细胞性贫血。
血液检验血常规检验英文缩写
血液检验血常规检验英文缩写、参考值
乙型肝炎病毒血清学检查
乙型肝炎五项检验内容的阳性和阴性结果可能有各种不同的组合方式,下面例举的10个模式可帮助你对不同的组合进行分析和判断。
注:+ 表示阳性,- 示阴性。
模式A:此情况少见,表示乙型肝炎潜伏期或急性期。
模式B:多见于乙型肝炎病人或病毒携带者,感染性较强。
模式C:在某些急慢性肝炎患者血清中可以见到此种表现,感染性中等。
模式D:急慢性乙型肝炎和病毒携带者,感染性较低。
模式E:急慢性乙型肝炎和病毒携带者中可见,一般预后较好,感染性较低。
模式F:见于以往有过病毒感染,HBsAb降低到不能检测出的水平,还见于乙型肝炎恢复期。
模式G:见于近期被乙型肝炎病毒感染过。
模式H:为乙型肝炎感染的恢复期,除说明有过感染外还说明已有一定的免疫力。
模式I:表示曾经有过乙型肝炎病毒的感染,现已完全恢复,并已有一定的免疫力。
模式J:说明曾经有过乙型肝炎病毒的感染,并有了一定的免疫力;也说明曾经注射过乙型肝炎疫苗或HBsAb免疫球蛋白。
心肌标志物检验英文缩写、参考值
·labsky 发表于2006-7-8 9:05:25。
2.1-血液检查.
临床意义
Clinical significance
1、 RBC及Hb增高
绝对增多:
原发性红细胞增多症(Primary erythrocytosis):属于慢 性骨髓增生性疾病,临床较常见,发病机制尚未明了,可 能与下列因素有关:
– 造血干细胞增生失控 – 红系祖细胞对EPO的反应性增强
22
临床意义
Clinical significance
Hct减低:
见于各种 anemia 不同类型的 anemia,RBC体积不同。故,Hct与RBC不一
定成比例变化 RBC数、Hb值及Hct值三个指标可基本限定RBC的大小及
色素浓淡 以上三指标可算出RBC若干平均参数,用于anemia鉴别
正常红细胞(normocyte)和正常色素性(normochromic) 小红细胞(microcyte)和低色素性(hypochromic) 大红细胞(macrocyte)、巨红细胞(magalocyte)和高
色素性(hyperchromic) 红细胞大小不均(anisocytosis) 嗜多色性(polychromatic)
均红细胞血红蛋白浓度) RDW:Red bool cell volume distribution width(红细胞体积
分布宽度) RET:Reticulocyte(网织红细胞)
5
检查指标的英文缩写解释
DC:Leukocyte differential count(白细胞分类计数) PLT:platelet(血小板) MPV:Mean platelet volume(血小板平均体积) Pct:plateletcrit(血小板比积) PDW:Platelet volume distribution width(血小板体积分布
血液一般检查讲稿双语
First section: Blood routine test (BRT)Has Someone here ever heard of BRT before? Yes! Very good many students have heard before. (NO? maybe you are all very healthy ).when you go to hospital, doctors always apply for a BRT as a reference to your disease. They can know about the red blood cells ,white blood cells and platelets et,al.So BRT is the most common examination in clinical laboratory. Today we will learn the blood routine test (the abbreviation is BRT) or complete blood count (CBC).1.Sample collectingfirst, we will learn about the collection of BRT sample. The blood can be collected from finger or vein. But we are always collecting blood from vein, Because the result come from a vein sample is more accurate and stable than from finger.But if it is very difficult to find a good vein to collect, for example ,when we meet with a baby. After we collected the sample, the blood must be anticoagulated with EDTA-K 2. Because we will count cells in it. We will learn in the later. Here please remember the anticoagulant----EDTA-K2. OK, lets take a look of the main contents of BRT. It conclude three parts, they are RBC,WBC,PLT.Now we will learn one by one.2. RBC related parametersAt first, will learn about the red blood cells. There are seven parameters related to it. They are:1)The number of red blood cells (RBC)2)The amount of hemoglobin in the blood(Hb)3)Hematocrit (Hct)4)mean corpuscular volume (MCV)5)Mean corpuscular hemoglobin(MCH)6)Mean corpuscular hemoglobin concentration (MCHC)7)Red blood cell volume distribution width(RDW)1)RBC and HbNow ,lets learn about RBC and hemoglobin. we put the two indexes together ,because theyhave the same clinical signifcance.(1)The normal valuesThe normal values of RBC is to male :the normal number of RBC is 4.0-5.5,to Female: is 3.5-5.0 million millions per liter . so it is different between male and female.Familiar to RBC, the normal value of hemoglobin is different between male and female too.All the values above are required to remember.The numbers of RBC or the concentrations of Hb is increased, it can be caused by relative factors or absolutely factors.For example , when we sicking \ burning or sweating too much ,much waters in our body will be lost, the plasma is concentrated, so the RBC numbers is relatively increasing.Some diseases, such as heart disease , lung disease, can also cause the number of RBC increasing. We all know that the main function of RBC is carry oxygen, when people got heart disease, for example, heart failure, the body will be lack of oxygen, so it will produce more RBC as compensation.(2)Clinical significanceIf the numbers of RBC or the concentrations of Hb is decreased, we call this anemia. Certainly it include physologic anemia and pathologic anemia.When people is pregnant or getting old , the physologic factors will cause the number of RBC decreased, this called physologic anemia. It neednt to cure.If the iron in the body is deficiency , the bone marrow cant produce enough RBC or the RBC which produced are abnormal. These all can be cause anemia. Anemia is very common in clinic. Please turn to page 268 , lets look at the table 4-2-2-the classification of anemia.2)HCT or PCV(P280)Ok, this is all of the numbers of RBC and hemoglobin.Now , we will learn another index of RBC--Hematocrit or packed cell volum (PCV).HCT is the ratio that the volumes of blood cells (mainly RBC) in the whole blood. So the calculate formula is V cell / V whole blood.Because the cells in the blood mainly is RBC, which is the reason why the blood is red, so the clinical significance of HCT is accord with the change of RBC. When the RBC or Hb increasing, HCT will increase too. And when the RBC or Hb decreasing ,HCT will decrease too.3)MCV,MCH,MCHC(P280)Now, lets learn three related indexes of RBC, they are MCV, MCH and MCHC.The MCV is the abbreviation of mean volume of each RBC, so from the definition, we can see that it represent the average size of RBC.Patients with IDA (iron deficient anemia) , their RBC are smaller than normal people, the MCV is decreased. So we can judge the RBC size from this index.MCH is the abbreviation of mean hemoglobin of each RBC, it represent the average hemoglobin of RBC. We also cite IDA as example, we all know, it is necessary that the iron in our body must be adequate in the course of hemoglobin producing, when the iron is deficiency, the hemoglobin in the RBC will be reduced, certainly the MCH is decreased.The MCHC is the mean corpuscular hemoglobin concentration,These three indexes can be calculated with the number of RBC, HCT and hemoglobin. When two indexes among them is known, the left index can be calculated too.MCV,MCH