涎腺病理
涎腺腺泡细胞癌临床病理分析

发病年龄
主要发生于中老年人,但 也可见于年轻人。
临床表现及诊断意义
症状
主要表现为无痛性肿块,位于腮 腺、下颌下腺等涎腺部位。部分 患者可出现面瘫、疼痛等症状。
体征
肿块质地较硬,边界不清,活动度 差。
诊断方法
细针穿刺活检、影像学检查(如CT 、MRI)等。正确的诊断对治疗方 案的选择和预后评估具有重要意义 。
t(6;9)(q22-23;p23)导致MYBNFIB基因融合,与肿瘤的发生和
发展密切相关。
诊断与鉴别诊断讨论
01
诊断要点
涎腺腺泡细胞癌的诊断需结合临床表现、影像学检查和病理组织学检查
。病理组织学检查见典型腺泡细胞癌细胞形态及免疫组化特征可确诊。
02 03
鉴别诊断
需与涎腺肌上皮瘤、涎腺基底细胞腺瘤等良性肿瘤相鉴别。此外,还需 与涎腺导管癌、腺癌等恶性肿瘤进行鉴别。鉴别诊断依赖于病理组织学 特点、免疫组化标记物及分子遗传学检查。
多模态治疗策略
探索手术、放疗、化疗和免疫治疗等多模态治疗在涎腺腺泡细胞 癌中的应用和疗效。
预后模型的优化
通过纳入更多的临床和病理参数,优化现有的预后模型,以更准 确地预测患者的预后。
对临床实践的指导意义
诊断标准的细化
病理医生应熟悉涎腺腺泡细胞癌的病理和免疫组化特征,以提高诊 断的准确性。
个性化治疗方案
肿瘤主要由胞质丰富、清晰或微嗜酸性的腺泡细胞构成,细胞 核位于基底部,核仁明显。
涎腺腺泡细胞癌在免疫组化染色中通常表达某些特定的标记物 ,这有助于进一步确认诊断。
尽管涎腺腺泡细胞癌生长缓慢,但其具有局部浸润和复发的倾 向。远处转移较少见,但仍可能影响患者的预后。
未来研究方向与目标
涎腺腺泡细胞癌36例临床病理分析

[2 . b , . e a h , . . u a , . hi r h b M K - 1 ]M A i a K B nSl a M A G / t H C e h u o , . h d a ra ko n
l b, Kh b r , F i m R. ai M. n Ama a, I B y o t i A. a ie F. rl a, Mz l f d a, B e r M. . e r i n a e 1 Th o i s u o a la y t mo p n r a :T  ̄s 8 a d lt ta . e s l p e d p pi r d l u ro a c e s wo et n i- f e
忱, 傅德 良. 胰腺 实性假乳头状 瘸的诊断和治疗 [ ] 中 国实 J.
性颗粒 , 无假 乳头状结构排列 , 免疫组化 结果 C 、nIiae阳 K Isl s l n
性 , O一1一 A 而 t T阴性 …。
用外科杂志 ,0 82 ( ) 39— 5 . 2 0 ,8 5 :4 3 0
柱状黏液上皮 , 呈乳头状 或实性 团快状 排列 , 细胞 核大 明显异 型, S ’ 而 聃 为假乳头排 列 , 无黏 液上 皮 j ( )胰 腺腺 泡细 。 4
学分析 [ ] 中国癌症杂志,0 4 1 ( )2 7 2 9 J. 2 0 。 3 :3 — 3 . 4
[ ] 谭文莉 , 6 汤如 勇 , 吴元佐 , 胰腺 实性假乳头状瘤 的 C 、 R 诊 等. TMI 断 []同济大学学报医学版 ,072 6 :5 —6. J. 20 , 8( )6 8 ( 】 BaoP Na nWH, a e E ca 伽 n , gl adct 7 hnt ,e o l W lr M, / i i ,n y - s I. 咖.l g o
唾液腺常见疾病--新

病原菌:金黄色葡萄球菌、链球菌 (一)病因 1、严重的全身疾患,机体抵抗力降低;高
热、脱水、咀嚼功能减少→唾液分泌减 少→机械冲洗作用降低→逆行性感染
6
2、严重的代谢紊乱,如胃肠外科手术后→ 唾液分泌减少→逆行性感染
3、邻近组织急性炎症的扩散和腺体的损伤 4、慢性炎症急性发作 (二)病理
主要依据临床表现和腮腺造影
18
↑
儿童复发性腮腺炎造影表现
腮腺造影显示:末梢导
管呈点状、球状扩张
排空迟缓,主导管和
腺内导管无明显异常。
19
四、鉴别诊断 儿童——流行性腮腺炎 成人——舍格伦综合征伴感染
五、治疗 具有自愈性 原则:增强抵抗力,防止继发感染,减少
发作
20
慢性阻塞性腮腺炎 (Chronic obstructive parotitis)
1、局部因素(异物、炎症、唾液淤积) 2、全身因素(无机盐代谢)
涎石病好发于颌下腺的原因?
