Sciences grant P30-ESO9106. Address reprint requests to
Simplex
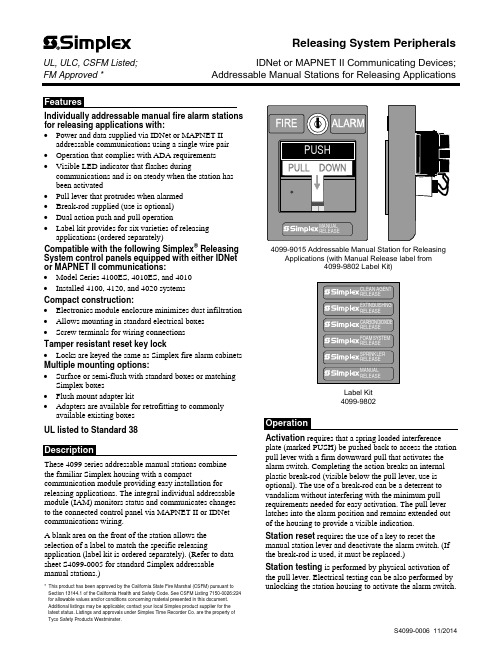
Individually addressable manual fire alarm stations for releasing applications with:∙Power and data supplied via IDNet or MAPNET II addressable communications using a single wire pair∙Operation that complies with ADA requirements∙Visible LED indicator that flashes duringcommunications and is on steady when the station hasbeen activated∙Pull lever that protrudes when alarmed∙Break-rod supplied (use is optional)∙Dual action push and pull operation∙Label kit provides for six varieties of releasing applications (ordered separately)Compatible with the following Simplex® Releasing System control panels equipped with either IDNet or MAPNET II communications:∙Model Series 4100ES, 4010ES, and 4010∙Installed 4100, 4120, and 4020 systemsCompact construction:∙Electronics module enclosure minimizes dust infiltration ∙Allows mounting in standard electrical boxes∙Screw terminals for wiring connectionsTamper resistant reset key lock∙Locks are keyed the same as Simplex fire alarm cabinets Multiple mounting options:∙Surface or semi-flush with standard boxes or matching Simplex boxes∙Flush mount adapter kit∙Adapters are available for retrofitting to commonly available existing boxesUL listed to Standard 38These 4099 series addressable manual stations combinethe familiar Simplex housing with a compact communication module providing easy installation for releasing applications. The integral individual addressable module (IAM) monitors status and communicates changes to the connected control panel via MAPNET II or IDNet communications wiring.A blank area on the front of the station allows the selection of a label to match the specific releasing application (label kit is ordered separately). (Refer to data sheet S4099-0005 for standard Simplex addressable manual stations.)* This product has been approved by the California State Fire Marshal (CSFM) pursuant to Section 13144.1 of the California Health and Safety Code. See CSFM Listing 7150-0026:224 for allowable values and/or conditions concerning material presented in this document. Additional listings may be applicable; contact your local Simplex product supplier for the latest status. Listings and approvals under Simplex Time Recorder Co. are the property of Tyco Safety Products Westminster.4099-9015 Addressable Manual Station for Releasing Applications (with Manual Release label from4099-9802 Label Kit)Label Kit4099-9802Activation requires that a spring loaded interference plate (marked PUSH) be pushed back to access the station pull lever with a firm downward pull that activates the alarm switch. Completing the action breaks an internal plastic break-rod (visible below the pull lever, use is optional). The use of a break-rod can be a deterrent to vandalism without interfering with the minimum pull requirements needed for easy activation. The pull lever latches into the alarm position and remains extended out of the housing to provide a visible indication.Station reset requires the use of a key to reset the manual station lever and deactivate the alarm switch. (If the break-rod is used, it must be replaced.)Station testing is performed by physical activation of the pull lever. Electrical testing can be also performed by unlocking the station housing to activate the alarm switch.Releasing System PeripheralsUL, ULC, CSFM Listed;IDNet or MAPNET II Communicating Devices; FM Approved *Addressable Manual Stations for Releasing ApplicationsAddressable Manual StationsModelDescription4099-9015 Double action, Push operation, Addressable manual station; red housing with white letters and white pulllever; requires label kit 4099-98024099-9802Label kit, white lettering on red background; select the label required for the specific releasing application; types include: Clean Agent, Extinguishing, Carbon Dioxide, Foam System, Sprinkler, and ManualAccessoriesModelDescriptionReference2975-9178 Surface mount steel box, redRefer to page 3 for dimensions 2975-9022 Cast aluminum surface mount box, red2099-9813 Semi-flush trim plate for double gang switch box, red Typically for retrofit, refer to page 4 2099-9814 Surface trim plate for Wiremold box V5744-2, red 2099-9819 Flush mount adapter kit, black Refer to page 4 for details2099-9820Flush mount adapter kit, beige2099-9804 Replacement break-rodPower and Communications IDNet or MAPNET II communications, 1 address per station, up to 2500 ft (762 m) from fire alarm control panel, up to 10,000 ft (3048 m) total wiring distance (including T-Taps)Address Means Dipswitch, 8 positionWire ConnectionsScrew terminal for in/out wiring, for 18 to 14 AWG wire (0.82 mm 2 to 2.08 mm 2)UL Listed Temperature Range 32° to 120° F (0° to 49° C) intended for indoor operation Humidity Range Up to 93% RH at 100° F (38° F) Housing Color Red with white raised letteringMaterialHousing and pull lever are Lexan polycarbonate or equal Pull Lever ColorWhite with red raised letteringHousing Dimensions 5” H x 3 ¾” W x 1” D (127 mm x 95 mm x 25 mm) Installation Instructions579-11354" (102 mm) square box, 2-1/8" (54 mm) minimum 4" Square Box MountSemi-Flush Mount Side ViewSingle Gang Box MountSingle gang box, 2-1/2" deepPreferred Mounting. For surface mounting of theseaddressable manual stations, the preferred electrical boxes are shown in the illustration to the right.Additional MountingReference. Refer to page 4 for Wiremold box mounting compatibility.2975-9178 Box5-3/16" H x 4" W x 2-3/16" D (132 mm x 102 mm x 56 mm)Knockouts located top and bottom2975-9022 Cast Box 5" H x 3-7/8" W x 2-3/16" D (127 mm x 98 mm x 56 mm)4099-9015 Addressable Manual StationFor retrofit and new installations, additional compatible mounting boxes and the required adapter plates are shown in the illustration to the right.Front ViewFlush mount adapter kit Side ViewTyco Fire Protection Products • Westminster, MA • 01441-0001 • USAS4099-0006 11/2014TYCO, SIMPLEX, and the product names listed in this material are marks and/or registered marks. Unauthorized use is strictly prohibited. Lexan is a trademark of the General Electric Co. Wiremold is a trademark of the Wiremold Company.。
一种兼具心功能信息采集的脉搏波诊断系统[发明专利]
![一种兼具心功能信息采集的脉搏波诊断系统[发明专利]](https://img.taocdn.com/s3/m/0f7f5facb307e87100f6964d.png)
