Raymond Kozody MD FRCP(C),
加拿大可用益生菌补充剂的临床指南:2016版说明书

Clinical Guide to PROBIOTIC SUPPLEMENTS AVAILABLE IN CANADA: 2016 Edition Indications, Dosage Forms, and Clinical Evidence to DateAuthor: Dragana Skokovic-Sunjic BScPhm RPh NCMPReviewers: Dr Vivien Brown MDCM CCFP FCFP NCMP, Dr Bradley C. Johnston PhD, Iris Krawchenko BScPhm RPh ACPR, Dr John Marshall MD MSc FRCPC AGAF,Dr Eamonn Quigley MD FRCP FACP MACG FRCPI, Dr Tom Smiley BScPhm PharmD Medical Editor: Ivana Sunjic MScDownload PROBIOTIC GUIDE mobile app for freeNEW INDICATIONFOR 20161AAD Antibiotic associated diarrhea - Prevention IBD-UC IBD - Ulcerative colitis – Adjunct to standard therapyBG Reduces blood glucose in Type II Diabetes(FBG and HA1c)IBS Irritable bowel syndromeC Constipation ID Infectious diarrheaCDAD Clostridium difficile associated diarrhea - Prevention LDL-C Reduces LDL and total cholesterolCE/AD Childhood eczema/Atopic dermatitis NEC*Necrotizing Enterocolitis (newborn)*as per hospital protocol, not for self-administrationCID Common infectious disease NI Nosocomial infections prevention FAP Functional abdominal pain OH Oral healthHP Helicobacter pylori - Adjunct to standard eradication therapy Regurg/GI MotReduces regurgitation/Improves gastrointestinal motilityIBD-P Inflammatory bowel disease - Pouchitis TD Traveler’s diarrheaCFU = Colony forming units (number of viable bacteria), M = million, B = billion, L. = Lactobacillus, B. = BifidobacteriumN E W1.2.3. • • •* as per hospital protocol, not for self-administrationT - Product requires refrigeration* as per hospital protocol, not for self-administrationT - Product requires refrigeration1.2.3.4.5.6.7.8.9.10.11.12.13.14.15.16.17. 18.19.20.21.22.23.24.25.26.27.28.29.30.31.32.33.34.35.36.37.38.39.40.41.42.43.44.45.46.47.48.49.50.51.52.53.54.55.56.57.58. 59.60.61.62.63.64.65.66.67.68.69.70.71.72.73.74.75.76.77.78.79.80.81.82.83.84.85.86.87.88.89.90.91.92.93.94.95.96.97.98.99. 100. 101. 102. 103.104. 105.106. 107.108. 109.110. 111. 112. 113. 114. 115. 116. 117. 118. 119. 120. 121.122. 123. 124. 125. 126. 127. 128. 129. 130. 131. 132. 133. 134. 135. 136. 137. 138. 139. 140. 141. 142. 143. 144. 145. 146. 147. 148. 149. 150. 151. 152. 153. 154. 155. 156.ALLIANCE MEMBERS。
火龙罐疗法联合常规治疗在AECOPD_患者中的应用效果
- 143 -*基金项目:广东省中医药局立项项目(202105211511578370)①梅州市中医医院 广东 梅州 510000火龙罐疗法联合常规治疗在AECOPD患者中的应用效果*韩文聪① 陈晓英① 郑小芬① 邹爱萍①【摘要】 目的:探讨火龙罐疗法联合常规治疗在慢性阻塞性肺疾病急性加重期(AECOPD)患者中的应用效果。
方法:选取2022年1—10月在梅州市中医医院住院的100例AECOPD 患者作为研究对象,根据临床实际情况以及患者意愿,且按是否接受火龙罐治疗分为治疗组与对照组,各50例。
对照组给予常规治疗,治疗组给予火龙罐疗法联合常规治疗。
比较两组治疗前后症状积分、血气指标[动脉血氧分压(PaO 2)、动脉血二氧化碳分压(PaCO 2)],治疗前及随访3个月、6个月生活质量(ADL)与6分钟步行试验(6MWT)变化,不良反应发生情况。
结果:治疗后,两组症状积分、PaCO 2较治疗前降低,且治疗组低于对照组,两组PaO 2较治疗前提高,且治疗组高于对照组,差异有统计学意义(P <0.05)。
随访3个月、6个月,两组ADL 评分、6MWT 距离较治疗前提高,随访6个月两组各指标较随访3个月提高,且治疗组高于对照组,差异有统计学意义(P <0.05)。
两组治疗期间不良反应发生率比较,差异无统计学意义(P >0.05)。
结论:火龙罐疗法联合常规治疗AECOPD 效果满意,可缓解患者的临床症状,改善血气指标,提高生活质量及步行能力,同时不增加不良反应发生率。