1、颌下腺为混合性腺体,分泌的唾液富含 粘蛋白,钙含量高,钙盐易沉集;
2、解剖因素:导管自下向上行走,在下颌 舌骨肌后缘有一弯曲。
27
二、临床表现 1、多发于20-40岁的中青年; 2、临床症状的轻重和导管阻塞的程度有关; 3、进食后腺体反复肿胀,疼痛,重者可出
腮腺管炎 一、病因病理
导管狭窄(多见),阻塞→远端导管 扩张→唾液淤积→导管上皮化生,导管 周围淋巴细胞浸润,管腔内大量浓缩的 分泌物;
腮腺导管系统狭长,易于唾液淤积, 也是导致阻塞性腮腺炎的原因之一。
21
二、临床表现 1、多发于中年,M略多于F , 常为单侧性; 2、反复发作,约半数患者肿胀与进食有关,
涎腺腺泡细胞癌临床病理分析

涎腺腺泡细胞癌临床病理分析涎腺腺泡细胞癌(salivary acinic cell carcinoma)是一种罕见的恶性肿瘤,起源于唾液腺的腺泡细胞,其病理特点和临床表现在很大程度上决定了该疾病的诊断和治疗方案。
本文将对涎腺腺泡细胞癌的病理特点进行详细分析。
一、涎腺腺泡细胞癌的病理特点涎腺腺泡细胞癌是一种多形性肿瘤,其形态学特点主要包括以下几个方面:1. 组织学特征涎腺腺泡细胞癌的组织学特征与正常腺泡细胞明显不同。
在病理切片中,可见癌细胞形态不规则,排列呈实腺状,细胞质呈玻璃状,胞质丰富,核深染。
癌细胞形态的异质性对诊断和鉴别诊断有重要意义。
2. 免疫组化特征涎腺腺泡细胞癌的免疫表型特点是其诊断的关键之一。
常用的免疫组化标记包括CK7、CK19、CK14、EMA、S-100、Ki-67等。
其中,CK19在涎腺腺泡细胞癌中表达较强,是其特异性免疫标记。
3. 分子遗传学特点涎腺腺泡细胞癌的分子遗传学特点是近年来研究的热点之一。
研究发现,该肿瘤的发生与部分基因的突变或异常表达密切相关。
如MYB-NFIB融合基因突变在涎腺腺泡细胞癌中常见,因此可用于辅助诊断。
二、涎腺腺泡细胞癌的临床表现涎腺腺泡细胞癌的临床表现具有一定的多样性,主要包括以下几个方面:1. 肿瘤部位涎腺腺泡细胞癌最常见于腮腺,其次是颌下腺和舌下腺。
少数病例也可见于其他唾液腺。
2. 疼痛和肿块患者常以颌下腺区域的局部疼痛和肿块就诊,有时可伴有面部肿胀和压痛。
3. 淋巴结转移涎腺腺泡细胞癌具有较高的淋巴结转移率,患者出现颌下、锁骨上等区域的淋巴结肿大,提示疾病的进展。
4. 远处转移少数病例可能出现远处器官的转移,如肺、肝、骨等,为晚期病例的典型表现。
三、涎腺腺泡细胞癌的治疗策略涎腺腺泡细胞癌的治疗策略主要包括手术治疗、放射治疗和化学治疗。
1. 手术治疗对于早期涎腺腺泡细胞癌,手术切除是首选治疗方法。
根据病变部位和范围的不同,可选择行局部切除、腮腺切除或颌下腺切除等手术方式。
涎腺腺泡细胞癌19例临床病理分析

细胞成分的器械 , 我们利用其 比检验室常 规分离器分离液体容量大 10倍 的特点 , 0 对本组病例 采集 2 0 l 5 m 大量胸 、 腹水 进行 离心取沉渣涂 片, 结果癌细胞检 出率 高达 2 . % 。显著高 于 常规 法 的 4 5 ( 16 . % P< 00 ) 提高 了癌 细胞检 出 阳性率 。本方 .5 , 法技术设备 要求简 单 , 方便易 行 , 在临床
9例仍在 临 床 诊察 外 , 都经 过 B超 、 T C、 MR 、 I病理组织诊 断等证 明为 恶性肿 瘤的 事实 。Ⅲ级 中病 理检 查证 实 3 3例 , 总正 确率 9 . % , 合率 较 高 。一 般 情 况 下 71 符 胸、 腹水 中癌 细胞稀 少 , 用常规 法从 小剂
l 6 中 国社 区医师 ・ 8 医学专 业 2 1 年 第 2 00 2期 ( 2 总 第27 第1卷 4 期
讨 论
所有病例均 为发现 涎腺 区肿块 前来 就诊 。其 中 l 6为活 动性肿 物 , 与周 围组 织分 界清 , 3例为 较 固定 的肿 物 , 皮肤 与 粘连 , 不易推动。6例伴有 肿物周 围间歇 乳头状型腺泡 细胞癌 的细胞 则为扁 平状 性疼痛 , 以夜间为重 。1 例伴 有面神 经麻 或低柱状 , 细胞 边 界 清楚 , 核小 , 圆而 带 痹。 角, 居基底侧 。③ 黏液 表皮 样癌 : 当腺 泡 3例较固定 的肿物体 积相对 较大 , 分 细胞 癌以透明细胞 为主时, 可用黏蛋白染 别为 2 8m、. c 3 8m。周 围 间质 内 色法 与黏 液表 皮 样癌 进行 鉴 别 , 者 阴 .c 3 2 m、. c 前 可 见 炎 性 细 胞 反 应 性 增 生 。直 径 32 m .c 性 , 者阳性 。 后 的肿瘤 其周围问质内有数团瘤细胞浸润 , 面神经 内也可见一 团瘤 细胞浸 润 , 临床上 参 考 文 献 伴有 面神经麻痹 。 1 谭郁彬 , 鑫. 张乃 外科 诊断病理学 . 天津 : 天 津科学技术出版社 ,0 0: 0— 4 . 20 4 4 41 1 0例肿瘤行单纯瘤体切除术 , 9例行 u n Roi ROS n ACK u- 局部 扩 大切 除术 。1 1例 术 前 行 放 射 治 2 J a s . AIAND ERMAN¥ S r g a P t l y i h[ . i l a o g n t M]北京 : c h o n 北京大学医 疗 。经随访 ,2例 在术后 1~ 1 5年肿瘤 复 学 出版 社 ,0 6 8 1—82 2 0 :9 9. 发 , 例 已于术后 8年死 亡。 1
93例涎腺肿瘤临床病理分析
首 发 症 状 多 为 涎 腺 区 缓 慢 生 长 的 无 痛 性 肿 物 , 为 恶 性 肿 瘤 如
则生长迅速 、 痛 。 别患者因出现面瘫而就 诊。 疼 个 1 4 诊 断 .