专利名称:一种兼具心功能信息采集的脉搏波诊断系统专利类型:发明专利
发明人:张海英,侯洁娜,耿兴光,张以涛
申请号:CN201610855574.6
申请日:20160927
公开号:CN106388788A
公开日:
20170215
专利内容由知识产权出版社提供
摘要:本发明公开了一种兼具心功能信息采集的脉搏波诊断系统。
系统包括:信息采集模块(101),采集待测人员个人信息及采集日期时间等信息;脉搏波采集模块(102),采集脉搏波;心功能信息采集模块(103),采集心功能信息。
数据处理模块(105),对脉搏波以及心功能信号进行处理;判断模块(106),根据数据处理分析模块的处理结果,得出脉搏波与心功能信息的相互关系;主控模块(104),包括数据处理模块与判断模块,并结合信息采集模块采集的信息、脉搏波和心功能信号处理结果以及脉搏波与心功能信号关系,一起传输给显示模块(107)。
本发明引入了心功能信息作为脉搏波诊断系统的辅助信息,提高了脉搏波诊断的准确性。
申请人:中国科学院微电子研究所
地址:100029 北京市朝阳区北土城西路3号
国籍:CN
代理机构:中科专利商标代理有限责任公司
代理人:乔东峰
更多信息请下载全文后查看。
一种用于评价虚拟现实环境下球类运动训练效果的方法及系统[发明专利]
![一种用于评价虚拟现实环境下球类运动训练效果的方法及系统[发明专利]](https://img.taocdn.com/s3/m/48c67a5cfd0a79563c1e72e8.png)
专利名称:一种用于评价虚拟现实环境下球类运动训练效果的方法及系统
专利类型:发明专利
发明人:王丹力,胡海琛,杨心盼
申请号:CN201711313769.9
申请日:20171212
公开号:CN108053864A
公开日:
20180518
专利内容由知识产权出版社提供
摘要:本发明公开了一种用于评价虚拟现实环境下球类运动训练效果的方法及系统。
本系统数据采集单元,用于采集A组待测试者在虚拟现实环境进行训练时的肌电信号及测试成绩、B组待测试者在真实环境进行训练时的肌电信号及测试成绩;以及在真实环境下两组待测试者的考核成绩;数据分析处理单元,用于根据A组待测试者的成绩得到任务绩效Sa;根据B组待测试者的成绩得到任务绩效Sb;根据A组、B组待测试者的肌电信号计算得到对应肌电特征数据;然后根据肌电特征数据的对比结果、任务绩效Sa与任务绩效Sb的对比结果,得到虚拟现实系统的训练效果评价结果。
本发明评价结果更全面、客观和可靠,提高了评价效率。
申请人:中国科学院软件研究所,中国科学院自动化研究所
地址:100190 北京市海淀区中关村南四街4号
国籍:CN
代理机构:北京君尚知识产权代理事务所(普通合伙)
代理人:司立彬
更多信息请下载全文后查看。
Distributed sensor array and method using a pulsed

专利名称:Distributed sensor array and method using a pulsed signal source发明人:Kim, Byoung Yoon,Shaw, Herbert John,Tur, Moshe,Brooks, Janet L.,Fesler, Kenneth A.申请号:EP87305541.2申请日:19870622公开号:EP0251632B1公开日:19930414专利内容由知识产权出版社提供摘要:A distributed sensor system using pulsed optical signals optionally produced by a short coherence length source (100) to provide a phase difference output signal representative of conditions affecting a selected sensor. In one preferred embodiment, an array of fiber-optical sensors (110) are organized in a ladder configuration, with the sensors (110) positioned in spaced relation and defining the rungs of the ladder. Light pulses (201) transmitted through the sensors (110) are multiplexed onto a return arm (114) of the ladder. The multiplexed signals (114) are received by an optical fiber compensating interferometer (200) which coherently couples portions of adjacent multiplexed light signals to produce a phase difference signal representing conditions influencing selected sensors (110). In other preferred embodiments, the system is configured to define a plurality of adjacent Mach-Zehnder interferometers (110) which provide output signal pairs (205) which coherently couple 'to yield a phase difference signal directly representing the environmental effects on a particular sensor (117). Functional equivalents of the Mach-Zehnder interferometer configurations comprise configurations including adjacent Michelson interferometers. A phase and amplitudemodulation technique and apparatus (Figure 8) is disclosure for providing heterodyned output signals from the distributed sensor system. I申请人:THE BOARD OF TRUSTEES OF THE LELAND STANFORD JUNIOR UNIVERSITY 地址:ENCINA 105 STANFORD UNIVERSITY; STANFORD CALIFORNIA 94305代理机构:Rushton, Ronald更多信息请下载全文后查看。
测试图形的选取方法和装置、构建光刻模型的方法和装置[发明专利]
![测试图形的选取方法和装置、构建光刻模型的方法和装置[发明专利]](https://img.taocdn.com/s3/m/2b038862d0d233d4b04e6984.png)
专利名称:测试图形的选取方法和装置、构建光刻模型的方法和装置
专利类型:发明专利
发明人:赵利俊,韦亚一,董立松,张利斌
申请号:CN201810054861.6
申请日:20180119
公开号:CN108153995A
公开日:
20180612
专利内容由知识产权出版社提供
摘要:本申请实施例公开了一种测试图形的选取方法和装置,该选取方法包括根据设计规则、实际电路版图和/或随机版图设计初始测试图形;根据简化模型对初始测试图形进行光学仿真,得到初始测试图形在预设参数取值范围内的分布;根据初始测试图形在预设参数取值范围内的分布从初始测试图形中选取关键测试图形,关键测试图形用于构建光刻模型中的参数校准。
利用该选取方法选出的测试图形用于构建光刻模型,能够提高光刻模型的建模效率以及光刻模型的准确度。
此外,本申请还尤其涉及一种构建光刻模型的方法和装置。
申请人:中国科学院微电子研究所
地址:100029 北京市朝阳区北土城西路3号中国科学院微电子研究所
国籍:CN
代理机构:北京集佳知识产权代理有限公司
更多信息请下载全文后查看。
与类风湿关节炎相关的单个基因单核苷酸多态性位点及其应用[发明专利]
![与类风湿关节炎相关的单个基因单核苷酸多态性位点及其应用[发明专利]](https://img.taocdn.com/s3/m/2d9eb42ebb4cf7ec4bfed09d.png)
专利名称:与类风湿关节炎相关的单个基因单核苷酸多态性位点及其应用
专利类型:发明专利
发明人:刘万里,孙晓麟,徐利玲,栗占国,沈志勋
申请号:CN201510079225.5
申请日:20150213
公开号:CN104630374A
公开日:
20150520
专利内容由知识产权出版社提供
摘要:本发明公开了与类风湿关节炎相关的单个基因单核苷酸多态性位点及其应用。
本发明所保护的技术方案是检测人基因组中rs1050501的多态性或基因型的物质在制备筛查类风湿关节炎患者产品中的应用和检测人基因组中rs1050501的多态性或基因型的物质在制备预测类风湿关节炎患者病情的产品中的应用。
可将检测rs1050501的多态性或基因型的物质与其它物质(如检测其它的与麻风病相关的单核苷酸多态性或基因型的物质)联合在一起制备筛查麻风病患者或预测类风湿关节炎患者病情的产品。
申请人:清华大学,北京大学人民医院
地址:100084 北京市海淀区100084信箱82分箱清华大学专利办公室
国籍:CN
代理机构:北京纪凯知识产权代理有限公司
更多信息请下载全文后查看。
Agilent Technologies Test and Measurement Call Cen

United States:Agilent TechnologiesTest and Measurement Call Center P .O. Box 4026Englewood, CO 80155-4026 (tel)180****4844Canada:Agilent Technologies Canada Inc.5150 Spectrum Way Mississauga, Ontario L4W 5G1(tel)187****4414Europe:Agilent Technologies Test & MeasurementEuropean Marketing Organisation P .O. Box 9991180 AZ Amstelveen The Netherlands(tel) (31 20) 547 9999For more information aboutAgilent Technologies test and measurement products, applications, services, and for a current sales office listing, visit our web site:You can also contact one of the following centers and ask for a test and measurement sales representative.Japan:Agilent Technologies Japan Ltd.Measurement Assistance Center 9-1, Takakura-Cho, Hachioji-Shi,Tokyo 192-8510, Japan (tel) (81) 426 56 7832(fax) (81) 426 56 7840Latin America:Agilent TechnologiesLatin American Region Headquarters 5200 Blue Lagoon Drive, Suite #950Miami, Florida 33126U.S.A.(tel) (305) 267 4245(fax) (305) 267 4286 Australia/New Zealand:Agilent Technologies Australia Pty Ltd 347 Burwood Highway Forest Hill, Victoria 3131(tel) 1-800 629 485 (Australia)(fax) (61 3) 9272 0749(tel) 0 800 738 378 (New Zealand)(fax) (64 4) 802 6881 Asia Pacific:Agilent Technologies24/F, Cityplaza One, 1111 King’s Road,Taikoo Shing, Hong Kong (tel) (852)-3197-7777(fax) (852)-2506-9284Related Agilent Literature8163ALightwave Multimeter Ordering Guide,p/n 5968-3582E8163ALightwave Multimeter Technical Specifications,p/n 5962-9321E 8163ALightwave Multimeter Configuration Guide,p/n 5968-3581ETechnical data is subject to change Copyright © 1999 Agilent Technologies Printed in Germany 12/99 (B.O.L.A.Y. GmbH)P/N 5968-3404E/comms/lightwave1981Agilent 8163ALightwave Multimeter•precise •reliable •fast/comms/lightwaveProduct Overview“Working together should be a standard.”The Agilent 8163A Lightwave Multi-meter is a basic measurement tool in the fiber optic industry . It ensures accurate and fast results, even for your most demanding measurements on optical components and systems.The 