临床化学分析方法:Alpha1-Antitrypsin
常用临床医学术语3

·serum monoamine oxidase (S-MAO)[血清单胺氧化酶]·serum cholinesterase (S-ChE)[血清胆碱酯酶]·serum ceruloplasmin[血清铜蓝蛋白]·serum α 1 -antitrypsin (S-α1A T)[血清α1抗胰蛋白酶]·serum protein[血清蛋白]·albumin[白蛋白]·globulin[球蛋白]·serum cholesterol esters[血清胆固醇酯]·blood ammonia[血氨]·serum bilirubin[血清胆红素]·serum bile acid[血清胆汁酸]7、其他[the others]·lunch test[试餐试验]·serum amylase[血清淀粉酶]·uric amylase[尿淀粉酶]·serum lipase[血清脂肪酶]·serum methemalbumin[血清高铁血白蛋白]·serum total cholesterol(CHOL)[血清总胆固醇]·serum triglyceride(TG)[血清甘油三酯]·serum high density lipoprotein(HDL)[血清高密度脂蛋白]·serum low density lipoprotein (LDL)[血清低密度脂蛋白]·serum free fatty acids(FFA)[血清游离脂肪酸]·serum creatin phosphokinase (S-CPK)[血清肌酸磷酸激酶]·serum CPK isoenzymes[血清肌酸磷酸激酶同功酶]·serum glutamate oxaloacetate transaminase(S-GOT)[血清谷草转氨酶]·serum lactate dehydrogenase(S-LDH)[血清乳酸脱氢酶]·serum LDH isoenzymes[血清乳酸脱氢酶同功酶]·serum potassium [血清钾]·血清钠[serum sodium]·serum chloride[血清氯]·serum calcium[血清钙]·inorganic phosphorum[无机磷]·serum magnesium[血清镁]·examination of malarial parasite from blood (bone marrow)smear[血(骨髓)涂片找原虫]·filaria examination from blood[血中找丝虫]·vitamin A assay[维生素A测定]·vitamin B1 assay[维生素B1测定]·vitamin B2assay[维生素B2测定]·Nicotinic acid assay[烟酸测定]·vitamin B6 assay[维生素B6]·vitamin B12 assay[维生素B12]·vitamin C assay[维生素C测定]·vitamin E assay[维生素E测定]·blood grouping [血型鉴定]·cross matching[交叉配合]·transfusion[输血]·A blood group[A血型]·B blood group[B血型]·AB blood group[AB血型]·O blood group[O血型]·Rh blood group[Rh 血型]8、内分泌试验[endocrine test]·luteinizing hormone(LH)[黄体生成素]·thyroid-stimulating hormone(TSH)[促甲状腺激素]·growth hormone(GH)[生长激素]·prolactin[催乳素]·adrenocorticotropic hormone(ACTH)[促肾上腺皮质激素]·follicular stimulating hormone(FSH)[卵泡剌激素]·serum protein-bound iodine assay(PBI)[血清蛋白结合碘测定] ·total 3,5,3`,5`-tetraiodothyronine(TT4)[总甲状腺素]·total 3,5,3`-triiodothyronine(TT3)[总三碘甲状腺原氨酸]·determina-tion of free T4and free T3[游离甲状腺素和游离三碘甲状腺原氨酸测定]·thyroxine-binding globulin as-say[甲状腺素结合球蛋白测定]·thyroidal uptake rate of 131I[甲状腺摄131碘率]·T3 suppression test[三碘甲状腺原氨酸抑制试验]·thyroid scintiscan[甲状腺闪烁扫描]·basal metabolic rate(BMR)[基础代谢率]·parathyroid hormone assay[甲状旁腺激素测定]·determination of calcitonin[降钙素测定]·urine 17-ketosteroids assay(17-KS)[尿17-酮类固醇测定]·urine 17-hydroxycorticosteroids assay(17-OHCS)[尿17-羟皮质类固醇测定]·urine free cortisol assay[尿游离皮质醇测定]·plasma cortisol assay[血浆皮质醇测定]·aldosterone assay[醛固酮测定]·corticosterone assay[皮质酮测定]·urine pregnanetriol assay[尿孕三醇测定]·ACTH stimulating test[促肾上腺皮质激素兴奋试验]·dexamethasone suppression test[地塞米松抑制试验]·urine catecholamine assay[尿儿茶酚胺测定]·urine vanillyl mandelic acid(VMA)[尿香草基杏仁酸]·testosterone assay[睾酮测定]·estradiol assay[雌二醇测定]·blood glucose assay[血糖测定]·glucose tolerance test(GTT)[葡萄糖耐量试验]·insulin releasing test[胰岛素释放试验]·serum C-peptide assay[血清C肽测定]·glucagon assay[胰升血糖素测定]·glycosylated hemoglobin assay[糖化血红蛋白测定]·plasma renin activity assay[血浆肾素活性测定]·5-hydroxytryptamine assay[5-羟色胺测定]·cyclic adenosine monophosphate (cAMP)[环磷酸腺苷测定]·cyclic guanosine monophosphate(cGMP)[环磷酸鸟苷测定]·prostaglandin assay(PG)[前列腺素测定]9、免疫学检查[immunological examination]·HbsAg[乙型肝炎表面抗原]·HbeAg[乙型肝炎e抗原]·anti-HBs[乙型肝炎表面抗体]·anti-HBc[乙型肝炎核心抗体]·anti-Hbe[乙型肝炎e抗体]·heterophil agglutination test[嗜异性凝集试验]·EB virus capsid antigen-lgA(VCA-lgA)[EB病毒壳抗原igA 抗体]·immunofluorescent anti-body test for epidemic hemorrhagic fever[流行性出血热免疫荧火抗体试验]·Weil-Felix reaction[外裴氏反应]·complement fixation test for Q fever[Q热补体结合试验]·cold agglutination test[冷凝集试验]·widal`s reaction[肥达氏反应]·Brucella agglutination test[布氏杆菌凝集试验]·antistreptolysin-O(ASO)[抗链球菌溶血素“O”]·serological test for syphilis[梅毒血清学试验]·Wassermann reaction[华氏反应]·[康氏试验Kahn test]·agglutination hemolysis test for leptospirosis[钩端螺旋体病血清凝集溶解试验]·intradermal test for schistosomiasis[血吸虫病皮内试验]·circumoval precipitin test for schistosomiasis[血吸虫病环卵沉淀试验]·cercarien hullen reaction for schistosomiasis[血吸虫病尾蚴膜反应]·indirect hemagglutination test for schistosomiasis[血吸虫病间接血凝试验]·enzyme-linked immunosorbent assay for schistosomiasis[血吸虫病酶联免疫吸附试验]·intradermal test for paragonimiasis[肺吸虫病皮内试验]·casoni`s intradermal test[包虫病皮内试验]·serum C-reactive protein(CRP)[血清C反应蛋白]·α-fetoprotein(AFP)[甲种胎儿蛋白]·carcinoembryonic antigen(CEA)[癌胚抗原]·E-rosette formation test[E花环形成试验]·lymphocyte transformation test(LTT)[淋巴细胞转化试验]·macrophage migration inhibition test(MMIT)[巨噬细胞移动抑制试验]·EAC-rosette formation test[EAC花环形成试验]·netroblue tetrazalium (NBT) reduction test[硝基蓝四氮唑还原试验]·determination of macrophage phagocytic function[巨噬细胞吞噬功能测定]·mixed lymphocytes culture test (LCT)[混合淋巴细胞培养试验]·serum immunoglobulin assay(Ig)[血清免球蛋白测定]·lg G[免疫球蛋白G]·lg A[免疫球蛋白A]·Ig M[免疫球蛋白M]·Ig D[免疫球蛋白D]·Ig E[免疫球蛋白E]·cryoglobulin test[冷球蛋白试验]·complement assay[补体测定]·circulating immune complex assay (CIC)[循环免疫复合物测定]·antinuclear antibodies assay(ANA)[抗核抗体测定]·anti-double-stranded DNA anti-body[抗双链DNA抗体测定] ·examination of lupus erythematosis cell(LE cell)[红斑狼疮细胞检查]·rheumatoid factors assay(RF)[类风湿因子测定]·antismooth muscle antibodies assay(SMA)[抗平滑肌抗体]·antimitochondrial antibodies(AMA)[抗线粒体抗体]·anti-parietal cell antibody(PCA)[抗胃壁细胞抗体]·anti-myocardial antibody[抗心肌抗体]·antithyroid antibodies[抗甲状腺抗体]10、血气分析[blood gas assay]·blood PH[血PH]·partial pressure of carbon dioxide (P CO2)[二氧化碳分压]·carbon dioxide combining power(CO2CP)[二氧化碳结合力]·standard bicarbonate(SB)[标准碳酸氢盐]·actual bicarbonate(AB)[实际碳酸氢盐]·buffer base(BB)[缓冲碱]·base excess(BE)[剩余碱]·total carbon dioxide(T CO2)[二氧化碳总量]·oxygen content(O2-C)[氧含量]·partial pressure of oxygen(P O2)[氧分压]·oxygen saturation(O2sat or SaO2)[血氧饱和度]11、大便检查[stool examination](1)exterior[外观]·formed[成形的]·dry[干的]·soft[软的]·loose[稀的]·watery[水样的]·liquid[液状]·sheep-dung[羊粪状]·yellow[黄的]·black[黑的]·acholic[无胆色的]·tarry[柏油样]·bloody[血性]·fatty[脂肪性]·rice water[米汤样]·mucous[粘液性]·mucopurulent[粘液脓性]·undigested[不消化的](2)镜检[microscopy]·RBC[红细胞]·WBC[白细胞]·pus cell[脓细胞]·phagocyte[吞噬细胞]·ova count[虫卵计数]·hatching test[卵化试验]·concentration of ovae[集卵试验]·ova of roundworm[蛔虫卵]·ova of hookworm[钩虫卵]·ova of pinworm[蛲虫卵]·ova of whipworm[鞭虫卵]·ova of schistosoma[血吸虫卵]·ova of clonorchis sinensis[华支睾吸虫卵]·ova of fasciolopsis[姜片虫卵]·ova of tapeworm[绦虫卵]·trichominad[滴虫]·trophozoites and cysts of entamoeba hestolytica[溶组织内阿米巴滋养体及包囊]·Endameba coli[结肠阿米巴]·trophozoites and cysts of Giardia lamblia[蓝氏贾第鞭毛虫滋养体及包囊]·Charcot-Leyden`s crystals[夏科—雷登氏结晶](3)化学检查[chemical examination]·occult blood test(OBT)[隐血试验]·coproporphyrins[粪卟啉]·fecal urobilin qualitative test[粪胆素定性试验]12、小便检查[urine examination](1)colour[颜色]·light yellow[淡黄]·milky[乳白]·bloody[血性]·red[红色]·thick tea in color[浓茶状](2)transparency[透明度]·clear[清晰]·cloudy[混浊](3)smell[气味]·ammoniacal smell[氨味]·apple smell[苹果味]·putrid smell[腐臭味](4)acid or alkaline[酸碱性]·acid[酸性]·alkaline[碱性]·PH urinary [尿PH](5)microscopy[镜检]·high power lens(HP)[高倍镜]·low power lens(LP)[低倍镜]·RBC[红细胞]·WBC[白细胞]·pus cell[脓细胞]·epithelial cell[上皮细胞]]·small round epithelial cell[小圆上皮细胞]·renal tubular epithelial cell[肾小管上皮细胞]·transitional epithelial cell[移行上皮细胞]·squamous epithelial cell[鳞状上皮细胞]·atypical cell[非典型细胞]·RBC:1-2 per high power field(=RBC 1-2/HP) [每高倍视野有1-2个红细胞]·cellular cast[细胞管型]·RBC cast[红细胞管型]·WBC cast[白细胞管型]·pus cast[脓细胞管型]·epithelial cast[上皮管型]·fatty cast[脂肪管型]·granular cast[颗粒管型]·hyaling cast[透明管型]·tube cast[肾小管型]·urate cast[尿酸盐管型]·waxy cast[蜡样管型]·calcium oxalate crystal[草酸钙结晶]·phospheate crystal[磷酸盐结晶]·urate crystal[尿酸盐结晶]·sulphanilamide crystal[磺胺结晶]·bilirubin crystal[胆红素结晶]·cholesterol crystal[胆固醇结晶]·mucous threads[粘丝]·spermatozoa[精子]·trichomonas parasite[滴虫](6)化学成分[chemical composition]·protein[蛋白质]·albumin[白蛋白]·Bence-Jone protein[本周氏蛋白]·sugar[糖]·ketobodies[酮体]·acetone[丙酮]·urobilinogen[尿胆原]·occult blood test(OBT)[隐血试验]·hemoglobin[血红蛋白]·myoglobin[肌红蛋白]·qualitative