【关键词】 慢性阻塞性肺疾病急性加重期 火龙罐疗法 康复 血气指标 doi:10.14033/ki.cfmr.2024.06.036 文献标识码 B 文章编号 1674-6805(2024)06-0143-04 Application Effect of Fire Dragon Cup Therapy Combined with Conventional Treatment in Patients with AECOPD/HAN Wencong, CHEN Xiaoying, ZHENG Xiaofen, ZOU Aiping. //Chinese and Foreign Medical Research, 2024, 22(6): 143-146 [Abstract] Objective: To investigate the application effect of Fire Dragon Cup therapy combined with conventional treatment in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD). Method: A total of 100 patients with AECOPD who hospitalized in Meizhou Traditional Chinese Medicine Hospital from January to October 2022 were selected as the research objects, according to the actual clinical situation and patients' wishes, they were divided into the treatment group and the control group according to whether they received Fire Dragon Cup treatment, with 50 cases in each group. The control group was given conventional treatment, and the treatment group was given Fire Dragon Cup therapy combined with conventional treatment. The symptom scores, blood gas indexes [arterial partial pressure of oxygen (PaO 2), arterial partial pressure of carbon dioxide (PaCO 2)] before and after treatment, quality of life (ADL) and 6-minute walking test (6 MWT) before treatment, 3 months and 6 months after follow-up, and incidence of adverse reactions were compared between two groups. Result: After treatment, the symptom scores and PaCO 2 of two groups were lower than those before 弹力纤维降解的影响及机制[J].中华实用诊断与治疗杂志,2020,34(1):9-12.[19] SAN NORBERTO E M,REVILLA Á,Fernandez-Urbon A,et al.Vascular calcification progression in patients with end-stage chronic kidney disease[J]. Int Angiol,2021,40(6):528-536.[20] LI H,YANG M. Ligustrazine activate the PPAR-γ pathwayand play a protective role in vascular calcification[J]. Vascular,2022,30(6):1224-1231.[21] WING T T,ERIKSON D W,BURGHARDT R C,et al. OPNbinds alpha V integrin to promote endothelial progenitor cell incorporation into vasculature[J]. Reproduction,2020,159(4):465-478.[22] OGATA H,FUKAGAWA M,HIRAKATA H,et al. Effect oftreating hyperphosphatemia with lanthanum carbonate vs calcium carbonate on cardiovascular events in patients with chronic kidney disease undergoing hemodialysis: the LANDMARK randomized clinical trial[J]. JAMA,2021,325(19):1946-1954.[23] SHIRAKAWA K,SANO M. Osteopontin in cardiovasculardiseases[J]. Biomolecules,2021,11(7):1047.[24] DE VRIESE A S,CALUW É R,PYFFEROEN L,et al.Multicenter randomized controlled trial of Vitamin K antagonist replacement by Rivaroxaban with or without Vitamin K 2 in hemodialysis patients with atrial fibrillation: the Valkyrie Study[J]. J Am Soc Nephrol,2020,31(1):186.(收稿日期:2023-08-22) 慢性阻塞性肺疾病(COPD)属于常见的一种慢性气道疾病,COPD分为稳定期与急性加重期[1]。
AVVIO RAPIDO Router mobili 5G 安装指南说明书
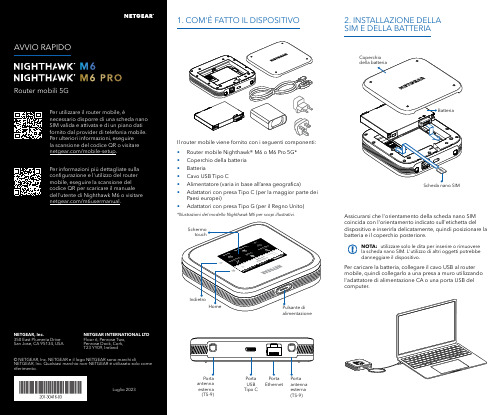