发 生 于 涎腺 恶性 肿 瘤 中 , 腺样 囊性 癌 为 较 为 常 见 。 中 以 腭部 其 最为多见 , 次为腮腺 、 下腺、 其 颌 口底 等 。 然 肿块 生 长缓 慢 , 多 虽 但 呈 浸 润性 生长 , 周 围组 织 界 限 不 清 、 与 固定 , 期 神 经 浸 润 是 本 瘤 早 的特点。 因此 临 床 出现 疼 痛 、 麻木 等症 状 。 液 表 皮 样 癌 是 一 种 以 粘 粘液 细 胞 、 皮 样 细 胞 和 中 间细 胞 组 成 的恶 性 肿 瘤 , 3 ~5 岁 多 表 以 0 0 见, 也是 儿 童 常 见 的 的 涎 腺 恶 性 肿 瘤 。 床表 现 与 肿 瘤 的 恶 性 程 临
涎 腺 组 织 的分 布 很广 , 涎 腺 包 括 腮 腺 、 下 腺 和 舌 下 腺 。 大 颌 涎
瘤来 自涎 腺 闰 管的 腺 上 皮 和 肌 上 皮 。 性 多 于 男 性 。 瘤 缓 慢 生 女 肿 长, 多为 圆 形 或 椭 圆 形 , 面 光 滑 , 节 状 或 分 叶 状 , 周 围 组 织 表 结 与
瘤 生 长缓 慢 , 程 多 为 3 年 。 瘤 为 低 度 恶 性 , 病 理 检 查 多 数 病 ~8 此 但 肿 瘤 有浸 润 , 故手 术 后 易复 发 , 处 转 移较 少 见 。 腺 恶 性 肿 瘤 手 远 涎 术 治 疗 后 应 根 据 情 况 进 行 化 疗 、 疗 , 少 复 发 , 高 疗效 [。 放 减 提 3 1
集2 0 年 至 2 1年 问9 例 各 类 涎腺 肿瘤 资料 , 行 回顾 的 分 析 与 00 01 3 进
腺多形性腺瘤及病变的病理诊断

From John K.C. Chan
可能与恶变有关
年龄大 体积大 显著透明变 核分裂较多 富于细胞
引自(Head and Neck Pathol 2013,7,S68; Mod Pathol.1996 Jun;9(6): 652-7 )
可能与复发有关
以黏液样物质为主 肿瘤有侵犯包膜的倾向 肿瘤出现包膜下裂隙 肿瘤结节穿破包膜
梭形细胞 嗜酸性透明物质
From John K.C. Chan
From John K.C. Chan
Plasmacytoid hyaline cells
Plasma cells
From John K.C. Chan
间质成分
• 酸性黏液物质 • 软骨 • 玻璃样物质
– 均质 – 纤维性
AIDS
涎腺肿瘤的发病率
(British Salivary Gland Tumor Panel, >3000 cases)
多形性腺瘤 Warthin 瘤 其它单形性腺瘤 嗜酸细胞瘤 癌在多形性腺瘤中 腺样囊性癌 各种腺癌 黏液表皮样癌 腺泡细胞癌
59.5% 11.2% 6.9% 0.7% 5.0% 4.5% 3.8% 2.6% 2.3%
腺多形性腺瘤及病变的病理诊 断
正常结构概述
涎腺又称唾液腺,除大涎腺(腮腺、下颌 下腺、舌下腺)外,还包括小涎腺(唇腺、 颊腺、腭腺、舌腺及磨牙后腺等)。
涎腺的组织结构
实质
分泌单位
腺泡 导管系统
闰管 分泌管(纹管) 排泄管
皮脂腺 肌上皮
间质
纤维结缔组织构成的被膜与小叶间隔 血管、淋巴管及神经
肌上皮/基底细胞 • Cytokeratin + • High M.W. cytokeratin + • p63 + • S100 protein -/+ • GFAP +/• Calponin, actin + (仅肌
口腔组织病理学——唾液腺
口腔组织病理学——第四章唾液腺是外分泌腺,其分泌物入口腔,即唾液,经导管入口腔。
25%的唾液来自腮腺、60%来自下颌下腺,5%来自舌下腺,5%~10%来自小唾液腺。
唾液有湿润黏膜、溶解食物和促进消化的作用。
第一节唾液腺的一般组织学结构唾液腺由实质和间质两部分组成。
实质由基本分泌单位、皮脂腺和肌上皮细胞组成。
基本分泌单位包括腺泡和导管系统。
导管系统由闰管、分泌管(纹管)和排泄管三部分组成。
一、腺泡的基本结构及种类由单层腺上皮细胞组成。
腺泡外周有一层薄的基底膜包绕,在腺细胞和基底膜间,有肌上皮细胞附于腺细胞上。
1)浆液性腺泡:1.呈球形2.酶原颗粒,嗜碱性。
2)黏液性腺泡:1.呈管状2.黏原颗粒,胞质透明呈网状,微嗜碱性。
3)混合性腺泡:半月板。
二、导管系统的结构唾液腺的导管系统分为闰管、分泌管(纹管)、排泄管三段。
管径由细变粗,细胞由扁平变为柱状,由单层变为复层,最后汇集成总排泄管,将分泌物排入口腔,混合形成唾液。
1.闰管是导管最细小的终末分支部分,连接腺泡与分泌管。
其长短不一。
光镜下,管壁上皮细胞为矮立方形,细胞质较少,染色较淡,细胞核位于细胞中央。
电镜下,闰管细胞有浆液细胞的某些特点。
在基底膜与细胞间有肌上皮细胞。
2.分泌管与闰管相延续。
管径较粗,管壁由单层柱状细胞所组成。
核圆形,位于细胞中央或近基底部。
细胞质丰富,呈强嗜酸性。
在基底部有垂直于基底面的纵纹,所以又称纹管。
上皮细胞能主动吸收钠,排出钾,并转运水,改变唾液的量和渗透压。
细胞底部的折叠与密集的线粒体则起“钠泵”作用。
3.排泄管小叶间导管与分泌管连续汇集成更大的总排泄管储备细胞:可能发挥干细胞作用在黏液聚集、慢性炎症,尤其在有结石的情况下,大导管上皮可化生为柱状纤毛上皮和复层鳞状上皮。