analysis of chyle[乳糜定性]·amylase[淀粉酶](7)尿电解质测定[lytes]·potassium assay[钾测定]·sodium assay[钠侧定]·chloride assay[氯测定]·calcium assay[钙测定]·magnesium assay[镁测定]·inorganic phosphorus assay[无机磷测定](8)尿其他检查[the others]·pregnance test[妊娠试验]·recovery of parasite from urine[尿中找寄生虫]·recovery of bacteria from urinary sediment[尿沉渣涂片找细菌]·recovery of mycobacterium from urinary smear[尿涂片找抗酸杆菌]·urinary three cups test[尿三杯试验]·antibody coated bacteria[抗体包裹细菌]·urinary lead assay[尿铅测定]·Congo red test[刚果红试验]·urinary protein electrophoresis[尿蛋白电泳]·urinary protein disc electrophoresis[尿蛋白圆盘电泳]·urinary fibrin (fibrinogen) degradation product(FDP)[尿纤维蛋白(原)降解产物]·urinary complement 3(C3)[尿补体3]·osmotic pressure assay[渗透压测定]·bacterial count of urine[尿菌落计数]13、脑脊液检查[CSF examination]·pressure[压力]·stookey test[压腹试验]·clear[清晰]·cloudy[混浊]·pellicle formation[薄膜形成]·bloody[血性]·yellow[黄色]·pink[粉红色]·purulent[脓性]·cell count[细胞计数]·Pandy`s test[潘氏试验]·protein electrophoresis[蛋白电泳]·immunoglobulin assay[免疫球蛋白测定]·glucose[葡萄糖]·chloride[氯化物]·LDH[乳酸脱氢酶]·bacteria[细菌] 14、浆膜腔液检查[fluid examination]·exfoliative cyte[脱落细胞]·appearance[外观]·specific gravity[比重]·cell count[细胞计数]·Rivalta test[李瓦他试验]·protein[蛋白质]·glucose[葡萄糖]·LDH[乳酸脱氢酶]·bacteria[细菌]15、消化液检查[GI fluid examination]·basal gastric quantity[基础胃液量]·basal acid output(BAO)[基础排酸量]·maximal acid output(MAO)[最大排酸量]·total acidity[总酸度]·free acid[游离酸]·cell[细胞]·bacteria[细菌]·occult blood test[隐血试验]·quantity[量]·colour[颜色]·transparancy[透明度]·cell[细胞]·crystal[结晶]·ova[虫卵]16、痰检查[sputum examination]·sputum quantity[痰量]·colour[颜色]·viscosity[粘稠度]·smell[气味]·WBC[白细胞]·RBC[红细胞]·cancer cell[肿瘤细胞]·lipophages[噬脂细胞]·Charcot-Leyden`s crystal[夏科-雷登氏结晶]·sputum smear[痰涂片]17、精液和前列腺液检查[examination of seminal and prostate fluid]·seminal fluid quantity[精液量]·sperm count[精子计数]·sperm morphology[精子形态]·sperm motility[精子活动度]·pH[酸碱度]·lecithin body[卵磷脂小体]·granular cell of prostate[前列腺颗粒细胞]·cancer cell[癌细胞]·bacteria[细菌]18、细菌培养[culture]·bacterial culture of blood[血培养]·bacterial culture of stool[粪培养]·urine culture[尿培养]·bacterial culture of CSF[脑脊液培养]·bacterial culture of sputum[痰液培养]·swabs culture of pharynx and tonsil[咽喉及扁桃体拭子培养] ·swabs culture of nose[鼻拭子培养]·swabs culture of ear[耳拭子培养]·swabs culture of eye[眼部拭子培养]·bacterial culture of gastric juice[胃液细菌培养]·bacterial culture of bile[胆汁细菌培养]·bacterial culture of pyogenic fluids[脓液培养]·anaerobic bacteria culture[厌氧菌培养]·spirochetes examination[螺旋体检查]·fungi examination[真菌检查]第十三章辅助检查[Diagnostic examination]1、X线检查[X-ray examination](1)肺[lung]·clear[清晰]·enlargement of hilar shadows[肺门阴影增大]·increase of lung markings[肺纹理增粗]·calcified[钙化灶]·cavitation[空洞]·circular lesion (coin lesion)[球形病灶]·a minimal area of density[小块阴影区]·scattered spot(plaque-like) shadows[散在的点(片)状阴影]·a poorly defined patchy density[边界不清的片状阴影]·a round density[圆形致密影]·pleural thickening[胸膜增厚]·hazziness(blunting, obliteration) of the costophrenic angle[肋隔角模糊(变钝、消失)]·elevation of diaphragm with limitation of movement[横膈抬高、活动受限]·encapsulated pleural effusion[包裹性胸腔积液]·hydropneumothorax[液气胸]·mediastinal displacement[纵膈移位]·hilar haze[肺门模糊]·increase of pulmonary hilar density[肺门密度增高]·pulmonary venous stasis(infarction)[肺淤血(梗塞)]·shadow[阴影性状]·hazziness[淡的]·clouding[云雾状]·diffuse[弥漫的]·veiling[面纱样]·streaky[线状]·patcky[絮状]·nodular[结节状]·massive[块状]·miliary[粟粒状]·confluent[融合状]·homogeneous[均匀的](2)心脏[heart]·left(right) atrial (ventricular) enlargement[左(右)房(室)增大]·a tortuous and prolonged aorta[主动脉屈曲延长]·“aortic type”(“mitral valve”)heart [主动脉型(二尖瓣型)心脏]·bulging pulmonary artery segment[肺动脉段突出]·a dilatation of the pulmonary artery[肺动脉扩张]·general enlargement of the heart shadow[心影普遍增大]·left(right) ventricular enlargement[左(右)心室增大]·left(right) atrial dilatation[左(右)心房增大]·boot-shaped heart[靴型心脏]·calcification of aorta[主动脉钙化]·waist of heart[心腰部]·vertical (slender; asthenic;horizontal;oblique)heart[垂位(狭长型;无力型;横位;斜位)心](3)腹部平片[KUB film]·calculus[结石]·calcified shadow[钙化影]·fluid levels with stepladder pattern[阶梯型液平]·gas-fluid level[液气平面]·subphrenic free air[膈下游离气体](4)胃肠道钡剂检查[barium enema examination]·gastroenterography[胃肠造影]·double contrast radiography[双重对比造影]·es·ophageal peristalsis sign[食管蠕动征]·duodenal flexure(impression)[十二指肠曲(压迹)]·mucosal fold shadow of small intestine[小肠粘膜皱襞影]·peristalsis and empting signs of colon[结肠蠕动与排空征]·delayed gastric emptying time[胃排空时间延长]·fasting retention of stomach[胃空腹潴留液]·filling defect[充盈缺损]·disappearance of the mucosal folds[粘膜皱襞消失]·hypotonicity (hypertonicity)[张力减低(增高)]·irritable cap[球部激惹现象]·vigorous peristaltic activity( hyperperistalsis)[蠕动增强]·bradydiastalsis[蠕动减弱]·hypernakinesia[蠕动消失]·accelerated(reduced) evacuation[排空加快(减缓)]·skipping phenomenon[跳跃现象]·broadened and tortuous mucosal fold[粘膜增宽和迂曲]·flat mucosal fold[粘膜皱襞平坦](5)胆道[bile tract]·oral cholecystography[口服胆囊造影]·intravenous cholecysto-cholangiography[静脉胆管胆囊造影]·trans-T-tube cholecystography[经T形管胆囊造影]·percutaneous transhepatic cholangiography(PTC)[经皮肝穿刺胆管造影]·dilated common duct[胆总管扩张]·gallblader concentrated satisfactorily[胆囊浓缩功能良好]·gallbladder with faint shadow, concentrated inadequately[胆囊显影不好,浓缩功能差]·contractibility[收缩功能](6)骨骼[skeleton]·cortical thickening of bone[骨皮质增厚]·“onion skin”appearance[洋葱皮样改变]·periosteal reaction[骨膜反应]·osteoporosis( rarefaction)[骨质疏松]·ossification [骨化]·deformity[畸形]·shortening[缩短]·displacement[移位]·luxation[脱位]·subluxation[半脱位]·malunion[连接不正]·greenstick fracture[青枝骨折]·multiple fracture[多发性骨折]·pathological fracture[病理性骨折]·joint space[关节间隙]·intervertebral space[椎间隙]·calcification shadow of costal cartilage[肋软骨钙化影]·osteomalacia(osteomalacosis)[骨质软化]·hyperostosis osteosclerosis[骨质增生硬化]·sequestrum[死骨]·bone necrosis[骨质坏死]·swelling (destruction; degeneration) of joint[关节肿胀(破坏;退行性变)]·ankytosis[关节强直]·epiphyseal seperation[骨骺分离]·good alignment[对线良好]·good apposition[对位良好](7)泌尿系统[urological system]·intravenous pyelography(IVP)[静脉肾盂造影]·retograde pyelography[逆行肾盂造影]·atrophy[萎缩]·deformity[移位]·distortion[扭曲]·filling defect[充盈缺损]·stricture[狭窄]·opaque(translucent) stone[不透光的(透光的)结石](8)X线检查位置[X-ray]·anteroposterior projection[前后位]·postero-anterior(PA) projection[后前位]·lateral projection[侧位]·upright positin[立位]·oblique projection[斜位]·right (left)anterior oblique(RAO/LAO) projection[右(左)前斜位]·anteroposterior oblique projection[前后斜位]·lordotic position projection[前凸位]·axial position[轴位]·cranial projection[头位]·caudal projection[尾位]2、心电图[ECG/EKG]·4:3 Atrioventricular block [4:3房室传导阻滞]·Aberrant conduction[差异性传导]·Abnormal T wave [T波异常]·Absolute refractory period[绝对不应期]·AC interference[交流电干扰]·Accelerated idioventricular rhythm[加速性室性自主心律]·Accelerated rhythm[加速性心律]·Advanced A-V block[重度房室传导阻滞]·Afterdepolarization[后除极]·Amplitude[幅度]·Anomalous atrioventricular conduction[异常房室传导]·Anterior myocardial infarction[前壁心肌梗死]·Antero-septal myocardial infarction[前间壁心肌梗死]·Antigrade conduction[顺向传导]·Anterolateral myocardial infarction[前侧壁心肌梗死]·Arrest[停搏]·Arrhythmia[心律失常]·artifact[伪差]·Asystole[停搏]·Atria echo[房性回波]·Atrial arrhyttmia[房性心律失常]·Atrial enlargement[心房扩大]·Atrial synchronous ventricular pacemaker[房室同步起搏器]·Atrioventricular block[房室传导阻滞]·Atrioventricular conduction ratio[房室传导比]·Atrioventricular dissociation [房室分离]·Atrioventricular junction[房室交界区]·Atrioventricular node [房室结]·Atropine test [阿托品试验]·Augmented lead[加压导联]·A V sequential pacemaker[房室顺序起搏器]·A VNRT/A-V node re-entry tachycardia[房室结折返性心动过速]·A VRT/A-V re-entry tachycardia[房室折返性心动过速]·Baseline[基线]·Bi-directional ventricular tachycardia[双向性室速]·Bifascicular block [双分支阻滞]·Bigeminy[二联律]·Bipolar Lead[双极导联]·Blocked PAC[房早未下传]·Bradycardia[心动过缓]·Brugada syndrome[布鲁加综合征]·Bundle branch block[束支传导阻滞]·Caliper[分规]·Capture[夺获]·Cardiac