肿瘤微创技术纳米刀(IRE)
肿瘤手术治疗的新技术有哪些
肿瘤手术治疗的新技术有哪些肿瘤,一直以来都是威胁人类健康的重大疾病之一。
随着医疗技术的不断进步,肿瘤手术治疗也迎来了一系列新技术,为患者带来了更多的希望和更好的治疗效果。
微创手术技术的发展是肿瘤手术治疗中的一大亮点。
其中,腹腔镜手术和机器人辅助手术在许多肿瘤的治疗中得到了广泛应用。
腹腔镜手术通过在腹部插入几个小的器械通道,医生可以在监视器上清晰地看到腹腔内的情况,进行肿瘤的切除操作。
相比传统的开腹手术,腹腔镜手术切口小,术后疼痛轻,恢复快,住院时间短,同时也减少了手术创伤和并发症的发生。
机器人辅助手术则进一步提升了手术的精准度和灵活性。
机器人的机械臂可以模仿人手的动作,并且能够在狭小的空间内进行复杂的操作,对于一些位置较深或难以触及的肿瘤,具有独特的优势。
冷冻消融术是另一种新型的肿瘤治疗技术。
它通过将极低温的探头插入肿瘤组织,使肿瘤细胞迅速冷冻并破裂,从而达到杀灭肿瘤细胞的目的。
这种技术适用于一些无法耐受手术或肿瘤位置特殊的患者。
例如,对于肺部的小肿瘤,冷冻消融术可以在局部麻醉下进行,避免了开胸手术的巨大创伤。
同时,冷冻消融术还可以重复进行,对于复发的肿瘤也有一定的治疗作用。
射频消融术也是肿瘤治疗的有效手段之一。
它利用高频电流产生的热能,使肿瘤组织凝固坏死。
射频消融术通常在影像设备的引导下进行,如超声、CT 等,能够精确地定位肿瘤位置,确保治疗的准确性。
对于肝脏、肾脏等器官的小肿瘤,射频消融术具有良好的疗效,并且可以与手术治疗相结合,提高肿瘤的治愈率。
纳米刀技术是近年来兴起的一种肿瘤消融新技术。
它通过释放微秒级的高压脉冲,在肿瘤细胞膜上形成不可逆的纳米级穿孔,导致肿瘤细胞凋亡。
纳米刀技术的优势在于对周围血管、胆管和神经等重要结构的损伤较小,适用于一些靠近重要结构的肿瘤治疗,如胰腺肿瘤等。
除了上述局部治疗技术,免疫治疗与手术的联合应用也为肿瘤治疗带来了新的思路。
免疫治疗通过激活患者自身的免疫系统来对抗肿瘤。
纳米刀可能使胰腺癌Ⅲ期患者生存率翻倍

纳米刀可能使胰腺癌Ⅲ期患者生存率翻倍根据最新的研究显示,癌症治疗领域一项最新的消融技术纳米刀(不可逆电穿孔),可以有效地延长局部晚期胰腺癌患者的生存期。
与传统治疗技术相比,纳米刀几乎使患者的生存率翻倍。
在2015美国外科协会年会上,有外科医生展示了他们的研究报告,显示传统的癌症治疗技术化疗和放疗,与不可逆电穿孔技术IRE相结合,可使患者的中位生存期达到23—28个月。
以前的大部分研究都显示,经过传统治疗的Ⅲ期胰腺癌患者,他们的中位生存期大概也就只有11-13个月。
超过五年生存期的也就只有6%。
而IRE却使得这部分患者的中位生存期提高了不止一倍。
“这些结果表明Ⅲ期胰腺癌是可以医治的,而非即刻死刑。
这一点需要向医学界肿瘤治疗领域强调。
明显地,持久生存期是可以通过化疗、IRE和放化疗多学科的综合治疗获得的。
”研究的首席作者罗伯特C.G. 马丁博士表示。
他是肯塔基州路易斯维尔大学肿瘤外科的主任和外科手术教授。
专家提醒这些数据来自一小部分的机构,该研究的样品并非随机抽取。
即使如此,对于肿瘤治疗领域而言,这项肿瘤消融技术应用于局部晚期胰腺癌的治疗可以取得好的疗效,前景让人兴奋。
美国每年有40,000人被诊断出胰腺癌,只有少数人可以进行手术切除。
对于那些无法手术切除的患者现在有了合适的消融技术治疗。
对于那些可以应用于其他肿瘤治疗的热消融技术,例如肝癌,并不适合胰腺癌,因为热消融会造成非肿瘤组织的大面积损伤。
“该技术可以给那些适于放化疗,没有转移,可以进行消融的患者提供了一项局部治疗的替换方案,而不用担心复杂的手术切除造成发病或死亡。
这是一个经过特别筛选的患者小组。
”基斯D.里尔摩尔医生表示。
他是麻省总医院的首席外科医师以及W·杰拉尔德·奥斯汀哈佛医学院的外科教授。
里尔摩尔医生没有参与该项研究,也并不使用IRE消融技术。
但他会推荐自己的病人去进行该项治疗。
他称该研究是令人鼓舞的,但强调需要进行多中心的随机跟踪访问。
纳米刀(Nanoknife)肿瘤消融治疗的临床应用与展望

纳米刀系统组成及应用
主要由发生器和同步器两部分组成。发生器是消融设备的主体包括19G的消融电极 针、治疗计划软件、可自动切换的电极输出端、触摸屏或键盘输入设备及脚踏板等。 消融电极分为单针双极(16G)和多针单极(19G)2种规格,可以根据病灶情况选 择使用。采用单极多针消融,应根据病灶大小,常常至少要有两个或更多电极。两 探针之间的最大距离为2cm,连续给予90次脉冲宽度为100纳秒(ns)、电压1500伏/ 厘米(V/cm)的高压直流脉冲,电流50A。电场可将细胞表面的磷脂双分子层击穿。 根据肿瘤的形状,可适形布针,纳米刀系统最多可连接6个电极。两个电极最大消融 体积为4 × 3 × 2 cm³。 , 2011年10月,美国Angiodynamics公司产品获美国FDA批 准应用于临床,同时还通过了欧盟的CE认证。