and MCHC reflect the size and hemoglobin concentration of individual cells.It is useful in the diagnosis of various types of anemia. P281,table 4-2-54)RDWOk, please come back to the slide.Lets learn the last index about RBC---RDW.At first lets see the definition: the RDW is the abbreviation of the RBC volume distribution width.It is a measure of the variation of RBC volume.In normal people, the RBC volume is homogeneous,is about 7um, but in certain anemia, some RBC become larger, some RBC become smaller, So the size of RBC become variety, the RDW will be increased.Application: P281,table 4-2-63.WBC related parametersNow lets learn about WBC, first lets see the parameters related to WBCThey are the number of white blood cells and the component of WBC,WBC are divided into five types: neutrophil, lymphocyte, monocyte, eosinophil and basophil. Each type cells can be described in two forms: the percentage and the absolute count. Mostly weuse the percentage to describe the component of WBCS.1)The function of WBC-Fight infection-Make antibodies2)Divided into Five types according to its shapeTypes of WBCs normally present in blood:- neutrophils (infection-fighters), 2 types:polys or segs = segmented neutrophils (mature)bands or stabs = banded neutrophils (young)- lymphocytes (immunity)- monocytes (phagocytosis)- eosinophils (allergy, parasites)- basophils (hypersensitivity)In neutropenia, most WBCs are lymphocytes. An early indication of recovery is the presence of monocytes,Non-malignant blasts are sometimes seen during neutrophil recovery following chemotherapy, especially in conjunction with GCSF/GMCSF therapy, as a result of an over stimulated bone marrow releasing immature cells into the peripheral circulation.Neutrophil (Ne)make up 55-70% of total WBC countvery tiny light staining granulesthe nucleus is frequently multi-lobedcan phagocytizing foreign cells, toxins, and virusesEosinophil (EO)make up 0.5-5% of total WBC countlarge granules stained pink (or red)the nucleus often has two lobesthe granules contain enzymesattacks parasites and any antigen complexesare also responsible for allergic responseBasophil (Ba)less than 1% of total WBC countgranules are large, stain deep blue to purplegranules often numerous ,can mask the nucleusgranules contain histaminesmediate hypersensitivity reactionslymphocyte (Ly)make up 20-40% of totle WBC countit is an agranular cell with very clear cytoplasmthe cytoplasm stains pale bluenucleus is very large for the size of the cell , stains dark purpleLymphocyte is much smaller than the three granulocytesplay an important role in our immune responseproduce antibodies and provide secondary immunityThe lymphocyte is an agranular cell with very clear cytoplasm which stains pale blue. Its nucleus is very large for the size of the cell and stains dark purple. (Notice that the nucleus almost fills the cell leaving a very thin rim of cytoplasm.) This cell is much smaller than the three granulocytes (which are all about the same size). These cells play an important role in our immune response. The T-lymphocytes act against virus infected cells and tumor cells. The B-lymphocytes produce antibodies.Monocyte (Mo)it is agranular, make up 4-10% of totle WBC countIt is the largest cell among the five typesthe cytoplasm is abundant and stains pale bluenucleus often shaped U or kidney bean , stains dark purpledevelop into large macrophagesphagocytize pathogens during infectionThis cell is the largest of the leukocytes and is agranular. The nucleus is most often "U" or kidney bean shaped; the cytoplasm is abundant and light blue. These cells leave the blood stream (diapedesis) to become macrophages. As a monocyte or macrophage, these cells are phagocyticand defend the body against viruses and bacteria.These cells account for 3-9% of all leukocytes. In people with malaria, endocarditis, typhoid fever, and Rocky Mountain spotted fever, monocytes increase in number. it can develop into large macrophages in the body tissues that phagocytize pathogens during infectionNormal valuesOk ,lets see the normal values of WBCS.To you all, the values in this slide must to remember.The number of WBC is 4-10 thousand millions per liter. And mainly is composed of neutrophil, contain 50-70 percentage, the second component is lymphocyte , normally is 20-40 percentage, and the normal value of monocyte is 3-8 percentage , eosinophil and basophil are scase to see in normal people, the normal value is 0.5-5 percentage and 0-1percentage respectively.Clinical significanceThe change of each component would lead to the number of WBC increased or decreased , but its clinical significance is different ,so we should distinguish which component is changed. Now lets learn the clinical significance of each component.First ,lets see the neutrophil:NeThe change of WBC is mostly changed by the neutrophil.In certain people such as pregnant ,the neutrophil will increase, and when we eat too much or after sport , it will increase temporarily. These are all physiologic increasing.Neutrophil increasing is seen often in clinic. Many acute disease can cause the neutrophil increasing, please notice the acute. Acute disease such as acute infection---mainly caused by bacteria, injury or acute hemolysis and bleeding. These are all acute disease. Besides acute disease , in most leukemia such as CML(chronic myelocytic leukemia) the neutrophil is increase too. Followed with the increasing of neutrophil , the number of WBC is always increasing.The decreasing of neutrophil is often occure in some certain infections, such as virus, typhia and paratyphoid. When people infected with virus, the lyphocyte will increasing, and when people infected with typhia or paratyphoid , the neutrophil is decreased, the number of WBC is also decreased.Morever, some hematonosis such as AA, IDA, PNH, and some external factors such as X ray、medcine can also cause neutrophil decreasing.We all know in the