8163A Lightwave Multimeter is the successor to the highly popular 8153A Lightwave Multimeter. It builds on all the key attributes that made the 8153A Lightwave Multimeter the standard in Research and Development and in Manufacturing.Its modular format makes it flexible enough to meet your changing mea-surement needs, whether you are measuring optical power , insertion loss or return loss for single- or multimode components.The lightwave multimeter systemincludes the mainframe and a variety of plug-in modules for set-ups requiring:•single or dual channel power meters,•single or dual fixed light sources,•compact tunable laser modulesThe 8163A Lightwave Multimeter helps ease your work-load by offering several advanced functions that turn your 8163A into a powerful measure-ment system.Without needing an external controller ,built-in application software guides you through the step-by-step proce-dures needed for measurement tasks such as measuring loss, monitoring stability or logging data.For example, for long term monitoring you only need to input the total mea-surement time and the averaging time per sample – the 8163A Lightwave Multimeter does the rest. After the test is complete, the result can be displayed numerically or graphically on the display or the result can be sent to a printer.You can easily integrate the 8163A Lightwave Multimeter into your test environment by using plug & play drivers over GPIB, or by using the configurable hardware input and out-put trigger ports.The New StandardFeatures and BenefitsH i g h B a n d w i d t hH i g h B a n d w i d t h“The Agilent family of optical component testequipment. Because workingtogether should be a standard.”Measurements requiring a tunable source If you need to make measurements at various fixed wavelengths, or if the test device must be characterized as a function of wavelength, then the compact tunable laser module is the ideal candidate for your test needs.In combination with a power sensor or an optical head you can setup a complete measurement system for wavelength dependent loss.Measurements requiring a stable fixed sourceTo take the uncertainty out of moni-toring loss over long periods of time,Agilent’s sources are stabilized and very insensitive to backreflections.For your convenience there are single and dual wavelength source modules,available with an output power of up to +13 dBm. The output power of the sources can be attenuated for applica-tions where you need lower power levels.Precise, sensitive, stable and fast power measurementsYou can be sure of the best possible measurement results thanks to the excellent accuracy , high linearity and low polarization dependent loss (PDL)of our full range of power sensors and optical heads.To meet your test requirements, our range of sensors and heads cover the important wavelengths and power ranges you need. And you will like the measurement speed which can come down to 100 µs. A broad variety of advanced interfaces and adapters makes it easy to connect your test devices.To help you work efficiently and quick-ly and to increase your throughput and yield, the input ports are desi-gned to eliminate multiple reflections – the cause of many measurement errors.The Agilent 8163A Lightwave Multimeter allows engineers to count on the accuracy of their measurements more than ever.Best possiblemeasurement resultsDWDMDWDMUpgradable FirmwareTo protect your investment for the future, the Agilent 8163A Lightwave Multimeter is designed for easy firm-ware upgrades as new modules and features become patibilityTo protect your existinginvestment the8163A main-frame is compatible with themodules from the 8153ALightwave Multimeter series.Also you can use both themodules of the 8163A and8153A series together in the8163A Lightwave MultimeterMainframe.The programming syntax used bythe 8163A Multimeter mainframe iscompatible with the 8164A LightwaveMeasurement System (the tunablelaser family), the 8166A LightwaveMultichannel System and with the8153A Lightwave Multimeter.The 8163A mainframe is compatiblein height and width with the 8153Aseries, making it easy for you to addor substitute the 8163A to your racksystems.Flexible enough to meet changingmeasurement needs.“Working togethershould be a standard.”High PrecisionHigh Precision8163A Lightwave MultimeterSelected Specifications 1)Display:Graphical display , monochrome Interfaces:GPIB, RS232C, Parallel Printer Interface (Centronics)Programming*:SCPI Standard, compatiblewith programming syntax of 8164A Lightwave Measurement System, 8166A Lightwave Multichannel System, 8153A Lightwave Multimeter.*for details please refer toProgramming guide P/N 08164-910161)For full specifications, and the test conditions, see the Technical Specifications p/n 5962-9321E 2)All optical heads have to be operated with the single (81618A) or dual (81619A) Interface Module.H typ ±0.003 dBH i g h B a n d w i d t hH i g h B a n d w i d t hThe 8163A Mainframe has two slots for any combination of the modules listed in this document, or modules of the 8153A Lightwave Multimeter series.Connector interfaces should also be ordered for each input and output, as well as any bare fiber adapters you require.If you want to use optical heads, you also need an interface module 81618A (single) or 81619A (dual) and you may need filter holders, filters, lenses and connector adapters.Ordering InformationConnection to Test DevicesThe 8163A Lightwave Multimetersupports a wide range of fiber connec-tors. For details please refer to the 8163A Configuration Guide. This gives information on the connector interfaces and bare fiber adapters for use with these modules, as well as the filter holders, filters, lenses and connector adapters required for the optical heads.Agilent 8163A Lightwave MultimeterStimulus Response SolutionDWDMDWDM“Working together should be a standard.”。
原位透射电镜 开放式样品池或液相芯片

原位透射电镜开放式样品池或液相芯片下载温馨提示:该文档是我店铺精心编制而成,希望大家下载以后,能够帮助大家解决实际的问题。