治疗后第1天
治疗后第3天
治疗后第7天
治疗后第14天
4.治疗时间短:典型的治疗时间不超过5分钟。 对于直径约 3cm大小的实体肿瘤,经典的IRE是使用 90个 100μs的脉冲 治疗。单次IRE灭活时间少于 1 分钟,即使是采用 3 到 4 次 的重复灭活,总的IRE治疗时间也不超過 5分钟。这归功于 利用极端高速的电场造成了细胞死亡。而热消融需要相应
两个微电极之间的单细胞膜电穿孔: a.局部电穿孔过程; b.多个微电极数量的局部电穿孔过程;
液滴的微流体电穿孔技术示意图; 通过(藻细胞的过程)聚二甲基硅氧烷(PDMS)
微电极(锯齿)聚焦胞内物质的电穿孔后细胞裂解示意图
机理
消融探针释放微秒级高压脉冲
吞噬细胞消除细胞碎片治疗区 域恢复正常
破坏肿瘤细胞膜形成纳米级不可逆电穿孔
肿瘤细胞快速凋亡
优势
1.组织选择性: IRE的细胞死亡是通过凋亡介导的。血管结构(由弹
纳米刀治疗恶性肿瘤
不可逆电穿孔定义 通过强大电 场产生微秒级的电脉 冲,在细胞膜上形成 多个纳米级的不可逆 电穿孔,破坏细胞内 外平衡,从而促使细 胞凋亡。
1. Lee et al., Gut and Liver, 4 (Suppl. 1) 99- 104, Sep. 2010
1
不可逆电穿孔治疗效果
脉冲电场 不可逆电穿孔 免疫系统反应3
4.消融彻底,消融边界清晰
5.使细胞凋亡而非蛋白质变性坏死
NO1.消融时间短
每对探针释放90个微秒级的超短脉冲,耗时 小于1分钟; 消融3cm的肿瘤耗时小于5分钟
No.2消融区的重要组织得以保留
血管 神经 胆囊、胆管
胰管
纳米刀治疗后的组织
组织结构未被破坏
输尿管
图片来自:Imaging Guided Percutaneous Irreversible Electroporation: Ultrasound and Immunohistological Correlation
纳米刀设备的组成部分
1. LCD显示器 2. 控制台和键盘 3. 探针面板 4.心电同步仪
5. 脚踏开关/脚踏板
纳米刀的附 件 纳米消融探针:
一次性使用的消融探针; 19G带刻度; 有长度为15cm及25cm两种规格可选; 针尖的暴露深度为0~4cm可调,步 进为0.5cm; 最大的插入深度为15或25cm。
细胞
细胞凋亡1,2
巨噬细胞清除细胞碎片
1天
3天
7天
14天
影像来自AngioDynamics – 猪肝脏的动物模型
1.Lee et al., Gut and Liver, 4 (Suppl. 1) 99- 104, Sep. 2010 2.Li et al., PLoS ONE, 6(4): e18831, April 2011 3.Lee et al., Technology in Cancer Research and Treatment, 6(4): 287-293, August 2007
纳米刀基本知识
纳米刀基本知识纳米刀基本知识1、纳米刀技术的原理早在20世纪90年代,科学家们发现使用高达1千伏的能量在细胞膜上产生可逆微孔的可逆电穿孔技术,可以让基因药物或化疗药物进入细胞,开启了基因治疗和电化学治疗的篇章。
国内在2002年左右逐渐开展不可逆电穿孔临床应用的基础研究和设备研发。
美国加州大学的Rubinsky及其同事的研究也发现,将靶区间的电压增加到3千伏,会在细胞膜上形成不可逆微孔,引起细胞凋亡,并激活单核-巨噬细胞系统,吞噬、清除凋亡细胞。
纳米刀是一种全新的尖端肿瘤消融技术,它通过释放高压脉冲在肿瘤细胞上形成纳米级永久性穿孔,破坏细胞内平衡,使细胞快速凋亡。
迄今,全球已有100多个核心肿瘤医院采用了该技术,治疗例数超过6000例。
治疗的癌肿包括胰腺、肝、肺、肾、前列腺以及其他实质器官以及软组织的肿瘤,特别适用于临近大血管、肝门区、胆囊、胆管、输尿管的肿瘤。
文献报告胰腺癌的治疗具有特别价值。
纳米刀技术由美国AngioDynamics公司研发,通过高达3千伏的电压在肿瘤细胞膜上形成不可逆微孔,引起细胞凋亡,并激活单核-巨噬细胞系统,吞噬、清除凋亡细胞。
迄今,全世界有100多个核心肿瘤医院采用了该技术,治疗例数超过6000例,疗效显著,随着该项新技术的推广,其影响仍在不断扩大。
近五年来,纳米刀治疗的研究取得快速发展,每年有数百篇论文在杂志及专业会议上发表。
2012年4月美国FDA批准纳米刀可作为临床对软组织肿瘤的消融治疗,并通过了欧盟的CE认证。
2、纳米刀技术的适应症及禁忌症适应症:纳米刀技术适用于位于特定器官内且不出现全身转移的肿瘤,一般直径在3-4cm的实质性单个病灶效果最佳。
适用于肝、肺、肾、胰腺、前列腺以及其他实体肿瘤,尤其对靠近肝门区、胆囊胆管、胰腺、输尿管的肿瘤具有独特优势。