肌上皮细胞:①位于腺泡、小导管的腺上皮与基底膜之间。
(腺泡、闰管)②扁平,发出4-8个分支突起,细胞核大而扁。
③该突起呈放射状包绕着腺泡表面,形似篮子,称篮细胞④肌上皮细胞有收缩功能。
涎腺腺泡细胞癌临床病理分析

涎腺腺泡细胞癌临床病理分析1.组织学特征:涎腺腺泡细胞癌主要由腺泡结构和基质组成。
腺泡结构由一层层细胞包围着,并在空腔内形成许多细小的腺泡。
这些腺泡细胞以独特的形态出现,细胞外形呈典型的玫瑰花形,具有高度染色性、核聚集现象和核裂变。
而基质主要由纤维组织和Ⅰ型和Ⅲ型胶原纤维组成。
2.形态学特征:涎腺腺泡细胞癌可分为三个亚型,分别为囊型、实性和管型亚型。
囊型亚型是最为常见的,腺泡腔内充满腺泡细胞,并伴有局灶性囊壁破裂形成的囊腔。
实性亚型则在囊型基础上,无明显的腔内结构,呈实性生长模式。
而管型亚型则表现为多个远离肿瘤中心的细小管腔。
3.免疫组化表达:涎腺腺泡细胞癌细胞内常显示神经内分泌样分泌颗粒、复合微小囊泡和链球菌样氨基酸激酶。
细胞膜上可表达雌激素受体,约30%-50%的病例高度表达p53蛋白。
此外,Ki-67指数也常用于判断细胞增殖活性和预后。
4.生长方式和浸润性:涎腺腺泡细胞癌具有高度浸润性、渗透性和侵袭性,可通过神经、淋巴和血管侵犯进入周围组织。
肿瘤细胞往往沿着神经纤维的走向逐渐扩散,导致肿瘤迁徙和复发。
此外,其浸润性生长也常导致手术切缘阳性。
5. 分子遗传学:最近的研究发现,染色体上一些关键基因的突变与涎腺腺泡细胞癌的发生和发展密切相关。
例如,K-ras基因、Pten基因和C-Kit基因的突变在此疾病中较为常见。
6.临床表现和预后:患者首发症状常为不疼痛的肿块,常伴有面部神经症状,如面瘫、感觉丧失等。
此外,涎腺腺泡细胞癌生长潜伏期长,易于距肿瘤手术切缘迁移和术后复发,因此预后较为差劲。
5年生存率仅为30%-40%。
总结起来,涎腺腺泡细胞癌是一种具有高度浸润性和侵袭性的恶性涎腺肿瘤。
其典型的组织学形态特点是腺泡结构的形成和独特的腺泡细胞形态。
临床上常表现为面部肿块和神经症状。
预后较差,容易术后复发。
全面的病理分析对于诊断和治疗该疾病具有重要意义。
涎腺疾病1

慢性阻塞性腮腺炎
临床表现: 1、多发于中年,男性稍多。多 为单侧。 2、反复肿胀、疼痛,与进食有 关。 3、导管口红肿,有雪花样或蛋 清样唾液溢出,导管变粗硬,呈 条索状。
慢性阻塞性腮腺炎
诊断: 1、病史、临床表现 2、腮腺造影:主导管、间叶、小间 叶导管部分狭窄,部分扩张,呈腊 肠样变 鉴别诊断: 1、成人复发性腮腺炎 2、舍格伦综合征
舍格伦综合征
临床表现: 5、唾液腺肿大:腮腺肿大较常见, 呈弥漫性双侧肿大,单侧少见。边 界不清,表面光滑,与周围组织无 粘连。无感染时腺体分泌减少,继 发感染时,腮腺反复肿胀,压痛, 挤压腺体,有雪花样或脓液溢出。 少数腺体内可见单个或多个大小不 等结节状肿块,质地中等,边界不 清,称肿瘤型舍格伦综合症。
舍格伦综合征
——是一种自身免疫性疾病,特 征表现为外分泌腺进行性破坏, 导致黏膜及结膜干燥,并伴有各 种自身免疫性病症。
舍格伦综合症
原发性舍格伦综合征:病变仅限 于外分泌腺本身。 继发性舍格伦综合征:同时伴有 其他自身免疫性疾病,如类风湿 性关节炎等。
舍格伦综合征 病因——不清 可能因素:
慢性复发性腮腺炎
临床表现: 1、5岁儿童多见,男性多见 2、腮腺区反复肿胀,不适,皮肤潮 红 3、导管口有脓液或胶冻状液体溢出 4、反复发作,间隔时间不等。年龄 小,间隔时间短。
慢性复发性腮腺炎
诊断——病史、临床表现及腮腺造 影 腮腺造影:末梢导管呈点状、 球状扩张,排空慢,主导管及腺内 导管无异常。 鉴别诊断: 1、流腮 2、舍格伦综合征
急性化脓性腮腺炎
鉴别诊断: 3、假性腮腺炎:化脓性淋巴结炎,发病 慢,症状轻,肿胀局限,导管口无红肿, 无导管口溢脓。 注意:急性化脓性腮腺炎不宜作腮腺造影 检查
口腔组织病理学唾液腺知识点

口腔组织病理学唾液腺知识点涎腺大涎腺小涎腺涎腺实质:腺上皮细胞形成的腺泡与导管间质:纤维结缔组织形成的被膜与叶间或小叶间隔,血管、淋巴管,神经腺泡浆液性腺泡黏液性腺泡混合性腺泡浆液性腺泡呈球状由浆液细胞组成细胞呈锥形胞浆嗜碱性胞核位于基底1/3 含酶原颗粒分泌物稀薄主要表达α-淀粉酶黏液性腺泡呈管状由黏液细胞组成细胞呈锥形含丰富的黏原颗粒胞浆呈网状分泌物黏稠混合性腺泡 mixed acinus 由黏液细胞和浆液细胞组成前者占大部,紧接闰管后者呈半月状导管(1)闰管导管系统终末部分管壁细胞呈矮柱状胞浆少,淡染胞核位于细胞中央发挥干细胞作用:分化为分泌细胞,肌上皮细胞或分泌管细胞(2)分泌管管径较粗管壁为单层柱状细胞胞浆丰富,强嗜酸性胞核位于中央基底部有垂直于基底面的纵纹(纹管):吸收Na+、排K+能改变唾液的渗透压(3)排泄管小叶间导管与分泌管连续汇集成更大的总排泄管储备细胞:可能发挥干细胞作用肌上皮细胞位于腺上皮和基底膜之间细胞体小,形扁平篮细胞,有肌动蛋白,收缩能力有助于腺细胞分泌物的排出内含肌动蛋白和肌球蛋白结缔组织包绕腺体形成被膜,伸入腺体内,将腺体分隔成许多腺叶和腺小叶来自B淋巴细胞的浆细胞能分泌多种免疫球蛋白,主要是IgA腮腺 parotid gland浅叶位于耳前方,深叶位于下颌后凹纯浆液腺闰管长,分泌管多内有淋巴结,是形成唾液腺良性淋巴上皮病变,腺淋巴瘤以及恶性淋巴瘤的组织学基础颌下腺位于下颌三角混合腺,以浆液细胞为主闰管比腮腺短分泌管比腮腺长舌下腺位于口底黏膜和下颌舌骨肌之间混合腺,以黏液腺泡为主闰管,分泌管不发达小涎腺唇腺是唾液分泌性IgA的主要来源,其浓度比腮腺高4倍。