文档下载后可定制随意修改,请根据实际需要进行相应的调整和使用,谢谢!并且,本店铺为大家提供各种各样类型的实用资料,如教育随笔、日记赏析、句子摘抄、古诗大全、经典美文、话题作文、工作总结、词语解析、文案摘录、其他资料等等,如想了解不同资料格式和写法,敬请关注!Download tips: This document is carefully compiled by the editor. I hope that after you download them, they can help you solve practical problems. The document can be customized and modified after downloading, please adjust and use it according to actual needs, thank you!In addition, our shop provides you with various types of practical materials, such as educational essays, diary appreciation, sentence excerpts, ancient poems, classic articles, topic composition, work summary, word parsing, copy excerpts, other materials and so on, want to know different data formats and writing methods, please pay attention!原位透射电镜在材料科学领域发挥着重要作用,通过其高分辨率、实时观察等优势,可以帮助研究人员深入了解材料的微观结构和性能。
小波阈值去噪方法、装置、设备及介质

专利名称:小波阈值去噪方法、装置、设备及介质专利类型:发明专利
发明人:勾钺,卢增雄,齐月静,李璟,胡丹怡,卢越峰申请号:CN202111139317.X
申请日:20210927
公开号:CN113971641A
公开日:
20220125
专利内容由知识产权出版社提供
摘要:本公开提供一种小波阈值去噪方法,包括:获取待去噪信号及理想信号;初始化去噪参数,利用去噪参数对待去噪信号进行去噪,得到第一噪声信号;计算待去噪信号与理想信号之间的均方误差作为第一适应度;计算第一噪声信号与理想信号之间的均方误差作为第二适应度;比较第一适应度及第二适应度,若第二适应度小于第一适应度,更新去噪参数,利用更新后的去噪参数对待去噪信号进行去噪,得到第二噪声信号;计算第二噪声信号与理想信号之间的均方误差,作为第三适应度;比较第三适应度及第二适应度,若第三适应度小于第二适应度,更新去噪参数进行去噪及适应度计算,以此迭代,直至获得最小适应度;利用最小适应度对应的去噪参数对待去噪信号进行去噪。
申请人:中国科学院微电子研究所
地址:100029 北京市朝阳区北土城西路3号
国籍:CN
代理机构:中科专利商标代理有限责任公司
代理人:王文思
更多信息请下载全文后查看。
光探测器及其制备方法

专利名称:光探测器及其制备方法
专利类型:发明专利
发明人:薛春来,王啸宇,丛慧,徐驰,万丰硕,徐国印,谢长江申请号:CN202111239248.X
申请日:20211025
公开号:CN113972295A
公开日:
20220125
专利内容由知识产权出版社提供
摘要:本发明公开了一种光探测器,包括:衬底;二氧化硅层,覆盖于衬底上;脊型波导结构,设置于二氧化硅层上,脊型波导结构包括:第一氮化硅层,设置于二氧化硅层上;石墨烯层,设置于第一氮化硅层上;绝缘层,设置于石墨烯层上,所述绝缘层上设有至少一对电极孔;以及第二氮化硅层,设置于绝缘层上,并位于成对的电极孔之间,使得第二氮化硅层相对于绝缘层突出,以形成脊形部;以及第一电极和第二电极,分别设置于成对的电极孔中,并与所述石墨烯层电连接。
申请人:中国科学院半导体研究所
地址:100083 北京市海淀区清华东路甲35号
国籍:CN
代理机构:中科专利商标代理有限责任公司
代理人:樊晓
更多信息请下载全文后查看。
一种海洋牧场声学监测系统和方法[发明专利]
![一种海洋牧场声学监测系统和方法[发明专利]](https://img.taocdn.com/s3/m/ef31f19b7fd5360cbb1adb7e.png)
专利名称:一种海洋牧场声学监测系统和方法专利类型:发明专利
发明人:张纯,许枫,司纪锋,鄔松,王耀宾,张乔申请号:CN201410829233.2
申请日:20141225
公开号:CN105785968A
公开日:
20160720
专利内容由知识产权出版社提供
摘要:本发明提供了一种海洋牧场声学监测系统及方法,所述系统包含:监测节点和数据处理模块;监测节点包含:换能器、收发控制单元及传感器;换能器,用于接收海洋牧场中海洋生物的回波信号,并将回波信号传输至数据处理模块;传感器,用于获取海洋牧场环境信息,并将海洋牧场环境信息传输至数据处理模块;收发控制单元,用于根据声学参数产生声波脉冲信号,并采用声波脉冲信号激励所述换能器将声波脉冲信号辐射至牧场水体中,同时接收海洋牧场中海洋生物的回波信号,并剔除回波信号中的噪声;数据处理模块:用于将各个监测节点上传的数据进行处理和信息融合,并通过统计和分析处理,以实时得到海洋牧场中海洋生物的活动情况、密度和生物资源量信息。
申请人:中国科学院声学研究所,中国科学院声学研究所北海研究站
地址:100190 北京市海淀区北四环西路21号
国籍:CN
代理机构:北京方安思达知识产权代理有限公司
更多信息请下载全文后查看。
A DNext 血液 DNA 试剂盒(磁珠法)说明书 (仪器配套使用)

产品储存产品可室温运输,收到后请于2~8℃贮存。
技术支持艾德科技(北京)有限公司研发部:e-mail: 电话:。
产品介绍本产品专为磁珠法核酸自动提取仪设计,适合从200 µl新鲜的或者是冷冻贮藏的抗凝全血中分离纯化总DNA。
试剂盒提供的试剂可预先分装到2.2 ml的96深孔板,配合磁珠法核酸自动化提取仪,只需在装有Buffer SL的孔中加入血样,即可由仪器自动化完成血液DNA 释放、吸附、洗涤及洗脱等一系列过程,最后获得的DNA溶解在Buffer TE中,并可立即用于各种分子生物学实验。
用户需自备的试剂与物品1.96深孔板(2.2 ml),如果用户需要预分装好试剂的96深孔板及磁力套,请另购产品序号为A-3012096的预分装磁珠法血液DNA试剂盒2.移液器吸头(为避免样品间的污染,请选用含有滤芯的移液器吸头)3.一次性手套及防护用品和纸巾4.磁珠法核酸自动化提取仪使用前准备1.在96深孔板第1列和第7列每孔加入600 µl Buffer SL;2.在96深孔板第2列和第8列每孔加入800 µl Buffer WA;3.在96深孔板第3列和第9列每孔加入900 µl Buffer WB;4.在96深孔板第4列和第10列每孔加入900 µl Buffer WC;5.在96深孔板第5列和第11列每孔加入900 µl Buffer MG;6.在96深孔板第6列和第12列每孔加入100 µl Buffer TE;操作步骤1.在已分装好试剂的96深孔板中的第1列和第7列各孔中加入200 µl抗凝全血,将96深孔板放入核酸自动化提取仪中。
2.按以下步骤设置核酸自动纯化仪中的程序:1)磁力棒深入到磁力套中,再插入第5列和第11列吸取磁珠,将磁珠转移到第1列和第7列各孔中,移出磁力棒。
2)用磁力套在第1列和第7列持续中速和快速间隔拍打混匀10分钟。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Phase II Clinical Trial Design for Noncytotoxic Anticancer Agentsfor which Time to Disease Progression is the Primary EndpointRunning title: Phase II Trial Design for Time to Progression Rosemarie Mick, M.S., John J. Crowley, Ph.D. and Raymond J. Carroll, Ph.D.Department of Biostatistics and Epidemiology, University of Pennsylvania School of Medicine, Philadelphia (R.M.), Program in Biostatistics, Fred Hutchinson Cancer Research Center, Seattle (J.J.C.) and Department of Statistics, Texas A&M University, College Station (R.J.C.)Dr. Carroll’s research was supported by National Cancer Institute grant CA-57030 and by the Texas A&M Center for Environmental and Rural Health via National Institute of Environmental Health Sciences grant P30-ESO9106.Address reprint requests to:Rosemarie Mick, M.S.University of PennsylvaniaDepartment of Biostatistics and Epidemiology609 Blockley HallPhiladelphia, PA 19104email: rmick@ABSTRACTPhase II evaluation is a critical screening step in the development of new cancer treatments. Historically, anticancer agents have been cytotoxic; they kill existing cells. As such, the primary endpoint for phase II evaluation has been tumor response rate, the percentage of patients whose tumors shrink >50%. Biotechnology has led to promising new anticancer agents that are cytostatic. In contrast to cytotoxics, these agents modulate tumor environments and/or cellular targets and are expected to delay tumor growth. Phase II evaluation of such agents may instead focus on failure time endpoints, such as time to disease progression. We examine a phase II trial design that evaluates clinical benefit by comparing sequentially-measured paired failure times within each treated patient. Clinical efficacy is defined by a hazard ratio.Assuming patients eligible for a phase II study of a new cytostatic agent have failed previous cancer treatment, their most recent prior time to progression interval, TTP1, is uncensored. Time to progression after the cytostatic agent, TTP2, may or may not be censored at analysis. The design is motivated by a “growth modulation index” (TTP2/TTP1) and the proposition that a cytostatic agent be considered effective if the index is greater than 1.33. A χ2 test statistic is employed to evaluate the paired failure time data (TTP1, TTP2). The degree of correlation between the paired failure times is a key feature of this design. Power of the test was evaluated through simulation of trials. Assuming a null hazard ratio equal to 1.0, a trial designed to detect an alternative hazard ratio equal to 1.3, based on accrual of 25 patients/year for 2 years (50 patients total) and with an additional 2 years of follow-up, has 25%, 46%, and 83% power based on correlations of 0.3, 0.5 and 0.7, respectively. These results demonstrate efficiency of the trial design, given moderate to strong correlations between paired failure times.KEY WORDS: Phase II trial, cytostatic agent, time to progression, paired failure times.INTRODUCTIONThe primary goals of phase II clinical trials are to estimate efficacy and toxicity of a new anticancer agent or combination of agents [1,2]. Phase II evaluation is a critical screening step in the development of new cancer treatments. Evidence of clinical efficacy demonstrated in a phase II trial often determines whether the new treatment warrants further