Per caricare la batteria, collegare il cavo USB al router mobile, quindi collegarlo a una presa a muro utilizzando l'adattatore di alimentazione CA o una porta USB del computer.Assicurarsi che l'orientamento della scheda nano SIM coincida con l'orientamento indicato sull'etichetta del dispositivo e inserirla delicatamente, quindi posizionare la batteria e il coperchio posteriore.NOTA: utilizzare solo le dita per inserire o rimuovere la scheda nano SIM. L'utilizzo di altri oggetti potrebbe danneggiare il dispositivo.1. COM'È FATTO IL DISPOSITIVO2. INSTALLAZIONE DELLA SIM E DELLA BATTERIAIl router mobile viene fornito con i seguenti componenti:• Router mobile Nighthawk® M6 o M6 Pro 5G*• Coperchio della batteria • Batteria• Cavo USB Tipo C• Alimentatore (varia in base all’area geografica)• Adattatori con presa Tipo C (per la maggior parte dei Paesi europei)•Adattatori con presa Tipo G (per il Regno Unito)*Illustrazioni del modello Nighthawk M6 per scopi illustrativi.antenna esterna (TS-9)antenna esterna (TS-9)USB Tipo CEthernetCONFORMITÀ NORMATIVA E NOTE LEGALIPer informazioni sulla conformità alle normative, compresala Dichiarazione di conformità UE, visitare il sito Web https:///it/about/regulatory/.Prima di collegare l'alimentazione, consultare il documento relativo alla conformità normativa.Può essere applicato solo ai dispositivi da 6 GHz: utilizzare il dispositivo solo in un ambiente al chiuso. L'utilizzo di dispositivi a 6 GHz è vietato su piattaforme petrolifere, automobili, treni, barche e aerei, tuttavia il suo utilizzo è consentito su aerei di grandi dimensioni quando volano sopra i 3000 metri di altezza. L'utilizzo di trasmettitori nella banda 5.925‑7.125 GHz è vietato per il controllo o le comunicazioni con sistemi aerei senza equipaggio.SUPPORTO E COMMUNITYDalla pagina del portale di amministrazione Web, fare clic sull'icona con i tre puntini nell'angolo in alto a destra per accedere ai file della guida e del supporto.Per ulteriori informazioni, visitare il sito netgear.it/support per accedere al manuale dell'utente completo e per scaricare gli aggiornamenti del firmware.È possibile trovare utili consigli anche nella Community NETGEAR, alla pagina /it.GESTIONE DELLE IMPOSTAZIONI TRAMITE L'APP NETGEAR MOBILEUtilizzare l'app NETGEAR Mobile per modificare il nome della rete Wi-Fi e la password. È possibile utilizzarla anche per riprodurre e condividere contenutimultimediali e accedere alle funzioni avanzate del router mobile.1. Accertarsi che il dispositivo mobile sia connesso a Internet.2. Eseguire la scansione del codice QR per scaricare l'appNETGEAR Mobile.Connessione con il nome e la password della rete Wi-Fi 1. Aprire il programma di gestione della rete Wi‑Fi deldispositivo.2. Individuare il nome della rete Wi‑Fi del router mobile(NTGR_XXXX) e stabilire una connessione.3. Only Connessione tramite EthernetPer prolungare la durata della batteria, l'opzione Ethernet è disattivata per impostazione predefinita. Per attivarla, toccare Power Manager (Risparmio energia) e passare a Performance Mode (Modalità performance).4. CONNESSIONE A INTERNETÈ possibile connettersi a Internet utilizzando il codice QR del router mobile da uno smartphone oppure selezionando manualmente il nome della rete Wi‑Fi del router e immettendo la password.Connessione tramite