禁忌症:1)纳米刀技术应尽量避免用于安装有心脏起搏器或患有严重心律失常的患者,因为纳米刀技术可能会干扰心脏或起搏器正常的电活动。
肿瘤纳米刀技术

04
肿瘤纳米刀技术的未来 展望
技术改进方向
提高精准度
通过改进纳米刀的导航系统和定位技术,提高对肿瘤的识别和命 中率,减少对周围正常组织的损伤。
增强治疗效果
研究更有效的纳米药物载体,提高纳米刀的释药性能和药效,以更 好地抑制肿瘤生长和扩散。
拓展适用范围
探索纳米刀技术在更多种类的肿瘤治疗中的应用,包括实体瘤和血 液肿瘤等。
进入21世纪,越来越多的研究机构和 企业开始投入肿瘤纳米刀技术的研发, 初步的临床试验取得了一定的效果。
技术原理
1 2
纳米级物质
肿瘤纳米刀技术利用纳米级的物质,如纳米药物、 纳米粒子等作为载体,将能量或药物传递到肿瘤 部位。
能量消融
在肿瘤部位,纳米级物质会产生局部的高热或强 电场等能量形式,实现对肿瘤的消融和杀灭。
在肺癌治疗中,肿瘤纳米刀技术通过纳米药物载体将药物输送到肺癌细胞内部, 这些药物可以抑制肺癌细胞的生长和扩散,同时还可以刺激免疫系统对肺癌细胞 的攻击。
案例三:乳腺癌治疗
总结词
乳腺癌是女性最常见的恶性肿瘤之一,肿瘤纳米刀技术在乳 腺癌治疗中取得了显著的效果。
详细描述
在乳腺癌治疗中,肿瘤纳米刀技术利用纳米药物载体将药物 输送到乳腺癌细胞内部,这些药物可以抑制乳腺癌细胞的生 长和扩散,同时还可以降低化疗药物的毒副作用,提高治疗 效果。
3
精确打击
由于纳米级物质具有高度的靶向性和特异性,肿 瘤纳米刀技术能够实现对肿瘤的精确打击,避免 对正常组织的损伤。
02
肿瘤纳米刀技术的优势 与局限性
优势
高精度定位
肿瘤纳米刀技术能够实现高精 度定位,对肿瘤进行精确打击 ,减少对周围正常组织的损伤
。
唯一非热消融治疗技术——不可逆电穿孔(IRE)
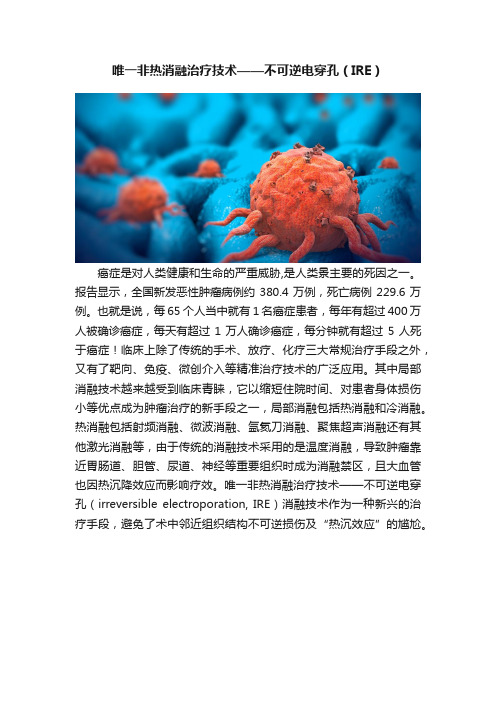
唯一非热消融治疗技术——不可逆电穿孔(IRE)癌症是对人类健康和生命的严重威胁,是人类景主要的死因之一。
报告显示,全国新发恶性肿瘤病例约380.4万例,死亡病例229.6万例。
也就是说,每65个人当中就有1名癌症患者,每年有超过400万人被确诊癌症,每天有超过1万人确诊癌症,每分钟就有超过5人死于癌症!临床上除了传统的手术、放疗、化疗三大常规治疗手段之外,又有了靶向、免疫、微创介入等精准治疗技术的广泛应用。
其中局部消融技术越来越受到临床青睐,它以缩短住院时间、对患者身体损伤小等优点成为肿瘤治疗的新手段之一,局部消融包括热消融和冷消融。
热消融包括射频消融、微波消融、氩氦刀消融、聚焦超声消融还有其他激光消融等,由于传统的消融技术采用的是温度消融,导致肿瘤靠近胃肠道、胆管、尿道、神经等重要组织时成为消融禁区,且大血管也因热沉降效应而影响疗效。
唯一非热消融治疗技术——不可逆电穿孔(irreversible electroporation, IRE)消融技术作为一种新兴的治疗手段,避免了术中邻近组织结构不可逆损伤及“热沉效应”的尴尬。
一、不可逆电穿孔(IRE)技术原理早在20世纪90年代,科学家们发现使用高达1千伏的能量在细胞膜上产生可逆微孔的可逆电穿孔技术,可以让基因药物或化疗药物进入细胞,开启了基因治疗和电化学治疗的篇章。
国内在2002年左右逐渐开展不可逆电穿孔临床应用的基础研究和设备研发。
美国加州大学的Rubinsky及其同事的研究也发现,将靶区间的电压增加到3千伏,会在细胞膜上形成不可逆微孔,引起细胞凋亡,并激活单核-巨噬细胞系统,吞噬、清除凋亡细胞。
纳米刀技术由美国AngioDynamics 公司研发,2018年有北京名赫医疗科技有限公司引入国内。
该技术是通过释放1500~3000 V的直流(25~50A)高压电脉冲,作用于肿瘤的细胞膜磷脂双分子层,导致细胞膜形成多个纳米级的不可逆孔道,破坏细胞内外平衡,从而促使细胞凋亡,体内吞噬细胞将细胞碎片吞噬掉,同时激活机体免疫反应,从而发挥控制肿瘤的作用。
2021年探讨胰头癌行纳米刀治疗的手术策略(全文)

2021年探讨胰头癌行纳米刀治疗的手术策略(全文)胰腺癌生长速度较快且生长时多包绕周围血管、胰管及神经组织,发现时已有约80%的患者无法接受外科手术切除治疗,寻找全新有效的治疗手段显得尤为重要。
近年来肿瘤消融技术迅速发展,其疗效得到广泛认可,针对不可切除的局部进展期胰腺癌更有其治疗价值。
但由于胰腺组织毗邻结构复杂,传统消融易引起出血、胆道损伤等严重并发症,限制了其在胰腺癌治疗中的应用。
不可逆电穿孔消融(irreversible electroporation,IRE)又被称为纳米刀,它利用微创电极针传递毫秒级电脉冲,改变细胞膜磷脂双分子层的跨膜电位,使细胞膜进行重排,细胞表面出现很多纳米级孔隙,造成不可逆的细胞损伤,引起细胞凋亡。
中国食品药物监督管理局于2015年6月18日正式批准美国Nano KnifeTM System设备应用于临床治疗胰腺癌。