study.Historically, anticancer agents have been cytotoxic; they work by killing existing cancer cells and/or by interfering with the generation of new cancer cells. Effectiveness is determined by the ability of the cytotoxic agent or combination of agents to shrink or eradicate tumors in patients. The primary endpoint for phase II trials has been tumor response rate, defined as the proportion of treated patients whose tumors shrink by more than 50%. To demonstrate clinical efficacy, a new agent must provide evidence for a meaningful clinical benefit. As such, phase II trials are designed to identify agents that yield a population-specific response rate (e.g., a true response rate >20%), which varies by cancer site, stage of disease and prior treatment history. It follows that a key assumption of any phase II trial is the selection of a reasonable target response rate. Most often, we rely on published studies to determine historical estimates which may be augmented within the phase II trial by randomization of a modest fraction of patients to an accepted standard treatment [3,4].Standard phase II trial designs for response rates exhibit a number of favorable features. In many cases, tumor response can be evaluated reliably after several courses of treatment such that timely evaluation of the trial results can be completed within months after the final patient has been treated. A number of multistage designs now exist that meet both statistical and ethical considerations [5-10]. These designs allow for sequential treatment and evaluation of modestly sized cohorts of patients. Early stopping of the trial is allowed if accumulated evidence for clinical efficacy is lacking. Randomized phase II designs allow for the simultaneous enrollment to and screening of several promising regimens [11]. These trials impose some balance in patient features and, although direct comparisons are not intended, they allow for an initial priority ranking among treatment arms.Recently, biotechnology has led to the discovery of many promising anticancer agents. Antiangiogenesis factors, growth modulators (e.g., farnesyl transferase and signal transduction inhibitors), monoclonal antibodies and adenovirus (gene therapy) vaccines are all poised for phase II evaluation. Interestingly, many of these agents are not cytotoxic but cytostatic. Instead of killing cells, they appear to modulate tumor environments and/or cellular targets. For example, antiangiogenesis factors block the growth of new blood vessels that surround and feed a tumor [12]. Without increased blood supply, a tumor cannot grow. It follows that many biologic agents, such as angiogenesis inhibitors, may not beexpected to shrink tumors, but are more likely to delay tumor progression. This mechanistic difference has become well-appreciated by those developing cytostatic agents [13-16]. Thus, the paradigm for drug development must be altered for noncytotoxic agents. In fact, several companies that develop matrix metalloproteinase inhibitors (MMPIs) have considered skipping phase II evaluation altogether, and proceeding instead directly to phase III trials. These adjuvant studies are designed to test the impact of MMPIs on disease recurrence [17-19].How do we design rational phase II trials that exploit the expected mechanisms of these novel agents? First, we must consider appropriate endpoints for clinical and biologic effects. For many agents, supporting endpoints, such as biomarkers that measure the mechanisms of biologic action, have not been discovered. Because a delay in disease progression is the expected clinical outcome, failure time endpoints are preferable to response rates. Time to progression, defined as the time from initiation of therapy to first documentation of disease progression or worsening of disease-related symptoms, is one such endpoint. Alternatively, progression-free survival may be employed in which death is included as failure. As with any phase II trial, definition of meaningful clinical benefit is a key issue. A population-specific failure-time endpoint (e.g., the median failure time or failure rate at a specific time point) is needed. Historical failure-time estimates are subject to the same sources of variability (e.g., types of patients treated or treatment intensity) and precision (e.g., study size) as historical response rate estimates. And because the precision of failure-time endpoints is also dependent on observed events, the maturity of historical studies must be considered.Trials with time to progression as the primary endpoint pose some challenges not previously encountered with phase II trials of event rates. Beyond the usual challenge of identifying trials of comparable historical controls, the definition and measurement of time to progression must be consistent with current usage. Study results may not be immediate as with standard phase II trials unless short term endpoints, such as 3- or 6-month failure-free rates, are employed. Multistage designs will not be feasible for certain patient populations, because extended follow-up for disease progression may be necessary, precluding early termination.PHASE II TRIAL DESIGNPhase II trial designs for failure-time endpoints that fall within a hypothesis testing framework and minimize accrual to inferior treatments are desirable because of statistical and ethical considerations [20]. The motivation for the proposed design stems from the “growth modulation index,” a method of evaluation suggested by Von Hoff in which each patient serves as his/her own historical control [14]. The growth modulation index is defined as the ratio of a patient’s time to progression on a phase II cytostatictreatment, TTP2, relative to the time to progression observed from the patient’s most recent prior anticancer treatment, TTP1, which serves as the patient-specific historical control value. Most recent time time to progression may be viewed as a clinical surrogate for tumor sensitivity at initiation of cytostatic treatment, an aggregate of patient- and tumor-level factors.Von Hoff suggested that a cytostatic agent be considered effective if the growth modulation index, the ratio TTP2/TTP1, is greater than 1.33, implying a null value of 1.0. Alternatively, one could hypothesize that by the natural