codice QR da uno smartphone 1. Toccare l'icona del codice QR sulla schermata inizialedello schermo LCD del router mobile.NOTA: quando è inattivo, lo schermo touch si oscura per risparmiare energia. Premere brevemente e rilasciare il pulsante di alimentazione per riattivare lo schermo.3. CONFIGURAZIONE DEL ROUTER MOBILETenere premuto il pulsante di accensione per due secondi, quindi seguire le istruzioni visualizzate sullo schermo per impostare un nome per la rete Wi‑Fi e una password univoci.La personalizzazione delle impostazioni Wi‑Fi consente di proteggere la rete Wi‑Fi del router mobile.Impostazioni APNIl router mobile legge i dati dalla scheda SIM e determina automaticamente le impostazioni APN (Access Point Name) corrette con i piani dati della maggior parte degli operatori. Tuttavia, se si utilizza un router mobile sbloccato con un operatore o un piano meno comune, potrebbe essere necessario immettere manualmente le impostazioni APN.Se viene visualizzata la schermata APN Setup Required (Configurazione APN richiesta), i dati APN dell’operatore non sono presenti nel nostro database ed è necessario inserirli manualmente. Immettere i valori fornitidall’operatore nei campi corrispondenti, quindi toccare Save (Salva) per completare la configurazione.NOTA: l’operatore determina le proprie informazioni APN e deve fornire le informazioni per il proprio piano dati. Si consiglia di contattare il proprio operatore per le impostazioni APN corrette e di utilizzare solo l’APN suggerito per il piano specifico.Schermata inizialeAl termine della configurazione, il router visualizza la schermata iniziale:Wi‑FiPotenza Carica Rete Codice QR connessione rapida Wi‑FiNome e Wi‑FiIcona del codice QR。
机械通气临床应用指南(中华重症医学分会2024)
机械通气临床应用指南中华医学会重症医学分会(2024年)引言重症医学是探讨危重病发生发展的规律,对危重病进行预防和治疗的临床学科。
器官功能支持是重症医学临床实践的重要内容之一。
机械通气从仅作为肺脏通气功能的支持治疗起先,经过多年来医学理论的发展及呼吸机技术的进步,已经成为涉及气体交换、呼吸做功、肺损伤、胸腔内器官压力及容积环境、循环功能等,可产生多方面影响的重要干预措施,并主要通过提高氧输送、肺脏爱护、改善内环境等途径成为治疗多器官功能不全综合征的重要治疗手段。
机械通气不仅可以依据是否建立人工气道分为“有创”或“无创”,因为呼吸机具有的不同呼吸模式而使通气有众多的选择,不同的疾病对机械通气提出了具有特异性的要求,医学理论的发展及循证医学数据的增加使对呼吸机的临床应用更加趋于有明确的针对性和规范性。
在这种条件下,不难看出,对危重病人的机械通气制定规范有明确的必要性。
同时,多年临床工作的积累和多中心临床探讨证据为机械通气指南的制定供应了越来越充分的条件。
中华医学会重症医学分会以循证医学的证据为基础,采纳国际通用的方法,经过广泛征求看法和建议,反复仔细探讨,达成关于机械通气临床应用方面的共识,以期对危重病人的机械通气的临床应用进行规范。
重症医学分会今后还将依据医学证据的发展及新的共识对机械通气临床应用指南进行更新。
指南中的举荐看法依据2024年ISF提出的Delphi分级标准(表1)。
指南涉及的文献依据探讨方法和结果分成5个层次,举荐看法的举荐级别依据Delphi分级分为A E级,其中A 级为最高。
表1 Delphi分级标准举荐级别A 至少有2项I级探讨结果支持B 仅有1项I级探讨结果支持C 仅有II级探讨结果支持D 至少有1项III级探讨结果支持E 仅有IV级或V探讨结果支持探讨课题分级I 大样本,随机探讨,结果清楚,假阳性或假阴性的错误很低II 小样本,随机探讨,结果不确定,假阳性和/或假阴性的错误较高III 非随机,同期比照探讨IV 非随机,历史比照和专家看法V 病例报道,非比照探讨和专家看法危重症患者人工气道的选择人工气道是为了保证气道通畅而在生理气道与其他气源之间建立的连接,分为上人工气道和下人工气道,是呼吸系统危重症患者常见的抢救措施之一。
CRRT的几个基本概念
Return Pressure Positive +50 to +150 mmHg
Effluent Pressure Negative or Positive >+50 to -150 mmHg
高通量旳滤器 面积 1.6-2.2平方米
HVHF
总之,对重症脓毒血症或合并休克患者, CRRT极难设定上限计量,尚需研究,超滤
率至少应≥35ml/kg/h。
Access Pressure Negative -50 to -150 mmHg
Filter Pressure Positive +100 to +250 mmHg
凝措施) 局部肝素抗凝法 局部枸橼酸盐抗凝法 低分子肝素抗凝法 无肝素抗凝法 前列腺素抗凝法
前列腺素抗凝法