本文就一列不可切除的胰腺癌患者行纳米刀治疗取得良好的治疗效果进行探讨,旨在为胰腺癌的消融治疗提供临床依据。
患者女,45岁,术前磁共振(如图1-2)诊断胰头占位性病变,胰腺癌可能性大。
给予患者行胰头癌纳米刀治疗(如图3),手术过程:全面生效后,平卧位,消毒铺巾,上腹正中切口,长约15cm,肝脏呈重度淤胆改变,肿瘤位于胰头,7*5*4cm大小,质地硬,侵犯十二指肠腔,可推动。
游离第一肝门,肝固有动脉未见肿瘤侵犯,游离十二指肠,游离胰腺下缘,见肿瘤侵犯肠系膜上静脉,静脉腔可触及癌组织侵犯。
反复尝试分离仍无法游离。
无法行根治性切除。
取胰头少许肿物术中冰冻结果(如图4)回报示:腺癌。
针对无法完整切除之胰头癌,给予患者行纳米刀治疗。
术中行超声确定肿瘤位置及大小,决定采取4针阵列对肿瘤进行纳米刀消融。
在超声引导下,首先在肿瘤上极边缘布下主针,同时在肿瘤内外侧缘及肿瘤内布下三枚副针。
每两针平行,间距为2cm,针暴露深度为1cm。
设定电场强度为1500V/cm,间距为2cm,脉宽90us,脉冲数为70,对肿瘤进行消融。
肿瘤纳米刀消融治疗技术管理规范
肿瘤纳米刀消融治疗技术管理规范为规范肿瘤纳米刀消融治疗(即Irreversible electroporation,不可逆电穿孔)技术临床应用,保证医疗质量和医疗平安,制定本规范。
本规范是医疗机构及其医务人员开展肿瘤纳米刀消融技术的最低要求。
本规范所称肿瘤纳米刀消融治疗技术是基于不可逆电穿孔原理开展起来的新型非热能消融治疗系统,通过将纳米刀电极穿刺到病灶内,电极之间产生高压直流电脉冲,在细胞膜打上纳米级的孔,形成不可逆的孔隙,通过改变细胞膜的通透性诱导细胞凋亡从而到达肿瘤细胞消融的目的。
治疗途径包括经皮、腔镜和开放手术下。
一、医疗机构基本要求(一)医疗机构开展肿瘤纳米刀消融治疗技术应当与其功能、任务和技术能力相适应。
(二)有卫生健康行政部门核准登记的、与肿瘤消融治疗技术相关的诊疗科目。
(三)开展与肿瘤消融治疗技术相关的临床诊疗工作8 年以上,肿瘤治疗床位不少于30张。
(四)麻醉后监测治疗室(PACU)和/或重症医学科。
1.设置符合规范要求,到达ni级洁净辅助用房标准,病床不少于6张,每病床净使用面积不少于15平方米,能意义:反映肿瘤消融治疗患者的远期疗效。
九、平均住院日定义:实施肿瘤纳米刀消融治疗的患者出院时占用总床日数与同期肿瘤纳米刀消融治疗患者出院人数之比。
计算公式:平均住院日二xioo%意义:反映肿瘤消融治疗技术水平,是分析本钱效益的重要指标之一。
注:1.肿瘤纳米刀消融治疗指征:(1)PTA>50%o(2)无器官功能障碍(按相应器官功能进行评价),如肝功能Child A、B级。
(3)ECOG 分级W2 级。
(4)麻醉评估:病情分级Will级(美国麻醉医师协会病情分级标准)。
满足上述四项并符合相应肿瘤纳米刀消融治疗适应症, 为肿瘤纳米刀消融指征选择正确。
2.临床病症有效缓解是指肿瘤引起的临床病症经纳米刀消融治疗后得到明显缓解,如疼痛降低2个级别以上。
3.肿瘤局部病灶控制是指纳米刀消融治疗后肿瘤完全消融。
纳米刀消融参数及临床应用
模拟布针情况:不同探针间距的影响
探针间距过大
(探针间距为2.5cm ,电压为最大电压3000 Volts)
1500
1000
2000
500
2500
0
3000
电压 (V)
2.5 cm
30 20 10
4Hale Waihona Puke 50060电流 (A)
探针间距小、高电流中止脉冲发生
探针间距太小
(间距为1.0cm ,电场强度为2000 V/cm)
四针阵列
五针阵列
五针阵列
六针阵列
退针消融法
纳米刀电极退针消融方法 进行连续的退针消融,以获得足够的消融边界 一旦确认所有探针对输送了有效电流,可以开始退
针,退针距离稍稍小于探针暴露深度 例如,探针暴露深度是1.0cm ,退针距离大概是
0.7-0.8cm
0.7 cm 0.7 cm
MRI enhanced scan showed a low signal change in the ablation area after 1 week of operation
可逆电穿孔区域 不可逆电穿孔区域
1000 V/cm 800 V/cm 600 V/cm 400 V/cm 200 V/cm 0 V/cm
电场的2D分布
750 V; d = 5mm
2250 V; d = 15mm
1000 V/cm 800 V/cm 600 V/cm 400 V/cm 200 V/cm 0 V/cm
反应评
估
CT 和 CT/PET, 或 MRI
肿瘤标志物 IRE后3个月
设备界面
1 手术信息
2 探针信息
3 布针
前列腺癌纳米刀消融治疗的优点