spleen , blood cells, including RBC, WBC and platelet, can be destroyed, so in some desease , the function of spleen become too strong, the blood cells will be destroyed too much , can cause the RBC WBC and platelets decreasing at the same time.In autoimmune disease such as SLE , RA, the antibody can bind with the blood cells , and the body will disposal the blood cells as external antigen, send it to the immune system to destroy it. Here lets see two terms, the first is leukopenia: it defines when the number of WBC are less than 4.0*109.The other is neutropenia: it defines when the number of neutrophil are less than 1.5*109. EoOk, lets see the eosinophil.You should remenber in two diseases the eosinophil will increasing , the two diseases are allergy and verminosis. The allergy can be caused by food , medicine or pollen. When people infected with parasite we called it verminosis.The decreasing of eosinophil has no important significance.So we should remenber when people with allergy or verminosis ,the eosinophil often increasing. BaLets see the basophil, the increasing of basophil is not often seen in clinic, it can be seen in some certain hematonosis such as CML, Bone marrow fibrosis and allergy. It will increasing fast when the CML is activity, so it is important to observe the disease whether it is become severity. LyLets see the lymphocyte, the lymphocyte include T lymphocyte and B lymphocyte, they are the main immunocyte, so when the immunity is activity ,the lymphocyte will increase. For example , when people infected with virus , or has tumors , or the exclusion of transplant is occurred, the lymphocyte will increase.In the other side, when the immunity is deficient , the lymphocyte will decrease. If people cured with cortin, do you know cortin? It is a hormone produced in kidney, it can restrain the immune system. Certain disease such as SLE , RA or people has transplant, it is commonly used. Moincreasing:certain infections(endocarditis),certain hematonosis( M5 )decreasing:no significancePLT related parametersThe number of platelets(PLT)normal value: (100-300)×109/LMean platelet volume(MPV)Platelet distribution width(PDW)MPV Similar with MCV , PDW similar with RDW.第二节血细胞自动化分析及临床应用1.血细胞自动化分析原理:1)三分类:电阻法原理(coulter原理)50年代初,库尔特(Coulter)发明并申请了粒子计数技术的设计专利,其原理是由于电解质是导体,血细胞是不良导体,当血细胞通过小孔时,会引起一个瞬间的电阻变化,将电阻的变化量转换成脉冲,脉冲的数量代表血细胞的数量,脉冲的大小反映血细胞的大小,血细胞类型根据细胞大小来判定。
Clinical Chemistry Examination临床检验
3. Normal value
Adult: TP: 60~80 g/L ALB: 36~50 g/L GLB: 24~30 g/L A/G: 1.5~2.5 : 1
Newborn: TP: 46~70 g/L ALB: 28~44 g/L GLB: 18~26 g/L
肝中 肌红蛋白、游离血红素 (分路胆红素)
非结合胆红素 ALB
blood
葡萄糖醛酸
liver
ALB
结合胆红素
随胆汁排泄
肝肠循环
尿胆原
门静脉
small intestine、colon
随粪便排出
经肾随尿排出
2.Normal value
⑴ STB Newbron 0~1 days: 34~103 μmol/L
丢失过多(肾病、烧伤、失血等)
GLB ↑: 慢性肝病 M蛋白血症(多发性骨髓瘤、淋巴瘤、巨球蛋 白血症) 自身免疫性疾病(SLE、风湿、类风湿) 慢性炎症和慢性感染(结核、麻风、疟疾)
GLB ↓: 生理性(3岁以下婴幼儿) 免疫功能抑制 先天性低球γ-蛋白血症 A/G 减低或倒转: 严重肝病和M蛋白血症
⑴ Serum Total Bilirubin
①判断黄疸有无及性度(隐/轻/中/高)μmol/L
②黄疸类型 阻塞性黄疸
340—570
不全梗阻性黄疸 170—265
肝细胞性黄疸
17—200
溶血性黄疸
<85
③结合血清胆红素分类判断黄疸类型
STB↑ UCB↑
溶血性黄疸
STB↑ CB↑
阻塞性黄疸
血液检验血常规检验英文缩写
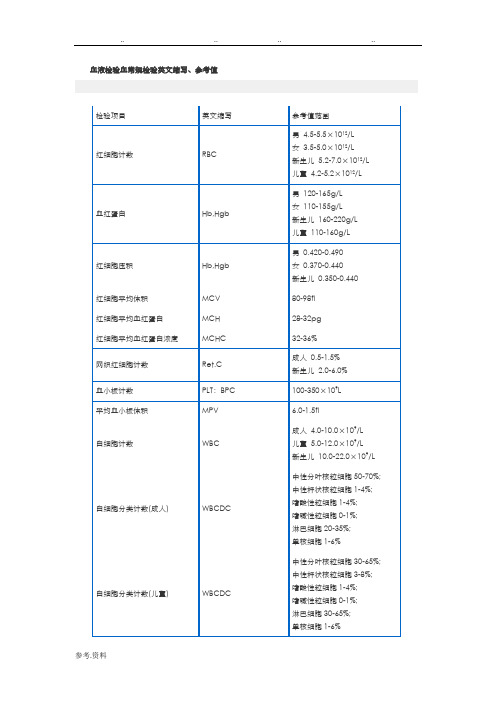
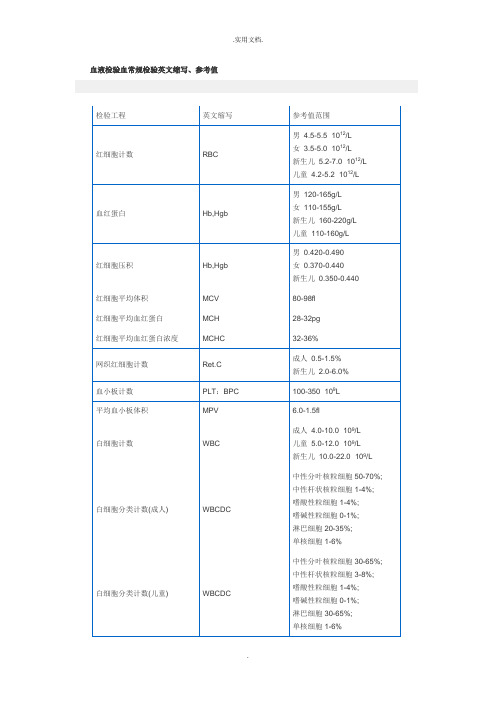
血液检验血常规检验英文缩写、参考值检验项目英文缩写参考值范围红细胞计数RBC 男4.5-5.5×1012/L女3.5-5.0×1012/L新生儿5.2-7.0×1012/L 儿童4.2-5.2×1012/L血红蛋白Hb,Hgb 男120-165g/L女110-155g/L新生儿160-220g/L 儿童110-160g/L红细胞压积Hb,Hgb 男0.420-0.490女0.370-0.440新生儿0.350-0.440红细胞平均体积MCV 80-98fl 红细胞平均血红蛋白MCH 28-32pg 红细胞平均血红蛋白浓度MCHC 32-36%网织红细胞计数Ret.C 成人0.5-1.5% 新生儿2.0-6.0%血小板计数PLT:BPC 100-350×109L 平均血小板体积MPV 6.0-1.5fl白细胞计数WBC 成人4.0-10.0×109/L儿童5.0-12.0×109/L新生儿10.0-22.0×109/L白细胞分类计数(成人) WBCDC 中性分叶核粒细胞50-70%; 中性杆状核粒细胞1-4%; 嗜酸性粒细胞1-4%;嗜碱性粒细胞0-1%;淋巴细胞20-35%;单核细胞1-6%白细胞分类计数(儿童) WBCDC 中性分叶核粒细胞30-65%; 中性杆状核粒细胞3-8%; 嗜酸性粒细胞1-4%;嗜碱性粒细胞0-1%;淋巴细胞30-65%;单核细胞1-6%嗜酸性粒细胞直接计数Eos.c 0.05-0.3×109/L出血时间BT 1-3分钟凝血时间玻片法CT 1-4分钟凝血时间试管法CCT 5-10分钟(以第3管时间为准) 血块收缩时间CRT 24小时完全收缩红细胞沉降率ESR 魏氏法:男:<15mm/第一小时女:<20mm/第一小时一氧化碳定性实验阴性(反应呈绿褐色) 阳性(反应呈橙红色)全血细胞分析BCA 以上同血细胞检查正常值(包括WBC;HGB;RBC;HCT;HCH;MCHC;MCV;PLT)尿常规检验英文缩写、参考值·labsky 发表于2006-7-6 14:00:31检查项目英文缩写参考值范围血糖Glu 3.89~6.11mmol/L 尿素UREA 3.0~7.2mmol/L尿酸UA 成人男性:210~420 umol/L女性:150~350 umol/L 儿童120~320 umol/L肌酐Cr 男:44~80 umol/L 女:70~115 umol/L二氧化碳结合力CO2-CP 20-34mmoI/L 钾K 3.5-5.5mmol/L 钠Na 135-45mmol/L 氯化物CL 96-106mmol/L钙Ca 成人2.03~2.54 mmol/L 儿童2.25~2.67 mmol/L磷P 成人0.96~1.62 mmol/L 儿童1.45~2.10 mmol/L淀粉酶 AMS <220u/L胆固醇 Chol 2.23~5.17 mmol/L 载脂蛋白A1 载脂蛋白B ApoAI ApoB ApoAI 1.00~1.60 g/L ApoB 0.60~1.10 g/L 甘油三酯 TG 0.56~1.69 mmol/L 肌酸激酶 CK 18~196u/L高密度脂蛋白 HDL-C 男 0.90~1.45 mmol/L 女 1.15~1.68 mmol/L 低密度脂蛋白 LDL-C 1.3~4.0 mmol/L 总胆红素 T-BIL 5.1~22 umol/l 直接胆红素D-BIL 1.7~6.8 umol/l 谷丙转氨酶/丙氨酸氨基转移酶 SGPT/ALT <40u/L 谷草转氨酶/天门冬氨酸氨基转移酶SGOT/AST <35u/L 乳酸脱氢酶 LDH 97-270Iu/L γ-羟丁酸脱氢酶 α-HBDH 72-182Iu/L 碱性磷酸酶 ALP 27-107u/L 酸性磷酸酶ACP男<4.7 女 <3.7 γ-转肽酶 γ-GT 男10~50u/L 女 7~32u/L 总蛋白 TP 60~80g/L 白蛋白Alb35~55 g/L 蛋白电泳 SPE白蛋白:54-74%球蛋白α1 0.5-5.0%α2 3.6-10% β5.0-12.5% γ10-24%乳酸脱氢酶同功酶 LDHIsoLDH 4 21-33% LDH 2 34-46%LDH 3 23-32% LDH 4 1-6% LDH 5 0-6%肌酸激酶同功酶CPKIso MB<6%CK-m B MM>93%碱性磷酸酶同功酶ALPIso 肝带31.1-64.6%脂蛋白电泳骨带33.1-64.6% HDL 男31;女38 LDL 男63;女56 VLDL男6.8;女9.3总胆汁酸TBA 0~12 umol/L前白蛋白PA 220~440 mg/L阴离子隙AGP 8~16 mmol/L镁Mg 0.67~1.04 mmol/L血清铁Fe 男性11~30 umol/L 女性9~27 umol/L糖化血红蛋白HbAlc HbAlc占总血红蛋白的6.5+1.5%;>8.0%为HhbAlc增高甲胎蛋白AFP 0~10 ng/ml免疫检验英文缩写、参考值·labsky 发表于2006-7-8 8:59:38实验名称实验方法参考值RF(类风湿因子)免疫速率比浊法0一20 IV/MLASO(抗链球菌溶血素“O”)免疫速率比浊法0一200IV/MLCRP(C反应蛋白)免疫速率比浊法0一8MG/DLIgG(免疫球蛋白IgG)免疫速率比浊法723一1685mg/dLIgA(免疫球蛋白IgA)免疫速率比浊法69一385mg/dLIgM(免疫球蛋白IgM)免疫速率比浊法63一277mg/dL补体C 免疫速率比浊法85一193mg/dL补体c 免疫速率比浊法12一36mg/dL脑脊液IgG 免疫速率比浊法0一6mg/d脑脊液IgA 免疫速率比浊法<1.1mg/dL脑脊液IgM 免疫速率比浊法<0.7mg/dL尿MA(微量白蛋白)免疫速率比浊法0一1.9mg/dL尿aM(微球蛋白)免疫速率比浊法0一1.3mg/dL尿TRU(转铁蛋白)免疫速率比浊法0一0.2mg/dL尿IgU(免疫球蛋白IgG)免疫速率比浊法0一0.1mg/dL HBSAG(乙型肝炎病毒抗体)ELISA 阴性anti-HCV(丙型肝炎病毒抗体)ELISA 阴性RPR(梅毒快速血浆凝集素反应)凝集法阴性THPA(梅毒抗体检测)明胶凝集阴性抗结核抗体ELISA 阴性抗幽门螺杆菌抗体ELISA 阴性嗜异性抗体检测胶乳凝集阴性支原体抗体明胶凝集滴度<1:40军团菌抗体凝集反应各血清型滴度均<1:8O肥达氏抗体凝集反应TO<1:80TH<1:160付伤寒A.B.C<1:80外斐氏反应凝集反应OX19,OX2,OXk<1:160 冷凝集反应凝集反应滴度<1:32检验项目英文缩写参考值范围红斑狼疮细胞LEC 阴性抗核蛋白试验DNP 阴性抗核抗体试验ANA <1:5~1<1:10抗平滑肌抗体SMA <1:10抗线粒体抗体AMA 阴性抗心肌抗体HRA 阴性抗胃壁细胞抗体APCA 阴性抗骨骼肌抗体ASA 阴性抗甲状腺抗体(球蛋白) ATGA 阴性抗甲状腺抗体(微粒体) ATMA 阴性抗dsDNA抗体(Farr) ds-DNA <20% 抗dsDNA抗体(TE-IF) ds-DNA 阴性抗肾上腺抗体阴性抗着丝点抗体ACA 阴性梅毒抗体试验FTA-ABS 阴性抗胰岛细胞抗体ICA 阴性囊虫酶联免疫吸附试验间接血凝试验OD值〉0. 