原理:阻断血小板粘附功能和汇集功能 有人以为比肝素安全,半衰期极短(2min) 缺陷:停用后抗血小板活性时间长(24H) 无中和制剂 调整需依赖血小板汇集试验 药物剂量依赖性低血压发生率高 应用
技术构成三
滤器 聚砜膜(AV400及AV600)滤器 聚丙烯腈膜(AN69)滤器
AN 69
AV600
血液滤过器旳构造
血液入口
透析液和滤 出液出口
横断面
空心纤维 膜
透析液入 口
血液出口
空心纤维外面 (滤出液) 空心纤维里面 (血液)
血滤器
种类
聚砜膜
聚丙烯晴膜
聚酰胺
膜通透性
低通量滤器 <10000D
治疗中旳经典压力
治疗中旳经典压力
动脉压Access Pressure
测量当血液离开病人血液通路(例如双腔导管)时 旳压力(体外旳)
Festo 移动控制系统指南说明书

Handling Guide Online con el paquete decontrol de movimiento FestoLa guía de manipulación en línea (HGO) es un sistema todo en uno de configuración y solicitud de pedidos.Esta exclusiva herramienta de ingeniería en línea lo apoya configurando y solicitando su sistema estándar de manipulación. El HGO reduce su tiempo de ingeniería y diseño al dimensionar un sistema perfecto. Además de ahorrarle más tiempo al generar automáticamente modelos y documentación 3D CAD. Pruebe HGO ahora en: /handling-guideGuía de manipulación en líneaPaquete de control de movimiento FestoEl paquete de control de movimiento Festo (FMCP) es un sistema de control que brinda movimiento coordinado hasta para 6 ejes, proporcionando una solución robótica integrada con cinemática para sistemas de pórtico estándar H, T, 2D & 3D Festo. Las aplicaciones de movimiento cartesiano pueden ser configuradas e integradas rápidamente con bloques de función o AOIs para varias marcas de controladores. El FMCP consta de unidades servo con circuito de seguridad, fuente de alimentación, enlace al bus de campo de su elección y circuito deprotección; todo precableado, probado y certificado listo para trabajar al llegar a su instalación. El HGO con FMCP ofrece control, movimiento y manipulación como un paquete integrado.+H G O /F M C P .P S I .M X e s 2020/09。
原发性醛固酮增多症(中英文

• 原醛症病人一般服用安体舒通1周后,尿 钾减少、血钾上升、血浆CO2结合力下 降,肌无力、四肢麻木等症状改善,夜 尿减少,约半数病人血压有下降趋势。
原醛的筛查
• 立,卧位的血ARR=ALDO/PRA。各种文 献对比值报道不一,>25可疑, > 50可能 性大。
• 如果同时运用下述标准:ALDO/PRA>30, ALDO>20ng/dl, 其诊断原醛的灵敏性为 90%,特异性为91% 。
原醛的确诊
FST
氟氢可的松0.1mg q6h,共4天 ➢测定立位ALDO>60pg/dl,立位PRA <1.0ng/ml ➢尿钠的排泄>3 mmol/kg/天 ➢血K正常。 ➢服药4天后10Am的血浆皮质醇必须低于7Am 的
皮质醇
盐负荷试验
• 静脉和口服 • 静脉:生理盐水2L,4小时内静注完,测
定血ALDO >5ng/dl,PA确诊。 • 口服:高钠饮食3天(300mmol钠/d),
测定24小时尿ALDO >10µg/d, PA确诊
盐负荷试验
• 高钠试验正常人及高血压病人血钾无明 显变化,原醛症患者血钾可降至3.5毫 摩尔/升以下
Schimenbach, Best Pract Res Clin Endocrinol Metab. 2006 Sep;20(3):369-84
机制
肾上腺皮质病变Aldo↑储NA排K 血容量↑ PRA↓
自主性
低K
BP↑
临床特点
1.BP↑ : 血容量↑,平滑肌内NA↑,Aldo增加血 管对NAR的反应. 最早最常见,病程进展, BP逐渐↑,轻中度.以DBP ↑为主 伴头晕,头痛.
type I) • FH type II (APA or IHA)
有机人名反应VilsmeierHaack甲酰化反应

Vilsmeier-Haack reaction
Now
• The application of Vilsmeier-Haack reaction in the synthesis of the agrochemicals such as fenpyroximate,imazaquin,furametpyr was reviewed
Vilsmeier-Haack reaction
Vilsmeier-Haack reaction
References
1 Vilsmeier,A.and Haack,A.Ber.1937,60,119. 2 Campaigne,E.and Archer W. L. Organic Syntheses, Coll.1963,Vol.4,p.331.1953,Vol.33,p.27. 3 Youssefyeh,R.D.Tetrahedron Lett.1964,5,2161. 4 Minkin,V.I.;Dorofeenko,G.N.Russian Chem. Commun.1960,599.(综述) 5 Arnold,Z.;Zemlicka,mun.1959,24,2385. 6 Stéphanie Hesse and Gilbert Kirsch Tetrahedron Lett.2002,43,1213.