history of the disease, one would expect TTP2 to be shorter than TTP1,which implies null values less than 1.0. If a biologic agent demonstrates an impact on this natural history then one may argue that meaningful clinical efficacy has been demonstrated. Thus, a range of index values, posed as null and alternative hypotheses, are discussed in the simulation sections that follow. The natural pairing of these failure times is the basis for the proposed trial design.Extensions of standard analytic methods such as proportional hazards or log-linear models have been explored for paired failure-time data [21]. Such data may arise from a single failure-time endpoint from two matched individuals or from two concurrently-measured endpoints (e.g., survival and progression-free survival) within an individual. In the proposed design, sequentially-measured paired failure times, TTP1 and TTP2, within an individual are the basis for the statistical framework. An important feature of this design is the inherent correlation between the paired observations. The assumed positive correlation stems from the widely-held premise that patients who experience relatively shorter (or longer) progression-free intervals under an initial treatment regimen, would also experience relatively shorter (or longer) intervals under a subsequent treatment regimen. The likelihood of settings supporting negative correlation is low, due to the fact that opposing paired outcomes, such as patients who experience relatively shorter progression-free intervals under an initial treatment regimen and relatively longer intervals under a subsequent treatment regimen, are much less frequent. As one would expect, if the positive correlation is strong, then the trial design may be highly efficient and require fewer patients.A sound statistical design that exploits such correlation and is efficient would satisfy both statistical and ethical considerations.ANALYSIS OF PAIRED FAILURE-TIME DATAA requirement of the design is that patients eligible for the trial of a new cytostatic agent must have failed at least one previous treatment for their cancer, thus TTP1is uncensored. This requirement may be achieved through study eligibility criteria. Time to progression on the cytostatic treatment, TTP2, may or may not be censored at the time of analysis. The statistical framework is defined by paired failure times (TTP1, TTP2), censoring status at TTP2 and null and alternative hypotheses about the effect of the cytostatic agent.Failure times are assumed to follow an exponential distribution which decays at some arbitrary hazard rate. Under the assumption of proportional hazards, a test about the efficacy of a treatment is determined by the value of the hazard ratio (HR). In this setting, a cytostatic agent may be considered effective if, on average, TTP2 > TTP1. Von Hoff’s proposed index suggests a null hazard ratio HR0 equal to 1.0 (no benefit) compared to an alternative hazard ratio HR A equal to 1.33 (meaningful benefit). Alternatively, if one expects increasingly shorter progression-free intervals with successive treatment, then a cytostatic agent may be considered effective if, on average, TTP2= TTP1. This setting suggests HR0 is less than 1.0 compared to HR A equal to 1.0. For example, testing HR0 equal to 0.7 compared to HR A equal to 1.0 translates into an effective hazard ratio of 1.43. It should be emphasized that in this latter setting, a hazard ratio equal to 1.0 would be evidence of clinical efficacy.Hypothesis tests about the hazard ratio from paired data may be conducted under alog-linear model [21]. A test of null HR0equal to 1.0 is equivalent to a test of ln[HR0] equal to 0 (similarly HR0 equal to 0.7 is equivalent to ln[HR0] equal to -0.3567). Under a log-linear model in which β0 denotes the null natural log hazard ratio, the values of natural log-transformed paired failure times are compared. Briefly, failure time pairs in which ln[TTP2] > ln[TTP1] + β0 or in which ln[TTP2] < ln[TTP1] + β0and for which TTP2is uncensored are scored as 1 or -1, respectively. Pairs in which ln[TTP2] < ln[TTP1] + β0 and for which TTP2 is censored, do not contribute to the test. Under β0, the score r s takes on the values –1 or 1, each with probability 0.5. Excluding pairs for which r s cannot be specified does not bias the test. The test statistic is a function of sums of squares of the scores for contributing failure-time pairs and has an approximate χ2distribution. Further details on the hypothesis testing framework for correlated failure times are described in the appendix.SIMULATION METHODSThe basis for the simulation was generation of correlated exponential failure times, assumed to arise in an individual patient. Hypothesis tests about the natural log hazard ratio (β) were then conducted on simulated patient data for trials of various sizes.The first step was to generate correlated exponential failure times to represent the uncensored failure time TTP1 and censored or uncensored failure time, TTP2. The distribution of TTP1 was defined to have a median value, m, equal to 1 year. The distribution of TTP2 was defined to have a median value equal to m[exp(β)], resulting in a hazard ratio equal to exp(β).We generated correlated exponential failure times as follows. Let X0, X1 and X2 be independent standard gamma random variables with shapes θ0, (1 - θ0) and (1 - θ0), respectively. Then, from properties of the gamma distribution, X0 + X1 and X0 + X2 are marginally exponential random variables with mean 1 and their covariance is var(X0) = θ0 and hence, their correlation = θ0 [22]. We defined TTP1 and TTP2 to beTTP1 = (X0 + X1)m and TTP2 = (X0 + X2)m[exp(β)] .ln[2] ln[2]These distributions have medians m and m[exp(β)], respectively, and correlation θ0.The next step of the simulation addressed censoring of TTP2. Two years of patient accrual and 2 additional years of follow-up (total duration 4 years) were assumed, as these were felt to reflect the conduct of most phase II investigations. Uniform censoring of TTP2 was assumed with minimum and maximum follow-up of 2 and 4 years, respectively (~U[2,4]). A patient’s TTP2 observation was generated and if it was greater than or equal to the censoring time, then TTP2 was set equal to the censoring time and the patient was