23血清效价在1:10(++)均为阳性肝包虫酶联免疫吸闲试验间接血凝试验OD值〉0.23血清效价在1:IO(++)均为阳性血吸虫Cag酶联免疫吸附试验IgGlgM 比弱阳性深者判为阳性OD值0.30比弱阳性深者判为阳性肺吸虫酶联免疫吸附试验OD值〉0.30旋毛虫酶联免疫吸附试验OD值〉0.30丝虫酶联免疫吸附试验OD值〉O.30弓形虫酶联免疫吸附试验OD值〉阳标的2.l倍者判为阳性已累热病酶联免反吸附试验OD值〉0.30阿米已酶联免反吸附试验OD值〉0.30钓端螺旋体酶联免疫吸附试验比弱阳性深者判为阳性莱姆病抗体检测比弱阳性深者判为阳性布氏杆菌凝集试验血清效价在1:IO0(++)均为阳性琥红试验任何程度的凝集均为阳性放射免疫检验英文缩写、参考值·labsky 发表于2006-7-8 9:00:59实验名称实验方法参考值三碘甲状腺原氨酸T3 化学发光法50-220ng/dl甲状腺素T4 化学发光法44-116ng/ml 甲状腺素摄取率Tu 化学发光法35-45%促甲状腺素TSH 化学发光法0.34-5.6uu/ml 游离三碘甲状腺素F3 化学发光法 2.4-5.6Pg/dl 游离甲状腺素F4 化学发光法0.87-1.56ng/dl 绒毛膜促性腺激素HCG 化学发光法<20u/ml皮质醇化学发光法86-23ug/dl 43- 11ug/dl泌乳素化学发光法男5-35ng/ml 女7-47ug/ml铁蛋白化学发光法男24-336ng/ml 女11-306ng/ml叶酸化学发光法3-17ng/ml维生素B12 化学发光法〈185pg/ml有意义胰岛素释放试验化学发光法空腹1.9-2.3uu/ml 餐后lh 32-119un/ml 2h 20-96un/ml3h 1.8-43uu/mlTG抗甲状腺球蛋白抗体放射免疫分析法阴性TG抗微粒体抗体放射免疫分析法阴性INS-AB胰岛素抗体放射免疫分析法<3.5%结合率C-P C-肽释放试验放射免疫分析法空腹295-378Pml/L 餐后1 937-1760pml/L2 863-1567pml/L3 650-939pml/LPTH甲状旁腺素放射免疫分析法10-70Pg/ml CT降钙素放射免疫分析法<50Pg/mlHGH生长激素放射免疫分析法10岁以上2-8ng/ml 10岁以下1-10ng/mlT睾酮放射免疫分析法男360-910ng/ml 女21-91ng/dlE2雌二醇放射免疫分析法男0-70Pg/ml 女25-30pg/mlPROG孕酮放射免疫分析法滤泡期0.14-1.61ng/ml 黄体期2.14-31.2ng/mlB2-MG微球蛋白放射免疫分析法 1.17-Z 29ug/mlALD醛固酮放射免疫分析法卧60-174pg/ml 立63-300Pg/ml胃泌素放射免疫分析法<146pg/ml 胆酸放射免疫分析法<260ng/ml肾素活性放射免疫分析法卧40.2 0.37mg/ml小时立2.97 1.02mg/ml小时血管紧张素放射免疫分析法卧40.2 12.0mg/ml小时立85.3 30.0mg/ml小时TRAB(TSH受体抗体)放射免疫分析法<13U/L血气检验英文缩写、参考值·labsky 发表于2006-7-8 9:03:20 英文缩写测定方法中文名称参考值范围血气血氧分析电解质测定PH 电极法血浆PH值7.35-7.45PCO2电极法动脉血二氧化碳分压35-45mmHgPO2电极法动脉血氧分压>90mmHg,随年龄增长逐渐降低CTHB 分光光度计法总血红蛋白13.8-16.4 g/mg(m)11.7-14.6 g/ml(f)SO2分光光度计法动脉血氧饱和度>95%FO2HB分光光度计?/TD>氧和血红蛋白百分含量94%-98%FCOHB 分光光度计法碳氧血红蛋白百分含量<1.0%FMETHB 分光光度计法高铁血红蛋白百分含量<1.0%FRHB 分光光度计法脱氧血红蛋白百分含量<6%乙型肝炎病毒血清学检查名称分析HBsAg 阳性见于急慢性乙型肝炎或健康携带者抗-HBs 阳性示乙型肝炎恢复期或注射过乙型肝炎疫苗抗-HBc 阳性示已受乙型肝炎病毒感染HBeAg 阳性为乙型肝炎病毒复制的标志抗-HBe 阳性示相对低的传染性HBv DNA 阳性为乙型肝炎病毒复制的最敏感指标乙型肝炎五项检验内容的阳性和阴性结果可能有各种不同的组合方式,下面例举的10个模式可帮助你对不同的组合进行分析和判断。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Introduction to Practical Haemmatology Introduction:-In the past humankind know about presence of blood, but a few centuries back science discovered that this blood circulates in our body. In Greek, Roman, and Unani medicine describe some disease due to blood abnormalities into: traumatic, inflammatory, infective, and neoplastic.DEFINATION OF BLOOD:Blood is highly specialized (sterile) connective tissues, which circulate in a closed system of vessels as a liquid with red coluor, but in out this system a solid phase will perform, which we called plug or blood clot.Haematology: is the science that study the blood, and it's structure, function, disease, and the convenience between structure and the function.BLOOD COMPONENTMainly we can divide blood into two parts:1) Plasma 2) Blood cells.The total amount of blood approximately 1/14 of the total body weight or 60-70 ml/ each kilogram of body weight.Blood flows through every organ of the body providing effective communication between tissues.PLASMA:Plasma is a pale yellow fluid in which blood cells are suspended in.Plasma forms about 55% of blood volume and composed of 95%or more water, and many solutes including proteins, minerals, ions, organic materials, hormones, enzymes, products of digestion, and waste products.BLOOD CELLS:1) Red blood cells (RBC).2) White blood cells (WBC).3) Platelets.FUNCTION OF BLOOD:□ Transportation and distribution:- Oxygen transportation by haemoglobin from lungs to the tissues.- Blood also can transport the nutrients absorbed by the digestive system to the tissues for use or storage.- Hormones are carried from endocrine glands to the organs.- Wastes are transported from tissues for excretion e.g.: carbon , dioxide, urea, createnine,…□ Regulatory:- Plasma maintain the PH. of blood (7.35-7.45), and in the tissues .- Osmotic pressure in plasma is regulate by proteins and salts (sodium, chloride) to prevent excessive loss of fluids from the blood into tissues.- Regulation of the body temperature.□ Protective:- Platelets and coagulation factors control the blood loss by thrombous formation.- Leukocytes defend and produce antibodies and toxin against infection and tumor cells.HAEMATOPOIESIS:In normal healthy person there is a constant break down and new formation of cells, and the procedure of blood cells formation called Haematopoiesis.NORMAL SITES OF BLOOD FORMATION:- Fetus:* Less than 2 months: in Yolk sac.* 2-7 months: in the liver and a few in the spleen.* Full term: in bone marrow for RBC, PLTs, and granulocytes, but lymphocytes and monocytes occures in spleen, lymph nodes and lymphoid tissues (liver and bone marrow with less numbers).- After birth:Mainly from bone marrow even monocytes, except lymphocytes still from spleen and lymph tissues.- In adult:Main sites of haematopoiesis are the vertebrae, ribs, sternum, skull bones, pelvis, sacrum, and proximal ends of femur and humerus.Haematopoiesis can be sub-divided into 3 stages:1) Mesoblastic period.2) Hepatic period.3) Myeloid period.ABNORMAL SITES OF HAEMATOPOIESIS:In certain disorders the fetal haematopoitic organs revert to their old function supported by the reticulum cells, this occurs when bone marrow can not fulfill the requirements or demand for new cells, this called EXTRA-MEDALLARY haematopoiesis, (Myeloid metaplasia).In some rare cases adrenal glands, cartilages, adipose tissues, intra thoracic areas, kidneys, and endo-sternum can produce blood cells.PRE-ANALYSIS MANAGEMENTThe clinical laboratory is useful to assist in diagnosis, and management of patient.A test request is a request for consultative services, to generate a laboratory report using to make clinical judgments.