B BUSINESSMAN USINESSFAMOUS DOCTOR名医说前列腺癌纳米刀消融治疗的优点126 | 中国商人 CBMAGCopyright©博看网 Bookan. All Rights Reserved.CBMAG 中国商人 | 127梁先生因尿频、排尿困难,到当地医院检查,被诊断为前列腺癌。
他既担心病情,又害怕外科手术,于是慕名找到中山大学肿瘤医院影像与微创介入中心吴沛宏教授,寻求治疗。
吴沛宏教授、李旺教授和麻醉科李伟教授等,细致研究患者病情,并与患者家属充分商量后,决定采用微创不可逆电穿孔(纳米刀)技术进行治疗。
梁先生的整个手术过程非常顺利,术后没有任何并发症,当天即下床活动,第二天即正常排尿并出院回家像正常人一样生活。
随着人们生活习惯改变和人均寿命的延长,世界范围前列腺癌发病率呈逐步上升的趋势,现已成为男性癌症相关死亡的第三大原因。
诊断技术的提高比如广泛的前列腺特异抗原 (PSA) 筛查、影像技术的进步等,让前列腺癌的早期发现成为可能。
前列腺癌主要的治疗方法有外科手术治疗、放射治疗、局部冷/热消融等微创治疗、放射性粒子植入治疗及内分泌等综合治疗。
但由于前列腺位置深入体内,毗邻直肠、尿道、会阴部神经、血管等结构,手术难度及风险较大,尿失禁、勃起及性功能障碍等并发症发生率高。
不可逆性电穿孔(irreversible electroporation,简称IRE),也称纳米刀,透过纳米电极间产生的极其短但强力的电场使得细胞膜上产生永久纳米孔的一种组织消融技术,透过扰动细胞稳态以让细胞凋亡并激发人体产生抗肿瘤免疫反应。
纳米电极的直径为19G,相当于普通牙签的三分之一,对患者损伤极小。
这种治疗技术导致细胞凋亡而不是其他基于冷/热消融、辐射的消融技术造成的细胞坏死。
纳米刀治疗前列腺癌有什么优势?对主要的血管、神经血管束、尿道、直肠、神经等都没有损伤,不会限制消融的范围,因此是一种可推广的治疗方法。
纳米刀消融参数及临床应用
纳米刀消融参数及临床应用纳米刀是一种新型的消融技术,以其独特的物理特性在医学领域引起了广泛。
这种技术的目标是实现更精确、更有效的肿瘤消融,同时减少副作用,提高患者的生活质量。
本文将深入探讨纳米刀的消融参数以及其在临床应用中的表现。
纳米刀是一种基于纳米级别的精确手术技术,其利用高强度聚焦超声(HIFU)产生局部高温,使肿瘤组织瞬间坏死。
与传统的手术刀相比,纳米刀具有无创、精确、安全、高效等优点。
频率与功率:纳米刀的消融效果受到频率和功率的影响。
一般来说,频率越高,功率越大,消融效果越好。
然而,这也可能导致热损伤和副作用的增加。
因此,选择合适的频率和功率是关键。
焦点深度:焦点深度决定了纳米刀能够消融的组织厚度。
一般来说,焦点深度需要根据肿瘤的大小和位置来选择。
消融时间:消融时间是指纳米刀工作的时间。
一般来说,消融时间越长,消融效果越好。
然而,过长的消融时间可能导致热损伤和副作用的增加。
肿瘤治疗:纳米刀因其无创、精确、安全、高效等优点,在肿瘤治疗中具有广泛的应用前景。
对于一些深部肿瘤,如胰腺癌、肝癌等,纳米刀提供了新的治疗手段。
疼痛治疗:纳米刀也可以用于疼痛治疗,如神经痛、关节痛等。
通过直接作用于疼痛部位,纳米刀可以在短时间内消除疼痛。
其他应用:除了肿瘤治疗和疼痛治疗,纳米刀还在其他领域有所应用,如子宫肌瘤治疗、前列腺增生治疗等。
纳米刀是一种具有巨大潜力的新型消融技术。
通过优化消融参数,我们可以更好地控制其治疗效果,减少副作用,提高患者的生活质量。
随着技术的不断进步和临床应用的不断拓展,纳米刀将在未来的医学领域中发挥越来越重要的作用。
射频消融减胎术是一种先进的妊娠管理技术,主要应用于多胎妊娠的治疗。
这项技术的目的是减少胎儿数量,以减轻母体和胎儿的并发症,并改善妊娠结局。
本文将详细介绍射频消融减胎术的临床应用。
射频消融减胎术主要是利用射频能量将特定部位的胎盘组织加热至60°C - 100°C,从而破坏胎盘组织,减少胎儿数量。
前列腺癌纳米刀消融治疗的优点
前列腺癌纳米刀消融治疗的优点作者:来源:《中国商人》2019年第05期梁先生因尿频、排尿困难,到当地医院检查,被诊断为前列腺癌。
他既担心病情,又害怕外科手术,于是慕名找到中山大学肿瘤医院影像与微创介入中心吴沛宏教授,寻求治疗。
吴沛宏教授、李旺教授和麻醉科李伟教授等,细致研究患者病情,并与患者家属充分商量后,决定采用微创不可逆电穿孔(纳米刀)技术进行治疗。
梁先生的整个手术过程非常顺利,术后没有任何并发症,当天即下床活动,第二天即正常排尿并出院回家像正常人一样生活。
随着人们生活习惯改变和人均寿命的延长,世界范围前列腺癌发病率呈逐步上升的趋势,现已成为男性癌症相关死亡的第三大原因。
诊断技术的提高比如广泛的前列腺特异抗原(PSA)筛查、影像技术的进步等,让前列腺癌的早期发现成为可能。
前列腺癌主要的治疗方法有外科手术治疗、放射治疗、局部冷/热消融等微创治疗、放射性粒子植入治疗及内分泌等综合治疗。