Vilsmeier-Haack reaction
• 维尔斯迈尔-哈克反应(Vilsmeier-Haack reaction)是指芳香化合物与二取代甲酰胺在三 氯氧磷作用下,反应生成芳环上甲酰化产物[1]。 该反应只reaction
Vilsmeier-Haack reaction
Vilsmeier-Haack reaction
Shut-off andor control element for a metallurgica

专利名称:Shut-off and/or control element for a metallurgical vessel发明人:BRUECKNER, RAIMUND,GIMPERA,JOSE,WALTENSPUEHL, ROLF申请号:EP90103288.8申请日:19900221公开号:EP0392168B1公开日:19921216专利内容由知识产权出版社提供摘要:A shut-off and/or control element for tapping liquid metal melt from a metallurgical vessel has an inner tube (2) secured on the vessel (5) and having at least one opening (14). A front edge (15) of a movable outer tube (3) encircles the inner tube (2). The outer tube (3) can be moved out of a closed position into an open position of the opening (14). In order to avoid the possibility of plugs of metal melt forming in openings (14) of the outer tube (3), the relative position of the opening (14) of the inner tube (2) and of the front edge (15) of the outer tube (3) is configured in such a way that, during the movement of the outer tube (3), the front edge (15) moves beyond the opening (14). Viewed in the direction (13) of the longitudinal axis, the front edge (15) is situated on one side of the opening (14) in the open position and on the opposite side of the opening (14) in the closed position.申请人:DIDIER-WERKE AG,DIDIER-WERKE AG地址:LESSINGSTRASSE 16-18; W-6200 WIESBADEN,LESSINGSTRASSE 16-18; W-6200 WIESBADEN代理机构:Brückner, Raimund, Dipl.-Ing.更多信息请下载全文后查看。
欧缔兰 突显完美抓握力及轻质性
欧缔兰突显完美抓握力及轻质性作者:暂无来源:《时代汽车》 2015年第7期本刊记者赵欢作为意大利高端奢华材料品牌,欧缔兰通过其独有的专利技术打造出100% 碳中和材料,成为了众多顶级汽车品牌的倾心之选。
对于追求自然运动感的汽车尤其是跑车而言,欧缔兰是极具功能性和美感的选择,其抓握性能和轻质性可提升汽车本身的“竞赛”气质。
凭借其在任何行驶环境中都能保持出色的摩擦性和透气性的两大优势,欧缔兰常被用于装饰汽车内饰,而应用最多的就是方向盘。
选择一辆汽车时需要考虑的标准有很多,而汽车的“运动感”起着决定性的作用。
保持汽车的“运动感”不仅需要现代又动力十足的设计、性能卓越的引擎、主被动安全系统,同时还需要考虑到驾驶人员在行驶时的舒适度和愉悦感,尤其是坐在符合人体工程学的优质座椅上,操控顶级品质的方向盘。
无论在赛道还是马路上,欧缔兰方向盘都能确保任意温度下的完美抓握触感,这常被定义为超跑式抓握感。
宝马5 系Sedan 的方向盘就选用了100% 意大利制造的欧缔兰奢华材料,开孔碳纤维和交叉缝纫中技艺精湛的缝线更加彰显这款车型运动感十足的时尚个性。
值得一提的是,欧缔兰方向盘也是兼具运动与优雅的车型的理想选择,这两大独特又具美感的元素被巧妙地融汇在保时捷Cayman GT4 和GT3 RS、宝马(包括MPerformance 系列)和奥迪RS 全系列中。
全球顶尖汽车制造商都不约而同地选择欧缔兰来满足客户需求,这源于他们对欧缔兰卓越品质的信任。