- Understanding of the test process and procedures, collection, and handling enables the laboratory staff to achieve more nearly optimal conditions and consequently to improve the accuracy and precision of each measurement.REASONS FOR ORDERING LAB. REQUEST:1) To confirm a clinical impression or diagnosis.2) To rule out a diagnosis.3) To monitor therapy.4) To establish prognosis.5) To screen for or detect disease.TEST REQUESTATION:The physician initiates the test request by writing an order for lab. examinations in the patient medical chart/record.- The orders are carry out to an appropriate lab. request form by the nursing station or secretary unit.- Each laboratory form has a list of test with reference intervals and a space for the result.- Patient data (demographics) include, patient name, sex, age, date of admission, date of test ordering, room number,……..must be clearly writing on the request, or patient's addressograph plate or computerized label are stamped onto the request.- The requests are given to the collect unit or to the phlebotomist /nurse to draw the specimen, specimen tube must be labeled be for the specimen is drawn.☼ It is essential to follow strict quality control procedures through all stages of test request to avoid several possible errors, such as, incorrect or missing test entering, ……- All requests should have a full, clear patient data, and correct sample labeling.- Samples quantity and anticoagulant should be suitable, and with no haemolysis, or clot.BLOOD SPECIMEN COLLECTION:A. SKIN PUNCTURE:Skin puncture is the method of choice in pediatric patients, especially infants.- Skin puncture can be used in adults with:* extreme obesity.* sever burn.* thrombotic tendencies.Technique:1) Select an appropriate puncture site, lateral or medial plantar heel surface for infants, in olderinfants the palmer surface of the last digit of the second, third, or forth fingers (big toe, and ear lobe can be used).-The site of puncture must not be edematous or a previous puncture site.2) Warm the puncture site with a warm moist towel, and clean the puncture site with 70%of aqueous isopropanol solution, allow the area to dray.3) Make the puncture with a sterile lancet with blade no longer than 2.4 mm.4) Discard the first drop of blood by wiping it away with a sterile pad.5) Collect the specimen in a suitable container (oral aspiration of blood is discouraged for a safety reasons ).5) Label the specimen container.B. VENOUS PUNCTURE:Technique:1) Identify the patient by checking identification card against the request, ask the conscious patient his/her full name and birth date (do not draw any specimen without properly identification).2) If fasting specimen is required , confirm that the fasting order has been followed.3) Inform the patient, what is to be done and reassure the patient to avoid as much tension as possible.4) Position the patient properly for easy, comfortable access to the antecubital fossa.5) Assemble equipments and supply (tubes, tourniquet, syringes…..).6) Ask the patient to make a fist –to make the veins more palpable – then select a suitable vein (veins of atecubital fossa , in particular the median and cephalic veins are preferred), wrist , ankle, and hands veins may also be used.If one arm has an intravenous line , use the other arm to draw a blood sample.7) Clean the venipuncture site with 70%isopropyl alcohol solution in a circular motion and allow the area to dray.8) Apply a tourniquet above the puncture site, "never leave the tourniquet longer than 1min.9) Use your thumb and middle finger or thumb and the index finger, to anchor the vein.10) Enter the skin with the bevel of the needle at 15 degree angle, to the arm with the arm, with the bevel up , insert the needle smoothly, and fairly fast.- If using a syringe pull pack on the barrel with a slow until the blood flows into the syringe (do not pull back too quickly to avoid the haemolysis or collapsing the vein).- If using a vacutainer, as soon as the needle is in the vein ease the tube fore ward in the holder, at the same time hold the needle firmly in place.11) At the end of the collection release the tourniquet.12) After all blood samples have been drawn, have the patient relax his fist.13) Place a clean, sterile, dray cotton ball over the site and withdraw the needle , and apply a pressure to the site , and bandage the arm.14) Mix the blood with the anticoagulant.15) Check the patient condition e.g.: whither he is faint, bleeding is under control,…..16) Dispose the contaminated materials.C. ARTERIAL PUNCTURE:Arterial blood is used to measure oxygen, carbon dioxide , and measurin g PH.,…Arterial punctures are technically more difficult to perform.Technique:1) Select the puncture site, the radial artery is the most common site, if the ulnar artery is absent, do not puncture the radial artery (use the Allen test to make sure of collateral circulation ).The femoral artery and the brachial artery, at the antecubital fossa provide alternative sites for puncture, scalp arteries are used in infant.2) Anesthetized the puncture site if necessary, prepare the syringe by aspirate an anticoagulant (usually heparin).3) Record the patient temperature and perform Allen test (for radial artery puncture) as follow:- compress the radial and ulnar arteries at the wrist until the palm of the hand becomes blanched. - Release the pressure from ulnar artery and observe that the hand becomes flushed, if the hand remains blanched DO NOT puncture the radial artery.4) Clean the site, place a finger over the artery and puncture the skin 5-10mm. distal to the finger . - Blood rushing into the needle, or pull back on the plunger and obtain the required amount of the blood.5) Quickly withdraw the needle and syringe , place a sterile cotton ball or dry gauze over thepuncture site.6) Apply firm pressure for at least 5 min.7) Expel any air bubble from the syringe.8) Remove the needle and cap it with a tight –fitting "Luer cap" and mix the anticoagulant by gentile inversing of the syringe.9) Label the sample and place it in an ice/ice water bath.10) Transport the sample on ice immediately to the lab.