但由于前列腺位置深入体内,毗邻直肠、尿道、会阴部神经、血管等结构,手术难度及风险较大,尿失禁、勃起及性功能障碍等并发症发生率高。
不可逆性电穿孔(irreversible electroporation,简称IRE),也称纳米刀,透过纳米电极间产生的极其短但强力的电场使得细胞膜上产生永久纳米孔的一种组织消融技术,透过扰动细胞稳态以让细胞凋亡并激发人体产生抗肿瘤免疫反应。
纳米电极的直径为19G,相当于普通牙签的三分之一,对患者损伤极小。
这种治疗技术导致细胞凋亡而不是其他基于冷/热消融、辐射的消融技术造成的细胞坏死。
纳米刀治疗前列腺癌有什么优势?对主要的血管、神经血管束、尿道、直肠、神经等都没有损伤,不会限制消融的范围,因此是一种可推广的治疗方法。
前列腺癌的纳米刀消融治疗有其优点:1、创伤小;2、治疗效果确切;3、对尿道无损伤;4、不伤及神经,特别是性神经;5、生活质量高;6、消融后引起的肿瘤细胞凋亡,即程序性死亡,诱导体内巨噬细胞清除凋亡肿瘤细胞,使正常前列腺组织得以重新修复。
肿瘤微创技术纳米刀(IRE)

肿瘤微创技术:纳米刀(IRE)納米刀是一種全新的腫瘤消融技術,它通過釋放高壓脈沖在腫瘤細胞上形成納米級永久性穿孔,破壞細胞內平衡,使細胞快速凋亡。
納米刀在2012年4月獲美國FDA批准應用於臨床,同時還通過了歐盟的CE認證,截止到2012年底,全球已有一百多個核心腫瘤醫院采用了納米刀技術。
通過眾多臨床研究表明,納米刀是一種安全而又高效的腫瘤治療技術,與其他腫瘤治療技術相比,它具有以下優勢:1.消融時間短治療直徑約3cm的實體腫瘤時,納米刀一般只需90個100毫秒的超短脈沖。
一組治療時間不到一分鍾。
因此即使有三個或四個相互重疊的消融區,全程的消融時間也不會超過5分鍾。
2. 治療區域的血管、神經等重要組織得以保留納米刀消融技術的另一個特點是它能夠保護消融區內重要的組織結構。
所有經過納米刀治療的肝組織中,其重要結構,如肝動脈,肝靜脈,門脈,肝內膽管均能得到良好的保護。
而傳統的消融方式,以升溫或降溫的方式讓蛋白質發生變性,各類蛋白質和DNA均被破壞,以上的結構便會遭到破壞無法修複。
3.不受熱島效應影響納米刀的消融主要是通過電脈沖擊穿細胞膜,在此過程中不會產生熱量,也不會受到其他外界溫度影響。
而傳統的熱消融或者冷消融,一旦消融區域內存在較大血管,其熱量就會被血流帶走,導致周邊消融不徹底,容易造成複發,而納米刀很好地避免了這個問題。
4. 治療徹底,治療邊界清晰納米刀的另一個優勢是,不管腫瘤所處的位置,尺寸大小以及形狀,它都能對腫瘤進行完整消融。
如上文所述,無論腫瘤是靠近血管的,還是形狀不規則或者是大腫瘤,IRE都能對其進行徹底消融。
此外,納米刀消融區邊界清晰,劃界厚度僅為1-2細胞單元。
去治療區和非治療區域涇渭分明,因此,對納米刀的有效性、治療結果以及後續跟蹤都能進行更准確的判斷和評估。
而其他像射頻或微波的消融方式,均會在消融區邊緣處出現“灰色區域”,即消融區的最外圍區域上還有大范圍沒完全滅活的腫瘤細胞。
這是造成日後腫瘤複發的主要隱患之一,而納米刀不存在這一問題。
医学交流课件:纳米刀的治疗进展

③ Overview table of current data on focal therapy for prostate cancer with IRE—前列腺癌的不可逆电穿孔消融
(n/m; not mentioned)
[1] Scheltema M J ,et al. Irreversible electroporation, a new modality in Focal Therapy for prostate cancer.[J]. Archivos españoles de urología, 2016, Vol.69 (6), pp.337-44。
IRE设备及配件
目前使用的IRE 装置是美国 AngioDynamics 公 司 制 造 的 NanoKnife 系统。该系统已接受 美 国 FDA 上 市 前 通 告 , 并 享 受 FDA的临床试验器械豁免 ,用 于临床试验。
IRE术中运用心电同步技术
电流可直接刺激神经肌肉接点,引起强力肌肉抽搐,因此治疗时需全身麻醉,使用肌松剂。电 流可刺激心脏,引起心律失常。应用心电同步激发,可避免此种并发症。如果组织内电导率不 均匀(如肺),IRE消融可能产生不均质性。
the inferior aspect of the pericardium (black arrowheads). (C) CT of liver
during portal venous phase 9 months after IRE ablation demonstrates a
markedly contracted, non-enhancing ablated scar in segment II (arrow).