欧缔兰材料为驾驶员带来最优质的驾驶体验,为诸如福特Edge、尼桑JukeNismo、标志2008 和RCZ R Bimota特别版以及阿尔法罗密欧GiuliettaQuadrifoglio 等车型,及顶级超级跑车系列,如阿斯顿马丁V12、Vantage GT3 和Vulcan、法拉利FXX K、兰博基尼Gallardo LP 570-4 Squadra Corse、兰博基尼Aventador SV 和Aventador“Pirelli Edition” 特别版、路特斯Evora 400、迈凯伦675 LT、本田NSX、玛莎拉蒂GranTurismo MC 和配有强劲GT-R 的尼桑Nismo 打造更为丰富的驾驶空间。
费森尤斯CRRT基础知识

CRRT主要模式
原理:对流 清除物质:中大分子
小分子
Page 19
Pre-post CVVH 治疗目的
更大对流剂量清除体内中分子、大分子毒素;纠正电解质紊乱、 调节酸碱平衡以及排出多余的水分。减少前、后稀释的弊端、 增加对流剂量。 适用于:脓毒血症等产生大量炎性介质、细胞因子的病人有一 定的益处。 使用置换液 mFt设备可调置换液范围 600-4800 ml/h mFt设备可调超滤率范围0~1800ml/h
Hct = 37.5%
3
2
TPC = 8 g/dl
TPC = 10 g/dl
1
超滤 5 4 3 2 1
Page 14
超滤率/血泵速率
UFR/BPR=(脱水速率+后稀释置换速率)/ 血泵速率
在这里血泵的流速是100 毫升/分钟,超滤率/血泵流 速显示为红颜色37%
血泵流量已经增加到 300 毫升/分钟和 超滤率/血泵 流量比率是减少12%
Page 23
各种净化技术对炎症因子的清除范围
血脂 蛋白
化学毒素 胆红素 维生素 尿素氮 肌酐 糖水 电解质 水份
(LDL,HDL) 免疫球蛋白 蛋白复合物 白蛋白 内毒素 细胞因子 炎症介质
大分子 中分子
双重 吸
过滤 附
血
疗
法 浆
灌
置
血
换
滤
流
血
小分子 透
Page 24
CRRT常用治疗模式比较(SOP2010)
使用透析液 mFt设备可调透析液范围 600-4800 ml/h mFt设备可调超滤率范围0~1800ml/h
Page 12
CRRT主要模式
原理:对流 清除物质:中大分子
海洋酸化常见问题及解答

海洋酸化常见问题及解答前言海洋酸化是一个新的研究领域,该领域的大部分研究结果都是在近十年才发表出来的。
因此,在这个领域有部分结果是确定的,但是还有很多需要解决的问题。
海洋酸化也是个多学科交叉的领域,其研究内容包括化学、古生物学、生物学、生态学、生物地球化学、模式和社会科学等。
而且,海洋酸化的一些研究领域,例如碳酸盐系统化学,是错综复杂的。
正因为这些原因,媒体和公众发现该领域的一些科学问题或结果很令人费解。
美国海洋碳和生物地球化学(Ocean Carbon and Biogeochemistry, OCB,)项目在欧洲海洋酸化计划(European Project on Ocean Acidification,EPOCA,http://www.epoca-project.eu/)和英国海洋酸化研究计划(UK Ocean Acidification Research Program,/research/programmes/oceanacidification/)的支持和帮助下整理了一些海洋酸化领域经常问到的问题(FAQs)。
这些问题被广泛地发布到海洋酸化研究领域,要求在综合目前认识的基础上起草准确的答案,而且力争通俗易懂。
然后这些答案通过公开评阅和修正,确保在不失科学性的前提下保证可读性。
领域内的响应非常热情,有来自5个国家,19个研究所的27名科学家参与了这个过程。
我们真心希望这个常见问题列表是有用的。
这个列表本身也是一个正在进行的过程,我们邀请每个人都去寻找更准确的答案或发送评论,并把您的建议或评论发给Sarah Cooley(scooley@),我们会根据大家的反馈来定期修正这个问题列表。
Joan Kleypas and Richard Feely (OCB), Jean-Pierre Gattuso (EPOCA), and Carol Turley (UK Ocean Acidification Research Programme)“海洋酸化”的名称海洋不是酸性的,而且模式的结果也表明海洋不会变成酸性的。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Key words
ANAESTHETIC TECHNIQUES: subarachnoid block; ANAESTHETICS, LOCAL: tetracaine; SYMPATHETIC NERVOUS SYSTEM, CATECHOLAMINES: epinephrine; SPINAL CORD: blood flow.
135 ± 2 138 ± 9 146 ± 7
7± 1 6± 1 6± 1
164 ± 26 167 ± 28 150 ± 27
178 ± 3 195 ± 13 175 ± 12
143 ± 7 108 ± 9* 113 ± 6 *
7± 1 10 ± 2 9± 1
5± 1 13 ± 2 11 ± 2
233 ± 19 229 ± 25 211+28
167 ± 12 161 ± 8 167 ± 14
n = 6 in each group. Results are Mean ± S.E.M. *p < 0.05 when compared to pre-injection measurements.