* Drawing problems:Occasionally, the phlebotomists are unable to obtain blood by ordinary venipuncture.- In some cases a skin puncture may suffice; if not, a physician draws the specimen using most commonly the femoral vain or jugular vain in children.REAGENTS:Reagent contain chemicals exist in varying degrees of purity. –all reagent should have a label identify the concentration , purity, amount, and compou nds,….- Reagents or chemicals arrived into lab. with a certain guarantee of purity ;once the seal is broken, the guaranteed analysis is strictly in the hands of the receiving lab.- Definite steps must be taken to ensure that the reagent/ chemicals are handled under optimal condition.- It extremely important to read the label for proper storage .- Never sample directly from the reagent bottle.- It essential that each lab. first evaluate a kit / reagent according to an established protocol, then monitor kit/reagent performance by appropriate quality control procedures.- In generally distilled water and deionized water most commonly used to prepare reagents.- The College of American Pathologist has drawn up specification and methods of quality control for reagent water.* Three grades of water are defined:▫ Type I reagent water:For procedures which require maximum water purity- Preparation of standard solutions- Ultra micro-chemical analysis.- Measurement of nanogram or sub nanogram concentration.▫ Type II reagent water:For most lab. testing, in chemistry, haematology, immunology, and other clinical tests.▫ Type III reagent water:For most qualitative testing; most procedure in urinalysis, parasitology and for washing glass ware. * Carbon dioxide free water is used in gasses such as Co2 , ammonia and O2 may affect analysis.SOME METHODOLGY PRINCIBLS USED IN CLINICAL LABORATORY□ PHOTOMERTRY:Photometric measurement defined as measurement of light intensity of multiple wave length. SPECTROPHOTOMETRY: meant measurement of light intensity in a much narrower wave length range.□ FLAME PHOTOMETRY:Heat energy of a flame makes the electrons in an atom excited and being unstable, then the electrons give up their excess energy to the environment as they change from the higher energy state (level) to a lower energy state as light, the light may consist of one or more than one energy level, therefore many different wave lengths; these wave lengths are individually characteristic for each element.□ FLUOROME RTRY:Fluorescence is a physical energy process that occurs when certain compounds absorb electromagnetic radiation and become excited, and then return to energy level slightly higher than or equal to their original energy level , the energy given off is less than or equal to that absorbed, and wave length will be longer or equal to that absorbed for excitation.□ TURBIDIMETRY:Turbidimetry measures the amount of light blocked by particulate matter as light passes throughthe cuvette.□ POTENTIOMETRY:The measurement of the potential voltage between two electrodes in solution from the basis for a variety of measurement that can be used to quantitate concentration of substance of interest.□ ION SELECTIVE ELECTRODES (ISE):There are three different basic ISE. Classes:- Ion selective glass.- Solid state electrode.- Liquid ion exchange membranes.□ CHROMATOGRAPHY:The purpose of chromatography involves separation of a mixture on the basis of specific difference of the physical – chemical characteristics of the components.* Steps involved in requesting, performing, and evaluating measured quantity :(I) Physician request a quantitative measurement of a constituent in biological specimen.(II) Laboratory personnel perform the assay:A. Pre-instrumental phase1- Preparation of the patient.2- Obtain the specimen3- Processing the specimen4- Storing the specimen prior the measuring steps.B. Instrumental phase1- Dispending a sample aliquot into a reaction vessel2- Combining the sample with one or more reagent3- Recording some physical/chemical consequence of the reaction4- Calculate the value of the quantity measuredC. Post-instrumental phase1- Lab. staff accept the value (result) as being of good quality2- The report is sent to the requesting physician(III) Physician evaluates the report:A. Physician assesses whether the measurement could be consistent with other known patient informationB. The physician makes a clinical decision at least partially based on the report measurement.INTRODUCTION TO QUALITY CONTROLClinical laboratories perform quantitative, semi-quantitative, and quantitative tests on a variety of biologic specimens.The basic principles on quality controls were set by "Shewhart" in 1931, the ways in which these basic principles have been extended to develop systems of quality assurance have been revered by" Grannis" (1977).The immediate aim of quality control is assure that the end product of the analytical values regularly produced by a clinical laboratory are sufficiently reliable for their intended use, and to assure that the laboratory procedure analytical values that meet acceptable standard of precision, and accuracy at all times.To attainment of these aims requires that all lab. personnel, technologists, supervisors, and directors be knowledgeable of the causes of the analytical inaccuracies and of the techniques that available for their detection, correction, and control.Quality control in laboratory medicine has been defined as the study of those errors which are responsibility of the laboratory to recognize and minimize them.An alternative term "quality assurance" has been used to represent the techniques available to ensure with a specified degree of the confidence that the result reported by the laboratory is correct.In order to have such confidence, the laboratory director must be assured that there is both "precision control and accuracy control" performed.