vector[心向量]·Coarse atrial fibrillation[粗房颤]·Compensatory pause [代偿间歇]·Concealed conduction[隐匿性传导]·Conduction system[传导系统]·Corrected QT interval[校正QT间期]·Coupling interval[配对间期]·DDD pacemaker [DDD起搏器]·Decremental conduction[递减性传导]·Deflection[偏离]·Delta wave [预激波]·Double Masters exercise test [二级梯运动试验]·Dual-chamber pacemaker[双腔起搏器]·Ectopic beat [异位搏动]·Electrical axis[电轴] ·Electrical vector[电向量]·Electromechanical dissociation [电机械分离]·End-diastolic PVC[舒张末期室早]·Enhanced antomaticity[自律性增高]·Escape rhythm[逸搏心律]·Exit block[传出阻滞]·Extensive anterior MI[广泛前壁心梗]·f wave [f波]·F wave [F波]·Fascicular block[束支传导阻滞]·Fibrillation[颤动]·Fine atrial fibrillation[细房颤]·First degree[一度]·Flutter[扑动]·Full compensatory pause[代偿间期完全]·Fusion beat[融合波]·High-degree atrioventricular block [高度房室传导阻滞] ·Holter[动态心电图]·Idionodal rhythm[结性自主心律]·Idioventricular[室性自主性]·Imcomplete compensatory pause [代偿间歇不完全] ·Inferior MI[下壁心肌梗死]·Interference and dissociation[干扰和脱节]·Interpolated PVC[间位性室早]·Inverted T wave [T波倒置]·Irregular[不规则/不齐]·J point [J点]·Junctional escape rhythm[交界性逸搏心律]·Lateral MI[侧壁心便]·LBBB[左束支传导阻滞]·Lead [导联]·Left anterior fasicular block[左前分支阻滞]·Left axis deviation [电轴左偏]·Long Q-T syndrome[长Q-T综合征]·Loose electrode [电极松动]·Low voltage[低电压]·Lown-Ganong-Levime syndrome [L-G-L综合征[·LVH/Left Ventricular Hypertrophy[左室肥厚]·Marked bradycardia[显著心动过缓]·MI/Myocardial infarction [心肌梗死]·Monophasic curve[单向曲线]·Multifocal PVC[多源性室早]·Multiform PVC [多形性室早]·Multistage stress test[多级运动试验]·Myocardial ischemia[心肌缺血]·Nonconducted PAC[房早末下传]·Non-Q wave MI[非Q波性心梗]·Nonsustained ventricular tachycardia [非持续性室速] ·Nontransmural MI[非透壁性心梗]·Normal sinus rhythm[正常窦性心律]·P mitrale[二尖瓣型P波]·P Pulmonale[肺型P波]·PAC/Premature atrial contractions[房性早搏] ·Pacemaker rhythm[起搏心律]·Paired PVC [成对室早]·Para-systole[并行心律]·Paroxysmal junctional(supraventricular)tachycardia [阵发性交界(室上)性心动过速]·Peri-infarction block[梗死周围阻滞]·Posterior MI[后壁心梗]·P-P interval [P-P间期]·P-R interval [PR间期]·P-R segment [PR段]·Precordial Leads [胸前导联]·Preexcitation syndrome[预激综合征]·Ptf value[心房终未电势]·Pulseless electrical activity[无脉性电活动]·PVC/Premature Ventricular Contractions[室性早搏]·Q(q) wave [Q(q)波]·QRS Complex [ORS波]·QT interval [QT间期]·Quadrigeminy[四联律]·RBBB [右束支传导阻滞]·Reciprocal rhythm[反复心律]·Right axis deviation [电轴右偏]·R-On-T phenomenon [R-on-T现象]·R-R interval [R-R间期]·RVH/Right Ventricular hypertrophy[右室肥厚]·Second degree[二度]·Secondary changes[继发性改变]·Septal MI[间隔心梗]·Sick sinus syndrome(SSS)[病态窦房结综合征]·Sinoatrial block [窦房阻滞]·Sinus arrest [窦性静止]·Sinus arrhythmia[窦性心律不齐]·Sinus bradycardia[窦性心动过缓]·Sinus p wave [窦性P波]·Sinus tachycardia[窦性心动过速]·Speed of ECG paper[心电图纸走速]·ST segment depression [ST段压低]·Standard Limb Leads[标准肢体导联]·Standstill[静止]·Strain[劳损]·Subepicardial ischemia [心外膜下缺血]·Supraventricular[室上性]·T wave [T波]·Ta wave[心房复极波]·Tachycardia[心动过速]·TDP/Torsade de pointes [尖端扭转型室速]·Third degree[三度]·TP segment [TP段]·Treadmill test[运动平板试验]·Trifascicular block [三分支阻滞]·Trigeminy[三联律]·U wave [U波]·Unifocal PVC [单源室早]·V A T/Ventricular activation time [心室激动时间]·Ventricular enlargement[心室扩大]·Ventricular fibrillation [室性颤动]·Ventricular flutter [室性扑动]·VT/Ventricular tachycardia [室性心动过速]·Vulnerable period[易损期]·Wandering atrial pacemaker[心房起搏点游走]·Wedensky effect[魏登斯基效应]·Wedensky facilitation[魏登斯基易化]·Wenckedach block[文氏阻滞]·Wenckebach phenomenon[文氏现象]·Wide QRS complex[宽QRS波]·Wolff-Parkinson-White(W-P-W)syndrome[W-P-W综合征] 3、超声波[ultrasonograph]·rare tiny reflection[稀疏微波]·many tiny reflection[较密微波]·dense tiny reflection[密集微波]·high reflection[高波]·tall reflection in bunches[高束波]·distracting reflection in bunches[分散束波]·fluffy reflection of high amplitude[绒毛样高波]·bundles of irregular high reflection[杂乱高波]·liquid flat segment[液平段]·linear scan[线阵扫查]·sector scan[扇形扫查]·rcflection[反射]·refraction[折射]·multiple reflection[多重反射]·artifact[伪象]·internal echo[内部回声]·central echo[中央回声]·strong echo;hyperecho[强回声]·high level echo[高回声]·equal echo(isoecho)[等回声]·low level echo( hypoecho,mildly echo)[低回声]·echo free area( anechoic area,echoless area)[无回声区]·echolucent area( sonolucent region)[透声区]·dark area(silent gone)[暗区]·solid area[实质区]·liquify area[液化区]·spotty echo[斑点回声]·echogonic dotts[点状回声]·acoustic window(AW)[声窗]·homogenous[均匀性]·inhomogenous[不均匀性]·vegetation(Veg)[赘生物]·hump sign[驼峰征]·strong echo(SE)[强光团]·double light hand[双光带]·macaroni sign[通心面征(即双光带)]·acoustic shadow(AS)[声影]·double edge shadow[双边影]·fluid-fluid level with floating material sign[液-液分层征]·falls sign[瀑布征]·dough sign[面团征]第十四章诊断(疾病名称)[Diagnosis(disignation of diseases)] ·病因诊断[pathogenic diagnosis (diagnosis of etiology)]·病理解剖诊断[diagnosis of pathological anatomy]·病理生理诊断[diagnosis of pathological physiology]·并发症[complication]·合并症(伴发疾病)[accompanying diseases](1)心内科疾病[heart diseases]·cardiac insufficiency (heart failure)[心功能不全(心衰)]·cardiogenic (hypovolemic, septic, anaphylactic, neurogenic) shock[心原性(低血容量性,感染性,过敏性,神经原性)休克]·sinus tachycardia (bradycardia, arrhythmia, arrest)[窦性(心动过速,心动过缓,心律不齐,停搏)]·sinus rhythm[窦性心律]·sick sinus syndrome(SSS)[病窦综合征]·Adams –stokes syndrome[阿-斯综合征]·junctional (ventricular) escape beat[交界性(室性)逸搏]·escape rhythm[逸搏心律]·left atrial rhythm[左房心律]·chaotic atrial rhythm[房性紊乱心律]·wandering rhythm[游走心律]·premature atrial(ventricular, junctional) beats[房性(室性,交界性)早搏]·multifocal (multimorphic)[多源性(多形性)]·bigeminy (trigeminy)[二(三)联律]·paroxysmal atrial (supraventricular, ventricular) tachycardia[阵发性房性(室上性,室性)心动过速]·sustained ventricular tachycardia[持续性室速]·sinus nodal reentrant tachycardia[窦房结折返性心动过速]·Torsade de pointes (TDP)[尖端扭转型室速]·A-V(A-V nodal)reentrant tachycardia[房室(房室结)折返性心动过速]·atrial flutter (fibrillation)[房扑(颤)]·ventricular flutter (fibrillation)[室扑(颤)]·sino-auricular (intra-auricular, intra-ventricular)block[窦房(房内,室内)传导阻滞]·first (second, third) degree atrioventricular (A-V)block[I(II、III)度房室传导阻滞]·second degree, type I(II) A-V block[II度I(II)型房室传导阻滞]·Wenckebach phenomena[文氏现象]·Mobitz type I(II)[莫氏I(II)型]·complete (incomplete) left (right) bundle branch block[完全性(不完全性)左(右)束支传导阻滞]·advanced (high grade) A-V block[高度房室传导阻滞]·left anterior (posterior) fascicular block[左前(后)分支阻滞] ·type A(B) wolff-parkinson-white syndrome (pre-excitation syndrome)[A(B)型预激(W-P-W)综合征]·Lown-Ganong-Levime (L-G-L) syndrome[L-G-L综合征(短P-R综合征)]·accelerated idioventricular (idiojunctional) rhythm[加速性室性(交界性)自主心律]·ectopic (junctional, reciprocal) rhythm[异位(交界性,反复)心律]·ventricular hypertrophy[心室肥厚]·left(right) atrial enlargement[左(右)房扩大]·idiopathic[特发性]·interfering atrioventricular dissociation[干扰性房室分离]·Brugada syndrome [Brugada 综合征]·cardiac arrest (sudden death)[心脏骤停(猝死)]·acute rheumatic fever [急性风湿热]·rheumatic carditis[风湿性心脏炎]·chorea[舞蹈病]·rheumatic heart disease[风湿性心脏病]·multivalve disease[多瓣膜病]·valvular heart disease[心瓣膜病]·mitral(aortic, pulmonary, tricuspid) stenosis[二尖瓣(主动脉瓣,肺动肪瓣,三尖瓣)狭窄]·mitral (aortic, tricuspid) regurgitation(insufficiency)[二尖瓣(主动脉瓣,三尖瓣)反流(关闭不全)]·coronary artery (heart) disease[冠心病]·acute coronary syndrome [急性冠脉综合征]·acute (old) myocardial infarction (MI)[急性(陈旧性)心肌梗死]·Q wave (non-Q wave) MI[Q波(非Q波)心梗]·unstable (stable) angina pectoris[不稳定(稳定)型心绞痛]·cardiogenic sudden death[心源性猝死]·initial onset angina peotoris[初发型心绞痛]·angina decubitus[卧位型心绞痛]·variant angina pectoris[变异型心绞痛]·intermediate syndrome [中间综合症]·post-infarction angina pectoris[梗死后心绞痛]·congenital heart disease[先天性心脏病]·pulmonary (aortic) stenosis[肺(主)动脉狭窄]·coartation of aorta[主动脉缩窄]·idiopathic (primary) pulmonary hypertension [原发性肺动脉高压]·persistent left superior vena cava[左侧上腔静脉永存]·superior vena caval obstruction syndrome[上腔静脉阻塞综合征]·dextro cardia[右位心]·marfan`s syndrome [马凡氏综合征]·atrial (ventricular) septal defect(ASD/VSD)[房(室)间隔缺损]·patent