considered censored.Trials with varied sample and effect sizes were simulated so that trends in power could be evaluated. We investigated trial sizes that ranged from 20 to 100 patients in increments of 10 patients. A number of null and alternative hazard ratios were investigated. A null hazard ratio equal to 1.0 was tested (employing log hazard ratio of zero) against alternative hazard ratios that ranged from 1.1 to 2.0 in increments of 0.1, while a null hazard ratio equal to 0.7 (log hazard ratio of -0.3567) was tested against alternative hazard ratios that ranged from 0.8 to 1.7.For each study, a significance test was performed on the paired observations using the method described in the appendix. One thousand trials were simulated for each sample size and effect size combination. Power was defined as the percentage of simulated trials that exhibited a significant result at the 0.05 level (χ2 > 3.84). Based on the normal approximation to the binomial and 1000 trials, the width of the 95% confidence interval for power can be no greater than 3%. All simulations were performed in S-PLUS Version 4.5 (MathSoft, Inc.)Since the magnitude of correlation and its impact on power were of particular interest, correlation between paired failure times was allowed to vary over a wide range (0.1 to 0.9). Weak, moderate and strong correlation among paired failure times, represented by Pearson correlation values of 0.3, 0.5, and 0.7, respectively, were selected for presentation. Three dimensional (X axis = study size, Y axis = alternative hazard ratio and Z axis = power) response surfaces were constructed for each level ofcorrelation. Nonparametric surfaces were fit with bivariate splines without smoothing using SAS (Version 6.12, SAS Institute, Inc) PROC G3GRID and plotted with SAS PROC G3D. Contour plots were then constructed based on the fitted response surfaces by SAS PROC GCONTOUR. Contours, also known as isoboles, of varying combinations of study size and effect size, represent constant values of power (e.g., 80%).SIMULATION RESULTSA total of 1620 unique combinations of study size, effect size and correlation among failure times was studied. Power properties were evaluated by 1000 simulated clinical trials for each combination of factors. Table 1 displays the results for a subset of simulations representing combinations of study and effect size and degree of correlation. Assuming a null hazard ratio equal to 1.0, a trial designed to detect an alternative hazard ratio equal to 1.3 (Von Hoff’s suggested definition of clinical efficacy), based on accrual of 50 patients over 2 years and with an additional 2 years of follow-up, has 25%, 46%, and 83% power based on correlations of 0.3, 0.5 and 0.7, respectively.In Figures 1a to 1f, a null hazard ratio equal to 1.0 was assumed. As noted in Figures 1a to 1c, the response surfaces crest in the upper left background, indicating expected increases in power for increasing effect size and study size. Power increased sharply with increasing correlation between paired failure times. In Figures 1d to 1f, 80%, 85% and 90% power contours are presented. A trial designed to accrue 50 patients over 2 years has 80% power to detect hazard ratios approximately equal to 1.90, 1.60 and 1.30 based on correlations of 0.3, 0.5 and 0.7, respectively.In Figures 2a to 2f, a null hazard ratio equal to 0.70 was assumed. As mentioned previously, a trial designed to detect an alternative hazard ratio equal to 1.0, as evidence of clinical efficacy, translates into an “effective” hazard ratio of 1.43. Figures 2a to 2c, again display increases in power with increasing effect and study size. Power increased with increasing correlation. A trial designed to detect an alternative hazard ratio equal to 1.0 with 50 patients accrued over 2 years has 46%, 69% and 99% power based on correlations of 0.3, 0.5 and 0.7, respectively. Figures 2d to 2f display 80%, 85% and 90% power contours.A trial designed to accrue 50 patients over 2 years has 80% power to detect hazard ratios approximately equal to 1.30, 1.10 and 0.90 based on correlations of 0.3, 0.5 and 0.7, respectively. These results clearly demonstrate the efficiency of the study design, in the presence of moderate to strong correlation.OBSERVED PAIRED FAILURE-TIME DATAIt is obvious that the implementation of the proposed phase II design relies on a reasonable estimate of the correlation between sequentially-measured paired failure times. There are no publishedreports that describe this correlation, although clinicians and biostatisticians have opinions on the range of relevant values. Table 2 displays correlations between sequentially-measured paired failure times obtained from three cancer cooperative group trials [23-25]. These studies are not drawn from a well-defined sampling strategy and therefore may not be representative. The Pearson correlations ranged from 0.19 to 0.56. Heterogeneity of correlations is expected among differing study populations due to variations in disease site and stage, degree of previous treatments and tumor sensitivity to second line treatments. Exclusion of a single outlier pair in CALGB 8751 resulted in Pearson and Spearman values of 0.25 and 0.43, respectively. For each patient, the ratio TTP2/ TTP1was calculated. Interestingly, the median of the distribution for the ratio was less than 1.0 for all three studies. When analyzed by the paired failure time method, none of these studies yielded a significant result in favor of the second failure time, relative to a null hazard ratio of 0.7.DISCUSSIONIt is evident that novel phase II trial designs are needed to evaluate new anticancer treatments that are expected to delay tumor growth but not shrink tumors, like standard cytotoxic agents. Clinicians involved in early development of such agents clearly understand this challenge and are seeking statistically sound solutions. Eckhardt et al. recently report on their completed phase I trial of SU101, an agent that interferes with signal transduction by inhibition of platelet-derived growth factor receptor-mediated cellular processes [26]. In contemplating the upcoming phase II evaluation of SU101, the authors acknowledge that cytostasis is an effect that will not be addressed adequately by standard phase II trials. They