唇腺活检是诊断舍格伦综合征的一种简便方法。
纯浆液腺味腺纯黏液腺腭腺,舌腭腺和舌后腺其余都是混合腺,以黏液腺泡为主。
涎腺腺泡细胞癌36例临床病理分析

涎腺腺泡细胞癌36例临床病理分析(作者:___________单位: ___________邮编: ___________)【摘要】目的探讨涎腺腺泡细胞癌的临床病理学特征、诊断和鉴别诊断、治疗和预后。
方法复习36例涎腺腺泡细胞癌手术切除标本的病理切片并做相应的免疫组织化学染色,结合临床资料进行分析。
结果涎腺腺泡细胞癌男女发病均等,各年龄组均可发病,好发于腮腺浅叶,生长缓慢,病程长,预后相对较好。
肉眼观:肿瘤直径3~10cm,呈浸润性生长,部分病例周围组织中可见小的瘤结。
切面灰白色或浅粉红色,质地较软,易碎。
镜检:五种类型的细胞组成四种组织类型。
免疫表型:CK18呈细胞膜型阳性、CK7阴性具有特异性。
结论涎腺腺泡细胞癌癌细胞类型和组织类型的多样性是该肿瘤的特征,不同的组织学类型应与其组织学形态相似的肿瘤鉴别,免疫表型起关键作用。
腺泡细胞癌发病少,属低度恶性肿瘤,治疗首选以根治性手术切除,病变范围广或复发病例可行术后放疗以减少局部复发和转移。
【关键词】涎腺腺泡细胞癌;细胞类型和组织类型;诊断和鉴别诊断;治疗和预后涎腺腺泡细胞癌是一种少见的恶性肿瘤,WHO(2003年版)头颈部肿瘤分类中,将涎腺腺泡细胞癌定义为:涎腺腺泡细胞癌是一种涎腺上皮性恶性肿瘤,至少有一些细胞有浆液性腺泡细胞分化,特征是胞质内酶原分泌颗粒;涎腺导管细胞也是该肿瘤的一部分[1]。
基于其细胞类型和组织类型的多样性,诊断有一定困难。
我们收集近15年来36例涎腺腺泡细胞癌结合临床资料,探讨其临床病理学特征、诊断和鉴别诊断、治疗和预后。
1材料与方法1.1材料收集四川省攀枝花市中心医院病理科1994-01~2008-10间诊断的36例涎腺腺泡细胞癌病例,参照WHO(2003年版)头颈部肿瘤的分类标准复查切片,并复习其临床病理资料和随访资料。
1.2方法所有标本均采用10%中性福尔马林固定,石蜡包埋,常规切片,HE染色,经光镜和免疫组织化学明确诊断。
涎腺常见疾病PPT

二、慢性复发性腮腺炎
(病因) (临床表现) (诊断及鉴别诊断) 诊断主要根据临床表现及腮
腺造影 (治疗) 儿童复发性腮腺炎具有自愈性,大
多在青春期后痊愈。因此,以增强抵抗力、 防止继发感染、减少发作为原则。
三、慢性阻塞性腮腺炎
慢性阻塞性腮腺炎又称腮腺管炎,以前与 复发性腮腺炎一起,统称为慢性化脓性腮腺炎。 (病因) (临床表现) (诊断及鉴别诊断) (治疗)
▪ 典型的涎石病诊断不难,有时需与下列疾病 鉴别:
▪ 1.舌下腺肿瘤 ▪ 2.颌下腺肿瘤 ▪ 3.慢性硬化性颌下腺炎 ▪ 4.颌下间隙感染 ▪ (治疗)
第二节 舍格伦综合征
(病因) (临床表现) (断) (治疗)
第三节 涎腺粘液囊肿
▪ 粘液囊肿是最常见的涎腺瘤样病变,其中包括一般 的粘液囊肿和舌
四、涎石病和颌下腺炎
▪ 涎石病是在腺体或导管内发生钙化性团块而 引起的一系列病变。
▪ 85%左右发生于颌下腺,其次是腮腺,偶见 于上唇及唇颊部的小涎腺,舌下腺很少见。
▪ (病因) ▪ (诊断及鉴别诊断)根据进食时颌下腺肿胀及伴
发疼痛的特点,导管口溢脓以及双手触诊可 扪及导管内结石等,临床可诊断为颌下腺涎 石并发颌下腺炎。确诊应作X线检查。
第四节 涎腺肿瘤
一、涎腺良性肿瘤
(一)多形性腺瘤 多形性腺瘤又名混合 瘤该瘤属“临界瘤”
(临床表现) 最常见于腮腺, (诊断) (治疗)
(二)沃辛瘤 沃辛瘤又名腺淋巴瘤
(临床表现) (诊断) (治疗)
二、涎腺恶性肿瘤
恶性肿瘤约占涎腺肿瘤的25%,其中以粘液 表皮样癌和腺样囊性癌为最常见。
(临床表现)
(诊断及鉴别诊断)
急性化脓性腮腺炎依靠病史及临床检查, 诊断并不困难。急 性化脓性腮腺炎不宜行腮 腺造影。
河北医大口腔组织病理学实验指导11涎腺

实验十一涎腺
[目的要求]
(1)掌握三对大涎腺的结构特征及开口部位。
(2)掌握涎腺的一般组织结构。
(3)熟悉各种小涎腺的分布及分泌物性质。
(4)了解涎腺的功能。
[观察内容及方法]
一、腺(男,中年,HE染色)
二、颌下涎(女,40岁,HE染色)402
三、舌下腺(男,七岁,HE染色)403
这三张切片的观察方法,要特别重视首先用低倍镜观察整体情况,找到结构典型的部位,换高倍镜观察:(1)腺泡,根据腺泡的着色性质确定腺泡类型;(2)导管,根据其结构特点及分布状况逐一进行分析比较(3)间质,注意脂肪细胞群和淋巴组织的显现情况。
并写入下列比较表内。
四、悬雍垂(女,24岁,HE染色)404
本片为纵(矢状)切面,游离缘及背腹两面皆由复层鳞状上皮覆盖,口咽面的上皮薄,黏膜下层为黏液腺,是腭腺的一部分,在腺的深层,悬雍垂根部的横纹肌为腭肌.
五、磨牙后腺(女,24岁,HE染色)405
取自上颌磨牙后区,为混合腺,以黏液腺泡为主。
六、舌前腺(女,24岁,HE染色)406
取自舌尖,腹侧,为混合腺,以黏液腺泡为主,位于横纹肌内。
(注):括号内的数字是切片号。