ductus arteriosus (PDA)[动脉导管未闭]·single atrium (ventricle)[单心房(室)]·endocardial cushion defect[心内膜垫缺损]·aortic sinus aneurysm[主动脉窦瘤]·coronary arteritis[冠状动脉炎]·coronary artery fistula[冠状动脉瘘]·malformation of coronary artery[冠状动脉畸形]·coronary arteriovenous fistula[冠状动静脉瘘]·tetralogy(trilogy) of Fallot[法乐氏四(三)联征]·complete (corrected) transposition of great vessels[完全性(纠正型)大血管转位]·double-outlet of right ventricle [右室双出口]·partial (complete) anomalous pulmonary venous drainage[部分(完全)性肺静脉畸形引流]·Eisenmenger (Ebstein) syndrome[艾生曼格综合征(埃勃斯坦畸形)]·persistent trumcus arteriosus[永存主动脉干]·congenital pulmonary arteriovenous fistula[先天性肺动静脉瘘]·primary (secondary) hypertension [原发(继发)性高血压]·hypertensive crisis (urgencies, emergencies)[高血压危象(急诊)]·hypertensive nephropathy (papillo-retinopathy, cerebral hemorrhage)[高血压性肾病(视乳头-视网膜病,脑出血)] ·acute (subacute) becterial endocarditis[急(亚急)性细菌性心内膜炎]·infective endocarditis[感染性心内膜炎]·acute (chronic) cor pulmonale[急(慢)性肺原性心脏病]·chronic pulmonary heart disease[慢性肺心病]·acute (chronic) pericarditis [急(慢)性心包炎]·constrictive pericarditis[缩窄性心包炎]·purulent (tuberculous) pericarditis[化脓(结核)性心包炎]·syphilitic heart disease[梅毒性心脏病]·acute viral myocarditis [急性病毒性心肌炎]·primary (specific) cardiomyopathy[原发(特异)性心肌病]·dilated (hypertrophic, restrictive) cardiomyopathy[扩张(肥厚,限制)型心肌病]·hypertrophic obstructive cardiomyopathy (HOCM)[肥厚型梗阻性心肌病]·arrhythmogenic right ventricula dysplasia(ARVD)[致心律失常性右室发育不全]·tachycardia induced cardiomyopathy[心动过速性心肌病]·hypertensive(alcoholic,ischemic,diabetic,peripartum,hyperthyr oid )cardio- myopathy[高血压(酒精,缺血,糖尿病,围生期,甲亢)性心肌病]·drug-induced cardiomyopathy[药物性心肌病]·keshan disease[克山病]·myxoma of left atrium[左房粘液瘤]·metastatic cardiac tumor[心脏转移性肿瘤]·cardiac neurosis[心脏神经官能症]·mitral prolapse syndrome[二尖瓣脱垂综合征]·long Q-T syndrome[长QT间期综合征]·aortic (dissecting) aneurysm[主动脉(夹层动脉)瘤]·multiple (primary) arteritis of aorta and main branches[多发性大动脉炎]·Takayasu arteritis [大动脉炎(高安动脉炎)]·Raynaud disease[雷诺氏病]·systemic vasculitis[系统性血管炎]·thromboangitis obliterans[血栓闭塞性脉管炎]·deep vein thrombosis[深静脉血栓形成]·superficial thrombophlebitis[血栓性浅静脉炎]·syndrome X[X 综合征]·peripheral arteriosclerosis obliteration[闭塞性周围动脉粥样硬化]·Churg-Strauss syndrome[变应性肉芽肿性血管炎]·radiofrequency catheter ablation(RFCA)[射频消融术]·percutaneous balloon mitral valvuloplasty (PBMV)[经皮二尖瓣球囊扩张术]·transluminal extraction catheter(TEC)[经皮腔内切吸导管]·percutaneous transluminal septal myocardial ablation(PTSMA)[经皮经腔间隔心肌消融术]·percutaneous transluminal coronary angioplasty (PTCA)[经皮腔内冠脉成形术]。
生化思考题
临床生化检验第六章掌握:➢酶活性的国际单位定义:酶活性单位1、惯用单位:常由发明者自行命名,结果无可比性;(20世纪50年代).2、国际单位: 在特定条件下,1分钟能转化1微摩尔底物(µmol/ min)的酶量为一个“国际单位”:(76年); 63年是25℃及最适条件下.3、Katal单位:在规定条件下,即每秒钟转化1个摩尔底物(mol /s)的酶量➢酶活性测定的连续监测法和定时法的概念定时法:将酶与底物在特定条件(缓冲液、温度等)下孵育,经过一定时间后,用终止液终止反应,通过化学或生物化学的方法测出底物或产物的总变化量,除以时间即可计算出底物消耗速度(-d[S]/min)或产物生成速度(d[P]/min),将速度换算为µmol/ min便是以国际单位表示的酶活性。
连续监测法:将酶与底物在特定条件(缓冲液、温度等)下孵育,每隔一定时间(2s∼60s)连续测定酶促反应过程中某一底物或产物的特征信号的变化,从而计算出每分钟的信号变化速率。
连续监测法是在多个时间点连续测定产物生成量或底物消耗量,选取线性期的速率来计算酶活性,又称速率法。
➢连续监测法的计算和分类;计算:分类:➢酶活性测定最适条件的概念和意义;最适条件(optimum condition):是指能满足酶发挥最大催化效率所需的条件1.合适的底物和最适底物浓度2.理想的缓冲液种类、最适离子强度和反应液的最适pH3.最适反应温度4.合适的辅因子、激活剂浓度5.酶偶联反应还需要确定指示酶和辅助酶的用量6.合理的测定时间,延滞期应尽量短暂并有足够的线性期7.合适的样品与反应试剂的比例及足够的检测范围8.尽量去除各种抑制剂➢ALT、AST、ALP、GGT、LD、CK、AMY、ChE的测定方法。
ALT:1.测定谷氨酸以酶电极法作代表,因需特殊仪器不适合临床检验2.测定丙酮酸①以赖氏法为代表的定时法②以IFCC推荐法为代表的连续监测法③偶联丙酮酸氧化酶法CK:1.比色法2.连续监测法3.荧光法4.化学发光法熟悉:血清酶变化的病理机制;酶动力学参数的含义;电泳法和免疫抑制法测定同工酶的原理。
1Bio-Rad质控品分类介绍_-susan解析
胆碱酯酶(Cholinesterase)(仅限2、3)
乙醇(Ethanol)(仅限1、2)
胰淀粉酶(Amylase,Pancreatic)(仅限2、3)
谷氨酸脱氢酶(GLDH)*(仅限1、3)
万古霉素(Vancomycin)(仅限1、3)
尿液定量生化控制品
▪ 可选择液体或干粉产品
▪ 人尿液基质
▪ 以376、377(Lyphochek定量尿液控制品) 为例,包括了葡萄糖(Glucose)、尿素 (Urea)、尿素氮(Urea Nitrogen)、 尿酸(Uric Acid)、肌酐(Creatinine)、 肌酸(Creatine)、微量白蛋白 (Microalbumin)、定性妊娠试验 (Pregnancy (Qualitative))、电介质、 各种微量元素、各种激素及其代谢产物 (如醛固酮(Aldosterone)、多巴胺 (Dopamine)、肾上腺素 (Epinephrine)、香草扁桃酸(VMA)、 高香草酸(HVA)等)等50多项常见的尿 液定量生化分析项目
甲状腺结合球蛋白(TBG)(仅限3)
补体C3(Complement C3)(仅限2、3)
前列腺特异性抗原(PSA)(仅限3)
补体C4(Complement C4)(仅限2、3)
人绒毛膜促性性激素-β亚基(hCG-Beta Subunit)(仅限3)
触珠蛋白(Haptoglobin)(仅限2、3)
摩尔渗透压浓度(Osmolality)(仅限1、2)
总卟啉(Porphyrins,Total)(仅限1)
血脂控制品
▪ 641/642 ▪ 液体产品 ▪ 人血清基质 ▪ 包括了载脂蛋白A-1(Apolipoprotein A-1)、载脂
芯片类检测:Luminex PLEXMAP BIOPLEX 液相芯片检测

sCD30 可溶性CD30
sCD40L可溶性CD40L
sEGFR可溶性表皮生长因子受体
sgp130 可溶性糖蛋白130
sIL-2Rα可溶性白细胞介素-2受体α
sIL-4R可溶性白细胞介素-4受体
sTNF RI 可溶性肿瘤坏死因子受体I
sTNF RII可溶性肿瘤坏死因子受体II
p70 S6 Kinase (Thr412) 磷酸化核糖体S6蛋白激酶β2抗体
STAT1 (Tyr701)磷酸化信号转导与转录激活因子1
STAT1 (Tyr707)磷酸化信号转导与转录激活因子1
STAT3 (Tyr705)磷酸化信号转导与转录激活因子3
STAT5A/B (Tyr694/699) 磷酸化信号转导与转录激活因子
ZAP-70 (pan Tyr)磷酸化zeta相关蛋白70
Syk (pan Tyr)磷酸化非受体型酪氨酸蛋白激酶
Active Caspase 3 活化半胱胺酸蛋白酶 3
Active Cleaved PARP活化切割的多腺苷二磷酸多聚酶
ATF2 (Thr69/71)活化复制因子2
BAD (Ser112)磷酸化相关死亡促进因子
IFNγ干扰素γ
IL-10白介素-10
IL-12 (p70) 白介素-12
IL-13白介素-13
IL-17白介素-17
IL-1ra白介素-1ra
IL-2白介素-2
IL-20 白介素-20
IL-28a 白介素-28a
IL-29 白介素-29
IL-4 白介素-4
IL-5 白介素-5
IL-8 白介素-8
IL-9 白介素-9
sIL-1RII可溶性白细胞介素-1受体II
LUMINE技术原理及应用

L u m i n e x的基本原理及应用传统的蛋白质分析主要采用双抗体夹心ELISA法。
此法长期以来被视为蛋白质定量分析的“标准方法”。
ELISA可以用来准确测定大批量生物样品,但每次实验只能分析一个目标分子,而不具备同时分析多种目标分子的能力。
在ELISA基础上发展出的 luminex技术,不仅同样通过双抗体选择而具有高特异性,同时也具有ELISA的高通量、操作简便、测量准确等优点,而且可以在一次实验中完成对多种目标分子的分析,从而改变了过去的分析模式,建立了更加高效快速的分析平台。
Luminex技术原理,在近年发表的文章中已有过详细的介绍和说明。
Luminex 技术应用微球和流式细胞仪的原理。
微球内部含有三种荧光免疫荧光,通过荧光不同的比例可以区分500种不同的微球。
每种微球可以用来检测一种不同的蛋白或基因。
因此,利用微球技术,可以同时检测高达500个蛋白或基因。
该技术供如何保证检测结果的特异性?检测的特异性取决于抗体高特异性。
试剂几乎全部来源于美国大公司,产品经过了严格的质量控制。
同时,我们检测公司也有近15年的经验、严格的操作程序和质量控制体系。
客户自己提供抗体,是否可以进行LUMINEX检测?Luminex和ELISA检测试剂都需要两个配套的特异性抗体。
我们公司具有开发Luminex试剂盒的经验。
但是,需要一系列的开发工作才能保证结果的特异性、重复性和可靠性。
除了蛋白,LUMINEX技术是否还可以用于其它指标的检测?可以用于基因表达,基因多态性和HLA配型分析。
检测周期多久?视待测蛋白的种类、数量和标本数量定。
一般来说,检测一组蛋白(1-50个,视蛋白种类定)和一组标本(多达360个标)需要3-4小时的操作时间及基本数据分析。
但是,检测周期也取决于公司当时的工作量。
一般来说,从标本收到起,检测应在1-2周完成;但是部分蛋白试剂盒需要收到订单后从美国进口,检测周期可能会延长到4-5周。
血浆蛋白质临床意义
血浆蛋白质临床意义(一)前白蛋白前白蛋白(prealbumin,PA),分子量5.4万,由肝细胞合成,在电泳分离时,常显示在白蛋白的前方,其半寿期很短,仅约12小时。
因此,测定其在血浆中的浓度对于了解蛋白质在营养不良和肝功能不全,比之白蛋白和转铁蛋白具有更高的敏感性。
PA除了作为组织修补的材料外,还可视作一种运载蛋白,可结合T4与T3,而对T3的亲和力更大。
PA与视黄醇结合蛋白形成复合物,具有运载维生素A的作用。
在急性炎症、恶性肿瘤、肝硬化或肾炎时其血浓度下降。
(二)白蛋白白蛋白(albumin,Alb)系由肝实质细胞合成,在血浆中的半寿期约为15-19天,是血浆中含量最多的蛋白质,占血浆总蛋白的40%-60%。
其合成率虽然受食物中蛋白质含量的影响,但主要受血浆中白蛋白水平调节,在肝细胞中没有储存,在所有细胞外液中都含有微量的白蛋白。
关于白蛋白在肾小球中的滤过情况,一般认为在正常情况下其量甚微,约为血浆中白蛋白的0.04%,按此计算每天从肾小球滤过液中排出的白蛋白即可达3.6g,为终尿中蛋白质排出量的30-40倍,可见滤过液中多数白蛋白是可被肾小管重新吸收的。
有实验证实白蛋白在近曲小管中吸收,在小管细胞中被溶酶体中的水解酶降解为小分子片段而进入血循环。
白蛋白可以在不同组织中被细胞内吞而摄取,其氨基酸可被用为组织修补。
白蛋白的分子结构已于1975年阐明,为含585个氨基酸残基的单链多肽,分子量为66458,分子中含17个二硫键,不含有糖的组分。
在体液pH7.4的环境中,白蛋白为负离子,每分子可以带有200个以上负电荷。
它是血浆中很主要的载体,许多水溶性差的物质可以通过与白蛋白的结合而被运输。
这些物质包括胆红素、长链脂肪酸(每分子可以结合4-6个分子)、胆汁酸盐、前列腺素、类固醇激素、金属离子(如Cu2+、Ni2+、Ca2+)药物(如阿司匹林、青霉素等)。
具有活性的激素或药物当与白蛋白结合时,可以不表现其活性,而视为其储存形式,由于这种结合的可逆性和处于动态平衡,因此在调节这些激素和药物的代谢上,具有重要意义。
α1-抗胰蛋白酶测定(α1-antitrypsin,α1-AT)

α1-抗胰蛋白酶测定(α1-antitrypsin,α1-AT)
α1-抗胰蛋白酶为一种糖蛋白,由肝细胞制造,分子量5.6kD,体内半衰期5.6d,在常规蛋白电泳上为α1-球蛋白的最主要成分,其生物学作用在于抑制胰蛋白酶、糜蛋白酶、透明质酸酶、纤溶酶、弹力蛋白酶等,为一种广谱蛋白酶抑制剂。
检测原理
α1抗胰蛋白酶与其相应特异抗体产生免疫复合物的浊度用透射法测定,其浊度高低与血清中α1-AT浓度成正比。
参考值
2~3g/L
临床意义
(1)增高:主要见于组织损伤,炎症,恶性肿瘤,妊娠,病毒性肝炎等。
(2)降低:主要见于遗传性α1-AT缺乏症,由于α1-AT缺乏而引起的肝硬化,支气管扩张,胰腺纤维化等。
对原因不明的肝硬化病人,检测α1-AT可协助诊断。
免疫组织化学方法在肺癌病理诊断中的应用
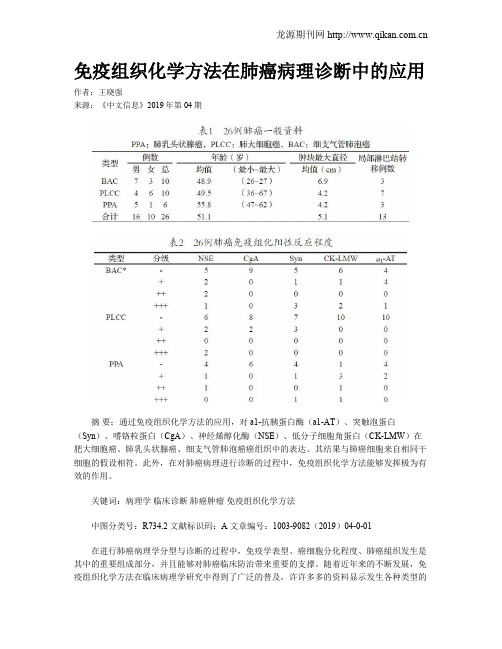
免疫组织化学方法在肺癌病理诊断中的应用作者:王晓强来源:《中文信息》2019年第04期摘要:通过免疫组织化学方法的应用,对a1-抗胰蛋白酶(a1-AT)、突触泡蛋白(Syn)、嗜铬粒蛋白(CgA)、神经烯醇化酶(NSE)、低分子细胞角蛋白(CK-LMW)在肥大细胞癌、肺乳头状腺癌、细支气管肺泡癌癌组织中的表达。
其结果与肺癌细胞来自相同干细胞的假设相符。
此外,在对肺癌病理进行诊断的过程中,免疫组织化学方法能够发挥极为有效的作用。
关键词:病理学临床诊断肺癌肿瘤免疫组织化学方法中图分类号:R734.2 文献标识码:A 文章编号:1003-9082(2019)04-0-01在进行肺癌病理学分型与诊断的过程中,免疫学表型、癌细胞分化程度、肺癌組织发生是其中的重要组成部分,并且能够对肺癌临床防治带来重要的支撑。
随着近年来的不断发展,免疫组织化学方法在临床病理学研究中得到了广泛的普及,许许多多的资料显示发生各种类型的肺癌组织,有很大可能是因为源自于共同的干细胞,这些干细胞来源于支气管黏膜上皮之中。
细胞在出现癌变的过程中,会产生多向性的分化,进而产生多样化的细胞表型,这为肺癌病理形态学的分型提供了重要的理论支撑。