suggest that efficacy may best be measured by time to progression, quality of life, symptomatic improvement or overall survival. Eisenhauer has proposed an alternative measure of clinical benefit, the progression rate, defined by the percentage of patients who progress in the first 8 weeks of treatment [27]. Based on her review of the National Cancer Institute of Canada Clinical Trials Group experience, several recently evaluated cytotoxic agents that demonstrated acceptable response rates during phase II evaluation also yielded low rates of on-treatment progression.Currently, phase II trials of failure-time endpoints are designed as single arm comparisons to historical control estimates. These trials have been sized by simple modification of a standard formula for censored failure-time endpoints employed for randomized controlled trials [28]. Employing this method, a single arm study that employs a historical control estimate and is designed to detect a hazard ratio = 1.3 at one-sided significance of 5% with 50 patients accrued over 2 years and with 2 additional years of follow-up would have 53% power. Interestingly, similar power (46%) was obtained by the paired failure-time design assuming moderate correlation of 0.5 and exploiting patient-specific historical data. Some clinicians find it difficult to interpret the relative merit of time to progression estimates from single armtrials, for which there is no active control group. Historically-based designs may also be augmented with concurrent controls, by randomizing a fraction of patients to an accepted standard treatment [29]. Yet, more innovative single and multiarm phase II and III trials are being developed to evaluate these agents, such as those under consideration for the antiangiogenesis (MMPI) agents.For example, patients might be randomized to either a cytotoxic/cytostatic or cytotoxic/placebo combination regimen, after which they would be followed for disease progression and/or survival. A more novel design would allow patients to receive multiple courses of standard chemotherapy until best tumor response is achieved and then be randomized to cytostatic treatment or placebo to evaluate delay in disease relapse or progression. Recently, a randomized continuation trial design has been suggested by Ratain, that initially allows all patients to receive the new agent for a short run-in period of 2 to 4 months [30]. Patients who are compliant, tolerate the agent and have at least stable disease are then randomized to additional courses of treatment or observation. Since the randomized population is comprised of patients who are likely to derive clinical benefit, the magnitude of difference in clinical outcome between the arms is increased, thereby improving study efficiency [31]. This design may be most useful for agents expected to require chronic administration.The trial design proposed here takes an alternative approach in that each patient serves as his/her own historical control by use of a paired failure-time statistical framework. The design appears to be efficient under conditions of moderate to strong correlation between paired failure-times. Increased power would be expected by application of a nonparametric rank test [32-35]. Recently, Bonetti and colleagues applied the growth modulation index to the analysis of their completed phase II trial, originally defined by a standard design [36]. There are several obvious limitations to this design. Firstly, it requires that patients eligible for these investigational studies must have failed a previous cancer treatment, resulting in a patient-specific historical failure-time. This requirement could be imposed through study eligibility criteria, yet the procurement of accurate progression-free interval information from prior treatments may not be feasible, especially for externally-referred patients. Secondly, it is unclear whether equal consideration would be given to patients with longer and shorter first intervals for cytostatic trials. If patients with longer first intervals were systematically favored for studies of cytostatic agents, then such studies may be biased toward the null hypothesis. Thirdly, a useful rule for early termination should be considered, although such a rule may be difficult to implement. An interim analysis would probably be biased towards the null because the interim cohort would most likely be comprised of early failures that exhibit shorter second stly, correlation between successive failure times may be highly variable among study populations within any cancer site. Moreover, misspecification of the expectedcorrelation would affect the realized power, in the event that the observed correlation differs from the expected correlation employed in the sample size calculations.Novel phase II trials with failure-time endpoints are likely to become the basis for evaluations for noncytotoxic agents. These evaluations may be augmented by relevant and reliable biomarkers, as these become identified. Phase II trial designs that are feasible, efficient and offer valid methods for clinical and statistical evaluation are needed.ACKNOWLEDGEMENTSThe authors would like express appreciation to: Daniel Von Hoff, M.D. for helpful discussions concerning the growth modulation index and development of cytostatic/biologic agents, J. Jack Lee, Ph.D. and Yasuo Ohashi, Ph.D. for helpful discussions on trial design issues and Sin-Ho Jung, Ph.D. for critical input on rank tests for paired failure times. We also wish to thank an Associate Editor and a reviewer for suggestions which markedly improved an earlier draft of the manuscript.The authors are also grateful to the following cooperative group investigators and statisticians for sharing their patient-level data, which allowed us to explore magnitude of correlation between paired failure times.Pediatric Oncology Group:Sharon Murphy, M.D., Group ChairPOG 8104N. McWilliams, M.D., Study ChairJ. Shuster, Ph.D., Study StatisticianSouthwest Oncology Group:Charles Coltman, M.D., Group ChairSWOG 8312C. Russell, M.D., Study ChairS. Green, Ph.D., Study StatisticianCancer and Leukemia Group B:Richard Schilsky, M.D., Group ChairCALGB 8751G. Canellos, M.D., Study ChairD. Niedzwiecki, Ph.D., Study StatisticianG. Petroni, Ph.D., Study Statistician。