涎腺肿瘤的病理诊断
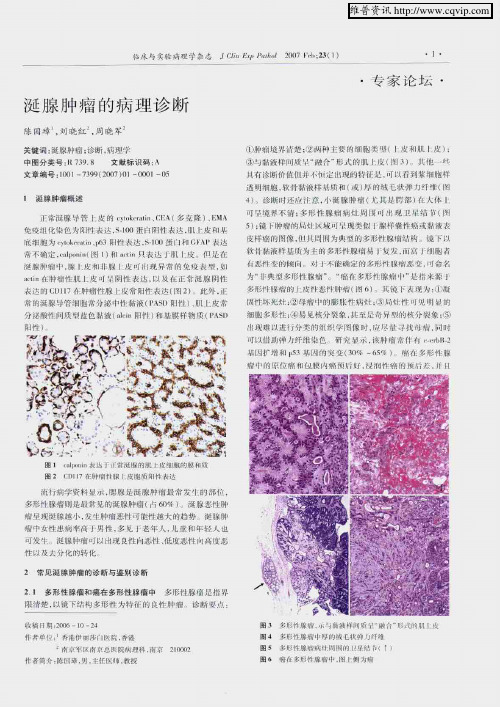
I 涎腺 肿 瘤概 述
常涎 隙 }管 【.皮 的 …h … A(多 璇 j、EMA
免痤州 化 邑 … 陛表 达 . l“)噩 闩阴性 表 . 上皮 州
底细 l拖 !l L ̄ketmin 1 3阳性 柱碴 stIM l'J和 ^I’搦
常 下 确定 i?alpo[ ̄ln【 l I)
n 表1 n }世 仇 址
涎 腺 恼 中 腺 l,出和 非腺 i心 nr 现 异常 呐免 崆 丧 .
往刖一癖 性 L啦
_曩 .姒 盟 lE常涎 脉 阴 性
丧选 的 CDII7 肿 癌性 腺 七戍常 肚表达 fi哥 2) J} 蚪 正 ^ 涎腺 管 细胞 常 舒泌 巾忡 骷液 {P;tSD 刚 ) …_上 庄 常
[肚坏 E灶 .口 坶 蜊 rI帕 嘭胀 性痈 .驯 - 灶 性 【
们
}魁 苇肛性 . ¨射 见俄 分 裂象 . 毫足岢 州 柑栈 仆 裂豫 ,
H1戚 难 以琏{ 舒 髓的 封1 学 像 眦 尽 精寻 找 斗 时
可 且_ J弹 纤维 色 圮 示 陵 帅 常 拌柯 ㈨
手 术 哪象
2 2 单 形 性腺瘤 尽忤 新 l:14J H__” 娄 B 他 』_j.们 降
名秫 勾一 百JII的慨急 辑词 .涵 一 I县 撤 洋
栅 良性 f 种 或 种 细胞 娄 犁 ,为缺 乏 敞 I谊
样 艚 憎 职悱腙 糯 也 捕 底 细 胞腺 啼 恃 k慷蝌
能 阡砸 体 时 方血 正沱 址 蛙』 强』 转佟 IF4J]]星 良 多形 隙
痈组 学I哥 nq转 穆 性 良性濉 台 乖 l。部 苻 彤 昧 前 的手 术 HJl 缘 电 {f} Ⅲ由多次 疆盘 I F水 畔敛癌 f十挤 凡静脖
涎腺疾病

[CT表现]
• ( 1 )良性肿瘤:圆形或类圆形,界限清楚, 边缘光滑,密度均匀, CT 值 30—45HU ,增强 扫描达60HU;皮下脂肪层及邻近结构清晰。 • ( 2 )恶性肿瘤:形态不规则,界限不清楚, 内部密度不均匀,皮下脂肪层模糊或消失,邻 近结构受累,聂骨岩部或乳突骨质破坏。 • (3)低度恶性肿瘤或具有侵袭性的良性肿瘤 • 界限清楚但边缘不光滑,分叶状,内部密度均 匀或不均匀
• 血红蛋白下降,血沉升高,白细胞计数 下降,淋巴细胞分类升高,唾液免疫球 蛋白SigA 、SigG升高。随年龄增长,临 床化验检查逐渐趋于正常。
[影像学表现]
• 检查方法:涎腺造影。 • 影像表现: • 主要是导管系统的变化,主导管:正常或轻度 扩张。 分支导管:稀少。(尚未发育成 • 熟)末梢导管:扩张呈点状、球状甚至腔状。 • 涎腺功能:排空功能迟缓。随年龄增长,逐渐 正常。
[临床表现]
• • • • 1年龄:中老年。 2性别:女性明显多见。 3临床症状:口干,影像进食、说话。 4体征:舌背丝状如头萎缩、舌面光滑, 可有舌裂;常伴有白色念珠菌感染及多 发龋。涎腺反复肿胀呈弥漫性肿大,有 时可有包块。
临床表现]
1年龄:中老年。 • 2性别:女性明显多见。 • 3临床症状:口干,影像进食、说话。 • 4体征:舌背丝状如头萎缩、舌面光滑, 可有舌裂;常伴有白色念珠菌感染及多 发龋。涎腺反复肿胀呈弥漫性肿大,有 时可有包块。
涎腺良性肥大
腮腺肿大,口干
涎腺良性肥大
• 非肿瘤性、非炎症性、慢性 、无痛性肿大。常 见于腮腺,颌下腺也可。与全身系统病(高血 压、糖尿病、内分泌失调等)有关。病理:腺 泡明显增大,腺泡腔消失,分泌颗粒消失; (唾液分泌功能减低)间质水肿,腺泡可消失, 被脂肪细胞代替。造影检查腺体形态正常,体 积增大,导管轻度扩张,末梢导管假性点扩。 B超体积增大,内部回声增强,彩色血流不变。
第三节 唾液腺黏液囊肿

唾液腺黏液囊肿
2ቤተ መጻሕፍቲ ባይዱ舌下腺囊肿
病 因:是由于舌下腺导管阻塞导致涎腺分泌潴留而成。 临床表现:最常见于青少年 ①单纯型:典型表现,占大多数。囊肿位于下颌舌骨肌以上 的舌下区,呈浅紫蓝色,柔软有波动感。常位于口底一侧。 较大的囊肿可将舌抬起,状似“重舌”。囊肿因创伤而破裂 后,流出黏稠而略带黄色或蛋清样液体。 ②口外型:又称潜突型。主要表现为下颌下区肿物,而口底 囊肿表现不明显。触诊柔软,与皮肤无粘连,不可压缩。 ③哑铃型:为上述两型的混合,即在口内舌下区及口外下颌 区均可见囊性肿物。
唾液腺黏液囊肿
4.舌下腺囊肿-诊断要点
(1)好发于儿童及青少年。 (2)囊肿位于口底一侧黏膜下,呈淡蓝色肿物,囊壁薄, 质地柔软。 (3)较大舌下腺囊肿可穿人下颌舌骨肌进入颌下区,也 可波及对侧口底。 (4)囊肿可因创伤而破溃,流出黏稠蛋清样液体,囊肿 暂时消失,数日后创口愈合囊肿长大如前。 (5)囊肿继发感染时,可出现口底部肿胀疼痛,影响进 食。
唾液腺黏液囊肿
3.舌下腺囊肿-易复发的原因 (1)囊肿破裂后创口自愈致再次复发; (2)手术未能将腺体组织切除干净造成复发; (3)口腔内有大量小黏液腺存在,外伤、手术摘除 后可造成邻近黏液腺损伤再发; (4)舌下腺囊肿单纯摘除而未摘除舌下腺复发; (5)术前诊断不明,特别是将舌下腺囊肿误诊为舌 下黏液囊肿而引起术后复发。
唾液腺黏液囊肿
二、临床表现
1.黏液囊肿