在实际研究的过程中,可以通过光镜进行细致的观察,细支气管肺泡癌逐渐分化为了大细胞癌,肺乳头状腺癌的柱状癌细胞对a1-抗胰蛋白酶(Alpha 1-antitrypsin,a1-A)进行表达等一系列的现象。
通过对相关医学报道的分析发现,上述现象和肺癌细胞的治疗、诊断、表型、分化和评估预后等各个方面有着怎样的联系,这些仍需要进一步的深入研究。
一、材料与方法1.资料与标本收集吉林省卫生学院结合肺肿瘤国际组织学分类准则,收集了其附属医院2013年、2015年、2016年(下半年)大细胞肺癌和肺腺癌27例,细支气管肺泡癌23例(共50例),挑选出26例,每一例挑选癌组织蜡块2—3块,连续切片8—9张,准备对这些切片进行免疫组化染色。
1Bio-Rad质控品分类介绍_-susan解析
产品特点区分
▪ 液体不定值临床化学控制 品
▪ 60+ 分析项目 ▪ 只有总胆固醇 ▪ 只有总胆红素 ▪ 包括 4 种血清蛋白 ▪ 成本低 ▪ 常规价格
▪ Multiqual
▪ 80+ 分析项目 ▪ 包括 HDL and LDL ▪ 稳定的低摩尔渗透压浓度值 ▪ 总, 直接和新生儿胆红素 ▪ 包括 9 种血清蛋白 ▪ 成本高 ▪ 价格高
阿米卡星(Amikacin)(仅限2、3)
铁蛋白(Ferritin)(仅限2)
铜蓝蛋白(Ceruloplasmin)(仅限2、3)
肌酸激酶同工酶CK-MB(CK-MB Isoenzyme)(仅限2)
载脂蛋白A-1(Apolipoprotein A-1)(仅限2、3)
甲胎蛋白(AFP)(仅限3)
载脂蛋白B(Apolipoprotein B)(仅限2、3)
效期和开瓶后稳定性的差异
产品
产品形式
691/692
液体
694/695/696/697 液体 /698/699
C-310-5/C-315- 干粉 5/731/732/C320-10/C-325-10
水平 2水平 3水平
2水平
效期 约2年 约3年
约3年
开瓶后稳定性 15天 14天
7天或30天
项目上的差异
Bio-Rad质控品 分类介绍
By Susan Wu (QSD Product Specialist)
血清临床化学控制品产品线
Multiqual 液体定值与不定值多项目控制品 Liquichek 液体不定值临床化学控制品 Lyphochek 冻干不定值临床化学控制品 Lyphochek 冻干定值临床化学控制品 Liquichek 脂类控制品 Liquichek 儿科控制品
病理学-呼吸系统疾病
pneumococcus
病变和临床表现
按其发展过程分四期:
1、充血水肿期: Stage of congestion
大体:肿胀、暗红、重量↑
镜下:肺泡壁充血
肺泡腔内有水肿液── 症状:
炎细胞
体征:
3.其他肺气肿:◆不规则型肺气肿 也称瘢 痕旁肺气肿;◆ 代偿性肺气肿;◆老年性 肺气肿
病变与临床
大体: 两侧肺肿胀-----桶状胸:缺氧征:---呼吸 困难、杵状指;听诊;影象检查;
镜下:肺泡扩张;肺大泡→自发性气胸 肺泡壁变窄 肺泡血管床↓ →肺功能障碍 肺心病
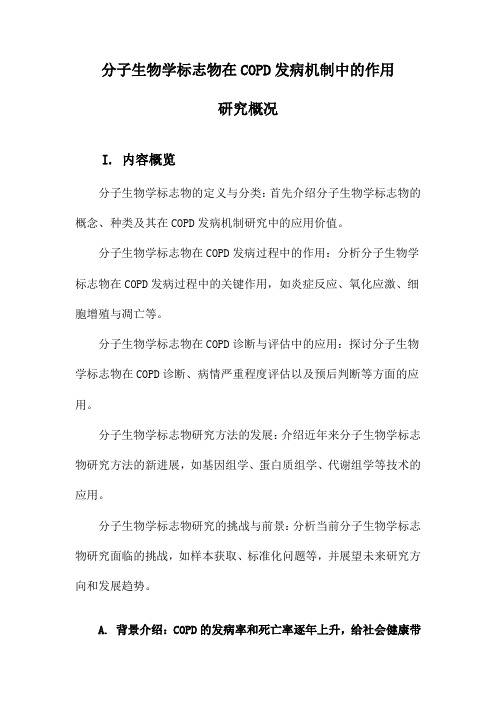
• 病理变化
Panacinar Emphysema. а1- antitrypsin deficiency. The lower lobe
肺炎
Pneumonia
概念:肺的急性渗出性炎症。 呼吸系统的常见病,多发病。
肺炎分类: 1.按病因分类:
(1)感染性: 细菌性、病毒性、支原体性、 真菌性和寄生虫性肺炎 (2)理化性: 放射性、吸入性和类脂性肺炎
(3)变态反应性: 过敏性和风湿性肺炎
2.按病变性质分类:
浆液性、纤维素性、化脓性、出血性、 干酪性、肉芽肿性和机化性肺炎等
临床--刺激性干咳;缺氧 征
2、重者炎症累及肺泡, 出现炎性渗出物及肺组织 坏死。
临床--咳嗽、湿性罗音等
3、透明膜形成---加重缺氧。 见于腺病毒、麻疹病毒、流感 病毒性肺炎。
4、多核巨细胞---见于麻疹病 毒肺炎
5、病毒包含体:诊断意义 腺V、单纯疱疹V、巨细胞 V --- 核内嗜碱性 合胞V --- 浆内嗜酸性 麻疹V --- 核、浆内均可
最新 肝癌转基因小鼠模型研究进展-精品
肝癌转基因小鼠模型研究进展HBV感染动物模型的发展对理解病毒复制、疾病发病机理,尤其是对鉴定HBV感染治疗的候选药物是很重要的。
下面是小编搜集整理的相关内容的论文,欢迎大家阅读参考。
摘要:肝细胞癌是全球范围内的恶性肿瘤,由于其进展迅速、易于复发转移,早期诊断和有效治疗一直是临床难题,对于肝癌的发病机制也亟待进一步阐明。
利用基因工程手段构建的肝癌转基因小鼠模型,为肝癌发病机制研究和药物筛选提供了宝贵的研究材料。
结合经典研究与近年进展,对常用肝癌转基因小鼠模型的构建方法、模型特点、特别是应用研究状况进行了分类介绍,并展望了未来发展的方向。
关键词:肝细胞癌;转基因;小鼠模型引言:1.肝细胞癌(Hepatocellularcarcinoma,HCC)是一种致死率很高的恶性肿瘤,2012年全球范围内发病率位居肿瘤第五位,死亡率高居肿瘤第二位[1]。
严峻的临床诊治形势对HCC发生及转移机制研究提出迫切需求,HCC相关机制的深入阐释对HCC早期诊断、药靶研发及治疗预后具有重要意义。
但HCC致病因素多,病程复杂,涉及通路广,因此研究难度较大,其发生发展机制目前尚不完全清楚。
2.动物模型作为重要的研究手段,在HCC发生发展机制研究中发挥了不可或缺的作用。
化学诱导、原位异位移植及转基因等方法在目前HCC动物模型构建中较为常用。
转基因动物模型与其他常用HCC动物模型相比,在研究特殊基因在HCC发生过程中的作用或不同基因间的相互作用,以及与肝脏特异性致癌物之间的关系中具有独特优势,迅速成为新的研究热点。
本文将对近年来常用的HCC转基因小鼠模型进行分类介绍,并对其在HCC相关机制研究及药物筛选中的应用进行综述,旨为相关领域研究者提供参考。
一、HCC转基因动物模型概况转基因动物模型是通过基因工程方法导入或敲除动物体内特定基因,从而影响动物性状表达并产生稳定遗传修饰的动物模型。
1982年,Gordon等[2]首次利用显微注射法成功构建转基因小鼠,此后转基因动物模型得到快速发展和广泛应用。
临床生物化学检验-第14章 蛋白质和含氮化合物的生物化学检验

()
Alb: 57%-68% 35~52g/L α1: 1.0%-5.7% 1.0 ~ 4.0g/L α2: 4.9%-11.2% 4.0 ~ 8.0g/L β: 7%-13% 5.0~10.0g/L γ: 9.8%-18.2% 6.0~13.0g/L
合成障碍: 急性或慢性肝脏疾病、蛋白质吸收不良等。 (2) 白蛋白丢失过多: ① 肾病综合征、
慢性肾小球肾炎、糖尿病、 SLE; ② 肠道炎症性症候群; ③ 严重烧伤、 渗出性皮炎等。 (3) 白 蛋白分解代谢增加:组织损伤(外科手术或创伤)或炎症(感染性疾病) 。 (4) 白蛋白分布异常: 白蛋白从血管内渗漏入腹腔 ,如肝硬化门静脉高压。 (5) 无白蛋白血症:是极少见的遗传性缺陷。
2. 临床意义: AAT对蛋白酶的抑制作用主要与血循环中M型蛋白的浓度有关。① 急性时相反应和雌 激素增多时 ,AAT增加。② ZZ型、SS型AAT常伴有早年(20~30岁)出现的肺气肿。③ ZZ表现型可引 起肝细胞的损害而致肝硬化。
8
( ) “1-
(“1-acid glycoprotein,AAG)
7
( ) “1-
(“1-antitrypsin, “1 - AT AAT)
血浆中的AAT 主要由肝脏合成,是具有蛋白酶抑制作用的一种急性时相反应蛋白, 占血浆中抑
制蛋白酶活力的90%左右。在醋酸纤维素薄膜电泳中 ,是α1区带的主要组分 (约90%) 。 单核细胞、 肺泡巨噬细胞和上皮细胞也可少量合成AAT ,在局部组织损伤调节中起重要作用。
16
() 需制备特殊的免疫抗血清 ,可采用免疫比浊法、免疫扩散法、化学发光免疫
法、放射免疫法测定 目前临床特定蛋白质多采用免疫比浊法测定 ,包括散射比浊法(需特定蛋白
alpha-1-antitrypsin凝血

alpha-1-antitrypsin凝血
alpha-1-antitrypsin(AAT)是一种由肝脏合成的蛋白质,主要作用是抑制蛋白酶的活性。
AAT 可以与多种蛋白酶结合,形成复合物,从而阻止这些蛋白酶对组织的破坏。
AAT 与凝血系统之间的关系较为复杂。
一方面,AAT 可以抑制凝血酶的活性,从而减缓血液凝固的速度。
另一方面,AAT 也可以与纤维蛋白原结合,促进纤维蛋白的形成,从而加速血液凝固的过程。
在一些疾病状态下,AAT 的水平可能会升高或降低,从而影响凝血系统的功能。
例如,在肝硬化等肝脏疾病中,AAT 的合成减少,导致其水平降低,从而增加了出血的风险。
相反,在一些炎症性疾病中,AAT 的水平可能会升高,从而抑制凝血酶的活性,增加了血栓形成的风险。
AAT 与凝血系统之间的关系是复杂的,需要根据具体情况进行评估和处理。
在临床实践中,医生可能会通过检测AAT 的水平来评估患者的凝血状态,并根据需要进行相应的治疗。
分子生物学标志物在COPD发病机制中的作用研究概况
分子生物学标志物在COPD发病机制中的作用研究概况I. 内容概览分子生物学标志物的定义与分类:首先介绍分子生物学标志物的概念、种类及其在COPD发病机制研究中的应用价值。
分子生物学标志物在COPD发病过程中的作用:分析分子生物学标志物在COPD发病过程中的关键作用,如炎症反应、氧化应激、细胞增殖与凋亡等。
分子生物学标志物在COPD诊断与评估中的应用:探讨分子生物学标志物在COPD诊断、病情严重程度评估以及预后判断等方面的应用。
分子生物学标志物研究方法的发展:介绍近年来分子生物学标志物研究方法的新进展,如基因组学、蛋白质组学、代谢组学等技术的应用。
分子生物学标志物研究的挑战与前景:分析当前分子生物学标志物研究面临的挑战,如样本获取、标准化问题等,并展望未来研究方向和发展趋势。
A. 背景介绍:COPD的发病率和死亡率逐年上升,给社会健康带来了严重威胁随着工业化进程的加快和环境污染的加剧,全球范围内COPD(慢性阻塞性肺疾病)的发病率和死亡率呈逐年上升趋势。
据世界卫生组织(WHO)统计数据显示,全球每年约有600万人死于COPD,占总死亡人数的10。
在中国COPD已成为第四大死因,仅次于心血管病、癌症和糖尿病。
COPD不仅对患者本人造成严重的身体和心理负担,还对家庭和社会产生巨大的经济和人力资源压力。
COPD的主要病理生理特征是气道炎症、黏液过度分泌和支气管收缩。
这些病变导致气道狭窄和气体交换受限,最终引发呼吸衰竭。
目前COPD的发病机制尚不完全清楚,但已有许多研究表明,炎症反应在COPD的发生和发展中起着关键作用。
因此寻找有效的分子生物学标志物来揭示COPD发病机制具有重要意义。
近年来随着分子生物学技术的不断发展,越来越多的生物标志物被发现并应用于COPD的研究。
这些生物标志物可以作为评估疾病进展、预测治疗效果和改善预后的指标。
然而目前关于分子生物学标志物在COPD发病机制中的具体作用仍需进一步研究。
血浆蛋白质代谢紊乱

编辑ppt
13
(六)α2-巨球蛋白
(α2-macroglobulin,α2-MG 或 AMG)
性质
能与多种离子和分子结合,特别是能 与蛋白水解酶结合而影响这些酶的活 性,可起到有选择地保护某些蛋白酶 活性的作用。
临 意义
低清蛋白血症,尤其是肾病综合征时, α2-MG含量可显著增高,是一种代偿 机制以保持血浆胶体渗透压。
临床 意义
①为急性时相反应的指标
②糖皮质激素增加可引起AAG升高
③营养不良、蛋白严重丢失等情况下
AAG降低
④雌激素使AAG降低
编辑ppt
11
(五)结合珠蛋白(haptoglobin,Hp)
性质
●分子中有α与β链形成α2β2四聚体,由于α1F、 α1S、α2三种等位基因编码形成αβ聚合体,因此 个体之间可有多种遗传表型。
(1)用于贫血的鉴别诊断
低血红素贫血 (缺铁性贫血)
再生障碍性贫血(红 细胞对铁利用障碍)
TRF↑、TIBC↑、铁饱和度↓ TRF↓、TIBC↓、铁饱和度↑
(2)在急性时相反应中含量降低 (3)作为营养状态的一项指标
编辑ppt
17
(九)C-反应蛋白(C-reactive protein,CRP)
性质
编辑ppt
18
三、急性时相反应蛋白
● 急性时相反应蛋白(acute phase proteins,APPs)— —在急性炎症性疾病如手术、创伤、心肌梗死、感染、肿 瘤等情况下,血浆中浓度显著变化的蛋白质。这种现象称 为急性时相反应。
● 急性时相反应是对炎症的一般反应,是机体防御机制的 一个部分,其详尽机制尚未十分清楚。
临床生物化学检验
血浆蛋白质与 含氮化合物的代谢紊乱
肝病常用英文

肝病常用英文【原创】一起学习肝病专业英语词汇肝硬化并发症:The complications of liver cirrhosis核苷类似物:Nucleoside analoguesNucleoside analogs乙肝肝硬化:Hepatitis B cirrhosis肾功能:renal function肾小球滤过率(GFR,glomerular filtration rate)指南:guide 亚肝会指南 APASL guide慢加急性肝衰竭:Acute-On-Chronic Liver Failure长期:over a long period of time;long-term Hemochromatosis:血色沉着病Phlebotomy:放血, 静脉切开放血术Copper Chelator:铜螯合剂Penicillamine:青霉胺Alpha-1 antitrypsin deficiencyalpha-1:抗胰蛋白酶缺陷症Ribavirin:三(氮)唑核苷,病毒唑(抗病毒药) Deferoxamine:去铁胺Pruritus:搔痒症Osteoprosis:骨质疏松症Scleroderma:硬皮病gallbladder distention 胆胀hypochondriac pain[disease] 胁痛[病] hepatic insufficiency肝衰竭hepatic lobule肝小叶hepatic tumor 肝瘤hepaptosis 肝下垂heparinization 肝素化heparinocyte 肝素细胞hepatalgia 肝痛hepatargia 肝衰竭hepatatrophia 肝萎缩hepatectomy 肝切除术hepatic amebiasis 肝阿米巴病hepatic bile 肝胆汁hepatic cell 肝细胞hepatic cirrhosis 肝硬变hepatic coma 肝性昏迷hepatic cords 肝细胞索hepatic echography 肝回波描记术hepatic failure 肝衰竭hepatic fetor 肝病性口臭hepatic insufficiency 肝衰竭hepatic lobule 肝小叶hepatic tumor 肝瘤hepatorrhea 肝液溢hepatorrhexis 肝破裂hepatoscintigram 肝闪烁图hepatoscopy 肝检查hepatosis 肝机能障碍hepatosplenography 肝脾x 线照相术hepatosplenomegaly 肝脾大hepatotherapy 肝剂疗法hepatotomy 肝切开术hepatotoxemia 肝性毒血病hepatotoxicity 肝毒性BILIRUBIN - Chemical breakdown product of hemoglobin. Measured in blood specimen by laboratory to assess function of liver.胆红素——血色素化学损坏的产物。
血清蛋白地分类与特征

血清蛋白的分类与特征(以区带电泳为主要技术分类)一、白蛋白(albumin,Alb)由肝实质细胞合成,分子量6、64万,等电4~5、8,半寿期(15~19天,占血浆总蛋白的40%~60。
血浆白蛋白浓度可以受饮食中蛋白质摄入的影响,在一定程度上可以作为个体营养状态的评价指标,有较广泛的载体功能。
正常参考值:35~50g/L。
血浆白蛋白增高较少见,在严重失水时,对监测血浓缩有诊断意义。
低白蛋白血症,可见于以下几种原因:(1)白蛋白合成减低:常见于急性或慢性肝病。
(2)由于营养不良或吸收不良。
(3)遗传性缺陷:无白蛋白血症。
(4)组织损伤(外科手术或创伤)或炎症(感染性疾病)引起的白蛋白分解增加。
(5)白蛋白异常丢失:如肾病综合征、慢性肾小球肾炎、糖尿病、系统性红斑狼疮、溃疡性结肠炎、肿瘤、烧伤所致渗出性皮炎。
(6)白蛋白分布异常:如门脉高压时,大量蛋白质从血管内渗入腹腔。
目前已发现20种以上白蛋白的遗传性变异,这些个体可以不表现病症,在电泳分析时其白蛋白区带可以出现1条或2条宽带,有人称之为双白蛋白血症。
当某些药物大量应用(如青霉素大量注射使血浓度增高时)而与白蛋白结合时,也可使白蛋白出现异常区带。
二、α1区带球蛋白或AAT)就是具有蛋白酶抑制作用的一种急性时相反应蛋1、α1-抗胰蛋白酶(α1-antitrypsin,α1AT白,分子量为5、5万,等电点4、8,半寿期4天,电泳中位与α1区带,就是这一区带的主要组分。
正常参考值:成人780~2000mg/L、新生儿1450~2700mg/L。
低血浆AAT可以发现于胎儿呼吸窘迫综合症,AAT先天缺陷易导致肺气肿与肝硬化。
2、α1-酸性糖蛋白(α1-acid glycoprotein,AAG)早期称之为乳清类粘蛋白,分子量4万,等电点2、7~3、5,半寿期5天,电泳位于α1区带,成人正常参考值:500~1500mg/L。