in the femoral artery and vein. A left inguinal incision was used for the retrograde insertion of a catheter through the femoral artery into the left ventricle, using continuous pressure monitoring. The position of the left ventricular catheter was subsequently validated by post-mortem examination. A Swan-Ganz thermodilution catheter was inserted into the pulmonary arterial circulation using the left jugular vein. Following the surgical preparation each animal was allowed to stabilize for 40 minutes. Statham transducers were used for measuring mean arterial blood pressure (MABP) and pulmonary capillary wedge pressure (PCWP). The transducers were calibrated to zero at the mid-thoracic level. Heart rate (HR) and MABP were continuously recorded, while PCWP was determined prior to and between flow determinations. Data was recorded using a Hewlett-Packard monitor (Model 7758C) and a recorder (Model 7758A). Cardiac output was determined in duplicate prior to flow determinations. The cardiac output was measured by the thermodilution of 5 ml of room temperature physiological saline using an Edwards CO Computer (Model 9520A). A variation of five per cent or less between cardiac output measurements was accepted. Core temperature was continuously measured using the thermistor on the thermodilution catheter.
Spinal cord and spinal dural blood flow in the cervical, thoracic and lumbosacral regions were measured in dogs using the radioactive microsphere technique. Measurements were taken before and 20 and 40 minutes after lumbar subarachnoid injection of one of the following: (1) physiologic saline; (2) tetracaine 20 mg or (3) tetracaine 20 mg with epinephrine 200 ixg. No significant change in spinal cord or spinal dural blood flow occurred following subarachnoid physiologic saline or tetracaine with epinephrine. Dogs receiving subarachnoid tetracaine demonstrated a significant increase in lumbosacral spinal cord, and thoracic and lumbosacral dural blood flow at 20 and 40 minutes following injection. Cervical dural blood flow was significantly increased at 40 minutes after subarachnoid tetracaine. Lumbar subarachnoid tetracaine (20 mg) produces a regional spinal cord and generalized dural hyperemia which is prevented by the addition of epinephrine (200 (xg).
From the Department of Anaesthesia, University of Manitoba, Winnipeg, Manitoba. Address correspondence to: Dr. Raymond Kozody, Department of Anaesthesia, Health Sciences Centre, 700 William Avenue, Winnipeg, Manitoba, Canada R3E0Z3. Supported by the Health Sciences Centre Research Foundation and the University of Manitoba Faculty Fund. CAN ANAESTH SOC J 1985 / 32: 1 / pp 23-9
24
TABLE I injection
CANADIAN ANAESTHETISTS' SOCIETY JOURNAL Haemodynamic parameters in dogs prior to and following intrathecal
Groups Saline
MABP (mmHg)
PCWP (mmHg)
C.I. (ml-kg- •min~')
H.R. (beatstmin)
Pre-injection 20 min post-injection 40 min post-injection Tetracaine Pre-injection 20 min post-injection 40 min post-injection
23
Raymond Kozody MD FRCP(C), Richard J. Palahniuk MD FRCP(C),
Maureen O. Cumming RN BSC
Spinal cord blood flow following subarachnoid tetracaine
Prolongation of tetracaine spinal anaesthesia through the use of epinephrine as an adjunct has been well documented.1"4 The mechanism of epinephrine induced prolongation of tetracaine spinal anaesthesia is however controversial. Classical theory has lead to the concept that prolongation of spinal anaesthesia by the use of epinephrine is through vasoconstriction of the regional circulation. Studies using intrathecal lidocaine and bupivacaine with epinephrine have shown that the duration of clinically useful spinal anaesthesia is not prolonged by the addition of epinephrine.4"6 These studies suggest that regional vasoconstriction may not be an important factor. Other studies suggest that epinephrine may augment spinal analgesia by a direct spinal neuronal antinociceptive mechanism.7'8 We recently demonstrated that lumbar subarachnoid epinephrine (200 jxg) did not affect the spinal cord circulation but did produce regional dural vasoconstriction.9 In view of the present uncertainty this study was undertaken to determine the effects of subarachnoid tetracaine with and without epinephrine on the spinal cord and spinal dural circulations. Methods Eighteen mongrel dogs of either sex weighing 15-32 kg (19.8 ± 4.4, mean ± S.D.) were studied. The animals were anaesthetized with pentobarbitone, 30 mg-kg"1 induction dose followed by a maintenance dose of 2-5 ing-kg^-hr" 1 . After tracheal intubation, the animals were ventilated using an Ohio Model 300 ventilator with 100 per cent oxygen at a tidal volume of 15 ml-kg" 1 . The respiratory rate was adjusted to maintain a PaCO2 of 35-43 torr. The University of Manitoba guidelines for the humane use of animals were followed. The surgical preparation consisted of a right inguinal incision for insertion of poly vinyl catheters