最常见。好发于下唇及舌尖腹侧。 病 因:舌体运动常受下前牙摩擦以及自觉或不自觉的 咬下唇动作使黏膜下腺体受伤。 临床表现:位于黏膜下,半透明、浅兰色的小泡,质地软 有弹性。破裂后流出蛋清样透明粘稠液体-消失-复发-较厚的 白色瘢痕状突起。 治 疗 : 可在抽干净囊液后 ,向囊腔内注入 2 %碘酊 0.2 ~ 0.5ml ,停留 2 ~ 3 分钟,再将碘酊抽出。目的是破坏上 皮细胞,使其失去分泌功能而不再形成囊肿。但最常用的治 方法为手术切除。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
解放军总医院病理科 石怀银
小涎腺肿瘤活检病理诊断 涎腺肿瘤的组织学分级
口腔是小涎腺肿瘤最多见部位,但由于活检组
织较少,一般观察不到边界情况,给病理诊断带 来困难。
口腔常见良性肿瘤包括多形性腺瘤、基底细胞腺
瘤;恶性肿瘤包括腺样囊性癌、多形性低度恶性 腺癌,粘表等。
在上述肿瘤中,除粘表外,其他肿瘤在组织学形
特殊染色及免疫组化
特殊染色对肿瘤鉴别诊断帮助不大。肿瘤均有
细胞外粘液阳性物质,但胞浆粘液染色阴性。多 数肿瘤均含有细胞内糖原。 大部分肿瘤均含有上皮和肌上皮成分,因此免 疫组化染色帮助不大。上皮成分表达广谱CK、 低分子量CK如CK7和CAM52,CEA, EMA;而 肌上皮表达广谱CK, Vimentin, P63, Calponin, SMA, S100,GFAP等。 有文献报道CD117,SMA, KI67在腺样囊性癌 中明显高于多形性低度恶性腺癌。但也有文献报 道CD117也表达于多形性腺瘤和基底细胞腺瘤。
态上有重叠,包括均无包膜、多种组织学结构、 细胞异型性小、含有上皮和肌上皮成分、分裂相 少见等。
免疫组化染色特点也有重叠。
小涎腺肿瘤的边界、包膜和浸润情况
良性或恶性口腔小涎腺肿瘤均无包膜。 良性或恶性口腔小涎腺肿瘤均可表现为边界清楚
,但恶性肿瘤表现为浸润性生长,比如累及周围正 常组织、神经、血管等。 见到明确的浸润可以诊断为恶性,但小活检或穿 刺活检往往仅包含肿瘤成分,难以观察到边界。
CK
S100
CK
P63
S100
VIM
CD117
穿刺活检标本判断良恶性困难的原因:
穿刺组织局限,难以评估浸润情况 代表恶性的形态学特征如多形性、异常核分裂相、坏
死、转移等学有交叉,如基底细胞腺瘤和基底细
胞腺癌;多形性腺瘤和多形性低度恶性腺癌等。
周围细胞的栅栏样排列多见于基底细胞肿瘤,但
也不是诊断该病的特异性形态特征。
多形性低度恶性腺癌常常见到周围细胞的漩涡状
排列,也可以见到肿瘤细胞的列兵样排列,还可 以看到正常粘液性涎腺腺泡裹挟于肿瘤内,但都 不是特异的形态学特点。
小涎腺肿瘤细胞形态学特点
肿瘤细胞异型性通常不明显,分裂相少见,
肿瘤间质
软骨粘液样基质支持多形性腺瘤诊断。 软骨粘液样间质由肌上皮产生,可见基质内肌
上皮融入现象。 多形性低度恶性腺癌可以见到浅蓝色粘液透明 样基质;腺样囊性癌可见充满嗜碱性或嗜酸性物 质的假腔。 透明变性胶原间质多见于基底细胞腺瘤,尤其 是膜型。还可以见到分布于肿瘤细胞中的胶原小 球。
很少有坏死。 腺样囊性癌细胞核浆比大,基底样,有角, 核仁不明显。但这种核形也可见于基底细胞肿 瘤甚至多形性腺瘤。 多形性低度恶性腺癌细胞核常常空泡状,常 常可见小核仁。 鳞化多见于基底细胞腺瘤,尤其是膜型;但 多形性腺瘤和多形性低度恶性腺癌也可出现鳞 化。腺样囊性癌鳞化很少见。 透明细胞和嗜酸性细胞可见于多种肿瘤内。
Acinic cell carcinoma
Acinic
Cell Carcinoma was described by Nasse in 1892 as a benign tumor; it was only in 1953 that its malignant potential was realized with the description of 5 aggressive cases by Buxton et al.
小唾液腺肿瘤内上皮细胞成分
肿瘤性上皮细胞呈柱状、立方或扁平状。 可以形成管状、囊状或实性细胞巢结构。 管腔内可以看到PAS阳性的粘液样物质。 基底细胞腺瘤、腺样囊性癌以基底样细胞为主
,但也可以看到多少不等的管腔,而且有些亚型 如管状型基底细胞腺瘤以管腔结构为主。
上皮细胞可以发生鳞化、嗜酸性化生、透明细
AciCC
is generally has a favorable prognosis. According to a National Cancer Database review (1985 to 1995), the 5-year disease-specific survival for AciCC was shown to be 91%
The
current WHO classification refers to ACC tumors by predominant pattern rather than actually assigning a numeric grade.
ACC