♦ Quality control can be divided into two major types: Internal QC and External QC.Laboratory managementThe purely scientific and clinical approach to laboratory medicine is no longer sufficient. The bridge between the basic sciences and clinical medicine is now buttressed by essential support derived by form computer sciences , management techniques ,and industry. In recent years the relationship between laboratory medicine and industry has become bi-directional.In addition to the patient care service role , most individuals in laboratory medicine also have role as educator and many have roles as research and developmental scientists.To be successful person in laboratory medicine , must be skilled in all these functions and be aware of all those external influences affecting the practice of laboratory medicine.The five characteristics essential to success for an executive in medical laboratory :Motivation & skills.Vision & knowledge.Decision making ability .Good health & fitness (physically and mentally).Humility and recognition of other favor.The ten indicators of lack of management and communication skills in medical laboratory . Inability to maintain an adequate staff.Recurring or persistent misunderstanding with the hospital administration.Frequent or recurrent confusion concerning requisitions or reports of laboratory work.Frequent rush order for supplies.Low morale in the laboratory.Requests for deserved pay raise by competent workers.Excessive cost of operation.Ignorance of the cost of operation .Expenditure of much of the director's time in making decisions.Inability to do one or more tests when a "key individual" has a day off.Motivation:Maslon develop a theory of human motivation based of the belief that man is a wanting "animal".X- management theory :Based on the assumption that people dislike work ,that they have to be driven , threatened and punished to achieve goals, and that they lack ambition and want only security .Y- management theory:Based on assumption that work a natural need as natural as rest or play ; people don’t have to be threatened or forced to work , and people want responsibility in the proper environment when given the opportunity .Although theory X and theory Y may be considered as "extremes" in styles of management.Z- management theory:A new approach suggests that the involvement of workers is a key for increased productivity , motivation of employees may be enhanced by combination of trust , subtlety and intimacy provided by management.The director or supervisor must be able to use the appropriate management tool for the situation or person with which one is dealing at the moment.There are others management styles like, objective management and total quality assurance management.Personnel management:Policy manual:All laboratories should have readily available administration police manuals.Job description :Is a summary of all the important or significant fact about a particular job.Job description should have a clear and easily understood description for the duties and responsibilities for the employees, It also helpful to define the purpose of the job and to show it's relationship to other jobs in the organization.Position classification :Job description and class or kinds of the employees are the basis upon which the individual positions are assigned at the appropriate level (class).Orientation:The important step of introducing the employee to his/her new environment comes after the selection and hiring process. An orientation program is a probably on of the most overlooked tools available to the manager.In service continuing education:Because of the rapidly changing nature of laboratory medicine , it is essential to have a continuing education programs .The staff should be given the time and encouraged to attend appropriate meeting programs in laboratory medicine.Intra laboratory staff meetings:Meeting of the laboratory director ,supervisors , and staff should be held on a regular basis to discuss.(Administrative professional and technical problems:Periodic full laboratory staff meeting are also useful as a forum for discussingproblems , new policies and procedures and planning ).Personnel records :Access to confidential and personal information should be limited to appropriate individuals.Evaluation:An important part of employee development , is evaluation of performance.Discipline and Dismissal :Because of the seriousness of some acts, the laboratory director or supervisors may elect the acceptable discipline actions depend on the type of infraction and the circumstances surrounding it , some acts needs to recommend dismissal of the employee immediately.However, the procedure for such dismissals would include consultation with personnel department .Success in handling disciplinary problems comes with consistency of approach , promptness and equity in dealing with all personnel.ANTICOAGULANTSAnticoagulants are substances (natural made e.g. heparin or industrial synthetic) used to prevent clot formation of the blood.Before taking a blood sample for haematologic analysis; it is important to mix the blood sample thoroughly. If the tube has been standing , this requires at least 60 gentle inversion of the tube or two minutes on a mechanical rotator.Precaution must be taken to prevent errors in analysis of blood cells as result of in vitro change in EDTA. blood.In blood kept at room temperature, swelling of erythrocytes between 6-24 hrs. raises the hematocrit and MCV. and lowers MCHC. and ESR.Ethylene diamine tetra acetic acid:- Acts as chelating agent by removal of calcium ions.- The most widely common used anticoagulant for haematologic procedures.- Useful for CBC, blood films, platelets count (because it prevents platelets clumping).- EDTA. Is not useful for factor V and VIII assay.* Preparation:□ LIQUID FORM:- Dissolve 3gm. of EDTA. salt in 100 ml. of 0.7% aqueous NaCl solution.- Use 0.5 ml. for each 9.5ml. of blood.