0
经皮 (53.8%)/腹 6
英国利兹大学:高科技“纳米刀”可有效摧毁癌细胞
英国利兹大学:高科技“纳米刀”可有效摧毁癌细胞来自英国利兹大学的研究人员运用一种新型的高科技纳米刀技术,第一次应用于肾脏肿瘤的治疗。
该技术通过利用脉冲高压电流,可以有效摧毁癌细胞。
该技术,又称影像引导下的不可逆电穿孔技术,之前已经在英国应用于肝癌和胰腺癌的治疗。
在圣詹姆士医院利兹癌症中心,介入放射科医生Tze Wah团队给一位来自迪尤斯伯里的59岁癌症患者艾伦.斯佩特进行了纳米刀手术,手术时长不超过两个小时。
Wah医生表示艾伦的肿瘤并不适用于传统的治疗方案。
他的肿瘤位置长得比较特殊,利用冷热消融都会对其肾脏造成损伤。
“纳米刀(IRE)的应用给我们提供了崭新的治疗方案,同时,该技术可以延长艾伦肾脏的使用期。
”Wah医生如是说。
这种技术需要一种特殊的“纳米刀”探针,以一种合适地距离来被准确插入到肿瘤中。
在整个手术治疗期间,需要通过CT扫描来确定探针的准确位置以及监控治疗过程,从而确保肿瘤附近的正常组织不会受到损伤。
一旦探针置于合适的位置,电脉冲就会对肿瘤中的癌细胞进行冲击作用,使细胞膜产生纳米级孔洞,导致癌细胞死亡。
Wah医生说:“每一项指标都显示纳米刀手术是成功的。
”艾伦第二天就回家了。
“我非常开心癌症治疗又多了一项新技术,纳米刀将给更多的癌症患者带来希望。
”纳米刀肿瘤治疗系统(NanoKnife System)源于不可逆电穿孔技术(Irreversible Electroporation,简称IRE),这是一种非热能的新型肿瘤微创消融技术,能更精准地诱导肿瘤细胞凋亡而对肿瘤进行完全的消融,且不会对消融区内的其他重要组织,如血管、胆管、神经等造成不可逆的损伤,从而减少其他传统消融方式所伴有的并发症。
纳米刀可应用于胰腺、肝、肺、肾、前列腺以及其他实体肿瘤,尤其对靠近胰腺、肝门区、胆囊、胆管、输尿管的肿瘤具有独特的优势。
纳米刀已经于2012年4月率先在美国得到FDA批准应用于临床取得良好效果,加拿大、欧洲、澳洲也已开始使用。
恶性肿瘤患者纳米刀介入治疗的护理配合

恶性肿瘤患者纳米刀介入治疗的护理配合费晓燕;戚倩【摘要】目的分析并总结应用纳米刀介入手术治疗恶性肿瘤患者的术中临床护理配合,制定相应的护理常规.方法回顾2015年11月-2017年10月我院33例恶性肿瘤患者应用纳米刀介入手术治疗的临床护理资料,重点总结包括纳米刀装置的使用配合及故障处理、术中体位放置、生命体征观察、管道与消融针的管理等问题.结果 33例患者均手术治疗成功,未发生因术中护理不当引起的术后并发症.与手术相关并发症4例(12.12%),其中2例房颤、2例术后出血,经相应并发症处理后,患者恢复良好.结论熟练掌握纳米刀介入手术相关知识及故障处理方法、术中的密切观察、正确主动的护理配合是保障手术顺利完成的不可缺少环节.【期刊名称】《护士进修杂志》【年(卷),期】2019(034)006【总页数】3页(P559-561)【关键词】纳米刀;不可逆性电穿孔;介入手术;恶性肿瘤;护理【作者】费晓燕;戚倩【作者单位】上海交通大学医学院附属瑞金医院放射介入科,上海200025;上海交通大学医学院附属瑞金医院放射介入科,上海200025【正文语种】中文【中图分类】R473;R473.73纳米刀(Nano Knife),又称不可逆电穿孔(Irreversible electroporation,IRE),是一种新兴的不依赖热量形式的肿瘤消融技术,原理主要是通过对肿瘤细胞实施瞬时、高频率、反复高电压脉冲致使肿瘤细胞膜不可逆性电穿孔而造成细胞调亡[1]。
自2011年10月通过美国食品药品监督管理局(FDA)及欧洲共同体质量(CE)认证批准[2]应用于临床后,已在肝癌、肺癌、胰腺癌、肾癌等实体肿瘤消融治疗领域中得到应用,并逐步体现出其无热沉效应及对邻近血管、神经、胆道损伤小等独特优势[3-5] 。
该手术方式比较新颖,护理除常规的术前、术中护理外,还需要重点关注装置的使用配合及故障处理、体位的放置、生命体征的观察、管道与消融针的管理等问题。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
肿瘤微创技术:纳米刀(IRE)納米刀是一種全新的腫瘤消融技術,它通過釋放高壓脈沖在腫瘤細胞上形成納米級永久性穿孔,破壞細胞內平衡,使細胞快速凋亡。
納米刀在2012年4月獲美國FDA批准應用於臨床,同時還通過了歐盟的CE認證,截止到2012年底,全球已有一百多個核心腫瘤醫院采用了納米刀技術。
通過眾多臨床研究表明,納米刀是一種安全而又高效的腫瘤治療技術,與其他腫瘤治療技術相比,它具有以下優勢:1.消融時間短治療直徑約3cm的實體腫瘤時,納米刀一般只需90個100毫秒的超短脈沖。
一組治療時間不到一分鍾。
因此即使有三個或四個相互重疊的消融區,全程的消融時間也不會超過5分鍾。
2. 治療區域的血管、神經等重要組織得以保留納米刀消融技術的另一個特點是它能夠保護消融區內重要的組織結構。
所有經過納米刀治療的肝組織中,其重要結構,如肝動脈,肝靜脈,門脈,肝內膽管均能得到良好的保護。
而傳統的消融方式,以升溫或降溫的方式讓蛋白質發生變性,各類蛋白質和DNA均被破壞,以上的結構便會遭到破壞無法修複。
3.不受熱島效應影響納米刀的消融主要是通過電脈沖擊穿細胞膜,在此過程中不會產生熱量,也不會受到其他外界溫度影響。
而傳統的熱消融或者冷消融,一旦消融區域內存在較大血管,其熱量就會被血流帶走,導致周邊消融不徹底,容易造成複發,而納米刀很好地避免了這個問題。
4. 治療徹底,治療邊界清晰納米刀的另一個優勢是,不管腫瘤所處的位置,尺寸大小以及形狀,它都能對腫瘤進行完整消融。
如上文所述,無論腫瘤是靠近血管的,還是形狀不規則或者是大腫瘤,IRE都能對其進行徹底消融。
此外,納米刀消融區邊界清晰,劃界厚度僅為1-2細胞單元。
去治療區和非治療區域涇渭分明,因此,對納米刀的有效性、治療結果以及後續跟蹤都能進行更准確的判斷和評估。
而其他像射頻或微波的消融方式,均會在消融區邊緣處出現“灰色區域”,即消融區的最外圍區域上還有大范圍沒完全滅活的腫瘤細胞。
這是造成日後腫瘤複發的主要隱患之一,而納米刀不存在這一問題。
5. 治療區域可恢複正常功能傳統的消融模式是通過溫度讓組織發生蛋白質變性,繼而出現凝固性壞死,壞死後整個消融區裏的組織結構便不複存在。
然後剩下對髒器有毒性的壞死組織,無法再恢複正常功能。
相反,納米刀則是誘導腫瘤細胞出現凋亡。
凋亡的優點之一就是它能夠利用免疫來促進細胞死亡,人體將把細胞凋亡識別為正常的細胞死亡過程,然後通過細胞吞噬作用將凋亡組織清除掉,促進正常組織的再生與修複。
6. 效果過程可實時監控納米刀治療能夠通過超聲、CT和MR進行影像導航和監控。
在影像設備的輔助下,可以對納米刀探針的定位、標靶區域的消融過程以及最終消融區的大小進行實時監控,而且影像中消融區邊界的精確度可與組織學上的精確度相媲美。
用超聲或CT監控到的消融區與病理分析中測量真實的消融區的尺寸偏差僅有幾毫米。
由此可見,納米刀消融的影像監控的精確度非常高。
影像中還能清楚顯示未消融的殘餘癌症細胞,於此醫生能夠對其再次進行消融。