AAG就是主要的急性时相反应蛋白,在急性炎症时增高,在风湿病、恶性肿瘤及心肌梗死患者亦常增高,在营养不良、严重肝损害等情况下降低。
银屑病血清α1抗胰蛋白酶抑制活力测定

银屑病血清α1抗胰蛋白酶抑制活力测定
陈华;高玉祥
【期刊名称】《蚌埠医学院学报》
【年(卷),期】1993(018)001
【摘要】α_1抗胰蛋白酶(α_1-antitrypsin简称α_1-AT)是一种血浆蛋白酶抑制剂。
自1903年Laurell首先在慢性阻塞性肺病患者血清中发现α_1-AT缺乏后,近来发现α_1-AT缺乏与某些免疫性疾病有一定关系。
本文对银屑病血清α_1抗胰蛋白酶抑制活力进行了初步测定。
【总页数】2页(P55-56)
【作者】陈华;高玉祥
【作者单位】不详;不详
【正文语种】中文
【中图分类】R758.630.2
【相关文献】
1.α1-抗胰蛋白酶的分离纯化及活力测定 [J], 何小维;刘玉;罗志刚
2.肝癌患者血清α1—抗胰蛋白酶抑制活力及其临床意义 [J], 薛侃;刘春日
3.酸稳定蛋白酶抑制剂抑制活力测定:附77例正常人血清和14例良,恶… [J], 何天源;薛侃
4.麻风血清中α<sub>1</sub>抗胰蛋白酶抑制活力的研究 [J], 陈华;高玉祥
5.大学生血清α_1-抗胰蛋白酶抑制活力与吸烟的关系 [J], 薛侃;朱光能;马栋柱;丁昌玉
因版权原因,仅展示原文概要,查看原文内容请购买。
抗胰蛋白酶缺乏症疾病详解

疾病名:α1-抗胰蛋白酶缺乏症英文名:α1-antitrypsin deficiency 缩写:别名:疾病代码:ICD:K86.8概述:α1-抗胰蛋白酶缺乏症(α1-antitrypsin deficiency)是以婴儿期出现胆汁淤积性黄疸、进行性肝功能损害和青年期后出现肺气肿为主要临床表现的一种常染色体隐性遗传性疾病。
常有家族发病史。
流行病学:α1-抗胰蛋白酶缺乏症最初(1963)见于成人慢性阻塞性肺疾患。
Sharp 等(1969)报道了来自6 个不同亲缘家庭内的 10 例小儿肝硬化,经实验室检查证明均伴α1-抗胰蛋白酶(α1-AT)缺乏,从此α1-AT 缺乏与小儿肝病的关系引起注意,病例报道陆续增多。
根据遗传学研究,本症有不同的表型。
PiZZ 核型的发病率为1/4000~1/2000,在新生儿肝炎中PiZZ 大约占20%。
病因:本症为常染色体隐性遗传性疾病。
α1-AT 是一种多肽糖蛋白,分子量为5.2 万,在肝细胞中合成、分泌并释放至血清中。
维持血清正常水平。
其正常血清浓度为1.5~2.5g/L。
新生儿偏高为2.7g/L。
它是血清α1-球蛋白的主要组成部分,约占α1球蛋白的 80%。
此酶属于蛋白酶抑制系统(protease inhibitor system,Pi 系统)。
它能抑制胰蛋白酶(trypsin),纤维蛋白溶酶(plasmin)、凝血酶 (thrombin) 、糜蛋白酶(chymotrypsin)、嗜中性白细胞弹性硬蛋白酶(neutrophilelastase),以及细菌死亡后所释放出的蛋白溶解酶等。
在炎症、组织坏死或损伤时,血清浓度可代偿增高2~4 倍,用以清除过多的由各类细胞和细菌所释放的蛋白溶解酶,以保护正常细胞不受此类蛋白溶解酶的损害。
目前了解Pi 系统至少有33 个等位基因型,M 是最常见的基因型,正常人群中以PiMM 型最多见,在美国大约95%的人是PiMM 表现型。
其血清α1-AT 含量基本正常。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Kaplan: Clinical Chemistry, 5th EditionClinical References - Methods of Analysisα1-AntitrypsinJohn Beilby iNames:α1-Antitrypsin, α1-protease inhibitorClinical significance: α1-Antitrypsin deficiency associated with lung and liver disease Molecular mass: 52,000 DChemical class:GlycoproteinMost common allelic types:PiM, PiS, PiZRefer to Chapter 52, Diseases of Genetic Origin, in the 5th edition of Clinical Chemistry: Theory, Analysis, Correlation.Students’ Quick Hyperlink Review•Principles of analysis and current usage•Reference and preferred methods•Specimen•Interferences•Alpha 1-antitrypsin reference intervals•Interpretation•Alpha 1-antitrypsin performance goals•References•Alpha 1-antitrypsin methods tablePrinciples of Analysis and Current UsageThe clinical importance of the measurement of α1-antitrypsin serum levels is to detect people with deficient states. Severe deficiency (OMIM #107400) is clinically under-recognized [1,2] and is associated with a substantially increased risk for the development of pulmonary emphysema by the 3rd and 4th decades of life. It is also associated with the risk of hepatic disease, cutaneous panniculitis, arterial aneurysm, bronchiectasis, and renal disease [3]. α1-Antitrypsin is responsible for approximately 90% of the trypsin-inhibitory capacity of serum [4,5]. It is a member of the serine protease inhibitor or serpin superfamily [6] and is also knowni Alpha1-antitrypsinPrevious and current authors of this method: First edition: Not doneMethods edition: Gayle JacksonSecond edition: Not updatedThird edition: Steven C. Kazmierczak Fourth edition: Gayle JacksonFifth edition: John Beilbyas α1-protease inhibitor because of its ability to inhibit a broad range of protease enzymes, including trypsin, chymotrypsin, pancreatic elastase, neutral proteases of polymorphonuclear leukocytes and macrophages, and a number of other enzymes [7]. It is a globular glycoprotein that is found in the α1 region of an agarose electrophoresis pattern at pH 8.6. It has a molecular mass of 52 kDa and consists of a 418 amino acid single polypeptide chain with four carbohydrate side chains. α1-Antitrypsin is found in serum and in a number of body fluids such as saliva, tears, lymph, semen, cervical mucus, synovial fluid, and human milk [7]. The half-life of exogenous α1-antitrypsin in serum is approximately a week, with catabolism taking place in the liver.Quantitationα1-Antitrypsin concentrations in serum are measured by immunochemical techniques. In the past, electro-immunodiffusion and radial immunodiffusion techniques were used. Today, automated immunoturbidimetric and immunonephelometric methods are widely used in laboratories. These quantitative methods determine α1-antitrypsin concentrations in humanserum or plasma by measuring the absorbance change due to light scattering caused by insolu complexes that form between anti-αble n concentration. 1-antitrypsin antibodies and α1-antitrypsin in the sample. The amount of light scattering is dependent upon the α1-antitrypsin concentration in the sample and can be quantified by comparison with calibrators of known α1-antitrypsiSerum ElectrophoresisOccasionally, α1-antitrypsin deficiency can be detected by close examination of the α1-globulin band on serum electrophoresis gels. Since α1-antitrypsin composes approximately 90% of the α1-globulin band, a severe deficiency results in the almost complete absence of α1-globulins. It should be noted that the densitometer scan might give a normal value for the α1-globulins, even though visual inspection clearly shows an absence of the band. Other α1-proteins such as α1-lipoprotein may stain to give a diffuse background, thus accounting for the discrepancy between the visual inspection and the scan results.Phenotypingα1-Antitrypsin deficiency is inherited as an autosomal co-dominant disorder, with more than 100 alleles identified [8]. The 12.2 kb gene is located on the long arm of chromosome 14 (14q31-32.3) and consists of seven exons and six introns. Different phenotypes are classified by a coding system in which the inherited alleles are usually letters that denote the migration of the molecule in an isoelectric pH gradient from A (for anodal variants) to Z (for slower migrating variants). The MM phenotype indicates individuals who are homozygous for the normal allele, and ZZ indicates that they are homozygous for the Z allele. The Z variant consists of a glutamine substitution for a lysine residue at codon 342, causing an α1-antitrypsin-deficient state and a dysfunctional protein [9]. The S variant is due to a substitution of valine for glutamine at codon 264, causing intracellular degradation of the protein [10]. Low serum concentrations of α1-antitrypsin must be confirmed by Pi (Protease Inhibitor) phenotyping [11].The gold standard for the identification of α1-antitrypsin variants is the phenotyping of serum samples by isoelectric focusing on thin-layer gels in a pH gradient [11]. This can be done on polyacrylamide or agarose gels. In this procedure, a stable, stationary pH gradient is obtained by the use of ampholytes which are polyamino-polycarboxylic acids. Since α1-antitrypsin proteinshave isoelectric points in the pH region from 4.2 to 4.65, ampholines with a pH range of 4 to 5 are used. This technique separates the various isoforms of α1-antitrypsin based on their migration in a pH gradient. Each isoform migrates to the position within the pH gradient at which the overall net charge of the protein is zero. The separated protein bands are visualized by a protein stain such as Coomassie blue R-250 [12]. Acid-starch gel electrophoresis followed by crossed antigen-antibody electrophoresis [13] has been used in the past (Table 1, Meth od 6). Isoelectric focusing is a technically challenging test and requires a highly skilled scientist to perform the test and interpret the results. Samples of known Pi types are not readily available and can only be found by testing many samples. In addition, severe