with high-grade transformation (ACC-HGT) is a rare, highly aggressive variant of ACC characterized by areas of pleomorphic mitotically active high-grade carcinoma. Conventional ACC is a biphasic tumor with ducts and myoepithelial myoepithelial cells, but the transformed component in ACC-HGT is purely of a ductal phenotype with a solid or cribriform appearance. Transformed components show prominent nuclear size and chromatin variability. Common features include fibrocellular desmoplasia, abundant mitoses, necrosis, and microcalcifications. Unique patterns in HGT include micropapillary and squamoid growth.
腺样囊性癌
5-year
survival is favorable at roughly 75% to 80%, but 15year survival is poor at about 35%. cytomorphologically bland and monomorphic, yet among the most infiltrative of carcinomas. ACC does not seem to have much risk of lymphatic spread as regional lymph nodes are involved in only about 5% of case. Thus, many institutions may not perform neck dissections routinely on ACC patients.
Carcinoma
ex pleomorphic adenoma (CAxPA) comprises 10% to 15% of all salivary gland malignancies. the carcinomatous components are typically high grade or of an aggressive histologic type, with high-grade adenocarcinoma, not otherwise specified, and salivary duct carcinoma being the most common histologic subtypes. However, as many as 15% of tumors are low grade and may behave in a more indolent manner with regard to histologic subtype, a myoepithelial carcinomatous component has been correlated in a recent study with more aggressive behavior. As such, the carcinomatous component should be characterized as to type and grade. A rough quantitation of the carcinomatous component is recommended.
与预后关系最密切。
粘液表皮样癌
粘液表皮样癌的组织学分级系统包
括AFIP、Brandwein、和修订的Healey 系统。
Brandwein系统:
在一些预后不良相关指标中(边界侵袭、实性
巢状生长、神经累及等),如果一项都没有,属 于low grade, 如果有一项不利指标,属于 intermediate grade,2项以上属于high grade。
Intracapsular
CAxPA describes a carcinomatous component that is confined to within a pleomorphic adenoma, whereas minimally invasive CAxPA describes a tumor with minimal extent beyond the capsule The WHO definition for minimal invasion is less than 1.5mm of invasion beyond the capsule. Both these subgroups are considered indolent variants that should not be considered equivalent to the typical CAxPA. Katabi et al indicated as many as 25% of their intracapsular or minimally invasive CAxPA behaved in an aggressive fashion.