□ DRAY SALTS:- Dissolve 10 gm. of EDTA. salts into 100ml. of distilled water.- Pipette 0.1 ml. of this solution into each container (vial) to be used for 5ml. of whole blood specimen collection.- Allow to dry at room temperature or into oven at low temperature , without cover, put cover after dry.2) HEPARIN:- Naturally producing by liver.- Neutralize thrombin which prevents the blood clotting mechanism.- Useful for red cell fragility test, electrolytes studies, L.E.cells.- Not useful in CBC, blood films.3) SODIUM CITRATE:- Sodium citrate combines with calcium to form insoluble calcium citrate.- 3.2% sodium citrate is the most commonly used for coagulation studies (1volume of anticoagulant to 9 volume of blood).- For ESR. ( 4 volume of tri sodium citrate to 1volume of blood).4) ACID CITRATE DEXTROZE (ACD):- Commonly used in blood banking.- 63 ml. of ACD. is sufficient for 450ml. of whole blood.5) OXALATE:- Sodium oxalate can be used in chemistry, haematocrite, coagulation tests.- Replaced by Sodium citrate.- Double oxalate is replaced by EDTA.PREPARATION OF BLOOD FILMS*THICK BLOOD FILM:- A large drop of blood is taken on the centre of a clean labeled slide ( a drop of finger puncture or from well mixed EDTA. tube of blood by capillary tube or pipette).- With an other slide corner spread the drop over 1/2 an inch square area (20 mm.) in diameter.- When dry the thickness should be such that printed litters can be seen through it.- Thick blood films used for detecting Malaria parasites and Microfila ria …..* THIN BLOOD FILM:Making of spreaders:- Select a slide with smooth edge ( a high quality polished side slides can be used).- Using a glass cutter, cut across a corner of the slide.- Break off the corner by holding the slide corner between piece of cloth.Making a thin film:- Put one small drop of blood on a clean (grease-free) labeled slide.- Hold the spreader at 30-45degree angle against the surface of the slide.- Move the spreader back to touch the drop of blood and allow the blood to extend along the edge of the spreader.- Push the spreader with a steady hand across the slide.- Air dry the film.FIXING OF THIN BLOOD FILMS:* With absolute methanol, by immersing in a container of absolute methanol for 2 minutes.* When absolute methanol is no available absolute ethanol can be used.* Methanol containing water must not be used to fix blood films.STAINING OF THIN BLOOD FILMSRomanowsky stain :-Stains contain Eosin Y (acidic) and Azure B and other thiazine dyes "Methyline Blue" .Eosin stains the basic components of blood cells e.g. haemoglobin stains Pink-Red and granules of eosinophils stains Orange -Red .Azure B and Methylene blue stain the acidic component of cells.Buffers:-The ideal PH for staining blood films is 6.8 and in order to maintains this , buffered distilled water is used .Buffer solution :--sodium hydroxide (NaOH) 8gm.-distilled water 1000cc-Potassium dihydrogen phosphate (KH2Po4 ) 27.2gm.-distilled water 1000cc.Take 23.7 cc of solution 1 , add 50cc of solution 2.Take 20cc of distilled water.To make 1 liter PH 6.8 buffer water using Na2HPo4 and KH2Po4 :-Di-sodium Hydrogen Phosphate anhydrous (Na2HPo4)----- 0.47gPotassium di-hydrogen phosphate anhydrous (KH2Po4 )----- 0.46gDistilled water-----up to 1 liter.Giemsa stain 500 ml stock :-Giemsa powder---------------------------3.8gmGlycerol-----------------------------------250 mlMethanol----------------------------------250 mlweight giemsa powder and put it in 500 ml dry browen bottle with a few glass beads.place the bottle of stain I water bath at 50-60 c for 2 hours.measure the methanol and add it to the stain mix well.label the bottle.filtrate the stain before using.Leishman stain 400 ml :-Leishman powder -------------------0.6gMethanol -----------------------------400mlweight the stain powder on a dark brown bottle with a few glass beads.measure the methanol and add it to the stain ,mix well.place the bottle at 37 c water bath to help to dissolve the dye.label it and keep it at room temp.filtrate the stain before using.New methylene blue (100 ml "1%w/v):-new methylene blue powder ----------------------1g.soudium citrate -------------------------------------0.6gsodium chloride ------------------------------------0.7gdistilled water---------------------------------------100mlweight the sodium citrate an sodium chloride then dissolve both in distilled water. add the new methyline blue powder and mix it and put it in dark brown bottle.lable it and filtrate befor using.Wright's stain (400ml):-wright's stain powder -------------------------1gmethanol --------------------------------------400mlweight the wright's stain powder and put in dark brown bottle with a few glass beads.place the bottle in 37c water bath to help day to dissolve.label the bottle.allow 3-5 days before using the fresh stain , filtrate before using.Fields stain:-Stain A:methylen blue powder ------------------1.3gdi-sodium hydrogen phosphate -------12,6gpotassium di hydrogen phosphate ----6.25gdistilled water ---------------------------500mldissolve the methylene blue and di- sodium hydrogen phosphate in 50 ml of distilled water in flask. put the flask in water bath at 50-60c for half hour.dissolve the potassium dihydrogen phosphate in 450ml of distilled water and add it to the flask mix it well and keep it for 24 hour and filtrate.Stain B:eosin powder ---------------------------------1.3gdisodium hydrogen phosphate ------------12.6gdistilled water --------------------------------500mldissolve the stain powder with the disodum hydrogen phosphate in 50 ml of distilled water.mix it well in water bath at 50-60c.add potassium di hydrogen phosphate to 450ml distilled water and add it to the flask.keep it for 24hour and filtrate befor using.For staining:Dip the dry thick film in methanol for 1-2 sec.Dip the smear in stain A for 1-2 sec then in stain B for 1-2 sec.Dip the smear at buffered water for a few second and allow to dry.。