deficiency is relatively uncommon. Screening for heterozygous α1-antitrypsin deficiency or for intermediate deficiencies does not seem worthwhile, because these phenotypes do not correlate statistically to respiratory problems [14].The medically important variants are those associated with α1-antitrypsin deficiency—namely, the S and Z variants and the rare null (non-production) variant. Approximately 6% of people of northern European descent carry the S gene, and 3% to 4% carry the Z variant [15]. GenotypingGenotyping can largely replace the isoelectric focusing technique. The molecular assay is readily automated using real time PCR, and the interpretation is straightforward, unlike the isoelectric focusing method. The PCR assay detects the most common disease-associated alleles, Z and S. An algorithm for quantitation, genotyping, and phenotyping of α1-antitrypsin has been described [16]. In this approach, α1-antitrypsin was quantitated and genotyped when the serum concentrations were less than 70 mg/dL (0.7g/L). If the results were concordant, they were released with an interpretative comment. If the quantitation and genotype results were discrepant, isoelectric focusing was performed, and all results were reported with an interpretative comment. Snyder et al. [16] demonstrated that 2% of all results were discordant. In another study, all samples without an observed S or Z variant and a serum concentration of less than 100 mg/dL (1.0g/L) were phenotyped [17]. Using this technique, Bornhorst et al. [18] identified 6.5% of patients at risk of developing α1-antitrypsin-related symptoms owing to the presence of rare deficiency alleles not detected by the genotyping assay. A variation on this approach was genotyping by direct sequencing all patient samples with α1-antitrypsinconcentrations less than 100 mg/dL (1.0g/L) [18]. This approach identified all deficient alleles and two new null alleles. Genotyping is quick and easy to perform but needs to be complemented by either phenotyping or direct sequencing so that disease associated variants are not missed.Reference and Preferred MethodsThere is no reference method for the determination of serum α1-antitrypsin levels. Automated immunoturbidimetric and immunonephelometric methods are currently used with the immunoturbidimetric group having the best imprecision (see performance goals below). Reference material for serum proteins, CRM 470 was released in 1993 and has resulted in an improvement in between-laboratory variability of serum protein results [19].SpecimenSerum samples are preferred, but plasma samples are acceptable for α1-antitrypsin concentration determination. Samples may be stored at 4°C for up to 7 days prior to testing. For long-term storage or for samples suspected of a severe deficiency of α1-antitrypsin, storage at −70°C is recommended.Serum or plasma samples may be used for phenotyping. Samples with α1-antitrypsin concentrations of 50% of normal or above may be stored on a long-term basis at −70°C. Storage at −20°C is acceptable for 1 or 2 weeks. Unfortunately, samples with severe α1-antitrypsin deficiency cannot prevent normal activation of intrinsic proteolytic enzymes and may become degraded rapidly, even if stored at less than −20°C. Bacterial contamination or improper storage results in altered migration rates of the bands with eventual loss of banding [20]. Samples suspected of a severe deficiency should be phenotyped as soon as possible after collection. InterferencesSome work has been published on assay interferences for α1-antitrypsin concentration determination. However, the results appear to be variable, depending on the technique used and the manufacturer of the instrumentation [21]. To identify the interferences associated with each method, the user should refer to the manufacturer’s kit insert.α1-Antitrypsin Reference IntervalIn 1995, fifteen professional societies and twelve diagnostic companies agreed on a procedure for uniform reporting of protein reference intervals [19]. The α1-antitrypsin reference interval was reported as 90 to 200 mg/dL (0.9 to 2.0g/L) for subjects with the MM genotype. Age- and gender-related differences in reference interval have been reported. Following birth, concentrations fall during the first 6 months but rise to adult concentrations by 1 year of age [22]. Females have higher concentrations than men across all ages [23].InterpretationA number of factors have been reported to increase α1-antitrypsin concentration, including inflammatory disorders, malignancy, trauma, increases in estrogen concentrations with puberty, pregnancy, or the use of the oral contraceptive pill [23]. However, values rarely increase more than fourfold. These factors can cause considerable overlap in measured concentration between mildly and moderately α1-antitrypsin-deficient subjects and concentrations in normal subjects [7].Severe α1-antitrypsin deficiency is a genetic disorder that affects about 1 in 2000 to 5000 individuals [1]. The World Health Organization guidelines recommend screening all patients with chronic obstructive pulmonary disease and adults and children with asthma [24]. Any α1-antitrypsin concentration less than 100 mg/dL (1.0g/L) should be genotyped or phenotyped to detect α1-antitrypsin variants. In the few cases where the genotype does not agree with the α1-antitrypsin concentration, the sample should be further investigated by phenotyping or DNA sequencing. Serum concentrations of α1-antitrypsin less than a protective threshold of 50mg/dL (0.5 g/L) by nephelometry are associated with an increasing risk of emphysema [25].Allelic types that result in deficiencies of serum α1-antitrypsin include PiS (mean plasma concentration, 60% to 70% of normal), PiZ (mean plasma concentration, 10% to 15% of normal), and Pi null [26]. The ANT concentration in severely deficient subjects rises only slightly in response to inflammatory disorders, malignancy, trauma, and increases in estrogen concentration.The prevalence of the various genotypes are approximately MM 91%, MS 6.1%, MZ 2.7%, SS 0.1%, SZ 0.1%, ZZ 0.02% and null-null. The risk of emphysema is 20% to 50% for the SS genotype, 80% to 100% for SZ, and 100% for the null-null genotype [1]. The null alleles do not produce α1-antitrypsin transcript, produce truncated protein, or produce unstable proteins that are essentially completely degraded before secretion. The risk of emphysema is greatly increased-antitrypsin deficiency if they smoke cigarettein a person with a severe αs.1α1-Antitrypsin Performance GoalsSurvey data from the 2007 College of American Pathologists Participant Summary Report show that 73% of laboratories use immunonephelometric techniques, and 27% use immunoturbidimetric techniques. The imprecision of the methods as determined by the coefficient of variation (CV%) at a mean α1-antitrypsin concentration of 53.9 mg/dL (0.54g/L) ranged from 4.3% to 6.7% for immunonephelometric techniques and from 2.6% to 5.8% for immunoturbidimetric techniques.Acceptable performance criteria (CLIA-88) for measurement of α1-antitrypsin require that laboratories be accurate to within ± 3SD of the peer group mean. The intra-individual variation of α1-antitrypsin in blood in healthy adults has been determined to be approximately 5.9%. Desirable specifications for analytical imprecision derived from studies of biological variation indicate an assay imprecision of no greater than 3.0% and a total error of no greater than 9.2% [27]. The immunonephelometric and immunoturbidimetric techniques are both within the desired performance criteria as defined by CLIA-88. However, only one immunoturbidimetric technique is within the analytical imprecision specification if biological variability defines required performance.References1. Stoller JK, Aboussouan LS. Alpha1-antitrypsin deficiency. Lancet 2005; 365: 2225-2236.2. Laurell CB, Eriksson, S. The electrophoretic alpha 1-globulin pattern of serum in alpha 1antitrypsin deficiency. Scand J Clin Lab Invest 1963; 25: 132-140.3. Mulgrew AT, Taggart CC, McElvaney NG. Alpha-1-antitrypsin deficiency: currentconcepts. Lung 2007; 185: 191-201.4. Crystal RG. The alpha 1-antitrypsin gene and its deficiency states. Trends Genet 1989; 5:411-417.5. Lisowska-Myjak B. AAT as a diagnostic tool. Clin Chim Acta 2005; 352: 1-13.6. Potempa J, Korzus E, Travis J. The serpin superfamily of proteinase inhibitors: structure,function, and regulation. J Biol Chem 1994; 269: 15957-15960.7. Morse JO. alpha1-antitrypsin deficiency (first of two parts). N Engl J Med 1978; 299:1045-1048.8. DeMeo DL, Silverman EK. Alpha1-antitrypsin deficiency. 