另外,實時監控還可以讓醫生觀察到消融區周圍組織的變化,從而推斷出並發症出現的可能性,保障病人的安全以及有助於其術後快速恢複。
7. 納米刀可適應更多複雜的病情傳統的消融治療中,一旦腫瘤靠近大血管、靠近膽管、胰管、肝門靜脈等危險區域,則無法進行治療,另外對於前列腺腫瘤或者脊椎附近腫瘤,消融容易導致神經受損而發生癱瘓、性功能喪失等情況。
由於納米刀不損及管道和神經,對於以上情況均能進行安全而有效的治療,對該類患者具有不可替代的作用。
附:來源: Irreversible Electroporation (IRE) | University of Maryland Medical Center Needle-like Probes Destroy Diseased Cells But Spare Healthy TissueIRE uses electrical energy to target tumors at the cellular level. Using short electrical pulses, IRE breaks open the tumor cell walls, causing these cancer cells to die1。
The key difference with IRE compared to other treatments is that this electrical field does not produce extreme heat or cold. It may selectively damage the cancerous cells, sparing healthytissue and structures that may be nearby, allowing us to provide more targeted treatment1,Doctors create a precise electrical field by first mapping the tumor using state-of-the-art computed tomography (CT) technology. The interventional radiologists have a CT scanner in the treatment room, so they are able to make up-to-the minute calculations on the size and location of the tumor.Once we determine the treatment area, we insert the electrode probes through the skin into the tumor, creating a field around the lesion. We then send short, intense electrical pulses - each less than 100 microseconds - between the probes, killing the tumor cells. Then the body's normal healing response takes over, naturally producing new cells and absorbing the cells that have been targeted2.IRE is performed under general anesthesia. The time it takes to place the needles varies based on the size and location of the tumor. Because the procedure is considered to be minimally invasive, recovery time may be faster when compared to some other treatments, with some soreness from the needles themselves. There is little scarring because of the way IRE causes the cancer cells to open and die, taking advantage of the body's natural healing ability.This procedure is another example of the commitment of University of Maryland faculty to bring cutting-edge technology to their patients, offering them another treatment option when traditional surgery may not be effective for their particular condition3.IRE may be a viable alternative for patients with tumors in areas we call ”˜high-rent' zones, difficult-to-treat locations that may be near or touching a blood vessel, nerve or duct4。
1.Ziv Haskal, M.D., professor of diagnostic radiology and surgery at the University of Maryland School of Medicine2.Fred Moeslein, M.D., Ph.D., assistant professor of diagnostic radiology and nuclear medicine at the University of Maryland School of Medicine, and interventional radiologist at the University of Maryland Medical Center.3.E. Albert Reece, M.D., Ph.D., M.B.A., vice president for medical affairs at the University ofMaryland and dean of the University of Maryland School of Medicine.4.Rahul Patel, M.D., assistant professor of diagnostic radiology and nuclear medicine at the University of Maryland School of Medicine, and interventional radiologist at the University of Maryland Medical Center.。