2: genetic aspects of alpha(1)-antitrypsin deficiency: phenotypes and genetic modifiers of emphysema risk. Thorax2004; 59: 259-264.9. Yoshida A, Lieberman J, Gaidulis L, Ewing C. Molecular abnormality of human alpha1-antitrypsin variant (Pi-ZZ) associated with plasma activity deficiency. Proc Natl Acad Sci USA 1976; 73: 1324-1328.10. Owen MC, Carrell RW, Brennan SO. The abnormality of the S variant of human alpha1-antitrypsin. Biochim Biophys Acta 1976; 453: 257-261.11. Stoller JK, Snider GL, Brantly ML, Fallat RJ, Stockley RA, Turino GM et al. [AmericanThoracic Society/European Respiratory Society Statement: Standards for the diagnosisand management of individuals with alpha1-antitrypsin deficiency]. Pneumologie 2005;59: 36-68.12. Kueppers F. Determination of alpha1-antitrypsin phenotypes by isoelectric focusing inpolyacrylamide gels. J Lab Clin Med 1976; 88: 151-155.13. Lieberman J, Gaidulis L, Garoutte B, Mittman C. Identification and characteristics of thecommon alpha 1 -antitrypsin phenotypes. Chest 1972; 62: 557-564.14. Morse JO, Lebowitz MD, Knudson RJ, Burrows B. Relation of protease inhibitorphenotypes to obstructive lung diseases in a community. N Engl J Med 1977; 296: 1190-1194.15. de Serres FJ. Worldwide racial and ethnic distribution of alpha1-antitrypsin deficiency:summary of an analysis of published genetic epidemiologic surveys. Chest 2002; 122:1818-1829.16. Snyder MR, Katzmann JA, Butz ML, Wiley C, Yang P, Dawson DB et al. Diagnosis ofalpha1-antitrypsin deficiency: An algorithm of quantification, genotyping, andphenotyping. Clin Chem 2006; 52: 2236-2242.17. Bornhorst JA, Procter M, Meadows C, Ashwood ER, Mao R. Evaluation of an integrativediagnostic algorithm for the identification of people at risk for alpha1-antitrypsindeficiency. Am J Clin Pathol 2007; 128: 482-490.18. Prins J, van der Meijden BB, Kraaijenhagen RJ, Wielders JP. Inherited ChronicObstructive Pulmonary Disease: New Selective-Sequencing Workup for α1-AntitrypsinDeficiency Identifies two Previously Unidentified Null Alleles. Clin Chem 2008; 54:101-107.19. Dati F, Johnson AM, Whicher JT. The existing interim consensus reference ranges andthe future approach. Clin Chem Lab Med 2001; 39: 1134-1136.20. Ritchie RF, Smith R. Immunofixation. II. Application to typing of alpha1-antitrypsin atacid pH. Clin Chem 1976; 22: 1735-1737.21. Bossuyt X, Blanckaert N. Evaluation of interferences in rate and fixed-timenephelometric assays of specific serum proteins. Clin Chem 1999; 45: 62-67.22. Ward AM, White PA, Wild G. Reference ranges for serum alpha 1-antitrypsin. Arch DisChild 1985; 60: 261-262.23. Ritchie RF, Palomaki GE, Neveux LM, Navolotskaia O, Ledue TB, Craig WY.Reference distributions for the positive acute phase serum proteins, alpha1-acidglycoprotein (orosomucoid), alpha1-antitrypsin, and haptoglobin: a practical, simple, and clinically relevant approach in a large cohort. J Clin Lab Anal 2000; 14: 284-292.24. Alpha 1-antitrypsin deficiency: memorandum from a WHO meeting. Bull World HealthOrgan 1997; 75: 397-415.25. American Thoracic Society/European Respiratory Society Statement: Standards for theDiagnosis and Management of Individuals with Alpha-1 Antitrypsin Deficiency. Am J Respir Crit Care Med 2003; 168: 818-900.26. Eriksson S, Elzouki AN. Alpha 1-antitrypsin deficiency. Baillieres Clin Gastroenterol1998; 12: 257-273.27. Ricos C, Alvarez V, Cava F, Garcia-Lario JV, Hernandez A, Jimenez CV et al. Currentdatabases on biological variation: pros, cons and progress. Scand J Clin Lab Invest 1999;59: 491-500.Clinical References - Methods of Analysis 10-8α1-Antitrypsin: Methods Summary TableMethod 1: Electrophoresis; quantitative; estimation of α1-globulins by physical separation Principle of analysis: Proteins separate based on class (albumin, gamma globulins)Comments: Serum; good screen for severe α1-antitrypsin deficiency. The α1-globulinband is absent on the electrophoretogram.Method 2: Electroimmunodiffusion (EID); quantitative; quantitation by size ofimmunoprecipitate in gelPrinciple of analysis: Electrophoresis of α1-antitrypsin into antibody-containing agarose gel; height of gel pattern (rocket) proportional to α1-antitrypsin concentrationComments: Serum; kits not available commercially; mainly of historical interest Method 3: Radial immunodiffusion; quantitative; quantitation by immunoprecipitate in gel Principle of analysis:α1-Antitrypsin diffuses into gel containing antibody, forming aring-shaped immunoprecipitate; diameter of ring proportional to concentrationComments: Serum; commercial plates readily available, not widely used in diagnosticlaboratoriesMethod 4: Nephelometry or immunoturbidimetry; quantitative; quantitation byimmunoprecipitate in solutionPrinciple of analysis: Reaction of α1-antitrypsin with its specific antibody results inimmunoprecipitate, which has light-scattering properties; amount of light scatterproportional to α1- antitrypsin concentrationComments: Serum; commercial kits readily availableMethod 5: Electrophoresis of serum on acid starch gel, followed by antigen-antibody crossed electrophoresis; phenotyping; physical separation of α1-antitrypsin variants followed by immunoprecipitin reaction in agarosePrinciple of analysis: Two-step procedure:1. Separation of α1-antitrypsin variants on acid-starch gel by electrophoresis2. A second electrophoresis causes the separated variants to migrateperpendicularly to the first separation into agarose containing antibody to α1-antitrypsin;precipitin peaks form; the second electrophoresis is necessary for separation of the Z and S variantsComments: Serum; original, standard method for phenotyping; time consuming (1½days) and technically difficult; mainly of historical interestMethod 6: Isoelectric focusing; separation of α1-antitrypsin variants on agarose or polyacrylamide gel based on surface-property chargePrinciple of analysis:α1-antitrypsin variants are electrophoresed on polyacrylamide or agarose gels containing ampholines with a pH range of 4 to 5. The variants migrate under the electric field until they reach a pH equal to their isoelectric point.Method 7: Genotyping for the separation of α1-antitrypsin variantsPrinciple of analysis: DNA extracted from whole blood is subject to real-time PCRamplifying the S and Z alleles in separate tubes. The different primer design anddetection probes have been described in several published articles [16, 17].。